https://ebookmass.com/product/atlas-of-wound-healing-atissue-regeneration-approach-1st-edition-soheila-s-
Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
ABC of Wound Healing 2nd Edition Annie Price
https://ebookmass.com/product/abc-of-wound-healing-2nd-edition-annieprice/
ebookmass.com
Tissue Barriers in Disease, Injury and Regeneration 1st Edition Nikolai V. Gorbunov (Editor)
https://ebookmass.com/product/tissue-barriers-in-disease-injury-andregeneration-1st-edition-nikolai-v-gorbunov-editor/
ebookmass.com
Therapeutic dressings and wound healing applications Boateng
https://ebookmass.com/product/therapeutic-dressings-and-wound-healingapplications-boateng/
ebookmass.com
Schemeringen 04 - Waarheid in het licht Hannah Hill
https://ebookmass.com/product/schemeringen-04-waarheid-in-het-lichthannah-hill-2/
ebookmass.com
Upper Hand: The Future of Work for the Rest of Us Sherrell Dorsey
https://ebookmass.com/product/upper-hand-the-future-of-work-for-therest-of-us-sherrell-dorsey/
ebookmass.com
Oxford Assess and Progress: Situational Judgement Test 4th Edition David Metcalfe
https://ebookmass.com/product/oxford-assess-and-progress-situationaljudgement-test-4th-edition-david-metcalfe/
ebookmass.com
Practical Approaches to Biological Inorganic Chemistry 2nd Edition Robert R. Crichton (Editor)
https://ebookmass.com/product/practical-approaches-to-biologicalinorganic-chemistry-2nd-edition-robert-r-crichton-editor/
ebookmass.com
Preparing Effective Business Plans: An Entrepreneurial Approach (2nd
https://ebookmass.com/product/preparing-effective-business-plans-anentrepreneurial-approach-2nd/
ebookmass.com
Law's ideal dimension First Edition. Edition Robert Alexy
https://ebookmass.com/product/laws-ideal-dimension-first-editionedition-robert-alexy/
ebookmass.com
The Art of Multiprocessor Programming 2nd Edition Maurice Herlihy
https://ebookmass.com/product/the-art-of-multiprocessorprogramming-2nd-edition-maurice-herlihy/
ebookmass.com
ATissueRegenerationApproach
EditorialBoard
AuthorandEditorialDirector:SoheilaS.Kordestani,PhD BiomedicalEngineeringFaculty,AmirkabirUniversityofTechnology,Tehran,Iran ManagingDirector,ChitoTechInc.,Tehran,Iran
ManagingEditor:FatemeFayyazbakhsh,PhD ProductDevelopmentManager,ChitoTechInc.,Tehran,Iran
ClinicalEditor:MitraSamiAbyaneh,MD TrainingManager,ChitoTechInc.,Tehran,Iran
ArtDirector:AtefehHeidari GraphicDesignerandSocialMediaDirector,ChitoTechInc.,Tehran,Iran
EditorialAssistant:FahimehS.Mohammadi R&DDepartment,ChitoTechInc.,Tehran,Iran
ClinicalCaseCoordinator:FatemehRezaee R&DDepartment,ChitoTechInc.,Tehran,Iran
AtlasofWound Healing ATissueRegenerationApproach
SOHEILAS.KORDESTANI
BiomedicalEngineeringFaculty
AmirkabirUniversityofTechnology
Tehran,Iran
ManagingDirector
ChitoTechInc.,Tehran,Iran
ATLASOFWOUNDHEALINGISBN:978-0-323-67968-8
Copyright 2019ElsevierInc.Allrightsreserved.
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans,electronicor mechanical,includingphotocopying,recording,oranyinformationstorageandretrievalsystem,without permissioninwritingfromthepublisher.Detailsonhowtoseekpermission,furtherinformationabout thePublisher’spermissionspoliciesandourarrangementswithorganizationssuchastheCopyright ClearanceCenterandtheCopyrightLicensingAgency,canbefoundatourwebsite: www.elsevier.com/ permissions
ThisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythePublisher (otherthanasmaybenotedherein).
Notices
Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgeinevaluating andusinganyinformation,methods,compoundsorexperimentsdescribedherein.Becauseofrapid advancesinthemedicalsciences,inparticular,independentverificationofdiagnosesanddrug dosagesshouldbemade.Tothefullestextentofthelaw,noresponsibilityisassumedbyElsevier, authors,editorsorcontributorsforanyinjuryand/ordamagetopersonsorpropertyasamatterof productsliability,negligenceorotherwise,orfromanyuseoroperationofanymethods,products, instructions,orideascontainedinthematerialherein.
Publisher: DoloresMeloni
AcquisitionEditor: CharlottaKryhl
EditorialProjectManager: RebekaHenry
ProductionProjectManager: KiruthikaGovindaraju
CoverDesigner: MilesHitchen
Preface
Theincreasingincidenceofwoundsintheagingpopulation,therisingprevalenceofdiabetesandthusdiabetic footulcer,andthelargenumberofotherchronicwounds associatedwithdiseasesandabnormalitiesmakeit imperativetohaveadeeperunderstandingofwounds anddevelopapreventiveapproachinthe firstinstance.
