Listofcontributors
AmidAbdullah,MD UniversityofCalgaryandCalgary LaboratoryServices,Calgary,AB,Canada
MariaP.Alfaro,PhD InstituteforGenomicMedicine, NationwideChildren’sHospital,Columbus,OH, UnitedStates
ChrisAltomare,BS DRUGSCANInc.,Horsham,PA, UnitedStates
LelandBaskin,MD UniversityofCalgaryandCalgary LaboratoryServices,Calgary,AB,Canada
LindsayA.L.Bazydlo,PhD DepartmentofPathology, UniversityofVirginia,Charlottesville,VA,UnitedStates
JessicaM.Boyd,PhD DepartmentofPathologyand LaboratoryMedicine,CummingSchoolofMedicine, UniversityofCalgary,Calgary,AB,Canada;Calgary LaboratoryServices,Calgary,AB,Canada
LarryA.Broussard,PhD DepartmentofClinicalLaboratory Sciences,LouisianaStateUniversityHealthSciencesCenter, NewOrleans,LA,UnitedStates
VioletaCha ´ vez,PhD DepartmentofPathologyand LaboratoryMedicine,UniversityofTexasMedicalSchoolat Houston,Houston,TX,UnitedStates
AlexChin,PhD UniversityofCalgaryandCalgary LaboratoryServices,Calgary,AB,Canada
AnthonyG.Costantino,PhD DRUGSCANInc.,Horsham, PA,UnitedStates
AmitavaDasgupta,PhD,DABCC DepartmentofPathology andLaboratoryMedicine,UniversityofTexasMcGovern MedicalSchool,Houston,TX,UnitedStates
PradipDatta,PhD SiemensHealthineers,Newark,DE, UnitedStates
RobertA.DeSimone,MD DepartmentofPathologyand LaboratoryMedicine,WeillCornellMedicine, NewYork-PresbyterianHospital,NewYork,NY, UnitedStates
UttamGarg,PhD DepartmentofPathologyandLaboratory Medicine,Children’sMercyHospitalsandClinics,The UniversityofMissouriSchoolofMedicine,KansasCity, MO,UnitedStates
NeilS.Harris,MD DepartmentofPathology,Immunology andLaboratoryMedicine,UniversityofFlorida,Collegeof Medicine,Gainesville,FL,UnitedStates
JoshuaHayden,PhD DepartmentofPathologyand LaboratoryMedicine,WeillCornellMedicalCenter, NewYork,NY,UnitedStates
SusanJ.Hsiao,MD,PhD DepartmentofPathologyandCell Biology,ColumbiaUniversityIrvingMedicalCenter, NewYork,NY,UnitedStates
LauraM.Jacobsen,MD DepartmentofPediatrics,Division ofEndocrinology,UniversityofFlorida,Collegeof Medicine,Gainesville,FL,UnitedStates
KamishaL.Johnson-Davis,PhD DepartmentofPathology, UniversityofUtahSchoolofMedicine,ARUPLaboratories, SaltLakeCity,UT,UnitedStates
StevenC.Kazmierczak,PhD DepartmentofPathology, OregonHealth&ScienceUniversity,Portland,OR, UnitedStates
ElaineLyon,PhD ClinicalServicesLaboratory, HudsonAlphaInstituteforBiotechnology,Huntsville,AL, UnitedStates
GwendolynA.McMillin,PhD DepartmentofPathology, UniversityofUtahSchoolofMedicine,ARUPLaboratories, SaltLakeCity,UT,UnitedStates
ChristopherNaugler,MD UniversityofCalgaryand CalgaryLaboratoryServices,Calgary,AB,Canada
ElenaG.Nedelcu,MD DepartmentofLaboratoryMedicine, UniversityofCaliforniaSanFrancisco,SanFrancisco,CA, UnitedStates
AndyNguyen,MD DepartmentofPathologyand LaboratoryMedicine,UniversityofTexasMcGovern MedicalSchool,Houston,TX,UnitedStates
OctaviaM.PeckPalmer,PhD DepartmentofPathology, UniversityofPittsburghSchoolofMedicine,Pittsburgh, PA,UnitedStates;DepartmentofCriticalCareMedicine, UniversityofPittsburghSchoolofMedicine,Pittsburgh,PA, UnitedStates;DepartmentofClinicalandTranslational Science,UniversityofPittsburghSchool,Pittsburgh,PA, UnitedStates
AmyL.Pyle-Eilola,PhD PathologyandLaboratory Medicine,NationwideChildren’sHospital,Columbus,OH, UnitedStates
S.M.HosseinSadrzadeh,PhD DepartmentofPathology andLaboratoryMedicine,CummingSchoolofMedicine, UniversityofCalgary,Calgary,AB,Canada;Calgary LaboratoryServices,Calgary,AB,Canada
JorgeL.Sepulveda,MD,PhD DepartmentofPathologyand CellBiology,ColumbiaUniversityVagelosCollegeof PhysiciansandSurgeons,NewYork,NY,UnitedStates
BrianRudolphShy,MD,PhD DepartmentofLaboratory Medicine,UniversityofCaliforniaSanFrancisco, SanFrancisco,CA,UnitedStates
AaronStella,PhD UniversityofMassachusettsLowell, Lowell,MA,UnitedStates
YvetteC.Tanhehco,PhD DepartmentofPathologyandCell Biology,ColumbiaUniversityIrvingMedicalCenter, NewYork-PresbyterianHospital,NewYork,NY, UnitedStates
AshokTholpady,MD DepartmentofPathologyand LaboratoryMedicine,UniversityofTexasMDAnderson CancerCenter,Houston,TX,UnitedStates
ChristinaTrambas,MD,PhD ChemicalPathologist, ChemicalPathologyDepartment,MelbournePathology, Collingwood,VIC,Australia
GeorgeVlad,PhD DepartmentofPathology&CellBiology, ColumbiaUniversityCollegeofPhysiciansandSurgeons, NewYork,NY,UnitedStates
AmerWahed,MD DepartmentofPathologyand LaboratoryMedicine,UniversityofTexasMcGovern MedicalSchool,Houston,TX,UnitedStates
WilliamE.Winter,MD DepartmentofPediatrics,Division ofEndocrinology,UniversityofFlorida,Collegeof Medicine,Gainesville,FL,UnitedStates;Departmentof Pathology,ImmunologyandLaboratoryMedicine, UniversityofFlorida,CollegeofMedicine,Gainesville,FL, UnitedStates
AlisonWoodworth,PhD PathologyandLaboratory Medicine,UniversityofKentuckyMedicalCenter, Lexington,KY,UnitedStates
Cliniciansmustmakedecisionsfrominformation presentedtothem,bothbythepatientandancillary resourcesavailabletothephysician.Laboratorydata generallyprovidequantitativeinformation,which maybemorehelpfultophysiciansthanthesubjective informationfromapatient’shistoryorphysicalexamination.Indeed,withtheprevalentpressurefor physicianstoseemorepatientsinalimitedtimeframe, laboratorytestinghasbecomeamoreessentialcomponentofapatient’sdiagnosticwork-up,partlyasatimesavingmeasurebutalsobecauseitdoesprovide informationagainstwhichpriororsubsequenttestresults,andhencepatients’health,maybecompared. Testsshouldbeorderediftheycouldbeexpectedto provideadditionalinformationbeyondthatobtained fromaphysician’sfirstencounterwithapatientandif theresultscouldbeexpectedtoinfluenceapatient’s care.Typically,cliniciansuseclinicallaboratorytesting asanadjuncttotheirhistorytakingandphysical examinationtohelpconfirmapreliminarydiagnosis, althoughsometestingmayestablishadiagnosis,for examplemoleculartestsforinbornerrorsofmetabolism. Microbiologicalculturesofbodyfluidsmaynotonly establishtheidentityofaninfectingorganism,butalso establishthetreatmentoftheassociatedmedicalcondition.Inoutpatientpracticecliniciansprimarilyorder teststoassistthemintheirdiagnosticpractice,whereas forhospitalizedpatients,inwhomadiagnosishas typicallybeenestablished,laboratorytestsareprimarily usedtomonitorapatient’sstatusandresponseto treatment.Testsoforganfunctionareusedtolookfor drugtoxicityandthemeasurementofthecirculating concentrationsofdrugswithnarrowtherapeuticwindowsisdonetoensurethatoptimaldrugdosingis achievedandmaintained.Theimportanceoflaboratory testingisevidentwhensomephysiciansrelymoreon laboratorydatathanapatient’sownassessmentasto howheorshefeels,openingthemtothecriticismof treatingthelaboratorydataratherthanthepatient.
Inthemodern,tightlyregulated,clinicallaboratory inadevelopedcountryfewerrorsarelikelytobemade, withthemajoritylabeledaslaboratoryerrorsoccurring outsidethelaboratoryitself.Onestudyfrom1995
showedthatwhenerrorsweremade75%stillproduced resultsthatfellwithinthereferenceinterval(when perhapstheyshouldnot) [1].Halfoftheothererrors wereassociatedwithresultsthatweresoabsurdthat theywerediscountedclinically.Suchresultsclearly shouldnothavebeenreleasedtoaphysicianbythe laboratoryandcouldlargelybeavoidedbyasimple reviewbyhumanorcomputerbeforebeingverified. However,theremaining12.5%oferrorsproducedresultsthatcouldhaveimpactedpatientmanagement. Theprevalenceoferrorsmaybelessnowthanpreviously,sincethequalityofanalyticaltestinghas improved,buttheramificationsofeacherrorarenot likelytobeless.Theconsequencesofanerrorvary dependingontheanalyteoranalytesaffectedand whetherthepatientinvolvedisaninpatientoroutpatient.Ifthepatientisaninpatientaphysician,if suspiciousabouttheresult,willlikelyhavetheopportunitytoverifytheresultbyrepeatingthetestorother testsaddressingthesamephysiologicalfunctions, beforetakingaction.However,iftheerroroccurswitha specimenfromanoutpatientcausinganabnormalresult toappearnormal,thatpatientmaybelosttofollow-up andpresentlaterwithadvanceddisease.Despitethe greatpreponderanceofaccurateresultscliniciansshould alwaysbewaryofanyresultthatdoesnotseemtofit withthepatient’sclinicalpicture.Itis,ofcourse,equally importantforphysiciansnottodismissanyresultthat theydonotlikeasa“laboratoryerror”.Theunexpected resultshouldalwayspromptanappropriatefollow-up. Thelaboratoryhasaresponsibilitytoensurethatphysicianshaveconfidenceinitstestresultswhilestill retainingahealthyskepticismaboutunexpectedresults.
Normallaboratorydatamayprovidesomeassurancetoworriedpatientswhobelievethattheymight haveamedicalproblem,anissueseeminglymore prevalentnowwiththereadyaccessibilityofmedical informationavailablethroughcomputersearchengines. Yetbothpatientsandphysicianstendtobecomeoverreliantonlaboratoryinformation,eithernotknowing orignoringtheweaknessoflaboratorytests,ingeneral. Aculturehasarisenofphysiciansandpatients believingthatthepublishedupperandlowerlimitsof
thereferencerange(orinterval)ofatestdefine normality.Theydonotrealizethatsucharangehas probablybeenderivedfrom95%ofagroupofpresumedhealthyindividuals,notnecessarilyselected withrespecttoalldemographicfactorsorhabitsthat wereanappropriatecomparativereferencefora particularpatient.Evenifappropriate,1in20individualswouldbeexpectedtohaveanabnormalresult forasingletest.Intheusualsituationinwhichmany testsareorderedtogethertheprobabilityofabnormal resultsinahealthyindividualincreasesinproportionto thenumberoftestsordered.Studieshavehypothesized thatthelikelihoodofallof20testsorderedatthesame timefallingwithintheirrespectivereferenceintervalsis only36%.Thestudiesperformedtoderivethereference limitsareusuallyconductedunderoptimizedconditionssuchasthetimesincethevolunteerlastate,hisor herpostureduringbloodcollectionand,oftenthetime ofday.Suchidealizedconditionsarerarelylikelytobe attainedinanofficeorhospitalpractice.
