Contributors
C.Basso,M.D.,Ph.D. UniversityofPaduaMedicalSchool, Padua,Italy
M.Bendeck,Ph.D. UniversityofToronto,Toronto,ON, Canada
J.M.Berthiaume,Ph.D. CaseWesternReserveUniversity, Cleveland,OH,USA
L.M.Buja,M.D.,MS,FCAP,FACC. TheUniversityofTexas HealthScienceCenteratHouston(UTHealth),Houston, TX,USA
J.Butany,MBBS,MS,FRCPC. UniversityHealthNetwork; UniversityofToronto;UniversityHealthNetwork/LaboratoryMedicineProgram,TorontoGeneralHospital,Toronto, ON,Canada,andBrighamandWomen’sHospitaland HarvardMedicalSchool,Boston,MA,USA
G.d’Amati,M.D.,Ph.D. SapienzaUniversityofRome,Rome, Italy
G.A.Fishbein,M.D. DavidGeffenSchoolofMedicineat UCLA,LosAngeles,CA,USA
M.C.Fishbein,M.D. DavidGeffenSchoolofMedicineat UCLA,LosAngeles,CA,USA
C.Giordano,M.D.,Ph.D. SapienzaUniversityofRome,Rome, Italy
A.I.Gotlieb,MDCM,FRCPC. UniversityofToronto,Toronto, ON,Canada
M.K.Halushka,M.D.,Ph.D. JohnsHopkinsHospital, Baltimore,MD,USA
J.L.Hammers,D.O. OfficeofChiefMedicalExaminer,Cityof NewYork,andNewYorkUniversitySchoolofMedicineand Post-GraduateMedicalSchool,NewYork,NY,USA
B.D.Hoit,M.D. CaseWesternReserveUniversity,Cleveland, OH,USA
B.C.Jensen,M.D. UniversityofNorthCarolina,ChapelHill, NC,USA
J.A.Kirk,Ph.D. JohnsHopkinsUniversitySchoolof Medicine,Baltimore,MD,USA
E.Ladich,M.D. CVPathInstitute,Gaithersburg,MD,USA
C.K.Lai UniversityofOttawa,Ottawa,ON,Canada
R.C.Lyon,Ph.D. UniversityofCalifornia,SanDiego, CA,USA
J.J.Maleszewski,M.D. MayoClinic,Rochester,MN,USA
B.M.McManus,M.D.,Ph.D.,FRSC,FCAHS. Providence HealthCare;UniversityofBritishColumbia;Institutefor Heart+LungHealth,andCentreofExcellenceforPrevention ofOrganFailure(PROOFCentre),Vancouver,BC,Canada
R.N.Mitchell,M.D.,Ph.D. HarvardMedicalSchool;Brigham andWomen'sHospital,andHarvard-MITPrograminHealth SciencesandTechnology,Boston,MA,USA
G.Ottaviani,M.D.,Ph.D. TheUniversityofTexasHealth ScienceCenteratHouston(UTHealth),Houston,TX,USA, andUniversityofMilan,Milan,Italy
M.J.Ranek,Ph.D. JohnsHopkinsUniversitySchoolof Medicine,Baltimore,MD,USA
V.Rao,M.D.,Ph.D.,FRCSC. UniversityofToronto,Toronto, ON,Canada
S.Rizzo,M.D.,Ph.D. UniversityofPaduaMedicalSchool, Padua,Italy
E.R.Rodriguez,M.D. ClevelandClinic,Cleveland,OH,USA
B.Sampson,M.D.,Ph.D. OfficeofChiefMedicalExaminer, CityofNewYork,andNewYorkUniversitySchoolof MedicineandPost-GraduateMedicalSchool,NewYork, NY,USA
F.J.Schoen,M.D.,Ph.D. BrighamandWomen’sHospitaland HarvardMedicalSchool,Boston,MA,USA
M.A.Seidman,M.D.,Ph.D. ProvidenceHealthCare, andSt.Paul’sHospital/UniversityofBritishColumbia, Vancouver,BC,Canada
A.Seki,M.D. DavidGeffenSchoolofMedicineatUCLA,Los Angeles,CA,USA
F.Sheikh,Ph.D. UniversityofCalifornia,SanDiego,CA,USA
P.Singhal,M.D. UniversityHealthNetwork,andUniversity of Toronto, Toronto, ON,Canada
J.R.Stone,M.D.,Ph.D. MassachusettsGeneralHospital, Boston,MA,USA
C.D.Tan,M.D. ClevelandClinic,Cleveland,OH,USA
P.Thavendiranathan,M.D. UniversityHealthNetwork, Toronto,ON,Canada
G.Thiene,M.D.,FRCP(Hon) UniversityofPaduaMedical School,Padua,Italy
M.Tolend,B.Sc. UniversityofToronto,Toronto,ON, Canada
P.Vaideeswar,M.D. SethGSMedicalCollege,Mumbai,India
J.P.Veinot,M.D.,FRCPC. UniversityofOttawa,and TheOttawaHospitalandtheChildren'sHospitalofEastern Ontario,Ottawa,ON,Canada
R.Virmani,M.D. CVPathInstitute,Gaithersburg,MD,USA
M.S.Willis,M.D.,Ph.D. UniversityofNorthCarolina,Chapel Hill,NC,USA
S.Xu,M.Sc. UniversityofToronto,Toronto,ON,Canada
Preface
Theconceptofatextbookofcardiovascularpathology stemmedfromthesuccessofaCoreCurriculumCourse inacquiredheartdiseasewhichinvolvedseveralleading cardiovascularpathologists.Dr.MalcolmD.Silver,now anemeritusprofessorofpathologyattheUniversityof Toronto,tookontheroleofeditorofthefirsteditionof cardiovascularpathologywhichwaspublishedin1983. Thiswasfollowedbythesecondeditionin1991,and thethirdeditionin2001,withDr.AvrumI.Gotlieb andDr.FredrickJ.SchoenjoiningDr.Silverascoeditors. Wenowarepleasedtoserveaseditorsofthefourthedition,withpublicationin2015.Inthisedition,wehave takenadvantageofadvancesinpublicationmethodology toprovidevirtuallyalloftheillustrationsincolor.Asin previouseditions,magnificationsareomittedonlight microscopicphotomicrographs,sincelow-,medium-, andhigh-powermicroscopicmagnificationsareobvious.
Muchprogressandchangehasoccurredinour understandingofcardiovasculardiseasesandtherapeuticapproachestodealwiththeseconditions.However, allfoureditionsofCVPhaveremainedtruetothevision ofDr.Silverandcolleaguestoprovideacomprehensive andcontemporarytreatiseofthepathologyofcardiovasculardiseasesbycombiningpresentationsofthe detailedpathologywithdiscussionsofcontemporary insightsintotheetiologyandpathogenesisofthese
conditions.Inthefourthedition,weaimtoachievethis goalofcomprehensiveandcontemporarycoveragewith alogicaldivisionofthesubjectmatterinto20chapters. Inthisedition,wehaveworkedwithourcolleaguesto placespecialemphasisonthegeneticsandmolecular biologyofthediseasesandadvancesintherapeutic approaches.Theexpertiseofourcollaboratingauthors hasbeenessentialinallowingustoachieveourvision forthisbook.
Weintendforcardiovascularpathologytoprovidea uniquecombinationofdetailsofpathologicanatomy essentialforpathologistsinvolvedintheevaluationof cardiovascularspecimensandcardiovasculardiseases coupledwithinformationofbroadinterestforanyone interestedinthenaturalhistoryandtherapeuticadvances inthecardiovascularfield.Thebookisintendedtoprovidevalueforallstudentsofcardiovasculardiseases, includingfirst-timelearnersandlife-longlearners.The contentofthebookalsomakesclearthatcardiovascular pathologistswillcontinuetohaveanimportantrolein definingtheimpactofnewtherapeuticapproacheson theoutcomesofpatientswithcardiovascularproblems. Ourultimategoalistoadvanceknowledgeofallaspects ofcardiovasculardiseaseinordertoenhanceprevention andreducethemorbidityandmortalityforpatientswith thesehighlyprevalentconditions.
L.MaximilianBuja,MD,MS,FCAP,FACC JagdishButany,MBBS,MS,FRCPC
Acknowledgments
Weareextremelygratefulandhavegreatadmirationforourcolleagueswhohaveprovidedthetimeandexpertise toproducethechaptersinthisbook.WealsowishtothankourElsevierpublishers,JeffreyRossettiandMaraConner, fortheirexpertiseandcombinationofpatienceandencouragementindealingwiththeinevitabledelaysinbringing thisprojecttocompletion.Wealsothankourartist,MarieDean,fortheartworkonthecoverandthecongenitalheart diseasechapter,andwethankCarolineJohnsonandcolleaguesontheproductionstaffatElsevierforproducinga high-qualitytext.
J.J.Maleszewskia,C.K.Laib,J.P.Veinotb,c
Cardiacandvasculargrossandmicroscopicanatomy hasbeenappreciatedformanyyears.Knowledgeofultrastructuralanatomyandphysiologyfollowed.Diseasewas notedlongbeforepathogenesiswasclarifiedanditishumblingtorealizethatthisisstillso.Wecontinuetolearn aboutbothnormalandabnormalheartfunction.
Cardiacspecimenswereoriginallypostmortemin nature.Surgicalproceduresontheheartarerelatively newinthehistoryofmedicine.Thepathologist(andsurgeon,radiologist,andinterventionalist)mustunderstand normalcardiacanatomybeforetheycanappreciatepathology.Oneisalsofacedwitharapidlychangingspecialtyof ourpeers.Newproceduresaredeveloped,structuresare repairedratherthanreplaced,andthereisaplethoraof interventionsanddevicesusedfortreatment.Molecular biologyandpersonalizedgenomicsarerapidlyevolving, changingthelandscapeofbothcardiologyandmedicine. Imaginghasalsoevolvedtothepointwheresomeeven postulateitmayreplace,oratleastcomplement,traditional pathologyexamination.Specimensaresmallerand expectationsarehigher.Facedwiththisgrowingbodyof knowledge,thepathologisthasbecomethedataintegrator, interpretingtheclinicalinformation,imaging,andpathologicalfindingstomakeaclinicallyrelevantdiagnosis.
