Due to the unique page numbering scheme of this book, the electronic pagination of the eBook does not match the pagination of the printed version. To navigate the text, please use the electronic Table of Contents that appears alongside the eBook or the Search function.
For citation purposes, use the page numbers that appear in the text.
Any screen. Any time. Anywhere.
Activate the eBook version of this title at no additional charge.
Elsevier eBooks for Practicing Clinicians gives you the power to browse and search content, view enhanced images, highlight and take notes—both online and offline.
Unlock your eBook today.
1. Visit expertconsult.inkling.com/redeem
2. Scratch box below to reveal your code
3. Type code into “Enter Code” box
4. Click “Redeem”
5. Log in or Sign up
6. Go to “My Library” It’s that easy!
Place Peel Off Sticker Here
For technical assistance: email expertconsult.help@elsevier.com call 1-800-401-9962 (inside the US) call +1-314-447-8300 (outside the US)
GOLDSMITH’S
Assisted Ventilation of the Neonate
An Evidence-Based Approach to Newborn Respiratory Care
This page intentionally left blank
GOLDSMITH’S
Assisted Ventilation of the Neonate
An Evidence-Based Approach to Newborn Respiratory Care
MARTIN KESZLER, MD, FAAP
Professor of Pediatrics
Warren Alpert Medical School
Brown University
Director of Respiratory Services
Department of Pediatrics
Women and Infants Hospital Providence, Rhode Island
K. SURESH GAUTHAM, MD, DM, MS, FAAP
Chair of Pediatrics and Pediatrician-in-Chief
Nemours Children’s Health System
Professor of Pediatrics
University of Central Florida College of Medicine
Orlando, Florida
Elsevier
1600 John F. Kennedy Blvd.
Ste 1800 Philadelphia, PA 19103-2899
GOLDSMITH’S ASSISTED VENTILATION OF THE NEONATE, SEVENTH EDITION
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions.
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notices
Knowledge and best practice in this field are constantly changing. As new research and experience broaden our understanding, changes in research methods, professional practices, or medical treatment may become necessary.
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds or experiments described herein. Because of rapid advances in the medical sciences, in particular, independent verification of diagnoses and drug dosages should be made. To the fullest extent of the law, no responsibility is assumed by Elsevier, authors, editors or contributors for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Previous editions copyrighted 2017, 2011, 2003, 1996, 1988, and 1981.
Library of Congress Control Number: 2021937544
Content Strategist: Sarah Barth
Content Development Manager: Kathryn DeFrancesco
Content Development Specialist: Ann Anderson
Publishing Services Manager: Deepthi Unni
Project Manager: Janish Ashwin Paul
Design Direction: Renee Duenow
Printed in India
Kabir Abubakar, MD
Professor of Clinical Pediatrics Director, Neonatal ECMO Program and Respiratory Services Division of Neonatology, M3400
MedStar Georgetown University Hospital Washington, DC
Namasivayam Ambalavanan, MBBS, MD Professor Department of Pediatrics University of Alabama at Birmingham Birmingham, AL
Robert Mason Arensman, BS, MD
Jayant Radhakrishnan Emeritus Professor of Pediatric Surgery Department of Surgery University of Illinois at Chicago Chicago, IL
Nicolas Bamat, MD, MSCE
Assistant Professor of Pediatrics Perelman School of Medicine at the University of Pennsylvania Division of Neonatology
Children’s Hospital of Philadelphia Philadelphia, PA
Eduardo H. Bancalari, MD Professor
Department of Pediatrics University of Miami Miami, FL
Keith J. Barrington, MB, ChB Professor Department of Paediatrics Université de Montréal Montréal, Québec, Canada
Monika Bhola, MD
Medical Director Professor of Pediatrics Division of Neonatology
Rainbow Babies and Children’s Hospital University Hospitals of Cleveland Cleveland, OH
David M. Biko, MD
Assistant Professor
The Children’s Hospital of Philadelphia Pediatric Radiologist Pennsylvania Hospital
The University of Pennsylvania Health System Philadelphia, PA
Laura D. Brown, MD
Associate Professor
Department of Pediatrics, Section of Neonatology University of Colorado School of Medicine Aurora, CO
Waldemar A. Carlo, MD
Edwin M. Dixon Professor of Pediatrics University of Alabama at Birmingham Codirector Division of Neonatology University of Alabama at Birmingham Birmingham, AL
Robert L. Chatburn, MHHS, RRT-NPS, FAARC
Clinical Research Manager Respiratory Care Cleveland Clinic Professor
Department of Medicine
Lerner College of Medicine of Case Western Reserve University Cleveland, OH
Nelson Claure, MSc, PhD Professor of Pediatrics and Biomedical Engineering Director Neonatal Respiratory Physiology Laboratory Department of Pediatrics, Division of Neonatology University of Miami Miller School of Medicine Miami, FL
Clarice Clemmens, MD
Associate Professor Department of Otolaryngology Medical University of South Carolina Charleston, SC
Christopher E. Colby, MD Professor of Pediatrics Neonatal Medicine – Division Chair Mayo Clinic Rochester, MN
Sherry E. Courtney, MD, MS Professor of Pediatrics University of Arkansas for Medical Sciences Little Rock, AR
Peter G. Davis, MBBS, MD Professor of Neonatology
The Royal Women’s Hospital University of Melbourne Melbourne, Victoria, Australia
Eugene M. Dempsey, FRCPI
Professor
Department of Paediatrics and Child Health
University College Cork
Professor
Irish Centre for Fetal and Neonatal Translational Research (INFANT)
University College Cork Cork, Ireland
Robert M. DiBlasi, RRT-NPS, FAARC
RT Research Manager
Respiratory Therapy
Seattle Children’s Hospital and Research Institute
Seattle, WA
Matthew Drago, MD, MBE
Assistant Professor of Pediatrics
Division of Newborn Medicine
The Icahn School of Medicine at Mount Sinai
New York, NY
Eric C. Eichenwald, MD
Professor of Pediatrics
Perelman School of Medicine
University of Pennsylvania
Chief, Division of Neonatology
Children’s Hospital of Philadelphia Philadelphia, PA
Jonathan M. Fanaroff, MD, JD
Professor of Pediatrics
Case Western Reserve University School of Medicine
Peter H. Grubb, MD Clinical Professor of Pediatrics University of Utah Salt Lake City, UT
Malinda N. Harris, MD Assistant Professor of Pediatrics Knoxville, TN East Tennessee Children’s Hospital
Helmut Hummler, MD, MBA Professor of Pediatrics Ulm University Hagnau, Germany
Erik B. Hysinger, MD, MS Assistant Professor Department of Pediatrics Cincinnati Children’s Hospital Medical Center Cincinnati, OH
Robert M. Insoft, MD, FAAP Professor of Pediatrics
Brown University Alpert Medical School Chief Medical Officer
Women and Infants Hospital Providence, RI
Erik Allen Jensen, MD, MSCE Assistant Professor Department of Pediatrics University of Pennsylvania Attending Neonatologist Children’s Hospital of Philadelphia Philadelphia, PA
Jegen Kandasamy, MBBS, MD Assistant Professor Department of Pediatrics University of Alabama at Birmingham Birmingham, AL
Lakshmi I. Katakam, MD, MPH Associate Professor of Pediatrics Division of Neonatology, Baylor College of Medicine
Medical Director of NICU, Texas Children’s Hospital Houston, Texas
Martin Keszler, MD Professor
Department of Pediatrics
Alpert Medical School of Brown University Director of Respiratory Services
Pediatrics
Women and Infants Hospital Providence, RI
Haresh Kirpalani, BM, MSc
Professor of Neonatology Department of Pediatrics
The Children’s Hospital of Philadelphia Philadelphia, PA
Emeritus Professor Clinical Epidemiology
McMaster University Hamilton, Ontario, Canada
Nathaniel Koo, BS, MD
Assistant Professor of Pediatric Surgery University of Illinois at Chicago Chicago, IL
Satyan Lakshminrusimha, MBBS, MD, FAAP Professor and Dennis and Nancy Marks Chair Department of Pediatrics
Pediatrician-in-Chief
University of California Davis Children’s Hospital Sacramento CA
Krithika Lingappan, MD, MS
Assistant Professor Department of Pediatrics
Baylor College of Medicine Houston, TX
Akhil Maheshwari, MD Professor of Pediatrics
Johns Hopkins University Baltimore, MD
Mark Crawford Mammel, MD Professor of Pediatrics University of Minnesota Minneapolis, MN
Brett J. Manley, MBBS (Hons), FRACP, PhD Neonatologist
Newborn Research
The Royal Women’s Hospital
Associate Professor Department of Obstetrics and Gynecology
The University of Melbourne Honorary Fellow
Murdoch Children’s Research Institute Melbourne, Victoria, Australia
Camilia R. Martin, MD, MS
Associate Director, NICU Department of Neonatology
Beth Israel Deaconess Medical Center
Associate Professor of Pediatrics
Harvard Medical School
Boston, MA
Richard John Martin, MBBS Professor
Department of Pediatrics, Reproductive Biology, and Physiology & Biophysics
Case Western Reserve University School of Medicine
Drusinsky/Fanaroff Professor of Pediatrics
Rainbow Babies & Children’s Hospital
Bobby Mathew, MBBS
Associate Professor of Pediatrics
Division of Neonatology, Department of Pediatrics
Oishei Children’s Hospital Buffalo, NY
Mark R. Mercurio, MD, MA Professor of Pediatrics
Chief, Division of Neonatal-Perinatal Medicine
Director, Program for Biomedical Ethics
Yale University School of Medicine
New Haven, CT
Andrew Mudreac, BS Resident Physician Department of Surgery
New York Presbyterian—Weill Cornell Medicine
New York, NY
Leif D. Nelin, MD Chief
Division of Neonatology Nationwide Children’s Hospital Professor and Chief of Neonatology
The Ohio State University Columbus, OH
Louise S. Owen, MBChB, MRCPCH, FRACP, MD Neonatologist, Newborn Research, Royal Women’s Hospital, Melbourne
Associate Professor, Principal Research Fellow, Department of Obstetrics and Gynaecology, University of Melbourne Research Fellow, Murdoch Children’s Research Institute, Melbourne, Australia
Allison Hope Payne, MD, MS Assistant Professor of Pediatrics/Neonatology
