https://ebookmass.com/product/diagnostic-pathologyintraoperative-consultation-2nd-edition-susan-c-lester/

https://ebookmass.com/product/diagnostic-pathologyintraoperative-consultation-2nd-edition-susan-c-lester/
https://ebookmass.com/product/a-seal-never-quits-holly-castillo-2/
ebookmass.com
This book is dedicated to all the pathologists whose hearts race when alerted by the frozen section pager, to the support staff in the intraoperative consultation room who are always there to assist them, to the surgeons who request essential information to help guide their operations, and most of all, to the patients who have entrusted their care into our hands.
Matthew R. Lindberg, MD
Assistant Professor Department of Pathology
University of Arkansas for Medical Sciences
Little Rock, Arkansas
Emily F. Mason, MD, PhD
Assistant Professor of Pathology
Vanderbilt University Nashville, Tennessee
Vania Nosé, MD, PhD
Associate Chief of Pathology
Director of Anatomic and Molecular Pathology
Massachusetts General Hospital
Professor of Pathology
Harvard Medical School
Boston, Massachusetts
Charles Matthew Quick, MD
Associate Professor of Pathology
Director of Gynecologic Pathology
Department of Pathology
University of Arkansas for Medical Sciences
Little Rock, Arkansas
Matija Snuderl, MD
Assistant Professor of Pathology
Director of Molecular Pathology and Diagnostics
NYU Langone Medical Center
New York, New York
Amitabh Srivastava, MD
Associate Professor of Pathology
Harvard Medical School
Associate Director, Surgical Pathology
Director, Surgical Pathology Fellowship Program
Brigham and Women’s Hospital Boston, Massachusetts
Karen S. Thompson, MD
Professor and Interim Chair, Department of Pathology
John A. Burns School of Medicine
University of Hawaii
Pan Pacific Pathologists, Clinical Laboratories of Hawaii
Kapiolani Medical Center for Women and Children
Honolulu, Hawaii
Stefan Kraft, MD
Rolf Pfannl, MD

Megg Morin, BA
Arthur G. Gelsinger, MA
Rebecca L. Bluth, BA
Nina I. Bennett, BA
Terry W. Ferrell, MS
Lisa A. Gervais, BS
Matt W. Hoecherl, BS
Jeffrey J. Marmorstone, BS
Lisa A. M. Steadman, BS
Richard Coombs, MS
Lane R. Bennion, MS
Laura C. Wissler, MA
Tom M. Olson, BA
Laura C. Wissler, MA
Angela M. G. Terry, BA
Emily C. Fassett, BA
SECTION 1: General
SECTION 2: Methods
SECTION 3: Contents

154 CerebralHemispheres:EvaluationforEpilepsy
MatijaSnuderl,MD,OlgaKrasnozhen-Ratush,MD,and RebeccaD.Folkerth,MD
160 Colon:DiagnosisandMargins
AmitabhSrivastava,MD
David
SusanC.
DavidP.Frishberg,MD
SusanC.Lester,MD,
DavidP.Frishberg,
SusanC.Lester,MD,
SusanC.Lester,MD,
