https://ebookmass.com/product/advances-in-cosmetic-surgery-
Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
McGraw-Hill Education SAT 2019 2019 edition Edition
Christopher Black
https://ebookmass.com/product/mcgraw-hill-educationsat-2019-2019-edition-edition-christopher-black/
ebookmass.com
2019 novel coronavirus (2019-nCoV) outbreak: A new challenge Tommaso Lupia
https://ebookmass.com/product/2019-novel-coronavirus-2019-ncovoutbreak-a-new-challenge-tommaso-lupia/
ebookmass.com
Fundamentals of HIV Medicine 2019 1st Edition
https://ebookmass.com/product/fundamentals-of-hiv-medicine-2019-1stedition/
ebookmass.com
Disability Through the Lens of Justice Jessica Begon
https://ebookmass.com/product/disability-through-the-lens-of-justicejessica-begon/
ebookmass.com
Kaufman's Clinical Neurology for Psychiatrists 8th Edition Edition David Myland Kaufman
https://ebookmass.com/product/kaufmans-clinical-neurology-forpsychiatrists-8th-edition-edition-david-myland-kaufman/
ebookmass.com
Corrosion Policy Decision Making: Science, Engineering, Management, and Economy Reza Javaherdashti
https://ebookmass.com/product/corrosion-policy-decision-makingscience-engineering-management-and-economy-reza-javaherdashti/
ebookmass.com
Lubkin’s Chronic Illness 10th Edition, (Ebook PDF)
https://ebookmass.com/product/lubkins-chronic-illness-10th-editionebook-pdf/
ebookmass.com
Interdisciplinary Applications of Shame/Violence Theory: Breaking the Cycle Roman Gerodimos
https://ebookmass.com/product/interdisciplinary-applications-of-shameviolence-theory-breaking-the-cycle-roman-gerodimos/
ebookmass.com
Famine: Its Causes, Effects and Management John R. K. Robson
https://ebookmass.com/product/famine-its-causes-effects-andmanagement-john-r-k-robson/
ebookmass.com
One Last Chance (Returning to Rocky Ridge Book 1) April Murdock
https://ebookmass.com/product/one-last-chance-returning-to-rockyridge-book-1-april-murdock/
ebookmass.com
ADVANCESIN COSMETICSURGERY
GregoryH.Branham,MD
JeffreyS.Dover,MD,FRCPC
HeatherJ.Furnas,MD,FACS
MarissaM.J.Tenenbaum,MD
AllanE.Wulc,MD,FACS
Director,ContinuityPublishing:TaylorBall
Editor:JessicaMcCool
DevelopmentalEditor:DonaldMumford
2019ElsevierInc.Allrightsreserved.
ThisperiodicalandtheindividualcontributionscontainedinitareprotectedundercopyrightbyElsevierandthefollowingterms andconditionsapplytotheiruse:
Photocopying
Singlephotocopiesofsinglearticlesmaybemadeforpersonaluseasallowedbynationalcopyrightlaws.PermissionofthePublisher andpaymentofafeeisrequiredforallotherphotocopying,includingmultipleorsystematiccopying,copyingforadvertisingor promotionalpurposes,resale,andallformsofdocumentdelivery.Specialratesareavailableforeducationalinstitutionsthatwish tomakephotocopiesfornon-profiteducationalclassroomuse. Forinformationonhowtoseekpermissionvisit www.elsevier.com/permissions orcall:(+44)1865843830(UK)/(+1)215239 3867(USA).
DerivativeWorks
Subscribersmayreproducetablesofcontentsorpreparelistsofarticlesincludingabstractsforinternalcirculationwithintheirinstitutions.PermissionofthePublisherisrequiredforresaleordistributionoutsidetheinstitution.PermissionofthePublisheris requiredforallotherderivativeworks,includingcompilationsandtranslations(pleaseconsult www.elsevier.com/permissions).
ElectronicStorageorUsage
PermissionofthePublisherisrequiredtostoreoruseelectronicallyanymaterialcontainedinthisperiodical,includinganyarticle orpartofanarticle(pleaseconsult www.elsevier.com/permissions).Exceptasoutlinedabove,nopartofthispublicationmaybe reproduced,storedinaretrievalsystemortransmittedinanyformorbyanymeans,electronic,mechanical,photocopying,recordingorotherwise,withoutpriorwrittenpermissionofthePublisher.
Notice
NoresponsibilityisassumedbythePublisherforanyinjuryand/ordamagetopersonsorpropertyasamatterofproductsliability, negligenceorotherwise,orfromanyuseoroperationofanymethods,products,instructionsorideascontainedinthematerial herein.Becauseofrapidadvancesinthemedicalsciences,inparticular,independentverificationofdiagnosesanddrugdosages shouldbemade.
Althoughalladvertisingmaterialisexpectedtoconformtoethical(medical)standards,inclusioninthispublicationdoesnot constituteaguaranteeorendorsementofthequalityorvalueofsuchproductoroftheclaimsmadeofitbyitsmanufacturer.
Reprints: Forcopiesof100ormoreofarticlesinthispublication,pleasecontacttheCommercialReprintsDepartment,ElsevierInc., 360ParkAvenueSouth,NewYork,NY10010-1710.Tel:212-633-3874;Fax:212-633-3820;E-mail: reprints@elsevier.com.
PrintedintheUnitedStatesofAmerica.
EditorialOffice: Elsevier,Inc.
1600JohnF.KennedyBlvd, Suite1800 Philadelphia,PA19103-2899
InternationalStandardSerialNumber:2542-4793
InternationalStandardBookNumber:13:978-0-323-65544-6
ADVANCESINCOSMETICSURGERY
EDITORS
GREGORYH.BRANHAM,MD
ChiefMedicalOfficer,Barnes-JewishWestCounty Hospital,CreveCoeur,Missouri;ProfessorandChief, FacialPlasticandReconstructiveSurgery,Department ofOtolaryngology-HNS,WashingtonUniversity SchoolofMedicine,StLouis,Missouri
JEFFREYS.DOVER,MD,FRCPC
Director,SkinCarePhysicians,ChestnutHill, Massachusetts;AssociateClinicalProfessorof Dermatology,YaleUniversitySchoolofMedicine, NewHaven,Connecticut;AdjunctAssociateProfessor ofDermatology,BrownMedicalSchool,Providence, RhodeIsland
HEATHERJ.FURNAS,MD,FACS
AdjunctAssistantProfessor,DivisionofPlasticand ReconstructiveSurgery,StanfordMedicalSchool, Stanford,California
MARISSAM.J.TENENBAUM,MD
AssociateProfessorandProgramDirector,Divisionof PlasticandReconstructiveSurgery,Departmentof Surgery,WashingtonUniversitySchoolofMedicinein St.Louis,StLouis,Missouri
ALLANE.WULC,MD,FACS
AssociateClinicalProfessor,Departmentof Ophthalmology,UniversityofPennsylvania, Philadelphia,Pennsylvania;AdjunctAssociate Professor,DepartmentofOtolaryngology,Temple University,Philadelphia,Pennsylvania
ADVANCESINCOSMETICSURGERY
CONTRIBUTORS
RACHELC.BAKER,BS
ResearchAssistant,SectionofPlasticSurgery, UniversityofMichigan,NorthCampusResearch Complex(NCRC),AnnArbor,Michigan,USA
DANIELJ.CALLAGHAN,MD
MohsMicrographicSurgeryFellow,SkinCare Physicians,ChestnutHill,Massachusetts,USA
FRANCISCOL.CANALES,MD
PrivatePractice,SantaRosa,California,USA
YUNYOUNGCLAIRECHANG,MD
Physician,UnionSquareLaserDermatology, NewYork,NewYork,USA
ANNECHAPAS,MD
Physician,UnionSquareLaserDermatology, NewYork,NewYork,USA
JUSTINCOHEN,MD,FACS
GlasgoldGroupPlasticSurgery,Princeton, NewJersey,USA
STEVENM.COUCH,MD,FACS
AssociateProfessorofOrbitalandOculofacialPlastic Surgery,DepartmentofOphthalmologyandVisual Sciences,WashingtonUniversityinSt.Louis,StLouis, Missouri,USA
JEFFREYS.DOVER,MD,FRCPC Director,SkinCarePhysicians,ChestnutHill, Massachusetts;AssociateClinicalProfessorof Dermatology,YaleUniversitySchoolofMedicine, NewHaven,Connecticut;AdjunctAssociateProfessor ofDermatology,BrownMedicalSchool,Providence, RhodeIsland,USA
GORANAKUKAEPSTEIN,MD FoundationforHairRestoration,Miami,Florida,USA
JEFFREYEPSTEIN,MD,FACS FoundationforHairRestoration,Miami,Florida, USA;AssistantClinicalProfessor,Departmentof Otolaryngology,UniversityofMiami,CoralGables, Florida,USA
JILLA.FOSTER,MD,FACS
PlasticSurgeryOhio/OphthalmicSurgeonsand ConsultantsofOhio,Inc,Departmentof Ophthalmology,TheOhioStateUniversity, Columbus,Ohio,USA
HEATHERJ.FURNAS,MD,FACS
AdjunctAssistantProfessor,DivisionofPlasticand ReconstructiveSurgery,StanfordMedicalSchool, Stanford,California,USA
ADELEHAIMOVIC,MD
TheRonaldO.PerelmanDepartmentofDermatology, NewYorkUniversityLangoneHealth,NewYorkCity, NewYork,USA
ANDREWHARRISON,MD
DepartmentofOphthalmologyandVisual Neurosciences,UniversityofMinnesotaMedical School,Minneapolis,Minnesota,USA
MORRISE.HARTSTEIN,MD,FACS
Director,OphthalmicPlasticSurgery,AssafHarofeh MedicalCenter,TelAvivUniversity-SacklerSchoolof Medicine,TelAviv-Yafo,Israel
LARRYKEVINHEARD,MD
ResidentPhysician,DepartmentofDermatology, UniversityofSouthFlorida,Tampa,Florida,USA
SARAHOGAN,MD,MPH
CosmeticandLaserDermatologicSurgeryFellow, SkinCarePhysicians,ChestnutHill,Massachusetts, USA
OMERIBRAHIM,MD
ChicagoCosmeticSurgeryandDermatology,Chicago, Illinois,USA
PRASANTHIKANDULA,MD
CosmeticandLaserDermatologicSurgeryFellow, SkinCarePhysicians,ChestnutHill,Massachusetts, USA
RYANC.KELM,BS
UnivsersityofOklahomaCollegeofMedicine, OklahomaCity,Oklahoma,USA
SHILPIKHETARPAL,MD
DepartmentofDermatology,ClevelandClinic Foundation,Cleveland,Ohio,USA
JENNIFERMACGREGOR,MD
Physician,UnionSquareLaserDermatology, NewYork,NewYork,USA
KAVITAMARIWALLA,MD
Founder,MariwallaDermatology,WestIslip, NewYork,USA
GUYMASSRY,MD
BeverlyHillsOphthalmicPlasticandReconstructive Surgery,BeverlyHills,California,USA;OrbitalCenter, Cedars-SinaiMedicalCenter,Departmentof Ophthalmology,DivisionofOculoplasticSurgery, KeckSchoolofMedicineofUSC,Universityof SouthernCalifornia,LosAngeles,California,USA
AMYPATEL,MD
