https://ebookmass.com/product/bone-2nd-edition-g-peturnielsen/
Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
Diagnostic Pathology: Bone, 3rd Edition Gunnlaugur Petur
Nielsen
https://ebookmass.com/product/diagnostic-pathology-bone-3rd-editiongunnlaugur-petur-nielsen/
ebookmass.com
A New Ecology: Systems Perspective 2nd Edition Soeren Nors
Nielsen
https://ebookmass.com/product/a-new-ecology-systems-perspective-2ndedition-soeren-nors-nielsen/
ebookmass.com
Community Ecology 2nd Edition Gary G. Mittelbach
https://ebookmass.com/product/community-ecology-2nd-edition-gary-gmittelbach/
ebookmass.com
Fortran for Scientists and Engineers 4th Edition Stephen
J. Chapman
https://ebookmass.com/product/fortran-for-scientists-andengineers-4th-edition-stephen-j-chapman/
ebookmass.com
John Loeser: The Man Who Reimagined Pain Jane C. Ballantyne
https://ebookmass.com/product/john-loeser-the-man-who-reimagined-painjane-c-ballantyne/
ebookmass.com
Women Writing the Neo-Victorian Novel: Erotic "Victorians" 1st ed. Edition Kathleen Renk
https://ebookmass.com/product/women-writing-the-neo-victorian-novelerotic-victorians-1st-ed-edition-kathleen-renk/
ebookmass.com
Tempered Illusions Whitney Hill
https://ebookmass.com/product/tempered-illusions-whitney-hill-2/
ebookmass.com
That Night Cyn Balog
https://ebookmass.com/product/that-night-cyn-balog/
ebookmass.com
System Architecture and Complexity Vol. 2: Contribution of Systems of Systems to Systems Thinking Printz
https://ebookmass.com/product/system-architecture-and-complexityvol-2-contribution-of-systems-of-systems-to-systems-thinking-printz/
ebookmass.com
Principles 5th Edition Joel D. Wisner
https://ebookmass.com/product/principles-of-supply-chain-management-abalanced-approach-5th-edition-joel-d-wisner/
ebookmass.com
SECOND EDITION NIELSEN | ROSENBERG DESHPANDE • HORNICEK • KATTAPURAM • ROSENTHAL SECOND EDITION G. Petur Nielsen, MD
Pathologist, Department of Pathology
Director of Electron Microscopy
Director of Bone & Soft Tissue Pathology
Massachusetts General Hospital Professor of Pathology
Harvard Medical School Boston, Massachusetts
Andrew E. Rosenberg, MD
Professor and Vice Chair
Director of Bone & Soft Tissue Pathology
Department of Pathology
Miller School of Medicine
University of Miami Miami, Florida
Vikram Deshpande, MD
Associate Pathologist
Department of Pathology
Massachusetts General Hospital
Associate Professor of Pathology
Harvard Medical School
Boston, Massachusetts
Francis J. Hornicek, MD, PhD
Chief, Orthopaedic Oncology Service
Co-Director, Center for Sarcoma and Connective Tissue Oncology
Massachusetts General Hospital
Director, Stephan L. Harris Chordoma Center
The Henry J. Mankin, MD, Endowed Scholar Professor
Harvard Medical School
Co-Leader, Dana Farber/Harvard Cancer Center Sarcoma Program
Boston, Massachusetts
Susan V. Kattapuram, MD
Associate Radiologist
Massachusetts General Hospital
Associate Professor of Radiology
Harvard Medical School
Boston, Massachusetts
Daniel I. Rosenthal, MD
Associate Radiologist-in-Chief
Massachusetts General Hospital Professor of Radiology
Harvard Medical School
Boston, Massachusetts
1600 John F. Kennedy Blvd.
Ste 1800 Philadelphia, PA 19103-2899
DIAGNOSTIC PATHOLOGY: BONE, SECOND EDITION
Copyright © 2017 by Elsevier. All rights reserved.
ISBN: 978-0-323-47777-2
No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/ permissions.
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notices Knowledge and best practice in this field are constantly changing. As new research and experience broaden our understanding, changes in research methods, professional practices, or medical treatment may become necessary.
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds, or experiments described herein. In using such information or methods they should be mindful of their own safety and the safety of others, including parties for whom they have a professional responsibility.
With respect to any drug or pharmaceutical products identified, readers are advised to check the most current information provided (i) on procedures featured or (ii) by the manufacturer of each product to be administered, to verify the recommended dose or formula, the method and duration of administration, and contraindications. It is the responsibility of practitioners, relying on their own experience and knowledge of their patients, to make diagnoses, to determine dosages and the best treatment for each individual patient, and to take all appropriate safety precautions.
To the fullest extent of the law, neither the Publisher nor the authors, contributors, or editors, assume any liability for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Publisher Cataloging-in-Publication Data
Names: Nielsen, G. Petur (Gunnlaugur Petur) | Rosenberg, Andrew, 1953-
Title: Diagnostic pathology. Bone / [edited by] G. Petur Nielsen and Andrew E. Rosenberg. Other titles: Bone.
Description: Second edition. | Salt Lake City, UT : Elsevier, Inc., [2017] | Includes bibliographical references and index.
Identifiers: ISBN 978-0-323-47777-2
Subjects: LCSH: Bones--Tumors--Handbooks, manuals, etc. | MESH: Bone Neoplasms--pathology--Atlases. | Bone Neoplasms--diagnosis--Atlases.
