Oxford University Press is a department of the University of Oxford. It furthers the University’s objective of excellence in research, scholarship, and education by publishing worldwide. Oxford is a registered trade mark of Oxford University Press in the UK and certain other countries.
Published in the United States of America by Oxford University Press 198 Madison Avenue, New York, NY 10016, United States of America.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by license, or under terms agreed with the appropriate reproduction rights organization. Inquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above.
You must not circulate this work in any other form and you must impose this same condition on any acquirer.
CIP data is on file at the Library of Congress ISBN 978–0–19–088772–8
This material is not intended to be, and should not be considered, a substitute for medical or other professional advice. Treatment for the conditions described in this material is highly dependent on the individual circumstances. And, while this material is designed to offer accurate information with respect to the subject matter covered and to be current as of the time it was written, research and knowledge about medical and health issues is constantly evolving and dose schedules for medications are being revised continually, with new side effects recognized and accounted for regularly. Readers must therefore always check the product infor mation and clinical procedures with the most up- to- date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulation. The publisher and the authors make no representations or warranties to readers, express or implied, as to the accuracy or completeness of this material. Without limiting the foregoing, the publisher and the authors make no representations or warranties as to the accuracy or efficacy of the drug dosages mentioned in the material. The authors and the publisher do not accept, and expressly disclaim, any responsibility for any liability, loss, or risk that may be claimed or incurred as a consequence of the use and/or application of any of the contents of this material.
9 8 7 6 5 4 3 2 1
Printed by Sheridan Books, Inc., United States of America
Contents
Series Editor’s Preface ix
Nathan R. Selden
List of Contributors xi
1. Nonaneurysmal Subarachnoid Hemorrhage 1
Peter Nakaji and Michael R. Levitt
2. Blister Aneurysm of the Internal Carotid Artery 5
Peter Nakaji and Michael R. Levitt
3. Posterior Communicating Artery Aneurysm Presenting with and without Third Nerve Palsy 15
Michaela H. Lee, Brandon D. Liebelt, Peter Nakaji, and Robert F. Spetzler
Index 307
Series Editor’s Preface
Dear Reader,
I am delighted to introduce this volume of Neurosurgery by Example: Key Cases and Fundamental Principles. Neurosurgical training and practice are based on managing a wide range of complex clinical cases with expert knowledge, sound judgment, and skilled technical execution. Our goal in this series is to present exemplary cases in the manner they are actually encountered in the neurosurgical clinic, hospital emergency department, and operating room.
For this volume, Drs. Peter Nakaji and Michael R. Levitt invited a broad range of expert contributors to share their extensive wisdom and experience in all major areas of vascular neurosurgery. Each chapter contains a classic presentation of an important clinical entity, guiding readers through the assessment and planning, decision-making, surgical procedure, aftercare, and complication management. “Pivot points” illuminate the changes required to manage patients in alternate or atypical situations.
Each chapter also presents lists of pearls for the accurate diagnosis, successful treatment, and effective complication management of each clinical problem. These three focus areas will be especially helpful to neurosurgeons preparing to sit for the American Board of Neurological Surgery oral examination, which bases scoring on these three topics.
Finally, each chapter contains focused reviews of medical evidence and expected outcomes, helpful for counseling patients and setting accurate expectations. Rather than exhaustive reference lists, chapter authors provide focused lists of high-priority additional reading recommended to deepen understanding.
The resulting volume should provide you with a dynamic tour through the practice of vascular neurosurgery, guided by some of the leading experts in North America. Additional volumes cover each subspecialty area of neurosurgery using the same casebased approach and board review features.
Nathan R. Selden, MD, PhD Campagna Professor and Chair Department of Neurological Surgery Oregon Health and Science University Portland, Oregon
Contributors
Adib A. Abla, MD
Associate Professor
Department of Neurological Surgery
University of California, San Francisco San Francisco, CA
Pankaj Agarwalla, MD
Skull Base and Cerebrovascular Fellow
Department of Neurosurgery and Brain Repair
University of South Florida Tampa, FL
Siviero Agazzi, MD, MBA
Professor
Department of Neurosurgery and Brain Repair
University of South Florida Tampa, FL
Felipe C. Albuquerque, MD
Professor
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
Rami O. Almefty, MD
Assistant Professor
Department of Neurosurgery
Lewis Katz School of Medicine at Temple University Philadelphia, PA
Dorothea Altschul, MD
Interventional Neurologist Neurosurgeons of New Jersey Ridgewood, NJ
Sepideh Amin-Hanjani, MD
Professor
Department of Neurosurgery
