TABLE1.1 RecentDefinitionsonGreenBuildings
ReferencesDefinitions
WorldWildlifeFund(2015) Physicalstructurethatusesadesignandplanningprocessthatisenvironmentallyresponsibleandresourceefficient
USEnvironmentProtection Agency(2014a)
RobichaudandAnantatmula (2011)
Practiceofcreatingstructuresandusingprocessesthatareenvironmentallyresponsibleandresourceefficientthroughout abuilding’slifecyclefromsitingtodesign,construction,operation,maintenance,renovationanddeconstruction. Further,thispracticeofgreenbuildingsandcomplementtheclassicalbuildingdesignconcernsofeconomy,utility, durability,andcomfort
Greenbuildingisaphilosophyandassociatedprojectandconstructionmanagementpracticesthatseekto:(1)minimize oreliminateimpactsontheenvironment,naturalresources,andnonrenewableenergysourcestopromotethe sustainabilityofbuiltenvironment;(2)enhancethehealth,well-beingandproductivityofoccupantsandwhole communities;(3)cultivateeconomicdevelopmentandfinancialreturnsfordevelopersandwholecommunities;and(4) applylifecycleapproachestocommunityplanninganddevelopment
HoffmanandHenn(2008) Greenbuildingisatermencompassingstrategies,techniquesandconstructionproductsthatarelessresourceintensiveor pollutionproducingthanregularconstruction
USGreenBuildingCouncil (2007)
ASHRAE(2006,p.4)
Efficientbuildingwithsavingsinenergycostsof20% 50%arecommonthroughintegratedplanning,siteorientation, energy-savingtechnologies,on-siterenewableenergy-producingtechnologies,light-reflectivematerials,naturaldaylight andventilation,anddownsizedHVACandotherequipment
Greenbuildingisonethatachieveshighperformance,overthefulllifecycle,intheareassuchasminimizingnatural resourceconsumptionthroughmoreefficientutilizationofnonrenewablenaturalresources,land,water,andconstruction materials,includingutilizationofrenewableenergyresourcestoachievenetzeroenergyconsumption,minimizing emissionsthatnegativelyimpactourindoorenvironmentandtheatmosphereofourplanet,especiallythoserelatedto IAQ,greenhousegases,globalwarming,particulates,oracidrain,minimizingdischargeofsolidwasteandliquid effluents,includingdemolitionandoccupantwaste,sewer,andstormwater,andtheassociatedinfrastructurerequiredto accommodateremoval,minimalnegativeimpactsonsiteecosystem,maximumqualityofindoorenvironment,including airquality,thermalregime,illumination,acoustics/noise,andvisualaspectstoprovidecomfortablehumanphysiological andpsychologicalperceptions
Cassidyetal.(2003)
Buildingswhichincreasetheefficiencyofsitesuseenergy,water,andmaterials,andreducebuildingimpactsonhuman healthandtheenvironment,throughbettersiting,design,construction,operation,maintenance,andremovalthroughout thecompletebuildinglifecycle
Wyatt(1994) hasdeemedgreenbuildingconstructiontoinclude“cradle tograve”appraisal,whichincludesmanagingtheserviceabilityofabuilding duringitslifetimeandeventualdeconstructionandrecyclingofresourcesto reducethewastestreamusuallyassociatedwithdemolition.Further, Kibert (1994) identifiedsevenprinciplesofsustainableconstruction.Theseseven principlesare:reduceresourceconsumption,reuseresources,userecyclable resources,protectnature,eliminatetoxics,applylifecosting,andfocuson quality.Theseprinciplescanbeappliedacrosstheentirelifecycleofconstruction,fromplanningtodemolition(Kibert,1994).Theseprinciplesconsidercarryingouttheconstructionbyreducingresourceconsumption, reusingresourcesandusingrecycledresources,whichtendstoprotectnature byeliminatingtoxics(LavyandFerna ´ ndez-Solis,2009).However,ingreen buildings,thereisapropermanagementputinplacefromtheinitialstages toguidethroughtheprocess.Therefore,theessenceofgreenconceptsisput intopracticethroughoutthegreenbuildinglifecycle.
Accordingto AustralianNationalAuditOffice(2001),therearefive mainphases,whicharedesign,purchaseandconstruction,operations,maintenance,developmentanddisposal.However,inthisclassificationthefirst threephasesoccurintheearlierstagesofthelifecycle.Theoperation,maintenance,anddevelopmentoccurthroughoutthebuildinglifecycle,and finally,thedisposalofthebuildingoccurs.Further,thereareusuallyfour stagesinanyproductdevelopment;namely,design,production,usage,and disposal(AsieduandGu,1998).Similarly,lifecycleofgreenbuildingscan alsobeillustratedinthesefourstages.Thedesignstageincludedthedesigningofthebuildingandtheproductionreferstotheconstructionphase. Usagephaseofthebuildingreferstotheoperationalphasewhichincludes maintenanceofthebuildingsandfinallythedisposalofthebuilding. Cao andFolan(2012) identifiedthreebasicstagesofproductdevelopment; namely,thebeginningoflife,themiddleoflife,andtheendoflife.Further, the“beginningoflife”stageincludestheconceptdevelopmentandthe manufacturingprocessandthe“middleoflife”processincludestheactual usageoftheproduct(CaoandFolan,2012).Intermsofgreenbuildinglife cycleperspective,thesethreestagescanbeidentifiedasthedesignand constructionphase,operationalandmaintenancephase,andfinally,the disposalphase.
Consideringthesephases, Fig.1.1 illustratesthegreenbuildinglifecycle andeachofthesignificantaspectsconsideredthroughoutthecycle.
Accordingto Fig.1.1,therearemainfourphasesingreenbuildinglife cycle.Designphasefocusesonthedecision-makingregardingthegreen building.Therearecriticalaspectsdiscussedinthisphasefocusingonthe design,procurementroute,landuse,accessibility,andsoon.Thesecond stageisconstructionphase.Thisisthephasewhereactualconstruction occurs.Whencomparedtoaconventionalbuilding,inagreenbuilding,there
isamoreenvironmentallyfriendlierapproachconductedduringtheconstruction.Nextistheoperationalandmaintenancestage.Inotherwords,thisis theperiodinwhichthebuildingfunctions.Throughoutthisphase,itconsumesenergy,water,andmanyresources,andinturnemitsmanyemissions totheenvironment.Accordingto WorldGreenBuildingCouncil(2015),ina greenbuilding,itisexpectedtoincuranincreaseof0.4% 12.5%ofdesign andconstructioncostwhileexperiencinganenergysavingofupto25% 30%.Theseenergysavingsareexperiencedduringtheoperationalstageof thebuildinglifecycle.Finalstageisthedisposalphase.Thisisthephase wherethebuildingisdeconstructed.Thismarkstheendofthelifecycleof thisgreenbuilding.Further,foragreenbuilding,managementfunctionis applicablethroughoutthebuildinglifecycle.
FIGURE1.1 Greenbuildinglifecyclestages.
1.3.1DesignStage
Asillustratedin Fig.1.1,thisstageincludescertainaspectsconsideredinthe initialdecision-making.Qualitydesign,procurementroute,accessibilityand transport,landuseandecology,sustainabletechnologyinnovationsarethe mainaspectsidentifiedinthisphase.
1.3.1.1QualityDesign
Thedesignitselfcontributessignificantlytowardthegreenfeatures. Accordingto AnastasandZimmerman(2003),therearemain12principles ofgreendesign.Theseprinciplesprovideaframework,whichmovesbeyond baselineengineeringqualityandsafetyspecificationstoconsiderenvironmental,economic,andsocialfactors. Fig.1.2 illustratesthe12principlesin detail.
Principle 12: Material and energy inputs should be renewable rather than depleting
Principle 11: Products, processes, and systems should be designed for performance in a commercial “afterlife”
Principle 10: Design of products, processes, and systems must include integration interconnectivity with available energy and materials flows
Principle 9: Material diversity in multicomponent products should be minimized to promote disassembly and value retention
Principle 8: Design for unnecessary capacity or capability (e.g., “one size fits all”) solutions should be considered a design flaw
Principle 1: Designers need to strive to ensure that all material and energy inputs and outputs are as inherently nonhazardous as possible
principles
Principle 2: It is better to prevent waste than to treat or clean up waste after it is formed
Principle 7: Targeted durability, not immortality, should be a design goal
Principle 3: Separation and purification operations should be designed to minimize energy consumption and materials use
Principle 4: Products, processes, and systems should be designed to maximize mass, energy, space, and time efficiency
Principle 5: Products, processes, and systems should be “output pulled” rather than “input pushed” through the use of energy and materials
Principle 6: Embedded entropy and complexity must be viewed as an investment when making design choices on recycle, reuse, or beneficial disposition
FIGURE1.2 12principlesofgreenengineeringdesign. AdaptedfromAnastas,P.T., Zimmerman,J.B.,2003.Peerreviewed:designthroughthe12principlesofgreenengineering. Environ.Sci.Technol.37(5),94A 101A.
Theseprinciplesgivenin Fig.1.2 illustratealltheaspectsofgreenbuildingdesign.Itdiscussesonthematerialselection,wasteminimization,energy efficiency,recyclingandreusing,andsoon.Therefore,ingreenbuilding designtheinitialdesignstageiscritical.Itlaysthebasisforthegreener buildingsconsideringthetriplebottomline;thatis,environmental,economical,andsocialsustainability.
