No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Notice
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds or experiments described herein. Because of rapid advances in the medical sciences, in particular, independent verification of diagnoses and drug dosages should be made. To the fullest extent of the law, no responsibility is assumed by Elsevier, authors, editors or contributors for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Previous editions copyrighted 2016, 2011, 2006, and 2001.
Geoffrey W. Cundiff retains copyright for figures/images in Chapter 120.
Library of Congress Control Number: 2020943813
Senior Content Strategist: Nancy Duffy
Senior Content Development Manager: Laura Schmidt
Publishing Services Manager: Catherine Jackson
Senior Project Manager: Claire Kramer
Design Direction: Margaret Reid Printed in China
This book is dedicated to my wife, Leslie Baggish; to my children, Mindy Baggish, Cindy Baggish, Julia Baggish, and Stuart Baggish; to my daughter-in-law, Pamela Baggish; to my grandchildren, Owen Baggish and Reagan Baggish; to the memory of my deceased son, Jeffrey Baggish; and to the memory of my sisters Rita Baggish Mayers and Francis Baggish Katzman, both of whom were struck down by coronavirus infections.
Michael S. Baggish, MD
This Atlas is dedicated to my wife, Mona; my children, Tamara, Lena, and Summer; and to the memory of my mother and father, Mike and Mary Karram. I have greatly appreciated all of their love, support, and guidance.
Mickey M. Karram, MD
Michael S. Baggish, MD
Mickey M. Karram, MD
CONTRIBUTORS
Brian J. Albers, MD, FACS
Margaret Mary Community Hospital Batesville, Indiana
Michael S. Baggish, MD, FACOG Professor of Obstetrics and Gynecology University of California, San Francisco San Francisco, California
Alfred E. Bent, MD Professor and Head Division of Gynecology IWK Health Center Dalhousie University
Halifax, Nova Scotia, Canada
Lesley L. Breech, MD
Associate Professor Division of Pediatric and Adolescent Gynecology University of Cincinnati Department of Obstetrics and Gynecology
Division Director
Pediatric and Adolescent Gynecology Cincinnati Children’s Hospital Medical Center Cincinnati, Ohio
Karen S. Columbus, MD Cincinnati Breast Surgeons, Inc. Cincinnati, Ohio
Geoffrey W. Cundiff, MD, FACOG, FACS, FRCSC
Head, Department of Obstetrics and Gynecology University of British Columbia Vancouver, British Columbia, Canada
Bradley R. Davis, MD, FACS, FASCRS
Associate Professor of Clinical Surgery Director Division of Education Director
Residency Program in General Surgery University of Cincinnati Cincinnati, Ohio
Roger Dmochowski, MD, FACS Professor of Urology Director, Pelvic Medicine and Reconstruction Fellowship Executive Physician for Safety Vanderbilt University Medical Center Nashville, Tennessee
Ashley M. Eskew, MD, MSCI
Assistant Professor Obstetrics and Gynecology
Reproductive Endocrinology and Infertility
Atrium Health
Charlotte, North Carolina
Tommaso Falcone, MD, FRCSC, FACOG Professor and Chair Obstetrics Cleveland Clinic Cleveland, Ohio
Cecile A. Ferrando, MD, MPH Assistant Professor of Surgery Obstetrics, Gynecology, and Women’s Health Institute Cleveland Clinic Cleveland, Ohio
John B. Gebhart, MD, MS Professor Departments of Obstetrics/Gynecology and Surgery Fellowship Director—Female Pelvic Medicine and Reconstructive Surgery Mayo Clinic Rochester, Minnesota
Audra J. Hill, MD
Fellow in Female Pelvic Medicine and Reconstructive Surgery Cleveland Clinic Cleveland, Ohio
Bradley S. Hurst, MD
Director of Reproductive Endocrinology and Infertility Obstetrics and Gynecology Atrium Health Carolinas HealthCare System Charlotte, North Carolina
Mickey M. Karram, MD Director of Urogynecology The Christ Hospital Clinical Professor of Obstetrics and Gynecology University of Cincinnati Cincinnati, Ohio
David J. Lamon, MD, FACS Naples Surgical Associates Naples, Florida
Michael Maggio, MD, FACS Good Samaritan Hospital Cincinnati, Ohio Dearborn County Hospital Lawrenceburg, Indiana
Javier F. Magrina, MD Professor of Obstetrics and Gynecology
Barbara Woodward Lipps Professor Mayo Clinic Arizona Phoenix, Arizona
Ayman Mahdy, MD, PhD
Associate Professor of Urology
Director of Voiding Dysfunction and Female Urology University of Cincinnati College of Medicine Cincinnati, Ohio
Chad M. Michener, MD
Assistant Professor of Surgery Cleveland Clinic
Obstetrics, Gynecology and Women’s Health Institute Cleveland, Ohio
Robert Neff, MD Division of Gynecologic Oncology TriHealth Cincinnati, Ohio
James Pavelka, MD
Director, Division of Gynecologic Oncology TriHealth Cincinnati, Ohio
W. Stuart Reynolds, MD Instructor in Urology Vanderbilt University Medical Center Nashville, Tennessee
Helmut F. Schellhas, MD
Senior Gynecologic Oncologist
Good Samaritan Hospital
Adjunct Professor Department of Obstetrics and Gynecology University of Cincinnati Medical Center Cincinnati, Ohio
Kevin Schuler, MD
Division of Gynecologic Oncology TriHealth Cincinnati, Ohio
Enrique Soto, MD, MSc
Associate Professor Florida International University Miami, Florida
Donna L. Stahl, MD
Breast Surgeon Private Practice Cincinnati, Ohio
Emanuel C. Trabuco, MD, MS
Assistant Professor of Obstetrics and Gynecology Department of Obstetrics and Gynecology Mayo Clinic Rochester, Minnesota
Mark D. Walters, MD
Professor and Vice Chair, Gynecology Obstetrics, Gynecology, and Women’s Health Institute Cleveland Clinic Cleveland, Ohio
James L. Whiteside, MD, MA, FACOG, FACS
Associate Professor Obstetrics and Gynecology Residency Program Director Department of Obstetrics and Gynecology Division of Female Pelvic Medicine and Reconstructive Surgery University of Cincinnati College of Medicine Cincinnati, Ohio
PREFACE
The Atlas of Pelvic Anatomy and Gynecologic Surgery was first published 20 years ago. The book has been revised according to an approximate 5-year cycle. With the publication of the fifth edition, the authors have followed past precedent by carrying out focused, timely revisions that affect several chapters throughout the book. In addition, new chapters have been added to strengthen the overall scope of the book. We have continued to balance nontediously written descriptions with color illustrations and photographs. Similarly, we continue to develop the art of hybrid technology, which uses actual photographs strategically altered via skilled, computer-generated manipulation. The authors of this atlas are mindful for the reasons behind the book’s existence: (1) All surgery reduced to its lowest common denominator is an anatomic dissection. (2) Surgical operations depend on precise knowledge of anatomic relationships. (3) Lengthy written descriptions of surgical procedures are tiresome when compared with viewing color illustrations and actual photographs. (4) The majority of gynecologists will not perform cadaver dissection beyond their medical school experience. To be remembered, anatomic exercises must demonstrate practical application(s). (5) Successful textbooks are used by a large population of residents, fellows, nurses, practitioners, and faculty as a reference source and as a tool to prepare for upcoming surgical procedures.