Factorsaffectingtheusefulnessoflaboratorydata mayariseinanyofthepreanalytical,analyticalorpostanalyticalphaseofthetestingcycle.Failurestoconsider thesefactorsdoconstituteerrors.Iftheseerrorsoccur priortocollectionofbloodorafterresultshavebeen produced,whilestilllikelytobelabeledaslaboratory errorsbecausetheyinvolvelaboratorytests,thelaboratorystaffsaretypicallynotliableforthem.Yetthe staffdoeshavetheresponsibilitytoeducatethoseindividualswhomayhavecausedthemtoensurethat sucherrorsdonotrecur.Ifpracticingclinicianswere abletousetheknowledgethatexperiencedlaboratorianshaveaboutthestrengthsandweaknessesof testsitislikelythatmuchmoreclinicallyusefulinformationcouldbeextractedfromexistingtests.Outside thelaboratory,physiciansrarelyareknowledgeable abouttheintra-andinterindividualvariationobserved whenserialstudiesareperformedonthesameindividuals.Forsometestsasignificantchangeforan individualmayoccurwhenhis/hertestvaluesshift fromtowardoneendofthereferenceintervaltoward theother.Thusatestvaluedoesnotnecessarilyhaveto exceedthereferencelimitsforittobeabnormalfora givenpatient.Ifthepreanalyticalstepsarenotstandardizedwhenrepeatedtestingisdoneonthesame person,itismorelikelythattrendsinlaboratorydata maybemissed.Thereisanonusoneveryoneinvolved intestorderingandtestperformancetostandardizethe processestofacilitatethemaximalextractionofinformationfromthelaboratorydata.Thecombinedgoal
shouldbeofpursuitofinformationratherthanjust data.Laboratoryinformationsystemsprovidethepotentialtointegratealllaboratorydatathatcanthenbe integratedwithclinicalandotherdiagnosticinformationbyhospitalinformationsystems.
Laboratoryactionstohighlightvaluesoutsidethe referenceintervalontheircomprehensivereportsoftest resultstophysicianswithcodessuchas“H”or“L”for highandlowvaluesexceedingthereferenceinterval havetendedtoobscuretheactualnumericalresultand tocementtheconceptthattheupperandlowerreference limitsdefinenormalityandthatthepresenceofoneof thesesymbolsnecessitatesfurthertesting.Theuseofthe referencelimitsaspublisheddecisionlimitsfornational programsforrenalfunction,lipidorglucosescreening hasagainplacedagreaterburdenonthevaluesthan theydeserve.Everymeasurementissubjecttoanalytical error,suchthatrepeateddeterminationswillnotalways yieldthesameresult,evenunderoptimaltestingconditions.Woulditthenbemoreappropriatetomake multiplemeasurementsanduseanaveragetoestablish thenumbertobeacteduponbyaclinician?
Muchoftheopportunitytoreduceerrors(inthe broadestsense)restswiththephysicianswhousetest results.Over-orderingleadstothepossibilityofmore errors.Inappropriateordering,forexamplerepetitive orderingoftestswhosepreviousresultshavebeen normal,ororderingthewrongtestorwrongsequence ofteststoelucidateaproblemshouldbeminimizedby carefulsupervisionbyattendingphysiciansoftheir traineesinvolvedinthedirectmanagementoftheir patients.Laboratoriansneedtobemoreinvolvedin teachingmedicalstudentssothatwhentheybecome residentstheirtestorderingpracticesarenotlearned fromseniorresidentswhohadlearnedtheirhabits fromthepreviousgenerationofresidents.Blanket applicationofclinicalguidelinesortestorder-setshas probablyledtomuchmisuseofclinicallaboratory tests.Manycliniciansandlaboratorianshaveattemptedtoreduceinappropriatetestordering,butthe overallconclusionseemstobethateducationis themosteffectivemeans.Unfortunately,theeducation needstobecontinuouslyreinforcedtohavealasting effect.Theeducationneedstoaddresstheclinical sensitivityofdiagnostictests,thecontextinwhich theyareorderedandtheirhalf-lives.Abovealleducationneedstoaddressissuesofbiologicalvariation andpreanalyticalfactorsthatmayaffecttestvalues, possiblymaskingtrendsormakingtheabnormal resultappearnormaland viceversa.
Thisbookprovidesacomprehensivereviewofthe factorsleadingtoerrorsinalltheareasofclinicallaboratorytesting.Assuchitwillbeofgreatvaluetoall laboratorydirectorsandtraineesinlaboratorymedicine andthetechnicalstaffwhoperformthetestsindaily practice.Byclearlyidentifyingproblemareas,thebook laysouttheopportunitiesforimprovement.Thisbook
shouldbeofequalvaluetoclinicians,astolaboratorians,astheyseektheoptimaloutcomefromtheir careoftheirpatients.
Reference
[1]GoldschmidtHMJ,LentRW.Grosserrorsandworkflowanalysis intheclinicallaboratory.KlinBiochemMetab1995;3:131 49.
DonaldS.YoungMD,Ph.D ProfessorofPathologyandLaboratoryMedicine UniversityofPennsylvaniaPerelmanCollegeof Medicine,Philadelphia,PA
Variation,errors,andqualityinthe clinicallaboratory
JorgeL.Sepulveda
DepartmentofPathologyandCellBiology,ColumbiaUniversityVagelosCollegeofPhysiciansandSurgeons, NewYork,NY,UnitedStates
INTRODUCTION
Recentstudiesdemonstratedthat invitro diagnostic testsareperformedinupto96%ofpatientsandthat upto80%ofclinicaldecisionsinvolveconsiderationof laboratoryresults [1].Inaddition,approximately 40 94%ofallobjectivehealthrecorddataarelaboratory results [2 4].Diagnosticerrorsaccountedfor26 78%of identifiedmedicalerrors [5] andnearly60%ofmalpracticeclaims [6],andwereinvolvedin17%ofadverse effectsduetomedicalerrorsinonelargestudy [7]. Undoubtedly,appropriateorderingandinterpretation ofaccuratetestresultsareessentialformajorclinicaldecisionsinvolvingdiseaseidentification,classification, treatment,andmonitoring.Factorsthatconstitutean accuratelaboratoryresultinvolvemorethananalytical accuracyandcanbesummarizedasfollows:
1. Therighttest,withtherightcostsandrightmethod, wasorderedfortherightpatient,attherighttime,for therightreason [8]:theimportanceofappropriatetest selectioncannotbeminimizedasstudieshaveshown thatatleast20%ofalltestordersareinappropriate [9], upto68%oftestsordereddonotcontributetoimprove patientmanagement [10] andconverselytestswerenot orderedwhenneededinnearly50%ofpatients [9]
2. Therightsamplewascollectedontherightpatient,at thecorrecttime,withappropriatepatient preparation.
3. Therighttechniquewasusedcollectingthesampleto avoidcontaminationwithintravenousfluids,tissue damage,prolongedvenousstasis,orhemolysis.
4. Thesamplewasproperlytransportedtothe laboratory,storedattherighttemperature,processed foranalysis,andanalyzedinamannerthatavoids artifactualchangesinthemeasuredanalytelevels.
5. Theanalyticalassaymeasuredtheconcentrationof theanalytecorrespondingtoits“true”level (comparedtoa“goldstandard”measurement)within aclinicallyacceptablemarginoferror(thetotal acceptableanalyticalerror(TAAE)).
6. Thereportreachingthecliniciancontainedtheright result,togetherwithinterpretativeinformation,such asareferencerangeandothercomments,aiding cliniciansinthedecision-makingprocess.
Failureatanyofthesestepscanresultinanerroneous ormisleadinglaboratoryresult,sometimeswithadverse outcomes.Forexample,interferenceswithpoint-of-care glucosetestingduetotreatmentwithmaltosecontaining fluidshaveledtofailuretorecognizesignificanthypoglycemiaandtomortalityorseveremorbidity [11].
ERRORSINCLINICALLABORATORY
Errorscanoccurinallthestepsinthelaboratory testingprocess,andsucherrorscanbeclassifiedas follows(see Table1.1):
1. Pre-analyticalsteps,encompassingthedecisionto test,transmissionoftheordertothelaboratoryfor analysis,patientpreparationandidentification, samplecollection,andspecimenprocessing.
2. Analyticalassay,whichproducesalaboratoryresult.
3. Post-analyticalsteps,involvingthetransmissionof thelaboratorydatatotheclinicalprovider,whouses theinformationfordecisionmaking.
Althoughminimizationofanalyticalerrorshasbeen themainfocusofdevelopmentsinlaboratorymedicine, theotherstepsaremorefrequentsourcesoferroneous
TABLE1.1 Typesoferrorintheclinicallaboratory.
PRE-ANALYTICAL
Testordering
• DuplicateOrder
• Orderingprovidernot identified
• Orderedtestnotperformed (includeadd-ons)
Samplecollection
• Unsuccessfulphlebotomy
• Traumaticphlebotomy
• Patientcomplaintabout phlebotomy
Specimentransport
• Inappropriatesample transportconditions
• Specimenleakedintransit
Specimenidentification
• Specimenunlabeled
• Specimenmislabeled:No NameorIDontube
• Specimenmislabeled:No Nameontube
• Specimenmislabeled: IncompleteIDontube
• Wrongspecimenlabel
• Wrongnameontube
• WrongIDontube
• Wrongbloodtype
Highpre-analyticalturnaroundtime
• Delayinreceivingspecimen inlab
• Delayinperformingtest
Specimenquality
• Specimencontaminatedwith infusionfluid
• Specimencontaminatedwith microbes
• Specimentoooldforanalysis
Specimencontainers
• Nospecimensreceived/ Missingtube
• Specimenlostinlaboratory
• Wrongspecimentype
• Inappropriatecontainer/tube type
• Wrongtubecollection instructions
• Ordermisinterpreted(test ordered <> intendedtest)
• Inappropriate/outmodedtest ordered
• Ordernotpulledbyspecimen collector
• Check-innotperformed(in theLIS)
• Wrongpatientpreparation (e.g.,non-fasting)
• Therapeuticdrugmonitoring testtimingerror
• Specimendamagedduring transport
• Specimendamagedduring centrifugation/analysis
• Date/timemissing
• Collector’sinitialsmissing
• Labelillegible
• Twocontradictorylabels
• Overlappinglabels
• Mismatchrequisition/label
• Specimeninformation misreadbyautomatedreader
TABLE1.1 Typesoferrorintheclinicallaboratory. cont’d
ANALYTICAL
• Highanalyticalturnaround time
• Instrumentcausedrandom error
• Instrumentmalfunction
• QCfailure
• QCnotcompleted
POST-ANALYTICAL
• Reportnotcompleted
• Delayinreportingresults
• Criticalresultsnotcalled
• Delayincallingcritical results
• Resultsreportedincorrectly
• Resultsreportedincorrectly fromoutsidelaboratory
• Resultsreportedtowrong provider
OTHER
• Proficiencytestfailure
• Productwastage
• Productnotdeliveredtimely
• Productrecall
• STATnotprocessedurgently
• Hemolyzed
• Clottedorplateletclumps
• Wrongpreservative/ anticoagulant
• Insufficientspecimen quantityforanalysis
• Tubefillingerror(toomuch anticoagulant)
• Tubefilingerror(toolittle anticoagulant)
• Emptytube
• Testperformby unauthorizedpersonnel
• Resultsdiscrepantwithother clinicalorlaboratorydata
• Testingnotcompleted
• Wrongtestperformed (differentfromtestordered)
• Reportedquestionable results,detectedby laboratory
• Reportedquestionable results,detectedbyclinician
• Failuretoappendproper comment
• Readbacknotdone
• Resultsmisinterpreted
• Failuretoactonresultsof tests
• Employeeinjury
• Safetyfailure
• Environmentalfailure
• Damagetoequipment
results.Ananalysisindicatedthatpre-analyticalerrors accountedfor62%ofallerrors,withpost-analyticalrepresenting23%andanalytical15%ofalllaboratoryerrors [12].Themostcommonpre-analyticalerrorsincluded incorrectordertransmission(atafrequencyofapproximately3%ofallorders)andhemolysis(approximately 0.3%ofallsamples) [13].Otherfrequentcausesofpreanalyticalerrorsincludethefollowing:
• Patientidentificationerror
• Tubefillingerror,emptytubes,missingtubes,or wrongsamplecontainer
• Samplecontaminationorcollectedfrominfusion route
• Inadequatesampletemperature
Particularattentionshouldbepaidtopatientidentificationbecauseerrorsinthiscriticalstepcanhavesevere consequences,includingfataloutcomes,forexample, duetotransfusionreactionsormisguidedtherapeutic decisions.Tominimizeidentificationerrors,health caresystemsareusingpoint-of-careidentificationsystems,whichtypicallyinvolvethefollowing:
1. Handhelddevicesconnectedtothelaboratory informationsystems(LIS)thatcanobjectively identifythepatientbyscanningapatient-attached barcode,typicallyawristband.
