Blueprints Neurology was first published more than 15 years ago as one of a series of books designed to help medical students prepare for USMLE Steps 2 and 3. As the study and practice of Medicine and Neurology and professional board examinations have evolved over the years, so too has Blueprints Neurology changed to assist students to learn Neurology in multiple evaluation and examination settings.
Examination preparation remains at the core of the series. To that end, the authors review the subject matter of the examination before each edition. The authors and editors work together to organize the most important, current, and factually correct material into a complete but concise review guide. Our goal remains integrating the depth of factual knowledge with the breadth of practice information in order to optimize both understanding and retention. We have been pleased to hear from our readers that the book is utilized by many medical students during their clinical rotations, as well as in preparation for shelf and board examinations. Residents in Internal Medicine, Emergency Medicine, and Family Practice, as well as nurse practitioners and physicians’ associates have found Blueprints helpful during the Neurology portion of their training. We believe the book’s applications have broadened with each edition due to the quality of our authors’ experience and their dedication to highlighting and clarifying a targeted range of basic but important topics that should be mastered.
Virtually all chapters are authored by experts in the content area, including neurologists from both academic medicine and busy private practice groups. They have incorporated suggestions received from medical students, faculty, clinicians, and program directors with regard to content and organization. Each chapter covers a single subject area for review; most can be read in under an hour. “Key Points,” highlighted throughout, facilitate quick review of the key concepts tested most frequently. Most chapters have Vignettes with characteristic clinical presentations to test one’s review of the chapter. The 100 Questions at the end of the book are also written in the “Clinical Vignette” style used in USMLE and Board examinations, as recommended
by student reviewers of the Blueprints series.
This fifth edition of Blueprints Neurology is the most thoroughly updated edition to date, with several new authors (generally closer in stage of education to the students for whom the book is written). It includes important updates on areas such as Multiple Sclerosis, Stroke, Epilepsy, Movement disorders and their genetic bases, Sleep disorders such as narcolepsy and cataplexy, and new drug and other treatments for each. Each chapter includes the most recent information and practice principles available and accepted at the time of publication.
We hope that readers of Blueprints Neurology will come to see the wonder of the human nervous system, how important it is to individuals in health and when it fails, and how the study and practice of Neurology is more helpful to patients than ever before.
Frank W. Drislane, MD
Aimee K. Boegle, MD, PhD
Alexandra Hovaguimian, MD
Courtney McIlduff, MD, MMSc
Andrew W. Tarulli, MD
Louis R. Caplan, MD
Acknowledgments
We thank our patients for the opportunity of working with them and learning Neurology; our colleagues and teachers (and particularly, upon his retirement, Michael Ronthal, MBBCh) at Beth Israel Deaconess Medical Center Neurology department for teaching us more fascinating concepts about the nervous system; and our families for tolerating the many hours spent writing and revising this book.
TORCH toxoplasmosis, other agents, rubella, cytomegalovirus, herpes simplex
TR time to repetition
TSC tuberous sclerosis complex
UMN upper motor neuron
VA visual acuity
VDRL Venereal Disease Research Laboratory
VOR vestibulo-ocular reflex
VP venous pulsation
VPL ventroposterolateral
WD Wilson’s disease
PART I BASICS OF NEUROLOGY
1
The Neurologic Examination
The care of patients in all specialties has been enhanced by the use of an increasingly sophisticated array of biomarkers, genetic tests, and imaging modalities. Yet even in the setting of these critical advancements, the physical examination remains of utmost importance in Neurology. We glean valuable information from listening to the manner in which concerns are expressed, observing how patients walk into the clinic or lie in a hospital bed, and performing maneuvers designed to interrogate the functional integrity of nervous system components. Ultimately, the examination is a tool we use to pinpoint the nature and origin of abnormalities. The resultant picture can narrow the list of possible diagnoses and guide further investigation.
