https://ebookmass.com/product/advances-in-oral-and-
Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
Contemporary Oral and Maxillofacial Surgery 7th Edition
https://ebookmass.com/product/contemporary-oral-and-maxillofacialsurgery-7th-edition/
ebookmass.com
Fundamentals on Oral and Maxillofacial Surgery Divya Mehrotra
https://ebookmass.com/product/fundamentals-on-oral-and-maxillofacialsurgery-divya-mehrotra/
ebookmass.com
Orthodontics for the Oral and Maxillofacial Surgery
Patient 1st Edition Michael R. Markiewicz
https://ebookmass.com/product/orthodontics-for-the-oral-andmaxillofacial-surgery-patient-1st-edition-michael-r-markiewicz/
ebookmass.com
(eTextbook PDF) for Global Banking 3rd Edition by Roy C. Smith
https://ebookmass.com/product/etextbook-pdf-for-global-banking-3rdedition-by-roy-c-smith/
ebookmass.com
The British Newspaper Industry: The Future of the Regional Press John Hill (Auth.)
https://ebookmass.com/product/the-british-newspaper-industry-thefuture-of-the-regional-press-john-hill-auth/
ebookmass.com
The Oxford Handbook of Experimental Syntax Jon Sprouse
https://ebookmass.com/product/the-oxford-handbook-of-experimentalsyntax-jon-sprouse/
ebookmass.com
Saddled with Murder Eileen Brady
https://ebookmass.com/product/saddled-with-murder-eileen-brady-2/
ebookmass.com
Program Evaluation for Social Workers: Foundations of Evidence Based Programs 7th Edition, (Ebook PDF)
https://ebookmass.com/product/program-evaluation-for-social-workersfoundations-of-evidence-based-programs-7th-edition-ebook-pdf/
ebookmass.com
Financial Accounting, 11e ISE 11th/ISE Edition Robert Libby
https://ebookmass.com/product/financial-accounting-11e-ise-11th-iseedition-robert-libby/
ebookmass.com
Precarious Ties: Business and the State in Authoritarian
https://ebookmass.com/product/precarious-ties-business-and-the-statein-authoritarian-asia-meg-rithmire-2/
ebookmass.com
ELSEVIER
1600JohnF.KennedyBoulevard Suite1800 Philadelphia,Pennsylvania,19103-2899
http://www.oralmaxsurgery.theclinics.com
ORALANDMAXILLOFACIALSURGERYCLINICSOFNORTHAMERICAVolume31,Number4 November2019ISSN1042-3699,ISBN-13:978-0-323-70898-2
Editor:JohnVassallo; j.vassallo@elsevier.com
DevelopmentalEditor:LauraFisher
ª 2019ElsevierInc.Allrightsreserved.
ThisperiodicalandtheindividualcontributionscontainedinitareprotectedundercopyrightbyElsevier,andthefollowingterms andconditionsapplytotheiruse:
Photocopying
Singlephotocopiesofsinglearticlesmaybemadeforpersonaluseasallowedbynationalcopyrightlaws.Permissionofthe Publisherandpaymentofafeeisrequiredforallotherphotocopying,includingmultipleorsystematiccopying,copyingfor advertisingorpromotionalpurposes,resale,andallformsofdocumentdelivery.Specialratesareavailableforeducational institutionsthatwishtomakephotocopiesfornon-profiteducationalclassroomuse.Forinformationonhowtoseekpermission visit www.elsevier.com/permissions orcall:(144)1865843830(UK)/(11)2152393804(USA).
DerivativeWorks
Subscribersmayreproducetablesofcontentsorpreparelistsofarticlesincludingabstractsforinternalcirculationwithintheir institutions.PermissionofthePublisherisrequiredforresaleordistributionoutsidetheinstitution.PermissionofthePublisheris requiredforallotherderivativeworks,includingcompilationsandtranslations(pleaseconsult www.elsevier.com/permissions).
ElectronicStorageorUsage
PermissionofthePublisherisrequiredtostoreoruseelectronicallyanymaterialcontainedinthisperiodical,includinganyarticleor partofanarticle(pleaseconsult www.elsevier.com/permissions).Exceptasoutlinedabove,nopartofthispublicationmaybereproduced,storedinaretrievalsystemortransmittedinanyformorbyanymeans,electronic,mechanical,photocopying,recording orotherwise,withoutpriorwrittenpermissionofthePublisher.
Notice
NoresponsibilityisassumedbythePublisherforanyinjuryand/ordamagetopersonsorpropertyasamatterofproducts liability,negligenceorotherwise,orfromanyuseoroperationofanymethods,products,instructionsorideascontainedin thematerialherein.Becauseofrapidadvancesinthemedicalsciences,inparticular,independentverificationofdiagnoses anddrugdosagesshouldbemade.
Althoughalladvertisingmaterialisexpectedtoconformtoethical(medical)standards,inclusioninthispublicationdoesnot constituteaguaranteeorendorsementofthequalityorvalueofsuchproductoroftheclaimsmadeofitbyitsmanufacturer. OralandMaxillofacialSurgeryClinicsofNorthAmerica (ISSN1042-3699)ispublishedquarterlybyElsevierInc.,360Park AvenueSouth,NewYork,NY10010-1710.MonthsofissueareFebruary,May,August,andNovember.BusinessandEditorial Offices:1600JohnF.KennedyBlvd.,Suite1800,Philadelphia,PA19103-2899.PeriodicalspostagepaidatNewYork,NYand additionalmailingoffices.Subscriptionpricesare$401.00peryearforUSindividuals,$720.00peryearforUSinstitutions, $100.00peryearforUSstudentsandresidents,$474.00peryearforCanadianindividuals,$863.00peryearforCanadian institutions,$520.00peryearforinternationalindividuals,$863.00peryearforinternationalinstitutionsand$235.00peryear forCanadianandforeignstudents/residents.Toreceivestudent/residentrate,ordersmustbeaccompaniedbynameor affiliatedinstitution,dateofterm,andthe signature ofprogram/residencycoordinatoroninstitutionletterhead.Orderswill bebilledatindividualrateuntilproofofstatusisreceived.Foreignairspeeddeliveryisincludedinall Clinics subscriptionprices. Allpricesaresubjecttochangewithoutnotice. POSTMASTER: Sendaddresschangesto OralandMaxillofacialSurgery ClinicsofNorthAmerica, ElsevierPeriodicals CustomerService,11830WestlineIndustrialDrive,St.Louis,MO63146. Tel:1-800-654-2452(U.S.andCanada);314-447-8871(outsideU.S.andCanada).Fax:314-447-8029.E-mail: journals customerservice-usa@elsevier.com (forprintsupport); journalsonlinesupport-usa@elsevier.com (foronlinesupport)
Reprints. Forcopiesof100ormore,ofarticlesinthispublication,pleasecontacttheCommercialReprintsDepartment,Elsevier Inc.,360ParkAvenueSouth,NewYork,NY10010-1710.Tel.:212-633-3874;Fax:212-633-3820;Email: reprints@elsevier.com OralandMaxillofacialSurgeryClinicsofNorthAmerica iscoveredin MEDLINE/PubMed (IndexMedicus), ScienceCitationIndex Expanded(SciSearch ), JournalCitationReports/ScienceEdition,and CurrentContents /ClinicalMedicine PrintedintheUnitedStatesofAmerica.
