https://ebookmass.com/product/a-pharmacology-primertechniques-for-more-effective-and-strategic-drugdiscovery-6th-edition-terry-kenakin/
Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
A Pharmacology Primer: Techniques for More Effective and Strategic Drug Discovery 5th Edition Terry P. Kenakin
https://ebookmass.com/product/a-pharmacology-primer-techniques-formore-effective-and-strategic-drug-discovery-5th-edition-terry-pkenakin/
ebookmass.com
Comprehensive Pharmacology 7 Volume Set Terry P. Kenakin
(Editor)
https://ebookmass.com/product/comprehensive-pharmacology-7-volume-setterry-p-kenakin-editor/
ebookmass.com
Towards More Effective Global Drug Policies 1st ed. Edition Caroline Chatwin
https://ebookmass.com/product/towards-more-effective-global-drugpolicies-1st-ed-edition-caroline-chatwin/
ebookmass.com
International Business 3rd Edition Klaus Meyer
https://ebookmass.com/product/international-business-3rd-editionklaus-meyer/
ebookmass.com
Annelie Sjölander-Lindqvist
https://ebookmass.com/product/anthropological-perspectives-onenvironmental-communication-annelie-sjolander-lindqvist/
ebookmass.com
Japanese from Zero books 1 to 5 plus kana and kanji all 7 books in just about complete series Yukari Taken
https://ebookmass.com/product/japanese-from-zero-books-1-to-5-pluskana-and-kanji-all-7-books-in-just-about-complete-series-yukari-taken/
ebookmass.com
Conflicts, Crimes and Regulations in Cyberspace, Volume 2 Sebastien-Yves Laurent
https://ebookmass.com/product/conflicts-crimes-and-regulations-incyberspace-volume-2-sebastien-yves-laurent/
ebookmass.com
Fundamentals on Oral and Maxillofacial Surgery Divya Mehrotra
https://ebookmass.com/product/fundamentals-on-oral-and-maxillofacialsurgery-divya-mehrotra/
ebookmass.com
(eBook PDF) Social Inequality: Forms, Causes, and Consequences 10th Edition
https://ebookmass.com/product/ebook-pdf-social-inequality-formscauses-and-consequences-10th-edition/
ebookmass.com
Coding for Kids 5 Books in 1: Javascript, Python and C++
Guide for Kids and Beginners (Coding for Absolute Beginners) Mather
https://ebookmass.com/product/coding-for-kids-5-books-in-1-javascriptpython-and-c-guide-for-kids-and-beginners-coding-for-absolutebeginners-mather/ ebookmass.com
APharmacologyPrimer
Please view supplementary content for this volume on the Companion website:
https://www.elsevier.com/books-and-journals/book-companion/9780323992893 A Pharmacology Primer, 6e Terry Kenakin, Author
Available Resources:
• Interactive quiz
APharmacologyPrimer TechniquesforMoreEffectiveandStrategic
DrugDiscovery
SixthEdition
TerryP.Kenakin
ProfessorofPharmacology
TheUniversityofNorthCarolinaSchoolofMedicine ChapelHill,NC,UnitedStates
AcademicPressisanimprintofElsevier 125LondonWall,LondonEC2Y5AS,UnitedKingdom 525BStreet,Suite1650,SanDiego,CA92101,UnitedStates 50HampshireStreet,5thFloor,Cambridge,MA02139,UnitedStates TheBoulevard,LangfordLane,Kidlington,OxfordOX51GB,UnitedKingdom
Copyright © 2022ElsevierInc.Allrightsreserved.
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans,electronicormechanical,including photocopying,recording,oranyinformationstorageandretrievalsystem,withoutpermissioninwritingfromthepublisher. Detailsonhowtoseekpermission,furtherinformationaboutthePublisher’spermissionspoliciesandourarrangements withorganizationssuchastheCopyrightClearanceCenterandtheCopyrightLicensingAgency,canbefoundatourwebsite: www.elsevier.com/permissions
ThisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythePublisher(otherthanasmay benotedherein).
Notices
Knowledgeandbestpracticeinthis fieldareconstantlychanging.Asnewresearchandexperiencebroadenourunderstanding, changesinresearchmethods,professionalpractices,ormedicaltreatmentmaybecomenecessary.
Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgeinevaluatingandusingany information,methods,compounds,orexperimentsdescribedherein.Inusingsuchinformationormethodstheyshouldbe mindfuloftheirownsafetyandthesafetyofothers,includingpartiesforwhomtheyhaveaprofessionalresponsibility.
Tothefullestextentofthelaw,neitherthePublishernortheauthors,contributors,oreditors,assumeanyliabilityforany injuryand/ordamagetopersonsorpropertyasamatterofproductsliability,negligenceorotherwise,orfromanyuseor operationofanymethods,products,instructions,orideascontainedinthematerialherein.
ISBN:978-0-323-99289-3
ForinformationonallAcademicPresspublicationsvisitourwebsiteat https://www.elsevier.com/books-and-journals
Publisher: StacyMasucci
AcquisitionsEditor: AndreG.Wolff
EditorialProjectManager: ZsereenaRoseMampusti
ProductionProjectManager: OmerMukthar
CoverDesigner: VickyPearsonEsser
TypesetbyTNQTechnologies
Dedication
Asalways . forDebbie.
Thispageintentionallyleftblank
1. Whatispharmacology?
1.1Aboutthisbook 1 1.2Whatispharmacology? 1 1.3Thereceptorconcept 3
1.4Pharmacologicaltestsystems 4
1.5Thenatureofdrugreceptors 7
1.6Fromthesnapshottothemovie 7
1.7Pharmacologicalinterventionandthe therapeuticlandscape 8
1.8System-independentdrugparameters: affinityandefficacy 11
1.9Whatisaffinity? 13
1.10TheLangmuiradsorptionisotherm 14 1.11Whatisefficacy? 15
1.12Dose responsecurves 17
1.12.1Potencyandmaximalresponse 18
1.12.2 P-scalesandtherepresentation ofpotency 18
1.13Chaptersummaryandconclusions 20
1.14Derivations:conformationalselection
2. Howdifferenttissuesprocessdrug response
2.1The‘eyestosee’:pharmacologicassays 23
2.2Thebiochemicalnatureofstimulus responsecascades 25
2.3Themathematicalapproximationof stimulus responsemechanisms 27
2.4Influenceofstimulus response cascadesondose responsecurve slopes 29
2.5Systemeffectsonagonistresponse: fullandpartialagonists 30
2.6Differentialcellularresponseto receptorstimulus 33
2.6.1Choiceofresponsepathway
2.6.3Differencesinreceptordensity
2.7Receptordesensitizationand tachyphylaxis 37
2.8Themeasurementofdrugactivity 40
2.9Advantagesanddisadvantagesof differentassayformats 40
2.10Drugconcentrationasanindependent variable 41
2.10.1Dissimulationindrug concentration 41
2.10.2Freeconcentrationofdrug 43
2.11Chaptersummaryandconclusions 43 2.12Derivations 43
2.12.1Serieshyperbolaecanbe modeledbyasingle hyperbolicfunction 44
2.12.2Successiverectangularhyperbolicequationsnecessarily leadtoamplification 44
2.12.3Saturationofanystepina stimuluscascadebytwo agonistsleadstoidentical maximalfinalresponsesfor thetwoagonists 44
2.12.4Proceduretomeasurefree drugconcentrationinthe receptorcompartment 45 References 45
3. Drug receptortheory
3.1Aboutthischapter 47
3.2Drug receptortheory 47
3.3Theuseofmathematicalmodelsin pharmacology 48
3.4Somespecificusesofmodelsin pharmacology 49
3.5Massactionbuildingblocks 55
3.6Classicalmodelofreceptor function 56
3.7Theoperationalmodelofreceptor function 57
3.8Two-statetheory 58
3.9Theternarycomplexmodel 59
3.10Theextendedternarycomplexmodel 59
3.11Constitutivereceptoractivityand inverseagonism 60
3.12Thecubicternarycomplexmodel 62
3.13Multistatereceptormodelsand probabilistictheory 63
3.14Chaptersummaryandconclusions 65
3.15Derivations 65
3.15.1Radioligandbindingto receptordimersdemonstrating cooperativebehavior 65
3.15.2EffectofvariationinanHIV-1 bindingmodel 66
3.15.3Derivationoftheoperational model 67
3.15.4Operationalmodelforcing functionforvariableslope 67
3.15.5Derivationoftwo-statetheory 68
3.15.6Derivationoftheextended ternarycomplexmodel 68
3.15.7Dependenceofconstitutive activityonreceptordensity 69
3.15.8Derivationofthecubicternary complexmodel 69 References 69
4. Pharmacologicalassayformats: binding
4.1Thestructureofthischapter 71
4.2Bindingtheoryandexperiment 71
4.2.1Saturationbinding 74
4.2.2Displacementbinding 76
4.2.3Kineticbindingstudies 79
4.3Complexbindingphenomena:agonist affinityfrombindingcurves 80
4.4Experimentalprerequisitesforcorrect applicationofbindingtechniques 84
4.4.1Theeffectofproteinconcentrationonbindingcurves 84
4.4.2Theimportanceofequilibration timeforequilibriumbetween twoligands 85
4.5Bindinginallostericsystems 87
4.6Chaptersummaryandconclusions 91
4.7Derivations 92
4.7.1Displacementbinding: competitiveinteraction 92
4.7.2Displacementbinding: noncompetitiveinteraction 92
4.7.3Displacementofaradioligand byanallostericantagonist 92
4.7.4RelationshipbetweenIC50 and KI forcompetitiveantagonists 93
4.7.5Maximalinhibitionofbinding byanallostericantagonist 94
4.7.6RelationshipbetweenIC50 and KI forallostericantagonists 94
4.7.7Two-stagebindingreactions 94
4.7.8EffectofG-Proteincouplingon observedagonistaffinity 94
4.7.9Effectofexcessreceptorin bindingexperiments:saturation bindingcurve 94
4.7.10Effectofexcessreceptorin bindingexperiments:displacementexperiments 95
4.7.11Derivationofanallostericbindingmodel 95 References 96
5. Drugtargetsanddrug-target molecules