Rainbow Babies and Children’s Hospitals/Case Western Reserve University Cleveland, OH
Jeffrey M. Perlman, MB, ChB Professor of Pediatrics
Weill Cornell New York, NY
Division Chief Newborn Medicine
New York Presbyterian Hospital New York, NY
Joseph Piccione, DO, MS
Pulmonary Director
Center for Pediatric Airway Disorders
The Children’s Hospital of Philadelphia
Associate Professor of Clinical Pediatrics
Division of Pediatric Pulmonary Medicine
University of Pennsylvania School of Medicine
Philadelphia, PA
J. Jane Pillow, BMedSci(Dist), MBBS, FRACP, PhD(Dist)
Professor, NHMRC Leadership Fellow
School of Human Science
University of Western Australia
Lead, Cardiorespiratory Health
Telethon Kids Institute
Associate Editor, Neonatology
School of Human Sciences
Perth, Western Australia, Australia
Richard Alan Polin, BA, MD
Director Division of Neonatology
Department of Pediatrics
Morgan Stanley Children’s Hospital
William T Speck Professor of Pediatrics
Columbia University College of Physicians and Surgeons
Executive Vice Chair Department of Pediatrics
Columbia University
New York, NY
Francesco Raimondi, MD, PhD
Professor of Pediatrics
Neonatal Intensive Care Unit and Regional Transport Program
Università Federico II di Napoli
Naples, Italy
Tonse N.K. Raju, MD, DCH, FAAP Program Officer
Office of the Director
Environmental Influences on Child Health Outcomes (ECHO)
National Institutes of Health
Bethesda, MD,
Adjunct Professor of Pediatrics
Uniformed Services University, Bethesda, MD,
Lawrence Rhein, MD, MPH
Associate Professor
Department of Pediatrics
University of Massachusetts Medical School
Chief, Division of Neonatology
Chair, Department of Pediatrics
UMass Memorial Health
Worcester, MA
Guilherme Sant’Anna, MD, PhD, FRCPC
Professor of Pediatrics
Neonatal Division McGill University Health Center
Associate Member of the Division of Experimental Medicine
McGill University
Montreal, Quebec, Canada
Georg Schmölzer, MD, PhD
Associate Professor
Faculty of Medicine & Dentistry, Department of Pediatrics, Division of Neonatal-Perinatal Care (NICU)
University of Alberta Neonatologist
Northern Alberta Neonatal Program, AHS Director
Centre for the Studies of Asphyxia & Resuscitation
Royal Alexandra Hospital Edmonton, Alberta, Canada
Andreas Schulze, MD
Professor Emeritus of Pediatrics
University of Munich Perinatal Center
Department of Pediatrics Division of Neonatology Munich, Germany
Grant Shafer, MD, MA Neonatologist
Division of Neonatology
Children’s Hospital of Orange County Orange, CA
Assistant Professor of Pediatrics
Division of Neonatology
University of California Irvine School of Medicine Irvine, CA
Wissam Shalish, MD, FRCPC
Assistant Professor Department of Pediatrics Division of Neonatology
McGill University Health Center Montreal, Quebec, Canada
Edward G. Shepherd, MD Chief
Section of Neonatology
Nationwide Children’s Hospital
Associate Professor of Pediatrics
Department of Pediatrics
The Ohio State University College of Medicine Columbus, OH
Billie Lou Short, MD Chief of Neonatology
Children’s National Hospital Professor
Department of Pediatrics
The George Washington University School of Medicine Washington, DC
Thomas L. Sims Jr., MD
Assistant Professor
Department of Surgery
University of Illinois at Chicago Chicago, IL
Nalini Singhal, MBBS, MD, FRCP
Professor of Pediatrics
Alberta Children’s Hospital Cumming School of Medicine
University of Calgary Calgary, Alberta, Canada
Roger F. Soll, MD
H. Wallace Professor of Neonatology Department of Pediatrics University of Vermont Burlington, VT
Professor of Pediatrics Department of Pediatrics, Cumming School of Medicine University of Calgary, Alberta, Canada Medical Director, NICU Foothills Medical Centre, Calgary, Alberta, Canada
Nishant Srinivasan, MD
Assistant Professor of Clinical Pediatrics Associate Program Director Neonatal-Perinatal Fellowship Director for Neonatal Simulation Division of Neonatal-Perinatal Medicine Department of Pediatrics
Children’s Hospital at the University of Illinois (CHUI) Chicago, IL
Raymond C. Stetson, MD
Assistant Professor of Pediatrics
Neonatal Medicine
Mayo Clinic Rochester, MN
Sarah N. Taylor, MD, MSCR
Associate Professor Department of Pediatrics
Yale School of Medicine
New Haven, CT
Colm P. Travers, MD
Assistant Professor Department of Pediatrics University of Alabama at Birmingham Birmingham, AL
Payam Vali, MD
Assistant Professor Department of Pediatrics University of California Davis Sacramento, CA
Anton H. van Kaam, MD, PhD Professor of Neonatology
Emma Children’s Hospital Amsterdam UMC Amsterdam, the Netherlands
Maximo Vento, MD, PhD Professor
Division of Neonatology
University & Polytechnic Hospital La Fe Professor
Neonatal Research Group
Health Research Institute La Fe Valencia, Spain
Michele Walsh, MD, MSEpi Professor
Department of Pediatrics
UH Rainbow Babies & Children’s Hospital Professor
Department of Pediatrics
Case Western Reserve University Cleveland, OH
Gary Weiner, MD
Associate Clinical Professor
Neonatal-Perinatal Medicine
University of Michigan Ann Arbor, MI
Gulgun Yalcinkaya, MD
Assistant Professor of Pediatrics Division of Neonatology
Medical Director of Transitional Care Nursery
UH Rainbow Babies and Children’s Hospital
Case Western University School of Medicine Cleveland, OH
Vivien Yap, MD
Associate Professor of Clinical Pediatrics
Pediatrics
New York Presbyterian–Weill Cornell Medicine New York, NY
Bradley A. Yoder, MD Professor
Department of Pediatrics University of Utah School of Medicine Salt Lake City, UT
Huayan Zhang, MD
Attending Neonatologist Director, The Newborn and Infant Chronic Lung Disease Program Division of Neonatology, Department of Pediatrics Children’s Hospital of Philadelphia Philadelphia, PA
Associate Professor of Clinical Pediatrics University of Pennsylvania Perelman School of Medicine Philadelphia, PA
Chief, Division of Neonatology and Center for Newborn Care Guangzhou Women and Children’s Medical Center Guangzhou, Guangdong, China
FOREWORD
Assisted Ventilation of the Neonate is one of the few textbooks in our subspecialty that I consider iconic. The first edition of this book was published 40 years ago, and at least two generations of trainees and practicing neonatologists have considered it the “bible” of respiratory management of critically ill infants.
As I think back to the beginning of my training in the 1970s, I am amazed how much progress has been made in respiratory support of the newborn infant. The first large case series of “near-terminal” preterm neonates with “hyaline membrane disease” by Papadopoulos and Swyer in 1964 provided a framework for ventilation to reverse acid–base disturbances but was associated with almost 100% mortality. It is noteworthy that Patrick Bouvier Kennedy (President John F. Kennedy’s son) born at 34 weeks’ gestation was treated with hyperbaric oxygen rather than positive-pressure ventilation and is a prime example of the skepticism surrounding ventilation of the newborn infant in the mid-1960s. The problem was twofold. First, there was a general lack of understanding of neonatal respiratory physiology and disease pathophysiology, including the importance of positive end expiratory pressure and surfactant in maintaining alveolar stability. Second, most neonatal intensive care units were using ventilators designed for adults in modes that were never meant for newborns. Beginning in the 1970s, a new generation of ventilators designed for neonates became commercially available. However, those ventilators were still not refined. They did not allow infants to breathe when the ventilator was not cycling (intermittent mandatory ventilation was not available) or were associated with difficult regulation of delivered tidal volumes, resulting in pneumothoraces and chronic lung injury. Since the initial publication of Assisted Ventilation of the Neonate, the mortality rate for infants with respiratory distress syndrome has plummeted. The improvement in mortality is multifactorial but is likely secondary to a variety of clinical advancements (including widespread administration of surfactant), greater use of
noninvasive ventilation strategies, a better understanding of transitional and postnatal physiological disturbances, smarter clinicians, and increasingly sophisticated ventilators. However, increasingly complex ventilators allowing multiple modes of ventilation has increased the opportunity for operator errors because of the number of ventilator decisions clinicians must make. As with every edition of this textbook, the editors and authors provide a clear way forward to take much of the guesswork out of mechanical ventilation.
The seventh edition of this textbook has the subtitle of “an evidence-based approach.” The editors have successfully integrated the “art” of ventilation with current best evidence. As a foundation to those sections, there are in-depth discussions of respiratory physiology and control of breathing, pulmonary function testing, newer radiographic techniques to assess lung pathology, use of oxygen, and delivery room stabilization. Each of the newest strategies for ventilating neonates is presented in great detail along with how to manage infants with diverse respiratory diseases. Finally, the editors have wisely chosen to include chapters on home ventilation, transport, intraoperative management of the neonate, ethical and medical-legal issues, pharmacotherapies, nursing care, and respiratory care in resource-limited setting.
The seventh edition of Goldsmith’s Assisted Ventilation of the Neonate, edited by Martin Keszler and K. Suresh Gautham, is an outstanding compendium of well-written chapters, which not only guides care providers in how to care for neonates with respiratory diseases but also provides the basis for their recommendations. The editors of this book and authors of the chapters are to be congratulated for producing another superb edition.