Contributors
CONSULTINGEDITOR
RUIP.FERNANDES,MD,DMD,FACS, FRCS(Ed)
ClinicalProfessorandChief,DivisionofHead andNeckSurgery,DepartmentsofOraland MaxillofacialSurgery,Neurosurgery,and OrthopaedicSurgeryandRehabilitation, UniversityofFloridaHealthScienceCenter, UniversityofFloridaCollegeofMedicine, Jacksonville,Florida,USA
EDITORS
JOSEM.MARCHENA,DMD,MD,FACS
AssociateProfessor,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Chiefof OralandMaxillofacialSurgery,BenTaub Hospital,Houston,Texas,USA
JONATHANW.SHUM,DDS,MD,FACS, FRCD(C)
AssociateProfessor,FellowshipDirector, MaxillofacialOncologyandMicrovascular Reconstruction,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Houston, Texas,USA
JONATHONS.JUNDT,DDS,MD,FACS
AssistantProfessor,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Houston, Texas,USA
AUTHORS
DAVIDY.AHN,DMD
OralandMaxillofacialSurgeon,DavidGrant USAFMedicalCenter,Fairfield,California, USA;UnitedStatesAirForce,FormerFellow EndoscopicMaxillofacialSurgery, MassachusettsGeneralHospital,Boston, Massachusetts,USA
DAVIDALFI,DDS,MD
AttendingSurgeon,DepartmentofOral andMaxillofacialSurgery,Houston MethodistHospital,Houston,Texas,USA; AssociateProfessorofClinicalOraland MaxillofacialSurgery,WeillCornellMedical College,NewYork,NewYork,USA
JONATHANALFI,MA
ProjectSpecialist,SurgicalPlanning Laboratory,DepartmentofOraland MaxillofacialSurgery,HoustonMethodist ResearchInstitute,Houston,Texas,USA
SHAHIDAZIZ,DMD,MD
Professor,DepartmentofOraland MaxillofacialSurgery,RutgersSchoolof DentalMedicine,Newark,NewJersey, USA
JAMESBAKER,DDS
Founder,OMSPartners,Houston,Texas, USA
CALEBBLACKBURN,DDS
DepartmentofOralandMaxillofacialSurgery, TheUniversityofTennesseeMedicalCenter, Knoxville,Tennessee,USA
MATTHEWJ.BREIT,DMD
Resident,DepartmentofOralandMaxillofacial Surgery,TheUniversityofTexasHealth ScienceCenteratHouston,Houston,Texas, USA
KAMALF.BUSAIDY,BDS(Lond),FDSRCS (Eng),FACS
Professor,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Houston, Texas,USA
MARCUSCOUEY,DDS,MD
SurgicalFellow,HeadandNeckOncologicand MicrovascularReconstructiveSurgery, ProvidencePortlandMedicalCenter,Portland, Oregon,USA
NAGIDEMIAN,DDS,MD,FACS
Professor,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Houston, Texas,USA
YIDENG,MD
AssistantProfessor,Departmentof AnesthesiologyandCriticalCareMedicine, BaylorCollegeofMedicine,Houston,Texas, USA
JAGTARDHANDA,BSc(Hons),BDS,MFDS RCS(Eng),MBBS,MRCS(Eng), FRCS(OMFS),PhD
SeniorConsultant,Maxillofacial/Headand NeckSurgery,QueenVictoriaHospital,East Grinstead,UnitedKingdom
ROBERTEMERYIII,DDS
PrivatePractice,CapitalCenterforOral andMaxillofacialSurgery,Washington,DC, USA
MOHAMEDA.HAKIM,DDS
EndoscopicMaxillofacialSurgery
Fellow,DepartmentofOralandMaxillofacial Surgery,MassachusettsGeneral Hospital,Instructor,HarvardSchoolof DentalMedicine,Boston,Massachusetts, USA
ISSAHANNA,DDS
AssociateProfessor,DepartmentofOral andMaxillofacialSurgery,TheUniversityof TexasHealthScienceCenteratHouston, ChiefofOralandMaxillofacialSurgery, LyndonB.JohnsonHospital,Houston,Texas, USA
JACKHUA,DDS,MD
Resident,DepartmentofOralandMaxillofacial Surgery,TheUniversityofTexasHealth ScienceCenteratHouston,Houston,Texas, USA
ANDREWT.HUANG,MD
AssistantProfessor,Otolaryngology–Headand NeckSurgery,BaylorCollegeofMedicine, Houston,Texas,USA
MICHAELF.HUANG,DDS,MD
AttendingSurgeon,DepartmentofOraland MaxillofacialSurgery,HoustonMethodist Hospital,Houston,Texas,USA;Assistant ProfessorofOralandMaxillofacialSurgery, WeillCornellMedicalCollege,NewYork, NewYork,USA
JONATHONS.JUNDT,DDS,MD,FACS AssistantProfessor,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Houston, Texas,USA
AUSTINLEAVITT,MS,CFP
FinancialPlanner,TheFinancialAdvisory Group,Houston,Texas,USA
LAITHMAHMOOD,DDS,MD
PrivatePractice,ParkwayOralSurgery andDentalImplantCenter,Houston,Texas, USA
VICTORIAA.MAN ˜ O ´ N,DDS
Resident,DepartmentofOralandMaxillofacial Surgery,TheUniversityofTexasHealth ScienceCenteratHouston,Schoolof Dentistry,Houston,Texas,USA
JOSEM.MARCHENA,DMD,MD,FACS AssociateProfessor,DepartmentofOral andMaxillofacialSurgery,TheUniversityof TexasHealthScienceCenteratHouston, ChiefofOralandMaxillofacialSurgery, BenTaubHospital,Houston,Texas, USA
SANDEEPMARKAN,MD
AssociateProfessor,Departmentof AnesthesiologyandCriticalCareMedicine, BaylorCollegeofMedicine,Houston,Texas, USA
JOSEPHP.MCCAIN,DMD,FACS
EndoscopicMaxillofacialSurgeryFellowship Director,DepartmentofOralandMaxillofacial Surgery,MassachusettsGeneralHospital, FacultyMember,HarvardSchoolofDental Medicine,Boston,Massachusetts,USA
JAMESC.MELVILLE,DDS,FACS
Oral,HeadandNeckOncologyand MicrovascularReconstructiveSurgery, AssociateProfessor,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Schoolof Dentistry,Houston,Texas,USA
JOVANYCRUZNAVARRO,MD
AssistantProfessor,Departmentsof AnesthesiologyandNeurosurgery, BaylorCollegeofMedicine,Houston,Texas, USA
NEERAJPANCHAL,DDS,MD,MA
AssistantProfessor,UniversityofPennsylvania SchoolofDentalMedicine,SectionChief,Penn PresbyterianMedicalCenter,SectionChief, PhiladelphiaVeteransAffairsMedicalCenter, Philadelphia,Pennsylvania,USA
ZACHARYS.PEACOCK,DMD,MD,FACS
AssistantProfessor,DepartmentofOraland MaxillofacialSurgery,MassachusettsGeneral Hospital,HarvardSchoolofDentalMedicine, Boston,Massachusetts,USA
CRAIGPEARL,DDS
AssistantProfessor,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Houston, Texas,USA
ANDREWP.PERRY,DDS
Resident,DepartmentofOralandMaxillofacial Surgery,TheUniversityofTexasHealth ScienceCenteratHouston,Houston,Texas, USA
ARMANDORETANA,DDS,MD
PrivatePractice,CapitalCenterforOraland MaxillofacialSurgery,Washington,DC,USA
JUSTINSEAMAN,DDS,MD
AssistantProfessor,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Houston, Texas,USA
JONATHANW.SHUM,DDS,MD,FACS, FRCD(C)
AssociateProfessor,FellowshipDirector, MaxillofacialOncologyandMicrovascular Reconstruction,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Houston, Texas,USA
MARIAJ.TROULIS,DDS,MSc,FACS
W.C.GuralnickProfessorandChair, DepartmentofOralandMaxillofacialSurgery, MassachusettsGeneralHospital,Harvard SchoolofDentalMedicine,Boston, Massachusetts,USA
DAVIDQ.WAN,MD
AssociateProfessorofRadiology,Department ofDiagnosticandInterventionalImaging, McGovernMedicalSchool,TheUniversityof TexasHealthScienceCenteratHouston, Houston,Texas,USA
JAMESWILSON,DDS,FACS
ProfessorEmeritus,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Houston, Texas,USA
TIMOTHYCHARLESWOERNLEYIII,DDS AssistantProfessor,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Houston, Texas,USA
SIMONYOUNG,DDS,MD,PhD
AssistantProfessor,DepartmentofOraland MaxillofacialSurgery,TheUniversityofTexas HealthScienceCenteratHouston,Schoolof Dentistry,Houston,Texas,USA
Contents
Preface:TheEvolutionofTechnologicalAdvancementsinOralandMaxillofacial Surgery xi
JoseM.Marchena,JonathanW.Shum,andJonathonS.Jundt
VirtualSurgicalPlanninginOralandMaxillofacialSurgery
JackHua,ShahidAziz,andJonathanW.Shum
Virtualsurgicalplanningprovidestheabilitytovisualizethepatientanatomyand pathologiccondition,establishpertinentreferencepoints,andsimulateosteotomies andreconstructiondesigninadvanceofthesurgery.Virtualsurgicalplanningisalso anidealenvironmentforimprovedcommunicationbetweenthepatientandthesurgicalteam.
SurgicalNavigationforOralandMaxillofacialSurgery
NagiDemian,CraigPearl,TimothyCharlesWoernleyIII,JamesWilson,andJustinSeaman
Thisarticlereviewsthebasicsetupandfunctionofsurgicalnavigationanddisplaysa varietyofapplicationsinoralandmaxillofacialsurgery.Theuseofsurgicalnavigationfordentalimplantplacementisdiscussedelsewhereinthisissue.
DynamicNavigationforDentalImplantSurgery
NeerajPanchal,LaithMahmood,ArmandoRetana,andRobertEmeryIII
Dynamicnavigation(DN)hasbeenusedbymanyfieldspreviouslyandrecently appliedtodentalimplantsurgery.DNallowstheimplantsurgeontoevaluateapatient,scanthepatient,plantheimplantposition,andperformtheimplantsurgeryin thesamedaywithoutthedelayorcostoffabricationofastaticsurgicalguidestent. ThecurrentDNworkflowrequires(1)cone-beamcomputedtomographywithfiducials,(2)virtualimplantplanning,(3)calibration,and(4)implantplacementinaccordancetothe3-Dimageonthenavigationscreen.Thistechnologyallowsfor improvedprecisionandaccuracyintheplacementofdentalimplants.
EvolvingTechnologiesforTissueCutting
JonathonS.Jundt,JoseM.Marchena,IssaHanna,JagtarDhanda,MatthewJ.Breit, andAndrewP.Perry
Thisarticlereviewsevolvingandlesserknowntechnologiesfortissuecuttingand theirapplicationinoralandmaxillofacialsurgery.
MinimallyInvasiveEndoscopicOralandMaxillofacialSurgery
MohamedA.Hakim,JosephP.McCain,DavidY.Ahn,andMariaJ.Troulis
Advancesintechnologyandspecializedinstrumentationallowsurgeonstostudy, refine,andmodifyminimallyinvasivesurgery(MIS)toreplacestandardoperations. Thishasoccurredacrossmanysurgicalspecialties.ThebenefitsofMISincludeless swelling,lesspain,shorterhospitalstay,andfasterreturntodailyactivities.Oraland
519
531
539
549
561
maxillofacialendoscopictechniquesareusedforaccesstotheramuscondyleunit, maxillarysinus,zygoma,orbit,temporomandibularjoint,andsalivaryductalsystem. Althoughendoscopictechniquesarealsousedinfacialcosmeticsurgery,thisdiscussionfocusesonnoncosmeticprocedures.
