Functional Bakery Products: Novel Ingredients and Processing Technology for Personalized Nutrition Weibiao Zhou
https://ebookmass.com/product/functional-bakeryproducts-novel-ingredients-and-processingtechnology-for-personalized-nutrition-weibiaozhou/
Download more ebook from https://ebookmass.com
More products digital (pdf, epub, mobi) instant download maybe you interests ...
Handbook of Banana Production, Postharvest Science, Processing Technology, and Nutrition Jasim Ahmed
https://ebookmass.com/product/handbook-of-banana-productionpostharvest-science-processing-technology-and-nutrition-jasimahmed/
Functional Food Ingredients from Plants Isabel C. F. R. Ferreira
https://ebookmass.com/product/functional-food-ingredients-fromplants-isabel-c-f-r-ferreira/
Nutrition and Functional Foods for Healthy Aging 1st Edition Ronald Ross Watson (Eds.)
https://ebookmass.com/product/nutrition-and-functional-foods-forhealthy-aging-1st-edition-ronald-ross-watson-eds/
Sweet potato : chemistry, processing and nutrition Mu
https://ebookmass.com/product/sweet-potato-chemistry-processingand-nutrition-mu/
The Role of Alternative and Innovative Food Ingredients and Products in Consumer Wellness Charis
M. Galanakis
https://ebookmass.com/product/the-role-of-alternative-andinnovative-food-ingredients-and-products-in-consumer-wellnesscharis-m-galanakis/
Snack Foods: Processing and Technology Suvendu
Bhattacharya
https://ebookmass.com/product/snack-foods-processing-andtechnology-suvendu-bhattacharya/
Valorization of fruit processing by-products Charis M. Galanakis
https://ebookmass.com/product/valorization-of-fruit-processingby-products-charis-m-galanakis/
Wardlaw’s Contemporary Nutrition: A Functional Approach
Gordon M. Wardlaw
https://ebookmass.com/product/wardlaws-contemporary-nutrition-afunctional-approach-gordon-m-wardlaw/
Nutrition and Functional Foods in Boosting Digestion, Metabolism and Immune Health Debasis Bagchi
https://ebookmass.com/product/nutrition-and-functional-foods-inboosting-digestion-metabolism-and-immune-health-debasis-bagchi/
ADVISORYBOARDS
DavidRodríguez-Lázaro
Loong-TakLim
MichaelEskin
IsabelFerreira
CrispuloGallegos
Se-KwonKim
KeizoArihara
SERIESEDITORS
GEORGEF.STEWART(1948–1982)
EMILM.MRAK (1948–1987)
C.O.CHICHESTER(1959–1988)
BERNARDS.SCHWEIGERT(1984–1988)
JOHNE.KINSELLA(1989–1993)
STEVEL.TAYLOR(1995–2011)
JEYAKUMARHENRY(2011–2016)
FIDELTOLDRÁ (2016– )
AcademicPressisanimprintofElsevier
50HampshireStreet,5thFloor,Cambridge,MA02139,UnitedStates 525BStreet,Suite1650,SanDiego,CA92101,UnitedStates TheBoulevard,LangfordLane,Kidlington,OxfordOX51GB,UnitedKingdom 125LondonWall,London,EC2Y5AS,UnitedKingdom
Firstedition2022
Copyright©2022ElsevierInc.Allrightsreserved.
Nopartofthispublicationmaybereproducedortransmittedinanyformorbyanymeans,electronic ormechanical,includingphotocopying,recording,oranyinformationstorageandretrievalsystem, withoutpermissioninwritingfromthepublisher.Detailsonhowtoseekpermission,further informationaboutthePublisher’spermissionspoliciesandourarrangementswithorganizationssuch astheCopyrightClearanceCenterandtheCopyrightLicensingAgency,canbefoundatourwebsite: www.elsevier.com/permissions.
Thisbookandtheindividualcontributionscontainedinitareprotectedundercopyrightbythe Publisher(otherthanasmaybenotedherein).
Notices
Knowledgeandbestpracticeinthisfieldareconstantlychanging.Asnewresearchandexperience broadenourunderstanding,changesinresearchmethods,professionalpractices,ormedical treatmentmaybecomenecessary.
Practitionersandresearchersmustalwaysrelyontheirownexperienceandknowledgeinevaluating andusinganyinformation,methods,compounds,orexperimentsdescribedherein.Inusingsuch informationormethodstheyshouldbemindfuloftheirownsafetyandthesafetyofothers,including partiesforwhomtheyhaveaprofessionalresponsibility.
Tothefullestextentofthelaw,neitherthePublishernortheauthors,contributors,oreditors,assume anyliabilityforanyinjuryand/ordamagetopersonsorpropertyasamatterofproductsliability, negligenceorotherwise,orfromanyuseoroperationofanymethods,products,instructions,orideas containedinthematerialherein.
ISBN:978-0-323-85557-0
ISSN:1043-4526
ForinformationonallAcademicPresspublications visitourwebsiteat https://www.elsevier.com/books-and-journals
Publisher: ZoeKruze
AcquisitionsEditor: SamMahfoudh
DevelopmentalEditor: JhonMichaelPeñano
ProductionProjectManager: VijayarajPurushothaman
CoverDesigner: MatthewLimbert
TypesetbySTRAIVE,India
1.Towardsthecreationofpersonalizedbakeryproductsusing3D foodprinting1
LuZhang,MartijnNoort,andKjeldvanBommel
1. Introduction2
2. 3Dprintingtechnologyforbakeryproducts4
3. Recentdevelopmentin3D-printedbakeryproducts14
4. Personalizationin3D-printedbakeryproducts23
5. Conclusions30 Acknowledgments31 References31
2.Dietaryfiberinbakeryproducts:Source,processing,andfunction37 SuyunLin
1. Introduction38
2. Dietaryfibers(DFs)40
3. Trendsinfiber-enrichmentinbakeryproducts48
4. EffectsofDFsondoughprocessing57
5. EffectofDFsonqualityofbakeryproducts60
6. EffectofDFsonphysiologicalfunctionalityofbakeryproducts67
7. ImprovingthecompatibilityofDFsinbakeryproducts77
8. Conclusions83 References83
3.Therealmofplantproteinswithfocusontheirapplicationin developingnewbakeryproducts101 FatmaBoukid
1. Introduction102
2. Realmofplantproteins103
3. Impactofproteinfortificationonbakeryproducts117
4. Conclusionandfutureoutlooks121 References122
4.Guidingtheformulationofsoftcerealfoodsfortheelderly populationthroughfoodoralprocessing:Challengesand opportunities137
MelissaAssad-Bustillos,GillesFeron,andGuyDellaValle
1. Introductionandcontext:Whydevelopfoodfortheelderly?138
2. Theroleoffoodoralprocessinginperceptionanddigestion139
3. Theelderly:Physiologyandnutritionalneeds153
4. Formulationofsoftcerealfoodstargetedfortheelderly162
5. Conclusionsandperspectives176 References178
5.Gluten-freebakeryproducts:Ingredientsandprocesses189 ManuelGómez
1. Introduction190
2. Ingredients192
3. Processes211
4. Nutritionalqualityofgluten-freeproducts221
5. Conclusions225 References225
6.Enhancinghealthbenefitsofbakeryproductsusing phytochemicals239
JingGao,AudreyHuiSiKoh,andWeibiaoZhou
1. Introduction240
2. Catechinsfromgreentea241
3. Anthocyanins254
4. Fucoidanfrom Undariapinnatifida 267
5. Quercetin269
6. Conclusions272 References273
7.Sugar,saltandfatreductionofbakeryproducts283 NantawanTherdthai
1. Healthconcerns:Thedrivingforcetoreducesugar,saltandfatinbaked products284
2. Roleofsugar,saltandfatinbakedproducts285
3. Techniquestoreducesugarinbakedproducts295
4. Techniquestoreducesaltinbakedproducts303
5. Techniquestoreducefatinbakedproducts306
6. Summary321 References322
Contributors
MelissaAssad-Bustillos
FoodProcessEngineeringGroup,InstituteofFood,NutritionandHealth,ETHZurich, Zurich,Switzerland
FatmaBoukid
FoodSafetyandFunctionalityProgramme,FoodIndustryArea,InstituteofAgricultureand FoodResearchandTechnology(IRTA),Monells,Catalonia,Spain
GuyDellaValle
INRAEBiopolyme ` resInteractionsetAssemblages,Nantes,France
GillesFeron
CentredesSciencesduGou ˆ tetdel’Alimentation,AgroSupDijon,CNRS,INRAE, UniversiteBourgogneFranche-Comte,Dijon,France
JingGao
DepartmentofFoodScienceandTechnology,NationalUniversityofSingapore,Singapore, Singapore
ManuelGo ´ mez
FoodTechnologyArea,CollegeofAgriculturalEngineering,UniversityofValladolid, Palencia,Spain
AudreyHuiSiKoh
DepartmentofFoodScienceandTechnology,NationalUniversityofSingapore,Singapore, Singapore
SuyunLin
KeyLabforNaturalProductsandFunctionalFoodsofJiangxiProvince,CollegeofFood ScienceandEngineering,JiangxiAgriculturalUniversity,Nanchang,China
MartijnNoort
WageningenUniversity&Research,WageningenFood&BiobasedResearch, Wageningen,TheNetherlands
NantawanTherdthai
DepartmentofProductDevelopment,FacultyofAgro-Industry,KasetsartUniversity, Bangkok,Thailand
KjeldvanBommel
EquipmentforAdditiveManufacturingDepartment,NetherlandsOrganisationforApplied ScientificResearch(TNO),Eindhoven,TheNetherlands
LuZhang
WageningenUniversity&Research,LaboratoryofFoodProcessEngineering,Wageningen, TheNetherlands
WeibiaoZhou
DepartmentofFoodScienceandTechnology,NationalUniversityofSingapore,Singapore, Singapore
Preface
Thisvolumeof AdvancesinFoodandNutritionResearch iscompilingseven chaptersthatdescribethelatestdevelopmentsinfunctionalbakeryproducts, withaspecialfocusonnovelingredientsandprocessingtechnologyfor personalizednutrition.Asconsumersbecomeincreasinglymorehealthconsciousandhaveadeeperappreciationoftheadage“youarewhatyou eat”,demandforfunctionalfoodsisgainingmomentum.Asonesizedoes notfitall,developingfunctionalbakeryproductsneedstobetailoredto specificdietaryrequirementorrestrictionsoftheconsumers.Thisbookvolumeisdevotedtoprovidinganin-depthreviewoftherecentadvancesin developingbakeryproductstoaddresschallengesofthereductionofsugar, fat,salt,andgluten,aswellastomeettheneedsofnovelproteins,dietary fibre,andfunctionalingredients,fortargetedconsumers(e.g.,elderly) andwithinnovativetechnology(e.g.,3Dprinting).
Chapter1 providesthemostrecentdevelopmentsin3D-printingof bakeryproducts,includingprintingsystem,doughformulationandpossible personalizationfortexture,nutrients,andsatietymodulation. Chapter2 presentsthedevelopmentoffibre-enrichedbakeryproductswithincreased nutritionalvalueandappealingpalatability.Thetrendsindietaryfibresupplementation,itsimpactondoughprocessing,quality,andphysiological functionalityofbakeryproducts,aswellasapproachestoimprovethecompatibilityofdietaryfibreinbakeryproductsarediscussed. Chapter3 reviews theapplicationofplantproteinindevelopingnewbakeryproductsforabetter amino-acidprofileandahigherproteinintake.Specificfunctionalproperties andnutritionalvaluesofbothconventionalandemergingplantprotein sourcesarecoveredinthischapter. Chapter4 bringsnewinsightsinto howtoguidetheformulationofsoftcereal-basedfoodsforelderlypopulation throughfoodoralprocessing.Itprovidesanoverviewofthevariousaspects involvedintheoralprocessingandformulationofsoftcereal-basedfoods, translatingthemintochallengesandopportunitiesthatareofrelevanceto thedesignofrealisticsoftcereal-basedfoodstargetingtheelderlywhilebeing nutritiousandsensoryappealing. Chapter5 focusesonthedevelopmentof gluten-freebakeryproductsthroughingredientandprocessinginnovations. Specifically,theuseofgluten-freestarch/flour,glutenreplacer,fiber,and proteiningluten-freebakeryproductsaswellasadaptationofprocessing methodsduetoreformulationarediscussed. Chapter6 summarizesthelatest
developmentoffunctionalbakeryproductsusingphytochemicals,specifically catechins,anthocyanins,fucoidanandquercetinextractedfromvarious plantresources.Detailedexamplesoftheirapplicationsaswellastheimpact onproductquality,consumeracceptanceandpotentialhealthbenefitsare provided. Chapter7 coversstrategiesforthereductionofsugar,salt,and fatinbakeryproducts.Itstartswithadiscussionontheroleofeachingredient inbakedproducts.Ingredientsandadditivesthatcansubstitutefat,sugar,and salttoproducedesirablebakerycharacteristicsarereviewedintermsoftheir advantagesanddisadvantages.Furthermore,alternativeprocessestoreduce theuseoffat,sugarandsaltareproposedinthischapter.
Weareparticularlygratefulfortheexcellentcontributionbyoutstanding foodscientistsandengineersfromaroundtheworld.Thisvolumeisthe combinedeffortsof13professionalsfrom8countries(i.e.,Netherland, China,Spain,Switzerland,France,Singapore,andThailand)withavariety ofbackgroundandexpertise.Lastbutnotleast,wewouldliketoacknowledgethekindencouragementfromProfessorFidelToldra,Editorofthe bookseries AdvancesinFoodandNutritionResearch andthehigh-quality editorialassistanceprovidedbyElsevierformakingthepublicationofthis bookpossible.
