DiabetesandFundusOCT
Elsevier
Radarweg29,POBox211,1000AEAmsterdam,Netherlands TheBoulevard,LangfordLane,Kidlington,OxfordOX51GB,UnitedKingdom 50HampshireStreet,5thFloor,Cambridge,MA02139,UnitedStates
©2020ElsevierInc.Allrightsreserved.
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans,electronicor mechanical,includingphotocopying,recording,oranyinformationstorageandretrievalsystem,without permissioninwritingfromthepublisher.Detailsonhowtoseekpermission,furtherinformationaboutthe Publisher’spermissionspoliciesandourarrangementswithorganizationssuchastheCopyrightClearance CenterandtheCopyrightLicensingAgency,canbefoundatourwebsite: www.elsevier.com/permissions.
ThisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythePublisher (otherthanasmaybenotedherein).
Notices
Knowledgeandbestpracticeinthisfieldareconstantlychanging.Asnewresearchandexperiencebroadenour understanding,changesinresearchmethods,professionalpractices,ormedicaltreatmentmaybecome necessary.
Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgeinevaluatingandusing anyinformation,methods,compounds,orexperimentsdescribedherein.Inusingsuchinformationormethods theyshouldbemindfuloftheirownsafetyandthesafetyofothers,includingpartiesforwhomtheyhavea professionalresponsibility.
Tothefullestextentofthelaw,neitherthePublishernortheauthors,contributors,oreditors,assumeanyliability foranyinjuryand/ordamagetopersonsorpropertyasamatterofproductsliability,negligenceorotherwise,or fromanyuseoroperationofanymethods,products,instructions,orideascontainedinthematerialherein.
LibraryofCongressCataloging-in-PublicationData
AcatalogrecordforthisbookisavailablefromtheLibraryofCongress
BritishLibraryCataloguing-in-PublicationData AcataloguerecordforthisbookisavailablefromtheBritishLibrary
ISBN:978-0-12-817440-1
ForinformationonallElsevierpublications visitourwebsiteat https://www.elsevier.com/books-and-journals
Publisher: StacyMasucci
AcquisitionsEditor: TariK.Broderick
EditorialProjectManager: SamanthaAllard
ProductionProjectManager: MariaBernard
CoverDesigner: MatthewLimbert
TypesetbySPiGlobal,India
Contributors
WaleedHabibAbdulla DepartmentofElectrical,ComputerandSoftwareEngineering, TheUniversityofAuckland,Auckland,NewZealand
EdiAbdurachman BinusGraduateProgram,BinaNusantaraUniversity,Jakarta, Indonesia
AhmedAboelfetouh InformationSystemsDepartment,FacultyofComputersand Information,MansouraUniversity,Mansoura,Egypt
MarahTalalAlhalabi ElectricalandComputerEngineeringDepartment,AbuDhabi University,AbuDhabi,UnitedArabEmirates
ZahraAmini MedicalImageandSignalProcessingResearchCenter,SchoolofAdvanced TechnologiesinMedicine,IsfahanUniversityofMedicalSciences,Isfahan,Iran
PunalM.Arabi BMEDept,ACSCollegeofEngineering,Bangalore,India
SandraAvila InstituteofComputing,UniversityofCampinas(Unicamp),Campinas, Brazil
FrancescoBandello DepartmentofOphthalmology,UniversityVita-Salute,Scientific InstituteSanRaffaele,Milan,Italy
EnricoBorrelli DepartmentofOphthalmology,UniversityVita-Salute,ScientificInstitute SanRaffaele,Milan,Italy
WidodoBudiharto BinusGraduateProgram,BinaNusantaraUniversity,Jakarta, Indonesia
AdrianoCarnevali DepartmentofOphthalmology,UniversityMagnaGraecia,Catanzaro, Italy
RenohJohnsonChalakkal DepartmentofElectrical,ComputerandSoftware Engineering,TheUniversityofAuckland,Auckland;oDocsEyeCareLtd.,Dunedin, NewZealand
EleonoraCorbelli DepartmentofOphthalmology,UniversityVita-Salute,Scientific InstituteSanRaffaele,Milan,Italy
PremaDaigavane ElectronicsEngineering,G.H.RaisoniCollegeofEngineering,Nagpur, India
GlanDevadas ElectronicsandInstrumentationEngineering,VimalJyothiEngineering College,Kannur,Kerala,India
D.AntoSahayaDhas ElectronicsandCommunicationEngineering,VimalJyothi EngineeringCollege,Kannur,Kerala,India
NabilaEladawi BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
AymanEl-Baz BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
MohammedElmogy BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
AlexandreFerreira InstituteofComputing,UniversityofCampinas(Unicamp), Campinas,Brazil
HarryW.Flynn,Jr BascomPalmerEyeInstitute,DepartmentofOphthalmology, UniversityofMiamiMillerSchoolofMedicine,Miami,FL,UnitedStates
MohammedGhazal ElectricalandComputerEngineeringDepartment,AbuDhabi University,AbuDhabi,UnitedArabEmirates
ShengChiongHong oDocsEyeCareLtd.,Dunedin,NewZealand
G.Indumathi MepcoSchlenkEngineeringCollege,Sivakasi,India
GayatriJoshi BMEDept,ACSCollegeofEngineering,Bangalore,India
AnoopBalakrishnanKadan ElectronicsandCommunicationEngineering,VimalJyothi EngineeringCollege,Kannur,Kerala,India
RaheleKafieh MedicalImageandSignalProcessingResearchCenter,SchoolofAdvanced TechnologiesinMedicine,IsfahanUniversityofMedicalSciences,Isfahan,Iran
NikitaKashyap ElectronicsandCommunicationEngineering,Dr.C.V.RamanUniversity, Bilaspur,Chhattisgarh,India
RobertKeynton BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
AshrafKhalil ComputerScienceDepartment,CollegeofEngineering,AbuDhabi University,AbuDhabi,UnitedArabEmirates
RosaLozada DepartmentofOphthalmology,UniversityofPuertoRicoSchoolof Medicine,SanJuan,PR,UnitedStates
AliH.Mahmoud BioengineeringDepartment,UniversityofLouisville,Louisville,KY, UnitedStates
HatemMahmoud DepartmentofOphthalmology,FacultyofMedicine,Al-Azhar University,Cairo,Egypt;BioengineeringDepartment,UniversityofLouisville, Louisville,KY,UnitedStates
K.C.Manoj ElectronicsandCommunicationEngineering,VimalJyothiEngineering College,Kannur,Kerala,India
ElahehMousavi MedicalImageandSignalProcessingResearchCenter,Schoolof AdvancedTechnologiesinMedicine,IsfahanUniversityofMedicalSciences,Isfahan,Iran
WaniPatil ElectronicsEngineering,G.H.RaisoniCollegeofEngineering,Nagpur,India
RamonPires InstituteofComputing,UniversityofCampinas(Unicamp),Campinas, Brazil
GiuseppeQuerques DepartmentofOphthalmology,UniversityVita-Salute,Scientific InstituteSanRaffaele,Milan,Italy
LeaQuerques DepartmentofOphthalmology,UniversityVita-Salute,ScientificInstitute SanRaffaele,Milan,Italy
HosseinRabbani MedicalImageandSignalProcessingResearchCenter,Schoolof AdvancedTechnologiesinMedicine,IsfahanUniversityofMedicalSciences,Isfahan,Iran
AlaaRiad InformationSystemsDepartment,FacultyofComputersandInformation, MansouraUniversity,Mansoura,Egypt
AndersonRocha InstituteofComputing,UniversityofCampinas(Unicamp),Campinas, Brazil
T.V.Roshini ElectronicsandCommunicationEngineering,VimalJyothiEngineering College,Kannur,Kerala,India
BoySubirosaSabarguna BinusGraduateProgram,BinaNusantaraUniversity,Jakarta, Indonesia
RiccardoSacconi DepartmentofOphthalmology,UniversityVita-Salute,Scientific InstituteSanRaffaele,Milan,Italy
PerumalSankar ElectronicsandCommunicationEngineering,TOCHInstituteofScience andTechnology,Ernakulam,Kerala,India
V.Sathananthavathi MepcoSchlenkEngineeringCollege,Sivakasi,India
ShlomitSchaal DepartmentofOphthalmologyandVisualSciences,Universityof MassachusettsMedicalSchool,Worcester,MA,UnitedStates
StephenG.Schwartz BascomPalmerEyeInstitute,DepartmentofOphthalmology, UniversityofMiamiMillerSchoolofMedicine,Miami,FL,UnitedStates
DharmendraKumarSingh ElectricalandElectronicsEngineering,Dr.C.V.Raman University,Bilaspur,Chhattisgarh,India
