Visit to download the full and correct content document: https://ebookmass.com/product/neurologic-complications-of-critical-illness-contempor ary-neurology-series-team-ira-4th-edition-eelco-f-m-wijdicks/
More products digital (pdf, epub, mobi) instant download maybe you interests ...
Critical Care Neurology Part II 1st Edition Edition
Jasper R. Daube, MD, and Devon I. Rubin, MD, Editors
76 PERIPHERAL NEUROPATHIES IN CLINICAL PRACTICE
Steven Herskovitz, MD, Stephen N. Scelsa, MD, and Herbert H. Schaumburg, MD
77 CLINICAL NEUROPHYSIOLIOGY OF THE VESTIBULAR SYSTEM
Fourth Edition
Robert W. Baloh, MD, and Kevin A. Kerber, MD
78 THE NEURONAL CEROID LIPOFUSCINOSES (BATTEN DISEASE)
Second Edition
Sara E. Mole, PhD, Ruth D. Williams, MD, and Hans H. Goebel, MD, Editors
79 PARANEOPLASTIC SYNDROMES
Robert B. Darnell, MD, PhD, and Jerome B. Posner, MD
80 JASPER’S BASIC MECHANISMS OF THE EPILEPSIES
Jeffrey L. Noebels, MD, PhD, Massimo Avoli, MD, PhD, Michael A. Rogawski, MD, PhD, Richard W. Olsen, PhD, and Antonio V. Delgado-Escueta, MD
81 MYASTHENIA GRAVIS AND MYASTHENIC DISORDERS
Second Edition
Andrew G. Engel, MD
82 MOLECULAR PHYSIOLOGY AND METABOLISM OF THE NERVOUS SYSTEM
Gary A. Rosenberg, MD
83 SEIZURES AND EPILEPSY
Second Edition
Jerome Engel, Jr., MD, PhD
84 MULTIPLE SCLEROSIS
Moses Rodriguez, MD, Orhun H. Kantarci, MD, and Istvan Pirko, MD
85 FRONTOTEMPORAL DEMENTIA
Bruce L. Miller, MD
86 AUTONOMIC NEUROLOGY
Eduardo E. Benarroch, MD
87 EVALUATION AND TREATMENT OF MYOPATHIES
Second Edition
Emma Ciafaloni, MD, Patrick F. Chinnery, FRCP, FMedSci, and Robert C. Griggs, MD, Editors
88 MOTOR NEURON DISEASE IN ADULTS
Mark Bromberg, MD
89 HYPERKINETIC MOVEMENT DISORDERS
Roger M. Kurlan, MD, Paul E. Green, MD, and Kevin M. Biglan, MD, MPH
90 THE NEUROLOGY OF EYE MOVEMENTS
Fifth Edition
R. John Leigh, MD, FRCP, and David S. Zee, MD
91 MIGRAINE
Third Edition
David W. Dodick, MD, and Stephen D. Silberstein, MD
92 CLINICAL NEUROPHYSIOLOGY
Fourth Edition
Devon Rubin, MD and Jasper Daube, MD, Editors
93 NEUROIMMUNOLOGY
Bibiana Bielekova, MD, Gary Birnbaum, MD, and Robert P. Lisak, MD
94 PLUM AND POSNER’S DIAGNOSIS AND TREATMENT OF STUPOR AND COMA
Fifth Edition
Jerome B. Posner, MD, Clifford B. Saper, MD, PhD, Nicholas D. Schiff, MD, and Jan Claassen, MD, PhD
95 CLINICAL NEUROPHYSIOLOGY
Fifth Edition
Devon I. Rubin, MD, Editor
96 PARKINSON DISEASE
Roger L. Albin, MD
97 NEUROLOGIC COMPLICATIONS OF CRITICAL ILLNESS
Fourth Edition
Eelco F. M. Wijdicks, MD, PhD
NEUROLOGIC COMPLICATIONS OF CRITICAL ILLNESS
Fourth Edition
Eelco F. M. Wijdicks, MD, PhD, FACP, FNCS
Professor of Neurology
Neurocritical Care Services
Department of Neurology, Mayo Clinic
Rochester, Minnesota
Oxford University Press is a department of the University of Oxford. It furthers the University’s objective of excellence in research, scholarship, and education by publishing worldwide. Oxford is a registered trade mark of Oxford University Press in the UK and certain other countries.
Published in the United States of America by Oxford University Press 198 Madison Avenue, New York, NY 10016, United States of America.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Oxford University Press, or as expressly permitted by law, by license, or under terms agreed with the appropriate reproduction rights organization. Inquiries concerning reproduction outside the scope of the above should be sent to the Rights Department, Oxford University Press, at the address above.
You must not circulate this work in any other form and you must impose this same condition on any acquirer.
Library of Congress Cataloging-in-Publication Data
Names: Wijdicks, Eelco F. M., 1954– author. | Mayo Foundation for Medical Education and Research, sponsoring body. Title: Neurologic complications of critical illness / Eelco F.M. Wijdicks. Other titles: Contemporary neurology series.
Description: 4. | New York, NY : Oxford University Press, [2023] | Series: Contemporary neurology series | Includes bibliographical references and index. Identifiers: LCCN 2022040676 (print) | LCCN 2022040677 (ebook) | ISBN 9780197585016 (hardback) | ISBN 9780197585030 (epub) | ISBN 9780197585047 (online)
Subjects: MESH: Critical Illness | Neurologic Manifestations | Critical Care
LC record available at https://lccn.loc.gov/2022040676
LC ebook record available at https://lccn.loc.gov/2022040677
DOI: 10.1093/med/9780197585016.001.0001
This material is not intended to be, and should not be considered, a substitute for medical or other professional advice. Treatment for the conditions described in this material is highly dependent on the individual circumstances. And, while this material is designed to offer accurate information with respect to the subject matter covered and to be current as of the time it was written, research and knowledge about medical and health issues is constantly evolving and dose schedules for medications are being revised continually, with new side effects recognized and accounted for regularly. Readers must therefore always check the product information and clinical procedures with the most up-to-date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulation. The publisher and the authors make no representations or warranties to readers, express or implied, as to the accuracy or completeness of this material. Without limiting the foregoing, the publisher and the authors make no representations or warranties as to the accuracy or efficacy of the drug dosages mentioned in the material. The authors and the publisher do not accept, and expressly disclaim, any responsibility for any liability, loss, or risk that may be claimed or incurred as a consequence of the use and/or application of any of the contents of this material.