PRINCIPLES
It is useful to conduct a complete examination at least once for every Neurology patient. The neurologic examination may be unique in its length, but it is worthwhile to complete a thorough assessment at least once with each Neurology patient for several reasons. First, that examination provides a baseline assessment of neurologic status which can be particularly valuable in the hospital, where examinations can evolve in important and sometimes unforeseen ways. Second, a full examination may uncover unexpected abnormalities. One might be tempted to skip a full mental status examination for a patient who can exchange pleasantries normally only to be surprised when the patient identifies the year as 1962. Because neurologic problems can present with discrete deficits, formal testing in each domain is sensible. Third, abnormalities on basic tests can point out the need for more in-depth, specialized evaluations. For example, the emergence of diplopia on testing extraocular movements might prompt a search for fatigable eyelid
weakness that can raise concern for myasthenia gravis. In this way, the neurologic examination becomes tailored for each individual patient. Fourth, the examination allows one to directly confirm or refute hypotheses about contributory problems suggested by the history. Foot drop is more likely to result from a lumbosacral radiculopathy if accompanied by back pain; a positive straight leg raise test can help corroborate this explanation. Finally, the examination can show a pattern of abnormalities that provides a clue as to where in the nervous system the problem lies.
The goal is to localize the problem. The nervous system is extensive. Broadly, we can characterize elements as central or peripheral. The central nervous system includes the brain and spinal cord. The peripheral nervous system (PNS) incorporates nerve roots, plexi, peripheral nerves, neuromuscular junctions, and muscles. Dysfunction originating from each of these locations can translate into distinctive examination findings (Table 1-1); recognizing characteristic patterns is often the key to localizing a deficit. Using this approach, the exam can help determine whether left hand weakness stems from carpal tunnel syndrome, a brachial plexus injury, cervical radiculopathy, or a middle cerebral artery stroke. These distinctions are important because the diagnostic steps, prognoses, and therapies differ for each of these conditions.
Findings should be interpreted in the context of the history. In performing a comprehensive neurologic examination, it is not uncommon to detect incidental abnormalities. Particularly at the start of one’s career, it can be difficult to discern whether certain abnormalities are important. One should assign greater weight to findings related to the presenting symptoms or a patient’s medical history. For instance, abnormal sensation in a football-shaped region over the anterolateral thigh may be a key finding in an obese person who developed burning in this area after wearing tight-fitting pants, but an unimportant (or untrustworthy) discovery in an individual who presents with an acute change in mental status.
TABLE
1-1. Localizing Patterns of Sensorimotor Abnormalities
Location of Lesion Characteristic Distribution
Brain Right or left hemi-body (face, arm, and leg)
Brainstem
Crossed face and limbs (e.g., right face, left limbs)
Spinal cord At a sensory level on one or both sides of the posterior torso (at or above the site of the lesion)
Nerve root
Plexus
Peripheral nerves (polyneuropathy)
Neuromuscular junction
Muscle
●
●
●
Along an individual nerve root (i.e., a dermatome if a sensory change, or a myotome if weakness)
Patchy in affected upper or lower extremity
Distal, symmetric sensorimotor changes
Fatigable weakness
Proximal, symmetric weakness
KEY POINTS
A complete neurologic examination is important to identify and characterize patterns of abnormalities
The goal of the examination is to localize lesions in the nervous system. Findings should always be interpreted in the context of the clinical history.
ELEMENTS OF THE EXAMINATION
The details of the neurologic examination (Table 1-2) should be tailored to fit the patient’s presenting symptoms and identified abnormalities on a basic exam.
MENTAL STATUS
The mental status exam is performed to identify cognitive deficits related to specific regions in the brain. The first step is to assess level of consciousness, which can range from awake and alert to unarousable even with noxious stimulation. Rather than using medical terms such as stuporous or obtunded in the latter setting, it is more helpful to describe what external stimuli are required to arouse a patient or maintain wakefulness. The level of consciousness frames further testing of cognitive function. Attention is tested, typically by asking patients to recite spans of numbers, months, or words such as “world,” forward and backward. A specific form of inattention is referred to as neglect. Patients with dense neglect may fail to describe items on one side of a picture or of their surroundings or fail to bisect a line properly. Subtle neglect may manifest as extinction to double simultaneous
stimulation; in this scenario, a patient can sense a single visual or sensory stimulus on either side of the body but reports it on the nonneglected side alone when bilateral stimuli are presented. In some cases, it is not possible to perform formal tests of attention because patients become focused on one detail or task and keep repeating it (“perseveration”). Deficits in attention are important to recognize because they can compromise the ability to complete other tasks in the mental status examination. Orientation is tested by asking a patient to identify his or her name and location as well as the day, date, month, year, and current situation.