Richard A. Polin, MD
William T. Speck Professor of Pediatrics
Columbia University, College of Physicians and Surgeons
In 1978, before there were exogenous surfactants, inhaled nitric oxide, high-frequency ventilators, and other modern therapies, a young overly confident neonatologist (JPG) thought that there needed to be a primer on newborn assisted ventilation for physicians, nurses, and respiratory therapists entrusted with treating respiratory failure in fragile neonates. In the preceding decade, ventilation of neonates was undertaken only in major medical centers, and in 1963, the late preterm son of the President of the United States, John F. Kennedy, died of lack of adequate respiratory support. As the first edition of this text was being written, assisted ventilation had become widely available in hundreds of hospitals in the United States and around the world. Even in the early days of this new subspecialty called neonatology, respiratory support was an essential part of neonatal intensive care. However, there was little guidance in standard neonatal textbooks regarding the proper techniques in neonatal ventilatory support. The initial publication was conceived to fill a void and provide a reference to the caretakers in this new and exciting field but was not intended as a “license in assisted ventilation” for the novice. The neonatologist, only 2 years out of his fellowship, recruited his young partner (EHK) and they prevailed upon their former teachers and mentors to write most of the chapters of the text, while they served mostly as organizers in this initial project. The result exceeded their most optimistic expectations in creating a “how to” guide for successful ventilation of the distressed newborn. The first edition, published in 1981, was modeled after the iconic text of Marshall Klaus and Avroy Fanaroff, Care of the High-Risk Neonate, which was the standard clinical reference for practicing neonatal caregivers at the time. Dr. Klaus wrote the foreword, and the first edition of Assisted Ventilation of the Neonate was born.
The preface to the first edition started with a quotation from Dr. Sydney S. Gellis, then considered the Dean of Pediatrics in the United States:
“As far as I am concerned, the whole area of ventilation of infants with respiratory distress syndrome is one of chaos. Claims and counterclaims about the best and least harmful method of ventilating the premature infant make me lightheaded. I can’t wait for the solution or solutions to premature birth, and I look forward to the day when this gadgetry will come to an end and the neonatologists will be retired.”
Year Book of Pediatrics (1977)
After over four decades and seven editions of the text, we are still looking for the solutions to premature birth despite decades of research on how to prevent it, and neonatal respiratory support is still a mainstay of neonatal intensive care. Initially, there were concerns regarding the experience and competence of those managing these new ventilation devices with an unacceptable rate of complications such as bronchopulmonary dysplasia (BPD), pulmonary air leaks (especially with high
frequency ventilation), unplanned extubations, plugged endotracheal tubes, nasal trauma with continuous positive airway pressure (CPAP) devices, and others. In the past 40 plus years, pharmacological, nutritional, technological, and philosophical advances in the care of newborns, especially the extremely premature, have continued to refine the way we manage neonatal respiratory failure. Microprocessor-based machinery, information technology, an emphasis on safety, quality improvement, and evidence-based medicine have affected our practice as they have all of medical care. However, the wide variance in outcomes of this most vulnerable population is striking among even the most sophisticated university-based neonatal intensive care units (NICUs). The Vermont Oxford Network, through their Nightingale data collecting system, reports that in the most advanced NICUs (Type C, n 5 158), BPD secondary to assisted ventilation varied in 2020 from a median of 20.7% in the first quartile to 38% in the third quartile in neonates born under 1500 g or 32 weeks’ gestation. Literature reports of BPD vary even more widely, documenting a reported incidence of 5% to 6% in one institution to as high as 50% to 60% in others. Mere survival is no longer the only goal; the emphasis of neonatal critical care has changed to improving functional outcomes of even the smallest premature infant. While the threshold of viability has been lowered only modestly in the past decade, there have been decreases in morbidities, even at the smallest weights and lowest gestational ages. However, the large institutional variation in morbidities such as BPD, even in the era of widespread administration of antenatal corticosteroid administration to mothers, can no longer be attributed to differences in the populations treated. The uniform application of evidence-based therapies and quality improvement programs has shown significant improvements in outcomes, but unfortunately, not in all centers. We have recognized that much of neonatal lung injury (i.e., ventilator induced lung injury) is due to our ventilatory techniques and occurs predominantly in the most premature infants. Our perception of the ventilator has shifted from that of a lifesaving machine to a tool that can also cause harm—a double-edged sword. However, the causes of this morbidity are multifactorial, and its prevention remains controversial and elusive. This is not a new concept. As early as 1745, Fothergill cautioned regarding the deleterious effects of mechanical ventilation: “Mouth to mouth resuscitation may be better than using a mechanical bellows to inflate the lung because the lungs of one man may bear, without injury, as great a force as those of another can exert, which by the bellows cannot always be determined” (J Philos Trans R Soc, Lond. 1745). Specifically, attempts to decrease the incidence of BPD have concentrated on ventilatory approaches such as earlier and more extensive use of CPAP, noninvasive ventilation, volumetargeted modes, various devices to synchronize ventilator and spontaneous breathing, and adjuncts such as caffeine and vitamin A. Yet, some of these therapies remain unproven in large
clinical trials, and the national incidence of BPD in large databases for very low birth weight infants exceeds 30%. Thus, until there are social, pharmacological, and technical solutions to prematurity, neonatal caregivers will continue to be challenged to provide respiratory support for the smallest premature infants without causing lifelong pulmonary or central nervous system injury.
In this, the seventh edition, the transition to two new editors, Dr. Keszler and Dr. Gautham, has been completed. Martin Keszler, MD, Professor of Pediatrics and Medical Director of Respiratory Care at Brown University, is internationally renowned for his work in neonatal ventilation. Kanekal Suresh Gautham, MD, DM, MS, is the Chairman of Pediatrics and Pediatrician-in-Chief at Nemours Children’s Hospital and a Professor of Pediatrics at the University of Central Florida College of Medicine, Orlando, FL. He is a Deputy Editor of The Joint Commission Journal on Quality and Safety, is a Senior Editor for the Neonatal Review Group of the Cochrane Collaboration, and is regarded as one of the foremost authorities on quality improvement in neonatal care.
Since the sixth edition, new ventilatory devices have been introduced, and support has continued to shift from an invasive to a noninvasive approach, which has resulted in significant improvements in some outcomes, but also new challenges for providers. Recent improvements to ventilatory devices have also not come without cost. The new generation of ventilators has added a new level of complexity as well as expense to neonatal care. While some clinicians may be attracted to the advanced features of new devices, the new technology may pose risks to patients as devices may not be fully understood or misapplied by multiple caretakers at the bedside. More commonly, many of the new ventilator features are infrequently used in clinical practice. Unfortunately, many providers do not use or understand how to apply important adjuncts to care, such as pulmonary graphics. Hopefully, these deficiencies can be addressed by texts such as this.
The seventh edition of Assisted Ventilation of the Neonate has been extensively updated and rewritten, with many new contributors and several new chapters. The text is divided into six sections. The first section covers general principles and concepts and includes chapters on physiologic principles, ethical and medical-legal aspects of respiratory care, and quality and safety. The second section reviews assessment, diagnosis, and
monitoring methods of the newborn in respiratory distress, including chapters on physical assessment, imaging, blood gas monitoring, and pulmonary function and graphics. Essential aspects of respiratory support are covered in the third section with discussions on delivery room management, oxygen therapy, and all types of ventilatory modes and strategies. A new chapter on respiratory gas conditioning has been added to this section. Adjunctive interventions such as pulmonary and nursing care, nutritional support, and pharmacologic therapies are the subjects of the fourth section. The fifth section reviews special situations and outcomes, including chapters on BPD care, surgical and medical considerations of the airway, intraoperative management, and new chapters on persistent pulmonary hypertension and congenital diaphragmatic hernia. Finally, the sixth section reviews complications, transition from hospital to home, pulmonary and neurologic outcomes, care in resource limited settings, and a new final chapter on gaps in knowledge and future directions.
During the four-plus decade and seven-edition life of this text, neonatology has grown and evolved in the nearly 1000 NICUs in the United States. The two young neonatologists, now past-due for retirement, have turned over the leadership of this and future editions of the text to the new editors. We have seen new and unproven therapies come and go, and despite our frustration at not being able to prevent death or morbidity in all our patients, we continue to advocate for evidence-based care and robust clinical trials before the application of new devices and therapies. We hope this text will stimulate its readers to continue to search for better therapies as they use the wisdom of these pages in their clinical practice. We are honored to have Dr. Richard Polin, the American Academy of Pediatrics 2021 Apgar Award winner and editor/author of his own classic text on Fetal and Neonatal Physiology, favor us with the foreword to this edition. And as we wait for the solution(s) to prematurity, we should heed the wisdom of the old Lancet editorial: “The tedious argument about the virtues of respirators not invented over those readily available can be ended, now that it is abundantly clear that the success of such apparatus depends on the skill with which it is used” (Lancet. 1965;2:1227).