University of Illinois at Chicago Chicago, IL
Adam Arthur, MD, MPH
Professor
Department of Neurosurgery
University of Tennessee Health Sciences Center and Semmes–Murphey Clinic Memphis, TN
Nicholas C. Bambakidis, MD
Vice President and Director, The Neurological Institute
University Hospitals of Cleveland Professor of Neurological Surgery
Case Western Reserve University School of Medicine
Cleveland, OH
Jacob F. Baranoski, MD
Resident Physician
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
Evgenii Belykh, MD
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
Department of Neurosurgery
Irkutsk State Medical University
Irkutsk, Russia
Phillip A. Bonney, MD
Resident Physician
Department of Neurological Surgery
Keck School of Medicine
University of Southern California Los Angeles, CA
Denise Brunozzi, MD Fellow
Department of Neurosurgery
University of Illinois at Chicago Chicago, IL
Jan-Karl Burkhardt, MD
Assistant Professor
Department of Neurosurgery
Baylor College of Medicine Houston, TX
Brandon Burnsed, MD
Neurosurgeon
Raleigh Neurosurgical Clinic
Raleigh, NC
Claudio Cavallo, MD
Neurosurgery Research Fellow
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
Fady T. Charbel, MD
Professor and Chair
Department of Neurosurgery
University of Illinois at Chicago
Chicago, IL
Vincent Cheung, MD
Resident Physician
Department of Neurosurgery
University of California, San Diego La Jolla, CA
Tyler S. Cole, MD
Resident Physician
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
E. Sander Connolly, Jr., MD
Professor and Vice Chairman
Department of Neurosurgery
Columbia University
New York, NY
Brian M. Corliss, MD
Resident Physician
Lillian S. Wells Department of Neurological Surgery
University of Florida Gainesville, FL
William T. Couldwell, MD, PhD
Professor and Chair
Department of Neurosurgery
University of Utah Salt Lake City, UT
Dale Ding, MD
Assistant Professor
Department of Neurosurgery
University of Louisville School of Medicine Louisville, KY
David Dornbos III, MD
Resident Physician
Department of Neurological Surgery
The Ohio State University Wexner Medical Center
Columbus, OH
Andrew F. Ducruet, MD
Assistant Professor
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
Ilyas Eli, MD
Resident Physician
Department of Neurosurgery
Clinical Neurosciences Center
University of Utah Salt Lake City, UT
Basavaraj Ghodke, MBBS
Professor
Departments of Radiology and Neurological Surgery
University of Washington Seattle, WA
Steven L. Giannotta, MD
Professor and Martin H. Weiss Chair Department of Neurological Surgery
Keck School of Medicine
University of Southern California Los Angeles, CA
Raghav Gupta, BS Medical Student
Rutgers New Jersey Medical School
Rutgers, State University of New Jersey Newark, NJ
Brian L. Hoh, MD
Professor and Chair
Lillian S. Wells Department of Neurological Surgery
University of Florida Gainesville, FL
Adeel Ilyas, MD
Resident Physician
Department of Neurosurgery
University of Alabama at Birmingham Birmingham, AL
Alexander A. Khalessi, MD, MS
Professor and Chair
Department of Neurosurgery
University of California, San Diego La Jolla, CA
Louis Kim, MD
Professor and Vice Chair
Department of Neurological Surgery
Professor
Department of Radiology
Stroke and Applied Neuroscience Center
University of Washington Seattle, WA
Robert Kim, MD
Resident Physician
Department of Neurosurgery
University of Utah Salt Lake City, UT
Andrew L. Ko, MD
Assistant Professor
Department of Neurological Surgery University of Washington Seattle, WA
Sean D. Lavine, MD
Professor Departments of Neurological Surgery and Radiology
Columbia University New York, NY
Michael T. Lawton, MD
Professor and Chair
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
Michaela H. Lee, MD Neurosurgeon
Anacapa Surgical Associates Ventura, CA
Michael R. Levitt, MD
Assistant Professor
Departments of Neurological Surgery, Radiology, and Mechanical Engineering; and Stroke and Applied Neuroscience Center
University of Washington Seattle, WA
Elad I. Levy, MD, MBA
L. Nelson Hopkins III MD Chair of Neurosurgery
Professor of Neurosurgery and Radiology
Jacobs School of Medicine and Biomedical Sciences
Gates Vascular Institute at Kaleida Health
Canon Stroke and Vascular Research Center
University at Buffalo Buffalo, NY
Brandon D. Liebelt, MD
Assistant Professor
Department of Neurosurgery
Larner College of Medicine
University of Vermont Burlington,VT
Harry Van Loveren, MD
Associate Dean
College of Medicine
Professor and Chair
Department of Neurosurgery and Brain Repair
University of South Florida Tampa, FL
Alex Lu, MD
Resident Physician
Department of Neurological Surgery
University of California, San Francisco San Francisco, CA
William J. Mack, MD
Professor
Vice Chair, Academic Affairs
Department of Neurological Surgery
Keck School of Medicine
University of Southern California Los Angeles, CA
Grace K. Mandigo, MD
Assistant Professor
Department of Neurological Surgery
Columbia University New York, NY
Philip M. Meyers, MD
Professor
Departments of Neurological Surgery and Radiology
Columbia University New York, NY
J. Mocco, MD, MS
Professor and Vice Chair
Department of Neurosurgery
Icahn School of Medicine at Mount Sinai Hospital
New York, NY
Jacques J. Morcos, MD
Professor
Departments of Neurosurgery and Otolaryngology
Miller School of Medicine
University of Miami Miami, FL
John F. Morrison, MD
Resident Physician
Department of Neurosurgery
Brown University Providence, RI
Stephan A. Munich, MD
Endovascular Neurosurgery Fellow
Jacobs School of Medicine and Biomedical Sciences