GirishKumarSingh ComputerScienceandApplications,Dr.HarisinghGourUniversity, Sagar,MadhyaPradesh,India
BambangKrismonoTriwijoyo BinusGraduateProgram,BinaNusantaraUniversity, Jakarta;BumigoraUniversity,Mataram,Indonesia
VictorM.Villegas DepartmentofOphthalmology,UniversityofPuertoRicoSchoolof Medicine,SanJuan,PR;BascomPalmerEyeInstitute,DepartmentofOphthalmology, UniversityofMiamiMillerSchoolofMedicine,Miami,FL,UnitedStates
JacquesWainer InstituteofComputing,UniversityofCampinas(Unicamp),Campinas, Brazil
Computer-aideddiagnosissystem basedonacomprehensivelocal featuresanalysisforearlydiabetic retinopathydetectionusingOCTA
NabilaEladawia,MohammedElmogya,MohammedGhazalb, HatemMahmoudc,AliH.Mahmouda,AshrafKhalild, AhmedAboelfetouhe,AlaaRiade,RobertKeyntona,AymanEl-Baza a BIOENGINEERINGDEPARTMENT,UNIVER SITYOFLOUISVILLE,LOUISVILLE,KY, UNITEDSTATES b ELECTRICALANDCOMPUTERENGINEERINGDEPARTMENT, ABUDHABIUNIVERSITY,ABU DHABI,UNITEDARABEMIRATES c DEPARTMENTOFOPHTHALMOLOGY,FACULTYOF MEDICINE,AL-AZHAR UNIVERSITY,CAIRO, EGYPT d COMPUTERSCIENCEDEPARTMENT,C OLLEGEOFENGINEERING,ABU DHABIUNIVERSITY,ABUDHABI,UNITEDARABEMIRATES e INFORMATIONSYSTEMS DEPARTMENT,FACULTYOFCOMPUTERSAND INFORMATION,MANSOURAUNIVERSITY, MANSOURA,EGYPT
1Introduction
Retinovasculardiseasesconstituteamajorcauseofvisionloss.Diabetesoveralongperiod givesrisetodeteriorationofsmallretinalbloodvessels.Theseretinalbloodvesselsleak fluidsandblood,whichcauseretinaltissueswelling.Asaresult,itmaycausediabeticretinopathy(DR),whichisasignificantcomplicationofdiabetes[1].Theclinicalfeatures, suchasneovascularization,microaneurysms,andhemorrhages,areseeninpeoplesufferingfromDR.Neovascularizationistheappearanceofnewunusualbloodvesselsinmany partsoftheeyecontaining,ofcourse,theretina.Thewallsofthesenewvesselsareweak andmaybreakandbleed.Oneoftheprimaryeffectsofneovascularizationandbleedingis theappearanceofnewvascularcrossoverandbifurcationpointsintheretinalvasculature network[2].Therefore,earlyandaccuratedetectionofthesesignsisimportanttoprevent blindnessandavoidDRcomplications.Manualdiagnosisandanalysisoftheretinal imagesisatime-consumingandtediousprocess.Thus,automaticdetectionanddiagnosiswillminimizetimeandeffort,whichwillhelpintheearlydetectionofthedisease[3]. Therearevariousimagingmodalitiesforretinathatestimatethestateoftheblood vasculaturenetwork.Theseincludefluoresceinangiography(FA),colorfundus,andoptical
coherencetomographyangiography(OCTA)images.TheOCTAisanewnoninvasiveimagingmodality,whichcapturesthebloodvasculaturenetworkinvariousplexusestoindicate differentlayersoftheretina.ByusingOCTAimagingmodality,theophthalmologistcaneasilyexamineavascularcapillary,superficialcapillary,anddeepcapillaryplexusesinaddition tochoroidandchoriocapillarisplexusesseparately[4].TheotheradvantageofOCTAisthat itallowsophthalmologiststomeasurefovealavascularzone(FAZ)andnonperfusionarea bilaterallywithoutobscurationbyleakageoffluoresceindye[5].Therefore,inthischapter, wehaveanalyzedOCTAimageswithtwodifferentretinalplexusestodetectanddiagnose mildDRcasesanddistinguishthemfromnormalcases.
Intheliterature,retinalimageanalysisisaveryrichresearcharea.Therearemany studiesthathavebeendonetodiagnosevariousretinaldiseasesbyanalyzingretinalblood vessels,retinallayers,orboth.Forinstance,Agemyetal.[6]haveintroducedamethod usingOCTAtomapretinalvascularperfusiondensityandtocomparevariousstagesof DR.Theyhavenoticedaconsiderabledecreaseinthedensityvaluesofthecapillary perfusionasDRprogresses.
Hwangetal.[7]haveintroducedamethodusingOCTAtodemonstratethechanges occurredintheareaofFAZinDRpatients.Theyhavenoticedthatthetotalareaofthe FAZisgreaterinDRthaninnormalcases.Hwangetal.[8]haveinvestigatedthemoresignificantfeaturesthatcanberetrievedfromOCTAscansforDRpatients.Stangaetal.[9] havedifferentiatedbetweenhealthyandDRpatientsinOCTAscansbasedontheenlargementoftheFAZareaforDRcases.
Takaseetal.[10]evaluatedtheFAZareausingOCTAimages.Theyhavenoticedthat diabeticeyesshowanincreaseinFAZareaascomparedwithhealthyeyes,irrespective oftheexistenceofDR.Bhanushalietal.[11]haveanalyzedtheareaoftheFAZ,thevessel density,thespacingbetweensmallvessels,andthespacingbetweenlargeonesbyapplyinglocalfractalanalysistothesuperficialanddeepretinalOCTAimages.Krawitzetal.[12] usedOCTAimagestoexaminetheaxisratiooftheFAZtodistinguishbetweenhealthyand diabeticpatients.Theyfoundasignificantdifferencebetweenthevaluesfornormalcases anddiabeticcases.
Tarassolyetal.[13]haveconductedanexperimenttoseethecapabilityofOCTAin detectingtheabnormalitiesintheimagesofDRpatientsandcompareditwithfundusfluoresceinangiography(FFA).Using120DReyes,theywereabletodetectmicroaneurysms, intraretinalmicrovascularabnormalities,andneovascularization.Theyconcludedthat OCTAhasahigherdetectionrateforintraretinalmicrovascularabnormalitiesthanFFA.
Ishibazawaetal.[14]haveevaluatedhowOCTAimagescancapturethefeaturesofDR. Theycollected47eyesforDRpatients.TheyhaveconcludedthatOCTAcouldobviously detectmicroaneurysms,neovascularization,andretinalnonperfusedareasinDR patients.TheyhavealsoconcludedthatOCTAimagescouldbeusedeffectivelytoevaluate thetreatmentofDR.
Soaresetal.[15]haveperformedanobservationalstudytocomparetheabilityFAand OCTAinclassifyingpatientswithDR.Theyused50DReyes,26ofthemfromDRpatients, andtwograderstogradeandclassifytheimages.TheyfoundoutthatOCTAisbetterin
gradingthecentralsubfieldandparafovealmaculavasculaturethanFAespeciallyforFAZ andcapillarydropout.
Freibergetal.[16]haveconductedanexperimenttoanalyzethedifferenceinFAZ dimensionsinhealthycontrolsandDRpatientsusingOCTAimages.Theyhaveused 29imagesofDRpatientsand25ofhealthycontrols.Inthesuperficiallayer,theyhave noticedanenlargementoftheFAZdiameterinDRsubjects.Thedifferencewasevenmore noticeableinthedeeplayer.TheyhaveconcludedthatOCTAcanaccuratelydistinguish betweennormalandDRpatientsusingFAZdimensions.
Youetal.[17]haveused22DRpatientsand15healthycontrolstoinvestigatetheability ofOCTAinmeasuringthevesselsdensityandhowaccuratelythesemeasurescandifferentiatebetweennormalanddiseasedsubjects.TheyhaveconcludedthatOCTAwasable tomeasurethevesseldensityinallsubjectsaccurately.Theresultsdemonstratedthat vesseldensityinDRpatientsislessthanthatinnormalsubjects.
Fromtheliteraturementionedearlier,itmaybenoticedthatmostofthepublished workconcentratedonprocessingtheOCTAimagesmanually.Also,ifitisautomatically processed,mostlyitwillbefundusimagesthatlackdepthinformation.Finally,mostof thecurrentcomputer-aideddiagnosis(CAD)systemsbasetheirdiagnosisonfeaturesthat wereextractedglobally.TodetecttheDRinitsearlystage,thesefeaturesmaynotbesufficient.Inthischapter,wehavetriedtoeliminatethelimitationsmentionedpreviouslyby presentingaCADsystemthatisabletosegmentbloodvesselsfromdifferentretinal plexusesusingOCTAimages.Then,fournewlyderivedlocalfeatureswereextractedto characterizetheappearanceandspatialstructureoftheretinalbloodvesselstoaidthe CADsysteminitsdiagnosis.
Therestofthechapterisorganizedasfollows. Section2 discussesthestructureofthe proposedOCTA-baseddiagnosissystem.Thefourextractedfeaturesareelucidatedin detail. Section3 describestheexperimentalresults.Finally, Section4 presentstheconclusionandthefuturework.