Printed by Integrated Books International, United States of America
Preface xiii
PART I CRITERIA, URGENCY, AND IMPORTANCE
1. INDICATIONS FOR A NEUROLOGIC CONSULT IN THE INTENSIVE CARE UNIT 3
CATEGORIES OF CONSULTS 4
BENEFITS OF A CONSULTATION 6
2. CONSULTING IN THE INTENSIVE CARE UNIT 9
PREPARATION AND HISTORY-TAKING 9
COMMON REQUESTS FOR CONSULTS IN THE ICU 10
PART II GENERAL CLINICAL NEUROLOGIC PROBLEMS IN THE INTENSIVE CARE UNIT
3. ACUTE CONFUSIONAL STATE IN THE INTENSIVE CARE UNIT 19
TERMINOLOGY 20
ASSESSMENT OF DELIRIUM 21
NEUROLOGIC EXAMINATION OF THE ACUTELY CONFUSED PATIENT 23
MANAGEMENT OF DELIRIUM 24
4. COMA AND OTHER STATES OF ALTERED AWARENESS IN THE INTENSIVE CARE UNIT 27
DEFINITIONS OF ALTERED STATES OF CONSCIOUSNESS 27
NEUROLOGIC EXAMINATION OF THE COMATOSE PATIENT 32
CAUSES OF COMA 39
NEUROLOGIC EXAMINATION IN BRAIN DEATH 39
5. NEUROLOGIC MANIFESTATIONS OF MUSCLE RELAXANTS AND DRUGS USED FOR ANALGESIA AND ANESTHESIA IN THE INTENSIVE CARE UNIT 47
PRINCIPLES OF PHARMACODYNAMICS AND PHARMACOKINETICS IN CRITICAL ILLNESS 48
EFFECT OF DRUGS ON NEUROMUSCULAR JUNCTION 51
EFFECT OF DRUGS ON LEVEL OF CONSCIOUSNESS 55
6. SEIZURES IN THE INTENSIVE CARE UNIT 63
GENERALIZED TONIC–CLONIC SEIZURES 64
DRUG-INDUCED AND DRUG-WITHDRAWAL SEIZURES 64
SEIZURES AND ACUTE METABOLIC DERANGEMENTS 67
SEIZURES AND STRUCTURAL CENTRAL NERVOUS SYSTEM ABNORMALITIES 68
CONVULSIVE STATUS EPILEPTICUS 68
NONCONVULSIVE STATUS EPILEPTICUS 72
MANAGEMENT OF SEIZURES AND STATUS EPILEPTICUS 73
OUTCOME 79
7. GENERALIZED WEAKNESS IN THE INTENSIVE CARE UNIT 85
GENERAL CONSIDERATIONS 86
DISORDERS OF THE SPINAL CORD 86
DISORDERS OF PERIPHERAL NERVES 88
DISORDERS OF THE NEUROMUSCULAR JUNCTION 92
DISORDERS OF SKELETAL MUSCLE 93
8. ACUTE FOCAL NEUROLOGIC FINDINGS AND ASYMMETRIES IN THE INTENSIVE CARE UNIT 103
GENERAL CONSIDERATIONS IN LESION LOCALIZATION 103
BRAIN INJURY PATTERNS 108
9. ACUTE MOVEMENT ABNORMALITIES IN THE INTENSIVE CARE UNIT 111
SEMIOLOGY 112
EMERGENT AND URGENT MOVEMENT ABNORMALITIES 115
PART III NEUROLOGIC COMPLICATIONS IN MEDICAL AND SURGICAL INTENSIVE CARE UNITS AND TRANSPLANTATION UNITS
10. NEUROLOGIC COMPLICATIONS OF INVASIVE PROCEDURES IN THE INTENSIVE CARE UNIT 123
NEUROTOXICITY OF RADIOLOGIC CONTRAST AGENTS 124
CHOLESTEROL EMBOLIZATION 124
AIR EMBOLISM 126
NEUROLOGIC COMPLICATIONS ASSOCIATED WITH SPECIFIC PROCEDURES 127
11. NEUROLOGIC MANIFESTATIONS OF ACUTE BACTERIAL INFECTIONS AND SEPSIS 147
BACTERIAL MENINGITIS 147
SPINAL EPIDURAL ABSCESS 151
INFECTIVE ENDOCARDITIS 154
CLOSTRIDIAL SYNDROMES 161
SEPSIS 164
12. NEUROLOGIC MANIFESTATIONS OF VIRAL OUTBREAKS 175
WEST NILE VIRUS NEUROINVASIVE DISEASE 176
TICK- AND MOSQUITO-BORNE ENCEPHALITIS 179
ENDEMIC INFLUENZA 180
SARS-COV-2 (COVID-19) PANDEMIC 183
13. NEUROLOGIC COMPLICATIONS OF CARDIAC ARREST 189
GENERAL CONSIDERATIONS IN RESUSCITATION MEDICINE 190
POSTRESUSCITATION ENCEPHALOPATHY 193
SUPPORTIVE CARE 203
SPECIFIC TREATMENT AND TARGETED TEMPERATURE MANAGEMENT 204
14. NEUROLOGIC MANIFESTATIONS OF ACID–BASE DERANGEMENTS, ELECTROLYTE DISORDERS, AND ENDOCRINE CRISES 215
ACID–BASE DISORDERS 215
ELECTROLYTE DISORDERS 219
ENDOCRINE EMERGENCIES 232
15. NEUROLOGIC COMPLICATIONS OF ACUTE RENAL DISEASE 249
UREMIC ENCEPHALOPATHY 249
DIALYSIS DYSEQUILIBRIUM SYNDROME 253
POSTERIOR REVERSIBLE ENCEPHALOPATHY SYNDROME 255
NEUROMUSCULAR DISORDERS 260
16. NEUROLOGIC MANIFESTATIONS OF ACUTE HEPATIC FAILURE 269
GENERAL CONSIDERATIONS 270
HEPATIC ENCEPHALOPATHY 270
BRAIN EDEMA IN FULMINANT HEPATIC FAILURE 275
17. NEUROLOGIC COMPLICATIONS ASSOCIATED WITH DISORDERS OF THROMBOSIS AND HEMOSTASIS 289
GENERAL CONSIDERATIONS 289
DISSEMINATED INTRAVASCULAR COAGULATION 290
THROMBOLYSIS AND ANTICOAGULATION 291
NEOPLASTIC COAGULOPATHIES 295
THROMBOTIC THROMBOCYTOPENIC PURPURA 297
18. NEUROLOGIC COMPLICATIONS OF ACUTE VASCULITIS SYNDROMES 305
GENERAL CONSIDERATIONS 305
LARGE-VESSEL VASCULITIS 307
POLYARTERITIS NODOSA 308
CHURG-STRAUSS SYNDROME 312
GRANULOMATOSIS WITH POLYANGIITIS 313
DRUG-INDUCED VASCULITIS 315
19. NEUROLOGIC COMPLICATIONS IN THE CRITICALLY ILL PREGNANT PATIENT 321
NEUROLOGY OF PREGNANCY 321
ECLAMPSIA 323
HELLP SYNDROME 326
AMNIOTIC FLUID EMBOLISM 328
NEUROLOGIC COMPLICATIONS OF TOCOLYTIC AGENTS 328
20. NEUROLOGIC COMPLICATIONS OF CANCER IN THE ICU 333
GOALS OF CARE IN CRITICAL ILLNESS AND ADVANCED CANCER 334
NEURO-ONCOLOGIC EMERGENCIES 334
PARANEOPLASTIC ENCEPHALITIS 336
COMPLICATIONS OF RADIATION AND CHEMOTHERAPY 338
COMPLICATIONS OF CANCER IMMUNOTHERAPY 340
21. NEUROLOGIC COMPLICATIONS OF AORTIC SURGERY 343
SCOPE OF THE PROBLEM 344
VASCULAR ANATOMY OF THE SPINAL CORD 346
NEUROLOGIC FEATURES OF SPINAL CORD INFARCTION 348
DIAGNOSTIC EVALUATION OF SPINAL CORD INFARCTION 350
THERAPEUTIC OPTIONS 353
PLEXOPATHIES 354
AORTIC DISSECTION 354
22. NEUROLOGIC COMPLICATIONS OF CARDIAC SURGERY 361
GENERAL CONSIDERATIONS 362
ISCHEMIC STROKE 366
NEUROPSYCHOLOGIC IMPAIRMENT 373
SEIZURES 374
RETINAL DAMAGE 374
PERIPHERAL NERVE DAMAGE 375
23. NEUROLOGIC COMPLICATIONS OF ACUTE ENVIRONMENTAL INJURIES 385
THERMAL BURNS 385
SMOKE INHALATION 389
ELECTRICAL BURNS 392
LIGHTNING INJURY 393
ACCIDENTAL HYPOTHERMIA 395
HEAT STROKE 397
NEAR-DROWNING 399
24. NEUROLOGIC COMPLICATIONS OF DRUG OVERDOSE, POISONING, AND TERRORISM 407
THE PRESENTING EMERGENCY AND PRINCIPLES OF TREATMENT 408
SPECIFIC POISONINGS 410
BIOLOGICAL AND CHEMICAL WARFARE 419
25. NEUROLOGIC COMPLICATIONS OF TRAUMATIC BRAIN INJURY 429
CLINICAL SPECTRUM OF HEAD INJURY 430
NEURORADIOLOGIC FINDINGS IN HEAD INJURY 430
GENERAL PRINCIPLES OF MANAGEMENT 440
MANAGEMENT OF INCREASED INTRACRANIAL PRESSURE 442
MANAGEMENT OF TRAUMATIC INTRACRANIAL HEMATOMAS 444
WAR-RELATED BRAIN INJURY 446
MANAGEMENT OF TRAUMATIC CEREBRAL ANEURYSM 446