Thischapterattemptstogivesomeprerequisiteanatomicinformationusefulfordiagnosis.Appreciationof grossandmicroscopicanatomyallowsthepathologist tounderstandtherangeofnormalfindings.Herein,we outlinerecommendationsforgrossheartexamination, providesomegeneralsuggestionsforsurgicalspecimen triageandexamination,andgiveanin-depthoverview ofnormallightandelectronmicroscopicfeaturesofthe heartandbloodvessels.
GROSSEXAMINATIONOFTHEHEART
Thepathologistmustdissecttheheartsothatitbest exhibitsalterationsofcardiacstructurebroughtonbydisease.Numerouspreparationanddissectionmethodsare availableandtheprosectormustchoosethebestmethod foraparticularheart(Table1.1).Understandingofthe clinicalpictureisrequisiteforplanningtheapproachto dissectionandevaluation.Regardlessofthemethodchosen,asystematicapproachtotheexaminationofcardiac specimensisnecessary.Inadditiontothegross
TABLE1.1 CardiacSpecimenHandlingTechniquesandTheir Indications
Preparation techniqueIndication
Perfusion fixation
Photographicdocumentation,creationofteaching specimens,generalcardiacevaluation
RadiographyAssessmentofcalcificationofcoronaryarteries, valves,pericardium,andmyocardium. Localizationofdevices(stents,valves,pacemaker leads)
AngiographyLocalizationandquantitationofcoronaryartery disease
DecalcificationEvaluationofcalcifiedtissue
Stent Dissolution
Dissection technique
Short-axiswith inflow-outflow
Tomographicplanes
Leftventricular long-axis
Evaluationofstentedsegmentofvessel
Indication
Routineevaluation
AssessmentoftheLVoutflowtract (hypertrophiccardiomyopathy,chronicaortic stenosis)
4-ChamberDemonstrationof: Atrialdilatation
Diseaseoftheatrioventricularvalves
BaseofheartDemonstrationof: Valvularheartdisease
Rightventricular long-axis
Variationsincoronaryarterydisposition
Demonstrationof: Atrialseptaldefects
Leadplacement
Inflow-outflowCongenitalheartdisease
examination,acomprehensivediagnosisisusuallyformulatedinconjunctionwithwell-chosenhistologic, ultrastructural,andhistochemical/immunohistochemicalstudies.Moreover,samplesmayalsobeprocured formicrobiologic,serologic,biochemical,ormolecular andgeneticstudies.Eveniftherehasbeennoindication ofsuspectedheartdisease,forethoughtonthepartofthe pathologistandhisorherteammaypromptappropriate
samplingoftissuesthatcanbeusedforfuturediagnostic orresearchstudies.
Ultimately,everymemberofthecardiacteamstudies thecardiaccellanditsadaptation,injury,ordeath.The pathologististheteammemberbestacquaintedwithcellularmorphologyandbesttrainedtointerpretthecause andmechanismofdiseaseatthecellularandmolecular level.Intheheart,morethanmostotherorgans,cellular adaptationsareattendedbyhighlypredictablegrossand histologicalterations.Thisallowsthepathologisttoadd substantiallytotheoverallunderstandingofthedisease anditscourse.
PositionintheChest
Theheartandgreatvesselsaresituatedinthemidthoraxwithinthemediastinum.Themediastinumis dividedintofourspecificregions:anterior,middle,posterior,andsuperior.Theheartislocatedwithinthemiddlemediastinum,theaorticarchwithinthesuperior mediastinumandthedescendingthoracicaortainthe posteriormediastinum.Anteriorly,itisoverlaidoneither sidebythelungsandpleura,whichalsocoverthelateral bordersoftheheart.Thecardiacapexisnormally directedleftward,anteriorly,andinferiorly.
Boththelocationandorientationoftheheartwithin thechestcanbeaffectedbyunderlyingcardiacmalformationsand/orabnormalitiesofadjacentstructures.Terms suchaslevocardia,dextrocardia,andmesocardiaare commonlyemployedtodescribeposition,butarenot specifictowhichpointtheyareaddressing.Therefore, withrespecttopositioninthechest,heartlocationand apicaldirectionshouldbedescribedindependentlyto avoidanyambiguity.Descriptionterminologysuchas left-sided(normal),right-sided,ormidlinecanbe employedforcardiaclocation.Likewise,apicaldirection canbedescribedasleftward(normal),rightward,or midline.
DeterminationofSidedness(Situs)
Beginningitsembryologicdevelopmentasbilateral structuresthatfusetoformasinglemidlinestructure, thecardiovascularsystemlateracquiresasymmetry andistherebycharacterizedbysidedness(situsorhandedness)[1].Sidednessisgeneticallydeterminedandmay benormal,mirror-image,isomeric,orindeterminate. Whileabnormalitiesofsidednessmayaffecttheentire body(asintotalmirror-imagesidednessorsitusinversus totalis),theycanalsoinvolveindividualorgansystems. Therefore,sidednessofindividualorgansystemsshould beindependentlydescribed.
Cardiacsidednessisdeterminedbythepositionofthe morphologicrightatrium.Itisnotdeterminedbythe
apicaldirection,cardiacposition,orsidednessofthenoncardiacviscera.Therefore,accuratedistinctionbetween leftandrightatrialmorphologyisvital(seebelow). Therightatriumisnormallyright-sided(situssolitus), butisleft-sidedinmirror-imageheart(situsinversus). Bilateralrightatriadefinerightcardiacisomerismand bilateralleftatriaconnoteleftcardiacisomerism(both consideredformsofsitusambiguous).Incircumstances whereatrialmorphologycannotbedetermined,theterm indeterminatesidednessmaybeemployed.
PericardiumandPericardialReflections
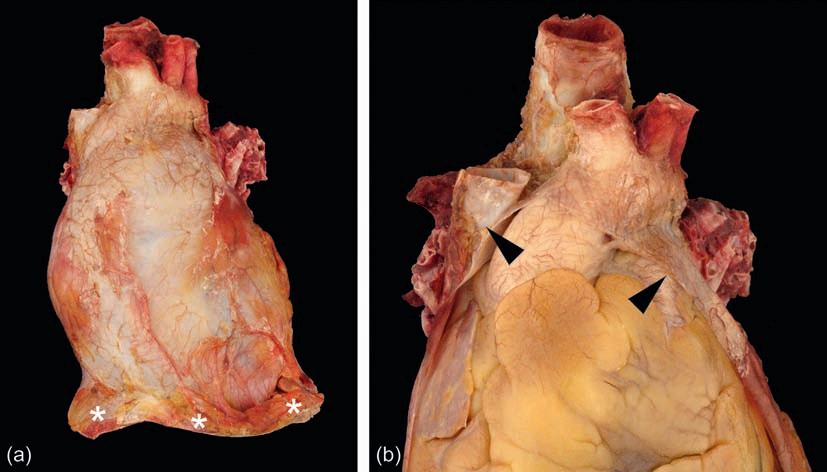
Thepericardiumisaroughlyconicalstructurethat bothcoversandsurroundstheheartastheserousvisceral andfibrousparietalpericardia,respectively(Figure1.1a). Betweenthesetwolayers,inaspacecalledthepericardial sac,iscontained15-50mLofstraw-colored,serous fluid[2].
Theparietalpericardiumattachesalongthegreatvesselssuchthattheascendingaorta,mainpulmonary artery,terminalsuperiorvenacava,andterminalpulmonaryveinsareintrapericardial(Figure1.1b).Thepericardiumisattachedtothecentraltendonofthediaphragm andtheadjacentdiaphragmaticmuscleatitsbase.The parietalpericardiumconsistsofanouterfibrouslayer withaninnerlayerofmesothelialcells.Itsoutersurface alsocontainsvariableamountsofadiposetissuethatmay contributetothecardiacsilhouetteradiologically.The densecollagenlimitstheacutedistensibilityoftheparietalpericardiumsuchthataslittleas200mLofrapidly accumulatedfluidcancompromisediastolicfilling(cardiactamponade)(see Chapter13).
Thevisceralpericardium(alsocalledtheepicardium) consistsofaliningofmesothelialcellswithvariable depositsofsubjacentadiposetissue.Typically,thevisceralpericardiumistransparentwiththesubjacentstructuresreadilyvisible;however,focalpalewhitethickening canbeencounteredinmanystructurallynormalspecimens.Oftenreferredtoas “soldier'splaques,” theincidenceoftheseepicardialcollagenplaquesriseswith ageandmayrepresenthealedpericarditis(Figure1.2) [3].Thefattydepositsaremostpronouncedintheregion oftheatrioventricular,interventricular,andinteratrial grooves.Prominentfattagsalsocovertheoriginsof thecoronaryarteriesbetweentheaortaandatrial appendages.
Embryologically,rapidbulboventriculargrowth pushesthedevelopingheartintothepericardialspace analogoustoafluid-filledballoonwithafistbeing pressedintoit.Theparietalandvisceralpericardia meetalongthegreatvesselsatthepericardialreflection. Likewise,thepericardiumreflectsaroundtheregionof thegreatveins,formingtheobliquepericardialsinus
FIGURE1.1 Pericardium.(a)Theparietal(fibrous)pericardiumcoverstheheartandproximalgreatarteries.Thediaphragm(asterisks)canbe seenalongtheinferiorborder.(b)Withtheanteriorparietalpericardiumremoved(arrowheads),therelationshipwiththeheart(investedwith visceralpericardium)canbeappreciated.
FIGURE1.2 Epicardialcollagenplaque(soldier'spatch).Thesefocal tan-whitefibrouspatches(arrowhead)aremostoftenlocatedonthe anterioraspectoftheheart.
immediatelyposteriortotheleftatrium.Atunnel-shaped reflectionisalsoformedbythegreatarteriesandthe atrialwalls,calledthetransversepericardialsinus.The appreciationofthesesinusesisincreasinglyimportant withcatheter-basedintrapericardialproceduresbeing developed.
RemovaloftheHeart
Ifthereisnoreasontosuspectamajorcardiacmalformationaftercarefulexternalassessment insitu (see below),theheartisbestexaminedafteritsremoval fromthechestorfromthethoracicorganblock.Thedissectionmethodbelowdescribesremovalfromthethoracicorganblockafterithasbeenremovedfromthe chestcavity.Ifindicated,andbeforeproceeding,a pericardialfluidsamplecanbeobtainedbyneedlepuncturethroughanareaofthepericardiumthathasbeen searedforsterilization.Theanteriorparietalpericardium isthenincised insitu andthepericardialcontentsare noted;15-50mLofclear,straw-coloredfluidisanormal finding[2].
