CONTRIBUTORS
GonzaloAllo
DepartmentofEndocrinology,HospitalUniversitario 12deOctubre,Madrid,Spain
CristinaAlonso-Bouzón
GeriatricDepartment,HospitalUniversitariode Getafe,UniversidadEuropeadeMadrid, CoordinatorofCIBERFES(CIBERoffrailtyand HealthyAgeing),Madrid,Spain
AnaAnuashvili
NationalNutritionCentre,Tbilisi,Georgia TheClinicalCenterforDevelopmentofNephrology, Tbilisi,Georgia
AlejandroAyala
DivisionofEndocrinology,MillerSchoolofMedicine, UniversityofMiami,Miami,FL,UnitedStates
MarcR.Blackman
WashingtonDCVeteransAdministrationMedical Center,GeorgetownUniversitySchoolofMedicine, GeorgeWashingtonUniversitySchoolofMedicine, Washington,DC,UnitedStates
RaffaeleCarraro
DepartmentofEndocrinologyandInstitutode InvestigaciónSanitariadelHospitalUniversitario LaPrincesa,Madrid,Spain DepartmentofMedicine,AutonomousUniversity ofMadrid,Madrid,Spain
CarlosCarrera-Boada
DepartmentofEndocrinology,CaracasClinical Hospital,Caracas,Venezuela
EmilianoCorpas
HLAandHospitalUniversitariodeGuadalajara, Guadalajara,Spain FacultyofMedicine,UniversityofAlcalá,Madrid, Spain
RicardoCorrea DivisionofEndocrinology,Veterans AdministrationMedicalCenter,Universityof ArizonaCollegeofMedicine,Phoenix,AZ, UnitedStates
MeriDavitadze
Georgian-AmericanFamilyMedicineClinic “Medical House”,Tbilisi,Georgia
VishnuGarla
DivisionofEndocrinology,UniversityofMississippi MedicalCenter,Jackson,MS,UnitedStates
JaredGollie
WashingtonDCVeteransAdministrationMedical Center,GeorgeWashingtonUniversitySchoolof MedicineandHealthSciences,Washington,DC, UnitedStates
RicardoGómez-Huelgas DepartmentofInternalMedicine,HospitalCarlos HayadeMálaga,FacultyofMedicine,Universityof Málaga,Málaga,Spain
S.MitchellHarman DivisionofEndocrinology,VeteransAdministration MedicalCenter,UniversityofArizonaCollegeof Medicine,Phoenix,AZ,UnitedStates
FedericoHawkins ResearchInstitutei+12,HospitalUniversitario12de Octubre,FacultyofMedicine,Complutense University,Madrid,Spain
StephanieKristofic VeteransAdministrationMedicalCenter,Phoenix,AZ, UnitedStates
ÁlvaroLarrad-Jimenez EndocrineSurgery,UnidaddeMedicinayCirugía Endocrino-Metabólica,HospitalNuestraSeñora delRosario,Madrid,Spain
MingLi DivisionofEndocrinology,VeteransAdministration MedicalCenter,UniversityofArizonaCollegeof Medicine,Phoenix,AZ,UnitedStates
MaríaDoloresLópez-Carmona DepartmentofInternalMedicine,HospitalCarlos HayadeMálaga,FacultyofMedicine,Universityof Málaga,Málaga,Spain
MariMalazonia
NationalNutritionCentre,Tbilisi,Georgia DavidTvildianiMedicalUniversity,Tbilisi,Georgia Georgian-AmericanUniversity,Tbilisi,Georgia
DavidMales DepartmentofEndocrinology,HospitalUniversitario 12deOctubre,Madrid,Spain
AntonioMartin-Duce EndocrinologySurgery,HospitalNISA,Madrid, UniversityofAlcalá,Madrid,Spain
LauraMola
DepartmentofEndocrinology,HospitalUniversitario 12deOctubre,Madrid,Spain
RamfisNieto-Martinez
MiamiVeteransAffairsMedicalCenter,Geriatric Research,EducationandClinicalCenter(GRECC), MiamiVAHealthcareSystem,Miami,FL, UnitedStates
DepartmentofGlobalHealthandPopulation,Harvard THChanSchoolofPublicHealth,Harvard University,Boston,MA,UnitedStates FoundationforClinic,PublicHealth,and EpidemiologyResearchinVenezuela(FISPEVEN), Caracas,Venezuela
ConcepciónPeiró DepartmentofPharmacologyandTherapeutics, AutonomousUniversityofMadrid,Madrid,Spain InstitutodeInvestigaciónSanitariadelHospital UniversitarioLaPaz(IdiPAZ),Madrid,Spain
PeterReaven
DivisionofEndocrinology,VeteransAdministration MedicalCenter,UniversityofArizonaCollegeof Medicine,Phoenix,AZ,UnitedStates
LeocadioRodríguez-Mañas
GeriatricDepartment,HospitalUniversitariode Getafe,UniversidadEuropeadeMadrid, CoordinatorofCIBERFES(CIBERoffrailtyand HealthyAgeing),Madrid,Spain
CassandraRoeca UniversityofColorado,DepartmentofObstetrics& Gynecology,Aurora,CO,UnitedStates
TaniaRomacho DepartmentofPharmacologyandTherapeutics, AutonomousUniversityofMadrid,Madrid, Spain
InstitutodeInvestigaciónSanitariadel HospitalUniversitarioLaPaz(IdiPAZ),Madrid, Spain
AntonioRuiz-Torres FacultyofMedicine,AutonomousUniversityof Madrid,Madrid,Spain
CarlosF.Sánchez-Ferrer DepartmentofPharmacologyandTherapeutics, AutonomousUniversityofMadrid,Madrid, Spain
InstitutodeInvestigaciónSanitariadelHospital UniversitarioLaPaz(IdiPAZ),Madrid, Spain
FrancoSánchez-Franco CentrodeEndocrinología,NutriciónyDiabetes, Madrid,Spain
NanetteSantoro UniversityofColorado,DepartmentofObstetrics& Gynecology,Aurora,CO,UnitedStates
ÁlvaroSerrano-Pascual UrologicalLaparoscopicSurgery,Complejo HospitalarioRuberJuanBravo,Madrid,Spain
SonieSunny
DivisionofEndocrinology,VeteransAdministration MedicalCenter,Phoenix,AZ,UnitedStates
NatiaVashakmadze
DavidTvildianiMedicalUniversity,Tbilisi,Georgia Georgian-AmericanUniversity,Tbilisi, Georgia
KaryneVinales
DivisionofEndocrinology,VeteransAdministration MedicalCenter,UniversityofArizonaCollegeof Medicine,Phoenix,AZ,UnitedStates
FabianWayar
CentroMedicoCurare,ScientificSocietyGroup, LaPaz,Bolivia
ACKNOWLEDGMENTS
Editor
Dr.EmilianoCorpas wishestothankhiswifeTrinidadandhisdaughterSandrafortheirlove, unwaveringsupport,andendlesspatience.Healsostateshisappreciationtoallstaffmembersof theEndocrinologyDivisionofthePhoenixVeteransAdministrationMedicalCenterfortheir professionalcollaboration,andexpresseswarmgratitudetoDrs.RicardoCorrea,CarolinaChen, andKaryneVinales,andDarrenKristoficandStephanieKristoficRN,fortheirhospitalityand friendship.Theparticipation,support,andinputofsomanycolleaguesandpersonsinvolvedinthis book,especiallyfromElsevier,areverymuchappreciated.Hewouldliketoacknowledgeas wellthebrilliantcontributionsandadviceofhislong-termfriends,colleagues,andauthors, Drs.MarcR.Blackman,S.MitchellHarman,ÁlvaroLarrad-Jim enez,FrancoSánchez-Franco, andAntonioRuiz-Torres,andthepaintingsonthebookcoverscreatedbyhisfriend,Antonio HerasVillanueva.
