Activate the eBook version of this title at no additional charge.
Elsevier eBooks for Practicing Clinicians gives you the power to browse and search content, view enhanced images, highlight and take notes—both online and offline.
Unlock your eBook today.
1. Visit expertconsult.inkling.com/redeem
2. Scratch box below to reveal your code
3. Type code into “Enter Code” box
4. Click “Redeem”
5. Log in or Sign up
6. Go to “My Library” It’s that easy!
Place Peel Off Sticker Here
For technical assistance: email expertconsult.help@elsevier.com call 1-800-401-9962 (inside the US) call +1-314-447-8300 (outside the US)
Use of the current edition of the electronic version of this book (eBook) is subject to the terms of the nontransferable, limited license granted on expertconsult.inkling.com. Access to the eBook is limited to the first individual who redeems the PIN, located on the inside cover of this book, at expertconsult. inkling.com and may not be transferred to another party by resale, lending, or other means.
Campbell-Walsh-Wein HANDBOOK of
urology
urology Campbell-Walsh-Wein HANDBOOK of
Alan W. Partin, MD, PhD
Professor and Director
Department of Urology
The Johns Hopkins School of Medicine
Baltimore, Maryland
Louis R. Kavoussi, MD, MBA
Professor and Chair
Department of Urology
Zucker School of Medicine at Hofstra/Northwell Hempstead, New York; Chairman of Urology
The Arthur Smith Institute for Urology Lake Success, New York
Associate Editors
Christopher S. Cooper, MD, FAAP, FACS
Professor and Vice Chairman of Urology
Department of Urology
University of Iowa; Senior Associate Dean of Medical Education
University of Iowa Carver College of Medicine
Iowa City, Iowa
Kirsten L. Greene, MD, MAS, FACS
Professor and Chair
Department of Urology
University of Virginia Charlottesville, Virginia
Craig A. Peters, MD
Chief, Pediatric Urology
Children’s Health Texas; Professor of Urology
UT Southwestern Dallas, Texas
Roger R. Dmochowski, MD, MMHC, FACS
Professor, Urologic Surgery, Surgery and Gynecology
Vice Chair for Faculty Affairs and Professionalism
Section of Surgical Sciences
Associate Surgeon-in-Chief
Vanderbilt University Medical Center Nashville, Tennessee
Alexander Gomelsky, MD
B.E. Trichel Professor and Chairman
Department of Urology
Louisiana State University Health Shreveport Shreveport, Louisiana
Robert M. Sweet, MD, FACS
Professor, Department of Urology and Surgery (Joint)
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www. elsevier.com/permissions
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notice
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds or experiments described herein. Because of rapid advances in the medical sciences, in particular, independent verification of diagnoses and drug dosages should be made. To the fullest extent of the law, no responsibility is assumed by Elsevier, authors, editors or contributors for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Library of Congress Control Number: 2021948424
Senior Content Strategist: Belinda Kuhn
Content Development Specialist: Denise Roslonski/Laurie Gower
Publishing Services Manager: Deepthi Unni
Project Manager: Beula Christopher
Design Direction: Amy Buxton
Printed in United States of America
Last digit is the print number: 9 8 7 6 5 4 3 2 1
Preface
“Learning
is a treasure that will follow its owner everywhere.”
Chinese proverb
Access to all forms of information has become increasingly easy and exceedingly rapid, whereas access to knowledge does not always follow. Our age of information overload has become a blessing and a challenge that we must manage with care. As we edited the Campbell’s Urology textbook over the past decade, it became evident that our colleagues’ demand for practical knowledge had evolved, and with this handbook, we have attempted to address this evolving need. Using the wealth of experience and knowledge of the authors of the Campbell’s textbook distilled into a clinically oriented and succinct presentation of the key elements of urology, we have attempted to meet the needs of the clinical urologic student, resident, fellow, or early career provider in an easy access format. We also recognize the need for information review in an efficient format to assist in preparation for exams and other required routine knowledge assessments. This book attempts to provide the basic information and cognitive framework needed by urology providers to both care for patients and assist in examination preparation. We hope the knowledge obtained from using this text will translate into improved care and health for all urologic patients.