Theparietalandvisceralpericardialserosalmembranesareinspected insitu;theirsurfaceisnormally smoothandshiny.Papillaryfibroustags,whichareof nosignificance,maybeobservedonthevisceralpericardiumcoveringtheatrialappendages[4].Thevascular connectionsoftheheartaredefined insitu,including theligamentumarteriosumthatjoinstheoriginoftheleft mainpulmonaryarterytotheaorticarch,incasethereisa patentductusarteriosus.Apersistentleftsuperiorvena cava,seenexternallytojointheleftatrium,issometimes foundinanotherwisenormalcardiovascularsystem;it drainsintothecoronarysinus,which,asaresult,hasa prominentandenlargedostiumintherightatrium.Otherwise,itsremnant,theligamentofMarshall,canbe identifiedattheleftedgeofthetransversepericardial sinus.Theazygosandhemiazygosveinsarebestviewed insitu whiletheyarestillfilledwithblood.
Themainpulmonaryarteryisthenincisedand opened,anditslumenandthoseofitsrightandleft branchesareexploredbydigitalprobingforthrombus, embolus,orotherpathology.Similarly,thesuperiorvena cavaistransectedapproximately1cmaboveitsconnectiontotherightatriumandsimilarlyexplored.Turningto theposteriorsurfaceofthethoracicblock,theposterior parietalpericardiumisincisedatthemidline,inferior tosuperior,tothelevelofthecarina.Anotecanbemade ofthesitusandappearanceofthebronchi.Reflectingthe leftandrighthalvesoftheposteriorparietalpericardium totheirrespectivesideswillrevealthepulmonaryveins, usuallytwooneachside(anupperandalower).These canbetracedoutandtransectedapproximately1cm fromtheirconnectiontotheleftatrium.Theaortaand thepulmonaryarteryarethentransected0.5-1cmdistal totheirvalvecommissures.Atthispoint,theheartwillbe heldtothethoracicblockbythedorsalmesocardium, whichcanbecutalongtheinferioredgeofthepulmonary arteries.
ExternalAnatomyandLandmarks
Theamountofepicardialfatshouldbegaugedatthis stage.Normally,itfillstheatrioventricularandinterventriculargrooves,encasingtheepicardialcoronaryarteries. Whenfatisincreased,itmayblankettheepicardialsurface ofallchambers,especiallyalongthecourseofcoronary bloodvessels;inextremecases,morethanhalfoftheheart weightmaybecomposedoffat[5].Epicardialfatdoes tendtopositivelycorrelatewithvisceraladiposity,ingeneral[6].Fatalsoextendsanteriortothelunghilaand spreadsintothemyocardiumbetweenthemyocytesand alongtheintramyocardialvessels,particularlyintheright ventricleandatrialseptum[7–11].Grossly,ina “fatty heart” (alsocalledpathologicadiposity),typicallyonly theouterhalfortwo-thirdsofthemyocardiumcontains adipocytes.Thiscontrastswiththepatternseeninarrhythmogeniccardiomyopathy(see Chapters10 and 11).
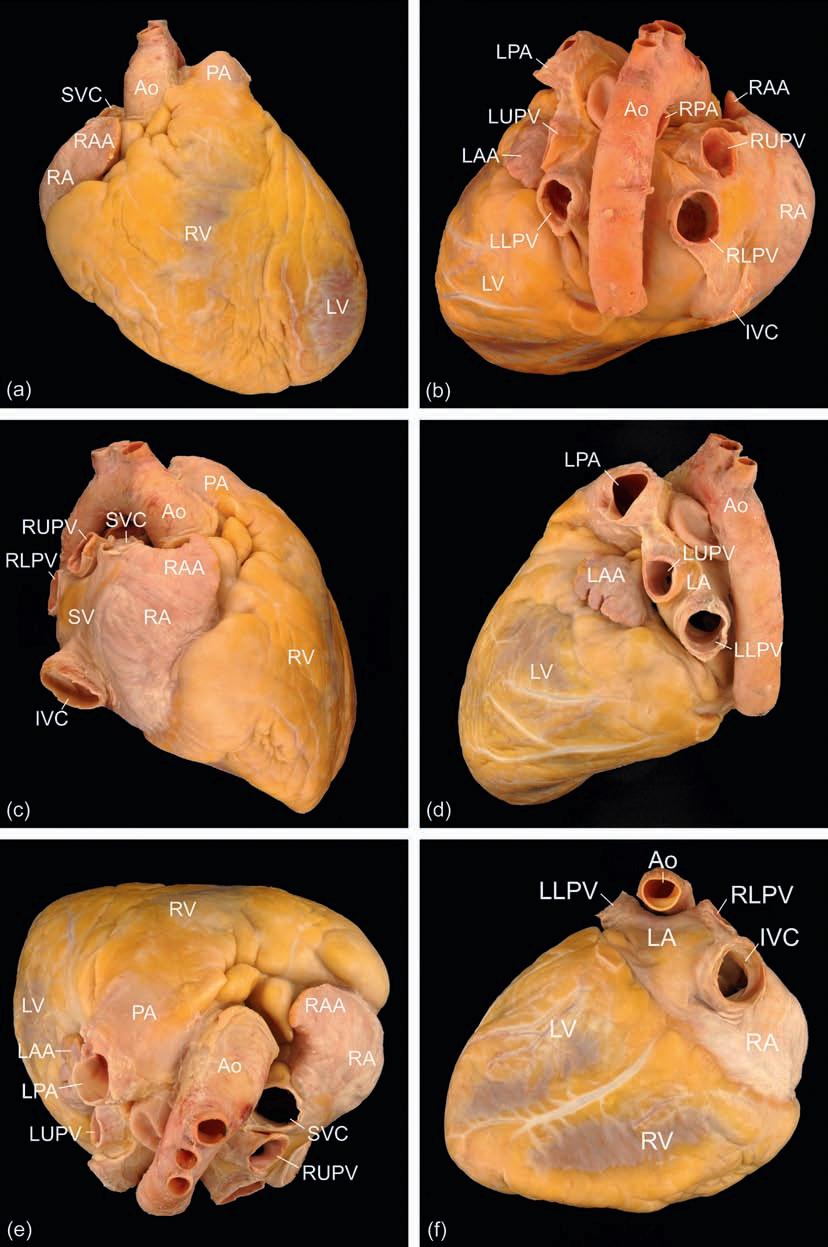
Therightventricleformstheanteriorborderofthe heart,beinglocatedbehindthesternum(Figure1.3). Therightatriumformstherightlateralborderofthe heart,receivingboththesuperiorandinferiorvenacavae. Theleftventricleformstheposterior,inferior,andleftlateralsurfacesoftheheart,withtheleftatriumoccupyinga midline-posteriorposition.Mostcommonly,fourpulmonaryveinswilldrainbacktoconnecttotheleftatrium (twofromtheleftlungandtwofromtherightlung).
GreatVessels
Therelationshipbetweenthegreatvesselsandthe investingpericardiumisbestunderstoodwhentheir rootsareviewedafterremovaloftheheart(Figure1.4). Aninvestmentofserouspericardiumenclosesthegreat
arteries,andasecondcontainsalltheveins.Thus,the pericardiumenclosesthedistalhalfofthesuperiorvena cava,mostoftheascendingaorta,andpulmonarytrunk. Compromiseofanyportionofthevascularwall,within theencasedarea,mayresultinhemopericardium.
Themainpulmonaryarteryarisesfromtherightventricleandtravelstotheleftoftheascendingaorta, directedtowardtheleftshoulder.Atitsbifurcation,the leftpulmonaryarterycontinuesovertheleftbronchus, whereastherightpulmonaryarterycoursesbeneath theaorticarchandposteriortothesuperiorvenacava.
Theaortaarisesattheleveloftheaorticvalveannulus andterminatesatitsbifurcationintothecommoniliac arteries.Itcanbedividedintofourdistinctregions:the ascendingaorta(beginningattheaorticannulusand extendingtotheoriginofthebrachiocephalicartery),aorticarch(extendingtotheligamentumarteriosum),descendingthoracicaorta(extendingtothediaphragm), andtheabdominalaorta(extendingtotheiliacbifurcation).Theascendingaortaincludesbothabulboussinus portionatitsproximalendandamoretubularportion extendingtowardthearch.Theregionsoftheaortaare differentiatednotonlybytheirlocationbutalsobytheir embryologicderivation.Theaorticrootisderivedfrom thesecondheartfield(lateralplatemesoderm),the ascendingaortaandarchfromtheneuralcrest,andthe descendingaortafromtheparaxialmesoderm[12].
CoronaryVessels
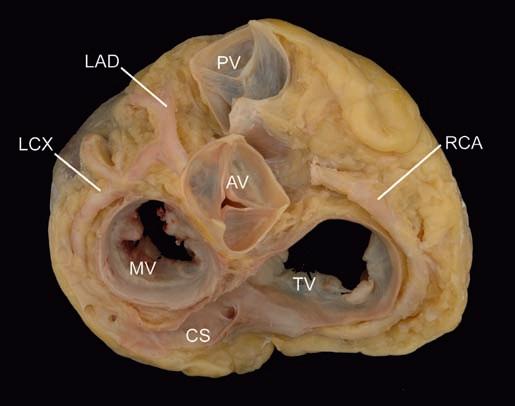
Theepicardialcoronaryarteriesareexaminedbefore incisingtheheartchambers.Therightandleftcoronary arteriesarisefromtheirrespectiveaorticsinuses(ofValsalva)(Figure1.4).Theirostiaarisemidwaybetweenthe aorticvalvecommissures,justbelowthesinotubular junction(theridgewithintheascendingaortaformed bythevirtualringconnectingthetipsoftheaorticvalve commissures).Therightcoronaryartery(RCA)usually arisesperpendiculartotheaorticsinus,whereastheleft maincoronaryarterywilloftenariseatanacuteangle andtraveldownward,beforebranchingtobecomethe leftanteriordescending(LAD)andcircumflex(LCX)coronaryarteries.TheLCXandRCAtravelintheirrespectiveatrioventriculargrooves,definingtheplaneofthe cardiacbase.Theanteriorandposteriordescendingarteriestravelintheirrespectiveinterventriculargroovesand willindicatetheplaneoftheventricularseptum.The RCAwillsupplytheposteriordescendingcoronary arteryin70%ofindividuals,so-calledright-sidedcoronarydominance[13].TheLCXwillsupplytheposterior descendingcoronaryarteryin10%ofindividuals (left-sidedcoronarydominance),withtheremaining individuals(20%)havingsharedcoronarydominance (co-dominance).