WEIBIAO ZHOU JING GAO
Towardsthecreation ofpersonalizedbakeryproducts using3Dfoodprinting
LuZhanga,*,MartijnNoortb,andKjeldvanBommelc
aWageningenUniversity&Research,LaboratoryofFoodProcessEngineering,Wageningen,TheNetherlands
bWageningenUniversity&Research,WageningenFood&BiobasedResearch,Wageningen, TheNetherlands
cEquipmentforAdditiveManufacturingDepartment,NetherlandsOrganisationforAppliedScientific Research(TNO),Eindhoven,TheNetherlands
*Correspondingauthor:e-mailaddress:lu1.zhang@wur.nl
Contents
1. Introduction2
2. 3Dprintingtechnologyforbakeryproducts4
2.1 Extrusion-based3Dprinting4
2.2 Other3Dprintingtechnologiesforbakeryproducts12
3. Recentdevelopmentin3D-printedbakeryproducts14
3.1 Developingdoughformulationsforextrusion-based3Dprinting14
3.2 3D-printedbakeryproductscontainingnovelingredients19
4. Personalizationin3D-printedbakeryproducts23
4.1 Personalizedtexture24
4.2 Personalizednutrients27
4.3 Personalizedsatietytomodulateeatingbehavior28
4.4 Consumeracceptance28
4.5 Towardpersonalizednutrition29
5. Conclusions30 Acknowledgments31 References31
Abstract
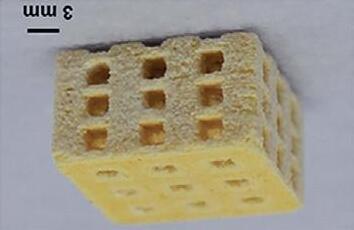
Bakeryproductswithinterestingcolor,shapeandtexturehavebeencreatedusing3D foodprinting.Currentresearchfocusesonthedevelopmentofnewformulationsand theoptimizationoftheprintingandpost-printingtreatmentprocesses,inorderto obtainhigh-quality3D-printedbakeryproducts.Knowledgeaboutfoodrheologyisusefulforthedevelopmentofdoughformulationswithgood3D-printability.Additives suchashydrocolloidscouldimprovetheprintabilityofdough,andnovelingredients areintroducedvia3Dprintingtoproducefunctionalbakeryproductswithpotential healthbenefits.Oneofthemainfuturepromisesof3Dprintingliesinitsabilityto
producebakeryproductsthatarepersonalizedintermsofsensorialpropertiesand nutritionalcomposition,inordertomeetthepreferencesanddietaryrequirements ofindividualconsumers.Thischapteraddressesthemostrecentdevelopmentsin 3D-printedbakeryfoodsandhighlightssomeimportantresearchtopicstofurther advancethisfield. 1.Introduction
3Dprinting,alsoknownasadditivemanufacturing,isatechnology characterizedbyalayer-by-layerdepositionofmaterialsaccordingtoadigitaldesignfile.3Dprintingoffoodwasfirstintroducedbyresearchersfrom CornellUniversity,andthedevelopedFab@Homemodelwasusedtoprint paste-likefoodmaterialsbyextrusion(Periard,Schaal,Schaal,Malone,& Lipson,2007).3Dprintingprovidesanewwayofcreatingfoodproducts. Itspotentialadvantagesincludepossibilitiestocustomizefooddesignsthat cannotbeeasilyachievedwithconventionalmanufacturingmethods(e.g. complexgeometryandinternalstructures);simplifyingthesupplychain throughflexible,local,on-demandfoodmanufacturing( Jayaprakash etal.,2020);broadeningtherangeofingredientsusedforfoodproduction (e.g.theutilizationoffoodwaste/by-stream)(UpprintingFood,2021);providingfoodcompanieswithnewopportunitiestointeractwiththeirconsumers(Blurhapsody,2021);andlastlyenablingpersonalizednutrition (Liu&Zhang,2019)andconsumerempowerment(Caulier,Doets,& Noort,2020).
Todate,various3Dfoodprintingtechnologieshavebeendeveloped, includingextrusion-basedprinting,binderjetting,inkjetprintingand selectivelasersintering.Amongthesetechnologies,extrusion-basedfood printingisthemostpopularmethodinfoodprintingowingtoitssimplicity (Sun,Zhou,Yan,Huang,&Lin,2018)andthefactthatextrusionprocesses arewell-knownandwidelyappliedinconventionalfoodprocesses.Food materialsthathavebeenusedforextrusion-basedprintingarecookiedough (Pulatsu,Su,Lin,&Lin,2020),proteingel(Liu,Bhandari,Prakash, Mantihal,&Zhang,2019; Liu,Zhang,etal.,2019),surimi(Gudjo ´ nsdo ´ ttir, Napitupulu,&PettyKristinsson,2019),tomatopaste(Zhu,Stieger,van derGoot,&Schutyser,2019)andchocolate(Hao,Li,Gong,&Xiong, 2019),tonameafew.
Bakeryproductsareprimarilybasedoncerealingredients.Theyhavean importantnutritionalroleasamainsourceofmacronutrientsandessential micronutrientsinourdailydiet.Besidestheirnutritiouscerealcontent, sugarsandfatsareaddedtomanybakeryproducts,whichareoverconsumed
andareconsideredlesshealthy.Thus,reducingtheamountofthoseingredientswhilekeepingtheattractivenessofbakeryproductsisanimportant targetforproductreformulationforfoodscientistsandthefoodindustry. Also,inrecentyears,functionalbakeryproductshavereceivedincreasing attentioninscientificstudies.Functionalfoodscanbedefinedasmodified foodorfoodingredientsthatcanprovidehealthbenefitstoconsumers beyondtheirbasicnutrients(Zhang,2018).Theconceptoffunctionalfoods involvesthreemainaspects,specificallyhealthbenefits,nutritionalfunction andtechnologicalprocesses(Bigliardi&Galati,2013).Thetechnological processesaspectinvolves(i)thedevelopmentoffunctionalfoodsbyoptimizingconventionalprocesses,e.g.fortifyingfoodswithdietaryfiber; (ii)thedesignoftechnologieswhichpreventthedeteriorationofactive ingredients,e.g.(micro)encapsulation;and(iii)thedevelopmentofnew technologiesthataimtodesignandmanufacturefoodsfunctionalizedto theneedsofindividualconsumers,e.g.byapplyingresultsfromnutrigenomics tocreatepersonalizedfoodsthrough3Dprinting.
Novelbakeryproductsandhealthyingredientshavebeenstudiedinthe fieldof3Dfoodprinting,forexampleprobiotic-containingcookies(Zhang, Lou,&Schutyser,2018),cereal-basedsnacksenrichedwithedibleinsects (Severini,Azzollini,Albenzio,&Derossi,2018)orwithmicroalgae (Uribe-Wandurragaetal.,2020),andpersonalizedsnacksforsoldiers (Caulieretal.,2020).Theresultsfromthesestudiesindicatethat3Dfood printingcouldbeausefultoolforthecreationofpersonalizedbakeryproductswithtunabletexture,flavor,appearance,satietyperception,andeven nutritionalcontent.
Inthischapter,weaimtoillustraterecentadvancesandchallengesrelated tothedevelopmentof3D-printedpersonalizedbakeryproducts.Morespecifically,weintroducetheprincipleofextrusion-based3Dprinting,the developmentofextrusion3Dprintingsystemsandthepost-processingtreatmentusedtoobtainedibleproductsindetailin Section2.Inaddition,we willbrieflydiscussother3Dfoodprintingtechnologiesusedforfabricating bakeryproducts.Subsequently,wediscusstherecentdevelopmentof 3D-printedbakeryproductsin Section3,withafocusontheusageof extrusion-basedprinting.Additionally,novelingredientsusedin3Dprintedbakeryproductssuchasprobiotics,microalgaeandedibleinsects areaddressedinthissection.In Section4,weprovideamoredetaileddiscussionon3Dprintingofpersonalizedbakeryfoods.Finally,thischapteris concludedwithdiscussionsofremainingchallengesandfutureresearch directionsrelevantforthedevelopmentofpersonalizedbakeryproducts using3Dfoodprinting.
2.3Dprintingtechnologyforbakeryproducts
Sincethefirstexplorationin2007,avarietyoftechnologieshavebeen developedfor3Dprintingfoodmaterials,includingextrusion-based3D printing,binderjettingprinting,selectivesinteringprintingandinkjetprinting(Baiano,2020). Table1 describestheprintingmechanismofthesefour printingtechnologies.Various3D-printedbakeryproductshavebeencreatedusingthesedifferenttechnologies,asshownin Table1.Basedonliterature,themostwidely-studiedprintingtechniqueforbakeryproductsis extrusion-based3Dprinting.Therefore,inthischapter,wewillmainlydiscussextrusion-basedprintingofbakeryproducts,andonlybrieflyaddress theothertechnologies.
2.1Extrusion-based3Dprinting
2.1.1Extrusion-based3Dprintingofbakeryproducts
Extrusion-based3Dprintingisoftenusedtofabricatecereal-basedfoods. Duringextrusion-based3Dprinting,asemi-solidfoodmaterial(suchas dough)inasyringeisextrudedfromanozzleontotheprintingplatform. Theextrudedfilamentoffoodmaterialsisdepositedinalayer-by-layerfashiontoforma3Dstructure.Theextrusionprocessofthefilamentcanbe drivenbyairpressure,mechanicalforce,orextrusionrotationinapneumatic,piston-basedorascrew-basedsystem,respectively(Sunetal., 2018).Ideally,foodmaterialsusedforextrusion-basedprintingshouldbe pseudoplasticfluidsthatshowshear-thinningbehaviorsotheycanbeeasily extruded.Inaddition,thematerialsshouldhavearapidstructuralrecovery afterdeposition,inordertoformaself-supportingstructure.Manyfoodformulationscanbeextrudedatambienttemperature(e.g.doughorvegetable pureeprinting).Forcertainfoodmaterialssuchaschocolateorproteingel, thefilamentisextrudedatelevatedtemperature,andtheextrudedfilament showsaphasetransitionfromaliquid-liketoasolid-likestructureupon coolingatambienttemperature.Theselectionoftheprintingtemperature dependsonmaterials’thermalpropertiessuchasthemeltingpointofchocolateandthegelationtemperatureofproteindispersion.
Ingeneral,theadvantagesofextrusion-basedprintingincludethewide choiceoffoodmaterialsandtherelativesimplicityoftheprintingsystem. However,printingofdoughformulationsandcreatingcomplexdesigns ofcereal-basedfoodstructureswithahighresolutionremainchallenging. Forexample,theprinted3Dstructureofdoughmaydeviatefromthedigital
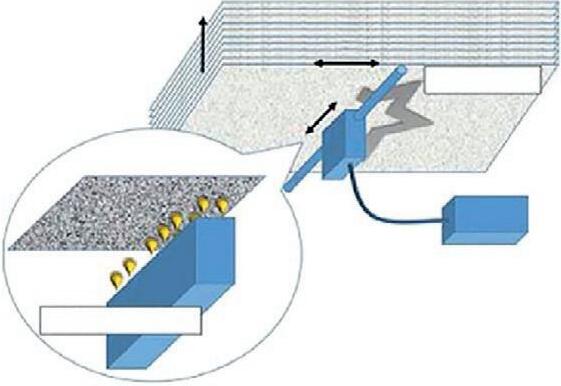
Table1 Principles,schematicdiagramsof3Dfoodprintingtechnologies(Sun,Zhou,Huang,Fuh,&Hong,2015)andcorrespondingexamplesofbakeryproducts thatarecreated:extrusion-based3Dprinting(Zhang,Lou,&Schutyser,2018),binderjetting(Holland,Foster,&Tuck,2019),selectivelasersintering(Noort,Van Bommel,&Renzetti,2017)andinkjetprinting(Foodjet,2021).
MethodExtrusion-based3DprintingBinderjettingSelectivesinteringprintingInkjetprinting Schematic
PrincipleSemi-solidfoodmaterialisextrudedviaa nozzleontoaplatformlayerbylayer; materialformsaself-supporting3D structure.Bothroomtemperatureprinting andhot-extrusionareused,dependingon materials’properties.
Powderparticlesaredistributedevenlyon theprintbed,andaliquidbinderis depositedontothetargetareatobindthe powders.Anewlayerofpowderisthen addedtotheprintbedandthesame depositionprocessisrepeatedaccordingto thedigitaldesign.
Heatingsource(e.g.laserandhotair)fuses powderparticlestoformasolidlayerwhile unsinteredpowderprovidessupporttothe printedstructure.Afterprinting,sintered structurecanberemovedfromthepowder bed.
Astreamofdroplets/liquidisdispensed fromaprintheadinadrop-on-demand manner,andsolidifiedtoa“2.5 dimensional”imageonthesurfaceofthe substrates.
Decoratedbakerygoods(left:cavity filling;right:surfacedeposition)
Fig.1 Threestagesoftheextrusion-based3Dprintingprocessincludingformulation development,printingprocessandpost-printingprocessing;andselectiveindicators ofproductqualityarelisted.
design,whichcouldbecausedbyimperfectionsduringprintingsuchaslackof continuousstructureandlossoflayerdifferentiation(e.g.collapsingofthe structure)(Pulatsuetal.,2020).Inaddition,post-printingheattreatment (e.g.baking)isoftenrequiredtoobtainediblecereal-basedfoods.Heating, however,canoftenresultinaloweringofviscosityandhenceinduceflow ofthematerial,whichmeansthattheproductlosesits3Dshapeduring post-processing(Liu,Zhang,Bhandari,&Wang,2017).Additionally,expansionofthe3Dstructuremayoccurduringbakingduetothepresenceof leaveningagentintheprintingmaterial.Suchexpansionmayresultinasignificationdeformationofthecarefullydepositeddesign,possiblyleadingtoa failedprintedresultsafterbaking.Thisisespeciallyproblematicwhenaiming forasophisticatedgeometricaldesignwithadetailedinfillpatternoraspecific poreorvoidpercentage.Therefore,whenoptimizingtheproductionprocess of3D-printedbakeryfoods,oneneedstoconsidertheeffectsofformulation design,printingsettings,andtheconditionsusedduringpost-printingtreatmentonthepropertiesandqualityofthefinalproducts(see Fig.1).Somekey factorsthatinfluencetheperformanceofeachstageduringprintingareselectivelylisted.Thosefactorsneedtobewellcontrolledinordertoachievea successfullyprintedproductswithhighquality,whichwillbeelaboratedmore laterinthissection.
2.1.2Extrusionprintingsystems
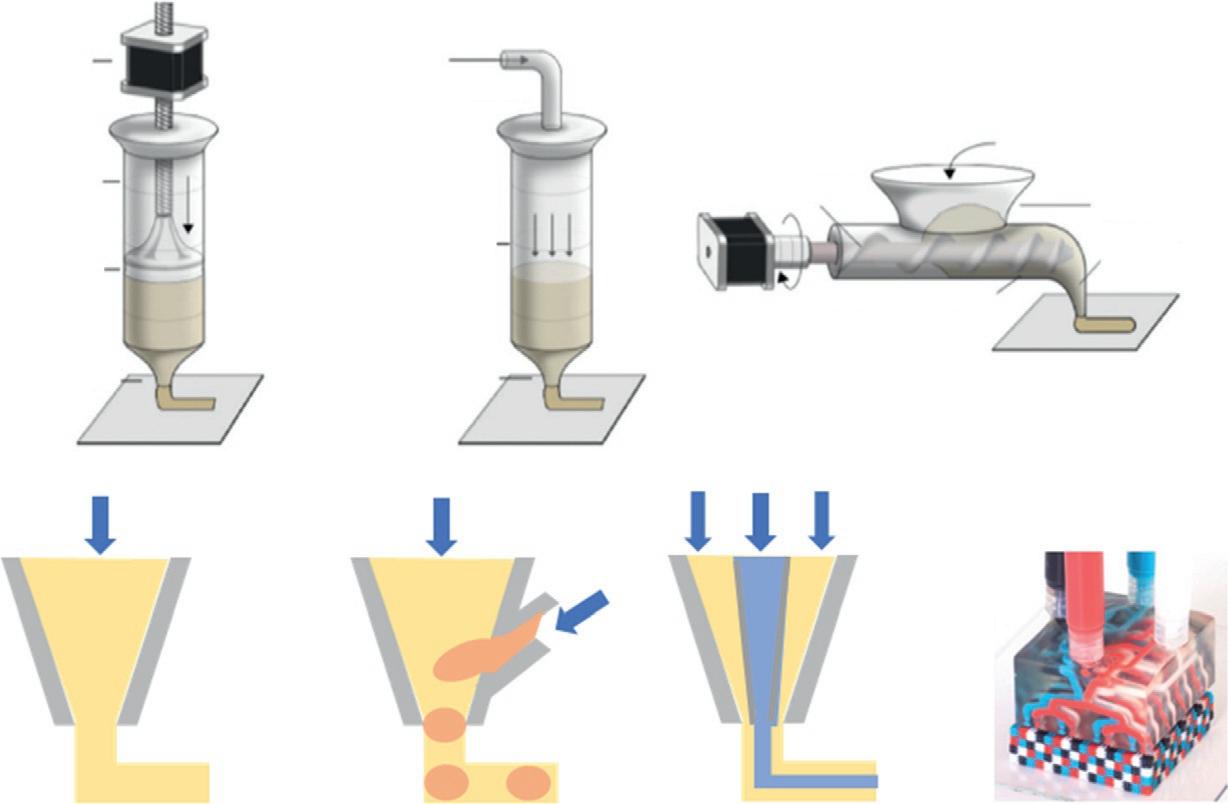
Asmentionedearlier,threeextrusionmechanismshavebeendevelopedin extrusion-based3Dprinting,i.e.piston-,pneumatic-,orscrew-driven (Schwabetal.,2020),amongwhichthepiston-drivenmechanismisthe mostcommonlyusedmechanismforfoodmaterials(see Fig.2A).