Gates Vascular Institute at Kaleida Health
University at Buffalo Buffalo, NY
Peter Nakaji, MD
Professor
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
Anil Nanda, MD, MPH
Professor and Chairman
Peter. W.Carmel M.D. Endowed Chair of Neurological Surgery
Rutgers-New Jersey Medical School, Newark
Rutgers-Robert Wood Johnson Medical School, New Brunswick
Senior Vice President of Neurosurgical Services, RWJBarnabas Health
New Brunswick, NJ
Vinayak Narayan, MD, MCh, DNB Fellow
Department of Neurosurgery
Rutgers-Robert Wood Johnson Medical School
New Brunswick, NJ
Sabareesh K. Natarajan, MD, MS
Assistant Professor
Department of Neurological Surgery
University of Massachusetts Medical School Worcester, MA
Jeffrey T. Nelson, MD
Resident Physician
Department of Neurological Surgery
Case Western Reserve University School of Medicine Cleveland, OH
Christopher S. Ogilvy, MD
Professor
Department of Neurosurgery
Beth Israel Deaconess Medical Center
Harvard Medical School Boston, MA
J. Scott Pannell, MD
Assistant Professor
Departments of Radiology and Neurosurgery
University of California, San Diego La Jolla, CA
Colin J. Przybylowski, MD
Resident Physician
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
Kristine Ravina, MD
Clinical Research Associate
Department of Neurological Surgery
Keck School of Medicine
University of Southern California Los Angeles, CA
Zeguang Ren, MD, PhD
Assistant Professor
Department of Neurosurgery and Brain Repair
University of South Florida Tampa, FL
Jonathan J. Russin, MD
Assistant Professor
Department of Neurological Surgery
Keck School of Medicine
University of Southern California Los Angeles, CA
W. Caleb Rutledge, MD
Resident Physician
Department of Neurological Surgery
University of California, San Francisco San Francisco, CA
David R. Santiago-Dieppa, MD
Resident Physician
Department of Neurosurgery
University of California, San Diego La Jolla, CA
Ahsan Satar, MD
Interventional Neurologist Neurosurgeons of New Jersey Ridgewood, NJ
Philip G. R. Schmalz, MD
Resident Physician Department of Neurosurgery
University of Alabama at Birmingham Birmingham, AL
Richard H. Schmidt, MD, PhD
Associate Professor Department of Neurosurgery University of Utah Salt Lake City, UT
Laligam N. Sekhar, MBBS
Professor and Vice Chair Department of Neurological Surgery University of Washington Seattle, WA
Rajeev D. Sen, MD
Resident Physician
Department of Neurological Surgery University of Washington Seattle, WA
Hussain Shallwani, MD
Resident Physician Department of Neurosurgery
Gates Vascular Institute at Kaleida Health University at Buffalo Buffalo, NY
Jason P. Sheehan, MD, PhD
Professor
Departments of Neurological Surgery and Neuroscience University of Virginia Charlottesville,VA
Matthew J. Shepard, MD
Resident Physician
Department of Neurological Surgery
University of Virginia Charlottesville,VA
Adnan H. Siddiqui, MD, PhD
Professor
Departments of Neurosurgery and Radiology
Jacobs School of Medicine and Biomedical Sciences
Gates Vascular Institute at Kaleida Health
Canon Stroke and Vascular Research Center
University at Buffalo Buffalo, NY
Parampreet Singh, MD Fellow
Department of Neurological Surgery
Keck School of Medicine
University of Southern California Los Angeles, CA
Robert A. Solomon, MD
Professor and Chair Department of Neurosurgery
Columbia University New York, NY
Robert F. Spetzler, MD
Emeritus Chair
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
Philipp Taussky, MD
Associate Professor
Departments of Neurological Surgery and Radiology and Imaging Sciences
University of Utah
Salt Lake City, UT
Kunal Vakharia, MD
Resident Physician
Department of Neurosurgery
Gates Vascular Institute at Kaleida Health University at Buffalo Buffalo, NY
Arvin R. Wali, MD, MAS
Resident Physician
Department of Neurosurgery
University of California, San Diego La Jolla, CA
Gabrielle A. White-Dzuro, MD
Resident Physician
Department of Anesthesia, Critical Care and Pain Medicine
Massachusetts General Hospital Boston, MA
Robert T. Wicks, MD
Cerebrovascular and Skull Base Fellow
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
John R. Williams, MD
Resident Physician
Department of Neurological Surgery University of Washington Seattle, WA
Ethan A. Winkler, MD, PhD
Resident Physician
Department of Neurological Surgery
University of California, San Francisco San Francisco, CA
Kurt Yaeger, MD
Resident Physician
Department of Neurosurgery
Icahn School of Medicine at Mount Sinai Hospital
New York, NY
Benjamin Yim, MD, MS
Resident Physician
Department of Neurological Surgery
Keck School of Medicine
University of Southern California Los Angeles, CA
Joseph M. Zabramski, MD
Emeritus Professor
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
Xiaochun Zhao, MD
Fellow
Department of Neurosurgery
Barrow Neurological Institute
St. Joseph’s Hospital and Medical Center Phoenix, AZ
Nonaneurysmal Subarachnoid Hemorrhage
Peter Nakaji and Michael R. Levitt
Case Presentation
A 69-year-old male presented to the emergency department with the worst headache of his life that was sudden in onset and accompanied by nausea and vomiting. There was no loss of consciousness. He did not have a history of frequent or severe headaches. On neurological examination, the patient was alert and oriented to person, place, time, and situation, although slightly slower to respond to questions than baseline. He was otherwise fully intact on examination, including normal cranial nerve, motor, sensory, and cerebellar function.