2Materialsandmethods
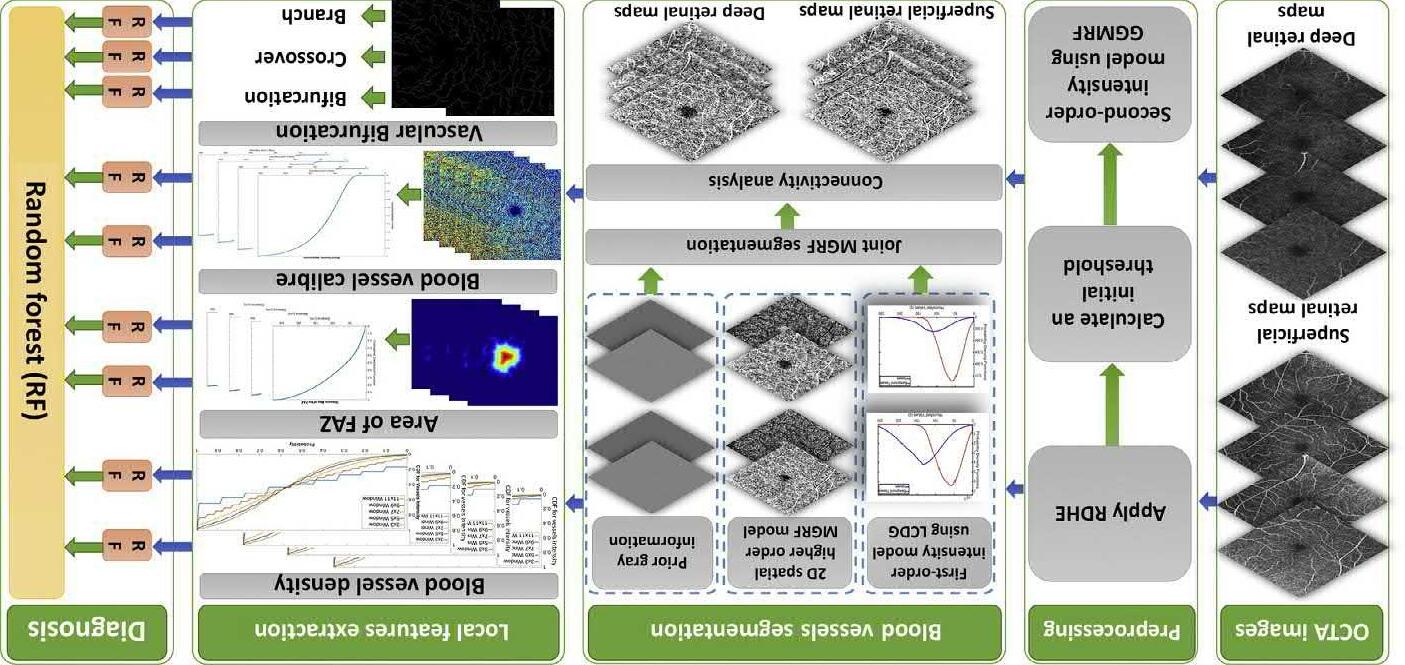
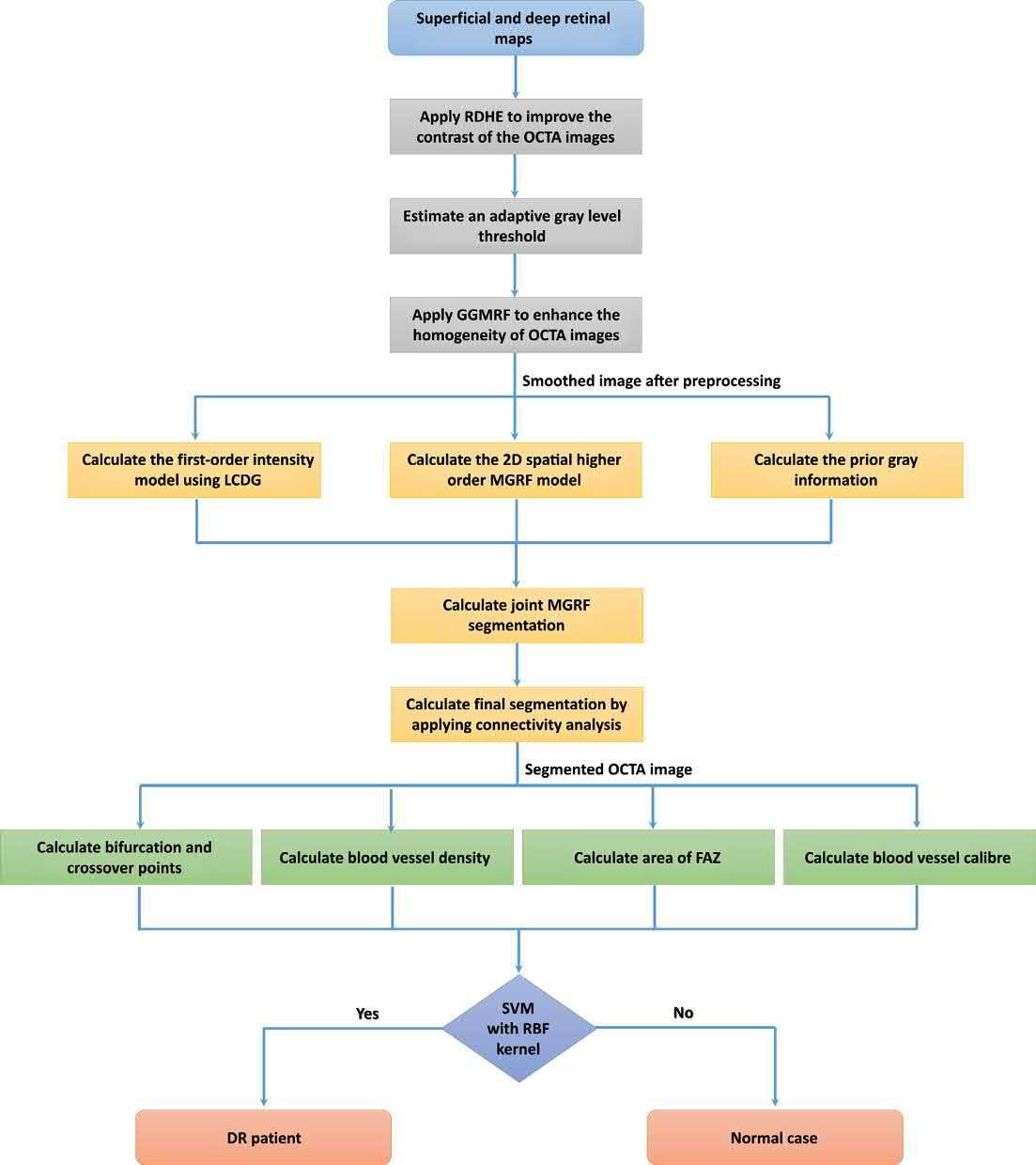
OurCADsystemconsistsoffourm ajorphases,asillustratedin Fig.1 .First,apreprocessingphaseisdevelopedtoimproveth econtrastoftheprocessedOCTAimages inadditiontoreductioninthenoiseeffect.Second,anautomatedsegmentation phaseisimplementedtoextracttheretinal bloodvesselsfromot herbackgroundtissues.Then,thefeatureextractionphaseisdevelopedtoextractfourvariouslocalfeaturesfromthesegmentedsuperficialand deepretinalOCTAplexuses.Theselocal featuresarethewidthoftheFAZarea,theret inalbloodvesseldensity,thebloodvesselcaliber,andthevascularbifurcationandcrossoverpoints.Finally,atwo-stage randomforest(RF)classifieristrainedbyusingtheseextractedfeaturestodistinguishthenormalcasesfrompatientswithmildDR. Fig.2 showstheflowchartof theproposedsystem.Inthefollowingse ctions,thephasesoftheproposedsystem aredescribedindetail.
FIG.1 TheproposedOCTAdiagnosissystemforearlysignsofmildDR.
FIG.2 TheflowchartoftheproposedOCTAdiagnosissystemforearlysignsofmildDR.
2.1Contrastenhancementandnoiseelimination
Inthebeginning,weneedtoimprovethecontrastandhomogeneityinadditiontodecrease thenoise,whichcanbefoundintheOCTAplexusesbeforesegmentingtheretinalblood vessels.First,theregionaldynamichistogramequalizationisappliedtogeneratea
uniformlydistributedgraylevelsfortheprocessedimages.Then,acombinationofthegeneralizedGauss-Markovrandomfieldmodelandanadaptivegraylevelthresholdestimation techniqueisutilizedtoimprovethehomogeneityoftheprocessedimages[18].Theresultingsmoothedimageisusedasaninputtotheretinalbloodvesselsegmentationstage.
2.2Vesselsegmentation
Thevesselsegmentationphaseisdevelopedtoretrieveandseparatetheretinalbloodvessels fromotherbackgroundtissuesfordifferentretinalOCTAplexuses,suchassuperficialand deepplexuses.Tosegmentbloodvessels,thesegmentationtechniquecombinesthreedifferentmodels,whicharepriorintensity,currentintensity,andhigher-orderspatialmodels. First,thepriorgrayintensitymodelisgeneratedfromasetoftrainingimages,whichare manuallylabeledbythreedifferentretinaexperts.Second,anenhancedversionofthe ExpectationMaximizationalgorithmisusedtogeneratethecurrentintensitymodel.Finally, thehigher-orderMarkov-Gibbsrandomfield(HO-MGRF)isusedtocalculatethehigherorderspatialmodel.BoththeHO-MGRFandcurrentintensitymodelswereusedtohandle overcomethelowcontrastbetweenthebackgroundtissuesandthebloodvessels.Finally,a NaıveBayes(NB)isappliedbylabelingandanalyzingtheconnectedcomponentstogeneratearefinedfinalresult. Fig.3 showstheoutputofthepreprocessingandsegmentation

FIG.3 TheoutputofthepreprocessingandsegmentationstagesfornormalandmildDRsubjectsbyusingsuperficial anddeepOCTAplexuses.
stagesfornormalandmildDRsubjectsbyusingsuperficialanddeepOCTAplexuses.For moredetailaboutthesegmentationtechnique,thereaderisreferredtoRef.[19].
2.3Localfeatureextractionanddiagnosis
Inthisstage,wehaveextractedfourdistinguishingfeaturesthatareusedinthefinalstep toclassifytheimagesintomildDRornormalcases.Thedetailsofthosefeaturesaregiven inthefollowingsections.