The fifth edition is organized by section/chapter and follows a logical plan of anatomy first, followed by a spectrum of operations that are structured, step by step, from beginning to end. Gynecologic operations are shown by abdominal and vaginal approaches, as well as by hysteroscopic, laparoscopic, robotic, and cystoscopic routes. Regardless of the route, a hysterectomy should be performed with the same model and technique. Laparoscopic surgery should mimic laparotomy through the best effort of the surgeon. The logical progression of chapters follows the format in the previous edition, which makes the book easy to navigate. Among the key foundations relative to the aforesaid, high-quality illustrations are the backbone on which this unique textbook rests. Twenty years ago, our artist’s half-tone illustrations, which were showcased in our first edition, eclipsed the rather simple line drawings featured in competing textbooks. Following each subsequent edition, color has
replaced the black-and-white format to the extent of shifting the standard for contemporary illustrations. The wider use of photographs that show cadaver dissections, operative procedures, and autopsies has increased with each subsequent edition and will reach its highest volume in the fifth edition.
The authors of the Atlas of Pelvic Anatomy and Gynecologic Surgery are in fact truly authors, not editors, wherein the latter is characteristic of most other large textbooks. We have personally written the majority of the chapters in the fifth edition. We have carefully selected contributors for the remaining chapters. Only the most knowledgeable and skilled surgeons were invited to participate, with the idea that they would add to the overall quality of the book.
The last four editions of this book have witnessed global appeal. Our goal for this fifth edition is directed toward increasing the interest of domestic, as well as international, audiences. A frequently asked question relates to cost—particularly, why a textbook of this sort is so much more costly than some other surgical textbooks. The greatest costs center around book production and artwork. The former includes editing, production of proofs, design of cover, and layout of interior pages. One of the most critical decisions requires the selection of high-quality paper on which the contents will be printed. As authors, we lobby for high-weight glossy paper that shows our photographs and color illustrations very clearly. A substantial portion of the budget is devoted to artwork, which translates to paying our medical artist, as it is very costly to create the anatomically correct drawings made for this edition. All in all, production is a complex, expensive process.
Finally, creating a book of 1500 pages is akin to a birth process. Following a prolonged gestation, the book comes together as a completed manuscript. The best contributors get their chapters in on time, and the building blocks of completed work will disclose the essence of the future book. The creative spirit of the authors comes to the fore when the book is finally published. Behold our baby is born!
Michael S. Baggish, MD
Mickey M. Karram, MD
ACKNOWLEDGMENTS
First and foremost, the authors wish to thank our artist, Joe Chovan, for his essential contribution to the fifth edition of the Atlas of Pelvic Anatomy and Gynecologic Surgery. In fact, Joe did the excellent illustrations for our preceding four editions. The artwork created by Joe Chovan has established a standard of skill not seen since the time of Frank Netter and Max Brödel.
Drs. Baggish and Karram thank Laura Schmidt and Claire Kramer of Elsevier for their valuable, untiring work relative to the development and production of this fifth edition.
We thank Nancy Anastasi Duffy, senior content strategist at Elsevier, for overseeing the completion of the “atlas.” Finally, the authors wish to recognize Sarah Barth who launched this project of behalf of Elsevier.
PART
1
Principles of Pelvic Anatomy and Gynecologic Surgery, 1
SECTION 1
Pelvic Anatomy, 3
1 Basic Pelvic Anatomy, 5
2 Advanced Pelvic Anatomy, 59