Jay P. Goldsmith, MD, FAAP
November 2021
SECTION 1 History, Pulmonary Physiology, and General Considerations
1 Introduction and Historical Aspects,1
Jay P. Goldsmith and Tonse N. K. Raju
2 Physiologic Principles,11
Martin Keszler and Kabir Abubakar
3 Control of Ventilation, 33
Richard J. Martin and Eric C. Eichenwald
4 Ethical Issues in Assisted Ventilation of the Neonate, 39
Matthew Drago and Mark R. Mercurio
5 Evidence-Based Respiratory Care, 47
Krithika Lingappan and K. Suresh Gautham
6 Quality and Safety in Respiratory Care, 56
K. Suresh Gautham and Grant Joseph Dat Chiu Shafer
7 Medical and Legal Aspects of Respiratory Care, 64
Jonathan M. Fanaroff
SECTION 2 Patient Evaluation and Monitoring
8 Physical Examination, 70
Edward G. Shepherd and Leif D. Nelin
9 Imaging: Radiography, Lung Ultrasound, and Other Imaging Modalities, 76
Erik A. Jensen, María V. Fraga, David M. Biko, Francesco Raimondi, and Haresh Kirpalani
10 Blood Gases: Technical Aspects and Interpretation, 94
Colm Travers and Namasivayam Ambalavanan
11 Noninvasive Monitoring of Gas Exchange, 111
Bobby Mathew and Satyan Lakshminrusimha
12 Pulmonary Function and Graphics, 124
Georg Schmölzer, MD, PhD and Helmut Hummler, MD, MBA
13 Airway Evaluation: Bronchoscopy, Laryngoscopy, and Tracheal Aspirates, 144
Clarice Clemmens, Erik B. Hysinger, and Joseph Piccione
SECTION 3 Delivery Room Stabilization, Oxygen Therapy, and Respiratory Support
14 Delivery Room Stabilization and Respiratory Support, 151
Louise S Owen, Gary Weiner, and Peter G Davis
15 Exogenous Surfactant Therapy, 172
K. Suresh Gautham and Roger F. Soll
16 Oxygen Therapy, 185
Maximo Vento
17 Respiratory Gas Conditioning, 196
Andreas Schulze
18 Noninvasive Respiratory Support, 201
Brett J. Manley, Peter G. Davis, Bradley A. Yoder, and Louise S. Owen
19 Overview of Assisted Ventilation, 221
Martin Keszler
20 Basic Modes of Synchronized Ventilation, 232
Martin Keszler and Mark C. Mammel
21 Principles of Lung-Protective Ventilation, 241
Anton H. van Kaam
22 Volume-Targeted Ventilation, 249
Martin Keszler, MD and Kabir Abubakar, MBBS
23 Special Techniques of Respiratory Support, 263
Nelson Claure and Eduardo Bancalari
24 High-Frequency Ventilation, 269
Martin Keszler, J. Jane Pillow, and Sherry E. Courtney
26 Weaning and Extubation From Mechanical Ventilation, 303
Wissam Shalish, Guilherme Sant’Anna, and Martin Keszler
27 Common Devices Used for Mechanical Ventilation, 315
Robert L. Chatburn and Waldemar A. Carlo
28 Extracorporeal Membrane Oxygenation, 351
Robert M. Arensman, Billie Lou Short, Nathaniel Koo, and Andrew Mudreac
SECTION 4 Bedside Care, Nutritional and Pharmacologic Support
29 Respiratory Care of the Newborn, 363
Robert DiBlasi
30 Nursing Care, 384
Debbie Fraser
31 Nutritional Support, 397
Laura D. Brown, Camilia R. Martin, and Sarah N. Taylor
32 Pharmacologic Therapies, 408
Jegen Kandasamy and Waldemar A. Carlo
33 Common Hemodynamic Problems in the Neonate Requiring Respiratory Support, 424
Keith J. Barrington and Eugene M. Dempsey
SECTION 5 Treatment of Specific Conditions, Surgical Interventions and Other Considerations
34 Diagnosis and Management of Persistent Pulmonary Hypertension of the Newborn, 429
Satyan Lakshminrusimha and Martin Keszler
35 Care of the Infant with Congenital Diaphragmatic Hernia, 446
Satyan Lakshminrusimha, Martin Keszler, and Bradley A Yoder
36 Management of the Infant With Bronchopulmonary Dysplasia, 458
Huayan Zhang and Nicolas Bamat
37 Medical and Surgical Interventions for Respiratory Distress and Airway Management, 473
Nathaniel Koo, Thomas Sims, Robert M. Arensman, Nishant Srinivasan, Saurabhkumar Patel, Akhil Maheshwari, and Namasivayam Ambalavanan
38 Intraoperative Management of the Neonate, 491
Christopher E. Colby, Raymond C. Stetson, and Malinda N. Harris
SECTION 6 Complications of Respiratory Support, Special Considerations, and Outcomes
39 Complications of Respiratory Support, 501
Lakshmi Katakam
40 Neonatal Respiratory Care in Resource-Limited Countries, 505
Amuchou Soraisham and Nalini Singhal
41 Transport of the Ventilated Infant, 516
Robert M. Insoft
42 Discharge and Transition to Home Care, 526
Lawrence Rhein
43 Neurologic Effects of Respiratory Support in the Neonatal Intensive Care Unit, 532
Vivien Yap and Jeffrey M. Perlman
44 Pulmonary and Neurodevelopmental Outcomes Following Ventilation, 541
Allison H. Payne, Monika Bhola, Gulgun Yalcinkaya, and Michele C. Walsh
45 Gaps in Knowledge and Future Directions for Research, 549
Tonse N.K. Raju, Payam Vali, and K. Suresh Gautham
Appendices, 565
Jay P. Goldsmith Index, 587
Introduction and Historical Aspects
Jay P. Goldsmith and Tonse N. K. Raju
KEY POINTS
• The birth and early death of a premature son to President John F. Kennedy and Jacqueline Kennedy in 1963 focused the world’s attention on prematurity and the treatment of hyaline membrane disease (HMD), leading to the research and development of pulmonary surfactants, ventilatory devices and improved ventilatory techniques that heralded the modern era of neonatology.
• Although the first reference to providing assisted ventilation to a child is found in the Old Testament, the first 15 centuries ad of recorded attempts to ventilate the neonate or child were crude and generally unsuccessful.
• The early understanding of general cardiorespiratory physiology in the fifteenth through nineteenth centuries led to some anecdotal success of basic ventilatory devices that improved neonatal resuscitation efforts and offered some long term respiratory support to children.
• The first half of the twentieth century witnessed the introduction of many devices that proved mostly unsuccessful in the respiratory treatment of neonates with respiratory failure. In the second half of this century, improved understanding of the physiology of respiratory distress syndrome, the application of end expiratory pressure, and enhancing pulmonary maturation with antenatal steroids and pulmonary surfactant therapy were major advances in the treatment of premature lung disease.
• The major reduction in morbidity and mortality from respiratory failure of newborns seen from 1970 to 2010 has been followed by only modest improvement in the last decade. Further gains in reducing chronic pulmonary morbidities associated with assisted ventilation will depend on translational research and quality improvement initiatives from the bench to the bedside.
The birth of a premature son to President John F. Kennedy and Jacqueline Kennedy on August 7, 1963, focused the world’s attention on prematurity and the treatment of hyaline membrane disease (HMD), then the current appellation for respiratory distress syndrome (RDS). Patrick Bouvier Kennedy was born by cesarean section at 34 weeks’ gestation at Otis Air Force Base Hospital in Massachusetts. He weighed 2.1 kg and was transported to Boston’s Massachusetts General Hospital, where he died at 39 hours of age (Fig. 1.1).1 The Kennedy baby was
treated with the most advanced therapy of the era, hyperbaric oxygen,2 but he died of progressive hypoxemia. There was no neonatal-specific ventilator in the United States to treat the young Kennedy at the time. In response to his death, The New York Times reported: “About all that can be done for a victim of hyaline membrane disease is to monitor the infant’s blood chemistry and try to keep it near normal levels.”1 The Kennedy tragedy, followed only 3 months later by the president’s assassination, stimulated a heightening of interest and research in neonatal respiratory diseases and the treatment of prematurity. This interest resulted in increased federal funding in these areas as well as the proliferation of special areas (neonatal intensive care units [NICUs]) for the care of sick and premature infants at birth in hospitals around the country.
With the possible exception of pediatric oncology, no branch of medicine has seen such dramatic progress in the last half century as has the field of neonatal-perinatal medicine. Less than five decades ago, many centers would not routinely resuscitate infants under 28 weeks of gestation and, in some cases, even those under 1500 g birth weight. A dramatic shift in the physician response and public expectations of care to the very (,1500 g) and extremely low birth weight (,1000 g) newborn occurred largely because of significant advances in perinatal and neonatal care during this period. The improvements in the neonatal areas of respiratory, nutritional, and cardiac care as well as other technological advances gave support to the perception that most preterm infants can be treated effectively and saved from the disorders of prematurity, but also that an overwhelming majority survive without significant long-term disabilities. Specifically, the major technologic advances in ventilatory support, especially over the past two decades, have helped push the concept of the borderline of viability well into the mid second trimester of pregnancy.3 Improved perinatal care also helped contribute to improved neonatal outcomes, especially the improved assessment of fetal wellbeing, enhancing fetal lung maturation and optimizing the time and method of delivery. The results of these advances have made death from respiratory failure relatively infrequent in the neonatal period
unless there are significant underlying conditions such as severe sepsis, necrotizing enterocolitis, major intraventricular hemorrhage, or pulmonary hypoplasia. Thus, there is little doubt that had Patrick Bouvier Kennedy been born today, he would have survived without significant long-term sequelae.
Nonetheless, the long-term consequences of respiratory support continue to be a major issue in neonatal intensive care. Chronic lung disease (CLD), also known as bronchopulmonary dysplasia (BPD), oxygen toxicity, and ventilator-induced lung injury (VILI), continue to afflict a significant number of babies, particularly those with birth weights less than 1500 g.
The focus today is not only to provide respiratory support, which will improve survival, but also to minimize the pulmonary and neurologic complications of these treatments. Quality improvement programs to reduce the unacceptably high rate of CLD and other morbidities of prematurity are an important part of translating the improvements in our technology to the bedside. However, many key issues in neonatal respiratory support still need to be answered and many knowledge gaps persist. These include the optimal ventilator strategy for those babies requiring respiratory support; the role of noninvasive ventilation; the best use of pharmacologic adjuncts such as surfactants, inhaled nitric oxide, methylxanthines, and others; the management of the ductus arteriosus; and many other controversial questions. The potential benefits and risks of many therapies represent dilemmas which are discussed in subsequent chapters and will hopefully assist clinicians in their bedside management of newborns requiring respiratory support.
The purpose of this chapter is to provide a brief history of neonatal assisted ventilation with special emphasis on the evolution of the methods devised to support the neonate with respiratory insufficiency to provide the reader with a perspective of how this field has evolved over the past several thousand years.
HISTORY OF NEONATAL VENTILATION: EARLIEST REPORTS
The exact purpose of breathing for survival remained elusive to ancient physicians although cessation of breathing, or respiratory failure, was well recognized as a cause of death for all age groups, including newborn infants. Hwang Ti (2698–2599 BC),
the Chinese philosopher and emperor, noted that respiratory failure occurred more frequently in children born prematurely.4 Moreover, the medical literature of the past several thousand years contains many references to early attempts to resuscitate infants at birth.
The Old Testament contains the first reference to providing assisted ventilation to a child (II Kings 4:32–35, King James version). “And when Elisha was come into the house, behold the child was dead, and laid upon his bed…. He went up, and lay upon the child and put his mouth upon his mouth, and his eyes upon his eyes, and his hands upon his hands: and he stretched himself upon the child; and the flesh of the child waxed warm…and the child opened his eyes.”5 This description of the first reference to mouth-to-mouth resuscitation suggests that we have been fascinated with resuscitation for millennia.