Thenewthinkinginhealthcareandtheadventof advancedwoundcaremodalities,whichhasbecomeone ofthemajorareasinregenerativemedicine,hasprovided relativelybettermoisttissueenvironment,accelerated theinflammatoryresponse,qualitygranulationtissue
formation,andinfectioncontrolduringwoundhealing. Moderndressingsprovideanappropriatespacetofacilitatethecellularactivities(i.e.,migrationandproliferation)andevokethesolublemediatorstoregeneratethe damagedtissuesfaster.
ThisAtlasofWoundistheoutcomeofapproximately 14yearsofdedicatedeffortstocollecttheresultofusing advancedwoundcaremodalitiesonalargenumberof patientsofdiverseethnicitieswithdifferenttypesof acuteandchronicwoundsofdifferentetiologies.Ihope itcanbeofbenefitformedicalcommunity.
Thispageintentionallyleftblank
Acknowledgments
Preparingthis “AtlasofWound” washarderthanI imagined.Noneofthiswouldhavebeenpossible withoutChitoTechnursesandwoundcarespecialists workingdayandnightonthewoundsofmany patients.SpecialthankstoDr.SamiAbyanehandDr. Fayyazbakhsh,fortakingthisdifficulttaskaseditors, andourdedicatedR&Dteam.Iamalsoeternally gratefultothedoctors,surgeons,andnursesinmany hospitalsthroughoutIranforcooperatingwithusto useChitoTechadvancedwounddressingsonthe patients.
Iwouldliketoexpressmysinceregratitudetothe followinghospitalsfortheirsupport:
l ImamKhomeiniHospital,Tehran,Iran
l ChamranHospital,Tehran,Iran
l ShahidMotahariBurnsHospital,Tehran,Iran
l ShariatiHospital,Tehran,Iran
l ValiAsrsubspecialtyHospital,Tehran,Iran
l ShohadayeTajrishHospital,Tehran,Iran
l ImamRezaHospital 501AJA,Tehran,Iran
l MasihDaneshvariHospital,Tehran,Iran
l RasoulAkramHospital,Tehran,Iran
l Dr.Mo’eiriHospital,Tehran,Iran
l ImamRezahospital,Qom,Iran
l GharaziHospital,Sirjan,Kerman,Iran
l ImamKhomeiniHospital,Urmia,Iran
l PasteurnoHospital,Tehran,Iran
l NaftCompanyHospital,Tehran,Iran
l SinaHospital,Tehran,Iran
l LoghmanHakimHospital,Tehran,Iran
l Children’sMedicalCenter,Tehran,Iran
l ShohadayeHaftomeTirHospital,Tehran,Iran
l FiroozgarHospital,Tehran,Iran
l StateWelfareOrganizationofIran(JalaeiPour Clinic),Tehran,Iran
l BaharlooHospital,Tehran,Iran
l KashaniHospital,Tehran,Iran
l BahramiChildrenHospital,Tehran,Iran
l RaziHospital,Tehran,Iran
Lastbutnotleast,Iwouldliketothankmyhusband,mycompanionforthatlast35years,whohave alwayssupportedmeineveryworkIhavedoneandmy sonanddaughterforsupportingme.
Thispageintentionallyleftblank
AbouttheAuthor
Dr.Kordestaniisaproteinchemist,graduatedfrom LeedsUniversityin1990,andworkedasaresearch fellowattheDepartmentofMedicineatBirmingham University.Shehasbeenworkinginthe fieldofWound HealinginIranforthelast20years.Sheisafaculty memberandalecturerinBiomedicalEngineering DepartmentattheAmirkabirUniversityofTechnology,
andherprimaryteachingfocusisonthetopicof woundhealingandtheroleofbiomaterials,aimedat graduatestudents.Shehasextensiveindustrycontacts asthefounderofaknowledge-basedcompany, manufacturingadvancedwoundcareproducts.The biomaterialusedintheseproductshasbeenprotected by fiveinternationalandEuropeanpatents.
