No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or any information storage and retrieval system, without permission in writing from the publisher. Details on how to seek permission, further information about the Publisher’s permissions policies and our arrangements with organizations such as the Copyright Clearance Center and the Copyright Licensing Agency, can be found at our website: www.elsevier.com/permissions
This book and the individual contributions contained in it are protected under copyright by the Publisher (other than as may be noted herein).
Chapters written by Dr H. Nida Sen are in the public domain.
Notices
Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds or experiments described herein. Because of rapid advances in the medical sciences, in particular, independent verification of diagnoses and drug dosages should be made. To the fullest extent of the law, no responsibility is assumed by Elsevier, authors, editors or contributors for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, products, instructions, or ideas contained in the material herein.
Library of Congress Control Number: 2020952350
ISBN: 9780323480147
Content Strategist: Kayla Wolfe
Content Development Specialist: Louise Cook
Project Manager: Julie Taylor
Design: Patrick Ferguson
Illustration Manager: Narayanan Ramakrishnan
Marketing Manager: Kate Bresnahan
Printed in India
Foreword by Rubens Belfort Jr, vi Preface to the Fifth Edition, vii
PART 1 Fundamentals
1 Elements of the Immune System and Concepts of Intraocular Inflammatory Disease Pathogenesis, 1
H. Nida Sen
PART 2 Diagnosis
2 Medical History in the Patient with Uveitis, 29
Scott M. Whitcup
3 Clinical Examination of the Patient with Uveitis, 31
Scott M. Whitcup
4 Development of a Differential Diagnosis, 42
Scott M. Whitcup
5 Diagnostic Testing and Imaging, 50
Scott M. Whitcup
6 Optical Coherence Tomography in Uveitis, 63
Scott M. Whitcup
7 Evidence-Based Medicine in Uveitis, 69
Scott M. Whitcup
PART 3 Medical Therapy and Surgical Intervention
8 Approaches to Medical Therapy, 73
H. Nida Sen
9 Role of Surgery in the Patient with Uveitis, 103 H. Nida Sen
PART 4 Infectious Uveitic Conditions
10 Bacterial and Fungal Diseases, 116
Scott M. Whitcup
11 Spirochetal Diseases, 127
Scott M. Whitcup
12 Acquired Immunodeficiency Syndrome, 145
Scott M. Whitcup
13 Acute Retinal Necrosis and Progressive Outer Retinal Necrosis, 160
Scott M. Whitcup
14 Other Viral Diseases, 169
Scott M. Whitcup
15 Ocular Toxoplasmosis, 179
H. Nida Sen
16 Ocular Histoplasmosis, 197
H. Nida Sen
17 Ocular Toxocariasis, 206
Scott M. Whitcup
18 Onchocerciasis and Other Parasitic Diseases, 215
Alan G. Palestine
19 Postsurgical Uveitis, 229
Alan G. Palestine
PART 5 Noninfectious Uveitic Conditions
20 Anterior Uveitis, 237
Scott M. Whitcup
21 Scleritis, 252
Scott M. Whitcup
22 Intermediate Uveitis, 259
Scott M. Whitcup
23 Sarcoidosis, 269
Scott M. Whitcup
24 Sympathetic Ophthalmia, 282
H. Nida Sen
25 Vogt-Koyanagi-Harada Syndrome, 296
H. Nida Sen
26 Birdshot Chorioretinopathy, 310
H. Nida Sen
27 Behçet Disease, 326
H. Nida Sen
28 Retinal Vasculitis, 350
Alan G. Palestine
29 Serpiginous Choroiditis, 368
Scott M. Whitcup
30 White-Dot Syndromes, 378
Alan G. Palestine
31 Masquerade Syndromes, 395
Scott M. Whitcup
Appendix, 408 Index, 410
FOREWORD
Our knowledge of basic immunology, the human immune response, and how to either augment or inhibit this response has exploded over the last decade. These advances have led to changes in the way we assess and treat patients with uveitis. In addition to furthering our understanding of the pathogenesis of a large number of uveitis conditions, we have been challenged with new infectious causes of uveitis diseases caused by viruses including the Zika virus, Ebola virus, and West Nile virus. Finally, advances in diagnostic testing and imaging have changed the way we diagnose uveitis and monitor our patients’ response to therapy. It is the perfect time for a new edition of Whitcup and Nussenblatt’s Uveitis: Fundamentals and Clinical Practice. I was very happy to see Dr. Whitcup take on the leadership role for the new 5th edition, and for ensuring that this important book continues to be available to clinicians around the world.
This textbook remains the go-to guide for diagnosing and managing patients with uveitis. It is both comprehensive, covering all the key topics related to uveitis, but also practical, readable, and useful to both ophthalmologists and other clinicians managing patients with inflammatory eye diseases. I have known and worked closely with both Dr. Whitcup and Dr. Nussenblatt for over 40 years, and spent time seeing patients with both of them for many years. Their organized and thoughtful approach to diagnosing, treating, and managing patients with uveitis is clearly elucidated in this book. Although Dr. Nussenblatt was not involved with this edition of the book, having passed away suddenly in 2016, his imprint on the book continues.
Part 1 of the book provides an overview of the basic science of ocular immunology with specifics on the role of the immune response on disease pathogenesis. It also discusses advances in our understanding of ocular inflammation and how these advances have led to novel therapies for autoimmune and inflammatory disease.
Part 2 of the book concentrates on the diagnosis of uveitis. As expected, the section discusses advances in testing such as the use of polymerase chain reaction (PCR) in diagnosing infectious causes of uveitis. However, an important part of this section is a practical approach to diagnosis by detailing tips on obtaining the medical history, examining the uveitis patient, and developing a differential diagnosis. We as clinicians tend to overlook the benefits and pitfalls of diagnostic testing, and this is beautifully discussed in the chapter on diagnostic testing. Finally, a new chapter on the use of optical coherence tomography (OCT) in uveitis has been added in this edition.
Part 3 of the book concentrates on the treatment of uveitis: both medical and surgical. What is useful in this section is that in addition to the multitude of new immunotherapies, the book also supplies a philosophy and approach to treatment decisions in patients with uveitis.
Part 4 focuses on infectious causes of uveitis. It covers the usual suspects in uveitis like syphilis and tuberculosis (TB), with up to date information on diagnostic tests and antimicrobial therapy. It also covers new infectious causes of uveitis like Ebola and Zika.
The last section of the book, Part 5, covers noninfectious causes of uveitis, more specifically, those not caused by an active acute infection. In addition, the section includes chapters on anterior uveitis, scleritis, and the masquerade syndromes.