2.3.1Bloodvesseldensityestimation
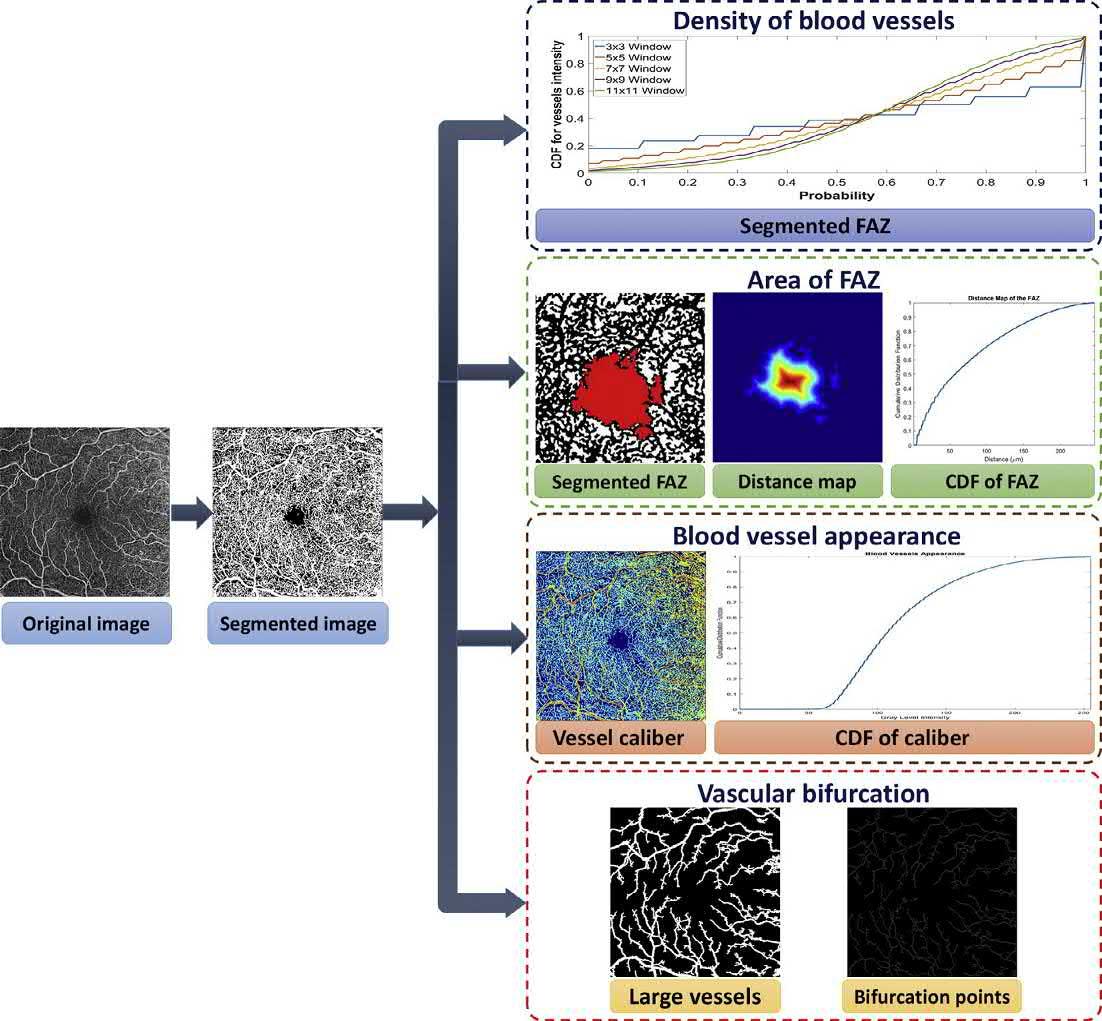
Manyretinaldiseasescanbeobservedbyanalyzingthevasculatureoftheretina.Todetect thealterationsinthebloodvesselsoftheretina,adetailedanalysisofthevasculatureis required[20].Accordingtotheliteratureandintheopinionofourretinaexperts,theblood vesseldensitywillbechangedincaseofDRpatients.Therefore,itcanbeusedasafeature todifferentiatethenormalfromDRcases.TocapturethevesseldensitychangesinOCTA images,thelocalbloodvesseldensityiscalculatedforbothretinalOCTAplexuses. AParzenwindowtechniquewasimplementedtocomputethelocaldensityoftheblood vessels.Usingagivenwindowsize,theParzenwindowtechniquecalculatesthevascular density(PPWPW(Br))atspecificlocation r.Thislocationdependsontheneighboringpixels totheprocessedpixelinthesegmentedOCTAimages(Br).Wehavetestedfivedifferent squaredParzenwindowsizes(3 3,5 5,7 7,9 9,and11 11)toestimatethedensity toensurethatoursystemisnotsensitivetothechoiceofthewindowsize.Finally,weused thecumulativedistributionfunction(CDF)torepresentthedensityofthebloodvessels foreachtestedwindowsize.ThegeneratedCDFswereusedasfeaturestohelpindisseminatingthenormalfromDRcases.TheminimumincrementalvaluefortheCDFischosen tobe0.01.Therefore,eachCDFforspecificwindowsizewillberepresentedas100elementsvector.Thesevectorsaresuppliedtotheclassifiertoassistindiagnosingtheprocessedimages. Algorithm1 liststhestepsforcalculatingthedensityofbloodvesselsby usingParzenwindowtechniquewithdifferentwindowsizes. Fig.4 showsanexample ofthefourextractedfeatures.
nnn
Algorithm1Theproposedbloodvesselsdensityestimationalgorithm.
Data: Thesegmentedsuperficialanddeepplexuses,Parzenwindowsizes,andincrementvalue ofCDF(0.01)
(1) ReadtheParzenwindowsize.
(2) Calculate PPW(Br) foreachpixelinthesegmentedimage.
(3) Countthenumberofoccurrencesofeachprobabilityvalueintheimage.
(4) ReadtheincrementvalueoftheCDF.
(5) CalculatetheCDF(PCDF:PW(N))forthecurrentwindowsize.
Result: TheCDFsofthesuperficialanddeepplexusesatdifferentwindowsizes
FIG.4 ThefourextractedlocalfeaturesofasuperficialretinalplexusformildDRcase.
2.3.2Retinalbloodvesselcaliber
Ithastheabilitytodistinguishthesmallandlargeretinalvesselsbyanalyzingtheintensity levelsandappearanceofsegmentedbloodvesselsfrombothOCTAplexuses.First,the segmentedOCTAplexusismultipliedbytheoriginalplexustoobtainthevalueofintensitiesforthesegmentedvessels.Then,CDFisgeneratedfortheresultingintensityvalues thatindicatethevariationsofretinalbloodvesselcaliber.Theincrementalvalueforthe generatedCDFwaschosentobe0.02.So,eachoneoftheseCDFswillberepresented asa128-elementvector. Fig.4 showsthesegmentedbloodvesselcaliberanditsCDFcurve fromasuperficialplexusforaDRcase,respectively.Thebluecolorindicatesthelowest
appearancelevelforthebloodvessel(i.e.,thesmallvessels),whereastheredcolorindicatesthehighestappearancelevel(i.e.,thelargevessels).
2.3.3WidthoftheFAZ
OneoftheimportantsignsofthechangeinthevisualacutenessistheFAZarea.An enlargementoftheFAZareaisusuallyfoundasaresultofthelossofcapillariesinDRcases [21].TheregiongrowingalgorithmisimplementedtosegmenttheFAZareafromthesegmentedOCTAplexuses.Thecentralpointofthesegmentedplexusischosenasaseed point(rseed),asallourimagesarecenteredatthemacula.Morphologicalfiltersareapplied aftertheregiongrowingalgorithmtofillsmallholesandtoremovediscontinuousregions intheFAZarea.Amedianfilterisappliedtosmooththesegmentedarea.Torepresentthe extractedFAZareaasalocalfeature,thedistancemapiscalculated.Thedistancemapis formedusingtheEuclideandistancebetweeneachpixelintheextractedFAZanditsclosestboundarypixel.TheresultingdistancesrepresentedasaCDFcurveiscalculatedwith anincrementalvalueof0.03.EachCDFcurveisintroducedasa150-elementvector,which indicatesthemaximumvalueofthedistancemapoftheFAZarea. Fig.4 showsthe extractedFAZareawithitsdistancemapandtheCDFcurvefromasuperficialplexus forDRcase.
2.3.4Bifurcationpoints
Inretinalimages,vascularbifurcation,branch,andcrossoverpointscanbeconsidered speciallandmarksforpredictingmanyretinaldiseases.Thechangesthatoccurinbifurcationandcrossoverpointsmaybeanindicationofanillness[22].Thebifurcationpoints canberecognizedeasilybecauseoftheirT-shapewiththreesurroundingbranches[23]. Onbifurcation,avesselisdividedintotwovessels.Thebranchisasmallervesselthat comesoutorgrowfromawidervessel.Acrossoverappearswheretwovessels(artery andvein)crosseachother.Ourmainconcernhereistodetectbifurcationpoints.Todetect bifurcationpoints,wefirstextractthelargevesselsbymultiplyingtheoriginalimageby thesegmentedimagethenapplyingathreshold,asshownin Fig.4.Then,athinningtechniqueisusedtoerasepixelsofthebordersandreturntheskeletonofthevesselswithout affectingtheconnectivityorthedirectionofthebloodvessels.Bifurcationpointsarecalculatedbyanalyzingtheneighborhoodpixelsforeachpointinthegeneratedskeletonby usingthefollowingequation:
where N(X) isthenumberoftheintersectionsthatiscomputedforeachpoint(X)ofthe skeletonand Mi(X)arethenumberofneighborhoodpixelsof X thatisconsecutively namedclockwise.Eachpointwillbemarkedasoneoffourtypesaccordingtoitsnumber ofintersections.Itisavesselendpointif N(X) ¼ 1.Itisaninternalvesselpointif N(X) ¼ 2.It isavesselbifurcationpointif N(X) ¼ 3.Finally,itisavesselcrossoverpointif N(X) ¼ 4.