Thispageintentionallyleftblank
ListofFigures
Fig.2.1 Awoundwithdiscontinuityin skinandprobablydamagein underlyingtissues 3
Fig.2.2 Awoundtypicallyinvolves severaltissues 4
Fig.2.3 Humantissuetypes 5
Fig.2.4 Skinfunctions 5
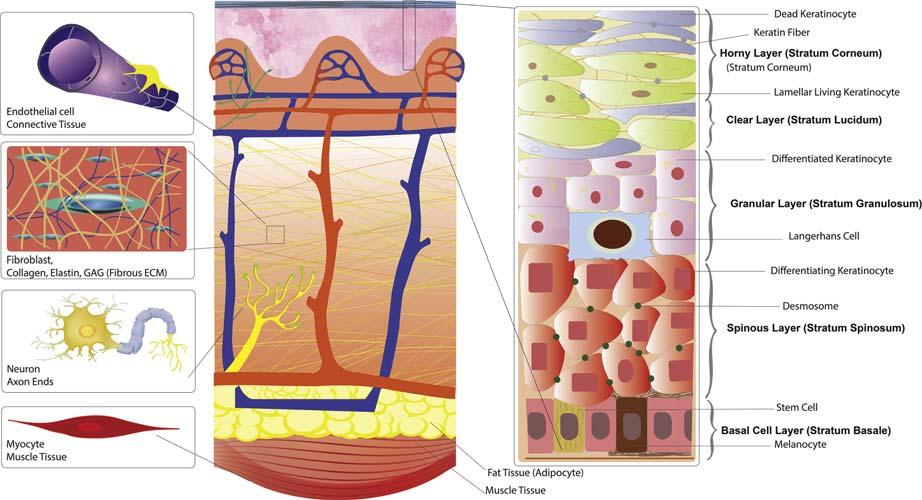
Fig.2.5 Anatomyoftheskinandits underlyingtissues 6
Fig.2.6 DifferentcellsandECMscanbe foundinawoundincluding epidermis,dermis,hypodermis, vessel,muscle,nerve,and lymphaticvessel 7
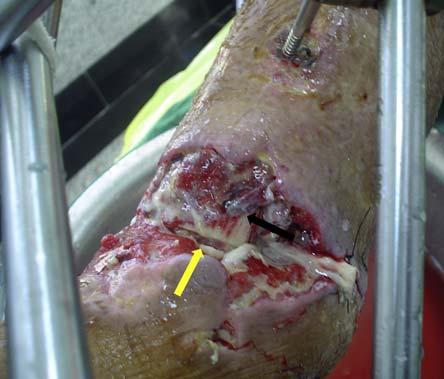
Fig.2.7 Atraumaticwoundwith damagedmuscle(blackarrow) andtendonrapture(yellow arrow) 7
Fig.2.8 Exposedbonecanbeoccurin differenttypesofwound(A)a traumaticwoundcausedbycar accident(B)adiabeticfootulcer (C)and(D)aninfectedsurgical wound 8
Fig.3.1 Thefourphasesofwoundhealing(hemostasis,inflammatory, proliferative,andremodeling) 11
Fig.3.2 Woundhealingphases:maincell types,ECM,andtissues 12
Fig.3.3 Yellowarrowsindicatethe epithelialtissuethatappears fromthewoundedge 14
Fig.3.4 Woundcontraction 15
Fig.3.5 Necrotictissue:Blackeschar 17
Fig.3.6 Necrotictissue:Whiteeschar 17
Fig.3.7 Sloughtissue 17
Fig.3.8 Scablayer 18
Fig.3.9 Callustissue 18
Fig.3.10 Granulationtissue 18
Fig.3.11 Typesofwoundhealing 19
Fig.3.12 Maceratedwoundtissue 21
Fig.3.13 Woundbiofilmisanimpermeablelayeronthewoundsurface 22
Fig.4.1 Differentpartsofthewound 23
Fig.4.2 Keyparametersinwound assessment 24
Fig.4.3 Anatomiclocationofwound 24
Fig.4.4 Schematicofwoundsizemeasurementinthreedimensions 25
Fig.4.5 Measuringthelengthofwound byapaperruler 25
Fig.4.6 Placingthetipofaswabinthe deepestpartofthewound,and markingtheskinleveltomeasure thedepthofthewound 25
Fig.4.7 Erythemaaroundtheskin 26
Fig.4.8 Differenttypesofwoundexudate 27
Fig.4.9 Tunnelingisanarrowopening, whichhasextendedthroughthe softtissue 28
Fig.4.10 Woundunderminingmayextend inoneormanydirections underneaththewoundedges 28
Fig.4.11
HealAppmeasuresthewound areabydrawingwoundboundariesandmeasuringtheareausingapapertagas2Dscale 29
Fig.4.12 HealAppmeasuresthewound areaandreportsthearea quantitatively 29
Fig.4.13 Woundhealingprogression againsttime 29
Fig.5.1 Differentpartsofwoundcare management 31
Fig.5.2 Woundtreatmenttechniques 33
Fig.5.3 Skingraft 33
Fig.5.4
Effectofdressingonthequality ofwoundhealing.Afterapplying thehydrogel,keratinocyte migration,growthfactorsregulation,andvascularizationwill improveduetoprovidingmoist environment.Inaddition,the dressingactsasaphysiochemical barrieragainstmicroorganisms 36
Fig.5.5 Debridementtechniques 39
Fig.5.6 Surgicaldebridementforapressureulcerinanoperatingroom 39
Fig.5.7 Sharpdebridementforachronic traumaticulcer 40
Fig.5.8
Autolyticdebridementwithout woundedgemaceration 41
Fig.5.9 Autolyticdebridementwith maceratedwoundedges,which canimpairwoundhealingand maketheskinmorevulnerableto infection 41
Fig.5.10
Normaltissueversusscarredtissue.Collagen fibersareformedin tiledpatterninnormaltissue, whileformedparallelizedinscar tissue,whichisresultsinmore stiffnessinscartissue.Furthermore,theskinappendages,for example,hairfollicles,sebaceous glands,andsweatglands,are disappearedinscartissue 43
Fig.5.11 Normalscar 43
Fig.5.12 Hypertrophicscar 44
Fig.5.13 Acutewoundtreatment algorithm(CIP) 45
Fig.5.14 Chronicwoundtreatment algorithm(DIP) 46
Fig.6.1 Differentclassificationsofwound 49
Fig.6.2 Thedifferencesbetweenacute andchronicwounds:thesignificantincreaseinpopulationof keratinocytesand fibroblastsas wellasmoregrowthfactorsand lesspathogensinacutewound (A)versuschronicwound(B) 50