AdjunctiveStrategiesforBenignMaxillofacialPathology
ZacharyS.Peacock
Benigncystsandneoplasmsofthemaxillofacialregioncanvaryinbehavior,with somegrowingrapidlyandresultingindestructionofsurroundingstructures.Despite theirbenignhistology,manyrequireoften-morbidtreatmenttopreventrecurrenceof theselesions.Severallessinvasiveandadjunctivemedicaltreatmentshavebeen developedtolessenthemorbidityofsurgicaltreatment.Asthemolecularand genomicpathogenesisoftheselesionsisbetterunderstood,moredirectedtreatmentsmaylessentheburdenforpatients.
CurrentMethodsofMaxillofacialTissueEngineering
JamesC.Melville,VictoriaA.Mañón,CalebBlackburn,andSimonYoung
Forseveraldecades,themultidisciplinaryfieldoftissueengineeringhasstrivento improveconventionalmethodsofdental,oral,andcraniofacialrehabilitationformillionsofpeopleannually.Severalbonetissueengineeringstrategiesarenowreadily availableintheclinic.Enrichmentofautologousproducts,growthfactors,andcombinationapproachesarediscussedaswaystoenhancethesurgeon’straditional armamentarium.Lastly,cutting-edgeresearchsuchascustomized3-dimensional printedbonescaffolds,tissueengineeringstrategiesforvolumetricmuscleloss, andtemporomandibularjointdiscandcondyleengineeringarebrieflydiscussed asfutureapplications.
TheUseofPatient-SpecificImplantsinOralandMaxillofacialSurgery
MichaelF.Huang,DavidAlfi,JonathanAlfi,andAndrewT.Huang
Thisarticlesummarizesthecurrentuseofpatient-specificimplantsinoralandmaxillofacialsurgery.
PracticeManagementinOralandMaxillofacialSurgery
JamesBaker,AustinLeavitt,andJonathonS.Jundt
Managinganoralandmaxillofacialsurgery(OMS)practicehasundergonedramatic changes.Electronichealthrecords,privacylaws,revenuecyclemanagement,onlinemarketing,andtheriseofdentalserviceorganizations(DSOs)presentincreased dailycomplexityfororalandmaxillofacialsurgeonsinprivatepractice,hospitalbasedemployees,andacademicsurgeons.Thisarticleisstructuredtodiscuss theroleofDSOs,privateequityinOMS,onlinepracticemarketing,accounting andtaxconsiderations,andmodernessentialsofpracticemanagement.
AdvancesinAnesthesiaMonitoring
YiDeng,JovanyCruzNavarro,andSandeepMarkan
Duringsurgery,oneoftheprimaryfunctionsoftheanesthesiologististomonitorthe patientandensuresafeandeffectiveconductofanesthesiatoprovidetheoptimum
569
579
593
601
611
operatingconditions.Standardguidelinesforperioperativemonitoringhavebeen firmlyestablishedbytheAmericanSocietyofAnesthesiologists.However,inrecent years,newadvancesintechnologyhasledtothedevelopmentofmanynewmonitoringmodalities,especiallyinvolvingtheneurologicandcardiovascularsystems. Thisarticlepresentsatargetedreviewtodiscussthefunctionsandlimitationsof thesenewmonitorsandhowtheyareappliedinthemodernoperatingroomsetting. AdvancesinSurgicalTrainingUsingSimulation
KamalF.Busaidy
Simulationinvolvesthere-creationofreal-lifesituations,processes,orstructuresfor thepurposeofimprovingsafety,effectiveness,andefficiencyofhealthcareservices:simulationprovidesacontrolledandsafeenvironmentfortrainingandassessment.Inanageinwhichregulatoryburdens,fiscalchallenges,andrenewedfocus onpatientsafetyincreasinglyconstrainsurgicalresidencyprograms,innovationin teachingisvitalforthefutureoforalandmaxillofacialsurgery(OMS)training.Of thesimulationtechnologiesinmoderndayhealthcareeducation,manyhavefound theirwayintoOMStraining.Thisarticlereviewsthesetechnologies,andsomeexamplesoftheirusesinOMS.
AdvancesinFunctionalImagingintheAssessmentofHeadandNeckCancer
DavidQ.Wan
ThisarticlediscussestheapplicationoffludeoxyglucosePET/computedtomography(CT)technologyinheadandneckcancerdiagnosisandmanagement,aswell asadvantagesanddisadvantagesrelativetotraditionalimagingmodalities.Asuccessfulscanreliesonprecisepatientpreparation,andcompliancetospecificprotocolsbeforeandduringthescan.Finally,thisarticlebrieflyintroducesaPET/CT scanrecentlyapprovedbytheFoodandDrugAdministrationforneuroendocrine tumors.
PreparationoftheNeckforAdvancedFlapReconstruction
JonathanW.Shum,JamesC.Melville,andMarcusCouey
Microvascularfreetissuetransferhasrevolutionizedthereconstructionofcomplex maxillofacialdefects.Thesecasesoftennecessitatea2-teamedapproach,withan ablativesurgeonattheheadandareconstructivesurgeonatadistantsiteforflap harvest.Carefulattentiontorecipientvesselidentificationandpreservationestablishesthefoundationforsuccessfulreconstruction.Thisarticledescribesthesurgicallandmarksofthefrequentlyutilizedarteriesandveins,vesselhandling techniques,andgeneralprinciplesforthepreparationoffreetissuetransferrecipient sitesinheadandneckreconstruction.
621
627
637
VirtualSurgicalPlanning inOralandMaxillofacial Surgery
JackHua, DDS,MDa,ShahidAziz, DMD,MDb,JonathanW.Shum, DDS,MDa,*
KEYWORDS
Virtualsurgicalplanning Maxillofacialreconstruction Maxillofacialtrauma Jawreconstruction Computer-aideddesign Computeraidedmanufacture Imagingmodality Dataacquisition
KEYPOINTS
Virtualsurgicalplanningisaprocessthatbeginsatthecollectionofimagingdata.
Atreatmentplanisderivedthroughthemanipulationimagingdatatovisualizeandpredictaneffectivesurgicalapproachand/orreconstructiveplan.
Advantagesfortheuseofvirtualsurgicalplanningincludeimprovedsurgicalefficiency,andreconstructionstohaveahigherdegreeofaccuracywhencomparedbetweenpreoperativeandpostoperativeimaging.
INTRODUCTION
Sincethe1980s,systematicapplicationof computeraideddesignandmanufacturingin healthcarehasrevolutionizeddiagnosticand interventionalmedicine.1 Thedigitalmanipulation oflarge-scaleimagingdatain3dimensions,specificallyvirtualsurgicalplanning(VSP),provides theabilitytoreproducedetailedanatomic models,andtofabricatesurgicalguidesand customimplants. 2 Theseadvancementshave becomeaninvaluabletoolfororalandmaxillofacialsurgeons.Thesuccessofthesevirtually plannedcasesdependsoneachstepofthe workflowprocess:choiceofimagemodality, dataacquisition,patientworkup,virtualplanning session,andsurgicalexecution.Although eachstepofthecaseiscritical,meticulous effortplacedintheearlyplanningphaseswillincreasethelikelihoodofsuccessintheoperating room.
IMAGINGMODALITY
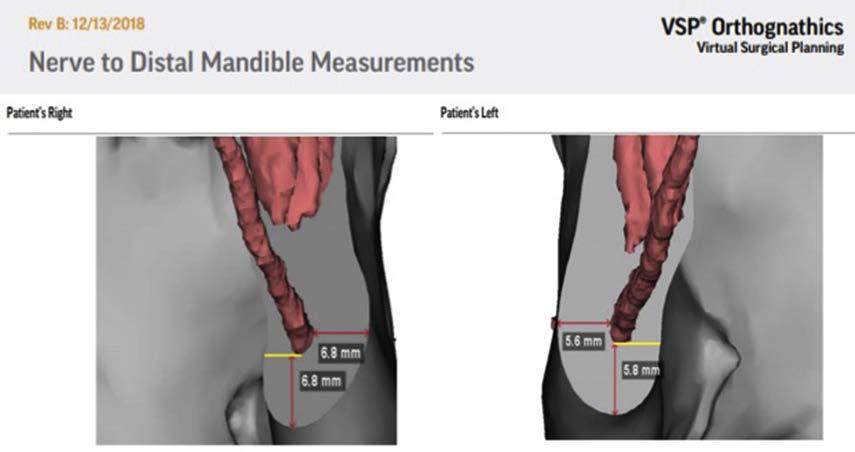
Selectingtheappropriateimagingmodalityisan importantinitialstepanddependsontheadvantagesinspatialandcontrastresolution.Spatial resolutionistheabilityforanimagemodalityto differentiatebetween2separateobjectsina radiographicimage(ie,anervecanalwithinthe mandible)(Fig.1),whereascontrastresolutionis theabilitytodifferentiateimageintensitiesbetween2areas(ie,fatstrandingvsnormaladipose tissue).3 Computedtomography(CT)scanninghas highspatialresolution,butissomewhatlimitedin contrastresolution.Forthisreason,CTscansare idealfororalandmaxillofacialcasesbecause theyofteninvolvehardtissueinterventions,such assurgeryonthebonesandteeth.Similarly, conebeamCThasmanyadvantageswhenused intheappropriatesurgicalsetting.Conebeam CTscansofferhighspatialresolutionwithlessradiationexposurecomparedwithCTscans,butat
DisclosureStatement:Theauthorshavenothingtodisclose. a DepartmentofOralandMaxillofacialSurgery,TheUniversityofTexasHealthScienceCenteratHouston, 6560FanninStreet,Suite1900,Houston,TX77030,USA; b DepartmentofOralandMaxillofacialSurgery, RutgersSchoolofDentalMedicine,90BergenStreet,Suite7700,Newark,NJ07103,USA
*Correspondingauthor.