From the Editors
Contributors
Gregory M. Amend, MD
Fellow
Department of Urology
University of California San Francisco
San Francisco, California
James Anaissie, MD, BSE
Resident
Scott Department of Urology
Baylor College of Medicine
Houston, Texas
Angela M. Arlen, MD
Associate Professor Department of Urology
Yale University School of Medicine
New Haven, Connecticut
Ramasamy Bakthavatsalam, MS, FRCS (G)
Professor Department of Surgery and Urology
University of Washington Seattle, Washington
Michael S. Borofsky, MD
Assistant Professor Department of Urology
University of Minnesota
Minneapolis, Minnesota
Robert E. Brannigan, MD
Professor, Director of Andrology Fellowship
Department of Urology
Northwestern University, Feinberg School of Medicine
Chicago, Illinois
Benjamin N. Breyer, MD, MAS
Professor of Urology and Epidemiology and Biostatistics
Department of Urology
University of California San Francisco
San Francisco, California
Michael C. Chen, MD
Resident Physician
Department of Urology
Kaiser Permanente Southern California
Los Angeles Medical Center
Los Angeles, California
Caitlin T. Coco, MD Fellow
Children’s Health Texas Department of Urology
University of Texas Southwestern
Dallas, Texas
Christopher S. Cooper, MD, FAAP, FACS
Professor and Vice Chairman of Urology
Department of Urology
University of Iowa;
Senior Associate Dean of Medical Education
University of Iowa Carver College of Medicine
Iowa City, Iowa
Nicholas G. Cost, MD
Associate Professor Department of Surgery, Division of Urology University of Colorado School of Medicine Aurora, Colorado
Jessica C. Dai, MD Assistant Instructor UT Southwestern Medical Center Dallas, Texas
Atreya Dash, MD Associate Professor Department of Urology University of Washington Seattle, Washington
Richard J. Fantus, MD Andrology Fellow Department of Urology Northwestern University, Feinberg School of Medicine Chicago, Illinois
Alexander Gomelsky, MD
B.E. Trichel Professor and Chairman Department of Urology Louisiana State University Health Shreveport Shreveport, Louisiana
Kirsten L. Greene, MD, MAS, FACS Professor and Chair Department of Urology University of Virginia Charlottesville, Virginia
Sumit Isharwal, MD Assistant Professor Department of Urology University of Virginia Charlottesville, Virginia
Emily F. Kelly, MD Resident Department of Urology Louisiana State University Health Shreveport Shreveport, Louisiana
Mohit Khera, MD, MBA, MPH Professor of Urology Scott Department of Urology
Baylor College of Medicine Houston, Texas
Aaron Krug, MD Resident Physician Department of Urology Kaiser Permanente Southern California
Los Angeles Medical Center Los Angeles, California
David A. Leavitt, MD Assistant Professor Department of Urology Vattikuti Urology Institute, Henry Ford Health System Detroit, Michigan
Gina M. Lockwood, MD, MS, FAAP Assistant Professor Department of Urology University of Iowa Iowa City, Iowa
Alan W. Partin, MD, PhD
Professor and Director
Department of Urology
The Johns Hopkins School of Medicine
Baltimore, Maryland
Craig A. Peters, MD
Chief, Pediatric Urology
Children’s Health Texas; Professor of Urology
UT Southwestern Dallas, Texas
Lauren H. Poniatowski, MD, MS
Urology Resident
Department of Urology
University of Washington
Seattle, Washington
Polina Reyblat, MD
Chief of Service
Department of Urology
Kaiser Permanente Southern California
Los Angeles Medical Center
Los Angeles, California
W. Stuart Reynolds, MD, MPH
Associate Professor
Department of Urology
Vanderbilt University Medical Center
Nashville, Tennessee
Elizabeth Rourke, DO, MPH
Female Pelvic Medicine and Reconstructive Surgery Fellow
Department of Urology
Vanderbilt University Medical Center
Nashville, Tennessee
Bogdana Schmidt, MD, MPH
Assistant Professor Division of Urology University of Utah
Salt Lake City, Utah
Bradley F. Schwartz, DO, FACS
Professor and Chairman
Department of Urology
Southern Illinois University School of Medicine
Springfield, Illinois
Elisabeth Sebesta, MD