26. NEUROLOGIC COMPLICATIONS OF TRAUMA TO THE SPINE, SPINAL CORD, AND NERVES 455
TRAUMA OF SPINE AND SPINAL CORD 455
ACUTE SPINAL CORD INJURY 464
POSTTRAUMATIC NEUROPATHIES ASSOCIATED WITH FRACTURES 467
FAT EMBOLISM SYNDROME 468
27. NEUROLOGIC COMPLICATIONS OF ORGAN TRANSPLANTATION 473
SURGICAL TECHNIQUES OF ORGAN TRANSPLANTATION 474
NEUROLOGIC COMPLICATIONS IN TRANSPLANT RECIPIENTS 479
NEUROLOGIC COMPLICATIONS OF GRAFT-VERSUS-HOST DISEASE 501
28. OUTCOME OF ACUTE INJURY TO THE CENTRAL NERVOUS SYSTEM 513
DESCRIPTION OF OUTCOME CATEGORIES 514
OUTCOME IN ENCEPHALOPATHIES 516
OUTCOME IN STROKE 522
OUTCOME IN HEAD INJURY 524
OUTCOME IN TRAUMATIC SPINE INJURY 525
OUTCOME IN CENTRAL NERVOUS SYSTEM INFECTIONS 525
PART V CONSULTATIVE NEUROLOGY AND END-OF-LIFE CARE IN THE INTENSIVE CARE UNIT
29. THE NEUROLOGIST AND END-OF-LIFE CARE IN THE INTENSIVE CARE UNIT 533
GENERAL CONSIDERATIONS 534
LEGAL ASPECTS OF WITHDRAWAL OF TREATMENT 534
DECISIONS IN WITHDRAWAL OF TREATMENT 535
WITHDRAWAL OF TREATMENT 536
WITHDRAWAL OF TREATMENT IN SPECIAL NEUROLOGIC CIRCUMSTANCES 537
BRAIN DEATH AND ORGAN DONATION 538
CARDIAC DEATH AND ORGAN DONATION 539
30. THE NEUROLOGIST AND ICU ETHICAL DILEMMAS 545
PRINCIPLES OF COMMUNICATION WITH FAMILIES 546
HOPE 547
FUTILITY 548
GUIDING A FAMILY CONFERENCE 548
THE ETHICS OF COMPASSIONATE SEDATION 550
THE COURTS 550
Index 553
Preface
Writ large in this book is the premise that the evaluation of a critically ill patient with a neurologic manifestation or complication is the most demanding neurology consultation. This book, when first published in 1995, provided a practical guide for every disquieted neurologist who entered the intensive care unit (ICU). Just about what, as a young neurologist, I would have liked to have known. Keeping this book up to date requires multiple editions because intensive care is one of the fastest growing and changing specialties. Now, more than 25 years later, we can look back at the extraordinary expansion in knowledge of critical illness and better understanding of this field of neurology. Intensivists understand the issues involved and appreciate that a neurologic complication in any medical or surgically critically ill patient is a major cause of mortality and later morbidity. If recognized in time, treatment of a neurologic complication may greatly improve the outcome. But neurocritical care in all its forms is also at times informed uncertainty, and many clinical observations are not understood.
The framework of consults has also changed. New diseases have appeared, such as neurologic complications of cancer immunotherapy, and older diseases, such as cyclosporine neurotoxicity in transplant patients, have become rare occurrences. Neurotoxicities of drugs are better understood (e.g., serotonin syndrome and cefepime neurotoxicity). Recent mosquito- and tick-borne illness (e.g., Zika virus, Chikungunya, and Eastern equine encephalitis) in the United States has resulted in intensive care admissions. The world since 2019 has been shaken by the SARS-CoV-2 pandemic with its multiple surges and no ICU spared. The pandemic has been a revelation, certainly since the end of 2021, when ICUs (and morale) were at a breaking point as a result of treating an unacceptably large number of unvaccinated patients who became infected with the delta variant. Neurologic complications of SARS-CoV-2 infection have emerged, and this damaging respiratory virus became the most common reason to consult neurologists, who, like their colleagues in other specialties, had the disadvantage of dealing with a new disease. It is a prime example of how suddenly ICU populations can change and have changed again in 2023.
The new edition has responded to changes in ICU care and changes in the ICU population and is now thoroughly updated. I have added criteria for consultation and how to co-manage patients. A consultation is often contingent on the following five perceptions: (1) an evolving situation that requires neurologic expertise; (2) “something” might not be recognized; (3) an unusual CT scan that does not appear to explain the condition; (4) movements that could indicate seizures requiring expert evaluation and electroencephalography (EEG); and (5) the patient’s condition looks grim but needs corroboration, and the family may request a neurologic opinion. All this is addressed. Neurologic consultations are often requested when patients remain comatose after CPR, and the neurologist is asked to have the last word. Failure to awaken after surgery or after extended sedation has been discontinued are other typical examples that trigger a request. We have an obligation to provide the best evaluation and management when the outcome can go either way. We also have an obligation to evaluate for futility. Neurologic consultation not only provides diagnostic, therapeutic, and prognostic advice but may also change the approach to the patient. This is a major responsibility and not one to be taken lightly.
This edition also has new chapters on the interpretation of focal findings, acute movement disorders in critical illness, cancer immunotherapy, and ethical dilemmas. A separate section on interpretation of EEG requests (and how to use it in critically ill patients) is added. Several new drugs (direct oral anticoagulants [DOACs] and chimeric antigen receptor T-cell therapy [CAR-T]) have made their way into the ICU and are discussed in detail because their side effects require specific intervention. There is a wealth of new tables, algorithms, and neuroimaging. I have added a new section of advice for practical management to each chapter to reconcile theory and practice.