Fig.7.1 Stagesofpressureulcer 52
Fig.7.2 StageIpressureulcer 52
Fig.7.3 StageIIpressureulcer 53
Fig.7.4 StageIIIpressureulcer 53
Fig.7.5 StageIVpressureulcerwith exposedboneandtendon 54
Fig.7.6 Unstageablepressureulcer 55
Fig.7.7 Suspecteddeeptissue injury(DTI) 55
Figs.7.8 7.47 Pressureulcer 56 75
Fig.8.1 DFUleadstoamputationin1% ofpatientseveryyear 77
Fig.8.2 Malumperforanspedis 78
Fig.8.3 DFUwithdeformedfoot,i.e., Charcot 78
Fig.8.4 Assessingthesensoryneuropathy usingmonofilament 79
Fig.8.5 DFU 79
Fig.8.6 Grade1DFU 80
Fig.8.7 Grade2DFU 80
Fig.8.8 Grade3DFU 80
Fig.8.9
Grade4DFU 81
Fig.8.10 Grade5DFU 82
Fig.8.11 SchematicgradingofDFU 82
Figs.8.12 8.44 DFU 83 99
Fig.9.1 First-degreeburncausedby sunexposure 101
Fig.9.2 Blistersformedinasuperficial second-degreewound 102
Fig.9.3 Deepsecond-degreeburn wounds 102
Fig.9.4 Third-degreeburnwounds 103
Fig.9.5 Degreesofburnwound 103
Fig.9.6 Ruleofninesrefersacertain percentagetoeachpartofthe body 104
Figs.9.7 9.25 Burn 105 114
Fig.10.1 Schematicviewofvascularulcers progressionagainsttime 115
Fig.10.2 Differenttypesofvascularulcers 116
Fig.10.3 Venousulcer 116
Fig.10.4 Arterialulcer 116
Fig.10.5 Lymphaticulcer 116
Fig.10.6 Arterialpulsepoints 117
Figs.10.7 10.14 Vascularulcer 119 122
Fig.11.1 Traumaticwoundillustration 123
Fig.11.2 Cutwound 123
Fig.11.3 Separationofskinandunderlyingtissuesinwhichtheedgesare tornandirregularinalaceration woundcausedbyaccident 123
Fig.11.4 Contusionsaftertrauma 124
Fig.11.5 Puncturewoundcausedbyarod 124
Fig.11.6 Secondarytraumaticwoundafter removalofapieceofwoodfrom apuncturewound 124
Fig.11.7 Abrasionwounds 125
Fig.11.8 Scorpionbite 125
Fig.11.9 Woundcausedbygunshot 125
Figs.11.10 11.17 Traumaticwound 126 130
Fig.12.1 Asurgicalincisionwithsharp edgesafterexcisionofapilonidal sinus 131
Fig.12.2 Surgicalwoundsdehiscence 131 Fig.12.3 Wounddehiscencedueto infection 132
Figs.12.4 12.22 Surgicalincision 132 141
Fig.13.1 Malignantulcer 143
Fig.13.2 Pemphigusvulgarisulcer 144
Fig.13.3 EBwound 144
Figs.13.4 13.28 Atypicalwound 145 156
ListofTables
Table3.1
Table3.2
Table3.3
Table4.1
Table4.2 WoundEdgeCharacteristics
Table5.1
Table5.2
Table6.1 CharacteristicsofAcuteand ChronicWounds
Table8.1 ClinicalCharacteristicsofThree MajorTypesofDFU(Neuropathic, Ischemic,andNeuroischemic)
Table10.1 ClinicalCharacteristicsofDifferent TypesofVascularUlcer
Thispageintentionallyleftblank
Thispageintentionallyleftblank
CHAPTER1
Introduction
Theincreasingincidenceofwoundsintheagingpopulation,therisingprevalenceofdiabetesandthusdiabetic legulcer,andthelargenumberofotherchronicwounds associatedwithdiseasesandabnormalitiesmakeit imperativetohaveadeeperunderstandingofwound anddevelopapreventiveapproachinthe firstinstance.
Whenthereisawound,thesurroundingtissuesare damagedintheorganinvolvedandthelocalenvironmentwithinthatorganisdamaged;therefore,wound healingisacomplexprocessinvolvingmanycellpopulations,theextracellularmatrix,andsolublemediators suchasgrowthfactorsandcytokines.Toreducethe burdenofwoundinhealthcare,itisnecessarytohave adeepunderstandingofpathophysiologicalprocesses ofhealing.Evenmoresoitisessentialtoviewwound healingastissuehealingandunderstandtheinterrelated processestakingplacebetweencell cell,cell ECM (ExtraCellularMatrix),vasculartissues,andmanybiomoleculesactivatedduringthehealingprocess.