2. Currentlaboratoryorderscanberetrievedfrom theLIS.
3. Ideally,collectioninformation,suchascorrecttube types,isdisplayedinthedevice.
4. Bar-codedlabelsareprintedatthepatient’sside, minimizingthepossibilityofmisplacingthelabelson thewrongpatientsamples.
5. Afterattachingtocontainerswiththepatient samples,bar-codedlabelsshouldbescannedto confirmthattheywereappliedtotherightpatient, especiallyifanysignificantdelayhasoccurred betweenlabelprintingandsamplecollection.Inthis case,rescanningofpatient-attachedidentifiersshould bedoneinclosetemporalproximitytosample scanning.
Analyticalerrorsaremostlyduetointerferenceor otherunrecognizedcausesofinaccuracy,whereas instrumentrandomerrorsaccountedforonly2%ofall laboratoryerrorsinonestudy [12].Accordingtothat study,mostcommonpost-analyticalerrorsweredueto communicationbreakdownbetweenthelaboratory andtheclinicians,whereasonly1%weredueto miscommunicationwithinthelaboratory,and1%of theresultshadexcessiveturnaroundtimeforreporting [12].Post-analyticalerrorsduetoincorrecttranscription oflaboratorydatahavebeengreatlyreducedbecauseof theavailabilityofautomatedanalyzersandbidirectional interfaceswiththeLIS [12].However,transcription errorsandcalculationerrorsremainamajorareaof concerninthosetestingareaswithoutautomated interfacesbetweentheinstrumentandtheLIS.Further developmentstoreducereportingerrorsandminimize thetestingturnaroundtimeincludeauto-validationof testresultsfallingwithinpre-establishedrule-based parametersandsystemsforautomaticpagingofcritical resultstoproviders.
Whenclassifyingsourcesoferror,itisimportantto distinguishbetween cognitiveerrors,ormistakes,which areduetopoorknowledgeorjudgment,and noncognitiveerrors,commonlyknownasslipsandlapses,due tointerruptionsinaprocessthatisroutineorrelatively automatic.Whereasthefirsttypecanbepreventedby increasedtraining,competencyevaluation,andprocess aidssuchaschecklistsor“cheatsheets”summarizing importantstepsinaprocedure,noncognitiveerrorsare bestaddressedbyprocessimprovementandenvironmentre-engineeringtominimizedistractionsand fatigue.Furthermore,itisusefultoclassifyadverse occurrencesas active thatis,theimmediateresultof anactionbythepersonperformingatask oras latent or systemerrors,whicharesystemdeficienciesdueto poordesignorimplementationthatenableoramplify activeerrors.Inonestudy,onlyapproximately11%of theerrorswerecognitive,allinthepre-analyticalphase,
andapproximately33%oftheerrorswerelatent [12] Therefore,thevastmajorityoferrorsarenoncognitive slipsandlapsesperformedbythepersonneldirectly involvedintheprocess.Importantly,92%ofthepreanalytical,88%ofanalytical,and14%ofpost-analytical errorswerepreventable.Undoubtedly,humanfactors, engineering,andergonomics optimizationofsystems andprocessredesigningtoincludeincreasedautomation anduser-friendly,simple,andrule-basedfunctions, alerts,barriers,andvisualfeedback aremoreeffective thaneducationandpersonnel-specificsolutionsto consistentlyincreaselaboratoryqualityandminimize errors.
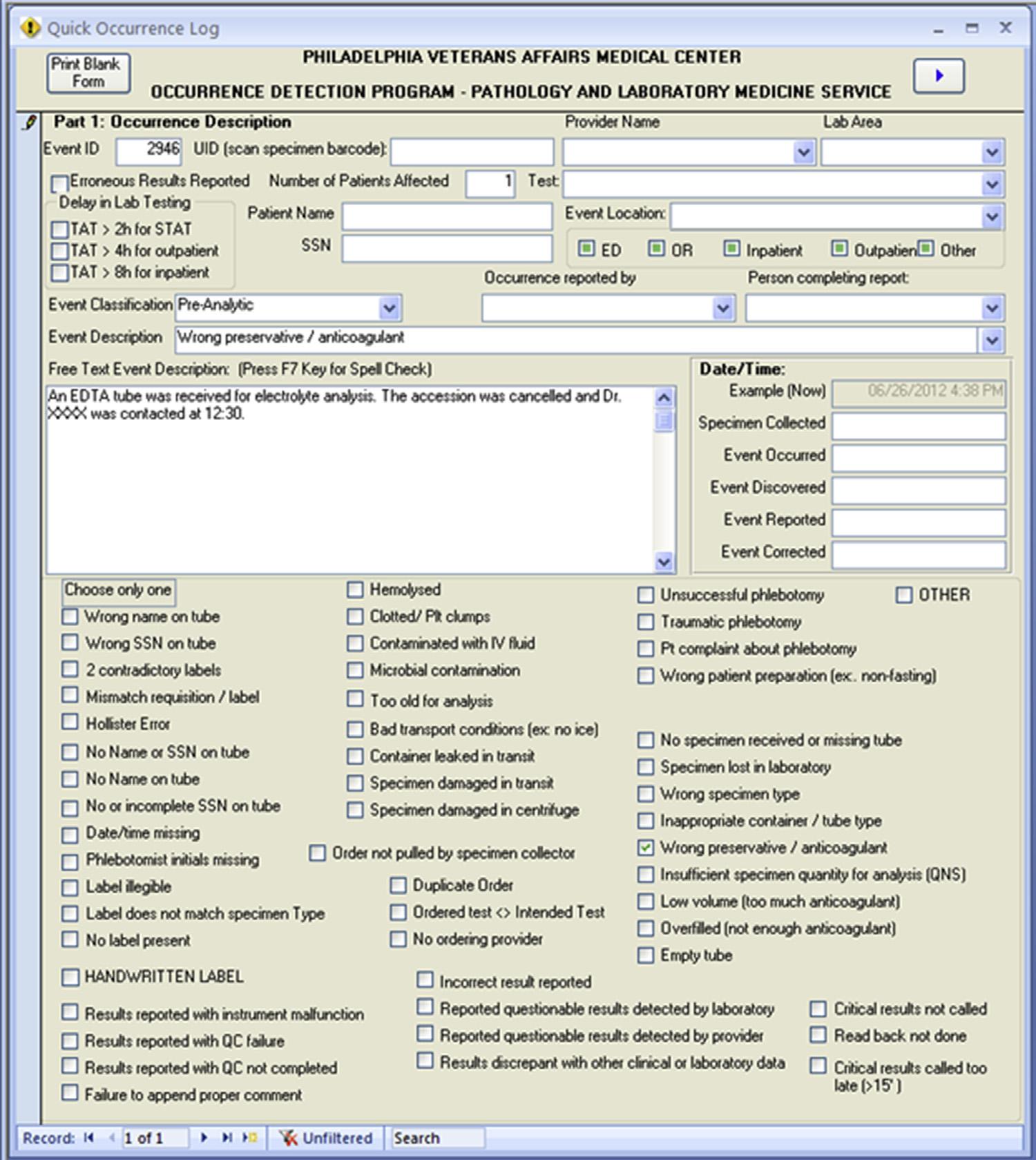
Immediatereportingoferrorstoadatabaseaccessible toallthepersonnelinthehealthcaresystem,followed byautomaticalertstoqualitymanagementpersonnel, isimportantforaccuratetrackingandtimelycorrection oflatenterrors.Inourexperience,reportingisimproved byusinganonlineformthatincludescheckboxesforthe mostcommontypesoferrorstogetherwithfree-textfor additionalinformation(Fig.1.1).Reviewerscansubsequentlyclassifyerrorsascognitive/noncognitive, latent/active,andinternaltolaboratory/internalto institution/externaltoinstitution;determineand classifyrootcausesasinvolvinghumanfactors(e.g., communicationandtrainingorjudgment),software,or physicalfactors(environment,instrument,hardware, etc.);andperformoutcomeanalysis.Outcomesoferrors canbeclassifiedasfollows:
1. Targetoferror(patient,staff,visitors,orequipment).
2. Actualoutcomeonaseverityscale(fromunnoticed tofatal).
3. Worstoutcomelikelihoodiferrorwasnotintercepted onthesameseverityscale,sincemanyerrorsare correctedbeforetheycauseinjury.
Errorswithsignificantoutcomesorlikelihoodsof adverseoutcomesshouldbediscussedbyqualitymanagementstaffandlaboratorydirectorstodetermine appropriatecorrectiveactionsandprocessimprovement initiatives.
Clearly,effortstoimproveaccuracyoflaboratory resultsshouldencompassallofthestepsofthetesting cycle,aconceptexpressedas“totaltestingprocess” or“brain-to-braintestingloop” [14].Approachesto achieveerrorminimizationderivedfromindustrialprocessesincludetotalqualitymanagement(TQM) [15]; leandynamicsandToyotaproductionsystems [16]; rootcauseanalysis(RCA) [17];healthcarefailuremodes andeffectsanalysis(HFMEA) [18,19];failurereview analysisandcorrectiveactionsystem(FRACAS) [20]; andSixSigma [21,22],whichaimsatminimizingthe variabilityofproductssuchthatthestatisticalfrequency oferrorsisbelow3.4permillion.Adetaileddescription
oftheseapproachesisbeyondthescopeofthisbook,but laboratoriansandqualitymanagementspecialists shouldbefamiliarwiththeseprinciplesforerrorprevention,errordetection,anderrormanagementto achieveefficient,high-qualitylaboratoryoperationand patientcare [15].