Memory is assessed by asking patients to repeat several words immediately and again after intervals (e.g., 30 seconds and 3 minutes). The examiner should make note of whether the patient is aware of current events. Language is assessed in several ways: by listening to the fluency and prosody of spontaneous speech, identifying word substitutions (i.e., paraphasic errors), and assessing the ability to repeat phrases, read, write, and name common and uncommon objects. Furthermore, the examiner can ask the patient to name as many words as possible starting with the letter “F,” “A,” or “S” in 1 minute, paying attention not only to the number of words generated but also to the manner in which they are named. For example, does the patient recognize whether she or he repeated words? Were words volunteered in identifiable categories? In addition to insight into language function, these details provide insight into how well patients can plan and organize information (i.e., frontal lobe executive function). To assess verbal comprehension, check to see if patients can follow spoken midline, appendicular, and cross-body commands.
TABLE 1-2.
Commonly Performed Elements of the Neurologic Examination
Mental Status
Attention Serial backward tasks (months of the year, digit span)
Language Fluency of speech, repetition, comprehension of commands, naming objects, reading, writing
Memory Recall of words after 5 minutes
Visuospatial function Clock drawing; complex figure copying
Neglect Line bisection, double simultaneous stimulation
Frontal lobe function Generation of word lists; performance of learned motor sequence; test of inhibition
Cranial Nerves
II
III, IV, VI
V, VII
IX, X, XII
Motor
Visual acuity, fields, pupils, funduscopic exam
Extraocular movements
Facial sensation and movement
Palate and tongue movement
Bulk Inspection for atrophy
Tone Evaluation for rigidity, spasticity
Power Observational tests (pronator drift, rising from chair, walking on heels and toes), direct confrontation strength testing
Reflexes
Muscle stretch reflexes Assessment at sites including biceps, brachioradialis, triceps, knee, ankle
Babinski sign Stroking lateral sole of foot
Sensory
Pinprick and temperature
Vibration and joint position sense
Mapping of pinprick, cold sensation
Timing appreciation of tuning fork stimulus at joints, assessing perception of location of limbs in space
Romberg sign Unsteady, when standing with feet together, then closing eyes
Coordination
Accuracy of targeting Finger-to-nose, heel-to-shin tests
Rhythm of movements Rapid alternating movements, rhythmic finger or heel tapping
Gait
Stance
Evaluation of narrow or wide base
Stride and arm swing Assessment for shuffling, decreased arm swing
Ataxia Evaluation of ability to tandem walk
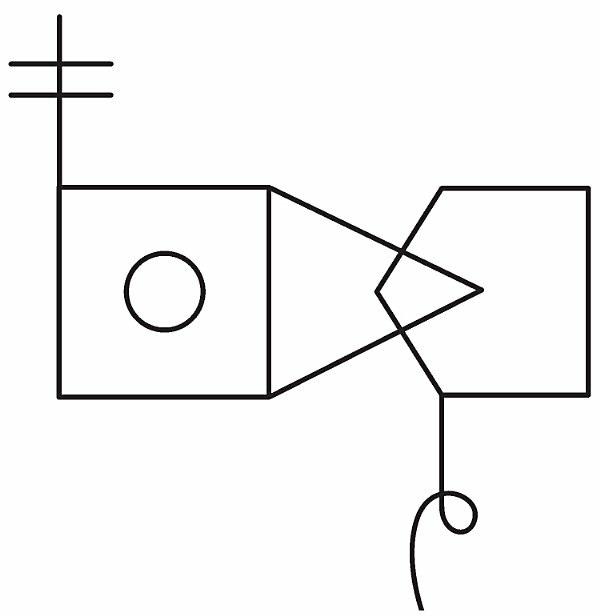
Calculation ability can be tested by asking patients to perform simple arithmetic (e.g., the number of quarters in $1.50). One can check for apraxia by asking patients to pantomime a learned motor task optimally one that requires use of both hands, for example, cutting a loaf of bread. Visuospatial function and nonverbal learning can be tested in a variety of ways. Patients can be asked to draw numbers in a circle to form a clock; alternatively, they can be asked to copy a complex figure drawn by the examiner (Fig. 1-1).