5.1Definingbiologicaltargets 97
5.2Specifictypesofdrugtargets 100
5.2.1G-protein-coupledreceptors 100
5.2.2Ionchannels 102
5.2.3Enzymes 103
5.2.4Nuclearreceptors 111
5.2.5Nucleotide-baseddrugtargets 112
5.3Smalldrug-likemolecules 114
5.3.1Hybridmolecules 116
5.3.2Chemicalsourcesforpotential drugs 121
5.4Biologics 126
5.4.1Replacementproteins 127
5.4.2Eliminating‘undruggable’proteinsthroughPROTACs 130
5.4.3Peptides 131
5.4.4Antibodies 135
5.4.5Immunotherapy 141
5.4.6Vaccines 141
5.4.7Nucleicacid baseddrugspecies 142
5.5Summaryandconclusions 147 References 147 Furtherreading 149
6. Agonists:themeasurementofaffinity andefficacyinfunctionalassays
6.1Functionalpharmacological experiments 151
6.2Thechoiceoffunctionalassays 152
6.3Recombinantfunctionalsystems 156
6.4Functionalexperiments:dissimulation intime 159
6.5Experimentsinrealtimeversus stop-time 160
6.6Quantifyingagonism:theBlack Leff operationalmodelofagonism 162
6.6.1Affinity-dependentversus efficacy-dependentagonist potency 166
6.6.2Secondaryandtertiarytesting ofagonists 168
6.7Biasedsignaling 169
6.7.1Receptorselectivity 175
6.8Nullanalysesofagonism 175
6.8.1Partialagonists 175
6.8.2Fullagonists 179
6.9Comparingfullandpartialagonist activities:Log(max/EC50) 182
6.10Chaptersummaryandconclusions 183
6.11Derivations 183
6.11.1RelationshipbetweentheEC50 andaffinityofagonists 183
6.11.2MethodofBarlow,Scott,and Stephensonforaffinityof partialagonists 184
6.11.3Maximalresponseofapartial agonistisdependenton efficacy 184
6.11.4Systemindependenceoffull agonistpotencyratios 184
6.11.5Measurementofagonist affinity:methodofFurchgott 184
6.11.6Agonismasapositive allostericmodulationof receptor signalingprotein interactiontoderive DLog(max/EC50)ratios 185 References 187
7. Orthostericdrugantagonism
7.1Introduction 189
7.2Kineticsofdrug receptorinteraction 189
7.3Surmountablecompetitiveantagonism 192
7.3.1Schildanalysis 192
7.3.2PatternsofDose Response curvesthatprecludeschild analysis 197
7.3.3Bestpracticefortheuseof schildanalysis 198
7.3.4Analysesforinverseagonistsin constitutivelyactivereceptor systems 199
7.3.5Analysesforpartialagonists 201
7.3.6ThemethodofLewandAngus: nonlinearregressionanalysis 203
7.4Noncompetitiveantagonism 204
7.5Agonist antagonisthemiequilibria 208
7.6Resultantanalysis 210
7.7Antagonisminvivo 210
7.7.1Antagonistswithefficacyin vivo 212
7.7.2Kineticsoftargetcoverage 214
7.7.3Kineticsofdissociation 216
7.7.4Estimatingantagonist dissociationwithhemiequilibria 219
7.8Blockadeofindirectlyactingagonists 219
7.9Irreversibleantagonism 220
7.10Chemicalantagonism 222
7.11Chaptersummaryandconclusions 226
7.12Derivations 227
7.12.1DerivationoftheGaddum equationforcompetitive antagonism 227
7.12.2DerivationoftheGaddum equationfornoncompetitive antagonism 227
7.12.3Derivationoftheschild equation 228
7.12.4Functionaleffectsofan inverseagonistwiththe operationalmodel 228
7.12.5pA2 measurementforinverse agonists 228
7.12.6Functionaleffectsofapartial agonistwiththeoperational model 229
7.12.7pA2 measurementsforpartial agonists 229
7.12.8MethodofStephensonfor partialagonistaffinity measurement 229
7.12.9DerivationoftheMethodof Gaddumfornoncompetitive antagonism 230
7.12.10RelationshipofpA2 andpKB forinsurmountable orthostericantagonism 230
7.12.11Resultantanalysis 230
7.12.12Blockadeofindirectlyacting agonists 231
7.12.13Chemicalantagonism: abstractionofagonist concentration 231
7.12.14Chemicalantagonism: abstractionofantagonist concentration 231
References 232
8. Allostericmodulation
8.1Introduction 233
8.2Thenatureofreceptorallosterism 233
8.3Uniqueeffectsofallostericmodulators 235
8.4Functionalstudyofallostericmodulators 240
8.4.1Phenotypicallostericmodulation profiles 242
8.4.2Allostericagonism 243
8.4.3Affinityofallostericmodulators 243
8.4.4Negativeallostericmodulators 246
8.4.5Positiveallostericmodulators 250
8.4.6QuantifyingPAMactivityinvivo 254
8.4.7NAM/PAMinducedagonistbias 255
8.4.8Optimalassaysforallosteric function 255
8.5Functionalallostericmodelwith constitutiveactivity 256
8.6Internalchecksforadherencetothe allostericmodel 257
8.7Methodsfordetectingallosterism 260
8.8Chaptersummaryandconclusions 262
8.9Derivations 262
8.9.1Allostericmodelofreceptor activity 262
8.9.2Effectsofallostericligandson response:changingefficacy 263
8.9.3Schildanalysisforallosteric antagonists 263
8.9.4ApplicationofLog(Max/R50) valuesfromR50 curvesto quantifytheeffectsofPAMs 264
8.9.5Quantifyingallosterically mediatedinducedbiasin agonism 264
8.9.6Functionalallostericmodelwith constitutivereceptoractivity 265 References 266
9. Theoptimaldesignof pharmacologicalexperiments
9.1Introduction 269
9.2Theoptimaldesignofpharmacological experiments 269
9.2.1Drugefficacy 270
9.2.2Affinity 283
9.2.3Orthostericversusallosteric mechanisms 292
9.3Nullexperimentsandfittingdatato models 293
9.4Interpretationofexperimentaldata 296
9.5Predictingtherapeuticactivityinall systems 299
9.5.1Predictingagonism
9.5.2Predictingbinding 301
9.5.3Drugcombinationsinvivo
9.7.1IC50 CorrectionFactors: competitiveantagonists 304
9.7.2RelationshipofpA2 andpKB for InsurmountableOrthosteric antagonism
9.7.3RelationshipofpA2 andpKB for InsurmountableAllosteric
10. Pharmacokinetics
10.1Introduction
11. Safetypharmacology
11.2.3Hepatotoxicityincontextin vivo 372
11.3Cytotoxicity 372 11.4Mutagenicity 374
11.5hERGactivityand Torsadesde Pointes 376
11.6Autonomicreceptorprofilingand off-targeteffects 376
11.7Generalpharmacology 377
11.8Clinicaltestinganddrugtoxicity 379
11.9Summaryandconclusions 381 References 381
12. Thedrug-discoveryprocess
12.1Somechallengesformoderndrug discovery 383
12.2Thedrug-discoveryprocess 384
12.3Target-baseddrugdiscovery 384
12.3.1Targetvalidationandthe useofchemicaltools 385
12.3.2Recombinantsystems 388
12.4Systems-baseddrugdiscovery 390
12.5High-throughputscreening 393
12.5.1Structure-baseddrugdesign andvirtualscreening 404
12.5.2Phenotypicscreening 405
12.6Theleadoptimizationprocess 409
12.7Drugeffectiveness 413
12.7.1Clinicaltesting 414
12.7.2Determiningdetailedprofiles ofcandidateefficacy 416
12.7.3Assaysincontext 417
12.7.4Characterizationofcandidate efficacies 418
12.8Summaryandconclusions 419 References 420 Furtherreading 422
13. Selectedpharmacologicalmethods
13.1Bindingexperiments 423
13.1.1Saturationbinding 423
13.1.2Displacementbinding 423
13.2Functionalassays 426
13.2.1Determinationofequiactive concentrationsonDose Responsecurves 426
13.2.2MethodofBarlow,Scott, andStephensonfor measurementoftheaffinity ofapartialagonist 427
13.2.3MethodofFurchgottforthe measurementoftheaffinity ofafullagonist 428
13.2.4Schildanalysisforthe measurementofcompetitive antagonistaffinity 429
13.2.5MethodofStephensonfor measurementofpartial agonistaffinity 431
13.2.6MethodofGaddumfor measurementofnoncompetitiveantagonistaffinity 433
13.2.7Methodforestimatingaffinityofinsurmountableantagonist(dextraldisplacement observed) 434
13.2.8Resultantanalysisfor measurementofaffinityof competitiveantagonists withmultipleproperties 436
13.2.9Measurementoftheaffinity andmaximalallosteric constantforallostericmodulatorsproducingsurmountableeffects 436
13.2.10Methodforestimating affinityofinsurmountable antagonist(nodextral displacementobserved): detectionofallostericeffect 438
13.2.11MeasurementofpKB for competitiveantagonists fromapIC50 441
13.2.12Statisticalassessmentof selectivity 442
13.2.13Measurementofsurmountableallostericantagonism 447
13.2.14Measurementof insurmountableallosteric antagonism(second method) 448
13.2.15MeasurementofPAM activity 450
Thispageintentionallyleftblank
Prefacetosixthedition
Pharmacologistsalmostalwaysareworkinginsystems theydonotfullyunderstand.Thishasengenderedaunique “nullsystem” ofcomparisons(beforeandafterdrug)that hassustainedthe field.Ourviewofwhatisactually happeninginourexperimentisobtainedthroughourassay, andastheNobelLaureateSirJamesBlackwrote “ The prismaticqualitiesoftheassaydistortourviewinobscure waysanddegrees. ” (1993;NobelLectures:Physiology andMedicine).Whatthismeanstothedisciplineisthatitis uniquelydependentupontechnologyunveilingwhatwedo notunderstandaboutphysiologyandastechnologyadvancesthefrontierofunderstanding,sotoodoesthe perceptionofpharmacologicalmechanismsandtheeffect ofdrugsonphysiology.Inessence,astheacuityofthe
pharmacologicalprismimproves,sotoodoesourunderstandingofdrugmechanisms.Thepracticaloutcomeofthis isthatabookonpharmacologymustbeupdatedeveryfew yearstokeepupwiththenewunderstandinggainedfrom technologies “neweyestosee.” Thisvolumehasbeen updatedandhasaddedmajorchaptersonbiologicsandthe drugdiscoveryprocessthatreflectsthechanginglandscape ofdrugtherapyaswellasviewsofhistorical findings modi fiedbynewknowledge.
