https://ebookmass.com/product/handbook-of-diagnosticendocrinology-3rd-edition-william-e-winter-2/
Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
Handbook of Diagnostic Endocrinology 3rd Edition William E. Winter
https://ebookmass.com/product/handbook-of-diagnosticendocrinology-3rd-edition-william-e-winter-2/
ebookmass.com
Oxford Textbook of Endocrinology and Diabetes 3rd Edition John Wass
https://ebookmass.com/product/oxford-textbook-of-endocrinology-anddiabetes-3rd-edition-john-wass/
ebookmass.com
Bioquímica Clínica : Aspectos Clínicos e Metabólicos 3rd edition. Edition William J. Marshall (Editor)
https://ebookmass.com/product/bioquimica-clinica-aspectos-clinicos-emetabolicos-3rd-edition-edition-william-j-marshall-editor/
ebookmass.com
(eBook PDF) The Essential World History 9th Edition
https://ebookmass.com/product/ebook-pdf-the-essential-worldhistory-9th-edition/
ebookmass.com
Smokefur Protector: A Wolf Shifter Romance (Applecross Mountain Shifters Book 4) Mattie Waters
https://ebookmass.com/product/smokefur-protector-a-wolf-shifterromance-applecross-mountain-shifters-book-4-mattie-waters/
ebookmass.com
Untouchable: (Unstoppable - Book 1) Danielle Hill
https://ebookmass.com/product/untouchable-unstoppable-book-1-daniellehill/
ebookmass.com
Pretty Guilty Women: A Novel Gina Lamanna
https://ebookmass.com/product/pretty-guilty-women-a-novel-ginalamanna/
ebookmass.com
Fairytale and Gothic Horror: Uncanny Transformations in Film 1st ed. Edition Laura Hubner
https://ebookmass.com/product/fairytale-and-gothic-horror-uncannytransformations-in-film-1st-ed-edition-laura-hubner/
ebookmass.com
Office-Based Buprenorphine Treatment of Opioid Use Disorder Second Edition
https://ebookmass.com/product/office-based-buprenorphine-treatment-ofopioid-use-disorder-second-edition/
ebookmass.com
Leech
https://ebookmass.com/product/leech-hiron-ennes/
ebookmass.com
HandbookofDiagnostic Endocrinology
HandbookofDiagnostic Endocrinology
ThirdEdition
Editedby
WilliamE.Winter
DepartmentsofPathology,Immunology&LaboratoryMedicine,Pediatrics,andMolecular GeneticsandMicrobiology,UniversityofFloridaCollegeofMedicine,Gainesville,FL, UnitedStates
BrettHolmquist
EndocrineSciences,LaboratoryCorporationofAmerica,Calabasas,CA,UnitedStates
LoriJ.Sokoll
DepartmentofPathology,JohnsHopkinsUniversitySchoolofMedicine, Baltimore,MD,UnitedStates
RogerL.Bertholf
DepartmentofPathologyandGenomicMedicine,HoustonMethodistHospital, Houston,TX,UnitedStates PublishedincooperationwithAACC
AcademicPressisanimprintofElsevier 125LondonWall,LondonEC2Y5AS,UnitedKingdom 525BStreet,Suite1650,SanDiego,CA92101,UnitedStates 50HampshireStreet,5thFloor,Cambridge,MA02139,UnitedStates TheBoulevard,LangfordLane,Kidlington,OxfordOX51GB,UnitedKingdom Copyright©2021ElsevierInc.Allrightsreserved.
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans, electronicormechanical,includingphotocopying,recording,oranyinformationstorageand retrievalsystem,withoutpermissioninwritingfromthepublisher.Detailsonhowtoseek permission,furtherinformationaboutthePublisher’spermissionspoliciesandour arrangementswithorganizationssuchastheCopyrightClearanceCenterandtheCopyright LicensingAgency,canbefoundatourwebsite: www.elsevier.com/permissions.
Thisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythe Publisher(otherthanasmaybenotedherein).
Notices
Knowledgeandbestpracticeinthisfieldareconstantlychanging.Asnewresearchand experiencebroadenourunderstanding,changesinresearchmethods,professionalpractices,or medicaltreatmentmaybecomenecessary.
Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgein evaluatingandusinganyinformation,methods,compounds,orexperimentsdescribedherein. Inusingsuchinformationormethodstheyshouldbemindfuloftheirownsafetyandthesafety ofothers,includingpartiesforwhomtheyhaveaprofessionalresponsibility.
Tothefullestextentofthelaw,neitherthePublishernortheauthors,contributors,oreditors, assumeanyliabilityforanyinjuryand/ordamagetopersonsorpropertyasamatterof productsliability,negligenceorotherwise,orfromanyuseoroperationofanymethods, products,instructions,orideascontainedinthematerialherein.
AboutAACC
Dedicatedtoachievingbetterhealththroughlaboratorymedicine,AACCbringstogethermore than50,000clinicallaboratoryprofessionals,physicians,researchscientists,andbusiness leadersfromaroundtheworldfocusedonclinicalchemistry,moleculardiagnostics,mass spectrometry,translationalmedicine,labmanagement,andotherareasofprogressing laboratoryscience.Since1948,AACChasworkedtoadvancethecommoninterestsofthefield, providingprogramsthatadvancescientificcollaboration,knowledge,expertise,andinnovation. Formoreinformation,visit www.aacc.org.
BritishLibraryCataloguing-in-PublicationData
AcataloguerecordforthisbookisavailablefromtheBritishLibrary
LibraryofCongressCataloging-in-PublicationData
AcatalogrecordforthisbookisavailablefromtheLibraryofCongress
ISBN:978-0-12-818277-2
ForInformationonallAcademicPresspublications visitourwebsiteat https://www.elsevier.com/books-and-journals
Publisher: StacyMasucci
AcquisitionsEditor: AnaClaudiaGarcia
EditorialProjectManager: PatGonzalez
ProductionProjectManager: MariaBernard
CoverDesigner: MilesHitchen
TypesetbyMPSLimited,Chennai,India
Dedications
WilliamE.Winter,MD—Thisbookisdedicatedtotheuntiringsupport providedtomebymyspouseNancyS.Hardt,MD,mychildren,WilliamP. Winter,MPH,RNandKatherineH.Winter,MPH,MD,myson-in-law, AbidH.Ahmed,MD,andmygrandson,KianWinterAhmed.Ialsowishto recognizemyfellowshipmentorsArlanL.Rosenbloom,MDandNoelK. Maclaren,MDforlaunchingmyacademiccareerandRogerL.Bertholf,PhD, IshwarlalJialal,MD,PhD,andRobertDufour,MDfortheirsupportduring myprofessionalcareer.