Classification: LCC RC280.B6 N54 2017 | NLM WZ 17 | DDC 616.8’4--dc23
International Standard Book Number: 978-0-323-47777-2
Cover Designer: Tom M. Olson, BA
Printed in Canada by Friesens, Altona, Manitoba, Canada
Last digit is the print number: 9 8 7 6 5 4 3 2 1
Dedications To my wife and family.
GPN
To my daughters, Olivia and Miranda, who are my lifelong joy; my parents, Philip and Evelyn, who did their best; my siblings, David, Stuart, and Elaine, who have been supportive; my friend and colleague, Al, who always has my back; my teachers who have helped show me the way; my colleagues with whom I have had the honor to be in the trenches; and the patients who have given me their trust. AER
To my father, Dhirendra, and mother, Shashi.
Preface The pathology of the skeleton is complex and is the morphologic expression of a broad spectrum of diseases, including those caused by genetic (sporadic and inherited), malformative, inflammatory, metabolic, circulatory, traumatic, iatrogenic, and neoplastic disorders. Bone tumors, including both neoplasms and various conditions that may simulate them, are the focus of our book. This topic is one of the most challenging areas in surgical pathology for several reasons: Bone tumors are uncommon, making it difficult to acquire the necessary experience with their histological variants and mimics; the correct diagnosis usually requires the careful integration of radiological imaging studies and clinical findings; the implications of a diagnosis on a patient can be life changing; and medical schools and pathology training programs often have insufficient expertise to provide medical students and young pathologists with the skills needed to diagnose these lesions accurately and precisely.
This book reflects the philosophy and high standards practiced by the truly multidisciplinary team of physicians at the Massachusetts General Hospital and University of Miami, who have diagnosed and surgically treated tens of thousands of patients with bone tumors for many decades. Also important to acknowledge are the contributions of the many fellows and residents who participated in the efforts of patient care.
The authors are subspecialized physicians who have dedicated their professional lives to the diagnosis and surgical management of bone tumors. As a result, the figures include beautiful and classic examples and unusual variants of many of the diseases discussed and are the product of painstaking correlations between the clinical, imaging, macroscopic, histological, immunohistochemical, and molecular characteristics of bone tumors. The text synthesizes the literature and our combined extensive experience, and the images have been selectively culled from the patient files of the Massachusetts General Hospital, the University of Miami Miller School of Medicine, and the private consultations of the authors. The book is constructed in a thematic format with sections representing groups of related diseases and the chapters discussing individual entities and their differential diagnosis.
Accordingly, this textbook serves as an excellent resource for medical students, residents, fellows, and practicing physicians in the disciplines of pathology, radiology, and orthopedics. Medical and radiation oncologists who treat bone tumors will also find it valuable. Our opportunity to participate in the care of patients with bone tumors has been our call and honor, and we hope to do it justice by sharing our experience with the medical community—our goal is to enhance diagnostic accuracy and to provide the biological basis for optimal treatment.
G. Petur Nielsen, MD
Pathologist, Department of Pathology
Director of Electron Microscopy
Director of Bone & Soft Tissue Pathology
Massachusetts General Hospital
Professor of Pathology
Harvard Medical School
Boston, Massachusetts
Andrew E. Rosenberg, MD
Professor and Vice Chair
Director of Bone & Soft Tissue Pathology
Department of Pathology
Miller School of Medicine
University of Miami Hospital
Miami, Florida
Acknowledgments Text Editors Arthur G. Gelsinger, MA
Nina I. Bennett, BA
Lisa A. Gervais, BS
Karen E. Concannon, MA, PhD
Matt W. Hoecherl, BS
Megg Morin, BA
Image Editors Jeffrey J. Marmorstone, BS
Lisa A. M. Steadman, BS
Illustrations Laura C. Sesto, MA
Richard Coombs, MS
Lane R. Bennion, MS
Art Direction and Design Tom M. Olson, BA
Laura C. Sesto, MA
Lead Editor Terry W. Ferrell, MS
Production Coordinators Angela M. G. Terry, BA
Rebecca L. Bluth, BA
Emily C. Fassett, BA
Sections SECTION 1: Benign Bone-Forming Tumors
SECTION 2: Malignant Bone-Forming Tumors
SECTION 3: Benign Cartilage Tumors
SECTION 4: Malignant Cartilage Tumors
SECTION 5: Fibrous and Fibrohistiocytic Tumors
SECTION 6: Fibroosseous Tumors
SECTION 7: Malignant Small Round Cell Tumors