FIGURE 1-1. Example of a complex figure to be copied by the patient as test of visuospatial function.
Other tests of frontal lobe function include learning and then repeating a simple motor sequence of hand postures (i.e., the Luria manual sequencing task). Another test of appropriate inhibition, the go/no go test, comprises tapping the table when only one letter (e.g., “B”) is said aloud in a string of letters. Perseveration is also considered a frontal deficit. If cognitive impairment emerges as a concern, the examiner should consider looking for the presence of primitive reflexes, which are signs of “frontal release” or disinhibition. Examples include the palmo-mental, snout, and rooting reflexes; of note, the examiner should be careful not to overinterpret these reflexes, because they can occur in normal subjects with age or may not be relevant to the presenting problem.
KEY POINTS
The mental status exam should begin with assessment of level of consciousness and attention because these can affect the interpretation of subsequent tests Memory, language, calculation, praxis, visuospatial, and frontal lobe function are other key elements of the mental status exam that can suggest focal brain lesions.
CRANIAL NERVES
One way to test cranial nerves is to start at eye level and move down the face in approximate numerical order (Table 1-3).
Olfaction (I) is rarely tested. When patients report alterations in the ability to smell, each nostril should be tested separately. A non-noxious stimulus, such as coffee or vanilla, can be used.
Optic nerve (II) function is assessed in several ways. Visual acuity is investigated with a near card. Visual fields are tested by having the patient cover one eye and focus on the examiner’s nose; they are then asked to signal when they can appreciate a small red object enter the field of view from each of four quadrants when the object is held halfway between the patient’s eye and the examiner’s (the limits of the patient’s visual fields should correspond to those of the examiner’s). Direct visualization of the optic nerve can be achieved by fundoscopy. The afferent limb of the pupillary light reflex is also mediated by the optic nerve; the efferent limb is subtended by CN III.
Extraocular movements (III, IV, and VI) are tested in three main ways: by having the patient pursue a moving target (e.g., an examiner’s finger drawing of the letter “H” in front of the face; i.e., pursuit); by directing the patient’s gaze to various stationary targets or directions (saccades); and by having the patient fixate on an object while the head is turned passively (vestibuloocular movements). The presence of nystagmus should be noted.
Muscles of mastication (V) are tested by assessing the strength of jaw opening and palpating the contraction of the masseter when the jaw is clenched. Facial sensation can be tested to all modalities over the forehead (V1), cheek (V2), and jaw (V3) regions. The afferent limb of the corneal reflex is mediated by CN V; the efferent limb is controlled by CN VII.
Muscles of facial expression (VII) are tested by having patients raise the eyebrows, squeeze the eyes shut, puff the cheeks, or show the teeth. Though uncommonly tested, taste over the anterior two-thirds of the tongue is mediated by this nerve and can be evaluated with sugar or another nonnoxious stimulus.
Hearing (VIII) may be evaluated in each ear simply by whispering or rubbing fingers; more detailed assessment of hearing loss may be accomplished with the Weber and Rinne tuning fork (512 Hz) tests. Vestibular function can be tested in many ways, including evaluation of eye fixation while the patient’s head is turned rapidly or by observation for a gradual rotation of gait direction while the patient is walking in place with the eyes closed.