QUALITYIMPROVEMENTINCLINICAL LABORATORY
Quality isdefinedasallthefeaturesofaproductthat meettherequirementsofthecustomersandthehealth caresystem.Manyapproachesareusedtoimprove andensurethequalityoflaboratoryoperations.The conceptofTQMinvolvesaphilosophyofexcellence concernedwithallaspectsoflaboratoryoperations thatimpactonthequalityoftheresults.Specifically,
TQMapproachesapplyasystemofstatisticalprocess controltoolstomonitorqualityandproductivity(quality assurance)andencourageeffortstocontinuously improvethequalityoftheproducts,aconceptknown as continuousqualityimprovement.Amajorcomponent ofaqualityassuranceprogramis qualitycontrol (QC), whichinvolvestheuseofperiodicmeasurementsof productquality,thresholdsforacceptableperformance, andrejectionofproductsthatdonotmeetacceptability criteria.Mostnotably,QCisappliedtoallclinical laboratorytestingprocessesandequipment,including testingreagents,analyticalinstruments,centrifuges, andrefrigerators.Typically,foreachclinicaltest, externalQCmaterialswithknownperformance,also knownas controls,areruntwoorthreetimesdailyin parallelwithpatientspecimens.Controlsusuallyhave preassignedanalyteconcentrationscoveringimportant medicaldecisionlevels,oftenatlow,medium,and
FIG.1.1 Exampleofanerrorreportingformfortheclinicallaboratory.
highconcentrations.GoodlaboratoryQCpractice involvesestablishmentofalaboratory-andinstrumentspecificmeanandstandarddeviationforeachlotof eachcontrolandalsoasetofrulesintendedtomaximize errordetectionwhileminimizingfalserejections,suchas Westgardrules [23].Anotherimportantcomponentof qualityassuranceforclinicallaboratoriesisparticipation inproficiencytesting(orexternalqualityassessmentprogramssuchasproficiencysurveyssentbytheCollegeof AmericanPathologists),whichinvolvesthesharingof sampleswithalargenumberofotherlaboratoriesand comparisonoftheresultsfromeachlaboratorywithits peers,usuallywithreportingofthemeanandstandard deviation(SD)ofallthelaboratoriesrunningthesame analyzer/reagentcombination.CriteriaforQCrules andproficiencytestingacceptabilityshouldtakeinto considerationtheconceptoftotalacceptableanalytical errorbecausedeviationssmallerthanthetotalanalytical errorsareunlikelytobeclinicallysignificantandthereforedonotneedtobedetected.
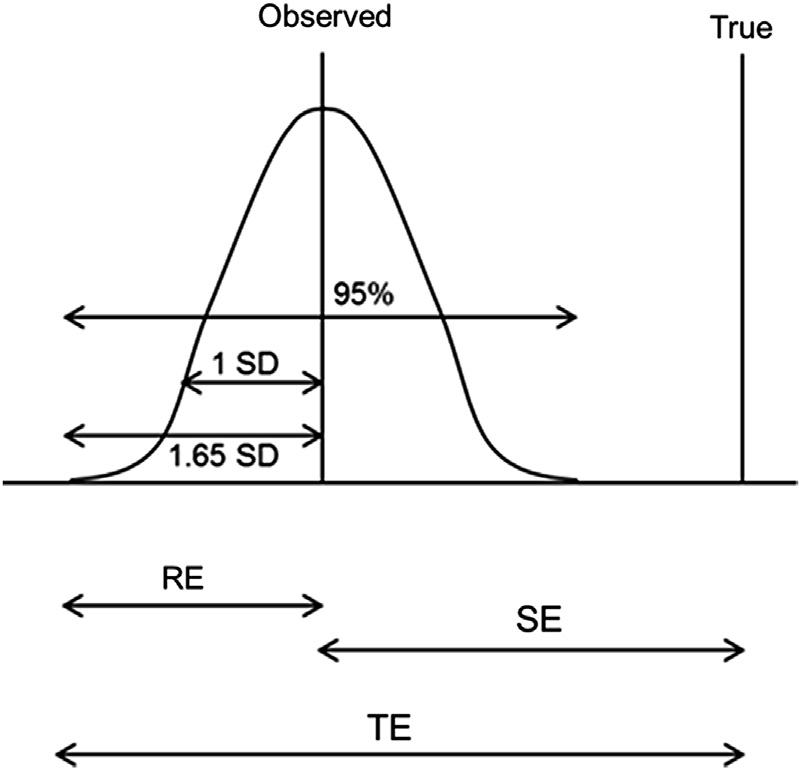
Totalanalyticalerror(TAE)isusuallyconsideredto combinethefollowing(Fig.1.2):(1)systematicerror (SE),orbias,asdefinedbydeviationbetweenthe averagevaluesobtainedfromalargeseriesoftestresults andanacceptedreferenceorgoldstandardvalue,and (2)randomerror(RE),orimprecision,representedby thecoefficientofvariationofmultipleindependenttest resultsobtainedunderstipulatedconditions(CVa). Assuminganormaldistributionofrepeatedtestresults, atthe95%confidencelevel,theREisequalto1.65times theCVa forthemethod;consequently.
FIG.1.2 Totalanalyticalerror(TE)components:randomerror(RE), orimprecisionandsystematicerror(SE),orbias,whichcausethe differencebetweenthetruevalueandthemeasuredvalue.Random errorcanincreaseordecreasethedifferencefromthetruevalue. Becauseinanormaldistribution,95%oftheobservationsarecontained withinthemean 1.65standarddeviations(SDs),thetotalerrorwill notexceedbias þ 1.65 SDin95%oftheobservations.
TAE ¼ 1 65 CVa þ bias
Clinicallaboratoriesfrequentlyevaluateimprecision byperformingrepeatedmeasurementsoncontrolmaterials,preferablyusingrunsperformedondifferentdays (between-dayprecision),whereasbias(ortrueness)is assessedbycomparisonwithstandardreferencematerialswithassignedvaluesandalsobypeercomparison, whereeitherthepeermeanormedianareconsidered thereferencevalues.
Oneimportantconceptthatsomecliniciansdisregard isthatnolaboratorymeasurementisexemptoferror; thatis,itisimpossibletoproducealaboratoryresult with0%biasand0%imprecision.Theroleoftechnologicdevelopments,goodmanufacturingpractices, proficiencytesting,andQCistoidentifyandminimize themagnitudeoftheTAE.Apracticalapproachisto considertheclinicallyacceptabletotalanalyticalerror orTAAEforeachtest.Clinicalacceptabilityhasbeen definedbylegislation(e.g.,theClinicalLaboratory ImprovementAct(CLIA)),byclinicalexpertopinion, andbyscientificandstatisticalprinciplesthattake intoconsiderationexpectedsourcesofvariation.For example,CallumFraserproposedthatclinicallyacceptableimprecision,orrandomerror,shouldbelessthan halfoftheintraindividualbiologicvariationfortheanalyteandlessthan25%ofthetotalanalyticalerror [24] Thesystematicerror,orbias,shouldbelessthan25% ofthecombinedintraindividual(CVw)andinterindividualbiological(CVg)variation:
< 1 65 0 5 CVw þ 0 25 CV2w þ CV2 g q
Tablesofintra-andinterindividualbiologicalvariation,withcorrespondingallowableerrors,areavailable andfrequentlyupdated [25].See Table1.2 forexamples. Importantly,theallowableerrorsmaybedifferentat specificmedicaldecisionlevelsbecauseanalytical imprecisiontendstovarywiththeanalyteconcentration,withhigherimprecisionatlowerlevels.Also, biologicalvariationmaybedifferentinthevarious clinicalconditions,andavailabledatabasesarestarting toincorporatestudiesofbiologicvariationindifferent diseases [25].
Arelatedconceptisthe referencechangevalue (RCV), alsocalled significantchangevalue (SCV) thatis,the variabilityaroundameasurementthatisaconsequence ofanalyticalimprecision,within-subjectbiologicvariability,andthenumberofrepeatedtestsperformed [24,26,27].Assuminganormaldistribution,atthe95% confidencelevel,RCVcanbecalculatedasfollows:
¼ 1:96 2p CV2 a þ CV2w q
Becausemultiplerepeatsdecreaseimprecisionerrors, ifthechangeisdeterminedfromthemeanofrepeated
TAAE95%
RCV95%
tests,theformulacanbemodifiedtotakeintoconsiderationthenumberofrepeatsineachmeasurement (n1 and n2) [27]:
RCV95% ¼ 1 96 2 n1 n2 s CVa2 þ CVw2 p
Forexample,foraserumcreatininemeasurement withananalyticalimprecision(CVa)of7.6%and within-subjectbiologicvariationof5.95%,theRCVat 95%confidenceis26.8%withonemeasurementfor eachsample.Withtwomeasurementsforeachsample, theRCVis18.9%.Therefore,achangebetweentworesultsthatdoesnotexceedtheRCVhasagreaterthan
95%probabilitythatitisduetothecombinedanalytical andintraindividualbiologicalvariation;inotherwords, thedifferencebetweenthetwocreatinineresults (measuredwithoutrepeats)shouldexceed26.8%tobe 95%confidentthatthechangeisduetoapathological condition.Conversely,foranychangeinlaboratory values,theRCVformulacanbeusedtocalculatethe probabilitythatitisduetoanalyticalandbiological variation [24,26,27].See Table1.2 forexamplesofRCV atthe95%confidencelimit,usingpublishedintraindividualvariationandtypicallaboratoryimprecisionfor eachtest.Ideally,futureLISshouldintegrateavailable knowledgeandpatient-specificinformationandautomaticallyprovideestimatesofexpectedvariationbased
TABLE1.2 Allowableerrorsandreferencechangevaluesforselectedtests.
Amylase5.38.728.33014.64.47.428.2
Alanineaminotransferase2.819.441.62027.489.711.4854.3
Albumin2.63.24.75104.071.61.4311.4
Alkalinephosphatase4.26.4526.13012.043.236.7221.3
Aspartateaminotransferase2.212.323.12016.696.156.5434.6
Bilirubintotal10.021.828.42026.9410.98.9566.5
Chloride2.41.21.551.50.60.57.4
Cholesterol2.75.9515.3109.012.984.118.1
Cortisol5.321.746.22530.6610.8512.7661.9
Creatinekinase3.622.8403030.311.411.564.0
Creatinine7.65.9514.7158.872.983.9626.8
Glucose3.44.55.8105.52.31.815.6
HDLcholesterol3.37.321.23011.633.655.6122.2
Iron2.526.523.22030.713.38.873.8
Lactatedehydrogenase(LDH)2.58.614.72011.44.34.324.8
Magnesium2.85.611.3257.82.83.217.4 pCO2 1.54.85.385.72.41.813.9
Protein,total2.62.754.7103.631.381.3610.5
Thyroxine(T4)4.84.910.92072.5319.0
Triglyceride3.919.932.72525.999.959.5756.2
Urate2.98.617.51711.974.34.8725.2
Ureanitrogen6.212.118.7915.556.055.5737.7
Allvaluesarepercentages.BioTAAE,totalallowableanalyticalerrorbasedoninterindividualandintraindividualvariation;CLIATAAE,totalallowableanalyticalerror basedonClinicalLaboratoryImprovementAct(CLIA);CVa,analyticalvariabilityinatypicalclinicallaboratory;CVg,interindividualvariability;CVw,intraindividual variability.Allowableimprecision ¼ 50%ofCVw.Allowablebias ¼ 0 25 CV2w CV2 g q .RCV95,referencechangevalueat95%confidencebasedonCVw andCVa BasedonWestgardJ.Desirablespecificationsfortotalerror,imprecision,andbias,derivedfromintra-andinter-individualbiologicvariation. 2014.Availablefrom: http://www. westgard.com/biodatabase1.htm
onthepreviousformulastofacilitateinterpretationof changesinlaboratoryvaluesandguidelaboratorystaff regardingthemeaningofdeviationsfromexpected results.Insummary,theuseofTAAEandRCVbrings objectivitytoerrorevaluation,QCandproficiency testingpractices,andclinicaldecisionmakingbased onchangesinlaboratoryvalues.