SECTION 8: Notochordal Tumors
SECTION 9: Giant Cell-Rich Tumors
SECTION 10: Cystic Lesions of Bone
SECTION 11: Vascular Tumors
SECTION 12: Hematopoietic Tumors
SECTION 13: Miscellaneous Mesenchymal Tumors
SECTION 14: Metastatic Tumors
SECTION 15: Bone Tumor Mimics
TABLE OF CONTENTS SECTION1:BENIGNBONE-FORMING TUMORS
4BoneIsland/Osteopoikilosis
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
10Osteoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
16OsteoidOsteoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
22Osteoblastoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
SECTION2:MALIGNANTBONE-FORMING TUMORS
32ConventionalOsteosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
52Well-DifferentiatedIntramedullaryOsteosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
58ParostealOsteosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
68PeriostealOsteosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
72High-GradeSurfaceOsteosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
76SecondaryOsteosarcoma
VikramDeshpande,MD,G.PeturNielsen,MD,and AndrewE.Rosenberg,MD
SECTION3:BENIGNCARTILAGETUMORS
82VascularCartilaginousHamartomaofChestWall
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
84Osteochondroma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
94MultipleHereditaryOsteochondromatosis
VikramDeshpande,MD,AndrewE.Rosenberg,MD,and
G.PeturNielsen,MD
98Enchondroma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
110Enchondromatosis
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
116PeriostealChondroma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
120Chondroblastoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
128ChondromyxoidFibroma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
SECTION4:MALIGNANTCARTILAGE TUMORS
138ConventionalChondrosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
150DedifferentiatedChondrosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
156ClearCellChondrosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
162MesenchymalChondrosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
SECTION5:FIBROUSAND FIBROHISTIOCYTICTUMORS
172FibrousCorticalDefect/NonossifyingFibroma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
178DesmoplasticFibroma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
184MyofibromaandMyofibromatosis
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
188Fibrosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
194BenignFibrousHistiocytoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
196SolitaryFibrousTumor/Hemangiopericytoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
SECTION6:FIBROOSSEOUSTUMORS
200FibrousDysplasia
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
212LiposclerosingMyxofibrousTumor
G.PeturNielsen,MD,AndrewE.Rosenberg,MD,and VikramDeshpande,MD
SECTION7:MALIGNANTSMALLROUND CELLTUMORS
218EwingSarcomaandRelatedTumors
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
230MelanoticNeuroectodermalTumor
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
SECTION8:NOTOCHORDALTUMORS
234Ecchordosis
VikramDeshpande,MD,AndrewE.Rosenberg,MD,and G.PeturNielsen,MD
236BenignNotochordalCellTumor
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
242Chordoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
TABLE OF CONTENTS SECTION9:GIANTCELL-RICHTUMORS
256GiantCellTumor
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
270BrownTumor
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
274GiantCellReparativeGranuloma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
SECTION10:CYSTICLESIONSOFBONE
282IntraosseousGanglion
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
286UnicameralBoneCyst
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
294AneurysmalBoneCyst
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
306EpidermoidInclusionCyst
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
SECTION11:VASCULARTUMORS
310ConventionalHemangioma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
318Lymphangioma/Lymphangiomatosis
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
320EpithelioidHemangioma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
328PseudomyogenicHemangioendothelioma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
334EpithelioidHemangioendothelioma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
340Angiosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
SECTION12:HEMATOPOIETICTUMORS
346LangerhansCellHistiocytosis(Eosinophilic Granuloma)
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
352PrimaryLymphoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
360PlasmaCellMyeloma
VikramDeshpande,MD,G.PeturNielsen,MD,and AndrewE.Rosenberg,MD
368MastCellDisease
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