Currently,severalclinicallyprovenstrategieshave beendevelopedforwoundtreatment.Despitetheir relativeeffectivenessinwoundhealing,thesestrategies facemultiplechallengesincludinginadequatetissue repair,scartissueformationwithoutanyskinappendages,limitedvascularization,poorinfectioncontrol, andhighcost.
Tissueregeneration,asoneofthemajorareasof regenerativemedicine,hasbeendevelopedtomake upfordonortissueshortages,tissuereplacementrejections,anddelayedinflammationresponses.Tissue regenerationstrategiesforwoundhealinghavebeen focusedonprovidingmoisturizedenvironments,acceleratingtheinflammatoryresponse,qualitygranulation tissueformation,andinfectioncontrolduringtissue regeneration.Moderndressingsprovideanappropriate spacetofacilitatethecellularactivities(i.e.,migration andproliferation)andevokethesolublemediatorsto regeneratethedamagedtissuesfaster[1 4].
Aseverythingintheworld,includingmedicalcare systems,isbecomingdigitized,inthisatlasanew techniqueforwoundareameasurementhasbeen
introduced: “HealApp” isapowerfulcognitivemobile application,whichmeasuresthewoundareaquantitativelyusingartificialintelligence.
Thisatlasistheoutcomeofapproximately14yearsof dedicatedeffortsonalargenumberofpatientsofdiverse ethnicitieswithdifferenttypesofwoundanddifferent etiologies.Thesewoundswerehealedusingabrandof novelwoundcareproductscalled “ChitoTech”.These productsarebasedonanaturalbiopolymer,chitosan.
PREVALENCEANDBURDENOFWOUNDS
Owingtoasigni ficantincreaseintheglobalaveragelife expectancyandhence,theage-relateddiseasesand alteredlifestyle,theprevalenceofchroniculcershas beenincreasedamongelderly(e.g.,pressureulcers) [2].Theglobalburdenofdiabeteshasbeenrising rapidly,anditisestimatedthatmorethan425million peoplesufferfromdiabetesallovertheworld, increasingto628millionby2045[3].International DiabetesFederationhasestimatedthat19% 34%of diabeticpatientswillexperienceadiabeticfootulcer, andfootulcersaffect9.1 26.1millionpeoplewith diabetesannuallyallovertheworld[4].
Reportsindicatethat1 3millionpeopleinthe UnitedStatessufferfrompressureulcerannuallythat causesaremarkable financialburdenforhealthcare system[5].
Accordingtothe firstcomprehensiveinvestigationof Medicarebasedon2014claimsdata,approximately 8.2millionpeopleintheUnitedStateshadexperienced oneofthewoundtypesorinfectionwithtotalspending rangedfrom$28.1to$96.8billion[5].
Onepercentoftheglobalburdenofdiseasesis relatedtoburns,leadingtomorethan7.1million injuriesand265,000deathsallovertheworld annually[6].
Accuratewoundassessmentanddeterminingthe bestwoundcareplancansignificantlyreducethe financialburden.
Thispageintentionallyleftblank
WoundAnatomy
Awoundisaninjurytothelivingtissuecausedby accident,violence,surgery,orsomechronicdiseases; thatistypicallyde fi nedbybreakingoftheskinmembraneandusuallydamagetounderlyingtissuesor organs. Fig.2.1 showsawoundwithdisruptionin skincontinuity.
Anatomically,awoundisdefinedbyanexternalor internalbreakdowninthenormalcontinuityofExtra CellularMatrix(ECM)andepithelium;andthelossof theprotectivefunctionoftheskin,withorwithout damagetotheunderlyingconnectivetissue(i.e.,vessels, nerves,muscles,orbone).
FIG.2.1 Awoundwithdiscontinuityinskinandprobably damageinunderlyingtissues.
Appropriateinitialwoundmanagementisvitalfor acceleratedhealingandsuccessfultreatment.Therefore, understandingtheanatomyandphysiologyofthe wound-involvedtissuesandknowingtheirremodeling processarecriticalforeffectivetreatment.Woundrelatedtissuesareshownin Fig.2.2
WHICHTISSUESMIGHTBEDAMAGEDIN WOUNDS?