Female Pelvic Medicine and Reconstructive Surgery Fellow
Department of Urology
Vanderbilt University Medical Center
Nashville, Tennessee
Douglas W. Storm, MD
Associate Professor Department of Urology
University of Iowa Hospitals and Clinics
Iowa City, Iowa
Peter Sunaryo, MD Fellow
Department of Urology
University of Washington
Seattle, Washington
Robert M. Sweet, MD, FACS
Professor
Department of Urology and Surgery (Joint)
Adjunct Professor
Bioengineering Chief Division of Healthcare Simulation Science
University of Washington Seattle, Washington
Matthew D. Timberlake, MD
Assistant Professor Urology and Pediatrics
Texas Tech University Health Sciences Center Lubbock, Texas
Ernest Tong, MD Resident
Department of Urology
Louisiana State University Health Shreveport Shreveport, Louisiana
Samuel Washington III, MD
Assistant Professor Department of Urology University of California, San Francisco
San Francisco, California
Dana A. Weiss, MD
Assistant Professor Department of Urology University of Pennsylvania; Attending Physician Department of Urology
The Children’s Hospital of Philadelphia Philadelphia, Pennsylvania
Jonathan T. Wingate, MD Assistant Professor Uniformed Services University of the Health Sciences Madigan Army Medical Center Tacoma, Washington
28 Evaluation and Management of Localized Renal Tumors
ATREYA DASH AND ROBERT M. SWEET
29 Evaluation and Management of Advanced Renal Cell Carcinoma and Upper Tract Urothelial Tumors 748
ATREYA DASH AND ROBERT M. SWEET 30 Pathophysiology, Evaluation, and Management of Adrenal Disorders 769
BRADLEY F. SCHWARTZ AND ROBERT M. SWEET
31 Complications of Urologic Surgery
JESSICA C. DAI, PETER SUNARYO, CRAIG A. PETERS, AND ROBERT M. SWEET
1
Evaluation of the Urologic Patient: History, Physical Examination, Laboratory Tests, Imaging, and Hematuria Workup
LAUREN H. PONIATOWSKI, JONATHAN T. WINGATE AND ROBERT M. SWEET
CONTRIBUTORS OF CAMPBELL-WALSH-WEIN,
12TH EDITION
Sammy E. Elsamra, Erik P. Castle, Christopher E. Wolter, Michael E. Woods, Jay T. Bishoff, Ardeshir R. Rastinehad, Bruce R. Gilbert, Pat F. Fulgham, Michael A. Gorin, and Steven P. Rowe
PATIENT HISTORY AND PHYSICAL EXAMINATION
A proper history and physical examination is essential in evaluating the urologic patient. Completing this assessment reliably and comprehensibly allows for gathering information essential for diagnosis, counseling, treatment, and next steps.
CLINIC VISIT SET-UP
The clinic visit should be comforting and nonthreatening to the patient. The patient room or telehealth visit set-up should include ideal provider-patient positioning and ability to make proper eye contact.
PATIENT HISTORY
Chief Complaint (CC)
The CC is the reason why a patient is seeking urologic care and is the focus of the visit.
History of Present Illness (HPI)
The HPI covers multiple factors related to the CC with the purpose of developing a differential diagnosis.
Constitutional Symptoms. These symptoms include fever, chills, night sweats, anorexia, weight loss, fatigue, and/or lethargy. Pain. Elicit pain location, radiation, palliative factors, provocative factors, severity (1-10 scale), and timing (including onset and change over time).
• Renal pain (flank pain) – Renal pain is located at the ipsilateral costovertebral angle (CVA) lateral to the spine and inferior to the 12th rib and often radiates toward the abdomen or scrotum/ labia.
• Ureteral pain – This is often due to ureteral obstruction and may be present in the ipsilateral abdominal lower quadrant. The pain is often acute in onset and intermittent and may be referred to the scrotum/penis.
• Bladder pain – This type of pain may be due to inflammation (cystitis) or bladder distension (urinary retention). Suprapubic in location with possible improvement after voiding.
• Prostatic pain – This is a deep pelvic pain that may be confused with rectal pain. There are often associated irritative voiding symptoms (urinary frequency, urgency, dysuria).