I met Bob Nussenblatt at the ARVO meeting in 1976 and for over four decades was able to follow his academic and scientific career as he flourished at the National Eye Institute and developed an international reputation as a model for the clinician-scientist. One of his many qualities was his ability to identify and nurture colleagues both nationally and internationally, forming other great leaders in the field of uveitis. This book is part of Bob’s legacy. Bob and Scott Whitcup had similar backgrounds, both completing residencies in internal medicine in addition to ophthalmology. This solid knowledge of medicine, ophthalmology, and basic science contribute to the strong foundation of the book. Importantly, their high ethical standards, always placing the patient first, gives the book a unique tone and perspective. Two giants working together under a friendship and professional partnership for decades also comes through in reading the book. In spite of working at one of the most advanced technological medical centers in the world, Bob never lost his special and humble way of interacting with patients and colleagues in a friendly way. That was Bob. I am sure he would continue to be proud of Scott, Nida, and Alan and the latest edition of the book. This edition under the leadership of Scott will continue to help ophthalmologists practice their best medicine, exactly as Bob did his whole life.
I was happy to hear that Dr. Nida Sen had become involved with this edition of the book. Nida is an outstanding clinician-scientist and heads the uveitis program at the National Eye Institute. I was also pleased to see that Alan Palestine has contributed several chapters to the book. As with Dr. Whitcup, Dr. Palestine spent time at the National Eye Institute and has been a major contributor to the uveitis literature for several decades. In summary, Whitcup and Nussenblatt’s Uveitis is both an authoritative review of the subject with a practical approach that clinicians will find useful. It is a book that I and others frequently pull off the shelf and that improves the care of our patients.
Rubens Belfort Jr, MD, PhD, MBA Vision Institute, Federal University of Sao Paulo, Brazil President, National Academy of Medicine, Brazil 2020
PREFACE TO THE FIFTH EDITION
Over the past decade there has been a scientific explosion in both interest and research in immunology and the role it plays in disease. Not only have we learned more about how the immune system leads to disease pathogenesis, but we have also advanced our understanding on how modulating the immune response can lead to meaningful improvements in therapeutic outcomes. This research on downregulating the immune response has led to the development of new immunomodulatory agents that block the immune system at different sites of action including T cells, B cells, and cytokines. These new therapies provide clinicians with a number of additional therapeutic options for treating a host of immune-mediated inflammatory diseases including uveitis.
However, from an immunologic perspective, the last 10 years of research are likely to be remembered as the decade of cancer immunotherapy. Data now show that augmenting the existing antitumor immune responses results in the most significant clinical responses and the best opportunities for long-term disease remission and cure. These immunotherapies include the checkpoint inhibitors and chimeric antigen receptor T-cell therapy (CAR-T). But how do these new immunotherapies relate to uveitis? First, uveitis has occurred as an adverse effect of some immunotherapies. For example, both anterior and posterior uveitis have been reported in patients treated with checkpoint inhibitors. These observations provide further insight into the immune mechanisms of ocular inflammatory disease and identify novel potential therapeutic targets for uveitis. Second, it is interesting that this new-found success in cancer therapy is based on enhancing the body’s own anticancer immune response. This is analogous to advances in treating autoimmune and inflammatory diseases. Despite development of new immunosuppressive drugs like methotrexate and cyclosporine for inflammatory diseases, corticosteroids remain the mainstay of treatment for most forms of uveitis today. Hench and colleagues described the antirheumatic effects of the hormones released by the adrenal gland including adrenocorticotropic hormone (ACTH) in 1949 and corticosteroids were used to treat uveitis shortly thereafter. Similarly, recent advances in the treatment of autoimmune diseases have resulted not from the synthesis of new anti-inflammatory compounds, but by specifically modulating the patient’s immune response, for example, with monoclonal antibodies against key proinflammatory cytokines like tumor necrosis factor (TNF)-alpha, IL-17, and IL-23.
It is clear that studies on the pathogenesis of uveitis have furthered our understanding of ocular immunology and provided novel targets for therapeutic interventions, but this science has been the foundation for examining the role of inflammation in other nonuveitis conditions including age-related macular degeneration (AMD) and diabetic retinopathy. AMD is the leading cause of central vision loss in developed countries and is a great example of how our understanding of ocular immunology has augmented our knowledge about diseases other than uveitis. Genetic data from genome wide association studies and rare variant analyses pointed to involvement of the complement system in AMD. Other studies have supported the role of inflammation in the development or severity of AMD including inflammasome activation and dysregulated para-inflammation. Para-inflammation was defined by Medzhitov as a low level of inflammation that can exist between basal homeostasis and a progressive and more active inflammatory response. These data have supported the development of immune strategies for the treatment of atrophic AMD, including drugs to block the complement system.
In addition to progress in our understanding of the immune response, there have been a number of other advances that have
improved the treatment of uveitis. Prompt and accurate diagnosis of uveitis remain crucial to patient outcomes. There have been a couple of key technical advances that aid clinicians in the diagnosis of uveitis. Greater availability and accuracy of polymerase chain reaction (PCR) related tests for a number of infectious agents have improved our diagnosis of infectious uveitis, and these are discussed in the chapters that discuss viral, bacterial, and fungal causes of disease. Improvements in optical coherence tomography (OCT) have increased the utility of the instrument in characterizing inflammatory disease in the eye and in assessing the response to therapy.
There have also been changes in how we deliver drugs locally to the eye. The treatment of uveitis has always utilized local therapy of drugs to the eye. This started with topical corticosteroids for anterior uveitis in the 1950s followed by periocular corticosteroid injections for intermediate and posterior uveitis. Starting with the use of intravitreal injections of ganciclovir and foscarnet, uveitis specialists became aware of both the safety and efficacy of delivering drugs into the vitreous for treating CMV retinitis. Clinical trials of intravitreal injections of the anti-VEGF agents added to the safety and efficacy of this approach. Today, intravitreal injections of triamcinolone or sustained-release corticosteroid implants is increasing, while the use of periocular injections of corticosteroids is decreasing.
As with previous editions of Uveitis: Fundamentals and Clinical Practice, our goal remains the same: to provide a comprehensive text that provides both a practical and coherent approach to the diagnosis and treatment of the various forms of the disease. The book reviews the basic immunology of uveitis but focuses on the clinical aspects of the underlying science. We also hope that our book will be of value to clinicians and scientists outside of eye care, including internists, rheumatologists, and researchers in the field of inflammation.