370Erdheim-ChesterDisease
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
376Rosai-DorfmanDisease
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
SECTION13:MISCELLANEOUS MESENCHYMALTUMORS
382OsteofibrousDysplasia
VikramDeshpande,MD,G.PeturNielsen,MD,and AndrewE.Rosenberg,MD
386Adamantinoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
392AdipocyticTumors
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
400Leiomyosarcoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
404Myoepithelioma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
410Schwannoma
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
414MyxopapillaryEpendymoma
VikramDeshpande,MD,G.PeturNielsen,MD,and AndrewE.Rosenberg,MD
416PhosphaturicMesenchymalTumor
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
SECTION14:METASTATICTUMORS
420MetastaticTumors
VikramDeshpande,MD,AndrewE.Rosenberg,MD,and G.PeturNielsen,MD
SECTION15:BONETUMORMIMICS
428BizarreParostealOsteochondromatous ProliferationandRelatedLesions
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
434Melorheostosis
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
438Amyloidoma
G.PeturNielsen,MD,AndrewE.Rosenberg,MD,and VikramDeshpande,MD
440GaucherDisease
G.PeturNielsen,MDandAndrewE.Rosenberg,MD
This page intentionally left blank
SECOND EDITION NIELSEN | ROSENBERG DESHPANDE • HORNICEK • KATTAPURAM • ROSENTHAL This page intentionally left blank
SECTION 1 Benign Bone-Forming Tumors Bone Island/Osteopoikilosis KEYFACTS
TERMINOLOGY
• Enostosis
CLINICALISSUES
• Incidentalradiographicfinding
• Largeboneislandsinchildrenmaybeconcerningfor osteosarcoma
• Rarelyneedtobebiopsied
• Multipleboneislandsrepresentosteopoikilosis
• Observationforsmallsolitarycharacteristiclesions,but thosethatarelargeorhaveunusualfeaturesmayrequire biopsy
IMAGING
• Mostfrequentsitesincludepelvis,proximalfemur,andribs
• Inosteopoikilosis,usuallyinvolveepiphysesofshorttubular bones
• Generallynotmuchlargerthan1cmindiameter
• Homogeneouslyradiodenselesionswithspiculated margins,whichmergewithsurroundingcancellousbone
MACROSCOPIC
• Hard,solid,tan-white
• Peripheryblendswithsurroundingcancellousbone
MICROSCOPIC
• Consistofcortical-typebonecontaininghaversian-like canals
• Predominatelylamellarbutmaybefocallywoven
• Osteopoikilosisboneislandtumorsareidenticalto sporadic,solitaryboneislands
TOPDIFFERENTIALDIAGNOSES
• Well-differentiatedosteosarcoma
• Scleroticmetastases
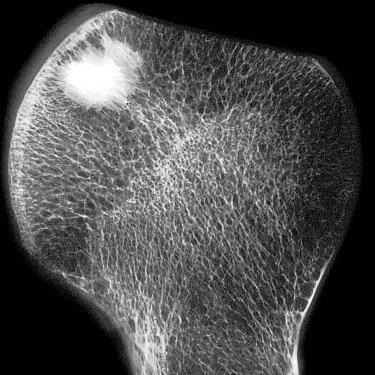
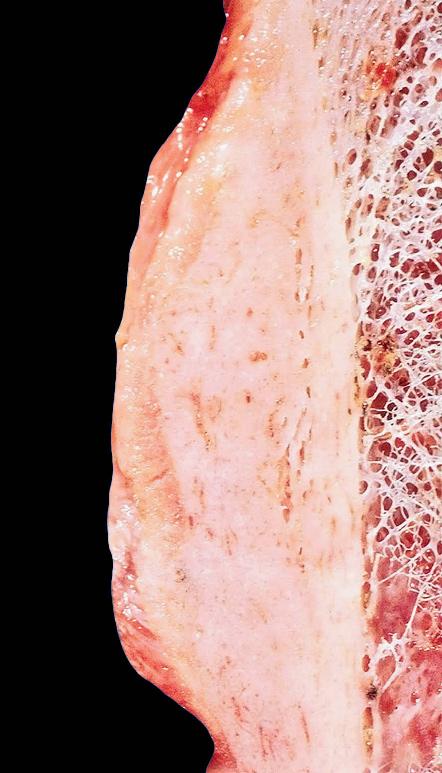
(Left)Specimenradiograph showsexcisedfemoralhead containingaboneisland.The boneislandisovaland radiodense.Theperipheryhas astellatemarginmergingwith theneighboringcancellous bone.(Right)Gross photographoffemoralhead showsboneislandbeneaththe articularsurface.Thebone islandisdense,tan-white,and hasaspiculatedborderasit mergeswiththeadjacentbony trabeculae.
(Left)Radiographofthepelvis demonstratesauniformly denseboneisland.The spiculatedmarginsrepresent extensionsfromthelesion, whichmergewiththe surroundingcancellousbone. (Right)CTofaboneisland demonstratesthatitisofthe samedensityascorticalbone. Theabsenceofalytic componentcanbedifficultto confirmwithoutadditional cross-sectionalimaging,an importantfeatureto distinguishboneislandfrom other,moresinisterboneforminglesions.
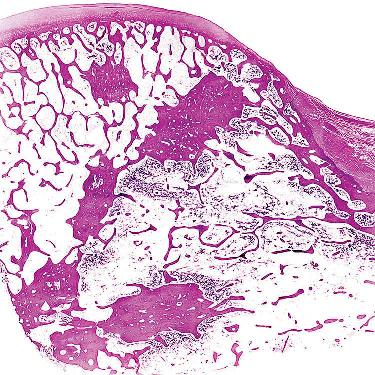
SpecimenRadiographofBoneIsland
GrossPhotographofBoneIsland
BoneIslandInvolvingPelvis
CTScanofPelvicBoneIsland
Bone Island/Osteopoikilosis TERMINOLOGY
Synonyms
• Enostosis
• Spottedbonedisease
Definitions
• Benignbone-formingtumorcomposedofcortical-type bonethatdevelopswithinmedullarycavity
• Osteopoikilosis
○ Syndromecharacterizedbypresenceofmultiple(usually many)boneislands
○ CanbeassociatedwithBuschke-Ollendorffsyndrome andmelorheostosis-likelesions
ETIOLOGY/PATHOGENESIS Neoplasm
• Causeofboneislandisunknown
• Osteopoikilosismaybeinheritedinautosomaldominant fashion
○ AssociatedwithmutationsandlossoffunctioninLEMD3 locatedon12q14
CLINICALISSUES
Presentation
• Incidentalradiographicfindingandasymptomatic
○ Largeboneislandsmaybepainful
• Uncommoninchildren
• Lesionsinosteopoikilosismayundergoslow,progressive enlargementorinvolution
Treatment
• Observationforsmallsolitarylesionswithclassic radiographicfeatures
• Largervariantsorcasesinadolescentsmayrequirebiopsy toexcludemoreaggressivelesions,suchaswelldifferentiatedosteosarcomaandscleroticmetastasesin adults
Prognosis
• Excellent
• Malignanttransformationdoesnotoccur
IMAGING
GeneralFeatures
• Location
○ Mostfrequentsitesarepelvis,ribs,andproximalfemur
○ Inadults,incidenceinpelvicbones(1.0%)andribs(0.5%)
○ Epiphysealintubularbones
○ Osteopoikilosisisbilateralandsymmetricalin distributionandinmetaphysealandepiphysealregions oftubularbones
– Anybonemaybeaffected,includingtarsalandcarpal bones