AssociateEditors
Dr.MarcR.Blackman wishestothankhiswife,Linda,forherunstintingsupportand endlesspatienceduringthewritingandeditingprocess.Hewouldalsoliketothankhislong-term friendsandcolleagues,Dr.EmilianoCorpas,forhisinspiringandtirelesseffortsinbringingthis bookfromconcepttoreality;Dr.S.Mitchell(Mitch)Harman,forsharinghisdeepknowledgeand wisdom;Drs.RicardoCorreaandAntonioRuiz-Torres,fortheirwritingandeditorialexpertise;all themanycoauthors,fortheirexpertandinformativecontributions.Hewouldalsoliketothankthe Elsevierstafffortheirexceptionalprofessionalismandhelpfulness;andallpatientswithagerelatedendocrinologicalandmetabolicdisordersaswellasthehealthproviderswhocarefor them,towhomthisbookisdedicated.
Dr.RicardoCorrea firstwantstothankGodforgivinghimthestrengthtoparticipateinthis amazingpieceofartandmedicine.ThankstohiswifeCarolinaandchildren(Matthewand Elizabeth)fortheirsupport,cheering,andforthetimethathewasnotabletospendwiththem. Thankstohismentor,Dr.Harman,forbelievinginhim,andtoDr.Corpasfortrustinghimwiththis bigprojectandforbecomingafriendandfamilymember.SpecialthankstoStephanieKristofic, RN,andDr.KaryneVinalesforalwaysbeingwillingtohelp,andtoalltheendocrinefellows (Ghada,Kelvin,Matthew,Mike,andSonie)forservingastheinspirationforthisbook.Teachingthe nextgenerationofendocrinologistsandfocusingonendocrinologyintheelderlygiveusthe strengthtocontinue.
Dr.S.MitchellHarman wouldliketoacknowledgetheunswervingsupportofhiswife Carolwho “keptthehomefiresburning” duringthewritingandeditingofhischaptersaswellas theinsightfulcollaborationofhislong-termpersonalandprofessionalfriendandcoauthor, Dr.MarcR.Blackman;thesharedclinicalandlinguisticinsightsoftheenergeticandenthusiastic Dr.RicardoCorrea;andmostofallthevisionandinspirationofhisdearcolleague,Professor EmilianoCorpas,withoutwhoselifetimededicationtotheexpansionofknowledgein endocrinologythiswonderfulopuswouldneverhaveseenthelightofday.
Dr.AntonioRuiz-Torres wouldmainlyliketothankscientistsWalterBeier(Leipzig),Gerhard Hofecker(Vienna),andthelateBernhardStrehler(UnitedStates),whosebasicinvestigation contributedtoabetterunderstandingoftherelationshipsbetweenclinicalmanifestationsandthe agingprocess,alsoinendocrinology.Dr.Ruiz-Torres’ contributiontothisbookisbasedonthe resultsandtheoriesofthosebasicresearchers.Healsoexpresseshisthankstotheassociate editors,especiallytoeditorDr.EmilianoCorpasforhisidealisticengagement,dedication,andhard worktomakethisbook.
BASICPRINCIPLESOFTHEAGING
PROCESSWITHENDOCRINEAND NUTRITIONALIMPLICATIONS, AGINGANDDISEASEIN ENDOCRINOLOGY
AntonioRuiz-Torres a,EmilianoCorpas b,c,RicardoCorrea d,Marc R.Blackman e,andS.MitchellHarman d aFacultyofMedicine,AutonomousUniversityofMadrid,Madrid,Spain bHLAandHospitalUniversitariodeGuadalajara,Guadalajara,Spain cFacultyofMedicine,UniversityofAlcalá,Madrid,Spain dDivisionof Endocrinology,VeteransAdministrationMedicalCenter,Universityof ArizonaCollegeofMedicine,Phoenix,AZ,UnitedStates eWashington DCVeteransAdministrationMedicalCenter,GeorgetownUniversity SchoolofMedicine,GeorgeWashingtonUniversitySchoolofMedicine, Washington,DC,UnitedStates
CHAPTEROUTLINE
INTRODUCTION2 WhatIsAging?2
SenescentCellsandSenolysis2
BASICPRINCIPLESOFTHEAGINGPROCESS WITHENDOCRINEANDNUTRITIONAL IMPLICATION3
GROWTHVELOCITYASDETERMINANTOF LIFESPANPOTENTIAL4
NUTRITIONALINFLUENCEONTHERATEOF AGING5
WEARANDREGULATION:TWOMECHANISMS THATDETERMINETHEAGINGPROCESS5
ImportanceofEndocrineSystem5
WearRegulation.ItsImportancefortheCourse ofAging6
PROBLEMSANDRISKSOFHORMONAL TREATMENTOFTHEAGINGPROCESS7
THEFALLACYOFHORMONAL “REPLACEMENT"AS"ANTIAGING MEDICINE"9
AGINGANDDISEASEIN ENDOCRINOLOGY9
SUMMARYOFPHYSIOLOGICALAGINGAND ENDOCRINESYSTEM9
ENDOCRINOPATHIESINADVANCEDAGE. CHARACTERISTICSANDCONSIDERATIONS FORDIAGNOSISANDTHERAPY10
BIBLIOGRAPHICALREFERENCES11
INTRODUCTION
WHAT IS AGING?