Epicardialbranchesincludediagonalsarisingfromthe LADandmarginalsarisingfromtheRCAandLCX(acute
FIGURE1.3 Externalcardiacanatomy.(a)Anteriorperspective.(b)Posteriorperspective.(c)Rightlateralperspective.(d)Leftlateralperspective.(e)Superiorperspective.(f)Inferiorperspective.Ao,aorta;IVC,inferiorvenacava;LA,leftatrium;LAA,leftatrialappendage;LPA,leftpulmonaryartery;LLPV,leftlowerpulmonaryvein;LUPV,leftupperpulmonaryvein;LV,leftventricle;RA,rightatrium;RAA,rightatrialappendage; RLPV,rightlowerpulmonaryvein;RUPV,rightupperpulmonaryvein;RV,rightventricle;PA,pulmonaryartery;SV,sinusvenosus;SVC,superior venacava.
FIGURE1.4 Baseoftheheart.Thecardiacbase(withatriaremoved) demonstratestherelationshipofthefourmajorcardiacvalvesaswell asthedispositionoftheepicardialcoronaryarteriesandcoronary sinus.AV,aorticvalve;CS,coronarysinus;LAD,leftanteriordescendingcoronaryartery;LCX,leftcircumflexcoronaryartery;MV,mitral valve;PV,pulmonaryvalve;RCA,rightcoronaryartery;TV, tricuspidvalve.
andobtuse,respectively).In60%ofindividuals,thefirst branchoftheRCAistheconuscoronaryartery,which suppliestherightventricularoutflowtract(conusor infundibulum);intheremaining40%,thearteryarises independentlyfromtherightaorticsinus,whenaseparateostiumwillbenoted[14].Thesinoatrialnodalartery arisesfromtheRCAinapproximately60%ofheartsand fromtheLCXinthebalance.TheAVnodalartery,incontrast,willarisefromthedominantcoronaryartery,with theRCAsupplyingitinapproximately90%ofhearts.
Iftheprosectorhasreadyaccesstopostmortemradiography,dissectioncanbecomplementedbypostmortemangiography,whichcanindicatethepresenceof calcificcoronaryarterydiseaseaswellasassessthediseaseburden.Otherwise,palpationofthecoronaryarteriesshouldbeperformedtoevaluateforcalcification.If identified,theentireepicardialarterialtree must bedissectedfromtheheartanddecalcified(Table1.1).Each arteryshouldberemovedandplacedinaseparatecontainer.Decalcificationpreventsartifactualdamage causedbycuttingthroughacalcifiedarterialwall,crushingthelumenandplaquedisruption.Performingdecalcificationisthebestwaytopreparecalcifiedcoronary arterialtissueforhistologicexamination.Intheabsence ofanysuspicionofcoronaryarterydisease,especiallyif thepatientisyoungandvesselsareapparentlynoncalcified,theymaybeopened insitu,bycrosssectioningat 0.2-0.5cmintervals.Openingthevesselslongitudinally isnotoptimalasitbecomesdifficulttoassessdisease severityandluminalnarrowing.Diseasedareasshould besubmittedforhistology(4-6crosssectionsper
cassette),toincludebothhematoxylin-eosinstaining andanelasticstain(e.g.,Verhoeff-vanGieson,Movat pentachrome,etc.).Dividingeachofthecoronaryarteries intothirds(proximal,middle,anddistal)anddesignating assuchcanfacilitateinterpretationandreporting.
Thepresenceofcoronaryarterystentspresentsa uniquechallengeintheevaluationofcoronaryarterydisease.Methodsthatinvolvecuttingthestentedvesselwith adiamondmicrotome,electrolyticstentdissolution,and physicalstentremovalhaveallbeendescribed[15–17]. Regardlessofthemethodchosen,effortshouldbemade toevaluatetheseregionsofthevesseltoevaluatefordiseaseprogressionaswellasdevicefailure.
Coronaryveinsfollow,inanantiparallelfashion,the courseofthearteries.Theyaremoresuperficialintheepicardialfatandeventuallyjointhecoronarysinus,which passesfromlefttorightintheposterioratrioventricular groovetoopenintotheposteriorwalloftherightatrium justanteriortotheinferiorvenacava.Somesmall(accessory)coronaryveinsdrainthefreewalloftherightventricle andopendirectlyintotheanteriorwalloftherightatrium. Thesmallestveins,Thebesianorluminalveins,formwithin themyocardiumanddraindirectlyintoeachoftheheart chambers[18].Theyareremnantsofsinusoidalintramyocardialbloodvesselspresentintheembryonicheart,at thestageofthenoncompacted(spongy)myocardium.
Thecoronarysinus(Figure1.4)isthemosteasilyevaluatedcardiacveinandisguardedbythevalveofthecoronarysinus(Thebesianvalve)atitsopeningintotheright atrium.Itmaybelargerthannormalifitdrainsanomalousvessels(e.g.,apersistentleftsuperiorvenacavavia anobliqueveinofMarshallorvesselsfromthelung anomalouspulmonaryvenousdrainage)orinthepresenceofsevererightheartfailure.Alternatively,thecoronarysinusopeningmaybesmallerthannormaloreven atreticifcoronarysinusbloodispassingfromtheheart throughapersistentleftsuperiorvenacavatotheinnominateveinand,thence,viaarightsuperiorvenacavato therightatrium.Thecoronarysinusmaybeabsent,as inthoseconditionsinwhichaleftsuperiorvenacavaconnectsdirectlytotheleftatrium(anunroofedsinus).Such variationsinthesizeofthecoronarysinusmaybeisolatedandincidental,buttheyoftenaccompanyserious cardiacmalformations.
Acardiaclymphaticsystemhasbeenwelldescribed [19,20].Lymphaticplexiwithinthesubendocardium, myocardium,subepicardium,andpericardiumhaveall beendemonstrated.Whenengorged,thesecangrossly manifestaswhitestreakingintheheart.
OpeningtheHeart
Followingexternalexamination,theheartshouldbe openedtoevaluatetheinternalcardiacanatomy.Avarietyofdissectionmethodsareavailableandtheprosector
shouldbeguidedbytheclinicalcircumstancesandthe grossfindingsoftheexternalcardiacexaminationwhen choosingwhichwillbeemployed(Table1.1).Themethod describedbelowisanexcellentgeneraldissectiontechniquethatcanbeusedforbothnormalandabnormalcardiacspecimensafterexternalexaminationandevaluation oftheepicardialcoronaryarteries.Additionally,itleaves thevenousconnectionsintactanddoesnotdisruptthe majorconductionsystemcomponents(sinoatrialnode, atrioventricularnode,bundleofHis,andproximalbundlebranches).
Alongbladeisusedtocutalongtheshortaxisat1cm intervalsfromtheapextothemidventricularlevel,leavingthetopsofthepapillarymusclesstillattachedtothe tendinouscords.Thesectionsareconsecutivelylaidout (apicalsurfacesup)andthemyocardiumisevaluated formuralthicknessandgeneraluniformity.Anylesion shouldbedocumented,bothinsizeandlocation.With respecttolocation,thechamber(leftventricle,rightventricle,orventricularseptum),level(apicalormidventricular),andanatomicdirection(anterior,inferior,or lateral)shouldbenoted.
Attentioncanthenbeturnedtothecardiacbase.Startingattherightatrium,usingscissors,acutcanbemade approximately1cmanteriortotheorificeoftheinferior venacava,justproximaltothetricuspidvalveannulus. Thiscutisthenextendedsuperiorlytothetipoftheright atrialappendage.Therightatrialfreewallcanthenbe reflectedback,andthechambercanbeinspected.Assessmentforapatentforamenovalecanbedoneatthistime aswell.Incisingbetweenthesuperiorandinferiorvena cava,whileadvocatedbysome,isdiscouragedprimarily becauseitmaydisruptthesinoatrialnodeaswellasa Chiarinetwork(ifpresent).
Movingdownwardtotherightventricle,acutcanbe madethroughtheinflowportionoftheventricleapproximately1cmawayfromtheventricularseptum,through theposteriortricuspidvalveleaflet.Theoutflowtractof therightventriclecanbeopenedbycuttingalongthe anteriorportionoftheventricularseptum,throughthe infundibulumandoutthepulmonaryvalve.Generally, themoderatorband(trabeculumseptomarginalis)will becutatthispoint.Stayingalongtheventricularseptum willusuallydirectthecuttothecommissurebetweenthe anteriorandleftpulmonaryvalvecusps.
Theleftatriumisbestapproachedfromtheposterior aspect.Averticalcut,usingscissors,ismadebetween theleft-andright-sidedpulmonaryveins.Thecutis extendedsuperiorlytothetopoftheatrialdomeandthen inferiortowardthemitralvalveannulus.Atthelevelof themitralannulus,theincisionisextendedleftward aroundtheleftatrium,paralleltheleftatrioventricular groove,tothetipoftheleftatrialappendage.Evaluation formuralthrombusisimportant,astheleftatrialappendageisacommonsitetofindsuch[21].
Theinflowportionoftheleftventricleisincisedby positioningalongbladedownthroughthemitralvalve (sharpendtowardthefreewall)inthemiddleoftheanteriorleaflet.Thefreewallisthencut(atthemidportionof theP2segmentoftheposteriormitralvalveleaflet).Cuttingthelateralleftventricularwallbetweenthepapillary musclesmayalsobedone.Openingtheleftventricular outflowtractisbestdone,usingeitherscissorsoralong blade,fromtheventricleouttotheaorta.Stayingwithin 1cmoftheventricularseptumwillhelpensurethatthe anteriormitralvalveleafletisnotinadvertentlydamaged intheprocess.Thisfinalcutwillusuallycutthroughthe leftaorticvalvecusp.
RightAtrium
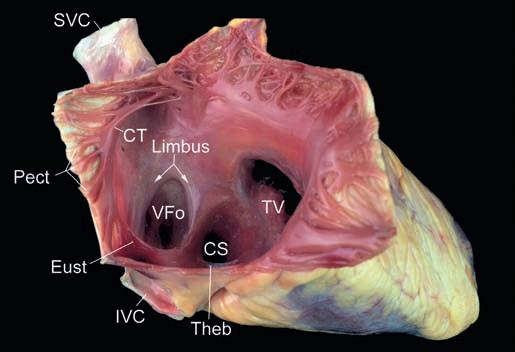
Therightatriumservesasthereceivingchamberfor bloodreturningfromthesystemicveinsandliesposterior totherightventricleandanteriortotheleftatriumina rightlateralposition(Figure1.5)[22,23].Itsbasicanatomiccomponentsarethatofthefreewallandtheseptum.Ithasvariablethickness,measuring2-6mmin someregionsand <1mminothers.