Inaddition,askeletonfilteringstepisperformedtodeleteunrealpoints.So,wehave deletedtheonesthatareshorterthananestablishedthreshold,whichisthemaximum vesselwidthexpectedintheimage.Tousethesedetectedbifurcationpointsasafeature inoursystem,wehavedividedtheimageinto8 8,16 16, …,1024 1024windows. Then,wecalculatedthenumberofbifurcation,crossover,andbranchpointsineachwindowsize.Window128 128gaveusthebestresultandwehaveusedthatinoursystem. Algorithm2 liststhestepsforgeneratingfeaturevectorsforbifurcation,crossover,and branchpoints.
nnn
Algorithm2Theproposedalgorithmforextractingthevascularbifurcationpoints.
Data: Theoriginalandsegmentedsuperficialimages.
(1) Multiplytheoriginalsuperficialimagebythesegmentedimage.
(2) Applyathresholdtoextractthelargebloodvessels.
(3) Applythethinningtechniquetogeneratethevessels’skeleton.
(4) Calculatethenumberofvesselendpoints,internalvesselpoints,vesselbifurcationpoints, andvesselcrossoverpoints.
(5) Applyskeletonfilteringtechniquetodeleteunrealpoints.
(6) Generatethefeaturevectors:
• Dividetheimageinto8 8,16 16, ,1024 1024windows.
• Calculatethenumberofbifurcation,crossover,andbranchpointsineach windowsize.
• Findthebestwindowsize.
• Generatethefeaturevectorsforbifurcation,crossover,andbranchpoints.
Result: Thefeaturevectorsforbifurcation,crossover,andbranchpoints.
2.4MildDRdiagnosis
ItisthefinalphaseinourproposedsystemwheretheclassificationoftheimagesasnormalormildDRtakesplace.Theclassifierusesthefourfeaturesthathavebeenextractedin thepreviousphasetohelpinclassificationprocess.Thefirstthreefeatures,thevesseldensity,thevesselscaliber,andthedistancemapoftheFAZarea,aresuppliedtotheclassifier asCDFcurvesforbothsuperficialanddeepplexuses.Thefourthfeature,whichisthe avascularbifurcation,isrepresentedasthreevectorsthatrepresentthenumberofbifurcation,branch,andcrossoverpointsinspecificwindowsize(128 128)forthesuperficial retinalplexus.TheproposedCADsystememploystheRFclassifier,whichachievedthe bestresultsascomparedwithotherstate-of-the-artclassifiers,toclassifytheimages. Thediagnosisphaseisatwo-stageclassificationprocess,asshownin Fig.1.Thefirststage processeseachextractedfeatureindependently.Thesecondstagefusestheresultofthe firststagetogetafinaldiagnosisdecision.
3Experimentalresults
Adatasetof133caseswasusedtoevaluateourdiagnosissystem(34fornormaland99for mildDRcases).AZEISSAngioPlexOCTAngiographymachine[24]wasusedtocapturethe images.Thismachineprovidesanoninvasivevascularimagingplatformforbloodflowin theretina.Asmentionedearlier,ourpresentedsystemwastestedonbothdeepandsuperficialretinalplexuses.Weusedtheimagesizeof1024 1024.TheOCTAimageswere6 6mm2 sectionscenteredonthefovea.Fivedifferentmetricswereusedtoevaluateour diagnosissystem.Weusedaccuracy(ACC),sensitivity(Sens.),specificity(Spec.),thearea underthecurve(AUC),anddicesimilaritycoefficient(DSC).Twocross-validationtechniqueswereused:twofoldandfourfoldcross-validations.Inaddition,theperformanceof theproposedsystemwasevaluatedagainstfivestate-of-the-artclassifiers,suchasthe supportvectormachine(SVM)withlinearkernel,SVMwithradialbasisfunction (RBF),SVMwithpolynomialkernel,classificationtree,andK-nearestneighbor(KNN). Table1 liststheresultsoftheclassificationbasedonthefourextractedfeaturesforthe testedclassifiers.ItshowsthattheRFclassifieroutperformstheotherstate-of-the-art techniquesandprovidespromisingresults.
Wehaveconductedsixexperimentstounderstandtheeffectoffourextractedfeatures andtheirdifferentintegrationonthediagnosisresult.First,wehaveevaluatedthesystem byusingthedensityfeaturewithagivenwindowsizeforsuperficialplexusonlyandthen fordeepplexus.Second,wecombineddensityfeatureforbothtestedplexuseswithgiven windowsize.Thewindowsizeof11 11providedthebestresultsinthefirsttwoexperiments.Therefore,wefixedthewindowsize11 11inotherexperimentsforthevessel density.Inaddition,thecombinationofthedensityfeaturesinbothplexusesachieved thebestresultsamongtheothers.Third,thedensityfeatureisgatheredwiththevessel caliberforbothplexuses.Fourth,thedensityfeatureiscombinedwiththedistance
Table1 Theresultsoftheclassificationbasedonthedensityofthebloodvessels (11 11window),theretinalbloodvesselcaliber,thedistancemapoftheFAZ, andbifurcationpointsfromboththesuperficialanddeepretinalmaps.
ClassifiersValidationACC(%)Sens.(%)Spec.(%)AUC(%)DSC(%)
SVM(linear)Fourfold88.695.773.984.891.8 Twofold68.685.134.859.978.4 SVM(polynomial)Fourfold91.495.782.689.293.8 Twofold708343.563.278.8 SVM(RBF)Fourfold88.695.773.984.891.8 Twofold85.791.573.982.789.6 KNNFourfold9095.778.38792.8 Twofold9093.682.688.192.6 ClassificationtreeFourfold84.391.569.680.588.7 Twofold84.393.665.279.488.9 RFFourfold 94.397.98792.495.8 Twofold 97.197.995.796.897.9
Boldtextpresentsthebestresults.
Table2 Theresultsofsomefeaturecombinationsonbothsuperficialandretinal plexusesusingRFclassifierwithtwofoldcross-validation.
FeaturesACC(%)Sens.(%)Spec.(%)AUC(%)DSC(%)
Vesselsdensity+vesselscaliber9095.778.38792.8 Vesselsdensity+FAZ81.485.173.979.586 Bifurcationpoints+vesselsdensity84.391.569.980.588.7 Bifurcationpoints+vesselscaliber71.485.143.564.380 Bifurcationpoints+FAZ72.997.721.759.882.9 Vesselsdensity+vesselscaliber+bifurcationpoints9091.58789.292.5 Vesselsdensity+vesselscaliber+FAZ+bifurcation points 97.197.995.796.897.9
Boldtextpresentsthebestresults.
mapoftheFAZareaforbothplexuses.Fifth,thefirstthreeextractedfeaturesareusedto evaluatetheproposeddiagnosissystem.Finally,thefourfeaturesareusedtoevaluatethe system.Wefoundthatthelastscenariogetsthebestresultsascomparedwithotherscenarios. Table2 liststheresultsoftheclassificationbasedonthefourextractedfeaturesfor RFclassifierbasedontwofoldcross-validation.
4Conclusions
AnOCTA-baseddiagnosissystemforthedetectionoftheearlysignsofDRhasbeendiscussed.First,weextractedthebloodvesselsfrombothdeepandsuperficialOCTAimages. Then,fourlocalfeaturesthatrepresenttheshapeandappearancewereextracted.Oursystemwasabletoextractthebloodvesselcaliber,bloodvesseldensity,distancemapofthe FAZ,andthebifurcationpoints.TotrainanRFclassifier,thesefeatureswereused.Using 133subjects,thesystemobtainedanaccuracyof97%.Thisresultdemonstratesthatour systemhastheabilitydetecttheearlysignsofDR.Wewilltrytoextractmorefeaturesin thefuturetohelpinenhancingthediagnosticcapabilityofoursystem.Wewillalsotryto applythesystemtodetectotherdiseasesinearlystagesandmeasureitsaccuracy.
Thisstudycouldalsobeusedforvariousotherapplicationsinmedicalimaging,such asthekidney,theheart,theprostate,thelung,andthebraininadditiontotheretina,as wellasseveralnonmedicalapplications[25–28].
Onesuchapplicationisrenaltransplantfunctionalassessment,especiallywiththe developmentofdevelopingnoninvasiveCADsystemsforrenaltransplantfunction assessment,utilizingdifferentimagemodalities(e.g.,ultrasound,computedtomography [CT],MRI,etc.).Accurateassessmentofrenaltransplantfunctioniscriticallyimportant forgraftsurvival.Althoughtransplantationcanimproveapatientwell-being,thereisa potentialposttransplantationriskofkidneydysfunctionthat,ifnottreatedinatimely manner,canleadtothelossoftheentiregraft,andevenpatientdeath.Inparticular, dynamicanddiffusionMRI-basedsystemshavebeenclinicallyusedtoassesstransplantedkidneyswiththeadvantageofprovidinginformationoneachkidneyseparately.
Formoredetailsaboutrenaltransplantfunctionalassessment,thereadersarereferredto Refs.[29–56].
Thisstudyalsofindsanimportantapplicationincardiacimaging.Theclinicalassessmentofmyocardialperfusionplaysamajorroleinthediagnosis,management,andprognosisofischemicheartdisease.Thus,therehavebeenongoingeffortstodevelopautomated systemstoaccuratelyanalyzemyocardialperfusionusingfirst-passimages[57–73].
