DiabetesandRetinopathy
Editedby
Elsevier
Radarweg29,POBox211,1000AEAmsterdam,Netherlands TheBoulevard,LangfordLane,Kidlington,OxfordOX51GB,UnitedKingdom 50HampshireStreet,5thFloor,Cambridge,MA02139,UnitedStates
©2020ElsevierInc.Allrightsreserved.
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans,electronicor mechanical,includingphotocopying,recording,oranyinformationstorageandretrievalsystem,without permissioninwritingfromthepublisher.Detailsonhowtoseekpermission,furtherinformationaboutthe Publisher’spermissionspoliciesandourarrangementswithorganizationssuchastheCopyrightClearance CenterandtheCopyrightLicensingAgency,canbefoundatourwebsite: www.elsevier.com/permissions
ThisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythePublisher(other thanasmaybenotedherein).
Notices
Knowledgeandbestpracticeinthisfieldareconstantlychanging.Asnewresearchandexperiencebroadenour understanding,changesinresearchmethods,professionalpractices,ormedicaltreatmentmaybecome necessary.
Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgeinevaluatingandusing anyinformation,methods,compounds,orexperimentsdescribedherein.Inusingsuchinformationormethods theyshouldbemindfuloftheirownsafetyandthesafetyofothers,includingpartiesforwhomtheyhavea professionalresponsibility.
Tothefullestextentofthelaw,neitherthePublishernortheauthors,contributors,oreditors,assumeanyliability foranyinjuryand/ordamagetopersonsorpropertyasamatterofproductsliability,negligenceorotherwise,or fromanyuseoroperationofanymethods,products,instructions,orideascontainedinthematerialherein.
LibraryofCongressCataloging-in-PublicationData
AcatalogrecordforthisbookisavailablefromtheLibraryofCongress
BritishLibraryCataloguing-in-PublicationData
AcataloguerecordforthisbookisavailablefromtheBritishLibrary
ISBN:978-0-12-817438-8
ForinformationonallElsevierpublications visitourwebsiteat https://www.elsevier.com/books-and-journals
Publisher:StacyMasucci
AcquisitionsEditor:TariK.Broderick
EditorialProjectManager:SamanthaAllard
ProductionProjectManager:MariaBernard
CoverDesigner:MatthewLimbert
TypesetbySPiGlobal,India
Contributors
MichaelD.Abra ` moff DepartmentofElectricalandComputerEngineering;Department ofBiomedicalEngineering;DepartmentofOphthalmologyandVisualSciences,Carver CollegeofMedicine,UniversityofIowa,IowaCity,IA,UnitedStates
GaryAbrams DepartmentofOphthalmology,VisualandAnatomicalSciences,Wayne StateUniversitySchoolofMedicine,Detroit,MI,UnitedStates
MuhammadUsmanAkram DepartmentofComputer&SoftwareEngineering,National UniversityofSciencesandTechnology,Islamabad,Pakistan
YasminaAlKhalil DepartmentofElectricalandComputerEngineering,AbuDhabi University,AbuDhabi,UnitedArabEmirates
MarahAlhalabi DepartmentofElectricalandComputerEngineering,AbuDhabi University,AbuDhabi,UnitedArabEmirates
ImranBasit DepartmentofOphthalmology,ArmedForcesInstituteofOphthalmology, Rawalpindi,Pakistan
EtsuoChihara Sensho-kaiEyeInstitute,Uji,Kyoto,Japan
GalinaDimitrova DepartmentofOphthalmology,CityGeneralHospital“8thof September”,Skopje,NorthMacedonia
AymanEl-Baz BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
AdelElmaghraby ComputerScienceandComputerEngineeringDepartment,University ofLouisville,Louisville,KY,UnitedStates
Marı´aIsabelFerna ´ ndez OphthalmologicalInstituteGo ´ mez-UllaandDepartmentof Ophthalmology,UniversityHospitalofSantiagodeCompostela,Santiagode Compostela,Spain
LuayFraiwan DepartmentofElectricalandComputerEngineering,AbuDhabiUniversity, AbuDhabi,UnitedArabEmirates
WinstonFurtado BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
MohammedGhazal DepartmentofElectricalandComputerEngineering,AbuDhabi University,AbuDhabi,UnitedArabEmirates;BioengineeringDepartment,University ofLouisville,Louisville,KY,UnitedStates
GuruprasadGiridharan BioengineeringDepartment,UniversityofLouisville,Louisville, KY,UnitedStates
FranciscoGo ´ mez-Ulla OphthalmologicalInstituteGo ´ mez-UllaandDepartmentof Ophthalmology,UniversityHospitalofSantiagodeCompostela,Santiagode Compostela,Spain
AnjuGoyal DepartmentofOphthalmology,VisualandAnatomicalSciences,WayneState UniversitySchoolofMedicine,Detroit,MI,UnitedStates
TaimurHassan DepartmentofComputer&SoftwareEngineering,NationalUniversityof SciencesandTechnology,Islamabad,Pakistan;CenterforCyber-PhysicalSystems,Khalifa UniversityofScienceandTechnology,AbuDhabi,UnitedArabEmirates
AshrafKhalil ComputerScienceDepartment,CollegeofEngineering,AbuDhabi University,AbuDhabi,UnitedArabEmirates
AshrafKhallaf BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
DipenKumar WayneStateUniversitySchoolofMedicine,Detroit,MI,UnitedStates
AliH.Mahmoud BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
RayyanManwar DepartmentofBiomedicalEngineering,WayneStateUniversity,Detroit, MI,UnitedStates
JoaquimdeMoura DepartmentofComputerScience;CITIC-ResearchCenterof InformationandCommunicationTechnologies,UniversityofACorun ˜ a,ACorun ˜ a,Spain
JorgeNovo DepartmentofComputerScience;CITIC-ResearchCenterofInformationand CommunicationTechnologies,UniversityofACorun ˜ a,ACorun ˜ a,Spain
MarcosOrtega DepartmentofComputerScience;CITIC-ResearchCenterofInformation andCommunicationTechnologies,UniversityofACorun ˜ a,ACorun ˜ a,Spain
ManuelG.Penedo DepartmentofComputerScience;CITIC-ResearchCenterof InformationandCommunicationTechnologies,UniversityofACorun ˜ a,ACorun ˜ a,Spain
GabrielaSamagaio CITIC-ResearchCenterofInformationandCommunication Technologies;DepartmentofComputerScience,UniversityofACoruna,ACoruna,Spain
HarpalSandhu DepartmentofOphthalmologyandVisualSciences;Departmentof Ophthalmology,SchoolofMedicine,UniversityofLouisville,Louisville,KY,UnitedStates
ShlomitSchaal OphthalmologyandVisualSciencesDepartment,Universityof MassachusettsMedicalSchool,Worcester,MA,UnitedStates
MohamedShaban ElectricalandComputerEngineering,UniversityofSouthAlabama, Mobile,AL,UnitedStates
AbhayShah DepartmentofElectricalandComputerEngineering,UniversityofIowa, IowaCity,IA,UnitedStates
AhmedShalaby BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