The Ebers Papyrus from sixteenth century bc Egypt reported increased mortality in premature infants and the observation that a newborn crying at birth will probably survive but the one with an expiratory grunt will die.6
Descriptions of artificial breathing for newly born infants and inserting a reed in the trachea of a newborn lamb can be found in the Jewish Talmud (200 bc to 400 ad).7 Hippocrates (c. 400 bc) first recorded his experience with intubation of the human trachea to support pulmonary ventilation.8 Soranus of Ephesus (98–138 ad) described signs to evaluate the vigor of the newborn (possibly a medieval precursor to today’s Apgar score) and criticized the immersion of the newborn in cold water as a technique for resuscitation.4
Galen, who lived between 129 and 199 ad, used a bellows to inflate the lungs of dead animals via the trachea and reported that air movement caused chest “arises.” The significance of Galen’s findings was not appreciated for many centuries thereafter.9
Around 1000 ad, the philosopher and physician Avicenna (980–1037 ad) described the intubation of the trachea with “a cannula of gold or silver.” Maimonides (1135–1204 ad), the famous rabbi and physician, wrote about how to detect respiratory arrest in the newborn infant and proposed a method of manual resuscitation. In 1472 ad, Paulus Bagellardus published the first book on childhood diseases and described mouth-tomouth resuscitation of newborns.4
During the Middle Ages, the care of the neonate rested largely with midwives and barber surgeons, delaying the next significant advances in respiratory care until 1513 when Eucharius Rosslin’s book first outlined standards for treating the newborn infant.6 Contemporaneous with this publication was the report by Paracelsus (1493–1541), who described using a bellows inserted into the nostrils of drowning victims to attempt lung inflation and using an oral tube in treating an infant requiring resuscitation.6
SIXTEENTH AND SEVENTEENTH CENTURIES
In the sixteenth and seventeenth centuries, advances in resuscitation and artificial ventilation proceeded sporadically with various publications of anecdotal short-term successes, especially in animals. Andreas Vesalius (1514–1564 ad), the famous Belgian anatomist, performed a tracheostomy, intubation, and
Fig. 1.1 Front page of The New York Times. August 8, 1963. (Copyright 1963 by The New York Times Co. Reprinted by permission.)
ventilation on a pregnant sow. Perhaps the first documented trial of “long-term” ventilation was performed by the English scientist Robert Hooke (1635–1703 ad), who kept a dog alive for over an hour using a fireside bellows attached to the trachea.
The scientific renaissance in the sixteenth and seventeenth centuries rekindled interest in the physiology of respiration and in techniques for tracheostomy and intubation. By 1667, simple forms of continuous and regular ventilation had been developed.9 A better understanding of the basic physiology of pulmonary ventilation emerged with the use of these new devices. However, even at this early stage, some physicians recognized the potential for lung injury by mechanical devices with inspired pressures or volumes too great for the human lung to withstand. In 1745, John Fothergill (1712–1780 ad), an English physician, noted in a lecture to the Royal Society: “Mouth to mouth resuscitation may be better than using a mechanical bellows to inflate the lung because…the lungs of one man may bear, without injury, as great a force as those of another can exert, which by the bellows cannot always be determined.”10
Various descriptions of neonatal resuscitation during this period can be found in the medical literature. These anecdotal descriptions by midwives included a variety of interventions to revive a depressed neonate, such as giving a small spoonful of wine into the infant’s mouth in an attempt to stimulate respirations (first described by Bourgeois in 1609) as well as some more detailed descriptions of mouth-to-mouth resuscitation.11
EIGHTEENTH AND NINETEENTH CENTURY
In Europe, medical teaching was dominated by the Church until the French Revolution. The physician Cangiamila was appointed inquisitor by Benedict XIV and wrote a comprehensive textbook describing improved efforts to resuscitate newborns before baptism was allowed.6 Three different types of crude ventilators were described by Hunter (1755), Chaussier (1780), and Gorcy (1790) in the second half of the eighteenth century.6 In the early 1800s, there were sporadic attempts to resuscitate and offer mechanical ventilation to the newborn. In 1800, Fine from Geneva described nasotracheal intubation as an adjunct to mechanical ventilation.12 At about the same time, a better understanding of the principles for mechanical ventilation in adults was evolving. This included the concept of offering rhythmic support of breathing using mechanical devices and, on occasion, passing tubes into the trachea to provide ventilatory support.
In 1806, Vide Chaussier, professor of obstetrics in the French Academy of Science, described his experiments with the intubation and mouth-to-mouth resuscitation of asphyxiated and stillborn infants.13 The work of his successors led to the development in 1879 of the Aerophore Pulmonaire (Fig. 1.2), the first device specifically designed for the resuscitation and shortterm ventilation of newborn infants.8 This device was a simple rubber bulb connected to a tube. The tube was inserted into the upper portion of the infant’s airway, and the bulb was alternately compressed and released to produce inspiration and passive expiration. Subsequent investigators refined these early attempts by designing devices that were used to ventilate laboratory animals.
Charles-Michel Billard (1800–1832) wrote one of the finest early medical texts dealing with clinical-pathologic correlations of pulmonary disease in newborn infants. His book, Traite des maladies des enfans nouveau-nes et a la mamelle, was published in 1828.14
Billard’s concern for the fetus and intrauterine injury is evident, as he writes: “During intrauterine life man often suffers many affectations, the fatal consequences of which are brought with him into the world…children may be born healthy, sick, convalescent, or entirely recovered from former diseases.”14 His understanding of the difficulty newborns may have in establishing normal respiration at delivery is well illustrated in the following passage: “…the air sometimes passes freely into the lungs at the period of birth, but the sanguineous congestion which occurs immediately expels it or hinders it from penetrating in sufficient quantity to effect a complete establishment of life. There exists, as is well known, between the circulation and respiration, an intimate and reciprocal relation, which is evident during life, but more particularly so at the time of birth…. The symptoms of pulmonary engorgement in an infant are, in general, very obscure, and consequently difficult of observation; yet we may point out the following: the respiration is labored; the thoracic parietals are not perfectly develop(ed); the face is purple; the general color indicates a sanguineous plethora in all the organs; the cries are obscure, painful and short; percussion yields a dull sound.”14 It is remarkable that these astute observations were made nearly 200 years ago.
Arguably, James Blundell (1790–1878), the British obstetrician, was perhaps the first to successfully resuscitate apparently stillborn newborn infants by intubation of the trachea using a silver pipe. In his brilliant 1834 paper, he describes how, using the left forefinger as a guide, one can introduce the pipe into the trachea and inflate the infant’s lungs by blowing into it.15
The advances made in the understanding of pulmonary physiology of the newborn and the devices designed to support a newborn’s respiration undoubtedly were stimulated by the interest shown in general newborn care that emerged in the latter part of the nineteenth century and continued into the first part of the twentieth century.16 The reader is directed to multiple references that document the advances made in newborn care in France by Dr. Étienne Tarnier and his colleague Pierre Budin. Budin may well be regarded as the “father of neonatology” because of his contributions to newborn care, including introducing gavage feeding, publishing survival data, and establishing follow-up programs for high-risk newborn patients16 (Fig. 1.3).
In Edinburg, Scotland, Dr. John William Ballantyne, an obstetrician working in the latter part of the nineteenth and early
twentieth centuries, emphasized the importance of prenatal care and recognized that syphilis, malaria, typhoid, tuberculosis, and maternal ingestion of toxins such as alcohol and opiates were detrimental to the development of the fetus.16
O’Dwyer17 in 1887 reported the first use of long-term positive-pressure ventilation in a series of 50 children with croup. The best known of the early American devices for positive-pressure insufflation on the lungs was described by Fell in 1889. This device became known as the Fell-O’Dwyer apparatus (Fig. 1.4).
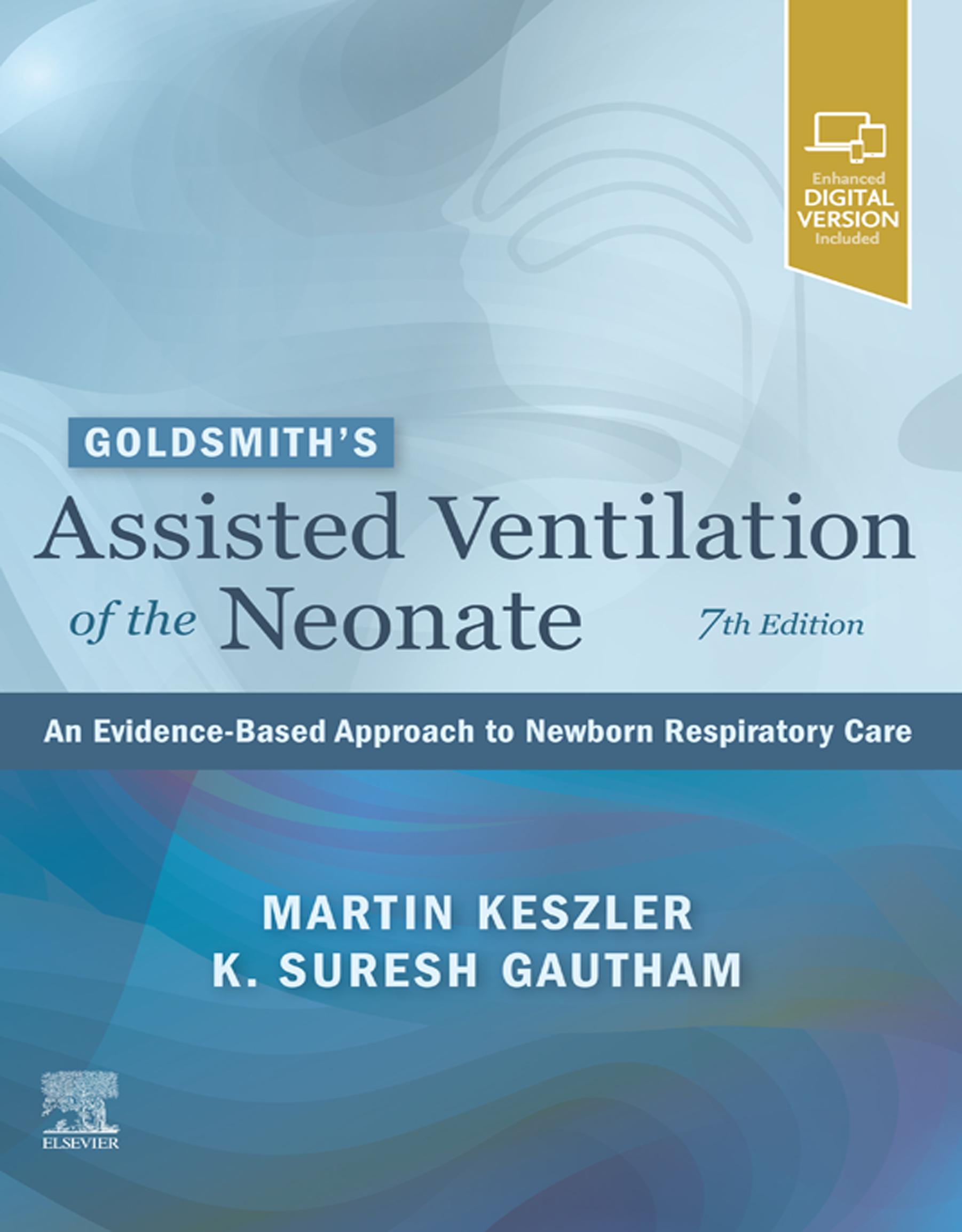
Shortly thereafter, Egon Braun and Alexander Graham Bell independently developed intermittent body-enclosing devices for the negative-pressure/positive-pressure resuscitation of newborns (Fig. 1.5).18 One might consider these seminal reports as the stimulus for the proliferation of work that followed and the growing interest in mechanically ventilating newborn infants with respiratory failure.