1.3.1.2ProcurementRoute
Projectprocurementhasbeendescribedasanorganizedmethodorprocess andprocedureforclientstoobtainoracquireconstructionproducts(Abdul Rashidetal.,2006).Usingthebest-suitedprocurementrouteisveryimportantforanyconstruction.Forgreenbuildingdevelopmentalsoitisnotan exception.Procurementrouteissignificantinmanagingtheprojectobjectivesandtodealwiththerisksinconstructionintermsofcostfluctuations, time,qualityconcerns,andsoon.Greenbuildingsareresourceandenergy efficientstructurescomparedtoconventionalbuildingsandthereforeinnovativetechnologiesareputforthtoachievegreenbuildingrequirements. Therefore,theriskingreenbuildingconstructionishighercomparedtothe conventionalbuildings.Further,thereisaninitialcostpremiumforgreen buildingsaswell.Asaresult,selectingthesuitableprocurementrouteis verymuchimportant.Procurementiscriticalasitdeterminestheoverall frameworkembracingthestructureofresponsibilitiesandauthoritiesforparticipantswithinthebuildingprocess(Cheungetal.,2001).
Therearemainfactorsconsideredinprocurementselection.Therisktakingabilityoftheclient,timeforconstruction,cost,qualitystandards,complexityoftheproject,andtheextentofclientinvolvementaresomeofthe factorsaffectingtheselectionofprocurementroute.Indecidingtheprocurementroutetherearethreeaspectstobefinalized.Thesearetheworking arrangement,tenderingprocess,andtheformofcontract.Workingarrangementdefinestherolesanddutiesoftheclient/consultantandthecontractor andthepaymentmethods.Greenbuildingprojectsdemandopenlinesof communicationbetweendisciplinesduetothemorecomplexinterdependenciesbetweenbuildingsystemsandprojectorganizationsthantraditionalprojects(Rileyetal.,2003).Therefore,accordingto Rileyetal.(2003), integratedprojectteamsaremoresuitableforgreenbuildings.Asanexample,thereareseveralworkingarrangementssuchastraditionalprocurement, designandbuilding,designandmanagementpath.Therearevariantstoeach oftheseworkingarrangements.Furtherdependingontherequirementsofthe greenbuildingtheworkingarrangementisestablishedclearlydefiningthe rolesandresponsibilities.Thewayinwhichenvironmentalrequirementsare stipulatedinprocurementdocumentsissignificantforthedevelopmentofa project’senvironmentalfeatures(Sterner,2002).
Another random document with no related content on Scribd:
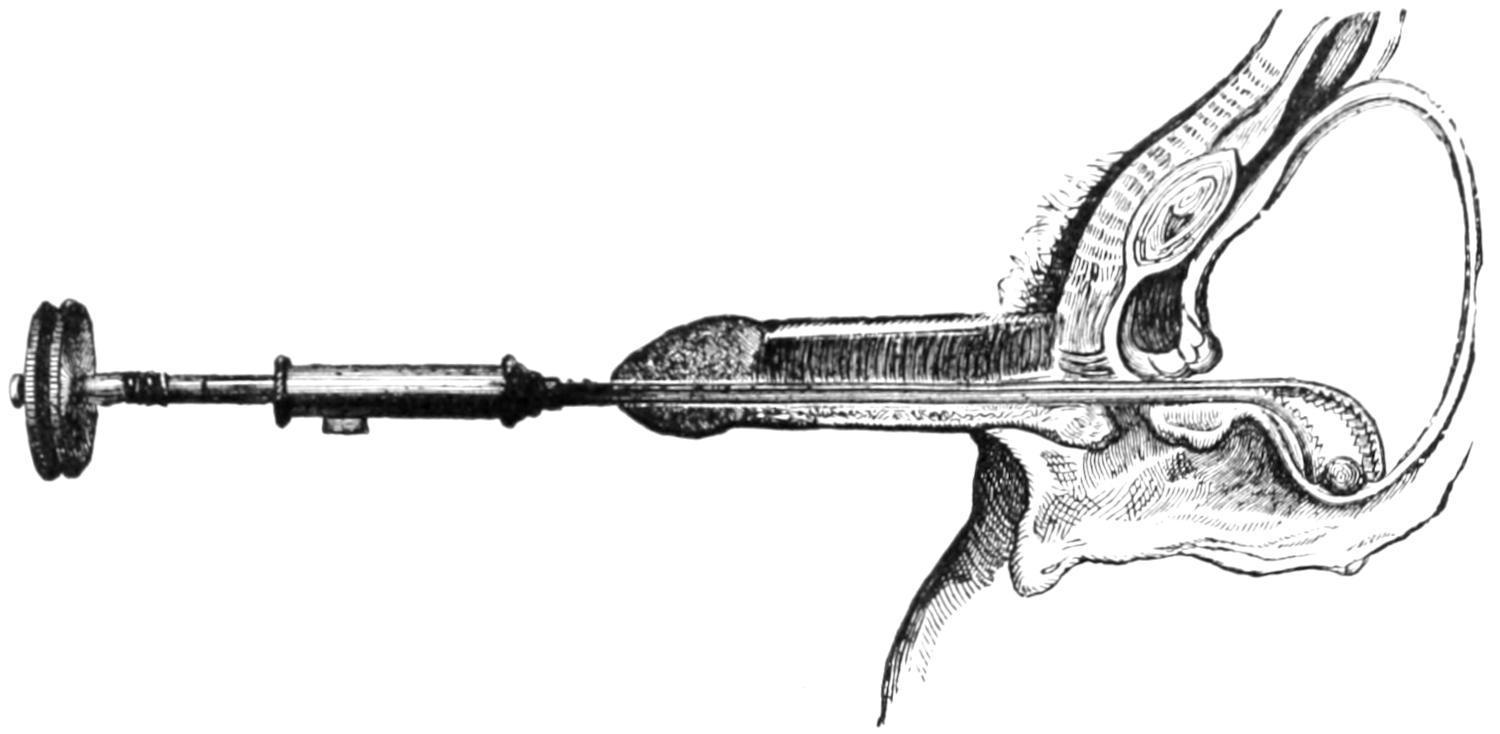
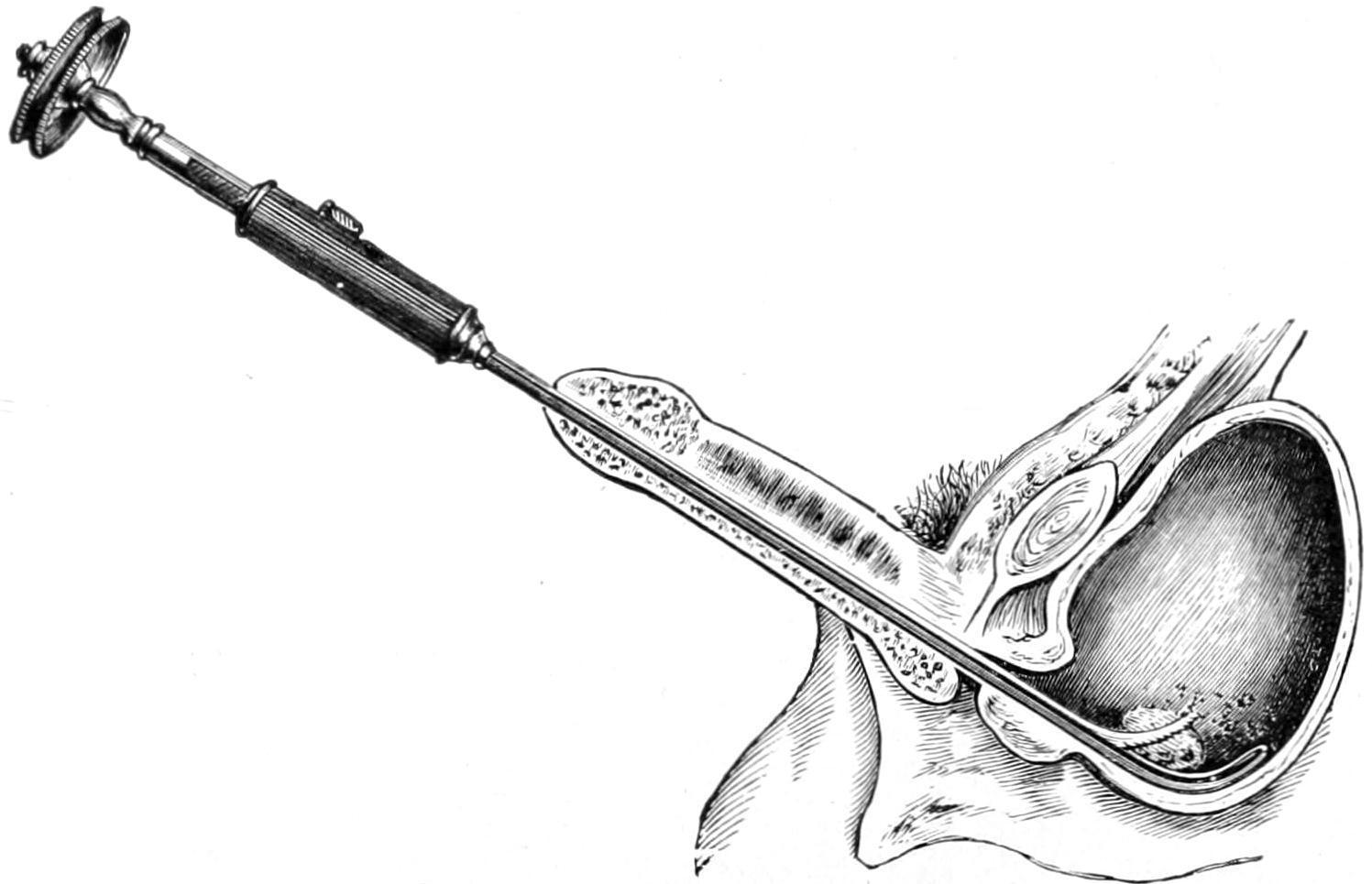
The attempt will not be made here to picture nor go into a minute description of the various forms of the cystoscope. Their use, like that of the ophthalmoscope, requires special aptitude and training. With the latter they are of great value; without them they confuse and complicate. The cystoscope may be used for ordinary purposes of inspection, for aid in introducing the ureteral catheter, or even for photographic purposes, for it is now possible with the latest instruments to photograph the image thus obtained of the bladder interior. To one not accustomed to viewing the field seen in such an instrument these revelations are of little interest. To the expert, however, they may be made of the greatest value. Without further description, then, allusions made below to the use of the instrument must presuppose some familiarity with it, and the advantages and even necessity of securing special training in its use.