AhmedA.Sleman BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
AhmedSoliman BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
JasjitS.Suri AtheroPointLLC;GlobalBiomedicalTechnologies,Inc.,Roseville,CA; DepartmentofElectricalEngineering,IdahoStateUniversity,Pocatello,ID,UnitedStates
FatmaTaher CollegeofTechnologicalInnovation,ZayedUniversity,Dubai,UnitedArab Emirates
AlanTruhan WayneStateUniversityPhysicianGroup,KresgeEyeInstitute,Detroit,MI, UnitedStates
Pla ´ cidoL.Vidal DepartmentofComputerScience;CITIC-ResearchCenterofInformation andCommunicationTechnologies,UniversityofACoruna,ACoruna,Spain
XiaodongWu DepartmentofElectricalandComputerEngineering;Departmentof RadiationOncology,UniversityofIowa,IowaCity,IA,UnitedStates
Complementarycapabilities ofphotoacousticimagingtoexisting opticalocularimagingtechniques
DipenKumara,AnjuGoyalb,AlanTruhanc,GaryAbramsb, RayyanManward
a WAYNESTATEUNIVERSITYSCHOOLOFMEDICINE,DETROIT,MI,UNITEDSTATES
b DEPARTMENTOFOPHTHALMOLOGY,VISUAL ANDANATOMICALSCIENCES,WAYNESTATE UNIVERSITYSCHOOLOFMEDICI NE,DETROIT,MI,UNITEDSTATES c WAYNESTATEUNIVERSITY PHYSICIANGROUP,KRESGEEYEINSTITUTE,DETROIT,MI,UNITEDSTATES d DEPARTMENTOF BIOMEDICALENGINEERING,WAYNESTATEUNI VERSITY,DETROIT,MI,UNITEDSTATES
Since1886,whenthefirstpictureofthehumanretinawastaken,ocularimaginghas playedacrucialroleinthediagnosisandmanagementofophthalmicdiseases [1].One ofthebiggestcontributorstotheadvancementofocularimagingistheadoptionofoptical imagingtechniques.Opticalimagingisamethodoflookingintothebodyinanoninvasive way,likeX-rays.However,unlikeradiologicalimagingtechniquesthatuseionizingradiation,opticalimaginguseslightandthepropertiesofphotonstoproducedetailedimages rangingfromstructuresassmallascellsandmoleculestostructuresaslargeastissuesand organs.Thereareplentyofadvantagesofusingopticalimagingcomparedtoradiological imaging.Forone,opticalimagingismuchsaferforpatientssinceitusesnonionizingradiationtoexciteelectronswithoutcausingdamage.Additionally,sinceitisfastandsafe, opticalimagingcanbeusedtomonitoracuteandchronicdiseases,aswellastreatment outcomes.Opticalimagingisalsousefulforimagingsofttissuesincedifferenttypesof tissuesabsorbandscatterlightdifferently.Finally,opticalimagingcanadvantageously usevaryingcolorsoflighttoseeandmeasuremultiplepropertiesoftissuesatatime. Therefore,itisnosurprisethattheopticalimagingmodalitiesoffundusphotography inthe1920s [2],scanninglaserophthalmoscope(SLO)imagingin1981 [3] andoptical coherencetomography(OCT)in1991 [4] havetouteda“goldenage”inophthalmic imagingapplications [5].Althoughthesetechnologieshaveadvancedthefieldofocular imagingandarecommonlyusedinclinicalpractice,theyarenotwithouttheirflaws. Anewtechnology,photoacousticimaging,hasbeenshowntohavepromisingfeatures thatcouldmakeitthenextmajorimagingtechniqueinophthalmology.Additionally, photoacousticimaging(PAI)cancombinewithpreexistingopticalmicroscopicimaging modalitiestoachievemultimodalimagingoftheeye.Inthischapter,wepresentabrief
overviewoffundusphotography,SLO,andOCTwhilediscussingthepotentialofPAIasthe nextmajorocularimagingmodality.
Firstintroducedin1920andextensivelyusedsince1960,fundusphotographycontinuestobeastapletechniqueinophthalmology [2].Initially35mmfilmwasthestandard forfundusphotographybutithaslongbeenreplacedbydigitalacquisition [5].Fundus photographyworksinasimilarmannerasanindirectophthalmoscope.Lightisfocused byaseriesoflensesonaring-shapedaperture,whichthenispassedintoacentralaperture toformaringwhichthenpassesthroughthecameraobjectivelensandcorneatoilluminatetheretina.Thereflectedlightfromtheretinathenpassesthroughadarkholeinthe annulusformedbytheilluminationsystempreviouslydescribed.Thereisminimalreflectionofthelightsourceinthecapturedimagebecausethelightraysofthetwosystemsare independent.Apicturecanthenbetakenbyusingonemirrortointerruptthelightfrom theilluminationsystemsothatthelightfromaflashbulbcanpassintotheeye.Another mirrordropsatthesametimeinfrontoftheobservationtelescopetodirectthereflected lightontofilmoradigitalcharge-coupleddevice(CCD).Monochromaticlightcanalsobe usedratherthanwhitelightsincemonochromaticlightallowsforincreasedcontrastof anatomicaldetailsofthefundus [6].Normallyfundusphotographycanonlycapturea smallfieldofview(FOV)whilethepupilisdilated,butitcanbeincreasedwithasmall aperturestopatthecostofresolution [2].Themaximumfieldofviewis50degreesbut itcanbeincreasedto60degreesifusingamydriaticcamera [2].Additionally,byusing aspecial Montage software,individualimagescanbeputtogethertoformacollagethat cancoverupto110degrees [2].Furthermore,fundusphotographycanbecombinedwith wideangleimagingtoachieveafieldofviewbetween45and140degrees,butthereisproportionallylessretinalmagnification [5].Themainadvantagesoffundusphotographyare easeofuse,fullcolor,lowcostcomparedtootherimagingtechniques,andhighpatient compliance [2].Currently,fundusphotographyisusedtomonitortheprogressionofdiseaseslikediabeticretinopathy,age-relatedmaculardegeneration(ARMD),glaucoma,and neoplasmsoftheeye [5].
InSLO,theretinaisscannedinarectangularpatternofparallelscanninglinesfollowed bytheelectronbeamonaTVorcomputerscreen(rasterpattern) [2] usingamonochromatic,narrowlaserbeam.Thebeamisusuallydeflectedusingoneslowverticalandone fasthorizontalgalvanometerscanner [7].Bymodulatingthescanningbeam,projectionof graphicsintherasterisachieved.Sinceitusesarasterpattern,earlySLOscouldoutputto aTVmonitorandberecordedonvideotapes.TheSLOhasbeenfurtherimprovedbycombiningitwithothertechnologies.Confocalscanninglaserophthalmoscope(cSLO)combinestheprinciplesofconfocalimagingtoincreasecontrastanddepthresolution. Confocalmicroscopywasinventedin1955byMarvinMinsky [8].Confocalmicroscopy usesapinhole(confocalfilter),whichisinanopticallyconjugateplaneinfrontofadetectorandpointilluminationtoremoveout-of-focussignal [2].Muchofthelightthatis reflectedisblockedbythepinholesincelightisonlyreflectedbystructurescloserto thefocalplane.Two-dimensional(2D)imagingoccursinarasterpatternoverthespecimenbutthree-dimensional(3D)imagingispossiblebychangingtheaxialresolution.