TWENTIETH CENTURY
A variety of events occurred in the early twentieth century in the United States, including most notably the improvement of public health measures, the emergence of obstetrics as a full-fledged surgical specialty, and the assumption of care for all children by pediatricians.16 In Europe, there were multiple attempts to create a mechanical respirator that would treat respiratory failure in children. A short-term mobile respirator (“the Pulmonator”) using alternating positive and negative pressure was introduced by Draeger and Blume in 1907, but the neonatal version received mixed reviews.6 In 1914, the use of continuous positive airway pressure (CPAP) for neonatal resuscitation was described by Von Reuss.4 Henderson advocated positive-pressure ventilation via a mask with a T-piece in 1928.19 In the same year, Flagg recommended the use of an endotracheal tube with positive-pressure ventilation for neonatal resuscitation.20 The equipment he described was remarkably similar to that in use today.
Modern neonatology was born with the recognition that premature infants required particular attention with regard to temperature control, administration of fluids and nutrition, and protection from infection. In the 1930s and 1940s, premature infants were given new stature, and it was acknowledged that of all of the causes of infant mortality, prematurity was the most common contributor.16
Similar advances were being made in basic science and physiology. Sir Joseph Barcroft (1872–1947) of Cambridge inaugurated the modern era in the study of fetal physiology. After an illustrious career studying high-altitude cardiorespiratory physiology, Barcroft began a new line of research when he turned age
Fig. 1.3 Pierre Budin (1846–1907), Professor of Obstetrics, Hospital de la Charite, Paris, France, the “Father of Neonatology.”
Fig. 1.4 Fell-O’Dwyer apparatus for insufflation of the lungs. (From Mushin WW, Rendell-Baker L (eds): The Principles of Thoracic Anesthesia. Springfield, IL, Charles C Thomas, 1953, with permission. Copyright Wiley-Blackwell.)
Fig. 1.5 Alexander Graham Bell’s negative-pressure ventilator, c. 1889. (From Stern L, Ramos AD, Outerbridge EW, Beaudry PH: Negative pressure artificial respiration: use in treatment of respiratory failure of the newborn. Can Med Assoc J 102(6):595–601, 1970.)
60 years—the study of mammalian fetal physiology. He adopted a method reported by A. St. Huggett of exteriorizing fetal sheep delivered into a saline bath and maintaining an intact placental circulation. With this and other models, Barcroft and colleagues studied the mechanisms of fetal-placental gas exchange; placental blood volume; fetal cardiovascular reflexes; cardiac output and distribution; the nutrient functions of oxygen, glucose, fat, proteins, and amino acids; and many facets of fetal growth and growth restriction.21 He also trained future scientists from around the world, including Clement Smith of Boston and Donald Baron of Gainesville, Florida. These efforts helped establish a firm foundation for the study of cardiorespiratory physiology of the newborn—a welcome addition to the early and fledging efforts by his junior contemporaries trying to develop methods of support for breathing in newborn infants.
The years following World War II were marked by soaring birth rates, the proliferation of labor and delivery services in hospitals, the introduction of antibiotics, positive-pressure resuscitators, miniaturization of laboratory determinations, Xray capability, and microtechnology that made intravenous therapy available for neonatal patients. These advances and a host of other discoveries heralded the modern era of neonatal medicine and set the groundwork for developing better methods of ventilating neonates with respiratory failure.
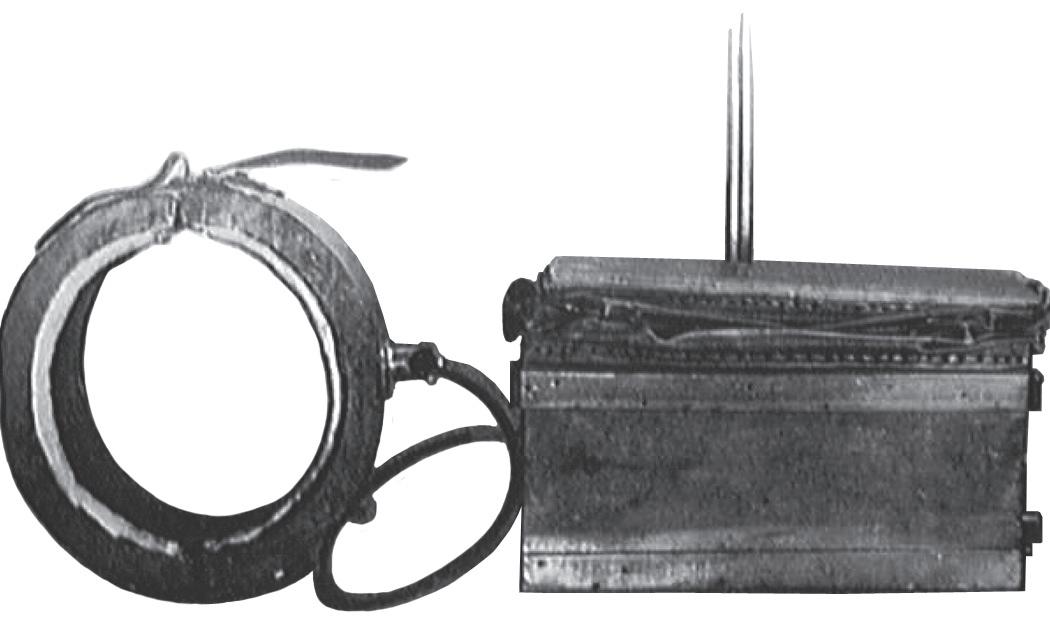
Improvements in intermittent negative-pressure and positivepressure ventilation devices in the early twentieth century led to the development of a variety of techniques and machines for supporting ventilation in infants. In 1929, Drinker and Shaw22 reported the development of a technique for producing constant thoracic traction to produce an increase in end-expiratory lung volume. In the early 1950s, Bloxsom23 reported the use of a positive-pressure air lock for resuscitation of infants with respiratory distress in the delivery room. This device was similar to an iron lung; it alternately created positive and negative pressure of 1 to 3 pounds per square inch at 1-minute intervals in a tightly sealed cylindrical steel chamber that was infused with warmed humidified 60% oxygen.24 Clear plastic versions of the air lock quickly became commercially available in the United States in the early 1950s (Fig. 1.6). However, a study by Apgar and Kreiselman in 195325 on apneic dogs and another study by Townsend involving 150 premature infants26 demonstrated that the device could not adequately support the apneic newborn, which is not surprising, because the infant’s face was enclosed in the device and thus there was no pressure gradient between the outside air and the infant’s lungs. The linkage of high oxygen administration to retinopathy of prematurity and a randomized controlled trial of the air lock versus care in an Isolette® incubator at Johns Hopkins University27 revealed no advantage to either study group and heralded the rapid decline in the use of the Bloxsom device.
In the late 1950s, body-tilting devices were designed that shifted the abdominal contents to create more effective movement of the diaphragm. Phrenic nerve stimulation28 and the use of intragastric oxygen29 also were reported in the literature but had little clinical success and did not gain wide acceptance.
In the first half of the twentieth century, multiple devices were designed by Flagg, Kreiselman, and others including the Engström device using volume control, but none was particularly effective
for the ventilation of preterm neonates. By 1960, Abramson listed 21 ventilators designed for neonates in his text on newborn resuscitation.6
In the 1950s and early 1960s, many centers also used bag and tightly fitting face mask ventilation to support infants for relatively long periods of time. Unfortunately, there was a high complication rate of intracranial hemorrhage which curtailed the use of these devices.
To the best of our knowledge, Professor Ian Donald and his group from Glasgow, UK, were among the first scientists who successfully provided assisted ventilation for prolonged periods of time for newborn infants with respiratory distress. In 1953, Donald reported the results of “augmented respiration” given to 28 infants from Cape Town, South Africa. Three of the 28 infants lived at least for three or more hours.30 In 1958, they followed this reporting with pulmonary function test results (using transesophageal electromanometry and spirometry) in 38 infants, 16 of whom had respiratory distress. They also reported that of the 151 newborn infants treated with “augmented respiration,” 50 survived, including 11/62 infants with a birth weight ranging between 2 lb and 2 lb 15 oz31 (907 g and 1332 g).
Two other historical milestones approximately overlapped the efforts of Donald and colleagues in providing assisted ventilation to preterm newborn infants in respiratory distress. In the fall of 1961, Dr. Mildred Stahlman at Vanderbilt University devised a negative pressure ventilator and treated her first patient with severe HMD.32 In a talk given in 1980, she said, “After placing an umbilical venous catheter in the left atrium, the baby was sealed in the tank where she remained for five very tiring, but enormously instructive days…” The infant survived, and currently, at age 59, she is a registered nurse working at the same institution where she was cared for as a newborn.33 In 1965, Delivoria-Papadopoulos and colleagues from Canada reported that of the 18 patients offered assisted ventilation using positivepressure ventilation, one infant who weighed 1.8 kg at 34 weeks’ gestation survived, was discharged on the 47th day and appeared to be doing well at age 6 months.34 These efforts, besides being
Fig. 1.6 Commercial Plexiglas version of the positive-pressure oxygen air lock. Arrival of the unit at the Dansville Memorial Hospital, Dansville, NY, June 1952. (Photo courtesy of James Gross and the Dansville Breeze. June 26, 1952.)
of historical significance, should be viewed as great success stories because they attempted to treat infants who were extremely ill, and in some cases, “terminal” or “near-terminal.”35
Partially in response to the Kennedy baby’s death in 1963, several intensive care nurseries around the country (most notably at Yale, Children’s Hospital of Philadelphia, Vanderbilt, and the University of California at San Francisco) began programs focused on respiratory care of the premature neonate and the treatment of HMD. The initial success with ventilatory treatment of HMD reported by Delivoria-Papadopoulos34 and Stahlman32 resulted in the use of modified adult ventilatory devices in these and other medical centers across the United States. However, these successes also led to the emergence of a new disease, BPD, first described in a seminal paper by Northway et al.36 in 1967. Initially, Northway attributed BPD to the use of high concentrations of inspired oxygen, but subsequent research by others demonstrated that the cause of BPD was much more complex. Besides high concentrations of inspired oxygen, intubation, barotrauma, volutrauma, infection, and other factors were involved, superimposed on the immature lungs and airways of premature infants. Chapters 21 and 36 discuss the current theories for the multiple causes of BPD or VILI.