3 Max Brödel’s Pelvic Anatomy, 75
SECTION 2
Basic Foundations for Gynecologic Surgery, 95
4 Instrumentation, 97
5 Suture Material, Suturing Techniques, and Knot Tying, 111
6 Energy Devices, 131
7 Positioning and Nerve Injury, 143
PART 2
Abdominal Surgery, 157
SECTION 3
Anterior Abdominal Wall, 159
8 Anatomy of the Lower Abdominal Wall, 161
9 Abdominal Incisions, 171
SECTION 4
Uterus, 183
10 Intra-abdominal Pelvic Anatomy, 185
11 Dilatation and Curettage, 211
12 Foundations of Laparoscopy, 219
13 Abdominal Hysterectomy, 231
14 Radical Hysterectomy, 265
15 Endometrial Carcinoma With Lymph Node Sampling, 281
16 Myomectomy, 283
17 Surgical Treatment of Unusual Myoma Conditions, 293
18 Unification of Bicornuate Uterus, 297
SECTION 5
Abdominal Surgery During Pregnancy, 305
19 Abdominal Cerclage of the Cervix Uteri, 307
20 Cesarean Section, 311
21 Cesarean Section Hysterectomy, 319
22 Hypogastric Artery Ligation, 323
23 Trophoblastic Disease, 325
SECTION 6
Adnexa, 335
24 Ovarian Cystectomy and Cystotomy, 337
25 Surgery for Pyosalpinx, Tubo-ovarian Abscess, and Pelvic Abscess, 343
26 Adhesiolysis, 349
27 Surgical Management of Pelvic Endometriosis, 357
28 Surgical Management of Ectopic Pregnancy, 365
29 Surgical Management of Ovarian Residual and Remnant, 377
30 Ovarian Tumor Debulking, 379
31 Tuboplasty, 383
32 Tubal Sterilization, 389
SECTION 7
Retropubic Space, 399
33 Anatomy and Surgical Exposure of the Retropubic Space, 401
34 Retropubic Urethropexy for Stress Incontinence and Retropubic Paravaginal Repair, 419
SECTION 8
Retroperitoneum and Presacral Space, 431
35 Anatomy of the Retroperitoneum and the Presacral Space, 433
36 Identifying and Avoiding Ureteral Injury, 449
37 Presacral Neurectomy, 463
38 Uterosacral Nerve Transection, 469
39 Lymph Node Sampling, 473
SECTION 9
Abdominal Operations for Enterocele and Vault Prolapse, 479
40 Native Tissue Suture Repair of Vaginal Vault Prolapse: Laparoscopic, Robotic, and Open Abdominal Approaches, 481
41 Abdominal Sacral Colpopexy and Colpohysteropexy, 489
PART 3
Cervical, Vaginal, Vulvar Surgery, 503
SECTION 10
Cervical Surgery, 505
42 Anatomy of the Cervix, 507
43 Colposcopy of the Cervix, 513
44 Conization of the Cervix, 529
45 Cervical Polypectomy, 543
46 Relief of Cervical Stenosis, 547
47 Cervical Cerclage, 551
48 Cervical Stump Excision (Trachelectomy), 557
SECTION 11
Vaginal Surgery, 565
49 Anatomy of the Vagina, 567
50 Anatomy of the Support of the Anterior and Posterior Vaginal Walls, 585
51 Vaginal Hysterectomy, 595
52 Native Tissue Vaginal Repair of Cystocele, Rectocele, and Enterocele, 623
110 Pelvic Anatomy From the Laparoscopic View, 1277
111 The Operating Room Suite and Instrumentation, 1283
112 Trocar Placement, 1285
113 Diagnostic Laparoscopy, 1293
114 Laparoscopic Hysterectomy, 1297
115 Laparoscopic Adnexal Surgery, 1305
116 Laparoscopic Surgery for Stress Urinary Incontinence (Burch Colposuspension), 1313
117 Laparoscopic Surgery for Pelvic Organ Prolapse, 1317
118 Robotic Surgery in Gynecology, 1321
119 Major Complications Associated With Laparoscopic Surgery, 1333
SECTION 19
Cystourethroscopy, 1371
120 Cystourethroscopy, 1373
PART 6
Surgery for Transgender Conditions, 1403
SECTION 20
Surgery for Transgender Conditions, 1405
121 Surgery for Transgender Conditions, 1407
VIDEO CONTENTS
Fresh Cadaver Dissection
Video 1 Anatomy of Posterior Vaginal Wall
Mickey M. Karram, MD
Video 2 Abdominal Wall
Video 3
Michael S. Baggish, MD
Intra-abdominal and Retroperitoneal Anatomy
Michael S. Baggish, MD
Video 4 Obturator Fossa Dissection
Michael S. Baggish, MD
Video 5 Pelvic Veins
Michael S. Baggish, MD
Video 6 Presacral Space
Michael S. Baggish, MD
Video 7 Right Retroperitoneal Space and Right Ureter Dissection
Michael S. Baggish, MD
Video 8 Left Ureter Dissection
Michael S. Baggish, MD
Video 9 Anatomy of Anterior Vaginal Wall
Mickey M. Karram, MD
Video 10 Hypogastric Plexus
Michael S. Baggish, MD
Video 11 Hypogastric Vessels
Michael S. Baggish, MD
Video 12 Perineum and Lower Vagina
Michael S. Baggish, MD
Video 13 Perineum and Anal Sphincter
Michael S. Baggish, MD
Video 14 Retropubic Space
Michael S. Baggish, MD
