EpidemiologyofThyroid Disorders
JAHANGIRMOINI,MD,MPH
ProfessorofScienceandHealth(Retired), EasternFloridaStateCollege, PalmBay,FL,UnitedStates
KATHERINEPEREIRA,DNP,FNP-BC,FAANP,FAAN ProfessorofNursing, DukeUniversitySchoolofNursing, NC,UnitedStates
MOHTASHEMSAMSAM,MD,PHD
ProfessorofMedicine, BurnettSchoolofBiomedicalSciencesandCollegeofMedicine, UniversityofCentralFlorida, FL,UnitedStates
Elsevier
Radarweg29,POBox211,1000AEAmsterdam,Netherlands
TheBoulevard,LangfordLane,Kidlington,OxfordOX51GB,UnitedKingdom 50HampshireStreet,5thFloor,Cambridge,MA02139,UnitedStates
Copyright©2020ElsevierInc.Allrightsreserved.
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans, electronicormechanical,includingphotocopying,recording,oranyinformationstorageand retrievalsystem,withoutpermissioninwritingfromthepublisher.Detailsonhowtoseek permission,furtherinformationaboutthePublisher’spermissionspoliciesandourarrangements withorganizationssuchastheCopyrightClearanceCenterandtheCopyrightLicensingAgency, canbefoundatourwebsite: www.elsevier.com/permissions .
Thisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythe Publisher(otherthanasmaybenotedherein).
Notices
Knowledgeandbestpracticeinthisfieldareconstantlychanging.Asnewresearchand experiencebroadenourunderstanding,changesinresearchmethods,professionalpractices,or medicaltreatmentmaybecomenecessary.
Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgein evaluatingandusinganyinformation,methods,compounds,orexperimentsdescribedherein.In usingsuchinformationormethodstheyshouldbemindfuloftheirownsafetyandthesafetyof others,includingpartiesforwhomtheyhaveaprofessionalresponsibility.
Tothefullestextentofthelaw,neitherthePublishernortheauthors,contributors,oreditors, assumeanyliabilityforanyinjuryand/ordamagetopersonsorpropertyasamatterofproducts liability,negligenceorotherwise,orfromanyuseoroperationofanymethods,products, instructions,orideascontainedinthematerialherein.
BritishLibraryCataloguing-in-PublicationData
AcataloguerecordforthisbookisavailablefromtheBritishLibrary
LibraryofCongressCataloging-in-PublicationData
AcatalogrecordforthisbookisavailablefromtheLibraryofCongress
ISBN:978-0-12-818500-1
ForInformationonallElsevierpublications visitourwebsiteat https://www.elsevier.com/books-and-journals
Publisher: StacyMasucci
AcquisitionEditor: TariBroderick
EditorialProjectManager: TimothyBennett
ProductionProjectManager: KiruthikaGovindaraju
CoverDesigner: MarkRogers
TypesetbyMPSLimited,Chennai,India
Globalepidemiologyofthyroid disorders
Contents
Worldpopulation 3
Agingofthepopulation4
Lifeexpectancy 6
Distributionofthyroiddisordersbygenderandage8
Population-basedmodelsofthyroiddisorders10
Globalprevalenceofthyroiddisorders11
Globalepidemiologyofthyroiddisorders12
Globalpreventionofthyroiddisorders12
Globaldeathratesfromthyroiddisorders15
Disability-adjustedlifeyearsforthyroiddisorders17
Burdenofthyroiddisorders18
Furtherreading 18
Thyroiddisordersareverycommonthroughouttheworldandcauseproblemsbecause ofoverfunctioningorunderfunctioningofthethyroidgland.Thesedisordersmaylead toenlargementofthethyroidgland,causingdirectsymptomssuchasdifficultyinswallowingandneckdiscomfort.Withtoday’sincreasedelderlypopulationandbetterdiagnosticmethods,thyroiddisordersaredocumentedmoreoften.Themostsignificant problemrelatedtothyroidisglobaliodinedeficiency,whichresultsingoiterandhypothyroidism.Thyroiddisordersaffectpeopleofallagesandaremorecommoninfemales thanmales.Thehighestincidenceofoverthyperthyroidismisinpeoplemorethanthe ageof65.Hashimoto’sthyroiditisisthemostcommontypeofthyroiditis.Graves’ diseaseisanautoimmunedisorder,whichiseighttimesmoreprevalentinfemalesand twiceascommoninAfricanAmericansasinothergroups.Morethan75%ofthyroid cancersoccurinfemalesbetweenages20and55.Inthischapterthefocusesareonthe incidenceandprevalenceofthyroiddisordersthroughouttheglobalpopulation.