• Penile pain – Penile pain has a variable presentation with wide differential, including paraphimosis, penile lesions, referred pain, Peyronie’s disease, or priapism.
• Scrotal pain – This type of pain may be superficial (skin) or involve the scrotal contents. Testicular torsion is a urologic emergency.
Hematuria. Hematuria is defined as presence of blood in the urine and is divided into categories of gross (visible) versus microscopic (.3 RBC/HPF on microscopic examination) versus pseudohematuria (redness in urine of non-urologic origin). Obtain the presence or absence of associated voiding symptoms, smoking history, chemical exposure history, trauma, urinary tract infections, or recent urologic procedures. Please refer Hematuria section below for more details.
Lower Urinary Tract Symptoms (LUTS). LUTS may be obstructive or irritative in nature. Obstructive symptoms include urinary frequency, intermittency, incomplete emptying, weak stream,
hesitancy, and straining with voiding. Irritative symptoms include urinary frequency, urgency, dysuria, or nocturia and may be caused by chronic bladder outlet obstruction, overactive bladder, cystitis, prostatitis, bladder stones, or bladder cancer. The International Prostate Symptom Score (IPSS) is the AUA symptom score with the addition of a quality-of-life score and is a useful tool for assessing LUTS (Table 1.1) (see Chapter 21).
Urinary Incontinence
• Stress incontinence – Involuntary passage of urine with activities that increases intra-abdominal pressure including Valsalva, cough, sneeze, laugh, and/or heavy lifting.
• Urge incontinence – Involuntary passage of urine associated with sudden urge to void. This is often associated with overactive bladder, cystitis, neurogenic bladder, or poorly compliant bladder.
• Mixed incontinence – When a patient experiences both stress and urge incontinence.
• Continuous incontinence – Constant leakage of urine independent of urination patterns or intraabdominal pressure. This is often due to congenital cause or urinary fistula.
• Pseudoincontinence – Incontinence-like symptoms due to nonurologic cause such as vaginal discharge or labial fusions causing retention of urine.
• Overflow incontinence – Leakage of urine due to volume of urine exceeding bladder capacity. This is common in bladder outlet obstruction.
• Functional incontinence – Leakage of urine due to patient immobility or inadequate access to facilities. Patients otherwise have normal urologic anatomy/physiology. See Chapter 16.
Erectile Dysfunction (ED). ED is defined as the inability to attain/ maintain penile erection sufficient for satisfactory sexual intercourse. It is important to obtain history related to timing and situational factors of erections. Validated questionnaires for characterizing ED includes the International Index of Erectile Function (IIEF) and the abbreviated IIEF-6 or Sexual Health Index for Men (SHIM). See Chapter 14.
Other Urologic Conditions. Additional topics often covered in a urologic-based HPI include loss of libido, abnormal ejaculation, anorgasmia, hematospermia, pneumaturia, and/or urethral discharge.
Table 1.1 International Prostate Symptom Score
1. Incomplete Emptying
Over the past month, how often have you had a sensation of not emptying your bladder completely after you finished urinating?
2. Frequency
Over the past month, how often have you had to urinate again less than 2 hours after you finished urinating?
3. Intermittency
Over the past month, how often have you found you stopped and started again several times when you urinated?
4. Urgency
Over the past month, how often have you found it difficult to postpone urination?
5. Weak Stream
Over the past month, how often have you had a weak urinary stream?
6. Straining
Over the past month, how often have you had to push or strain to begin urination?
7. Nocturia
Over the past month, how many times did you most typically get up to urinate from the time you went to bed at night until the time you got up in the morning?
SYMPTOM
TOTAL INTERNATIONAL PROSTATE SYMPTOM SCORE
QUALITY OF LIFE DUE TO URINARY SYMPTOMS
If you were to spend the rest of your life with your urinary condition just the way it is now, how would you feel about that?
From Cockett A, Aso Y, Denis L. Prostate symptom score and quality of life assessment. In: Cockett ATK, Khoury S, Aso Y, et al., eds. Proceedings of the Second International Consultation on Benign Prostatic Hyperplasia (BPH); 27-30 June 1993, Paris, Channel Island: Jersey: Scientific Communication International, 1994:553-555.
Past Medical/Surgical History
It is essential to obtain a complete medical and surgical history (including prior genitourinary or abdominal surgeries). Obtain operative reports when applicable.