Byincreasingthenumericalapertureordecreasingthediameterofthepinholeonecan increasethedepth.Onecanthenscanmanythinsectionsthroughasamplewhichcan becombinedwithSLOtoallowcSLOtoacquiredepthinformation [9].Animprovement tocSLOismultispectralSLOsthatusemultiplelasersofdifferentwavelengths.These laserstendtobecoaxialviaacoupleofdichroiccombiningmirrorsandthegoalistointroducecolortomatchimagesfromfundusphotography.Thelasersareeithermultiplexedor firedsimultaneouslyonanX-Yscanningmirrorthatcausesthelighttofocusonasquare areaofseveralmillimetersontheretina.Thereflectedlightthentraversestoabeamsplitterthatdirectsaportionofthelighttothedetector [2].MultispectralSLOsareusedfor retinalvesseloximetry,reflectometry,angioscotometry,andfundusperimetry [10–14]. Overall,cSLOisadvantageouscomparedtopreviousimagingtechniquessinceitallows forbetterimages,patientcomfort,videocapability,andtheabilitytoimagepupilsthat donotdilatewell.Ithasbeenshowntobeeffectiveindetectingbiomarkersfordiabetic retinopathy [15],age-relatedmaculardegeneration [16],scanningthenerveheadinglaucoma [17],andimagingtheretinalnervefiberlayer(RNFL) [18].Themostcommonuseof theSLOiswithultrawide-fieldimagingof200degreesusingtheOptosSystem.Thisuses anSLOwithanellipsoidallenstovisualizetheperipheralretina.About82%oftheretina canbeimaged.Advantagesincludelowlightlevelforpatientcomfortandgoodimages canoftenbeobtainedwithoutdilationofthepupil.Fundusautofluorescence,fluorescein angiography,andindocyaninegreenangiographycanbedonewiththeOptossystem. AmorerecentadaptationtoSLOisadaptiveopticsSLO(AOSLO).Adaptiveopticswas atechnologyoriginallycreatedforastronomythathasbeencombinedwithSLOtoreduce theeffectsofwavefrontdistortionscausedbyopticalaberrations.Thisisdonebymeasuringthewavefrontdistortionsandcompensatingforthembyusingdevicessuchasa deformablemirror [19].Thesedistortionsdiminishthequalityoftheimagebeing reflectedbytheeyewhichpreventedmicroscopicresolutionofstructuressuchascapillariesandcells [3].AOSLOmostcommonlyusesaShack-Hartmannsensortomeasure thesedistortionsbycalculatingthelocalphaseerrorsinthewavefront.Aphasemodulator,suchasadeformablemirror,canbeusedtocorrecttheseerrorssincethephaseerrors canbeusedtoreconstructthewavefrontwhichinturncancontrolthedeformablemirror. Anotheraspecttohaveahighmagnificationofsmallstructuresisimagestabilization. Recently,eyetrackingandstimulusdeliverymethodhavebeenimplementedinAOSLO toachieveit [20].
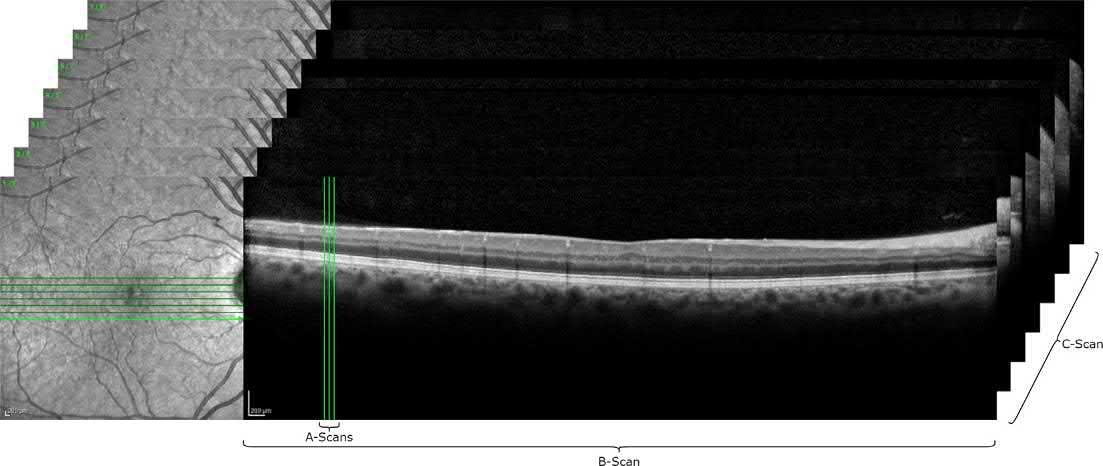
OCTisanoninvasive,micronlevel,high-resolutionimagingtechniquebasedonthe principleofMichelsoninterferometerthatprovidesreal-timeimagesoftheretina.Asis withMichelsoninterferometer,aninterferencepatternisproducedbysplittinglightinto twoarms:asamplearmfromscanningtheretinaandareferencearmfromamirror.These armsarethenrecombinedbysemitransparentmirrorsandredirectedtoaphotodetector orcamera [21].Iftheinterferenceisconstructivebetweenthetwoarms,thesignalis strongatthedetectorandiftheyaredestructive,thesignalisweakatthedetector. Areflectivityprofile,alsocalledanA-scan,canbegatheredbyscanningthemirrorin thereferencearmwhichcontainsinformationonspatialdimensionsandlocationof
thestructuresintheretina.Across-sectionaltomograph,otherwiseknownasaB-scan, canbeobtainedbycombiningaseriesofA-scans.OCTuseslow-coherenceinterferometry asopposedtoconventionalinterferometrythatuseslongcoherencelength [22].Lowcoherenceinterferometryuseslow-coherencelightwhichislightthatconsistsofabroad rangeoffrequenciesratherthanjustasinglefrequency.Thebroadbandlightallowsfor low-coherenceinterferometrytoshortentheinterferencetomicrometers,perfectfor itsusageinophthalmology.Additionally,itshouldbenotedthatOCTusuallyutilizes near-infrared(NIR)lightsincetherelativelylongwavelengthallowsforNIRtopenetrate deeperthancSLOintoscatteringmedialiketheretina.Sinceitsinceptionin1991,OCT hasmadehugeadvancementsandimprovementstoincreasetherateofimagingandresolutionofOCT.TimedomainOCTs(TDOCTs)havelargelybeenreplacedbyspectral domainorFourier-domainOCT(SD-OCT)sincecurrentstate-of-the-artonescanproducebetween40and70,000A-scansperminute,whichismuchfasterthanTDOCTs [5].Themajoradvantagesofitbeingfasterarethatthescantakeslesstimeanditisless impactedbyartifactsandaberrationscausedbyblinkingoreyemovement [5].LikeSLO, OCThasbeencombinedwithadaptiveoptics(AO-OCT)todecreasetheaberrations causedbyimperfectionsinthecurvatureofthecorneaandlens [23].Also,AO-OCThas theadvantageofhigheraxialresolutioncomparedtoAO-SLO [23].OCTusedtobelimited bythefactthatitcouldnotbeusedforbloodflowanalysisduetoapoordelineationof bloodvesselsfromthescatteringoflightaserythrocytesmovethroughthem [24].However,threetypesofOCThaveshownpromiseinthisregard:DopplerOCT,OCTangiography(OCTA),andvisiblelightOCT(vis-OCT).DopplerOCTcombinesOCTwiththe