Fixed Cadaver Dissection
Video 15 Left Retroperitoneum Dissection
Michael S. Baggish, MD
Video 16 Femoral Triangle Dissection
Michael S. Baggish, MD
Video 17 Right Retroperitoneal Dissection
Michael S. Baggish, MD
Video 18 Presacral Space and Psoas/Iliacus Dissection
Michael S. Baggish, MD
Video 19 Deep Dissection Right Ureter
Michael S. Baggish, MD
Video 20 Deep Dissection of Left Ureter
Michael S. Baggish, MD
Video 21 Retroperitoneum
Michael S. Baggish, MD
Video 22 Hypogastric Nerve Plexus
Michael S. Baggish, MD
Video 23 Left Retroperitoneal Dissection
Michael S. Baggish, MD
Video 24 Ureter at Broad Ligament
Michael S. Baggish, MD
CHAPTER
Basic Pelvic Anatomy
Michael S. Baggish
The anatomy taught in this book is based on actual cadaveric dissection. This section consists entirely of color drawings constructed from anatomic models (cadavers). This section was added to help the reader orient the dissection photographs to the overall geography of abdomen, pelvis, breasts, and extremities. In several pictures, our artist has used actual photographs of body parts (pelvic bone) into which muscles and ligaments were sketched with a computer.
The following terms are used in this section to provide directive relationships: (1) cranial = toward the head; (2) caudal = toward the foot; (3) superior = above; (4) inferior = below; (5) deep = to the interior; (6) superficial = to the surface; (7) medial = toward the midline; (8) lateral = toward the side; (9) beneath = under; (10) anterior = to the belly; and (11) posterior = to the back.
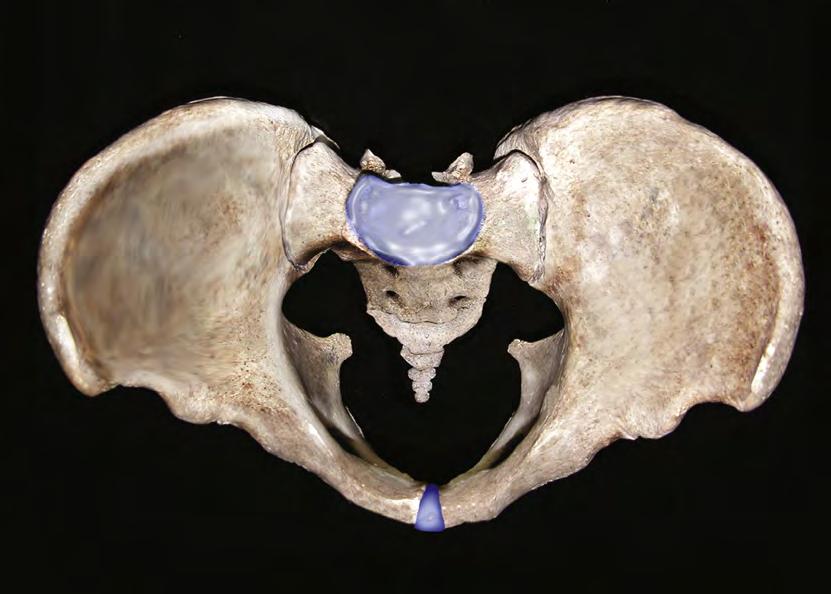
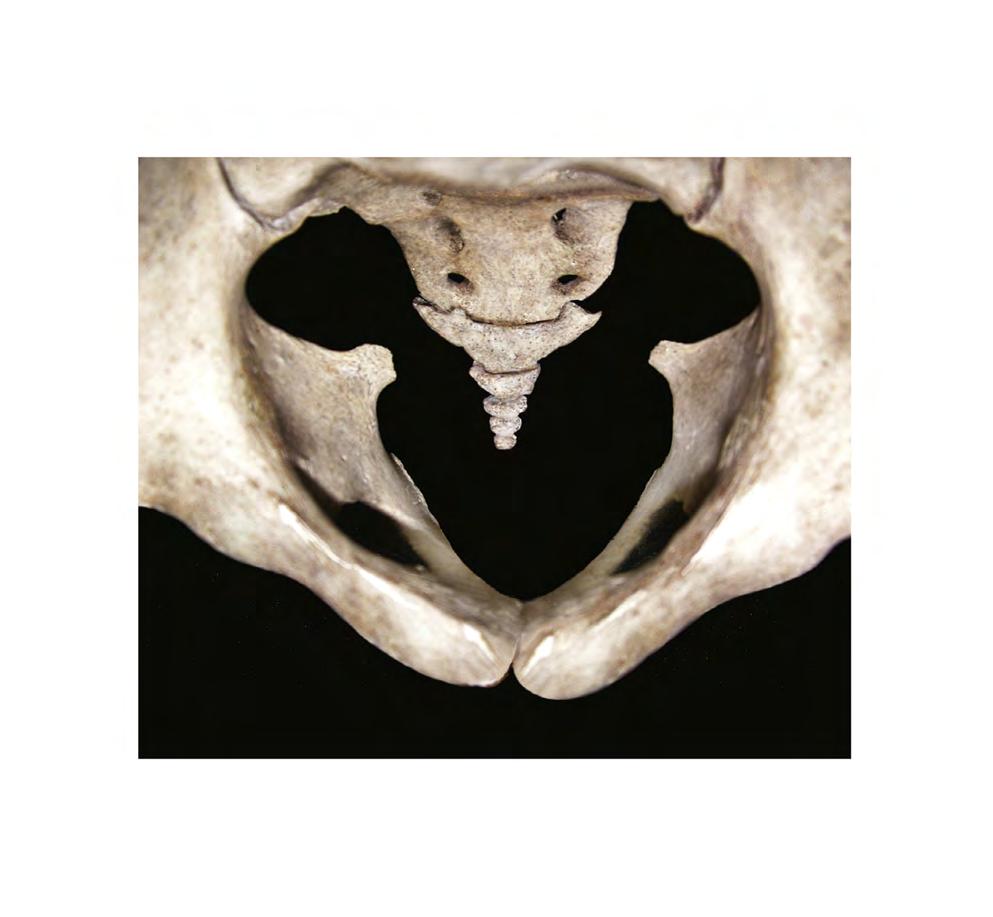
The surgeon needs to be familiar with certain bony landmarks. The pelvic bones consist of the sacrum and coccyx, the ilium, the pubic bone, and the ischium (Fig. 1.1). The first anterior projection of the sacral vertebra is the sacral promontory, and the exaggerated transverse processes form the sacral ala (Fig. 1.2). On both anterior and posterior surfaces are the holes, or foramina, from which nerve roots exit. Articulating with the last sacral vertebra is the coccyx (Fig. 1.3). When the pelvis is observed from above (see Fig. 1.2), the iliac fossa, iliac crest, and anterior superior iliac spine are prominent. The articulations at the sacroiliac joint and the symphysis pubis mark major posterior and anterior joints, respectively. Between the two are the iliopectineal lines and the linea terminalis. Facing the pelvis, the anterior superior iliac spine and the pubic tubercle mark the boundaries of the inguinal ligament. The two pubic bones form an arch beneath the symphysis pubis. The rhomboid space between ischial and pubic bones is the obturator foramen (see Fig. 1.1). The lowest portion of the ischium forms a broad, rounded accumulation of bone referred to as the ischial tuberosity. Above that structure is a hemispheric socket (acetabulum), where the head of the femur articulates (see Fig. 1.1).
When one faces the back of the pelvis, the sacrum and the sacral canal are visible. The ischial tuberosity, ischial spines, and greater and lesser sacral sciatic notches are identified (Fig. 1.4). From the side, the iliac crest, ischial tuberosity, ischial spine, greater sciatic notch, and lesser sciatic notch are seen, as is the obturator foramen (Fig. 1.5).
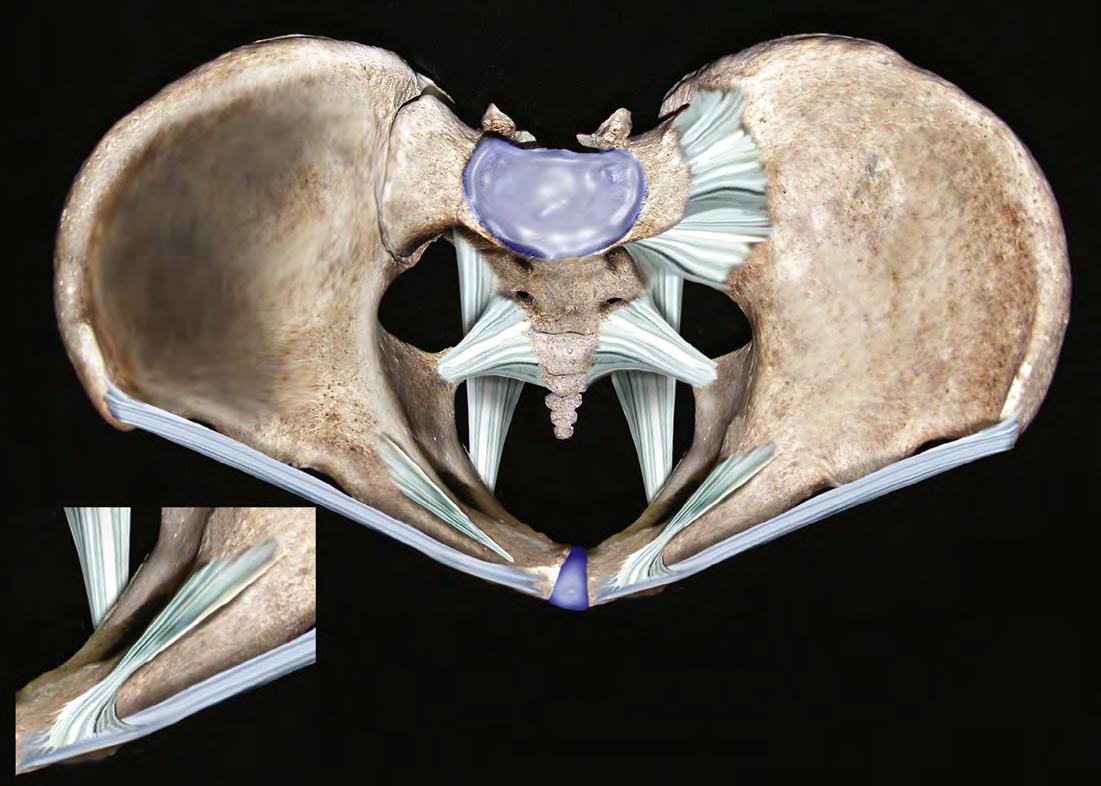
The following ligamentous structures can be observed: Cooper’s ligaments, the sacroiliac ligaments, the symphysis fibrocartilage, the sacrospinous and sacrotuberous ligaments, the inguinal ligament, the lacunar ligament, and the obturator membrane (Figs. 1.6 through 1.8). The sacrospinous and
Cooper’s ligaments are utilized in pelvic reconstructive surgery, as are the pubic symphysis and the anterior longitudinal ligament (overlying the anterior sacral surface, not sketched). Large vessels and nerves cross from the abdomen to the thigh beneath the inguinal ligament and through the obturator foramen. The lacunar ligament forms the medial abutment of the femoral canal and sometimes is referred to as the pectineal portion, or extension, of the inguinal ligament.