AllocationforSpecialStudiesandBanking
DeborahA.Dillon,MD 78
RadioactiveSeedLocalization
BethT.Harrison,MD
LymphNodes:MolecularMethodsforEvaluation
BethT.Harrison,MD SECTION
86 AdrenalandParaganglia:Diagnosis
VaniaNosé,MD,PhD
96 AnteriorMediastinalMass:Diagnosis
MatthewR.Lindberg,MD
102 Appendix:Diagnosis
AmitabhSrivastava,MD
106 BoneLesion/Tumor:DiagnosisandMargins
MatthewR.Lindberg,MD
116 Breast:Diagnosis
BethT.Harrison,MD
122 Breast:ParenchymalMargins
BethT.Harrison,MD
126 Breast:NippleMarginEvaluation
BethT.Harrison,MD
130 BronchusandTrachea:Diagnosis
MatthewR.Lindberg,MD
132 CerebellumandBrainstem:Diagnosis
RebeccaD.Folkerth,MD,OlgaKrasnozhen-Ratush,MD,
andMatijaSnuderl,MD
142 CerebralHemispheres:Diagnosis
MatijaSnuderl,MD,OlgaKrasnozhen-Ratush,MD,and
RebeccaD.Folkerth,MD
164 Colon:EvaluationforHirschsprungDisease
KarenS.Thompson,MD
170 Esophagus:DiagnosisandMargins
AmitabhSrivastava,MD
176 FallopianTube:Diagnosis
CharlesMatthewQuick,MD
182 HeadandNeckMucosa:DiagnosisandMargins
VickieY.Jo,MDandJeffreyF.Krane,MD,PhD
186 Kidney,Adult:DiagnosisandMargins
RoniMichelleCox,MD
198 Kidney:EvaluationofAllograftPriorto Transplantation
LynnD.Cornell,MD
204 KidneyNeedleBiopsy:EvaluationforAdequacy
LynnD.Cornell,MD
208 Kidney,Pediatric:IndicationsandUtility
KarenS.Thompson,MD
216 Larynx:DiagnosisandMargins
VickieY.Jo,MD,StefanKraft,MD,andJeffreyF.Krane, MD,PhD
220 Liver,CapsularMass:Diagnosis
AmitabhSrivastava,MD
222 Liver:EvaluationofAllograftPriorto Transplantation
AmitabhSrivastava,MD
228 Liver,IntrahepaticMass:DiagnosisandMargins
AmitabhSrivastava,MD
232 Lung,Ground-GlassOpacitiesandSmallMasses: Image-GuidedResection
LucienR.Chirieac,MD
240 Lung:Margins
MatthewR.Lindberg,MD
246 Lung,NonneoplasticDiffuseDisease:Diagnosis
MatthewR.Lindberg,MD
250 LungMass:Diagnosis
MatthewR.Lindberg,MD
258 LymphNodes,Axillary:Diagnosis
BethT.Harrison,MD
266 LymphNodesBelowDiaphragm:Diagnosis
DavidP.Frishberg,MD
274 LymphNodes:DiagnosisofSuspected LymphoproliferativeDisease
EmilyF.Mason,MD,PhD
284 LymphNodes,HeadandNeck:Diagnosis
VickieY.Jo,MDandJeffreyF.Krane,MD,PhD
CASSARINO • CHIRIEAC • CORNELL • COX • DILLON • FOLKERTH
FRISHBERG • HARRISON • JO • KO • KRANE • KRASNOZHEN-RATUSH • LINDBERG • MASON NOSÉ • QUICK • SNUDERL • SRIVASTAVA • THOMPSON
•Intraoperativeconsultation(IOC)hassignificantdifferences comparedtogeneralpathologypractice
○Majorpurposeistoansweraspecificquestionrequired fordirectingsurgery
–Diagnosishasimmediateimpactoncareofpatient
○Definitivediagnosisgenerallynotnecessaryoroptimal
–Informationshouldbelimitedtothatessentialfor immediatemanagementofpatient