Thefreewall,internally,hasasmooth-walledposteriorportion,derivedfromtheembryologicalsinusvenosusthatreceivesbloodfromthevenacavaeandthe coronarysinus.Theremainingfreewallisderivedfrom theprimitiveatriumandcontainsprominentsmallmuscularridgesarrangedinparallel,calledpectinatemuscles.Thecristaterminalis,correspondinginternallyto theexternalsulcusterminalis,servesasthedividingline betweenthesetwoportions.
Pectinatemusclesarisefromthecristaterminalis, whichisaprominentC-shapedridgeofmusclethatseparatesthesmooth-walledportionoftheatriumfromthe
FIGURE1.5 Internalanatomyoftherightatrium.Withthefreewall opened,theanatomyofboththefreewallandseptumcanbeappreciated. CT,cristaterminalis;CS,coronarysinusostium;Eust,Eustachianvalve; IVC,inferiorvenacava;Pect,pectinatemuscles;SVC,superiorvenacava; Theb,Thebesianvalve;TV,tricuspidvalve;VFo,valveofthe foramenovale.
trabeculatedportion.Theinferioraspectoftheright atrium,betweentheostiumofthecoronarysinus,posteriorly,andthetricuspidannulus,anteriorly,isaregion referredtoasthecavotricuspidisthmus.Itisinthisregion oftheheartwhereatrialflutterisfrequentlythoughtto arise[24].Themidportionoftheisthmuscontaininga shallowpouchwithtrabeculatedliningiscalledthe sub-EustachiansinusofKeith[25].
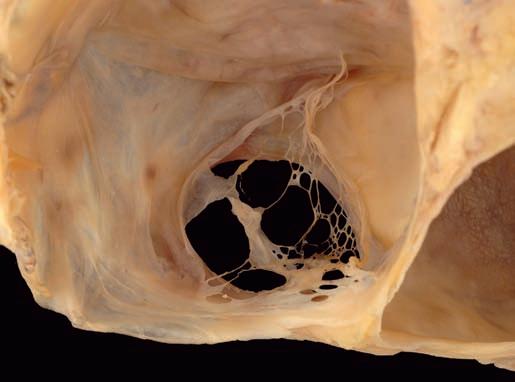
Threedistinctvalvescanbevisualizedinsideofthe rightatrium:thevalveoftheinferiorvenacava(Eustachian),thevalveofthecoronarysinus(Thebesian),and thevalveofthefossaovalis.Thefirsttwovalves,remnantsoftherightvenousvalve,varygreatlyinsize andmaybefenestratedorabsent,buttheEustachian valveiswelldevelopedinapproximately90%ofnormallyformedhearts[26].TheThebesianvalveisgenerallylesswelldeveloped,coveringtheostiumofthe coronarysinusinapproximately40%ofsubjectswith normalheartweight[27].AChiarinetwork,usuallya weborlace-likesheetoftissue,mayspantheatrialcavity fromtheregionoftheThebesianortheEustachianvalve toinsertintothecristaterminalis(Figure1.6)[22].Theleft venousvalveisusuallyabsorbedintotheatrialseptum, butremnantsmaybefoundasbandsoftissuebridging theposteroinferiormarginofthefossaovalis.
Themostprominentfeatureoftheseptalportionofthe rightatriumisthatofthefossaovalis(Figure1.5).This structurecanbeaslargeas3.5cmindiameterandisusuallywelldefinedsuperiorlyandanteriorlybytheraised limbusofthefossaovalis[28].Thehorseshoe-shapedlimbussurroundsarelativelythinmembrane,thevalveof thefossaovalis.Thisvalveisthinandtranslucentearly inlife,butprogressivelythickensthroughoutlife[29]. Probingunderthelimbusanteriorlyshowswhetherthe
FIGURE1.6 Chiarinetwork.Thisweb-likestructurerepresentsa fenestratedremnantoftherightvenousvalvesandcanbeseenatthe ostiumoftheinferiorvenacava,thecoronarysinus,orboth.
foramenovaleisobliteratedorpatent;thelattermaybe seeninathirdofpeoplebeyondthefirstyearoflife[23].
Ananeurysmalbulgeoftheseptumprimummay occurthroughthefossaovalisintoeitheratrium[30]. Theassociationinadultsofaneurysmsofthefossaovalis withincreasedfrequencyofembolicstrokehasbeen attributedtoitssignificantassociationwithmitralvalve prolapse,dilatedatria,intracardiacthrombi,andpatent foramenovale;thelatterconditionispresentin70%of suchsubjects[31].Ananeurysmofthefossaovalisbulgingtotheleftatriumisalsoseenduringfetallifeandis associatedwithfetalarrhythmiaandothercausesoffetal heartfailure[32].
Bytransillumination,partofthemembranousinterventricularseptumisseenintherightatriumjustproximaltothetricuspidannuluswhereitjoinsthebaseofthe septalleafletofthetricuspidvalve.Adefectinthisarea permitscommunicationbetweentheleftventricleand therightatrium,whereasadefectdistaltotheseptalleafletisamembranousventricularseptaldefectatitsmost commonlocation.Usually,theanteriorandseptalleaflets ofthetricuspidvalvecrossthemembranetomeetattheir commissure.Rarely,theyinsertattheedgeofthemembranewithoutformingacommissure.Thisdoesnot producevalvularregurgitation.Therightaorticsinus isalsocloselyrelatedtotherightatriumandmaycause asmoothprotuberanceoftherightsideoftheanterosuperioratrialseptum,thetorusaorticus[33].Theinterventionalistshouldbemindfulofthisanatomicrelationship duringproceduressuchastransseptalpunctureorplacementofaseptaloccluderdevice.
ThetendonofTodaroisaligamentattachedtothe fibrousskeletonoftheheart.ItmayrepresentthecommissureoftheEustachianandThebesianvalves.Thistendonprobablyfunctionsduringfetallifetostrengthenthe freeedgeoftheEustachianvalveandhelpstodirect venousreturnfromtheinferiorvenacavaacrosstheforamenovale[34].ThetendonofTodaroissometimesseen inadulthearts,butitismoreobviousinchildren.Thetendonisawhitecorddeeptotherightatrialendocardium, passingfromthesinusseptum,whichseparatestheostia oftheinferiorvenacavaandthecoronarysinus,toward themembranousseptum.Whenthistendonisvisible,itis ausefullandmarkfortheatrioventricularnode,which lieswithinananatomictriangle(thetriangleofKoch, describedbelow).
TricuspidValve
Thetricuspidvalveisathree-leafletvalvewithasaddleshapedannulusanditsvalvularplanefacingtowardthe rightventricularapex[35–38].Itsnormalannularcircumferenceis10-11.1cminwomenand11.2-11.8cminmen [39].Thethreeleafletshangfromthevalveringlikea veil,withtheseptalandposteriorleafletsagainsttheseptal andinferiorwallsoftherightventricle,respectively
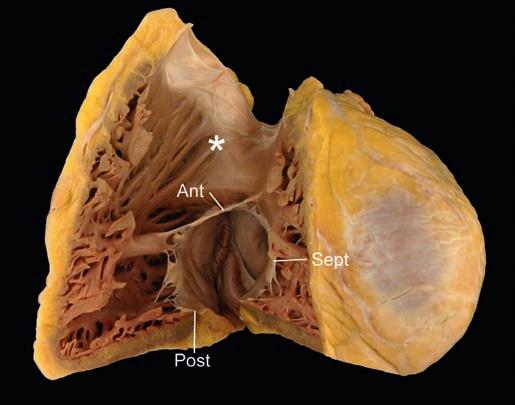
FIGURE1.7 Internalanatomyoftherightventricle.Therightventricle,openedalongtheinflowandoutflowportionsexhibitsthethree tricuspidvalveleaflets(Ant,anteriortricuspidvalveleaflet;Post,posteriortricuspidvalveleaflet;Sept,septaltricuspidvalveleaflet).The courseapicaltrabeculations,septalcordalattachmentsandthemuscular outflowtract(asterisk)serveasmorphologicdifferentiatorsfromtheleft ventricle.
(Figure1.7).Theanteriorleafletformsadiagonalcurtain separatingtheinflowandoutflowtractsoftherightventricle.Apapillarymuscleislocateddirectlybeneatheach commissure,sendingtendinouscordsuptotheadjacent leaflets(roughlyhalftoeach)[38].Eachleaflethasadistal roughzoneandaproximalbasalzoneintowhichthecords insert,aswellasaclearzonefreeofcordinsertionthatlies betweentheroughandthebasalzones.
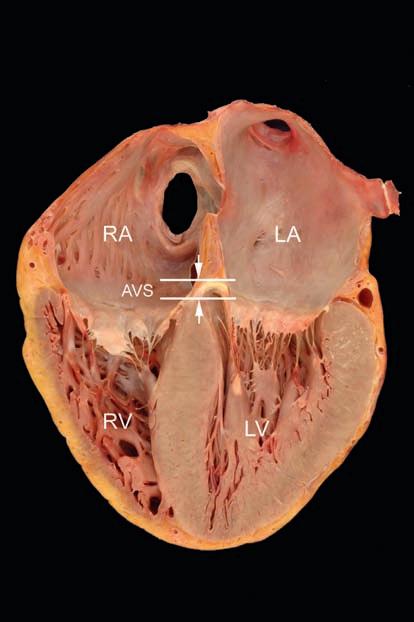
Theannulusofthetricuspidvalveismoreapicallypositionedthanthatofthemitralvalveannulus(Figure1.8). Thisnonplanararrangementoftheatrioventricularvalves allowsforthreedistinctregionstobedefinedintheseptumthatdividetherightandleftheart:theinteratrial component(atrialseptum),separatingtherightandleft atria;theatrioventricularcomponent(atrioventricular septum),separatingtherightatriumfromtheleftventricle; andtheinterventricularcomponent(ventricularseptum), separatingrightandleftventricles.