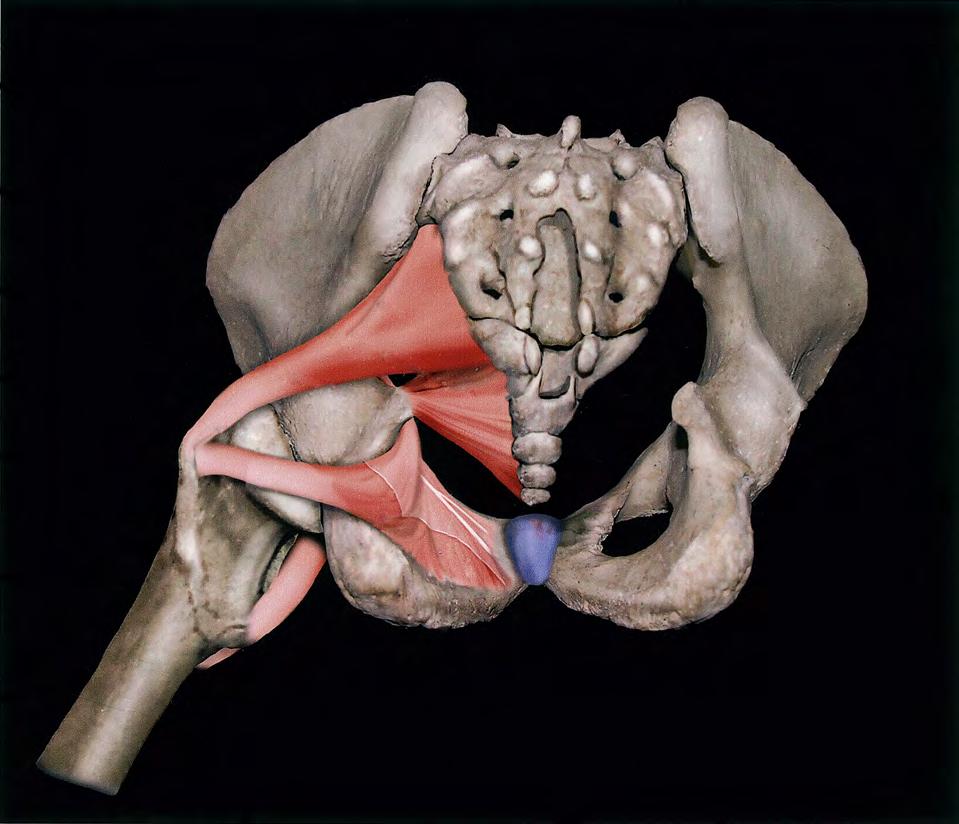
The muscles of the pelvis that have practical and special importance for our discussion are the obturator internus muscle, which constitutes the “pelvic side wall” or “ovarian fossa,” the coccygeus, the piriformis, and the levator ani muscles (Fig. 1.9).
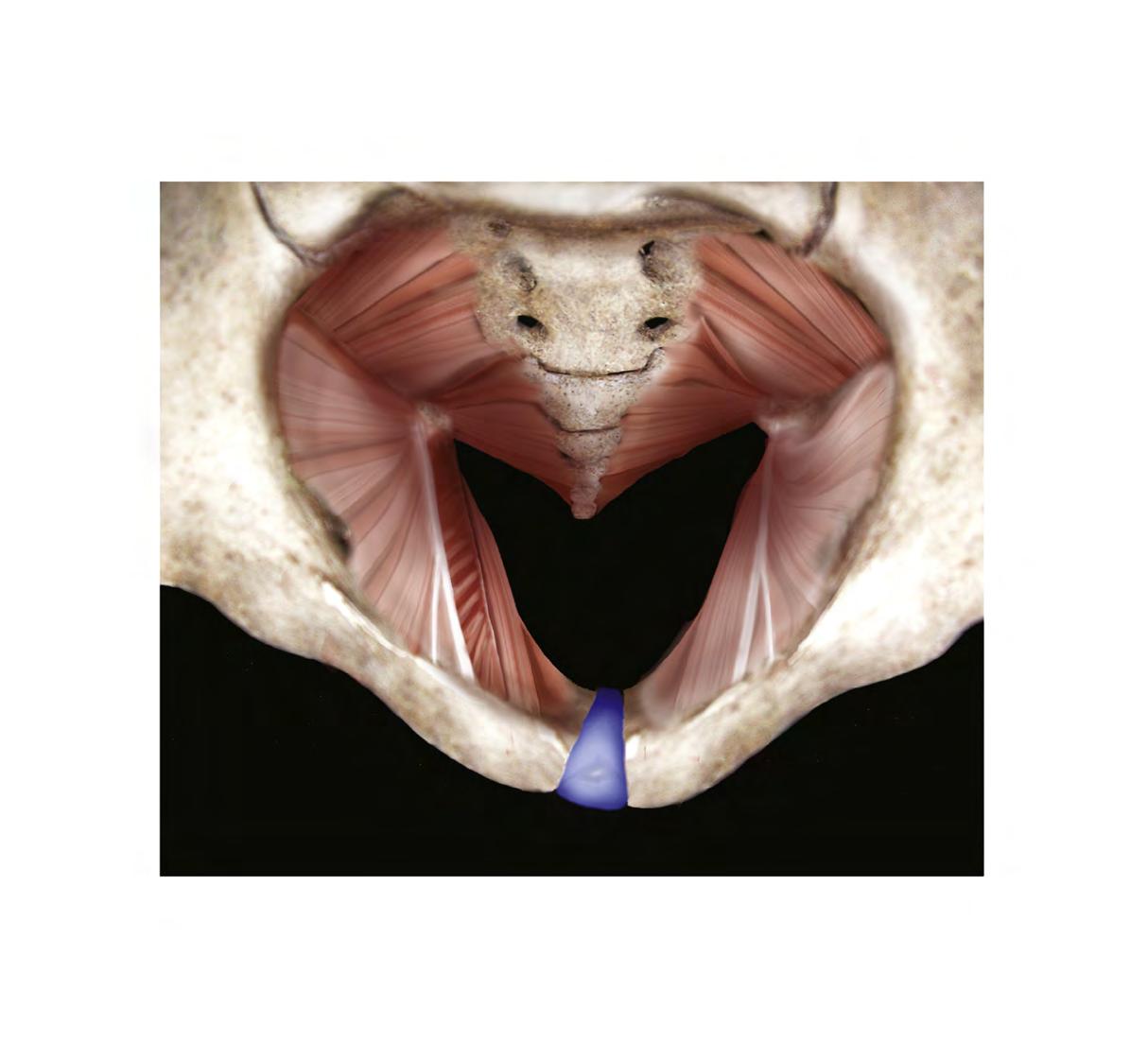
The obturator fascia is a well-defined, tough structure. A particularly thickened portion of the obturator fascia is named the arcus tendineus, or white line (Fig. 1.10). The line stretches from the inner aspect of the ischial spine across the belly of the obturator internus muscle and terminates at the lower margin of the posterior pubic bone (Fig. 1.11).