The book is divided into five parts. The first part reviews the fundamentals of immunology and pathogenesis of ocular inflammatory disease. The second part focuses on diagnosis, including medical history, clinical examination, and diagnostic testing. A chapter on evidence-based medicine in uveitis is also included in this section. Part 3 reviews the principles of medical therapy for uveitis and details the commonly used drugs. A discussion of the role of surgery in the management of uveitis is also included in this part. The infectious causes of uveitis are included in the chapters in Part 4. These include bacterial, viral, fungal, and parasitic diseases. This section also includes a chapter on postsurgical causes of uveitis, because many of these are due to infection. Finally, the last section includes chapters on uveitis conditions that are predominantly caused by noninfectious etiologies: often autoimmune diseases or masquerade syndromes like cancer or toxicity. However, it is important to note that some of these conditions, like white dot syndromes, may have infectious causes.
There have been a number of important additions and updates to this edition of the book. Because of the increase in use of OCT in both the evaluation and management of the uveitis patient, a new chapter on OCT has been added (Chapter 6). With advances in our understanding of immunology and the development of a number of new medications for the treatment of uveitis, the chapters on fundamentals (Chapter 1) and medical therapy (Chapter 8) have been extensively updated. Chapters in the section on infectious causes of uveitis have also been extensively revised, incorporating information on new diagnostic testing such as PCR. Furthermore, there have been a number of new infectious causes of uveitis, like Ebola virus, and most recently severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), that
have been added to this section. Importantly, we have added many new figures to better illustrate clinical features of uveitis and added new case histories where useful.
This edition of Whitcup and Nussenblatt’s Uveitis: Fundamentals and Clinical Practice is the first I have written without my colleague and friend Bob Nussenblatt. Bob passed away in 2016. To those of us who know Bob, we have lost a friend who inspired us every day. The entire clinical immunology community has lost a great researcher, teacher, and clinician. Bob arrived at the National Institutes of Health (NIH) in 1977 as a clinical associate and held key leadership positions there, including chief of the National Eye Institute Laboratory of Immunology, Clinical Director, Scientific Director, Deputy Director for Intramural Research, and an NIH Distinguished Investigator. He was a mentor who loved teaching and a clinician-scientist who focused on the bench to bedside path every day. At its heart, the book stems from patient discussions with Bob at the National Eye Institute (NEI). My hope is that the heart of the book remains.
I would like to thank a number of people who are important to this edition of the book. First, I would like to thank the other two contributors to the book, Dr. H. Nida Sen and Dr. Alan Palestine. Nida is the director of the Uveitis Fellowship Program at the NEI and Professor at the George Washington University School of Medicine.
She is an accomplished researcher and clinician and is an integral part to this fifth edition. It is also great to have Alan involved in this 5th edition of the book. Dr. Palestine is currently the Chief of the Uveitis and Ocular Immunology Section and Director of Resident Research at the University of Colorado School of Medicine. Alan was involved with the early editions of the book and brings a wealth of practical experience to some key chapters of this edition. I also want to thank Chi-Chao Chan, Igal Gery, and Rachel Caspi, whose knowledge, inquisitiveness, and insight contributed to the evolution of this textbook. As a friend and colleague, I greatly appreciate that Dr. Rubens Belfort has both contributed many clinical photographs and written the foreword to the book. This edition has a new chapter on the use of OCT in uveitis, and I thank Elias Reichel for contributing a number of OCTs for the chapter and reviewing the text. I also must thank the staff of the NEI, including the technicians and photographers. Most importantly, I would like to thank our patients who have participated in clinical research and valued the opportunity to contribute to our understanding of uveitis in an attempt to help others.
Finally, I would like to thank family and friends for their support of this latest edition and again to Bob for his continued inspiration.
Scott M. Whitcup, MD
We would like to thank our colleagues for their input over the years and for supplying many of the outstanding images that help bring our text to life. We especially want to thank Igal Gery and Chi-Chao Chan for their assistance with the basic science of the book, Elias Reichel for his review of the new chapter on ocular coherence tomography, and to Rubens Belfort Jr. for authoring the Foreword for our book. We also thank the photographers and ophthalmic technicians of the National Eye Institute for their assistance in obtaining photographs, angiograms, OCT images, and other materials for the book. We also would like to thank Julie Taylor, Louise Cook, and the staff at Elsevier for their expertise and assistance in putting the book together. Importantly, we thank our patients for their willingness to participate in clinical trials and contribute to our understanding of uveitis and its treatment in the quest to help others.
We dedicate this fifth edition of the book to Robert B. Nussenblatt.
Bob was a founding leader in ocular immunology, an outstanding scientist, a caring physician, and a dedicated teacher. He treasured learning, valued scientific collaboration, and loved his family. Bob saw the importance of a uveitis textbook that combines the basic science of immunology and ocular inflammatory disease with clinical discussions focused on the patient. We hope that this edition of the book continues to educate and help improve the lives of our patients.
To our families, friends, colleagues, and patients.
Elements of the Immune System and Concepts of Intraocular Inflammatory Disease Pathogenesis
H. Nida Sen
KEY CONCEPTS
• T cells play an important role in the pathogenesis of uveitis.
• The eye is very active immunologically, with ocular resident cells interacting with the immune system.
• Uveitogenic antigens are expressed in the eye, and immunization of animals with these antigens induces experimental uveitis, which resembles human uveitis in many aspects.
In an ever-changing field, a review of the immune system is the subject of numerous books, courses, and scientific articles. However, certain principles have been established, and in the main, these have survived the test of time and rigorous scrutiny. The aim of this chapter is to provide the reader with the essentials needed to follow a discussion on the mechanisms proposed for intraocular inflammatory disease; therefore topics relevant to the understanding of that subject are addressed. In addition, selected themes thought to be important in understanding the unique ocular immune environment and pathogenesis are covered.
The development of the immune system is an extraordinary product of evolution. Its goal is to recognize what is different from self, so its initial role is to respond to foreign antigens with an innate immune response that is geared to rapidly clear the body of the foreign invader. “Innate immunity” is restricted to the non–antigen-specific immune response, including phagocytic cells that engulf and destroy invaders (macrophages and polymorphonuclear cells [PMNs]); populations of lymphocytes that include innate lymphoid cells [ILCs], i.e., natural killer [NK] cells and natural killer T cells (NKTCs); and humoral factors, such as the complement system, and the receptors on antigenpresenting cells, such as phagocytes, called toll-like receptors (TLRs), which interact with the invaders’ molecules. This activates the antigenpresenting cell to initiate the “adaptive” immune response. Clearly, the invader may return, in which case the adaptive immune response is in place to respond. The adaptive immune response is antigen specific and deals with the invaders that escaped the innate immune mechanism or have returned. The adaptive immune response consists of both B and T cells, and portions of these populations acquire the properties of the memory cells of the secondary immune response. This adaptive immune response connotes an immune memory, hence the development of a complex way in which high-affinity molecules and cell-surface markers can distinguish between the invader and self. A given of this concept is that self-antigens are not attacked; that is, an immune tolerance exists. Part of our story deals with the immune
system’s appropriate response to outside invaders (e.g., Toxoplasma) and the other part deals with understanding (and trying to explain) the response to autoantigens. The dynamic is not as simple as outlined; in fact, it starts as an appropriate response to a foreign antigen and then changes to an abnormal response against the eye. Many mechanisms, such as molecular mimicry, have been proposed.