CONCLUSIONS
Asinotherareasofmedicine,errorsareunavoidable inthewholediagnosticprocessinvolvinglaboratory testing.Agoodunderstandingofthesourcesoferror, frequentlyinvolvingpre-analyticalfactors,together withaquantitativeevaluationoftheclinicalsignificance ofthemagnitudeofanalyticalerrors,aidedbytheestablishmentoflimitsofacceptabilitybasedonstatistical principlesofanalyticalandintraindividualbiological variation,arecriticaltodesignaqualityprogramto minimizetheclinicalimpactoferrorsintheclinical laboratory.
References
[1]RohrUP,BinderC,DieterleT,GiustiF,MessinaCG,ToerienE, etal.Thevalueofinvitrodiagnostictestinginmedicalpractice: astatusreport.PLoSOne2016;11(3):e0149856.
[2]ForsmanRW.Thevalueofthelaboratoryprofessionalinthe continuumofcare.ClinLeadershManagRev2002;16(6):370 3.
[3]ForsmanRW.Whyisthelaboratoryanafterthoughtformanaged careorganizations?ClinChem1996;42(5):813 6.
[4]HallworthMJ.The‘70%claim’:whatistheevidencebase?Ann ClinBiochem2011;48(Pt6):487 8.
[5]SandarsJ,EsmailA.Thefrequencyandnatureofmedicalerrorin primarycare:understandingthediversityacrossstudies.Fam Pract2003;20(3):231 6.
[6]GandhiTK,KachaliaA,ThomasEJ,PuopoloAL,YoonC, BrennanTA,etal.Missedanddelayeddiagnosesintheambulatorysetting:astudyofclosedmalpracticeclaims.AnnIntern Med2006;145(7):488 96.
[7]LeapeLL,BrennanTA,LairdN,LawthersAG,LocalioAR, BarnesBA,etal.Thenatureofadverseeventsinhospitalized patients.ResultsoftheHarvardMedicalPracticeStudyII. NEnglJMed1991;324(6):377 84.
[8]LippiG,BovoC,CiaccioM.Inappropriatenessinlaboratory medicine:anelephantintheroom?AnnTranslMed2017;5(4):82.
[9]ZhiM,DingEL,Theisen-ToupalJ,WhelanJ,ArnaoutR.Thelandscapeofinappropriatelaboratorytesting:a15-yearmeta-analysis. PLoSOne2013;8(11):e78962.
[10]MiyakisS,KaramanofG,LiontosM,MountokalakisTD.Factors contributingtoinappropriateorderingoftestsinanacademic medicaldepartmentandtheeffectofaneducationalfeedback strategy.PostgradMedJ2006;82(974):823 9.
[11]GainesAR,PierceLR,BernhardtPA.Fataliatrogenichypoglycemia:falselyelevatedbloodglucosereadingswithapoint-of-care meterduetoamaltose-containingintravenousimmuneglobulin product.2009[Updated06/18/2009].Availablefrom: http:// www.fda.gov/BiologicsBloodVaccines/SafetyAvailability/ucm15 5099.htm
[12]CarraroP,PlebaniM.Errorsinastatlaboratory:typesand frequencies10yearslater.ClinChem2007;53(7):1338 42.
[13]CarraroP,ZagoT,PlebaniM.Exploringtheinitialstepsofthe testingprocess:frequencyandnatureofpre-preanalyticerrors. ClinChem2012;58(3):638 42.
[14]PlebaniM,LippiG.Closingthebrain-to-brainloopinlaboratory testing.ClinChemLabMed2011;49(7):1131 3.
[15]ValensteinP,editor.Qualitymanagementinclinicallaboratories. Northfield(IL):CollegeofAmericanPathologists;2005.
[16]RutledgeJ,XuM,SimpsonJ.ApplicationoftheToyotaproductionsystemimprovescorelaboratoryoperations.AmJClinPathol 2010;133(1):24 31.
[17]DunnEJ,MogaPJ.Patientmisidentificationinlaboratorymedicine:aqualitativeanalysisof227rootcauseanalysisreportsin theVeteransHealthAdministration.ArchPatholLabMed2010; 134(2):244 55.
[18]ChiozzaML,PonzettiC.FMEA:amodelforreducingmedical errors.ClinChimActa2009;404(1):75 8.
[19]SouthardPB,KumarS,SouthardCA.AmodifiedDelphimethodologytoconductafailuremodeseffectsanalysis:apatient-centric effortinaclinicalmedicallaboratory.QualManagHealthCare 2011;20(2):131 51.
[20]KrouwerJ.Usingalearningcurveapproachtoreducelaboratory errors.AccredQualAssur2002;7(11):461 7.
[21]LlopisMA,TrujilloG,LlovetMI,TarresE,IbarzM,BioscaC,etal. Qualityindicatorsandspecificationsforkeyanalyticalextranalyticalprocessesintheclinicallaboratory.Fiveyears’experienceusingtheSixSigmaconcept.ClinChemLabMed2011; 49(3):463 70.
[22]GrasJM,PhilippeM.ApplicationoftheSixSigmaconceptinclinicallaboratories:areview.ClinChemLabMed2007;45(6):789 96.
[23]WestgardJO,DarcyT.Thetruthaboutquality:medicalusefulness andanalyticalreliabilityoflaboratorytests.ClinChimActa2004; 346(1):3 11.
[24]FraserCG.Biologicalvariation:fromprinciplestopractice. Washington(DC):AACCPress;2001.
[25]WestgardJ.Desirablespecificationsfortotalerror,imprecision, andbias,derivedfromintra-andinter-individualbiologicvariation.2014.Availablefrom: http://www.westgard.com/biodata base1.htm
[26]KrollMH.Multiplepatientsamplesofananalyteimprove detectionofchangesinclinicalstatus.ArchPatholLabMed 2010;134(1):81 9.
[27]FraserCG.Improvedmonitoringofdifferencesinseriallaboratoryresults.ClinChem2011;57(12):1635 7.
Errorsinpatientpreparation,specimen collection,anticoagulantandpreservativeuse:
howtoavoidsuchpre-analyticalerrors
LelandBaskin,AlexChin,AmidAbdullah,ChristopherNaugler
UniversityofCalgaryandCalgaryLaboratoryServices,Calgary,AB,Canada
INTRODUCTION
Patientpreparationandthespecimentypeareimportantpre-analyticalfactorstoconsiderforlaboratory assessment.Althoughtheclinicallaboratoryhaslimited capabilitiesincontrollingforthephysiologicalstateof thepatient,suchasbiologicalrhythmsandnutritional status,thesevariablesaswellastheeffectofpatient posture,tourniquets,andserum/plasmaindices(hemolysis,icterus,lipemia)onmeasurementofanalytesmust beunderstoodbyboththeclinicalteamandlaboratory personnel.Themostaccessiblespecimentypesinclude blood,urine,andoralfluid.Thenumerousfunctions associatedwithbloodmakeitanidealspecimento measurebiomarkerscorrespondingtovariousphysiologicalandpathophysiologicalprocesses.Bloodcanbe collectedbyskinpuncture(capillary),whichispreferred whenbloodconservationandminimalinvasivenessis stressed,suchasinthepediatricpopulation.Other modesofcollectionincludevenipunctureandarterial puncture,whereissuestoconsiderincludethephysical stateofthesiteofcollectionandpatientsafety.Bloodcan alsobetakenfromcathetersandotherintravascular lines,butcaremustbetakentoeliminatecontamination anddilutioneffectsassociatedwithheparinandother drugs.Clinicallaboratoryspecimensderivedfrom bloodincludewholeblood,plasma,andserum.However,noticeabledifferencesbetweenthesespecimentypes needtobeconsideredwhenchoosingtheoptimal specimentypeforlaboratoryanalysis.Suchimportant factorsincludethepresenceofanticoagulantsinplasma andinwholeblood,hematocritvariability,andthedifferencesinserumcharacteristicsassociatedwithblood
coagulation.Anticoagulantsforplasmaand/orwhole bloodcollectionincludeethylenediaminetetraacetic acid(EDTA),heparin,hirudin,oxalate,andcitrate, whichareavailableinsolidorliquidform.Optimal anticoagulant-to-bloodratiosarecrucialtopreventclot formationwhileavoidinginterferencewithanalytemeasurement,includingdilutioneffectsassociatedwith liquidanticoagulants.Giventheavailabilityofmultiple anticoagulantsandadditives,bloodcollectiontubes shouldbefilledaccordingtoaspecifiedordertominimizecontaminationandcarryover.Otherfactorsto considerregardingbloodcollectiontubesincludedifferencesbetweenplasticandglasssurfaces,surfactants, tubestopperlubricants,andgelseparators,whichall affectanalytemeasurement.
Thesecondmostpopularclinicalspecimenisurine, whichisessentiallyanultrafiltrateofbloodbefore eliminationfromthebodyandisthepreferredspecimentodetectmetabolicactivityaswellasurinary tractinfections.Propertimingmustbeensuredfor urinecollectionsdependingontheneedforroutine tests,patientconvenience,clinicalsensitivity,orquantitation.Furthermore,propertechniqueisrequiredfor cleancatchsamplesforsubsequentmicrobiological examination.Certainurinespecimensrequireadditivestopreservecellularintegrityforcytological analysisandtopreventbacterialovergrowth.Itis importanttorecognizethepre-analyticalvariables thataffectanalytemeasurementinpatientspecimens sothatproperlyinformeddecisionscanbemade regardingassayselectionanddevelopmentaswell astroubleshootingunexpectedoutcomesfromlaboratoryanalysis.
BIOLOGICALRHYTHMSAND LABORATORYTESTRESULTS
Predictablepatternsinthetemporalvariationof certainanalytes,reflectingpatternsinhumanneeds, constitutebiologicalrhythms.Differentanalyteshave differentrhythms,rangingfromafewhourstomonthly changes.Awarenessofsuchchangescanberelevant toproperinterpretationoflaboratoryresults.These changescanbedividedintocircadian,ultradian,and infradianrhythmsaccordingtothetimeintervaloftheir completion.
Duringa24-hperiodofhumanmetabolicactivity, programmingofmetabolicneedsmaycausecertain laboratoryteststofluctuatebetweenamaximumanda minimumvalue.Theamplitudeofchangeofthesecircadianrhythmsisdefinedasone-halfofthedifference betweenthemaximumandtheminimumvalues. Although,ingeneral,thesevariationsoccurconsistently, alterationinthesenaturalcircadianrhythmsmaybe inducedbyartificialchangesinsleep/wakecycles suchasthoseinducedbydifferentworkshifts.Therefore,insomeoneworkinganovernight(“graveyard”) shift,anelevatedbloodironleveltakenatmidnight wouldbenormalforthatindividual;however,the normisforhighironlevelstobeseenonlyinearly morning.
Patternsofbiologicalvariationoccurringoncycles lessthan24hareknownasultradianrhythms.Analytes thataresecretedinapulsatilemannerthroughoutthe dayshowthispattern.Testosterone,whichusually peaksbetween10:00a.m.and5p.m.,isanexampleof ananalyteshowingthispattern.
Thefinalpatternofbiologicalvariationisinfradian. Thisinvolvescyclesgreaterthan24h.Theexample mostcommonlycitedisthemonthlymenstrualcycle, whichtakesapproximately28 32daystocomplete. Constituentssuchaspituitarygonadotropin,ovarian hormones,andprostaglandinsaresignificantlyaffected bythiscycle.
PATIENTPREPARATION
Therearecertainimportantissuesregardingpatient preparationforobtainingmeaningfulclinicallaboratory testresults.Forexample,glucosetestingmustbedone afterthepatienthasfastedovernight.Theseissuesare discussedinthissection.