E-mailaddress: jonathan.shum@uth.tmc.edu
OralMaxillofacialSurgClinNAm31(2019)519–530 https://doi.org/10.1016/j.coms.2019.07.011 1042-3699/19/ 2019ElsevierInc.Allrightsreserved.
thecostofpoorcontrastresolution.4 Foradetailed evaluationofsofttissuestructures,MRIshavefar superiorcontrastresolutionwhencomparedwith CTscans.5 Asanadditionalmethodtoimprove theresolutionofsurfacestructures,3-dimensional (3D)laserscanningisnowusedtoprovidethefine detailnecessarytofacilitateprocedureswhere meticulousdetail,suchastheridgesandgrooves ofteeth,arenecessary.Forexample,thefabricationofocclusalsplintsusedinorthognathicsurgerycanbecreatedfromdataacquiredfrom lasertopography;inturn,traditionalstonemodels arenolongernecessary(Figs.2 and 3).Theseimagesareacquiredwitha3Dlasertopography scannerandstoredasastereolithographyfile. ThestereolithographydatawillundergoDigital
ImagingandCommunicationsinMedicine (DICOM)encapsulationtocreateareliablesuperimposed3Dimagetobeusedinconjunctionwith DICOMdatatocreateanaccuratevirtualrepresentationofanobject,thatis,dentitionand gingiva.Kauandcolleagues6 examinedfacial scansof40patientsandfoundthat90%ofthe caseshadlessthan1.0mmoferror.Schendel andcolleagues7 alsoevaluatedtheaccuracyof 3Dfacialscanninginorthognathicsurgeryand measured18cephalometriclandmarksamong 28patientsandfoundallofthesuperimposed landmarkswerenomorethana0.55mmapart. TheaforementionedmergedDICOM/stereolithographyimagescanbeusedtoaccuratelyfacilitate virtualmaxillofacialskeletalosteotomiesand movementsbasedonbothsoftandhardtissue referencepoints(see Fig.3; Fig.4).
DATAACQUISITION
Thefoundationofsuccessfulsurgicalplanningdependsontheabilityoftheacquireddatasetto replicateanatomicdetailandtranslateintovirtual modelingandeditingsoftwaretopermitsurgical planning.Forthisreason,theradiographicdata arestoredinDICOMformatsotheycanbeuniversallysharedandusedinhealthcareforavarietyof applications.WithrespecttoVSP,DICOMdata canundergoprocessingthatwillallowtranslation into3Dobjects,whichcanthenbemanipulated inadditionalsoftwareforVSP.Softwareprograms suchas MaterializeMimics canreadilyconvert DICOMimagestoa3Dobjectfiletypethatwill
Fig.1. CT-renderedinferioralveolarnervemeasurements.(Courtesyof 3DSystems,RockHill,SC.)
Fig.2. SuperimpositionofstonecastsonCTscan.
thenallowforsurgicalplanningorfabricationof themodelviaa3Dprinter(Fig.5).Computerassisteddesignsoftwaresuchas Proplan by Materialise(Leuven,Belgium)or Sculpt and GeomagicFreeform by3DSystems(RockHill,SC) arecommerciallyavailableforuse.Alternatively, onecouldcollaboratedirectlywithavendor tofacilitatethedatarendering,planning,and manufacturingstagesofVSP.Accesstoanengineeriswidelyavailable,andvideoconferencing
Fig.4. Three-dimensional–printedVSP-plannedinterdentalosteotomycuttingguide.
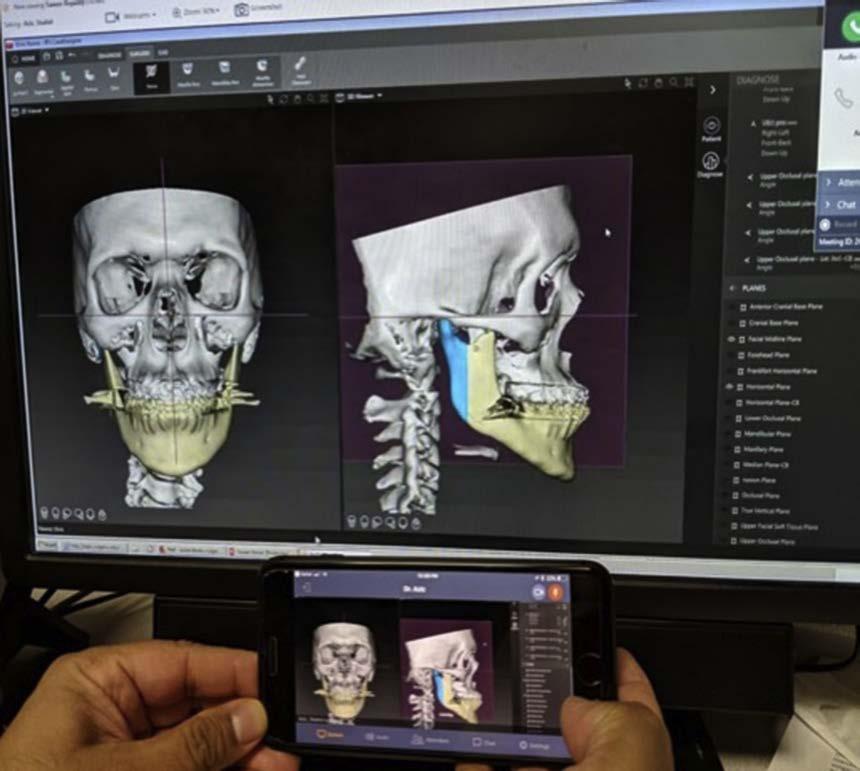
fortreatmentplanshasbecomeasconvenientas usingone’smobilephonetocompletethevirtual planning(Fig.6).Theseapplicationshavetheabilitytoedit,render,andanalyzethe3Dobjectstoa precisionof0.1mmandtoproduceafilethatcan thenbeforwardedtoadditionalprogramstofabricatetheguidesortocreatehardware.8 Common withtheseprogramsistheuseofhapticdevices toprovidetheuserwiththesenseoftouchto assistintheinteractionwiththevirtualobjects. Mosthardtissuereconstructioncasesrequire high-resolutionCTscans,withspecificationsfor theimageslicesrangingfrom0.625to1.500mm thin.9 Althoughthinnerslicesdocapturemore detailintothedataset,Hashemiandcolleagues10 examinedtemporalbonelengthobtainedfroma 1mm-slicedCTversusduringsurgeryandfound thattheradiographicmeasurementswerereliably similartointraoperativeones.Incontrast,Rajati andcolleagues10,11 foundthat1mm-slicedCTimagingalsoprovidereliabledetailinlocatingfacial nerveinjuryintemporalbonetrauma.Tolimitradiationexposureandoptimizeeffectiveness,1mmsliceCTscansareoftenadequatefororaland maxillofacialbonyreconstruction.Analternative toCTimagingistheuseofhigh-resolutionMRIs. ThestrengthofthemagnetsaremeasuredinTesla (T),whichareproportionatetotheabilitytocreate high-resolutionimages.12 Mosthospitalsuse1.5T and3TMRIsystemsthatproduceupto5and 3mmslices,respectively.High-powered7TMRI systemscanproducesubmillimeterslices;however,thesearecurrentlynotwidelyavailablein
Fig.3. Virtualcuttingguidebasedonosteotomies.
theUnitedStatesowingtocosts.12 Morerecently, blackboneMRItechniqueshavebeendeveloped tobeanonionizingalternativetoCTscansfor creating3Dprintedguidesinthepediatricpatient population.13 Suchytaandcolleagues14 compared osteotomiesincadaversfrompreoperativeguides fabricatedfromblackboneMRIscansversusCT scansandfoundnostatisticaldifferenceinaccuracybetweenthe2imagingmodalities.Hoving andcolleagues15 presented2successfulcases ofmandibularresectionfromanMRI-based3Dsurgicalplan,thus,demonstratingthatMRIbasedVSPisafeasiblealternativewithforeseeablebenefitsinthepediatricpopulation.14 These methodstoobtaindataapplytoallapplications ofmaxillofacialsurgery,includingthemanagementofpathology,trauma,anddentofacial abnormalities.Ultimately,whetherplanningfora tumorresection,panfacialreconstruction,or orthognathicsurgery,theacquiredanatomicdetail
Fig.5. Stereolithicprintedmodel.
Fig.6. Virtualplanningonmobiledevice.
mustbedigitizedandtranslatedintovirtualplanningsoftwaretocreatesurgicalguidesand customimplantstofacilitateasuccessfulsurgical outcome.Everyinaccuracyaccumulatedateach stepcannegativelyaffecttheoverallsurgicalcase.
