Institutions And Organizations: A Process View Trish Reay
https://ebookmass.com/product/institutions-and-organizations-aprocess-view-trish-reay/
ebookmass.com
Countries and Concepts Politics, Geography, Culture 12th Edition Michael G. Roskin
https://ebookmass.com/product/countries-and-concepts-politicsgeography-culture-12th-edition-michael-g-roskin/
ebookmass.com
Numbers and Narratives in Bangladesh's Economic Development 1st Edition Rashed A. M. Titumir
https://ebookmass.com/product/numbers-and-narratives-in-bangladeshseconomic-development-1st-edition-rashed-a-m-titumir/
ebookmass.com
I Kissed Shara Wheeler Casey Mcquiston
https://ebookmass.com/product/i-kissed-shara-wheeler-casey-mcquiston/
ebookmass.com
4 Bikers for the Doctor: An Age Gap Enemies to Lovers MC Reverse Harem Romance (Twisted Reapers MC-Series Book 1) Raven Blaire
https://ebookmass.com/product/4-bikers-for-the-doctor-an-age-gapenemies-to-lovers-mc-reverse-harem-romance-twisted-reapers-mc-seriesbook-1-raven-blaire/
ebookmass.com
Hazzard’s Geriatric Medicine and Gerontology, Eighth
Edition Jeffrey B. Halter
https://ebookmass.com/product/hazzards-geriatric-medicine-andgerontology-eighth-edition-jeffrey-b-halter/
ebookmass.com
Busam: Dermatopathology, 2e 9780323261913
Folpe and Inwards: Bone and Soft Tissue Pathology 9780443066887
Hsi: Hematopathology, 2e 9781437726060
Iacobuzio-Donahue and Montgomery: Gastrointestinal and Liver Pathology, 2e 9781437709254
Marchevsky, Abdul-Karim, and Balzer: Intraoperative Consultation 9781455748235
Nucci and Oliva: Gynecologic Pathology 9780443069208
O’Malley, Pinder, and Mulligan: Breast Pathology, 2e 9781437717570
Prayson: Neuropathology, 2e 9781437709490
Procop and Pritt: Pathology of Infectious Diseases 9781437707625
Thompson: Head and Neck Pathology, 2e 9781437726077
Zhou and Magi-Galluzzi: Genitourinary Pathology, 2e 9780323188272
To my teachers and mentors who inspired me, our trainees who constantly challenge and question, and my family who makes it all worthwhile.
Rebecca L. King, MD
Assistant Professor of Laboratory Medicine and Pathology Division of Hematopathology
Mayo Clinic
Rochester, Minnesota
Kandice Kottke-Marchant, MD, PhD
Medical Director Hemostasis and Thrombosis Department of Laboratory Medicine Cleveland Clinic Foundation; Professor of Pathology Cleveland Clinic Lerner College of Medicine Cleveland, Ohio
Paul J. Kurtin, MD
Professor of Laboratory Medicine and Pathology Division of Hematopathology
Mayo Clinic Rochester, Minnesota
Steven J. Kussick, MD, PhD
Director of Hematopathology and Flow Cytometry
PhenoPath Laboratories; Clinical Assistant Professor Department of Laboratory Medicine University of Washington Seattle, Washington
Pei Lin, MD Professor
Department of Hematopathology University of Texas–MD Anderson Cancer Center Houston, Texas
William R. Macon, MD Professor of Laboratory Medicine and Pathology Division of Hematopathology Mayo Clinic Rochester, Minnesota
Sara A. Monaghan, MD
Associate Professor Department of Pathology University of Pittsburgh School of Medicine Pittsburgh, Pennsylvania
Megan O. Nakashima, MD Department of Laboratory Medicine Cleveland Clinic Cleveland, Ohio
Phuong L. Nguyen, MD
Associate Professor of Laboratory Medicine and Pathology Division of Hematopathology Mayo Clinic Rochester, Minnesota
Robert S. Ohgami, MD, PhD
Assistant Professor, Associate Program Director for Anatomic Pathology Department of Pathology Stanford University Stanford, California
Jennifer L. Oliveira, MD Consultant, Assistant Professor Division of Hematopathology
Mayo Clinic
Rochester, Minnesota
Dennis P. O’Malley, MD
Hematopathologist
Neogenomics
Aliso Viejo, California
Jennifer Lee Picarsic, MD
Assistant Professor
Department of Pathology
University of Pittsburgh School of Medicine; Attending Pathologist Division of Anatomic Pathology
Children’s Hospital of Pittsburgh of UPMC Pittsburgh, Pennsylvania
Leticia Quintanilla-Martinez, MD Professor Institute of Pathology University Hospital, Eberhard-Karls-University Tübingen Tübingen, Germany
Heesun J. Rogers, MD, PhD
Staff Hematopathologist Department of Laboratory Medicine Cleveland Clinic Foundation Cleveland, Ohio
Jonathan W. Said, MD Professor of Pathology Department of Pathology
David Geffen School of Medicine; Vice Chair Research, Chief of Hematopathology Department of Pathology
David Geffen School of Medicine and UCLA Medical Center Los Angeles, California
Graham W. Slack, MD
Pathologist
Department of Pathology and Laboratory Medicine
British Columbia Cancer Agency; Clinical Associate Professor University of British Columbia Vancouver, British Columbia, Canada
Lauren Smith, MD
Associate Professor of Pathology, Section Head, Hematopathology, Director, Hematopathology Fellowship, Director, Medical School Path of Excellence in Ethics University of Michigan Ann Arbor, Michigan
