Visit to download the full and correct content document: https://ebookmass.com/product/quantum-leadershipbuilding-better-partnerships-for-s ustainable-health-ebook-pdf-version/
More products digital (pdf, epub, mobi) instant download maybe you interests ...
Community Policing: Partnerships for Problem Solving 8th Edition – Ebook PDF Version
https://ebookmass.com/product/community-policing-partnershipsfor-problem-solving-8th-edition-ebook-pdf-version/ Public Health Leadership 3rd Edition, (Ebook PDF)
https://ebookmass.com/product/public-health-leadership-3rdedition-ebook-pdf/
Quantum Computation and Quantum Information: 10th Anniversary Edition – Ebook PDF Version
https://ebookmass.com/product/quantum-computation-and-quantuminformation-10th-anniversary-edition-ebook-pdf-version/
Introduction to 80×86 Assembly Language and Computer Architecture – Ebook PDF Version
https://ebookmass.com/product/introduction-to-8086-assemblylanguage-and-computer-architecture-ebook-pdf-version/
Quantum Leadership:Creating Sustainable Value in Health Care 5th Edition
https://ebookmass.com/product/quantum-leadershipcreatingsustainable-value-in-health-care-5th-edition/
Medical Terminology for Health Professions, Spiral bound Version – Ebook PDF Version
https://ebookmass.com/product/medical-terminology-for-healthprofessions-spiral-bound-version-ebook-pdf-version/
Community Policing: Partnerships for Problem Solving 8th Edition, (Ebook PDF)
https://ebookmass.com/product/community-policing-partnershipsfor-problem-solving-8th-edition-ebook-pdf/
The Healing of America: A Global Quest for Better, Cheaper, and Fairer Health Care (Ebook PDF)
https://ebookmass.com/product/the-healing-of-america-a-globalquest-for-better-cheaper-and-fairer-health-care-ebook-pdf/
Mental Health Services: A Public Health Perspective –Ebook PDF Version
https://ebookmass.com/product/mental-health-services-a-publichealth-perspective-ebook-pdf-version/
Principle 7:Systems Thrive When Allof Their Functions Intersect and Interact
Principle 8:Equilibrium and Disequilibrium Are in Constant Tension
Principle 9:Change Is Generated from the Center Outward
Principle 10:Revolution Results from the Aggregation of LocalChanges
Conclusion
ChapterThree
Chapter Objectives
EvidentiaryLeadership:AnExpandedLens to DetermineHealthcareValue
Key Drivers for Change
AVery ComplexSystem
New Healthcare Valuation Model
Conclusion
ChapterFour Chapter Objectives
Innovationas aWayofLife:LeadingThrough theWhiteWaterofChange Drivingthe Culture of Innovation
Equity
DecisionalStructures
Drivingfrom the Point of Service
Alignment, Not Motivation
CreatingStakeholder Value
The ContextualRole of the Board
The C-Suite and the Context for Innovation
First-Line Leaders:The Pivot Point of Innovation
Creatinga Context That Supports the Innovator
Innovation and the Membership Community
BalancingInnovation with Value
DifferentiatingRoles in Innovation
Leadership and the Willto Innovate
Conclusion
ChapterFive InnovationLeadership Chapter Objectives
Rationale for Healthcare Innovation
Definitions and Concepts
Innovation and the Quantum Leader
Strategies to Integrate and Advance Innovation
Innovation LabelVersus Innovation Role
Conclusion
ChapterSix
Chapter Objectives
Growth and Transformation
AvoidingUnnecessary Conflict
Team-Based Conflict Issues
Identity-Based Conflict
Interest-Based Conflict
People and Behavior
Conclusion
ChapterSeven
Chapter Objectives
Normative Crisis
Early Warning
Conflict in the Human Community
The Human Resources Focus
Chaos, Complexity, and Crisis
Dynamic Cybernetic Team Model(DCTM)
Cybernetic and InteractingEnvironmentalScanningProcess
Crisis Preparedness
Conclusion
ChapterEight Chapter Objectives
Leadership Fitness in the New Millennium
Vulnerability
Power
The Cycle of Vulnerability
New Relationships
Complexity Communication
Collective Mindfulness
Strategies for CultivatingLeadership Vulnerability
Is There a Choice?