principlesoftheDopplereffectwhichresultsinimprovedresolutionandsensitivitythat allowsfortheevaluationofbloodflow,thevolumeofretinalandchoroidalvasculature, abnormalitiesinchoroidalvasculature [25],andabnormalitiesinretinalandchoroidal vessels [26].OCTAcameaboutduetotheimprovementsinOCTsensitivityandspeedover theyearswhichhasledtobetterdelineationofbloodvessels [27].OCTAcomparesconsecutiveB-scanstakenatratesofseveralhundredHz.TheadvantagesofOCTAarethatit doesnotrequiretheuseoffluoresceindyessuchassodiumfluoresceinandindocyanine green [28],theabilityforrepeatedscans,andtheabilitytoanalyzeflowinaspecificaxial locationoftheretinaorchoroid [29].Vis-OCT,whichusesvisiblelightratherthanNIR,has alsorecentlygainedattentionduetobetteraxialresolutionthanNIR-basedOCTsandbetterimagecontrastduetoscatteringpropertiesoftissuesinvisiblelight,albeitatthecostof imagedepth [30].Ontopofvisualizing3Dretinalstructure,vis-OCTcanquantifyblood oxygensaturation(sO2)inretinalcirculation [25].Duetoitsabilitytoshowcrosssections oftissuelayersatmicrometerresolution,OCTisheavilyusedinophthalmologyasa methodtoassessstructuralchangesintheretinaindiseasessuchasdiabeticretinopathy, veinocclusion,age-relatedmaculardegeneration,glaucoma,multiplesclerosis,andother diseasesthathaveocularsequelae.OCTisverysensitiveindetectingmacularedemaand ismoreaccuratethanclinicalexamination.OCThassignificantlyreducedfalsepositive referralsfordiabeticmacularedema(DME)duringdiabeticscreenings [31].Additionally, OCThasgiveninsightintoabnormalitiesatthejuncturebetweenvitreousandthemacula
inpatientswithDMEwhichcouldinfluencemanagementandprognosis [32].Furthermore,OCTisalsousefulintheearlydetectionofuveiticmacularedema [33] withtheidentificationofspecificOCTpatternsassociatedwiththedisease [34].Anotherdiseasethat OCTisusedforisARMD.FluoresceinangiographyhasbeenlargelyreplacedbyOCTasthe imagingmethodformonitoringARMDtreatmentandtheneedforfurtheranti-VEGF treatment [35].OCTisalsoheavilyusedincasesofglaucoma.Glaucomaprogressionis associatedwithRNFLandganglioncellthinning [36],soOCTcanbeusedforglaucoma detectionandprogression [37] .WhilemostofOCTtechnologyisfocusedonimagingof theretinaorpathologiesrelatedtotheretina,enhanced-depthimagingOCT(EDIOCT)canevaluatechoroidalthicknessandpo steriorsegmentinflammatorydisorders [5] .Asidefrommonitoringthechoroid,ithasbeenshowntobeusefulinmonitoring otherocularinflammatorydiseasessuchasVogtKoyanagiHaradadisease [38],sarcoidosis [39] ,birdshotchorioretinopathy [40],andinfectiouschoroiditis [41] .However, OCThasbeenwellestablishedinophthalmology;ithasalsobeenusedinothermedicaldisciplinessuchasdermatology [42–55] .
Whilefundusphotography,SLO,andOCTarestillconsistentlyusedtodayinophthalmology,theyarenotwithouttheirproblemsandlimitations.Tostart,fundusphotography requirespupildilationwithshort-actingmydriaticdropswhichcancausediscomfortfor patients [5].Therehavebeenrecentadvancementsincamerasthatdonotrequiremydriaticdropsbutthesecanbeaffectedbymediaopacity,suchascataracts,somydriatic camerasarestillthecamerasofchoice.Mydriaticcamerasareespeciallydesiredifthere isaneedtoimagetheperipheryoftheretina [56].Evenmoresothandiscomforttopatients, thesetechnologiessufferfromalackofquantitativedata,lackofabilitytotakephotographsofhighquality,poordepthresolution,difficultyincomparingserialphotographs, andtheneedtosubjectpatientstohigh-intensitylighttoilluminatetheretina [2].Asfor SLO,oneofthelimitationsisthatinvoluntaryeyemovementsaffectimagequality. AsolutiontothisistrackingSLO(TSLO)whichusesahigh-speedretinaltrackerto significantlyimproveimagequality [56].AnotherlimitationofSLOisthatcurrentcommercialSLOs,suchasOptosortheHeidelbergwidelens,donotprovideimagesoftheeyefrom oratoora [57].Additionally,thereisadistortionoftheimageontheperipheryoftheimage sinceitistakinga2Dimageofa3Dglobe [58].Also,themeasurementsoftheeye,such asdistanceandarea,maynotbetheactualdimensionsoftheeyesinceitdoesnotstandardizetheimagetoanyaxisoftheeye [5].Artifactsontheimagecanalsobecausedby severalthings:eyelashes,cataracts,intraocularlensimplants,pigmentsintheanteriorsegmentoftheeye,andvitreousopacitiestonameafew [59].Furthermore,thecostofequipmentandmaintenanceofSLOcanbealargebarrier [5].Finally,therearethelimitationsof OCT.OCTbyitselfisunabletomeasuresO2 andRPEmelanin.WhileOCTAexists,itis restrictedbyitslimitedfieldofview,lackofinformationonfillorflowspeed,andmotion artifacts [60].Vis-OCTsuffersfromlimitedimagedepthandcancausediscomfortforeye imaging [23].Finally,sinceallthreetechniquesareopticalscattering-basedmodalities, measurementsofbloodoxygensaturationintheeyeareaffectedbylightscattering,and fundusphotographyandSLOalsoneedtousecontrastagentstomeasurethem [61].