Inbrief,inapiston-drivensystem,asteppermotorisprogrammedto generatelinearmotionoftheplungertopushthefoodmaterialoutof thenozzle.Theextrusionrate(i.e.,volumetricflowrateofthematerial) canbecontrolledbyadjustingthemotorspeed,whichneedstobe
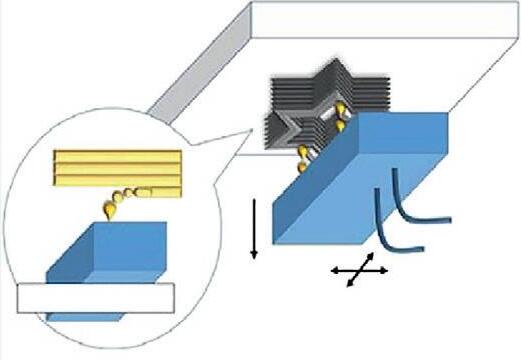
Fig.2 Extrusion3Dprintingsystem(A)threeextrusionmechanisms:piston-,pneumatic-, orscrew-drivensystems(fromlefttoright)(Sunetal.,2018);(B)schematicdrawingsof variousnozzleconfigurationdesigns:singlenozzle,nozzlewithside-inlet(modifiedfrom Schutyseretal.,2018),coaxial-nozzle(modifiedfrom Vancauwenberghe,Verboven, Lammertyn,andNicolaï,2018),complexnozzlefor(non-food)multi-materials(SkylarScott,Mueller,Visser,&Lewis,2019)(fromlefttoright),bluearrowsindicatetheflowdirectionofmaterial.
controlledtogetherwiththenozzlemovingspeedtoachieveadesiredfilamentformation.Thissystemhasbeenusedtoprintsemi-solidorsolidfood products(Sunetal.,2018).
Inpneumatic-drivensystem,airpressuregeneratedbythepneumatic pumppushesthefoodmaterialoutofthenozzle,andtheextrusionrate canbecontrolledbyadjustingtheairpressure(see Fig.2A).Thissystem isrelativelymoresuitableforprintingpasteorgel-likefoodmaterialswith arelativelylowviscosityduetothelimitedairpressure(e.g.upto5.5baras reportedin Schutyseretal.(2018)).Itisalsooftenusedinbio-printingapplicationstoprinthydrogels.
Inscrew-drivensystem,amotordrivesthemovementofthescrewthat continuouslypushesfoodmaterialsdownwardsandthroughthenozzle. Thissystemisparticularlysuitablefortheextrusionofmaterialswithhigh viscosity(upto104 Pas).Forexample, Mantihal,Prakash,Godoi,and Bhandari(2017) developedarotaryscrewextrusionmethodto3Dprint chocolate.Inaddition,continuousdosing/printingcouldpotentiallybe
Single nozzleNozzle with side-inletCoaxial nozzleComplex nozzle
(a) (b)
Another random document with no related content on Scribd:
devised with an intent of making a tunnel rather than a direct opening, through which, as needed, a soft rubber tube may be introduced, whose walls shall collapse at other times and close themselves, if necessary, with a little assistance, by pressure, thus preventing leakage. Sometimes it is possible to attain this ideal. At other times a rubber tube is worn a greater part at least of the twenty-four hours.
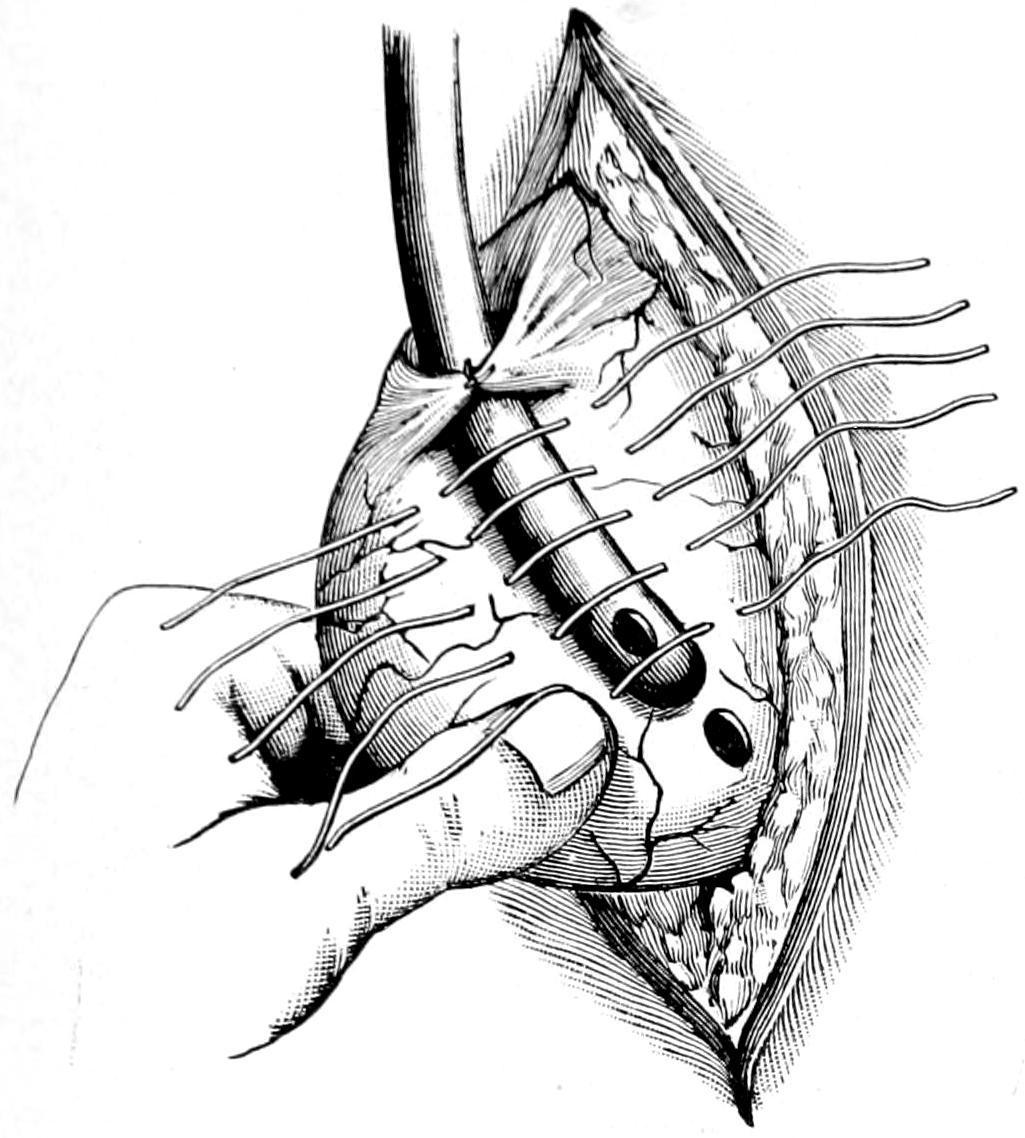
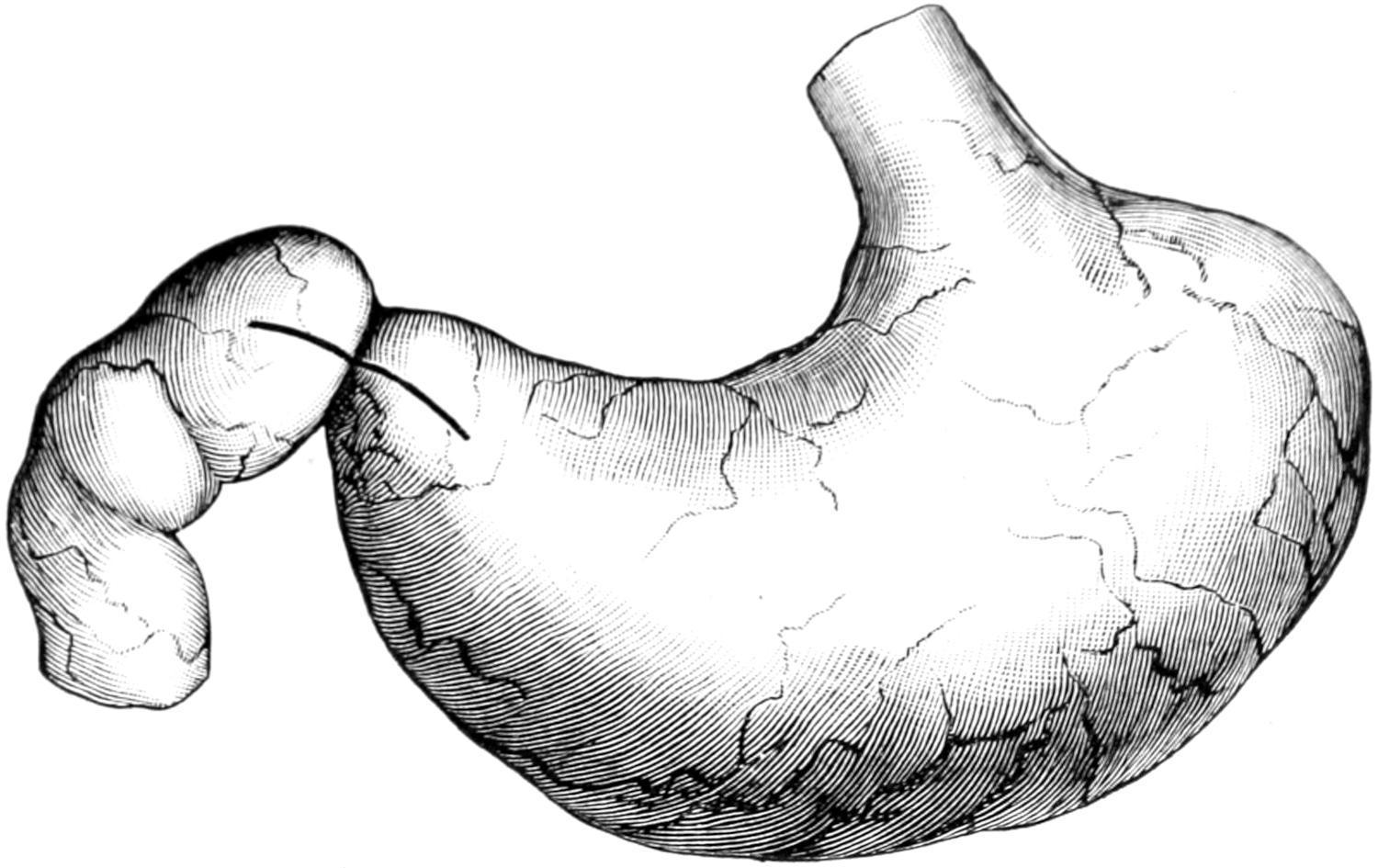
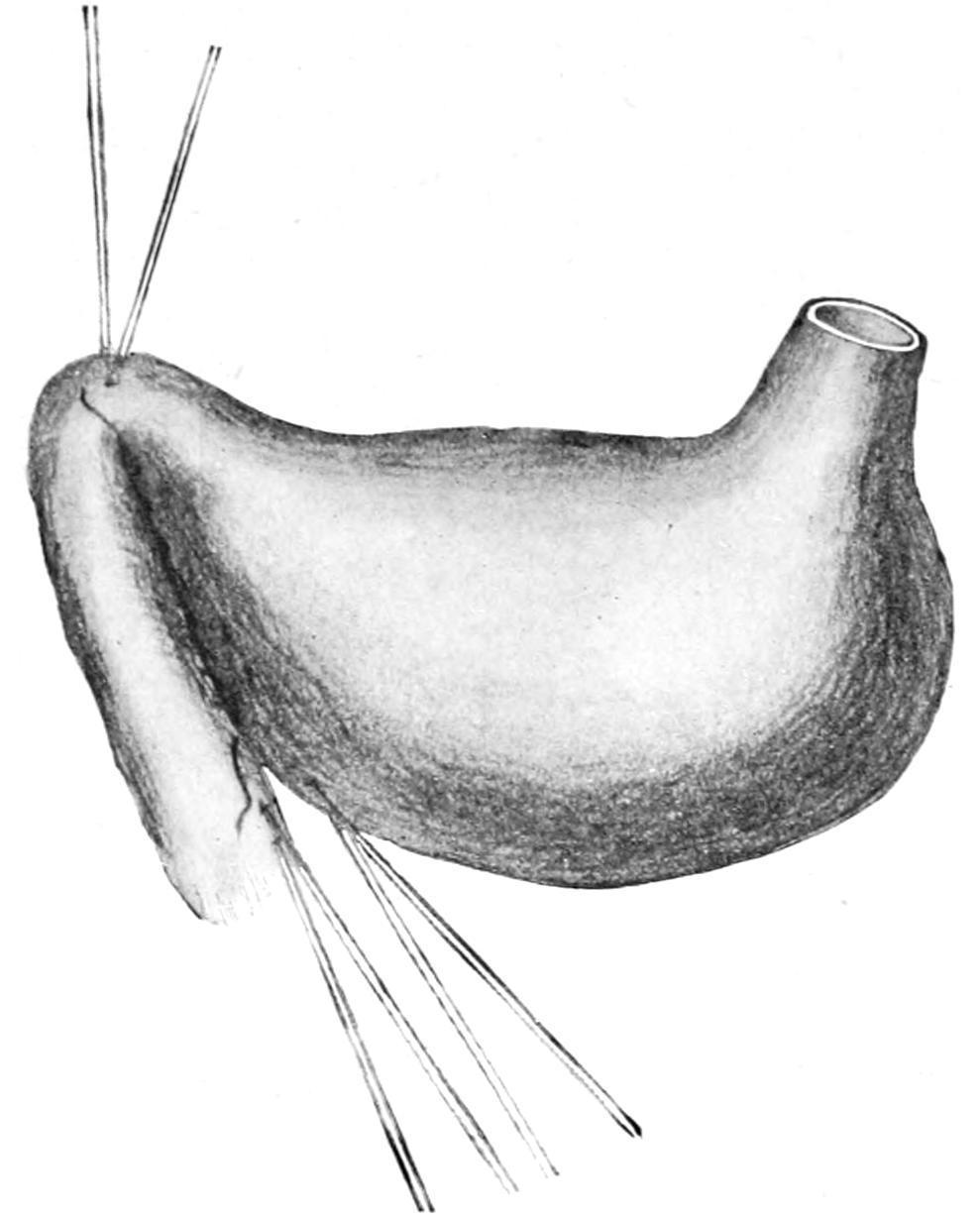
Gastrostomy: Witzel’s method. Tube in position; sutures ready to tie. (Richardson.)