BeverlyHillsOphthalmicPlasticandReconstructive Surgery,BeverlyHills,California,USA,USA;Orbital Center,Cedars-SinaiMedicalCenter,LosAngeles, California,USA
FORUMPATEL,MD
Physician,UnionSquareLaserDermatology, NewYork,NewYork,USA
ALIA.QURESHI,MD
AestheticSurgeryFellow,MarinaPlasticSurgery, MarinadelRey,California,USA
SHAWNROMAN,BS
BovieVicePresidentofResearch&Development, SafetyHarbor,Florida,USA
PETERM.SCHMID,DO,FAOCOOHNS,FAACS PrivatePractice,Longmont,Colorado,USA
LORELEYD.SMITH,MD
ResidentPhysician,DepartmentofOphthalmology andVisualSciences,WashingtonUniversityin St.Louis,StLouis,Missouri,USA
JONATHANSOH,MD
UniversityofRochesterMedicalCenter,Rochester, NewYork,USA
EMILYA.SPATARO,MD
AssistantProfessor,WashingtonUniversityinSt.Louis, StLouis,Missouri,USA;DivisionofFacialPlasticand ReconstructiveSurgery,WashingtonUniversitySchool ofMedicine,CreveCoeur,Missouri,USA
DANIELG.STRAKA,MD
PlasticSurgeryOhio/OphthalmicSurgeonsand ConsultantsofOhio,DepartmentofOphthalmology, TheOhioStateUniversity,Columbus,Ohio,USA
MARISSAM.J.TENENBAUM,MD
AssociateProfessorandProgramDirector,Divisionof PlasticandReconstructiveSurgery,Departmentof Surgery,WashingtonUniversitySchoolofMedicinein St.Louis,StLouis,Missouri,USA
SAMANTHAA.THIRY,MSN,FNP-C Dr.JenniferWalden,PLLC,Austin,Texas
MARAWEINSTEINVELEZ,MD
UniversityofRochesterMedicalCenter,NewYork, USA
JENNIFERL.WALDEN,MD,FACS
ClinicalAssistantProfessor,DepartmentofPlastic Surgery,TheUniversityofTexasSouthwesternMedical Center,PrivatePractice,Austin,Texas,USA
JENNIFERF.WALJEE,MD,MPH,MS
AssociateProfessor,SectionofPlasticSurgery, UniversityofMichigan,NorthCampusResearch Complex(NCRC),AnnArbor,Michigan,USA
YAOWANG,MD
DepartmentofOphthalmologyandVisual Neurosciences,UniversityofMinnesotaMedical School,Minneapolis,Minnesota,USA
SUSANWEINKLE,MD
AssistantClinicalProfessor,Departmentof Dermatology,UniversityofSouthFlorida,Tampa, Florida,USA
CHRISTINAWONG,MD
DepartmentofDermatology,ClevelandClinic Foundation,Cleveland,Ohio,USA
JACKZAMORA,MD
MedicalAdvisoryBoardofBovie,MedicalAdvisory BoardofVitroBiopharma,LimitlessMDFounder, JackZamoraM.D.CosmeticSurgery&Aesthetics, Denver,Colorado,USA
ADVANCESINCOSMETICSURGERY
EditorialBoard, iii
Contributors, v
Introduction, xi
ByGregoryH.Branham,JeffreyS.Dover,HeatherJ. Furnas,MarissaM.J.Tenenbaum,andAllanE.Wulc
Preface, xiii
ByGregoryHarrisBranham
TheLatestinCosmeticMedicine: Supplements,Hormones,andEvidence, 1
BySamanthaA.ThiryandJenniferL.Walden
Introduction, 1
Age-relateddiseases,2
Hormonalchangesinmenandwomen associatedwithage,symptoms,and treatmentoptions,3 Summary, 9
SculpturalAestheticSurfaceAnatomyof theFace, 11
ByPeterM.Schmid
Introduction:thesculptorandsurgeon, 11
Facialbeautyandattractiveness, 11
Physicalexamination:facialshapeandform, 12
Canons,Proportions,andShape,13
FacialStructuralPlatform,13
FacialSoftTissuePlatform,16 Summary, 19
TricksforPatientRetentionfor MaintenanceCare, 23
ByKavitaMariwalla
Natureoftheproblem, 23
Discountprograms, 25
Bundledpurchases, 25 Summary, 27
SurgicalSiteInfectionsinCosmetic Surgery, 29
ByEmilyA.Spataro
Introduction, 29
Background, 29
Summaryofcurrentguidelines, 30
Surgicalsiteinfectionsinplastic surgery, 30
Evidence-basedrecommendationsforthe preventionofsurgicalsiteinfectionsin plasticsurgery, 31
Procedure-specificsurgicalsiteinfection prevention, 32
Breastsurgery,32
Abdominoplasty,32
Liposuction,33
Rhytidectomy,33
Blepharoplasty,33
Rhinoplasty,34
Facialalloplasticimplantation,34
Skinresurfacing,34
Otherdermatologicprocedures,35
Riskfactors, 35 Summary, 36
PainControlintheAgeofanOpioid Epidemic, 41
ByRachelC.BakerandJenniferF.Waljee
Introduction, 41
Paincontrol:opioids, 42
Opioidprescribingforsurgicalcare, 42
Alternativeanalgesictreatments, 43
Alternativeanalgesictreatments:nonsteroidal anti-inflammatorydrugs, 43
Alternativeanalgesictreatments: acetaminophen, 43
Alternativeanalgesictreatments:behavioral techniques, 44 Summary, 44
Microneedling, 47
ByShilpiKhetarpal,JonathanSoh,MaraWeinstein Velez,andAdeleHaimovic
Videocontentaccompaniesthisarticleat http://www.advancesincosmeticsurgery. com.
Background, 47
Mechanismofaction, 47
Microneedlinginstruments, 48
Procedure, 48
Contraindicationsandtreatment considerations, 48
Adverseevents, 49
Microneedlingandrejuvenation, 49
Microneedlingandscars, 51
NewSynergisticTricks:Fillers
D Neuromodulators D Technology 5 More thantheSum, 55
ByRyanC.KelmandOmerIbrahim
Introduction, 55
Combiningsofttissuefillerswith neuromodulators, 55
Softtissuefillercombinations, 56
Combinationswithenergy-baseddevices, 58
Intensepulsedlight, 59
Lasers, 59
Nonablativelasers, 59
Ablativelasers, 60
Microfocusedultrasound, 62
Radiofrequency, 63
Radiofrequencywithmicroneedling, 63
Softtissuefillerandsyntheticdeoxycholic acid, 63
Summary, 64
FacialRejuvenation:FatTransferVersus Fillers, 69
ByAliA.QureshiandMarissaM.J.Tenenbaum
Theagingface, 69
Autologousfatinjection,69
Surgicaltechniqueforfatgrafting,70 Injection,71
Commonsideeffects,71 Filler, 72
Anesthesiaandpainmanagement,73 Commonsideeffects,74
Managementofvasoocclusion,74
Authors’ thoughtsonfatversusfiller, 74
SubmentalFatContouring:AComparison ofDeoxycholicAcid,Cryolipolysis,and Liposuction, 75
BySaraHogan,PrasanthiKandula, DanielJ.Callaghan,andJeffreyS.Dover Introduction, 75 Anatomyofthesubmentalarea, 75 Evaluationofthepatientwithsubmental fullness, 76
Deoxycholicacid, 76
Deoxycholicacidpatientevaluation, 76 Preprocedure,78 Procedure,79
Postprocedure,79 Adverseeffects, 79 Complications, 79 Clinicalresults, 80
Cryolipolysis, 80
Cryolipolysispatientevaluation, 80 Preprocedure,80 Procedure,82
Postprocedure,82 Clinicalresults, 82
Adverseeffects, 82 Submentalliposuction, 82 Submentalliposuctionpatientevaluation, 82 Preprocedure,84 Procedure,84 Postproceduralcare,84 Adverseeffects, 84 Summary, 84
SubcutaneousNeckSkinPlasma Tightening, 89
ByJackZamoraandShawnRoman
Videocontentaccompaniesthisarticleat http://www.advancesincosmeticsurgery.com. Introduction, 89 Surgicaltechnique, 90 Preoperativeplanning,90
Proceduralapproach, 90 Miniincisionsuperficialmusculoaponeurotic system/platysmaplication,90 Plasmaskintightening,91
TreatmentsfortheAgingLip, 97
ByLarryKevinHeardandSusanWeinkle
Videocontentaccompaniesthisarticleat http://www.advancesincosmeticsurgery.com.
Introduction:Natureoftheproblem, 97 Surgicaltechnique, 99 Preoperativeplanning,99
Preparationandpatientpositioning, 100
Proceduralapproach, 101
Injectingfillers,101
Injectingneurotoxin, 102
Immediatepostproceduralcareand rehabilitation, 103
Clinicalresultsintheliterature, 103
Potentialcomplications,risks,benefits,and limits, 103 Summary, 104
NonsurgicalPeriorbitalRejuvenation,
107
ByLoreleyD.SmithandStevenM.Couch
Videocontentaccompaniesthisarticleat http://www.advancesincosmeticsurgery. com.
Introduction, 107
Periorbitalskinresurfacing, 107 Chemicalpeels,107 LASERtherapy,109
Neuromodulators, 111 Surgicaltechnique,112 Dermalfillers, 115 Introduction,115 Surgicaltechnique,115
UpdateontheTreatmentof PostblepharoplastyLowerEyelid Retraction, 121
ByDanielG.StrakaandJillA.Foster
Introduction:thenatureoftheproblem, 121 Anatomy,122
RiskFactors,123
TranscutaneousorTransconjunctival?,124
Surgicaltechnique, 126
PreoperativePlanning,126
PreoperativeConsiderationsforPlanning SurgicalTechnique,127
PrepandPatientPositioning,129
ProceduralApproach,130
ImmediatePostproceduralCareand Recovery,133
Potentialcomplications, 133 Management, 133 Discussion, 133
UpdateontheTreatmentofthe SkeletonizedUpperEyelid, 135
ByMorrisE.Hartstein
Videocontentaccompaniesthisarticleat http://www.advancesincosmeticsurgery. com.
DefiningtheBrowFatPad:TheBrowFat PadSuspensionSuture, 143
ByYaoWang,AndrewHarrison,AmyPatel,and GuyMassry
Videocontentaccompaniesthisarticleat http://www.advancesincosmeticsurgery. com.
Introduction, 143 Surgicaltechnique, 144 Preoperativeplanning, 144 Preparationandpatientpositioning, 144 Proceduralapproach, 144 Immediatepostoperativecare, 145 Rehabilitationandrecovery, 145 Clinicalresultsintheliterature, 145 Potentialcomplications,risks,benefits,and limitations, 146 Complications,risks,andmanagement, 146 Benefits, 147 Limitations, 147 Summary, 148
Platelet-richPlasmaforHairGrowth, 151
ByChristinaWongandShilpiKhetarpal
Videocontentaccompaniesthisarticleat http://www.advancesincosmeticsurgery. com.
Introduction, 151 Proceduraltechnique, 152
Preoperativeplanning,152 PreparationandPatientPositioning,157 ProceduralApproach,158 ImmediatePostproceduralCare,158 RehabilitationandRecovery,158 Clinicalresultsintheliterature, 158
Potentialcomplications/risks/benefits/ limits, 159
Summary, 159
HairLossinMenandWomen:Medicaland SurgicalTherapies, 161
ByGoranaKukaEpstein,JeffreyEpstein,andJustin Cohen
Videocontentaccompaniesthisarticleat http://www.advancesincosmeticsurgery. com.