• Agingisduetoentropy,thenaturalprogressiontowarddisorder,andrandomness inanysystem
• Everythingages:Bothnonlivingobjectsandlivingorganisms
• Isolatedsystemscanachievealocalreversalofentropybyusingenergyfromoutside thesystem,butonlyatthecostofgreaterchaosinthelargerenvironment
• Biologicalagingis:
• Aprogressivedegradationoffunctionandcoordinationofinternalprocessesleading todiminutionoffitnessoftheorganism
• Thenetoutcomeofthebalancebetweenprocessesofdamageandself-repair/ regeneration
• Agingisheterogeneous
• Differentspeciesageatdifferentrates
• Individualsofthesamespeciesageatdifferentrates
• Systemswithinanindividualageatdifferentrates
• Specifictheoriesregardingtheagingprocessinclude:
• Accumulationofdamagetocellcomponents (proteins,lipidmembranes,andDNA) byfreeradicals
• Generatedbyinternalmetabolicprocesses
• Generatedbyexternalexposures(e.g.,cigarettesmoke)
• Opposedbyantioxidantenzymesand(possibly)nutrients
• Deteriorationofabilitytocarryoutcellreplacementandtissuerepair
• Stemcelldepletionorinactivation
• Immunosenescence (aspecialcaseofshiftincellpopulations)
• Telomereshorteningleadingtocellsenescence
• Accumulationofsenescentcellswhichproducetoxicby-products (including inflammatorycytokines)thathavedeleteriouseffects:
• Locallywithintissues(paracrine)
• Systemicallyduetocirculatingfactors(endocrine)
• Lossofsystemicbeneficial/growthfactors thatstimulategrowthandrepair (someofwhichareclassichormones)
• Allofthepreviouslydiscussedmayinteractto produceorganismalagingincluding changesinfunctionoftheendocrinesystems
SENESCENT CELLSAND SENOLYSIS
• Cellularsenescence
• Senescentcellsincreasewithaging inmice,monkeys,andhumansandinterventions thatincreaselifespaninanimals,includingcaloricrestrictionormutationsinthegrowth hormoneaxis,areassociatedwithdecreasedsenescentcellabundance
• Cellularsenescenceischaracterizedby:
• Irreversiblecell-cyclearrestaccompaniedbyasenescentassociatedsecretory phenotype(SASP)(e.g.,cytokines,tissue-damagingproteases,andothers)
• Senescentcellantiapoptoticpathways(SCAPs)whichmakecellsresistanttodeath
• Allthosemechanismsharmactivityoflocalnormalcellsthatdisplayincreased senescentcellnumbers
• Importantmarkersofsenescentcellsinclude: p16INK4A,p21CIP1,andSASPfactors (e.g.,IL-6,IL-8,monocytechemoattractantprotein-1,plasminogen-activatedinhibitor-1), andmanyothers
• Senescentcellsareassociatedandwithage-relatedpathologies inanimalmodels; experimentalstudieshaveshownthatyoungmilieuiscapableofprotectingagingtissues fromcellularsenescence
• Senolysis isbasedontargetingsenescentcellstobeeliminatedbygeneticor pharmacologicalapproaches
• Senolyticdrugs areagentsthatselectivelyinduceapoptosisofsenescentcellsactingon SCAPs.Importantfeaturestoconsider:
• Theseagentsexhibitahighdegreeofcell-typespecificity
• BriefdisruptionofSCAPscankillsenescentcells.Thussenolyticscouldtheoretically beadministeredintermittently
• Proof-of-principlestudies haveshowedthatselectivedepletionoreliminationof senescentcellscanpreventordelaychronicconditionsinanimalmodelsasfrailty, cardiacdysfunction,vascularhyporeactivityandcalcification,diabetesmellitus,liver steatosis,osteoporosis,vertebraldiskdegeneration,pulmonaryfibrosis,andradiationinduceddamage
• Earlyphaseclinicaltrialsareneeded toknowifchronicdiseasesasagrouporone-at-atimemightbepreventedordelayed,asinanimalmodelshasbeenobserved
• Cautionsmustbeemphasized,particularlyuntilclinicaltrialsarecompletedandthe potentialadverseeffectsofsenolyticdrugsareunderstoodfully
BASICPRINCIPLESOFTHEAGINGPROCESSWITH ENDOCRINEANDNUTRITIONALIMPLICATION
• Rateofregressionisequivalenttotherateofagingand dependsonthebalance oforganicwearandrepair.Glucocorticoidandotherhormonescanaffectthis balance
• Exogenousfactorsthatfavortheproductionoffreeradicals,suchastobaccoproducts aswellastheconsumptionofperoxidesappeartoacceleratetheagingratebyincreasing damagetotissuecomponents
• Theadministrationofdrugsorhormonesmayunbalance regulatoryprocessesand enhancetherateofaging
• Cholesterolisanimportantcomponentstabilizingcellmembranes andmayhelp protectagainstfreeradicals
• Thereisspeculationthatverylowcholesterollevelscouldaccelerateagingofmembranes
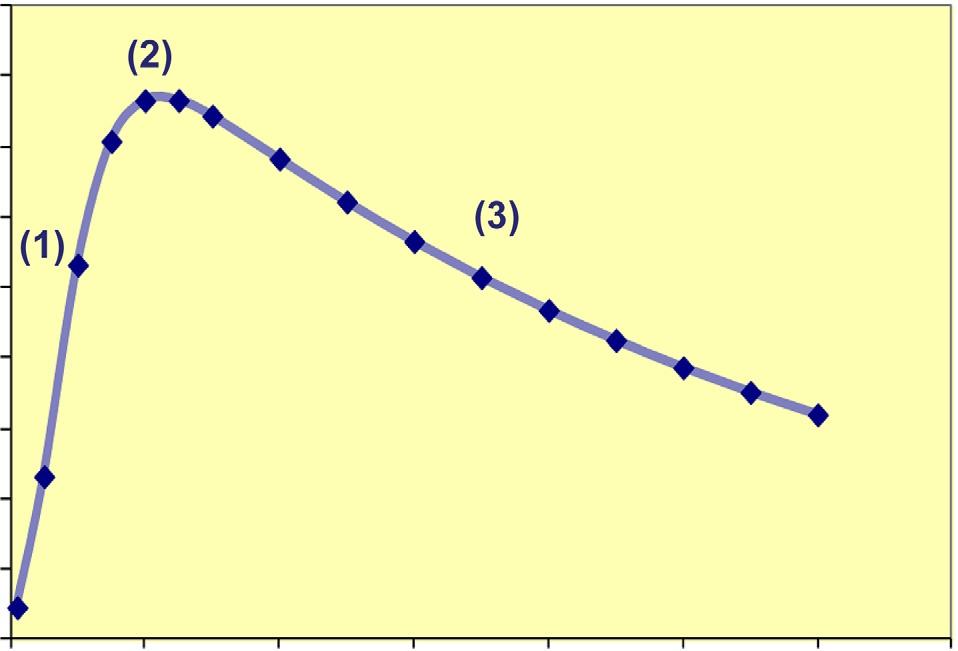
• Stagesofhumanlife arecomprisedbyaperiodofgrowthandincreasingvitality[(1)in thefollowingfigure]until20–24yearsofage,followedbyashortperiodofmaximum vitalityandreproductivecapacity(2),andfinallyaperiodoforganicregressionduring adulthoodwhichreflectsadecreasingvitality(3)untildeath
• Growthrateisinverselyproportionaltolifepotential,whichcouldexplainthelongevity ofGH-deficientandcastratedbeings,aswellashypophysectomizedanimals
• Theprocessoforganicandfunctionalregressionbegins,afterthestageof maximumvitality,ataround24yearsofage,whichextendsthroughouttheadult’slife andisidentifiedastheagingprocess,sothattheadultiscontinuouslysubjecttothat process
Periods of human life expressed as the course of vitality
Data from Beier W, Ruiz–Torres A. (1)Growingstage,(2)maximumvitalitystage,and(3)agingstage.Thecurveisrepresentedasamodel,usingfor k (growth rate)0.194,for μ 0.024,andfor α 0.0095.(ConceptofvitalityaccordingtoW.BeiermodifiedbyA.Ruiz-Torres.)
Themathematicalfunction vt ¼ exp(exp( kt )lnw0 β t )expressestheperiodsofhuman lifeinwhichparametersofgrowth(k),wear,andregulation(β )areinvolved(seepreviouspanel). β istheagingfactorwhosevalue β ¼ (μ α)resultsfromthesubtractionofthewear(μ)and regulation(α). w0 istheratioofmaximumstaturereached/statureatbirth.
GROWTHVELOCITYASDETERMINANTOFLIFESPAN POTENTIAL
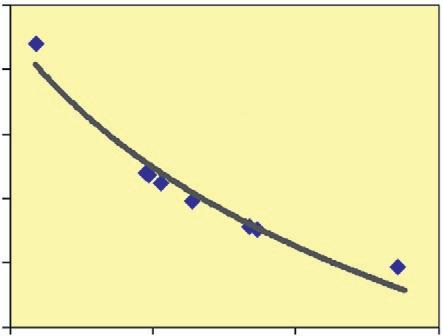
Thereisnoreductioninmaximumlifespanindwarfism;although,inthissample,anapparent inverserelationshipwiththeconstantofgrowthvelocityisdetected
GraphA: Inverserelationshipbetweengrowthvelocity(k),ontheabscissa,andaveragelifespan(T),ontheordinate,inasample ofpatientsaffectedbydwarfism. T ¼ 1/β (1/k)lnw0; k ¼ (1/tmw)•ln(lnwt/lnwm)reached);tmw:ageofmaximumgrowth; wt:statureatthatage;wm:máximumstature(Unpublisheddatafromauthor). TableB: Maximumstatureandcorresponding lifedurationcalculatedaccordingtoT.GHdeficiencyorlossofGHreceptorsisassociatedwithincreasedlifespan.