Achieving this complex but highly specific immune response requires multiple players. Some of these are reviewed in the first part of this chapter. In the second part, findings and theories of disease mechanisms relevant to ocular diseases are introduced and discussed.
ELEMENTS OF THE IMMUNE SYSTEM
The immune system consists of several cell types, including macrophages, dendritic cells, polymorphonuclear cells, and a variety of lymphocyte lines with specific functions. These components add up to a complex immune circuitry or “ballet,” which, in the vast number of individuals, responds in a way that is beneficial to the organism. The interactions among these cells and their movements are mediated by several families of molecules, including cytokines, chemokines, and adhesion molecules.
Macrophages/Monocytes
Phagocytic cells originate in bone marrow. The concept that phagocytosis is important for the immunologic defense of the organism was proposed by Metchnikoff at the end of the nineteenth century. The macrophage, which is relatively large (15 μm), has an abundant smooth and rough endoplasmic reticulum. Lysosomal granules and a well-developed Golgi apparatus are also found. Several functional, histochemical, and morphologic characteristics of these cells can be noted (Table 1.1). In addition to the phagocytic characteristics already alluded to, these cells contain esterases and peroxidases and bear membrane markers that are typical of their cell line (i.e., OKM1 antigen
TABLE 1.1 Macrophage Characteristics
Histochemical Surface Antigens
Receptors Functions
5´-Nucleotidase OKM1 Fc Phagocytosis
Esterase Class II antigens
Alkaline phosphodiesterase
Aminopeptidase
Insulin
Immunoglobulin M (IgM) Pinocytosis
Lymphokine Immune activation
Lactoferrin Secretory
Microbicidal
Cb3 Tumoricidal
Fibrinogen
Lipoprotein
Fig. 1.1 Macrophage differentiation.
and F4/80). Other cell-surface markers are also present, such as class II antigens, Fc receptors (for antibody), and receptors (for complement). These enzymes and cell markers help identify this class of cells and their state of activation. The presence of esterase is a useful marker to distinguish macrophages from granulocytes and lymphocytes. Monocytes will leave the bloodstream because of either a predetermined maturational process or induced migration into an area as a result of chemotactic substances, often produced during inflammatory events. After taking up residence in various tissues, they become macrophages, which are frequently known by other names (Fig. 1.1). Dendritic cells, such as Langerhans’ cells, are found in the skin and the cornea and play an important role in presenting antigens to lymphocytes.
Macrophages play at least three major roles within the immune system. The first is to directly destroy foreign pathogens and clear dying or diseased tissue. Killing of invading microbes is, in part, mediated by a burst of hydrogen peroxide (H2O2) activity by the activated macrophage. An example with ocular importance is the engulfment of the toxoplasmosis organism, with the macrophage often being a repository for this parasite if killing is inadequate. The second is to activate the immune system. Macrophages, dendritic cells, or other cells with similar characteristics are mandatory for antigen-specific activation of T lymphocytes. Internalizing and processing of the antigen by the macrophage are thought to be integral parts of this mechanism, and the macrophage or the dendritic cell is named antigen-presenting cell (APC). Other cells, such as B cells, can also serve this function. The macrophage and the lymphocyte usually need to be in close contact with each other for this transfer to occur. Another requirement is for the cells to have in common a significant portion of their major histocompatibility complex (MHC), genes that express various cell-surface membranes essential for cellular communication and function. Thus this MHC stimulation leads to the initiation of an immune response, ultimately with both T and B cells potentially
participating. Other cell-surface markers are needed for activation. This “two signal” theory has centered on other cell-surface antigens, such as the B7–CD28 complex. The engagement of B7 (on the macrophage side) with CD28 enhances the transcription of cytokine genes. Third, the macrophage is a potent secretory cell. Proteases can be released in abundance, and this can degrade vessel surfaces and perivascular areas. Degradation products that result from these reactions are chemotactic and further enhance an immune response. Interleukin (IL)-1, a monokine with a molecular weight of 15 kilodaltons (kDa), is produced by the macrophage (and other cells) after interaction with exogenous pathogens or internal stimuli, such as immune complexes or T cells. IL-1 release directly affects T-cell growth and aids this cell in releasing its own secretory products. IL-1 is noted to act directly on the central nervous system (CNS), with a by-product being induction of fever. Still other macrophage products stimulate fibroblast migration and division, all of which have potentially important consequences in the eye.
Macrophages also produce IL-12, IL-18, IL-10, and transforming growth factor (TGF)-β. In a feedback mechanism, interferon (IFN)-γ can activate macrophages, and the production of IL-12 by the macrophage plays an important role in T-cell activation. The role of macrophages in the eye remains to be fully explored.
Dendritic Cells
Although macrophages play an important role, it is conjectured that dendritic cells are important macrophage-like cells in tissues. They are a subset of cells, perhaps of different lineage from macrophages, and they can be distinguished by lack of persistent adhesion and by the bearing of an antigen, 33D1, on their surface, features that macrophages do not possess. The major role of dendritic cells is to serve as APCs for both CD4+ and CD8+ cells. Like macrophages, dendritic cells produce IL-12, an important activator of T-cell responsiveness. They are rich in MHC II intracellular compartments, an important factor in antigen presentation. The MHC class II compartments move to the surface of the cell when the dendritic cell matures, stimulated by IFN-γ and the CD40 ligand. Dendritic cells are special in that they inhabit tissues where foreign antigens may enter. Experiments with painting of the skin brought seminal observations. Antigens painted on the skin are “brought” to the draining lymph nodes by the dendritic cells of the skin (Langerhans’ cells) where T-cell activation can occur. What is interesting is the migratory nature of these cells: They constantly carry important information to the peripheral centers of the immune response. Whether dendritic APCs can activate T cells efficiently in the tissues themselves is an open question, and the answer is important to our understanding of immune responses in the eye. Dendritic cells are thought to be the APCs (or one of the major players) in corneal graft rejection. Thus the concept of removing dendritic cells from a graft has been proposed and used in experimental models. However, there is an opposing concept that peripheral immune tolerance, induced by antigens that foster programmed cell death (apoptosis), may depend on presentation of antigen by dendritic cells in the tissue.