• Size
○ Usually<1cmindiameter
○ Infrequently,"giant"boneislandsseveralcmindiameter occur
RadiographicFindings
• Small
• Oval ○ Longaxisofovalisusuallyparalleltomechanicalstresses onbone,representingadaptationtoWolfflaw
• Singleormultiple
• Largervariantsmayabutorbebasedonendostealsurface
○ Donotinvolvecortexanddonotelicitperiosteal reaction
• Homogeneouslyradiodenselesionswithspiculated marginsthatmergewithsurroundingcancellousbone
MRFindings
• DarkonT1WIandT2WI,similartonormalcorticalbone
CTFindings
• Smallstellatemedullarylesionwithcharacteristicsof cortical-typebone
BoneScan
• Canshowsomeuptakeofradionuclide
MACROSCOPIC
GeneralFeatures
• Hard,solid,andtan-white;peripheryblendsinto surroundingtrabeculae,whichaccountsforirregular spiculatedmargins
MICROSCOPIC HistologicFeatures
• Consistofcortical-typebonecontaininghaversian-like canals
• Predominatelylamellarbutmaybefocallywoven
• Osteoblastsliningsurfacesareflatandquiescent
• Osteocytesaresmallandcytologicallybanal
• Boneislandsinosteopoikilosisareidenticaltosporadic, solitaryboneislands
DIFFERENTIALDIAGNOSIS Well-DifferentiatedOsteosarcoma
• Infiltrative,composedofproliferatingmildlyatypical spindlecellsandwovenbone
ScleroticMetastases
• Usuallyinadultsandcontainhistologicallymalignantcells
DIAGNOSTICCHECKLIST
ClinicallyRelevantPathologicFeatures
• Multiplelesionsraisedifferentialdiagnosisofblastic metastases;multipleboneislandsseeninosteopoikilosis
PathologicInterpretationPearls
• Lesionisintramedullary,corticalintype,andpredominately lamellarinarchitecture
SELECTEDREFERENCES 1. KorkmazMFetal:Osteopoikilosis:reportofafamilialcaseandreviewofthe literature.RheumatolInt.ePub,2014
(Left)CTscanoftheshoulder demonstratesaverylarge boneislandſtofthescapula atthebaseofthecoracoid process.Thelesionis uniformlyandcompletely denseandabutsthecortex butdoesnotinvadeor transgressit.(Right)MRofa roundboneislandſtshows thatitisuniformly hypointenseandabutsthe cortexbutdoesnotinvadeor transgressit.Themarrow adjacenttotheossifiedlesion iscompletelynormal.
(Left)Aboneislandofthe centralportionofthe vertebralbodyshows characteristicfeatures: Uniformdensityand spiculatedmarginsſt.The lesionissurroundedby unremarkablecancellous bone,andthecortexis uninvolved.(Right)Agiant boneislandofthevertebrais shownſtalmostfillingthe entirevertebralbody.Such largelesionscanshowuptake onisotopebonescansdueto theirsize.Inotherrespects, thefeaturesaresimilarto conventionalboneislands.
(Left)SagittalCTscanshowsa largeboneislandinvolvingthe pedicleandfacetjointofT12 ſt.Thelesionfillsa significantportionofthe medullarycavityandmerges withtheoverlyingcortex.The intramedullarymarginis undulatingandfocally spiculated.Smallerlesionsare seenintheadjacentvertebra. (Right)AxialCTofalarge boneislandinvolvesthe pedicleandfacetjointofT12 ſt.Thetumorhasthesame densityasthecortex,whichis unremarkable.
CTScanofBoneIsland
MRofBoneIsland
BoneIslandofSpine
BoneIslandofSpine
BoneIslandInvolvingPedicle
BoneIslandofPedicle
(Left)APradiographofthe distalfemurdemonstratesa largeboneislandinvolvingthe metaphysis.Notethe spiculatedmarginproximally. Inthisparticularlesion,the elongatedshapeofthelesion isapparent,representing adaptationtomechanical stresses.(Right)Lateral radiographofthedistalfemur demonstratesalargebone islandoftheposteriorportion oftheboneſt.Thelesion appearstobebasedonthe endostealsurfaceandextends intothemedullarycavity.
(Left)AxialCTshowsagiant boneislandofthedistalfemur ſtwithuniformdensityof compactboneandspiculated margins.Thebroadbaseof thetumorisattachedtothe endostealsurfaceofthe posteriorcortex.(Right) Isotopebonescanshowsa smallamountofuptakeſtin thelateralaspectoftheright proximalhumerus.Asmall amountofuptakecanbe presentinboneislands becausetheyareactivelybone forming.Itshouldnotbe consideredamarkerof malignancy.
(Left)CTscandemonstratesa largeboneislandofthe proximalhumerusſt.The lesioniseccentric,abutsthe endostealsurfaceofthe cortex,andextendsinthe medullarycavityinan irregularfashion.(Right) CoronalT1-weightedMRof theboneislandofthe humerusdemonstratesthe homogeneouslowsignal intensityofthelesion.The boneislandisbasedonthe innersurfaceofthecortexand hasirregularmargins.The adjacentmarrowis unremarkable.
LargeBoneIslandofFemur
LargeBoneIslandofFemur
CTofBoneIslandofFemur
BoneScan
LargeBoneIslandofProximalHumerus MRofBoneIslandofHumerus
(Left)APradiograph demonstratesosteopoikilosis withmultipleboneislands involvingtheendsoftheshort tubularbones.Thesmall lesionsclusterattheendsof thebones.(Right)AP radiographofthekneesshows thetypicalfeaturesof osteopoikilosis.Alarge numberofsmallboneislands aresymmetricallydistributed inaprimarilyjuxtaarticular andmetaphysealdistribution. Despitetheirmultiplicity,each lesionindividuallyhasthe featurestypicalofabone island.