CONGENITAL MALFORMATIONS OF THE BLADDER.
The lesser malformations of the bladder include mainly irregularity in shape or the formation of diverticula, which are not extremely rare. These are especially likely to be met during hernia operations. I have repeatedly in operating for inguinal, and once in operating for femoral hernia, found a diverticulum of the bladder complicating the situation. Its possibility, then, should be borne in mind. It may be thin and lie in such close relation to the hernial sac as to be mistaken for the latter. When opened urine will escape and contaminate the wound. It would probably be best to close the bladder opening and discontinue the operation rather than run the risk of contamination of the peritoneal cavity, postponing further work for a few days. As the result of allantoic defects a double bladdermay be met, each perhaps having one ureter opening into it. More or less complete partitions in the bladder are more frequently met. These conditions could not be appreciated previous to opening the viscus or the use of the cystoscope.
More complete forms of acquired vesical hernia may be found in such conditions as cystocele, common in women after perineal lacerations, and frequently constituting a most serious condition.
Ectopia or Exstrophy of the Bladder.—By far the most serious and extensive of the congenital malformations are those constituted by more or less complete defects of the anterior portions not alone of the bladder, but of the abdominal wall which should cover it, and which are known as ectopia, exstrophy, or extroversion of the bladder. Of this condition there are different degrees, from a small cleft just behind the symphysis pubis, to that which is complicated by prolapse of the remaining posterior wall, the umbilicus being situated just above it, while the pubic arch itself is defective or rudimentary. Thus in the male there is usually epispadiasof a more or less rudimentarypenis, while in the female the clitorisis cleftand the vulva more or less opened, the urethra being defective or entirely wanting, the vagina often small, and the uterus generally infantile. Extreme cases of this condition constitute one of the most serious and deplorable congenital defects which are not inherently fatal. Obviously, with these conditions, there is constant escape of urine, usually with complete mechanical impotence, although in the female the ovaries are usually present, and practically always the testicles in the male. In the latter the opening of the seminal ducts may be frequently seen on the floor of the urethra, more or less concealed by folds of cystic mucous membrane. The condition is much more frequent in males than in females. The prostate is usually at least rudimentary and may be wholly wanting. Occasionally the testicles are undescended. Double uterus has also been seen in these conditions.
Regarding its causes there is but little known. Doubtless these have to do with allantoic defects, but the allantois is such a temporary organ that there would seem to be some other contributing cause not yet recognized.
Among its most distressing features are not only the lack of control of urine, but the irritation of the exposed mucous surfaces consequent upon friction with clothing, or decomposition of urine and consequent uncleanliness. There is, therefore, nearly always ulceration, with extreme irritability and more or less constant suffering. It is not strange, then, that for its relief surgeons have
taxed their ingenuity, or that adult patients, finding the conditions unbearable, are willing to submit to even extreme measures.
Treatment.
—So many operative measures have been devised that it is impossible to include them all. First of all the procedure should be adapted to the particular case. Much will depend, for instance, upon the extent of the defect in the abdominal wall, or in the pubic arch, and in the male upon the rudimentary condition of the penis or the extent of the urinary canal.
Operations for this condition may be divided into palliative and radical—i. e., those which are intended to make it more tolerable and those which are really entitled to the latter term. Thus if only the exposed mucous surface can be covered with a skin covering, the condition may be mitigated since a urinal or some device may be worn by which its worst features may be controlled. Trendelenburg has recently called attention to the fact that a wide separation of the pubic arch not only weakens the pelvis, but constitutes a serious difficulty in closing the defect. He has, therefore, combined direct operation with separation of the pelvic bones at the sacro-iliac joints, afterward enclosing the pelvis in a comprehensive bandage, or suspending the patient in an apparatus in such fashion that the bony defect in front shall be narrowed, if indeed it be not completely obviated. This, of course, is a measure to be carried out in the early years of childhood; in connection with it the bones may even be wired at the symphysis. In fact immediately after the birth of such an infant the attempt should be made to narrow the pelvis, by surrounding that part of the body with a wide rubber band, which shall influence growth without too much interfering with nutrition. Later subcutaneous osteotomy may be done if necessary. At all events, the growing pelvis should be surrounded with an enclosure by which a constant influence may be maintained.
The various plastic operations for this defect have the common purpose of affording a covering, which must unfortunately be without a sphincter to guard the outlet of the cavity. The best that can be accomplished, then, by plastic methods is the formation of a more perfect cavity without affording sphincteric control. A theoretically ideal method would be one which should permit raising
of skin flaps around the margin of the defect, and so turning them in that the skin should vicariate as mucous membrane. These flaps when united, and the anterior wall when thus formed, could be covered by other flaps or by skin grafts; but from these flaps hairs will grow into the bladder. These will become encrusted with urinary salts and an amount of irritation be produced which may become not only intolerable but locally destructive.
In the selection of any plastic method much will depend on the size of the defect and its completeness, the condition of the surrounding wall, and varying complications in the surrounding structures. The general method above suggested will answer especially for the smaller exstrophies. Beck has suggested an excellent device, namely, the dissection from the pubes of the recti muscles, their insertions being severed, and the partial division of the transversalis fascia until the muscles are so mobilized that they can be reflected and united, thus forming an anterior bladder covering. By a second operation these partially formed flaps may be again dissected off from the wall and a complete osteoplastic covering afforded. Practically no operation for extroversion can be completed in one sitting. Frequently repeated efforts have to be made, a little being accomplished at a time. One of the greatest difficulties met with is securing primary union along surfaces more or less bathed or in contact with escaping urine. These flaps, even if united, may separate in a few days as a result of this urinary maceration. Against this there is but little possible provision, save perhaps by catheterizing both ureters, and emptying them into a distinct receptacle.
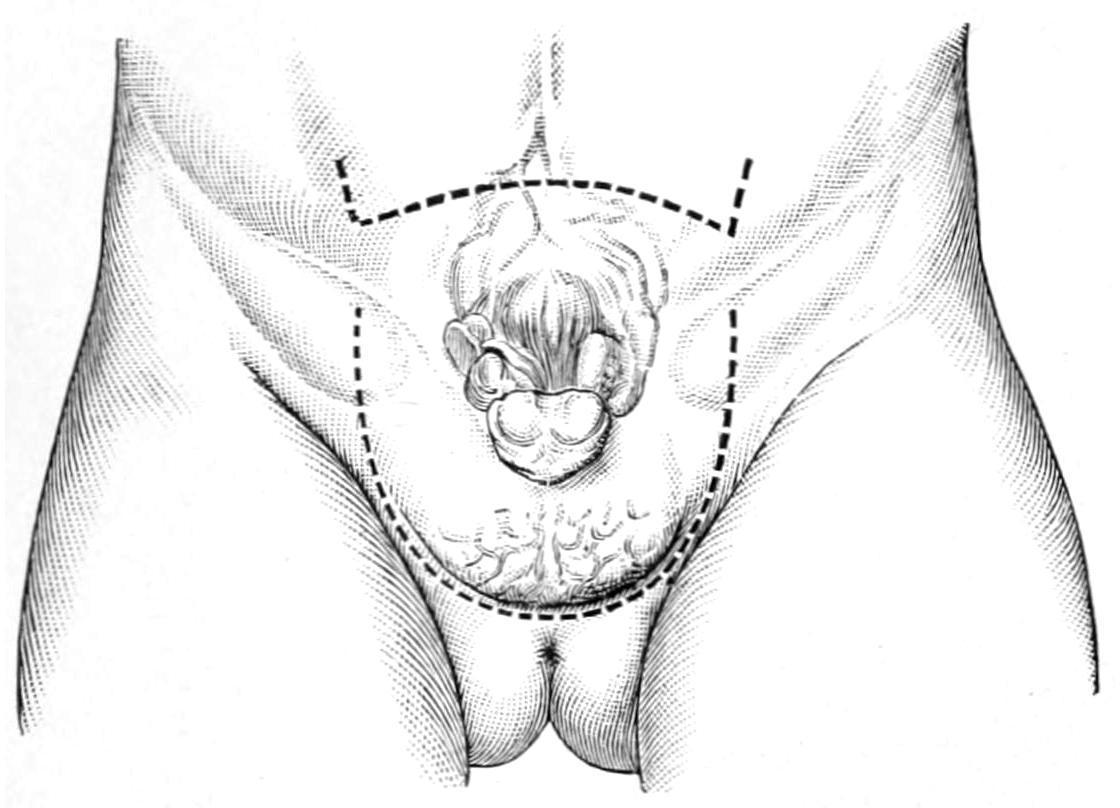
FIG. 649
Roux’s autoplastic method of raising a perineoscrotal flap with which to cover the defect. Lines of incision. (Hartmann.)