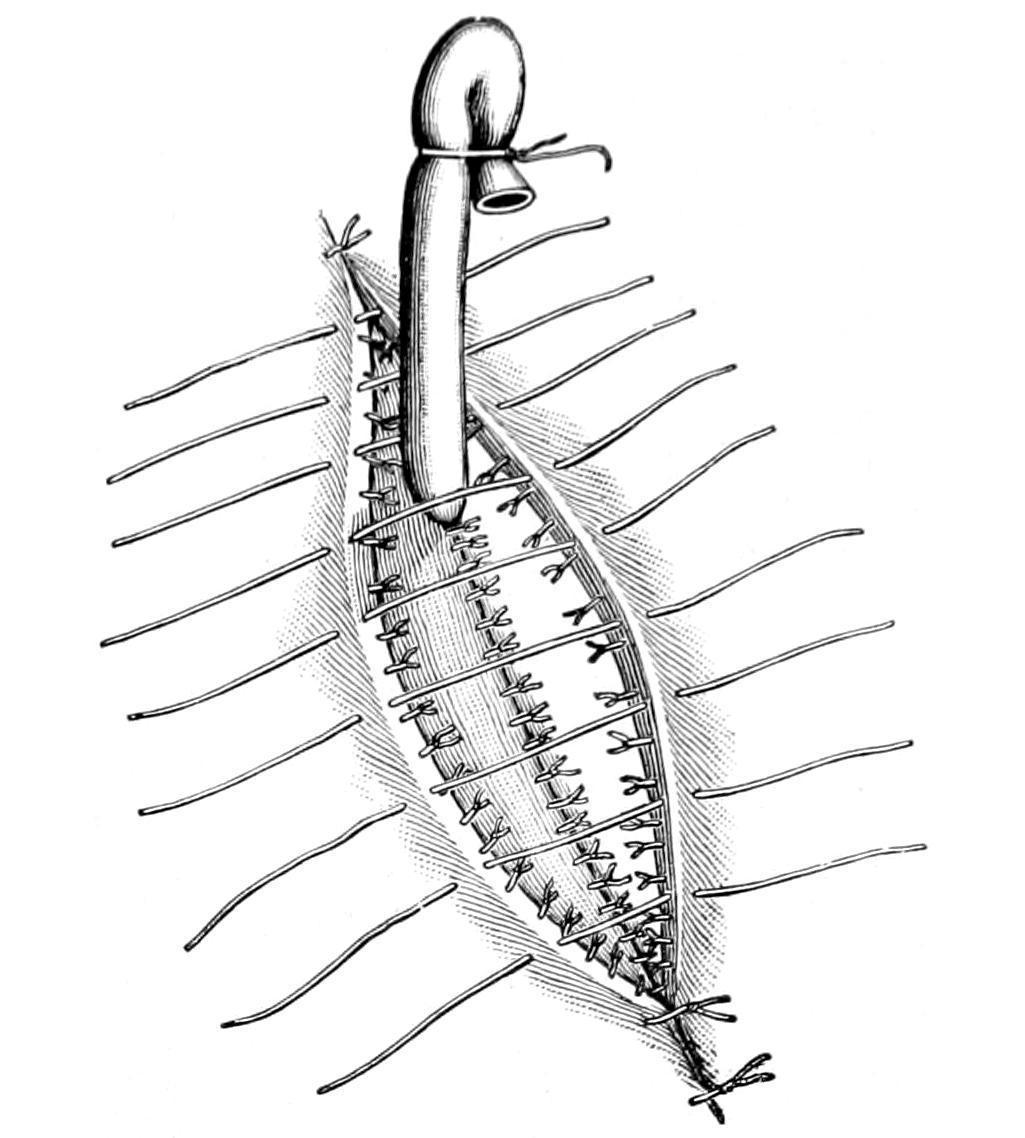
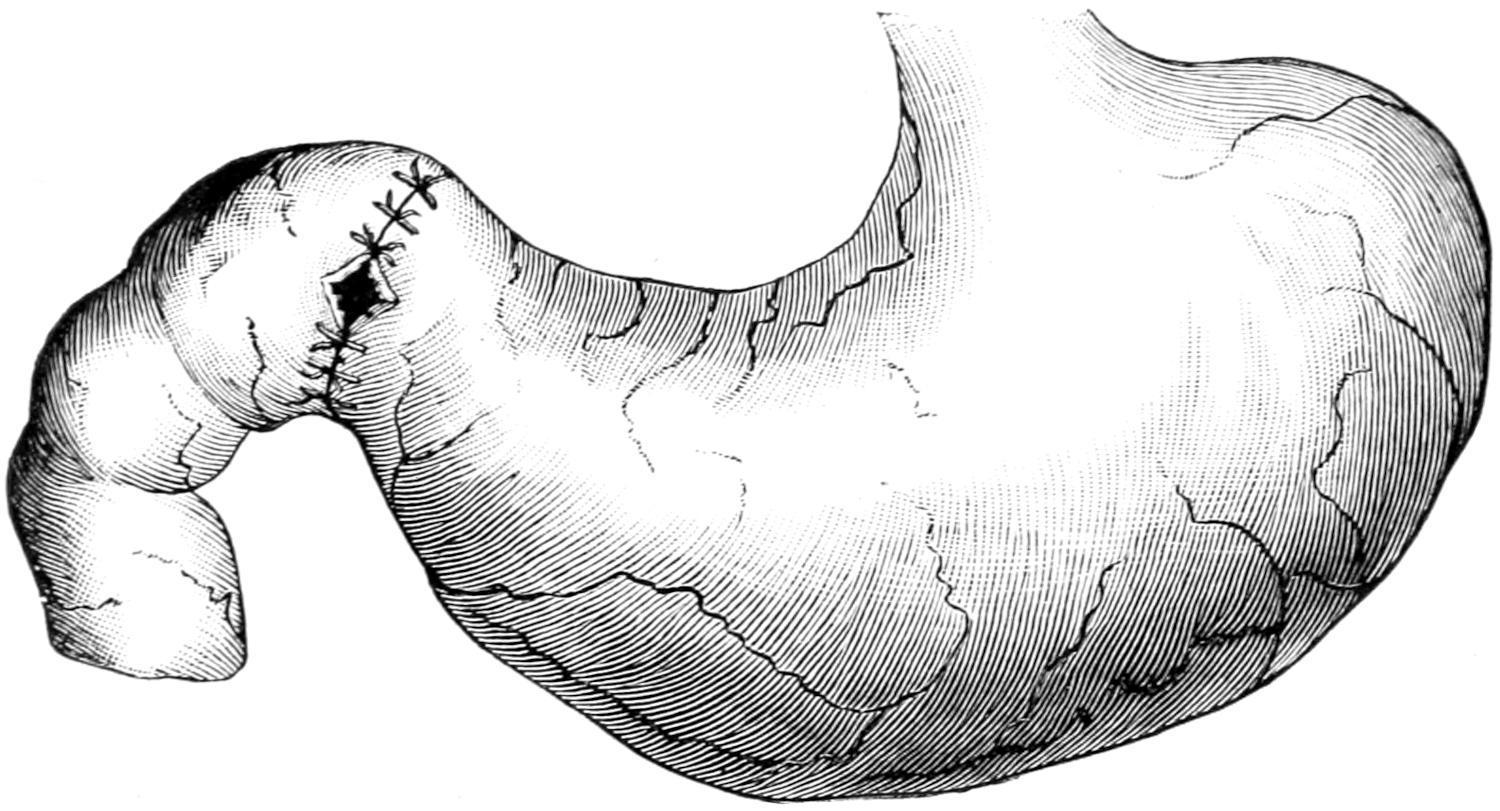
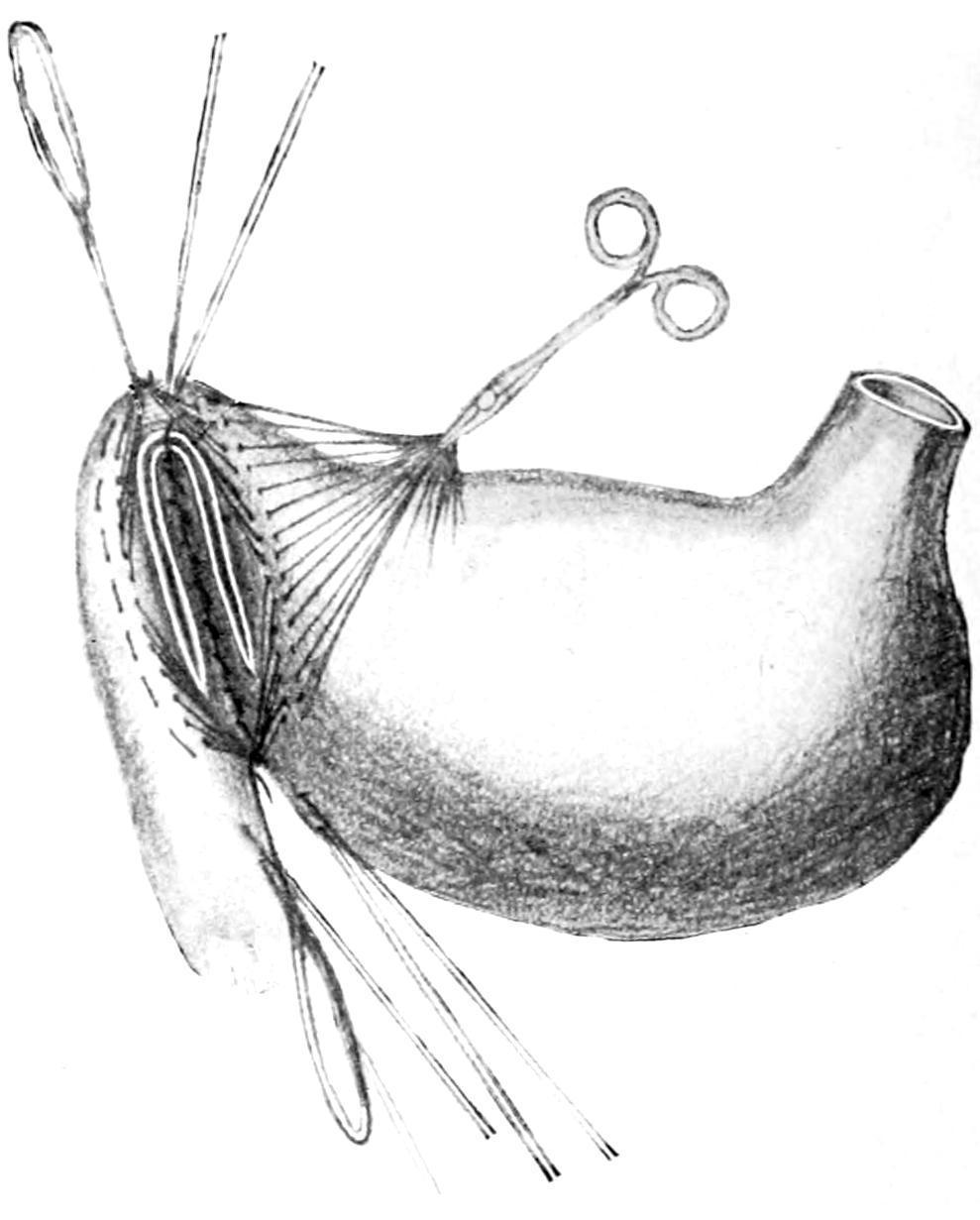
Gastrostomy: Witzel’s method. Tube in position; sutures ready to close abdominal wall. (Richardson.)