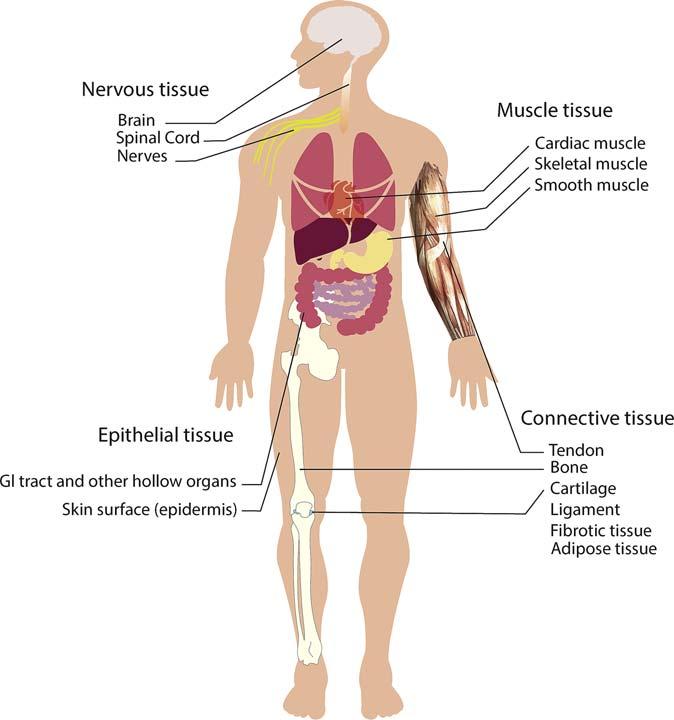
Therearefourmaintypesoftissueinthehumanbody: epithelial,muscle,connective,andnervoustissues, whicharemadeofspecializedcellsthataregrouped togetheraccordingtostructureandfunction. Fig.2.3 illustratestheschematicofthesetissues.
Dependingonthewoundsiteandseverity,anyof thefollowingtissuescanbeinvolved:
EPITHELIALTISSUE
Epithelium,oneofthefourbasictypesofmammalian tissue,coverstheoutmostsurfacesoforgansandblood vessels,aswellas,theinnersurfacesofmanyinternal organs.Epidermis,theoutermostlayerofnormal healthyskin,isthelargestepitheliumofthehuman body.
Epithelialtissuehasthreemaincelltypes:squamous (flat),columnar,andcuboidal,whichcanbearranged insingle,double,ormorelayersofcells.Epithelium hasmanyfunctionsincludingprotection,selective transcellulartransport,andsensing[6,7].
Therearenovesselsinepithelialtissues;thus,the underlyingconnectivetissuesdeliverthenutritionvia diffusionthroughthecelljunctionsofthebasement membrane.
Mostly,whenanopenwoundoccurs,theskinis damagedandlosesitscontinuityduetothebreakdown inepithelialtissue.Thus,comprehensiveknowledge ofstructureandfunctionsofthenormalhumanskinis essentialforunderstandingthewoundpathophysiology.
Skin
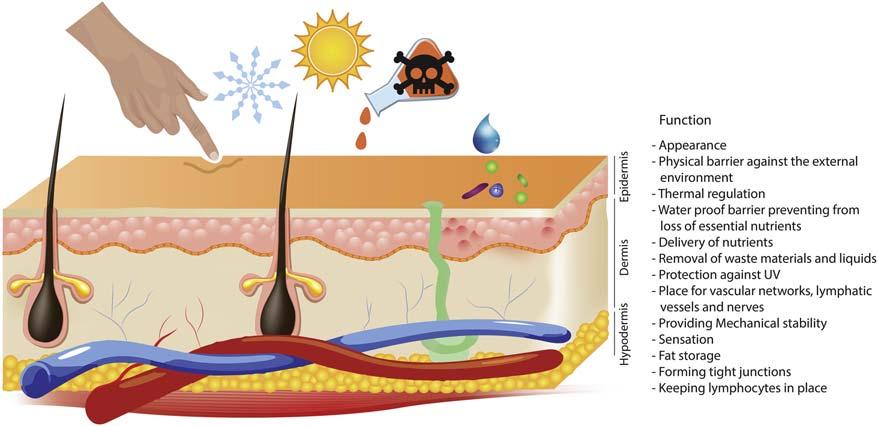
Skin,thelargestandprimaryprotectiveorganinthe humanbody,maintainsa first-orderphysicalbarrier betweentheinternalandexternalenvironmentsand actsasabarrieragainstoutsidepathogensandexcessive lossofwaterorothernutrients.Generally,indirectcontactwiththeoutsideenvironment,theskinplaysakey roleinimmunologicsurveillance,sensoryperception, regulationofbodytemperature,andprotectionagainst traumaandUVradiation.
Awoundtypicallyinvolvesseveraltissues.