Abnormalitiesofthelungcouldalsobeanotherpromisingareaofresearchanda relatedapplicationofthisstudy.Radiation-inducedlunginjuryisthemainsideeffect ofradiationtherapyinlungcancerpatients.Althoughhigherradiationdosesincrease theradiationtherapyeffectivenessfortumorcontrol,itcanleadtolunginjuryasagreater quantityofnormallungtissuesisincludedinthetreatedarea.Almostone-thirdof patientswhoundergoradiationtherapydeveloplunginjuryfollowingradiationtreatment.Theseverityofradiation-inducedlunginjuryrangesfromground-glassopacities andconsolidationattheearlyphasetofibrosisandtractionbronchiectasisinthelate phase.Earlydetectionoflunginjurywillthushelptoimprovemanagementofthetreatment[74–116].
Thisstudycanalsobeappliedtootherbrainabnormalities,suchasdyslexiainaddition toautism.Dyslexiaisoneofthemostcomplicateddevelopmentalbraindisordersthat affectchildren’slearningabilities.Dyslexialeadstothefailuretodevelopage-appropriate readingskillsinspiteofthenormalintelligencelevelandadequatereadinginstructions. Neuropathologicalstudieshaverevealedanabnormalanatomyofsomestructures,such asthecorpuscallosumindyslexicbrains.Therehasbeenalotofstudiesintheliterature thataimsatdevelopingCADsystemsfordiagnosingsuchdisorder,alongwithotherbrain disorders[117–139].
Forthevascularsystem[140],thisstudycouldalsobeappliedfortheextractionof bloodvessels,forexample,fromphasecontrastmagneticresonanceangiography (MRA).AccuratecerebrovascularsegmentationusingnoninvasiveMRAiscrucialfor theearlydiagnosisandtimelytreatmentofintracranialvasculardiseases[122, 123, 141–146].
References
[1] M.Purandare,K.Noronha,Hybridsystemforautomaticclassificationofdiabeticretinopathyusing fundusimages,in:Proceedingsof2016OnlineInternationalConferenceonGreenEngineeringand Technologies(IC-GET),2016,pp.1–5.
[2] M.Iqbal,A.Aibinu,M.Nilsson,I.Tijani,M.E.Salami,Detectionofvascularintersectioninretina fundusimageusingmodifiedcrosspointnumberandneuralnetworktechnique,in:Proceedings ofthe2008InternationalConferenceonComputerandCommunicationEngineering,2008, pp.241–246.
[3] J.Nayak,P.S.Bhat,R.AcharyaU,C.M.Lim,M.Kagathi,Automatedidentificationofdiabeticretinopathystagesusingdigitalfundusimages,J.Med.Syst.32(2)(2008)107–115.
[4] L.An,T.T.Shen,R.K.Wang,Usingultrahighsensitiveopticalmicroangiographytoachievecomprehensivedepthresolvedmicrovasculaturemappingforhumanretina,J.Biomed.Opt.16(10)(2011) 106013.
[5] T.Somkijrungroj,S.Vongkulsiri,W.Kongwattananon,P.Chotcomwongse,S.Luangpitakchumpol, K.Jaisuekul,Assessmentofvascularchangeusingswept-sourceopticalcoherencetomography angiography:anewtheoryexplainscentralvisuallossinBehcet’sdisease,J.Ophthalmol. 2017(2017)2180723.
[6] S.A.Agemy,N.K.Scripsema,C.M.Shah,T.Chui,P.M.Garcia,J.G.Lee,R.C.Gentile,Y.-S.Hsiao, Q.Zhou,T.Ko,etal.,Retinalvascularperfusiondensitymappingusingopticalcoherencetomographyangiographyinnormalsanddiabeticretinopathypatients,Retina35(11)(2015)2353–2363.
[7] T.S.Hwang,Y.Jia,S.S.Gao,S.T.Bailey,A.K.Lauer,C.J.Flaxel,D.J.Wilson,D.Huang,Opticalcoherencetomographyangiographyfeaturesofdiabeticretinopathy,Retina(Philadelphia,PA)35(11) (2015)2371.
[8] T.S.Hwang,S.S.Gao,L.Liu,A.K.Lauer,S.T.Bailey,C.J.Flaxel,D.J.Wilson,D.Huang,Y.Jia,Automatedquantificationofcapillarynonperfusionusingopticalcoherencetomographyangiography indiabeticretinopathy,JAMAOphthalmol.134(4)(2016)367–373.
[9] P.E.Stanga,A.Papayannis,E.Tsamis,F.Stringa,T.Cole,Y.D’Souza,A.Jalil,Newfindingsindiabetic maculopathyandproliferativediseasebyswept-sourceopticalcoherencetomographyangiography, in:OCTAngiographyinRetinalandMacularDiseases,vol.56,KargerPublishers,2016,pp.113–121.
[10] N.Takase,M.Nozaki,A.Kato,H.Ozeki,M.Yoshida,Y.Ogura,Enlargementoffovealavascularzone indiabeticeyesevaluatedbyenfaceopticalcoherencetomographyangiography,Retina35(11) (2015)2377–2383.
[11] D.Bhanushali,N.Anegondi,S.G.K.Gadde,P.Srinivasan,L.Chidambara,N.K.Yadav,A.S.Roy,Linkingretinalmicrovasculaturefeatureswithseverityofdiabeticretinopathyusingopticalcoherence tomographyangiography,Invest.Ophthalmol.Vis.Sci.57(9)(2016)OCT519–OCT525.
[12]B.D.Krawitz,S.Mo,L.S.Geyman,S.A.Agemy,N.K.Scripsema,P.M.Garcia,T.Y.P.Chui,R.B.Rosen, Acircularityindexandaxisratioofthefovealavascularzoneindiabeticeyesandhealthycontrols measuredbyopticalcoherencetomographyangiography,VisionRes.139(2017)177–186, https:// doi.org/10.1016/j.visres.2016.09.019.
[13]K.Tarassoly,A.Miraftabi,M.SoltanSanjari,M.M.Parvaresh,Therelationshipbetweenfovealavascularzonearea,vesseldensity,andcystoidchangesindiabeticretinopathy:anopticalcoherence tomographyangiographystudy,Retina38(8)(2018)(online),Availablefrom: https://journals. lww.com/retinajournal
[14]A.Ishibazawa,T.Nagaoka,A.Takahashi,T.Omae,T.Tani,K.Sogawa,H.Yokota,A.Yoshida,Optical coherencetomographyangiographyindiabeticretinopathy:aprospectivepilotstudy,Am.J. Ophthalmol.160(1)(2015)35–44.e1, https://doi.org/10.1016/j.ajo.2015.04.021
[15]M.Soares,C.Neves,I.P.Marques,I.Pires,C.Schwartz,M.A ˆ .Costa,T.Santos,M.Durbin,J.CunhaVaz,Comparisonofdiabeticretinopathyclassificationusingfluoresceinangiographyandoptical coherencetomographyangiography,Br.J.Ophthalmol.101(2017)62–68, https://doi.org/ 10.1136/bjophthalmol-2016-309424.
[16]F.J.Freiberg,M.Pfau,J.Wons,M.A.Wirth,M.D.Becker,S.Michels,Opticalcoherencetomography angiographyofthefovealavascularzoneindiabeticretinopathy,GraefesArch.Clin.Exp.Ophthalmol.254(6)(2016)1051–1058, https://doi.org/10.1007/s00417-015-3148-2 .
[17]Q.You,W.R.Freeman,R.N.Weinreb,L.Zangwill,P.I.C.Manalastas,L.J.Saunders,E.Nudleman, Reproducibilityofvesseldensitymeasurementwithopticalcoherencetomographyangiography ineyeswithandwithoutretinopathy,Retina37(8)(2017)(online),Availablefrom: https:// journals.lww.com/retinajournal.
[18]G.Gimel ´ farb,A.A.Farag,A.El-Baz,Expectation-maximizationforalinearcombinationofGaussians,in:Proceedingsofthe17thInternationalConferenceonPatternRecognition,2004.ICPR 2004,vol.3,2004,pp.422–425,ISSN1051–4651, https://doi.org/10.1109/ICPR.2004.1334556 .
[19] N.Eladawi,M.Elmogy,O.Helmy,A.Aboelfetouh,A.Riad,H.Sandhu,S.Schaal,A.El-Baz,Automatic bloodvesselssegmentationbasedondifferentretinalmapsfromOCTAscans,Comput.Biol.Med. 89(2017)150–161.
[20] S.G.K.Gadde,N.Anegondi,D.Bhanushali,L.Chidambara,N.K.Yadav,A.Khurana,A.SinhaRoy, Quantificationofvesseldensityinretinalopticalcoherencetomographyangiographyimagesusing localfractaldimensionvesseldensityinOCTAimages,Invest.Ophthalmol.Vis.Sci.57(1)(2016)246.
[21]M.H.AhmadFadzil,L.I.Iznita,H.A.Nugroho,Analysisoffovealavascularzoneforgradingofdiabeticretinopathy,Int.J.Biomed.Eng.Technol.6(3)(2011)232–250, https://doi.org/10.1504/ IJBET.2011.041463
[22]A.Bhuiyan,B.Nath,K.Ramamohanarao,Detectionandclassificationofbifurcationandbranch pointsonretinalvascularnetwork,in:2012InternationalConferenceonDigitalImageComputing TechniquesandApplications(DICTA),December,2012,pp.1–8, https://doi.org/10.1109/ DICTA.2012.6411742
[23]L.Chen,Y.Xiang,Y.Chen,X.Zhang,Retinalimageregistrationusingbifurcationstructures,in:2011 18thIEEEInternationalConferenceonImageProcessing,September,ISSN1522-4880,2011, pp.2169–2172, https://doi.org/10.1109/ICIP.2011.6116041
[24]ZEISS,AngioPlexOCTAngiography2017,Availablefrom: http://www.zeiss.com/meditec/us/c/octangiography.html.