Conclusion
ChapterNine HealingBrokenness:Erroras Opportunity Chapter Objectives
Error in General
Errors in Healthcare Service
Transforminga Punitive Culture
Healthcare Leadership:Errors and Opportunities
Conclusion
ChapterTen
Chapter Objectives
Underpinnings of EmotionalCompetence
Nature of EmotionalCompetence
EmotionalRisks of Leadership
Benefits of EmotionalCompetence in Health Care
DevelopingEmotionalCompetence
Emotionally Incompetent Behaviors
Team EmotionalCompetence
Connectingwith Generations of Workers
MeasuringEmotionalCompetence
Conclusion
ChapterEleven ToxicOrganizations andPeople:TheLeaderas Transformer
Chapter Objectives
HealingIs Our Business?
Toxic Behaviors
Ten Principles for MinimizingToxic Behavior in Organizations
Conclusion
ChapterTwelve CoachingforUnendingChange:Transforming theMembershipCommunity
Chapter Objectives
From Responsibility to Accountability
TransformingWork and the TransformingWorker
Evolution and Revolution
The LearningOrganization
Organizingfor Transformation
Dealingwith the Lack of Time
The Leader as Revolutionary
Innovation Coaching
MakingIntegration Work
AddressingProblems Head On
EliminatingFirefightingAltogether
Conclusion
Chapter Thirteen TheLeader’s CouragetoBeWilling:Buildinga ContextforHope
Chapter Objectives
AContext for Hope
Will
Strategies to Facilitate Willingness
Relightingthe Lamp
Conclusion
Chapter Fourteen SustainingtheSpiritofLeadership:Becominga LivingLeader
Chapter Objectives
Chaos and the Callto Leadership
Self-Management and Creativity
Creativity and Innovation
Exercisingthe Spirit
SpiritualIntelligence:Ten Rules of the Road
BecomingSelf
Listeningfor the Sounds of Change
FindingSpirit in the Chaos
The Compensations of Ignorance
Mystery
Synthesis and Synergy
Index
DEDICATION WededicatethisbooktoCathleenKrueger Wilson,PhD,RN,nurse,therapist, consultant,colleague,andfriend,whofirstconceivedthepossibilityofthiskindof bookonleadership.Her creativityandimaginationinapplyingleadershiptoall venues ofhealthservicewereaninspirationandajoytoall whoknew her.Cathleenwasarole model asnurse,mother,spouse,andfriendandbroughtthefull weightandenergyofher persontoher workandrelationships.Indeath,asinlife,shestill servestostimulate andencouragethebestinall whoselivesshetouched.
PREFACE Writingabookonleadershipinatimeofhealthcaretransformationisalmostafutile exercise notthatwritinganybookisn’tdifficult.Buildingonthepreviousthree editionsofthistextandupdatingcontentremindusofboththedegreeandthepaceof changingknowledgeandinsightonleadershipaswemovedeeper intoacomplexitygroundeddigital age.Becauseofour dedicationtoensuringthatthemostcurrentand relevantinformationiscontainedinthistext,wehavecommittedtoupdatingitscontents every2years.Thepeculiarityofbooksonleadershipisthattheycannever betruly finished.Leadershipisessentiallyaworkinprogress anever-endingjourneywith facetsandelementsthatadduptoabroadandcomplexmosaic.Embeddedinthe leadershiproleisahostofbehavioral,relational,interactional,andstructural considerationsthatgiveformtotheactivityofleading.Researchineachoftheseareas couldlinetheshelvesoflibrariesfor generations.Wesubmitthatnoonepersoncould comprehendall thathasbeensaidandwrittenaboutleadershipor all theactionsthat havebeendoneinitsname.
Furthermore,astheworldchanges,new notionsofhow toadvancetheworkof organizationsandpeopleemerge,new patternsofbehavior develop,andthesedemand somelevel ofexplicationandunderstanding.Infact,justlikeother segmentsofsociety, healthcareisgoingthroughthedramaandtraumaofreconceptualizingitsworkand prioritiestotakeintoaccountthenew global reality,real healthreform,value-driven caremodels,andthemostrecentadvancesintherapeuticsandclinical technology. Theseadvancesarealreadybearingfruitandradicallyalteringboththequantityand qualityoflife.Andthechangesyettocomewill haveanevengreater impactthandid thosethathavealreadyoccurred.Wehopethisfourtheditionhaskeptupwiththe changesandreflectsthebestthinkingonthestateoftheartofcontemporaryleadership.