TABLE 1-3. The Cranial Nerves
Nerve Name Exit through the Skull Function
I Olfactory Cribriform plate
II Optic Optic canal
III Oculomotor Superior orbital fissure
Olfaction (test using nonnoxious substance)
Vision (acuity, fields, color), afferent limb of pupillary reflex
Superior rectus, inferior rectus, medial rectus, inferior oblique, levator palpebrae, efferent limb of pupillary reflex
IV Trochlear Superior orbital fissure Superior oblique of contralateral eye
V Trigeminal Superior orbital fissure (V1), foramen rotundum (V2), foramen ovale (V3)
Muscles of mastication, tensor tympani, tensor veli palatini, facial sensation, afferent limb of corneal reflex
VI Abducens Superior orbital fissure Lateral rectus
VII Facial Internal auditory meatus
VIII Vestibulocochlear Internal auditory meatus
IX Glossopharyngeal Jugular foramen
X Vagus Jugular foramen
XI Accessory Jugular foramen
XII Hypoglossal Hypoglossal foramen
Muscles of facial expression, stapedius, taste on anterior two-thirds of tongue, efferent limb of corneal reflex
Hearing, vestibular function
Movement of palate, sensation over palate and pharynx, taste over posterior one-third of tongue, afferent limb of gag reflex
Movement of palate; sensation over pharynx, larynx, and epiglottis; efferent limb of gag reflex; parasympathetic function of viscera
Sternocleidomastoid and trapezius movement
Tongue movement
Palate elevation should be symmetric, and the voice should not be hoarse or nasal (IX and X). Failure of the right palate to elevate implies pathology of the right glossopharyngeal nerve. The gag reflex is also mediated by these nerves.
Sternocleidomastoid strength is tested by having the patient turn the head against resistance; weakness on turning to the left implies a right accessory nerve (XI) problem. The trapezius muscle is tested by having patients shrug the shoulders.
Tongue protrusion should be in the midline. If the tongue deviates toward
KEY POINTS
● the right, the problem lies with the right hypoglossal nerve (XII).
Cranial nerve testing is most easily performed and recorded in approximate numerical order. Key elements of the cranial nerve exam include assessment of vision and eye movements, facial movement and sensation, and movements of the palate and tongue.
MOTOR EXAM
First, bulk is assessed by observing and palpating the muscles and comparing each side to the other and the patient’s overall muscle bulk to that expected for age.
Tone is one of the most important parts of the motor exam. In the arms, tone is checked by moving the patient’s arm, flexing and extending at the elbow, moving the wrist in a circular fashion, and pronating and supinating the forearm rapidly using a handshake grip. Abnormalities of tone such as spasticity and rigidity are discussed in subsequent chapters. Tone in the legs can be tested well only with the patient supine. The examiner lifts the leg up suddenly under the knee; in the presence of increased tone, the heel comes off the bed. Increased tone can be characterized further as rigid or spastic. In rigid limbs, the examiner can sense increased resistance throughout the passive movements, but spasticity is speed dependent, with abnormalities emerging with quick movements (e.g., elbow extension).
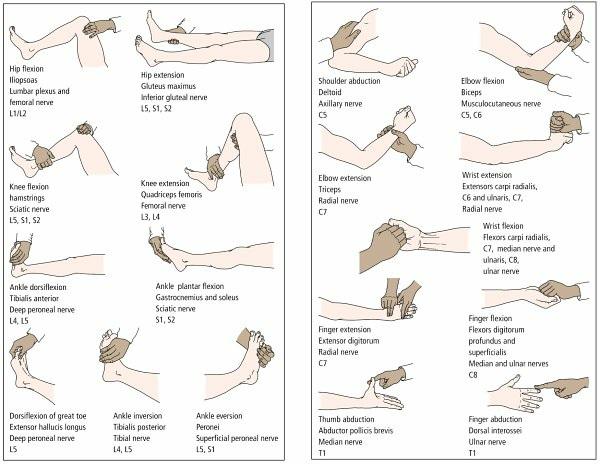
Strength is assessed by both observation and direct confrontation (Fig. 12). A pronator drift may be observed in an arm held supinated and extended in front of the body. The patient may be asked to rise from a chair without using the arms or to walk on the heels and toes. The power of individual muscles as assessed by direct confrontation testing is most often graded according to the Medical Research Council (MRC) scale (Table 1-4). In some settings, such as the intensive care unit, it is not possible to perform detailed motor assessments. In this case, the examiner can look to see if there is symmetry to voluntary limb movements. Another approach is to evaluate whether the patient can withdraw meaningfully (i.e., pull the examined limb away from a mildly noxious stimulus such as a pinch).