Fasting
Theeffectsofmealsonbloodtestresultshavebeen knownforsometime.Increasesinserumglucose,triglycerides,bilirubin,andaspartateaminotransferase
arecommonlyobservedaftermealconsumption.On theotherhand,fastingwillincreasefatmetabolism andincreasetheformationofacetone, b-hydroxybutyric acid,andacetoacetatebothinserumandinurine. Longerperiodsoffasting(morethan48h)mayresult inuptoa30-foldincreaseintheseketonebodies. Glucoseisprimarilyaffectedbyfastingbecauseinsulin keepstheserumconcentrationinatightrange (70 110mg/dL).Diabetesmellitus,whichresultsfrom eitheradeficiencyofinsulinoranincreaseintissue resistancetoitseffects,manifestsasanincreaseinblood glucoselevels.Innormalindividuals,afteranaverageof 2hoffasting,thebloodglucoselevelshouldbebelow 7.0mmol/L(126mg/dL).However,indiabeticindividuals,fastingserumlevelsareelevatedandthusconstituteonecriterionformakingthediagnosisofdiabetes. Otherwell-knownexamplesofanalytesshowingvariationwithfastingintervalincludeserumbilirubin,lipids, andserumiron.
Bodyposition
Physiologically,blooddistributiondifferssignificantlyinrelationtobodyposture.Gravitypullsthe bloodintovariouspartsofthebodywhenrecumbent, andthebloodmovesbackintothecirculation,away fromtissues,whenstandingorambulatory.Theseshifts directlyaffectcertainanalytesduetodilutioneffects. Thisprocessisdifferential,meaningthatonlyconstituentsofthebloodthatarenon-diffusiblewillrisebecause thereisareductioninplasmavolumeuponstanding fromasupineposition.Thisincludes,butisnotlimited to,cells,proteins,enzymes,andprotein-boundanalytes (e.g.,thyroid-stimulatinghormone,cholesterol,T4,and medicationssuchaswarfarin).Thereversewilltake placewhenshiftingfromerecttosupinebecausethere willbeahemodilutioneffectinvolvingthesamepreviouslymentionedanalytes.Posturalchangesaffect somegroupsofanalytesinamuchmoreprofound way attimesuptoatwofoldincreaseordecrease dependingonwhetherthesamplewasobtainedfrom asupineoranerectpatient.Mostaffectedarefactors directlyinfluencinghomeostasis,includingrenin,aldosterone,andcatecholamines.Itisvitalforlaboratory requisitionstospecifytheneedforsupinesamples whentheseanalytesarerequested.
WHOLEBLOOD,PLASMA,ANDSERUM SPECIMENSFORCLINICAL LABORATORYANALYSIS
Approximately8%oftotalhumanbodyweightis representedbyblood,withanaveragevolumeinfemalesandmalesof5and5.5L,respectively [1].Whole
bloodconsistsofacellularfraction(w45%)composedof erythrocytes(redbloodcells),leukocytes(whiteblood cells),andthrombocytes(platelets),andaliquidfraction (plasma)(w55%)thattransportstheseelements throughoutthebody.Bloodvesselsinterconnectallthe organsystemsinthebodyandplayavitalrolein communicationandtransportationbetweentissuecompartments.Bloodservesnumerousfunctions,including deliveryofnutrientstotissues;gasexchange;transport ofwasteproductssuchasmetabolicby-productsfor disposal;communicationtotargettissuesthrough hormones,proteinsandothermediators;andcellular protectionagainstinvadingorganismsandforeign material.Giventhesemyriadroles,bloodisanideal specimenformeasuringbiomarkersassociatedwith variousphysiologicalconditions,whetheritisdirect measurementofcellularmaterialandsurfacemarkers ormeasurementofsolublefactorsassociatedwith certainphysiologicalconditions.
Plasmaconsistsofapproximately93%water,withthe remaining7%composedofelectrolytes,smallorganic molecules,andproteins.Variousconstituentsofplasma aresummarizedin Table2.1.Theseanalytesarein transitbetweencellsinthebodyandarepresentinvaryingconcentrationsdependingonthephysiologicalstate ofthevariousorgans.Therefore,accurateanalysisofthe plasmaiscrucialforobtaininginformationregarding diagnosisandtreatmentofdiseases.Inclinical
TABLE2.1 Principalcomponentsofplasma.
ComponentReferencerangeUnits
Sodium136 145mmol/L
Potassium3.5 5.1mmol/L
Bicarbonate17 25mmol/L
Chloride98 107mmol/L
Hydrogenions40mmol/L
Calcium8.6 10.2mg/dL
Magnesium1.6 2.6mg/dL
Inorganicphosphate2.5 4.5mg/dL
Glucose70 99mg/dL
Cholesterol <200(Desirable)mg/dL
Fattyacids3.0g/L
Totalprotein
a
laboratoryanalysis,plasmacanbeobtainedfromwhole bloodthroughtheuseofanticoagulantsfollowedby centrifugation.Consequently,plasmaspecimensfor theclinicallaboratorycontainanticoagulantssuchas heparin,citrate,EDTA,oxalate,andfluoride.Therelativerolesoftheseanticoagulantsinaffectinganalyte measurementsarediscussedlaterinthischapter.In contrasttoanticoagulatedplasmaspecimens,serumis theclearliquidthatseparatesfrombloodwhenitis allowedtoclot.Furtherseparationoftheclearserum fromtheclottedbloodcanbeachievedthroughcentrifugation.Giventhatfibrinogenisconvertedtofibrininclot formationduringthecoagulationcascade,serumcontainsnofibrinogenandnoanticoagulants.Intheclinical laboratory,suitablebloodspecimensincludewhole blood,plasma,andserum.Keydifferencesinthese samplematricesinfluencetheirsuitabilityforcertain laboratorytests Table2.2.
Wholeblood
Inadditiontotheobviousadvantageofwholeblood fortheanalysisofcellularelements,thesespecimensare alsopreferredforanalytesthatareconcentratedwithin thecellularcompartment.Erythrocytescanbeconsideredtobeareadilyaccessibletissuewithminimalinvasiveproceduresandmaymoreaccuratelyreflecttissue distributionofcertainanalytes.Examplesofsuchanalytes,includingvitamins,traceelements,andcertain drugs,arelistedin Table2.3.Erythrocytesarethemost abundantcelltypeintheblood.Inadults,1 mLofblood containsapproximately4 6millionerythrocytes, 4000 11,000leukocytesand150,000 450,000platelets [2].(Theratiooferythrocytes:platelets:leukocytesis ontheorderof900:60:1.)Thehematocritisthevolumetricfractionoferythrocytesexpressedasapercentage ofpackederythrocytesinabloodsampleaftercentrifugation.Thenormalrangeforadultmalesis41 51%,and thatforadultfemalesis36 45% [2].Clearly,alterations inhematocritwilldirectlyaltertheavailableplasmawaterconcentration,whichinturnaffectsthemeasurement ofwater-solublefactorsinwholeblood.
Amajoruseforwholebloodspecimensisforpointof-careanalysis.Althoughpoint-of-caremeterscanbe locatedintheclinicallaboratory,theprimaryadvantage ofthistechnologyisnear-patienttestingofferingrapid andconvenientanalysisandusingsmallsamplevolumeswhiletheclinicianisexaminingthepatient.The mostcommonpoint-of-carespecimensaretakenby skinpuncture.Commonlycalledcapillaryblood,these samplesarecomposedofamixtureofbloodfromthe arterioles,venulesandcapillarieswithinterstitialand intracellularfluids.Furthermore,theextentofdilution withinterstitialandintracellularfluidisalsoaffected
TABLE2.2 Componentsofwholeblood,plasma,andserummatrices.
WholebloodPlasmaSerum
Cellularelements
Erythrocytes
Leukocytes
Thrombocytes
ProteinsProteinsProteins(excludingfibrinogen)
ElectrolytesElectrolytesElectrolytes
NutrientsNutrientsNutrients
Waste(metabolites)Waste(metabolites)Waste(metabolites)
HormonesHormonesHormones
GasesGasesGases
May containanticoagulants Contains anticoagulantsContains no anticoagulants
Patientontherapeutics
Specimenadditive
TABLE2.3 Examplesofanalytesmeasuredinbloodcelllysates.
HematologyVitaminsTraceelementsDrugsToxicelements
Hemoglobin
Redcellindices
Porphyrias
Cytoplasmicporphyrin metabolicenzymeactivity
Directmeasurement
VitaminE
VitaminB1 (thiamine)
VitaminB2 (riboflavin)
AlsoFMN,FAD
VitaminB6 (pyridoxine,pyridoxamine, pyridoxal)
PLP
Biotin
Folicacid(folate)a
Pantothenicacid
Functionalactivity
VitaminB1 (thiamine)
Transketolase
VitaminB2 (riboflavin)
FAD-dependentglutathionereductase
VitaminB6 (pyridoxine,pyridoxamine, pyridoxal)
AST,ALTactivity
VitaminB12 (cyanocobalamin)
Deoxyuridinesuppressiontest
Niacin
NAD/NADPratio
Cyclosporine Sirolimus(rapamycin)
Tacrolimus(FK506,Prograf)
ALT,alanineaminotransferase; AST,aspartateaminotransferase; FAD,flavinadeninedinucleotide; FMN,riboflavin-50 -phosphate; NAD,nicotinamideadenine dinucleotide; NADP,nicotinamideadeninedinucleotidephosphate; PLP,pyridoxal-50 -phosphate. aPlasmaorserumfolatemeasurementsareusuallypreferred.
bythehematocrit.Becausearteriolarpressureisgreater thanthatofcapillariesandvenules,arterialbloodwill predominateinthesesamples [2,3].Giventhesephysiologicaldifferences,analytesmeasuredinwholeblooddo notexactlymatchresultsobtainedfromanalysisof plasmaorserumsamples.Indeed,thereislesswater insideerythrocytescomparedtotheplasma;therefore, levelsofhydrophilicanalytessuchasglucose,electrolytes,andwater-solubledrugswillbelowerinthe capillarywholeblood [4]
Chromium Selenium Zinc
Asmentionedpreviously,itisapparentthatchanges inbothhematocritandplasmawaterlevelscontributeto thediscrepancyinanalytemeasurementsbetween wholebloodandplasmamethods.However,inthe caseofpoint-of-careglucosemeters,itwasproposed andlateradoptedbytheInternationalFederationof ClinicalChemistrythatageneralconversionfactorof 1.11beappliedtoobtainplasma-equivalentglucose molarity [5,6].Althoughthiswasanattempttoproduce moreharmonizedresultsregardingglucosemeasurementandreduceclinicalmisinterpretations,theapplicationofageneralconversionfactordoesnottakeinto accountthewidevariationsinbothhematocritand plasmawaterlevelsexhibitedbysomepatientsubpopulations.Indeed,theproportionoftotalerrors exceeding10and15%inglucosemeasurementshas beenfoundtoincreasewithpatientacuity [7].For thisreason,interpretationofanalytemeasurementsin wholebloodshouldbesensitivetothehemodynamic statusofthepatient.