Worldpopulation
Currently,theworldpopulationisgrowingatarateofapproximately1.07%peryear. Thecurrentaveragepopulationincreaseisestimatedtobe82millionpeopleannually. Thepeakannualgrowthratewasduringthelate1960s,whenitwasabout2%per
EpidemiologyofThyroidDisorders
https://doi.org/10.1016/B978-0-12-818500-1.00001-3
year.Itisestimatedtocontinuedecreasingannually,reachingonly1%growthbythe year2023.Worldpopulationdoubledbetweentheyears1959and1999.Evenwith thereductioninannualincreases,theUnitedNationsprojectsthattheworldpopulationwillreach10billionbytheyear2056.Thisdatacomesfrommanysources, includingtheUnitedNationsPopulationDivision,theWorldPopulationProspect, andtheInternationalProgramsCenterattheUnitedStatesCensusBureau.Asof May2019,censusbureausthroughoutvariouscountrieshaveestimatedthatthe worldpopulationpresentlyexceeds7.7billionpeople.Thetop10mostpopulated countriesareasfollows:
• China(1.4billion)
• India(1.3billion)
• UnitedStates(328million)
• Indonesia(269million)
• Brazil(212million)
• Pakistan(203million)
• Nigeria(200million)
• Bangladesh(167million)
• Russia(143million)
• Mexico(132million)
Agingofthepopulation
Theworldpopulationisalsoincreasinginage.Therearetwoprimaryreasonsforthis. Thefirstisthatwearesimplylivinglongerduetohealthierlifestylesandbettermedicaltreatments.Thesecondisthatthefertilityrateisdecreasing,resultinginfewer womenbecomingpregnant.TheaveragelifeexpectancyintheUnitedStatesishigher todaythanduringanyothertimeinhistory.TheUnitedNationsissuedareport showingthatpeopleages65yearsandolderincreasedfrom8%ofthetotalpopulation in1950to12%ofthetotalpopulationin2000.Thisfigureisexpectedtoincreaseto 20%bytheyear2050andwillprobablyrisesteadilyafterthat.Thisisprimarilydueto largeimprovementsinhealthcare,investmentinmedicalresearch,andbetterhealth insuranceavailability.FewerAmericansaredyingfromdiseases,suchasbreastcancer, coloncancer,prostatecancer,heartdisease,andHIV.
AccordingtotheWorldHealthOrganization,theglobalpopulationissimilarly increasinginage.Therewillsoonbehighernumbersofelderlypeoplethanchildren, andmorepeopleatextremeoldagethaneverinhistory(see Fig.1.1).Tounderstand thisphenomenon,wemustrealizethatin1900,themajorhealththreatswereinfectious andparasiticdiseases.Theseoftencausedthedeathsofinfantsandchildren.Today,noncommunicablediseasesthatmostlyaffectadultsandtheelderlyhavethegreatestimpact onglobalhealth.Thehealthandeconomicburdensofage-relateddisabilitycanbe
https://www.nia.nih.gov/sites/ default/files/2017-06/global_health_aging.pdf .
affectedbyenvironmentalfactorsthatdetermineifpeoplecanremainindependent, eventhoughtheymaybephysicallylimited.Thelongerpeopleremainmobileandtake careofthemselves,thelowerthecostswillbeforrequiredlong-termcare.
Thefactsaboutdecreasingfertility,onaglobalbasis,arealsoveryimportantto understand.Inmoredevelopedcountries,fertilityfellbelowthe “replacement” rateof twolivebirthsperwomaninthe1970s,whilewomeninthe1950saveragedthree livebirths.Inlessdevelopedcountries,fertilityratesfellevenfaster.In1950women inthesecountriesaveragedsixlivebirths,butby2006,theratewasatorbelowtwo livebirths.WhileNiger,anAfricancountry,hasthehighestfertilityrate,of7.1childrenperwoman,manycountrieswithlargepopulationsarenowtowardthelower endofthescale.Forexample,theUnitedStatesnowranks135thonthelistwith1.8 childrenperwoman.ThelowestfertilityrateisinTaiwanwith1.2childrenper woman,followedbyMoldova,Portugal,Singapore,Poland,Greece,SouthKorea, HongKong,Cyprus,andMacau.
Countriesthatarerapidly “shrinking” inpopulationincludeUkraine,whichwill decrease22%by2050.Poland,theRussianFederation,Italy,andSpainarealso shrinking.ThepopulationoftheEuropeanUnionisexpectedtopeakby2050and thengraduallydecline.Germanyhasexperienceddemographicdeclineformorethan agenerationandisestimatedtodrop7.7%inpopulationby2050,nottakinginto accounttherecentimmigrationintothecountry.Bulgariaisexpectedtoshrink27% by2050,andRomaniawillshrinkby22%.Japanwillhaveadecreaseinpopulation
Figure1.1 Changesinageoftheglobalpopulationsince1950.
by15%andby2030willactuallyhavemorepeoplemorethan80yearsthan below15years.China’sextremelylowfertilityratemeansthatthecountrywillhave 28millionlesspeopleby2050.
Focusonagingandthyroiddisorders
Itiswelldocumentedthattheprevalenceofthyroiddisordersincreaseswithage.However, sincesymptomsofthyroiddiseasearemoresubtleinolderpeople,theyareoftenattributed tonormalaging.Thereforetheyrequirespecialattention.Oneofeveryfivewomenmore than65yearsofagehasahigher-than-normalthyroid-stimulatinghormone(TSH)level,indicatinghypothyroidism.About25%oftheelderlypopulationhassomeformofmentalillness, andalargenumberofthesecasesmaybecausedbythyroiddisease.
Lifeexpectancy
Lifeexpectancy isalsoknownas longevity. Itiscalculatedbycreatinga lifetable that recordsthenumbersofdeathsandsurvivorswithinaspecificyear,forsuccessivelifespanintervals.Deaths,survivors,and age-specificdeathrates arecalculatedforvarious age-groups,suchas0 1year,1 5years,andthenforsuccessive5-yearage-groups afterthat.Thisdataisusedtocreateasecondlifetablethatrepresentsthetotalmortalityratesfrombirthtodeath,for100,000hypotheticallivebirths.Thisissubjectto age-specificdeathratesinthepopulationbeingstudiedforaparticularyear.Thisdata isusedtocalculatelifeexpectancyastheaveragelifeyearsforallmemberssincebirth. Lifeexpectancyequalstotalyearsoflifeforallmembersofthelivetable,dividedby thetotalnumberofpersonsatbirth.Thereforelongevityatbirthisthemeanyearsof life,basedtotallyonage-specificdeathratesforthepopulationandtheyearof interest.