A noncontrast computed tomography (CT) scan of the head was obtained in the emergency room (Figure 1.1), and consultation with the neurosurgeon was obtained.
Assessment and Planning
The neurosurgeon confronted with the classic pattern of subarachnoid hemorrhage must quickly determine the etiology of the bleed. Aneurysmal subarachnoid hemorrhage is most commonly suspected, although the differential diagnosis includes angiographicallynegative subarachnoid hemorrhage either in a classic pattern or in a perimesencephalic prepontine pattern, as well as less common causes such as hemorrhage from an arteriovenous malformation, dural arteriovenous fistula, cavernous malformation, tumor, or a bleeding diathesis or other hypocoagulable condition. The last of these should be ruled out by taking a thorough history, performing a physical examination for other signs of hemorrhage such as petechiae, and ordering a routine coagulation panel and platelet count. Aneurysmal subarachnoid hemorrhage accounts for approximately 80–85% of nontraumatic subarachnoid hemorrhage, with nonaneurysmal angiographicallynegative idiopathic hemorrhage accounting for 15–18% and the balance due to the other causes listed previously.
CT angiography has become standard of care in the acute setting to evaluate for the presence of a cerebral aneurysm. Frequently, an arteriovenous malformation or fistula can be diagnosed this way as well. It is believed that with current CT quality, CT misses a true aneurysmal source of bleeding in no more than 5% and possibly less than 1% of cases. If CT angiography is negative, a catheter angiogram should be performed. Catheter angiography should include injections of both carotid arteries and both vertebral arteries, as well as external carotid artery injections, for a total of 6 visualized vessels. Some angiographers will inject only one vertebral artery if reflux is seen down to the posterior inferior cerebral arteries. In general, a full examination is preferred. Each injection should be followed
Figure 1.1 Noncontrast CT of the head demonstrates diffuse subarachnoid hemorrhage in the basal cisterns, with associated ventriculomegaly.
well into the venous phase to rule out the full range of abnormalities. The most common missed lesions include blister aneurysms of the internal carotid artery, small saccular anterior communicating artery and middle cerebral artery aneurysms, and small distal fusiform aneurysms beyond the usual circle of Willis locations.
Oral Boards Review—Diagnostic Pearls
1. Consider noncontrast CT, CT angiography, catheter angiography, magnetic resonance imaging (MRI) of the brain, and delayed repeat catheter angiography in that order if the diagnostic workup continues to be negative.
2. A high index of suspicion for an aneurysmal cause of subarachnoid hemorrhage should be maintained even if the initial CT angiography and even the catheter angiogram are negative.
3. A meticulous angiogram that includes all vessels, including the external carotid arteries, both vertebral arteries to their origins, and all vessels through the entire venous phase, is mandatory to avoid missing some lesions.
4. Angiographic three-dimensional reconstruction can help identify small lesions that could otherwise be overlooked.
5. A classic aneurysmal bleed pattern can still prove to be angiographicallynegative subarachnoid hemorrhage and can have a benign course.
Surgical Procedure
In very rare cases, exploration of a possible but ill-defined source of bleeding is undertaken. This is usually in the setting of a classic pattern of subarachnoid hemorrhage when a possible bleeding source is identified on CT or catheter angiography. In this circumstance, the lesion of interest should be approached as if it is a true bleeding
source, adhering to the usual vascular principles of proximal control, distal control, and dissection of the neck and dome. If a lesion such as a blister aneurysm is found, the surgeon must be prepared for clip-wrapping or bypass. For this reason, the neck is often prepped for access in case proximal control is needed. The superficial temporal artery is preserved during the opening. The forearm or leg may be prepped to have the radial artery or saphenous vein available, respectively.
Oral Boards Review—Management Pearls
1. In the setting of a perimesencephalic pattern of bleeding, a more conservative management strategy can be considered. The underlying cause of such hemorrhage remains unknown.
2. Angiographically-negative perimesencephalic hemorrhage rarely, if ever, recurs.
3. Transcranial Doppler ultrasonography can be used to screen for vasospasm.
Pivot Points
1. If the pattern of bleeding includes more cortical/convexity subarachnoid hemorrhage, occult trauma or vasculitis should be considered.
2. If a bleeding diathesis is suspected, dural venous thrombosis or another manifestation of a hypercoagulable state should be considered, including factor V Leiden, protein C or S deficiency, lupus anticoagulant, and others.
Aftercare
Most commonly, conservative management is undertaken in this setting. Most patients will be observed in the intensive care unit for other sequelae of subarachnoid hemorrhage, including hydrocephalus and vasospasm. Blood pressure is usually maintained in the 120–160 mmHg systolic range. If needed for vasospasm management, induced hypertension may still be used.
When initial catheter angiography is negative, practice varies. If the pattern of hemorrhage is classically perimesencephalic/prepontine, some surgeons advocate no further workup. In other cases that are more equivocal, a MRI with and without contrast of the brain may be performed to look for cavernous malformation or tumor. An MRI of the cervical spine or even the entire spinal canal may be performed to rule out rare causes, such as spinal ependymoma or a spinal vascular malformation.
In case of a classic pattern of bleeding, repeat angiography can be considered 7–14 days after the initial hemorrhage to look for missed sources of bleeding, as enumerated previously, and to assess for the presence of vasospasm.
Complications and Management
As mentioned previously, hydrocephalus and vasospasm are the most common issues that arise in the care of patients with angiographically-negative subarachnoid hemorrhage.