Plasmaversusserumspecimens
Althoughitisclearthattherearecertainadvantages towholebloodspecimensinpoint-of-careandhematologicaltesting,plasmaandserumarethepreferred bloodspecimensformeasuringsolublefactorsinthe clinicallaboratory.Inadditiontotheirpreviously mentioneddiscrepanciesincomposition,plasmaand serumexhibitvariationsintheconcentrationofcertain analytes.Certainly,thecoagulationcascadecontributes toconsumptionofsomesubstances(e.g.,fibrinogen, platelets,andglucose)andtothereleaseofothers (e.g.,potassium,lactate,lactatedehydrogenase(LD), phosphate,andammonia).Forexample,thepresence offibrinogeninplasmacontributessignificantlytothe higherlevels( 5%)oftotalproteincomparedtoserum [8].Conversely,thereleaseofelementsorcelllysisassociatedwiththecoagulationcascadeisresponsibleforthe increaseinpotassium( 6%),inorganicphosphate ( 11%),ammonia( 38%),andlactate( 22%)inserum comparedtoplasma [8].Furthermore,anticoagulants, preservatives,andotheradditivesthataidorinhibit coagulationmayinterferewiththeassay,asdiscussed later.Also,thepresenceoffibrinogenmayinterfere withchromaticdetectionorbindinginimmunoassays ortheappearanceofapeakthatmaysimulateafalse monoclonalproteininthegammaregionduringprotein electrophoresis [8,9].
Therearemanyadvantagestousingplasmaover serumforclinicallaboratoryanalysis;however,for someanalytes,serumispreferredoverplasma.Characteristicsofserumandplasmaspecimensarecompared below.
Samplevolume
Ifbloodisallowedtoclotandisthencentrifuged, approximately30 50%oftheoriginalspecimenvolume iscollectedasserum.Conversely,plasmaconstitutes approximately55%ofthevolumeofuncoagulated bloodaftercentrifugation.Therefore,thehigheryield associatedwithplasmasamplesisgenerallypreferred, especiallywhensamplevolumemaybecriticalasin thecaseofthepediatricpopulation,smallerpatients, orinspecialcasesinwhichbloodvolumeneedstobe conserved.
Samplepreparationtime
Theprocessofclottingrequiresatleast30minunder normalconditionswithoutcoagulationaccelerators. Furthermore,coagulationmaystilloccurpostcentrifugationinserumsamples.Therefore,another advantageofplasmaisthatanalytedeterminationscan beachievedinwholebloodpriortoplasmaseparation providedthatasuitableanticoagulanthasbeenused. Forexample,ananticoagulatedwholebloodspecimen maybeusedforpoint-of-caremeasurementsfollowed byplasmaseparation,whichwouldavoidthedelay associatedwithobtaininganadditionalspecimenfor laboratoryanalysis.
Invitrohemolysis
Inadditiontothetimedelayassociatedwith bloodclotting,thereisanincreasedriskoflysisand consequentfalseincreasesinmanyintracellularanalytessuchaspotassium,iron,andhemoglobin(hgb) releasedfromerythrocytesinserumspecimens. Therefore,itisadvisedtoseparatetheserumas quicklyaspossible.Conversely,plasmaseparation canbeachievedathighercentrifugalspeedswithout riskingtheinitiationofhemolysisandthrombocytolysis [8] .
Specimencomposition
Anticoagulantsandadditivesinplasmaspecimens candirectlyinterferewiththeanalyticalcharacteristics oftheassay,proteinbindingwiththeanalyteofinterest,andsamplestability.Furthermore,liquidanticoagulantsmayleadtoimproperdilutionofthesample.For example,blooddrawnintubeswithsodiumcitrateis dilutedby10%,butthismayincreasedependingon whetherthedrawiscomplete.Moreover,incomplete mixingwithanticoagulantscanleadtotheriskof clotformation.Also,thechoiceofanticoagulantwill dependontheirrespectiveinfluencesonthevarious assaysofferedbytheclinicallaboratory,andtubes withanticoagulantsandadditivesareoftenmore expensive.
ANTICOAGULANTSAND PRESERVATIVES,ORDEROFDRAW, SEPARATORTUBEGELINTERFERENCE ANDVOLUME
Selectionofevacuatedbloodcollectiontubes(BCT) forspecimencollectionhasamajorimpactonclinical laboratoryresults.Appropriatequalityprocessesmust bemaintainedtoensureaccurateandreliablelaboratory results.Krickaetal. [10] demonstratedhowlaboratories canestablishtheirownprocessesusingcontrolmaterials toverifyinterferencesintheBCTtheyuse.Bowenetal. [11] providedacomprehensivereviewofthedifferent BCTcomponentsthatcancontributetoanalyticalerrors intheclinicallaboratory. Table2.4 summarizesthecomponentsofBCTandindicationsforuse.Theinclusionof additivesisnecessaryforreducingpre-analyticalvariabilityandforfasterturnaroundtimesinthelaboratory. BCTareavailablewithavarietyoflabelingoptionsand stoppercolorsaswellasarangeofdrawvolumes. Additivesaredesignatedtopreserveorstabilizeanalytesbyinhibitingmetabolicenzymes.Additivessuchas clotactivatorsareaddedtoplasticBCTtofacilitate clotting.Stoppersandstopperlubricantsaregenerally manufacturedtofacilitatecapping,de-capping,and bloodflowduringcollectionandtominimizeadsorption.Separatorgelsareusedtoseparatepackedblood cellsfromserumorplasma.Anticoagulantsareused topreventcoagulationofbloodorbloodproteins.For asummaryofcollectionadditives,referto Table2.5
Plasticandglasstubes
Mostclinicallaboratorieshaveroutinelymovedaway fromglasstoplasticBCTtocomplywithoccupational healthandsafetystandardsbecauseplasticBCTare safertouseandreducepotentialexposuretoblood [12].Comparedtoglass,thepolyethylenetetraphthalatematerialsusedinBCTaregenerallyunbreakable,canwithstandhighcentrifugationspeeds,areinert
TABLE2.4 Componentsinevacuatedbloodcollectiontubesand indicationsforuse.
ComponentsIndications
TubewallPlasticorglass:Plasticpreferable forsafetyreasons
StopperInertplasticizers
SurfactantsSiliconeminimizesadsorptionof analytes,cells
StopperlubricantsEaseofcapping,de-capping
ClotactivatorPromoteclottingtoobtainserum inplasticcollectiontubes
toadsorptionofanalytes,arelighter,andcanbeeasily incineratedfordisposal.Incontrasttoplasticsurfaces, therelativelyhydrophilicsurfaceofglassallowsfor clotadherenceandisidealforbloodflow.Also,thesilica surfaceofglassgreatlyfacilitatestheclottingofblood, allowingforacleanerseparationoftheclotfromserum duringcentrifugation.Forthesereasons,theinterior surfaceofplasticcollectiontubesandstoppersisnow routinelyspray-coatedwithsurfactantsandsilicate polymerstomakethesurfacepropertiessimilartothose ofglass.Afewclinicallysignificantdifferencesbetween glassandplasticexistforavarietyofdifferenttests rangingfromgeneralchemistrytospecialchemistry, moleculartesting,andhematology.
Surfactants
CommerciallyavailableBCTmaycontaindifferent typesofsurfactantsthatareoftennotlistedinthemanufacturer’spackageinsertbutarecommonlysiliconebasedpolymers.Althoughtheseareconsideredtobe inert,therehavebeenreportsofinterferencesinclinical assays.Generally,surfactantscanbindnonspecifically, displacefromsolidmatrixandcomplexwithormask detectionofsignalantibodiesinimmunoassayreagents, contributingtoincreasesinabsorbanceandturbidityto causeinterferences [13].Bowenetal. [14,15] showedthat thesurfactantSilwetL-720usedinBDSSTcollection tubesgavefalselyelevatedtotaltriiodothyronine(TT3) bytheImmulite2000/2500immunoassay.Onemechanismshownwasthatincreasingsurfactantconcentrationsdosedependentlydesorbedthecaptureantibody fromthesolidphaseamongothernonspecificeffects. However,thiswasmethod-dependentbecauseTT3 levelswereunaffectedbytheAxSYMimmunoassay,in whichantibodiesareadsorbedontothesolidphase withmorerobustbinding [14,15].ThisBCT manufacturerconfirmedsimilarinterferencesforavarietyofotherimmunoassays(folate,vitaminB12,folliclestimulatinghormone,hepatitisBsurfaceantigen,cancer antigen27,andcortisol)onavarietyofdifferentinstrumentplatformsandhassincedecreasedthesurfactant contenttoreducethisinterference [16,17].
Stoppersandstopperlubricants
Stopperlubricantscontainingglycerolorsilicone makecappingandde-cappingoftubeseasier,aswell asminimizeadherenceofcellsandclotstostoppers. Standardred-toppedBCTarecontaminatedwithzinc, aluminumandmagnesium;andallcontainvarying amountsofheavymetals [18].Forthisreason,most labshavespecificrequirementsforcollectionofspecimensforheavymetalassay.Componentssuchastris
TABLE2.5 Bloodcollectiontubes,additives,andgeneralapplications.
TubetypeAdditiveStoppercolorApplication
SERUM
GlassNoneRedTeststhatcannotbecollectedinto SSTtubes
Plastic(acidwashed)NoneRoyalblue(redbandlabel)Traceelementsserum(copper,zinc, aluminum,chromium,nickel)
PlasticClotactivatorRed/blackTeststhatcannotbecollectedwithgel; sometherapeuticdrugs (antidepressants)
PlasticalsocalledSSTClotactivator þ gelseparatorGoldManychemistryand immunochemistrytests;hepatitistests
PlasticalsocalledRSTThrombin þ gelseparatorOrangeRapidclotting(5min);general chemistrytestsforacutecare requiringurgentturnaroundtime
PLASMAORWHOLEBLOOD
PlasticalsoacalledPSTLithium-heparin þ gelseparatorLightmintgreenMostchemistrytestsforacutecare requiringfastturnaroundtime, ammonia
HeavymetalfreeNa2EDTAorK2EDTARoyalblue(withlavender orbluebandonlabel) Traceelementsblood(lead,arsenic, cadmium,cobalt,manganese, mercury,molybdenum,thallium)
PlasticAcidcitratedextrosesolution“A” (ACDA)
PaleyellowFlowcytometry(CD3,CD4,CD8); HLAtyping
PlasticSodiumfluoride,potassium oxalate,iodoacetate GrayPreservesglucoseupto5days;lactate, glucose(tolerance)
PlasticSodium,lithium,orammonium heparin(nogel) DarkgreenAminoacids,bloodgases,glucose phosphatedehydrogenase(G6PD)
PlasticSodiumcitrateLightbluePT(INR),PTT,othercoagulationtests
GlassSodiumcitrateBlackErythrocytesedimentrate
GlassSodiumheparinDarkgreenToxicologyandnutritionaltests
K2EDTAorK3EDTALavender/PurpleRoutinehematology,pretransfusion (bloodbank),HbA1c,antirejection drugs,parathyroidhormone
(2-butoxyethyl)phosphatefromrubberstoppertubes leachingintothebloodduringcollectionhavebeen showntodisplacedrugsfrombindingproteinsinblood [19].Manufacturershavereformulatedstopperplasticizercontenttominimizethiseffect.Triglycerideassays thatmeasureglycerolcanbefalselyelevatedbysuch effect.Stoppercomponentsandstopperlubricantscan alsobeapotentialsourceofinterferencewithmass spectrometry-basedassays [20]
Serumseparatorgeltubes(SST)
Separatorgelsarethixotropicmaterialsthatforma physicochemicalbarrieraftercentrifugationinBCTto separatepackedcellsfromplasmaorserum.Delayin
separatingclotresultsinintracellularleakageofpotassium,phosphate,magnesium,andLDintoserum, plasma,orwholeblood [21].Easeofuseofasingle centrifugationstep,improvedspecimenanalytestability,reducedneedforaliquoting,convenientstorage, andtransportinasingleprimarytubearereasonsfor preferentialusageofSSTintheclinicallaboratory.Itis veryimportanttofollowmanufacturerprotocolsforlaboratoryconditionssuchaspropertubemixingafter collection,centrifugationaccelerationanddeceleration speeds,temperature,andstorageconditions.Noncompliancemayresultinunexpecteddegradationof separatorgelorreleaseofgelcomponents.Geland oildropletsinterferewithaccuracyandliquid-level sensingofinstrumentpipettes,coatcuvettes,andbind
tosolidphaseinheterogeneousimmunoassays. Re-centrifugation,inadequateblood-drawvolume,storagetime,temperature,anddrugadsorptionmayaffect laboratoryresults.Hydrophobicityofthedrug,length oftimeonseparatorgel,storagetemperature,andmethodologysensitivityareimportantconsiderationswith regardtothestabilityoftherapeuticdrugsinBCT.Dasguptaetal. [22] demonstratedthathydrophobicdrugs suchasphenytoin,phenobarbital,carbamazepine,quinidine,andlidocaineareadsorbedontothegelwithsignificantdecreases(rangingfrom5.9to64.5%)inserum VacutainerSSTtubes.Reformulationoftheseparator gelinSSTIItubessignificantlyreducedabsorption andimprovedperformance [23].Schouwersetal. [24] demonstratedminimaleffectofseparatorgelinStarstedtS-Monovetteserumtubesforthecollectionof fourtherapeuticdrugs(amikacin,vancomycin,valproic acid,andacetaminophen)andeighthormonesand proteins.