(Left)ReformattedcoronalCT scanofthehipshowsmultiple smallboneislandsthatare juxtaarticularand metaphysealindistribution. Eachlesionisindividually indistinguishablefroma solitaryboneisland.(Right) T1-weightedMRofthekneein apatientwithosteopoikilosis demonstratesthatthebone islandsaresmall,rather uniforminsize,ovalinshape, anduniformlydense.Each lesionisindividually indistinguishablefroma solitaryboneisland.
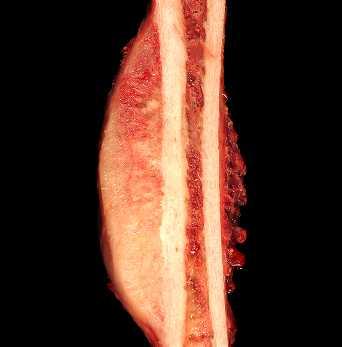
(Left)CoronalCT demonstratesan intramedullaryboneisland involvingtherightmandible ſt.Thelesionisscleroticwith thesamedensityasthe surroundingcortex.(Right) Grossphotographshowsrib andadjacentcostalcartilage. Anelongate,dense,andtanwhiteboneislandfillsthe involvedsegmentofthe medullarycavityſt.The adjacentcortexandcostal cartilageareunremarkable.
Osteopoikilosis
MRofOsteopoikilosis
BoneIslandofMandible
GrossPhotoofBoneIslandArisinginRib
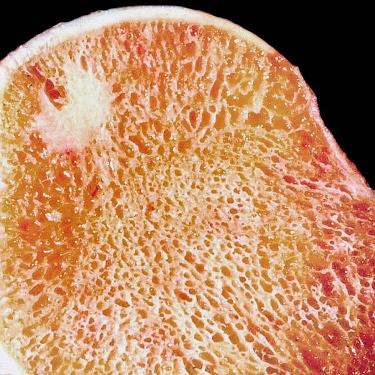
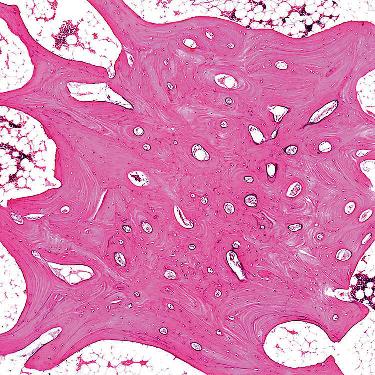
GrossPhotograph
Whole-MountSection
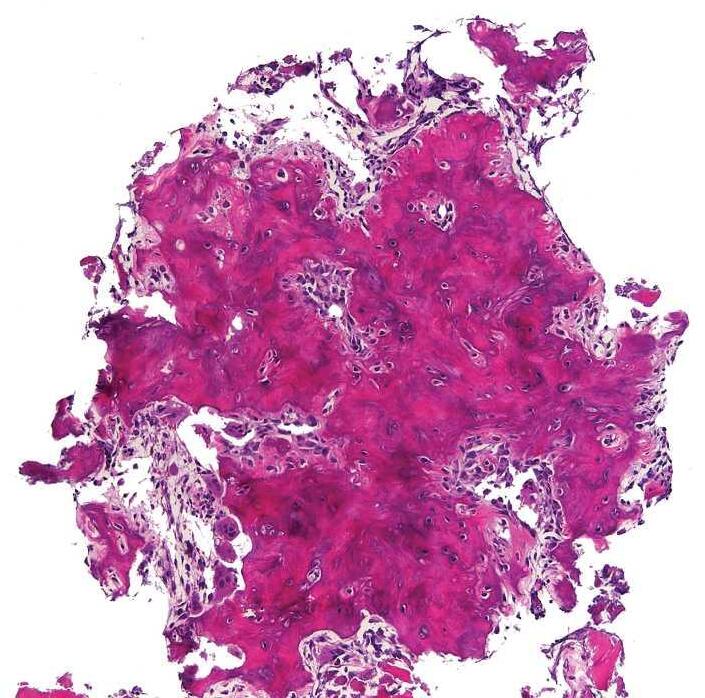
LightMicroscopy LightMicroscopy
(Left)Grossphotographshows anexcisedfemoralheadwith anincidentalboneisland. Thetumorislocatedbeneath thearticularcartilageand mergeswiththesurrounding trabecularbone.The neighboringmarrowisfatty andunremarkable.(Right) Low-powerviewshowsabone islandinvolvingthemedullary cavityoftheproximalfemur .Thelesioniscomposedof cortical-typebonethatblends imperceptivelywiththe surroundingtrabecularbone.
(Left)Histologicsectionofa solitaryboneislandisshown. Theboneislandiscomposed ofcortical-typebonewith haversian-likecanalsand transitionsintotheadjacent cancellousbone.The surroundingmarrowis predominatelyfattywith scatteredislandsof hematopoieticcells.(Right) Boneislandwithnumerous haversian-likesystems scatteredthroughoutthe lesionisshown.Theboneof thetumorissharply demarcatedfromtheadjacent marrow.