They are more common in patients with a classic aneurysmal pattern of bleeding than in those with the perimesencephalic prepontine form. Hydrocephalus in this setting can require placement of an external ventricular drain in the frontal horn of the lateral ventricle and even eventual ventriculoperitoneal shunting. Other medical problems that may supervene are the common problems found in intensive care unit patients in general, including pneumonia, urinary tract infection, myocardial infarction, and deep venous thrombosis.
Oral Boards Review—Complications Pearls
1. Patients with angiographically-negative subarachnoid hemorrhage should be managed as patients with aneurysm subarachnoid hemorrhage until it becomes clear that all tests are negative and the patients are showing a benign course.
2. Repeat hemorrhage should prompt immediate repeated diagnostic workup and evaluation of any missing imaging.
3. Hydrocephalus and vasospasm can still develop, requiring ventricular drainage and pharmacological/endovascular therapy, respectively.
Evidence and Outcomes
Although generally benign, angiographically-negative subarachnoid hemorrhage has a low but real chance of a poor outcome. Up to 11% of patients will not regain their premorbid level of function despite no cause of hemorrhage ever being found. However, the average outcome is still much better than that seen with aneurysmal subarachnoid hemorrhage.
Further Reading
Khan AA, Smith JD, Kirkman MA, et al.Angiogram negative subarachnoid haemorrhage: Outcomes and the role of repeat angiography. Clin Neurol Neurosurg. 2013;115(8):1470–1475. doi:10.1016/j.clineuro.2013.02.002.
Konczalla J, Schmitz J, Kashefiolasl S, Senft C, Seifert V, Platz J. Non-aneurysmal subarachnoid hemorrhage in 173 patients: A prospective study of long-term outcome. Eur J Neurol 2015;22(10):1329–1336. doi:10.1111/ene.12762.
Moscovici S, Fraifeld S, Ramirez-de-Noriega F, et al. Clinical relevance of negative initial angiogram in spontaneous subarachnoid hemorrhage. Neurol Res. 2013;35(2):117–122. doi:10.1179/1743132812Y.0000000147.
Rinkel GJ, Wijdicks EF, Hasan D, et al. Outcome in patients with subarachnoid haemorrhage and negative angiography according to pattern of haemorrhage on computed tomography. Lancet 1991;338(8773):964–968.
Blister Aneurysm of the Internal Carotid Artery
Peter Nakaji and Michael R. Levitt
Case Presentation
A 38-year-old male presented to the emergency department with sudden onset of the worst headache of his life. Initially, he had nausea and vomiting, and he collapsed but then regained consciousness. He stayed at home overnight before coming to the emergency department when his headache did not improve. He had previously been in good health and had no history of severe headaches. He was a nonsmoker, with no history of hypertension. On neurological examination, the patient was alert and oriented ×4 to person, place, time, and situation. He had normal cranial nerve, motor, sensory, and cerebellar function.
A noncontrast computed tomography (CT) scan of the head was obtained in the emergency department (Figure 2.1). A subsequent CT angiography (CTA) scan was interpreted as negative for vascular abnormality, and a consultation with a neurosurgeon was obtained.
Questions
1. What further workup should be pursued for a CTA-negative hemorrhage?
2. What medications should be investigated and what blood tests considered?
3. What constitutes a complete angiogram in a case such as this one? What lesions are most often missed on CTA or angiography?
Assessment and Planning
CTA can be falsely negative in 2–5% of patients.The neurosurgeon should inquire about the use of anticoagulant or antiplatelet medications, such as warfarin, heparin, aspirin, clopidogrel, and especially newer agents including apixaban (Eliquis) and dagibatran (Pradaxa). Testing should include blood coagulation studies (e.g., prothrombin time, partial thromboplastin time, international normalized ratio, platelet count, and aspirin response and P2Y12 inhibitor assays) and toxicology for stimulant drugs such as methamphetamine and cocaine. When patients present with the classic pattern of subarachnoid hemorrhage (SAH), the neurosurgeon should obtain a six-vessel catheter angiogram. A six-vessel study includes bilateral internal carotid arteries, bilateral external carotid arteries, and bilateral vertebral arteries. Alternatively, when only one vertebral artery is imaged, an angiogram is considered complete if contrast refluxes at least into the contralateral posterior inferior cerebellar artery. Both external carotid arteries should
Figure 2.1 Noncontrast head CT demonstrates the pattern of subarachnoid hemorrhage classic for aneurysmal rupture, as well as enlarged temporal horns suggesting hydrocephalus.