Beenu Thakral, MD
Assistant Professor
Department of Hematopathology
MD Anderson Cancer Center Houston, Texas
David
S. Viswanatha, MD Consultant, Professor
Division of Hematopathology
Mayo Clinic
Rochester, Minnesota
Sa A. Wang, MD
Associate Professor
Department of Hematopathology
MD Anderson Cancer Center
Houston, Texas
James
M. Ziai, MD Research Pathologist Genentech, Inc.
San Francisco, California
Since the first edition of this text in 2007, classifications have evolved to incorporate much more information that has an impact on the diagnosis and therapy of hematologic diseases. I am honored to have been asked to embark on a third edition of this book. New authors have been added and chapters updated and revised. I am pleased to have incorporated a more complete treatment of coagulation that serves to differentiate this book as one that now covers the spectrum of non-neoplastic hematopathology, neoplastic hematopathology, and coagulation. I believe this text will give the reader a solid foundation for learning and practicing hematopathology.
Importantly, it incorporates information and classifications relevant to the long-awaited 2016 WHO update. As in previous editions, I am indebted to the numerous expert contributors who have given of themselves to produce excellent and concise chapters (with a minimal amount of nagging from me …). They are the true resource and talent for this book, and it has been an honor to work with this group of outstanding pathologists and educators.
Eric D. Hsi, MD
Red Blood Cell/Hemoglobin Disorders*
■ Juehua Gao, MD, PhD ■ Sara A. Monaghan, MD
■ INTRODUCTION
The disorders of red blood cells can be divided into those of decreased red blood cell (RBC) mass (anemias) and those of increased RBC mass (erythrocytoses). Most of this chapter is devoted to various types of anemias, with only a short discussion of erythrocytosis.
From the pathophysiologic standpoint, anemias can be divided into three categories (Box 1.1): anemias of blood loss, anemias of decreased RBC production, and anemias caused by increased RBC destruction (hemolysis). Each of these categories can be subdivided further, as illustrated in Box 1.1 and subsequent sections.
This chapter focuses on commonly encountered conditions. Various rare causes of anemia and some disorders lacking characteristic changes in peripheral blood or bone marrow are omitted.
■ ANEMIAS OF BLOOD LOSS
Blood loss, the most common cause of anemia, can occur as obvious bleeding from trauma, occult bleeding (e.g., gastrointestinal ulcers, uterine fibroids), induced bleeding secondary to surgery, hemodialysis, or repeated diagnostic testing. Blood loss can be acute or chronic. The anemia of acute blood loss, such as that associated with major trauma, is not immediately evident based on complete blood cell count (CBC) parameters because losses consist of whole blood, and the vascular system contracts on the decreased blood volume. However, with intravascular volume repletion, the erythrocytes will be diluted and the degree of RBC and hemoglobin (Hb) loss will be manifest on the CBC. Chronic, low-level blood loss is initially compensated by increased marrow RBC production; therefore no anemia will
*We gratefully acknowledge the contribution of Steven H. Kroft, MD, who co-authored this chapter in previous editions.
be present, although reticulocytosis may be evident. With prolonged blood loss, body iron stores become depleted, the iron-deficient marrow is no longer able to compensate, and iron deficiency anemia (IDA) develops. Thus the anemia of chronic blood loss is essentially IDA (see the following section).
■ ANEMIAS OF DECREASED RED BLOOD CELL PRODUCTION
Anemias of decreased red blood cell production can be divided into those due to ineffective erythropoiesis and those due to a decrease in effective RBC production.