Ruiz –Torres A. (datos no publicados)
NUTRITIONALINFLUENCEONTHERATEOFAGING
• Slowestgrowthpredisposestolongevity. Asgraphshows,peoplefromplacesoflower economiclevelhavealsolowerstature,butpresenthighersurvivalrates(leftcolumn) thanthosewholiveintherichestareas(rightcolumn).Thereforeitseemsthatabetter dietenhancestheseculartrendofTannerreachinghigherstatures,butwithlower survival,thatistosay:
• Atahighereconomiclevels,betternutritionalstatusresultsingreaterstaturebut shorterlongevity
Data fromHolzerbergerM et al. Arch.GerontolGeriatr13:89-1001, 1991.
Survivaldataat70yearsofage,inrelationtoheightrecordedattheageofthemilitaryserviceinfourprovincesfromSpainwith ahigherpovertyindexcomparedwithotherfivericherprovinces,outofatotaloffifty(datafrom1858to1861tomilitary serviceand1910intherespectivesurvivingpopulation).
WEARANDREGULATION:TWOMECHANISMSTHAT DETERMINETHEAGINGPROCESS
IMPORTANCEOF ENDOCRINE SYSTEM
• Wearisthedeleteriousconsequenceof,forexample,freeradicalexposure. Thesynthesisofantioxidantenzymesappearstoaregulatoryoradaptiveresponsetothis influence
• Thereforewearwouldbethebasisforagingitselfandregulationthemechanism prolongingindividualsurvival
• Factorsgeneratingwearmaybeendogenousorexogenous.Forexample,both mitochondriaandcigarettesmokeproducefreeradicals.However,regulationismainly endogenous.Theendocrinesystemplaysanimportantroleinregulation.
SeeChapter14:BodyCompositionandMetabolicChangesWithAging
• Insulinoverproductionoccursinresponsetoincreasedperipheralinsulinresistance
• Adipogenesisinresponsetoinsulinincreasesinadvancedage,
• Maycontributetomaintenanceoffatmass,whichisimportantforsurvivalwhenfood isscarce
• Mayshortenlifespanduetometabolicsyndromewithconsequent inflammaging
• Itisofinteresttonotethatsupercentenarianstendtobeleanandmaintaininsulinsensitivity
• Thereforegreaterinsulinemiainadvancedagecouldbeeitherprotectiveordeleterious, dependingonenvironmentalfactors
Insulin resistance
Functionaladaptation ofbetacells
Compensatory hyperinsulinemia
Maintenanceof normoglycemia
Glucose intolerance Type2 diabetes Betacellfailure (insulindeficiency)
Regulatorymechanismsofinsulinresistance. Hyperinsulinemiamaycompensatewearcausedbylowerperipheralinsulin sensitivity(mainlyatmuscle).Whensecretorydefectsofinsulinappear,alsoduetoaging,whichcannotovercomeperipheral resistance,olderpeoplearepredisposedtodevelopglucoseintoleranceandtype2diabetes.
WEAR REGULATION.ITS IMPORTANCEFORTHE COURSEOF AGING
• Regulationofagingprocessconsistsinadaptingtothedeleteriousconsequencesofwear
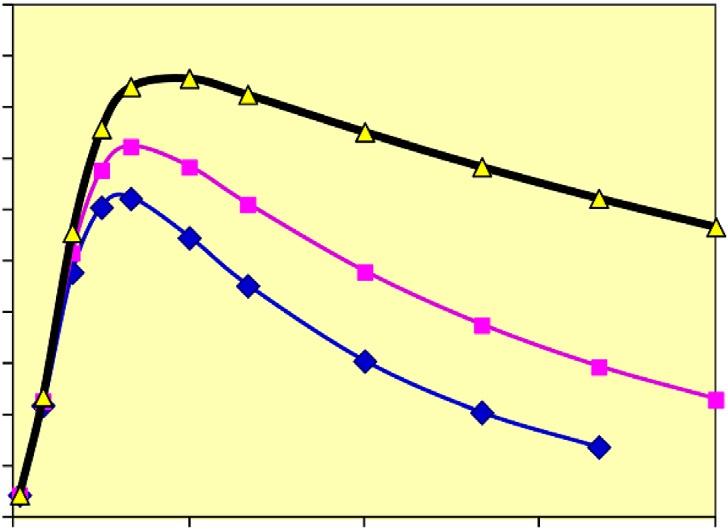
Theoretical behavior of vitality according to regulation degree
0306090120
(unidades teóricas) Age(years) (2) Wear regulationat 50% (3) Wear regulationat 100% (1)Wear without regulation
BeierW, Ruiz –Torres A. (Unpublisheddata)
Thisgraphshowsthetheoreticalbehaviorofvitalityaccordingtodegreeofregulationatasamewear.Thesteepestdeclinetakes place thatis,thehighestrateofaging whenthereisnoregulation(1).Curveslopeismarkedlyflattened,whenregulationofwear is50%andthereisatendencytowardlongevity(2).Iftheweariscompletelyregulated,at100%(3),itdoesnotimplyimmortality sincethiscurvealsoshowsaslope,althoughquiteminor,butpointingtowardanendwhichwouldbedeterminedbyentropy.
• Thereforegraphshowsthethreecomponentsthatdeterminetherateorspeedof aging:wearanditsregulationandentropy1
PROBLEMSANDRISKSOFHORMONALTREATMENT OFTHEAGINGPROCESS
• Hormonaladministrationmusthaveatherapeuticpurpose,thatis,totreatadisease otherthanaging,sinceagingisanormalprocess
• Hormonallevelsinagingmaybelow (testosteroneinmen,estrogenaftermenopause, IGF-1/GH) orhigh (PTH,insulin,TSH)comparedwithyoungadults,but,asexpressionsof normalaging,theydonotreflectpathologicaldeviations
• Hormonaladministrationto “normalize” thoselevels arenotofprovenbenefitandmay beharmful
• Hormonesactoncells,tissues,andorgans,withaging changesalreadymentioned, whoseresponsemaydifferfromyoungsubjects.Therefore “normalization” after hormonaltreatmentinsenescencedoesnotimplythattissueresponsewillbesimilarto thatintheyoungadult
Althoughhormoneadministrationhasimprovedcertainorganicparametersrelatedto aginginsomestudies,theriskofsuch “treatments” istheaccentuationoffrequencyand intensityofadverseeffectsasdescribedasfollows
• Testosteroneadministration:
• Parallelsbetweeneffectsofagingandthoseofhypogonadism2,3 changesinbody composition,sexualfunction,increasedinsulinresistance,depressive/cognitive disorders haveledtoadministrationoftestosteroneinlate-onsethypogonadism (seeChapters10and11:MaleHypogonadisminAdvancedAge)
• Thepotentialadverseeffectsoftestosterone,2,3,4 whichmayincreaseinadvancedage, includecardio-circulatorysideeffects,prostaticcancerorincreasedbenignhypertrophy, polycythemia,sleepapneasyndrome,orevenliverdamagewithsomeformulations
• Afavorablerisk/benefitratiooftestosteronetreatmentinelderlymen withclinicaland chemicalhypogonadism5 hasnotbeendemonstrated(seeMaleHypogonadisminOldAge)
• Testosteronereplacementisrecommendedandapprovedonlyforuse,inmenwith organichypogonadism thatishypothalamic-pituitaryortesticularinorigin,without contraindications,andwhenadequatemonitoringisdone3
• GHadministration:
• Intereststartedfromaninitialobservation6 andsubsequentstudiesofshort duration, 7 whichshowedthatGHadministrationtoelderlysubjects,toequalizeserum IGF-1withthatofyoungpeople,increasedleanmassandreducedbodyfatmass.Less constantresultsweretheslightincreaseinmusclestrengthandmaximumVO2oran increaseinproteinsynthesis
• Adverseeffects: Afterinitialenthusiasm,studiesdescribededema,arthralgias, hyperglycemia,carpaltunnelsyndrome,andgynecomastia,bothinhealthyelderly
1 Entropy,inthiscontext,istheenergythatexistsinthesystemgeneratedbyitsowndisorder;itisawasteenergywhichisnot thermodynamicallyusable.