Mostpeoplebornintheyear1900didnotlivepasttheageof50.Accordingto theCentersforDiseaseControlandPrevention,lifeexpectancyatbirthforpeople bornin2012intheUnitedStateswas78.8years.Today,nearly1in10girlswilllive pasttheageof100years,andnearly1in20boyswilllivepast100.Lifeexpectancy forfemalesis81.2yearsandformalesis76.4years.Thedifferencebetweenthemis 4.8years,whichhasremainedthesamesince2011.Asofnow,awomanturning65 in2019canexpecttolive,onaverage,untiltheageof86.6.Amanreaching65can expecttolive,onaverage,untiltheageof84.3.Intheyear2015theaverage Americanwomanreachingage65hadmorethanaone-in-threechanceofreaching theageof90.Thisismorethantheone-in-fourchancethatexisted50yearsago. ThecountrieswiththeoldestpopulationsincludeMonaco,Japan,Germany,Italy, Greece,Sweden,Spain,Austria,Bulgaria,andEstonia.InMonaco,forexample, 22.8%ofthepopulationisof65yearsorolder.In201913.1%oftheUSpopulation isof65yearsorolder(see Fig.1.2).

Figure1.2 Healthylifeexpectancy(HALE)atbirth,bothsexes,2016. gamapserver.who.int/maplibrary/files/maps/global_HALE_2016.png .
Peopleprovidinghealthcaretotheelderly,aswellasdisabledpatients,increased intheUnitedStatesfrommorethan621,000workersin2007tomorethan911,000 workersin2012.Asaresult,revenuesfromthishealthcareincreasedfrom$25.3billion in2007to$34.4billionin2012.Everycountrymustfindawaytohandlethe impendingcrisisofcaringforagingpopulations.Governmentsmustplandecades ahead,withnewmethodstobettermanagethesituation.Somecitiesarealready buildingage-friendlyhousingandotherinfrastructure.Forexample,Swedenhas implementedverylow-costapproachestocaringforelderlycitizens,whichareofferingextremelyhighqualityofcare.Inthesamecountry,mostelderlyhealthcareis fundedbymunicipaltaxesandgovernmentgrants.In2014whiletotalcostsforcare wereequivalentto$12.7billion,only4%ofthecostwasfinancedbypatientcharges. Privatizationofelderlycareisincreasing,allowingprivatecarecompaniestocontrol operations,whichnowprovidemorethan24%ofallelderlyin-homecare.Allrecipientsofcarecanchooseiftheywanttheircaretobeprovidedbypublicorprivate operators.
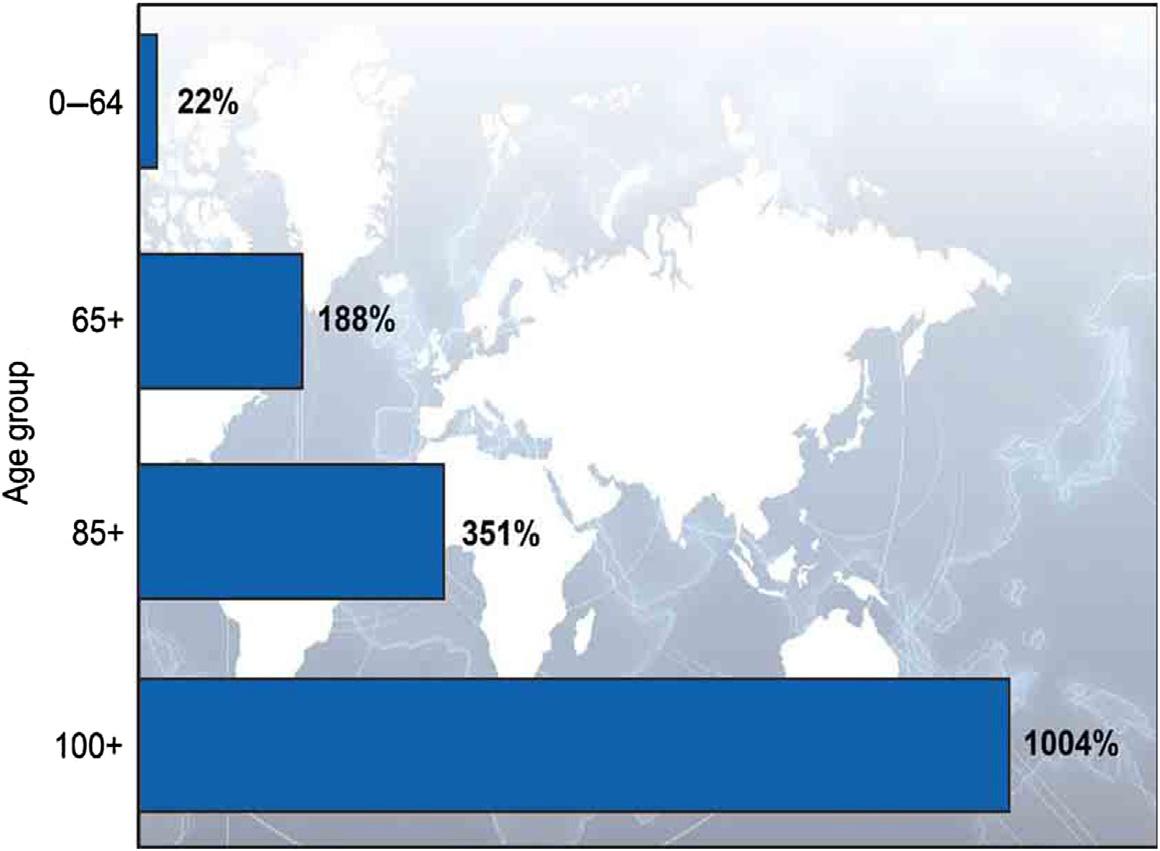
The “oldestold” (peopleaged85orolder)makeup8%oftheworld’selderly population,withtheterm elderly meaningage65orolder.Thisis12%inmoredevelopedcountriesand6%inlessdevelopedcountries.Inmanycountriesthe85-andoldergroupisthefastestgrowingpartofthepopulation.Globally,thisgroupis projectedtoincrease351%between2010and2050.Thisiscomparedtoa188%
increaseinthe65-and-oldergroup,and22%increaseinthepopulationunderage65. Peoplereaching100yearsofageareprojectedtoincreaseby10timesasmany between2010and2050.Ithasbeenestimatedthatoverthecourseofhumanhistory, oddsoflivinguptoage100haverisenfrom1ofevery20millionpeopleto onein every50people thisfigureisforfemalesinlow-mortalitycountriessuchasJapanand Sweden.Ofthepercentagechangeinworldpopulationbyageshownin Fig.1.3,the mostastoundingisthe100-and-olderage-group,witha 1004%increase
Focusonlifeexpectancy
Globally,peoplearelivinglongerandmoreproductivelivesthananytimepreviouslyinhistory.Theoldestaveragelifeexpectancyis83.7yearsinJapan.Thistakesintoaccountmales andfemalestoachievethe “average” figure.Usingsimilarmethods,Switzerlandand Singaporeranksecondandthird.TheUnitedKingdomisranked20th,andtheUnitedStates isranked31st(at79.3years).ThethreeworstaveragelifeexpectanciesareSierraLeone (50.1years),Angola(52.4years),andtheCentralAfricanRepublic(52.5years).