The levator ani muscle takes its origin from the inferior margin of the pubic bone and the entire arcus (obturator fascia). Several anatomy texts have divided the levator into anterior and posterior portions; however, these subdivisions are artificial and have little practical value (Fig. 1.12). Functionally, the gynecologist can feel this muscle contract by performing a rectovaginal examination and requesting the patient to tighten her muscles as if holding in a bowel movement. At a point 2 cm up (cranial) from the vaginal introitus, the U-shaped muscle is felt along the side and posterior vaginal walls. A similar contraction can be felt posterior to the rectum when the anal sphincter is contracted. Insofar as the rectum is concerned, the levator component can be palpated across the posterior rectal wall. The levator ani, in concert with the external sphincter ani, squeezes the rectum to narrow the bowel lumen while elevating the anorectum.
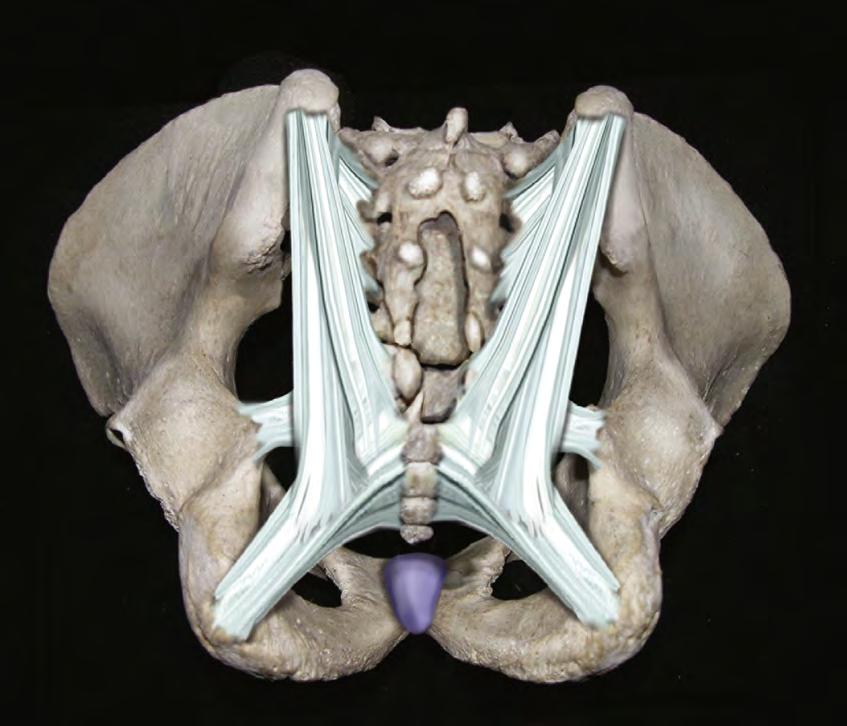
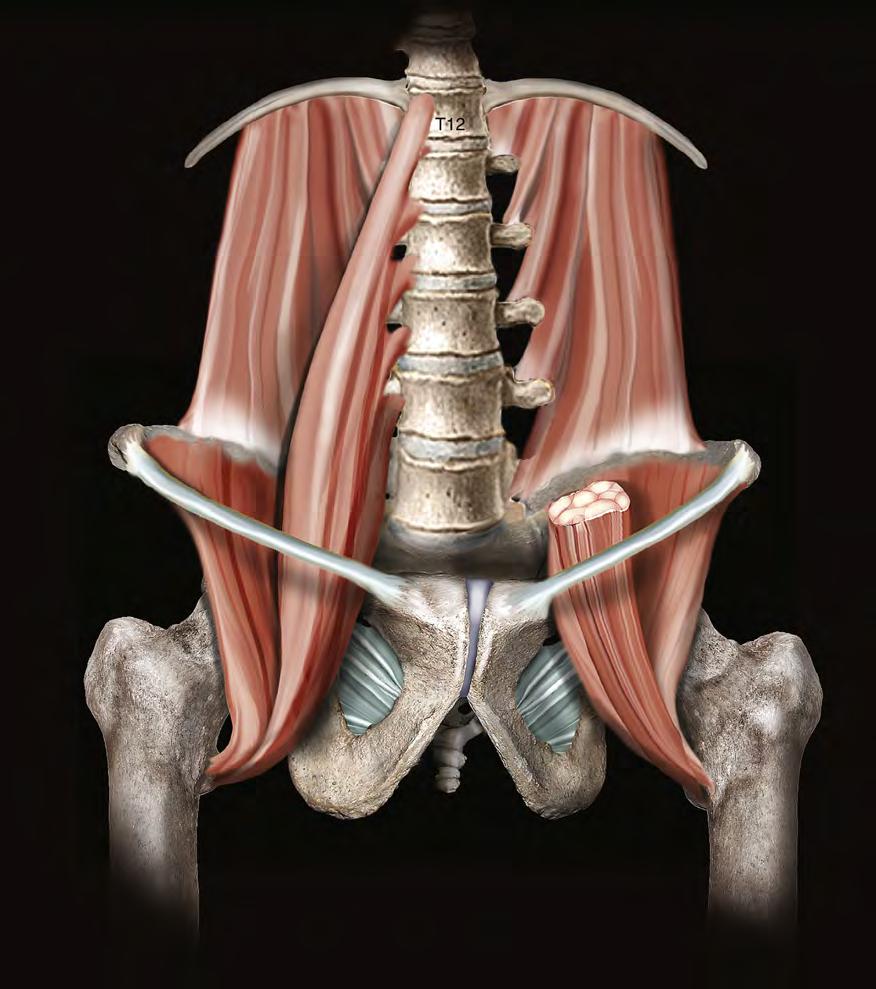
The muscles and ligaments divide notches into windows (foramina). The coccygeus is overlain (deep) by the sacrospinous ligament. The piriformis muscle exits the pelvis via the greater sciatic foramen and is partially overlain (deep) by the sacrotuberous ligament (see Figs. 1.7 through 1.9). Internally, the hollow iliac fossa is covered by the iliacus muscle. At the medial margin and slightly superficial to the iliacus muscles are the psoas major muscles. Together with the iliacus (iliopsoas), the psoas major muscles pass into the thigh beneath the inguinal ligament to insert on the femur (lesser trochanter). Occasionally, the psoas minor tendon may be seen on the anterior surface of the psoas major muscle (Fig. 1.13).