2 SnyderPJ.Approachtooldermenwithlowtestosterone.Uptodate2018.
3 BhasinSetal.TestosteroneTherapy.AnEndocrineSocietyClinicalPracticeGuideline.JClinEndocrinolMetab103: 1715–1744,2018.
4 EndocrineSocietystatementontheriskofcardiovasculareventsinmenreceivingtestosteronetherapy.www.endocrine.org.
5 CommiteeofInstituteofMedicine.NationalAcademyPress,2004.
6 RudmanDetal.NEnglJMed323:1–6,1990.
7 BlackmanMRetal.JAMA288:2282–2292,2002.
subjects7,8 andinpatientsolderthan60yearswithadultonsetofGHdeficiencyoforganic hypothalamic-pituitaryetiology9
• Experimentalstudies haveshownthatmicelackingeitherGHsecretionorGHreceptors livelonger10,11 thanwildtype,whichcontradictstheideaofGHasan “antiaging” hormone andsupportsthealreadydescribedconceptofgrowthaccelerationasadeterminantoflife potential
• TreatmentwithGHinadultsisonlyindicatedcurrently inselectedpatientswithtrue GHdeficiencyofpituitary-hypothalamicorigin
• Menopausalhormonetherapy(MHT):
• Therapyisindicatedonlyforthetreatmentofmenopausalsymptoms,butnotfor preventionofcardiovasculardiseases,osteoporosis,ordementia12
• UseofMHTinlate postmenopausalwomenisassociatedwithanincreaseinthe followingrisks:
• Inwomen > 60years(combinedwithmedroxyprogesterone(MPA),continuous therapy)13,14:Breastcancer,ovariancancer,coronaryvasculardisease(CVD)events, venousthrombosisandpulmonaryembolism,stroke,andpossiblydementia
• EstrogengivenwithoutMPAappearstoprotectagainstbreastcancerandisneutralwith regardtoCVDevents
• Whetherthereisreductioninprimaryriskofcoronaryheartdiseaseriskinearly menopauseiscontroversial12,13,14,15
• Itiswellknownthatestrogenincreasestheriskofendometrialcancerwhen administeredalone
• MHTisassociatedwithalowerriskofhipfracturesandcolorectalcancer, which doesnotcompensatefortheaforementionedrisks12,16
• MHTisasafeoptionforhealthy,symptomaticwomenwhoarewithin10years ofmenopause oryoungerthanage60yearsandwhodonothaveformal contraindications 12,16
• Estrogen-progestintherapyshouldbeusedforwomenwithauterusandonlyestrogen forthosewithoututerus12,16
• Thyroidfunction
• SincefreeT4andtotalT3donotchangesignificantlywithage, itsapplicationto elderlypeoplewithoutthyroiddiseasehasnotarousedtheinterestseenforother hormones(SeeChapter6:PhysiologyandDiseasesoftheThyroidGlandintheElderly. Hypothyroidism.Hyperthyroidism)
• However,aspreviouslymentioned,serumTSH < 0.1mU/L(subclinical hyperthyroidism), especiallyinadvancedage,increasestheriskofosteoporosis, arrhythmias,ischemia,and/ormyocardialhypertrophy
• Dehydroepiandrosteroneanditssulfate
• Althoughconcentrationsdecreasemarkedlywithage,17 theiradministrationtoelderly personstorestorecirculatingconcentrations 18 doesnotcausechangesininsulin sensitivity,norinbodycomposition,oxygenconsumption,ormusclestrength