Whenlightisreceivedbytheeye,itisprocessedbyboththeretinalpigmentepithelium (RPE)andtheretinawhichconsumesalargeamountofoxygenandenergy [62].Therefore,theretinaneedssupportingvasculaturewhichithasfromretinalandchoroidal circulation.Normallythesevasculaturesystemsbringoxygenandnutrientstotheretina [63],andstudieshaveshownthatvariationsinthesO2 andRPEmelaninplayaroleinoculardiseasessuchasdiabeticretinopathy [64],glaucoma [65],retinalvenousocclusion [66], andARMD [67].Thus,therehasbeenanincreasedeffortinthepastdecadetoquantifythe sO2 andRPEmelaninconcentrationintheeye.Fortunately,bothbloodandmelanin, withinthevisiblelightspectralrange,havehighopticalabsorptioncoefficientswhich allowthemtobemeasured [68].PAIhasbeenshowntomeasureopticalabsorptionpropertiesofbothbloodandmelanininanoninvasiveandprecisewayinotherlocationsofthe body [69,70].Therefore,PAIisarecenttechnologyforophthalmologyduetoitspotential clinicaluseinmeasuringretinalandchoroidalsO2 andtheRPEmelanin.Photoacoustic imaginghasbeenwellstudiedinseveralpreclinicalimagingapplications [71–80].Itis basedonthephotoacousticeffect,whichisthegenerationofultrasoundwavesdueto theabsorptionoflightandthermalexpansion [81].TheprimaryPAItechniqueisphotoacoustictomography(PAT).PATstartsbyusingalasertoilluminateandexcitethesample whereshort(nanosecond)laserpulsesareusedthatsatisfythestressandthermalconfinements.Thesamplethenexhibitsphotoacousticeffectasitabsorbsenergyfromthelaser whichresultsinheatemission,transientthermoelasticexpansion,andleadstogeneration ofultrasoundwave [69,70].Thegeneratedacousticwaveisdetectedbyultrasoundtransducersandrecordedasafunctionoftimewhichthenisconvertedbasedonthesound speedinthesampleintoaone-dimensionaldepth-resolvedimage,alsocalledan A-line.ByaligningtheA-linesbasedontheirspatiallocation,atransverselinearscan ofthepointlaserilluminationonthesamplecanmakea2Dimage.Fromtherea2Draster scanofthepointofilluminationcreatesa3Dimage.PATcanbecategorizedasphotoacousticcomputedtomography(PACT)orphotoacousticmicroscopy(PAM).PACTusesan arrayofultrasonictransducers(multiplesingleelement,linear,phased,ring,circular,or sphericalarrays)todetectPAwavesemittedfromanobjectatmultipleviewangles [82] whilePAMusestherasterscanningmethod [83].Eventhoughahigherpenetrationdepth canbeachievedusingPACT,itcomesattheexpenseofcoerceresolution,system,and computationalcosts [84].Ontheotherhand,higherresolutionPAMsystemscanbeclassifiedbasedontheirspatialresolutionorthetypeofscanningtheyusewithlimitedpenetrationdepth.Forspatialresolution,PAMsystemscanbeeitheracousticresolution wheretheimagingresolutionisbasedonthefocusoftheultrasonicdetector [85] oropticalresolutionwheretheresolutionisdeterminedbytheopticalfocalspot [86].Asforthe scanningclassifications,thereismechanicalscanningwhichsimultaneouslytranslates theopticalilluminationandultrasounddetectionforvolumetricimaging [87] andoptical scanningwherethereisasetofgalvanometerswhichmaintaintheultrasounddetection stationarywhiletheyscanafocusedopticalillumination [87].Currently,PAiscapableof imagingstructuresinboththeanteriorandposteriorsegmentsoftheeye.Originally,ithad beenusedtoexamineocularstructuressuchastheirisorretinalvasculaturequalitatively
[88],butcurrentPAIfocusesonthequantificationofpropertieslikesO2 [87] orretinaloxygenmetabolicrate(rMRO2) [89] intheeye.ThemajorstructurethatPAIcurrentlyfocuses onintheanteriorsegmentoftheeyeistheiris,specificallytheredbloodcellsinthemicrovasculatureandmelaninoftheiris [62].Whilebothmechanical-scanning acoustic-resolutionPAM(AR-PAM)andoptical-resolutionPAM(OR-PAM)havebeen usedtoimagetheiris,onlymechanical-scanningOR-PAMhasbeenabletoobtain high-resolutionimagesofirismicrovasculature [90].Thesystemworksbyfocusinglaser illuminationlightontotheirismicrovasculatureusingamicroscopeobjectivelens [91] Awatertankisplacedoverthesubject’seyesothatafocusedultrasonicdetectorcan receivetheultrasonicsignalsemittedfromtheiris [91] .Additionally,sO2 oftheiris microvasculaturecanbemeasuredbyusingtwo excitationwavelengthsthathavedifferentoxy-hemoglobinanddeoxy-hemoglobinabsorptioncoefficients [91].Irismelanin hasalsobeenmeasuredbyPAIusingmechanical-scanningOR-PAM [91] .However, unlikethesO2 oftheirismicrovasculatureonlyqualitativemeasuringofirismelanin hasbeenperformed [84].Insteadoftheiris,thefocusofPAIintheposteriorsegment istheredbloodcellsintheretinalandchoro idalmicrovasculaturealongwithmelanin intheRPE [62] .Bothmechanical-scanningOR-PAMandAR-PAMhavebeenusedto imagetheposteriorsegmentoftheeye [92],buttheresolutionistoolowtovisualize themicrovasculatureinAR-PAM [92] andinOR-PAMthelensattenuatestheultrasonic signalsresultinginreducedsignal-to-noiseratio(SNR)oftheimages [93].Toovercome this,optical-scanningPAmicroscopy(OS-PAM)wasdeveloped [87] .UnlikemechanicalscanningOR-PAM,OS-PAMusesapulsedlasercoupledtoa1 2-single-modeoptical fiber [87] .Oneoftheoutputsallowedforthecompens ationoflaserintensityvariation, whiletheotherwasdirectedtothecorneausingapairofgalvanometermirrorsanda pairoftelescopelenses [87].Additionally,OS-PAMusesanultrasonicneedletransducer todetectPAwaves,thuseliminatingtheneedforawatertank [62].Moreover,theneedle preventsmajorsignalattenuat ionresultinginhighSNRimages [62] .Lastly,althoughit hasnotbeenusedinPAIoftheeye,contrastagentsimprovePAimagequality [94] and extendthescopeofPAItothegeneticandmolecularlevel [95].Someofthecontrast agentsusedlikeEvansblue [96],indocyaninegreen [97],andnanoparticles [98] are alreadycommonophthalmiccontrastagentst husinvitingthepossibilityofusingthem withocularPAM.
Unfortunately,whilePAIshowsalotofpromiseasanupcomingocularimagingmodality,itisrelativelynewandhasmanylimitationsthatneedtobeaddressedbeforetheclinicaltranslation.First,photoacousticsignaldetectionrequiresphysicalcontactwiththe eye.Whetheritisawatertankoraneedletransducerwithultrasonicgel,bothcause patientdiscomfortandarenotsuitableforclinicalsettings [62].Additionally,physical motionforsaccadesorheadmovementcandisruptPAI.Whiletherehavebeenstrides takentofixthisproblem,therearemanyconcernsabouttheperformancestabilityand detectionsensitivitywiththesenoncontactPAmethods [62].Second,OS-PAMstill requiresextendedimagingdepthforboththeretinaandthechoroid,highresolution forRPEmelanin,andfastimagingspeedstoreducemotionartifacts.Fordepth,optical
clearingagentscouldbeused [99] buttheyarenotusableforinvivoimagingandNIRlight couldbeusedbutthehigh-powerexcitationisasafetyconcern [100].Forimprovingthe resolutionofPA,onecouldpotentiallyincreasethelateralresolutionbyusingthesyntheticaperturetechnique [101].Asforaxialresolution,abroadultrasonicbandwidthdoes increasetheaxialresolution;however,highersensitivityinOS-PAMisachievedwithanarrowerbandwidth [102].Abalanceneedstobedeterminedtomaximizebothaxialresolutionanddetectionsensitivity.Finally,higherimagingspeedcouldreducemotionartifacts andwhileincreasingthelaserrepetitionratecanincreaseimagingspeed,itislimitedby theultrasoundpropagationtimefromtheposterioreye.Lastly,beforePAIcanbeclinically adapted,itrequiresnumerousanimalstudiestoconfirmthelongitudinalperformance stabilityofPAmeasurementsintheeye.Furthermore,thereislimitedknowledgeabout PAIfortheearlydetectionofoculardisease [62].Finally,studieshaveshownthatvisual stimulationoftheretinacanresultinchangestoretinalvesseldiameter,bloodflow, andsO2 [103].Therefore,furtherstudiesareneededtoshedlightontheeffectofvisual lightilluminationonOS-PAMaccuracy.