Source: Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
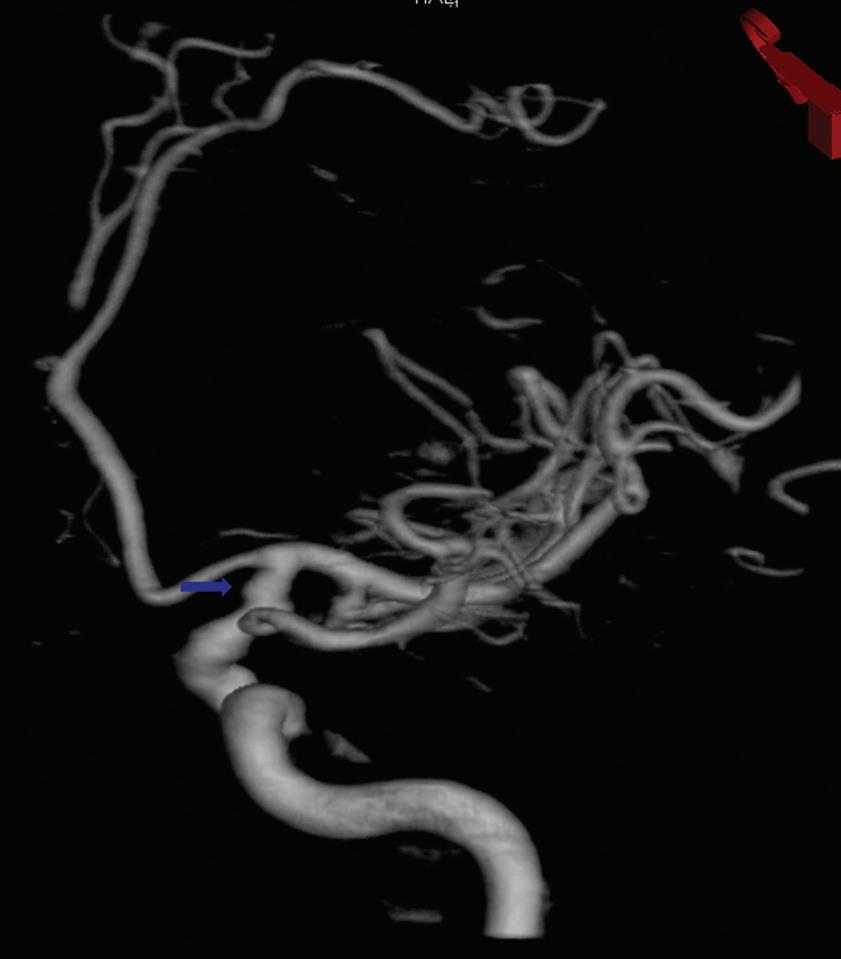
Figure 2.2 Three-dimensional rotational angiogram of the right internal carotid artery demonstrates a small, sessile, raised area (arrow) on the dorsal surface of the distal supraclinoid carotid artery.
Source: Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
be studied to rule out a dural arteriovenous fistula. In this patient, the angiogram revealed an abnormality in the supraclinoid segment of the right internal carotid artery (Figure 2.2).
Questions
1. What is significant about the location of this vascular abnormality?
2. What is important about the anatomy in this particular patient? What additional anatomical information may be particularly noteworthy in planning the treatment of this disease?
3. What are the management options for this patient?
Oral Boards Review—Diagnostic Pearls
1. Blister aneurysms are inflammatory lesions without a true neck.
2. The diagnosis of a blister aneurysm should be considered in patients with SAH when no saccular aneurysm is readily apparent.
3. Three-dimensional rotational angiography helps locate and define aneurysmal anatomy.
Decision-Making
The neurosurgeon should suspect a blister aneurysm when the aneurysm is not associated with a normal arterial branching point (e.g., the dorsally located aneurysm in the supraclinoid internal carotid artery of the previously discussed patient). This kind of aneurysm is an inflammatory lesion that creates a fusiform, or patch- like, weakening in the layers of the arterial wall. Because of their small size and atypical location, blister aneurysms can easily be missed on diagnostic studies, and patients can be mistakenly diagnosed as having angiographically negative hemorrhages. However, patients with blister aneurysms usually have a classically extensive subarachnoid bleeding pattern (see Figure 2.1) rather than a perimesencephalic, prepontine- type SAH. They may present with any Hunt and Hess grade, and they may manifest a relatively benign clinical appearance. Catheter angiography, including three- dimensional rotational angiography, is often required to help make the diagnosis.
Blister aneurysms are particularly unstable and are prone to rebleeding, both spontaneously and during either surgical or endovascular treatment. In contrast, carotid aneurysms located more proximally (i.e., close to the ophthalmic artery) are usually saccular ophthalmic artery aneurysms. Carotid aneurysms that are located proximally and medially may be superior hypophyseal or carotid cave aneurysms. Aneurysms that are ventral are generally posterior communicating artery (PCOM) or anterior choroidal artery aneurysms. Those located at the carotid terminus, rather than dorsally, are also more likely to be saccular aneurysms. Saccular aneurysms are more amenable to traditional microsurgical clipping or endovascular coiling than are blister aneurysms, which are often small, broad-based, and fragile.