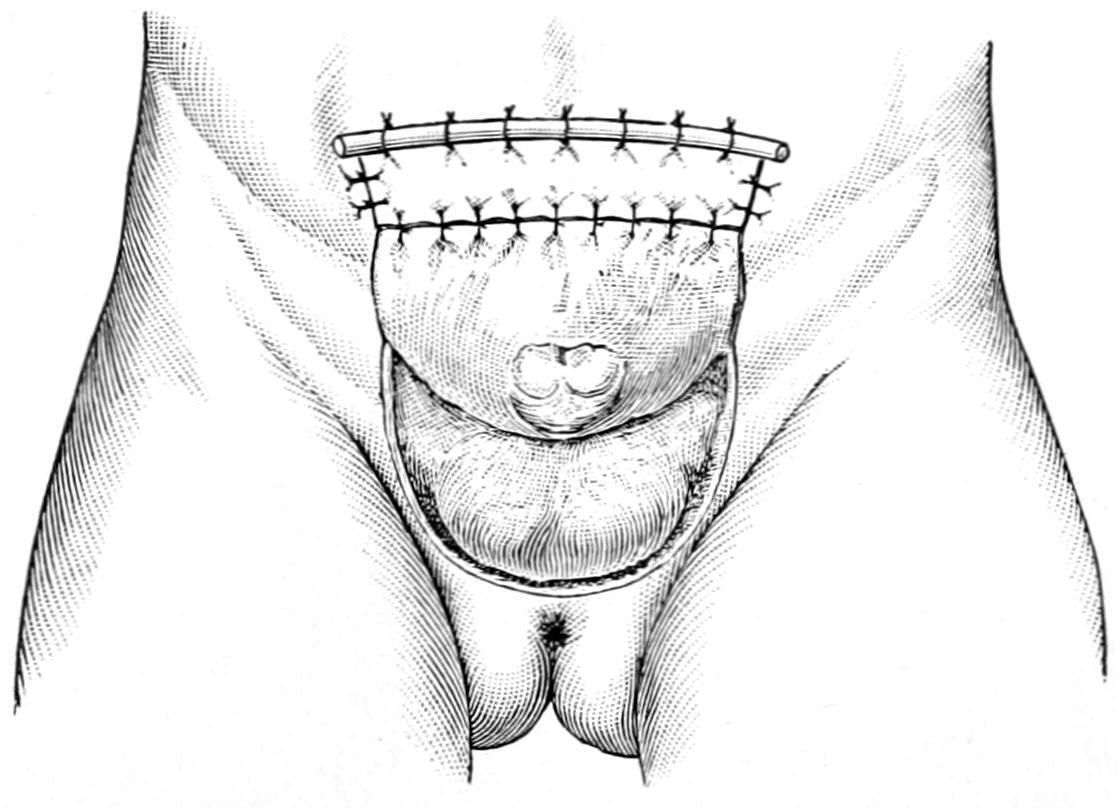
Roux’s autoplastic method of raising a perineoscrotal flap and its fixation. (Hartmann.)
More complicated methods of furnishing a complete cavity have been devised by Rutkowski and Mikulicz, both of whom have suggested to use a small loop of small intestine wherewith to complete the bladder cavity. In each of these methods the abdomen is opened, a loop of bowel brought down, a small portion completely separated by double division, end-to-end anastomosis of the main part being then made, while the separated part is in one method closed at one end, while the other end is fitted over the exposed bladder surfaces as a sort of cap. The method is exceedingly complicated and hazardous, and depends for local success upon a sufficient blood supply to the intestinal loop, which should be carefully ensured by caring for its vessels and mesentery. It has, nevertheless, been successful.
A far simpler method, perhaps the simplest of all, is that of Sonnenburg, which consists in extirpation of the bladder proper, with plastic closure of the opening, while the ureters are carefully separated and sutured into the upper portion of the urethral gutter. This removes all urinary cavity and provides only for continuous escape; but this latter is now provided in an accessible and
convenient place, while the wearing of a urinal permits the achievement of the main purpose of the operation. Sterson operates upon young girls by suturing the loosened ureters to the labia minora, which are then sewed together in the median line, after which a urinal can be worn.[68]
[68] Cantwell has suggested the following method for bladder exstrophy, namely, to pass catheters through a perineal fistula up into the ureters, then to dissect off the bladder wall, bringing it over a small rubber balloon, pushing the whole into position, and uniting the abdominal wall in front.
It has occurred to many operators to more completely divert the urinary stream by displacing the ureters and turning them into the rectum or the sigmoid. Operations for this purpose have been described especially by Maydl (Fig. 650), and by Moynihan, while modifications have been suggested by many others. In practically all of these procedures catheters are first passed into the ureters for their identification and control. Some would dissect out the trigone with both ureters, and, making a sufficiently large opening in the rectum, would transplant it in its entirety within that cavity, closing the opening. Moynihan improved on this by making a vertical incision and entirely dissecting away the bladder, separating it also from the prostate, thus completely isolating it. Then the portion containing the ureters is held upward, while at the bottom of the wound the rectum can either be seen or made visible. The peritoneal reflection is then lifted upward from the front of the rectum, which is opened along its anterior surface by an incision perhaps three inches in length. Into this opening the bladder is placed, being so reflected that its former anterior surface now looks posteriorly. The ureters, instead of passing forward, now pass backward and the catheters contained within them are passed into the rectum and out of the anus. The edge of the bladder and the cut edges of the rectum are carefully sutured, after which the abdominal wound is closed. The sphincter is then stretched, while the catheters remain in the ureters for four or five days.
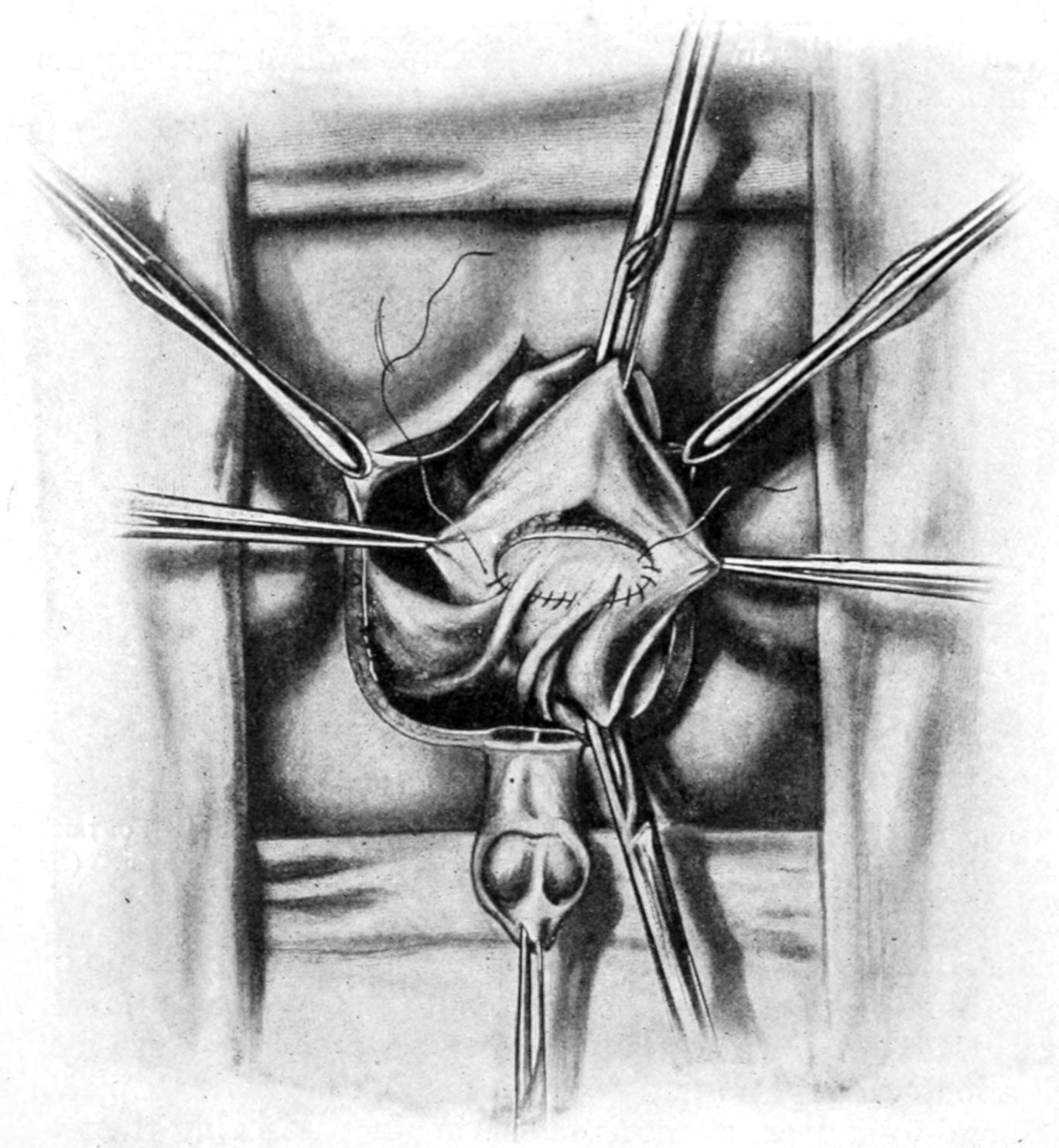
Maydl’s operation; diversion of ureters into rectum. (Hartmann.)