Distributionofthyroiddisordersbygenderandage
Thedistributionofthyroiddisordersbygenderandagevarieswitheachtypeofdisorder.Forexample,women,overall,havemorethyroiddisorders,butoften,theeffectsof thesedisorderswidelydiffer.Womenaremorelikelythanmentohaveiodinedeficiency(seeChapter3:Iodineandthyroidhormones).Whilewomendevelopgoiters moreoften,theeffectsofthemdifferinthatthemenstrualcycleisaffected,whilemale
Figure1.3 Percentagechangeinworldpopulationbyage. WHO’sGlobalHealthAgingPDF.
spermproductionisnot.Distributionof goiter isbasedonlevelsofiodinedeficiency(see Chapter4:Iodinedeficiencyandgoiter).Inseverelyiodine-deficientareas,prevalence maybeashighas80%,withfourtimesashigherdistributioninwomenthaninmen. Overallincidencedeclineswithage. Sporadicgoiter isseventoninetimesmorecommon infemales,withhighestincidenceatpubertyorinyoungadulthood. Nontoxicmultinodulargoiter and endemicgoiter,however,havethesamedistributionbetweenfemalesand males.However,theyaffectolderpeople,mostlyalongwith thyroidnodules and hypothyroidism (seeChapter5:Hypothyroidism).Actually,hypothyroidismis10timesmore commoninfemales,usuallyafterage40.About10%ofolderfemalesareaffected. Hypothyroidismalsoaffectsoneoutofevery3500 4000births.
Hyperthyroidism occursinpeoplemorethantheageof60yearsinupto15%of casesandaffects1in500pregnancies(seeChapter6:Hyperthyroidism).Again, femalesareaffectedmoreoften,mostcommonlywhentheyareintheirthirdand fourthdecades.Globally,hyperthyroidismis0.5% 2%moreprevalentinwomen.Itis also0.4% 2%prevalentinelderlypeople.Overthyperthyroidismaffects0.4ofevery 1000womenand0.1ofevery1000men,withalargevariancebetweenagesregardingsusceptibility.Theprevalenceofoverthyperthyroidisminpeopleaged65yearsor olderhasbeendocumentedasbeing0.33%ofthepopulation.Incidenceofovert hyperthyroidismduringpregnancyhasbeenestimatedbetween0.1%and0.4%ofthe population.Prevalenceofpreviouslyunsuspectedhyperthyroidismwas0.5%in women,andundetectableinmen.IntheUnitedStatesalone,thehighestincidenceof overthyperthyroidism,byage,is1.01ofevery1000peopleaged65andolder.The 56 64age-group,with0.78per1000affected,followsthis.Hyperthyroidismislowestinchildrenbetween12and17yearsofage,at0.26per1000affected.
Incidenceof Hashimoto’sthyroiditis increaseswithaging(seeChapter7:Thyroiditis andGraves’ disease).Itaffectsabout5%oftheglobalpopulation,usuallybetweenages 30and60,andis8 15timesmorecommoninfemales.Whenmenareaffected,they areusuallyalsoinmiddleage.Subacutethyroiditisisuncommon,affectingbothsexesof allages.However,itaffectswomenthreetofivetimesmoreoftenthanmen.Itismost commoninmiddleage,followedbyyoungadulthood,decreasinginfrequencywith increasedage.Infectiousthyroiditisisveryrare,mostcommonlyseeninchildrenand youngadults,betweenages20and40.Childrenareaffected92%ofthetimeandthe other8%areyoungadults.Malesandfemalesareaffectedatthesamerates.Another rareform, Riedel’sthyroiditis,affectsfemalesfivetimesmoreoftenthanmales,usually between30and60yearsofage,withpeakincidenceinthefifthdecadeoflife.
Graves’ disease iseighttimesmorecommoninfemales,usuallybeginningbetween ages20and40,withasecondcommononsetbetween40and60(seeChapter7: ThyroiditisandGraves’ disease).However,itcandevelopanytimeduringlife.An interestingfactisthatGraves’ diseaseaffectsAfrican-Americanmalesabout2.5times moreoftenthanothermalesandaffectsfemalesabouttwiceasoftenasotherfemales.