T cells
T-cell responses to antigens provide the basis for a large part of the inflammatory process. They are generated in bone marrow and mature in the thymus, the first lymphoid organ to develop. The thymus consists of two compartments, the cortex and the medulla. In the cortex, immature thymocytes develop through a complex process; their T-cell receptors (TCRs; see later) then interact with thymic epithelium, a process that determines their becoming CD4 (“helping”) or CD8 (“cytotoxic”) T cells. Thymocytes that fail this process die by apoptosis (“positive selection”), whereas thymocytes that succeed in this selection migrate to the thymic medulla, where epithelial and dendritic cells express all the body’s major autoantigens. Thymocytes
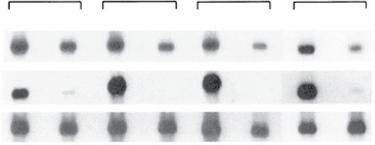
Fig. 1.2 Transcription of S-antigen (S-Ag) and interphotoreceptor retinoid-binding protein (IRBP) genes (uveitogenic antigens) in eyes and thymuses of mouse strains. S-Ag and IRBP are abundant in the eyes of all animals and S-Ag is found in the thymuses of all four strains tested. However, IRBP was seen only in thymuses of two strains –BALB/c and AKR/J – and not in those of B10.A or B10.RIII. The last two animals are susceptible to induction of uveitis with IRBP. (From Egwuagu CE, Charukamnoetkanok P, Gery I. Thymic expression of autoantigens correlates with resistance to autoimmune disease. J Immunol. 1997;159:3109–3112. Copyright 1997, The American Association of Immunologists, Inc.)
expressing TCRs with strong affinity to autoantigens are deleted (“negative selection”), and the remaining T cells enter the lymphoid system. Importantly, the negative selection is incomplete and T cells specific to autoantigens do escape the negative selection (see later).
A major component of the negative selection system is the autoimmune regulator (AIRE), a protein that is produced by medullary cells and that controls the expression of organ-specific antigens. Loss of the AIRE gene leads to autoimmunity,1 which is known to occur in humans who develop autoimmune polyglandular syndrome (APS) type I, an autoimmune disease that is inherited in an autosomal recessive fashion. In addition to adrenal insufficiency, mucocutaneous infections, and hypoparathyroidism, these patients can have diabetes, Sjögren syndrome, vitiligo, and uveitis.2
The expression of ocular self-antigens in the thymus was investigated in both mice and humans. Egwuagu et al.3 have shown in different mouse strains an inverted relationship between thymic expression of ocular-specific retinal antigens and the susceptibility to induction of experimental autoimmune uveitis (EAU): Thymic expression of retinal antigens causes lack of responsiveness to these antigens. An example of this phenomenon is shown in Fig. 1.2. Four inbred strains of mice were evaluated for the expression in their thymus of two uveitogenic antigens, interphotoreceptor retinoid-binding protein (IRBP) and S-antigen (S-Ag). All four strains were resistant to the induction of uveitis when S-Ag was used as the immunizing antigen, and all four expressed S-Ag in their thymus. However, two of the four strains, B10.A and B10.RIII, did not express IRBP in their thymuses and were susceptible to uveitis induction when IRBP was used as the immunizing antigen. These observations were extended to include other rodents and primates.4 In the Lewis rat, which is susceptible to both antigens, neither message was found in the thymus. These observations may provide an insight into the propensity for the disease in humans. Takase et al.5 evaluated 18 human thymus samples taken from patients undergoing surgery for congenital heart disease. They found that there was expression of the four antigens that can induce experimental uveitis (S-Ag, recoverin, RPE65, and IRBP) in the thymuses of the tested patients. However, the expression of the various antigens was very variable, with some thymus samples showing strong expression and others not. The implication of the findings from these studies is that expression of these antigens in the thymus is very variable in humans, similar to what is seen in the differences among various rodent strains. T cells with specificity to ocular self-antigens that escape the negative selection are found in the circulation, but do not induce uveitis. This observation is explained by two mechanisms: (1) the inhibitory effect of T-regulatory (Treg) cells, which are normally present in the body; and
(2) the retina being isolated from circulating cells by the blood–retina barrier. The normal presence of T cells is indicated by the finding of T cells specific to retinal antigens in healthy individuals with no eye disease.
One important quality possessed by T cells is their immunologic recall or anamnestic capacity after re-exposure to their specific target antigen. The exposure to the antigen increases the number of specific cells and changes them into a “memory” phenotype. A memory T cell to a particular antigen can retain this immunologic memory (see later) essentially for its lifetime. With a repeat encounter, this memory response leads to an immune response that is more rapid and more pronounced than the first. An example is the positive skin response seen after purified protein derivative (PPD) testing.
The central role of the T cell in the immune system cannot be overemphasized. T cells function as pivotal modulators of the immune response by helping production of antibody by B cells and augmenting cellmediated reactions through the release of molecules, named cytokines, which activate immune-related and other cells. T cells also may downregulate or prevent immune reactions through active suppression. (i.e., Treg cells). The cytotoxic (CD8) T-cell subset plays a major role in transplantation rejection crises. Accumulated evidence supports the importance of T cells in many aspects of the intraocular inflammatory process – from the propagation of disease to its subsequent downregulation.
A state of suspended animation can be induced in T cells; this is termed anergy. For T cells to be activated, several signals need to be given: one through the TCR and the other through costimulatory receptors, such as CD28; the third is the costimulant B7 linking to CD28 (which is on the T cell). If the TCR is activated but the costimulant is not, a growth arrest can be seen in these cells: They simply stop functioning but do not die. A second way this can occur is when a weakly adherent peptide is linked to the TCR, even if costimulation occurs. It would seem to be a mechanism to prevent unwanted or nuisance immune responses. The full response takes place only if all the appropriate interactions have occurred.