TerryP.KenakinPh.D.
ProfessorofPharmacology,
TheUniversityofNorthCarolinaSchoolofMedicine, ChapelHill,NC,UnitedStates
Thispageintentionallyleftblank
Chapter1
Whatispharmacology?
1.2Whatispharmacology?
Iwouldinparticulardrawtheattentiontophysiologiststo thistypeofphysiologicalanalysisoforganicsystemswhich canbedonewiththeaidoftoxicagents .. ClaudeBernard(1813 78).
1.1Aboutthisbook
Essentiallythisisabookaboutthemethodsandtoolsusedin pharmacologytoquantifydrugactivity.Receptorpharmacologyisbasedonthecomparisonofexperimentaldataand simplemathematicalmodels,witharesultinginferenceof drugbehaviortothemolecularpropertiesofdrugs.Fromthis standpoint,acertainlevelofunderstandingofthemathematicsinvolvedinthemodelsisusefulbutnotimperative. Thisbookisstructuredsuchthateachchapterbeginswiththe basicconceptsandthenmovesontothetechniquesusedto estimatedrugparameters,and, finally,forthosesoinclined, themathematicalderivationsofthemodelsused.Understandingthederivationisnotaprerequisiteforunderstanding theapplicationofthemethodsortheresultingconclusion; theseareincludedforcompletenessandareforreaderswho wishtopursueexplorationofthemodels.Ingeneral,facility withmathematicalequationsisdefinitelynotrequiredfor pharmacology;thederivationscanbeignoredwithoutany detrimenttotheuseofthisbook.
Second,thesymbolsusedinthemodelsandderivations,onoccasion,duplicateeachother(i.e., a isan extremelypopularsymbol).However,theuseofthese multiplesymbolshasbeenretained,sincethispreservesthe contextofwherethesemodelswere firstdescribedand utilized.Also,changingthesetomakethemuniquewould causeconfusionifthesemethodsweretobeusedbeyond theframeworkofthisbook.Therefore,careshouldbetaken toconsidertheactualnomenclatureofeachchapter.
Third,anefforthasbeenmadetominimizetheneedto cross-referencedifferentpartsofthebook(i.e.,whena particularmodelisdescribed,thebasicsarereiterated somewhattominimizetheneedtoreadtherelevantbut differentpartofthebookinwhichthemodelisinitially described).Whilethisleadstoasmallamountofrepeated description,itisfeltthatthiswillallowforamoreuninterrupted flowofreadinganduseofthebook.
Pharmacology (anamalgamoftheGreek pharmakos, medicineordrug,and logos,study)isabroaddiscipline describingtheuseofchemicalstotreatandcurediseases. TheLatinterm pharmacologia wasusedinthelate1600s, buttheterm pharmacum wasusedasearlyasthe4th centurytodenotetheterm drug or medicine.IntheGreek translations “Pharmakeia ” referstoSorcery/Witchcraft whichnodoubtwasevidentwhenparticularherbaltreatmentswereeffective.Therearesubdisciplineswithin pharmacologyrepresentingspecialtyareas. Pharmacokinetics dealswiththedispositionofdrugsinthehuman body.Tobeuseful,drugsmustbeabsorbedandtransported totheirsiteoftherapeuticaction.Drugswillbeineffective intherapyiftheydonotreachtheorgans(s)toexerttheir activity;thiswillbediscussedspeci ficallyin Chapter9, Pharmacokinetics,ofthisbook. Pharmaceutics isthestudy ofthechemicalformulationofdrugstooptimizeabsorption anddistributionwithinthebody. Pharmacognosy isthe studyofplantnaturalproductsandtheiruseinthetreatmentofdisease.Averyimportantdisciplineinthedrugdiscoveryprocessis medicinalchemistry,thestudyofthe productionofmoleculesfortherapeuticuse.Thiscouples syntheticorganicchemistrywithanunderstandingofhow biologicalinformationcanbequantifi edandusedtoguide thesyntheticchemistrytoenhancetherapeuticactivity. Pharmacodynamics isthestudyoftheinteractionofthe drugmoleculewiththebiologicaltarget(referredto genericallyasthe “receptor,” videinfra).Thisdiscipline laysthefoundationofpharmacologysincealltherapeutic applicationofdrugshasacommonrootinpharmacodynamics(i.e.,asaprerequisitetoexertinganeffect,alldrug moleculesmustbindtoandinteractwithreceptors).
Thehistoryofpharmacologyistiedtothehistoryof drugdiscovery see Chapter9,TheOptimalDesignof PharmacologicalExperiments.AsputbytheCanadian physicianSirWilliamOsler(1849 919;the “fatherof modernmedicine”), “ thedesiretotakemedicineis perhapsthegreatestfeaturewhichdistinguishesmanfrom animals ” Pharmacologyasaseparatescienceis approximately120 140yearsold.Therelationshipbetweenchemicalstructureandbiologicalactivitybegantobe studiedsystematicallyinthe1860s[1].Itbeganwhen
physiologists,usingchemicalstoprobephysiologicalsystems,becamemoreinterestedinthechemicalprobesthan thesystemstheywereprobing.Bytheearly1800s,physiologistswereperformingphysiologicalstudieswith chemicalsthatbecamepharmacologicalstudiesmoreaimed atthedefi nitionofthebiologicalactivityofchemicals.The firstformalizedchairofpharmacology,indicatingaformal universitydepartment,wasfoundedinEstoniabyRudolf Bucchiemin1847.InNorthAmerica,the firstchairwas foundedbyJohnJacobAbelatJohnsHopkinsUniversity in1890.Adifferentiationofphysiologyandpharmacology wasgivenbythepharmacologistSirWilliamPaton[2]:
Ifphysiologyisconcernedwiththefunction,anatomywith thestructure,andbiochemistrywiththechemistryofthe livingbody,thenpharmacologyisconcernedwiththe changesinfunction,structure,andchemicalpropertiesof thebodybroughtaboutbychemicalsubstances
W.D.M.Paton(1986).
Manyworksaboutpharmacologyessentiallydealin therapeuticsassociatedwithdifferentorgansystemsinthe body.Thus,inmanypharmacologytexts,chaptersare entitleddrugsinthecardiovascularsystem,theeffectof drugsonthegastrointestinal(GI)system,thecentralnervoussystem(CNS),andsoon.However,theunderlying principlesforalloftheseisthesame,namely,thepharmacodynamicinteractionbetweenthedrugandthebiologicalrecognitionsystemforthatdrug.Therefore,a prerequisitetoallofpharmacologyisanunderstandingof thebasicconceptsofdose responseandhowlivingcells processpharmacologicalinformation.Thisgenerallyis giventheterm pharmacodynamics or receptorpharmacology,where receptor isatermreferringtoanybiological recognitionunitfordrugs(membranereceptors,enzymes, DNA,andsoon).Withsuchknowledgeinhand,readers willbeabletoapplytheseprinciplestoanybranchof therapeuticseffectively.Thisbooktreatsdose responsedata genericallyanddemonstratesmethodsbywhichdrugactivitycanbequantifiedacrossallbiologicalsystemsirrespectiveofthenatureofthebiologicaltarget.