Introduction, 161
Understandingandrogenichairloss, 161
Medicaltherapies, 163
Addressingunderlyingconditions contributingtoandrogenicalopecia,163
Minoxidil,163
Finasteride,164
Low-levellaserlight,164
Platelet-richplasma,165
Microneedling,166
Mesenchymalregenerativecells,stromal vascularfraction,andadiposetissue injections,166
Surgicaltherapies, 166
Introduction,166
Historyofsurgeriesusedtotreatandrogenic alopecia,167
Surgicalproceduresotherthanhair transplants,167
Hairtransplantation,168
Surgicaltechnique, 169
Preoperativeplanning,169
Preparationandpatientpositioning,169
Proceduralapproach,171
Postprocedurecare,173
Futuretherapies, 175
SubcutaneousBodySkinTightening, 177
ByForumPatel,JenniferMacGregor,YunyoungClaire Chang,andAnneChapas
Introduction, 177
Radiofrequency,177
MicorfocusedUltrasound,181
Surgicaltechnique, 181
Preoperativeplanning,181
Preparationandpatientpositioning,181
Proceduralapproach,183
Immediatepostproceduralcare,185
Rehabilitationandrecovery, 185 Potentialcomplications/risks/benefits/ limits, 185 Management, 185 Summary, 185
HandRejuvenation, 189
ByPrasanthiKandula,SaraHogan, DanielJ.Callaghan,andJeffreyS.Dover
Introduction, 189
Agingprocessofthehands, 189 Treatment, 190
TopicalAgents,190
ChemicalPeels,190
Soft-tissueaugmentation, 190
HyaluronicAcid,190
CalciumHydroxyapatite,191
Poly-L-LacticAcid,191
AutologousFatTransfer,191
PotentialComplications,Risks,and Limitations,191
Veintreatments, 192
Sclerotherapy,192
Laser/lightsourcesandenergy-based devices, 192
IntensePulsedLight,192
NonablativeResurfacingLasers,192
AblativeResurfacingLasers,192
Q-SwitchedDevices,193
PhotodynamicTherapy,193
PulsedDyeandPulsedGreenPotassium TitanylPhosphateLasers,193 Summary, 193
NonsurgicalVaginalTreatments, 195
ByFranciscoL.CanalesandHeatherJ.Furnas Introduction, 195
Vaginalhealthissues, 196
Effectonwomen’slives, 196
Theriseofnonsurgicaloptionsforvaginal rejuvenation, 196
Vaginallaxity, 197
Radiofrequencydevices, 197
Lasersinvaginalrejuvenation, 198
Stressurinaryincontinence, 199
Foodanddrugadministrationwarning, 199
Introduction
GregoryH.Branham, MD
TJeffreyS.Dover,MD, FRCPC
FACS Editors
hedesireforcosmeticsurgeryhasinfiltrated cornersofsocietyneverseenbeforeandis onlyexpectedtogrowintheyearsahead.As thenumberofcosmeticsurgeryprocedurescontinues torisethroughouttheworld,sotoodoesthenumber ofspecialistsperformingtheseimportantprocedures. Whenworkingwithapatienttocreatetheirideal image,it ’ scriticaltohavethemostcurrentresources availabletoguideyourpracticeandinformyour decisions.
AdvancesinCosmeticSurgery,nowinitssecondvolume,aimstohighlighttheyear’slatestadvancements andbreakthroughsinthefieldofcosmeticsurgery. Expertsfromthefourcorespecialtieshavecome togethertobringyou,thereader,themostimportant advancesinthisrapidlyevolvingfield.
Subcutaneousbodyskintightening,platelet-rich plasmaforhairgrowth,mi croneedling,subcutaneousneckplasmaskintightening,facialrejuvenation, andtreatmentsfortheagingliparejustahandfulof topicscoveredinthisissue.High-qualityimagesand videosaccompanymanyofthearticles,helpingto furtherdeepenthereader ’ sunderstandingofthese techniquesandprocedures.Whetheryouareplanningtoperformtheproceduresdiscussedhereor learningaboutthemforthefirsttime,wethink
AllanE.Wulc,MD, FACS
youwillfindvalueinwhatthisexcitingserieshas tooffer.
Theeditorswouldliketothanktheauthorsfortheir insightfulcontributions,andallthepioneersinthisfield workingtobringusbettertools,techniques,andwaysof makingtheseeminglyimpossiblepossibleforourpatients.
Wehopeyouwillenjoyreadingthisissueasmuchas weenjoyedputtingittogether.Itisoursincerehope thatthearticlespresentedherewillhelpfurtherbreak downbarriersbetweenspecialtiesandshednewlight oncurrentcosmetictreatments.
GregoryH.Branham,MD
FacialPlasticandReconstructiveSurgery DepartmentofOtolaryngology-HeadandNeckSurgery WashingtonUniversitySchoolofMedicine StLouis,MO,USA
JeffreyS.Dover,MD,FRCPC SkinCarePhysicians ChestnutHill,MA,USA
YaleUniversitySchoolofMedicine NewHaven,CT,USA
BrownMedicalSchool Providence,RI,USA
https://doi.org/10.1016/j.yacs.2019.02.018
2542-4327/19/©2019PublishedbyElsevierInc.
HeatherJ.Furnas,MD,
MarissaM.J. Tenenbaum,MD
HeatherJ.Furnas,MD,FACS
DivisionofPlasticandReconstructiveSurgery
StanfordMedicalSchool Stanford,CA,USA
MarissaM.J.Tenenbaum,MD
PlasticandReconstructiveSurgery
WashingtonUniversitySchoolofMedicine StLouis,MO,USA
AllanE.Wulc,MD,FACS
DepartmentofOphthalmology
UniversityofPennsylvania Philadelphia,PA,USA
DepartmentofOtolaryngology
TempleUniversity Philadelphia,PA,USA
E-mailaddress: branhamg@wustl.edu
Preface
GregoryH.Branham,MD, Editor
Welcometothesecondvolumeof Advancesin CosmeticSurgery. Ourdiverseeditorialstaff hasonceagainsolicitedcontributionsthat willbeofinteresttoallthoseprovidingcosmeticsurgeryandprocedurestopatients.Whetheryouare engagedinasurgicallyorientedpracticeoranofficebasedorminimallyinvasivepractice,thereissomething foreveryoneinthisvolume.Ourlearningisenhanced immeasurablywhenweshareandcompareourtechniquesandresults.Tothatend,youwillseeseveralapproachestothesameproblemorissuethatyoumay encounterinyourpractice.
Inkeepingwithourcommitmenttobeattheforefrontofestheticpractice,wehavecuratedanexceptionalgroupoftopicsthatwillallowthereaderto developagraspofwhatisnewandpermitthereader tomakesenseofwhatiseffectiveandwhatisnot. Topicsinthisvolumerangefromcosmeticmedicines andpaincontrolintheageoftheopioidepidemicto surgicalandnonsurgicaltreatmentsforcorrectionof theoveroperatedpatient.
Therearesomanynewproductsandproceduresbeingdeveloped,andweareinatimeofaccelerateddevelopmentoftechnologyanddevices.Asyoureadthese articles,pleaseconsiderhowtheycanbeusedtoinform
youofwhatmightbeusefulinyourpracticeandalso whatshouldrequirecautionoratleastcarefulconsiderationpriortoadoption.
Manythankstoallofthecontributorswhohavetaken thetimetosharetheirexpertisewithusandallowedusto sharethatwithyou.Wehopethatyouwillfindthisvolumeasengagingandstimulatingasourfirstvolume.We seemtohaveanendlessflowofideasbutwould welcomeanysuggestionsforfuturetopicsthatyou wouldliketoseeincludedinfuturevolumes.
TheeditorswouldalsoliketothankJessicaMcCool andalltheeditorialstaffatElsevierwhohavemadethis volumepossible.Theircommitmenttoexcellencein thisendeavorisevidentinthequalityofthepublication,andwetrustthatwillbeapparenttoyouaswell.
GregoryH.Branham,MD
FacialPlasticandReconstructiveSurgery
Otolaryngology–HeadandNeckSurgery WashingtonUniversity 1020NorthMasonRoad StLouis,MO63141,USA
E-mailaddress: branhamg@wustl.edu
https://doi.org/10.1016/j.yacs.2019.03.001
2542-4327/19/©2019PublishedbyElsevierInc. XIII
TheLatestinCosmeticMedicine Supplements,Hormones,andEvidence
SamanthaA.Thiry,MSN,FNP-C*,JenniferL.Walden,MD,FACS 5656BeeCavesRoad,SuiteE201,Austin,TX78746,USA
KEYWORDS
KEYPOINTS
Provideropinionshaveaneffectontheuseofhormonereplacementtherapy(HRT)withinpractices.Itisimportantfor providerstobeeducatedregardingtheevidencebehindHRTsotheymaysafelyprescribeHRTforspecificpatientswho understandtherisksversusthebenefits.Apatient-centeredapproachshouldbeusedwiththistreatmentoption. ThetruerisksversusbenefitsofHRTanddiseaseprocesses,suchasprostatecancerandbreastcancerrisks,mustbe presentedtopatientsbyeducatedproviderswithoutbias.Ithasbeenprovedthatproviderattitudescontributetouseof antiagingmedicalmethods.Thiscan,inturn,negativelyaffectapatient’squalityoflifebynotprovidingthemwithsafe, monitored,andeffectivetreatment.
Supplementstohelppreventage-relateddiseasescontinuetoberesearchedfortheirtruebeneficialpossibilities. Evidenceexistsregardingspecificsupplementsandtheirchemopreventiveandantioxidantproperties.Cancerisanagerelateddiseaseandmanysupplementsareaimedatreducingtheriskofitsoccurrence.Supplementuseisapatientdrivendemand.
Providersmustbecomemoreinformedaboutsupplementsbyreceivingappropriateeducationregardingtheevidenceso theycangivepatientsappropriatefeed-backwhenpatientinquiriesarise.
INTRODUCTION
Patientsareseekingcaretostoptheeffectsofagingnot onlyfromanexternalstandpointbutalsofromaninternalstandpoint.Asthedemandforantiagingtherapy withhormonesandsupplementsincreases,itisimperativethathealthcareprovidersunderstandtheevidence supportingpropermanagementandinformation regardingalternativetreatmentoptionswithhormones andsupplements[1].
Age-relateddiseasescontinuetoberesearchedfor preventionandoptimization[2].Antiagingspecialists useamedicalframeworkthattargetsage-associated
diseasesassymptomsofaging.Theconceptofafountainofyouthhasbeenaroundforcenturiesbutnow, withmodernmedicineandadvancementsintechnology,antiagingpractitionershavedevelopedasa specialty,withtherequirementsofunderstandingdiseasesassociatedwithageandhowtophysiologically decreaseapatient’sriskofacquiringanage-relateddisease.Variousdietaryandpharmacologicinterventions havebeenshowntoincreaselifespan[3].Also, althoughagingisconsideredanaturallifeprocess,optimizationofqualityoflifecontinuestobeafocus.To meetthisdemand,anincreasinglypopularfocushas
DisclosureStatement:Theauthorshavenothingtodisclose.
*Correspondingauthor, E-mail address: Samantha.thiry.drwalden@gmail.com
https://doi.org/10.1016/j.yacs.2019.01.001
2542-4327/19/©2019ElsevierInc.Allrightsreserved.
beengearedtowardpreventingexistingdiseaseprocessesfromworsening,aswellastreatingdisease processesthroughtherapeuticmanagementwithhormonesorsupplementation[3,4].
Patientshaveshiftedthefocusofsurvivingto thrivingthroughouttheirlifetime.Improvingapatient’ s qualityoflifeisanimportantconceptinantiagingmedicine[2].Hormonalshiftsoccurduringtheagingprocessthatcauseseveralphysiologicchangesandclinical presentationofsymptoms.Forwomen,symptomsof menopausecanseverelyaffectoverallqualityoflifeas radicalshiftsandimbalancesofestrogenandtestosteronehormonesoccur[5].Andropause,definedasa continualdeclineintestosteronewithage,affectsboth menandwomen[5,6].Hormonetherapiesareeffective inthetreatmentofsymptomsofage-relatedhormonal changesformenandwomen,whichmakesitisimportanttounderstandtheevidenceregardingriskversus benefitofthetreatmentprescribed.Ithasbeenproved thatmanyproviders’ opinionsonhormonetherapies arenotcongruentandoftenmisinformed,causing bias[7].Thistendstocausealackofcredibilitywith specifictreatmentprotocols.Patientscanendup sufferingwithsymptomsofhormonalshiftsandthe physiologicchangesofageduetolackofappropriately prescribedcareandinformationregardingthetruerisks versusbenefitsoftreatment[7,8].