INEFFECTIVE ERYTHROPOIESIS
Anemias of ineffective erythropoiesis are characterized in general by a failure of the marrow to produce adequate mature erythrocytes, despite erythroid hyperplasia in the marrow, and often demonstrate morphologic abnormalities in erythroid precursors, mature RBCs, or both. The defect may be primarily one of nuclear maturation (megaloblastic anemia) or cytoplasmic maturation (iron deficiency). Myelodysplastic syndromes, although often characterized by ineffective erythropoiesis, are discussed in Chapter 18
MEGALOBLASTIC ANEMIA
The megaloblastic anemias are macrocytic anemias associated with characteristic morphologic features of hematopoietic cells. Cytopenias are due to impaired deoxyribonucleic acid (DNA) synthesis, which leads to abnormal nuclear maturation of hematopoietic precursors and ineffective hematopoiesis. The major causes of megaloblastic anemia are folate deficiency and cobalamin (Cbl; vitamin B12) deficiency. Folate in the form of tetrahydrofolate (THF) is a transporter of 1-carbon units, used for synthesis of purines, thymidine, and methionine
Box 1.1 Classification of Red Blood Cell Disorders
Anemias
Anemias of blood loss
Acute Chronic
Anemias of decreased red blood cell production
Ineffective erythropoiesis
Megaloblastic anemia
Iron deficiency
Myelodysplastic syndromes
Sideroblastic anemia
Congenital dyserythropoietic anemia
Decreased effective erythropoiesis
Stem cell defects
Marrow replacement processes
Anemia of chronic kidney disease
Anemia of chronic disease
Hemolytic anemias
Intrinsic red cell defects
Hemoglobin disorders
Structural hemoglobin disorders
Sickling diseases
Hemoglobin C disease
Thalassemias
Red cell membrane disorders
Hereditary spherocytosis
Hereditary elliptocytosis
Hereditary pyropoikilocytosis
Red cell enzyme disorders
Glucose-6-phosphate dehydrogenase deficiency
Paroxysmal nocturnal hemoglobinuria
Extrinsic red cell defects
Autoimmune hemolytic anemia
Warm
Cold
Microangiopathic hemolytic anemia
Parasitic hemolysis
Malaria
Babesia
Erythrocytosis
Relative erythrocytosis (decreased plasma volume)
Absolute erythrocytosis (polycythemia)
Primary
Polycythemia vera
Primary familial polycythemia
Secondary
Chronic hypoxia
Cardiac disorders
Pulmonary disorders
Sleep apnea
High-altitude residence
Hemoglobin abnormalities
High-oxygen-affinity hemoglobins
Increased carboxyhemoglobin (smokers)
Aberrant erythropoietin production by tumors
Other rare congenital causes of secondary polycythemia (e.g., Chuvash polycythemia)
(Fig. 1.1). Cbl is a required intermediate in an intracytoplasmic reaction that converts methyltetrahydrofolate, the main form of folate transported in plasma and taken up by cells, into THF while transferring the methyl group to homocysteine to generate methionine. Therefore either folate or Cbl deficiency impairs thymidine and methionine synthesis. Cbl also serves as a cofactor for intramitochondrial conversion of methylmalonyl-coenzyme A to succinyl-coenzyme A (not illustrated).
Because Cbl is produced in nature only by microorganisms, humans must obtain it from their diet. Food sources include red meat, seafood, and dairy products. After ingestion, Cbl is released from food in the stomach in the presence of pepsin and gastric acid and then binds to haptocorrins (R-proteins) secreted in saliva. However, in the alkaline milieu of duodenum, haptocorrins are degraded by pancreatic enzymes, permitting Cbl to bind to intrinsic factor secreted by gastric parietal cells. Intrinsic factor–Cbl binds to receptors specific for this complex on ileal enterocytes and is absorbed. A small proportion of Cbl can also passively diffuse through gastrointestinal mucosa. A fraction of Cbl is bound to the transporter protein, transcobalamin II (TC II), in the plasma and is the biologically active component available for receptormediated cellular uptake; however, a larger proportion of plasma Cbl is bound to haptocorrins. In summary, the Cbl absorption depends on adequate dietary intake, gastric acid and pepsin, pancreatic proteases, gastric-derived intrinsic factor, and ileal receptors for intrinsic factor–Cbl complex. Disruption of any factor along this pathway may lead to Cbl deficiency.
The body stores a large amount of Cbl; therefore it may take several years for deficiency to develop, even with the onset of severe dietary insufficiency or malabsorption. Cbl deficiency is most often caused by malabsorption. Autoimmune gastritis resulting in a lack of intrinsic factor (i.e., pernicious anemia) is a common cause, but malabsorption of Cbl may also be due to other gastric disease (e.g., atrophic gastritis, Helicobacter pylori infection), ileal disease (e.g., inflammatory bowel disease, tropical sprue), postsurgical malabsorption, pancreatic insufficiency, drugs (e.g., proton pump inhibitors, histamine H2–receptor agonists, biguanides), chronic alcoholism, and competition for dietary Cbl (e.g., intestinal bacterial overgrowth, fish tapeworm). Overt Cbl deficiency is rarely due to isolated dietary insufficiency, but a devastating exception to this occurs among exclusively breast-fed infants of mothers who have subclinical Cbl insufficiency that may be related to a vegan diet or occult malabsorption. These infants have increased risk for neural tube defects including spina bifida and anencephaly. In rare cases, Cbl deficiency can be caused by congenital deficiency of TC II.