Performance Status
Determine the functional ability of patient as a benchmark for his or her tolerance for undergoing challenging or invasive treatments. Assess a patient’s ability to perform activities of daily living (ADLs), dressing, eating, toileting, hygiene, preparing meals, shopping, maintaining a house, and interactions with family and community. Grading performance status can be completed using the Eastern Cooperative Oncology Group (ECOG) score or Karnofsky performance status.
Medications
Obtain full medication history including urologic medications and anticoagulants. Also consider medications with urologic side effects (Table 1.2).
Social History
Review where the patient lives, who lives at home with patient, and if there are family/friends in the area. Also obtain occupational history to give insight on socioeconomic status and possible industrial exposures. Review sexual history in a non-accusatory manner such as “Do you partake in sexual relations with men, women, or both? A single partner or multiple?” Obtain drug use history including tobacco, alcohol, illicit drug use. This is important for considering withdrawal or difficulty coping during possible procedures/hospitalizations.
Family History
Ask about urologic conditions/diseases/cancers as well as bleeding disorders, reactions to anesthesia and significant non-urologic conditions/disease/cancers.
Review of Systems
Comprehensive system-based checklist related to other symptoms that may or may not be included in HPI or related to CC.
Table 1.2 Drugs Associated with Urologic Side Effects
UROLOGIC SIDE
EFFECTS
Decreased libido
Erectile dysfunction
CLASS OF
DRUGS
Antihypertensives
Psychotropic drugs
Ejaculatory dysfunction a-Adrenergic antagonists
Psychotropic drugs
SPECIFIC EXAMPLES
Hydrochlorothiazide
Propranolol
Benzodiazepines
Prazosin
Tamsulosin
a-Methyldopa
Phenothiazines
Antidepressants
Priapism
Decreased spermatogenesis
Antipsychotics
Antidepressants
Antihypertensives
Chemotherapeutic agents
Drugs with abuse potential
Drugs affecting endocrine function
Phenothiazines
Trazodone
Hydralazine
Prazosin
Alkylating agents
Marijuana
Alcohol
Nicotine
Antiandrogens
Prostaglandins
Incontinence or impaired voiding
Direct smooth muscle stimulants
Others
Smooth muscle relaxants
Striated muscle relaxants
Urinary retention or obstructive voiding symptoms
Anticholinergic agents or musculotropic relaxants
Calcium channel blockers
Antiparkinsonian drugs
a-Adrenergic agonists
Antihistamines
Histamine
Vasopressin
Furosemide
Valproic acid
Diazepam
Baclofen
Oxybutynin
Diazepam
Flavoxate
Nifedipine
Carbidopa
Levodopa
Pseudoephedrine
Phenylephrine
Loratadine
Diphenhydramine
Table
1.2 Drugs Associated With Urologic Side Effects—cont’d
Note level of pain or distress, nutritional status, appearance and self-care, frailty, mobility. Look for stigmata associated with certain disease states.
Kidneys
The kidneys are located in the retroperitoneum and surrounded by the psoas and oblique muscles, peritoneum, and diaphragm. For adults, place the nonexamining hand posteriorly at the costovertebral angle and palpate the kidney with the examining hand through the anterior abdominal wall (Fig. 1.1). Kidneys are typically difficult to palpate and not visible on examination (unless large mass or very thin patient). Assess pain at kidney via percussion by contacting the patient with the closed hand of the examiner at the CVA. Be gentle; a simple tap should elicit a positive sign if present.
Bladder
To examine the bladder, palpate and percuss starting at level of pubic symphysis and ascend toward umbilicus to determine the level of distension. The bladder is palpable when it distends to level above the pubis (,150 cc). The bladder may be visualized when distended at ,500 cc in thin patients. Additionally, A bimanual exam may be performed to assess mobility of the bladder as well as cancer staging.
Penis
Inspect the skin for hair distribution, lesions, presence/absence of foreskin (in adults, retract foreskin to evaluate glans), and Tanner stage. Evaluate the urethral meatus (location, stenosis, presence of urethral discharge). Palpate for any subcutaneous plaques or curvature. Remember to reduce the foreskin at the end of the examination.