ICUs are challenged with an increasingly growing (and aging) population, and admissions are increasing. Neurologic complications will increase, too. This clinical text will be helpful to a very wide audience of healthcare providers and, in particular, for any intensivist and general neurologist who must manage these patients with extremely complex medical disorders, surgeries, comorbidity, and with different clinical trajectories. The book is also aimed at neurointensivists who consult in ICUs other than their own. This book reaches beyond neurology and additionally targets emergency physicians, neurosurgeons, transplant and vascular surgeons, internal medicine hospitalists, pharmacists, allied healthcare providers, and ICU nursing staff.
I appreciate the help of so many. Lea Dacy not only dutifully edited the full manuscript, but she has always been absolutely necessary to improve the prose. I am grateful for the work by the illustrators of Mayo Clinic Media Support service and, in particular, David Factor, who predictably provided beautiful and informative drawings. I appreciate my long-time working relationship with Oxford University Press, and they are peerless when it comes to academic work.
The interest in the acute neurosciences in practice is the unexpected. I have lived the subject matter for several decades, and our neurocritical care group sees several hundred patients in ICUs other than our own Neurosciences ICU each year. I hope the book I set out to write reflects that experience. The diagnosis and management of neurologic complications in critical illness, in my view, has always been one of the major pillars of neurocritical care.
March 2023
Eelco Wijdicks
PART I
Criteria, Urgency, and Importance
Chapter 1
Indications for a Neurologic Consult in the Intensive Care Unit
CATEGORIES OF CONSULTS
BENEFITS OF A CONSULTATION
Teamsworkinginintensivecareunits(ICUs)may bring in a neurologist and for all kinds of reasons.1 When called to action, most neurologists entering an ICU are immediately confronted with the complexity of critical illness. The modern ICU is a unique place, with patients presenting with an array of different conditions and with consultants having specific expertise in handling critical illness. Patients enter the ICU in a life-threatening state with failing organ systems and become hypotensive, hypoxemic, hypercapnic, and tachycardic; the initial resuscitation generally does not concentrate on neurologic manifestations. Most intensivists briefly check for pupil responses or major asymmetries, but they accept an altered level of consciousness as a common consequence of an evolving critical illness. Some manifestations may not be considered atypical enough for an urgent neurologic consult. This logically implies that neurologists will see a selection of neurologic manifestations in critical illness. ICU consultative neurology focuses on those patients admitted to medical and surgical ICUs
presenting with a de novo neurological problem related to their illness—questions ... and issues concerning the effects of antiseizure and antiparkinson medication for prior diagnosed illness are entirely different. These patients are seen in consultation for diagnosis and management—often expediently—but remain under the care of intensivists and surgeons. The complications observed may be quite specific (or mundane), but intensivists may intuitively feel uncomfortable in overseeing these new neurologic conditions themselves. They request not only assistance in identifying the neurologic disorder but also help in management. This is particularly pertinent with recurrent seizures or progressive neurologic decline. Once the patient is seen, continuous attention is necessary, which may involve prolonged bedside care and, later, calls at night from nursing staff or attending intensivists and, ultimately, direct management. Interpretation of electroencephalograms and neuroimaging is often repeatedly required.2
More than in any place in the hospital, ICU consultationsinvolvequestionsaboutde-escalating care.Theattendingteamandfamilymayconsider withdrawing intensive care or, at least, consider a do-not-resuscitate status and thus need a neurologist’s input. This involvement partly reflects the high prevalence of neurologic catastrophes in patients with a critical illness. Frequently, the clinical situation is clear, as in persistently comatose survivors after prolonged cardiopulmonary arrest and in elderly patients with polytrauma and severe traumatic brain injury; in other situations, the degree of brain injury may be more difficult to ascertain. Neurologists are asked to participate in family conferences, and they can be helpful in clarifying the bigger picture. Sometimes, the neurologic complication is a defining moment, and little more can be done for the patient. Neurologists can be conclusive and advise the managing ICU team against treating a patient in a futile situation. In other situations the neurologic situation could be misjudged as irrecoverably poor while there is a possibility for another more favorable trajectory. This is not an uncommon scenario, and neurologists can shed more light on why they think that way. Another fundamental rule of ICU consultation is to prognosticate decisively when certain but to hold back when information is incomplete or the clinical situation is not fully understood.
Critical illness increases the probability of a neurologic complication, and, according to current best estimates and excluding pervasive delirious states, approximately 10–20% of patients will develop some sort of neurologic manifestation. The neurology of critical illness is an important field that requires more prospective research. The rationale for neurologic
Table 1.1 The field of neurology of critical illness
Neurologic consultation in the ICU requires a broad base of medical knowledge
Neurologic consultation provides diagnostic, therapeutic, and prognostic advice
Neurologic consultation often involves assessment of abnormalities of responsiveness or seizures
Neurologic consultation may detect an unsuspected neurologic disorder
Neurologic consultation in the ICU may change approach to the patient
Neurologic consultation involves end-of-life decisions for patients
consultation is summarized in Table 1.1 and shows common clinical neurologic problems facing the intensive care specialist and consulting neurologist in everyday decisions.
CATEGORIES OF CONSULTS
We must assume that ICU consults are urgent or emergent. The urgency is often determined by an inability to understand the full clinical picture and particularly when the initial presentation is disturbing. Examples are ICU consults for acutely impaired consciousness, which require a quick but comprehensive assessment of the cause of coma and whether it can be immediately reversed. Upon receiving a call to consult in the ICU, we typically expect three clinical scenarios: acute loss of consciousness, failure of patients to awaken fully after recuperation from a major surgical procedure, and occasionally, coma in a developing but undiagnosed critical illness. We areoftenconsultedtoevaluateandtreatdelirium, and we now have a better sense of what this acute brain dysfunction could entail.3–6
Any consult in a critically ill neurologic patient must proceed through the steps outlined in Table 1.2. Any consult in a critically ill patient may lead to a diagnosis not initially considered by the managing team; in our experience, this occurs rather frequently.7 These recognized neurologic disorders may all have major consequences diagnostically, prognostically, and therapeutically.
Consultations may have a varying degree of complexity and may involve management of major acute neurologic injury. Consultation may evolve from a simple question, to being physically present, to continuously managing
Table 1.2 Essentials of a neurology consult in the intensive care unit
Assess details on severity of critical illness
Assess blood pressure and extent of blood pressure support
Assess drug administration over 5–7 days
Verify onset of symptoms with nursing staff
Assess major confounders
Assess for focal localizing sign
Assess for movements, twitching, new rigidity
Assess for drugs strongly related to movement disorders
Table 1.3
Reasons for a consult in the intensive care unit
Acutely comatose
Failure to awaken after resuscitation
Acute focal deficit
Acute agitation
New seizure(s)
Acute repetitive movements
Generalized weakness
Abnormal neuroimaging
Abnormal EEG
an acute injury to the brain or spine and, as such, may even involve palliation and end-oflife discussions (Table 1.3).