–Majorityofspecialstudiesnotavailable;diagnosis basedalmostexclusivelyonH&Eslides
–Onlylimitedsamplingoflargespecimenspossible withintimelimits
○Judiciousinterpretationoffindingsoftennecessary givenlimitationoffrozensections
–Conservativeapproach,butnottooconservative,is appropriate
–Degreesofuncertaintywhenadefinitivediagnosisis notpossiblemayneedtobesharedwithsurgeon
○Time-limitedconsultation
–Ideally,ananswerisavailabletosurgeonwithin20 minutes
–Takesprecedenceoverallotheractivities
–Inmostinstitutions,apathologistisavailableoncall forconsultationatalltimes
○Directinteractionbetweenpathologistandsurgeonis preferred
–Preciseoralandwrittencommunicationisessential
○Oftenoccursatasitedistantfrompathology department
–Pathologiststypicallypreferusingtheirown microscopeintheirownworkspace
○Doesnotoccuratpredeterminedtime
–Mayberequestedattimesoutsidenormalworking hours(e.g.,nightsandweekends)
○Referencematerialmaybelimitedordifficulttoaccess (e.g.,booksandjournals)
(Left)Closecooperationand communicationbetween surgicalandpathologyteams (preferablyinperson)is imperativetomakingsurethe patientreceivestheoptimal treatmentintheoperating room.[CourtesyL.Cheney,PA (ASCP)cm,andE.Rhei,MD.]
(Right)Intraoperative consultationhasfeaturesthat setitapartfromgeneral pathologypracticeinmany waysandrequiresa specializedskillsetand diagnosticacumenina challengingandtime-limited professionalsetting.(Courtesy W.Welch,MD.)
○Consultationwithcolleaguesoftennotpossible
○Notsubspecialized;pathologistsmayseespecimens outsidetheirareasofexpertise
•Pathologistplaysimportantroleinadvocatingforpatient duringIOC
○Shouldonlycomplywithrequestsforfrozensection whentheyareinbestinterestofpatient
○Shouldrequestadditionalbiopsieswhenreceived materialisnotsufficientfordiagnosis
○Mustensurethattissueisused1stfordiagnosisand clinicalcareandonly2ndforinvestigationalstudiesand otheruses
•Pearlsofknowledgearesuggestionsandadvice
○Pearlsstartasgrainofsandbutgainvalueovertime
○Knowledgeisgainedafterlongyearsofexperiencewith IOC,manyclosecalls,andafewerrors
○Learningfromerrorsisanexcellentmethodtoimprove practice(especiallywhenerrorsarenotyours)
•Thereare3principalreasonsforimmediatemicroscopic evaluationofspecimens
○ Diagnosistoguideintra-orperioperativepatient management
–Identificationorconfirmationofpathologicprocess
–Evaluationofmarginsforknownmalignancy
○ Confirmsufficientlesionaltissueispresentfor diagnosisonpermanentsections&/orafterspecial studies
–Definitivediagnosisisnotnecessaryintraoperative
–Pathologistconfirmstosurgeonthereisnoneedto removeadditionaltissue,resultinginpossible additionalmorbidity