Agreatstrengthofpharmacologyasadisciplineisthat itcontainsthetoolsandmethodstoconvert “descriptive data,” i.e.,datathatservetocharacterizetheactivityofa givendruginaparticularsystem,to “predictivedata.” This latterinformationcanbeusedtopredictthatdrug’sactivity inallorgansystems,includingthetherapeuticone.This definesthedrug-discoveryprocesswhichisthetestingof newpotentialdrugmoleculesinsurrogatesystems(wherea potentiallytoxicchemicalcandonolastingharm)before progressiontothenextstep,namely,testinginhuman therapeuticsystems.Themodelsandtoolscontainedin pharmacologytoconvertdrugbehaviorsinparticular
organstomolecularproperties(see Chapter2:How DifferentTissuesProcessDrugResponse)arethemain subjectofthisbook,andthestep-by-stepdesignofpharmacologicexperimentstodothisaredescribedindetailin Chapter8,TheOptimalDesignofPharmacologicalExperiments(afterthemeaningoftheparticularparameters andtermsisdescribedinpreviouschapters).
Thehuman genome isnowwidelyavailablefordrugdiscoveryresearch.Farfrombeingasimpleblueprintof howdrugsshouldbetargeted,ithasshownbiologiststhat receptor genotypes (i.e.,propertiesofproteinsresulting fromgenetictranscriptiontotheiraminoacidsequence)are secondarytoreceptor phenotypes (howtheproteininteracts withthemyriadofcellularcomponentsandhowcellstailor themakeupandfunctionsoftheseproteinstotheirindividualneeds).Sincethearrivalofthehumangenome,receptorpharmacologyasascienceismorerelevantthanever indrugdiscovery.Currentdrugtherapyisbasedonless than500moleculartargets,yetestimatesutilizingthe numberofgenesinvolvedinmultifactorialdiseasessuggest thatthenumberofpotentialdrugtargetsrangesfrom2000 to5000[3].Thus,currenttherapyisusingonly5% 10% ofthepotentialtroveoftargetsavailableinthehuman genome.
Ameaningfuldialogbetweenchemistsandpharmacologistsisthesinglemostimportantelementofthedrugdiscoveryprocess.Thenecessarylinkbetweenmedicinal chemistryandpharmacologyhasbeenelucidatedby Paton[2]:
Forpharmacologythereresultsaparticularlycloserelationshipwithchemistry,andtheworkmayleadquite naturally,withnospecialstressonpracticality,totherapeuticapplication,or(inthecaseofadversereactions)to toxicology.
W.D.M.Paton(1986).
Chemistsandbiologistsresideindifferentworldsfrom thestandpointofthetypeofdatatheydealwith.Chemistry isanexactsciencewithphysicalscalesthatarenotsubject tosystemvariance.Thus,thescalesofmeasurementare transferable.Biologydealswiththevagariesofcomplex systemsthatarenotcompletelyunderstood.Withinthis scenario,scalesofmeasurementaremuchlessconstantand muchmoresubjecttosystemconditions.Giventhis,agap canexistbetweenchemistsandbiologistsintermsofunderstandingandalsointermsofthebestmethodtoprogress forward.Intheworstcircumstance,itisagapofcredibility emanatingfromafailureofthebiologisttomakethe chemistunderstandthelimitsofthedata.Usually,however, credibilityisnottheissue,andthegapexistsduetoalack ofcommonexperience.Thisbookwaswritteninan attempttolimitor,hopefully,eliminatethisgap.
1.3Thereceptorconcept
Oneofthemostimportantconceptsemergingfromearly pharmacologicalstudiesistheconceptofthe receptor Pharmacologistsknewthatminuteamountsofcertain chemicalshadprofoundeffectsonphysiologicalsystems. Theyalsoknewthatverysmallchangesinthechemical compositionofthesesubstancescouldleadtohugedifferencesinactivity.Thisledtothenotionthatsomething onorinthecellmustspeci ficallyreadthechemicalinformationcontainedinthesesubstancesandtranslateitintoa physiologicaleffect.Thissomethingwasconceptually referredtoasthe “receptor” forthatsubstance.Pioneers suchasPaulEhrlich(1854 915, Fig.1.1A)proposedthe existenceof “chemoreceptors” (actuallyheproposeda collectionofamboreceptors,triceptors,andpolyceptors)on cellsfordyes.Healsopostulatedthatthechemoreceptors onparasites,cancercells,andmicroorganismswere differentfromhealthyhostandthuscouldbeexploited therapeutically.Thephysiologistturnedpharmacologist JohnNewportLangley(1852 926, Fig.1.1B),duringhis studieswiththedrugsjaborandi(whichcontainsthealkaloidpilocarpine)andatropine,introducedtheconceptthat receptorswereswitchesthatreceivedandgeneratedsignals andthattheseswitchescouldbeactivatedorblockedby specificmolecules.Theoriginatorofquantitativereceptor theory,theEdinburghpharmacologistAlfredJosephClark (1885 941, Fig.1.1C),wasthe fi rsttosuggestthatthe data,compiledfromhisstudiesoftheinteractionsof acetylcholineandatropine,resultedfromtheunimolecular
interactionofthedrugandasubstanceonthecellsurface. Hearticulatedtheseideasintheclassicwork TheModeof ActionofDrugsonCells [4],laterrevisedasthe Handbook ofExperimentalPharmacology [5].AsputbyClark
Itappearstothewriterthatthemostimportantfactshown byastudyofdrugantagonismsisthatitisimpossibleto explaintheremarkableeffectsobservedexceptbyassuming thatdrugsunitewithreceptorsofahighlyspecificpattern .Nootherexplanationwill,however,explainatitheof thefactsobserved.
A.J.Clark(1937).
Clark’snextstepformedthebasisofreceptortheoryby applyingchemicallawstosystemsof “infi nitelygreater complexity” [4].Itisinterestingtonotethescienti ficatmosphereinwhichClarkpublishedtheseideas.The dominantideasbetween1895and1930werebasedon theoriessuchasthelawofphasicvariationessentially statingthat “certainphenomenaoccurfrequently.” HomeopathictheoriesliketheArndt Schulzlawand Weber Fechnerlawwerebasedonlooseideasaround surfacetensionofthecellmembrane,buttherewaslittle physicochemicalbasisfortheseideas[6].Inthisvein, prominentpharmacologistsoftheday,suchasWalter Straub(1874 944),suggestedthatageneraltheoryof chemicalbindingbetweendrugsandcellsutilizingreceptorswas “ . goingtoofar . and . notadmissible” [6].TheimpactofClark’sthinkingagainsttheseconcepts cannotbeoveremphasizedtomodernpharmacology.

FIGURE1.1 Pioneersofpharmacology.(A)PaulEhrlich(1854 915).BorninSilesia,EhrlichgraduatedfromLeipzigUniversitytogoontoa distinguishedcareerasheadofinstitutesinBerlinandFrankfurt.Hisstudieswithdyesandbacteriaformedthebasisofearlyideasregardingrecognition ofbiologicalsubstancesbychemicals.(B)JohnNewportLangley(1852 926).ThoughhebeganreadingmathematicsandhistoryinCambridgein1871, Langleysoontooktophysiology.HesucceededthegreatphysiologistM.FostertothechairofphysiologyinCambridgein1903andbranchedoutinto pharmacologicalstudiesoftheautonomicnervoussystem.Thesepursuitsledtogerminaltheoriesofreceptors.(C)AlfredJ.Clark(1885 941).Beginning asademonstratorinpharmacologyinKing’sCollege(London),ClarkwentontobecomeProfessorofpharmacologyatUniversityCollegeLondon.From therehetookthechairofpharmacologyinEdinburgh.Knownastheoriginatorofmodernreceptortheory,Clarkappliedchemicallawstobiological phenomena.Hisbooksonreceptortheoryformedthebasisofmodernpharmacology.
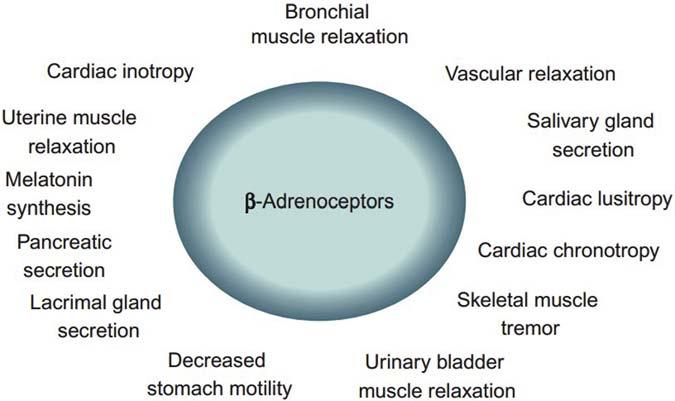
Itispossibletounderestimatetheenormoussigni ficanceofthereceptorconceptinpharmacologyuntilitis realizedhowrelativelychaoticthestudyofdrugeffect wasbeforeitwasintroduced.Specifi cally,considerthe myriadofphysiologicalandpharmacologicaleffectsof thehormoneepinephrineinthebody.Asshownin Fig.1.2 ,ahostofresponsesareobtainedfromtheCNS, cardiovascularsystem,smoothmuscle,andotherorgans. Itisimpossibletoseeathreadwhichrelatesthesevery differentresponsesuntilitisrealizedthatalloftheseare mediatedbytheactivationofasingleproteinreceptor, namely,inthiscase,the b -adrenoceptor.Whenthisis understood,amuchbetterideacanbegainedastohowto manipulatetheseheterogeneousresponsesfortherapeutic bene fi t;thereceptorconceptintroducedorderintophysiologyandpharmacology.