Anexampleofthisistheever-increasingdigitalizationandmobilityofhealth services,creatinganeedtoreconfiguretheseservicesandchangetherelationship betweenprovidersandthosetheyserve.Accountabilityfor choiceandproper action arecomingtorestmoreinthehandsofthe“users,”andhealthcareleadershavethe importantjobofenablingproviderstoalter their practicesaccordinglyandtoprepare theseuserstoassumetheaccountabilitythatisbeingtransferredlegitimatelytothem. Furthermore,technologyismakingitnotonlypossiblebutnecessarytobuildevidence thatclinical workistrulymakingadifferenceinthelivesofthoseweserveandinthe healthofour communities.
Aleadershipbooklikethisoneservesasadynamicsnapshot,ifyouwill,ofthe
leadershiproleataparticular momentintime.Inour attempttoidentifyanddescribe thecorrectbehaviorsandstrategiesfor therole,wefocusontheissuesthataremost representativeofthecurrentera.Oneoftheearmarksofour era,ofcourse,isthe acceleratingrateofchangeinthesubstantivereformattingofthedeliveryofhealthcare. Another istheobviouschallengesofensuringaccess,availability,andpaymentfor healthcarefor all Americans.All oftheseissuesprovideuniqueopportunitiesfor the effectiveexerciseofcontemporaryleadership.
Healthcareleadersmustpushtheir organizationsintothisfray.Theymustbeable notonlytoseeintothedarknessofthefuturebutalsotolivecomfortablyinsidethe potential thatrisky,unsettledspacebetweenthepresentandthefuture.Andbecause leaderscannotpull peopleintoafuturethatonlytheyhaveconceivedof,theymustbring everyonetothetabletoshapethefuturethroughcollectivedialogueandconcerted action.
Inthisfourthedition,wetrytoconceptualizethenewer complexity-basedrealities inhealthcareandusetheemergingfoundationsasatemplatetoprioritizeleadership skillsandbehaviors thoseskillsandbehaviorsthatleadersneedtousetoensurethat their organizationsareguidedaccuratelyandeffectively.Our strategyisfirsttoprovide aglimpseintothefutureandthentopresentsomeoftheimplicationsofthematuring sciencesofcomplexityandchaos,therebydelineatingthecontextoftheleadershiprole attheoutsetofthisnew centuryasleadersworktomakesenseofthiscontinuously emergentsociotechnical world.
Anticipatingchangerequirestheabilitytopredictandadapttotransformationand thecrisisthatbothstimulatesitandrepresentstheappropriateresponse.Leadersmust now recognizetheever-constantcompanyoftheserendipitousandtheunplanned occurrencesthatarereflectedinafast-pacedandhighlychangingenvironment.Leaders mustmodel andinculcateapredictiveandadaptivecapacityintothelifeoftheir organizationsandintotheskillsofthestaffateveryplaceintheorganization.Thereis simplynowaythatreformingandadvancinghealthcarecanunfoldwithoutagreatdeal ofconflict.Mostpeopleassumethatconflictintheworkplaceisbadandshouldbe avoided.Nothingcouldbefurther fromthetruth.Conflictisanormal elementofall interaction.Leadersmustunderstandthisandacquirethenecessaryskillstomanage conflictinawaythatyieldsthebenefitsthatitiscapableofdelivering.Byhandling conflictappropriately,leadersalsoarebetter positionedtocreateahealingenvironment for providersaswell asconsumersofhealthcareandtoundertakethehealingofawide varietyofemotional andspiritual injuriessufferedbypeopleastheystrugglewiththe workoftransformingthehealthcaresystem.Buildingahealthyenvironmentbybeing fullypresentanddemonstratingcompassionandaccountabilityisafundamental responsibilityofthecontemporaryleader.