Advances in ventilatory support for the neonate also influenced improvement in neonatal resuscitation. Varying techniques in the United States were published from the 1950s to the 1980s, but the first systematic approach was created by Bloom and Cropley in 1987 and adopted by the American Academy of Pediatrics and American Heart Association as a standardized teaching program.37 A synopsis of the major events in the development of neonatal resuscitation is shown as a timeline in Box 1.1.
In the decades following Donald’s pioneering efforts, the field of mechanical ventilation made dramatic advances; however, the gains were accompanied by several temporary setbacks. Because of the epidemic of poliomyelitis in the 1950s, experience was gained with the use of the tank-type negativepressure ventilators of the Drinker design.32 The success of these machines with children encouraged physicians to try modifications of these ventilators for use in the treatment of newborn infants and some anecdotal success was reported. However, initial efforts to apply intermittent positive-pressure ventilation (IPPV) to premature infants with RDS were disappointing overall. Mortality was not demonstrably decreased, and the incidence of complications, particularly that of pulmonary air leaks, increased.38 During this period, clinicians were hampered by the available types of ventilators and by a lack of physiologically based approaches for their use.
In accordance with the findings of Cournand et al.39 in adult studies conducted in the late 1940s, standard ventilatory technique often required that the inspiratory positive-pressure times be very short. Cournand et al. had demonstrated that the prolongation of the inspiratory phase of the ventilator cycle in patients with normal lung compliance could result in impairment of thoracic venous return, a decrease in cardiac output, and the unacceptable depression of blood pressure. To minimize cardiovascular effects, they advocated that the inspiratory phase of a mechanical cycle be limited to one-third of the entire
BOX 1.1 Neonatal Resuscitation Timeline
1300 BC: Hebrew midwives use mouth-to-mouth breathing to resuscitate newborns.
460–380 BC: Hippocrates describes intubation of trachea of humans to support respiration.
200 BC–500 AD: Hebrew text (Talmud) states, “we may hold the young so that it should not fall on the ground, blow into its nostrils and put the teat into its mouth that it should suck.”
98–138 AD: Greek physician Soranus describes evaluating neonates with a system similar to present-day Apgar scoring, evaluating muscle tone, reflex or irritability, and respiratory effort. He believed that asphyxiated or premature infants and those with multiple congenital anomalies were “not worth saving.”
1135–1204: Maimonides describes how to detect respiratory arrest in newborns and describes a method of manual resuscitation.
1667: Robert Hooke presents to the Royal Society of London his experience using fireside bellows attached to the trachea of dogs to provide continuous ventilation.
1774: Joseph Priestley produces oxygen but fails to recognize that it is related to respiration. Royal Humane Society advocates mouth-to-mouth resuscitation for stillborn infants.
1783–1788: Lavoisier terms oxygen “vital air” and shows that respiration is an oxidative process that produces water and carbon dioxide.
1806: Vide Chaussier describes intubation and mouth-to-mouth resuscitation of asphyxiated newborns.
1834: James Blundell describes neonatal intubation.
1874: Open chest cardiac massage reported in an adult.
1879: Report on the Aerophore Pulmonaire, a rubber bulb connected to a tube that is inserted into a neonate’s airway and then compressed and released to provide inspiration and passive expiration.
1889: Alexander Graham Bell designs and builds body-type respirator for newborns.
Late 1880s: Bonair administers oxygen to premature “blue baby.”
1949: Dr. Julius Hess and Evelyn C. Lundeen, RN, publish The Premature Infant and Nursing Care, which ushers in the modern era of neonatal medicine.
1953: Virginia Apgar reports on the system of neonatal assessment that bears her name.
1961: Dr. Jim Sutherland tests negative-pressure infant ventilator.
1971: Dr. George Gregory and colleagues publish results with continuous positive airway pressure (CPAP) in treating newborns with respiratory distress syndrome.
1987: American Academy of Pediatrics publishes the Neonatal Resuscitation Program (NRP) based on an education program developed by Bloom and Cropley to teach a uniform method of neonatal resuscitation throughout the United States.
1999: The International Liaison Committee on Resuscitation (ILCOR) publishes the first neonatal advisory statement on resuscitation drawn from an evidence-based consensus of the available science. The ILCOR publishes an updated Consensus on Science and Treatment Recommendations (CoSTaR) for neonatal resuscitation every 5 years thereafter. The NRP published every 5 years based on the ILCOR CoSTaR recommendations.
2020: Over 4 million health care providers trained in the NRP program by over 21,000 active instructors over the history of the NRP program.
cycle.39 Some ventilators manufactured in this period were even designed with the inspiratory-to-expiratory ratio fixed at 1:2. However, the recommendations by Cournand et al. were not applicable to patients with significant RDS, who had a complex combination of abnormal pulmonary mechanics. The dramatically reduced lung compliance and the highly compliant chest
wall, combined with a tendency for terminal airways and alveoli to collapse, were factors that led to poor responses to IPPV techniques without positive end-expiratory pressure (PEEP) that worked well in adults and older children. Clinicians were initially disappointed with the outcome of neonates treated with assisted ventilation using these adult oriented techniques.
BREAKTHROUGHS IN VENTILATION
The important observation of Avery and Mead in 1959 was that babies who died of HMD lacked a surface-active agent (surfactant), which increased surface tension in lung liquid samples and resulted in diffuse atelectasis.40 This finding paved the way toward the modern treatment of respiratory failure in premature neonates by suggesting the constant maintenance of functional residual capacity through some form of end expiratory pressure and the eventual creation of surfactant replacement therapies.
A major breakthrough in neonatal ventilation occurred in 1971 when Gregory et al.41 reported on clinical trials with CPAP for the treatment of RDS. Recognizing that the major physiologic problem in RDS was the collapse of alveoli during expiration, they applied continuous positive pressure to the airway via an endotracheal tube or sealed head chamber (“the Gregory box”) during both expiration and inspiration; dramatic improvements in oxygenation and ventilation were achieved. Although infants receiving CPAP breathed spontaneously during the initial studies, later combinations of IPPV and CPAP in infants weighing less than 1500 g were not as successful.38 Nonetheless, the concept of CPAP was a major advance. It was later modified by Bancalari et al.42 for use in a constant distending negative-pressure chest cuirass and by Kattwinkel et al.,43 who developed nasal prongs for the application of CPAP without the use of an endotracheal tube.
The observation that administration of antenatal corticosteroids to mothers prior to premature delivery accelerated maturation of the fetal lung was made in 1972 by Liggins and Howie.44 Their randomized controlled trial demonstrated that the risks of HMD and death were significantly reduced in those premature infants whose mothers received antenatal steroid treatment. However, this therapy did not gain wide acceptance for over 2 decades.
Meanwhile, Reynolds and Taghizadeh,45,46 working independently in Great Britain, also recognized the unique pathophysiology of neonatal pulmonary disease. Having experienced difficulties with IPPV similar to those noted by clinicians in the United States, Reynolds and Taghizadeh suggested prolongation of the inspiratory phase of the ventilator cycle by delaying the opening of the exhalation valve. The “reversal” of the standard (i.e., short) inspiratory-to-expiratory ratio (advocated by Cournand), or “inflation hold,” allowed sufficient time for the recruitment of atelectatic alveoli in RDS with lower inflating pressures and gas flows, which, in turn, decreased turbulence and limited the pulmonary effects on venous return to the heart. The excellent results of Reynolds and Taghizadeh shown in the United Kingdom could not be duplicated uniformly in the United States, perhaps because their American colleagues used different ventilators.
Until the early 1970s, ventilators used in NICUs were modifications of adult devices; these devices delivered intermittent gas flows, thus generating IPPV. The ventilator initiated every mechanical breath, and clinicians tried to eliminate the infants’ attempts to breathe between IPPV breaths (“fighting the ventilator”), which led to rebreathing of dead space air. In 1971, a new prototype neonatal ventilator was developed by Kirby and colleagues.47 This ventilator used continuous gas flow and a timing device to close the exhalation valve modeled after Ayre’s T-piece used in anesthesia (Fig. 1.7).47,48 Using the T-piece concept, the ventilator provided continuous gas flow and allowed the patient to breathe spontaneously between mechanical breaths. Occlusion of the distal end of the T-piece diverted gas flow under pressure to the infant. In addition, partial occlusion of the distal end generated PEEP. This combination of mechanical and spontaneous breathing and continuous gas flow was called intermittent mandatory ventilation (IMV).
IMV became the standard method of neonatal ventilation and has been incorporated into all infant ventilators since then. One of its advantages was the facilitation of weaning by progressive reduction in the IMV rate, which allowed the patient to gradually increase spontaneous breathing against distending pressure. Clinicians no longer needed to paralyze or hyperventilate patients to prevent them from “fighting the ventilator.” Moreover, because patients continued to breathe spontaneously and lower cycling rates were used, mean intrapleural pressure was reduced and venous return was less compromised than with IPPV.48
Meanwhile, progress was also being made in the medical treatment and replacement of the cause of RDS, the absence or lack of adequate surfactant in the neonatal lung. Building on the observations of Avery and Meade in 1959, Fujiwara et al.