Text continues on page 16
Pubis Ilium
Obturator foramen
Symphysis pubis
1.1 The pelvic bone consists of the ilium, ischium, and pubis. The ilium is bound to the sacrum at the sacroiliac joints. This anterior aspect of the pelvis shows the pubic arch, symphysis, and obturator foramen via a head-on view.
pubis
Pubic tubercle
Anterior superior iliac spine Acetabulum
Ischial spine
Ischial tuber
Pubic arch
Ischium
FIG.
First sacral vertebrae
Ischial spine
Iliac fossa
Symphysis
Iliopectineal line
Pubic tubercle
Ala
Iliac crest
Sacral promontory
Anterior sacral foramen
Anterior superior iliac spine
Coccyx Linea terminalis
FIG. 1.2 This overhead view details the pelvic inlet, which is bounded anteriorly by the pubic symphysis and the pubic tubercle; laterally by the iliopectineal line and the linea terminalis; and posteriorly by the sacral alae and the first sacral vertebra. This view also nicely shows the ischial spines.
Anterior sacral foramen
1.3 High-power detail viewed through the pelvic inlet shows the sacrum and coccyx. The anterior sacral foramina are distinct, as are the ischial spines and the subpubic arch.
Sacral promontory
Ischial spine
Subpubic arch
Symphysis
Iliopectineal line
Pubic tubercle
Linea terminalis
FIG.
Pubic ramus
Posterior superior iliac spine
Sacral hiatus
Ischial ramus
Symphysis pubis
Ischial spine
Posterior sacral foramen
Sacrosciatic notch
Ischial tuber
Sacrum
Coccyx
Sacral canal
FIG. 1.4 The posterior view of the pelvis is combined with an outlet “looking-in” perspective. The ischial tuberosity, ischial spine, and greater and lesser sacrosciatic notches are best seen from this vantage point. Posterior sacrum highlights include the sacral hiatus, sacral canal, and posterior sacral foramina.
Pubic ramus
Anterior superior iliac spine
Acetabulum
Ischial ramus
Ischial tuberosity
Ischial spine
Obturator foramen
Greater sciatic notch
Lesser sciatic notch
Sacrum
Ilium
FIG. 1.5 This right lateral view depicts the acetabulum, sacrosciatic notches, anterior superior iliac spine, and ischium.
Ischial spine
Iliac crest
Anterior superior iliac spine
Sacrum Sacrospinous ligament
Sacroiliac ligament
Sacrotuberous ligament Lacunar ligament
Iliopectineal line
Inguinal ligament Cooper's ligament
FIG. 1.6 The inguinal ligament stretches between the anterior superior iliac spine and the pubic tubercle. From the latter is reflected the lacunar ligament, which forms the medial boundary of the femoral canal. Cooper’s ligament is a stout structure that clings to the iliopectineal line (see inset). Between the ischial spines and the lateral aspect of the sacrum is the sacrospinous ligament. This ligament also creates the greater and lesser sacrosciatic foramina.
Posterior sacroiliac ligament
Posterior sacrococcygeal ligament
Sacrotuberous ligament
Acetabular labrum
Fat in acetabular fossa
Ligament of head of femur (cut)
Obturator membrane
Transverse acetabular ligament
Sacrospinous ligament
Articular cartilage
FIG. 1.7 This side view displays the obturator membrane, as well as the sacrotuberous ligament. The latter begins on the ischial tuberosity and terminates on the lateral margin of the sacrum.
Piriformis muscle
Coccygeus muscle
Ischial spine
Head of femur bone
Cut edge of obturator internus fascia
Greater trochanter of femur bone
White line
Obturator internus muscle
Tendon of lliopsoas muscle
Lesser trochanter of femur bone
Posterior sacroiliac ligament
Sacrospinous ligament
Sacrotuberous ligament
FIG. 1.8 Posterior view combined with outlet view. The sacrotuberous ligament and the sacrospinous ligament cross.
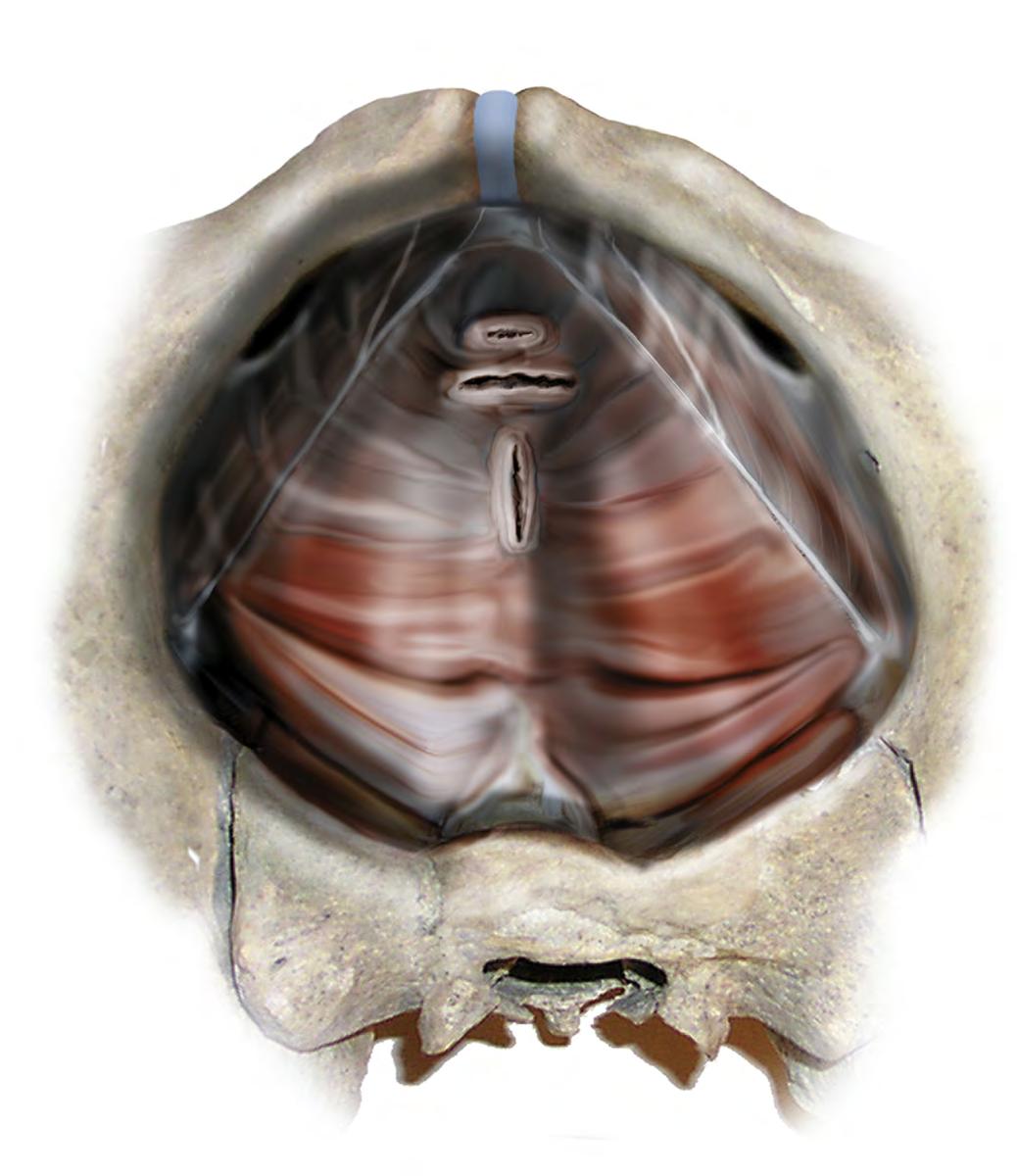
FIG. 1.9 The ligaments have been eliminated. Views are through the pelvic outlet. The obturator internus, piriformis, and coccygeus are seen in sharp detail.