A choice may be made, then, between some such method as that last described or that of Peters, who dissects out the ureters, retaining only a small circular patch of bladder wall, which is folded around the orifice of each, the rest of the bladder being extirpated.
Each ureter, with its button of bladder wall, is then drawn through a small slip in the rectal wall, made large enough to admit it, and the end of the ureter is then left hanging for 1 or 2 Cm. into the rectum. It would probably be better to hold the ureters in place by a stitch rather than run the risk of their retraction; but care must be taken that these stitches make no unnecessary constriction. Others have substituted the sigmoid for the rectum, the procedure being otherwise the same, all of these rectal implantations having for their purpose the utilization of the rectum as a cavity, which may not only contain urine, but retain it reasonably under control. In many respects they would be ideal were it not for the attendant dangers. These are (1) those immediately connected with an operation which is serious, and (2) those connected with secondary infection of the kidneys, which seems to occur in almost all cases, no matter how apparently successful at first.
INJURIES TO THE BLADDER.
Injuries to the bladder proper may be accompanied by those of the parts without, or may be isolated. They divide themselves mainly into ruptures and lacerations, or penetrations directly connecting with the exterior. Among the causes which predispose to rupture and other injuries may be mentioned intoxication, partly because it is often accompanied by overdistention, and partly because of the partial or incomplete insensibility of the patient. Distention, no matter how permitted, is an important predisposing cause. The injuries usually include blows, falls, and crushes, and gunshot or other perforations.
The location of the rent is more commonly in the upper and posterior portion of the bladder i.e., in its weakest part. Such tears may vary from one-half to four inches in length. When accompanyingfracture ofthepelvisthe peritoneum is more likely to be injured.
The most significantsymptomsare a desire to urinate and inability to do more than perhaps expel a few drops of bloody fluid. Of course the passage of any blood or bloody urine will suggest the
occurrence of such an injury. Patients are usually unable to stand upright, and also show a strong tendency to flexion of the thighs. The introduction of a catheter and the withdrawal of bloody urine do not necessarily settle the question as to whether there has been any possible laceration. Some surgeons have taught that normal urine is comparatively harmless and that it is no more likely to produce infection than the catheter used for diagnostic purposes; but this is not safe teaching today. A clean metal instrument is of no more danger than a clean probe under other circumstances. Weir has suggested a valuable test, consisting of removal of all the urine possible, after which a measured quantity of sterile fluid is injected. If on using a catheter again this be all recovered it may be assumed that the bladder is not ruptured, otherwise the contrary. If hours after the injury a catheter be used and no urine secured, this fact will be most suggestive. The cystoscope is usually disappointing, since a bladder so injured cannot often be satisfactorily examined.
Another class of serious injury to the bladder includes the perforations, such as may be effected by gunshot or stab wounds, or, as in one case of my own, where a lad sat down upon an iron spike, about three-quarters of an inch square and nearly six inches in length. The point of the spike entered the anus, and the consequence of the injury was a perforation of the anterior wall of the rectum and the posterior wall of the bladder, with injury to its anterior wall without complete perforation. Prompt operation saved this case, as it will most such instances, although it was shown that a piece of his trousers had been carried into and left in the bladder. I opened the abdomen above the pubis, to be sure that the peritoneum was not injured, and then drained by a tube passed into the anus and out just above the pubis, after removing the piece of cloth. Prompt recovery followed.
The bladder may also be injured by rude manipulation of instruments, especially the metal catheter, by one unaccustomed to using it, or when serious difficulties are offered by prostatic enlargement.
Treatment.
—Diagnosis or even serious suspicion of such injuries to the bladder as above described require either perineal or
abdominal section, the choice of the procedure being based upon circumstances. If there be reason to suspect intraperitoneal extravasation, then the abdomen should be opened, carefully cleaned, the bladder rent sought and sutured, the mucosa being first closed with hardened gut, while the peritoneal aspect may be sutured with silk or thread. The bladder should be drained, at least by retention of a catheter, passed if necessary by perineal section, and the abdomen drained. In the female drainage may be made through the cul-de-sac. If there be urinary extravasation behind the perineum, then perineal section should be made, and the bladder, thus freely opened, should be drained with a sufficiently large tube; while in the female it will probably be sufficient to dilate the urethra and insert a tube of sufficient size. It is not always easy to discover an opening placed posteriorly in the bladder wall, and after a wide exposure, with emptying and cleansing of the pelvis, it may be of great assistance to place the patient in the Trendelenburg position. Under rare circumstances the rent may be so placed as to justify a suprapubic drainage of the bladder.
FOREIGN BODIES IN THE BLADDER.
Foreign bodies other than calculi occur in the bladder in consequence of both accident and of design. The former are, e.g., represented by pieces of broken catheter, while the latter are materials introduced from without in consequence of sexual perversion, during intoxication, or from some other vicious tendency. The latter occur more often in girls and women, the former more often in men. In such a collection of cases as was made by Poulet (Foreign Bodies in Surgery) almost every imaginable object that could be introduced into the bladder is mentioned. Some of these have slipped in accidentally after external manipulation, as in masturbation, and some have been deliberately introduced. Perhaps as common an object as any is the ordinary hairpin. It is the short urethra of women which is made the much more frequent resort for such practices than the long urethra of men, in which latter foreign
bodies are often entangled or arrested before they reach the bladder.
Any object allowed to remain in the bladder will serve as a nidus for the formation of a calculus, which will form in time, and it may result that not until the removal of the calculus and examination of its interior structure will the original foreign body be found.
All objects of this kind should be removed as early as possible after their introduction. Such removal may be easy and accomplished by dilatation of the female urethra, with or without the use of the cystoscope; or the bladder may require to be opened, either above the pubis, through the perineum, or through the vagina, in order that the object in question may be extracted.
INCONTINENCE, RETENTION, AND SUPPRESSION OF URINE.
Students often confuse not only terms but conditions, and it is necessary to be accurate in teaching regarding these subjects. Suppressionofurineis purely a matter of cessation of renal function, and has nothing to do with the bladder. Retention of urine, on the other hand, has nothing to do with the kidneys, but is purely a bladder affair. It may be due to spasm of the bladder outlet, or to its obstruction by calculi, other foreign body, or by prostatic enlargement, or it may be a consequence of paralysis of bladder muscle. Such retention is the inevitable consequence of fracture of the spine, since paraplegia is to be expected in such cases, and the condition is to be atoned for by careful and regular catheterization. Retention, again, is occasionally seen in hysterical patients. It furnishes the distressing and sometimes permanent or even fatal consequences of prostatic enlargement in old men. No matter how produced,it must berelieved, for urine tends to accumulate and to distend the bladder, which will finally burst unless the difficulty be sufficiently overcome so that urine may in some way escape. Distention of the bladder under these circumstances is recognized by the formation of a rapidly increasing tumor, which finally rises to the level of the umbilicus, fluctuates, and is accompanied or not by pain
according to the nature of the cause of retention. In paralytic cases there will be little or no pain. In obstructive cases it will be agonizing.
By natural efforts final rupture of the bladder is usually prevented, as after a certain degree of distention has been attained urine begins to escape drop by drop. This is simply an expression of an overflow, and is not to be confused with incontinence in the proper sense of the term. It may be spoken of as stillicidium, due to retention. The young and indifferent practitioner may mistake this escape of urine for incontinence, which would be a most serious error. Under any circumstances, when such a condition may possibly occur, the lower abdomen should be palpated, when the presence of a distended bladder should be instantly recognized. The first indication is for its prompt relief by the use of the catheter, while the necessary catheterization should be done with the usual precautions. When the passage of an ordinary instrument is made difficult or impossible the cause of the retention is usually thereby revealed, and may be shown to be so serious as to necessitate further operative procedures.
When the bladder is distended and no catheter can be introduced it is advisable to aspirate, the aspirating needle being introduced through the sterilized skin just above the pubis, its point directed toward the centre of the mass formed by the distended bladder. Repeated aspiration may be necessary, and it has been suggested to make more or less permanent use of such a tube or hollow needle. At present no surgeon would continue this as a permanent measure, but simply as a temporary relief, even if repetition be necessary, until more radical procedure can be carried out. Whether this be the removal of a foreign body or calculus, or of an enlarged prostate, it is indicated just the same, the only exception to this statement being those cases already too seriously involved to justify more than perineal section (cystotomy for drainage). Retention ofurine,then, isalwaysapreventablecondition,anditscontinuanceisinexcusable.