FIG. 529
FIG. 530
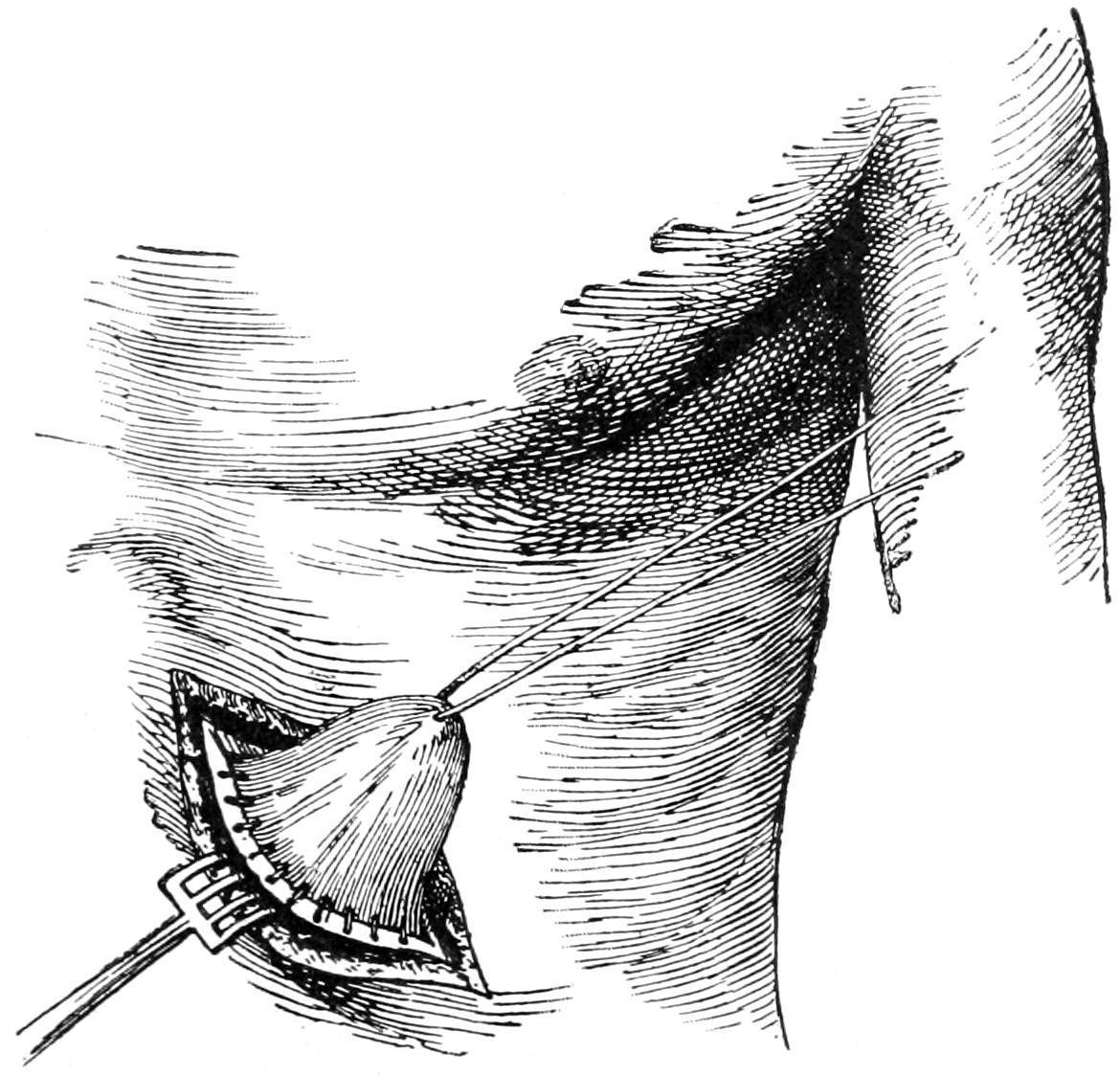
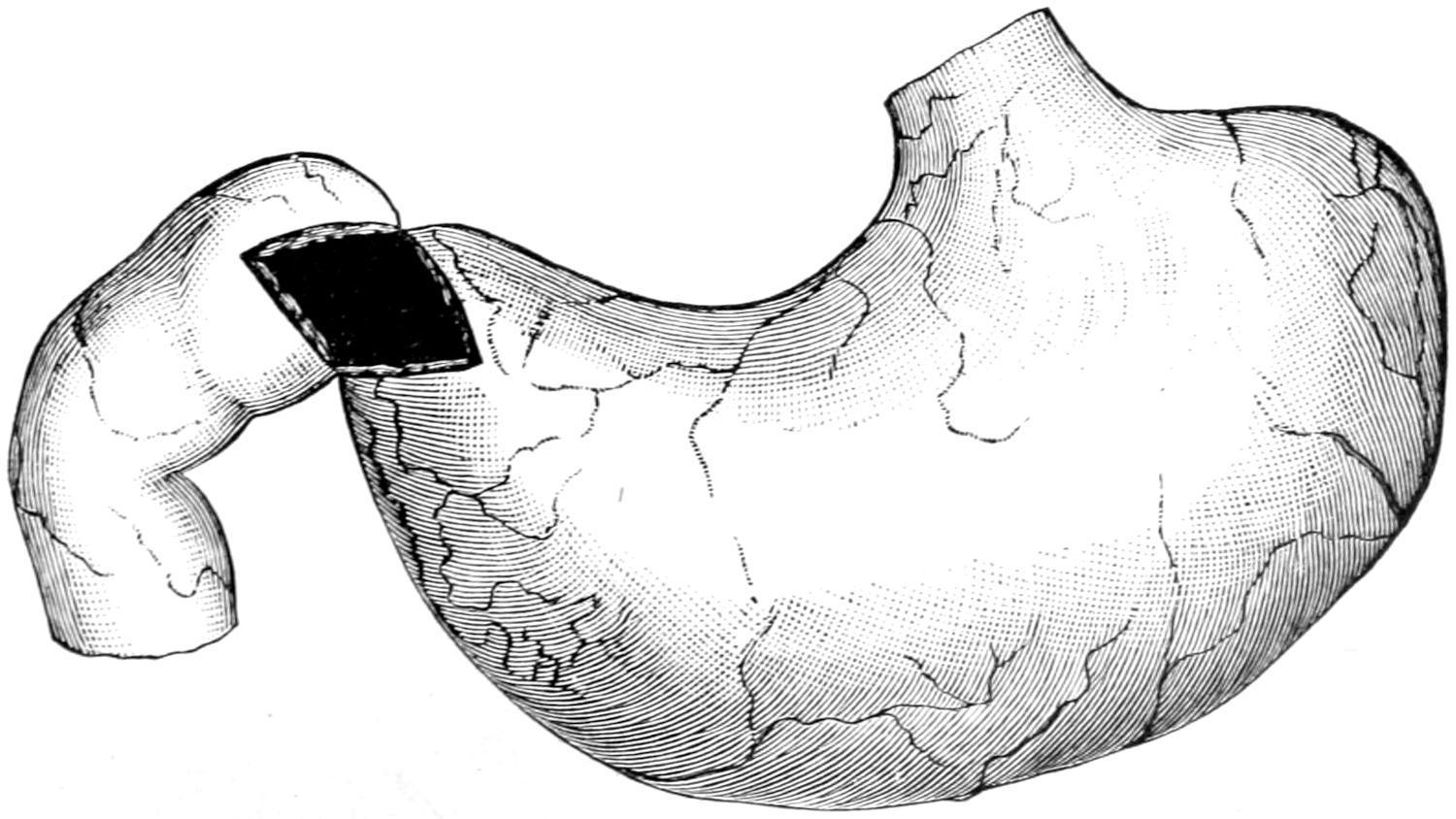
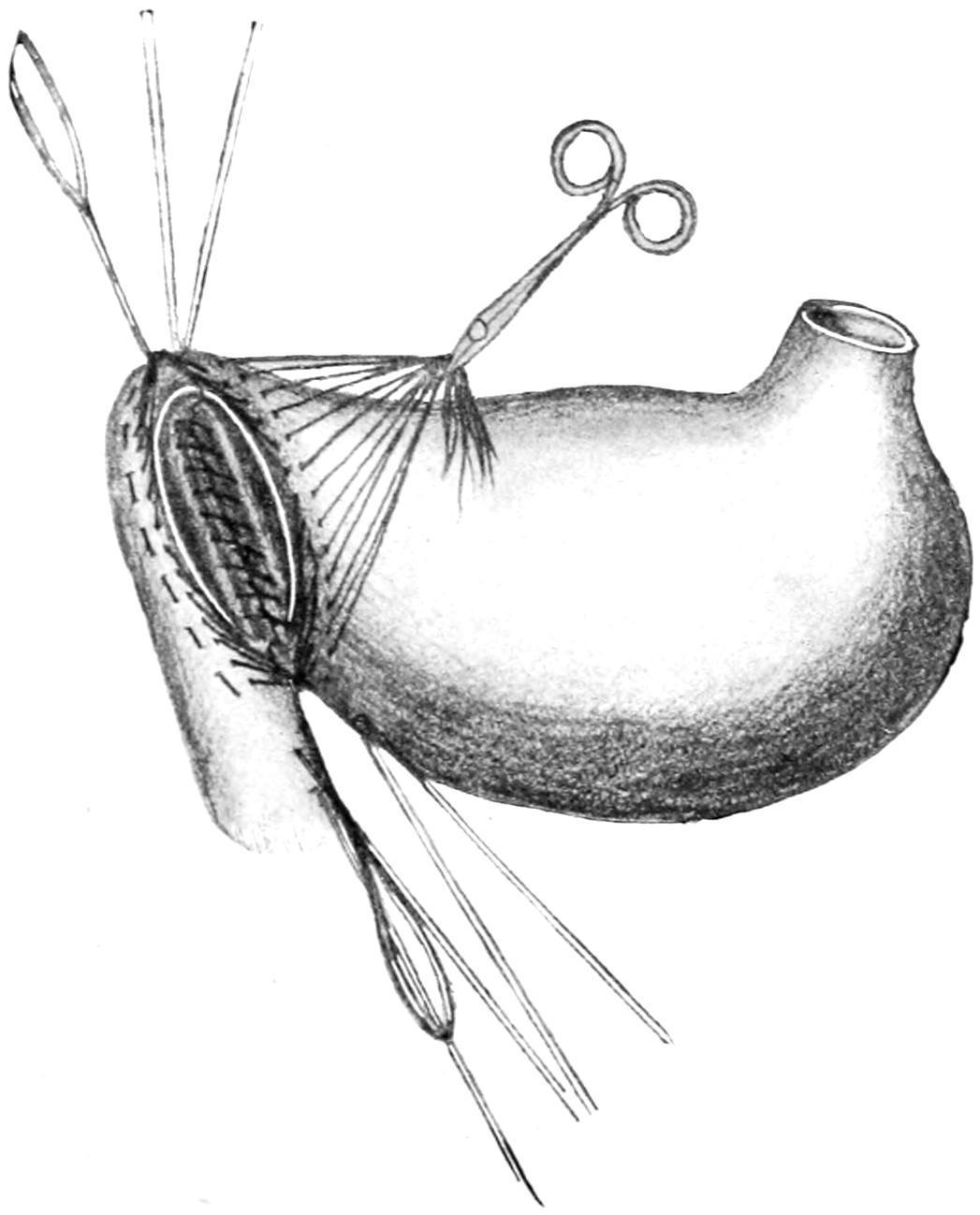
Gastrostomy by Frank’s method: cone of stomach stitched into the peritoneal wound. (Richardson.)
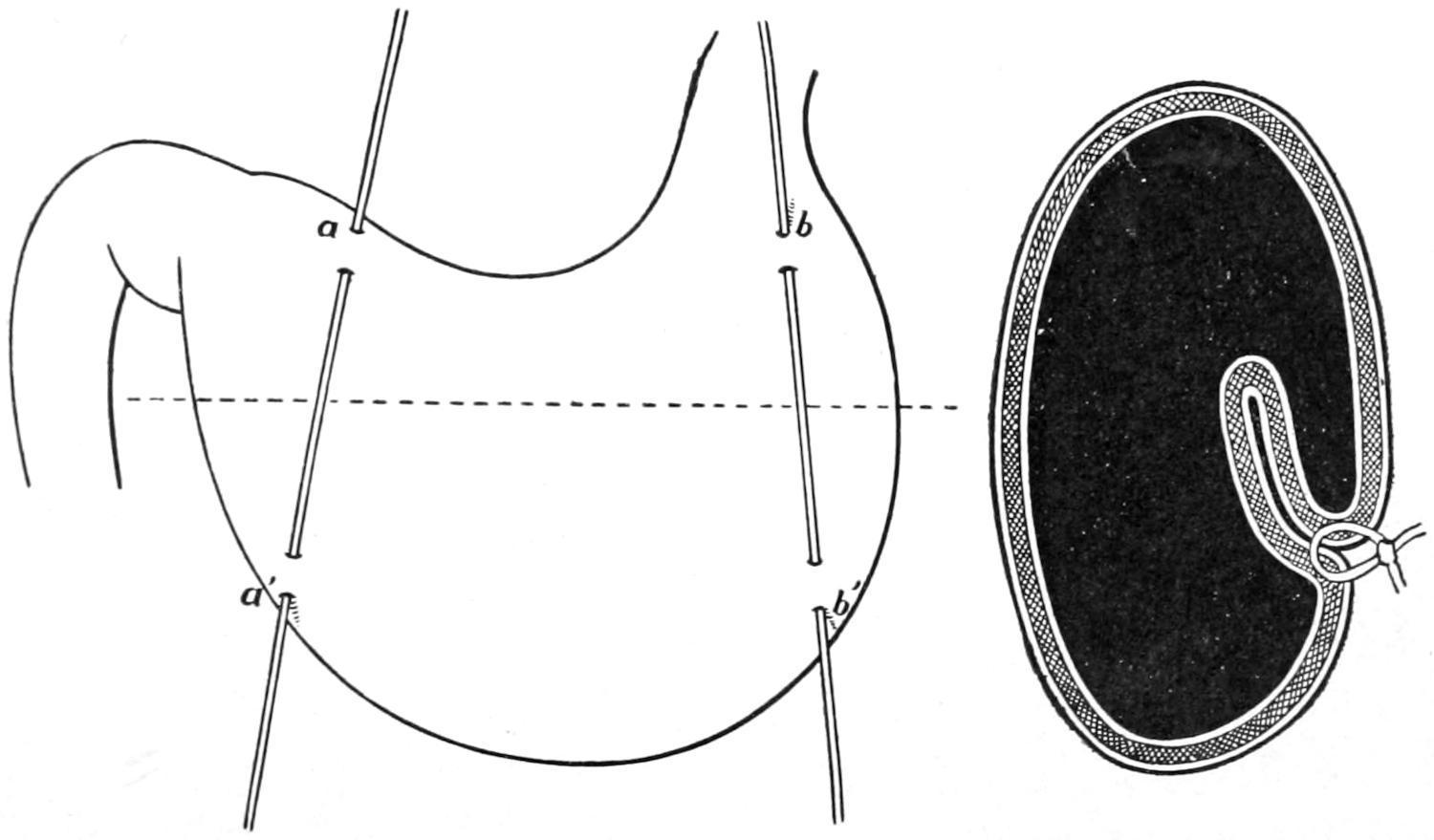
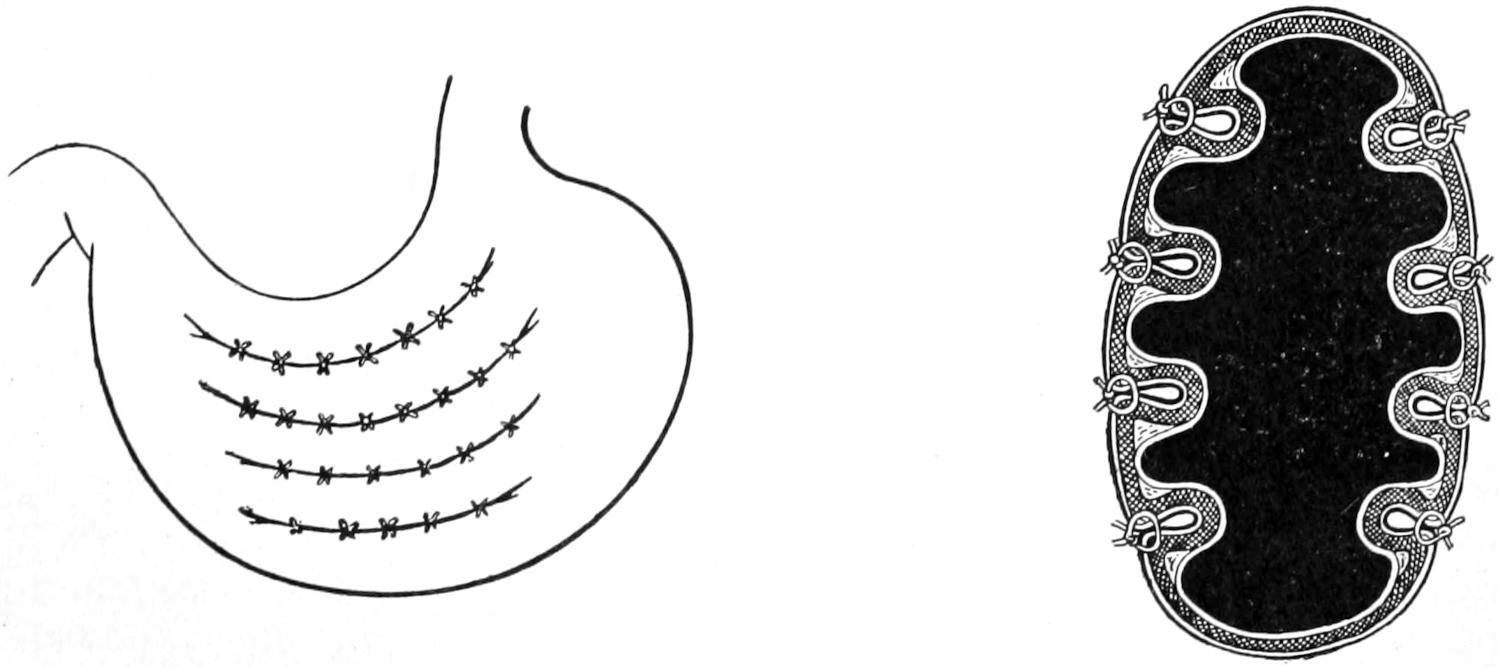
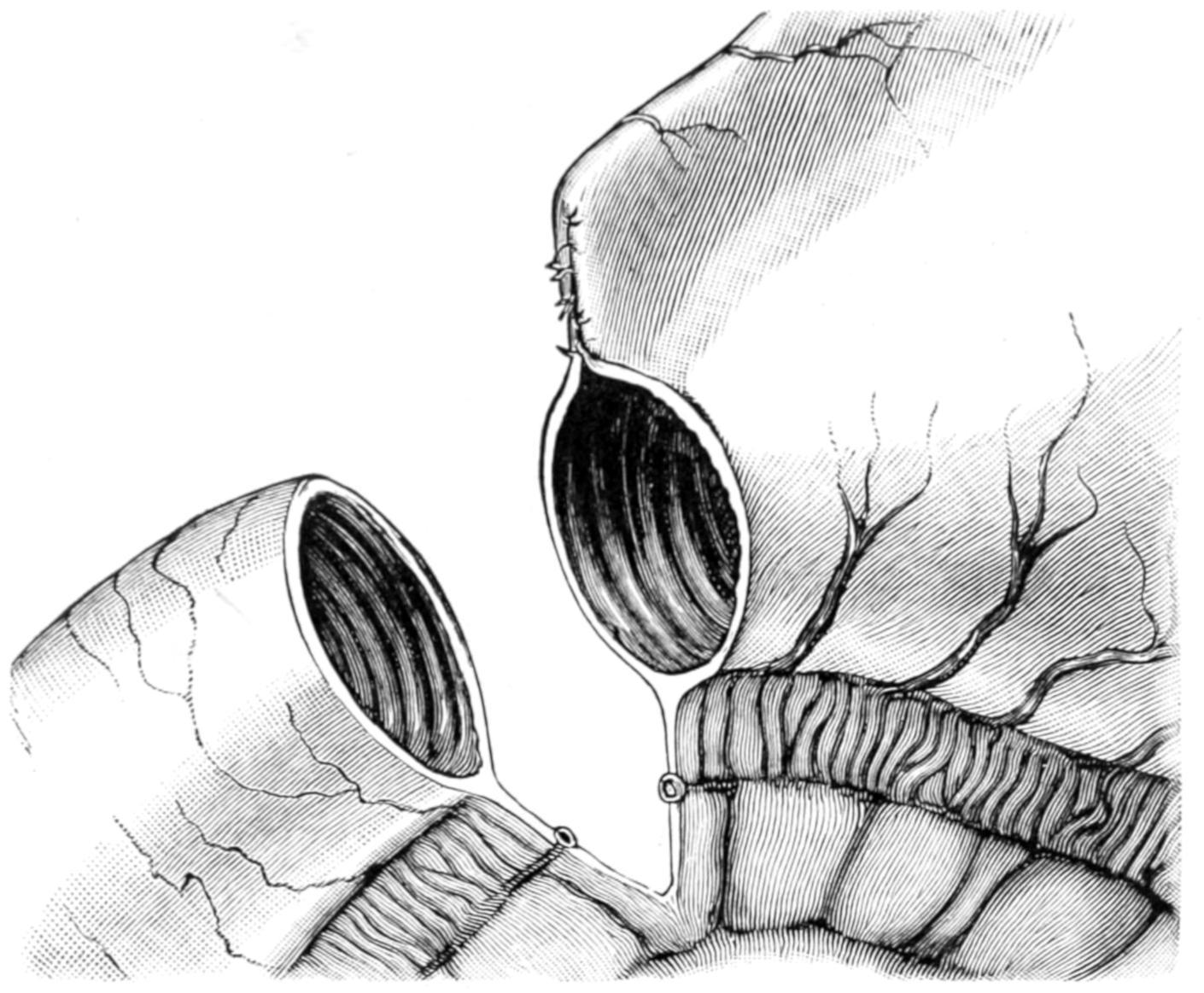
All operative methods include fixation and consequent adhesion of the anterior stomach wall to the parietal peritoneum, just below the border of the ribs. Of the many methods employed the following will be described, most of which can be easily appreciated in diagram: Figs. 529 and 530 illustrate, for instance, Witzel’s method, where a sterile, soft rubber catheter is infolded in the stomach wall, and
finally passed into its cavity through the smallest opening that may suffice for the purpose, after which the outer layer of the stomach is completely closed over it. The stomach itself is stitched to the deep margins of the external wound, and these are then closed without drainage. If everything has been neatly done feeding may be begun within a few hours. Care should be exercised about passing into a stomach which has long been without much food a quantity which may disturb it, or of a quality which may distress it. A procedure very much like Witzel’s is that described by Marwedel, who first sews the stomach to the abdominal wound after drawing it partly into the wound, in order to afford sufficient working material, and then infolds the tube and inserts its lower end through a small opening. This is perhaps preferable, since the stomach being so fastened up at once there is no possibility of leakage into the abdomen.