Theanteriorleafletisusuallythelongest(average 2.2cm).Itissemicircularorquadrangularandis3.7cm inaveragewidthatitsbase.Rarely,ithasadistinctscallopinitsmedialsideneartheanteroseptalcommissure. Theseptalleafletissemi-ovalandis1.6cmlongby 3.6cmwideonaverage.Itshowsacharacteristicfold onitsatrialsurfaceintheanglewhereitsbasepassesfrom theposteriorventricularfreewalltothemembranous area.Theposteriorleaflet,whichaverages2.0cmlong by3.6cmwideatitsbase,hasavariablenumberofscallops,usuallytwoorthree,producedbyindentationsinits freeedge.Thecordsareofvaryinglength(0.3-2.2cm)and thickness(0.05-0.15cm)[38].
FIGURE1.8 4-Chamberviewoftheheart.Inthistomographic plane,allfourcardiacchamberscanbevisualized.Additionally,the moreapicalpositionofthetricuspidvalveannulus(whencompared tothemitralannulus)canbeappreciated.Theseptumbetweenthe annuliiscalledtheatrioventricularseptum(AVS)thatseparatesright atrium(RA)fromleftventricle(LV).LA,leftatrium;RV,rightventricle.
Ofthethreepapillarymuscles,theanterioristhelargestandmostwellformed.Itmaybesingleorbifidand providescordalinsertionstotheanteriorandposterior leaflets.Theposteriorpapillarymusclearisesfromthe inferiorwallsendingcordstotheseptalandposterior leaflets.Themedialpapillarymuscle(alsocalledthepapillarymuscleoftheconusorthemuscleofLancisi)arises alongthesuperioraspectoftheseptalband,atthelevelof themembranousseptumandhascordalattachmentsto boththeseptalandanteriorleaflets.Itisimportanttonote thatinadditiontocordstothepapillarymuscles,thetricuspidvalvecharacteristicallyhascordstotrabeculations oftheseptum.Theseseptalcordattachmentsserveto helpdifferentiatethetricuspidfromthemitralvalvein thesettingofcongenitalheartdisease.
RightVentricle
Therightventricleliesanteriortotheotherheartchambers[35,36,40–43].Posteriorlyandtotheleft,itisrelated totheleftventriclefromwhichitisseparatedbytheinterventricularseptum,whichisverticallyorientedandlies ata45° angletothemedianplaneofthebody.Theright
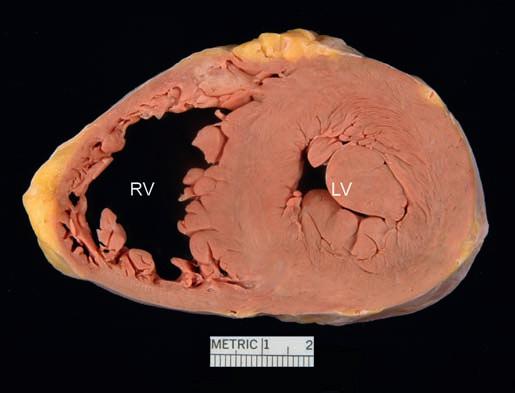
FIGURE1.9 Short-axisviewoftheheart.Thecirculargeometryof theleftventricle(LV)canbeseenaswellasthecrescent-shapedright ventricle(RV).Imaginarylinesdrawntangentialtotheanteriorandinferiorsurfacesoftheshort-axiswillformanacuteangleontherightside (acutemargin)andanobtuseangleontheleftside(obtusemargin).
ventricleiscrescenticinshapeinshort-axis(transverse) section(Figure1.9),withitsfreewallforminganacute angleoftenreferredtoastheacutemarginoftheheart.
Theanatomicrightventriclehasaninflowportion,an apicaltrabeculatedportionandanoutflowportion,the latterofwhichisoftenreferencedastheinfundibulum orconus.Theinfundibulumisseparatedanatomically fromthesinusbyamuscularcrestorarch,thecrista supraventricularis.Thiscrest,whichseparatestricuspid andpulmonaryvalves,mergesmediallywhereitmeets theseptum,withmuscularridgesofvariableprominence calledtheseptalandparietalbandsthatcourseinthose wallsoftherightventricle.Thesiteofinsertionofthe crestbetweenthesetrabeculationsmaybesmoothor markedbyeitheraverticalridgeoragroove.Thepapillarymuscleoftheconusarisesfromtheseptalwalljust proximaltothecrista;itisanimportantsurgicallandmarkfortheconductionsystem[44,45].
Thejunctionoftheinflowtractwiththeinfundibulum isdefinedanteriorlybytheupperedgeofanothersmooth archofmuscleformedbythejunctionoftheseptal band,themoderatorband,andtheanteriorpapillary muscle.Theapexofthepapillarymuscleoftenpoints towardthecommissurebetweentheanteriorandposteriortricuspidvalveleaflets.Themoderatorbandisnot alwaysasdistinctinhumanheartsasinthoseofanimals. Theentireluminalsurfaceoftherightventricle,withthe exceptionoftheseptalandparietalbandsandtheposteriorwalloftheinfundibulumabovethecrest(conus muscle),iscoarselytrabeculatedand,onsection,the trabeculationsformtheinnertwo-thirdsorthree-fourths oftheventricularwall.Aberrantventricularbands,usuallymuscularratherthanfibrotic,arecommoninthe
distalpartoftherightventricleandmaybecongenital oracquired[46].Theconusmuscleseparatesthepulmonaryvalveringfromtheaorticvalveringandisresponsibleforthehigherpositionbyapproximately1.5cmof theformerstructure(Figure1.7).Withinthismuscleis avariablefibrousattachmentbetweentheringsofthe twosemilunarvalves;theconusligament.
Ventricularseptaldefectsorthesitesofpatchrepair maybeseenproximalto,or,rarely,distaltothecrest. Iftherearedefectsbetweentheinflowportionsofthe ventricles,theywillopenamongthetrabeculationson theinterventricularseptum[42].Suchdefectsmaybe multiple,small,andtortuous.Smallonesoftenclose spontaneously,beingobliteratedeitherbyadherenttricuspidleaflettissueorbyendocardialproliferationabout theiredgesandsometimessmallaneurysmsresult.
PulmonaryValve
Thepulmonaryvalveliesbetweentheinfundibulum andthepulmonaryarteryandisattachedtothepulmonaryannulus,whichpointsposteriorly,superiorly,and totheleft(pointingtowardstheleftshoulder) [33,36,47,48].Itsringcircumferenceis5.7-7.4cmin womenand6.0-7.5cminmen[49].Thepulmonaryinfundibulumwindsacrosstheanterioraspectoftheaortic root,withtheannulusapproximately1.5cmhigherthan theaorticannulus.Thethreecuspsarenamedtheanterior,theright(closesttotherightaorticcusp),andtheleft (closesttotheleftaorticcusp).
Boththeaorticandpulmonarysemilunarvalvesconsistofanannulus,cusps,andcommissures.Semilunar valveslacktendinouscordsandpapillarymuscles;hence theiropeningandclosingareapassivefunctionofhemodynamics.Theannuliofthesemilunarvalvesareshaped likeatriradiatecrown,withthethreepointsrepresenting thethreecommissureswhereadjacentcuspsmeet.
Thethreepulmonarycuspsarehalf-moon(semilunar) shapedstructuresmadeoffibroelastictissue.Thedistal edgeisreferredtoasthefreeedge,beneathwhichlies abiscallopedridge,theclosingedgeormargin,along theventricularaspectofthecusp.Afibrousnodule, namedforbothArantiusandMorgagni,islocatedcentrallyonthefreeedgeofeachcusp.Extendingawayfrom thenodule,oneitherside,isacrescent-shapedarea, referredtoasthelunula,whichrepresenttheclosingsurfacesofeachcusp.
LeftAtrium
Theleftatrium,withawall0.3cminaveragethickness,liesinamidline-posteriorpositionimmediately anteriortotheloweresophagus[23,50].Thedescending thoracicaortaliesimmediatelytotheleftandthebifurcatedpulmonaryarteryandleftbronchus,superiorly.
Aswiththerightatrium,theleftatriumcanbedivided intoitsseptalandfreewalls.Theleftsideoftheatrial
septumcontainsthevalveofthefossaovalis,theremnant ofseptumprimum.Mostofthefreewallconsistsofa dome-shaped,smooth-walledportionthatreceivesthe fourpulmonaryveins.Likethesinusvenosusoftheright atrium,thissmooth-walledportionoftheleftatriumisof venousorigin(arisingfromthecommonpulmonaryvein, embryologically).Anteriorlyisthebaseoftheleftatrial appendage.
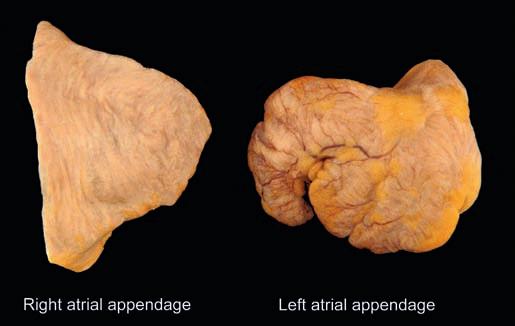
Unlikethepyramidalrightatrialappendage (Figure1.10),theleftatrialappendagehasamorevariablemorphologythathasbeentypedintofourmajor categories:cauliflower,cactus,windsock,andchicken wing.Ofnote,thelatteristhoughttobesomewhatprotectiveofthromboembolicevents[21].Theatrialappendageislinedbypectinatemuscleslikethoseintheright atrialappendage,butunliketherightatrium,thosein theleftarefine,radiallyarranged,anddonotexistoutsideoftheappendage.TheremaybetinyostiaofThebesianveinsintheleftatriumasthereareintheright;the largest,theostiaofLannelongue,arecentralinthewall. Theendocardialliningoftheleftatriumisthickerand moreopaquethanthatoftherightatrium,inkeeping withthehigherpressurewithintheleftsideoftheheart.
MitralValve
Themitralvalveisatwo-leafletvalvewithasaddleshapedannulusanditsvalvularplanefacinganteriorly, inferiorly,andtotheleft(Figure1.11)[37,51–53].The valve'snormalannularcircumferenceisbetween8.2 and9.1cminwomenand9.2and9.9cminmen[49]. Thetwoleaflets,anteriorandposterior,areattached aroundtheannulus,meetingatthecommissures.
Theanteriormitralleafletisinfibrouscontinuitywith theaorticvalveproximaltoitsposterior(noncoronary) andleftaorticcusps(Figure1.12)[54].Althoughtheentire annularcircumferenceconnectstotheatriumbecauseof
FIGURE1.10 Externalanatomyoftheatrialappendages.Theright atrialappendageispyramidalwithabroadbase.Theleftatrialappendagehasamorevariablemorphology,butisoftenvermiformorfingerlikeinmorphologywithamorenarrowbase.