○ Optimallyprocesstissueforancillarystudiestobe usedfordiagnosis,treatment,orresearch
–Lymphomas
–Sarcomas
–Pediatrictumors
–Othertumorsrequiringspecialhandling
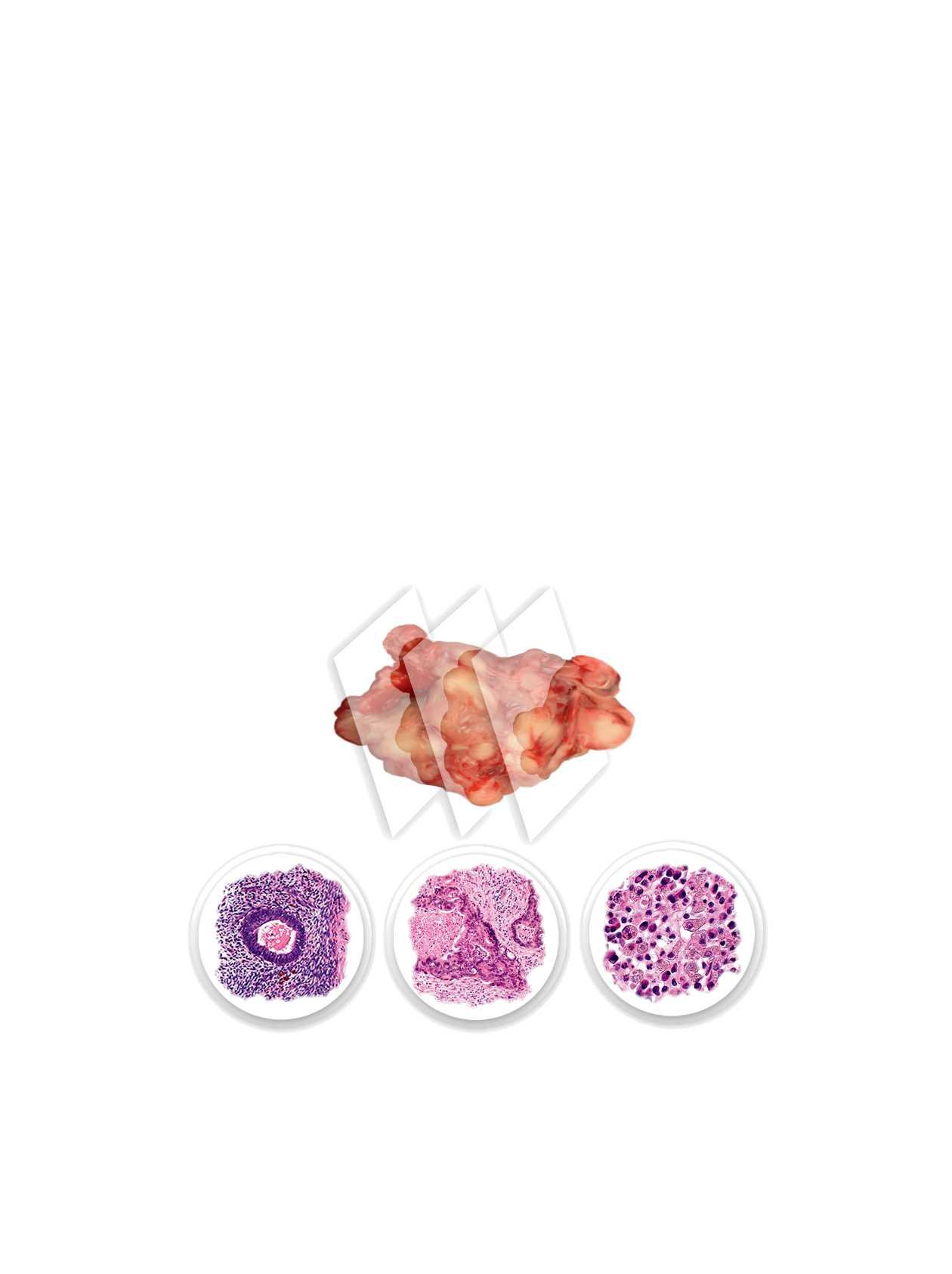
IntraoperativeConsultation:Gross Findings

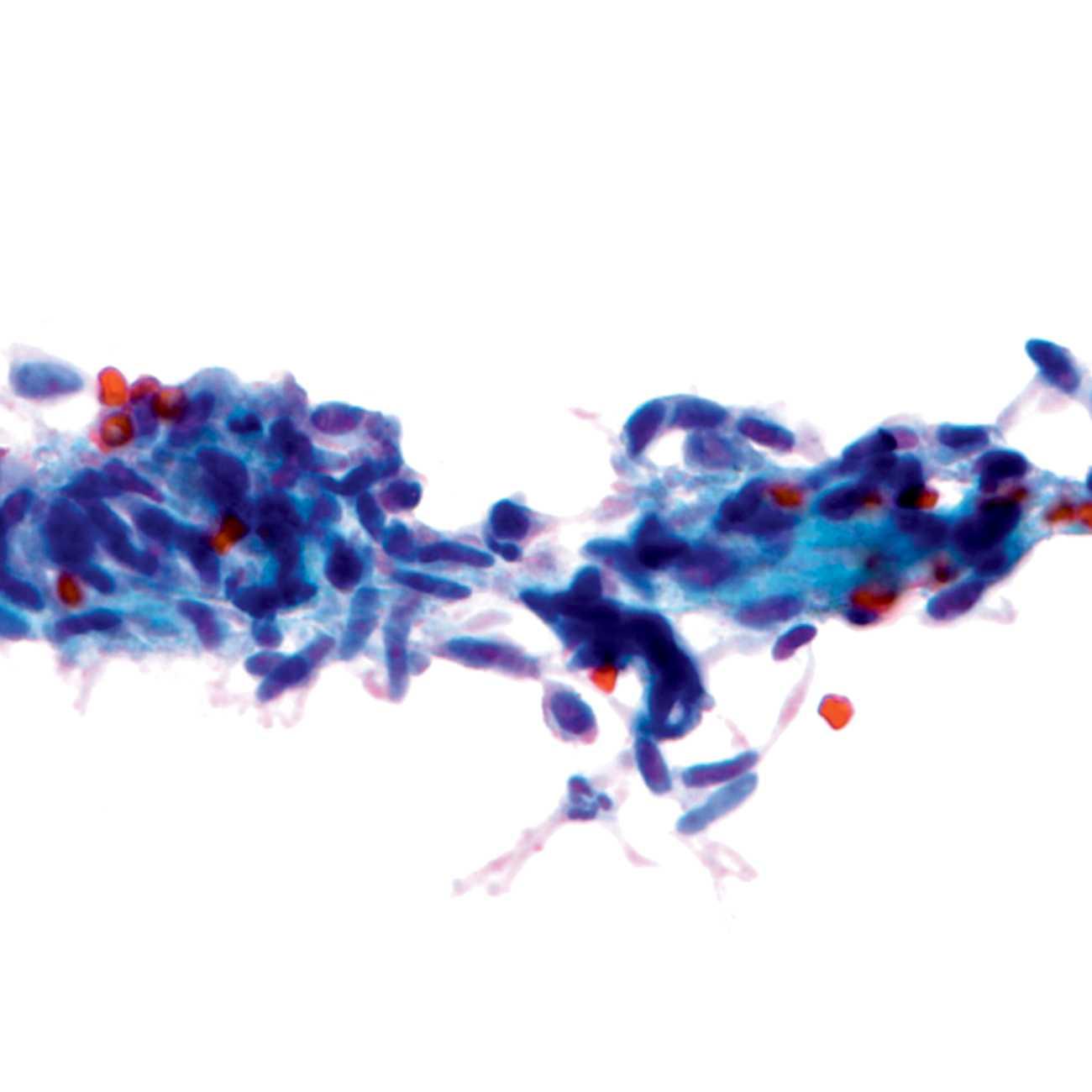
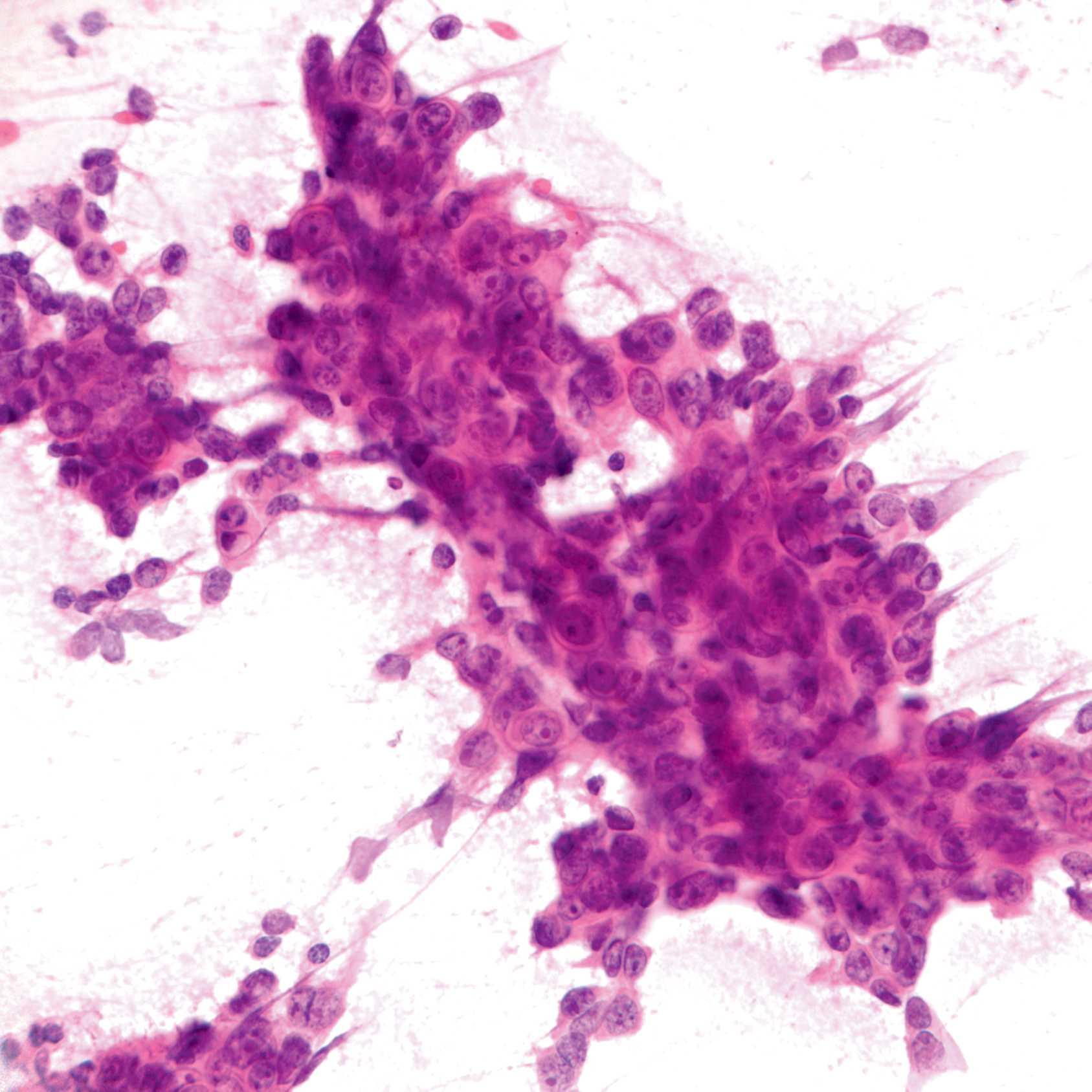
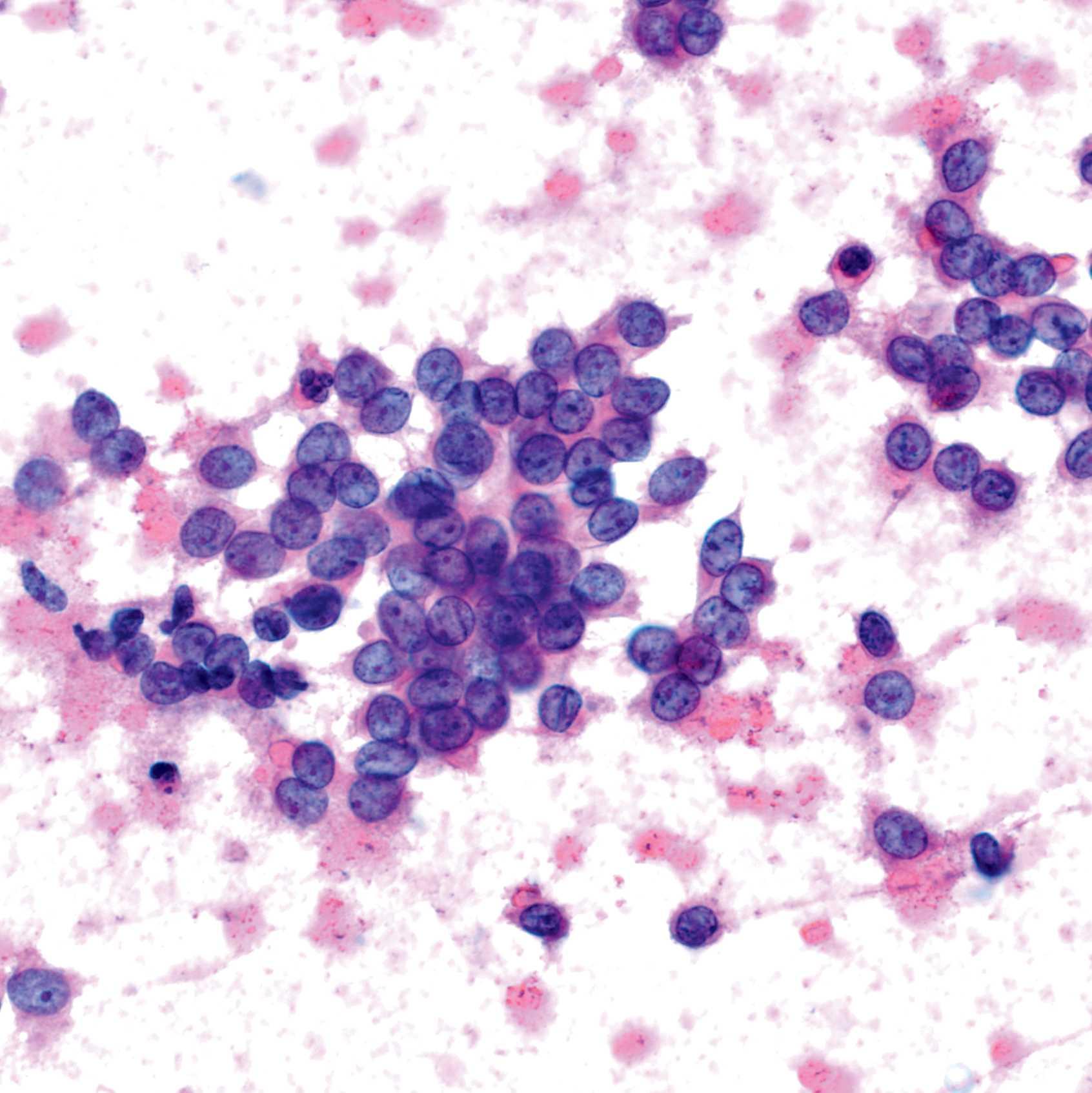
IntraoperativeConsultation:Microscopic Findings

• Diagnosisofprimarylesion(~20%)
○Inmanycases,preoperativediagnosisispossibleusing needleorendoscopicbiopsies
–Insomecases,priorattempttodiagnosemayhave beenunsuccessfulorcontraindicatedduetolocation ortypeoflesion
○Definitivediagnosisneedonlybeprovidedwhen relevanttoimmediatepatientmanagement
–Oftenbenignvs.malignantissufficientfor intraoperativemanagement
–Provisionaldiagnosiscanaidinallocationoftissuefor ancillarystudies
–Inmanycases(e.g.,lymphomas,smallroundbluecell tumors,andsofttissuetumors),ancillarystudiesare oftencritical;definitivediagnosisattimeofIOCis unnecessary
• Evaluationofmarginsforknownmalignanttumor(~ 40%)
○Additionaltissuemaybetakentoachievenegative marginsinasingleprocedure
○Accuracyisgenerallyveryhigh
• Identificationoflymphnodemetastasis(~20%)
○Resectionwithcurativeintentmaybecanceledif metastaticdiseaseisidentified
–Additionalnodesmaynotneedtobesampled
–Patientsmaybetreatedwithsystemictherapypriorto definitiveresection
○Ifapositivesentinelnodeisidentified,additionalnodes maybeexcised
• Adequacyoftissueforfuturediagnosis(~5%)
○Presurgicaltreatmentisbecomingmorewidelyusedto reducetumorburdenandasameasureoftumor response
○Tumorsmustbediagnosedwithcertaintypriorto treatment
–Freshtissuemayalsobedesirableforancillarystudies toidentifycellularconstituentsvulnerabletotargeted therapy
–Patientsmayalsoconsenttohavetissuetakenfor tumorbanks
○Pathologistmustrequestadditionaltissuewhen appropriate
• Evaluationoforganpriortotransplant(<5%)
○Scarcityoforganshasresultedindonorpoolbeing expandedtoincludedonorswithpossiblymarginally functionalorgans
○Intraoperativeassessmentisimportanttoavoid transplantationoforganswithhighlikelihoodoffailure
•NeedforIOCchangesastreatmentofpatientschanges
• Consultationsbecomingmorecommon
○Evaluationoflunglesionsdetectedbyscreening
–UnitedStatesPreventativeServicesTaskForceissued recommendationsforscreeningforlungcancerusing annuallow-dosecomputedtomographyfor individualsbetweentheagesof55-80with30-year historyofsmokingandwhocurrentlysmokeorhave quitsmokingwithinlast15years
–Lesionsdetectedbyscreeningaretypicallysmallorof lowdensity(groundglass)
–Lesionscanbedifficultorimpossibleforsurgeonto palpate