T-cell Receptor
Much interest has focused on the TCR. T cells need to produce the TCR on their cell surface to recognize the target immunogenic peptide on the MHCs of APCs. This complex interaction involves either CD4 or CD8 and their TCRs. The TCR is similar in structure to an immunoglobulin, having both α and β chains. The more distal ends of these chains are variable, and the hypervariable regions are termed V (variable) and J (joining) on the α chain and V and D (diversity) regions on the β chain. Compared with the number of immunoglobulin genes, there are fewer V genes and more J genes in the TCR repertoire. It is logically assumed that the target peptide, which has a special shape and therefore fits specifically in a lock-and-key fashion into the groove between the MHC and the TCR, would be the “cement” of this union. It has been suggested that of all the possible combinations of gene arrangements that could possibly produce the variable region believed to cradle the peptide, certain genes within a family seem to be noted more frequently in autoimmune disease. One such group is the Vα family, with Vβ8.2 receiving much attention. A small number of cells have a TCR made up not of α and β chains but, rather, of γ and δ chains (detailed later). In addition to these physiologic mechanisms, T cells may also be activated by “superantigens,” which are bacterial products, such as enterotoxins, or plant products, such as phytohemagglutinin. In addition, T cells may be activated by antibodies to certain surface antigens, mostly CD3 and CD28.
Major Populations of T Cells
The functions that have been briefly described are carried out by several subsets of CD4 T cells, identified by their products and functions. It was observed early on that T cells (and other cells) manifest myriad different molecules on their surface membranes, some of which are
Another random document with no related content on Scribd:
As soon as he reached the summer cottage, where he and Nurse Jane were stopping, Uncle Wiggily put on the stove in a kettle, a lot of sugar, molasses, butter, cocoanut and all such things as go into taffy. “I’m going to have a taffy pull myself!” laughed Mr. Longears, as he invited many animal boys and girls. “There’s going to be a terrible time here soon,” sighed Nurse Jane, rocking to and fro. “Terrible!”
“Well, I guess the taffy has boiled long enough now,” said Uncle Wiggily after a while. The kitchen was filled with delicious smells. “Now be careful!” called Nurse Jane. Uncle Wiggily said he would, but in carrying the kettle over to the table, he spilled some on the floor. “Oh, we can pry this up and eat it when it gets cold!” cried Sammie and Susie the rabbits. Nurse Jane cried: “Look out!”
“Accidents will happen!” laughed Uncle Wiggily as he poured the taffy from the kettle into a buttered pan, and waited for it to cool. “A little on the floor doesn’t matter.” Then he took up the lump of partly-cooled candy, and started to hang it on the stove poker he had bent into a hook like the Monkey Doodle’s. But, all of a sudden, the bunny gentleman found his paws stuck fast in the sticky taffy.
Nurse Jane put butter on Uncle Wiggily’s paws, and at last he got the lump of taffy off, and placed it on the poker hook for pulling. “Now we’ll soon have real salt water taffy!” he told the animal children. “Hurray!” bleated Billie the goat. Nurse Jane stood ready with a pitcher of water and a long spoon filled with butter, in case the bunny got stuck again. Uncle Wiggily pulled out a long candy strand.
Everything seemed to be going nicely, but all of a sudden, as Uncle Wiggily tried to throw a loop of candy rope around the hook, to pull it out again, he slung it around Nurse Jane. “Oh, I’m caught in the sticky candy!” cried the muskrat lady. “Uncle Wiggily lassoed Miss Fuzzy Wuzzy just like in a Wild West show!” barked Jackie Bow Wow. “Dear me! I didn’t mean to do this!” cried the bunny.
For a time it seemed that they would have to send for Dr. Possum. But at last Uncle Wiggily and the animal children got Nurse Jane free from the sticky candy rope. “Now I’ll try to pull the taffy again,” said the bunny. He threw another loop of the sticky stuff at the poker hook, but it tangled around the horns of Billie Wagtail. “Baa-aa-aa! Maa-aa-aa!” bleated Billie. “Dear me!” said the bunny.
After some little time Nurse Jane managed to get Billie loose from the sticky candy. “You’d better give up trying to make taffy,” she told the bunny. “This time I’ll make it,” he said, as he slung a big lump of the sticky stuff at the hook. But the poker came loose from the wall, down fell the candy and Uncle Wiggily sat right down in it! “Help! Help!” cried the bunny, and they all rushed to help him get up.
By using a kettle of warm water Nurse Jane managed to get Uncle Wiggily loose from the candy on the floor. The animal children with shovels, hoes and croquet-mallets also helped. Uncle Wiggily washed and dressed himself in his best. “Where are you going?” asked Nurse Jane as he hopped out the door. “I’m going to buy some taffy,” answered Mr. Longears. “It’s easier than making it.”
TRANSCRIBER’S NOTES
Page Changed from Changed to
Chapter Heading [omitted] UNCLE WIGGILY’S SILK HAT or A TALL SILK HAT MAY BE STYLISH AND ALSO USEFUL
1. Silently corrected obvious typographical errors and variations in spelling.
2. Retained archaic, non-standard, and uncertain spellings as printed.
*** END OF THE PROJECT GUTENBERG EBOOK UNCLE WIGGILY'S SILK
HAT
***
Updated editions will replace the previous one—the old editions will be renamed.
Creating the works from print editions not protected by U.S. copyright law means that no one owns a United States copyright in these works, so the Foundation (and you!) can copy and distribute it in the United States without permission and without paying copyright royalties. Special rules, set forth in the General Terms of Use part of this license, apply to copying and distributing Project Gutenberg™ electronic works to protect the PROJECT GUTENBERG™ concept and trademark. Project Gutenberg is a registered trademark, and may not be used if you charge for an eBook, except by following the terms of the trademark license, including paying royalties for use of the Project Gutenberg trademark. If you do not charge anything for copies of this eBook, complying with the trademark license is very easy. You may use this eBook for nearly any purpose such as creation of derivative works, reports, performances and research. Project Gutenberg eBooks may be modified and printed and given away you may do practically ANYTHING in the United States with eBooks not protected by U.S. copyright law. Redistribution is subject to the trademark license, especially commercial redistribution.
START: FULL LICENSE
THE FULL PROJECT GUTENBERG LICENSE
PLEASE READ THIS BEFORE YOU DISTRIBUTE OR USE THIS WORK
To protect the Project Gutenberg™ mission of promoting the free distribution of electronic works, by using or distributing this work (or any other work associated in any way with the phrase “Project Gutenberg”), you agree to comply with all the terms of the Full Project Gutenberg™ License available with this file or online at www.gutenberg.org/license.
Section 1. General Terms of Use and Redistributing Project Gutenberg™ electronic works
1.A. By reading or using any part of this Project Gutenberg™ electronic work, you indicate that you have read, understand, agree to and accept all the terms of this license and intellectual property (trademark/copyright) agreement. If you do not agree to abide by all the terms of this agreement, you must cease using and return or destroy all copies of Project Gutenberg™ electronic works in your possession. If you paid a fee for obtaining a copy of or access to a Project Gutenberg™ electronic work and you do not agree to be bound by the terms of this agreement, you may obtain a refund from the person or entity to whom you paid the fee as set forth in paragraph 1.E.8.