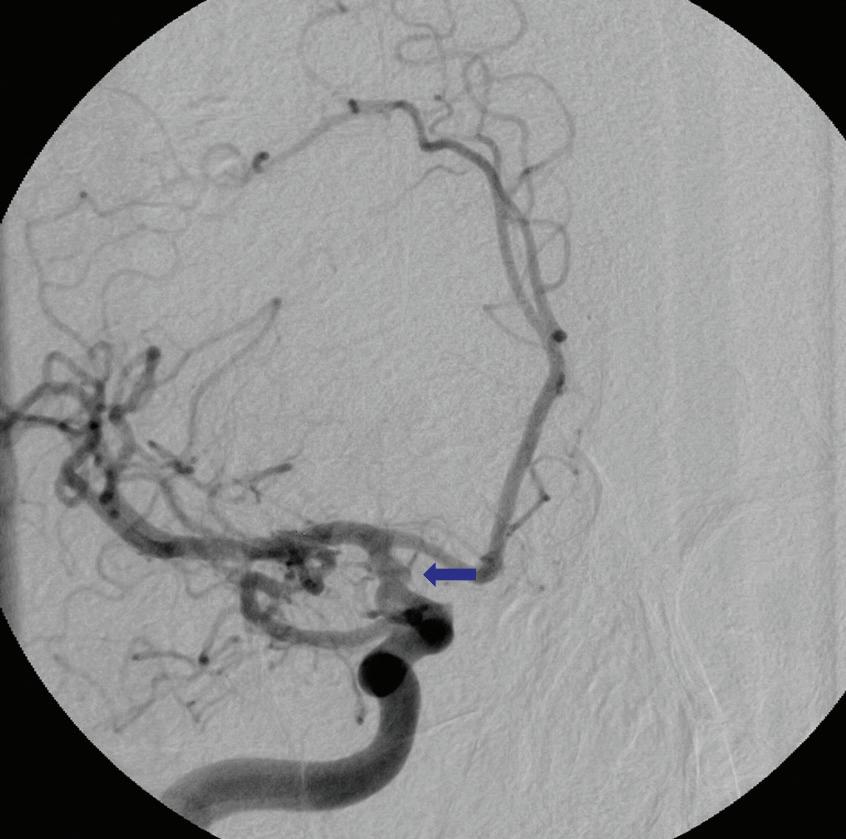
Assessment of the collateral circulation and options for vessel sacrifice are key considerations for internal carotid artery blister aneurysms. The anatomy of the aneurysm in this patient was complicated by the absence of an anterior communicating artery (ACOM) and the presence of a fetal-type PCOM directly opposite the aneurysm (Figure 2.3), which meant that in this patient the posterior cerebral artery distribution and the entire ipsilateral hemisphere were perfused only by the right carotid artery from which the blister aneurysm arose.
Options for intervention include surgical or endovascular treatment. Surgical clipping, clip-wrapping, or bypass and parent vessel sacrifice should all be considered. However, parent vessel sacrifice might be complicated in this patient because the blister aneurysm is located near the origin of key vessels (PCOM and anterior choroidal artery), which cannot be sacrificed without substantial risk of stroke and neurological deficit. These two arteries typically perfuse complementary vascular distributions. The sacrifice of either one is undesirable, and it is likely that the sacrifice of both would result in clinically significant neurological deficit.
The endovascular treatment of blister aneurysms (e.g., treatment with flow-diverting stents) is the focus of a growing number of published reports. In theory, endovascular treatment is appealing because it does not require much manipulation of the aneurysm. However, in patients with SAH, many surgeons are hesitant to start the dual antiplatelet therapy (most commonly aspirin and clopidogrel) required for stent placement because of the possibility of ventriculostomy-related complications. In addition, flow-diverting stent treatment of blister aneurysms does not always immediately occlude the aneurysm, which places the patient at risk of rebleeding during the immediate postoperative period. However, some endovascular therapists have documented success using this treatment strategy. In addition, hybrid strategies involving surgical clip-wrapping followed by
Figure 2.3 Anterior–posterior angiogram of the right internal carotid artery demonstrates blister aneurysm (arrow) close to the origin of the anterior choroidal artery and the origin of the fetal posterior communicating artery.
Source: Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
delayed stenting have been reported.The optimal treatment for these aneurysms remains undefined. Any institution treating blister aneurysms should be proficient with all the necessary techniques, including direct clipping, bypass, and endovascular therapy.
Patients and their families should be informed about the risks associated with treatment. Such risks include the high likelihood of intraoperative rupture and/or the need for bypass. In this case, an open surgical approach was undertaken.
Questions
1. What special surgical considerations and preparations should go into planning for surgery in this case?
2. How should you plan for and manage intraoperative rupture?
Surgical Procedure
This patient underwent a right pterional craniotomy, with preservation of the superficial temporal artery. The right cervical internal carotid artery was also exposed in case proximal control was required. Parent vessel sacrifice would not be achieved by occluding the common carotid artery because there is collateral flow via branches of the external carotid artery. Closing the internal carotid artery in the neck alone would also not fully stop flow through the supraclinoid internal carotid artery because of collateral circulation from the ophthalmic artery, ethmoidal arteries, and small branches in the skull base that would still provide enough arterial flow to maintain vessel patency.
Sacrifice of the internal carotid artery and placement of a high-flow bypass can be considered in most patients with blister aneurysms. However, as mentioned previously, occlusion of the internal carotid artery sufficient to close the aneurysm in this patient would likely also occlude the fetal PCOM, resulting in a stroke and subsequent neurological deficit.
Therefore, clip-wrapping was performed with an expanded polytetrafluoroethylene sling (Gore-Tex), and the carotid artery was partially clipped. Intraoperative rupture occurred but was quickly controlled with temporary clips, and the blistered area was clipped with cotton reinforcement. Additional flow was provided by quickly performing a superficial temporal artery-to-middle cerebral artery bypass. The aneurysm was incorporated into the clip construct with only mild narrowing of the carotid artery (Figure 2.4).
When blister aneurysms are being explored, adequate exposure is essential to ensure that proximal control is available. For aneurysms located near the skull base, proximal control may require exposure of the cervical internal carotid artery. Proximal control should be obtained as quickly as possible in the intradural supraclinoid segment. Distal control should then be obtained. The superficial temporal artery should be preserved as a possible donor vessel for bypass, and the radial artery in the forearm and the saphenous vein in the leg should be considered when a high- flow bypass is anticipated.