ThebiggestadvantageofOS-PAMisthatmultimodalimagingisachievablebycombiningOS-PAMwithotherimagingmodalities.Thedevelopmentofmultimodalmicroscopic imagingtechniqueshasbecomeincreasinglyimportantinthebiomedicalcommunityas itprovidescomprehensivephysiologicalinformationaboutbiologicaltissues [104].In thecaseofocularimaging,mostopticalimagemodalitiesworkbydetectingthescattering oflightreflectedfromtheeyeorfluorescentlightstimulatedinthesample.Theproblemis thatthesemodalitiesrequiretheback-travelingofphotonsfromthesample,sotheycannotmeasuretheopticalabsorption.Therefore,OS-PAMcomplementsthesemodalities wellbecauseitiscurrentlytheonlyopticalabsorption-basedimagingmodality [84].Thus, bycombiningthetwo,onecangetanatomicalinformation,likecellularlayerorganization oftheretina,frompreexistingocularimagingtechniquesandmolecularinformation, likesO2,fromOS-PAMwhichgivesaquantitative,holisticimageoftheeye.OS-PAM canbecombinedwithautofluorescenceimaging [105],fluoresceinangiography [65], SLO [84],andmostimportantlyOCT.OCTaddstoOS-PAMbyallowingfordetailed, high-resolution,retinalandchoroidalstructuralinformation [105].Additionally,byusing repeatedOCTscanning,completeretinalvasculaturemappingispossible [106].Furthermore,OCTcanquantitativelymeasureretinalbloodflowrateandvelocitybydetectingthe Dopplerphaseshiftsproducedbymovingblood [107].Finally,OCTcanbeusedtoguide OS-PAMsothatanareaofinterestonposteriorsegmentcanbeimaged [108].
Ocularimaginghascomealongwaysincethefirstimageoftheretinain1886.The additionofopticalimagingmodalitiestoophthalmologyhasintroducedfasterandmore precisemethodsforphysicianstomonitoranddiagnoseocularpathologies.Whilefundus photography,SLO,andOCThaveadvancedocularimagingtoalargedegree,theyhave clearlimitationsinbeingopticalscattering-basedimagingmodalitiesaspresentedin Table1.Therefore,theintroductionofphotoacousticimagingtoophthalmologycould leadtothedevelopmentofanovel,stand-alonemodalityand/oracomplimentarymodalitytoOCTandSLOthatcouldadvancethefieldofocularimaging.
Table1 Listofophthalmologicalimagingmodalitiesandtheirapplications, advantages,andlimitations.
TechnologyApplicationsAdvantagesLimitations
Fundus photography
Retinalfundusimaging, diabetes,ARMD,glaucoma, neoplasmsoftheeye
SLORetinalvesseloximetry, reflectometry, angioscotometry,fundus perimetrydiabeticretinopathy, age-relatedmacular degeneration,scanningthe nerveheadinglaucoma,and imagingtheretinalnerve fiberlayer
OCTMacularedema,macular degeneration,glaucoma, multiplesclerosis
Quickandsimpletechniqueto master,trueviewoftheretina, observesalargerretinalfieldat anyonetimecomparedwith ophthalmoscopy,highpatient compliance,abletomonitor progressionofdiseases,andlow costcomparedtootherimaging modalities
Highlateralresolution,fast imaging,high-qualityimages, patientcomfort,andvideo capability
Imageproducedis2D,difficulty observingandassessing abnormalitiesduetolackof depthappreciationonimages, lessmagnificationandimage clarity,conditionssuchas cataractsreduceimageclarity, artifacterrorsmayproduce unusualimages
Lowdepthresolution,high maintenancecost,affectedby motionartifacts,distortionof imageattheperipheryandlight scatteringaffectssO2
Highlateralanddepth resolution
PAOMsO2 andRPEimagingOpticalabsorptionbased, mediumdepthperception, andmultimodalimagingwith othermodalities
References
BasedOCThaspoordelineation ofbloodvesselsandlimitedfield ofviewinOCTangiography
Onlyopticalabsorptionimaging, currentlyrequiresphysical contact,needsmoretesting beforeclinicallyavailable
[1] A.Taruttis,V.Ntziachristos,Advancesinreal-timemultispectraloptoacousticimaginganditsapplications,Nat.Photonics9(4)(2015)219.
[2] B.I.Gramatikov,Moderntechnologiesforretinalscanningandimaging:anintroductionforthe biomedicalengineer,Biomed.Eng.Online13(1)(2014)52.
[3] R.H.Webb,G.W.Hughes,Scanninglaserophthalmoscope,IEEETrans.Biomed.Eng.7(1981) 488–492.
[4] D.Huang,etal.,Opticalcoherencetomography,Science254(5035)(1991)1178–1181.
[5] A.Bajwa,R.Aman,A.K.Reddy,Acomprehensivereviewofdiagnosticimagingtechnologiesto evaluatetheretinaandtheopticdisk,Int.Ophthalmol.35(5)(2015)733–755.
[6] D.Y.Lin,etal.,Thesensitivityandspecificityofsingle-fieldnonmydriaticmonochromaticdigital fundusphotographywithremoteimageinterpretationfordiabeticretinopathyscreening:acomparisonwithophthalmoscopyandstandardizedmydriaticcolorphotography,AmJ.Ophthalmol. 134(2)(2002)204–213.
[7] R.H.Webb,Opticsforlaserrasters,Appl.Opt.23(20)(1984)3680–3683.
[8] M.Minsky,Memoironinventingtheconfocalscanningmicroscope,Scanning10(4)(1988)128–138.
[9] P.Vieira,etal.,Tomographicreconstructionoftheretinausingaconfocalscanninglaserophthalmoscope,Physiol.Meas.20(1)(1999)1.
[10] P.Vieira,etal.,Truecolourimagingofthefundususingascanninglaserophthalmoscope,Physiol. Meas.23(1)(2001)1.
[11] A.E.Elsner,etal.,Reflectometrywithascanninglaserophthalmoscope,Appl.Opt.31(19)(1992) 3697–3710.
[12] A.Remky,E.Beausencourt,A.E.Elsner,Angioscotometrywiththescanninglaserophthalmoscope. Comparisonoftheeffectofdifferentwavelengths,Invest.Ophthalmol.Vis.Sci.37(11)(1996) 2350–2355.
[13] A.Lompado,etal.,Multispectralconfocalscanninglaserophthalmoscopeforretinalvesseloximetry,in:SpectralImaging:Instrumentation,Applications,andAnalysis,InternationalSocietyfor OpticsandPhotonics,2000.
[14] A.Remky,etal.,Blue-on-yellowperimetrywithascanninglaserophthalmoscope:smallalterations inthecentralmaculawithaging,JOSAA18(7)(2001)1425–1436.
[15] W.Wykes,A.Pyott,Y.Ferguson,Detectionofdiabeticretinopathybyscanninglaserophthalmoscopy,Eye8(4)(1994)437.
[16] A.Manivannan,etal.,Clinicalinvestigationofaninfrareddigitalscanninglaserophthalmoscope, Br.J.Ophthalmol.78(2)(1994)84–90.
[17] G.Seymenog ˘ lu,E.Bas ¸ er,B. Ozturk,Comparisonofspectral-domainopticalcoherencetomography andHeidelbergretinatomographIIIopticnerveheadparametersinglaucoma,Ophthalmologica 229(2)(2013)101–105.
[18] E.W.Chan,etal.,DiagnosticperformanceoftheISNTruleforglaucomabasedontheHeidelberg retinaltomograph,Transl.Vis.Sci.Technol.2(5)(2013)2.
[19] J.Liang,D.R.Williams,D.T.Miller,Supernormalvisionandhigh-resolutionretinalimagingthrough adaptiveoptics,JOSAA14(11)(1997)2884–2892.
[20] S.A.Burns,etal.,Large-field-of-view,modular,stabilized,adaptive-optics-basedscanninglaser ophthalmoscope,JOSAA24(5)(2007)1313–1326.