Thisarticleexaminesthemultifactorialapproachto antiagingmedicinewithhormonereplacementtherapy (HRT)andtreatmentusingnutraceuticalstohelppatientsachieveanimprovedqualityoflife,aswellas decreaseriskfordevelopmentofdiseaseprocessby optimizingtheirhealthfromaphysiologicevidencebasedstandpoint.Itexamineswhatsymptomsofaging canbeimproved,aswellashowagingisdefined,to improvepatients’ overallqualityoflife.Potentialrisks andbenefitsofHRT,aswellasnutraceuticalsupplementation,arediscussed.Assessmentofproviders’ knowledgeandtheoptionsofthesetypesoftherapies areexamined,aswellasappropriateassessmentand treatmentinmenandinwomen[4–8].
Age-relateddiseases
Antiagingmedicineisanevolvingmovementwiththe intenttohelppatientsdecreasethedevelopmentof age-relateddisease,aswellasimprovethequalityof thenormalagingprocess[2].Thismovementhas beeninplacefordecadesbuthasrecentlybecome muchmoreadvancedthroughresearchandtechnology.
Onewaytodefineagingisthatitistheresultof continuousinteractionbetweenanindividual’sgenetic makeupandenvironmentalfactors,characterizedby
lifelongdamageaccumulationandprogressivelossof tissueandorganfunctionality[9].Agingisdirectlyassociatedwithanincreasedriskofdiseasedevelopment. Commonage-relateddiseasesincludeneurodegenerativedisorders,cardiovasculardisease,diabetes,osteoarthritis,andcancer[9].Hypertension,highglucose, cholesterol,andtriglyceridelevelsareage-relatedrisk factorsformorbiditythatincreasewithage.Theconcept oftargetingage-relateddiseasesthroughpreventionon amolecularlevelisimportanttounderstandingwhich treatmentmethodswilldecreasetheeffectsofaging, notonlyfromaphysiologicstandpointbutalsofrom asymptomaticstandpoint[9].Directlytargetingtheagingprocessonamolecularlevelversustargetingagerelateddiseasesorsymptomsisaviablestrategy [9,10].Toslowtheagingprocess,therapiesthatare considerednonstandard,suchasblood-basedtherapies,arebeingprescribedandtried[9].
Aspatientscontinuetoseekoutwaystodiminishor decreasetheeffectsofaging,itisimportantforproviderstobeup-to-dateoncurrenttreatmentoptions. Hormonetherapiesandsupplementsarebecoming increasinglypopularastreatmentandpreventionof age-relatedconditions.Age-relatedconditionsarethe leadingcausesofdeath,notonlyintheUnitedStates butalsoworldwide.Theyarealsotheleadingcauseof healthcareexpenditures[9].Bydelayingtheagingprocess,thedelayofage-relateddiseasesoccurs.Delaying aging,resultingin2.2yearsofadditionallifeexpectance,wouldyieldtheUnitedStates$7trilliondollars insavingsover50years.Thetargetofsinglepathologic conditions,suchascancerorheartdisease,yieldsless savings[9].
Becauseantiagingsciencehashugepotentialfinancialbenefits,ithastremendouscommercialopportunities.Scientificbreakthroughshaveledtoantiaging sciencehavingamorevalidreputation[9].Provider opinionsandapproachesareoftenskewedwhenit comestosubjectssuchasoff-labeladministrationof medicationmanagement[7,8].Therefore,presenting theevidencebehindsomeHRTandnutraceutical blood-basedapproachesofantiagingisimportant whencreatingapatient-centeredplanofcare[1].Given themultiplegenes,processes,andpathwaysassociated withaging,therearemanyopportunitiestodevelop pharmaceuticalstotargetthesepathways[9].Tounderstandtheantiagingprocess,onemustfirstunderstand whatcausesagingandthespecificsignsandsymptoms oftheagingprocess[2,3].Thedescriptionofagingasa timeofdeclineandsufferingisevidentbecauseagerelateddiseasesoftencausethephysiologicdeclineof apatient,inturncausingthepatienttosuffer[2,3].
Hormonalchangesinmenandwomen associatedwithage,symptoms,and treatmentoptions
Age-relatedhormonalchangesinwomen
Asignificantage-relatedhormonalchangeforwomenis menopause.Menopauseisusedtodefinethenatural, systemicdecreaseofendogenousestrogenproduction fromtheovaries,causedbyphysiologicdepletionofa woman ’sovarianreserve[11].Thisprocessoccursin theagingwomanandmanifestsasthecessationof mensesandsubsequentendoffertility.Inmanywomen, vasomotorsymptomsoccur,aswellasotherphysiologic issues.Vasomotorsymptomscommonlyexperienced duringmenopauseincludevaginaldryness,hotflashes, andirregularmenstrualpattern.Menopausalsymptoms cangreatlyaffectawoman’soverallqualityoflifeandpatientswillbringthesetoaprovider’sattentioninsearch ofrelief[11,12].Aprogressivedeclineinandrogenlevels alsooccursasawomanincreasesinage.Serumconcentrationsoftestosteroneinwomenolderthantheageof 50yearsareapproximatelyhalfofthatofwomenin aged20to30years[13,14].Thereareseveralsymptoms ofandropauseinwomen,includingunexplainedfatigue, lowlibido,anddecreasedsenseofwellness.Testosterone therapyhasbeenadministeredtowomenfordecadesto improvesexualdysfunction[11,15].Femalesexual dysfunctionisanissueforapproximately43%ofwomen 18to59yearsofage[14].
Menopauseischaracterizedbyadecreasedproductionofbothestrogenandandrogen[5,11].Itisimportanttounderstandtheprocessofaromatization,which istheconversionofthebody’sexcesstestosteroneinto estrogen.Expressionofaromataseisimportanttothe adiposetissue,skin,andbonebecauseitslowsthe rateofpostmenopausalboneandcollagenloss[5]. Testosteronelevelsdeclinegraduallywithage,rather thanshowingaprecipitousdecreaseatthemenopause transition[13].DifferenttypicalHRTplansofcareare usedinpremenopausal,perimenopausal,andpostmenopausalwomenduetohormoneshiftsduring eachphaseofhersexualmaturation[11].Eachphase isassesseddifferentlyforrisksandbenefitsassociated withHRT,thereforemakingitincreasinglydifficultfor aprovidertomanageapatient’ssymptomstoimprove qualityoflifethroughHRT[11].
Femalesexualdysfunctionandhyposexualdesireare diagnosesthatarereviewedasissuesthatcanoccurinthe premenopausal,perimenopausal,orpostmenopausal phases[12].Somestudieshaveshownthatupto50% ofwomensufferfromfemalesexualdysfunction.Female sexualdysfunctionischaracterizedbylowsexualdesire,
diminishedsexualarousal,vaginaldryness,anddifficulty achievingorgasm.Somewomenenterintomenopause naturally,whereasothersenterintomenopauseviasurgicalmeanssuchasahysterectomy[11].IntheUnited States,anationalsurveyconcludedthatnearlyhalfof womenaged57to85yearsexperienceatleast1sexual problem,themostcommonissuebeinglowsexual desire.Therehasbeenalandmarkstudyperformedby Laumannandcolleagues[12]thatfoundthat32%of womenages30to39yearshadlowsexualdesire.Therefore,itisnotonlyperimenopausalandmenopausal womenwhoareseekingasolutionforadecreasedqualityoflifelikelyduetohormonaldisruption.Understandingthemechanismofactionofandrogensinrelationto thefemalebodyisimportantwhenconsideringtheoverallbenefitforpatientsseekingreliefofandrogendeficiencysymptoms[12].
Androgendeficiencyinwomen
Theorgansdirectlyresponsibleforproductionoftestosteroneinwomenaretheovariesandadrenalglands, althoughtestosteroneisalsoconvertedperipherally fromandrostenedione,whichisalsoproducedinthe ovariesandadrenals[11].Androgendeficiencyinwomen causesdecreasedleanbodymass,increasedbodyfat,thinningorlossofhair,osteopenia,orosteoporosis,which presentasclinicalsigns.Symptomsofandrogendeficiencyincludelowlibido,fatigue,lackofasenseofwellbeing,orgasmicdysfunction,arousaldisorder,vasomotor symptoms,insomnia,anddepression[11,16].
Betaendorphinsincreasewithtestosteronelevels, causingmood-enhancingeffects[5].Awoman’squality oflifeisgreatlyaffectedbyadecreaseinandrogens,not simplybecauseofsexhormones.Multipleorgansrely onandrogensforactionsuchasincreasingbonemass, causingerythropoiesis,augmentingcertaincognitive behaviors,stimulatingmusclegrowth,stimulatingkidneygrowth,andmodifyingthepatternofadiposetissue deposit[5].Interestingly,thethyroid,breast,endometrium,colon,lung,skin,andadrenalsareallaffected becauseandrogenshaveadirecteffectonthetissueof eachorgan[5].Androgensmayaffectsexualdesire, bonemineraldensity,musclemass,andstrength,as wellasadiposetissue.Theadditionoftestosteronetherapyintestosterone-deficientwomenhasaneffectonestrogenproductioninthebrain,bone,andskin fibroblasts,amongothertissues[5].
Assessmentoffemaleandrogendeficiency Femaleandrogendeficiencyisassessedthroughsubjectivequestionnairesand,therefore,alackofobjectiveinformationcancauselackofconsistencybetween
providerassessmentandthetreatmentplan.Theidea thatandrogendeficiencyisassessedthroughsubjective meanscausescontroversyamongproviders[8,12].There havebeenseveraltoolsdesignedtoscreenwomenfor hyposexualdesiredisorder(HSDD)[12].TheDecreased SexualDesireScreener(DSDS)isavalidateddiagnostic toolforgeneralized,acquiredHSDD.TheDSDSis meanttobeapproximatelysensitiveandspecificfor diagnosisofHSDDinwomen,independentofmenopausalstatus.The DiagnosticandStatisticalManualof MentalDisorders, 5thedition,listsspecificcriteriaforthe diagnosisoffemalesexualinterestorarousaldisorder; 3outof6symptomaticscreeningassessmentsmustbe answeredwithayesfordiagnosis[11].
Interpretationoflaboratorydataassociatedwith decreasedavailableandrogensforwomenincludethe reviewoffreeandtotaltestosterone,aswellassex hormone-bindingglobulin(SHBG)[13].Freetestosteroneisbiologicallyavailabletestosterone,whereas thebioavailabilityoftestosteronefortheconversion intoestrogensdependsonthelevelsofSHBG.Ina normalscenario,only1%to2%oftotaltestosteronecirculatesunbound.SHBGbindsabout66%oftotalcirculatingtestosterone.Therestoftestosteronecirculatingis boundbyalbumin.Itisassumedthatthenon–SHBGboundcirculatingtestosteroneisbiologicallyactive [13].EstrogenandthyroxineincreaseSHBG.Testosteroneandglucocorticoids,growthhormone,andinsulinsuppressSHBG.Itisdifficulttomeasuretestosterone levelsinwomenwhentheyareatverylowlevels[13].
Testosteronetherapyintheagingwoman
DatafromseveralstudiessuggestthatcombinedHRTandrogentherapymaybebeneficialtowomenwho arepostmenopausalwhocomplainoflowlibido despiteestrogentherapyorasmonotherapyinwomen whoarepostmenopausalwithfemalesexualdysfunction.Studieshaveconcludedthatnosignificantincrease ofliverenzymesorcardiovascularriskfactorsoccurred withtheadministrationoftestosteronetherapy[11]. Therearemultipleformsoftestosteronetherapyin variousroutesofadministrationavailabletowomen [5].Subcutaneoushormoneimplants;intramuscular injection;andtransdermal,oral,andvaginaladministrationofhormonereplacementareamongthose offeredtowomeninsearchofandrogendeficiency symptomrelief[5].