Anticoagulants
Anticoagulantsareusedtopreventcoagulationof bloodorbloodproteinstoobtainplasmaorwholeblood specimens.Themostroutinelyusedanticoagulantsare EDTA,heparin(sodium,ammonium,orlithiumsalts), andcitrates(trisodiumandacidcitratedextrose).Anticoagulantscanbepowdered,crystallized,solids,or lyophilizedliquids.Theoptimalanticoagulant:blood ratioisessentialtopreserveanalytesandpreventclot orfibrinformationviavariousdifferingmechanisms.
Inmostclinicallaboratories,potassiumEDTAisthe anticoagulantofchoiceforthecompletebloodcount, asrecommendedbytheInternationalCouncilofStandardizationinHematology [25] andtheClinicaland LaboratoryStandardsInstitute [26].Dipotassium,tripotassium,ordisodiumsaltsofEDTAareusedasdryor liquidadditivesinfinalconcentrationsrangingfrom 1.5to2.2mg/mLbloodwhentheevacuatedBCTis filledcorrectlytoitsstateddrawvolume.EDTAactsas achelatingagenttobindcofactordivalentcations (mainlycalcium)toinhibitenzymereactionsintheclottingcascade particularlytheconversionofprothrombintothrombinandsubsequentinhibitionofthe thrombolyticactiononfibrinogentofibrinnecessary forclotformation [27].Forthisreason,EDTAplasma isnotrecommendedforcoagulationtestssuchasprothrombintime(PT)andactivatedpartialthromboplastin time(aPTT) [28].EDTAisanexcellentpreservativeof bloodcellsandmorphologyparameters.Stabilityis 48hforhgband24hforerythrocytes.BecausethehypertonicactivitybyEDTAcanaltererythrocyticindices andhematocrit,smearsshouldbemadewithin2or3h oftheblooddraw.Thewhitebloodcellcountremains stableforatleast3daysinEDTAanticoagulatedblood
storedatroomtemperature.EDTAisadequatefor plateletpreservation;however,morphologicalchanges occurovertime [29].ClottingcanresultifthereisinsufficientEDTArelativetoblood.Thisisusuallycausedby overfillingthevacuumtubeorpoorsolubilityofEDTA (mostcommonlywithdisodiumsalts) [30].EDTAdraws waterfromcellstoartifactuallydiluteplasmaandis generallynotrecommendedforgeneralchemistrytests. EDTAchelatesothermetallicionssuchascopper,zinc, ormagnesiumandalterscofactor-dependentactivity ofmanyenzymes,suchasalkalinephosphataseandcreatinekinase,andhenceisnotusedforthesechemistry assays.EDTAisalsousedforbloodbankpretransfusion testing;flowcytometry;HemoglobinA1c (HbA1c);and mostcommonimmunosuppressiveanti-rejectiondrugs, suchascyclosporine,tacrolimus,sirolimus,andeverolimus.WholebloodEDTAinBCTtransportedoniceis preferableforthecollectionofunstablehormones susceptibletoproteolysis invitro,suchascorticotropin, parathyroidhormone,C-peptide,vasoactivepeptide (VIP),antidiuretichormone,carboxy-terminalcollagen cross-links,calcitonin,renin,procalcitonin,andunstable peptidessuchascytokines.Spray-driedpotassium EDTAisthepreferredanticoagulantforquantitative proteomicandmolecularassayprotocolssuchas viralnucleicacidextraction,geneamplification,or sequencing [27]
Heparin,aheterogeneousmixtureofanionicglycosaminoglycans,inactivatesserineproteasesinthecoagulationcascade primarilythrombinandfactorsII (prothrombin)andXa throughanantithrombindependentmechanism.Forthisreason,heparinized plasmaisnotusedforcoagulationtests.Typically, lyophilizedorsolidlithium,sodium,orammonium saltsofheparinareaddedtoBCTatvaryingfinalconcentrationsof10 30USPunits/mLofblood [26].Hygroscopicheparinformulationsareusedinsteadof solutionstoavoiddilutioneffects.Heparinistherecommendedanticoagulantformanychemistrytests requiringwholebloodorplasmabecausechelating propertiesandeffectsonwatershiftsincellsareminimal.Heparinizedplasmaisusefulfortestsrequiring fasterturnaroundtimesbecauseitdoesnotrequireclotting,minimizingtheriskofsamplepipettinginterferenceduetofibrinmicroclots [31].Heparinistheonly anticoagulantrecommendedforthedeterminationof pHbloodgases,electrolytes,andionizedcalcium [32]. Lithiumhepariniscommonlyusedinsteadofsodium heparinforgeneralchemistrytests [33].Obviously,additivesmaydirectlyaffectthemeasurementofcertain analytes.Forexample,lithiumheparinplasmacan havelithiumlevelsinthetoxicrange,greaterthan 1.0mmol/L;whenfilledcorrectly,sodiumheparintubes canelevatesodiumlevels1 2mmol/L;andammonium heparinincreasesmeasuredammonialevels [28].
Heparinshouldnotbeusedforcoagulationtestsandis notrecommendedforproteinelectrophoresisandcryoglobulintestingbecauseofthepresenceoffibrinogen, whichco-migrateswith b2 monoclonalproteins.Informationontubetypeperformanceonmanyanalytical testsaswellasspecimenstabilitycharacteristicsis availablefrommanufacturersuponrequest.TheBD DiagnosticPreanalyticalDivisionpublishesclinical “whitepapers”formostoftheirvariousBCTproducts [34].
TheBCTrecommendedbytheClinicalLaboratory StandardsInstitute(CLSIH21-A5-2008)forcoagulation testingistrisodiumcitratebuffered(tomaintainthe pH)orunbuffered,availableas3.2%(or3.8%)concentrations [35].Becausethedifferentconcentrationsproducedifferentresults,itisnecessarythatonlyone concentration(preferably3.2%)beusedconsistentlyby alaboratory.Thecombinationofsodiumcitrateand citricacidiscalledbufferedsodiumcitrate.Therecommendedpreservativeratiois9:1(blood:citrate).Citric acidanddextroseshouldnotbeusedbecausethiscombinationwilldilutetheplasmaandcausehemolysis. Differentcitrateconcentrationscanhavesignificant effectsonPTTandPTassays,resultinginvariable reagentresponsiveness.Itisnecessaryforlabsusing theinternationalnormalizationratio(INR)toensure thesamecitrateconcentrationisusedforthedeterminationoftheInternationalSensitivityIndex.Sodium citrateactsprimarilytochelatecalcium,andcoagulation factorsareunaffected.Thebindingeffectofcitratecan bereversedbyrecalcifyingthebloodorderivedplasma toitsnormalstate.Thisreversibleactionmakesithighly desirableforclottingandfactorassaystudies.Citrate alsohasminimaleffectsoncellsandplateletsandis usedforplateletaggregationstudies.
Hirudinisasingle-chain,carbohydrate-freepolypeptidederivedfromtheleech(Hirudomedicinalis).Hirudin bindsirreversiblytothefibrinogenrecognitionsiteof thrombinwithouttheinvolvementsofcofactorsto preventtransformationoffibrinogentofibrin.Theuse ofhirudinasamorepotentanticoagulantispromising forgeneralchemistry,hematology,andmolecular testing,althoughitisnotreadilycommerciallyavailable [36] .
Thrombininitiatesclottinginthepresenceofcalcium. Rapid5-minClotSerumTube(RST)containing thrombinasanadditiveisnowcommerciallyavailable fromBD.Laboratoriesfindtheseidealforobtaining serumforassaysrequiringafastturnaroundtime [37] Strathmannetal. [38] showedthatRSTtubeshavefewer false-positiveresultsandbetterreproducibility comparedtolithiumheparinPSTtubesfor28general chemistrytestsandimmunoassays.
Potassiumoxalateisusedincombinationwith sodiumfluorideandsodiumiodoacetatetoinhibit
enzymesinvolvedintheglycolyticpathway.Potassium oxalatechelatescalciumandcalcium-dependentenzymesandreactionstoactasananticoagulant.Sodium fluorideinhibitsenolaseandiodoacetateinhibitsglyceraldehyde-3-phosphatedehydrogenaseenzymeactivity topreventmetabolismofglucoseandethanol.Oxalate BCTisusefulspecificallyforglucose,lactate,and ethanoltests.Glycolysisenzymeinhibitionisnotimmediateandmaybedelayedupto4haftercollection, allowingglucoselevelstofallby5 7%perhourat roomtemperature.Forthisreason,theuseoffluoride anticoagulantsisundesirableforthecollectionof neonatalglucosespecimensincapillarywholeblood unlessthespecimensaretransportedonice.
ORDEROFDRAWOFVARIOUSBLOOD COLLECTIONTUBES
Toavoiderroneousresults,BCTmustbefilledor usedduringphlebotomyinaspecifiedorder.Astandardizedorderofdraw(OFD)minimizescarryover contaminationofadditivesbetweentubes. Table2.6 showsanexampleoftheOFDforbloodcollectionas usedatCalgaryLaboratoryServices.Manylaboratories haveestablishedtheirownprotocolsfortheOFDfor multipletubecollections,withslightvariationsbased onCLSIrecommendations.Thegeneralorderofdraw isasfollows:
1. Microbiologicalbloodculturetubes
2. Traceelementtubes(nonadditive)
3. Citratedcoagulationtubes
4. Non-anticoagulanttubesforserum(clotactivator,gel ornogel)
5. Anticoagulant:heparintubes(withorwithoutgel)
6. Anticoagulant:EDTAtubes
7. Acidcitratedextrosetubes
8. Glycolyticinhibitortubes
Tubeswithadditivesmustbethoroughlymixedby gentleinversionaspermanufacturerrecommended protocols.Erroneoustestresultsmaybeobtained whenthebloodisnotthoroughlymixedwiththeadditive.Adiscardtube(plastic/noadditive)issometimes usedtoremoveairandprimethetubingwhenawinged bloodcollectionkitisused.Tubesformicrobiological bloodculturesarefilledfirsttoavoidbacterialcontaminationfromepidermalflora.Whentracemetaltesting onserumisordered,itisadvisabletousetraceelement tubes.Royal-blueMonojecttraceelementBCTareavailableforthispurpose.Thesetubesarefreefromtraceand heavymetals;however,itisadvisabletoconsultthe manufacturer’spackageinserttodetermineuppertolerablelimitsoftraceandheavymetalcontaminationto determineacceptabilityforclinicaldiagnosticuse.