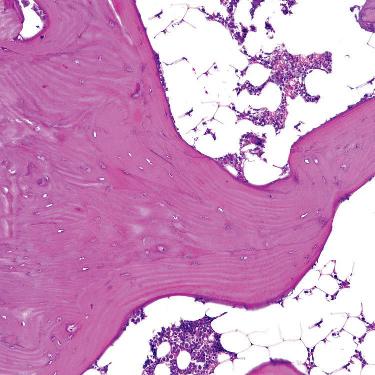
ofBoneIsland
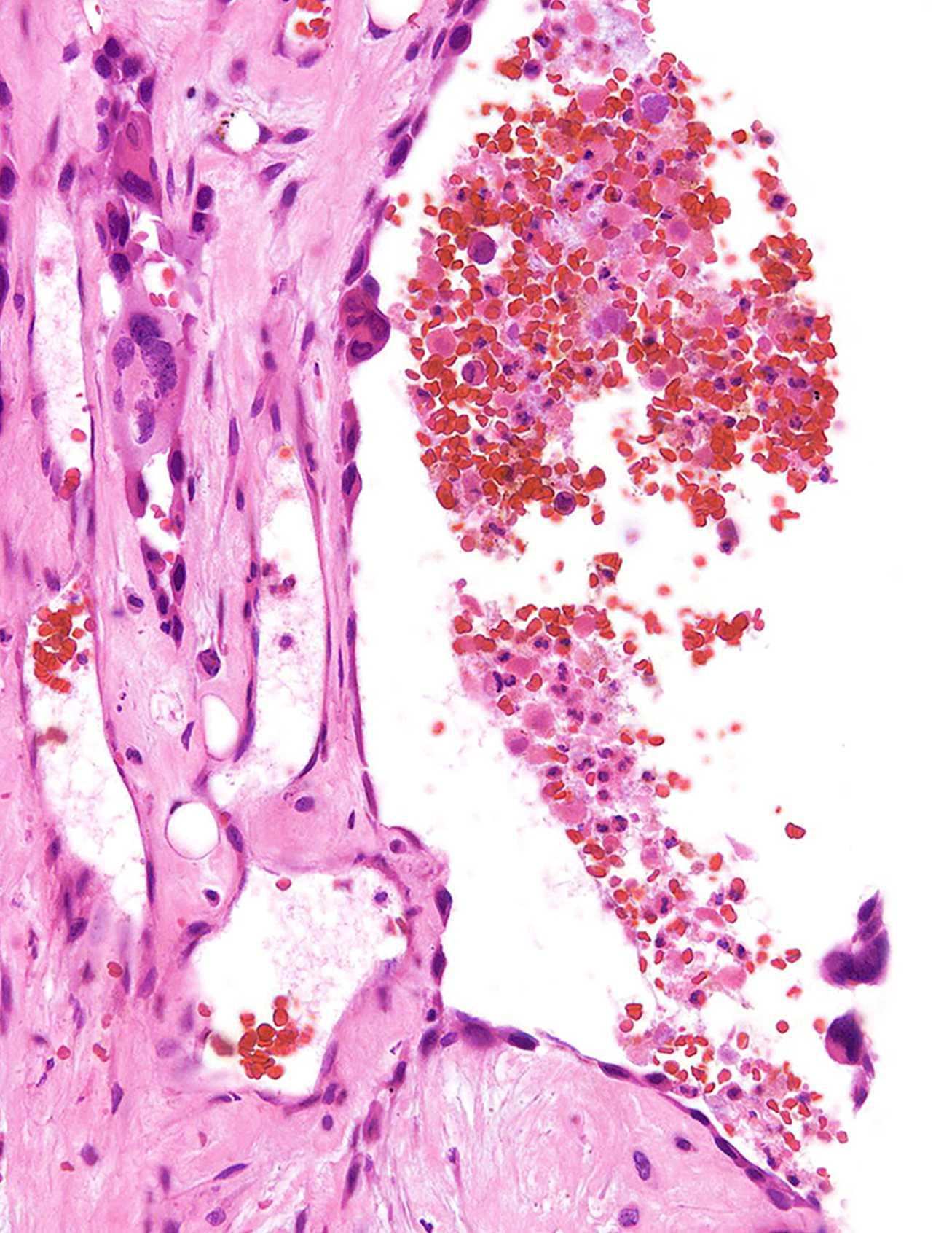
(Left)Closeviewofthe transitionbetweenthe peripheryoftheboneislandis shownasitmergeswithan adjacentbonetrabeculum. Theboneiswovenand lamellarandhasasharp borderwiththesurrounding fattyandhematopoietic marrow.(Right)Resected femoralheadfromapatient withosteopoikilosisshows thatnumerousboneislands arepresentwithinthe medullarycavity.Thelesions areroundtoovalandvaryin size.Themarginsareirregular andspiculated.