Safeadministrationofhormonereplacement therapyforwomen
Itisextremelyimportantforthepatientandprescriber tounderstandtherisksversusbenefitsofHRTfor
women.Eachindividual,duetofamilyandpersonal history,havevariablesthatareimportantforaprovider toconsiderwhendevelopingatailoredtreatmentplan forthepatient’sneeds.Womenmusthaveanactiverelationshipwiththeirobstetrician-gynecologist,anddocumentedhistorymustbereviewedbythetreating physician[11].
Abnormalmenses,hirsutism,elevatedbloodpressure,andmoodswingsaresomeoftheassociated issuesthatmayoccurduringandrogentherapyfor women[11].
Women,hormonereplacementtherapy,and cardiovascularevidence
Notably,estrogenhasantiatheroscleroticandantiinflammatorypropertiesthatmayprotectwomenfrom cardiovasculardiseasedevelopmentthroughmodificationofthelipidprofile[17].Itisnotedthatwomen whoarepremenopausalhavehigherhigh-densitylipoproteincholesterolandlowerlow-densitylipoprotein cholesterollevelscomparedwithmen,whichsignificantlyreversesaftermenopause[17].Testosteroneis knowntobeproducedbytheovariesandsomeofthe femalebody’stestosteroneisconvertedintoestrogen, primarilywhenandrogenlevelsarehigherduringthe premenopausalstate[5,17].Theconvertedestrogen hasbeneficialeffectsonvascularendotheliumand smoothmuscletissue.Menopauseandthepostmenopausalperiodmayberiskfactorsfordevelopingcoronaryheartdisease.Directlyfollowingmenopause, thereisahormonallyrelatedriskforthedevelopment ofhypertension,coronaryarterydisease,congestive heartfailure,andcerebrovasculardisease,whichare alsoage-relateddiseases[2,17].TheDanishOsteoporosisPreventionStudyrecentlynotedinacontrolled randomizedtrialthatmenopausalhormonetherapy canhavethebeneficialeffectofareducedrateofcoronaryarterydisease.Hormonaltherapymaybeharmful andisnotadvisedinthesettingofpreexistingcoronary disease,cerebrovasculardisease,orahistoryofthromboembolicdisease[11].Hormonaltherapymustbe observedforrisksandbenefitsbytheadministering providerusingapatient-centeredapproachandindividualizeddiscussion[11,17].
Hormonereplacementtherapyandbreast cancerconcerns Ithasbeenreviewedthattherearenovalidrandomized orobservationalclinicalstudiestoprovideappropriate evidencethattestosteronehasaninfluenceonbreast cancerriskwhenaddedtoconventionalpostmenopausalhormonetherapy[14].Thisisasignificantpoint
ofinformationtoprovidetopatientsinquiringabout HRT[14].Breastcancerdiagnosisrepresentsabout 23%ofallcancersinwomen.Itisnosurprisethatit isanimportantsubjectbecauseitistypicallyanagerelateddiseaseandisacommonconcernforpatients consideringHRT[18].Breastcancerincidenceis increasingworldwide.Weightgaininadulthoodisassociatedwithanincreasedriskofbreastcancerinpostmenopausalwomen.Studiessuggestthatweightgain beforeandaroundmenopausalagemaybea determinantforthedevelopmentofbreastcancerin postmenopausalwomen[18].Increasingawoman’ s testosteroneleveltoamoreoptimallevelhasthe benefitofdecreasingcentralvisceralfat,increasing metabolicrate,anddecreasingoreventreatingobesity. Testosteronealsohasthebenefitofincreasingthebeta endorphinsresponsibleforsenseofwellbeing[13].Ifa womanisfeelingabettersenseofwellbeingsheismore likelytobephysicallyandsexuallyactive[13]. Decreasingobesityriskforwomenbeforeandduring menopauseviatestosteronetherapydecreasesariskfactorforthedevelopmentofbreastcancer[18,19].Recent clinicaldatasupportarolefortestosteroneinbreast cancerprevention[19].Womenwithsymptomsofhormonedeficiencywhoaretreatedwithdosesoftestosteronealoneorincombinationwithanastrazolevia subcutaneousimplantshaveshownareducedincidenceofbreastcancer.Inaddition,testosteronetherapy alongwithanastrazolehasbeenstudiedtoalleviate symptomsofhormone-deficientbreastcancersurvivors andwasnotassociatedrecurrentdisease[19].
Studieshaveshownthattestosteroneandanastrazolesubcutaneousimplantsplacedintissuesurroundingmalignanttumorssignificantlyreducesbreast cancertumorsize.Testosteronetherapyhasbeen reviewedandthereareseveralsupportingdatathat notethedirectantiproliferative,protective,andtherapeuticeffects[19].
Provideropinionsofhormonereplacement therapydespiteevidence Therearedifferingopinionsregardinghormone replacementtherapiesthataffectnotonlyaphysician’ s willingnesstoprescribebutalsoapatient’swillingness tousehormonereplacementasatherapy.Partofthis disarrayisduetoalackofprotocolandcontinuedcontroversyaboutnormalandrogenlevelsinwomen.Itis alsodifficulttoassessforandrogendeficiencyin womenbecausethesymptomologyoverlapswith severalothermedicaldiagnoses[8,11].Theprovider mustruleoutothercomplicationsthatcouldbepresentingasriskstopatient’shealth.Providers’ opinions
havebeenobservedviasurveyandithasbeennoted thatrespondentscorrectlyidentifiedtherisksofHRT only28%ofthetime,and67%ofprovidersoverestimatedtherisksandbenefitsofHRT.
Multiplesourcesofvaliddatasuggestthatcombined HRT-androgentherapymaybebeneficialtowomen [11].Providersneedtobeeducatedregardingstudies thatconcludedthatnosignificantincreaseofliverenzymesorcardiovascularriskfactorsoccurredwiththe administrationoftestosteronetherapy[16].
Menandtestosteronesupplementation
TestosteronesupplementationintheUnitedStateshas increasedsubstantiallyovertheyears.Testosteroneprescriptionsincreasedby1700%from1994to2003and donotshowanysignsofdecreasinginpopularity[4]. Asthispatient-drivenpopularityoftestosteronesupplementationincreases,itisimportantforproviderstounderstandthesignsandsymptomsassociatedwiththe declineoftestosteroneinthemalebody,aswellas appropriatetreatmentoptionsandriskfactors[4].To ignoretheincreasedpatientdemandfortreatmentof theassociatedsymptomsofandropausecausesskewed perspectivesregardingthetruerisksandbenefitsofHRT formenthroughouttheagingprocess[4].
Menandandropause
Menundergoingtheagingprocess,especiallyandropauseortheprogressivedeclineoftestosterone,often searchforsymptomrelief.Decreasedtestosteronelevels arealsoreferredtoashypogonadism[20].Lowlibidois thesymptommostassociatedwithhypogonadism, althougherectiledysfunction,decreasedmusclemass andstrength,increasedtotalbodyfat,decreasedbone mineraldensity,anemia,gynecomastia,decreased mentalcapacity,andskinandhairalterationsalsooccur [20].Decreasedqualityoflife,adiminishedsenseof wellbeing,andinsomniaareadditionalsymptomspresentinandrogen-deficientmen.Onclinicalpresentation,decreasedmusclemassandstrength,decreasein bonemass,osteoporosis,andincreasedcentralbody fatmaybenotedinapatientwithtestosteronedeficiency[20,21].Whenassessingfortestosteronedeficiency,itisimportantfortheprovidertousean approachthatconsidersotherage-relateddiseasesby usingobjectiveinformation,suchaslaboratorywork, toassessthepatientforissuesthatmaybepresentin additiontoandrogendeficiency.
Testosteronedeficiencyisalsoassociatedwith increasedcardiometabolicrisk.Forexample,total testosteronelevelsareinverselyassociatedwithriskof cardiovascularevents.Testosteronedeficiencyis
associatedwithendotheliumdamageandtestosterone therapyenhancesendothelialrepairandfunction,and increasessynthesisandreleaseofendothelialnitricoxideinthebody’svascularsystem[20].Testosterone deficiencyisassociatedwithincreasedsystolicblood pressureandincreasedarterialstiffness,whicharerisk factorsthatcanleadtofurtherdevelopmentofagerelateddiseases,suchascoronaryarterydisease,hypertension,andhypercholesterolemia[2,4,20].
Diagnosinglowtestosteroneinmen
Thedeclineoftestosteroneformenisabout1%peryear aftertheageof30yearsandreachesa30%declineby theeighthdecadeoflife[4].TheAndrogenDeficiency intheAgingMale(ADAM)questionnaireisanimportantassessmenttoolwhenassessingformaleandrogen deficiency.Testosteronedeclinesasmenageandthe symptomsassociatedwiththisdeclinecauseanabundanceofunwantedpatientsymptomsthataffecttheir overallwellbeing[4].Assessmentregardingthesubjectivepresenceofthemostcommonlyreportedandrogen deficiency–associatedsymptomsmustbeperformedby adiagnosingprovider.Thesymptomsassociatedwith thisdeclinecauseanabundanceofunwantedpatient symptoms,suchasfatigueanddepression,anda decreasedsenseofwellbeing[4].Whenassessingfor thereasonsforexistingsymptomsofhypogonadism, itisimportanttocheckpatient’sserumtotaltestosterone,freetestosterone,andSHBG,aswellasthetotal prostate-specificantigen(PSA)ifappropriateforpatient’sagerange,whenconsideringprescribingtestosteronetherapy[21].
Testosteronetherapybenefitsreported Benefitsoftestosteronetherapyinmeninclude increasedlibido,sexualfunction,bonedensity,muscle mass,bodycomposition,mood,erythropoiesis,cognition,qualityoflife,anddecreasedcardiovascular disease.Improvedsexualdesire,function,andperformancearereportedbymenreceivingtestosterone replacementtherapy(TRT)[4,6,20].
Thecognitiveeffectsofandrogendeficiencyareassociatedwithdeclineinvisualandverbalmemory.Men withhigherratiosoftestosteronetoSHBGshowa decreasedriskofAlzheimerdisease.Thiswasfoundin theBaltimoreLongitudinalStudyofAging,aprospectivelongitudinalstudy.ItwasnotedthatriskforAlzheimerdiseasewasreducedby26%foreach10unit (mmol/mmol)increaseinfreetestosteroneat2,5, and10years.Therearealsowell-reporteddatafora strongcorrelationbetweenserumlevelsoftestosterone andcognitiveperformanceinmathematicalreasoning
andspatialabilities[6].Testosteronetherapyinhypogonadalmenmayhavesomebenefitforcognitiveperformance,especiallyinoldermenwhoareatan additionalriskofdevelopingdementiaorAlzheimer becausethesearetypicallyage-relateddiseases[6].
Glycometabolicandcardiometabolicfunctions,as wellasbodycompositions,arenegativelyaffectedby testosteronedeficiencyorhypogonadism[20].Testosteroneanditsmetabolite,5alpha-dihydrotestosterone, regulateenergymetabolism,musclegrowth,andmaintenanceandinhibitadipogenesis.Aninverserelationshipbetweentestosteroneandinsulinresistancehas beenpostulatedandhigherphysiologiclevelsoftestosteroneseemtobeprotectiveagainstthedevelopmentof typeIIdiabetesmellitus[20,21].Theprevalenceoftype IIdiabetesmellitusandmenwithhypogonadismisas highas33%[21].IthasbeenshownthatTRTcauses animprovementinglycemiccontrol,aswellasinsulin resistance,inmenwithtype2diabetes[21].Subcutaneoushormoneimplants,intramuscularinjection,transdermal,andsublingualadministrationofhormone replacementareamongthoseofferedtomeninsearch ofandrogendeficiencysymptomrelief[6].