APPLICATION
MaxillofacialTrauma
VSPprovidesthesurgeonanopportunitytominimizetheuncertaintyassociatedwithsurgery. Theabilitytovisualizeresectionmarginsandto designreconstructivestrategiesisasignificant benefittomanagementoffacialtrauma,craniofacialsurgery,andpathology.Inthesettingofmaxillofacialtrauma,VSPallowsforthefabricationof customimplants.16 Midfacetrauma,includingthe orbit,hasbenefitmostfromtheadvancementsin VSPandnavigation.AsystematicreviewbyAzarmehrandcolleagues17 clearlydefinestheadvantagesofcomputer-guidedtechniquesover conventionalnonguidedmethodsforthemanagementoffacialtrauma.VSPcoupledwithsurgical navigationisnotedtobemostusefulinorbital reconstructionowingtothelimitationsinsurgical access,therelationshiptosurroundingvital structures,andthestrictdemandforfunction andaestheticsoftheeye.18 Caiandcolleagues19 conductedaprospectivestudythatcompared ophthalmologiccomplications(ie,diplopia, infraorbitalhypoesthesia,ophthalmoplegia,and enophthalmos)of58patientsundergoingorbital reconstructionandfoundthattheVSP-guided grouphadsignificantlyfewercomplicationsthan theconventional(control)group.Similarly,Bly andcolleagues20 analyzed90patientsundergoing consecutivecomplexorbitalrepairsandfound thatVSP-guidedorbitalreconstructionhadstatisticallysignificantimprovementindiplopiaseverity andadecreaseintheincidenceofrevisionsurgery whencomparedwithnonguidedtechniques.In essence,theadvantagesofVSPinmidfacereconstruction,especiallyorbitalrepairhelpimprove outcomesofcomplexmaxillofacialtrauma.
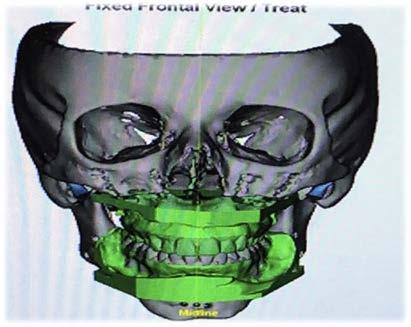
OrthognathicSurgery
VSPisidealfororthognathicsurgicalplanningas well—itprovidesforpreciseandpredictable movementsofthemaxillofacialskeletoninan efficientandeffectivemannercomparedwithconventionalmodelsurgery.21 Nolongerisitnecessaryforpatients,technicians,andsurgeons toundergonumerousdentalimpressions,face bowmeasurements,andlaboratoryworkups. Numerousopportunitiesforerrorandinaccuracies existinthetraditionalorthognathicworkup.Many ifnotalloftheproblemsassociatedwiththe
oneroussequenceofatraditionalorthognathic workupcanbeavoidedinaVSP-guidedworkflow.21 Azarmehrandcolleagues17 summarized orthognathicVSPliteraturetosuggestunanimous supportforVSPandnavigationguidancein orthognathicsurgeryowingtoitsaccuracyand efficiencyinpreoperativeplanningcompared withconventionalmodelsurgery.Additionally, numerousstudiesevaluatingtheeffectivenessof aVSP-drivenworkupconcludethismethodtobe aseffectiveandaccuratewhencomparingpretreatmentandpost-treatmentcephalometricmeasurements,withtheaddedbenefitofbeingmore efficientwiththeuseoftimeandresources.22,23 Resnickandcolleagues24 furtherexaminedoperativetimeandcostofbimaxillarysurgeriesof43patientstoshowthatoperativetimeandcostswere significantlyhigherinallthepatientswithconventionalorthognathicworkupcomparedwithVSP. Thesefindingsaresignificantbecauseaprolongedoperativetimeiscloselycorrelatedwith increasedpostoperativecomplications.25,26 The advantagesofVSPareclearandestablished;a standardorthognathicVSPworkflowisoutlined in Fig.7.
PathologyandReconstruction
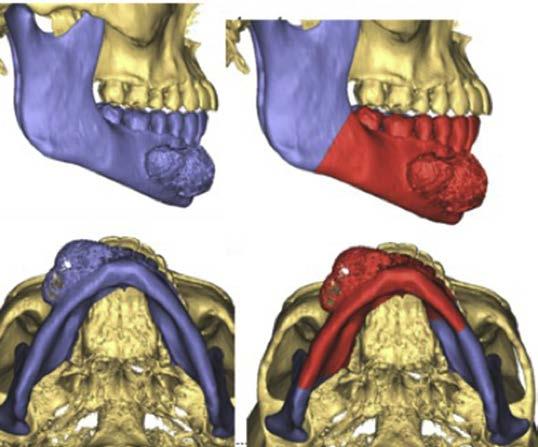