□Speciallocalizationtechniquesmayberequired
–Morelimitedsurgerymaybeconsideredfor adenocarcinomainsituorminimallyinvasive adenocarcinoma
○Evaluationofmarginsofpartialnephrectomies
–Smallrenaltumorsaredetectedbyimaging
–Increasedeffortisbeingmadetopreserverenal functiontoavoidneedfordialysis
○Radioactiveseedretrieval
–Theuseofradioactiveseedsratherthanwirestomark breastlesionshasmanyadvantagesforpatientsand surgeons
–RetrievaloftheseedintheIOCroommaybe preferredtoensureallseedsareidentified, documented,andstoreduntiltheycanbedisposedof safely
○Nipplemarginofmastectomies
–Nipple-andskin-sparingmastectomiesoffer cosmeticallysuperiorprocedureforcarefullyselected women
–Thebaseofthenipplemaybeexamined intraoperativelywithremovalofnipplewhen carcinomaisdetected
○Evaluationoforganspriortotransplant
○Evaluationofsmallbiopsiesforadequacy
• Consultationscurrentlyrarelyperformed
○Identificationofparathyroidadenomas
–Intraoperativemeasurementofparathyroidhormone levelisausefulfunctionalassaythatisusedtoguide surgery
○Sentinelnodeevaluationforbreastcarcinoma
–Studieshaveshowngoodoutcomesforcarefully selectedwomenwithpositivesentinelnodeswithout axillarydissection
–Theneedtodetermineifmetastaticcarcinomaisin sentinelnodeintraoperativelyhasdiminished
○Primarydiagnosisofbreastlesions
–Coreneedlebiopsiesarehighlyaccurateandallow decisionstobemadeconcerningchoiceofsurgery andsystemictherapy(neoadjuvantoradjuvant)
–Definitivesurgerycanbeplannedbasedonthecore needlebiopsydiagnosis
•Frozensectionsarenotequivalenttoevaluationof specimensonpermanentsections
○Diagnosesonfrozensectionshouldbelimitedto informationneededforintraoperativemanagementof patient
• Sampling
○Tissuesectionsmustbesmalltofreezewellandquickly
○Amountoftissueexaminedislessthanthatexaminedby permanentsections
○ Pearlofknowledge:Thepathologistevaluating microscopicslidesshouldalwaysperform,orbeaware of,thegrossfindings
–Ifmacroscopicandmicroscopicfindingsarenot compatible,pathologistshouldsuspecterror
–Tumorsforwhichimagingappearanceiscriticalfor finaldiagnosis(centralnervoussystemtumors,bone tumors)
○ Pearlofknowledge:Reviewingclinicalhistoriespriorto IOCleadstofasterandmoreconfidentdiagnosesand considerablylessanxiety
–Somepeoplebelievethatpathologistsshouldbeable todivineallclinicalinformationfromsurgical specimensastheharuspicesinancientRomewere abletodivineinformationfromexamining organs—thisisnottrue
•IOCrequiringtheallocationoftissueforpurposesbeyond diagnosismustbeidentified
○Tissuerequiredforpatienttreatmentshouldbe distinguishedfromtissuerequestedforresearch
–Patientsmayrequiretissuesamplingtobeeligiblefor clinicaltrials