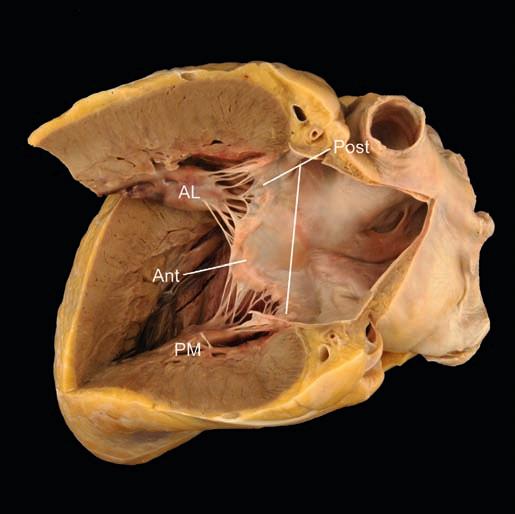
FIGURE1.11 Leftventricularinflowtract.Openedalongtheinflow tract,themitralvalvecanbeseen.Thesail-likeanteriorleaflet(Ant)as wellasthenarrow,scallopedposteriorleaflet(Post).Theanterolateral (AL)andposteromedial(PM)papillarymusclesarepositionedbeneath thetwomitralvalvecommissures.
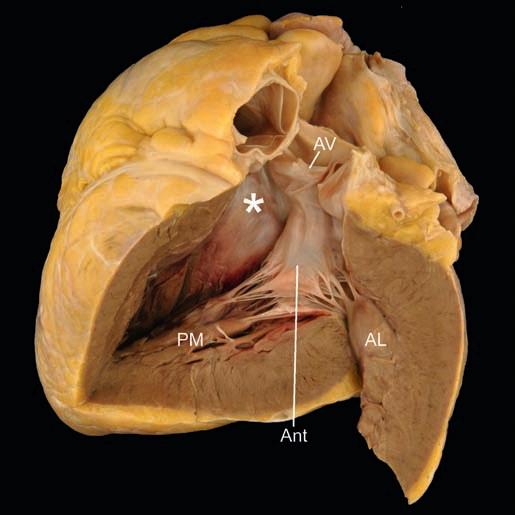
FIGURE1.12 Leftventricularoutflowtract.Openedalongtheoutflowtract,thevariousmorphologicfeaturesthatallowdiscrimination fromtherightventriclecanbeidentified.Theanteriormitralvalveleaflet(Ant)isinfibrouscontinuitywiththeaorticvalve(AV)andwiththe ventricularseptumformsamusculomembranousoutflowtract(asterisk).Theposteromedial(PM)andanterolateral(AL)papillarymuscles canalsobeidentified.
thisfibrouscontinuity,onlyaC-shapedportionattachesto theunderlyingleftventricularfreewall.Theanterior mitralleafletformsacurtainthat,liketheanteriortricuspidleaflet,separatestheinflowandoutflowportions ofitsrespectiveventricle.Theanteriorleafletislong(average3cm)andtriangular,oralmostsail-like,havingan averagewidthof3.3cmatitsbase.Aridgeonitsatrial aspect,0.8-1.0cmfromthefreeedge,definesthelineof valveclosure.Theroughzoneofcordalattachmenton theventricularsurfaceliesbetweenthelineofclosure andthefreeedge.
Theposteriormitralleafletattachestotheparietalpart ofthemitralannulus.Althoughmoreshallowthanthe anteriorleaflet,itoccupiesapproximatelytwo-thirdsof themitralannularcircumference[55].Itisdividedinto scallops,usuallythree:P1,P2,andP3.Theposteriorleaflethasanaveragewidthof4.8cm,andthelongestscallop,usuallythemiddleone,hasanaveragelengthof 1.3cm.Unliketheanteriorleaflet,theposteriorleaflet hasabasalzoneofcordattachmentthatisseparated fromtheroughzonenearthefreeedgebyanarrowclear zone.Thelineofvalveclosure,locatedontheatrial surfaceoftheleaflet,liesapproximately0.2cmfrom thefreeedge.
Themitralvalvecordsvaryinnumber,length,and thickness[56].So-calledprimarycordsattachtothefree edgeofthevalveandareresponsibleforleafletcoaptation, whilesecondarycordsattachtotheventricularsurfaceand servetohelpmaintainventriculargeometry[57,58].A large,thickcordcanusuallybeseenarisingfromeachpapillarymuscleandinsertingontheanteriormitralleaflet. Thesespecializedsecondarycordsareoftenreferredto asstrutcords.Commissuralcordsarealsorecognized.
Thetwopapillarymusclesoftheleftventriclearethe anterolateralandposteromedial.Theyareofapproximatelyequalsizeandareoftendoublethroughoutor bifidattheirtips,theposteriormuscleshowingsubdivisionintotwoormorecolumnsmoreoftenthantheanteriormuscle[52,59].Thepapillarymuscleshavebroad basesintheapicaltrabecularmuscle,andtheirtipsgive attachmenttocordsthattethertheadjacenthalvesofeach mitralleaflet.Thecordsfromtheanteriorpapillarymuscleattachtotheanteriorhalvesofeachleaflet.
Leftventricularpseudotendons(alsotermedfalse cords)arisefromapapillarymuscleandinsertontoeither theseptumortheoppositepapillarymuscle.Theseventricularbandsmaybeseeninupwardsof50%ofsubjects [60,61].Theirlackofattachmenttovalveshelpstodistinguishthemfromcongenitalbands(likethatseeninstraddlingvalvesassociatedwithatrioventricularcanal defects)[46].
LeftVentricle
Theleftventricleformstheposteriorandleftlateral surfacesoftheheart[35,41].Itiscircularinshort-axis
crosssection,butsomewhattriangularwhenviewed alongthelongaxis.Itsshapeapproximatesthatofatruncatedellipsoid.Trabeculationsarepresentintheleftventricularmyocardium,butarefinerandmorenumerous thanintherightventricle.Theymakeuplessthanthe innerone-fourthofthewall;theouterthree-fourthsis composedofcompactmuscle,spirallyarranged,from apextobase.
Liketherightventricle,theleftventriclehasthreedistinctregions:aninflowportion,apicalportion,andan outflowportion.Bloodflowingthroughtheleftventricle changesdirectionbynearly180° inpassingthefreeedge oftheanteriormitralleaflet.Theinflowportioncontains twopapillarymuscles,asdescribedpreviously;inacontractedheart,theyabutoneachotherandtheinterventricularseptumtovirtuallyobliteratetheventricularcavity. Theapicalportioncontainstrabeculationsthatareboth finerandmorenumerousthantheapicaltrabeculations oftherightventricle.Theoutflowportionhasasmooth septalwallformedbytheupperthirdoftheinterventricularseptumanteriorlyandtotheright,andbytheventricularsurfaceoftheanteriormitralleafletposteriorly andtotheleft(Figure1.12).Thesmoothmuscularinterventricularseptumbulgessomewhatintotheleftventricularoutflowtractandmaybecomemoreprominentwith increasingage,producinga “sigmoid” septum(see Chapter2)[39,41,62].
Thetriangularmembranousseptumliesproximalto andbetweentheposteriorandrightaorticvalvecusps andcanbetransilluminated.Aventricularseptaldefect mayoccurinthemembranousseptum,butcommonly involvesthemuscularseptumimmediatelyproximal andanteriortothisregion.Smallmuscularventricular septaldefectsoftenhealspontaneouslyandmaybe markedbygray-whiteendocardialdimplesorsmallseptalaneurysms.
AorticValve
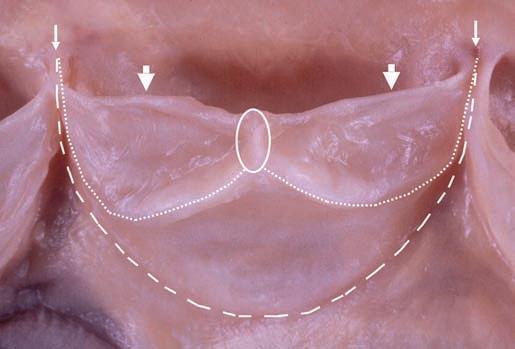
Theaorticvalveliesbetweentheleftventricularoutflowtractandtheaorta[33,36,48,63–68].Itsnormalannularcircumferenceis5.7-7.9cminwomenand6.0-8.5cm inmen[49].Thevalveannulusisamidlinestructure andoccupiesacentralpositioninthecardiacbase.The planeofthevalvepointsposteriorly,superiorly,andto theright(directedtowardtherightshoulder) (Figure1.4).Theannulusandcuspsareverysimilarto thoseofthepulmonaryvalve,aspreviouslydescribed. Thehigher,left-sidedpressurestypicallymaketheclosingedgeandmidlinecuspnodule(noduleofArantius) moreevidentthaninthatofthepulmonaryvalve (Figure1.13).Lamblexcrescencesarefrequentlyfound onthenodulesandalongthelineofvalveclosure (Figure 1.14)(see Chapte r 2).
Theposteriornoncoronarycuspisposteriorinposition,andtherightandleftcoronarycuspsareanterior
FIGURE1.13 Aorticvalvecusp.Thesemilunarvalvecommissures (smallarrows)arethepointsthatadjacentcuspsmeetalongtheannulus (largedashedline).Thefreeedge(largearrows)representthedistalmostportionofthecuspandthethickenedbiscallopedridge(smalldottedline)isthelineofclosurewhereadjacentcuspscomeintocoaptation. Theclosingedgemeetsatacentralnodularthickening,thenoduleof Arantius(circle).
FIGURE1.14 Lamblexcrescences.Thesefinger-likeprojections exhibitsimpleornobranchingandariseexclusivelyalongtheclosing surface(distaltothelineofclosure)ofthevalve.
(Figure1.4).Thevalvecuspsaresimilarinsize,though areusuallynotequal.Insomeinstances,thismayhasten calcification[65].Theaorticandmitralvalveringsare fused(intervalvularfibrosa)overthelengthofattachmentoftheanteriormitralleaflet,whichhasavariable degreeoffibrouscontinuitywiththeadjacenthalvesof theposteriorandleftaorticvalvecusps(Figure1.15)[54].