8 LiuHetal.AnnInternMed146:104–115,2007.
9 AttanasioAFetal.JClinEndocrinolMetab87:1600–1606,2002.
10 BartkeAetal.CurrTopDevBiol63:189–225,2004.
11 CoschiganoKT,etal.Endocrinology141:2608–2613,2000.
12 Stuenkeletal.Menopause:ESClinicalPracticeGuideline.JClinEndocrinolMetab100:3975–4011,2015.
13 WritingGroupfortheWomen ’sHealthInitiativeInvestigators.JAMA288:321–333,2002.
14 MansonJEetal.JAMA310:1353–1368,2013.
15 GradyD.HERSstudy.JAMA288:49–57,2002.
16 MartinKA,BarbieriRL.Menopausalhormonetherapy:Benefitsandrisks.Uptodate2018.
17 HarmanSM.Endocrinechangeswithaging.Uptodate.Lastupdated:November2016.
18 NairKSetal.DHEAinelderlywomenandDHEAortestosteroneinelderlymen.NEnglMed355:1647–1659,2006.
THEFALLACYOFHORMONAL “REPLACEMENT” AS “ANTIAGINGMEDICINE”
• Theclaimsofanantiagingmedicineisagainstscientific experiencetodate,since agingisaphysiologicalprocess,progressive,irreversible,andinevitableinall individuals
• Hormonaldeclinescharacteristicoftheagingprocessarephysiologicandshouldnot betakenasanindicationforreplacement,since,althoughtheapplicationofthe correspondinghormonemayleadtobloodlevelssimilartoyoungadults,agingdoesnot stopnoristhereevidenceofrejuvenation.Onthecontrary,patientswillbeexposedto collateraleffectsthatmayseriouslycompromisetheirhealth
• Medicineshouldonlybeadministeredwhenaconcomitantdiseaseacceleratesthe normalrateofaging (e.g.,chronicbronchitis,obesity,diabetes)whosespecific treatmentcanlessenthecourseofadeleteriousprocess.Likewise,extremecasesof pathologyinadvancedage,suchassenilemarasmus,couldbesusceptibletoatreatment withanabolichormones,inthiscase,forexample,withGH
AGINGANDDISEASEINENDOCRINOLOGY
SUMMARYOFPHYSIOLOGICALAGINGANDENDOCRINE SYSTEM
• Physiologicalagingis characterizedby:
• Organic wear asitscauseandessence. Regulation istheprotectivephenomenon (adaptative)oftheorganismagainstgradualfunctionalregression
• Startingaftergrowth anddifferentiationarecompleted
• Beingacontinuousprocess ofuncoordinatedlossofcellularandtissuefunction,which reducescapacityoftheorganismtoreproduceandsurvive
• Changesinhormonalandmetabolic responseswithdecreaseofsecretoryendocrine functionandtissueresponse
• Itisdifficulttodifferentiatebetweentheeffectsofaging onhormonalphysiologyand theeffectsofdiseases,includingnonendocrinedisorders
• Inpractice,aging-relatedendocrinechangesoccurinallsubjects,whilethoserelatedto diseasearelimitedtoasmallernumberofindividuals
• Endocrine-metabolicevaluation,clinicallyusefulintheelderlypopulation,derivesfrom measurementofhormonesormetaboliteconcentrationsinbloodandurine,whichare ultimatelyrelatedtoresponsesoftargettissuesorcellstothathormone
• Theagingprocessisassociatedwithotherchangesintheendocrinesystem that influencehormonalconcentrations,suchas:
• Massreductionandcellcomposition
• Decreaseinhormonalsecretionrateandcirculatingconcentrationofhormone-binding proteins
• Disturbancesinhormonaldegradationandexcretionrates
• Changesintheamplitudeandfrequencyinthespecificsecretionrhythmsofeachhormone
• Lowerhormonalsensitivityto feed-backregulation
• Changesinhormonalreceptors(number,affinity,structure,andfunction)aswellasin hormone-receptorinteraction
• Menopauseistheonlywell-defined,abrupt,anduniversalchange whichisafunction ofage.Itcausesthemostrelevantdeleteriousclinicalchangesinboneandlipid metabolismandinthevascularandgenitourinarysystems
• Thefollowingfunctionsdeclinewithage inmostsubjects:Secretoryfunctionof GH-IGF1,malehypothalamic-pituitary-gonadalaxis,andadrenalproductionof dehydroepiandrosterone
• Otherhormonalsecretionschangewithage butchangesarelessconstantanddefined
• Actionsofsomehormonesdecreasewithaging.Inresponsetoalowersensitivityof peripheraltissue,hormonalsecretionmayormaynotincrease
• Mostclinicallysignificantchanges takeplaceincarbohydratemetabolism,with decreaseinpancreaticsecretionofinsulinandincreaseininsulinperipheralresistance, aswellasinthethyroid(hypothyroidismofautoimmuneorigin)
ENDOCRINOPATHIESINADVANCEDAGE. CHARACTERISTICSANDCONSIDERATIONSFOR DIAGNOSISANDTHERAPY
• Thereareendocrine-metabolicdiseasestypicalofadvancedage including osteoporosisandtype2Diabetesaswellashigherprevalenceandseverityofthyroid diseaseandneuroendocrinetumors
• Thealterationsinimmunity withageconditionstheprevalenceofcertainprocesses (e.g.,Autoimmunehypothyroidism)
• Theappearanceoftheelderlyfrequentlysimulatesthatseeninendocrinediseases (e.g.,Hypothyroidism)
• Theelderlymayhavereduceclinicalsignsofmetabolicillness duetothelower peripheralhormoneresponses(e.g.,Apathetichyperthyroidism,depression/delirium inhypercalcemia)
• Difficultiesinstandardizingsomehormonalconcentrations intheelderly(e.g.,normal TSHvalues)
• Normalizationofdecreasedhormonalsecretioninadvancedage doesnotguaranteean adequatetissueresponsewhichoftenresultsinadverseeffects.
E.g.,Myocardialischemiaorrhythmdisordersofagedheartinresponsetothyroxine
• Replacementtherapymayactonagedorgansdifferentlythaninyoungersubjects. E.g.,Hypoglycemiaduetoinsulininelderlypatientswithdiabetesmellitusmaycause myocardialorcerebralischemia
• Changesinbodycomposition (leanmassdecreaseandrelativeincreaseinfatmass)and decreaseinproteinsynthesismaydeterminesecretion,transport,distribution,and hormonalaction
• Polypharmacyeffectsintheelderly:
• Alterationoftransportand/orbloodconcentrationofhormones.
E.g.,GlucocorticoidsmaydecreaseTBGandSHBGordecreaseFSH/LHandtestosterone
• Tissueresponsedisturbances.
E.g.,Spironolactoneblocksandrogenreceptorsandinducesgynecomastia
• Endocrinopathiescausedbydrugs.
E.g.,Thyroiddysfunctioncausedbyamiodarone
• Druginterferenceindiagnosistesting.
E.g.,Iodinecompoundsthatblockthyroiduptake
• Drugsthatsimulateendocrinologicalsyndromes. E.g.,Aminophyllinesuggestiveofhyperthyroidismsyndrome
• Interferenceofdrugswiththeabsorptionormetabolismofreplacementhormones.
E.g.,Absorptiondecreaseofthyroxinebysimultaneousferrotherapyorincreaseof catabolismbydiphenylhydantoin
• Slowdownofdrugmetabolicclearance.
E.g.,Reductionofsulfonylureaclearance(plusincreaseofhypoglycemicaction) bydecreaseinglomerularfiltrationrate
SELECTEDREFERENCES
2. SnyderPJ.Approachtooldermenwithlowtestosterone.Uptodate.www.uptodate.com.Last updated:May2018.Accessed:March2019.
3. BhasinSetal.TestosteroneTherapyinMenWithHypogonadism:AnEndocrineSocietyClinical PracticeGuideline.JClinEndocrinolMetab103:1715–1744,2018.
4. EndocrineSocietystatementontheriskofcardiovasculareventsinmenreceivingtestosterone therapy. https://www.endocrine.org/membership/email-newsletters/endocrine-insider/2014/ february-20-2014/society-statement-risk-of-cardiovascular-events-in-men-receivingtestosterone-therapy-available
5. CommiteeofInstituteofMedicine.NationalAcademyPress,2014.
6. RudmanDetal.Effectsofhumangrowthhormoneinmenover60yearsold.NEnglJMed323:1–6,1990.
7. BlackmanMRetal.Growthhormoneandsexsteroidadministrationinhealthyagedwomenand men:arandomizedcontrolledtrial.JAMA288:2282–2292,2002.
8. LiuHetal.Systematicreview:thesafetyandefficacyofgrowthhormoneinthehealthyelderly.Ann InternMed146:104–115,2007.
9. AttanasioAFetal.HumanGrowthHormonereplacementinadulthypopituitarypatients:long-term effectsonbodycompositionandlipidstatus 3-yearresultsfromtheHypoCCSDatabase.JClin EndocrinolMetab87:1600–1606,2002.
10. BartkeAetal.Lifeextensioninthedwarfmouse.CurrTopDevBiol63:189–225,2004.
11. CoschiganoKT,etal.AssessmentofgrowthparametersandlifespanofGHR/BPgene-disrupted mice.Endocrinology141:2608–2613,2000.
12. Stuenkeletal.Treatmentofsymptomsofthemenopause:AnEndocrineSocietyClinicalPractice Guideline.JClinEndocrinolMetab100:3975–4011,2015.
13. WritingGroupfortheWomen’sHealthInitiativeInvestigators.JAMA288:321–333,2002.
14. MansonJEetal.Menopausalhormonetherapyandhealthoutcomesduringtheinterventionand extendedpoststoppingphasesoftheWomen’sHealthInitiativerandomizedtrials.JAMA310: 1353–1368,2013.
15. GradyD.HERSstudy.JAMA288:49–57,2002.
16. MartinKA,BarbieriRL.Menopausalhormonetherapy:Benefitsandrisks.Uptodate.www. uptodate.com.Lastupdate:August2018.Accessed:April2019.
17. HarmanSM.Endocrinechangeswithaging.Uptodate.Lastupdated:November2016.Accessed: July2017.
18. NairKSetal.DHEAinelderlywomenandDHEAortestosteroneinelderlymen.NEnglMed355: 1647–1659,2006.
FURTHERFUNDAMENTALREADING*
SENESCENT CELLS AND SENOLYSIS
KirklandJLetal.Theclinicalpotentialofsenolyticdrugs.JAmGeriatrSoc65:2297–2301,2017. BussianTJetal.Clearanceofsenescentglialcellspreventstau-dependentpathologyandcognitive decline.Nature562:578–582,2018.