RogerL.Bertholf,PhD—Tomyfamily,Marsha,Aaron,andAbby,fortheirlove andsupport,andtothemanyprofessionalcolleagueswhohaveenriched mycareerwiththeirknowledgeandgenerosity,Idedicatemycontributions tothishandbook.
LoriJ.Sokoll,PhD—Mycontributionstothishandbookhonormymentorsat HahnemannUniversity,RayVanderlinde,PhDandFredKayne,PhD,andat JohnsHopkinsUniversity,DanielW.Chan,PhD,JimNichols,PhD,and MartinKroll,MD,fortheirwisdom,guidance,andencouragement.
BrettHolmquist,PhD—FormywifeCarrieandmychildrenAveryandGrant fortheirsupport,andtothecountlessmentorsIhavehadtheprivilege toworkwithsincedonningmyfirstlabcoat.
4.Disordersoftheadrenalgland
5.Endocrinedisordersofthereproductivesystem
AngelaM.FergusonandMarkA.Cervinski
6.Gastroenteropancreaticneuroendocrinetumors
NeerajRamakrishnan,SeongHyunAhnandIshwarlalJialal
WilliamE.Winter,DavidL.Pittman,SrideviDevaraj, DanniLiandNeilS.Harris
functionmutations,andENaCgain-of-functionmutations
LoriJ.SokollandDanielW.Chan
15.Pregnancyandthefetus
K.AaronGeno,MarkA.CervinskiandRobertD.Nerenz
WilliamE.Winter,PaulHiersandDinaN.Greene
ListofContributors
K.AaronGeno DepartmentofPathologyandLaboratoryMedicine,DartmouthHitchcockHealthSystem,Lebanon,NH,UnitedStates;TheGeiselSchoolof MedicineatDartmouth,Hanover,NH,UnitedStates
SeongHyunAhn CaliforniaNorthstateUniversity,CollegeofMedicine,CA,United States
RogerL.Bertholf DepartmentofPathologyandGenomicMedicine,Houston MethodistHospital,Houston,TX,UnitedStates;DepartmentofPathology, StanfordUniversity,PaloAlto,CA,UnitedStates
RaffickA.R.Bowen DepartmentofPathology,StanfordUniversity,PaloAlto,CA, UnitedStates
MarkA.Cervinski TheGeiselSchoolofMedicineatDartmouth,Hanover,NH, UnitedStates;DepartmentofPathologyandLaboratoryMedicine,DartmouthHitchcockHealthSystems,Lebanon,NH,UnitedStates
DanielW.Chan DepartmentofPathology,JohnsHopkinsUniversitySchoolof Medicine,Baltimore,MD,UnitedStates
ManishaChandalia BayAreaMetabolicHealth,DiabetesLipids&Endocrinology Clinics,Baytown,TX,UnitedStates
SrideviDevaraj TexasChildren’sHospital,Houston,TX,UnitedStates;Divisionof ClinicalChemistry,TexasChildren’sHospital,Houston,TX,UnitedStates
CharlotteC.Ellberg CaliforniaNorthstateUniversityCollegeofMedicine,Elk Grove,CA,UnitedStates
AngelaM.Ferguson DepartmentofPathologyandLaboratoryMedicine,Children’s MercyHospital,UniversityofMissouri-KansasCitySchoolofMedicine,Kansas City,MO,UnitedStates
EmilyGarnett DivisionofClinicalChemistry,TexasChildren’sHospital,Houston, TX,UnitedStates
ZilGoldstein Callen-LordeCommunityHealthCenter,NewYork,NY,UnitedStates
VerenaGounden DepartmentofChemicalPathology,InkosiAlbertLuthuliCentral Hospital,NationalHealthLaboratoryService,UniversityofKwa-ZuluNatal, Durban,SouthAfrica
DinaN.Greene WashingtonKaiserPermanente,Renton,WA,UnitedStates; UniversityofWashingtonMedicalCenter,Seattle,WA,UnitedStates
NeilS.Harris DepartmentofPathology,Immunology&LaboratoryMedicine, UniversityofFlorida,Gainesville,FL,UnitedStates
PaulHiers NortonChildren’sHospital,UniversityofLouisville,Louisville,KY, UnitedStates
DanielT.Holmes DepartmentofPathologyandLaboratoryMedicine,St.Paul’s Hospital,Vancouver,BC,Canada;DepartmentofPathologyandLaboratory Medicine,UniversityofBritishColumbia,Vancouver,BC,Canada
BrettHolmquist EndocrineSciences,LaboratoryCorporationofAmerica, Calabasas,CA,UnitedStates
IshwarlalJialal SacramentoVAMedicalCenter,CA,UnitedStates;Retired DistinguishedProfessor,UCDAVIS,CA,UnitedStates;CaliforniaNorthstate UniversityCollegeofMedicine,CA,UnitedStates
GregoryKline DivisionofEndocrinology,University ofCalgary,Calgary,AB,Canada
DanniLi DepartmentofLaboratoryMedicineandPathology,Universityof Minnesota,Minneapolis,MN,UnitedStates
RobertD.Nerenz DepartmentofPathologyandLaboratoryMedicine,DartmouthHitchcockHealthSystem,Lebanon,NH,UnitedStates;TheGeiselSchoolof MedicineatDartmouth,Hanover,NH,UnitedStates
DavidL.Pittman DepartmentofPathology,Immunology&LaboratoryMedicine, UniversityofFlorida,Gainesville,FL,UnitedStates
NeerajRamakrishnan CaliforniaNorthstateUniversity,CollegeofMedicine,CA, UnitedStates
TamarReisman IcahnSchoolofMedicineatMountSinai,NewYork,NY,UnitedStates
AlanT.Remaley LipoproteinMetabolismLaboratory,TranslationalVascular MedicineBranch,NationalHeart,Lung,andBloodInstitute,NationalInstitutesof Health,Bethesda,MD,UnitedStates
LoriJ.Sokoll DepartmentofPathology,JohnsHopkinsUniversitySchoolof Medicine,Baltimore,MD,UnitedStates
WilliamE.Winter DepartmentofPathology,Immunology&LaboratoryMedicine, Pediatrics,andMolecularGenetics&Microbiology,UniversityofFloridaCollege ofMedicine,Gainesville,FL,UnitedStates
AnnaWolska LipoproteinMetabolismLaboratory,TranslationalVascularMedicine Branch,NationalHeart,Lung,andBloodInstitute,NationalInstitutesofHealth, Bethesda,MD,UnitedStates
PrefaceandAcknowledgments
Thisthirdeditionofthe HandbookofDiagnosticEndocrinology isintended forlaboratorydirectors,technologists,clinicians,trainees,andindustryscientistswhoseekacomprehensiveone-volumetreatisethatfocusesonthediagnosisofbothcommonanduncommonendocrinedisorders.Geneticsand personalizedmedicinerevealthevarietyandcomplexityofdisordersexaminedinthishandbook.Newchaptersfocusondisordersofsexualdevelopment,transgendermedicine,andtheagingendocrinesystem.Adiscussionof themetabolicsyndromehasbeenincludedinthechapteronhyperglycemia.