Thesinus(ofValsalva)ofeachaorticcuspisthepocket enclosedbythecuspattachmentproximallyandaridge encirclingtheaorticliningatthelevelofthecommissures. Animaginarylineconnectingthetipsofthecommissures (prongsofthetriradiateannulus)formsthesinotubular junctionwheretheaorticsinusbecomesthetubular portionoftheascendingaorta.Thesinusis1.5times
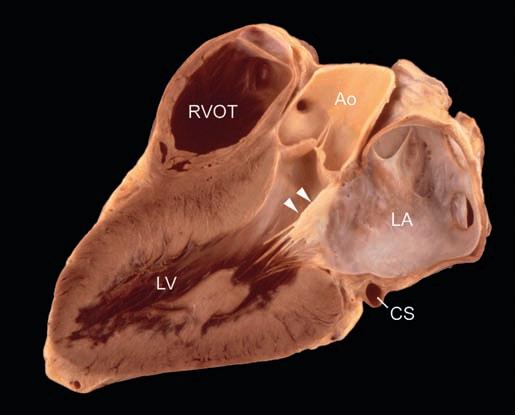
FIGURE1.15 Leftventricularlong-axisviewoftheheart (3-chamberview).Theplanethatbisectsthemitralandaorticvalve revealsthecontributionoftheanteriormitralvalveleaflettotheleftventricularoutflowtract(arrowheads).Theplanespassagethroughright ventricularoutflowtract(RVOT)allowsthreechamberstobevisualized thatincludetheleftatrium(LA)andleftventricle(LV).CS,coronary sinus;Ao,aorta.
widerthantheproximaltubularascendingaorta,butthis isbetterappreciatedinangiogramstakenduringlifethan ingrossspecimens.
Thecoronaryarterialostiamaybevariableinnumber, position,andsize.Themeandiameteroftherightvessel is0.32cm,andoftheleft,0.40cm.Theyareusuallysingle,centrallylocatedwithinthewalloftheaorticsinus, andapproximatelyequalinsize.Ifunequal,theleftis moreoftenlarger,buttherightisoftendouble,with oneostiumrepresentingtheconusarteryostium.
Normalvariationsofcoronaryostiaaredistinguished fromanomalies(e.g.,boththeleftanteriordescending arteryandthecircumflexcoronaryarterymayarisefrom thesamecoronarysinus)[69].Nevertheless,asolitary coronaryostium,stenosisofanostium,acuteangulation orarterialtakeoff,oranintussusceptionofanostiummay beassociatedwithsuddendeath(see Chapter10)[70,71].
ConductionSystem
Thecardiacconductionsystemconsistsofthesinus node,internodalpathways,andatrioventricularconductiontissues.Itsfunctionisinfluencedbytheinnervation oftheheart(describedbelow).Thesinusandatrioventricularnodesarebothrightatrialstructures.Itisimportant tonotethatallstructuresoftheconductionsystemare specializedcardiacmyocytes(notnerves)whoseprimary functionisimpulsepropagationratherthancontraction andrelaxation.
Thesinusnodeislocatedsubepicardially,alongthe superioraspectofthesulcusterminalis,nearthe
confluenceofthesuperiorvenacava,sinusvenosus,and muscularrightatrialfreewall.Theselattertwostructures arethereasonthesinusnodeissometimesreferredtoas thesinoatrialnode.Itisellipticalinshapewiththesinoatrialnodalartery,whichisoftengrosslyidentifiable, runningcentrallythroughthenodaltissue.
Theinternodalpathwaysserveaspreferentialtractsby whichimpulsepropagationistransmittedfromthe sinusnodetotheatrioventricularnode.Theyhavebeen describedintheatrialseptum,rightatrialfreewall, andthecristaterminalis.Whileelectrophysiologically identifiable,thesestructureshavenotbeendefinitively teasedoutmorphologically,exceptfortheBachman bundlebetweentheatria[72].
Theatrioventricularnodeislocatedsubendocardially (ratherthansubepicardially,likethesinusnode)within thetriangleofKoch.ThetriangleofKochistheanatomic regionborderedbythetricuspidannulus(oftheseptal tricuspidleaflet),theostiumofthecoronarysinus,and thetendonofTodaro(describedabove).Theapexof thetriangleisadjacenttothecentralfibrousbody.The atrioventricularnodalarterydoesnotnecessarilytravel intranodally,likethatofthesinusnodalartery.
Theatrioventricularbundle(bundleofHis)extends fromthenode,travelingthroughthecentralfibrous body,tothebasalventricularseptum,adjacenttothe membranousseptum.Itthensplitsintobothitsright andleftbundlebranches.Therightbundlebranchisa cord-likestructurethattravelssubendocardiallytothe moderatorbandandthenouttothefreewalloftheright ventricle.Thebroaderleftbundlebranchalsotravelssubendocardiallytowardtheleftventricularapex,whilefanningoutintofasciclesofPurkinjecells.
CardiacInnervation
Thenervesupplytotheheartisautonomic,including bothsympatheticandparasympatheticinnervationvia bothefferentandafferentfibers[73,74].Itisconveyedto thecardiacplexusinbranchesfromthevagusandphrenic nervesandalsofromthecervicalandthoraciccardiac nerves.Thecardiacplexusisagroupofnerveganglia locatedbetweenthearchoftheaortaandthebifurcation ofthetrachea.Thelargestganglion,theganglionofWrisberg,liesbelowthearchoftheaorta.Nervegangliaareseen frequentlyinmicroscopicsectionsofthesubendocardial muscleoftherightatrium,particularlyintheinteratrial septumandintheepicardiumneartherootsofthegreat vessels.Bothsympatheticandparasympatheticnerves innervatethenodes,myocardium,andcoronaryarteries.
HeartWeightandMeasurements
Theopenedheart,emptiedofpostmortemclotand vesselstrimmedtowithin1cmoftheheart,shouldbe
weighed,measurementsofvalveringsandventricular wallthicknessesshouldbemade,andtheresultscomparedwithacceptednormograms[49,75].Inindividual cases,normalityofheartweightshouldbejudgedbyconsiderationofbodysize,weight,andsex.Generically, thefollowingusefulguidelinesfor freshheartweight maybeused:
• Adultmaleheartweight:0.45%ofbodyweight,average 300g,range250-350g.
• Adultfemaleheartweight:0.40%ofbodyweight, average250g,range200-300g.
Heartweighttendstoberelatedtobodyweight [49,76]. Table1.2 predictsanormal(formalin-fixed)heart weightfromthebodyweightofadultmenandwomen; itisbasedonalargestudygroup[49].Bothincreasesand decreases(ofapproximately6%)havebeennotedfollowingformalinfixation[75,77].Heartweightisalsorelated tobodylength,butlesssothantobodyweight[49]. Althoughheartweightissaidtoincreasewithage,this ismorelikelytrueinwomenthaninmen,anditdecreases intheelderlyofbothsexes[49].Adultheartweightistypicallyreachedbetweentheagesof17and20years.Heart weightinchildrenisrelatedtoageandbodysize[78,79]. Table1.3 showsnormal(formalin-fixed)heartweightspredictedfrombodyweightsofmaleandfemalesubjectsup to19yearsofage[78].
Althoughtotalheartweighthasawidenormalrange, itisthemostpracticalandreproducibleguidetomyocardialhypertrophywhencombinedwithavisualassessmentofheartchambermusculature.Itshouldbe rememberedthattotalheartweightbestreflectsleft ratherthanrightventricularhypertrophy.Visualassessmentisparticularlyneededtojudgethepresenceofright ventricularhypertrophy.Hypertrophiedmuscleproducesbrawnyandprominenttrabeculations.Insomesituations(e.g.,pulmonaryarterialhypertension),itmaybe usefultoweightheventriclesindependentlyforamore detailedassessmentofthehypertrophy[80].Thispartitioningmethodinvolvesstrippingtheepicardialfat andcoronaryvasculaturefromthespecimen,removing theatriaandgreatarteries,andseparationoftheright ventricularfreewallfromtheheart(leavingtheseptum withtheleftventricularfreewall).Whenthetotalweight oftheventriclesis >250g,theratioofleftventricleto rightventricleis <2.1incasesofrightventricularhypertrophyand >3.3incasesofleftventricularhypertrophy [80,81].Becauseitcanbedifficulttomaintainorientation afterthespecimenhasbeenpartitioned,ithasbeen recommendedthatpartitioningoftheventriclesoccur afterdissectionanddescriptionusingtheshort-axis methoddescribedabove[82].
Inassessmentofcardiachypertrophy,anincrease (abovethemeanforageandbodysize)between26% and50%canbeconsideredmild,51%and100%as
P,predictednormalheartweight;L95,lower0.95%confidencelimit;U95,upper95%confidencelimit. FromRef.[49],p.137
moderate,and >100%asmarked.Thepresenceofcardiomegalytypicallycorrelateswitheithermoderateor markedhypertrophy.Itmaybeparticularlydifficultto gaugedegreeofhypertrophyinsurgicalexplants(where theatriahavebeenretainedinthepatient)orheartswith extensivepericardialadhesionsorinstalledhardware.In thesecases,theprosectorshouldusetheirjudgmentto bestadjusttheexpectedweightaccordingly.
Documentationofthicknessesofthecompactmyocardium(wallthickness)isalsorequisite.Thesemeasurementsaretypicallytakenatthemidventricular(papillary muscle)levelandshouldincludetheleftventricularfree wall,ventricularseptum,andrightventricle.Careshould betakennottoincludetrabeculationsorthepapillarymusclesinthemeasurements.Generally,theleftventricle inadultheartsis0.8-1.2cminthicknessandtheright
ventricleis0.3-0.5cminthickness.Theratioofthethickness oftheventricularseptumtothatoftheleftventricularfree wall(VS:LV)shouldbe <1.3.Aratioofgreaterthan1.3is consideredasymmetricseptalhypertrophyandmayraise concernforhypertrophiccardiomyopathy.
Chambersizesshouldalsobemeasuredanddocumentedatthemidventricularlevel.Whenviewedinshort axis,theleftventricleiscircular,andthechambersizeis generally <3.0cm(excludingtrabeculationsandpapillarymuscles).Thecrescent-shapedrightventricleisgenerally <3.5cmintheanterior-posteriordimensionand <5cminthelateraldimension.Theventricularwalls mayartifactuallythicken(emulatingsystole)inthepostmortemstate,owingtotheeffectofrigor(whichoccursin atime-andenvironment-dependentmanner)[75,83,84]. Similarly,decompositioncancauseartifactualchamber