Fig. 1.7 Ayre’s T-piece forms the mechanical basis of most neonatal ventilators currently in use. (A) Continuous gas flow from which an infant can breathe spontaneously. (B) Occlusion of one end of the T-piece diverts gas flow under pressure into an infant’s lungs. The mechanical ventilator incorporates a pneumatically or electronically controlled timecycling mechanism to occlude the expiratory limb of the patient circuit. Between sequential mechanical breaths, the infant can still breathe spontaneously. The combination of mechanical and spontaneous breaths is called intermittent mandatory ventilation. (From Kirby RR: Mechanical ventilation of the newborn. Perinatol Neonatol 5:47, 1981.)
reported in 1980 on the beneficial effect of exogenous surfactant in a small series of premature infants with HMD.49 Thereafter, several large randomized studies of the efficacy of surfactant were conducted, and by the end of the decade, the use of surfactant was well established. However, controversies continued for decades concerning surfactant treatment regiments, such as prophylactic versus rescue therapy, types of surfactants, and dosing schedules.50
From 1971 to the mid-1990s, a myriad of new ventilators specifically designed for neonates were manufactured and sold. The first generation of ventilators included the Babybird 1® (Fig. 1.8), the Bourns BP200®, and a volume ventilator, the Bourns LS 104/150®. All operated on the IMV principle and were capable of incorporating CPAP into the respiratory cycle (known as PEEP when used with IMV).51 The first edition of this text published in 1981 described these ventilators in detail.
The Babybird 1® and the Bourns BP200® used a solenoidactivated switch to occlude the exhalation limb of the gas circuit to deliver a breath. Pneumatic adjustments in the inspiratoryto-expiratory ratio and rate were controlled by inspiratory and expiratory times, which had to be timed with a stopwatch. A spring-loaded pressure manometer monitored peak inspiratory pressure and PEEP. These early mechanics created time delays within the ventilator, resulting in problems in obtaining short inspiratory times (,0.5 seconds).
In the next generation of ventilators, electronic controls, microprocessors, and micro-circuitry allowed the addition of light-emitting diode monitors and provided clinicians with faster response times, greater sensitivity, and a wider range of ventilator parameter selection. These advances were incorporated into ventilators such as the Sechrist 100® and Bear Cub® to decrease inspiratory times to as short as 0.1 second and to increase ventilatory rates to 150 inflations per minute. Monitors incorporating microprocessors measured inspiratory and expiratory times and calculated inspiratory-to-expiratory ratios
and mean airway pressure. Ventilator strategies abounded, and controversy regarding the best (i.e., least harmful) method for assisting neonatal ventilation arose. High-frequency positivepressure ventilation using conventional ventilators was also proposed as a beneficial treatment of RDS.52
Meanwhile, extracorporeal membrane oxygenation and true high-frequency ventilation (HFV) were being developed at a number of major medical centers.53,54 These techniques initially were offered as a rescue therapy for infants who did not respond to conventional mechanical ventilation. The favorable physiologic characteristics of HFV led some investigators to promote its use as an initial treatment of respiratory failure, especially when caused by RDS in very low birth weight (VLBW) infants, in the hopes of decreasing lung injury.55
A third generation of neonatal ventilators began to appear in the early 1990s. Advances in microcircuitry and microprocessors, developed as a result of the space program, allowed new dimensions in the development of neonatal assisted ventilation. The use of synchronized IMV, assist/control mode ventilation, and pressure support ventilation—previously only used in the ventilation of older children and adults—became possible in neonates because of the very fast ventilator response times. Although problems with sensing a patient’s inspiratory effort sometimes limited the usefulness of these new modalities, the advances gave hope that ventilator complications could be limited and that the need for sedation or paralysis during ventilation could be decreased. Direct measurement of some pulmonary functions at the bedside became a reality and allowed the clinician to make ventilatory adjustments based on physiologic data rather than on an educated “hunch.”
Since the turn of the century, an even newer generation of ventilators has been developed. These are microprocessor based, with a wide array of technological features, including several forms of patient triggering, volume targeting, and pressure support modes and the ability to monitor many pulmonary functions at the bedside with ventilator graphics. As clinicians become more convinced that VILI was secondary to volutrauma more than barotrauma, the emphasis to control tidal volumes especially in the “micropremie” resulted in major changes in the technique of ventilation. The chapters in Section III elaborate more fully on these advances and ventilatory strategies.
Concurrent with these advances came an increased complexity related to controlling the ventilator and, thus, more opportunity for operator error. Some ventilators are extremely versatile and can function for patients of extremely low birth weight (,1000 g) to 70-kg adults. Although these ventilators are appealing to administrators who purchase expensive machines for different categories of adult and pediatric patients in the hospital, they add increased complexity and patient safety issues in caring for neonates. Chapter 6 discusses some of these issues.
Respiratory support in the present-day NICU continues to change as new science and new technologies point the way to better outcomes with less morbidity, even for the smallest premature infants. However, as the technology of neonatal ventilators advanced, a concurrent movement away from intubation and standard ventilation was gaining popularity in the United States. In 1987, a comparison of eight major centers in the
National Institute of Child Health and Human Development Neonatal Research Network by Avery et al. reviewed oxygen dependency and death in VLBW babies at 28 days of age.56 Although all centers had comparable mortality, one center (Columbia Presbyterian Medical Center) had the lowest rate by far of CLD among the institutions. Columbia had adopted a unique approach to respiratory support of VLBW infants, emphasizing nasal CPAP as the first choice for respiratory support, whereas the other centers were using intubation, surfactants, and mechanical ventilation. Other centers were slow to adopt the Columbia approach, which used bubble nasal CPAP, but gradually institutions began using noninvasive techniques for at least the larger VLBW infants. A Cochrane review of multiple trials in 2012 concluded that the combined outcomes of death and BPD were lower in infants who had initial stabilization with nasal CPAP, and later rescue surfactant therapy if needed, compared with elective intubation and prophylactic surfactant administration (relative risk, 1.12; 95% confidence interval, 1.02 to 1.24).57 In recent years, “noninvasive” respiratory support with the use of nasal CPAP, synchronized noninvasive intermittent positive pressure ventilation, and neurally adjusted ventilatory assist (NAVA) have become more widely used techniques to support premature infants with respiratory distress in the hope of avoiding the trauma associated with intubation and VILI. Using a noninvasive approach as one potentially better practice is attractive, but quality improvement programs to lower the rate of BPD have had mixed success. Noninvasive ventilation has been supported by a number of retrospective and cohort studies, and reports suggest that the earlier use of noninvasive therapies such as CPAP started in the delivery room has a role in treating neonates with respiratory disease and preventing the need for intubation to treat respiratory failure.
RECENT ADVANCES AND OUTCOMES
The advances in neonatal ventilation over the past five decades has resulted in the mortality from HMD, later called RDS, to decrease dramatically from 1971 through 2019. The rate in the United States dropped from 268 per 100,000 live births in 1971 to 98 per 100,000 live births by 1985 and continued to drop further through the final decades of the twentieth century and into the twenty-first century.58 By 2007, the rate had decreased to 17 per 100,000 live births.59
In an epidemiological study of over 1.5 million preterm live births under 34 weeks’ gestation born between 2003 and 2014 reported by Donda et al., RDS was diagnosed in around 36% (554,409 cases). The all-cause mortality in this group decreased from 7.6% to 6.1%. The mortality among those under 28 weeks of gestation dropped from 21.7% to 16.8%, and among 29 to 34 weeks’ gestation, from 1.6% to 1.4% between 2003 and 2014, respectively.60
The late preterm infant (34 to 36 and 6/7 weeks’ gestation) has shown even more compelling improvements as compared with the state-of-the-art medical care available to Patrick Bouvier Kennedy in 1963. In the antenatal steroid trial for women in labor during late preterm gestation (defined in this study as
34 weeks 0 days to 36 weeks 5 days), the incidence of RDS was around 6% (168/2827 in the total cohort). There were only two deaths before hospital discharge, both from non-RDS causes.61 Similarly, Sekar et al. reported in 2019 that the RDS-related mortality was 2% among the 13,240 preterm infants, 25 to 36 weeks of gestation, born between 2010 and 2013.62 Based on the available data, we can safely conclude that the mortality from RDS occurs extremely rarely in the modern NICU, mostly confined to extremely preterm infants.
Thus, over a period of five decades, the mortality attributed to RDS has approached less than 2% owing in part to the improvements in ventilator technology, the development of medical adjuncts such as antenatal steroids and exogenous surfactants, and the skill of the physicians, nurses, and respiratory therapists using these devices while caring for these fragile infants.58-64
Although the advances made in providing assisted ventilation to our most vulnerable patients have improved survival (85%–90% in premature infants ,28 weeks’ gestation and/or 1000 g), morbidities remain troublesome. In recent years, the emphasis has shifted from just survival to survival without significant neurologic deficit, BPD, or retinopathy of prematurity. Nonetheless, benchmarking groups such as the VermontOxford Network have shown a wide variance in these untoward outcomes that cannot be explained by variances in the patient population alone. BPD in infants born at less than 1500 g birth weight (i.e., VLBW infants) varies from 6% to over 50% in various NICUs. Thus, it appears that overall advances in the morbidity and mortality rates of the VLBW infant group as a whole will be made from more uniform application of technology already available rather than the creation of new devices or medications. Moreover, despite continued technological advances in respiratory support in the last decade, the reduction in morbidity and mortality rates in high-resource countries has only seen modest improvement. Many of the large organizations of hospitals (Vermont-Oxford Network, Neonatal Research Network) as well as physician organizations (Perinatal Section of the American Academy of Pediatrics, Mednax) have played a major role in disseminating improved aspects of care to the nearly 1000 NICUs in this country. Perhaps entirely new approaches are necessary to produce major leaps forward in the treatment of neonatal respiratory failure. However, in resource-limited areas throughout the world, the use of basic respiratory support technologies (i.e., CPAP, resuscitation techniques) has begun to have a major impact on the outcomes of newborns (see Chapter 40).
Despite the wide array of technology now available to the clinician treating neonatal respiratory failure, there are still significant limitations and uncertainty about our care. We continue to research and discuss issues such as conventional ventilation versus HFV, noninvasive ventilation versus the early administration of surfactant, the best ventilator mode, the optimum settings, and the most appropriate approach to weaning and extubation. There are very few randomized controlled trials that demonstrate significant differences in morbidity or mortality related to new ventilator technologies or strategies. This is owing to the difficulty in enrolling neonates into clinical trials, the large number of patients needed to detect statistical differences in outcomes, the reluctance of device manufacturers