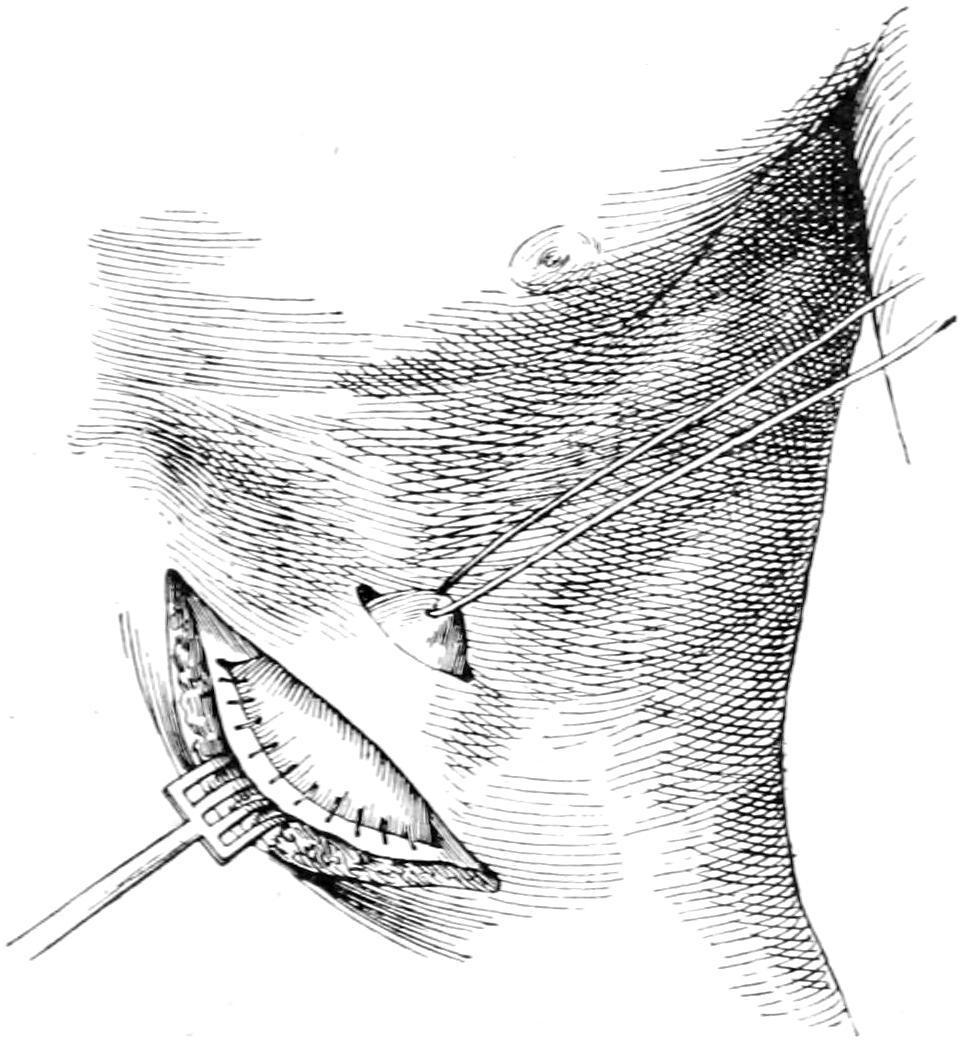
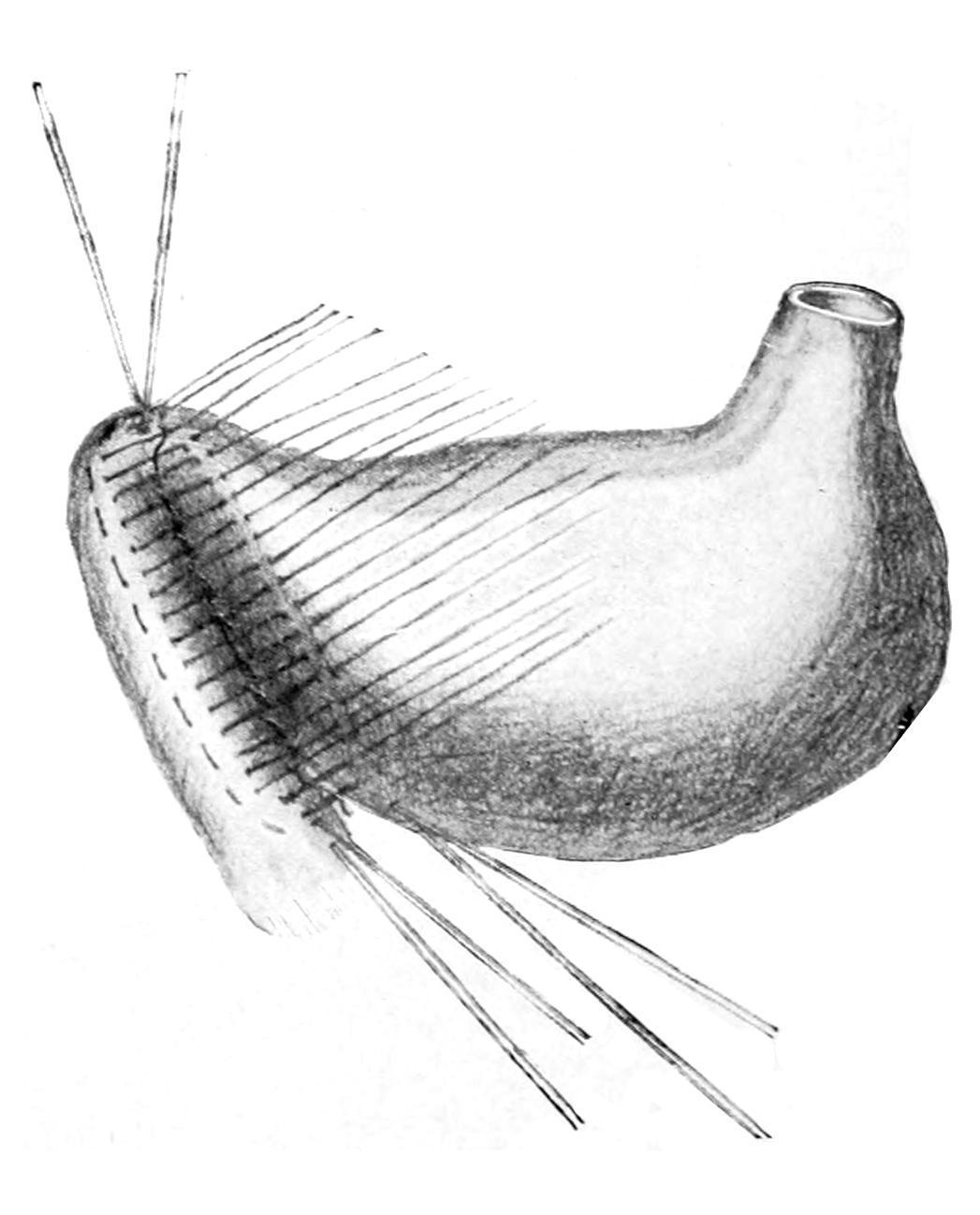
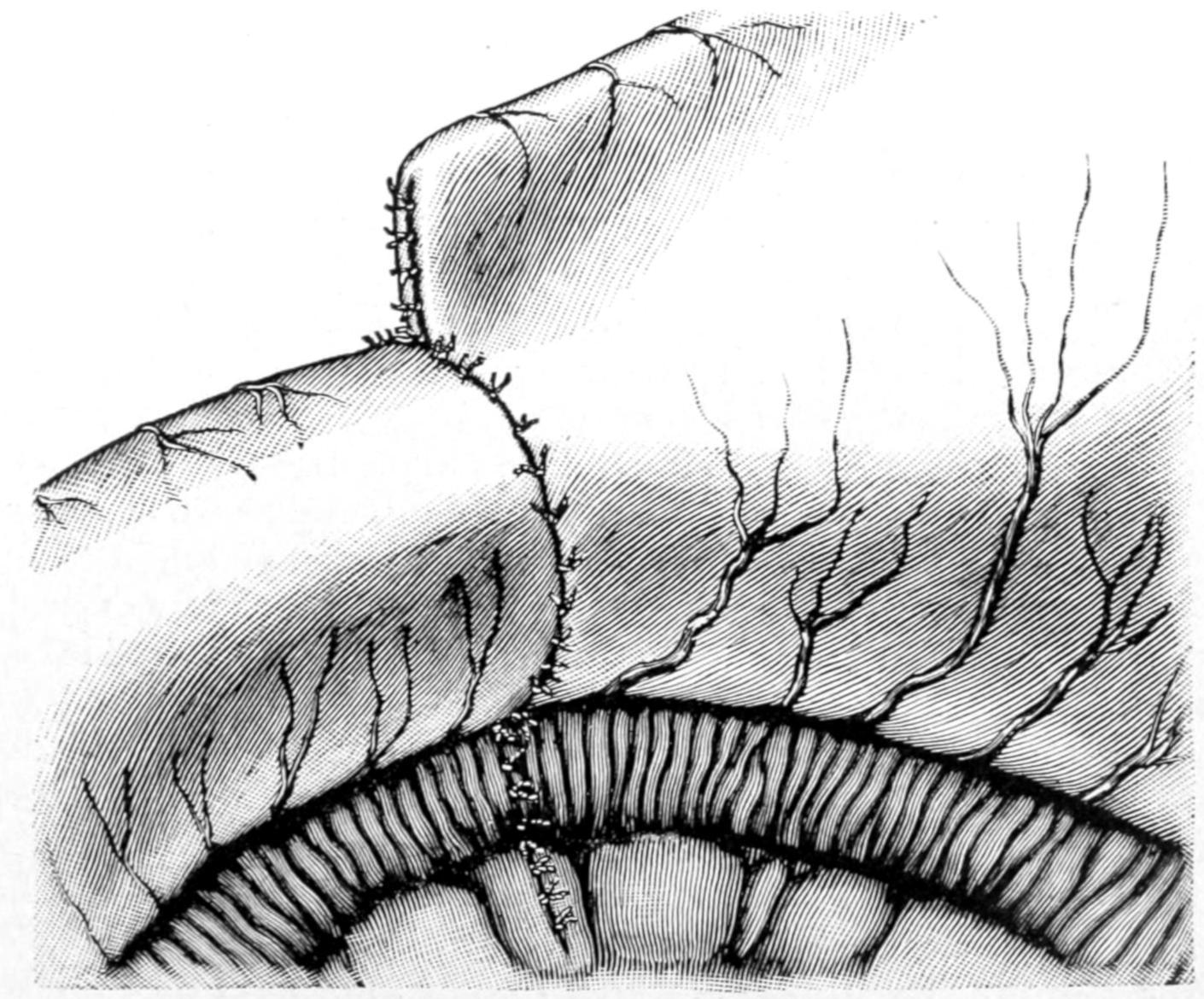
Figs. 531, 532 and 533 illustrate Frank’s method, where the stomach is pulled up through a sufficiently long incision and drawn out into a cone, whose apex is then brought out through a second small incision, parallel to the first and at a distance of an inch or so from it. Here an actual opening is made into the stomach, while the cone is fastened to the skin here and to the peritoneum through the other opening, which is then completely closed. This method cannot be applied to a contracted stomach.
Gastrostomy by Frank’s method: cone of stomach pushed through the second skin incision. (Richardson.)
Gastrostomy by Frank’s method: suture of abdominal wound; stomach stitched in the skin incision. (Richardson.)