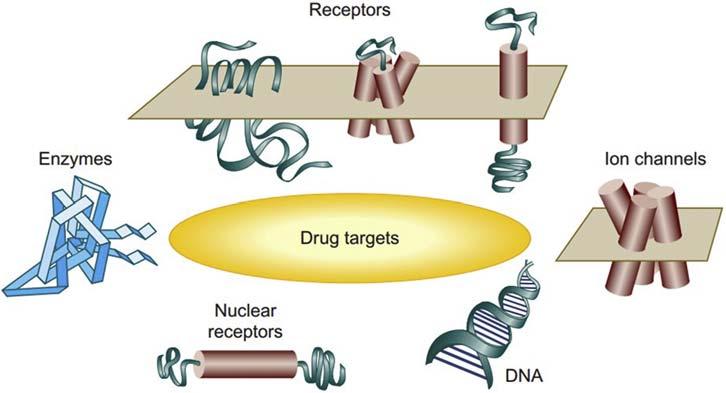
Drugreceptorscanexistinmanyforms,includingcell surfaceproteins,enzymes,ionchannels,membranetransporters,DNA,andcytosolicproteins(see Fig.1.3).There areexamplesofimportantdrugsforallofthese.Thisbook dealswithgeneralconceptswhichcanbeappliedtoarange ofreceptortypes,butmostoftheprinciplesareillustrated withthemosttractablereceptorclassknowninthehuman genome,namely, seventransmembrane(7TM)receptors (7TMRs) .Thesereceptorsarenamedfortheircharacteristic structurethatconsistsofasingleproteinchainthattraversesthecellmembraneseventimestoproduceextracellularandintracellularloops.Thesereceptorsactivate G-proteinstoelicitresponse,thustheyarealso commonlyreferredtoas G-protein-coupledreceptors (GPCRs);thisshouldnowbeconsideredalimitingmoniker astheseproteinssignaltoawidevarietyofsignaling moleculesinthecellandarenotconfinedtoG-protein
effects.Therearebetween800and1000[7]ofthesein thegenome[thegenomesequencepredicts650GPCR genes,ofwhichapproximately190(ontheorderof1%of thegenomeofsuperiororganisms)arecategorizedas known7TMRs[8]activatedbysome70ligands].Inthe UnitedStates,in2000,nearlyhalfofallprescriptiondrugs weretargetedtoward7TMreceptors[3].Thesereceptors, comprisingbetween1%and5%ofthetotalcellprotein, controlamyriadofphysiologicalactivities.Theyare tractablefordrugdiscoverybecausetheyareonthecell surface,andthereforedrugsdonotneedtopenetratethe celltoproduceeffect.Inthestudyofbiologicaltargetssuch as7TMRsandotherreceptors,a “system” mustbe employedthatacceptschemicalinputandreturnsbiological output.Itisworthdiscussingsuchreceptorsystemsin generaltermsbeforetheirspecifi cusesareconsidered.
1.4Pharmacologicaltestsystems
Molecularbiologyhastransformedpharmacologyandthe drug-discoveryprocess.Aslittleas20yearsago,screening fornewdrugentitieswascarriedoutinsurrogateanimal tissues.Thisnecessitatedaratherlargeextrapolationto spanthedifferencesingenotypeandphenotype.Thebelief thatthegapcouldbebridgedcamefromthenotionthatthe chemicalsrecognizedbythesereceptorsinbothhumans andanimalswerethesame(videinfra).Receptorsare uniqueproteinswithcharacteristicaminoacidsequences. While polymorphisms (spontaneousalterationsinamino acidsequence,videinfra)ofreceptorsexistinthesame species,ingeneraltheaminoacidsequenceofanatural ligand-bindingdomainforagivenreceptortypelargely maybeconserved.Thereareobviouspitfallsofusing
FIGURE1.2 Asamplingoftheheterogeneousphysiologicalandpharmacologicalresponsetothehormoneepinephrine.Theconceptofreceptorslinks thesediverseeffectstoasinglecontrolpoint,namely,the b-adrenoceptor.
FIGURE1.3 Schematicdiagramofpotentialdrugtargets.Moleculescanaffectthefunctionofnumerouscellularcomponentsbothinthecytosolandon themembranesurface.Therearemanyfamiliesofreceptorsthattraversethecellularmembraneandallowchemicalstocommunicatewiththeinteriorof thecell.
surrogatespeciesreceptorsforpredictinghumandrugactivity,anditnevercanbeknownforcertainwhether agreementforestimatesofactivityforagivensetofdrugs ensuresaccuratepredictionforalldrugs.Theagreementis verymuchdrugandreceptordependent.Forexample,the humanandmouse a2-adrenoceptorsare89%homologous andthusconsideredverysimilarfromthestandpointof aminoacidsequence.Furthermore,theaffinitiesofthe a2adrenoceptorantagonistsatipamezoleandyohimbineare nearlyindistinguishable(atipamezolehuman a2-C10 Ki ¼ 2.9 0.4nM,mouse a2-4HKi ¼ 1.6 0.2nM; yohimbinehuman a2-C10Ki ¼ 3.4 0.1nM,mouse a24HKi ¼ 3.8 0.8nM).However,thereisa20.9-fold differencefortheantagonistprazosin(human a2-C10 Ki ¼ 2034 350nM,mouse a2-4HKi ¼ 97.3 0.7nM) [9].Suchdatahighlightageneralthemeinpharmacological research,namely,thatahypothesis,suchasoneproposing thattworeceptorswhichareidenticalwithrespecttotheir sensitivitytodrugsarethesame,cannotbeproven,only disproven.Whileaconsiderablenumberofdrugscouldbe testedonthetworeceptors(thussupportingthehypothesis thattheirsensitivitytoalldrugsisthesame),thishypothesisisimmediatelydisprovenbythe firstdrugthatshows differentialpotencyonthetworeceptors.Thefactthata seriesofdrugstestedshowidenticalpotenciesmaymean onlythatthewrongsampleofdrugshasbeenchosento unveilthedifference.Thus,nogeneralstatementscanbe madethatanyonesurrogatesystemiscompletelypredictiveofactivityonthetargethumanreceptor.Thiswillalwaysbeadrug-speci ficphenomenon.
Thelinkbetweenanimalandhumanreceptorsisthefact thatbothproteinsrecognizetheendogenoustransmitter (e.g.,acetylcholine,norepinephrine),andthereforethehope
isthatthislinkwillcarryoverintootherdrugsthat recognizetheanimalreceptor.Thisimperfectsystem formedthebasisofdrugdiscoveryuntilhuman cDNA for humanreceptorscouldbeusedtomakecellsexpresshumanreceptors.Theseengineered(recombinant)systemsare nowusedassurrogatehuman-receptorsystems,andthe leapoffaithfromanimalreceptorsequencestohumanreceptorsequencesisnotrequired(i.e.,theproblemof differencesingenotypehasbeenovercome).However, cellularsignalingisanextremelycomplexprocessandcells tailortheirreceiptofchemicalsignalsinnumerousways. Therefore,thewayagivenreceptorgenebehavesina particularcellcandifferinresponsetothesurroundingsin whichthatreceptor findsitself.Thesedifferencesin phenotype(i.e.,propertiesofareceptorproducedby interactionwithitsenvironment)canresultindifferencesin boththequantityandqualityofasignalproducedbya concentrationofagivendrugindifferentcells.Therefore, thereisstillacertain,althoughsomewhatlesser,leapof faithtakeninpredictingtherapeuticeffectsinhumantissuesunderpathologicalcontrolfromsurrogaterecombinant orevensurrogatenaturalhuman-receptorsystems.Forthis reason,itisaprimaryrequisiteofpharmacologytoderive system-independentestimatesofdrugactivitythatcanbe usedtopredicttherapeuticeffectinothersystems.