* Thesereferencesarenotnumberedinthetext.
JeonOHetal.Senescentcellsandosteoarthritis:apainfulconnection.JClinInvest128:1229–1237, 2018.
ValentijnFAetal.Cellularsenescenceintheaginganddiseasedkidney.JCellCommunSignal12:69–82,2018.
HuangQetal.Ayoungbloodenvironmentdecreasesagingofsenilemicekidneys.JGerontolABiolSci MedSci73:421–428,2018.
GhoshAKetal.Adiposetissuesenescenceandinflammationinagingisreversedbytheyoungmilieu. JGerontolABiolSciMedSci.2018Dec26.doi:10.1093/gerona/gly290.
PalmerAKetal.Targetingsenescentcellsalleviatesobesity-inducedmetabolicdysfunction.AgingCell. 2019Mar25:e12950.doi:10.1111/acel.12950.
PostmusACetal.Senescentcellsinthedevelopmentofcardiometabolicdisease.CurrOpinLipidol. 2019Mar22.doi:10.1097/MOL.0000000000000602.
WalaszczykAetal.Pharmacologicalclearanceofsenescentcellsimprovessurvivalandrecoveryin agedmicefollowingacutemyocardialinfarction.AgingCell.2019Mar28:e12945.doi:10.1111/ acel.12945.
FarrJetal.Independentrolesofestrogendeficiencyandcellularsenescenceinthepathogenesisof osteoporosis:evidenceinyoungadultmiceandolderhumans.JBoneMinerRes34:1407–1418, 2019.
BASIC PRINCIPLESOFTHE AGING PROCESSWITH ENDOCRINEAND NUTRITIONAL IMPLICATION
McCayCMetal.Theeffectofretardedgrowthuponthelengthoflifespanandupontheultimativebody. JNutrition63-79,1935.
BeierWetal.BiophysikalioscheAspektedesAlternasmultizellulareSysteme.Fortschritteder experimentellenundtheoretischenBiophysik.Bd.16,VEBGeorgThiemeV.Leipzig,AkademieV. Berlin25-46,1973.
RudmanD.Growthhormone,bodycompositionandageing.JAmerGeriatrSoc33:800–807,1985.
HolzenbergerMetal.Deceleratedgrowthandlongevityinmen.ArchGerontolGeriatr13:89–101,1991.
DilmanVM,DeanW.Theneuroendocrinetheoryofaginganddegenerativediseases.TheCenterforBioGerontology,1992.
CorpasEetal.Growthhormoneandhumanaging.EndocrRev14:20–39,1993.
Ruiz-TorresAetal.Increaseininsulinsecretionwithage:Itsclinicalimportanceinevaluatingabnormal secretionfocussedondiabetestypeIIandobesity.ArchGerontolGeriatr22:39–47,1996.
LaronZ.W.Effectsofgrowthhormonesandinsulin-likegrowthfactor1deficiencyonageingand longevity.EndocrineFacetsofageing.Wiley:Chichester(NovartisFoundationSymposium242), 125–142,2002.
Ruiz-TorresAgeA,SoaresdeMeloM.Ageingandlongevityarerelatedtogrowthhormone/insulin-like growthfactor-1secretion.Gerontology48:401–407,2002.
MansonJEetal.Estrogenplusprogestinandtheriskofcoronaryheartdisease.NEnglJMed349:523–534,2003.
HolzenbergerMelal.IGF-1receptorregulateslifespanandresistancetooxidativestressinmice.Nature 42:182–187,2003.
Ruiz-TorresA,BeierW.Onhumanlifespan:Interdisciplinaryapproachaboutitslimits.AdvGerontol16: 14–20,2005.
Ruiz-TorresA.Onhowinsulinmayinfluenceageingandbecomeatherogenicthroughouttheinsulin-like growthfactor-1receptorpathway:invitrostudieswithhumansmoothmusclecells.Gerontology 51:225–230,2005.
Garcia-RuizCetal.Mitochondrialcholesterolinhealthanddisease.HistolHistopathol24:117–132, 2009.
SnyderPJetal.Lessonsfromthetestosteronetrials.EndocrRev39:369–386,2018.
SnyderPJ.Testosteronetreatmentofmalehypogonadism.Uptodate.www.uptodate.com.Lastupdate: January2019.Accessed:March2019.
AGINGAND DISEASEIN ENDOCRINOLOGY
CorpasE.EstudiotransversaldeunapoblaciónestabledeGuadalajara:aportaciónalainvestigacióndel envejecimientodepoblaciones.Tesisdoctoral.UniversidadAutónomadeMadrid.1988. https:// repositorio.uam.es/handle/10486/7297
CorpasE.Cambioshormonalesymetabólicosconlaedad.I.-Funciónhipotálamo-hipofisaria,tiroidea, adrenalygonadal.RevEspGeriatryGerontol25:158–167,1990.
CorpasE.Cambioshormonalesymetabólicosconlaedad.II.-Metabolismofósforo-cálcico, catecolaminas,peptidoatrialnatriuretico,páncreasendocrinoylipoproteínas.RevEspGeriatry Gerontol25:207–216,1990.
LópezdelaTorreM.Envejecimientoysistemaendocrino. http://www.elendocrino.com/linked/Archivos %20profesionales/GERONTO%202003.pdf
Ruiz-TorresA.Elmitodelalongevidadilimitada.EnNuevasmiradassobreelenvejecimiento.Colección deseriesManualesyGuíasn°.EditaMinisteriodeSanidadyPolíticaSocial.11-26,2009.
McDevittMA.Agingandtheendocrinesystem.Chapter20.Brocklehurst'sTextbookofGeriatric MedicineandGerontology,7thEdition.Ed.HMFillit,KRockwood,KWoodhouse.ElsevierEditorial. Philadelphia.123-126,2010.
Diamanti-KandarakisEetal.Agingandanti-aging:aCombo-Endocrinologyoverview.EurJEndocrinol 176:R283–R308,2017.
VandenBeldA.W.Ageingandendocrinology1:Thephysiologyofendocrinesystemswithageing. LancetDiabetesEndocrinol6:647–658,2018.
TaffetGE.Normalaging.Uptodate.Lastupdated:April2019.Access:August2019.