Periphery
Osteopoikilosis
Osteoma TERMINOLOGY
• Benignsurfacebone-formingtumor,usuallycomposedof cortical-typebone
CLINICALISSUES
• Usuallysmallandsolitary
• Commonlyasymptomaticandincidentalfinding
• Mostfrequentlydevelopincraniofacialskeleton
• Appendiculartumorsareveryuncommon
• MultiplelesionsraisepossibilityofGardnersyndrome
• Asymptomaticlesionscanbeobserved
• Symptomaticlesionscanbeconservativelyexcised
IMAGING
• Smallanduniformlyradiodense
• Sharplymarginatedwithwell-formedperiostealreaction
• Ovaltodome-shapedwithbroadattachmenttocortical surface
• Underlyingcortexisnotinvolved
MACROSCOPIC
• Generally<2cmindiameter;round,tan-white,andhard
• Resemblescorticalbonewithwhichitmerges
MICROSCOPIC
• Consistsmainlyoflamellarboneadmixedwithsomewoven bone
• Bonehascortical-typearchitecture
• Minorityofosteomascomposedoftrabecularbone
• Lesionalosteoblastsandosteocytesusuallyinconspicuous
DIAGNOSTICCHECKLIST
• Well-formedcorticalboneandbanalcytologydistinguishes osteomafromosteosarcoma
• Intactcortexandabsenceofcartilageexcludes osteochondroma
• Hypocellularityoflesionisevidenceagainstmyositis ossificans
• Melorheostosisandosteomaarehistologicallysimilar
OsteomaofFibula
OsteomaofLongBoneResectionSpecimen
Radiographofproximallowerlegshowsadense,welldefinedossificmassonthesurfaceoftheproximalfibula. Thereisthick,periostealboneappositionproximaltothe massthatistriangularinshape.
Osteomaiscomposedofhard,dense,compactbonewitha broadattachmenttotheunderlyingcortex.Atriangularshapedzoneofsubperiostealboneispresentproximaland distaltotheosteoma.
Osteoma TERMINOLOGY Abbreviations
• Osteoma(OS)
Synonyms
• Toruspalatinus(palate)andmandibularis(mandible)
Definitions
• Benignsurfacetumorcomposedofcortical-typebone
○ Minoritycomposedoftrabecularbone(trabecular osteoma)
CLINICALISSUES Epidemiology
• Incidence
○ Paranasalsinusosteoma:3-4%
○ Cranialosteomaatautopsy:4-5%
○ Accountsfor0.03%ofbiopsiedprimarybonetumors
• Age
○ Mostcommonin4thto6thdecadesoflife
• Sex
○ Nopredilection
Site
• Craniofacialskeletonmostcommon
○ Oftenlocatedinfrontalandethmoidsinuses(75%)
○ Sphenoidsinus,cranium,jaw
• Appendicularskeletonrare
○ Longtubularbones
– Femurandtibiamostcommon
Presentation
• Slow-growingsmalllesions;usuallyincidentalfinding
• Largelesions:Symptomsrelatedtoanatomiclocation
○ Sinustumors:Obstructionandmucocele
○ Orbitaltumors:Exophthalmosandvisiondisturbances
○ Oraltumors:Interferewithdenturesandmastication
○ Appendiculartumors:Palpablehardmass
• Usuallysolitary
○ MultipletumorsmaybeseeninGardnersyndrome
Treatment
• Observation
• Simpleexcision
Prognosis
• Excellent,norecurrence
IMAGING
GeneralFeatures
• Uniformlyradiodensesurfacelesionwelldemarcatedfrom softtissue
• Ovoidwithbroadbaseofattachmenttocortex
• Denseperiostealreactionalongmarginofattachmentmay bepresent
MRFindings
• LowsignalintensityonT1-andT2-weightedimages
○ Lesiondoesnotenhancewithcontrast
CTFindings
• Well-delineatedsurfacemasswithcorticaldensity
BoneScan
• Mayshowincreasedornoradiotraceruptake
MACROSCOPIC
GeneralFeatures
• Generally<2cmindiameter
• Oval,round,orhemispheric
• Hard
• Tantowhite
• Resemblescorticalbonewithwhichitmerges
• Well-formed,triangular-shapedsubperiostealreactivebone maysurroundattachmentsitetocortex
MICROSCOPIC
HistologicFeatures
• Admixtureoflamellarandwovenbonewithhaversian-like systems
• Infrequentlycomposedoftrabecularbone
• Growinglesionmayhavefibrouscomponentmimicking fibroosseoustumor
• Osteoblastsrimmingboneareinconspicuousandelongate
○ Growinglesionslinedbyplumpmetabolicallyactive osteoblasts
– Abundanteosinophiliccytoplasmandnucleipolarized awayfrombone-formingsurface
• Inactiveosteoblastsandosteocyteshavesmallrounddark nucleiandnonucleoli
DIFFERENTIALDIAGNOSIS
Bone-FormingLesions
• Parostealosteosarcoma
○ Containsprominentspindlecellcomponent
• Juxtacorticalmyositisossificans
○ Composedofhypercellularcancellousbone
• Melorheostosis
○ Drippingcandlewaxconfiguration
• Osteochondroma
○ Hascartilagecap
DIAGNOSTICCHECKLIST
PathologicInterpretationPearls
• Well-formedcorticalboneandbanalcytologydistinguishes osteomafromosteosarcoma
• Intactcortexandabsenceofcartilageexcludes osteochondroma
• Hypocellularityisevidenceagainstmyositisossificans
• Melorheostosisandosteomaarehistologicallysimilar
SELECTEDREFERENCES 1. HalawiAMetal:Craniofacialosteoma:clinicalpresentationandpatternsof growth.AmJRhinolAllergy.27(2):128-33,2013
2. GreenspanA.Benignbone-forminglesions:osteomaetal:clinical,imaging, pathologic,anddifferentialconsiderations.SkeletalRadiol.22(7):485-500, 1993
3. O'ConnellJXetal:Solitaryosteomaofalongbone.Acasereport.JBone JointSurgAm.75(12):1830-4,1993