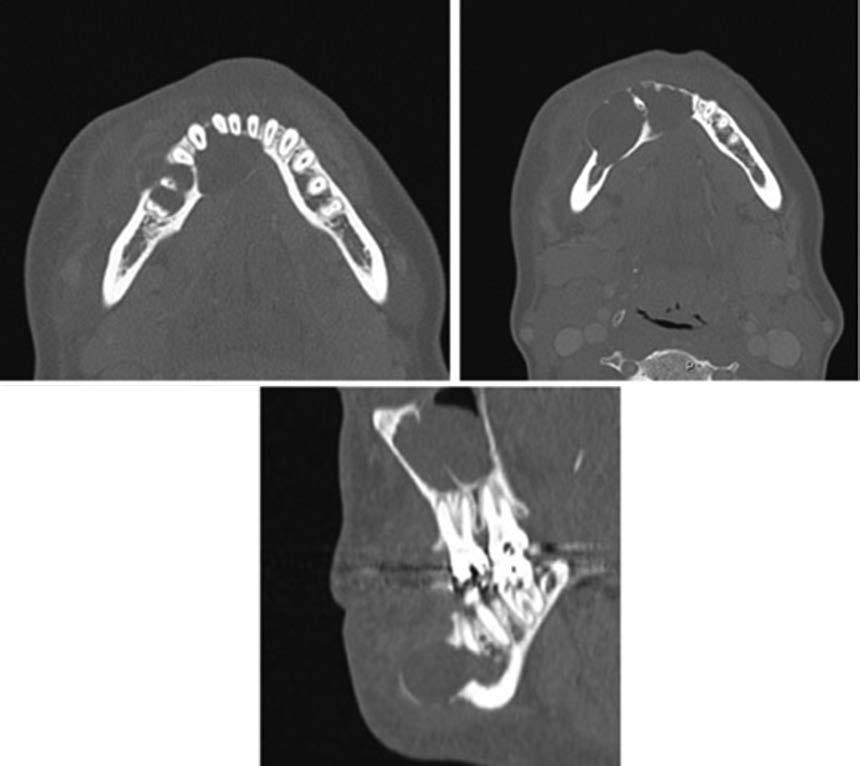
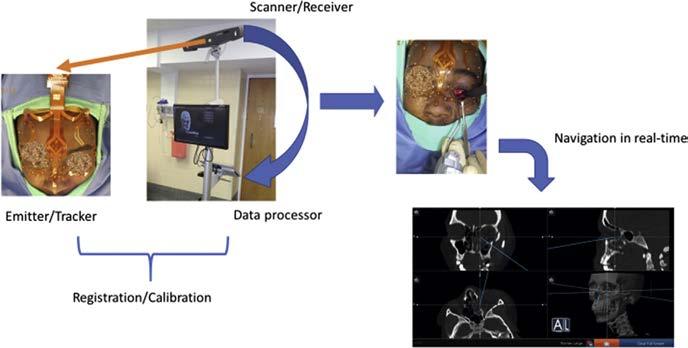
VSPisusedextensivelyinthemanagementof maxillofacialpathologyforitsabilitytovirtually visualizepathologyandtoprovideguidanceon thelocationofresectionmargins.26–28 Theapplicationofguidedosteotomiesismostbeneficial insurgicalresectionsofthemidfaceandforlarge tumorsthathavedeformedanatomiclandmarks (Figs.8 and 9).Characteristicsofmidfacepathologyincludethedifficultiesinremovingtumors withinthemaxillarysinusornasalcavity,where osteotomiesareoftenperformedwithoutdirect visualizationofthetumor.Surgicalplanningallows forsuchresectionstobeperformedwithgreater confidencewhenvisualcuesareabsent.Furthermore,theproximitytovitalstructuresoftheskull basecanbeaccountedforanddesignedintothe cuttingguidestopreventinadvertentinjury.The couplingofreal-time3DnavigationandVSP furtherenhancestheseadvantagestoprovideimmediatefeedbacktoconfirmpositionofguides andplannedosteotomies(Figs.10 and 11). RecentstudiesdemonstratethebenefitsofVSP andnavigationbyreportingastatisticallysignificantdifferencein91%ofpatientsinobtaininga clearmarginalongdeeptumormarginswithanaccuracyoflessthan5mmdifferenceoftheactual resectionmargincomparedwiththeplanned margin.29,30 Bernsteinandcolleagues31 andFoley andcolleagues32 compared224osteotomies
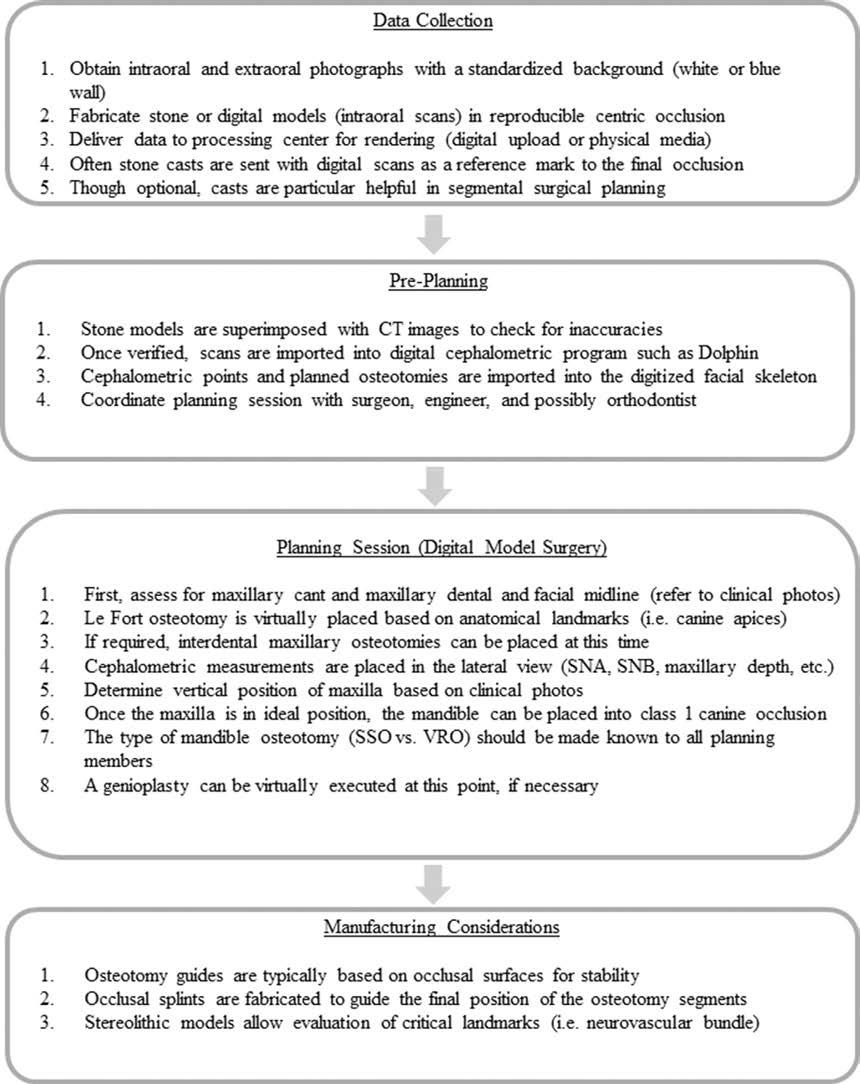
Fig.7. Orthognathicsurgeryworkflow.SNA,SellaNasion,A;SNB,SellaNasion,B;SSO,SagittalSplitOsteotomy; VRO,VerticalRamusOsteotomy.
madewith3D-navigatedvirtualcuttingguidesand 224withoutnavigationandfoundthatosteotomies madewith3Dnavigationtobemoreaccuratein distance,pitch,androll.Althoughmorestudies areneededtocompare3DnavigationandVSPbasedresectiontechniques,thepotentialis evidentinitsapplicationinthemanagementof pathology. Paralleltotheextirpationoftumorsisthereconstructionofsaiddefect.VSPhasmadeasignificantimpactonallaspectsofreconstruction.It hasmadereconstructionastreamlineprocess
Fig.8. Theresectionmarginsare definedandviewedonavirtualmodel.
Fig.9. ThecorrespondingdefinedresectionmarginscanreferencedontotheoriginalCTimagingtoensureclearancefromtheidentifiedtumor.
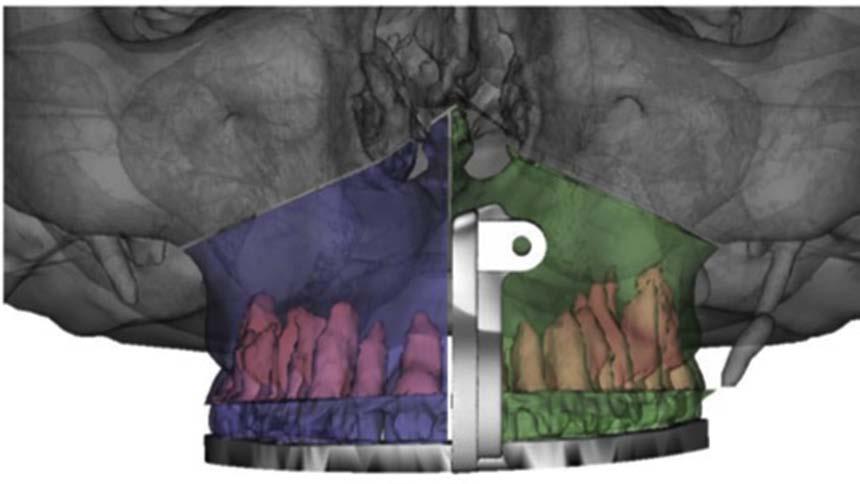
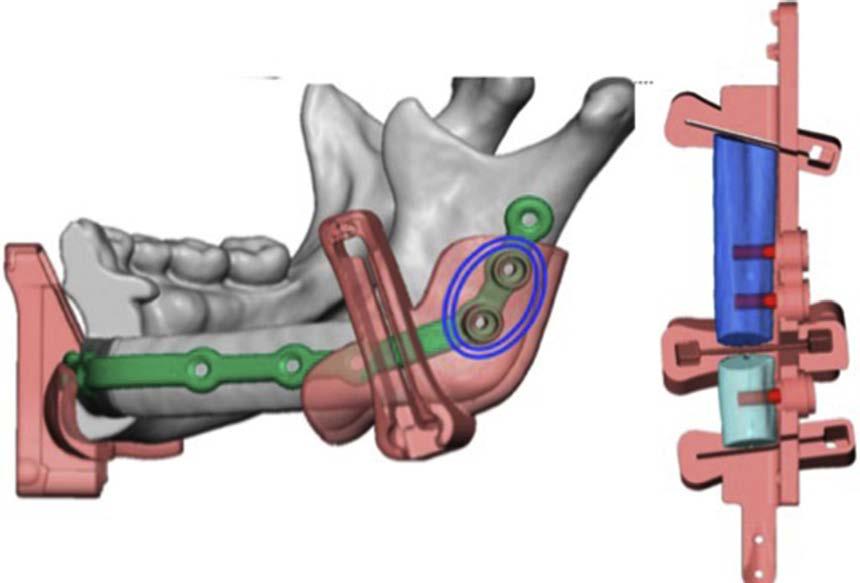
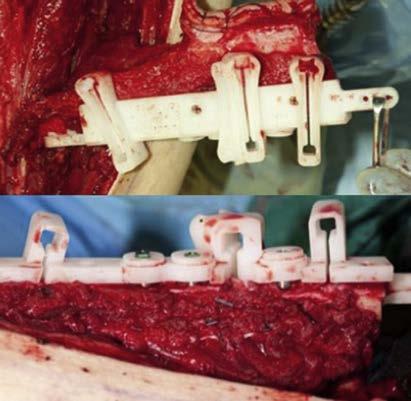
Fig.10. Virtualplannedcuttingguideswithpredictiveholestofacilitatehardwareplacement(bluecircle).Right fibulabonesegmentssecuredtocuttingtemplate,withvirtualfibulaandestimatedendosseousimplantstobe placedwhileinsituofdonorsite.
thatiscosteffective,withoutjeopardizingoutcomesorincreasingcomplicationrates.33 VSPguidedsurgeryisreportedly60to120minutes fasterinmicrovasculartissuetransfersusinga
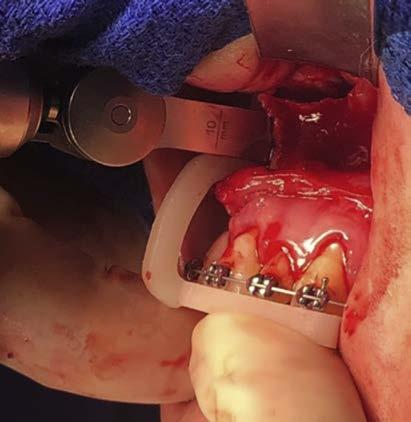
Fig.11. Intraoperativeviewofthecuttingtemplate securedtothefibulaosteocutaneousfreeflapwhile insituinleg.Right–endosseousimplantsareplaced withcuttingtemplate.
bonydonorsite,suchasthefibulaosteocutaneousfreeflap,whencomparedwithnonguidedsurgery.34,35 Complexbonyconstructstorestorethe midfaceanddefectsoftheanteriormandible
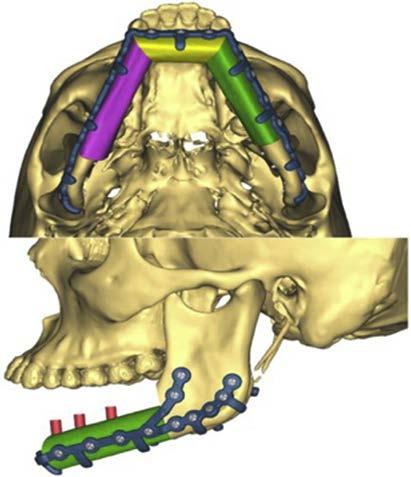
Fig.12. Virtualconstructofthe3D-printedplatewith registrationtabsandplanneddentalimplants.