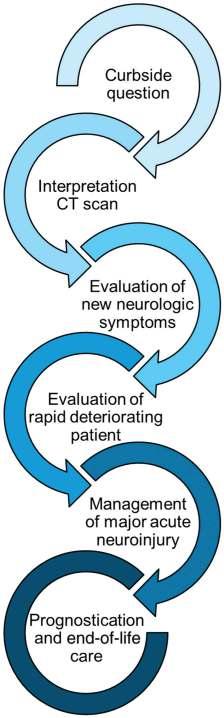
There is a spectrum of close participation with the consulting neurologist (Figure 1.1). In some cases, a consult consists of picking up the phone and asking an expert, and in many
intensive care practices, it is often easier to call a consultant rather than to ask for a formal consult. Both parties often agree that some type of advice will pragmatically direct testing or treatment. For the intensivist, there may be other immediately pressing priorities in the complex care of the patient, and a new neurologic problem is best solved quickly. Many of the neurology “curbsides” in the ICU are indeed simple phone calls to ask a simple question, but some questions should probably generate a formal consult. Consultants should generally and deliberately avoid a practice of mostly taking phone calls for curbsides, which are a set of quick questions that pertain to critical illness. These include interpretation of a CT scan of the brain, a question about electroencephalograph (EEG) interpretation, or the need for EEG monitoring. Other common questions are how to manage neurologic medication such as antiepileptic drugs, assess the risk of anticoagulation, or interpret specific neurologic manifestations of acute neurologic disease. It is often better to see the patient briefly and then determine if a formal consult can be helpful. The consulting neurologists will also have to consider the following questions. How can I best ask pointed questions? Am I able to provide advice with limited information and without having the opportunity to examine the patient in detail? Am I confident enough to dismiss or diagnose certain CT scan abnormalities? Does this clinical problem require a close follow-up and thus a formal consultation?
Acute (STAT) consults in the ICU are the most challenging in the hospital because (1) decisions may have to be made in an evolving situation; (2) the primary diagnosis may be unclear and puzzling; (3) neurologic examination can be compromised when patients are markedly swollen, jaundiced, immobile, bruised, or have major operation sites or an open chest; and (4) none of the neuroimaging and electrophysiology results may be particularly helpful. Any consulting neurologist will ask him- or herself the following additional questions: Are the neurologic findings commensurate with the cause and degree of critical illness? Are the focal findings significant or difficult to judge? How is neuroimaging or electrophysiology best interpreted in the setting of critical illness?2,8–10 Are there urgent treatment options or treatment adjustments that have not been considered? Will this neurologic manifestation set the patient back
Figure 1.1. Types of consultations.
permanently? Can I provide a reliable opinion on the future likelihood of full dependence for the patient, and could this opinion put an end to the aggressive, constantly escalating care?
BENEFITS OF A CONSULTATION
The need for broad knowledge of critical care could argue for a separate hospital service staffed by experienced neurohospitalists or neurointensivists. It goes to the heart of a longstanding academic and clinical question (and, in some centers, a charged debate): Who is best qualified to see these patients? Many of us are caught unaware by a variety of presentations, and as long as experience is gained, it is better gained by a specialized group. We have seen several conditions emerge more clearly as a result of covering all ICU consults with our neurocritical care services in both Mayoaffiliated hospitals.
Telemedicine could be ideal for these consults,11–16 but accurate metrics will need to be developed to show benefit. These could include (1) seizure control, (2) acute stroke care, (3) neurosurgical intervention, (4) control of intracranial pressure, and (5) limiting potent sedative drugs and avoiding drug-drug interactions. Ultimately, a full neurologic examination leads to new tests (EEG, somatosensory evoked potential [SSEP], CT scan, MRI, and CSF). All these tests are highly neurospecific, and recommendations of what to test or add to routine orders require good communication and, most importantly, accurate interpretation.
PRACTICAL ADVICE
• A major principle of consultation in the ICU is to see the patient immediately rather than paying a belated visit. A serious neurologic illness requiring immediate intervention might go unrecognized. Moreover, the entire clinical picture may be unclear and evolving, and neurologic expertise may point toward the right direction.
• Treatments may be inappropriate, incomplete, and incorrect. Errors happen easily eveninthebest-equipped,well-staffedICUs.
• Neurologists should appreciate the pharmacology of sedative drugs and use of analgesic drugs to provide a better assessment.
• Direct communication with the intensivist might provide a comprehensive clinical course and timeline of when events occurred.
• Direct communication with the surgeon on the surgical procedure and possible intraoperative events can decrease evaluation time and capture important intraoperative complications such as hypotension or even CPR.
• The circumstances surrounding critical illness could make the patient vulnerable to seizures. However, few patients in the ICU have seizures; many more undergo EEGs. Proportionality is necessary.
• A universal question is whether failure to wean from a ventilator is due to a previously unappreciated and undiagnosed neurologic disorder. Early diffuse weakness in ICU may be undiagnosed amyotrophic lateral sclerosis. Late diffuse weakness in ICU is often sepsis-related or critical illness–associated polyneuromyopathy.
REFERENCES
1. Wijdicks EFM. Why you may need a neurologist to see a comatose patient in the ICU. Crit Care. 2016 Jun 20;20(1):193.
2. Rabinstein AA. Continuous electroencephalography in the medical ICU. Neurocrit Care. Dec 2009;11(3):445–6. doi:10.1007/s12028-009-9260-6
3. Brown CH. Delirium in the cardiac surgical ICU. Curr Opin Anaesthesiol. Apr 2014;27(2):117–22. doi:10.1097/ACO.0000000000000061
4. Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. Apr 2004;291(14):1753–62. doi:10.1001/jama.291.14.1753
5. Hughes CG, Patel MB, Pandharipande PP. Pathophysiology of acute brain dysfunction: What’s the cause of all this confusion? Curr Opin Crit Care. Oct 2012;18(5):518–26. doi:10.1097/ MCC.0b013e328357effa
6. Pandharipande PP, Girard TD, Jackson JC, et al. Long-term cognitive impairment after critical illness. N Engl J Med. Oct 2013;369(14):1306–16. doi:10.1056/NEJMoa1301372
7. Mittal MK, Kashyap R, Herasevich V, Rabinstein AA, Wijdicks EF. Do patients in a medical or surgical ICU benefit from a neurologic consultation? Int J Neurosci. 2015;125(7):512–20. doi:10.3109/ 00207454.2014.950374
8. ClaassenJ,TacconeFS,HornP,etal.Recommendations on the use of EEG monitoring in critically ill patients: Consensus statement from the neurointensive care
section of the ESICM. Intensive Care Med. Aug 2013;39(8):1337–51. doi:10.1007/s00134-013-2938-4
9. Oddo M, Carrera E, Claassen J, Mayer SA, Hirsch LJ. Continuous electroencephalography in the medical intensivecareunit.CritCareMed.Jun2009;37(6):2051–6. doi:10.1097/CCM.0b013e3181a00604
10. Young GB. Continuous EEG monitoring in the ICU: Challenges and opportunities. Can J Neurol Sci. Aug 2009;36 Suppl 2:S89–91.