[25]A.H.Mahmoud,UtilizingRadiationforSmartRoboticApplicationsUsingVisible,Thermal,and PolarizationImages(Ph.D.thesis),UniversityofLouisville,2014.
[26] A.Mahmoud,A.El-Barkouky,J.Graham,A.Farag,Pedestriandetectionusingmixedpartialderivativebasedhistogramoforientedgradients,in:2014IEEEInternationalConferenceonImageProcessing(ICIP),IEEE,2014,pp.2334–2337.
[27] A.El-Barkouky,A.Mahmoud,J.Graham,A.Farag,Aninteractiveeducationaldrawingsystemusinga humanoidrobotandlightpolarization,in:2013IEEEInternationalConferenceonImage Processing,IEEE,2013,pp.3407–3411.
[28] A.H.Mahmoud,M.T.El-Melegy,A.A.Farag,Directmethodforshaperecoveryfrompolarizationand shading,in:201219thIEEEInternationalConferenceonImageProcessing,IEEE,2012, pp.1769–1772.
[29] A.M.Ali,A.A.Farag,A.El-Baz,Graphcutsframeworkforkidneysegmentationwithpriorshapeconstraints,in:ProceedingsofInternationalConferenceonMedicalImageComputingandComputerAssistedIntervention(MICCAI’07),Brisbane,Australia,October29–November2,vol.1,2007, pp.384–392.
[30] A.S.Chowdhury,R.Roy,S.Bose,F.K.A.Elnakib,A.El-Baz,Non-rigidbiomedicalimageregistration usinggraphcutswithanoveldataterm,in:ProceedingsofIEEEInternationalSymposiumonBiomedicalImaging:FromNanotoMacro(ISBI’12),Barcelona,Spain,May2–5,2012,pp.446–449.
[31] A.El-Baz,A.A.Farag,S.E.Yuksel,M.E.A.El-Ghar,T.A.Eldiasty,M.A.Ghoneim,Applicationofdeformablemodelsforthedetectionofacuterenalrejection,in:DeformableModels,Springer,NewYork, NY,2007,pp.293–333.
[32] A.El-Baz,A.Farag,R.Fahmi,S.Yuksel,M.A.El-Ghar,T.Eldiasty,ImageanalysisofrenalDCEMRIfor thedetectionofacuterenalrejection,in:ProceedingsofIAPRInternationalConferenceonPattern Recognition(ICPR’06),HongKong,August20–24,2006,pp.822–825.
[33] A.El-Baz,A.Farag,R.Fahmi,S.Yuksel,W.Miller,M.A.El-Ghar,T.El-Diasty,M.Ghoneim,AnewCAD systemfortheevaluationofkidneydiseasesusingDCE-MRI,in:ProceedingsofInternationalConferenceonMedicalImageComputingandComputer-AssistedIntervention(MICCAI’08),Copenhagen,Denmark,October1–6,2006,pp.446–453.
[34] A.El-Baz,G.Gimel’farb,M.A.El-Ghar,Anovelimageanalysisapproachforaccurateidentificationof acuterenalrejection,in:ProceedingsofIEEEInternationalConferenceonImageProcessing (ICIP’08),SanDiego,California,USA,October12–15,2008,pp.1812–1815.
[35] A.El-Baz,G.Gimel’farb,M.A.El-Ghar,Imageanalysisapproachforidentificationofrenaltransplant rejection,in:ProceedingsofIAPRInternationalConferenceonPatternRecognition(ICPR’08), Tampa,Florida,USA,December8–11,2008,pp.1–4.
[36] A.El-Baz,G.Gimel’farb,M.A.El-Ghar,Newmotioncorrectionmodelsforautomaticidentificationof renaltransplantrejection,in:ProceedingsofInternationalConferenceonMedicalImageComputingandComputer-AssistedIntervention(MICCAI’07),Brisbane,Australia,October29–November2, 2007,pp.235–243.
[37] A.Farag,A.El-Baz,S.Yuksel,M.A.El-Ghar,T.Eldiasty,Aframeworkforthedetectionofacuterejectionwithdynamiccontrastenhancedmagneticresonanceimaging,in:ProceedingsofIEEEInternationalSymposiumonBiomedicalImaging:FromNanotoMacro(ISBI’06),Arlington,Virginia, USA,April6–9,2006,pp.418–421.
[38] F.Khalifa,G.M.Beache,M.A.El-Ghar,T.El-Diasty,G.Gimel’farb,M.Kong,A.El-Baz,Dynamic contrast-enhancedMRI-basedearlydetectionofacuterenaltransplantrejection,IEEETrans. Med.Imaging32(10)(2013)1910–1927.
[39] F.Khalifa,A.El-Baz,G.Gimel’farb,M.A.El-Ghar,Non-invasiveimage-basedapproachforearly detectionofacuterenalrejection,in:ProceedingsofInternationalConferenceMedicalImageComputingandComputer-AssistedIntervention(MICCAI’10),Beijing,China,September20–24,2010, pp.10–18.
[40] F.Khalifa,A.El-Baz,G.Gimel’farb,R.Ouseph,M.A.El-Ghar,Shape-appearanceguidedlevel-set deformablemodelforimagesegmentation,in:ProceedingsofIAPRInternationalConferenceon PatternRecognition(ICPR’10),Istanbul,Turkey,August23–26,2010,pp.4581–4584.
[41] F.Khalifa,M.A.El-Ghar,B.Abdollahi,H.Frieboes,T.El-Diasty,A.El-Baz,AcomprehensivenoninvasiveframeworkforautomatedevaluationofacuterenaltransplantrejectionusingDCE-MRI, NMRBiomed.26(11)(2013)1460–1470.
[42] F.Khalifa,M.A.El-Ghar,B.Abdollahi,H.B.Frieboes,T.El-Diasty,A.El-Baz,DynamiccontrastenhancedMRI-basedearlydetectionofacuterenaltransplantrejection,in:2014AnnualScientific MeetingandEducationalCourseBrochureoftheSocietyofAbdominalRadiology(SAR’14),Boca Raton,Florida,March23–28,2014.
[43] F.Khalifa,A.Elnakib,G.M.Beache,G.Gimel’farb,M.A.El-Ghar,G.Sokhadze,S.Manning,P.McClure, A.El-Baz,3DkidneysegmentationfromCTimagesusingalevelsetapproachguidedbyanovelstochasticspeedfunction,in:ProceedingsofInternationalConferenceMedicalImageComputingand Computer-AssistedIntervention(MICCAI’11),Toronto,Canada,September18–22,2011, pp.587–594.
[44] F.Khalifa,G.Gimel’farb,M.A.El-Ghar,G.Sokhadze,S.Manning,P.McClure,R.Ouseph,A.El-Baz, Anewdeformablemodel-basedsegmentationapproachforaccurateextractionofthekidneyfrom abdominalCTimages,in:ProceedingsofIEEEInternationalConferenceonImageProcessing (ICIP’11),Brussels,Belgium,September11–14,2011,pp.3393–3396.
[45] M.Mostapha,F.Khalifa,A.Alansary,A.Soliman,J.Suri,A.El-Baz,Computer-aideddiagnosissystemsforacuterenaltransplantrejection:challengesandmethodologies,in:A.El-Baz,L.Saba, J.Suri(Eds.),AbdomenandThoracicImaging,,Springer,NewYork,NY,2014,pp.1–35.
[46] M.Shehata,F.Khalifa,E.Hollis,A.Soliman,E.Hosseini-Asl,M.A.El-Ghar,M.El-Baz,A.C.Dwyer, A.El-Baz,R.Keynton,Anewnon-invasiveapproachforearlyclassificationofrenalrejectiontypes usingdiffusion-weightedMRI,in:2016IEEEInternationalConferenceonImageProcessing(ICIP), IEEE,2016,pp.136–140.
[47] F.Khalifa,A.Soliman,A.Takieldeen,M.Shehata,M.Mostapha,A.Shaffie,R.Ouseph, A.Elmaghraby,A.El-Baz,KidneysegmentationfromCTimagesusinga3DNMF-guidedactive contourmodel,in:2016IEEE13thInternationalSymposiumonBiomedicalImaging(ISBI),IEEE, 2016,pp.432–435.
[48] M.Shehata,F.Khalifa,A.Soliman,A.Takieldeen,M.A.El-Ghar,A.Shaffie,A.C.Dwyer,R.Ouseph, A.El-Baz,R.Keynton,3DdiffusionMRI-basedCADsystemforearlydiagnosisofacuterenalrejection,in:2016IEEE13thInternationalSymposiumonBiomedicalImaging(ISBI),IEEE,2016, pp.1177–1180.
[49] M.Shehata,F.Khalifa,A.Soliman,R.Alrefai,M.A.El-Ghar,A.C.Dwyer,R.Ouseph,A.El-Baz,Alevel set-basedframeworkfor3DkidneysegmentationfromdiffusionMRimages,in:2015IEEEInternationalConferenceonImageProcessing(ICIP),IEEE,2015,pp.4441–4445.
[50] M.Shehata,F.Khalifa,A.Soliman,M.A.El-Ghar,A.C.Dwyer,G.Gimel’farb,R.Keynton,A.El-Baz, Apromisingnon-invasiveCADsystemforkidneyfunctionassessment,in:InternationalConference onMedicalImageComputingandComputer-AssistedIntervention,Springer,2016,pp.613–621.
[51] F.Khalifa,A.Soliman,A.Elmaghraby,G.Gimel’farb,A.El-Baz,3Dkidneysegmentationfrom abdominalimagesusingspatial-appearancemodels,Comput.Math.MethodsMed.2017(2017) 1–10.