Piriformis muscle
Coccygeus muscle
Obturator internus muscle with fascia
Obturator foramen
Cut edge of levator ani muscle
White line
internus muscle
internus without fascia
1.10 The large obturator internus muscle covered with tough obturator fascia forms the pelvic sidewall. The arcus tendineus, or white line, is produced by a thickened area of obturator fascia. The levator ani muscle arises from the arcus. The cut edge of the levator is shown on the patient’s right side (viewer’s left side). The left levator has been removed. The enclosure of the pelvis is completed by the piriformis and coccygeus muscles.
Obturator
Obturator
FIG.
Coccygeus muscle
Piriformis muscle
Levator ani muscle
Arcus tendineus of levator ani muscle
Symphysis pubis
Iliopectineal line
Vagina
Rectum
Urethra
Obturator internus muscle
Obturator foramen
FIG. 1.11 This view shows the intact levator ani muscle arising along the length of the arcus tendineus. Note the exposed retropubic space, together with the cut edges of the urethra and vagina.
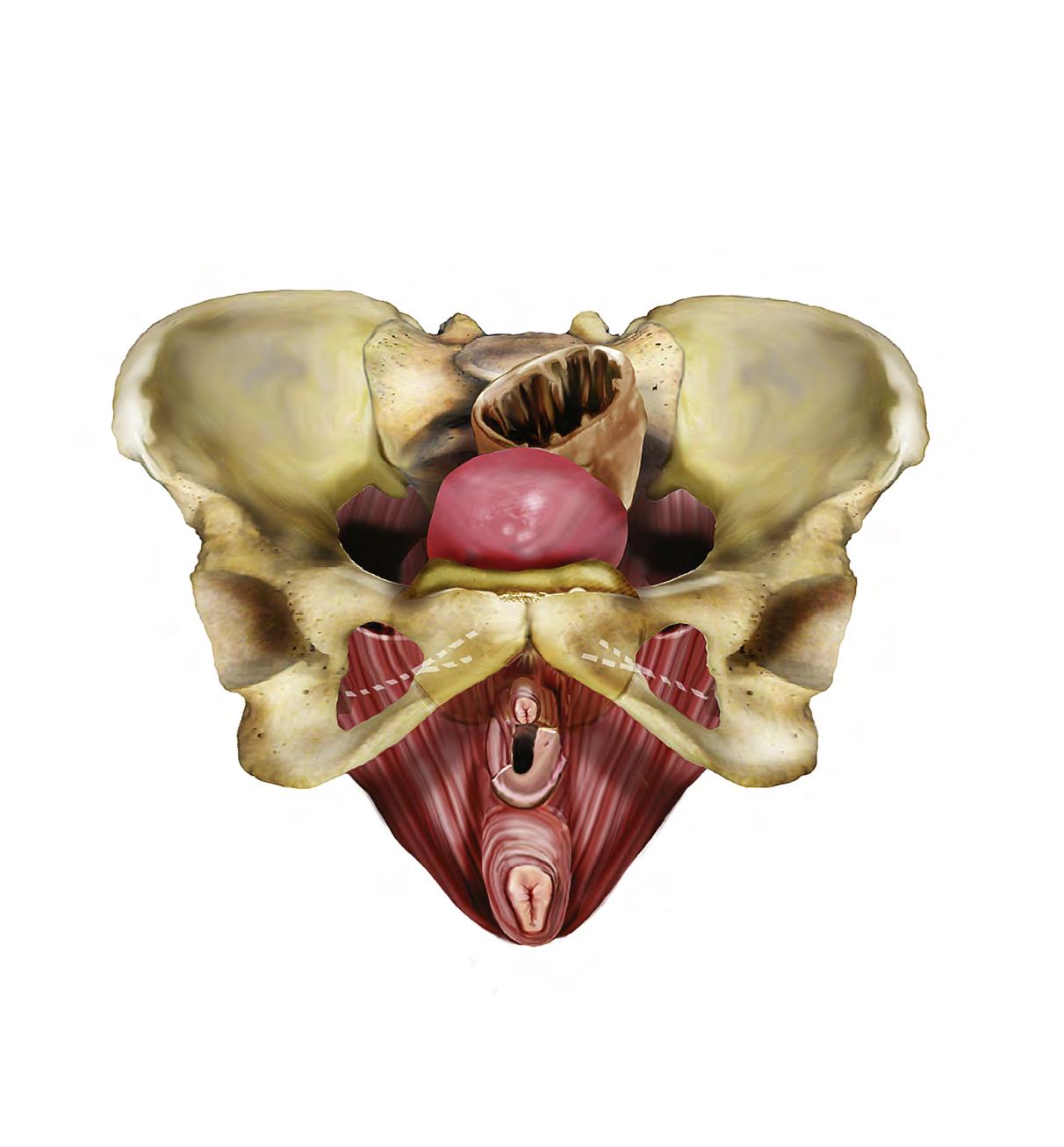
Frontal view of the funnel-like levator ani and its relationship to the vulva and superficial muscles of the perineum. The levator arises in part from the inferior margins of the pubic bone. The artist has superimposed the arcus tendineus (dashed white line) onto the obturator internus and pubic bone.
Rectum
Obturator internus muscle
Ischial spine
Levator ani muscle
Uterus
Bladder
Sigmoid colon
Vagina
Urethra
Piriformis muscle
Arcus tendineus fasciae pelvis (white line)
Anal sphincter
FIG. 1.12
Quadratus lumborum muscle
Psoas major muscle
Iliacus muscle
Inguinal ligament
Psoas major (cut)
12th rib
Obturator membrane
Lesser trochanter of femur
Iliopsoas muscle
FIG. 1.13 The large muscles of the retroperitoneum include the psoas major muscle, iliacus muscle, and quadratus lumborum muscle. The psoas and iliacus (iliopsoas) depart the abdomen and enter the thigh beneath the inguinal ligament.