[21] C.A.Puliafito,etal.,Imagingofmaculardiseaseswithopticalcoherencetomography, Ophthalmology102(2)(1995)217–229.
[22] A.Fercher,K.Mengedoht,W.Werner,Eye-lengthmeasurementbyinterferometrywithpartially coherentlight,Opt.Lett.13(3)(1988)186–188.
[23] M.Pircher,R.J.Zawadzki,ReviewofadaptiveopticsOCT(AO-OCT):principlesandapplicationsfor retinalimaging,Biomed.Opt.Express8(5)(2017)2536–2562.
[24] W.Drexler,etal.,Opticalcoherencetomographytoday:speed,contrast,andmultimodality, J.Biomed.Opt.19(7)(2014)071412.
[25] J.A.Izatt,etal.,InvivobidirectionalcolorDopplerflowimagingofpicoliterbloodvolumesusing opticalcoherencetomography,Opt.Lett.22(18)(1997)1439–1441.
[26] R.A.Leitgeb,etal.,Real-timemeasurementofinvitroflowbyFourier-domaincolorDoppleroptical coherencetomography,Opt.Lett.29(2)(2004)171–173.
[27] M.Ang,etal.,Opticalcoherencetomographyangiography:areviewofcurrentandfutureclinical applications,GraefesArch.Clin.Exp.Ophthalmol.256(2)(2018)237–245.
[28] S.S.Gao,etal.,Opticalcoherencetomographyangiography,Invest.Ophthalmol.Vis.Sci.57(9) (2016)OCT27–OCT36.
[29] P.A.Keane,S.R.Sadda,Retinalimaginginthetwenty-firstcentury:stateoftheartandfuturedirections,Ophthalmology121(12)(2014)2489–2500.
Chapter1 •Complementarycapabilitiesofphotoacousticimaging11
[30] X.Shu,L.J.Beckmann,H.F.Zhang,Visible-lightopticalcoherencetomography:areview,J.Biomed. Opt.22(12)(2017)121707.
[31] H.Koizumi,M.C.Pozzoni,R.F.Spaide,Fundusautofluorescenceinbirdshotchorioretinopathy, Ophthalmology115(5)(2008)e15–e20.
[32] T.Otani,S.Kishi,Y.Maruyama,Patternsofdiabeticmacularedemawithopticalcoherencetomography,AmJ.Ophthalmol.127(6)(1999)688–693.
[33] A.Hassenstein,A.A.Bialasiewicz,G.Richard,Opticalcoherencetomographyinuveitispatients,Am J.Ophthalmol.130(5)(2000)669–670.
[34] N.N.Markomichelakis,etal.,Patternsofmacularedemainpatientswithuveitis:qualitativeand quantitativeassessmentusingopticalcoherencetomography,Ophthalmology111(5)(2004) 946–953.
[35] I.Krebs,etal.,Activityofneovascularlesionstreatedwithbevacizumab:comparisonbetweenopticalcoherencetomographyandfluoresceinangiography,GraefesArch.Clin.Exp.Ophthalmol. 246(6)(2008)811–815.
[36] I.I.Bussel,G.Wollstein,J.S.Schuman,OCTforglaucomadiagnosis,screeninganddetectionofglaucomaprogression,Br.J.Ophthalmol.98(Suppl.2)(2014)ii15–ii19.
[37] J.W.Jeoung,etal.,Macularganglioncellimagingstudy:glaucomadiagnosticaccuracyofspectraldomainopticalcoherencetomography,Invest.Ophthalmol.Vis.Sci.54(7)(2013)4422–4429.
[38] I.Maruko,etal.,SubfovealchoroidalthicknessaftertreatmentofVogt–Koyanagi–Haradadisease, Retina31(3)(2011)510–517.
[39] Y.S.Modi,etal.,Multimodalimagingofsarcoidchoroidalgranulomas,J.OphthalmicInflamm. Infect.3(1)(2013)58.
[40] P.A.Keane,etal.,Characterizationofbirdshotchorioretinopathyusingextramacularenhanced depthopticalcoherencetomography,JAMAOphthalmol.131(3)(2013)341–350.
[41] D.Goldenberg,etal.,Vitreal,retinal,andchoroidalfindingsinactiveandscarredtoxoplasmosis lesions:aprospectivestudybyspectral-domainopticalcoherencetomography,GraefesArch.Clin. Exp.Ophthalmol.251(8)(2013)2037–2045.
[42] A.Hojjatoleslami,M.R.N.Avanaki,OCTskinimageenhancementthroughattenuationcompensation,Appl.Opt.51(21)(2012)4927–4935.
[43] M.R.N.Avanaki,etal.,SpatialcompoundingalgorithmforspecklereductionofdynamicfocusOCT images,IEEEPhoton.Technol.Lett.25(15)(2013)1439–1442.
[44] S.Hojjatoleslami,M.Avanaki,A.G.Podoleanu,Imagequalityimprovementinopticalcoherence tomographyusingLucy–Richardsondeconvolutionalgorithm,Appl.Opt.52(23)(2013)5663–5670.
[45] M.R.Avanaki,etal.,Quantitativeevaluationofscatteringinopticalcoherencetomographyskin imagesusingtheextendedHuygens–Fresneltheorem,Appl.Opt.52(8)(2013)1574–1580.
[46] M.R.N.Avanaki,etal.,Investigationofbasalcellcarcinomausingdynamicfocusopticalcoherence tomography,Appl.Opt.52(10)(2013)2116–2124.
[47] M.R.N.Avanaki,A.Hojjat,A.G.Podoleanu,Investigationofcomputer-basedskincancerdetection usingopticalcoherencetomography,J.Mod.Opt.56(13)(2009)1536–1544.
[48] S.Adabi,etal.,Universalinvivotexturalmodelforhumanskinbasedonopticalcoherencetomograms,Sci.Rep.7(1)(2017)1–11.
[49] M.R.N.Avanaki,A.Hojjatoleslami,Skinlayerdetectionofopticalcoherencetomographyimages, Optik124(22)(2013)5665–5668.
[50] S.Adabi,etal.,Opticalcoherencetomographytechnologyandqualityimprovementmethodsfor opticalcoherencetomographyimagesofskin:ashortreview,Biomed.Eng.Comput.Biol. 8(2017).1179597217713475.
[51] A.Taghavikhalilbad,etal.,Semi-automatedlocalizationofdermalepidermaljunctioninoptical coherencetomographyimagesofskin,Appl.Opt.56(11)(2017)3116–3121.
[52] M.Faiza,etal.,High-resolutionwavelet-fractalcompressedopticalcoherencetomographyimages, Appl.Opt.56(4)(2017)1119–1123.
[53] M.R.Avanaki,A.Podoleanu,En-facetime-domainopticalcoherencetomographywithdynamic focusforhigh-resolutionimaging,J.Biomed.Opt.22(5)(2017)056009.
[54] Z.Turani,etal.,Opticalradiomicsignaturesderivedfromopticalcoherencetomographyimagesto improveidentificationofmelanoma,CancerRes.79(8)(2019)2021–2030.
[55] S.Adabi,etal.,Anoverviewofmethodstomitigateartifactsinopticalcoherencetomographyimagingoftheskin,SkinRes.Technol.24(2)(2018)265–273.
[56] T.J.Bennett,C.J.Barry,Ophthalmicimagingtoday:anophthalmicphotographer’sviewpoint—a review,Clin.Exp.Ophthalmol.37(1)(2009)2–13.