Safeadministration:prostatecancerriskand othertestosteronereplacementtherapy considerations
Prostatecancerandtheroleoftestosteroneinthedisease oftenresultsinconfusion.Ithasnotbeenassessedthat testosteronereplacementdirectlycausesprostatecancer, althoughitsadministrationinthepresenceofacarcinomacanenhancethecarcinomapresent[4].Prostate cancerisacommon,androgen-dependentcancer.Therefore,testosteroneadministrationisabsolutelycontraindicatedinmenwithclinicalprostatecancer.Somemen arediagnosedwithprostatecancerlessthan4,therefore establishingabaselineisimportant[4].Assessingfor prostatecancerriskisimportantwhenassessingtherisks versusbenefitsoftestosteronetherapyinsymptomatic, androgen-deficientmen.Datahaveshownthatsuggest administrationoftestosteroneinandrogen-deficient mencanproducemodestincrementalincreaseinserum PSAlevels.Theseincrementsshouldgenerallybeless than0.5ng/mL;increasesexceeding1.0ng/mLover3 to6monthsareunusual.Recommendationsformonitoringprostate-relatedadverseexperiencesduringTRT inoldermenincludeabaselineevaluationofadigital rectalexamination,serumPSA,andanAUAsymptom scoreforbenignprostatichypertrophy.Also,follow-up evaluationsshouldoccurat3,6,and12months,then annually,withreviewofthepreviouslymentioned monitoringtools[4].
SomeclinicianspracticesafeadministrationofTRT inmenbyperformingaprostatebiopsywhenthereis aclinicalpresentationofprostatecancerriskbeforeprescriptionofTRT.High-gradeprostaticintraepithelial neoplasia(PIN)hasbeenpostulatedtobeaprecancerouscondition[21].Anexaminationofprostates removedatradicalprostatectomyforprostatecancer revealedhigh-gradePINin86%ofcases.Ithasbeen shownthattherewasnoincreasedriskofprostatecancerinhypogonadalmenwithPINtreatedwithtestosteronefor1year[21].Continuedstudiesmustbe performedforlong-termanalysis.Todate,nostudy hasdefinitivelyshownarelationshipbetweenTRT andprostatecancer.Manyprovidersarehesitanttotreat patientsforandrogendeficiencyowingtofearof increasingtheriskforprostatecancer,whereasevidence doesnotsupportthisclinicalprecaution[21].Therefore,prescribersrefrainfromprescribingTRTtomen whosufferandrogendeficiencysymptomsandsideeffectsowingtopresumptionsthatarenotevidencebased[21].
PSAlevelsincreasewithageinmenregardlessof prostatecancerstatus,whichiswhyproperthoroughexaminationandevaluationwithestablishedbaselines aresuchimportantcomponentswhenconsidering TRTrisksversusbenefitsoftherapy[21].
LackofconsistencyregardingtheprescriptionofTRT formenwithhypogonadismleadstoproviderconfusion.Duringtheassessment,theprovidermustunderstandtheprocessofdecidingwhatspecificsymptoms ofagingneedtobeaddressed.Androgendeficiency symptomscommonlyaffectanindividual’squalityof lifeandvitalphysiologicfunctions[4,6].Torestore overallwellbeing,balancingthesehormonestothe levelsofayounger,moreyouthful,andmorewellself isoftenthegoalofHRT[4,6].Itisthoughtthataconsistentdeclineintestosteroneoccursasadirectcauseof age;therefore,restoringtestosteronelevelstothatofa youngerageisthoughttohelpreducecertainagerelatedsignsandsymptoms[4,6,12,20,21].Thishas beenevidentbecausepatientshavehadpositivephysiologicandpsychologicaloutcomesassociatedwithTRT. Becauseofarecentparadigmshift,itisimportantfor providerstobeeducatedaboutthetruerisksoftherapy andtounderstandwhenreferraltoagynecologistor urologistisanappropriateandvitalcomponentfor safeadministrationofTRT[13,22].
PotentialrisksofTRTmustbediscussedwiththepatientandinformedconsentofreceivingthisknowledge shouldbedocumented[13].TRTcancauseerythrocytosis,whichinturncanhaveadversecardiovascularor neurologicevents.TRTcanalsocausetesticularatrophy
andinfertility.SymptomsofBPHmayworsenwith therapy,althoughtheycouldalsoimprove.Acneand otherskindisorders,suchashirsutism,aswellasexacerbationofsleepapnea,mayoccurwithTRT[20].
Nutraceuticalsandantiaging
Anextensiveamountofresearchisstillrequiredto exploretheprofilesandextentsofthebenefitsthatnaturalcompoundsprovide,althoughthereisincreasing evidencethatanutritionalapproachprovidesatool tocombatage-relateddiseases.Senescentcellshave beenidentifiedasthecauseoforganismalaging.Both naturalandsyntheticcompoundshavebeensuggested tohaveantisenescenceactivities,otherwiseknownas senolytics[9].Understandingproinflammatorysignals andprooxidantsignalsisimportanttodevelopmanagementwithantioxidantsandantiinflammatorycompoundsforhealthieraging[9].Polyphenol-richfoods areoneofnature’santisenescentcompounds[9].Specifictypesofpolyphenolshavepropertiesthatnot onlypromotecelldeathofagingcellsbutalsodelay thedeathofhealthytissue.Manysupplementsusepolyphenolextracttoproduceconcentratedpolyphenol withtheintentofhealthpromotionfortheconsumer. Antioxidantandantiinflammatorypropertiesofpolyphenolsreducetheriskofdevelopingage-relateddisease[9].
Thereisevidencethatpolyphenolscontaincardioprotectiveandneuroprotectivefunctionssuchasthe reductionofpostprandialhyperlipemiaandinsulin resistance.Areductioninglucoseuptakeintumorcells inducedbycertainpolyphenolssuggestsananticancer effectinseveralhumancancers[9].Although polyphenol-richnutrientsareasourceofchemopreventive,antioxidant,andantiagingproperties,thereare othernutrientsthathavebeenobservedandareviewed ashavingsimilareffectsonthehumanbody.The followingdescriptionsexplorepopularformsofsupplementationwidelyavailableandsometimesmarketed withantiagingproperties.Chemopreventiveandantisenescentpropertiesarethefocusofpropertiesofeach nutraceuticalorsupplementdescribed[9].
Curcumin
Curcuminisapolyphenol-richsourceoftenusedinthe formofaspice.Curcuminisarootalsoknownas turmericor Curcumalonga.Itisaningredientthatis oftenusedincookingandisoneoftheingredientsin currypowder.Curcuminoidsarethebioactivecomponentsofcurcumin[1,9,23].Thesehavebeenofinterest foryearsinchemopreventionbecausetheycaninhibit carcinogenactivationbywayofcytochromeenzymes.
Curcuminoidsalsoexhibitantioxidantandantiinflammatoryproperties[1,23].Thereisevidenceofcurcumin’sabilitytoinhibitgrowthofcancerstemcells; therefore,thissupplementhasbeenhypothesizedto havethepotentialtoactasanadjuncttreatmentto conventionalcancertreatments,includingchemotherapy[1].
Curcuminispoorlyabsorbedbythebody,therefore makingtherapyachallenge[1].Muchoftheavailable researchoncurcuminfocusesonthepreventionofcolorectalcancer.Thethoughtisthatbecauseofpoorabsorptionofcurcuminbythebody,thespicehasdirect mucosalcontactwiththecolorectaltract[1,23].Curcumintreatmenthasbeenseentoincreasethelifespanin someanimalmodels.Owingtotheobstacleofpoorabsorptionofitshydrophobicityandpoororalbioavailability,newstrategies,suchascurcumin-loaded micelles,arebeingexploredtoimprovedeliveryofcurcumintothebody[9].Animportantstudywasconductedin2006byCruz-Correaandcolleaguesin whichparticipantswhohadfamilialadenomatouspolyposisreceivedcurcumin480mgandquercetin20mg orally3timesadayfor9months.Participantshadan averagedecreaseofpolypnumberby60.4%frombaselineandthemeandecreaseinpolypsizefrombaseline withtreatmentwas50.9%.Additionalstudiesmustbe completedtounderstandthetruebenefitsofcurcumin, althoughthereareevidentbenefitsofsupplementation concludedfrompriorresearch[1,9,23].
Probiotics
Probioticshavereceivedincreasingpopularityfor healthbenefitsandmanypatientsareinquiringhow theymaybeofbenefit.Probioticsarelivemicroorganismsfoundinfermentedfoodssuchasyogurtandkefir. Probioticsarefoundinconcentratedformsinsupplementproducts[1].Probioticsmayhavechemopreventivebenefitsforthegastrointestinaltractandareof particularinterestinpreventingcolorectalcancers. Lactobacillus speciesarecommonlyprovidedinprobioticsupplementcapsules. Bifidobacterium isanother colonizedorganismthatprovestohaveguthealthbenefits[1].Theirmechanismsofaction,whicharethought tobechemopreventive,aremany.Probioticshavethe abilitytoaltergutmicrobiotaand,asaresult,inhibit orinducecolonicenzymesthatregulategrowthof harmfulbacteria,whichinturnbenefitsimmunefunctionandstimulatesactiveanticancermetaboliteproduction.Yogurtisfermentedmilkthatbreedsthe organismsusedinprobioticsupplements.Studiesin womenhavefoundaninverseassociationbetweenconsumptionoffermentedmilkandbreastcancerrisk[1].
TheEPICItalystudyfollowed45,241adultsfor12years andfoundthatyogurtconsumptionmayreducetherisk ofcolorectalcancerbyupto35%.Thisconclusionsuggestsapromisingroleforprobioticorganismsandthe preventionofcolorectalcancer.Trialsareongoingto researchthebenefitsofprobiotics.Thechemotherapeuticeffecthasalsobeennotedinpatientsdiagnosed withsuperficialbladdercancer.Thosetakingoralsupplementationhadahigher3-yearrecurrence-freesurvivalrate[1].Increasingevidencenotesthatthegut microbiotaisinvolvedinthedevelopmentofhuman diseasessuchasobesity,metabolicsyndrome,diabetes, cardiovasculardisease,cancer,andneurodegenerative disorders,whicharecommonlyassociatedwithagerelateddiseases[1,9].
Bvitamins
Bvitaminscontinuetoberesearchedfortheirnecessary roleinaperson’shealthstatusandthereisevidencethat supportsspecificphysiologicfunctionsofBvitamins.VitaminsB3(niacin),B6(pyroxene),B9(folate),andB12 (cobalamin)workinasynergisticfashionaswatersolublevitaminswithprovenvitalrolesinbrainand nervefunctionbysupportinggeneralmetabolicfunction asamechanismofaction[1].Wholegrains,dairyproducts,potatoes,legumes,andbananas,aswellasfish,organmeats,andpoultry,arecommonlyconsumedfood sourcesthatcontainBvitamins[1].IntheUnitedStates, aswellasmanyothercountries,Bvitaminsareincluded asanenrichmentinflour.Thereissomeobservational evidencethathassuggestedtheprotectiveroleofBvitaminsagainstsomecancers.VitaminB3(niacin)protects DNAfromdamagewhenconsumedinhighdoses.There arealsostudiesthatshowthatdailysupplementationof folicacidandvitaminB12over2yearsresultedina methylationofgenesassociatedwithabnormalcell developmentandcarcinogenesis[1].VitaminB9(folate) originatesmainlyingreenleafyvegetables,aswellas certainfruits,andisrequiredforDNAsynthesisand DNAmethylation.ThebiologicalrolesofBvitamins continuetobeexploredanditishypothesizedthat theycouldpotentiallybeimportantincancerprevention [18].TheprotectiveroleofBvitaminsonDNAcontinuestobeexplored,includingtheirroleinbreastcancerbecauseprotectiveeffectshavebeenobservedin populationswithlowfolatestatus.However,more researchisneededtodevelopmoreconclusivesupport forthishypothesis[18].Arandomizedcontrolledstudy completedinNewZealandandAustraliashowedthat dailysupplementationwithvitaminB3wasassociated withlowerincidenceofnonmelanomaskincancers. ResearchregardingBvitaminscontinuestobe
performedandisneededtodrawmoreconclusions regardingBvitaminbenefitstothebody’simmunologic systemandtheirabilitytosupportDNAinpreventionof carcinogeniceffects[18].