Scrotum and Contents
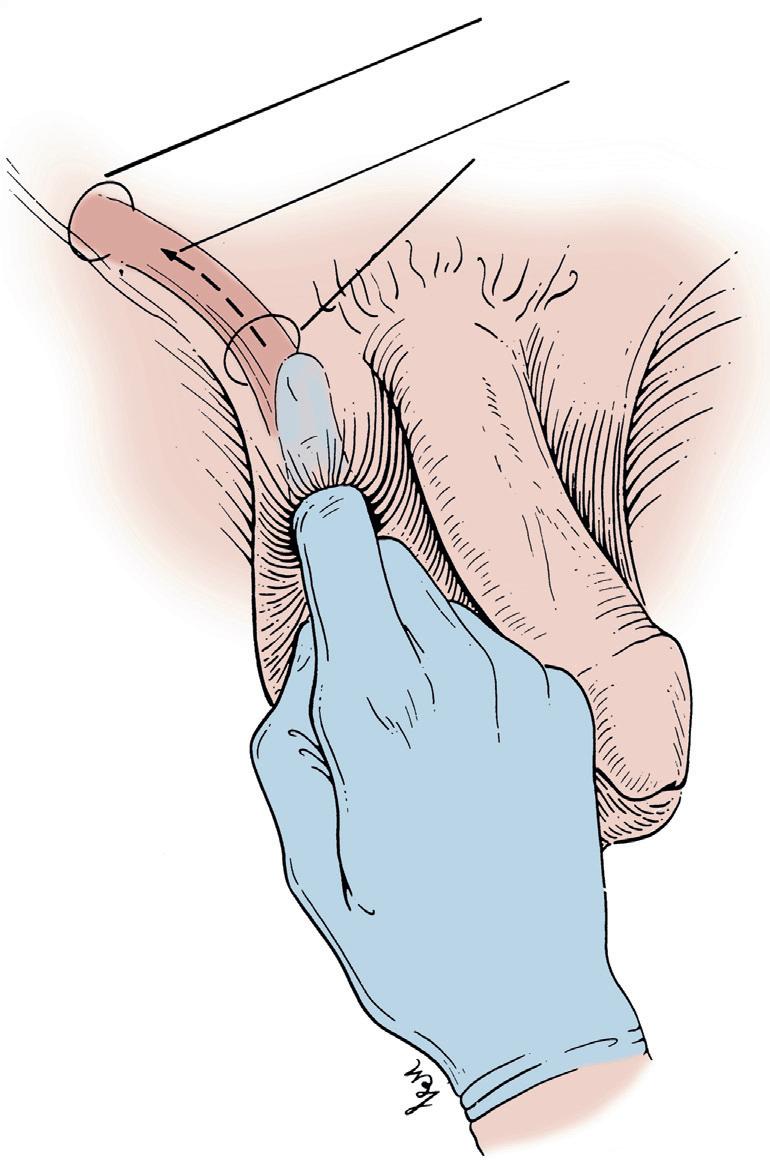
Inspect the scrotal skin for hair distribution, lesions, and infection. Be sure to evaluate the entire scrotum toward the perineum, especially in those with limited mobility or poor self care. Palpate the testicles for size, orientation, pain, or masses. Evaluate for hydrocele, varicocele (patient supine, standing, standing with Valsalva). Palpate the vas deferens. Check for an inguinal hernia by sliding
FIG. 1.1 Bimanual examination of the kidney.
Internal inguinal ring
Internal canal
External inguinal ring
FIG. 1.2 Examination of the inguinal canal. (From Swartz MH. Textbook of physical diagnosis. Philadelphia: Saunders, 1989:376.)
the index finger over testis and invaginating the scrotum up toward external ring (Fig. 1.2).
Digital Rectal Examination (DRE)
The DRE is used to assess prostate size and perform screening for prostate cancer. For positioning, the patient should bend 90 degrees at the waist while supporting hand or elbows on the table. Lateral decubitus position with legs flexed at hips is another alternative. The examiner’s gloved finger with adequate lubrication then is advanced until the prostate is palpable. A normal prostate is smooth and somewhat soft, whereas nodular firmness is concerning and may warrant biopsy. A bimanual examination (DRE with concurrent