[57] D.X.Hammer,etal.,Compactscanninglaserophthalmoscopewithhigh-speedretinaltracker,Appl. Opt.42(22)(2003)4621–4632.
[58] B.Chou,Limitationsofthepanoramic200Optomap,Optom.Vis.Sci.80(10)(2003)671–672.
[59] R.F.Spaide,Peripheralareasofnonperfusionintreatedcentralretinalveinocclusionasimagedby wide-fieldfluoresceinangiography,Retina31(5)(2011)829–837.
[60] R.W.Dunphy,etal.,Structuralfeaturesanteriortotheretinarepresentedinpanoramicscanning laserfundusimages,OphthalmicSurg.LasersImagingRetina39(2)(2008)160–163.
[61] M.Zhang,etal.,Projection-resolvedopticalcoherencetomographicangiography,Biomed.Opt. Express7(3)(2016)816–828.
[62] W.Liu,H.F.Zhang,Photoacousticimagingoftheeye:aminireview,Photo-Dermatology4(3)(2016) 112–123.
[63] D.-Y.Yu,S.J.Cringle,Oxygendistributionandconsumptionwithintheretinainvascularisedand avascularretinasandinanimalmodelsofretinaldisease,Prog.Retin.EyeRes.20(2)(2001)175–208.
[64] P.A.Campochiaro,Molecularpathogenesisofretinalandchoroidalvasculardiseases,Prog.Retin. EyeRes.49(2015)67–81.
[65] S.H.Hardarson,E.Stefa ´ nsson,Retinaloxygensaturationisalteredindiabeticretinopathy,Br.J. Ophthalmol.96(4)(2012)560–563.
[66] O.B.Olafsdottir,etal.,Retinaloximetryinprimaryopen-angleglaucoma,Invest.Ophthalmol.Vis. Sci.52(9)(2011)6409–6413.
[67] S.H.Hardarson,E.Stefansson,Oxygensaturationincentralretinalveinocclusion,AmJ.Ophthalmol.150(6)(2010)871–875.
[68] T.T.Berendschot,etal.,Influenceofluteinsupplementationonmacularpigment,assessedwithtwo objectivetechniques,Invest.Ophthalmol.Vis.Sci.41(11)(2000)3322–3326.
[69] S.L.Jacques,Opticalpropertiesofbiologicaltissues:areview,Phys.Med.Biol.58(11)(2013)R37.
[70] M.Xu,L.V.Wang,Photoacousticimaginginbiomedicine,Rev.Sci.Instrum.77(4)(2006)041101.
[71] M.Nasiriavanaki,etal.,High-resolutionphotoacoustictomographyofresting-statefunctional connectivityinthemousebrain,Proc.Natl.Acad.Sci.111(1)(2014)21–26.
[72] J.Yao,etal.,Noninvasivephotoacousticcomputedtomographyofmousebrainmetabolisminvivo, NeuroImage64(2013)257–266.
[73] M.Mozaffarzadeh,etal.,Linear-arrayphotoacousticimagingusingminimumvariance-baseddelay multiplyandsumadaptivebeamformingalgorithm,J.Biomed.Opt.23(2)(2018)026002.
[74] J.Xia,etal.,Wide-fieldtwo-dimensionalmultifocaloptical-resolutionphotoacoustic-computed microscopy,Opt.Lett.38(24)(2013)5236–5239.
[75] A.-R.Mohammadi-Nejad,etal.,Neonatalbrainresting-statefunctionalconnectivityimaging modalities,Photoacoustics10(2018)1–19.
[76] S.Mahmoodkalayeh,etal.,Lowtemperature-mediatedenhancementofphotoacousticimaging depth,Sci.Rep.8(1)(2018)4873.
[77] N.Meimani,etal.,Anumericalanalysisofasemi-drycouplingconfigurationinphotoacoustic computedtomographyforinfantbrainimaging,Photo-Dermatology7(2017)27–35.
[78] R.Manwar,M.Hosseinzadeh,A.Hariri,K.Kratkiewicz,S.Noei,R.Mohammad,N.Avanaki,Photoacousticsignalenhancement:towardsutilizationoflowenergylaserdiodesinreal-timephotoacousticimaging,Sensors18(10)(2018)3498.
[79] L.Mohammadi,H.Behnam,M.Nasiriavanaki,Modelingskull’sacousticattenuationanddispersion onphotoacousticsignal,in:PhotonsPlusUltrasound:ImagingandSensing,InternationalSociety forOpticsandPhotonics,2017.
[80] M.Zafar,etal.,Developmentoflow-costfastphotoacousticcomputedtomography:systemcharacterizationandphantomstudy,Appl.Sci.9(3)(2019)374.
[81] J.Yao,etal.,Label-freeoxygen-metabolicphotoacousticmicroscopyinvivo,J.Biomed.Opt.16(7) (2011)076003.
[82] A.Fatima,etal.,Reviewofcostreductionmethodsinphotoacousticcomputedtomography,PhotoDermatology15(2019)100137.
[83] S.Hu,etal.,Functionaltranscranialbrainimagingbyoptical-resolutionphotoacousticmicroscopy, J.Biomed.Opt.14(4)(2009)040503.
[84] B.T.Cox,etal.,Quantitativespectroscopicphotoacousticimaging:areview,J.Biomed.Opt.17(6) (2012)061202.
[85] L.V.Wang,L.Gao,Photoacousticmicroscopyandcomputedtomography:frombenchtobedside, Annu.Rev.Biomed.Eng.16(2014)155–185.
[86] M.Xu,L.V.Wang,Universalback-projectionalgorithmforphotoacousticcomputedtomography, Phys.Rev.E71(1)(2005)016706.
[87] W.Xing,etal.,Integratedoptical-andacoustic-resolutionphotoacousticmicroscopybasedonan opticalfiberbundle,Opt.Lett.38(1)(2013)52–54.
[88] K.Maslov,etal.,Optical-resolutionphotoacousticmicroscopyforinvivoimagingofsinglecapillaries,Opt.Lett.33(9)(2008)929–931.
[89] W.Song,etal.,Integratingphotoacousticophthalmoscopywithscanninglaserophthalmoscopy, opticalcoherencetomography,andfluoresceinangiographyforamultimodalretinalimaging platform,J.Biomed.Opt.17(6)(2012)061206.
[90] S.Jiao,etal.,Photoacousticophthalmoscopyforinvivoretinalimaging,Opt.Express18(4)(2010) 3967–3972.
[91] S.N.Hennen,etal.,Photoacoustictomographyimagingandestimationofoxygensaturationof hemoglobininoculartissueofrabbits,Exp.EyeRes.138(2015)153–158.
[92] S.Hu,etal.,Label-freephotoacousticophthalmicangiography,Opt.Lett.35(1)(2010)1–3.
[93] J.M.Thijssen,H.J.M.Mol,M.R.Timmer,Acousticparametersofoculartissues,UltrasoundMed. Biol.11(1)(1985)157–161.
[94] G.P.Luke,D.Yeager,S.Y.Emelianov,Biomedicalapplicationsofphotoacousticimagingwithexogenouscontrastagents,Ann.Biomed.Eng.40(2)(2012)422–437.
[95] W.Li,X.Chen,Goldnanoparticlesforphotoacousticimaging,Nanomedicine(London,England) 10(2)(2015)299–320.
[96] J.Yao,etal.,Evansbluedye-enhancedcapillary-resolutionphotoacousticmicroscopyinvivo, J.Biomed.Opt.14(5)(2009)054049.