1.B. “Project Gutenberg” is a registered trademark. It may only be used on or associated in any way with an electronic work by people who agree to be bound by the terms of this agreement. There are a few things that you can do with most Project Gutenberg™ electronic works even without complying with the full terms of this agreement. See paragraph 1.C below. There are a lot of things you can do with Project Gutenberg™ electronic works if you follow the terms of this agreement and help preserve free future access to Project Gutenberg™ electronic works. See paragraph 1.E below.
1.C. The Project Gutenberg Literary Archive Foundation (“the Foundation” or PGLAF), owns a compilation copyright in the collection of Project Gutenberg™ electronic works. Nearly all the individual works in the collection are in the public domain in the United States. If an individual work is unprotected by copyright law in the United States and you are located in the United States, we do not claim a right to prevent you from copying, distributing, performing, displaying or creating derivative works based on the work as long as all references to Project Gutenberg are removed. Of course, we hope that you will support the Project Gutenberg™ mission of promoting free access to electronic works by freely sharing Project Gutenberg™ works in compliance with the terms of this agreement for keeping the Project Gutenberg™ name associated with the work. You can easily comply with the terms of this agreement by keeping this work in the same format with its attached full Project Gutenberg™ License when you share it without charge with others.
1.D. The copyright laws of the place where you are located also govern what you can do with this work. Copyright laws in most countries are in a constant state of change. If you are outside the United States, check the laws of your country in addition to the terms of this agreement before downloading, copying, displaying, performing, distributing or creating derivative works based on this work or any other Project Gutenberg™ work. The Foundation makes no representations concerning the copyright status of any work in any country other than the United States.
1.E. Unless you have removed all references to Project Gutenberg:
1.E.1. The following sentence, with active links to, or other immediate access to, the full Project Gutenberg™ License must appear prominently whenever any copy of a Project Gutenberg™ work (any work on which the phrase “Project
Gutenberg” appears, or with which the phrase “Project Gutenberg” is associated) is accessed, displayed, performed, viewed, copied or distributed:
This eBook is for the use of anyone anywhere in the United States and most other parts of the world at no cost and with almost no restrictions whatsoever. You may copy it, give it away or re-use it under the terms of the Project Gutenberg License included with this eBook or online at www.gutenberg.org. If you are not located in the United States, you will have to check the laws of the country where you are located before using this eBook.
1.E.2. If an individual Project Gutenberg™ electronic work is derived from texts not protected by U.S. copyright law (does not contain a notice indicating that it is posted with permission of the copyright holder), the work can be copied and distributed to anyone in the United States without paying any fees or charges. If you are redistributing or providing access to a work with the phrase “Project Gutenberg” associated with or appearing on the work, you must comply either with the requirements of paragraphs 1.E.1 through 1.E.7 or obtain permission for the use of the work and the Project Gutenberg™ trademark as set forth in paragraphs 1.E.8 or 1.E.9.
1.E.3. If an individual Project Gutenberg™ electronic work is posted with the permission of the copyright holder, your use and distribution must comply with both paragraphs 1.E.1 through 1.E.7 and any additional terms imposed by the copyright holder. Additional terms will be linked to the Project Gutenberg™ License for all works posted with the permission of the copyright holder found at the beginning of this work.
1.E.4. Do not unlink or detach or remove the full Project Gutenberg™ License terms from this work, or any files
containing a part of this work or any other work associated with Project Gutenberg™.
1.E.5. Do not copy, display, perform, distribute or redistribute this electronic work, or any part of this electronic work, without prominently displaying the sentence set forth in paragraph 1.E.1 with active links or immediate access to the full terms of the Project Gutenberg™ License.
1.E.6. You may convert to and distribute this work in any binary, compressed, marked up, nonproprietary or proprietary form, including any word processing or hypertext form. However, if you provide access to or distribute copies of a Project Gutenberg™ work in a format other than “Plain Vanilla ASCII” or other format used in the official version posted on the official Project Gutenberg™ website (www.gutenberg.org), you must, at no additional cost, fee or expense to the user, provide a copy, a means of exporting a copy, or a means of obtaining a copy upon request, of the work in its original “Plain Vanilla ASCII” or other form. Any alternate format must include the full Project Gutenberg™ License as specified in paragraph 1.E.1.
1.E.7. Do not charge a fee for access to, viewing, displaying, performing, copying or distributing any Project Gutenberg™ works unless you comply with paragraph 1.E.8 or 1.E.9.
1.E.8. You may charge a reasonable fee for copies of or providing access to or distributing Project Gutenberg™ electronic works provided that:
• You pay a royalty fee of 20% of the gross profits you derive from the use of Project Gutenberg™ works calculated using the method you already use to calculate your applicable taxes. The fee is owed to the owner of the Project Gutenberg™ trademark, but he has agreed to donate royalties under this paragraph to the Project Gutenberg Literary Archive Foundation. Royalty
payments must be paid within 60 days following each date on which you prepare (or are legally required to prepare) your periodic tax returns. Royalty payments should be clearly marked as such and sent to the Project Gutenberg Literary Archive Foundation at the address specified in Section 4, “Information about donations to the Project Gutenberg Literary Archive Foundation.”
• You provide a full refund of any money paid by a user who notifies you in writing (or by e-mail) within 30 days of receipt that s/he does not agree to the terms of the full Project Gutenberg™ License. You must require such a user to return or destroy all copies of the works possessed in a physical medium and discontinue all use of and all access to other copies of Project Gutenberg™ works.
• You provide, in accordance with paragraph 1.F.3, a full refund of any money paid for a work or a replacement copy, if a defect in the electronic work is discovered and reported to you within 90 days of receipt of the work.
• You comply with all other terms of this agreement for free distribution of Project Gutenberg™ works.
1.E.9. If you wish to charge a fee or distribute a Project Gutenberg™ electronic work or group of works on different terms than are set forth in this agreement, you must obtain permission in writing from the Project Gutenberg Literary Archive Foundation, the manager of the Project Gutenberg™ trademark. Contact the Foundation as set forth in Section 3 below.
1.F.
1.F.1. Project Gutenberg volunteers and employees expend considerable effort to identify, do copyright research on, transcribe and proofread works not protected by U.S. copyright
law in creating the Project Gutenberg™ collection. Despite these efforts, Project Gutenberg™ electronic works, and the medium on which they may be stored, may contain “Defects,” such as, but not limited to, incomplete, inaccurate or corrupt data, transcription errors, a copyright or other intellectual property infringement, a defective or damaged disk or other medium, a computer virus, or computer codes that damage or cannot be read by your equipment.