Incontinenceimplies a paralytic condition, usually of the expulsive muscles, but sometimes of the sphincter apparatus in either sex, by which urinary control is lost and urine escapes involuntarily. It may
be a temporary and occasional phenomenon, occurring under the influence of strong excitement or during sleep, especially in children, or it may be due to spinal disease or traumatisms, with paralysis of the lower segments of the cord and nerves given off from them. When originating in the latter way it is usually a hopeless condition, but nocturnalincontinenceof children, or even of adults, or that due to hysterical or other neurotic conditions, may usually be benefited. For this purpose the surgeon should search for the cause from which the reflex proceeds. This may be extreme acidity of urine, the irritation of a tight prepuce in either sex, the presence of worms, intestinal disturbances, or any one of a great number of possible causes of disturbance of nerve control. Some of them permit of surgical relief; others require simpler measures. Children thus suffering should be given no fluid late in the evening, but should be made to empty the bladder before retiring, and perhaps be aroused once or twice through the night for the same purpose. In all cases the urine should be examined and hyperacidity overcome. All forms of genital excitement should be obviated. In the adolescent and in adults thus annoyed, and in the insane, it has been shown to be of great benefit to make a few intraspinal injections of sterile salt solution, as for local anesthetic purposes, a little cerebrospinal fluid being first withdrawn, and then from 2 to 10 or 15 Cc. of the solution being introduced. This seems to have been empirically suggested by a French surgeon, but has been found of value by Valentine and others, including the writer.
The above forms of incontinence are to be distinguished from intense irritability of the bladder, with frequent calls to empty it, which accompany many such conditions as cystitis, tuberculosis, tumors, calculi, and the like. This is the extreme irritability of local disease rather than true incontinence. But there is also a form, in women, characterized by falling away of the urethra and neck of the bladder from the pubis, due usually to injuries received during parturition, with consequent sacculation or dilatation of the urethra and formation of a cystocele. (Dudley.) This may also be associated with other results of perineal laceration. Here loss of urine is not constant, but occasional or frequent. For its treatment the following
methods have been suggested: the injection of paraffin; partial torsion of the urethra (Gersuny), i. e., a partial dissection of the urethra and revolution upon its own axis, with subsequent suture, by which incontinence may be overcome, but at the possible risk of sloughing. Finally, Dudley has proposed the method of advancement of the urethra. He makes a horseshoe denudation, between the meatus and the clitoris, down on either side of the urethra, and nearly its entire length. Its anterior end is then loosened sufficiently so that the meatus can be drawn forward and secured below the clitoris by two sutures. The balance of the wound is then closed, the effect of the operation being to replace and retain the urethra and prevent its sagging. Other surgical treatment, as for cystocele, laceration, etc., may be added as needed.
CYSTITIS.
The condition of true cystitis arises invariably either from the irritation of a foreign body or the presence of bacteria; the former need not necessarily be large, and minute and irritating crystals are often sufficient to produce at least some of its features. Sooner or later, however, the germ element enters, and from that time on cystitis is a bacterial infection. Furthermore this infection is usually secondary, rarely if ever primary, and may come from without or within. Thus it may be the consequence of the introduction of unclean instruments; is a very frequent consequence of gonorrhea, including all forms of urethritis; or may be the result of local tuberculous processes or those travelling downward from the kidneys; or, again, of more general toxic or septic conditions, such as typhoid and other infectious fevers. Certain conditions predispose, such as the presence of calculi or the occurrence of traumatism. Again, a bladder weakened by overdistention or paralysis, as in cases of spinal injury, loses its natural resisting power and succumbs to infection abnormally easily. It should be emphasized that the absolutely healthy bladder wall is resistant to all germ activity, but this resistance is easily lost or modified in the presence of disease, either close by or distant. A bladder whose normal shape has been
greatly changed by enlargement of the prostate is again rendered not only unhealthy, but incapable of acting normally. It becomes, therefore, easily infected, and cystitis is a frequent accompaniment ofprostatichypertrophy. FIG. 651
Internal appearance of bladder in some cases of inveterate cystitis; mucosa sacculated by columns of hypertrophied tissue. (Launois.)
Symptoms.
—The cardinal symptoms of cystitis are three in number, i. e., pain, frequency of micturition, and pyuria, the latter being the consequence of changes in the urine, as well as in the bladder wall, while the pain and the thamuria are expressions of irritation, especially of the base of the bladder and the posterior urethra. In fact, all the more violent expressions of cystitis are found at the lower part of the bladder rather than in its upper portion. Obviously, then, irritation of adjoining organs is more easily
accounted for, e. g., of the urethra, the seminal vesicles, the prostate, and the lower ends of the ureters.
The painmay be severe, and is especially complained of with each act of urination. It is referred not only to the region of the bladder proper, but along the urethra to the end of the penis in the male, and down the thighs in both sexes. With frequency of urination there is also distressing urgency, so that once the necessity be felt nothing can restrain the promptness of the act. In fact so powerful is the expulsive tendency that the tenesmus affects not only the bladder but often the rectum, while the feeling or desire to urinate continues after the bladder has been emptied of its last drop, even for several minutes, and may cause the patient to sit in agony for some time. The distress produced in acute cases of cystitis is excessive, and sedatives and anodynes constitute no small part of the treatment.
The amount of puscontained in the urine will vary with the degree of acuteness and the stage of the disease. At first it is but slight, but rapidly increases, until the urine may contain thick mucus and pus up to one-third or more of its volume. Finally bloodmay appear, by whose appearance a serious degree of inflammation is betokened.
Later, at a variable date, the putrefactive element is introduced; and when the urine begins to smell of ammonia—i. e., when ammoniacal decomposition has once begun—the bladder is thereby the more irritated and the case made still worse.
No vesical mucosa left suffering from such acute inflammation will remain unaffected in its tissue elements, but will rapidly become more or less thickened. In fact the entire bladder wall undergoes a process of thickening, from hypertrophy of its inner and its muscular or middle coats, the latter due to extra activity in consequence of the constant tenesmus. There results in time a marked eccentric hypertrophy, whose result is really a contraction of the bladder cavity and a distortion of its lining. Under these circumstances, also, the mucosa becomes sacculated, and numerous little pockets, which may contain decomposing urine, serve to complicate the situation; while, finally, more or less incrustationor calculousdegenerationand implantation modify the character of the mucous coat. For all these changes to occur requires time, but their combined effect is such
thickening and contraction of the bladder as to permanently alter it and lead to a final concentrichypertrophy.
Tuberculous Cystitis.
—The picture presented by tuberculous disease of the vesical mucosa is, in the beginning, one of miliary or disseminated involvement; but later, when ulcerative changes have taken place, the end results are scarcely different from those rehearsed above, save that the ulcerative element is more predominant, and there is great probability of involvement of the ureters or of any of the adjoining organs. As conditions do not essentially vary, neither do symptoms, and a diagnosis of tuberculous cystitis often must, in the early stages, be reached by a process of exclusion, corroborated perhaps by the cystoscope.
Postoperative Cystitis.
—A different clinical type of irritation, or mildly infective cystitis, is known to be a sequel of certain operations, not alone those upon the pelvis. In the majority of cases it occurs when catheterization has been required, the first event being urinary retention, by which the bladder mucosa must be more or less disturbed. It may be perhaps accounted for by the fact that the urethra is practically never free from germs, which, in that canal, seem to be innocent, but which, carried upward into an irritated bladder may excite serious inflammation. These cases are perhaps more frequent after pelvic operations for cancer. There seems, however, no doubt but that repeated catheterization for several days lowers bladder resistance.
Treatment.
—When the occurrence of cystitis is imminent prophylactic or preventive treatment is recommended. This should consist in administration of large quantities of fluid, with urinary antiseptics, in lavage of the bladder itself, and in reliable antiseptic precautions in catheterization. Thus to operate upon a bladder which has long held seriously infected or decomposed urine, without previously cleansing it as much as possible, is simply to invite further trouble.
The medicinal treatment of cystitis, on which we mainly rely, consists in dilution of the urine by large amounts of fluid ingested, in overcoming hyperacidity by the administration of alkalies, and in combating putrefactive conditions, so far as possible, by antiseptics
which are eliminated through the kidneys. Balsams have been long held in great repute; but remedies like urotropin and other synthetic compounds have taken their place. Of them all, and especially in the presence of ammoniacal urine, urotropin and the alkaline salts of benzoic acid seem most reliable. Excessive irritability may be overcome by local measures, such as frequent hot rectal douches, hot sitz baths; by quieting irritation of the genitospinal centres by administration, e. g., of cannabis indica, in doses pushed to the physiological limit; by local anodynes, as by opium suppositories, or in extreme cases by general anodynes like morphine.
Theoretically a seriously infected bladder should be washed out and cleansed as any other pus cavity, but when so inflamed the bladder becomes so intolerant and exquisitely irritable that the mere act of washing can only with difficulty be borne by the patient. Retention of a catheter, which might be advisable under most circumstances, may also be impossible for the same reason. The condition of a patient under extremes of this kind is pitiable, and resort to general anodynes unavoidable. Still it is possible with patience and the use of selected drugs to gradually allay even a most acute cystitis. Confinement in bed and an almost fluid diet are also necessary features of treatment.
If the introduction of an instrument can be borne it may be possible to leave in the bladder some soothing solution after it has been washed, such as a mild cocaine solution containing a little morphine, or olive oil containing orthoform, or a mild preparation of ichthyol. Even if these be retained but for a short time they will usually afford relief.
Finally in severe forms of cystitis the bladder may beopened for the purpose of giving it physiological rest, selecting either the suprapubic or the median perineal route. The relief thus afforded is usually gratifying, while drainage may be maintained until the local treatment has been sufficiently effective to permit either spontaneous closure of the drainage opening or its repair by suture. This measure is known as cystostomyforthereliefofcystitis.
Obviously if cystitis be due to the presence of any foreign body its treatment becomes necessarily surgical, the same being true of
VESICAL CALCULUS.