Theeditorsarefromdiversebackgrounds,representingacademicsand industry,andcomingfrombotheastandwestcoasts,southandsouth-central UnitedStates.Theauthorsofindividualchaptersareaninternationalgatheringofexperts.Tables,graphs,andillustrationshelpdemonstratetheorganizationandbreadthofdisordersthataffecthormones,theirreceptors,and postreceptorsignaling.Manychaptersincludedetailedstudiesofthemolecularbiologyofendocrinesystems;examplesincludedisordersofsexual development,endocrine-associatedhypertension,hyper-andhypoglycemia, andcalciumhomeostasis.
Acknowledgments
TheeditorswishtothankthestaffatElsevier,particularlyPatGonzalezfor theassemblyofthishandbookandTariS.Broderickforherinitialdevelopmentoftheconcept.Wealsothanktheauthorswhosetirelesseffortsmade thisvolumepossible.Lastly,theeditorswishtothanktheprevioushandbook editors,DanielW.Chan,PhD(firstedition)andIshwarlalJialal,MD,PhD (firstandsecondeditions),fortheircontributions.
Chapter1
Maximizingthevalueof laboratorytests
RaffickA.R.Bowen1,RogerL.Bertholf2 andBrettHolmquist3 1DepartmentofPathology,StanfordUniversity,PaloAlto,CA,UnitedStates, 2Departmentof PathologyandGenomicMedicine,HoustonMethodistHospital,Houston,TX,UnitedStates, 3EndocrineSciences,LaboratoryCorporationofAmerica,Calabasas,CA,UnitedStates
Theprimaryfunctionofaclinicallaboratoryistoprovideaccurateandclinicallyrelevantdataforthediagnosisofmedicalconditionsinpatients. Laboratorydatacanalsobeusedtoprovidepatientswithamanagement planthatwillhelpthemachieveadesirableoutcome.Errorsinthelaboratory testresultsaffectpatientcarewhentheymisleadcliniciansintofalsediagnosesorindicateatestisnormalwhenitisnot.Withregardtolaboratorytests, therearethreepotentialsourcesoferror:errorsmayoccurbeforetesting begins(preanalyticalerrors),duringthetestprocedure(analyticalerrors), andfollowingcompletionofthetest(postanalyticalerrors).
Althougherrorscanoccurinanylaboratorytestresult,immunoassays seemtobeparticularlyvulnerabletoanalyticalerrors,duetothenatureof antibody antigeninteractionsandthepotentialforinterferencefromcrossreactivespecies.Bytheirverynature,antibodieshavehighbutnotabsolute specificityfortheantigentheyareintendedtodetect,andthereforedetection ofknownorunknownantigenswithwhichtheantibodyreactslimitsthe specificityofimmunoassays.Inaddition,reagentantibodiescanalsobeantigenic,causingfalse-positiveorfalse-negativesignalsduetothereactionof endogenousantibodieswiththereagent.Althoughthefrequencyofmedicallyimportantimmunoassayinterferenceisprobablylessthanafewpercent [1] whenitoccurs,itcanoftenleadtounnecessarytreatmentorundetected disease.Manyoftheanalytesmeasuredbyimmunoassays,suchastumor markers,cannoteasilyorcost-effectivelybecorroboratedbyotherlaboratory tests.Immunoassayinterference,therefore,canleadtomisinterpretationof patient’sstatus,misdiagnosis,unnecessaryandcostlyradiologicalprocedures,and/orunnecessarytreatment.
Immunoassayinterferencescanoriginatefromeitherexogenousor endogenoussources.Exogenousinterferencesarecausedbytheadditionof externalfactorsorconditionseitherinvivoorinvitrothatarenotnormally presentinanative,properlycollected,andstoredsample [2].Forexample, hemolysis,lipemia,bloodcollectiontubeadditives,andadministrationof radioactiveorfluorescentcompounds,drugs,herbalmedicines,nutritional supplements,andsamplestorageareallexogenousinterferencesthatcan adverselyaffectimmunoassays [2 5].Interferencefromexogenousfactors isanoften-overlookedprobleminimmunoassays.
Endogenousinterferencesarecausedbyfactorsthatmayexistinthe patient’sbloodundereitherphysiologicalorpathophysiologicalconditions [2].Endogenousfactorsoftenaredifficulttodetectandeliminatebecause theycanvaryconsiderablybetweenpatients,andfromtimetotimeinany givenpatient.Examplesofendogenousinterferencesincludehumanantianimal,heterophilicantibodies,autoantibodies [6 8],rheumatoidfactors,and bindingproteins [2,9,10].Knowledgeoftheexogenousandendogenous interferencesandthemechanismsthroughwhichtheyinterferewithimmunoassaysisessentialtominimizethepotentialforanalyticalerrors.
Althoughmuchofthischapterwillbedevotedtosourcesoferrorin immunoassay,becauseitisthemostcommonanalyticalmethodusedfor measurementofhormones,manyofthemechanismsbywhichendogenous andexogenouscompoundsinterferewithimmunoassaysareanalogousto interferencesinchemicaltests.Thelaboratoryevaluationofendocrinedisordersisnotlimitedtoimmunoassays,andinthishandbook,youwillfind manyreferencestolaboratoryteststhatdonotinvolveantibodies.However, moreconsiderableattentionisgiventoimmunoassaysbecausetheyarecommonlyusedinthisdomainandareuniquelysusceptibletosomeoftheinterferencesdiscussedinthisbook.