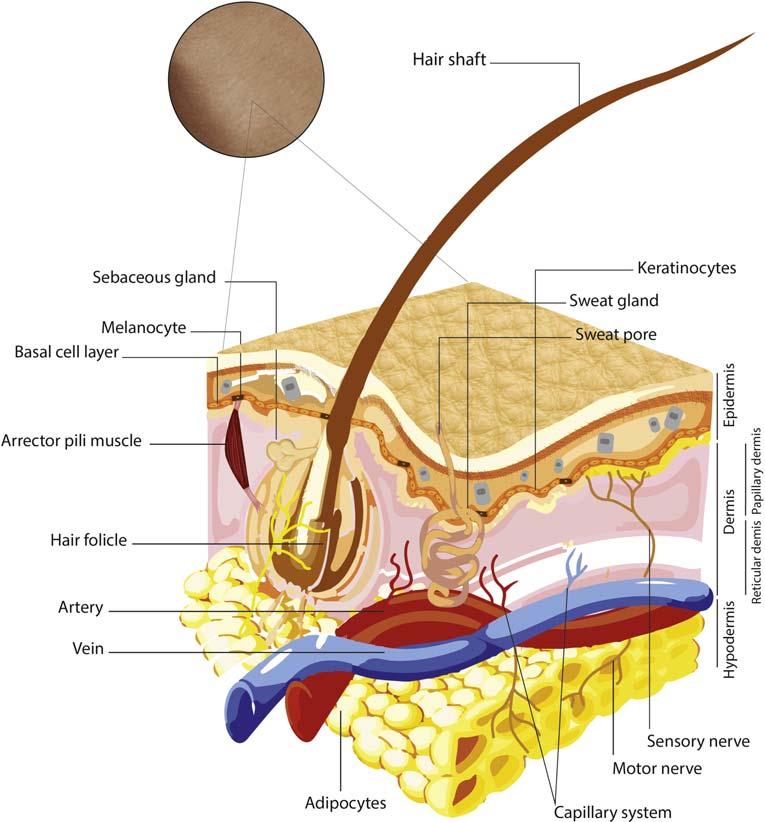
Theskiniscomprisedofthreelayers:epidermis, dermis,andhypodermis,whichareconservedacross specieswithslightbutsignificantdifferences.These well-separatedlayersworktogethertoprovidethe multifunctionalperformanceofskin[8 10]. Figs.2.4 and2.5 showfunctionsandstructureoftheskin, respectively.
Epidermis
Theepidermisistheexternallayeroftheskinwithanarrowedstratifiedstructureformedby fivewell-defined epithelialsublayers.Themajorcelltypeinthislayeris keratinocyte,whichundergoesgradualdifferentiation fromtheboundarylayertotheskinsurfacetoprovide aneffectivehierarchicalbarrier.Theouterlayercells aredeadandlosetheirnucleusandcytoplasm,instead ofcontainingatough,resistantproteincalledkeratin thatmakestheepitheliumwaterproof.Keratinocytes areresponsibleforkeratinsynthesis,aswellasthe essentialcytokinesforwoundhealing.ThislayerprotectstheinnerorgansagainstUVandoutsideenvironmentthroughmelanocytesandLangerhanscells [11,12].
Dermis
Thedermis,locateddeepintheepidermis,betweenthe basementmembraneandsubcutaneousfat,houses
connectivetissues,nerves,bloodvessels,lymphaticvessels,hairfollicles,sebaceousglands,andsweatglands.
Thethicknessofthedermisvariesfromlessthan 1mmintheeyelidsandover5mminthebackandis approximately15 40timesthickerthantheepidermis. Fibroblastisthemajorcelltypeofthedermiswitha specializedECMintwoforms: fibrousproteinsand groundsubstances.
Collagen fiberscomposedapproximately75%ofthe dryweightand30%ofthevolumeofthedermiswith 75%collagentypeIand15%typeIII.Theamount andqualityofcollagendecreaseduringaging.Elastin isanotherprominent fiberindermisECM,associated withtheelasticityandsynthesizedduringthefetallife by fibroblasts.
Thegroundsubstances,asagel-likeamorphous network, fillthespacebeneaththebasalmembrane, andthecellsandthe fibrousECMimmersedinthem. Themaincomponentsofgroundsubstancesareproteoglycans,glycoproteins,andhyaluronicacidthatare mostlysynthetizedby fibroblasts[11,13].Different cells,ECMenvironments,andunderlyingtissuesof theskinsublayersareshownin Fig.2.6.
Hypodermis
Thehypodermisisthedeepestlayeroftheskinthatis responsibleforattachingthedermistomusclesand
FIG.2.2
FIG.2.3 Humantissuetypes.
FIG.2.4 Skinfunctions.
bones,housesthebloodvesselsandnerves,andhasa keyroleincontrollingthebodytemperature.Themajor celltypeinthislayerisadipocyte,andthemaincomponentisadiposetissuemadeoftriglyceridethathouses thebodynaturalfat[10].
MUSCLES
Muscleisasoftandspecializedtissue,whichcauses contractingandapplyingforcestovariouspartsofthe body.Therearethreetypesofmuscletissue:skeletal orstriatedmuscle,smoothornonstriatedmuscle,and cardiacmuscle.Fibrousmusclecells,thatis,myocytes,
connecttogetherandformspecializedmuscletissues insheets(cardiacmuscle)and fibers(skeletalmuscles). Whenthereisawound,differenttypesofmuscletissue canbeinjureddependingonthewounddepthand severity,includingunderlyingskeletalmuscle,andthe striatedmusculartissueofthevascularsystem.
SkeletalMuscle
Insomewounds,theskeletalmuscletissueispartially involved.Themostcommoninjuryofmusclesisstrain, atypeofacuteinjurythatoccurstothemuscleor tendon,withadifferentlevelofseverity.Skeletal
FIG.2.5 Anatomyoftheskinanditsunderlyingtissues.
FIG.2.6 DifferentcellsandECMscanbefoundinawoundincludingepidermis,dermis,hypodermis,vessel, muscle,nerve,andlymphaticvessel.