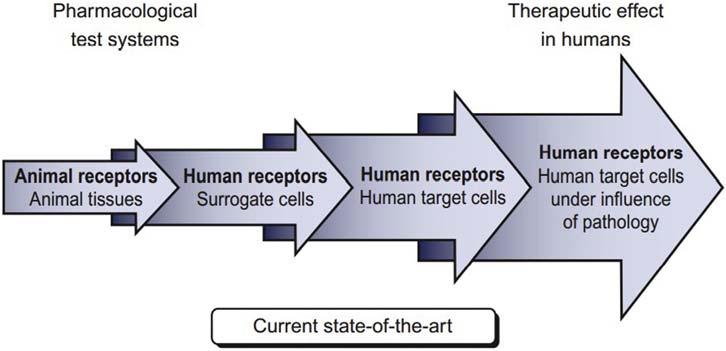
Aschematicdiagramofthevarioussystemsusedin drugdiscovery,inorderofhowappropriatetheyareto therapeuticdrugtreatment,isshownin Fig.1.4.Asdiscussedpreviously,earlyfunctionalexperimentsinanimal tissuehavenowlargelygivenwaytotestinginrecombinant cellsystemsengineeredwithhuman-receptormaterial.This hugetechnologicalstepgreatlyimprovedthepredictability ofdrugactivityinhumans,butitshouldbenotedthatthere
FIGURE1.4 Ahistoryofthedrug-discoveryprocess.Originally,theonlybiologicalmaterialavailablefordrugresearchwasanimaltissue.Withthe adventofmolecularbiologicaltechniquestocloneandexpresshumanreceptorsincells,recombinantsystemssupplantedanimal-isolatedtissuework.It shouldbenotedthattheserecombinantsystemsstillfallshortofyieldingdrugresponseinthetargethumantissueundertheinfluenceofpathological processes.
stillaremanyfactorsthatintervenebetweenthegenetically engineereddrug-testingsystemandthepathologyofhuman disease.
Afrequentlyusedstrategyindrugdiscoveryistoexpresshumanreceptors(through transfection withhuman cDNA)inconvenientsurrogatehostcells(referredtoas “target-based” drugdiscovery;seeChapter10:Safety Pharmacologyforfurtherdiscussion).Thesehostcellsare chosenmainlyfortheirtechnicalproperties(i.e.,robustness,growthrate,stability)andnotwithanyknowledgeof verisimilitudetothetherapeuticallytargetedhumancell type.Therearevariousfactorsrelevanttothechoiceof surrogatehostcell,suchasaverylow-backgroundactivity (i.e.,acellcannotbeusedthatalreadycontainsarelated animalreceptorforfearofcross-reactivitytomolecules targetedforthehumanreceptor).Humanreceptorsareoften expressedinanimalsurrogatecells.Themainideahereis thatthecellisareceptacleforthereceptor,allowingitto producephysiologicalresponses,andthatactivitycanbe monitoredinpharmacologicalexperiments.Inthissense, humanreceptorsexpressedinanimalcellsarestillatheoreticalstepdistancedfromthehumanreceptorinahuman celltype.However,evenifahumansurrogateisused(and therearesuchcellsavailable),thereisnodefinitiveevidencethatasurrogatehumancellisanymorepredictiveof anaturalreceptoractivitythanananimalcellwhen comparedtothecomplexreceptorbehaviorinitsnatural hostcelltypeexpressedunderpathologicalconditions. Receptorphenotypedominatesintheendorgan,andthe exactdifferencesbetweenthegenotypicbehaviorofthe receptor(resultingfromthegeneticmakeupofthereceptor) andthephenotypicbehaviorofthereceptor(duetothe interactionofthegeneticproductwiththerestofthecell) maybecellspeci fic.Therefore,thereisstillapossiblegap
betweenthesurrogatesystemsusedinthedrug-discovery processandthetherapeuticapplication.Moreover,most drug-discoverysystemsutilizereceptorsasswitching mechanismsandquantifywhetherdrugsturnonorturnoff theswitch.Thepathologicalprocessesthatwestriveto modifymaybemoresubtle.AsputbypharmacologistSir JamesBlack[10]:
angiogenesis,apoptosis,inflammation,commitmentof marrowstemcells,andimmuneresponses.Thecellular reactionssubsumedintheseprocessesareswitchlikein theirbehavior biochemicallywearelearningthatinall theseprocessesmanychemicalregulatorsseemtobe involved.Fromtheliteratureonsynergisticinteractions,a controlmodelcanbebuiltinwhichnosingleagentis effective.Ifanumberofchemicalmessengerseachbring informationfromadifferentsourceandeachdeliveronlya subthresholdstimulusbuttogethermutuallypotentiateeach other,thenthedesiredinformation-richswitchingcanbe achievedwithminimumriskofmiscuing.
J.W.Black(1986).
Suchcomplexendpointsaredif ficulttopredictfrom anyoneofthecomponentprocessesleadingtoyetanother leapoffaithinthedrug-discoveryprocess.Forthesereasons,anemergingstrategyfordrugdiscoveryistheuseof naturalcellularsystems.Thisapproachisdiscussedinsome detailinChapter11,TheDrugDiscoveryProcess. Evenwhenanactivedrugmoleculeisfoundandactivityisveri fiedinthetherapeuticarena,therearefactors thatcanleadtogapsinitstherapeuticprofile.Whendrugs areexposedtohugepopulations,geneticvariationsinthis populationcanleadtodiscoveryof alleles thatcodefor mutationsofthetarget(isogenes),andthesecanleadto variationindrugresponse.Suchpolymorphismscanleadto
resistantpopulations(i.e.,resistanceofsomeasthmaticsto the b-adrenoceptorbronchodilators[11]).Intheabsenceof geneticknowledge,thesetherapeuticfailuresforadrug couldnoteasilybeavertedsincetheyinessenceoccurred becauseofthepresenceofnewbiologicaltargetsnot originallyconsideredinthedrug-discoveryprocess.However,asnewepidemiologicalinformationbecomesavailable,thesepolymorphismscannowbeincorporatedinto thedrug-discoveryprocess.
Therearetwotheoreticalandpracticalscalesthatcan beusedtomakesystem-independentmeasuresofdrug activityonbiologicalsystems.The fi rstisameasureofthe attractionofadrugforabiologicaltarget,namely,its af fi nity forareceptor.Drugsmustinteractwithreceptors toproduceaneffect,andtheaf fi nityisachemicalterm usedtoquantifythestrengthofthatinteraction.Thesecondismuchlessstraightforwardandisusedtoquantify thedegreeofeffectimpartedtothebiologicalsystemafter thedrugbindstothereceptor.Thisistermed ef fi cacy .This propertywasnamedbyStephenson[ 12 ]withinclassical receptortheoryasaproportionalityfactorforthetissue responseproducedbyadrug.Thereisnoabsolutescale foref fi cacy,butratheritisdealtwithinrelativeterms (i.e.,theratiooftheef fi cacyoftwodifferentdrugsona particularbiologicalsystemcanbeestimatedand,under idealcircumstances,willtranscendthesystemandbe applicabletoothersystemsaswell).Itistheforemosttask ofpharmacologytousethetranslationsofdrugeffect obtainedfromcellstoprovidesystem-independentestimatesofaf fi nityandef fi cacy.Beforespeci fi cdiscussion ofaf fi nityandef fi cacy,itisworthconsideringthemolecularnatureofbiologicaltargets.
1.5Thenatureofdrugreceptors
WhilesomebiologicaltargetssuchasDNAarenotprotein innature,mostreceptorsare.Itisusefultoconsiderthe propertiesofreceptorproteinstoprovideacontextforthe interactionofsmallmoleculedrugswiththem.Animportantpropertyofreceptorsisthattheyhavea3Dstructure. Proteinsareusuallycomposedofoneormorepeptide chains;thecompositionofthesechainsmakesuptheprimaryandsecondarystructureoftheprotein.Proteinsalso aredescribedintermsofatertiarystructure,whichdefines theirshapein3Dspace,andaquaternarystructure,which definesthemolecularinteractionsbetweenthevarious componentsoftheproteinchains(Fig.1.5).Itisthis3D structurewhichallowstheproteintofunctionasarecognitionsiteandeffectorfordrugsandothercomponentsof thecell;inessence,theabilityoftheproteintofunctionasa messenger,shuttlinginformationfromtheoutsideworldto thecytosolofthecell.For7TMRs,the3Dnatureofthe receptorformsbindingdomainsforotherproteinssuchas
G-proteins(theseareactivatedbythereceptorandthengo ontoactivateenzymesandionchannelswithinthecell;see Chapter2:HowDifferentTissuesProcessDrugResponse) andendogenouschemicalssuchasneurotransmitters,hormones,andautacoidsthatcarryphysiologicalmessages. Thisimportantclassofdrugtargetisnamedforacharacteristicstructureconsistingof7TMdomainsloopinginto theextracellularandintracellularspace see Fig.1.6 Thesemoleculesarethemaintransferpointsofinformation fromtheoutsidetotheinsideofthecell,andsuchtransfers occurthroughchangesintheconformationofthereceptor protein(videinfra).Forotherreceptors,suchasionchannelsandsingletransmembraneenzymereceptors,the conformationalchangeperseleadstoaresponse,either throughanopeningofachanneltoallowthe flowofionic currentortheinitiationofenzymaticactivity.Therapeutic advantagecanbetakenbydesigningsmallmoleculesto utilizethesebindingdomainsorother3Dbindingdomains onthereceptorproteininordertomodifyphysiologicaland pathologicalprocesses.