○Specialproceduresmayberequired
–Steriletissueisnecessaryforcellcultures(e.g.,vaccine studies)
–Warmischemiatime(inoperatingroom)andcold ischemiatime(untiltissueisfrozenorplacedin fixativeshouldbeminimized)
○ Patientcaremustalwaystakeprecedenceoveruseof tissueforresearchthatdoesnotdirectlyimpactpatient
•ObtaininginformationpriortoIOCispreferable,when possible
○DoesnotextendthetimeoftheIOCwhilepatientis underanesthesia
○Allowstimetoreviewpriorpathologyorimagingstudies whenavailable
•Well-designedelectronicmedicalrecordscanfacilitate obtainingkeyinformationpriortotheoperation
ImportantInformationforPathologicInterpretation
•Age:Likelihoodofdiagnosiscanbehighlydependenton age
•Gender:Sometumorshavegender-specificfrequencies
•Priorhistoryofmalignancy
○Metastaticdiseasemustalwaysbeconsidered
○Typeofmalignancy,stage,andpriortreatmentareall importantfactors
○Treatment-relatedchangescanbemistakenfor malignancy
○Tumorswithtreatmenteffectmaybedifficultto recognize
•Priorhistoryofsurgery
○Surgicalchangescanbemistakenformalignancy
•Druguseortherapy
○Drugusecancausechanges(e.g.,increasedmitoses)that canbemistakenformalignancy
•Currentpregnancyorlactation
○Benignbreastlesionscanhaveincreasedmitoticrate &/ornecrosis
–Thesechangescanmimicmalignancy
•Knownorsuspectedinfection
○Somediseasesmayrequiremodificationstoprotect pathologypersonnel
–Specialrespiratorymasksarerequiredtoprotectfrom Mycobacteriumtuberculosis
–SpecimensfrompatientswithsuspectedCreutzfeldtJakobdiseaseshouldnotbeexamined
○Specimensshouldbekeptsterileinordertoobtain cultures
•Imagingfindings
○Insomesettings,appearanceonimagingiscritical
–Essentialtodevelopdifferentialdiagnosis
–Particularlyimportantforbrainlesions,bonetumors, andlunglesions
–Maybenecessarytolocatelesioninlargeresections
InformationProvidedatTimeofIntraoperative
Consultation
• Requisitionform
○Patientidentification,surgeonname,operatingroom number(includingphonenumber)areallessential information
–Knownorsuspectedinfectiousdiseasesshouldbe specified
○Typeofspecimensubmitted
–Location
–Biopsyorcompleteexcision
–Orientation
○Purposeofconsultation
–Inmanycases,willbeclearfromtypeofspecimen submittedandoperativeprocedure
–Ifpurposeisnotclear,pathologistshoulddiscusswith surgeon
– Pearlofknowledge:Ifthereasonforexamining specimenisnotimmediatelyclear,itisanunusualcase andbestcourseofactionistocontactsurgeon
• InformationobtainedduringIOC
○Ifinformationisobtainedfromsurgeonthatishelpful forinterpretationoffrozensection,thiswillalsobe helpfulforfinaldiagnosis
○Informationshouldberecordedonrequisitionformand availabletopathologistreviewingcaseforfinalsignout