PHYSIOLOGYANDDISEASESOF THEHYPOTHALAMIC-PITUITARY AXISINTHEELDERLY
EmilianoCorpas a,b,RicardoCorrea c,S.MitchellHarman c , MarcR.Blackman d,andAntonioRuiz-Torres e aHLAandHospitalUniversitariodeGuadalajara,Guadalajara,Spain bFaculty ofMedicine,UniversityofAlcalá,Madrid,Spain cDivisionofEndocrinology, VeteransAdministrationMedicalCenter,UniversityofArizonaCollegeof Medicine,Phoenix,AZ,UnitedStates dWashingtonDCVeterans AdministrationMedicalCenter,GeorgetownUniversitySchoolofMedicine, GeorgeWashingtonUniversitySchoolofMedicine,Washington,DC,United States eFacultyofMedicine,Autonomous UniversityofMadrid,Madrid, Spain
CHAPTEROUTLINE
HYPOTHALAMIC-PITUITARYAXISAND AGING 16
CHANGESOFPROLACTINWITHAGE 18
CHANGESOFGHANDIGF-1WITHAGE 19
PITUITARYDISEASESINTHEELDERLY 24
PituitaryTumors 24
PrevalenceandAnatomicalPathology 24
ClinicalPresentationatDiagnosis 25
PituitaryApoplexy 26
NeuroradiologicDiagnosis 26
NeuroradiologicalStages 27
FunctionalDiagnosticFeaturesof Hypopituitarism 30
Hypopituitarism.FunctionalDiagnosis:Endocrine SocietyClinicalPracticeGuidelines 32
PituitaryIncidentaloma:EndocrineSociety ClinicalPracticeGuidelines 33
TranssphenoidalSurgery 35
SecretoryPituitaryTumors 36
Acromegaly 36
Prolactinoma 47
Diagnosis 47
Hiperprolactinemia 47
DiagnosticAlgorithm 47
HyperprolactinemiaCausedbyDrugs 48
HyperprolatcinemiaDuetoDisinhibitionof PRLSecretion 48
SpecificsofTherapyinOlderPatients 48
TreatmentWithDopaminergicAgonists 49
TreatmentofNontumoral
Hyperprolactinemia 51
DiagnosisandTreatmentof Hyperprolactinemia:EndocrineSociety ClinicalPracticeGuidelines 52
ACTHSecretingAdenomas 52
PituitaryTumors.Radiotherapy 53
HYPOPITUITARISM:TREATMENT 53
Hypocortisolism 54
CentralHypothyroidism 56
GHReplacementTherapy 57
ReplacementWithSexSteroids:Testosterone ReplacementTherapyinMen 58
CentralDiabetesInsipidus 60
DrugsandReplacementDoses 61
BIBLIOGRAPHICALREFERENCES 61, 65
EndocrinologyofAging:ClinicalAspectsinDiagramsandImages. https://doi.org/10.1016/B978-0-12-819667-0.00002-0
Copyright © 2021EmilianoCorpas.PublishedbyElsevierInc.Allrightsreserved.
HYPOTHALAMIC-PITUITARYAXISANDAGING
QuestionsRelatedtoAgingandPituitaryFunction
WereviewinthischapterchangeswithageintheproductionofPRLandGH-IGF-1.Changes intheotherhypothalamo-pituitary-glandularaxeswillbetreatedinthechaptersrelatedto eachspecificgland
• Aretheresystematicchangesinhormonesecretionofoneormorehypothalamicpituitaryaxesduringnormalaging?
• Ifso,aretherephysiological,functional,and/orphenotypicagingchangesthatresemble thoseknowntobeassociatedwithpituitaryhormonedeficienciesorexcess?
• Aresuchchangesclinicallysignificant?
• Ifso,whatshouldwedoaboutthem?
NormalAgingandPituitaryHormoneAxisDysfunction:SimilaritiesandDifferences
Agingisaccompaniedbymuscleandboneloss,aswellastotalbodyandabdominalfatgain,insulinresistance,andincreased serumlipids.Thesechangescoincidewithdecreasesofthemainanabolichormones,suchasGH-IGF-Iandsexsteroids, whichlikelycontributetotheaforementionedmetabolicandbodycompositionchangeswithaging.
• Healthyagingoftheneuroendocrinesystemisamultifactorialprocess with considerableinterindividualvariability
• Agingofthehumanadenohypophysisisassociatedwithareductioninsize, increased fibrosis,alteredvascularization,andagreaterfrequencyofmicroadenomas
• Secretionofhypothalamicandanteriorpituitaryhormonesispulsatileandfollowsa circadianrhythm. Inoldage,changesintherhythmandamplitudeofACTHandGH secretionareofprobableclinicalrelevance, whereaschangesinthoseofTSHandother pituitaryhormonesareofminorimportance
• Themostsignificantfunctionalchangeswithaging inthehypothalamic-pituitaryaxis arethoseof reproductivehormonesandGH
• Becauseofthecomplexrhythmicityofhypothalamic-pituitarysecretion, 24-hfrequent samplingtechniquesarerequiredtostudythesubtlechangeswhichoccurin advancedage.Relativelyfewsuchstudieshavebeenconductedinagingpopulations, especiallyinpatientsolderthan80years
• Studiesofthehypothalamic-pituitaryaxisinagingpopulationsarelimitedby several featuresthatcanaffectresults,suchas:
1.Differentcomorbidities,withorwithoutincreasedinflammatorymediators
2.Sex-specificeffects,sometimesnotwellclarified
3.Deficiencyorreplacementofgonadalsteroids
4.Sleepdisorders
5.Modificationsofbodycompositionbyagingandtheirpathologicaldeviations
6.Individualfactors,includingdecreasedphysicalactivity,disabilityand/orfrailty,nutritional deficiency,ortheuseofdifferentdrugs
• Evidence-basedevaluationsrequireapplicationofmethodologiesthataredifficultto implementinolderpopulations, aswellaslongitudinal,properlypoweredfollow-upand studiesthatallowforcomparisonwithhighlydefinedcontrolgroups
• Therearewell-documentedchangesinhypothalamic-pituitaryfunctionduringthe normalagingprocess
• Changesintheadrenalandthyroidaxesareinconsistent andappeartooccurina minorityofagingpersons.Whetherthesechangesarerelatedtotheagingphenotype isunclear(seeChapters6:HypothyroidismandChapter9:AdrenalGland)
• Inmen,therearedecreasedcirculatingconcentrationsoftotalTwithincreasedSHBG, thusproducingamorepronouncedloweringoffree/bioavailableT.Consequently,a significantnumberofmenoverage65arechemically “hypogonadal” (seeChapter10: MaleHypogonadism)
• Theage-relateddecreaseinTisprobablyduetoaprimaryfailureinTproduction by Leydigcellsandtoalesserextent,decreasedsecretionofLH
• Studiesofsomatotropicfunctionconsistentlyreport decreaseswithaginginGHand IGF-I, inparticular,withdiminishedsleeprelatedGHsecretion(seebelow)
• StudiesofandrogenandGHtreatmentofthehealthyelderlyareinconclusive, but suggestthatimprovedbodycompositionisobtainedwithTorGHandthatcombiningT andGHmayexertadditiveorevensynergistic(seebelowandChapters1,10,and11)
• Potentialfunctionalbenefitsofandrogenand/orGHtreatmentofhealthyoldmenhave notbeensubstantiatedandtheclinicalsignificanceofadverseeffectsiscontroversial, sothatcurrentrecommendationsvis-à-vistreatmentmustremainconservative.Current clinicalguidelinesfortreatmentofcorrespondingendocrinedisordersshouldbefollowed
CHANGESOFPROLACTINWITHAGE
• PRLsecretionisbothpulsatile(50%)andtonic(50%); eachmodeexhibitsa predominantlynocturnalrhythm
• Inwomen:
• Menopausediminishes24h(predominantlynocturnal) secretionbyabout40%,in associationwithdecreasedestrogensecretion
• ThePRLdeclinehasbeeninterpretedasadaptative,ashigherserumconcentrations appeartoincreasetheriskofdevelopingbreastcancerinpostmenopausalwomen
• Inmen:24hPRLsecretionisincreasedorminimallydecreasedinadvancedage, withanirregularpatternofsecretion
• Circulatingconcentrationsofestrogensandincreasedadiposity accentuatepulsatile secretorydynamics
• MechanismsfordecreasedPRLsecretioninclude: (1)Increaseddopamineinhibition; (2)decreasedstimulationbyPRLreleasingfactor,and/orby(3)agreaterinhibitionof lactotrophcellsbyadipokines