1.6Fromthesnapshottothemovie
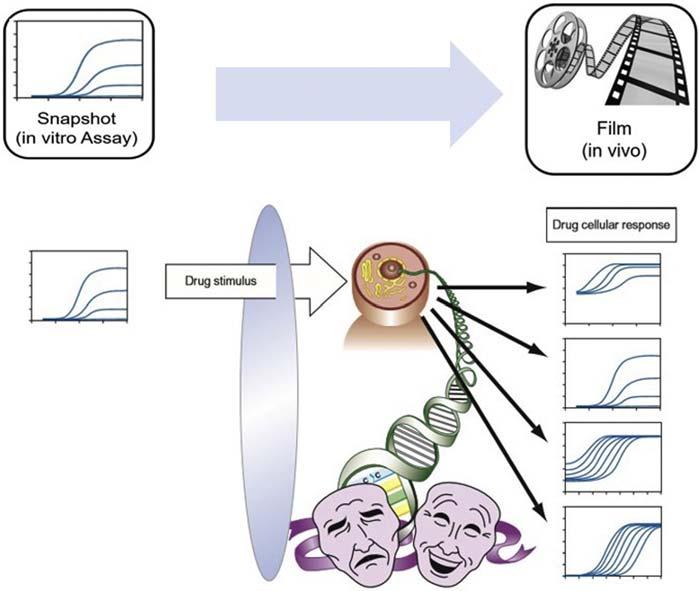
Drugsinteractwithlivingphysiologyandtheoutcomeof theinteractioniscontrolledbyacombinationofthe intrinsicpropertiesofthedrugandthesensitivityofthe systemtointervention.Thisbeingthecase,drugscanhave differentprofilesofactivityindifferenttissuesdepending onthetissuesensitivityandsetpointofphysiology. Throughthemechanicsofmathematicalmodelsofdrug activityandthesystem-independentscalesofdrugactivity (i.e.,affinity,efficacy),pharmacologicalproceduresare uniquelyabletoconvertasingleobservationofdrugactivityinatestsystem(the ‘snapshot’)toapredictionofthe completerealmofactivitiesforthatsamedruginarangeof tissuesofvaryingsetpointsofphysiology(the ‘movie’). Thisisanessentialpropertyofpharmacologyindrugdiscoveryasallinitialevaluationsofnewdrugactivityare madeinisolatedsystemsandassessmentsofwhatthenew moleculewilldoinothersystemsmustbemade.In essence,thecellularhostsystemcompletelycontrolswhat theexperimenterobservesregardingtheeventstakingplace atthedrugreceptor.Drugactivityisthusrevealedthrough a “cellularveil” thatcan,inmanycases,obscureorsubstantiallymodifydrug receptoractivity(Fig.1.7).Minute signals,initiatedeitheratthecellsurfaceorwithinthe cytoplasmofthecell,areinterpreted,transformed,amplifi ed,andotherwisealteredbythecelltotailorthatsignalto itsownparticularneeds.Theapplicationofpharmacologicalprinciplesandmodelingenable ‘snapshots’ ofdrug activityobtainedisexperimentstoguidetheprogressof moleculestowarddrugcandidatestatus see Chapter3 for furtherdetails.
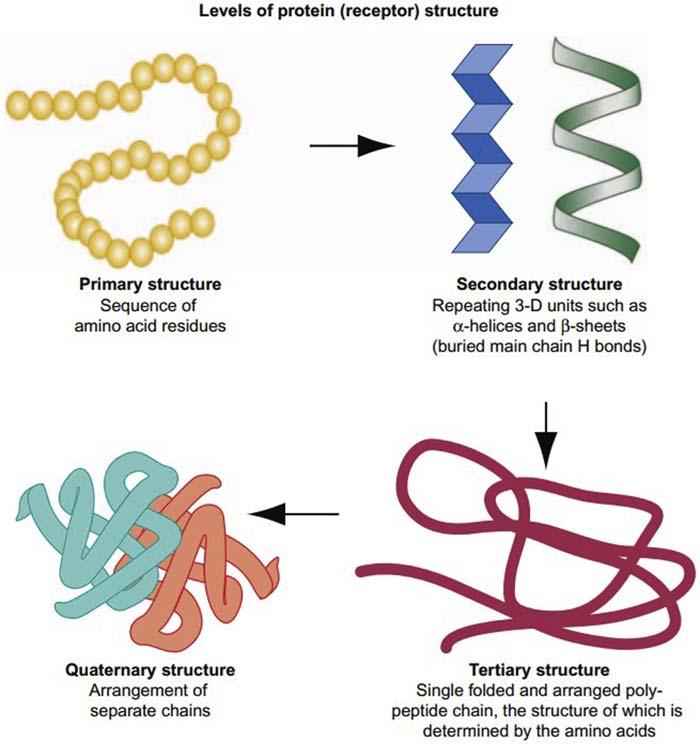
FIGURE1.5 Increasinglevelsofproteinstructure.Aproteinhasagivenaminoacidsequencetomakepeptidechains.Theseadopta3Dstructure accordingtothefreeenergyofthesystem.Receptorfunctioncanchangewithchangesintertiaryorquaternarystructure.
1.7Pharmacologicalinterventionand thetherapeuticlandscape
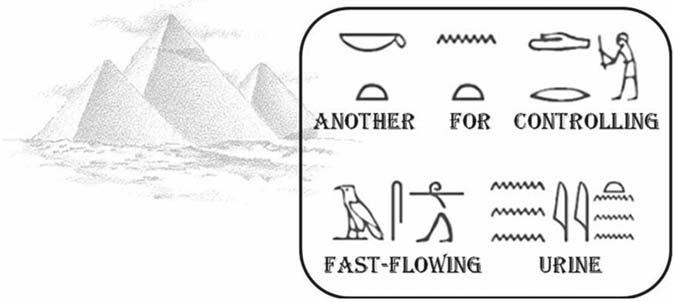
Itisusefultoconsiderthetherapeuticlandscapewith respecttotheaimsofpharmacology.AsstatedbySir WilliamOssler(1849 919) “ theprimedistinctionbetweenmanandothercreaturesisman’syearningtotake medicine. ” Thenotionthatdrugscanbeusedtocurediseaseisasoldashistory.Oneofthe firstwrittenrecordsof actual “prescriptions” canbefoundinthe EbersPapyrus (c.1550BCE): “ . fornightblindnessintheeyes . liver ofox,roastedandcrushedout reallyexcellent! “ see Fig.1.8.Nowitisknownthatliverisanexcellentsourceof vitaminA,aprimetreatmentfornightblindness,butthat chemicaldetailwasnotknowntotheancientEgyptians. Diseasecanbeconsideredundertwobroadcategories: thosecausedbyinvaderssuchaspathogensandthose causedbyintrinsicbreakdownofnormalphysiological function.The firstgenerallyisapproachedthroughthe invader(i.e.,thepathogenisdestroyed,neutralized,or removedfromthebody).Theoneexceptionofwherethe hostistreatedwhenaninvaderispresentisthetreatmentof HIV-1infectionleadingtoAIDS.Inthiscase,whilethere aretreatmentstoneutralizethepathogen,suchasantiretroviralstoblockviralreplication,amajornewapproach istheblockadeoftheinteractionoftheviruswiththe proteinthatmediatesviralentryintohealthycells,the chemokinereceptorCCR5.Inthiscase,CCR5antagonists areusedtopreventHIVfusionandsubsequentinfection. Thesecondapproachtodiseaserequiresanunderstanding ofthepathologicalprocessandrepairofthedamageto returntonormalfunction.
Thetherapeuticlandscapeontowhichdrugdiscovery andpharmacologyingeneralcombatdiseasecangenerallybedescribedintermsofthemajororgansystemsof thebodyandhowtheymaygoawry.Ahealthycardiovascularsystemconsistsof aheartabletopumpdeoxygenatedbloodthroughthelungsandtopumpoxygenated bloodthroughoutacirculatorysystemthatdoesnot undulyresistblood fl ow.Sincetheheartrequiresahigh
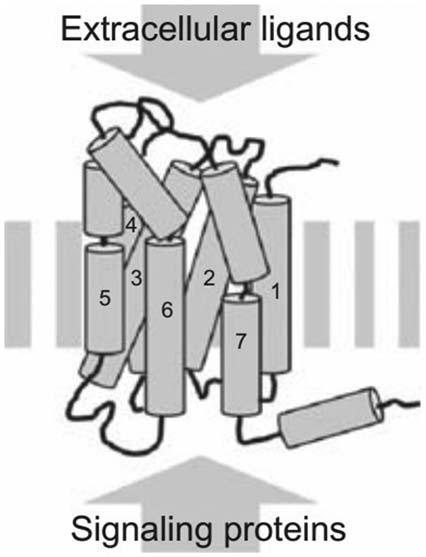
FIGURE1.6 Depictionofthestructureofseventransmembranedomain receptors,oneofthemostifnotthemostimportanttherapeutictargets availableinthehumangenome.Chemicalsaccessthereceptorthroughthe extracellularspacebybindingtotheextracellulardomainsoftheprotein. Thiscausesaconformationalchangeintheproteinthatalterstheinteractionofsignalingproteinsinthecellcytosol.Thislatterprocessresultsin theinitiationofcellularsignaling.