11. GuinemerC,BoekerM,FurstenauD,etal.Telemedicine in intensive care units: Scoping review. J Med Internet Res. Nov 2021;23(11):e32264. doi:10.2196/32264
12. Lilly CM, McLaughlin JM, Zhao H, et al. A multicenter study of ICU telemedicine reengineering of adult critical care. Chest. Mar 2014;145(3):500–507. doi:10.1378/chest.13-1973
13. Lilly CM, Zubrow MT, Kempner KM, et al. Critical care telemedicine: Evolution and state of the art. Crit Care Med. Nov 2014;42(11):2429–36. doi:10.1097/ CCM.0000000000000539
14. Weiss B, Paul N, Balzer F, Noritomi DT, Spies CD. Telemedicine in the intensive care unit: A vehicle to improve quality of care? J Crit Care. Feb 2021;61:241–6. doi:10.1016/j.jcrc.2020.09.036
15. Welsh C, Rincon T, Berman I, et al. TeleICU interdisciplinary teams. Crit Care Nurs Clin N Am. 2021;33:459–70.
16. O’Shea AM, Reisinger HS, Panos R, et al. Association of interactions between Tele-critical care and bedside with length of stay and mortality. J Telemed Telecare. 2022 Jun 29. doi: 10.1177/1357633X221107993
Chapter 2
Consulting in the Intensive Care Unit
PREPARATION AND HISTORY-TAKINGCOMMON REQUESTS FOR CONSULTS IN THE ICU
As implied earlier, consults in the intensive care unit (ICU) to evaluate and manage an acute neurologic clinical problem are in stark contrast to other requested hospital consults. As this book demonstrates, neurologic complications of critical illness are usually of considerable complexity.1–11 Even entering the ICU can make one feel unsettled, especially when patients have major trauma, open chest or abdominal wounds, multiple ongoing medical complications, and certainly when patients are connected to an extracorporeal membrane oxygenation machine. Some comatose patients are markedly swollen, jaundiced, and immobile. And then there is polypharmacy with many potent sedatives. In these situations, an adequate neurologic assessment may seem a worthless undertaking (Figure 2.1).
The clinical interpretation of a vexing neurologic problem in the ICU requires skill and full understanding of its immediacy. Before we dive into the nitty-gritty of neurological consultation in the medical and surgical ICU, this chapter paints the larger picture of what a neurologic consult in the ICU could entail.
PREPARATION AND HISTORY-TAKING
First and foremost, gathering essential information may be difficult, with some of this information hidden in not easily accessible drop-down menus on the patient’s monitor. In other cases, particularly in recently transferred patients with long ICU stays, information must be abstracted from an excessive number of notes of variable granularity.
The second step is to gain an understanding of the severity of the patient’s critical illness. Two main factors must be taken into consideration: history and recent clinical course. In the ICU, the history is often reconstructed from fragments of observations by the patient’s family, nursing observations, attending consultant notes, and, less often, from communication with the patient. Therefore, the patient’s history could be potentially inaccurate, seriously limiting a full assessment of neurologic complications. A simple matter-of-fact question such as “When were these signs first noted?” may be difficult to answer reliably. In such complex cases, direct communication with the
attending intensivist or surgeon is required and could decrease evaluation time substantially. As a rule, consultants evaluating patients with a postoperative complication also need to have a good understanding of the operative technique and surgical decisions (e.g., avoidance measures, anesthetic interventions). Consultants evaluating patients with neurologic manifestations of the CNS in the setting of a major medical illness must be aware of the patient’s prior hemodynamic instability, degree of organ dysfunction, coagulation status, and pharmacy regimen. For patients with generalized weakness, consultants must determine the patient’s prior use of neuromuscular blockers and intravenous corticosteroids and should be able to correctly interpret electrodiagnostic studies.
COMMON REQUESTS FOR CONSULTS IN THE ICU
Most consults are prompted by very specific neurologic signs that have been detected by the nursing staff or attending physician during rounds. Obviously, the threshold for consulting a neurologist is variable and depends on the
recognition of neurologic signs and the comfort level of some intensivists—less familiar with disorders of the nervous system—in handling these complications. In other circumstances, the patient’s failure to improve medically (e.g., inability to be liberated from the ventilator), acute coma, or failure to become fully coherent and alert over a matter of days after surgery may trigger a consultation.1,3,7 There may also be a convincing need to transfer the patient to a more specialized neurosciences ICU.
These situations are challenging for both the neurologist approaching the bedside and the intensivist trying to grasp the full clinical picture. The quality and amount of information available to the consulting neurologist can be disconcerting. The consult request may be summarized in only a few words (“new neurologic event,” “periodic twitching,” or “unresponsive”). Several consults are about pupil asymmetries (because the eyes are examined frequently), and most are not concerning. Another common but potentially urgent category is the patient with “altered mental status.” The term “altered mental status” has achieved classic standing, although not for its accuracy because it may mean anything. This category of neurologic deficits—patients who are agitated and less responsive—may
Figure 2.1. Critically ill 77-year-old man in a cardiovascular intensive care unit. The complexity of care (mechanical ventilation, dialysis, and multipharmacy) can seriously hinder the neurologic examination for consulting physicians.
appear less worrisome. Patients are confused and may not respond quickly, rarely fixate on objects, and cannot follow simple commands. Some can speak; others are unable to respond. We assume that, in most situations, these patients have an acute brain dysfunction from sepsis-associated encephalopathy, new-onset acute renal or liver failure, or a combination. Posterior reversible encephalopathy syndrome (PRES) is so prevalent that it is often listed at the top of the differential diagnosis and, if the circumstances are right, should be investigated with MRI. Unfortunately, for many years, neurologists had a tendency to describe any patient with an encephalopathy as having “multifactorial metabolic encephalopathy” and would list the abnormalities that make up the patient’s critical illness. None of this advanced an understanding of these complicated patients. More experience in examining and following these patients has resulted in better efforts to understand the true nature of acute brain dysfunction. One principle is to set apart the major driver of neurologic manifestations, but it is equally accepted now to consider other possible explanations such as structural injury.
Acute confusional state or delirium may trigger a consult, but many intensivists recognize this entity and treat it appropriately.3–6 Without a doubt, the most difficult situation is to assess a patient with decreased or increased arousal, abnormal perception, abnormal attention, and incoherent language. Within this category of patients are those with apraxia and aphasia (Chapter 3). Many ICU patients have agitated delirium or “sundowning” due to preexisting dementia or alcohol withdrawal. An unexplained observation is that delirium correlates with prolonged ICU stay (and increased mortality), but none of the clinical trials that have aggressively treated patients in delirium have shown an improved mortality rate.
There are some other urgent consults. Consults for new-onset seizures or new movement abnormalities are comparatively frequent. A new focal finding (e.g., hemiparesis or marked asymmetry) is less common. Consults are often for newly perceived asymmetries. It is a major challenge to recognize an acute stroke during a critical illness or after a major vascular procedure. Patients may have a delayed presentation or delayed recognition, particularly when anesthetic drugs have been used and are still washing out in the postoperative phase
of surgery. The challenge here is early recognition to allow an endovascular intervention because IV thrombolysis is contraindicated. Acute ischemic stroke may warrant endovascular treatment if the situation allows. (CT scan may already show a matured infarct.) Consults in surgical and trauma ICUs are often related to diagnostic evaluation of new spinal cord injury and traumatic brain injury, but in most instances, other specialties are involved (i.e., neurosurgery).
A special category is consultation for a transplant recipient. This may have already started before transplantation (e.g., fulminant hepatic failure) because the attending intensivist or surgeon values the presence of a neurologist. Another special category is the patient admitted with a left ventricular assist device (LVAD) and new neurologic symptoms. Discussions on discontinuing or improving anticoagulation often involve a neurologist.
In the surgical ICU, consults may involve the sudden appearance of paraplegia after awakening from anesthesia. Acute spinal cord infarction might indicate immediate placement of a lumbar drain to reduce CSF spinal pressure and improve residual spinal blood flow. In each of these scenarios, prompt decisions are warranted and can improve outcome if proper measures are taken. Urgent consultation for a possible complication of carotid artery surgery involves assessment for possible ischemic stroke or management of blood pressure and heart rate instability. (The latter is mostly managed by a neurointensivist, but a general neurologist should be aware of this major complication involving damage to the baroreceptors.)