Interferencesassociatedwithmassspectrometry
Beginningintheearly2000s,theuseofhigh-performanceliquidchromatography(LC)withtandemmassspectrometricdetectionhastransformedand vastlyimprovedtheanalysisofsmallmolecules,includingsteroidhormones. Beginningin2010,theCentersforDiseaseControl(CDC)hasworkedto standardizesteroidhormoneanalysiswiththeirHormoneStandardization (HoST)projectandVitaminDStandardizationProject(VDSP) [11].In2013 theendocrinesocietybeganrequiringmassspectrometry(MS)forsexsteroidassaysforpublicationintheJournalofClinicalEndocrinologyand Metabolism [12,13].TheuseofMSormoreoftenLC-MS/MShashistoricallybeenlaboratory-developedtests;however,in2017thefirstLC-MS/MS testfor25-hydroxyvitaminDwasclearedbyFoodandDrugAdministration (FDA) [14].TheLC-MS/MSplatform,owingtoitscoretechnologyand granularityofdatacollection,iswidelyconsideredmorespecific,more
selective,andlesspronetointerferencethanmostimmunoassaysforsmall molecule(steroid)analysis.Thereare,however,someparticularareasthat laboratoriansmustaddressduringvalidationofLC-MS/MSassays [15]. Whenchoosingalaboratoryanddiagnostictest,itisimportanttoworkwith alaboratorythatisexperienced,accredited,usingmoderntools,andvalidatingtocurrentexpectationsbasedonClinicalLaboratoryStandardsInstitute (CLSI)guidelinesincludingC50-AandC62 [16,17].Inadditiontosteroid analysis,MSisnowbeingusedforpeptideandproteinanalysiswithinthe endocrinespaceforselectedanalytes,includinginsulin-likegrowthfactor1, thyroglobulin,andplasmareninactivity(angiotensinI).Proteinanalysisby MSismorechallengingthantheanalysisofsmallmoleculesbutoffers extraordinarypotentialforbiomarkeranalysis.
Exogenousinterference
Hemolysis,lipemia,andicterus
Hemolysis,icterus,andlipemiacaninterferewithmanylaboratorytests. Hemolysiscanaffecttheabsorbanceoflightinspectrophotometricmeasurementssincehemoglobinisachromophorethatabsorbsbroadlyintheultraviolet(UV)-visiblerangeoftheelectromagneticspectrum.Hemolysisoccurs whenerythrocytesaredisrupted;thenormalconcentrationofhemoglobinin theplasmaisverylow.Whenerythrocytesaredisrupted,theircytoplasmic contentsaddsolublefactorstotheplasmafractionthatremainaftercentrifugation.Thesesolublefactorsmaybindtotheanalyteandblockantibodybindingsitesorcross-reactwiththereagentantibodies.Hemolyzedspecimensmaybeunacceptableforimmunoassaysoflabileanalytessuchasinsulin,glucagon,calcitonin,parathyroidhormone(PTH),adrenocorticotropic hormone(ACTH),andgastrinbecauseproteolyticenzymesreleasedfrom erythrocytescandegradepeptidehormones [18].Hemolysismayalsointerferewithsignalgenerationstepsincludedinvariousimmunoassays [18]. Hemolysismayinterferewithspectrophotometricmeasurementsdueto absorptionbyhemoglobin;thisisahemolysisinterferencethatisnotspecific toimmunoassays.Finally,forsomeanalytes,theintracellularconcentration ismuchgreaterthantheextracellularconcentration;thereforedisruptionof theerythrocytesincreasestheanalyteconcentrationintheplasmaaboveits physiologicallevel.Ingeneral,grosslyhemolyzedspecimensshouldnotbe usedforeitherchemicalassaysorimmunoassays.
Lipemiacanresultfromhighconcentrationsoftriglycerides,cholesterol, orboth,andmayproduceerroneousresultsinsomeassaysbyinterfering withantigenbinding,evenwhenantibodiesarelinkedtoasolidsupport. Lipemiahasalsobeenshowntocauseinterferencewithimmunoassaysthat haveturbidimetricend-pointsbecauseofthelightscattercausedbylipid micelles [2].Interferencesbynonesterifiedfattyacidshavebeenwell
documentedforfreethyroxineassays.Nonesterifiedfattyacidscompetewith thyroxineanditsderivativesusedaslabelsforendogenousproteinbinding sitesand,dependingontheassayformat,maycauseeitherfalselyhighor falselylowfreethyroxinevalues [19 21].Nonesterifiedfattyacidsmay alsoinhibitsteroidbindingtoproteins.Hypertriglyceridemiahasbeenshown tocausefalselyelevatedresultsinsomeendocrinologyassays,usingsecond antibodyandpolyethyleneglycolseparationtechniques [22].Itisdesirable tocollectspecimensfromindividualsafteranovernightfasttoreducethe immunoassayinterferencefromlipids.Alternatively,ultracentrifugationto removeanyexcesslipidsorenzymaticcleavagebylipasemaybeusedto treatsamplesbeforeanalysis [18].
Itshouldalsobekeptinmindthatbloodcontainsthreedistinctfractions: acellularfractionthatincludeserythrocytes,leukocytes,andplatelets;an aqueousfractionthatincludesprimarilywaterandvarioussmallmolecules, includingpeptides;andanextracellularnonaqueousfractionthatconsistsof lipidmicellesandglobularproteins.Thecellularfractioncomprisesapproximately45%ofthetotalbloodvolume.Whenaspecimeniscentrifuged,the noncellularfractionisusuallyabout95%aqueous,withtheremaining5% comprisedoflipidmicelles(suchaslipoproteins)andglobularproteins, includingimmunoglobulins.Thereforeanyanalytethatisexclusivelyinthe aqueousfractionofblood(electrolytes,organicacids,catecholamines, unboundsteroidhormones)isonlyoccupyingaround95%ofthetotalvolumeofplasma.Theexcludednonaqueousvolumeintroducesanerrorwhen concentrationsarebasedonthetotalvolumeofthespecimen.Formost assays,thissmallerrorisinconsequential.However,inhyperlipidemicor hyperproteinemicstates,thenonaqueousvolumecanbe10% 15%,which cancauseasignificanterrorinthecalculationofanalyteconcentrations.For electrolytes,directpotentiometrysolvesthisproblembecausemeasurements madeinundilutedspecimensarevolume-independent—thatis,thevolume occupiedbynonaqueouscomponentsinplasmaisnotrelevant.However, therearenodirectpotentiometricmethodsformeasuringhormones,anditis anotherreasonwhyhyperlipidemicspecimensshouldnotbeusedforlaboratorytestsunlessthelipidsareremovedbyultracentrifugation.
Excessbilirubinaffectsmanydifferenttypesofassays,eitherdueto spectrophotometricinterferenceorchemicaloxidationoftheanalytebybilirubin.Aswiththecaseforhemolysisandlipemia,theusershouldfollowthe recommendationsofthemanufacturertodeterminethesuitabilityoficteric samplesforanalysis.