degreeofoxygenitselftofunction,myocardialischemia canbedevastatingtoitsfunction.Similarly,aninabilityto maintainrhythm(arrhythmia)orlossinstrengthwith concomitantinabilitytoempty(congestiveheartfailure) canbefatal.Thelatterdiseaseisexacerbatedbyelevated arterialresistance(hypertension).Awiderangeofdrugs areusedtotreatthecardiovascularsystem,including coronaryvasodilators(nitrates),diuretics,renin angiotensininhibitors,vasodi lators,cardiacglycosides, calciumantagonists,betaandalphablockers,antiarrhythmics,anddrugsfordyslipidemia.Thelungsmust extractoxygenfromtheair,deliverittotheblood,and releasecarbondioxidefromthebloodintoexhaledair. Asthma,chronicobstructivepulmonarydisease(COPD), andemphysemaareseriousdisordersofthelungsand airways.Bronchodilators(betaagonists),antiinfl ammatorydrugs,inhaledglucocorticoids,anticholinergics,andtheophyllineanalogsareusedfortreatmentof thesediseases.TheCNScontrolsallconsciousthought andmanyunconsciousbodyfunctions.Numerousdiseasesofthebraincanoccur,includingdepression,anxiety,epilepsy,mania,degeneration,obsessivedisorders, andschizophrenia.Brainfunctionssuchasthose
controllingsedationandpainalsomayrequiretreatment. AwiderangeofdrugsisusedforCNSdisorders, includingserotoninpartiala gonistsanduptakeinhibitors, dopamineagonists,benzodiazepines,barbiturates,opioids,tricyclics,neuroleptics,andhydantoins.TheGItract receivesandprocessesfoodtoextractnutrientsand removeswastefromthebody.Diseasessuchasstomach ulcers,colitis,diarrhea,nausea,andirritablebowelsyndromecanaffectthissystem.Histamineantagonists, protonpumpblockers,opioi dagonists,antacids,andserotoninuptakeblockersareusedtotreatdiseasesoftheGI tract.
Theinflammatorysystemisdesignedtorecognizeself fromnonself,andtodestroynonselftoprotectthebody.In diseasesoftheinflammatorysystem,theself-recognition canbreakdown,leadingtoconditionsinwhichthebody destroyshealthytissueinamisguidedattemptatprotection. Thiscanleadtorheumatoidarthritis,allergies,pain,COPD, asthma,fever,gout,graftrejection,andproblemswith chemotherapy.Nonsteroidalantiin flammatorydrugs, aspirinandsalicylates,leukotrieneantagonists,andhistaminereceptorantagonistsareusedtotreatinflammatory disorders.Theendocrinesystemproducesandsecretes hormonescrucialtothebodyforgrowthandfunction. Diseasesofthisclassoforganscanleadtogrowthand pituitarydefects diabetes;abnormalityinthyroid,pituitary,adrenalcortex,andandrogenfunction;osteoporosis; andalterationsinestrogen progesteronebalance.The generalapproachtotreatmentisthroughreplacementor augmentationofsecretion.Drugsusedarereplacement hormones,insulin,sulfonylureas,adrenocorticalsteroids, andoxytocin.Inadditiontothemajororganandphysiologicalsystems,diseasesinvolvingneurotransmissionand neuromuscularfunction,ophthalmology,hemopoiesisand hematology,dermatology,immunosuppression,anddrug addictionandabuseareamenabletopharmacological intervention.
Cancerisaseriousmalfunctionofnormalcellgrowth. Intheyearsfrom1950to1970,themajorapproachto treatingthisdiseasewastotargetDNAandDNAprecursorsaccordingtothehypothesisthatrapidlydividing cells(cancercells)aremoresusceptibletoDNAtoxicity thannormalcells.Sincethattime,awiderangeofnew therapiesbasedonmanipulationoftheimmunesystem, inductionofdifferentiation,inhibitionofangiogenesis,and increasedkillerT-lymphocytestodecreasecellproliferationhasgreatlyaugmentedthearmamentariumagainst neoplasticdisease.Previously,lethalmalignanciessuchas testicularcancer,somelymphomas,andleukemiaarenow curable.
Threegeneraltreatmentsofdiseasearesurgery,genetic engineering(stillanemergingdiscipline),andpharmacologicalintervention.Whileearlymedicinewassubjectto thetheoriesofHippocrates(460 357BCE),whosaw
FIGURE1.7 Thecellularveil.Drugsactonbiologicalreceptorsincellstochangecellularactivity.Theinitialreceptorstimulususuallyaltersa complicatedsystemofinterconnectedmetabolicbiochemicalreactions,andtheoutcomeofthedrugeffectismodi fiedbytheextentoftheseinterconnections,thebasalstateofthecell,andthethresholdsensitivityofthevariousprocessesinvolved.Thiscanleadtoavarietyofapparentlydifferent effectsforthesamedrugindifferentcells.Receptorpharmacologystrivestoidentifythebasicmechanisminitiatingthesecomplexevents.
FIGURE1.8 TheEbersPapyrusisa110-pagescroll(20mlong)thoughttohavebeenwrittenin1550BCEbutcontaininginformationdatingfrom 3400BCE.ItisarecordofEgyptianmedicineandcontainsnumerous “prescriptions” someofwhich,thoughempirical,arevalidtherapeuticapproaches todiseases.
healthanddiseaseasabalanceoffourhumors(i.e.,black andyellowbile,phlegm,andblood),bythe16thcentury pharmacologicalconceptswerebeingformulated.These couldbestatedconciselyasthefollowing[13]:
l Everydiseasehasacauseforwhichthereisaspecifi c remedy.
l Eachremedyhasauniqueessencethatcanbeobtained fromnaturebyextraction(“doctrineofsignatures”).
l Theadministrationoftheremedyissubjecttoadose responserelationship.
Thebasisforbelievingthatpharmacologicalinterventioncanbeamajorapproachtothetreatmentofdiseaseis thefactthatthebodygenerallyfunctionsinresponseto chemicals. Table1.1 showspartiallistsofhormonesand neurotransmittersinthebody.Manymoreendogenous chemicalsareinvolvedinnormalphysiologicalfunction.
TABLE1.1 Someendogenouschemicalscontrollingnormalphysiologicalfunction.
Acetylcholine
ATP
Epinephrine
Galanin
Histamine
Hormones
Thyroid-stimulatinghormone
Prolactin
Thyrotropin-releasinghormone
Growth-hormone-releasinghormone
Melatonin
Parathyroidhormone
Estrogen(s)
Androgens
Amylin
Calciferol
Secretin
Insulin-likegrowthfactor
ATP,adenosinetriphosphate.
Neurotransmitters
2-Arachidonylglycerol
Corticotropin-releasinghormone
Aspartate
Glutamate
Norepinephrine
Follicle-stimulatinghormone
Adrenocorticotropin
Oxytocin
Corticotropin-releasinghormone
Thyroxin
Glucocorticoid(s)
Progesterone
Insulin
Erythropoietin
Atrial-natriureticpeptide
Cholecystokinin
Angiotensinogen
Leptin
Thefactthatsomanyphysiologicalprocessesare controlledbychemicalsprovidestheopportunityfor chemicalintervention.Thus,physiologicalsignalsmediatedbychemicalscanbeinitiated,negated,augmented,or modulated.Thenatureofthismodi ficationcantakethe formofchangesinthetype,strength,duration,orlocation ofsignal.
1.8System-independentdrug parameters:affinityandefficacy
Theprocessofdrugdiscoveryreliesonthetestingofmoleculesinsystemstoyieldestimatesofbiologicalactivityin aniterativeprocessofchangingthestructureofthemolecule untiloptimalactivityisachieved.Itwillbeseeninthisbook thattherearenumeroussystemsavailabletodothis,andthat eachsystemmayinterprettheactivityofmoleculesin differentways.Someoftheseinterpretationscanappearto beinconflictwitheachother,leadingtoapparentcapricious patterns.Forthisreason,thewayforwardinthedrug developmentprocessistouseonlysystem-independentinformation.Ideally,scalesofbiologicalactivityshouldbe
Anandamide
Dopamine
Gamma-aminobutyricacid
Glycine
Serotonin
Luteinizinghormone
Antidiuretichormone
Gonadotropin-releasinghormone
Somatostatin
Calcitonin
Mineralocorticoid(s)
Chorionicgonadotropin
Glucagon
Calcitriol
Gastrin
NeuropeptideY
Ghrelin
usedthattranscendtheactualbiologicalsysteminwhichthe drugistested.Thisisessentialtoavoidconfusionandalso becauseitisquiteraretohaveaccesstotheexacthuman systemunderthecontroloftheappropriatepathology availableforinvitrotesting.Therefore,thedrug-discovery processnecessarilyreliesonthetestingofmoleculesin surrogatesystemsandtheextrapolationoftheobservedactivitytoallsystems.Theonlymeanstodothisistoobtain system-independentmeasuresofdrugactivity,namely,affinityandefficacy.
Ifamoleculeinsolutionassociatescloselywithareceptorprotein,ithasaffinityforthatprotein.Theareawhere itisboundisthebinding domain or locus.Ifthesame moleculeinterfereswiththebindingofaphysiologically activemoleculesuchasahormoneoraneurotransmitter (i.e.,ifthebindingofthemoleculeprecludesactivityofthe physiologicallyactivehormoneorneurotransmitter),the moleculeisreferredtoasan antagonist.Therefore,apharmacologicallyactivemoleculethatblocksphysiologicaleffectisanantagonist.Similarly,ifamoleculebindstoa receptorandproducesitsowneffect,itistermedan agonist. Italsoisassumedtohavethepropertyofefficacy.Efficacyis