FIGURE 1-2. Power testing of individual movements. For each movement, the predominant muscle, peripheral nerve, and nerve root are given. (Reproduced with permission from Ginsberg L. Lecture Notes: Neurology. 8th ed. Oxford: Blackwell Publishing; 2005:40–41.)
The presence of involuntary abnormal movements should be noted. For instance, fasciculations appear as small twitches underneath the skin. Myoclonus and asterixis can cause a limb to jump or transiently lose tone from a given posture. Chorea has a writhing quality. Tremor can appear as an alternating movement of the arm, leg, or head.
TABLE 1-4. Medical Research Council Grading of Muscle Power
0 No contraction of muscle visible
1 Flicker or trace of contraction visible
2 Active movement at joint, with gravity eliminated
3 Active movement against gravity
4 Active movement against gravity and some resistance
5 Normal power
KEY POINTS
The motor exam begins with assessment of bulk and tone (including an assessment for spasticity and rigidity).
Strength testing involves both functional observation and confrontation testing of individual muscle power
Strength is graded on the MRC scale from 0 to 5
REFLEXES
Muscle stretch (or “deep tendon”) reflexes can be useful aids in localizing or diagnosing both central and PNS problems (Fig. 1-3).
FIGURE 1-3. Muscle stretch (“deep tendon”) reflexes. (Reproduced with permission from Ginsberg L. Lecture Notes: Neurology. 8th ed. Oxford: Blackwell Publishing; 2005:44.)
In the arms, the biceps, brachioradialis, and triceps reflexes are most commonly tested. A pectoral reflex can be assessed by tapping the pectoralis muscle and looking for adduction of the proximal arm. Thumb flexion stimulated by flicking the distal phalanx of the middle finger is a positive Hoffmann sign, an indication of hyperreflexia. In the legs, patellar (knee jerk) and ankle reflexes are commonly tested. The adductor reflex can also be tested by striking the medial thigh and looking for thigh adduction. The Babinski sign is sought by stroking the lateral sole of the foot while observing for extension of the great toe. Clonus, if present, can be elicited by forcibly dorsiflexing the ankle when it is relaxed. In some cases, an exaggerated jaw jerk can localize a problem above the level of the cervical spine.
SENSORY EXAM
The sensory examination assesses small-fiber (pinprick, temperature) and large-fiber (vibration, proprioception) function. Pinprick and temperature information is carried in the spinothalamic tract. Vibration and proprioception require dorsal column tract integrity. It is generally helpful to start distally and move proximally when testing each modality because polyneuropathy, one of the most common causes of sensory abnormality, generally shows up first in the toes. Nevertheless, it makes sense to test sensory function more extensively in any affected limb even if more distal function is normal to look for other patterns of abnormality.
Pinprick: Using a sterile instrument (e.g., special pins designed for the neurologic exam), the examiner starts to prick the toes and gradually moves up the leg to assess if there is a gradient to sensation. The process can be repeated starting in the fingers and moving up the arm. If there is concern for a spinal cord lesion, it is important to perform pinprick along the length of the torso to identify a “level” where sensation transitions from abnormal to normal. If the patient reports facial symptoms, the pin should be used to assess sensation in areas representing each branch of the trigeminal nerve.
Temperature: Using a similar approach, a cold tuning fork can be used to assess temperature sensation.
Vibration: After striking the 128-Hz tuning fork, the stem is placed against a joint, and the duration for which the stimulus is appreciated is recorded.
In general, this great toe is tested first, with the examiner testing increasingly proximal joints if the distal findings are abnormal.
Proprioception: Proprioception, or joint position sense, is tested in an order similar to that used for vibration assessment. Usually, the examiner starts by holding the sides of the great toe and asking the patient to report when it is being moved upward and downward by a few millimeters.