Matrixeffects
Clinicalspecimensareincrediblycomplexandcontainavariablemixtureof proteins,carbohydrates,lipids,smallmolecules,andsalts.Amatrixeffectis aninterferencearisingfromanyoftheabovesubstancespresentathigh
enoughconcentrationtoaffectthemeasurementofananalyte.Inaddition, theviscosity,pH,andionicstrengthofthespecimenmayalsocontributeto matrixeffects.Matrixinterferenceinimmunoassayshasbeenthoroughly investigatedandreviewed [2].Antigenandantibodyreactionsareoftenquite sensitivetovariationsinproteinandlipidconcentrations,pH,andionic strength.Differencesinthematrixmayaltertheefficiencyofseparationof boundandunboundfractionsandtheextentofnonspecificbindingofthe tracer.Matrixeffectsarehighlydependentontheassayformatandtheantibodyselectedtocaptureanalyte;thereforevariousimmunoassaysare affectedindifferentways.Matrixeffectscanbeimportantsourcesofdiscrepanciesamongpatientsamples,calibrators,standards,qualitycontrols,and externalproficiencymaterialsthatarenotbasedonhumanserum [23 26].
Additionally,matrixeffectscanmakecertaintypesofbodyfluids unsuitableforanalysis [27].Thusmatrixinterferencesinclinicalassayscan beminimizedbycarefulassaydesign.Examplesofmethodstoreduceor eliminatematrixinterferencesincludetheuseofhigh-affinityantibodiesof certainsubtypesorantibodyfragments,dilutionofthespecimen,additionof animmunoglobulintotheassaybuffertosaturateanyinterferingantibodies, andoptimizingtemperatureandincubationtimes.Whenitisnecessaryto diluteasamplewithahighconcentrationbeyondthelinearrangeofthe assay,itisimportanttouseadiluentrecommendedbythemanufacturer withthepropermatrixtoavoidanyartifacts.
Bloodcollectiontubes
Bloodcollectiontubesarenotinertcontainersforbloodbuthaveseveral constituents,includinganticoagulants,surfactants,andlubricantsforrubber stoppers,clotactivators,andseparatorgelsthatcanpotentiallyinterferewith theassays.
Tubewall
SerumseparatortubesandVacuettetubesaremadefrompolyethyleneterephthalate.Siliconizedplastictubeshavebeenshowntocausea30% 60% decreaseincorticotropin(ACTH)measurementswhenmeasuredbyradioimmunoassay,possiblyduetointerferencewiththeformationofeitherthe biotin-avidincomplexortheantibody antigen antibodysandwich [28] Besidestubewalls,itisimportanttonotethatothersyntheticmaterialsthat comeincontactwithblood,suchasindwellingcathetertubing,havealso beenreportedtoaffectimmunoassayresults [29].Certaindrugs,suchas tacrolimus,cantightlybindtothecathetertubingwall,resultinginspuriouslyelevateddrugconcentrationswhenbloodiscollectedthroughcatheters, evenafterflushingthelinewithsaline [29].
Rubberstopper
Tomaintainthevacuuminbloodcollectiontubes,itiscommontousestoppersmadefromisobutylene-isopropenerubberorchlorinatedisobutyleneisoprenerubberalongwithastopperlubricant [30,31].Rubberstoppersused insomecommercialbloodcollectiontubeshavebeenfoundtocontaina plasticizer,tris(2-butoxyethyl)phosphate,whichcandisplacequinidine,propanolol,lidocaine,tricyclicantidepressants,fluphenazine,andchlorpromazinefrom α1-acidglycoprotein [18,32,33].Displacementofthesedrugsfrom theirbindingproteinresultsintheredistributionofthedruginblood,causing anincreaseindruguptakebyredbloodcellsandadecreaseinplasmaor serumconcentration [32,33].Mostmanufacturershavereformulatedtheir rubberstopperswithlowextractablerubbertominimizethisinterference.
Anticoagulants
Historically,mostassayswereperformedinserum,butplasmamaybepreferablebecauseiteliminatesthetimerequiredforclotting,therebyreducing theprocessingtime [34].Ifplasmaisused,caremustbetakentoselectan anticoagulantthatdoesnotinterferewiththeassay.
Ethylenediaminetetraaceticacid(EDTA)bindsdivalentmetalionsandpreventscoagulationbybindingtocalcium.EDTAalsobindssomemetalionsthat areaconstituentoflabels:forexample,europium,orenzymecofactorsessential fortheiractivity(e.g.,alkalinephosphataserequireszincions) [34].Elevated EDTAconcentrationsinasample-reagentmixtureduetoinsufficientsample volumecanresultinthemoreefficientchelationofmagnesiumandzincand canaffecttheactivityofthealkalinephosphataseenzymelabelusedinchemiluminescenceassays [34].FillingofEDTAsampletubesto , 50%affects,for example,intactPTH [35] andACTHmeasurements bytheImmuliteassays [34].Manyproteinsbinddivalentcations—typicallycalciumormagnesium— andtheantibodiesagainsttheseproteinsmayrecognizeanepitopethatisaltered whenthecationisabsent [36].
HeparinpreventscoagulationprimarilybyformingacomplexwithantithrombinIII.Theheparin-antithrombinIIIcomplexenhancestheinhibitory effectsofthrombinandactivatedFactorXtopreventclottingoractivation ofthrombin,whichinturnpreventstheformationoffibrinfromfibrinogen. However,heparinmayinterferewithsomeantibody antigenreactions. Heparindecreasestherateofreactionofsomeantibodies,particularlyatthe precipitationstepinsecond-antibodysystems;however,theuseofsolidphasesystemshasminimizedthisproblem.Heparincanprecipitatecryofibrinogen;thereforethisanticoagulantshouldnotbeusedforcryoproteinmeasurements.Theinfluenceofexogenouslyadministeredheparinonserum levelsofthyroidhormonesandotheranalyteshasalsobeeninvestigated. Heparinhasalsobeenshowntocauseinvivostimulationoflipoprotein lipasewithsubsequentreleaseofnonesterifiedfattyacids.Nonesterifiedfatty
acidsinhibitedthebindingofradiolabeledthyroxinetothyroid-bindingglobulinwithanapparentincreaseinthethyroxineresult.Samplescollectedinto tubescontainingsodiumfluoridemaybeunsuitableforsomeenzymatic immunoassaysduetoinhibitionoftheenzymeactivitybyfluoride.