Diindolylmethanesupplementorcruciferous vegetables
Diindolylmethane(DIM)andindolearemajorbioactive moleculesofcruciferousplantsknowntoactonenzymes responsibleforthemetabolismofestrogen[24].The mostpotentdietaryindoleisDIMbecauseitisthe mostpotentestrogenblockerassociatedwithlowering riskofbreastcancer[24].ThecancerpreventativepotencyofDIMisunderclinicalinvestigationbecauseof itsimportantroleofblockingestrogenviaitsabilityto maintainhigherlevelsof2-hydroxesterolne.Higher levelsofestrogensareassociatedwithbreast,uterine, andcervicaldysplasia.DIM’sabilitytoreducethesespecificestrogenscausesareductioninclinicalpresentation ofbreast,uterine,andcervicaldysplasia.Cruciferousvegetableshavemanyotherphysiologicfunctionsthatare chemopreventive.DIMsupplementsarewidelyavailable andusedasachemopreventivenutraceutical[24].
SUMMARY
Patientsareseekingtreatmentoptionstoreducethe signsandsymptomsassociatedwithageandagerelateddiseases[2].Antiagingmedicinemustcontinue tobeexplored,streamlined,researched,andbetterunderstoodbyprovidersandpatients,including decreasingriskofage-relateddiseasesthroughhormone replacementtherapiesandwithsupplementsthathave provenhealthbenefits,[1,2,10].
Asthepopularityofhormonalandnutraceutical supplementaltherapiesincreases,itbecomesincreasinglyimportantforprovidersdevelopbetterinformationsetsforpatientsandtonotallowtheiropinions toobscurethefactsthatpresentthebenefitsandrisks ofsupplementationandHRT.UseofHRTandsupplementsasameansofphysiologicallydecreasingtheeffectsofagingmustbedonewithproperknowledgeof therisksversusthebenefitswhencreatinganindividualizedplan.Usingapatient-centeredapproach,therisk ofdevelopmentofseveralage-relateddiseaseprocesses canbereduced[1].Althoughmuchoftheresearch regardingTRTfocusesontreatmentofmen,women alsosubstantiallybenefitfromtreatmentwithtestosterone[5,6,12].
REFERENCES
[1] SandersK,MoranZ,ShiZ,etal.Naturalproductsfor cancerprevention:clinicalupdate2016.SeminOncol Nurs2016;32(3):215–40
[2]MykytynCE.Anti-agingmedicine:apatient/practitioner movementtoredefineaging.SocSciMed2006;62(3): 643–53.Availableat:http://ezproxy.lib.utexas.edu/ login?url5http://search.ebscohost.com/login.aspx?direct5 true&db5cmedm&AN516040177&site5ehost-live.AccessedOctober30,2018.
[3] deMagalhãesJP,StevensM,ThorntonD.Thebusinessof anti-agingscience.TrendsBiotechnol2017;35(11): 1062–73
[4]BhasinS,SinghAB,MacRP,etal.Managingtherisksof prostatediseaseduringtestosteronereplacementtherapy inoldermen:recommendationsforastandardized monitoringplan.JAndrol2003;24(3):299–311.Availableat:http://ezproxy.lib.utexas.edu/login?url5http:// search.ebscohost.com/login.aspx?direct5true&db5cmedm&AN512721204&site5ehostlive.AccessedSeptember 12,2018.
[5] MaiaHJr,CasoyJ,ValenteJ.Testosteronereplacement therapyintheclimacteric:benefitsbeyondsexuality.GynecolEndocrinol2009;25(1):12–20
[6]BassilN,AlkaadeS,MorleyJE.Thebenefitsandrisksof testosteronereplacementtherapy:areview.TherClinRisk Manag2009;5(3):427–48.Availableat:http://ezproxy. lib.utexas.edu/login?url 5 http://search.ebscohost.com/ login.aspx?direct5true&db5cmedm&AN519707253&site5ehost-live.AccessedOctober1,2018.
Whenassessingforriskfactorsofage-relateddiseases,itisimportanttouseappropriateassessment toolsanddiagnosticprocedurestounderstandwhen appropriatereferralsmustbemade[11].Bybuilding credibilitythroughincreasededucationofproviders regardingevidenceofthebenefitsofdietaryandnutraceuticalsupplements,aswellasHRT,patientswillstart toreceivethetreatmentofsymptomsandhealthissues thathaveasignificantimpactontheirqualityoflife [1,13].Thisarticleexaminesthemultifactorialapproach toantiagingmedicinewithtreatmentusingHRTand nutraceuticalstohelppatientsachieveanimproved qualityoflife,aswellasdecreasetheriskfordevelopmentofdiseaseprocessbyoptimizingtheirhealth fromaphysiologic,evidence-basedstandpoint.Understandingsignsandsymptomsofagingisimportant whenmanagingapatient’squalityoflifethrough HRTandsupplementation.Potentialrisksandbenefits ofHRT,aswellasnutraceuticalsupplementation,must bepostulatedonacase-by-casebasisforthesafest,most effectiveapproachinmanagementbytheresponsible provider.Assessmentofproviders’ knowledgeandoptionsofthesetypesoftherapiesasappropriatetreatmentinmenandinwomenmustcontinuebe explored[1,5,6,11].
[7]LevensE,WilliamsRS.Currentopinionsandunderstandingsofmenopausalwomenabouthormone replacementtherapy(HRT)-theUniversityofFloridaexperience.AmJObstetGynecol2004;191(2):641–6.Available at:http://ezproxy.lib.utexas.edu/login?url5http://search. ebscohost.com/login.aspx?direct5true&db5cmedm&AN5 15343254&site5ehost-live.AccessedAugust29,2018.
[8]WilliamsRS,ChristieD,SistromC.Assessmentofthe understandingoftherisksandbenefitsofhormone replacementtherapy(HRT)inprimarycarephysicians. AmJObstetGynecol2005;193(2):551–6.Availableat: http://ezproxy.lib.utexas.edu/login?url 5 http://search. ebscohost.com/login.aspx?direct5true&db5cmedm&AN5 16098892&site5ehost-live.AccessedAugust29,2018.
[9] GurauF,BaldoniS,PrattichizzoF,etal.Anti-senescence compounds:apotentialnutraceuticalapproachto healthyaging.AgeingResRev2018;46(1):14–31
[10]JansonM.Orthomolecularmedicine:thetherapeuticuse ofdietarysupplementsforanti-aging.ClinIntervAging 2006;1(3):261–5.Availableat:http://ezproxy.lib.utexas. edu/login?url5http://search.ebscohost.com/login.aspx? direct 5true&db5 cmedm&AN5 18046879&site 5 ehostlive.AccessedSeptember10,2018.
[11] SwordsKE.Hormonetherapyformenopausalwomenin theprimarycaresetting.JNursePract2017;13(8):562–9
[12] KheraM.Testosteronetherapyforfemalesexualdysfunction.SexMedRev2015;3(3):137–44
[13]DavisSR,TranJ.Testosteroneinfluenceslibidoandwellbeinginwomen.TrendsEndocrinolMetab2001;12(1): 33–7.Availableat:http://ezproxy.lib.utexas.edu/login? url 5 http://search.ebscohost.com/login.aspx?direct 5true&db5cmedm&AN511137039&site5ehost-live.AccessedAugust28,2018.
[14] BitzerJ,KenemansP,MueckAO.Breastcancerriskin postmenopausalwomenusingtestosteroneincombinationwithhormonereplacementtherapy.Maturitas2008; 59(3):209–18
[15] ShufeltCL,BraunsteinGD.Safetyoftestosteroneusein women.Maturitas2009;63(1):63–6.
[16] dePaulaFJF,SoaresJMJr,HaidarMA,etal.Thebenefits ofandrogenscombinedwithhormonereplacement therapyregardingtopatientswithpostmenopausalsexualsymptoms.Maturitas2007;56(1):69–77.Available at:http://ezproxy.lib.utexas.edu/login?url5http://search. ebscohost.com/login.aspx?direct5true&db5cmedm&AN5 16822626&site5ehost-live.AccessedOctober29,2018.
[17] SvatikovaA,HayesS.Menopauseandmenopausalhormonetherapyinwomen:cardiovascularbenefitsand risks.RevistaColombianadeCardiología2018;25(S1): 30–3
[18] ChajesV,RomieuI.Nutritionandbreastcancer.Maturitas2014;77(1):7–11
[19] GlaserR,DimitrakakisC.Testosteroneandbreastcancer prevention.Maturitas2015;82(3):291–5
[20] TraishAM.Benefitsandhealthimplicationsoftestosteronetherapyinmenwithtestosteronedeficiency.Sex MedRev2018;6(1):86–105
[21]RhodenEL,MorgentalerA.Testosteronereplacement therapyinhypogonadalmenathighriskforprostate cancer:resultsof1yearoftreatmentinmenwithprostatic intraepithelialneoplasia.JUrol2003;170(6Pt1): 2348–51.Availableat:http://ezproxy.lib.utexas.edu/ login?url5http://search.ebscohost.com/login.aspx?direct5true&db5cmedm&AN514634413&site5ehost-live.AccessedAugust30,2018.
[22] PatrickSelphJ,CarsonCC.Testosteronereplacement therapyinmenwithprostatecancer:whatistheevidence?SexMedRev2013;1(3):135–42
[23] VemuriS,BanalaRR,SubbaiahGPV,etal.Anti-cancer potentialofamixofnaturalextractsofturmeric,ginger andgarlic:acell-basedstudy.EgyptJBasicApplSci 2017;4(4):332–4
[24] ManchaliS,KotamballiN,MurthyC,etal.PatilCrucial factsabouthealthbenefitsofpopularcruciferousvegetables.JFunctFoods2012;4(1):94–106
SculpturalAestheticSurfaceAnatomy oftheFace
PeterM.Schmid,DO,FAOCOOHNS,FAACS PrivatePractice,1308SumnerStreet,Suite100,Longmont,CO80501,USA
KEYWORDS Aestheticsurgery
KEYPOINTS
Artistictrainingemphasizesline,shape,andforminhumananatomy. Sculptingteachesperfectpractice.
Lightingcriticallydisclosesnuancesofsurfaceform.
Aestheticanatomydirectscosmetictherapy. Comparativeanatomydefinesgenderdifferences.
Tocapturenature,youmustseeandunderstandher.
EDOUARDLANTERI(SCULPTOR)
INTRODUCTION:THESCULPTORAND SURGEON
Cosmeticsurgeonsarethesculptorsofhumanform.To surgicallyalterthehumanface,bestpracticesrequirea profoundunderstandingofanatomicform,function, structuralaesthetics,andharmony(Fig.1).Complex bydesign,outwardappearanceisfabricatedbyage,genetics,gender,andethnicity,whichareallcontinuously remodeledovertime.Althoughculturesimpartunique biasesoniconicbeauty,thechallengetoaestheticsurgeryistoappealtothepatient’svisualandemotional needs.