[52] E.Hollis,M.Shehata,F.Khalifa,M.A.El-Ghar,T.El-Diasty,A.El-Baz,Towardsnon-invasivediagnostictechniquesforearlydetectionofacuterenaltransplantrejection:areview,Egypt.J.Radiol.Nucl. Med.48(1)(2016)257–269.
[53] M.Shehata,F.Khalifa,A.Soliman,M.A.El-Ghar,A.C.Dwyer,A.El-Baz,Assessmentofrenaltransplantusingimageandclinical-basedbiomarkers,in:Proceedingsof13thAnnualScientificMeeting ofAmericanSocietyforDiagnosticsandInterventionalNephrology(ASDIN’17),NewOrleans, Louisiana,USA,February10–12,2017.
[54] M.Shehata,F.Khalifa,A.Soliman,M.A.El-Ghar,A.C.Dwyer,A.El-Baz,Earlyassessmentofacute renalrejection,in:Proceedingsof12thAnnualScientificMeetingofAmericanSocietyforDiagnosticsandInterventionalNephrology(ASDIN’16),Pheonix,Arizona,USA,February19–21,2016,2017.
[55] A.Eltanboly,M.Ghazal,H.Hajjdiab,A.Shalaby,A.Switala,A.Mahmoud,P.Sahoo,M.El-Azab, A.El-Baz,Levelsets-basedimagesegmentationapproachusingstatisticalshapepriors,Appl.Math. Comput.340(2019)164–179.
[56] M.Shehata,A.Mahmoud,A.Soliman,F.Khalifa,M.Ghazal,M.A.El-Ghar,M.El-Melegy,A.El-Baz, 3DkidneysegmentationfromabdominaldiffusionMRIusinganappearance-guideddeformable boundary,PLoSONE13(7)(2018)e0200082.
[57] F.Khalifa,G.Beache,A.El-Baz,G.Gimel’farb,Deformablemodelguidedbystochasticspeedwith applicationincineimagessegmentation,in:ProceedingsofIEEEInternationalConferenceon ImageProcessing(ICIP’10),HongKong,September26–29,2010,pp.1725–1728.
[58] F.Khalifa,G.M.Beache,A.Elnakib,H.Sliman,G.Gimel’farb,K.C.Welch,A.El-Baz,Anewshapebasedframeworkfortheleftventriclewallsegmentationfromcardiacfirst-passperfusionMRI, in:ProceedingsofIEEEInternationalSymposiumonBiomedicalImaging:FromNanotoMacro (ISBI’13),SanFrancisco,California,April7–11,2013,pp.41–44.
[59] F.Khalifa,G.M.Beache,A.Elnakib,H.Sliman,G.Gimel’farb,K.C.Welch,A.El-Baz,Anewnonrigid registrationframeworkforimprovedvisualizationoftransmuralperfusiongradientsoncardiac first-passperfusionMRI,in:ProceedingsofIEEEInternationalSymposiumonBiomedicalImaging: FromNanotoMacro(ISBI’12),Barcelona,Spain,May2–5,2012,pp.828–831.
[60] F.Khalifa,G.M.Beache,A.Firjani,K.C.Welch,G.Gimel’farb,A.El-Baz,Anewnonrigidregistration approachformotioncorrectionofcardiacfirst-passperfusionMRI,in:ProceedingsofIEEE InternationalConferenceonImageProcessing(ICIP’12),LakeBuenaVista,Florida,September 30–October3,2012,pp.1665–1668.
[61] F.Khalifa,G.M.Beache,G.Gimel’farb,A.El-Baz,AnovelCADsystemforanalyzingcardiacfirst-pass MRimages,in:ProceedingsofIAPRInternationalConferenceonPatternRecognition(ICPR’12), TsukubaScienceCity,Japan,November11–15,2012,pp.77–80.
[62] F.Khalifa,G.M.Beache,G.Gimel’farb,A.El-Baz,Anovelapproachforaccurateestimationofleft ventricleglobalindexesfromshort-axiscineMRI,in:ProceedingsofIEEEInternationalConference onImageProcessing(ICIP’11),Brussels,Belgium,September11–14,2011,pp.2645–2649.
[63] F.Khalifa,G.M.Beache,G.Gimel’farb,G.A.Giridharan,A.El-Baz,Anewimage-basedframeworkfor analyzingcineimages,in:A.El-Baz,U.R.Acharya,M.Mirmedhdi,J.S.Suri(Eds.),HandbookofMulti
ModalityState-of-the-ArtMedicalImageSegmentationandRegistrationMethodologies,vol.2, Springer,NewYork,NY,2011,pp.69–98,ISBN978-1-4419-8203-2(Chapter3).
[64] F.Khalifa,G.M.Beache,G.Gimel’farb,G.A.Giridharan,A.El-Baz,Accurateautomaticanalysisof cardiaccineimages,IEEETrans.Biomed.Eng.59(2)(2012)445–455.
[65] F.Khalifa,G.M.Beache,M.Nitzken,G.Gimel’farb,G.A.Giridharan,A.El-Baz,Automaticanalysisof leftventriclewallthicknessusingshort-axiscineCMRimages,in:ProceedingsofIEEEInternational SymposiumonBiomedicalImaging:FromNanotoMacro(ISBI’11),Chicago,Illinois,March30–April2,2011,pp.1306–1309.
[66] M.Nitzken,G.Beache,A.Elnakib,F.Khalifa,G.Gimel’farb,A.El-Baz,Accuratemodelingoftagged CMR3Dimageappearancecharacteristicstoimprovecardiaccyclestrainestimation,in:201219th IEEEInternationalConferenceonImageProcessing(ICIP),Orlando,Florida,USA,September,IEEE, 2012,pp.521–524.
[67] M.Nitzken,G.Beache,A.Elnakib,F.Khalifa,G.Gimel’farb,A.El-Baz,Improvingfull-cardiaccycle strainestimationfromtaggedCMRbyaccuratemodelingof3Dimageappearancecharacteristics, in:20129thIEEEInternationalSymposiumonBiomedicalImaging(ISBI),Barcelona,Spain,May, IEEE,2012,pp.462–465(selectedfororalpresentation).
[68] M.J.Nitzken,A.S.El-Baz,G.M.Beache,Markov-Gibbsrandomfieldmodelforimprovedfull-cardiac cyclestrainestimationfromtaggedCMR,J.Cardiovasc.Magn.Reson.14(1)(2012)1–2.
[69] H.Sliman,A.Elnakib,G.M.Beache,A.Elmaghraby,A.El-Baz,Assessmentofmyocardial functionfromcinecardiacMRIusinganovel4Dtrackingapproach,J.Comput.Sci.Syst.Biol. 7(2014)169–173.
[70] H.Sliman,A.Elnakib,G.M.Beache,A.Soliman,F.Khalifa,G.Gimel’farb,A.Elmaghraby,A.El-Baz, Anovel4DPDE-basedapproachforaccurateassessmentofmyocardiumfunctionusingcinecardiacmagneticresonanceimages,in:ProceedingsofIEEEInternationalConferenceonImageProcessing(ICIP’14),Paris,France,October27–30,2014,pp.3537–3541.
[71] H.Sliman,F.Khalifa,A.Elnakib,G.M.Beache,A.Elmaghraby,A.El-Baz,Anewsegmentation-based trackingframeworkforextractingtheleftventriclecavityfromcinecardiacMRI,in:Proceedingsof IEEEInternationalConferenceonImageProcessing(ICIP’13),Melbourne,Australia,September 15–18,2013,pp.685–689.
[72] H.Sliman,F.Khalifa,A.Elnakib,A.Soliman,G.M.Beache,A.Elmaghraby,G.Gimel’farb,A.El-Baz, MyocardialborderssegmentationfromcineMRimagesusingbi-directionalcoupledparametric deformablemodels,Med.Phys.40(9)(2013)1–13.
[73] H.Sliman,F.Khalifa,A.Elnakib,A.Soliman,G.M.Beache,G.Gimel’farb,A.Emam,A.Elmaghraby, A.El-Baz,AccuratesegmentationframeworkfortheleftventriclewallfromcardiaccineMRI, in:ProceedingsofInternationalSymposiumonComputationalModelsforLifeScience (CMLS’13),Sydney,Australia,27–29November,vol.1559,2013,pp.287–296.
[74] B.Abdollahi,A.C.Civelek,X.-F.Li,J.Suri,A.El-Baz,PET/CTnodulesegmentationanddiagnosis:a survey,in:L.Saba,J.S.Suri(Eds.),MultiDetectorCTImaging,Taylor&Francis,NewYork,NY,pp. 639–651,2014,ISBN978-1-4398-9397-5(Chapter30).
[75] B.Abdollahi,A.El-Baz,A.A.Amini,Amulti-scalenon-linearvesselenhancementtechnique,in:2011 AnnualInternationalConferenceoftheIEEEEngineeringinMedicineandBiologySociety,EMBC, IEEE,2011,pp.3925–3929.
[76] B.Abdollahi,A.Soliman,A.C.Civelek,X.-F.Li,G.Gimel’farb,A.El-Baz,AnovelGaussianscalespacebasedjointMGRFframeworkforpreciselungsegmentation,in:ProceedingsofIEEEInternational ConferenceonImageProcessing(ICIP’12),IEEE,2012,pp.2029–2032.
[77] B.Abdollahi,A.Soliman,A.C.Civelek,X.-F.Li,G.Gimel’farb,A.El-Baz,Anovel3DjointMGRFframeworkforpreciselungsegmentation,in:MachineLearninginMedicalImaging,Springer,2012, pp.86–93.