Light touch is often not useful to test in isolation because it relies on a combination of pathways. By itself it is unlikely to provide clues to localization or diagnosis.
KEY POINTS
Pinprick and temperature information is carried in the spinothalamic pathway, whereas vibration and joint position sense are relayed in the dorsal columns It is important to use an organized approach (e g , always moving distal to proximal along a limb) when testing sensory function.
COORDINATION
Coordination of the limbs and the trunk should be assessed. Finger-to-nose testing can identify dysmetria (inaccuracy of targeting) or types of tremor in the arms. Heel-to-shin testing can elicit incoordination in the legs. To test axial abnormalities, the patient can be asked to sit upright and unsupported, with the eyes closed.
Rapid alternating movements, rhythmic finger tapping, and heel tapping are particularly sensitive to coordination problems. In some disorders, such as Parkinson’s disease, there can be a hesitation, decremental slowing (i.e., damping), or increasingly small excursions with repetitive movements. Patients may also have trouble with the timing, or cadence, of these movements. Dysdiadochokinesis is the term used to describe difficulty with rapid alternating movements.
GAIT
Ambulation is one of the most important elements of the neurologic examination. Normal gait requires the proper functioning of many different aspects of the nervous system, so it is one of the most sensitive ways to detect
an abnormality. Furthermore, some patterns of gait abnormality herald the presence of specific disorders (e.g., parkinsonism). Routinely, posture, base, initiation, stride length, turning, arm swing, and overall balance are considered.
Posture should be upright. The patient with a normal base, or stance, maintains the feet at about hip-width apart. In general, healthy individuals start walking without any hesitation. Stride length should be full, with clearance of the feet from the floor. Short-stepped and shuffling gaits are characterized by decreased stride length and limited excursion of the feet from the ground. The arms normally swing fully in the opposite direction from their respective legs during ambulation. Decreased arm swing is often a feature of extrapyramidal disorders. A normal turn can be executed in two steps; patients with Parkinson’s disease may take multiple small steps to turn “en bloc.”
Ataxia of gait results in an inability to walk in a straight line; patients may stagger from one side to the other or list consistently toward one side. Ataxia is typically associated with a wide-based stance. Ataxia can be brought out most obviously by having the patient attempt to walk heel to toe (tandem). A Romberg sign is present when the patient maintains a steady stance with feet together and eyes open but sways and falls with feet together and eyes closed; its presence usually implies a deficit of joint position sense, not cerebellar dysfunction.
KEY POINTS
Gait is one of the most important elements of the neurologic exam because it is sensitive for many deficits, and certain diseases have characteristic gait disorders. Base, initiation, stride length, turning, arm swing, and the ability to perform tandem gait should be assessed
A positive Romberg sign suggests a deficit in joint position sense
2 Neurologic Investigations
CEREBROSPINAL FLUID ANALYSIS
Cerebrospinal fluid (CSF) bathes the internal and external surface of the brain and spinal cord. It is produced by the choroid plexus of the ventricles and is absorbed through the villi of the arachnoid granulations that project into the dural venous sinuses. CSF is produced continually at a rate of about 0.5 mL per minute; the total volume is approximately 150 mL. The entire CSF volume is thus replaced about every 5 hours. Lumbar puncture (LP) at the L3–L4 or L4–L5 interspace is the most commonly used means of obtaining CSF for analysis. LP is contraindicated by the presence of a space-occupying lesion that is causing mass effect in the central nervous system (CNS), raised intracranial pressure, local infection or inflammation at the planned puncture site, or a significant coagulopathy.
TECHNIQUE
Optimal positioning is the key to a successful and atraumatic LP. LP is best performed with the patient in the lateral decubitus position with the legs flexed up over the abdomen. Ideally, a pillow should be placed between the legs, and the patient should lie on the edge of the bed where there is better support to keep the back straight. The anterosuperior iliac spine is at the level of the L3–L4 vertebral interspace. The LP may be performed at this level, one interspace higher, or one to two interspaces lower. (Remember that the spinal cord ends at the level of L1–L2.) The needle is inserted with the bevel facing upward, so that it will enter parallel to the ligaments and dura that it pierces rather than cutting them transversely. The needle is directed slightly rostrally to coincide with the downward angulation of the spinous processes. The needle is advanced gently until CSF is obtained. To measure the opening
pressure reliably, the patient’s legs should be extended slightly and note should be made of fluctuation of the CSF meniscus within the manometer with respiration.