In the urinary bladder as well as in the gall-bladder mineral elements held in solution by the contained fluids are precipitated, the consequence being the formation of calculi or stones in the bladder, which vary in size from the smallest concretions to those weighing many ounces, and in number from one to scores, a large proportion of these representing original concretions passed down from the kidneys, i. e., minute renal calculi. Every calculus has a nucleus, and in many instances this may be a clot, or clump of cells encrusted with salts, which have formed within the bladder and not come down from above. Such foreign bodies will become the nidus for a calculus, while in vesical calculi are frequently found pieces of catheter, of straw, chewing-gum, hairpins, and the like, which have been introduced from without. These stones are constituted mainly of the ordinary urinary salts, i. e., phosphates, urates, or oxalates, deposited as described above. Much more rarely cystin and xanthin are found. Instead of urates crystallized uricacidwill be occasionally seen. The oxalates are mostly those of calcium, while the phosphates are those of calcium, magnesium, or ammonium, more or less combined. The first requisite for a calculus is a nidus, the second the deposition of one or more of these salts. Calculi are sometimes composite in structure, some having a uric or urate nucleus becoming later encrusted with phosphates. The oxalic calculi are exceedingly hard and usually rough, being often spoken of as mulberry. They rarely attain large size. The rapidly forming phosphatic calculi are often so small as to disintegrate or break in the process of removal. Thus there may be great differences in density of these stones. Their formation is particularly favored by retention of alkaline urine, as in many cases of prostatic enlargement.
Symptoms. those forms due to or connected with hypertrophy of the prostate. It is impossible to accomplish a cure here until the mechanical difficulty is first overcome.
—Discomforts and symptoms produced by bladder stone depend upon their size, number, roughness, movability, and location. The larger and rougher stones, which are more or less easily moved inside a tender and irritable bladder, will cause a large amount of discomfort and actual pain, while a small calculus, which may be formed within a pocket or become encysted at some distance from the urethral opening may remain unnoticed. The indications of calculi are essentially those of cystitis, pain, frequency of urination, and pyuria, sometimes with hematuria. The pain is local and referred, especially along the urethra, to the glans in the male, and is often aggravated by the final expulsive movements of the bladder at the termination of urination. Local discomfort is aggravated by active exercise. Reflex pains have been known in distant parts of the body. The frequency of urination is increased by exposure to cold or by activity. Pyuria and hematuria do not differ from those of noncalculous cystitis. A most significant feature is sudden stoppage of theurinarystream, with more or less pain. Statements to this effect, especially if accompanied by a history of renal calculi in time past, are most suggestive.
Unless, however, particles of calcareous material have been passed the positive diagnosis of calculus rests upon its detection by examination, either with a stone searcher or with the cystoscope. The former is essentially a short-beaked, light sound, which may be more easily manipulated after introduction within the bladder. In using it the same precautions are taken as for catheterization or sounding, while the deep urethra may be made less sensitive by a cocaine solution. The instrument is introduced exactly as is a sound, and its beak is carried completely into the bladder. Sometimes even before this has been accomplished will be noted the rough, grating sensation which indicates contact with a stone. At other times it is only after considerable search that a small stone is “touched.” A stone easily found is within the possibilities of unskilled manipulation, but to accurately examine a bladder, especially behind a large prostate, is a fine art. For this purpose the bladder should be partially distended with fluid, the patient should be in the horizontal position, and the stone searcher so manipulated that its beak may
be made to traverse every portion of the lower part of the bladder and to come into contact with its wall, for only in this way can an encysted calculus be discovered. The beak must, moreover, be rotated so as to be carried down into the pocket behind an enlarged prostate, as in such pockets many calculi nestle. Some stones are felt even in introducing a soft catheter; others are discovered only after such manipulation as the above. Nothing but necrosed bone or a foreign body can convey to the metal instrument, and through it to the finger, the peculiar sensation produced by contact with a stone. By attaching an auscultatory tube to the instrument a characteristic sound may also be heard.
With the cystoscope in the hands of an expert it is possible to orient one’s self definitely concerning the size and location of a calculus, but much information can also be obtained by the use of the ordinary searcher.
It has occasionally happened that calculi have been discovered by accident, either during a suprapubic or some other pelvic operation. The presence of vesical calculus being established, there is but one rational treatment, i. e., its removal. It remains, then, only to select the method of operation and to perform it. Vesical calculi are removed by two general kinds of operations: by crushingandevacuationoffragmentsthroughthenaturalpassages, or by a cuttingoperation andextractionentire. The former is known as lithotrity, or, as now performed in one sitting, litholapaxy, and the other as lithotomy, which may be performed either above the pubis, through the perineum, through the vagina, or through the rectum. Each method has certain obvious advantages. Thus in favor of crushingthere is freedom from an open wound, with its dangers of infection and of hemorrhage, while it appeals to the sentiment of those patients who “dread the knife.” One objection to it is that even when performed with skill assurance cannot be given that the bladder shall be freed from all calcareous particles, one of which may, by remaining, serve as a nidus for another calculus. In favorof thecuttingoperationsare their brevity, i.e., the celerity with which they may be performed, the relief afforded by drainage, which can be carried out through the lithotomy wound, and which is often
Treatment.
indicated in bladders that have been long tortured by the presence of calculi; while, finally, their simplicity, at least in most instances, makes lithotomy attractive to the operator of limited ability. It may be added that certain calculi, especially of the oxalic type, are so dense and resistant that even when secured in the grasp of an instrument they can scarcely be crushed. It may be urged also that septic urine is just as harmful in a bladder whose mucous membrane has been slightly injured here and there in the process of crushing as in one which has been more or less opened by a lithotomy.
Between cutting methods choice varies also according to the taste and views of various operators, as well as the nature of the case. When the prostate is large a suprapubic operation was held the simpler for the removal of calculus, and this earlier teaching is not abandoned. In the young the urethra is small and the bladder lies high in the pelvis, and both these conditions favor the suprapubic method. Again it enjoys repute because there is no danger of injury to the prostatic urethra or the seminal ducts or vesicles, and because it leaves the genital apparatus absolutely untouched. It is also free of possibility of harm to the rectum, which was by no means unknown in the hands of the older operators who resorted to the perineal route. But the removal of a large stone by the suprapubic route entails an opening of considerable size, and it is not unlikely that a large calculus may need to be fragmented and removed in pieces rather than leave a large opening at a point where urinary fistulas would likely ensue. It will be seen, then, that even lithotomy is not always to be performed without crushing of the calculus.
Of the perineal routes only two are in vogue today, the median and the lateral. The median is resorted to for stones of moderate dimensions, while the lateral will be required for large calculi. The vaginal route is often selected in women, although, rather than make an extensive opening between the bladder and the vagina, it will probably be easier and better to dilate the urethra, and, through it, crush a calculus which, in the female, could thus be made more accessible than in the male. Therefore in the female the suprapubic route or a litholapaxy is usually adopted. The operation through the rectum has been long since abandoned.
After a calculus has been removed by crushing a self-retaining catheter should be inserted, for at least a day or two, and the bladder washed, while at the same time treatment for the cystitis, which is still present, should not be discontinued. After opening the bladder the wound is drained for at least a day or two. Drainage has this disadvantage, that if long continued it leaves a urinary fistula, often slow to close, but a metal, glass, or hard or soft rubber tube may be placed in a median perineal opening, around which should be packed gauze to check oozing, and left in this condition for two or three days. Usually within a week after its removal the deep sphincters have recovered their retentive power, and the patient can retain urine for some time, while generally within two weeks the entire wound is closed. In all these cases a sound or bougie should be passed at suitable intervals for the purpose of preventing stricture formation in the deep urethra at the site of the operation.