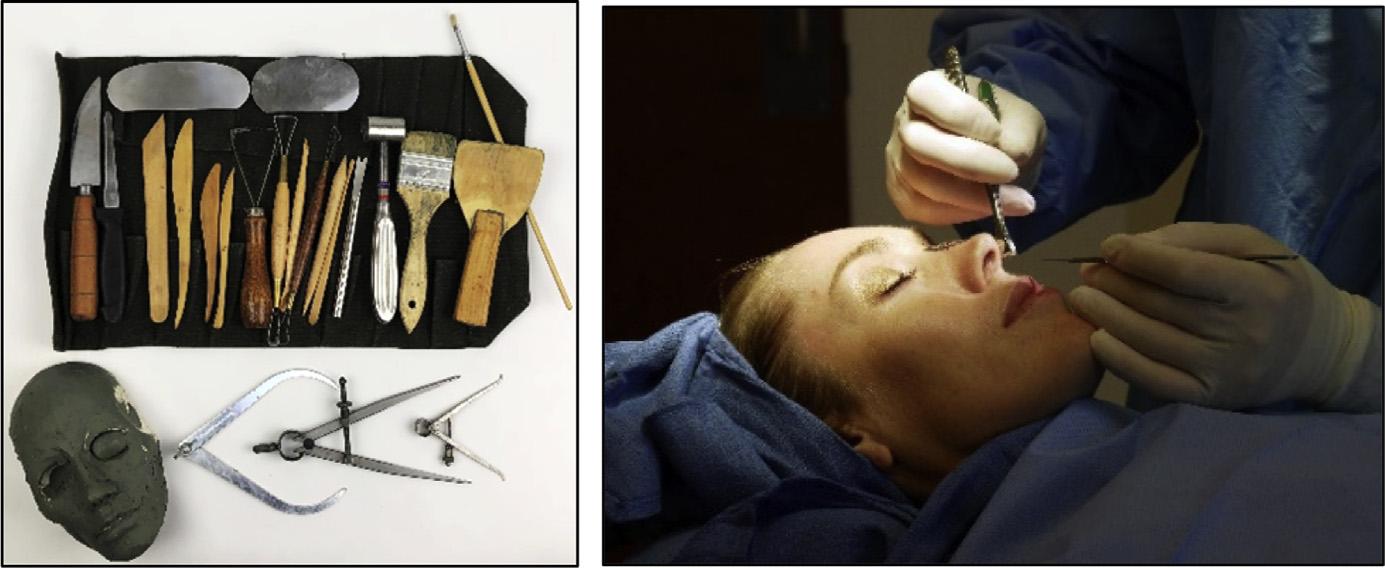
Anidealtrainingmodelforstudyingaestheticfacial anatomyisthrougharteducation.Sculptinginclayis apowerfuldisciplinethattrainstheeyeandhones thesurgeon’svisualassessment,dexterity,acumen, andfinessetooptimizeone’ssurgicalresults.Itallows themindtocreatevisual,tactile,andcommunicative
E-mailaddress: drs@iaprs.com
https://doi.org/10.1016/j.yacs.2019.02.015
2542-4327/19/©2019ElsevierInc.Allrightsreserved.
connectionsotherwisemissed.Suchtrainingdeepens theunderstandingofaestheticanatomy,itsconstruction,andnuancesof3-dimensionalfacialform.It broadensperspectiveandperceptions,andfromsense (theabilitytorecognizeshapes)istranslatedfromthe skeletontothesurfaceofthebody.Workingfromthe livehumanmodelandusingsculpturalprinciples,the facialstructureisappraisedbysculpturalratios,proportion,symmetry,silhouettelines,anglesandplanes, mass,shape,volume,form,interrelationships,distinction,andphysicalrhythm(Fig.2).
AlbertEinsteinoncestatedthat “afteracertainlevel oftechnicalskillisachieved,scienceandarttendtocoalesceinesthetics,plasticityandform.” Assuch,theintegrationofartintoscienceasthesculpturalprinciplesof facialanatomyfollows.
FACIALBEAUTYANDATTRACTIVENESS
Humansarehardwiredtorespondtovisualimagesof thehumanfaceandbody,andthisresponseislikely linkedtoevolutionaryties[1].Attractivefacespossess
aconstellationofmature,neotenous,andexpressive facialfeatures.Aestheticjudgmentsoffacialbeautyare groundedinmathematicalaverageness,symmetry, youthfulness,sexualdimorphism,familiarity,sizingup,andotherspecifictangibles[2].Attractiveand youthfulfacesexudepleasingharmonythroughvibrant skintone,balancedvolumetricfullness,andcomplementaryfeatures.Thetissueshapesareblendedinto
homogenous3-dimensionalcurvesandarrangements, preciselylayeredoverskeletalform,resultingineven reflectivehighlights,andinsomepredominantlight andshadoweffectsportrayingvolumetric sculptural aestheticmarkers (Box1).
Beautyisanordertoform,asubtlesynergistic compositionofgeometry,proportion,volumes,and planes.Themoresymmetrictheface,themoreattractiveisitsperceptioninbothsexes.Facialbeauty,however,iscuriouslyintriguingforitssubtleimperfections anddifferences.Asymmetrytoamillimeterordegree createsaninterestanduniqueaesthetictoappearance incertainindividuals.
Womanattractivebeautyisoutlinedbyflowing curvilinearshapesandforms,whereasmanattractivenessisframedbydefinition,planes,squareness,andangularity.Thesurgeonmustremainvigilanttodiscerning thesedimorphicdiscrepanciesofgender-specificanatomyorthevariationsofformthatoccurinthetypical ortheagingpatient.
PHYSICALEXAMINATION:FACIALSHAPE ANDFORM
Facialappearanceiscomposedoforganicshapes arisingfromthefoundationofthecranialandfacial bones,juxtaposedbysofttissueandcomplementary features.Facialcharacteristicsshouldbestudiedlike thesculptor,bybothvisualinspectionandsofttissue palpation.Keenobservationdiscernsthesubtletiesof formuniqueontothepatient,andrelevanttogender, ethnicity,age,orthefootprintsofprevioussurgeries.
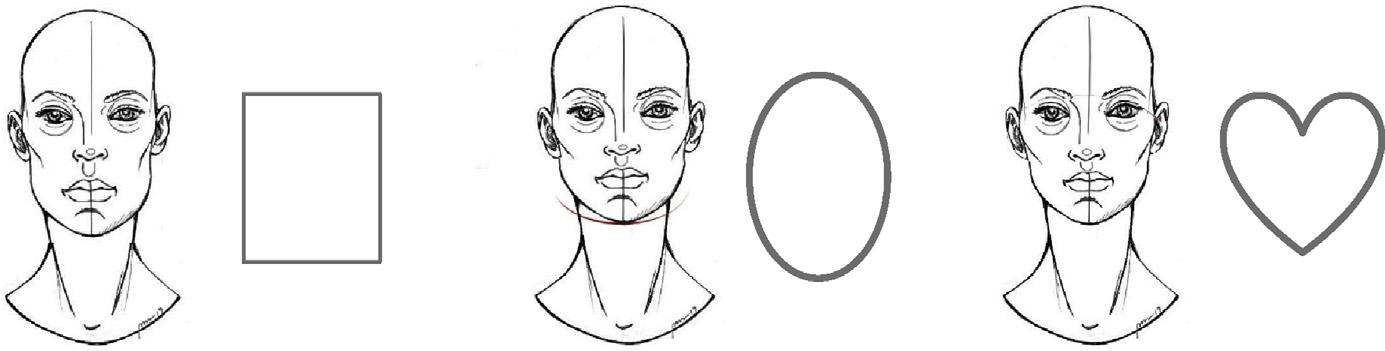
Thefaceisinitiallyexaminedasa “whole,” saving thefacialdetailsandsubcomponentsforlast.Facial shapeandformshouldbeappreciated(oval,round, oblong,heart,triangularsquare,rectangulardiamond,
FIG.1 Appraisingfacialharmony.( 2019PeterM.Schmid.)
FIG.2 Integrationofartandscience.( 2019PeterM.Schmid.)
BOX1
Sculpturalaestheticmarkers
Lateralorbitalrim(f)
Malareminence(f)
Lipvolumeandshape(f)
Temporalplateau(m)
Submalarplane(f 1 m)
Mandibleshapeanddefinition(f 1 m)
Abbreviations: f,female;m,male.
inverted,pear,peanut,andothers)astheyrelatetothe shapeoftheneckandjawline(Fig.3).
Underadequatelighting,theseatedpatientshouldbe examinedinmultiperspectiveviews,tostudyfacialshape, asymmetries,apparentorvirtualsilhouetteprofilelines, andvolumetricdistributionsorimbalances(Fig.4).
High-contrastlightingshouldbeusedtoappraise anatomiclandmarks,bonyprominences,facialplanes, dominantreflectivehighlightsandshadows,andunderlyingsofttissuedeficiencies,depressions,flatness,or curvedistortions.Softambientlightingexposesskin qualities,softtissuediscrepancies,andsurfaceirregularitiessecondarytosubtleunderlyinganatomicshapes andmasses.Facialfeaturesarereviewedlast(Fig.5).
Thefacialbonesandsofttissuesshouldbedelicately palpatedtoassessposition,densities,anddeficiencies. Tissuesshouldbemanuallyrepositionedtopresent proposalsexemplifyingrestorationofform.Facialanimationprovidesinsightintosofttissuedispositions, ptosis,andredistributions.Achronologicphotogallery ofthepatient’sagingimagesshouldbereviewed. Communicationviaamirror,computerizeddigitalimaging,andsculpturaldialogueestablishescommensurateobjectivesandtrust.
Canons,Proportions,andShape
Canons,proportions,andthegoldenratio(phi; 1:1.618)provideageneralreferencesystemforfacial
analysis.Thebalancedfaceisdividedintoequalvertical halves,byequalverticalfacialfifths(note:beyond widthofskull),orbyhorizontalfacialthirds(note: hairlinetothechin)(Fig.6).Thelowerfacialthird canbesubdividedintoanupperthirdbygaugingthe lengthoftheupperlip,withthelowertwo-thirds fromthestomiumtothementum[3].Artisticcanons serveasobjectiveguidelinestoestablishconversation withthepatient,educatingthemabouttheirpresenting clinicalfacialfindings,whetherasymmetries,disproportions,imbalances,orattributes.
FacialStructuralPlatform
Thebonycraniofacialarmaturesuspendingthesofttissuesandretainingligamentsofthefaceimpartsexquisitecurvilinearcontourandshape.Thefacialframework consistsofintegratedstructuralplatforms,namely,the cranial,midfacial,mandibular,andnasalcomplexes (Fig.7).
Uniquefacialheightanddimensionsequateto craniofacialgrowthinfluencedbygeneticsandgender. Thewomanskullandfacialbonesarepetite,andthe mancounterpartsarethickandrobust.Definingbony landmarkspresentinbotharethefrontalprominence, supraciliaryarch,nasalbones,malareminences,angles ofthemandible,andthementaltubercle,eachdisplayinguniquesurfaceformandreflectivehighlights.The faceasaunitiswideposteriorlyandtapersanteriorly bycurvilinear3-dimensionalform.Thegreatestwidth oftheskullisatthebiparietaleminence,camouflaged bythescalp.
Theupper cranialplatform insetswithinthemidfacial maxilla-zygomaticcomplex.Thesphericalhumanskull isinterfacedwithconvexities,concavities,ridges,and planes.Thewomanskullbynatureis70%to90%the sizeofthemancranium[4].Theforeheadofthe womanisverticallyshortandbroadspanning,demonstratingacentralfrontalroundnesswithhighlightsasit blendssoftlyintothelateraltemporoparietalregions andflowsdownwardontotheorbitalrims.Themasculineforehead,incomparison,oftenreflects5distinct