1.F.2. LIMITED WARRANTY, DISCLAIMER OF DAMAGES - Except for the “Right of Replacement or Refund” described in paragraph 1.F.3, the Project Gutenberg Literary Archive Foundation, the owner of the Project Gutenberg™ trademark, and any other party distributing a Project Gutenberg™ electronic work under this agreement, disclaim all liability to you for damages, costs and expenses, including legal fees. YOU AGREE THAT YOU HAVE NO REMEDIES FOR NEGLIGENCE, STRICT LIABILITY, BREACH OF WARRANTY OR BREACH OF CONTRACT EXCEPT THOSE PROVIDED IN PARAGRAPH 1.F.3. YOU AGREE THAT THE FOUNDATION, THE TRADEMARK OWNER, AND ANY DISTRIBUTOR UNDER THIS AGREEMENT WILL NOT BE LIABLE TO YOU FOR ACTUAL, DIRECT, INDIRECT, CONSEQUENTIAL, PUNITIVE OR INCIDENTAL DAMAGES EVEN IF YOU GIVE NOTICE OF THE POSSIBILITY OF SUCH DAMAGE.
1.F.3. LIMITED RIGHT OF REPLACEMENT OR REFUND - If you discover a defect in this electronic work within 90 days of receiving it, you can receive a refund of the money (if any) you paid for it by sending a written explanation to the person you received the work from. If you received the work on a physical medium, you must return the medium with your written explanation. The person or entity that provided you with the defective work may elect to provide a replacement copy in lieu of a refund. If you received the work electronically, the person or entity providing it to you may choose to give you a second opportunity to receive the work electronically in lieu of a refund.
If the second copy is also defective, you may demand a refund in writing without further opportunities to fix the problem.
1.F.4. Except for the limited right of replacement or refund set forth in paragraph 1.F.3, this work is provided to you ‘AS-IS’, WITH NO OTHER WARRANTIES OF ANY KIND, EXPRESS OR IMPLIED, INCLUDING BUT NOT LIMITED TO WARRANTIES OF MERCHANTABILITY OR FITNESS FOR ANY PURPOSE.
1.F.5. Some states do not allow disclaimers of certain implied warranties or the exclusion or limitation of certain types of damages. If any disclaimer or limitation set forth in this agreement violates the law of the state applicable to this agreement, the agreement shall be interpreted to make the maximum disclaimer or limitation permitted by the applicable state law. The invalidity or unenforceability of any provision of this agreement shall not void the remaining provisions.
1.F.6. INDEMNITY - You agree to indemnify and hold the Foundation, the trademark owner, any agent or employee of the Foundation, anyone providing copies of Project Gutenberg™ electronic works in accordance with this agreement, and any volunteers associated with the production, promotion and distribution of Project Gutenberg™ electronic works, harmless from all liability, costs and expenses, including legal fees, that arise directly or indirectly from any of the following which you do or cause to occur: (a) distribution of this or any Project Gutenberg™ work, (b) alteration, modification, or additions or deletions to any Project Gutenberg™ work, and (c) any Defect you cause.
Section 2. Information about the Mission of
Project Gutenberg™ is synonymous with the free distribution of electronic works in formats readable by the widest variety of computers including obsolete, old, middle-aged and new computers. It exists because of the efforts of hundreds of volunteers and donations from people in all walks of life.
Volunteers and financial support to provide volunteers with the assistance they need are critical to reaching Project Gutenberg™’s goals and ensuring that the Project Gutenberg™ collection will remain freely available for generations to come. In 2001, the Project Gutenberg Literary Archive Foundation was created to provide a secure and permanent future for Project Gutenberg™ and future generations. To learn more about the Project Gutenberg Literary Archive Foundation and how your efforts and donations can help, see Sections 3 and 4 and the Foundation information page at www.gutenberg.org.
Section 3. Information about the Project
Gutenberg Literary Archive
Foundation
The Project Gutenberg Literary Archive Foundation is a nonprofit 501(c)(3) educational corporation organized under the laws of the state of Mississippi and granted tax exempt status by the Internal Revenue Service. The Foundation’s EIN or federal tax identification number is 64-6221541. Contributions to the Project Gutenberg Literary Archive Foundation are tax deductible to the full extent permitted by U.S. federal laws and your state’s laws.
The Foundation’s business office is located at 809 North 1500 West, Salt Lake City, UT 84116, (801) 596-1887. Email contact links and up to date contact information can be found at the Foundation’s website and official page at www.gutenberg.org/contact
Section 4. Information about Donations to the Project Gutenberg Literary Archive Foundation
Project Gutenberg™ depends upon and cannot survive without widespread public support and donations to carry out its mission of increasing the number of public domain and licensed works that can be freely distributed in machine-readable form accessible by the widest array of equipment including outdated equipment. Many small donations ($1 to $5,000) are particularly important to maintaining tax exempt status with the IRS.
The Foundation is committed to complying with the laws regulating charities and charitable donations in all 50 states of the United States. Compliance requirements are not uniform and it takes a considerable effort, much paperwork and many fees to meet and keep up with these requirements. We do not solicit donations in locations where we have not received written confirmation of compliance. To SEND DONATIONS or determine the status of compliance for any particular state visit www.gutenberg.org/donate.
While we cannot and do not solicit contributions from states where we have not met the solicitation requirements, we know of no prohibition against accepting unsolicited donations from donors in such states who approach us with offers to donate.
International donations are gratefully accepted, but we cannot make any statements concerning tax treatment of donations received from outside the United States. U.S. laws alone swamp our small staff.
Please check the Project Gutenberg web pages for current donation methods and addresses. Donations are accepted in a number of other ways including checks, online payments and
credit card donations. To donate, please visit: www.gutenberg.org/donate.
Section 5. General Information About Project Gutenberg™ electronic works
Professor Michael S. Hart was the originator of the Project Gutenberg™ concept of a library of electronic works that could be freely shared with anyone. For forty years, he produced and distributed Project Gutenberg™ eBooks with only a loose network of volunteer support.
Project Gutenberg™ eBooks are often created from several printed editions, all of which are confirmed as not protected by copyright in the U.S. unless a copyright notice is included. Thus, we do not necessarily keep eBooks in compliance with any particular paper edition.
Most people start at our website which has the main PG search facility: www.gutenberg.org.
This website includes information about Project Gutenberg™, including how to make donations to the Project Gutenberg Literary Archive Foundation, how to help produce our new eBooks, and how to subscribe to our email newsletter to hear about new eBooks.