Because of the propensity for intraoperative rupture, and the possibility of parent vessel sacrifice, proximal control should be obtained early in the operation, and the surgical team should prepare for a possible bypass before the final dissection of the blister
Figure 2.4 Intraoperative right common carotid artery angiogram shows good distal filling past a mild narrowing of the carotid artery associated with the aneurysm clip.
Source: Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
aneurysm. The aneurysm should be wrapped when primary clipping or complete sacrifice of the parent vessel is deemed inadvisable.Wrapping can be accomplished by placing a sling of Gore-Tex or Hemashield carotid patch circumferentially around the entire diseased segment of the vessel and then cinching it down with a clip to hold it in place over the aneurysm.
Oral Boards Review—Management Pearls
1. Surgery for internal carotid blister aneurysms involves the following steps:
a. Prepare the ipsilateral neck for proximal control.
b. Prepare a saphenous vein or a radial artery to serve as a bypass donor vessel (if needed).
c. Have blood available for transfusion.
d. Be prepared to use adenosine for temporary cardiac arrest, including placing cardioversion pads on the chest.
e. Have available encircling (Sundt-type) clips and/or wrapping material (e.g., Gore-Tex).
f. Achieve proximal and distal control early and before dissecting the blister aneurysm.
g. Follow surgery with postoperative angiography to document the stability of the aneurysm because these lesions are known to progress after clipping more often than saccular aneurysms.
Pivot Points
1. If the patient does not have a fetal PCOM, there is a greater chance that the carotid artery can be sacrificed safely at the blister point. In this case, bypass would be more strongly considered.
2. If the ACOM was larger, the possibility of carotid sacrifice could also be considered. However, neither collateral circulation nor a bypass is likely to completely replace the blood flow formerly provided by the carotid artery. Thus, the patient is at greater risk of ischemia from subsequent vasospasm if blood flow is already compromised.
3. A patient who is an otherwise poor surgical candidate could be more strongly considered for endovascular treatment.
Aftercare
Careful management of blister aneurysm patients is necessary to achieve a good outcome. Blister aneurysms are known to re-rupture after clipping more often than saccular aneurysms. Induced hypertension, which is used to treat clinical or radiographic vasospasm, may be used with more caution in patients with blister aneurysms than in patients with saccular aneurysms that have been clipped. Patients with blister aneurysms, like patients with saccular aneurysms, have a risk of vasospasm that remains proportionate to the amount of SAH at presentation.
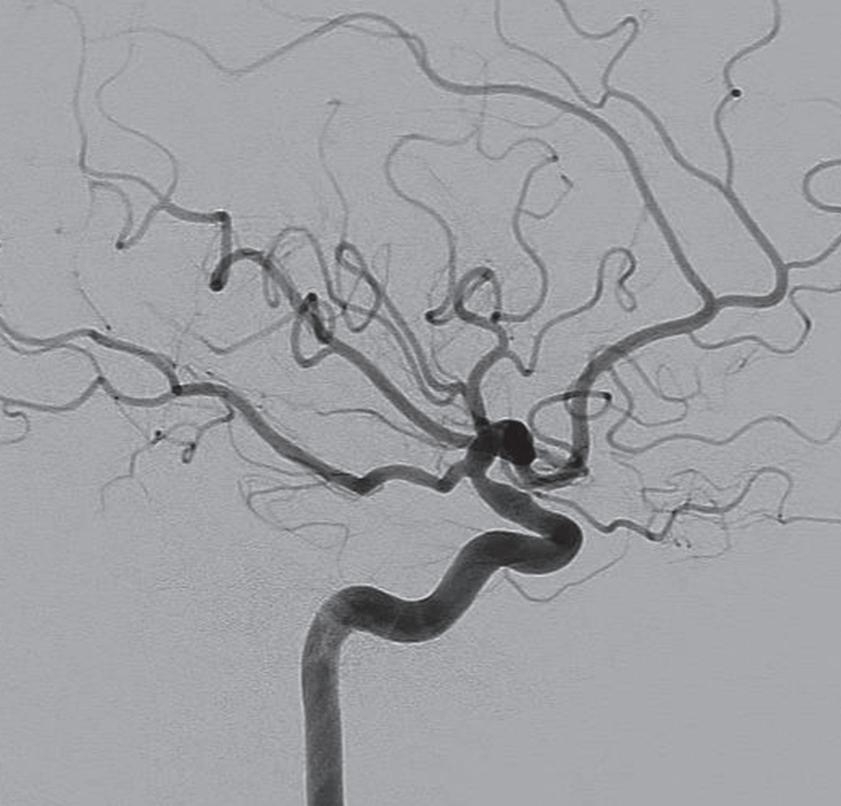
When the neurosurgeon is looking for propagation of the blister aneurysm along the wall of the internal carotid artery, postoperative angiography should be performed more frequently than it usually is performed for saccular aneurysms. Longer term follow-up angiograms are also necessary after the acute phase has passed because late progression of the aneurysm has been observed in some patients weeks to months later (Figure 2.5).
Figure 2.5 Lateral projection angiogram of the right internal carotid artery at followup shows mild narrowing of the carotid artery at the former location of the blister aneurysm, without progression.
Source: Used with permission from Barrow Neurological Institute, Phoenix, Arizona.