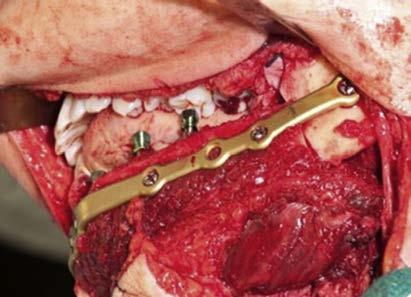
Fig.13. Thefibulaosteocutaneousflapformsaneomandibleasitissecuredtothenativeremaining mandiblebyreconstructionplate.TheendosseousimplantsarepreciselypositionedbasedonVSP.
demonstratethehighestdegreeofaccuracyand precisionwiththeuseofVSP.33,36,37 Additionally, fewernonunionsarereportedandbone-to-bone contactisoptimizedbetweenosteotomysegments.Delayedandimmediatedentalrehabilitationwithendosseousimplantshavealsobecome possiblebecauseoftheprecisionofVSP-guided reconstructions.Thishaspermittedmorereconstructionsofthejawstoattainafunctionaldental rehabilitationeitherimmediatelyorinastaged manner(Figs.12 and 13).Approximately40%to 50%ofpatientswhohaveundergonemicrovascularreconstructionofajawdefectanddental implantplacementobtainafunctionaldentalprosthesiscomparedwithonly15%to20%inpatients whohaveundergonenon–VSP-guidedreconstructionsofthejaws.38–40 BeforeVSP,the inabilitytoaccuratelypredictthelocationof
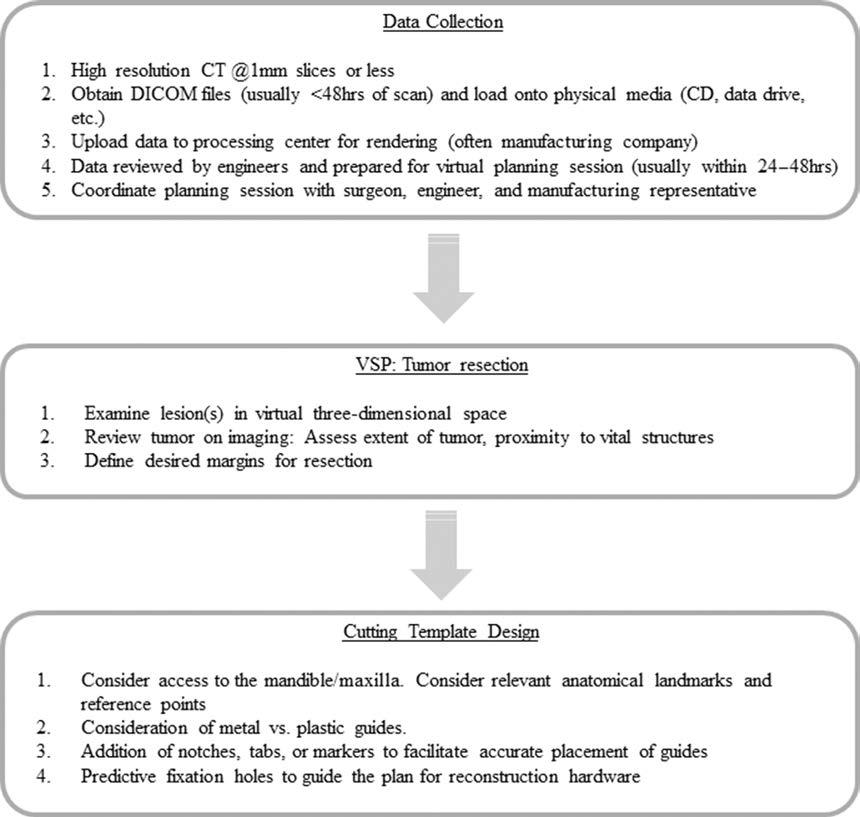
Fig.14. Oralandmaxillofacialjawresectionworkflow.
thefibulasegmentsandtheirrelationshiptothe opposingarchseverelylimitedtheplacementor functionofdentalimplants.
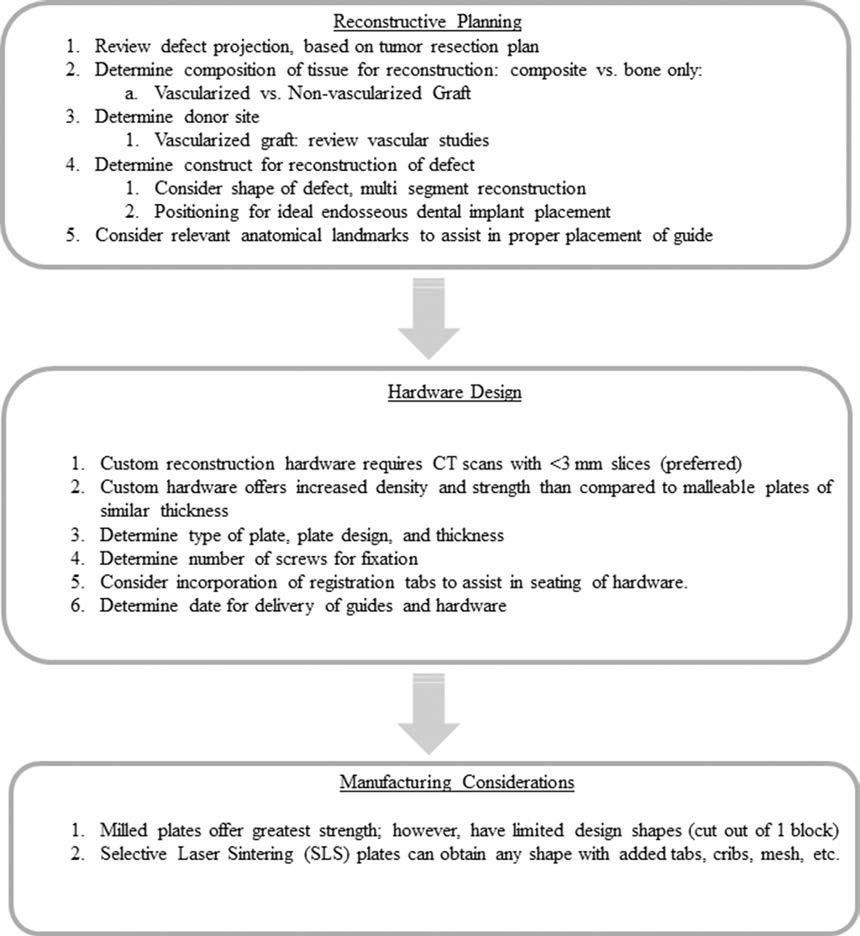
TheseadvantagesderivedfromVSPwill continuetoevolveandrefinetheefficiencyand precisionofcomplexsurgeriesoftheheadand neck.Anexampleworkflowoftheextirpationofa tumor(squamouscellcarcinoma)(Fig.14)and(fibulafreeflap)reconstruction(Fig.15)isprovided.
LIMITATIONS
AlthoughVSPcanimprovetheoutcomesofmany complexandtechnicallychallengingsurgeries,it
haslimitationsthatarecurrentlybeyondthesurgeons’control.Barrierstotheeffectiveuseof VSPareassociatedwiththeinherentdelaysassociatedwithcurrentmanufacturingcapabilitiesand humanerror.Onaverage,theauthors’experience withtheturnoverbetweenVSPplanningsessionto deliveryofimplant/guidescanrangebetween7to 14daysforpre-bentandmilledhardware, whereas3Dprintedplatesandlasersinteredhardwarecanbeproducedin14to17days.Theselimitationsareduetothelogisticsinvolvedinthe processing,qualitycontrol,andtransportationof theprostheses.Severaloptionsareavailableto Fig.15. Oralandmaxillofacialreconstructionworkflow.
reducetheturnaroundtime,throughtheuseofin office3Dprintersandinstitutionalresources.
Humanerrorisinevitableandcanbeappliedto everyaspectoftheVSPprocess.Potentialsources ofinaccuraciesinthepreoperativesettingwouldbe relatedtomiscommunicationbetweenphysicians, technicians,andassistants.Thecoordinationof careisessentialforeffectivehealthcaredelivery; however,thespecificationsforimagingoftenare notconveyedaccuratelytotheradiologycenter orthedatamaynotbeprocessedadequately, andtheresultingeffectisDICOMfilesthatarenot compatiblewiththeplanningsoftware.Subsequently,thediscoveryofinadequatedataleadsto delaysrelatingtotheneedforadditionalimaging anduseofresources.Intheoperatingroom,surgeonerrorcanberelatedtotheapplicationof guidestodesignatedreferencepoints.Errorsmay occurifoneisnotfamiliarwiththehardwareandinstrumentsorifasurgeonoverlooksdetailsofthe surgicalplan.Themostcommonpointforerroris theapplicationoftheresectionguideorofthe reconstructionguidetothedonorsite,followed byinadequatetechnique,suchasperformingan osteotomyatthewrongangle.Thesenuances canresultindeviationsfromtheidealoutcome; however,theyservemoreassourcesoffrustration thansignificantadverseevents.