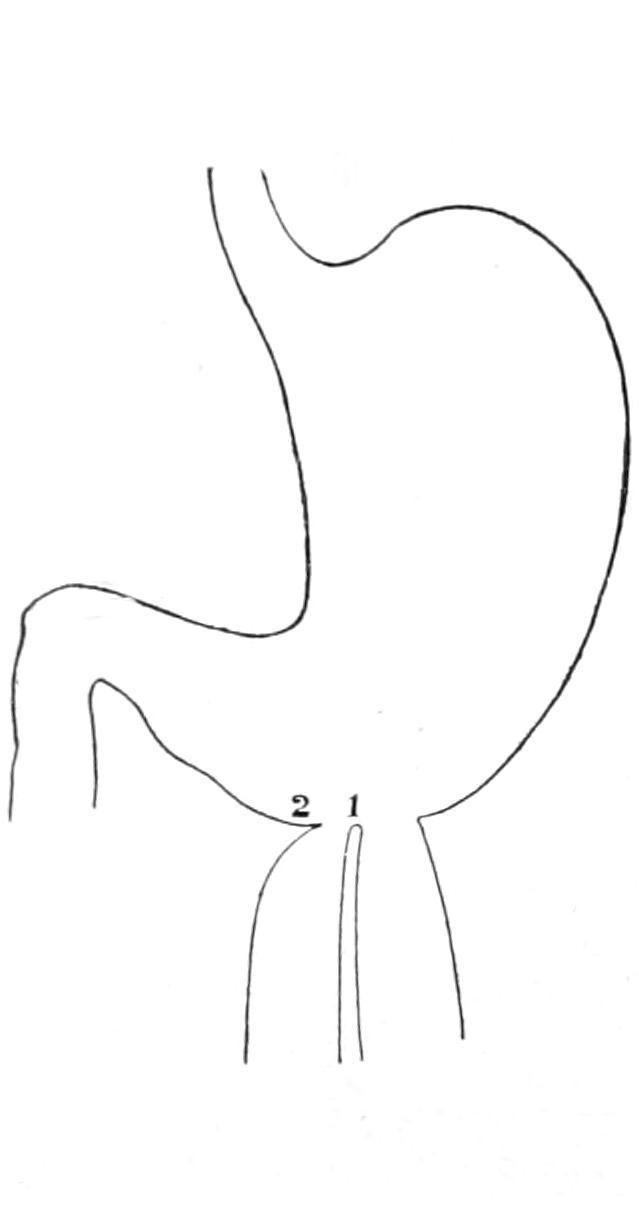
Cardiospasm.
—Operation for this condition consists essentially in a gastrotomy as above, the opening being made sufficiently near to the cardia in order that either with finger or with suitable dilating instrument passed upward from below, the contracted cardiac orifice may be stretched, or, if necessary, nicked at several points, and then forcibly dilated, in this latter procedure great care should be given that stress be distributed as much as possible. If it be practicable to introduce any dilating instrument a four-bladed uterine dilator would probably be ideal for the purpose.
Operations for Pyloric Stenosis.
Among the earliest suggestions of a method of pylorodiosis was that of Loreta, who opened the stomach near the pyloric end and deliberately introduced through the constricted pyloric ring a dilating instrument, fashioned much after the shape of the ordinary glove stretcher, which, in fact,
might be used for such a purpose should emergency require. The operation is simple and but slightly dangerous, but it was found that strictures here as elsewhere tend to contract, even after forcible dilatation, and that the method, while temporarily successful, was but seldom permanently so. It was applicable only to the cicatricial, i.e., the non-malignant cases.
A plastic method was then suggested independently by Heinecke and Mikulicz, with which their names are often connected and which is referred to as pyloroplasty. It consists essentially in making a buttonhole incision in one direction and then closing it in the opposite, as illustrated in Figs. 534, 535 and 536.
IG. 534
Linear pyloroplasty. Seat and length of cut. (Richardson.)
Linear pyloroplasty. Appearance of cut sutured transversely. Two more sutures to be applied. (Richardson.)
Pyloroplasty. Shape of cut when more than a linear incision is desirable. (Richardson.)
When cicatricial tissue is not too dense, and the parts not infiltrated, it has given satisfactory results. Even here it has been found to be frequently reduced in size by subsequent contraction, and the method suggested by Finney is more serviceable.
Finney’s pyloroplasty: posterior suture. (Bergmann.)
Finney’s pyloroplasty: anterior sutures drawn aside; incision made. (Bergmann.)
Finney’s pyloroplasty: posterior suture of mucous membrane. (Bergmann.)
Finney’s pyloroplasty: anterior stitches inserted but not tied. (Bergmann.)
Finney’s pyloroplasty consists in making an anastomotic opening between the pyloric end of the stomach and the first part of the duodenum, and will be best appreciated from the accompanying illustrations (Figs. 537, 538, 539, 540 and 541).
FIG. 540
Finney’s pyloroplasty: anterior suture completed. (Bergmann.)
The opening can be made as extensively as desired, and it is not easy to see how it can be subsequently reduced to a degree disadvantageous to the patient.
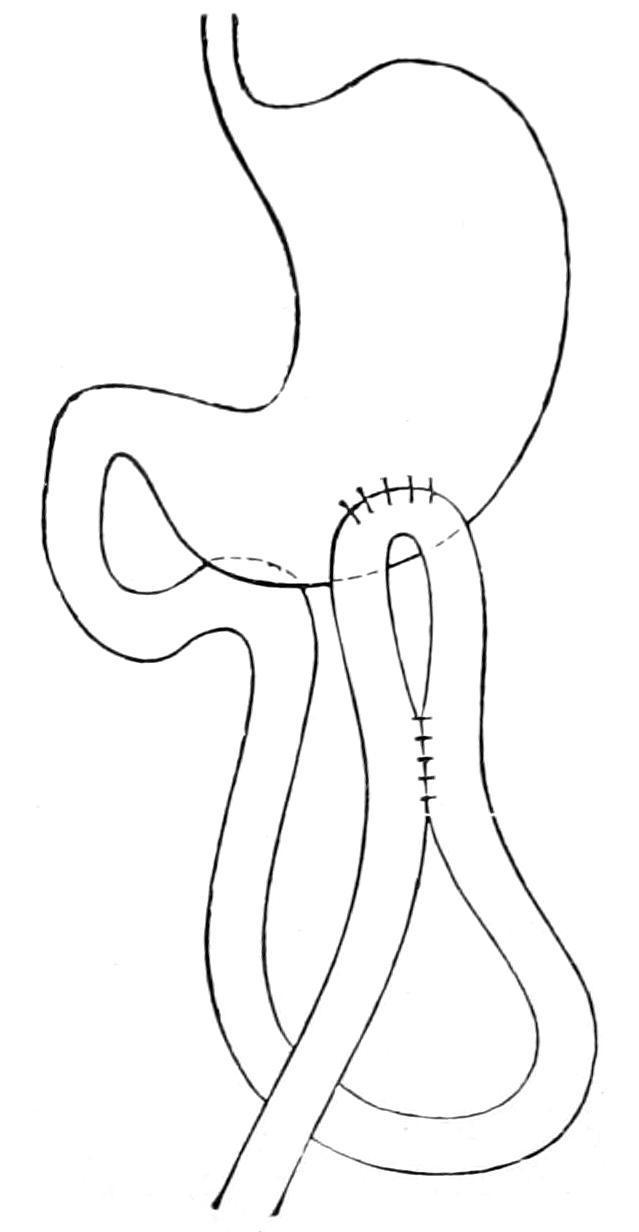
Gastro-enterostomy may be needed in non-malignant cases, because of fixation and the impossibility of bringing the pyloric end of the stomach out sufficiently to make operation feasible. It will be required in cases of cancer when pylorectomy is not indicated. The method of making gastro-enterostomy will be described later.
Operations for Dilatation of the Stomach.
—Gastroplication consists of taking a number of “tucks” in the stomach wall and thus
reducing its capacity. The purpose and the method of the operation will be appreciated by the accompanying illustrations. These operations are mainly indicated, however, in the absence of pyloric stenosis, for if a free opening be afforded from the dilated stomach into the upper bowel the gastric enlargement will usually be spontaneously reduced (Figs. 542 and 547).
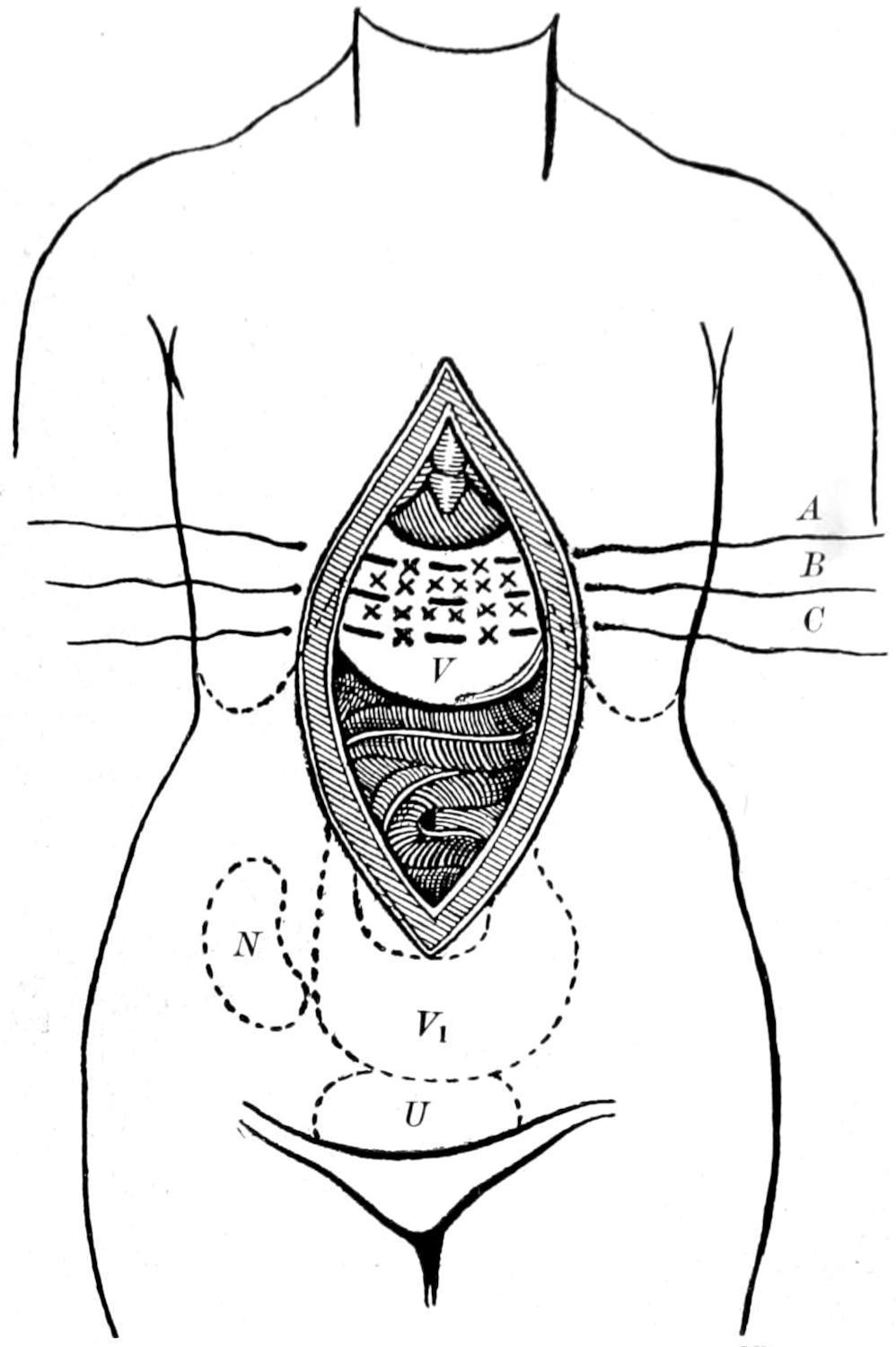
Gastropexy is a term applied to fixation of the stomach to the anterior abdominal wall. It has been thus stitched up in a few cases when greatly dilated or depressed into the lower abdomen. Fig. 548 illustrates the method. The stomach has also been suspended by shortening the gastrohepatic and gastrophrenic ligaments, as illustrated in Fig. 549.
Gastroplication. When the threads a a´, bb´are drawn up a fold is formed. (Bircher.)
Sectional view to show result of operation.
Operations for Gastric Ulcer.
—In dealing surgically with an ulcer of the stomach the selection has to be made between anastomosis and direct exposure of the stomach wall with the performance of a gastrotomy (i.e., opening the stomach) and then discovering the site of the ulcer, either treating it with the actual cautery, the curette, or, preferably, when this general method is adopted, completely excising the involved area and bringing the margins of the wound thus made together with sutures, which over the mucosa only may be of chromic gut. Should it seem advisable to excise the entire thickness of the stomach wall it would be better to suture in two layers, making the external one of thread or silk, while the inner one may be made of reliable chromic catgut. If this operation be attempted the incision into the stomach should be made sufficiently large to permit of thorough exploration. Nothing being found in the anterior wall, the gastrocolic omentum should be opened and the entire stomach palpated between the operator’s hands. Any suspiciously indurated spot on the posterior wall may then be so manipulated as to be brought into view through the anterior opening. Other surgeons besides myself have noted the occurrence of serious hemorrhage, which, upon exposure, must have come from small fissures or cracks in the mucous membrane. In fact the lesion which may furnish a considerable amount of blood may thus be so small and concealed as to be really difficult of exposure. However, exploration should be made as thoroughly as possible. The stomach having been opened and the ulcer found, it should be treated by one of the above methods. If, on the other hand, nothing be found the surgeon still has the measure of gastroenterostomy. Any ulcer, however, which is threatening perforation can usually be recognized by the sense of touch alone, corroboration being afforded by inspection. An ulcer which is recognized and found to be favorably situated may be completely excised. It has been found, however, that this ideal measure of local attack gives but little better results than does the general procedure of gastroenterostomy, while, on the other hand, it is less satisfactory in some respects and seems to be an equally if not more dangerous procedure.

Surface view of the result. Sectional view of the result when two folds are turned in.
Gastroplication. (Brandt.)
Sectional view of the result.
The rationale of making an anastomotic opening between the stomach and the upper end of the bowel is simply this: that thereby the stomach is given a degree of physiological rest to which it has long been a stranger, and that food may pass easily from the stomach into the upper bowel without irritating or aggravating the ulcerated portion, which is usually at the pyloric end. It should be understood, then, that gastro-enterostomy, done for this purpose, is simply a means of carrying out the universally applicable canon of physiological rest for diseased organs or surfaces. The operation of making this anastomosis will be described below.
Pylorectomy and Gastrectomy.
—A complete removal of the pyloric end of the stomach is usually referred to as pylorectomy, while still more extensive extirpation of portions of the stomach proper are spoken of as gastrectomies. In a few instances it has been possible to practically remove the entire stomach, this having first been done by Schlatter. Such an operation would be spoken of
as totalgastrectomy. These operations are done almost exclusively for removal of areas involved in cancerous growth. Obviously the more extensive the growth the greater the amount of stomach which should be removed. For some reason as yet unknown cancer of the stomach rarely transgresses the pyloric ring, and thus the first part of the duodenum usually escapes involvement, even though the stomach be extensively diseased. All these operations, therefore, include simply the removal of a part terminating with the pyloric ring proper. It is seldom necessary to take away any of the duodenum. Removal of the pylorus may be also applicable in certain cases of benign strictures, where the mere plastic operations would seem insufficient, as well as in the cases of ulcers encroaching upon the pyloric ring itself.