In contrast to Cbl, the amount of folate body stores is sufficient for only about 4 months, and, thus folate deficiency is more often related to a poor diet. Important dietary sources for folate include leafy vegetables, fruit, cereals, and fortified flour and grains. Other causes of folate deficiency are increased demand (e.g., pregnancy, prematurity, chronic hemolytic anemia, severe exfoliative dermatitis, leukemias), loss due
MEGALOBLASTIC ANEMIA—FACT SHEET
Definition
■ Macrocytic anemia due to folate deficiency, cobalamin deficiency, and other causes, resulting in impaired DNA synthesis, abnormal nuclear maturation, and ineffective hematopoiesis
Incidence and Location
■ Folate deficiency is rare in countries with mandatory food fortification
■ Dietary cobalamin deficiency is rare, except among vegans and populations with low intake of animal-source foods
Morbidity and Mortality
■ Increased risk of fetal neural tube defects in folate/Cbl-deficient pregnancy
■ Peripheral neuropathy, subacute combined degeneration of the spinal cord, and cognitive abnormalities that may be only partially reversible (cobalamin deficiency)
■ Increased risk of gastric adenocarcinoma and carcinoid tumor (patients with pernicious anemia)
Prevalence
■ Prevalence estimates based on low red blood cell (<140 ng/mL) and serum (<3 ng/mL) folate levels among women of childbearing age in the United States is 4.5% and 0.3%,
respectively (2005–2006 National Health and Nutrition Examination Survey)
■ Increased incidence of cobalamin deficiency in breast-fed infants and young children among populations at risk of dietary insufficiency (strict vegans and developing countries)
■ Prevalence of cobalamin deficiency owing to malabsorption increases with age
Clinical Features
■ Gradual onset of macrocytic anemia
■ Evidence of hemolysis (jaundice, elevated lactate dehydrogenase, elevated total bilirubin, low haptoglobin)
■ Atrophic glossitis
■ Neuropsychiatric effects (cobalamin deficiency)
– Paresthesias
– Loss of position and vibration sense
– Ataxia
– Cognitive impairment (impaired memory, dementia)
– Psychosis (rare)
Prognosis and Therapy
■ Treatment of the underlying cause of the deficiency
■ Intramuscular injection (or large oral doses) of vitamin B12
■ Oral folate supplementation (parenteral administration needed in some cases)
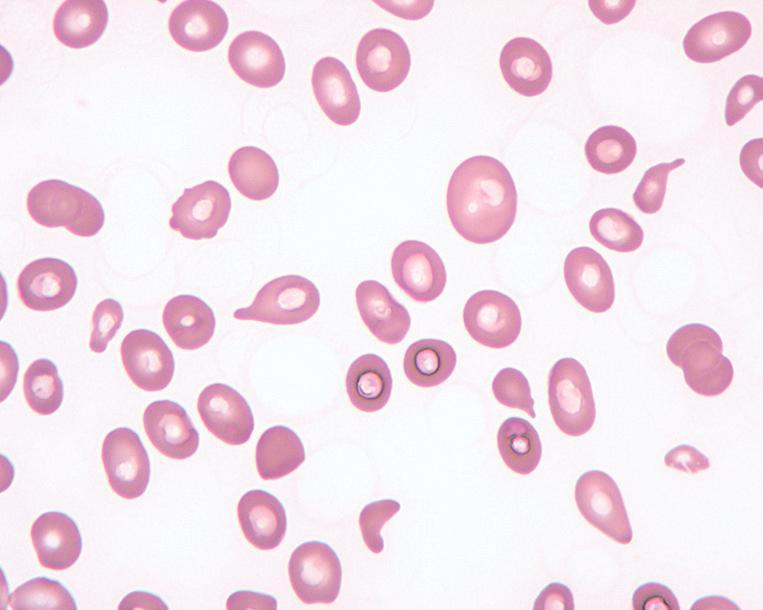
Megaloblastic anemia, peripheral blood findings. This blood smear from a patient with severe megaloblastic anemia demonstrates prominent anisopoikilocytosis, including large oval cells (oval macrocytes), microcytes, and teardrop cells.
FIG. 1.2