Virtualsurgicalplanningwillcontinueto improve,andmethodstoacquireandprocesspatientdatawillbecomemorerefined.Meticulous attentiontoeachstepisnecessarytoensurea positiveoutcome.Futuretrendswilllikelyinclude widespreadavailabilityof3Dprintingand manufacturingtechnologyandanincreasingnumberofsurgeonstakingontheroleoftheengineer.
REFERENCES
1. DoiK.Computer-aideddiagnosisinmedicalimaging:historicalreview,currentstatusandfuturepotential.ComputMedImagingGraph2007;31(4–5): 198–211
2. EfanovJI,RoyAA,HuangKN,etal.Virtualsurgical planning:thepearlsandpitfalls.PlastReconstrSurg GlobOpen2018;6(1):e1443
3. Allisy-RobertsP,WilliamsJ.Farr’sphysicsformedicalimaging.NewYork:W.B.SaundersCompany; 2007
4. PauwelsR,BeinsbergerJ,StamatakisH,etal.Comparisonofspatialandcontrastresolutionforconebeamcomputedtomographyscanners.OralSurg OralMedOralPatholOralRadiol2012;114(1): 127–35
5. LinE,AlessioA.Whatarethebasicconceptsof temporal,contrast,andspatialresolutionincardiac CT?JCardiovascComputTomogr2009;3(6):403–8
6. KauCH,RichmondS,ZhurovAI,etal.Reliabilityof measuringfacialmorphologywitha3-dimensional laserscanningsystem.AmJOrthodDentofacialOrthop2005;128(4):424–30
7. SchendelSA,JacobsonR,KhalessiS.3-dimensionalfacialsimulationinorthognathicsurgery:isit accurate?JOralMaxillofacSurg2013;71(8): 1406–14
8. ProPlanCMF3.0.1instructionsforsoftwareuse.Plymouth(MI):MaterialiseInc;2017.p.3
9. CernigliaroJG.ACRpracticeparameterforperformingandInterpretingdiagnosticcomputedtomography(CT).Reston(VA):RadiologyACo; 2014.p.2
10. HashemiJ,RajatiM,RezayaniL,etal.Temporal bonemeasurements;acomparisonbetween renderedspiralCTandsurgery.IranJRadiol 2014;11(3):e9400
11. RajatiM,PezeshkiRadM,IraniS,etal.Accuracyof high-resolutioncomputedtomographyinlocating facialnerveinjurysitesintemporalbonetrauma. EurArchOtorhinolaryngol2014;271(8):2185–9
12. PetridouN,ItaliaanderM,vandeBankBL,etal. Pushingthelimitsofhigh-resolutionfunctionalMRI usingasimplehigh-densitymulti-elementcoil design.NMRBiomed2013;26(1):65–73
13. EleyKA,Watt-SmithSR,GoldingSJ."BlackBone" MRI:anovelimagingtechniquefor3Dprinting.DentomaxillofacRadiol2017;46(3):20160407
14. SuchytaMA,GibreelW,HuntCH,etal.Using blackbonemagneticresonanceimagingincraniofacialvirtualsurgicalplanning:acomparative cadaverstudy.PlastReconstrSurg2018;141(6): 1459–70
15. HovingAM,KraeimaJ,SchepersRH,etal.Optimisationofthree-dimensionallowerjawresection marginplanningusinganovelBlackBonemagnetic resonanceimagingprotocol.PLoSOne2018;13(4): e0196059
16. HerfordAS,MillerM,LauritanoF,etal.Theuseofvirtualsurgicalplanningandnavigationinthetreatmentoforbitaltrauma.ChinJTraumatol2017; 20(1):9–13
17. AzarmehrI,StokbroK,BellRB,etal.Surgicalnavigation:asystematicreviewofindications,treatments,andoutcomesinoralandmaxillofacial surgery.JOralMaxillofacSurg2017;75(9): 1987–2005
18. JansenJ,SchreursR,DuboisL,etal.The advantagesofadvancedcomputer-assisteddiagnosticsandthree-dimensionalpreoperativeplanningonimplantpositioninorbitalreconstruction. JCraniomaxillofacSurg2018;46(4):715–21
19. CaiEZ,KohYP,HingEC,etal.Computer-assisted navigationalsurgeryimprovesoutcomesinorbital reconstructivesurgery.JCraniofacSurg2012; 23(5):1567–73
20. BlyRA,ChangSH,CudejkovaM,etal.Computerguidedorbitalreconstructiontoimproveoutcomes. JAMAFacialPlastSurg2013;15(2):113–20
21. ZhangN,LiuS,HuZ,etal.Accuracyofvirtualsurgicalplanningintwo-jaworthognathicsurgery:comparisonofplannedandactualresults.OralSurg OralMedOralPatholOralRadiol2016;122(2): 143–51
22. VandenBemptM,LiebregtsJ,MaalT,etal.Toward ahigheraccuracyinorthognathicsurgerybyusing intraoperativecomputernavigation,3Dsurgical guides,and/orcustomizedosteosynthesisplates:a systematicreview.JCraniomaxillofacSurg2018; 46(12):2108–19
23. ZinserMJ,SailerHF,RitterL,etal.Aparadigmshift inorthognathicsurgery?Acomparisonofnavigation,computer-aideddesigned/computer-aided manufacturedsplints,and"classic"intermaxillary splintstosurgicaltransferofvirtualorthognathic planning.JOralMaxillofacSurg2013;71(12):2151. e1-21
24. ResnickCM,InversoG,WrzosekM,etal.Istherea differenceincostbetweenstandardandvirtualsurgicalplanningfororthognathicsurgery?JOralMaxillofacSurg2016;74(9):1827–33
25. ChengH,ChenBP,SoleasIM,etal.Prolongedoperativedurationincreasesriskofsurgicalsiteinfections:asystematicreview.SurgInfect(Larchmt) 2017;18(6):722–35
26. ChimH,WetjenN,MardiniS.Virtualsurgicalplanningincraniofacialsurgery.SeminPlastSurg 2014;28(3):150–8
27. ShenY,SunJ,LiJ,etal.Specialconsiderationsin virtualsurgicalplanningforsecondaryaccurate maxillaryreconstructionwithvascularisedfibulaosteomyocutaneousflap.JPlastReconstrAesthet Surg2012;65(7):893–902
28. KimNK,KimHY,KimHJ,etal.Considerationsand protocolsinvirtualsurgicalplanningofreconstructivesurgeryformoreaccurateandestheticneomandiblewithdeepcircumflexiliacarteryfreeflap. MaxillofacPlastReconstrSurg2014;36(4):161–7
29. TarsitanoA,RicottaF,BaldinoG,etal.Navigationguidedresectionofmaxillarytumours:theaccuracyofcomputer-assistedsurgeryintermsof controlofresectionmargins-afeasibilitystudy. JCraniomaxillofacSurg2017;45(12):2109–14
30. RicottaF,CercenelliL,BattagliaS,etal.Navigationguidedresectionofmaxillarytumors:cananew
volumetricvirtualplanningmethodimproveoutcomesintermsofcontrolofresectionmargins? JCraniomaxillofacSurg2018;46(12):2240–7
31. BernsteinJM,DalyMJ,ChanH,etal.Accuracyand reproducibilityofvirtualcuttingguidesand3D-navigationforosteotomiesofthemandibleandmaxilla. PLoSONE2017;12(3).e0173111
32. FoleyBD,ThayerWP,HoneybrookA,etal.Mandibularreconstructionusingcomputer-aideddesign andcomputer-aidedmanufacturing:ananalysisof surgicalresults.JOralMaxillofacSurg2013;71(2): e111–9
33. TotoJM,ChangEI,AgagR,etal.Improvedoperativeefficiencyoffreefibulaflapmandiblereconstructionwithpatient-specific,computer-guided preoperativeplanning.HeadNeck2015;37(11): 1660–4
34. ZweifelDF,SimonC,HoarauR,etal.Arevirtual planningandguidedsurgeryforheadandneck reconstructioneconomicallyviable?JOralMaxillofacSurg2015;73(1):170–5
35. ChangEI,JenkinsMP,PatelSA,etal.Long-term operativeoutcomesofpreoperativecomputed tomography-guidedvirtualsurgicalplanningforosteocutaneousfreeflapmandiblereconstruction. PlastReconstrSurg2016;137(2):619–23
36. AntonyAK,ChenWF,KolokythasA,etal.Useofvirtualsurgeryandstereolithography-guidedosteotomyformandibularreconstructionwiththefree fibula.PlastReconstrSurg2011;128(5):1080–4
37. LiuXJ,GuiL,MaoC,etal.Applyingcomputertechniquesinmaxillofacialreconstructionusingafibula flap:amessengerandanevaluationmethod. JCraniofacSurg2009;20(2):372–7
38. AvrahamT,FrancoP,BrechtLE,etal.Functional outcomesofvirtuallyplannedfreefibulaflapreconstructionofthemandible.PlastReconstrSurg2014; 134(4):628e–34e
39. vanGemertJT,vanEsRJ,RosenbergAJ,etal. Freevascularizedflapsforreconstructionofthe mandible:complications,success,anddental rehabilitation.JOralMaxillofacSurg2012;70(7): 1692–8
40. IizukaT,HafligerJ,SetoI,etal.Oralrehabilitationaftermandibularreconstructionusinganosteocutaneousfibulafreeflapwithendosseousimplants. Factorsaffectingthefunctionaloutcomeinpatients withoralcancer.ClinOralImplantsRes2005; 16(1):69–79