AsianorPacificIslanderwomenhavea78%increasedriskcomparedtoCaucasian women,whereasmenhaveathreetimeshigherriskthanCaucasianmen.Age-specific ratesrevealthatwomenhavethehighestincidencebetween30and34yearsofage, followedby35 39,then25 29.Thelowestincidenceinfemalesisbetweenages15 and19.Inmales,Graves’ diseaseismostprevalentbetweenages25and49,andleast prevalentbetweenages70and75.
Inmiddle-agedandelderlypeople,thyroidnodulesmayprogressto adenomas in about5%ofcases(seeChapter10:Globalepidemiologyofthyroidneoplasms). However,studieshaverevealedthatnodulesarepresentinabout50%ofolderadults. Morethan75%of thyroidcancer casesoccurinfemales,mostlybetweenages20and 55.However,amajorityofnewcasesoccurafterage45.Actually,thehigherpercentagesareinthe45 54age-group.Thelowestpercentagesareforpeopleyounger than20orolderthan84.
Focusongender,age,andthyroiddisorders
Ingeneral,womenaremuchmorelikelytodevelopdisordersofthyroidthanmen.For example,womenarethreetimesmorelikelytogetthyroidcancer.Thyroiddiseasesarevery commoninmiddle-agedandolderadults.
Population-basedmodelsofthyroiddisorders
Invariouspopulations,multinodulargoiterornodularthyroidenlargementaffectsas manyas12%ofadults.AccordingtotheAmericanThyroidAssociation,in2019, morethan12%oftheUSpopulationwilldevelopathyroidcondition.Agoiterprevalenceof5%orhigherinschool-agechildrenindicatesiodinedeficiency.In Germany,thyroidnoduleslargerthan1cmwerefoundin12%ofthepopulation. Whentherewasonlyonepalpablenodule,20% 48%hadadditionalnodulesdetected byultrasound.Between1%and10%ofadultsintheUnitedStateshavesolitarythyroidnodules,butinendemicgoitrousregions,ratesaremuchhigher.Thyroidnodules arisingfromthyroidfolliclesarerelativelycommon,and90% 95%arebenign. However,thereisahigherrateofthyroidnodulesinareaswithsignificantradiation exposure.
About33%oftheglobalpopulationlivesinareasofiodinedeficiency,which increaseschancesforthedevelopmentofhypothyroidism.IntheUnitedStates,about 4.6%ofthepopulationaged12yearsandolderhashypothyroidism,butusually,these casesaremild.Thesixpopulationsathighestriskforhypothyroidismincludeolder patients,thosewithischemicheartdisease,pregnantwomen,patientswithpersistent symptomsevenwithproperdosesoflevothyroxine,thosewithsubclinicalhypothyroidism,andthosesuspectedofhavingmyxedemacoma. Celiacdisease patientsmay
havea4.4timesincreasedriskforhypothyroidismthanthegeneralpopulation. Hyperthyroidismisalsovariedinpopulations,basedoniodinesufficiency.Primary hyperthyroidismisincreasinginvariousareasoftheworld,suchasScotlandand Denmark.IntheUnitedStates,about1.2%ofthepopulationhashyperthyroidism, whichisslightlymorethan1ofevery100people.
CaucasiansdevelopHashimoto’sthyroiditismorethananyotherethnicgroup,by 67% 78%.Theotherformsofthyroiditisarenotsignificantlyhigherinanyspecific population.However,Graves’ diseaseretainsamuchhighersignificanceinAfrican Americans,Asians,andPacificIslandersthaninCaucasiansorotherpopulations. ThyroidcanceraffectsmaleswhoareCaucasianornon-Hispanicatthehighestrates (7.8outofevery100,000),andatthelowestratesinAfricanAmericans(3.8outof every100,000).Forwomen,thyroidcanceraffects22.8ofevery100,000Caucasians, justslightlymorethan22.1ofevery100,000non-Hispanics,andonlyaffects13.4of every100,000AfricanAmericans.
Globalprevalenceofthyroiddisorders
Globally,approximately200millionpeoplehavethyroiddisordersofvarioustypes, withmorethan50%remainingundiagnosed.Manycasesareundiagnosedbecause symptomsmaybeeasilymistakenfordepression,menopause,orbecauseofobesity. Thismeansthatthyroiddiseaseisacurrent,silentepidemic.Itisestimated,forexample,thatgoitersaffectupto200millionofthe800millionpeoplewhohaveiodine deficiency.Thyroidnodulesareextremelycommon,withupto50%ofallindividuals havingatleastonenodulebytheageof60years.About5%oftheglobalpopulation hashypothyroidism,andabout2%hashyperthyroidism.Thyroiditishasbeenseenin asmanyas12.5%ofpopulationsinvariouscountries.Graves’ diseaseaffects2% 5% offemalesand0.2% 0.7%ofmalesglobally.Therearemorethan560,000newcases ofthyroidcancerreportedeveryyeararoundtheworld.
InEuropethemeanprevalenceofundiagnosedthyroiddysfunctionwas6.71%of thepopulation.Prevalenceofundiagnosedhypothyroidismwas4.94%andofundiagnosedhyperthyroidismwas1.72%.Themeanprevalenceoftotalthyroiddysfunction inEuropewas3.82%.Theprevalenceofpreviouslyknownandundiagnosedhypothyroidismwas3.05%andhyperthyroidismwas0.75%.IntheWickhamstudyfrom theUnitedKingdom,16%ofthepopulationhadgoiter.IntheUnitedStatesthe prevalenceofthyroiddisordersisinmorethan25millionpeople.Thisisabout1of every13people,or7.35%.Therearemorethan13millionestimatedundiagnosed thyroiddisordersinthiscountry,whichisaboutoneofevery25,or4.78%ofthe population.Oneineightwomenhasariskforthyroiddisordersduringlife.