• Informationobtainedinoperatingroom
○Insomeinstitutions,itmaybepossibleforthe pathologisttodirectlyobserveoperativefieldandto discussthecasefacetofacewiththesurgeon
•Diagnosisiswrittenandsignedbyattendingpathologist
○Mostlaboratorieshaveaspecificformforthispurpose
○Formshouldbelabeledwithpatientname,medical recordnumber,andsurgicalpathologynumber
○Specificspecimenandsubdesignationforfrozensection areincluded
•Thediagnosisshoulddirectlyaddressthequestionposed bythesurgeontosuccessfullycompletetheoperation
○ Pearlofknowledge:Diagnosesshouldbebriefand includeonlytheinformationnecessary(e.g.,"notumor present"or"metastaticcancerpresent")
–Longandwordyreportsaredifficulttocommunicate orallyandmorelikelytobemisunderstood
○Avoidusingabbreviations
–Anabbreviationsavestimefor1personand aggravateseveryoneelse
Era ClinicalSetting Surgery
Pre-1800s Cancerlesscommonaspatientsoften dieduetootherdiseasesatearlyages
1800s Patientscometomedicalattentionlate indiseasewhencancersarelocally advanced
1891
Firstrecordedintraoperative consultation
Early1900s Awarenessofutilityofearlydiagnosis andnewimagingtechniquesresultsin patientspresentingwithsmallertumors
Usually,rapidbrutalprocedures performedlateincourseofdisease; doesnotchangeultimateoutcome
Anesthesiaandaseptictechniqueallow earliersurgeryandbetteroutcomes; malignanttumorseasilyidentifiedby grossfeatures;radicalsurgical proceduresperformed
WilliamS.Halstedrequests intraoperativeconsultationon mastectomyspecimen
Grossexaminationnotsufficientto identifysmallertumorsasbenignor malignant;growingimpetusformore limitedsurgery;"Whencancerbecomes amicroscopicdisease,theremustbe tissuediagnosisintheoperatingroom"
(JosephColtBloodgood,1927)
Pathology
Capacitytoevaluatetumorsby microscopicexaminationnotavailable
Advancesinmicroscopy,microtomes, formalin,andtissuedyesallow identificationandclassificationoftumors
WilliamH.Welchperformsfrozen section,butprocedurerequiresanhour andresultsarenotavailableuntilafter operationhasbeencompleted
In1905,LouisB.Wilsonpublishesfrozen sectiontechniquethatcanbeperformed inafewminutes
Current Screeningandmodernimaging modalitiesdetectmanycancersatearly stage;canceristrulymicroscopic diseaseformanypatients
Modernsurgeryminimizestissue removedtomaintainfunctionand optimizecosmesis
–Abbreviationsmayvaryamongspecialtiesandmaybe misunderstood
□Forexample,pathologistsunderstand"c/w"to mean"consistentwith,"whereasradiologists understand"c/w"tomean"comparedwith"
○Superfluousinformation(typicallyhistologictypeor grade)isunnecessaryandcancreatepotential discrepancieswiththefinaldiagnosis