Surfactants
Surfactantsarecommonlyaddedtoimmunoassayreagents [37] todecreaseor eliminatenonspecificadsorptionoftheanalyte,improvereagentstability,ormodifythesolid-phasesurfacetorenderitlesshydrophobic,thusminimizingtheloss ofnoncovalentlyboundantibody [30,31].Athighconcentration,surfactantsmay inhibitpassiveadsorptionofantibodyfromthesolidphase,amongothernonspecificeffects.Previousreportshaveshownthatsilicone-coatedcollectiontubescan interferewithion-specificelectrode determinationsof ionizedmagnesium [24,38 40] andlithium [41],causingfalselyincreasedconcentrations.Inaddition, thewater-solublesiliconepolymercoatingtheinteriorofserumseparatortubes caninterferewiththeformationofanavidin-biotincomplexinimmunoradiometricassaysforthyrotropin,prolactin,andhumanchorionicgonadotropin(hCG) [22].Bowenetal. [42] identifiedacommonorganosilanesurfactant(SilwetL720)inBectonDickinsonSSTbloodcollectiontubesthatcausedafalselyelevatedtriiodothyronineandotheranalytes.Whenpresentinexcessamountsin bloodcollectiontubes,thissurfactantcausesinterferencesbydesorbingthecaptureantibodyfromthesolidphaseusedintheImmulite2000/2500triiodothyronineimmunoassayandhadasimilareffectonimmunoassaysfromother manufacturers [42].Otherstudieshaveshownthatsiliconeformsacomplexwith C-reactiveprotein,enhancingtheantigen antibodyreactionintheVitrosCreactiveproteinassayandfalselyelevatingresults [43].
Clotactivators
Bloodcollectedinevacuatedtubeswithoutanticoagulantsshouldforma denseclotasrapidlyandcompletelyaspossibletoenableclearseparationof theclotfromtheserumlayerbycentrifugation [42 45].Toachievethis end,bloodcollectiontubesincludeaclotactivatorwithacarriersuchas polyvinylpyrrolidone [31,44].Examplesofclotactivatorsincludediatomaceousearth,particlesofinorganicsilicates,andbiochemicalssuchasellagic acid,thrombin,andthromboplastin.Occasionally,clotactivatorparticles maynotpelletcompletelywiththeclotandinsteadremainintheserum layer,causinginterferenceswithsomeassays.
Separatorgel
Separatorgelsarewidelyusedinbloodcollectiontubestoformabarrier betweenserumorplasmaandthecellularfractionuponcentrifugation.The separatorgelisathixotropicliquidthatissolidatrest,butwhencompressed bycentrifugation,itbecomesliquid [45].Ithasbeenshownthatthe
separatorgelcanadsorbsomehydrophobicleadingtofalselylowresults [46 49].Fragmentsofseparatorgelordropletsofoilmaybeseenwithin theseparatedserumorplasmafollowingthecentrifugationofsomegelcontainingbloodcollectiontubes.Thegeloroildropletscanclogthesample probe,coattubes,andcuvettes,andphysicallyinterferewithsolid-phase immunoassaysystems.Tominimizeinterferences,itisimportanttofollow thetubemanufacturer’srecommendationsandnotusethetubesattemperatures,centrifugationspeeds,ororientationsthatarenotwithinlimitsspecifiedbythemanufacturer.
Labelinterferences
Allimmunoassayrequiresameasurableindicatortoquantifytheantigen antibodycomplex.Somesamplesmaycontaincompoundsthatincrease ordecreasethemagnitudeoftheindicatorresponsewithoutaffectingantigen antibodybinding.Diagnosticortherapeuticadministrationofradioisotopeshasthepotentialtointerferewithradioimmunoassaysifthesame isotopeisusedastheindicator [50].Whentheindicatorisafluorophore, interferencecanoccurduetoendogenousfluorescence,fluorescentdrugs,or fluoresceinadministeredforretinalangiography [23].Fluorescencequenchersmayalsobepresentinsomeclinicalspecimens.Forenzyme-labeled immunoassays,thepresenceofenzymeinhibitorsoractivatorsinthesample mayaltertheenzymeactivity,andthustheresultsfromtheimmunoassay [27,51,52].
Drugsandherbalmedicine
Amajorsourceofexogenousinterferenceinimmunoassaysisthepresence ofdrugs,nutritionalsupplements,andherbalmedicineintheblood.These interferenceshavebeenwidelyreviewed [53 58].Manyoftheinterferences involvecross-reactivityofexogenouscompoundswiththecaptureantibody. Cross-reactingsubstancesmaybeaprecursorofthecompoundtobemeasured,oritcanbethemetaboliteoftheanalyte.
Timingofsamplecollection
Althoughnotstrictlyaninterference,itisimportanttorealizethatsomeanalyteshaveamarkeddiurnalpatternofphysiologicalreleaseand/orcanbe affectedbyvariablephysiologicfactorsortherapies.Asaresult,theseanalytesmustbemeasuredatspecifictimestoensurethatresultscanbeinterpretedappropriately.Cortisolconcentration,forexample,variessignificantly fromapeaknearmidnighttoanadirat7 8a.m.,andreferencerangesare appliedaccordingly [59].
Storage/freeze-thaw
Inappropriatesampletype,specimenprocessing,andstoragecanchangethe propertiesofthesampleovertimeandaffectimmunoassayresults.For example,ACTHisonlystablefor18hat4 C,incontrastto18otherhormonesthatarestablefor . 120h [60].Mosthormonesarerelatively stableinserumorurineiftheyarerapidlyfrozenandstoredat 70 C;however,repeatedfreezingandthawingofanalytescanleadtodenaturation, aggregation,andlossofantigenicityofsomeproteins [60].SpecimenscollectedinEDTAoftenaremorestablethanserumorheparinizedplasmaspecimensbecauseEDTAchelatescalciumandmagnesiumions,whichare cofactorsforsomeproteaseenzymes.Theadditionofproteaseinhibitors (e.g.,aprotinin)tobloodsamplesmayalsoimproveanalytestability [59,61]
Analyticalerrors
Carryover
Automatedchemistryandimmunoassaysystemsuseautomatedsamplehandlingdevices.Ifasampletobeassayedisprecededbyasamplewitha veryhighconcentrationofananalyte,thereisapotentialfortheanalytein thefirstsampletocontaminatethesecondsampleduetoinadequaterinsing oftheprobebetweenspecimens.Thereforeitisimportanttoroutinelytest anynewanalyzerforpotentialcarryover.Itistheresponsibilityofthelaboratorytoassessthepotentialforcarryoverineachassayitperformsand incorporatetheappropriateactiontotakeinthestandardoperating procedure.