INTERPRETATION OF RESULTS
CSF is a clear, colorless fluid. The glucose content is about two-thirds that of blood, and it contains up to 40 to 50 mg/dL protein. Fewer than five cells are present, and these are lymphocytes. The opening pressure measured by LP in the lateral recumbent position is about 60 to 150 mm H2O.
Xanthochromia refers to the yellow discoloration of the supernatant of a spun CSF sample. Its presence helps to distinguish an in vivo intrathecal hemorrhage from a traumatic tap (in which red blood cells [RBCs] have not lysed, so the supernatant is still colorless).
The implications of various CSF findings are summarized in Table 2-1. CSF findings in a variety of common conditions are summarized in Table 22. Special tests may be performed as indicated. Some examples include cytology for suspected malignancy, oligoclonal banding for suspected immune-mediated processes such as multiple sclerosis, 14-3-3 protein for Creutzfeldt–Jakob disease, and a variety of polymerase chain reactions and serologic tests to detect infections of the nervous system.
SAFETY, TOLERABILITY, AND COMPLICATIONS
Cerebral or cerebellar herniation may occur when LP is performed in the presence of either a supratentorial or infratentorial mass lesion. A computed tomography (CT) scan should be performed prior to an LP when there are examination findings raising concern for increased intracranial pressure, focal neurologic findings, or severe encephalopathy. Radiologic contraindications to LP include closure of the fourth ventricle and quadrigeminal cistern. Lowpressure headache is the most common complication of LP. It is most effectively prevented by using smaller (higher gauge) LP needles, inserting the bevel of the LP needle parallel rather than perpendicular to the dural fibers, and replacing the stylet after obtaining CSF. Should a post-LP headache develop, it is treated initially by having the patient lie flat and increase his or her intake of liquids and caffeine. In patients who do not respond to these conservative measures, it may be necessary to administer an epidural blood patch (see Chapter 10).
COMPUTED TOMOGRAPHY AND MAGNETIC RESONANCE IMAGING
TECHNICAL CONSIDERATIONS
CT measures the degree of X-ray attenuation by tissue. Attenuation is defined simply as the removal (by absorption or scatter) of X-ray photons and is quantified on an arbitrary scale (in Hounsfield units) that is represented in shades of gray. Differences in the shades directly reflect the differences in the X-ray attenuation of different tissues, a property that depends on their atomic number and physical density. Images are usually obtained in either an axial or a coronal plane. Three-dimensional reconstruction and angiography are possible with new-generation spiral CT scanners.
Magnetic resonance imaging (MRI) is similar to CT in that radiant energy is directed at the patient and detected as it emerges from the patient. MRI differs, however, in its use of radiofrequency (RF) pulses rather than X-rays. The images in MRI result from the varying intensity of radio-wave signals emanating from the tissue in which hydrogen ions have been excited by an RF pulse. A detailed understanding of magnetic resonance physics is not necessary for the interpretation of routinely used MRI sequences. It is sufficient to understand that the patient is placed in a magnet and that an RF pulse is administered. Signal intensity is measured at a time interval, known as time to echo (TE), following RF administration. The RF pulse is administered many times in generating an image; the time to repetition (TR) is the time between these RF pulses.
Two basic MRI sequences in common usage are T1-weighted (short TE and TR) and T2-weighted (long TE and long TR) images. Fat is bright on a T1-weighted image, which imparts a brighter signal to the myelin-containing white matter. Water (including CSF) is dark on T1 and bright on T2. T2 images are most useful in evaluating the spinal cord (Fig. 2-1). Gadolinium is the contrast agent used in MRI, and gadolinium-enhanced images are usually