○ Pearlofknowledge:Itiscriticaltoknowthe consequencesofadiagnosis(e.g.surgeryforpotential cureterminatedorcontinued)whenmakingdiagnostic judgementcallswhenadefinitivediagnosisisnot obvious
–Theharmofafalse-negativevs.afalse-positive diagnosisforapatientisoftennotequivalent
•Copyofreportismadeandprovidedforpatient'smedical record
•WrittenreportsofIOCmaynotbeavailabletopatient's caregiversforhourstodays
○Whenpossible,documentationofIOCinmannerthatis availableinpatient'srecordispreferable
○Inelectronicmedicalrecords,thismaybepossibleusing holdnote
•Finaldiagnosisiscalledbacktooperatingroom
○Itispreferabletoreadwrittenreportexactly
•Whenpossible,informationshouldberelayeddirectlyto surgeon
○ Pearlofknowledge:Complexorunusualdiagnosesare bestcommunicateddirectlybetweenpathologistand surgeon
–Thereishighrateofmiscommunicationwhen diagnosisisotherthan"benign"or"malignant"
Intraoperativediagnosisplaysimportant roleinprovidinginformationsurgeon needstoensuretumorshavebeen removedandmarginsareclear
–Reportsincludingtermsindicatingdegreesof certainty("suspiciousfor,""cannotexclude," "atypical")canbeinterpreteddifferentlyby pathologistandsurgeon
–Similarterms(e.g.,"carcinoid"and"carcinoma")must beclearlydistinguished
•Thepersonreceivinginformationshouldwritedown informationandreaddiagnosisbacktopathologist
○ThisisrequirementofTheJointCommission(TJC), formerly,TheJointCommissiononAccreditationof HealthcareOrganizations(JCAHO)
1. NorganAPetal:Implementationofasoftwareapplicationforpresurgical casehistoryreviewoffrozensectionpathologycases.JPatholInform.8:3, 2017
2. SamsSBetal:Discordancebetweenintraoperativeconsultationbyfrozen sectionandfinaldiagnosis.IntJSurgPathol.25(1):41-50,2017
3. McIntoshERetal:Frozensection:guidingthehandsofsurgeons?AnnDiagn Pathol.19(5):326-9,2015
4. RoySetal:Frozensectiondiagnosis:istherediscordancebetweenwhat pathologistssayandwhatsurgeonshear?AmJClinPathol.140(3):363-9, 2013
5. WintherCetal:Accuracyoffrozensectiondiagnosis:aretrospectiveanalysis of4785cases.APMIS.119(4-5):259-62,2011
6. TaxyJB:Frozensectionandthesurgicalpathologist:apointofview.Arch PatholLabMed.133(7):1135-8,2009
7. GalAAetal:The100-yearanniversaryofthedescriptionofthefrozen sectionprocedure.JAMA.294(24):3135-7,2005
8. LechagoJ:Thefrozensection:pathologyinthetrenches.ArchPatholLab Med.129(12):1529-31,2005
9. AcsGetal:Intraoperativeconsultation:anhistoricalperspective.Semin DiagnPathol.19(4):190-1,2002
10.WrightJRJr:Thedevelopmentofthefrozensectiontechnique,the evolutionofsurgicalbiopsy,andtheoriginsofsurgicalpathology.BullHist Med.59(3):295-326,1985