Endogenousinterference
Excessantigeninterference(hookeffect)
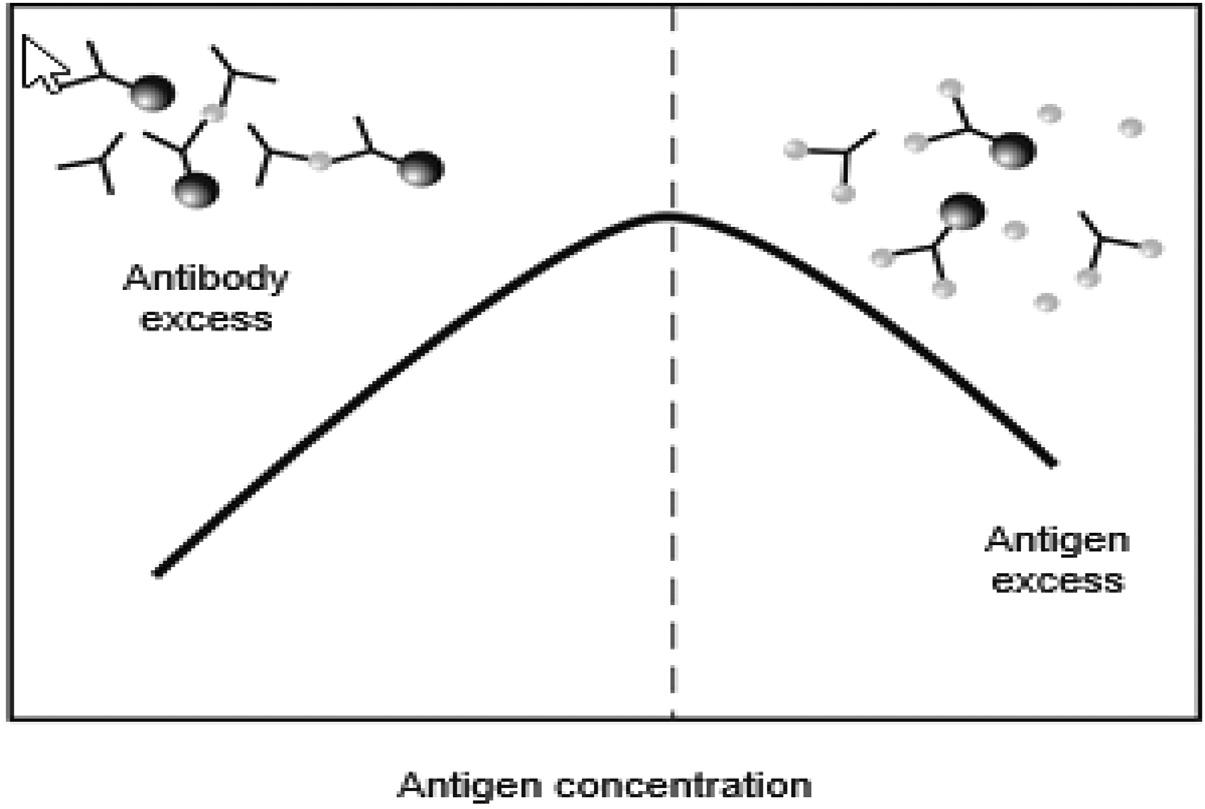
Excessantigeninterferenceoccurswhenthereisanunusuallyhighconcentrationofantigen,whichparadoxicallymayleadtoafalselylowresult.This phenomenoniscommonlyreferredtoasa“hook”orprozoneeffect [62,63] Thistypeofinterferenceismostlikelytooccurwhentheanalytecanhavea verywiderangeofconcentrations,asdohCG,manytumormarkers,and serologicaltests [64,65].Asshownin Fig.1.1,2-siteimmunometricassays areespeciallypronetothehookeffect.Theseassaysdependupontheformationofacomplexbetweentheantigenandtheprimary(or“capture”)and secondaryantibodiestogenerateasignal.Theseassaysareusuallydesigned sothattherearealwaysexcessantibodiesrelativetotheantigen.When thereisanexcessantigen,however,acomplexdoesnotformbecauseall oftheantigen-bindingsitesareoccupiedbyasingleantigen,thuspreventing asingleantigenmoleculefrombridgingtheprimaryandsecondary
10 Maximizingthevalueoflaboratorytests
FIGURE1.1 Diagramofimmunoassayinterferenceoncompetitiveandnoncompetitiveassays byantibodyinterference.
antibodies [66].Afterafinalwashstep,thesecondaryantibodiesthatgeneratethesignalareremovedwhenthereisanexcessantigen,thusresultingin aspuriouslylowvalue.
Antigenexcessinterferencecanbepreventedbyperformingtheassayon adilutedsampleorbytheadditionofavastexcessofantibodytoensure thatthereisalwaysasufficientconcentrationofantibodies,evenforthose sampleswithunusuallyhighconcentrationsoftheanalyte.Manufacturersof assaysforanalytesthatarecommonlyaffectedbyantigenexcessusually provideasufficientamountofantibodiestopreventthisproblem.Inaddition,sequentialtwo-stepimmunometricassaysarelesspronetothisproblem becauseawashstepisincludedbeforetheadditionofthesecondantibody; thiswashremovesanyexcessantigen,preventinganerroneouslylowresult. Finally,animportantconsiderationinimplementinganynewassaythatmay besusceptibletothehookeffectistodeterminewhetherthelinearrange describedbythemanufacturerencompassesthelikelyconcentrationrange thatwillbemeasuredinthelaboratory.
Antibodyspecificity(cross-reactivity)
Specificityisanimportantcharacteristicofanyassaybecauseitdescribesits abilitytoreactwithonlytheanalyteofinterestinasample.Amajorsource ofbiasinanimmunoassayisthelackofspecificityoftheantibodies used,resultingincross-reactivity.Cross-reactivityismoreproblematicwith polyclonalantibodiescomparedtomonoclonalantibodies.Polyclonal
Maximizingthevalueoflaboratorytests Chapter|1 11
antibodiestypicallyhavehighavidity,butmonoclonalantibodieshavea higheraffinityandthereforearemoreselectivetowardaspecificantigen. Selectionofmonoclonalantibodiesmayreducecross-reactivity,butclosely relatedmoleculesmaystillberecognizedbytheantibody,especiallyanalytes,suchassteroidsanddrugs.Cross-reactivityismorecommonwithcompetitiveimmunoassayscomparedtononcompetitiveimmunoassayssincethe useofanantibodyagainstasecondepitopeontheanalytereducesthelikelihoodofacross-reactingantigenhavingbothepitopestestedforbythenoncompetitiveimmunoassays.However,noncompetitiveimmunoassaysdonot alwaysexhibitgoodspecificitybecausenonspecificbindingmayarisedueto manyendogenoussubstancespresentinthepatientsample,suchasrheumatoidfactor,complementproteins,orbacterialproteins [67].