Generalized weakness in the ICU is very common and nearly always prompts a neurologic consult. Most neurologists expect (and diagnose) critical illness polyneuropathy, critical illness myopathy, or both. One could argue that, in fact, this myopathy is the most common cause of weakness in the ICU. The prevalence of ICU-acquired weakness is high in survivors of critical illness and will increase as more patients survive multiorgan failure, sepsis, and other fulminant infections. Failure to wean off the ventilator (or unexplained reintubations) is another trigger for a comprehensive neurologic assessment, and a neurologic disorder other than critical illness polyneuropathy may be found. Finally, consults may involve an explanation of neuroimaging findings or the
interpretation of an ordered electroencephalograph (EEG) in a patient with an undefined repetitive movement).
Failure to awaken or prolonged unconsciousness is a very common consult, and requests may be vague and not immediately alarming (“altered mental status”). Such a consult needs an immediate response; the neurologist must see and examine the patient.
Several issues are pertinent. (More details on examination and classification are found in Chapter 4.)
First, a patient’s failure to awaken after urgent cardiovascular repair is an ominous sign. A devastating ischemic stroke involving multiple arterial territories is a frequent cause of failure to awaken.7 Its mechanism may be hypotension or multiple emboli. Hypotension can be implicated only if it persists for a considerable period. In addition to perioperative hypotension and cardiac resuscitation during surgery, multiple embolic events are possible reasons for multiple cerebral infarctions. In some patients, the surgical approach and anesthetic support were without obvious distress to the patient, and the cause for multiple cerebral infarctions may remain unresolved. However, the risk of embolization is significant for patients with severe atherosclerotic disease of the ascending aorta, and embolization almost certainly occurs at the time of clamping.
Second, evaluation of impaired consciousness in patients requiring intensive care for acute medical illness starts with a series of important questions (Table 2.1). The answers could narrow down the list of causes of impaired consciousness by a simple process of elimination.
Because triggers such as hypotension and coagulopathies are common, neurologists shouldfocusonfindingstructuralcausesevenifa
pharmacologic cause of coma is likely. Therefore, after location is determined, neuroimaging follows, and the combination of clinical and neuroimaging results can lead to specific actions. CT of the brain (or CT angiogram in cases suggesting an embolus to a major cerebral artery) is a mandatory diagnostic test and currently has an acquisition time of less than 10 min. A CT can document generalized cerebral edema, cerebral hemorrhage, and ischemic stroke with swelling, but its diagnostic yield is low for anoxic–ischemic brain injury and in the period early after traumatic head injury. If structural damage is present, it should be correlated to the depth of coma.
A significant shift of the midline structures (septum pellucidum, calcified pineal gland) due to a new mass, hydrocephalus, or intraventricular hemorrhage must be recognized in patients with rapidly deepening coma.
A normal CT scan in a patient with a metabolic derangement or organ dysfunction does not exclude a structural cause and, if feasible, should be followed by MRI. Causes of coma in patients with initially normal CT results are presented in Table 2.2 for easy reference.
MRI has come to the fore as a diagnostic tool in ICUs, and if anesthesia support is available, it may be used to identify or exclude structural damage for comatose patients. However, transport to the MRI suite takes the critically ill patient out of the critical care environment, and, once there, necessary support (vasopressors, mechanical ventilator) is inadequate and, in some instances, can jeopardize the patient’s safety. In our experience, fewer than half of comatose patients can be transported to the MRI suite without difficulties. Therefore, the yield of abnormalities and consequences for management should be high before ordering an MRI.
Table 2.1 Questions to family members and nursing staff concerning patients in the intensive care unit with impaired consciousness
Family Nursing staff or attending consultant
• Illicit drug use?
• Alcohol abuse?
• Circumstance in which patient was found (apneic, cyanotic, seizing)?
• Prior illness or constitutional symptoms?
• Recent medication adjustments or newly started drugs?
• Prior, comorbid conditions?
• Intraoperative cardiopulmonary resuscitation?
• Intraoperative hypotension?
• Presence of asymptomatic interval after surgery?
• Hypotension requiring vasopressors?
• Hypoxemia requiring high level of positive end-expiratory pressure?
• Myoclonus, eye deviation, eyelid blinking?
Table 2.2
Probable causes of coma in critically ill patients with normal initial CT findings
Anoxic–ischemic encephalopathy
Drug overdose
Neurotoxicity from chemotherapeutic agents or immunosuppressive agents
Diffuse axonal brain injury
Acute central nervous system infection
Fat embolization
Acute basilar artery occlusion
Cholesterol embolization
Central pontine myelinolysis
Diffuse intravascular coagulation
Thrombotic thrombocytopenic purpura
Central nervous system vasculitis
Prolonged hypoglycemia
Acute severe hyponatremia
Acute severe hypercalcemia
Acute nonketotic hyperglycemia
Metabolic acidosis
Acute hypercapnia with hypoxemia
Adrenal crisis
Acute hypothyroidism
Acute hyperthyroidism
Acute uremia
Acute hyperammonemia
Recent laboratory values should be obtained, and the medical records should be scrutinized for trends. CSF examination is needed when meningitis is suspected and should be considered in critically ill patients with spinal anesthesia, traumatic brain injury, trauma, and evidence of paranasal sinusitis.
The role of EEG, including its place in the detection of nonconvulsive status epilepticus, is discussed in other chapters, but all too often, only dysrhythmic slowing and triphasic waves are seen.7 Except for documentation of subtle seizures, EEG has generally lost its practical value in these situations, relinquishing usefulness to neuroimaging, particularly diffusionweighted MRI. Whether nonconvulsive status epilepticus is underdiagnosed in critically ill patients remains debatable, and we have documented only a few verifiable instances of nonconvulsive status epilepticus in the medical or surgical ICU over the past decades.
Third, another reason for consultation is a request to explain failure of patients to awaken after discontinuation of sedation, and this may, despite everything, be a common cause of impaired consciousness. A prolonged, lingering
Table 2.3 Information gathering for a critically ill patient with impaired consciousness and prior use of sedation
• Chart drugs, doses, and serum levels (if available)
• Review drug toxicology screen, serum-urine (if available)
• Assess factors that delay washout of drugs (e.g., liver or kidney function)
• Assess and reconstruct any plausible pharmacodynamic and pharmacokinetic effects; calculate 5 × half-life period
sedative effect is an obvious consideration but could be difficult to quantify, let alone prove (Table 2.3). Reconstruction of the pharmacodynamics and pharmacokinetics is useful. Often alkalosis, drug interactions, and large doses of sedative drugs change elimination to zero-order kinetics, which directly contributes to prolonged sedation (Chapter 2). Drug levels should be measured if possible. For any drug, the consultant should obtain the metabolic half-life and calculate the time remaining to clearance, assuming full elimination. Patients who do not fully awaken after withdrawal of sedatives, narcotic agents, or combinations of these agents are frequently jaundiced and often have recently been given a benzodiazepine (midazolam) or a narcotic drug (fentanyl). Both drugs are designed to clear through the liver and therefore may accumulate. Prolonged sedation occurs after many days of accumulated metabolites, and further observation over time may be required.