FIG.2.7 Atraumaticwoundwithdamagedmuscle(black arrow)andtendonrapture(yellowarrow).
musclesarerelativelymorevulnerabletoacuteinjuries suchastraumaorburn,duetotheirsuperficiallocation [14]. Fig.2.7 showsatraumaticwoundwithinjured muscle.However,theskeletalmusclecanbedamaged inchronicwoundsduetothehypoxiaandinsufficient bloodsupply.
CONNECTIVETISSUE
Connectivetissueischaracterizedbya fibrousECM, richincollagenandelastin.Thistypeoftissueisfound everywhereinthebodyandcontains fivemajorcell types: fibroblasts,adipocytes,macrophages,mastcells, andendothelialcells.
Whenawoundoccurs,skinasthemostinvolvedorganlosesitsintegrityanditsstructuralframework.In addition,theunderlyingconnectivetissue,thatis, epidermis,adiposetissue,bone,tendon,andfascia (the fibroticmembranethatcoversmuscles,bones, bloodvessels,andnerves)canbedamageddepending ontheextentofinjuryandthesurroundingECMloses itsconsistencyandfunctions[15].
Bone
Boneisatypeofdenseconnectivetissuewithamineralizedporousbutrigidstructure.Fourtypesofcellcan befoundinthebone:osteocytes,osteoblasts,osteoclasts,andboneliningcells.Boneexertsimportant functionsinthebody,suchasmobility,support,and protectionofsoftinternaltissues,calciumandphosphatestorage,andharboringofbonemarrow[16].
Severetraumasorsomethird-degreeburnscancause boneinjuriesorboneexposurewhilediabeticwounds canbediagnosedwiththeexposedboneandosteomyelitis,whichleadtofootamputation,systemic
FIG.2.8 Exposedbonecanbeoccurindifferenttypesofwound (A) atraumaticwoundcausedbycar accident (B) adiabeticfootulcer (C) and (D) aninfectedsurgicalwound.
infection,anddeath.Theexposedbonemaybefound invarioustypesofwound,suchastraumaticwounds, pressureulcers,anddiabeticulcers. Fig.2.8 shows exposedboneinanacutewoundandachroniculcer.
Commonly,thehealthyexposedboneappearsin whiteorpaleyellow.Toavoidtheadverse consequencesoftheexposedbonesuchasnecrosis andinfection,thewoundsurfaceshouldbemoisturized toencouragethegranulationtissueformation,which coverstheexposedbone.Ifthewounddoesnotheal, itisimportanttoruleoutosteomyelitisasacausefor impairedhealing.Ifosteomyelitisisleftwithout
treatment,thewoundclosureisdelayedandincreases theriskofamputationorsystemicinfection[17].
BloodVessels
Therearetwomaintypesofbloodvessels:arteriesand veins,withathickandstrongwallcomposedofconnectivetissueandsmoothmuscle.Theparticularpartofthe vascularsystemassociatedwithskinislocatedinthe dermaldeeplayertoformahorizontalnetworkconsistingoftwointerconnectedplexuses:thesuperficial plexusatthejunctionofthepapillaryandreticular dermiscomposedofpostcapillaryvenulesthatsupplies
(A)(C) (D) (B)
thedermalpapillae.Thedeeperplexusatthedermis hypodermisinterface,whichissuppliedbylargerblood vessels[18].Arterialorvenousdisorderscancause chronicwoundscalledvascularulcers.
LymphaticVessel
Thelymphaticcapillariesareextendedthroughthe postcapillarylymphvesselstothedermalandsubcutaneouslymphvessels,andtheirstructureisnotregular asthatofthebloodvessels.Theendothelialcellsofthe lymphcapillariesarethinandaresurroundedbyloose collagenandelastic fibers.Lymphaticulcerscan developbecauseofdamagetothelymphaticvessels orlymphedema[18].
NERVES
Intheperipheralnervoussystem,abundleofaxons, thatis,nerve,transmitselectrochemicalsignalsfrom axonstotheperipheralorgans.Nervebundleswith microvesselsarefoundinneurovascularbundlesof thedermis.DermalpapillaehousesMeissnercorpuscles,whichenabletouchinthehandsandfeet[18].
Generally,therearethreetypesofnerves:(1)Motor nervessendimpulsesfrombrainandspinalcordto muscles.(2)Thesensorynervestransmittactile,pressure,pain,andtemperaturesensation.(3)Theautonomicnervesareresponsibleforthefunctionof bloodvesselsandsweatglands[13].Inuncontrolled diabetes,autonomicneuropathydestroysthesympatheticcomponentoftheautonomicnervoussystem thatcontrolsvasoconstrictioninperipheralblood vessels[19,20].
Dependingontheextentofinjury,axonsand surroundingconnectivetissuesinnervescanbe damaged.Themostsevererepairableinjuryoccursin thirddegreewounds,wheretheaxonsandinnerlayer ofconnectivetissue(endoneurium)aredamagedwhile theouterthickerlayers(perineuriumandepineurium) remainintact.Inmoreseveredamageswheretheentire connectivetissueisdisrupted, fibroblasts fillthe damagedsiteby fibrousECMthatpreventsthecut axonfromregeneratingandconnectingtotheoriginal nervecell[21].