Antibodyinterference
Circulatingantibodiesinpatientsamplesmayinterferewithimmunoassays [68].Usually,endogenousantibodiesinterferebyreactingwiththereagent antibodiesinimmunoassays,butalltheothercomponentsofimmunoassays, suchastheantigen,enzyme-substrate,andsignalmolecule,canalsobeatargetofendogenousantibodies,adverselyaffectingimmunoassayresults. Previousstudieshaveshownthatinterferingendogenousantibodiesare presentinupto30% 40%ofpatientsamples [68],butestimatesvary widely [1,69],andtheirpracticaleffectisfarless.Interferingantibodies includeheterophilicantibodiesthathavemultiplespecificitiesforantigens, aswellasproteins,suchasrheumatoidf actor;humanantianimalantibodies (HAAAs),especiallyhumanantimouseantibodies(HAMAs);orautoantibodies.Thepresenceofinterferingantibodiescanaffectbothnoncompetitiveandcompetitiveimmunoassaysandproduceeitherfalselyelevatedor falselydecreasedresults,dependingonthespecificantibodyorprotein withwhichtheheterophilereacts.The natureoftheantibodyinterference dependsonthetypeofassayusedandthesitewheretheantibodybindsto theanalyte [2,70]
Heterophileantibodies
HeterophileantibodiescanbeimmunoglobulinG(IgG),immunoglobulinM (IgM),immunoglobulinA,andIgGisotypesthatarepoorlydefinedandreact withawidespectrumofantigens [6,71,72].Ifexposuretoaspecificanimal immunogenisknown,thecorrecttermforthatheterophileantibodyshould refertothespecificanimalthatproducedtheantigensuchas“humanantimouseantibody,”or“humanantirabbitantibody.”Heterophileantibodiesare usuallylow-titer,weak-avidityantibodiesfoundintheserumofpatientswith nohistoryoftreatmentordiagnosticproceduresinvolvingantianimalimmunoglobulins [73,74].Heterophileantibodieshavebeenreportedtobepresent in30% 40%ofpatientsamples [68,75] andareawell-recognizedcauseof
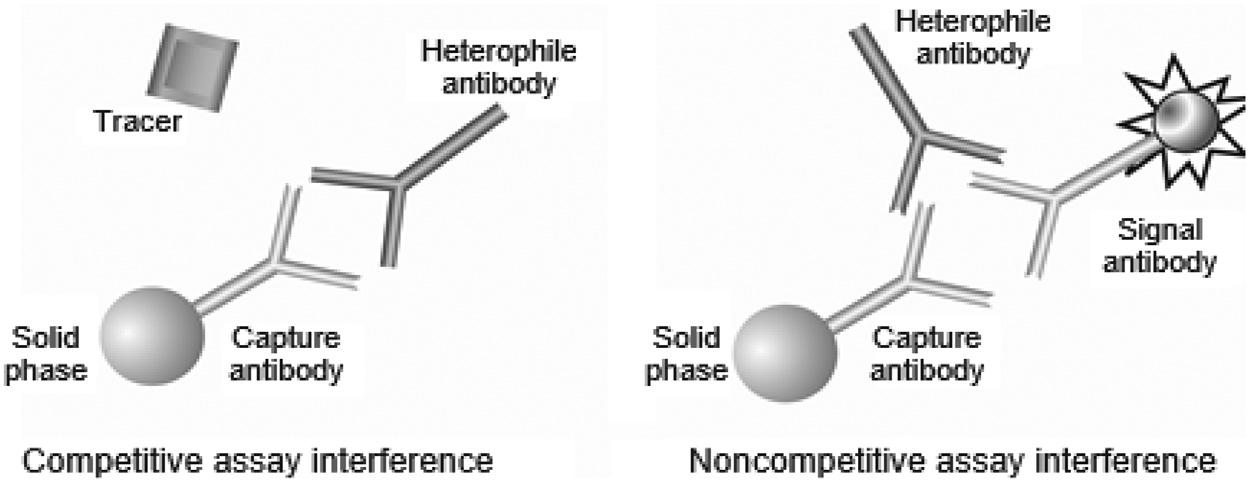
interferenceinimmunoassays [76,77] .Whenheterophileantibodiesare present,itisoftenverydifficulttopr edictthedirectionandmagnitudeof theimmunoassayinterference.Interferencesmayoccurincompetitiveor noncompetitiveassays,butthelatterismorecommon [36,78] .Incompetitiveimmunoassays,thepresenceofheterophileantibodiesmaydecrease thenumberofavailablebindingsitesontheprimaryantibodybysterichindranceofthespecificantigen,( Fig.1.2)andinsomecompetitiveimmunoassayformats,reducethebindingof asecondantibody,causingapositive interference.Innoncompetitiveimmunoassays,heterophileantibodiescan interferebybridgingthecaptureanddetectionantibodies [68,75] ,causing false-positiveresults(Fig.1.2).Incontrast,heterophileantibodiescanalso causefalse-negativeresultsbybindingdirectlytothecaptureantibody, thusblockingthereactivesitefrombindingtheanalyteofinterest.The sameantibodymayreactdifferentlyfordifferentantibodycombinations, thuscausingfalselyelevatedresultsinoneassaybutalowerresultin anotherassay.Immunoassaymanufacturerstypicallyaddblockingagents (nonimmuneglobulinsofvariousspecies)totheirassayformulationsto saturateandminimizeoreliminateth eeffectsofheterophileantibodies; however,notallheterophileinterferencecanbepreventedbyblocking agents [79] .Heterophileantibodiesmayshowreactivitytoidiotypesthat arenotpresentintheblockingagent [80] .Priorextractionoftheanalyte fromthesamplebyproteinA,proteinG ,cation-exchange,orgelfiltration chromatographyisalsoeffectivei nremovingheterophileantibodies [6,63,72,81 84].Reactionconditionscanalsobemodifiedtominimize heterophileantibodyinterference [80] Heatandacidtreatmentofsamples arenotveryusefulsincetheseantibody-denaturingconditionswilldestroy mostanalytes.
Humanantianimalantibodies
HAAAsarehigh-affinity,specificpolyclonalantibodiesthatreactwith immunoglobulinsfromaspecificanimal.Forantianimalantibodieselicited
FIGURE1.2 Diagramofimmunoassayinterferencefromexcessantigen.