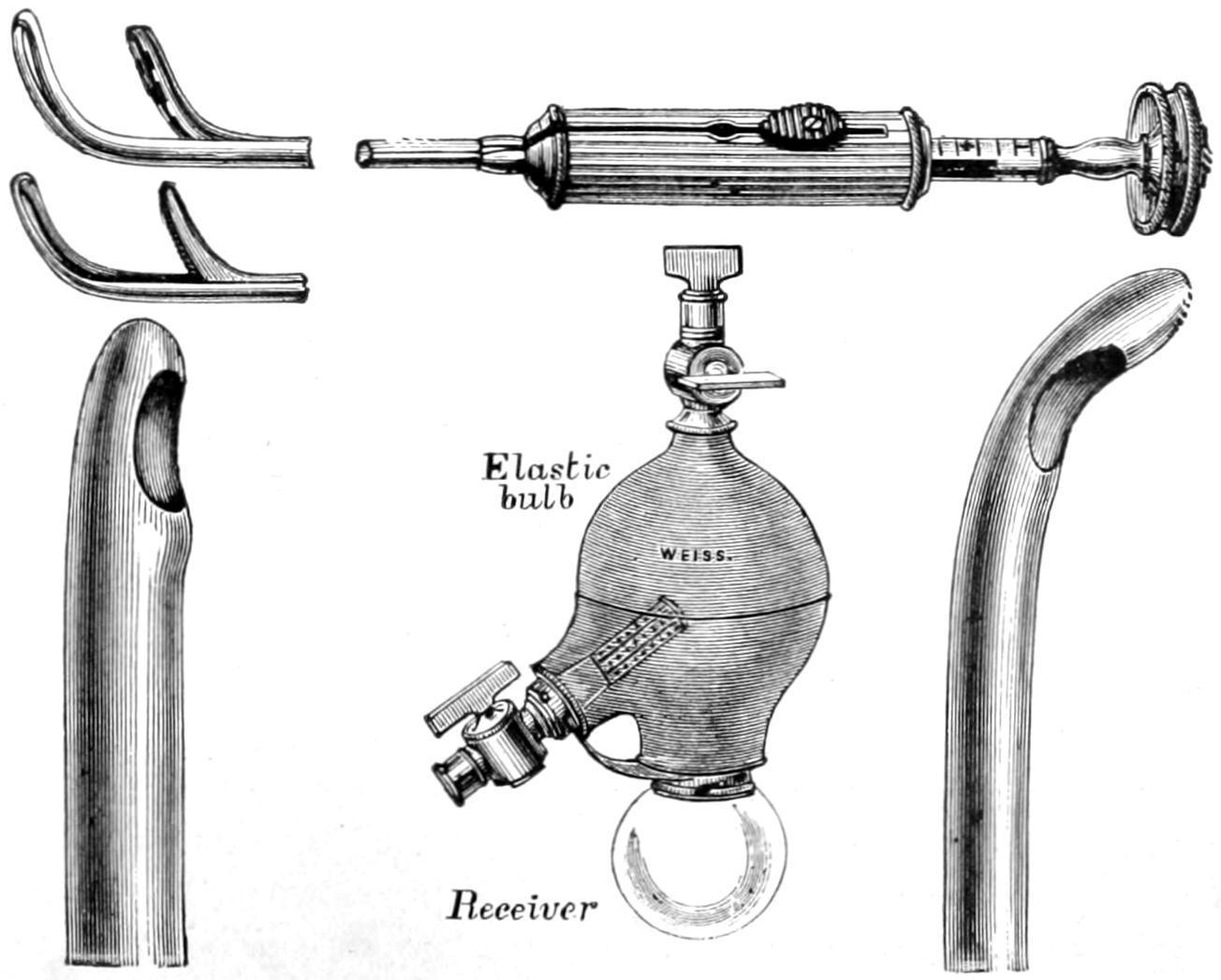
Litholapaxy is performed by first crushing the stone between the beaks of an instrument known as the lithotrite, which is constructed in various forms, yet all conforming to one type, which is introduced into the bladder through the urethra, after which its blades are separated and manipulated until the stone is felt to be entangled or secured between them. By a device at the handle the blades are then locked, and screw power exerted, also from the handle, by which the blades are forced together and the stone between them more or less broken (Figs. 652 and 653). By repetition of this process each fragment is seized separately and crushed until the bladder contains more or less debris resulting from the manipulation. The lithotrite is then removed and a washing tube or catheter of large dimension inserted, and connected with a so-called washing bottle, which is compressible and permits a stream of water to be violently thrown into the bladder, thus stirring up the fragments and particles, and which is an instant later withdrawn by suction in such a way as to carry them with it. Escaping into the washing bottle they drop by gravity into a glass receptacle at its base, where they become at once visible. This process is repeated until everything has been washed out of the bladder which will come. The lithotrite is then substituted and the maneuver repeated, and as many times as
may seem desirable. In this way calculi, especially soft ones of large size, may be disintegrated and removed in small fragments. The final test of success is failure to aspirate any more particles or to discover them with the cystoscope (Fig. 654). The time consumed in the operation will depend on the operator’s skill and the size or hardness of the stone. It is frequently performed under local anesthesia, the bladder being injected with a weak cocaine solution, or under spinal anesthesia.
Lithotomy, by either of the above methods, is performed by utilizing a grooved sound known as a staff, which is first inserted into the bladder, and serves not merely the purpose of a grooved director, but to indicate the course of the urethra.
For the suprapubic operation the staff is passed deeply, and its handle depressed between the thighs, so that the end of the instrument rises behind the pubis and carries the bladder up toward the surface. A median incision above the pubis permits access between the recti muscles to the prevesical space (space of Retzius), which is more or less filled with fatty and connective tissue. If the bladder has been previously distended with fluid and elevated on the point of the staff, there is but little danger of wounding the peritoneum, although its reflection may be sought and carried out of harm’s way. It is a convenience to pass a silk suture with a stout, full-curved needle through the bladder wall after it has been exposed, on either side of the point of the staff which elevates it, and to pass this through in such a way as to have thus a double loop, or two retractors, by which it may be more conveniently manipulated after it has been opened and would otherwise collapse. The bladder should be opened upon the point of the staff, whose groove may then serve as a guide in still further nicking or incising it, the silk sutures on each side preventing it from collapsing as it otherwise would after the gush of escaping fluid. The surgeon should now endeavor so far as possible to dilate rather than to merely cut this opening, and thus give it a size sufficient to permit the introduction of the finger, by which intravesical exploration and orientation are effected. Calculi having been identified and located, suitable forceps are then introduced, and with them the stone or
stones seized and withdrawn through the opening, which may be stretched still farther for the purpose unless their size make it advisable to crush them and remove them in fragments.
Method of seizing the stone behind the prostate.
Ordinary position in seizing the stone.
Bigelow’s lithotrites, catheters, and evacuator.
This is suprapubic cystotomy or epicystostomy, according to the purpose for which it is intended. It serves not only for removal of calculi but for extirpation of tumors, or enlarged prostates, and perhaps for permanent drainage. By the silk loops at first introduced the bladder wall may be attached to the abdominal wound, while other stitches may be added to any desired extent. In most instances it is desirable to reduce the opening, for which purpose buried and superficial sutures may be used. As leakage, however, may produce infection it is customary either to provide for drainage by insertion of a catheter through the urethra, or by the implacement of a small tube, whose lower extremity shall reach the
base of the bladder and serve for drainage, which latter may be made more effective by siphonage.
PERINEAL LITHOTOMY.
Perinealsectionfor exploration, drainage, or stricture is practically accomplished as follows: The patient is first placed in the so-called lithotomy position, i. e., upon the back with the limbs flexed and knees parted, the feet or legs being held either by assistants or in suitable leg holders upon the operating table. This is the position in which nearly all perineal operations in both sexes are made.
A grooved staff, with large curve and long beak, is introduced into the bladder, and not only held in the vertical position by an assistant, but in such a manner as to make its curve bulge the perineum as much as possible toward the operator. The rectum, which should have been previously thoroughly cleaned, may be utilized for identification or for necessary assistance during the operation. The scrotum is held up out of the way by the assistant who holds the staff. The perineum being thus put upon the stretch may be most quickly opened by a straight, sharp-pointed bistoury, which is inserted a little posteriorly to the scrotal junction, its point driven through the tissues and made to engage in the groove of the staff, from which it should not escape until finally withdrawn. As the instrument is pushed backward the handle is depressed; a triangular-shaped opening is thereby effected, whose apex is in the membranous urethra and whose base occupies the raphé of the perineum, to the extent of perhaps one and a half inches. The entire incision may be made with one effort. Its effect is to open the membranous urethra. Into the groove of the staff, the knife being withdrawn, may be introduced either a species of grooved director or the finger-nail of the index finger, which may be passed backward and made to enter the prostatic urethra, while at the same time the staff is withdrawn. If the prostatic urethra be constricted it will be difficult to enter the bladder with the finger, otherwise it will readily yield to pressure, and it is thus possible to enter the bladder within a few seconds after the first incision is begun (Fig. 655).
It is preferable in all these cases to have first washed out the bladder, and then to have filled it with a mild antiseptic solution. This will escape instantly an outlet is made from below. If there is a small calculus within the bladder the effect of the stream will be to carry it toward this outlet, where it is identified by the finger.
The prostatic urethra will bear a considerable amount of gradual dilatation, which will make it more than easily accommodate an ordinary finger. In this way a sufficient channel is made, through which forceps may be introduced and calculi of small or medium size withdrawn. They should be seized as carefully as possible within the proper grasp of these instruments, so that a minimum of laceration may be effected as they are extracted. A small calculus will be easily removed; a large and soft one may crumble in consequence of the pressure made upon it during its extraction. In this event the fragments should be separately removed, the bladder then repeatedly washed out, and the finger finally used to make sure that no particles remain.
Whether one stone or several be present the opportunities for the purpose of their extraction afforded by this median operation are the same. The bladder having been emptied and washed out a selfretaining drainage tube, or a hard rubber or metal perineal tube should be inserted, with such gauze packing around it as may be necessary for its retention and for the checking of hemorrhage. The intent of the tube is a double one, it being intended to serve for easy drainage and for gentle pressure. Sometimes the prostate is more or less torn in the process of dilatation, and in this case will bleed more freely than is comfortable. Such oozing may be checked by plugging gauze around the drainage tube.
Lateral lithotomy may be combined with median section, by deliberately passing a blunt bistoury into the prostatic urethra, and making with it an incision in the prostatic substance, the cut being directed toward a point midway between the anus and the ischiatic tuberosity, and carried to a depth of one-half or three-quarters of an inch. This affords a much larger opening through which to remove larger calculi. Obviously it will bleed more freely and will usually require packing. The old lateral method was to begin the external
incision at a point, in the middle line, a little behind the scrotum, and direct it for one and a half or two inches backward and outward to a point between the tuberosity and the anus. The incision was then deepened through the perineal fascia until the index finger-nail of the left hand could identify the staff within the urethra, after which the urethra was opened at this point (i. e., just behind the bulb), when the knife was again introduced and made to divide the prostate obliquely as above. In this way the membranous urethra and lateral aspect of the prostate were divided to the requisite depth. If such incision be extended too far backward and outward the internal pudic artery might be divided, which would at least be awkward and necessitate ligature, and this would be somewhat difficult because it would require further division of tissues.