Fourth, consults are requested for patients who become acutely comatose while they are critically ill, and these patients commonly have a catastrophic neurologic illness. A large proportion of patients in our experience have a devastating intracerebral hematoma or subarachnoid hemorrhage. These disorders, which may be the inaugural presentation, typically occur in patientswithsystemicfungemia,coagulopathies, or a ruptured mycotic aneurysm from endocarditis. Acute basilar artery occlusion due to an emboluscancomplicatedissectionofthethoracic aorta, valve repair, and cardiac transplantation. Rapidly deepening loss of consciousness in patients with multiple traumatic injuries should point to fat embolization, evolving epidural or
subdural hematoma, or enlarging hemorrhagic contusions with mass effect and edema. Acute coma can occur after correction of hyponatremia, cardiac resuscitation, and carbon monoxide poisoning, all of which are manifestations of extensive demyelination of both hemispheres. Typically, patients who seem to be doing very well suddenly and unexpectedly lapse into a deep coma and succumb.
If failure to awaken occurs after traumatic brain injury and the patient has been admitted directly to the operating room from the emergency department, intracranial contusion or extraparenchymal hematoma should be considered. Patients taken directly to the operating room with life-threatening, blunt abdominal trauma may have additional head injury, subdural hematoma, or epidural hematoma that was not apparent on initial examination. A unilateral, fixed pupil may suddenly occur during surgical repair of a vascular injury or abdominal exploration for trauma. (Pupillary light reflexes are the only brainstem reflexes that can be monitored during general anesthesia.) Extraparenchymal hematomas may become evident on CT after 24 hr.
Acute electrolyte imbalance is a relatively frequent cause of postoperative confusion, progressive drowsiness, or coma. Increased levels of antidiuretic hormone associated with decreased serum osmolality and hyperosmolar urine are typical during the first few postoperative days. When hypotonic fluids are used, renal handling of free water is impaired because renal function decreases after the use of inhalational anesthetics, barbiturates, and opioids. Hyponatremia can occur rapidly and typically results in seizures, apnea, and cardiac arrhythmias, often at sodium levels below 110 mEq/L. Other common causes of acute postoperative hyponatremia are administration of large doses of hypotonic fluids to patients with impaired ability to excrete water after transurethral prostatectomy and administration of oxytocin to patients during obstetric procedures.
Fifth, failure to awaken after transplantation requires a separate discussion. Neurologic complications in the early postoperative phase of cardiac transplantation have decreased in recent years. Much of the decrease is due to meticulous attention to removing all residual atrial tissues or thrombi. Also, the use of a more precise everting anastomosis may have
decreased intracardiac thrombus formation on the suture interface and thereby the resultant massive embolic showers and cerebral infarctions. Therefore, impaired consciousness after heart transplantation is infrequently due to a structural lesion in the CNS. Without localizing neurologic findings, the most common cause of unresponsiveness is drug-induced coma. Narcotic agents are often used liberally in cardiac transplant recipients to decrease pain and overcome postoperative hypertension. These agents (usually morphine and fentanyl) may cause significant postoperative sedation. Typically, high doses of narcotic agents are given intraoperatively such as fentanyl (with diazepam) or sufentanil (with lorazepam). Naloxone (0.04–0.08 mg) reverses the effects of narcotic agents. However, failure to awaken may originate with the marked hypotension that occurs intraoperatively, with episodes of significant hypoxemia, or more often, with cardiac resuscitation for asystole or ventricular fibrillation. Cardiac arrest can occur in the immediate postoperative phase and can be devastating.Inthesepatients,themostcommon clinical problems associated with perioperative cardiac arrest are hypovolemia, tamponade, and overdose of potent vasodilators.
Neurologic evaluation in the first several days after a lung transplant is difficult because most patients are sedated, paralyzed, and mechanically ventilated. Some programs dictate continuing mechanical ventilation to decrease stress on the critical tracheal anastomosis, but most patients are rapidly weaned within 36 hr. Pulmonary hemorrhage and infection may dominate the early postoperative course. Impaired consciousness, therefore, may reflect the hypoxemia associated with pulmonary edema from reperfusion injury to the graft.
Impaired consciousness and acute confusional state occur in a large proportion of patients with liver transplantation. Many metabolic abnormalities are present, but none significantly contributes to the diminished alertness of the patients. With a new functioning liver, the level of alertness should improve rapidly.
Patients with fulminant hepatic failure are prone to increased intracranial pressure because of brain edema, and liver transplantation is their only hope for survival. Return of consciousness to baseline level takes days, and these patients typically have more prolonged
awakening in the postoperative phase. In addition, the use of barbiturates perioperatively to control increased intracranial pressure may contribute substantially to postoperative altered consciousness.
Treatment of comatose patients involves management of increased intracranial pressure, neurosurgical evacuation of a new mass, treatment of seizures, and correction of laboratory abnormalities. Patients who remain comatose need careful examination to determine the chances of awakening and to prognosticate later disability if they improve. Supportive care can be provided if prognosis is uncertain and should include placement of a tracheostomy and percutaneous gastrostomy, meticulous skin and eye care, and physiotherapy measures to prevent contractions. A comprehensive discussion on care can be found in another text.5
Finally, another common issue is whether the patient has an undiagnosed neurologic disease of the peripheral nervous system. Acute exacerbation of chronic obstructive pulmonary disease often leads to mechanical ventilation and, frequently, a tracheostomy, and these patients, if not already in a poor nutritional state before admission, will have an emaciated appearance. It is therefore not unthinkable that the
combination of CO2 retention before endotracheal intubation, difficulty with liberating from the ventilator, and abnormal pulmonary function tests (inspiratory and expiratory pressures) points toward a neuromuscular disorder. Clinical distinction between a myopathy, a polyneuropathy, or a neuromuscular disorder is difficult if all four limbs are flaccid and other signs are lacking.
Electrodiagnostic testing is often a part of the evaluation, but interpretation requires expertise, and muscle or nerve biopsy may bring a more definitive classification. Quantitative analysis of motor unit potentials, which requires cooperation by the patient, may be difficult in very weak, confused, and agitated patients. At least three motor nerves (distal latency, amplitude, and conduction velocity) and three sensory nerves (amplitude and conduction velocity) should be studied and followed by needle insertion in multiple muscles. The most common electrophysiologic abnormalities are listed in Table 2.4, and more details on the differential diagnosis can be found in Chapter 7.
Phrenic nerve stimulation in a patient with diffuse muscle weakness strongly points to a critical illness polyneuropathy if both sides are abnormal.6 Abnormal blink reflexes are found
Table 2.4 Electrophysiological features of major neuromuscular disorders associated with critical illness
DisorderNCV and EMG findingsSpecial considerations
Critical illness myopathy
Critical illness polyneuropathy
Myasthenia gravis or prolonged NMBA effect
Acute polyradiculopathy (GBS or CIDP)
Reduced CMAP amplitude, short duration, early recruitment
Reduced CMAP amplitude, decremental response with 3-Hz repetitive stimulation
Prolonged distal latency, reduced motor velocities, conduction block
Motor neuron diseasePolyphasic waveforms with late components, poor recruitment, widespread fibrillation potentials, normal SNAP
Lack of direct stimulation of muscle may be diagnostic
Reduced sensory potentials may be due to ankle edema or underlying systemic illness, such as diabetes mellitus; phrenic nerve stimulation abnormalities are diagnostic
Higher diagnostic yield with proximal muscles than with distal muscles, higher yield with facial stimulator
Absence of blink responses and prolonged F-wave latency may be diagnostic
Typical asymmetrical distributions, early abnormal phrenic nerve CMAP and diaphragm denervation