For all of these operations the stomach is exposed through a median incision, or, if a tumor presents distinctly upon the right side, the incision may be made even far to the right and near the semilunar line. Through an opening sufficiently liberal the stomach and the movable part of the duodenum are withdrawn and carefully examined. When the pylorus is so fastened by dense adhesions within the abdomen that it cannot be withdrawn it is best to abstain from this particular procedure, as the mechanical difficulties too greatly enhance its dangers. Suitable clamps, whose blades are protected with soft rubber, are essential in order that the duodenum may be clamped beyond the line of its division, and that the stomach as well may be fixed between their blades, for the double purpose of controlling hemorrhage and preventing escape of contents. The omentum along the involved part of the stomach should then be carefully tied off, in a series of loops, before its vessels are cut, and one should take great pains to hunt out enlarged lymph nodes and include them in the area to be removed, or else make a separate incision for those that cannot be thus extirpated. To leave lymph nodes which are perceptibly involved in the cancerous process is to invite the speediest possible return of the disease, even though the operation should be successful. The upper and lower borders of the stomach being thus freed, the surgeon is then at liberty to cut away all the diseased portion, going at least an inch beyond the apparent
limit of the disease. There will result from any such operation two divided ends of the alimentary canal, i. e., one, that of the divided stomach, much larger than the other, which is the upper end of the duodenum.
Rovsing’s operation for gastroptosis: V, stomach; V₁, position of the stomach before operation; U, urinary bladder; N, right kidney; A, B, C, silk sutures; x, x, scarifications. (Bergmann.)
Two procedures are now open to the surgeon: He may entirely close each of these openings with sutures and then make a posterior gastro-enterostomy, making new openings for this purpose, and by the common method described below, or he may reduce the size of the stomach opening and endeavor to fit it to that of the duodenum in such a way as to bring the two openings opposite each other, where they are then approximated as in ordinary end-to-end resection of the intestine. The earlier operation of Billroth and his followers was made according to the latter plan. It has been found usually easier and more successful to adopt the former method, as it is easier thus to prevent leakage and consequent infection; that is, the majority of operators would today probably completely close the stomach and the duodenum, and proceed at once to make a posterior gastrojejunostomy.

Suspension of stomach by three rows of interrupted stitches through the gastrohepatic and gastrophrenic ligaments: 1, 2, 3, single stitches of the three rows. (Beyea.)
Resection of the pylorus. Suture completed. (Richardson.)
Figs. 550, 551 and 552 give a fair idea of the procedure of end-toend reunion. The edges of the mucosa should be united with chromic gut, the stitches being close to each other, to prevent leakage and to control hemorrhage from small vessels. The external sutures of silk or thread should be placed sufficiently deep to afford a strong bond of union, and, at the same time, to escape the mucosa. Some difficulty is met here, for the thin wall of the duodenum should be attached to the thick wall of the stomach, but with care it can be done. When the divided stomach end has been reduced or trimmed off in such a way as to leave only a portion to
be matched with the duodenal opening, there is need for extreme care at the corners and angles of the suture margins, as here tearing of stitches or separation by tension, perhaps during the act of vomiting, are most likely to occur. Fig. 553 indicates the first of the procedures above mentioned.
Resection of the pylorus. This figure illustrates the method of fitting the duodenum to the stomach when the gap in the stomach is too large to fit the duodenum. (Richardson.)
Resection of the pylorus. (The same as Fig. 551). Suture of the stomach to the duodenum completed. (Richardson.)
In performing complete gastrectomy the cardiac end of the stomach is brought down and fitted to the upper end of the divided duodenum, after removal of the stomach, which will usually be possible under favorable circumstances, but which exposes the patient to great risks of tearing apart reunited surfaces by undue tension.
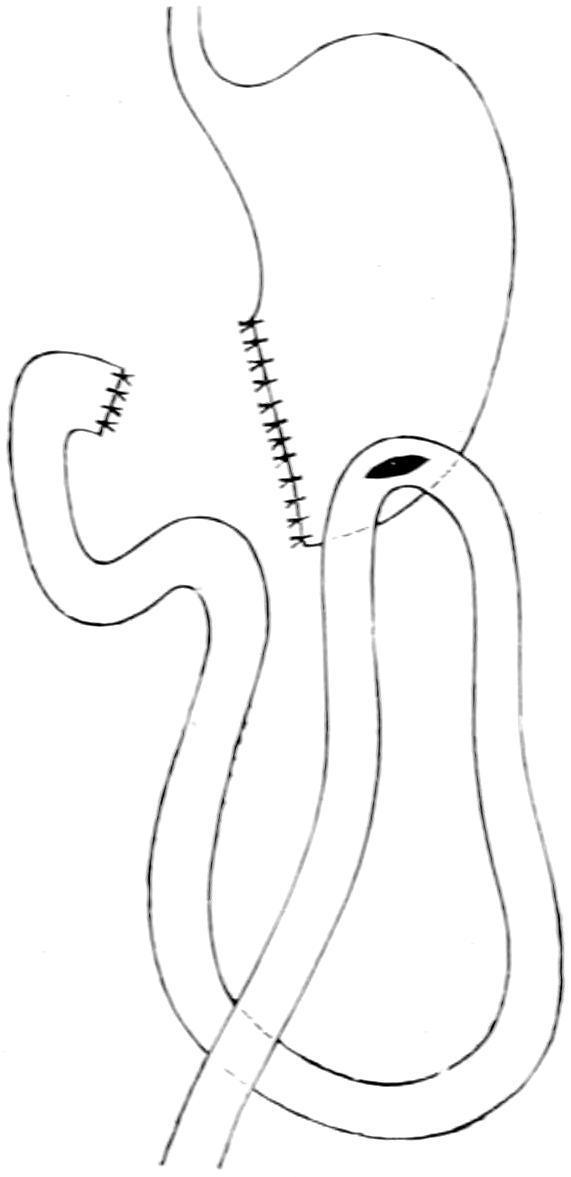
This consists in making an anastomotic opening between the stomach and the uppermost part of the jejunum, the duodenum proper being too bound down in its course to permit of its utilization for this purpose. Gastro-enterostomy, then, should be referred to as
Resection of the pylorus according to Billroth’s second method. (Bergmann.)
Gastric Anastomosis.gastroj
ejunostomy. In brief, it consists in making an opening by which the stomach shall empty directly into the upper bowel, and while, for this purpose, one of the uppermost loops would theoretically suffice, it has been found that the shorter the loop, i. e., the portion between the duodenum proper and the upper part of the bowel used for this purpose, the better for the patient.
Gastrojejunostomy is, first of all, referred to as anterior or posterior, according to whether a loop of bowel be brought up in front of the omentum and around it, and attached to the anterior and exposed wall of the stomach, or whether the lesser peritoneal cavity be opened by perforating the omentum behind the colon and below the stomach, so that the posterior wall of the latter is found, drawn into the wound, and made accessible and utilized for the purpose. The anterior operation is the easier of performance, but the posterior is far preferable in most instances. Should it be found that the posterior wall of the stomach is far more involved in cancerous infiltration than the anterior, the anterior operation should be performed.
Simple as is the procedure in theory there are about it one or two complications which were not at first foreseen. Perhaps the most important of these is that bile emptied into the duodenum passes downward until it has an opportunity to escape through the opening directly into the stomach, usually in the direction of least resistance. This may then carry it where it is a most undesirable fluid, and prevent its passage onward into the intestine, where it is physiologically needed. This circulation of bile has been spoken of as the “vicious circle” and it is the formation of a vicious circle which has complicated not a few of the anastomotic stomach cases, and which has engaged the attention of not a few clinicians and operating surgeons.
The second objection is that the contact of stomach contents with the mucous membrane at a point below where the bowel is normally prepared for it, and before intestinal contents have been prepared by bile or materials alkalinized by this fluid, sometimes leads to the formation of ulcer just opposite the opening, and this has been referred to as pepticulcerofthejejunum. This is a possible though not a frequent complication, but has added weight to the other considerations regarding the best way of performing anastomosis. Again, it has been feared that this anastomotic opening would contract in time, or sometimes completely close. This objection obtains especially with anastomosis, made with a Murphy button, or its equivalent, and can rarely be made against the ordinary suture methods. Again, if the opening in the intestine be made too long the intestine itself may be narrowed, for too much of the circumference of the bowel may be taken up in the formation of the anastomosis, and thus there will be mechanical obstruction with vicious circle.
“Vicious circle” produces symptoms which do not appear until the lapse of at least three days after the operation. If vomiting should persist and retain a bilious character it is to be feared that some complication of this kind has occurred. Under these circumstances when lavage is practised a large amount of fluid mixed with bile, perhaps blood, may be returned.
Much depends also on the exact location of the attachment of the intestinal loop to the stomach. Other difficulties arise from possible
twisting of the loop of small intestine, or its strangulation by being entangled beneath the bridge of the jejunum, which is always made in every anastomosis. Again the small intestine may become incarcerated in an imperfectly closed opening made in the mesocolon. It will thus be seen that the posterior method has disadvantages which need to be fully appreciated. On the other hand it has this great advantage, that it permits of drainage or emptying of the stomach into the jejunum by gravity, in almost any position which the patient would ordinarily assume, either sitting or lying. Many operators have devised methods of preventing formation of the vicious circle.
Fig. 554 illustrates how valves may form which there is no sure method of preventing. Fig. 555 represents the suggestion of Braun, to make a second anastomotic opening between the small intestine above the stomach opening and below it, hoping that in this way bile, for instance, may pass directly through this opening, which it will first meet, into the intestine below, and thus not pass on and into the stomach. Others have divided the loop of jejunum after making the second anastomosis, in this way planting the efferent portion of the bowel in the stomach and then planting the afferent portion of the bowel into the side of the efferent part. This is the socalled Y-gastrojejunostomy. Roux does much the same thing, save that his method is all carried out behind the colon instead of in front of it. The principal argument in favor of the use of the Murphy button, in this procedure, is that vicious circle is less frequent after its use than after most of the suture methods, all of which would simply indicate that vicious circle is largely a matter of valve formation, and that by the time the button is loosened and passed on the danger period seems to have elapsed, and the current in the new direction to be well established. Nevertheless the button is now discarded by almost everyone in favor of the suture.
IG. 554
Formation of valves in gastroenterostomy: 1, intestinal valve; 2, rightsided gastro-intestinal valve.
(Bergmann.)
Gastro-enterostomy with enteroanastomosis according to Braun. (Bergmann.)
Gastro-enterostomy. Artificial anastomotic opening between the cavity of the stomach and some part of the intestine below is indicated in a number of conditions, which have been discussed. It is
FIG. 555
done mainly, however, for two good reasons: first, to atone for pyloric stenosis, and, secondly, to give the stomach a more physiological rest in cases of gastric ulcer, permitting food to pass readily from it into the jejunum, with a minimum of gastric activity or disturbance. This particular form of anastomosis is but the application to these viscera of a general principle, which in various ways, in different parts of the body, has constituted one of the greatest features in the advance of modern surgery.
The operation is practised in two ways. In the anterior operation the highest accessible loop of small intestine is brought up in front of the omentum, or else the omentum is fenestrated in such a way that the bowel shall be brought through its window, and then attached to the anterior wall of the stomach, where the latter is much more accessible. In this operation there is less handling of the stomach and bowel, and, in general, it is easier of performance. Nevertheless the bowel loop itself may become adherent to the abdominal wound and give rise to pain, or even obstruction simulating the vicious circle. Volvulus of the jejunum has also followed it. Another objection is that as the patient gains flesh the weight of the transverse colon and omentum sometimes causes dragging upon the loop, which may cause serious trouble. The opening thus made is not where gravity will afford the best drainage of the stomach, and it is now considered undesirable in almost all cases save those where one is compelled to its performance, either by necessity for haste, or because the posterior wall of the stomach is so involved in cancerous infiltration as to afford no suitable area for fixation and opening. This method is of use mainly in dealing with malignant disease.
The posterior operation calls for all the resources of a perfected technique, and takes longer in performance. Nevertheless when once the anastomosis is safely effected it is more satisfactory.
The posterior operation alone, therefore, will be described at length in this place, and only that form of it which discards the anastomotic loop, the writer quite agreeing with the Mayos, who have had larger experience with this operation than any other surgeons, and who advise the direct attachment of the jejunum, as
near as possible to the termination of the duodenum, without further complication by operative procedure. The direction of active propulsion from the stomach comes from its pyloric end, the larger end of the stomach being mainly for storage purposes and having thus a forceful action; consequently the preferable site for the stomach opening is on a line with the longitudinal part of the lesser curvature, with its lower end at the bottom of the stomach. The Mayos have abandoned reversing the jejunum and now apply it directly to the posterior wall of the stomach from right to left exactly as it lies under normal conditions, having had better results with this method than with any other.
In brief the operation is as follows: Incision is made a little to the right of the median line, the transverse colon is withdrawn by steady traction to the right and upward, and the mesocolon made to follow it until the jejunum comes into view. The latter is then grasped at a distance of three or four inches from its origin. When, now, it is drawn tight the fold of peritoneum which covers the so-called ligament of Treitz is demonstrated; this is a small band containing muscle fibers, having its origin on the transverse mesocolon and extending down to the beginning of the jejunum, thus acting as a suspensory ligament. It leads to the base of the vascular arch of the middle colic artery, and indicates the place where the mesocolon should be torn through in order to expose the posterior wall of the stomach. At this point, in the least vascular area which can be discovered, the mesocolon is first incised and then torn, until a good liberal opening is made, through which the posterior wall of the stomach is easily exposed, and, later, drained. It should be forced through this opening by combined manipulation with one hand introduced above it and gently urging it through the opening where it presents. It may be easily identified by its resemblance to its anterior surface in its thickness, the arrangement of its vessel and the like. The posterior wall alone is then secured and drawn through the mesocolic window, in such a way that after the jejunum is attached to it the anastomotic opening can be made at a point one inch above the greater curvature and ending at the bottom of the stomach two and a half inches to the left of the pylorus. This area
having been exposed and prepared, a considerable portion of it is drawn into a pair of specially constructed clamps (Doyen’s or Moynihan’s), whose blades are usually protected with rubber. The Mayos prefer to have the handles lying to the right and to direct the forceps transversely to the body axis. Moynihan prefers to reverse this direction and make them point to the right shoulder. The stomach being thus protected, and prevented from slipping by suitable tightening of the clamps, the jejunum is similarly secured with forceps lying in a direction parallel to the first, having within their grasp a portion of the gut extending between points one and a half and three and a half inches from its origin. If this be properly effected the left low point of the stomach lies in the grasp of one pair of clamps and the first part of the jejunum in that of the other, and these two portions should be easily brought into close contact with each other. A gauze pad having been placed behind the damps in order to avoid soiling, should there be any leakage of intestinal contents, the clamps should now be carefully and attentively held by an assistant, and their distal ends may even be bound together in such a way that, after the suturing process has once begun, nothing shall disturb the perfect contact between the surfaces thus mutually applied. The first row of sutures, usually of the ordinary continuous type, is made of silk or thread, the serous and muscular coats being seized and united over a line some two inches in length, the suture being carefully secured at either end of this line. Next, with a scalpel, an incision is made through the serous and muscular coats, parallel to the line of sutures, at a distance of about one-quarter of an inch, and over a length a trifle less than that of the line which they occupy. Here the vessels will bleed freely and forceps may be momentarily used for their securement. Through the opening thus made the mucous membrane will prolapse. Moynihan especially has shown that it is not enough to merely incise this membrane in the same direction as the other coats, but that a narrow elliptical portion of it should be excised, since it tends to prolapse. Therefore with knife or scissors a strip of the mucosa, perhaps a half-inch in width, should be cut away from either surface, thus widely opening into and exposing the interior respectively of the stomach and of the gut.