Focusoncongenitalhypothyroidism
In2010astudyreportedtheincidenceofcongenitalhypothyroidismat100%higherin HispanicnewbornsthaninCaucasiannewborns,and44%higherinnewbornsofAsianor NativeHawaiian/PacificIslanderbackgrounds.Theincidencewasalso30%lowerinAfricanAmericannewbornsthaninCaucasians.
Globalepidemiologyofthyroiddisorders
TheincidenceoftotalthyroiddysfunctioninEuropeis259per100,000annually, withaclearfemalepreponderanceof420per100,000toonly85per100,000men. Morethan90%ofcasesofgoiterarelinkedtoiodinedeficiency,withmanymore womenaffectedthanmen.Thyroidnodulesdetectablebypalpationaffect2% 6%of thepopulation.However,ultrasounddetectsthyroidnodulesin19% 35%,and autopsiesrevealupto65%ofpatientshavingthem.Incidencerateofhypothyroidism was226per100,000annuallyoverall.Ofthisnumber,370per100,000womenand 72per100,000menwereaffected.Theoverallincidencerateofhyperthyroidismwas 51per100,000annually.Ofthisnumber,82per100,000womenand16per100,000 menwereaffected.Thyroiditisisthreetofivetimesmorecommoninwomen,globally.Itismostcommonincertainregionswherethesummerandfallweatherismore severe.Graves’ diseaseincidenceisabout0.5%ofpeople,being7.5timesmorecommoninwomenthaninmen.
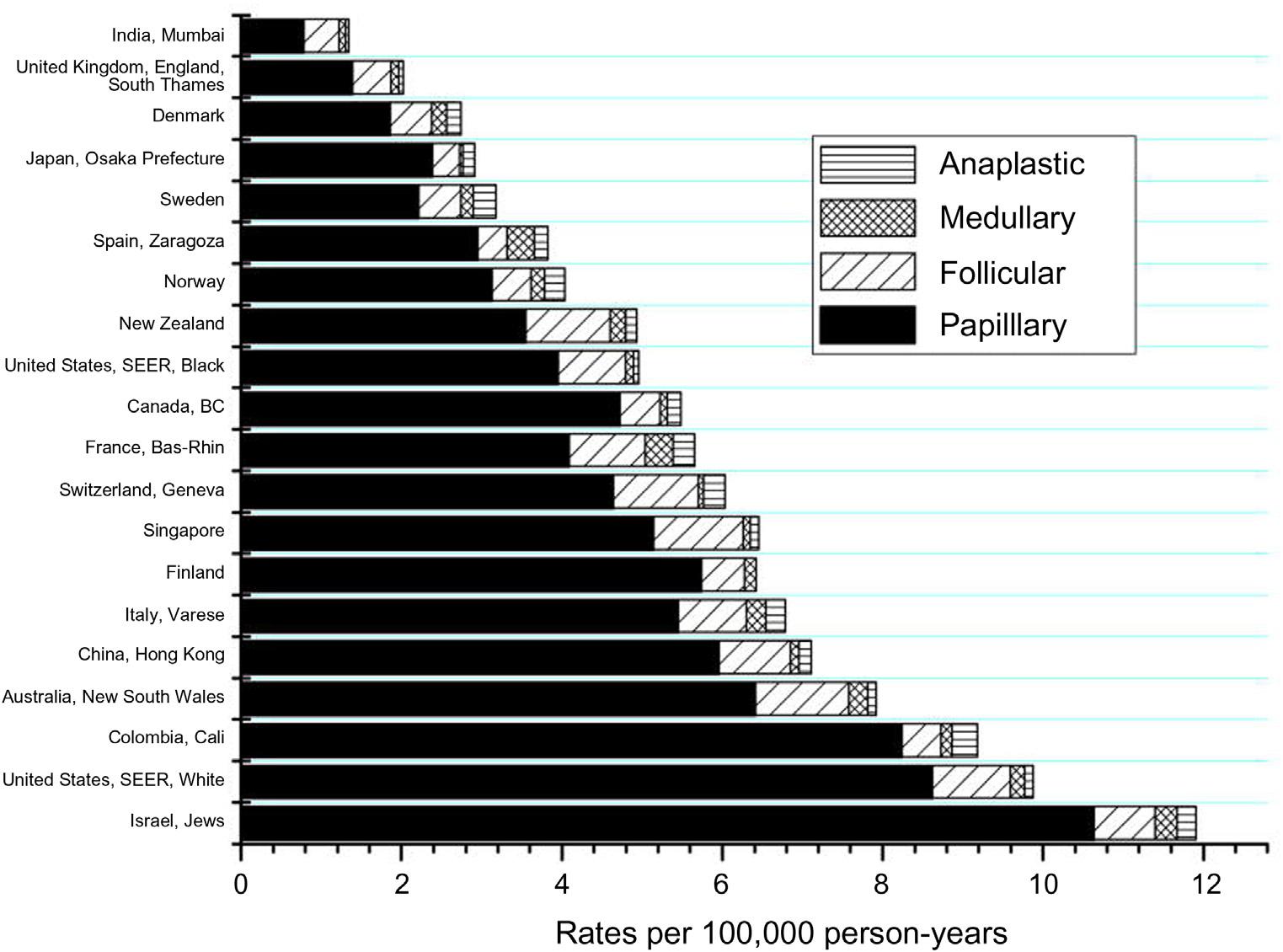
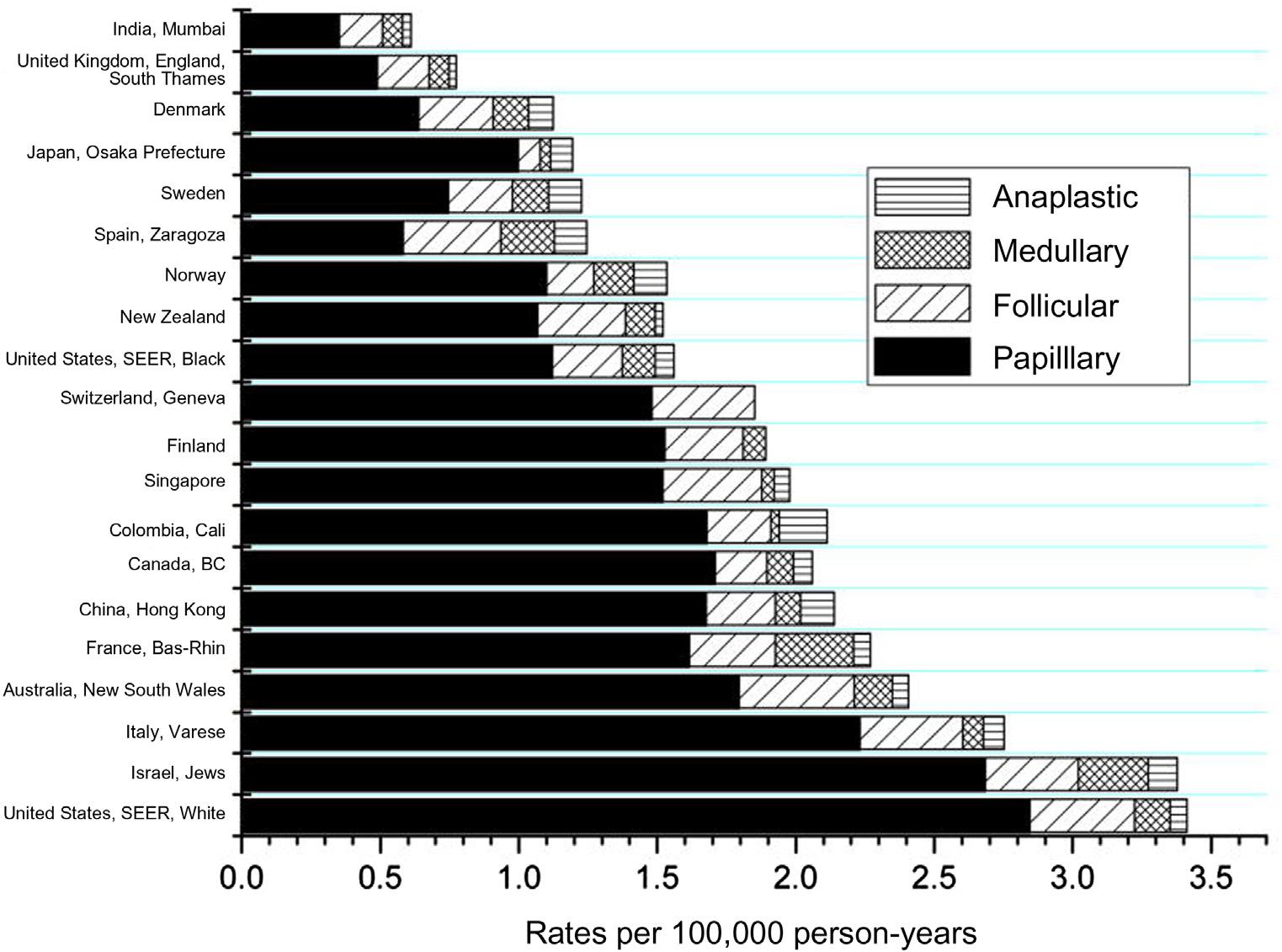
Thyroidcancerincidenceis3.2millionpeoplearoundtheworld mostlywomen. Ratesofthyroidcancer,ina30-yearstudy(between1972and2002),haverevealed thatthediseaseisincreasinginmostcountries,exceptforSweden,inwhichitisactuallydecreasing.Overthestudyperiodtheaverageincreasewasabout67%infemales and48%inmales.InSweden,therewasanapproximate18%decrease,betweenboth genders.Generally,thyroidcanceraffectsthreetimesmorewomenthanmen. Figs.1.4and1.5 showincidenceratesofthyroidcancerforfemalesandmales,respectively,invariouscountriesbetween1998and2002.
Globalpreventionofthyroiddisorders
Globalpreventionofthyroiddisordersisamostlyattainablegoalbutinvolvesgovernmentaleffortstoreduceriskfactors.Correctingiodinedeficiencyisoftheutmost importanceinpreventingthyroiddisorders.Thisoffersimprovedqualityoflifeand survivalrates,eliminationofcretinism(seeChapter5:Hypothyroidism),andlesser degreesofneuromotororcognitivedysfunction.Iodineissparselydistributedonthe Earth’ssurface.Thereforeiodinedeficiencydisordershavebeenextremelycommonin manypopulations.TheybecamemuchlessprevalentintheUnitedStates,for
Figure1.4 Incidenceratesofthyroidcancerforfemales(per100,000person-years),agestandardized,between1998and2002. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2788231/ .
example,iodinewasintroducedintodietarysalt.Theeffortsofpreviousdecadeshave madeextensiveadvancesineliminatingiodinedeficiencythroughuniversalsalt iodization.Thekeytopreventionismonitoringoftheiodinesupplyineacharea,andthe impactofthepreventionprogramuponthetargetpopulation.Thisincludesmonitoringoffactories,importers,retailers,andevenconsumersregardingappropriatelevels ofdietaryiodine.
Anotherdietarypreventionmethodiseatinglesssoy-basedfoods.Thoughsoyis goodforoverallhealth,inextremelylargeamounts,itmaybedetrimentaltothyroidfunction.Ifsomeoneistakinglevothyroxine,itisimportanttowaitfor4hours beforeconsuminganysoy-basedfoods,sincesoy,alongwithcalcium,fiber,and iron,interfereswiththeabsorptionoflevothyroxine.Abstainingfromsmokingisa definitepreventionmethod.Cigarettesmokecontainstoxinssuchasthiocyanate, whichdisruptsiodineuptakeandblocksproductionofthyroidhormones. Generally,smokingcauseselevatedthyroxinelevelsandaslightdecreaseinTSH levels.CigarettesmokersaremorelikelytodevelopGraves ’ diseaseandits complications.
Figure1.5 Incidenceratesofthyroidcancerformales(per100,000person-years),agestandardized,between1998and2002. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2788231/
Selenium supplementsaresuggestedaspreventivemeasures.Seleniumispredominantlyconcentratedinthebodyinsidethethyroid.Seleniumsupplementsalsohelp boosttheimmunesystemandlower thyroperoxidase antibodiesinpeoplewith Hashimoto ’sdiseaseaswellasinpregnantwomen.Thisdecreasessymptomsof hypothyroidism.Inpregnantwomen,seleniumsupplementationalsodecreases chancesofdevelopingpermanentpostpartumthyroiditis.Sincethebodyabsorbsthe organicformofselenium,knownasselenomethionine,betterthantheinorganic form(sodiumselenite),itisbettertouseselenomethionineasasupplement.When receivingX-rays,patientsshouldrequesta thyroid-protectingcollar.ThisisespeciallytrueforX-raysofthemouth,head,neck,spine,orchest.Thethyroidcollaris heavyandlinedwithlead.
Periodically,theneckshouldbeself-checkedforlumps,bumps,orswellingofthe thyroid.Additionalmethodsofpreventingthyroiddisordersincludeavoidingdrinking wellwater,whichmaycontainperchlorates.Theseareodorlessandcolorlesssaltsdissolvedinwellwater.Commercially,theyareusedtomanufacturefireworks,explosives,androcketmotors.Anyonedevelopingceliacdisease,whichisanautoimmune
condition,isthreetimesmorelikelytodevelopHashimoto’sthyroiditisorGraves’ disease.Celiacdiseasecausespoorabsorptionofiodineandselenium,triggeringthyroid dysfunction.Overall,regularcheckupsbyaphysicianareimportanttomonitorthyroidandoverallhealth,inordertopreventseriousdiseasesfromdeveloping.
Preventionalsoinvolvestheextremelyyoung.AneonatalTSHscreeningprogram, universallyapplied,wouldgoalongwayasapreventivemeasureforthyroiddisorders. Newbornscreening,forexample,forcongenitalhypothyroidism,isamajorachievementthathasresolvedthisconditioninmanydevelopedcountries.However,itisstill aprobleminmanydevelopingcountries.Thismustbereversed,becausehypothyroidisminthenewbornperiodisnearlyalwaysoverlooked,delayingdiagnosis,andleading tomentalretardation.ThefirstscreeningprogramwasperformedinCanadain1972, whichdetectedsevenhypothyroidinfantsoutof47,000screenednewbornsovera 3-yearperiod.Thefocusofnewbornscreeningprogramsmustbetodetectallcases withthyroiddiseaseasearlyaspossible.Otherconditionsthatmaybescreenedfor include hypothyroxinemia (lowT4andnormalTSH),isolated hyperthyrotropinemia (normalT4andelevatedTSH),andlowT4withelevatedTSH.
Theiodizationofbreadandevenwaterhasbeenusedincountries,suchasThe Netherlands,Russia,Tasmania,Thailand,Indonesia,Italy,andChina.Itistimefor governmentstoimprovetheirpolicies,programs,technologies,andfinancialsupport concerningiodinedeficiency.Therearefiveguidingprinciplesregardingefforts towarduniversalsaltiodization,whichincludeasecurepoliticalcommitment,formationofpartnershipsandcoalitions,availabilityofadequatelyiodizedsalt,bettermonitoringsystems,andmaintenanceofeducationandcommunication.TheWorldBank estimatesthateverydollardedicatedtopreventionofiodinedeficiencydisordersyields againof$28inproductivity.Thisshowsthattheeliminationofiodinedeficiencyis alsooneoftheworld’smostcost-effectiveprograminterventions.
Focusonincreasingcasesofthyroidcancer
Thyroidcancerisoneofthefewtypesofcancerthathasincreasedinincidenceratesover thepastthreedecades.Itoccursinallage-groupsfromchildrenthroughtheelderly.Nearly allofthisincreaseinvolvespapillarythyroidcarcinoma.Thereasonforthisisnotclear,but environmentalfactorsareprobablyhighlysignificant,includingreleasesofradiationdueto nuclearreactoraccidents.
Globaldeathratesfromthyroiddisorders
Alargeamountofstudiesconcerningglobaldeathratesfromthyroiddisordershave givendifferentresults.Overtandsubclinicalhyperthyroidism,forexample,isassociatedwithanincreasedriskof all-causemortality,ordeathfrommajoradversecardiovascularevents,andheartfailure.Isolatedheartattackandstrokeriskswerenotincreased