Notonlyisitnecessarytohandleconflicteffectively,itisnecessarytosee organizationsasbeinginconstantfluxandsubjecttocontinuouschange.Leadersnow mustbothpredictandadapttothepatternsofchangethataffecttheir peopleandtheir organizations.Thisadaptiveandpredictivecapacityisnolonger anoptionfor good leadersiftheir organizationsaregoingtocontinuetothriveandchangeasnew conditionsandtechnologydemand.Developingtheseinsightsandtheskill ofpredictive andadaptivecapacityprovidesagoodskill foundationtoensuretheorganizationsofthe futurecontinuetochangeandsustainthemselves.
Over thepreviousdecade,ahostofauthorsandresearchersremindedusthat leadersmustpossessnotjustintellectual abilitybutalsoemotional competence.After all,establishingandmaintainingrelationshipsareessential partsofleadership,andall relationshipshaveanemotional component.Toensurethattheir relationshipsexhibit emotional maturity,leadersneedtounderstandthenatureofemotional competenceand thustouchtheemotional center inthemselvesandothers.Thevalueofemotional maturityfor leadershipisjustbeginningtobeunderstood.
Behavior doesnotexistinavacuum,andthusthecontextwithinwhichpeople interactandworktogether requiresasmuchconsiderationaswhattheydo.The enormouschangesthatareoccurring,someofthemverytraumatic,causepeopletosee themselvesawashinaseaofmovementthatdoesnotmakemuchsense.Staffmembers oftenfail tounderstandthedirectioninwhichtheir leadersaretakingthemandbeginto losehopeandanysensethattheir workismeaningful.Leaders,intheir actions,needto providethefoundationsfor hopeandmeaningandvalue.Theymustfirstfindthese thingsfor themselvesandthentranslatethemintoalanguagethatotherscancomprehend andown.
Whyaresomeleadersmoresuccessful thanothersatleadinganorganizationthrough transformational change?Whydosomecreateanenvironmentofhopeandcalmdespite difficultor evendesperatecircumstances?Theanswerscanbefoundinthenotionof personal willingness.Willingleadersaretheco-creatorsofchange.Theyrecognizethat noonepersonor situationcantakeawaytheir personal peace,joy,or senseof competence.Theytransmitthesefeelingstoothersinawaythatencouragesandenables themtoembracethenew scriptandshareinthewritingofit.
Whether welikeitor notwenow liveinavalue-drivenage.Asprofessionals,itis becomingincreasinglyimportanttobuildanevidentiaryfoundationthatprovidesaclear demonstrationoftherelationshipbetweentheprocessesandtheimpactofour work.For toolong,thefocusofprofessional workhasbeenontheworkitself: thequalityofthat work,thecontentofthework,andhow well theworkwasdone.Increasingly,the challengesbetweenappropriateresourceuseandtheoutcomesofclinical workhave raisedthespecter ofincongruityandour oftenfrequentfailuretoadvancethehealth
statusofthoseweserve.Valuenow callsfor healthprofessionalstomakeastrongcase for practiceandestablishafirmfoundationthatdemonstratesagoodnessoffitbetween theactionofclinical practiceandtheimpactofadvancingsocial health.Andnow,this mustbedonewithinthecontextofequity-basedprovider teamscommittedtoadvancing thehealthofthosetheyserve.Evidentiarydynamicsisnow afundamental subsetofboth leadershipandclinical work.Improvementsciencesandvalue-basedpracticesand paymentnow requirebothtechnological andpracticeframesthatelicitbestpractices andadvancetheuser experience.Ultimately,leadershaveanobligationtoensurethat thereisatightrelationshipbetweentheaggregatednethealthstatusofthecommunity andtheresourcesusedtoobtainandsustainit.
Inthecontemporarycontextfor healthcare,acapacityfor innovationisnolonger optional.Everyleader now mustoperatewithinaninnovationmental model.Leaders now needtodemonstrateanavailabilitytotheinventiveandthecreativesomuchapart ofour fast-pacedsociotechnical existence.Innovationismorethanaprocess.Itis increasinglyevidentthatthereisasciencethatdrivesit.Aswebecomemoreawareof theactionofcomplexityanditsconsonancewiththemovementofsystems,theroleof theemergentandtransformational substrateofexistencebecomesmoredefinitive.Itis theroleofaleader tocreatebothcontextandconditionsthatharnessthisenergyand facilitatethediscourse,discovery,andapplicationofthisknowledgeinadvancingthe qualityoflifeandour humanexperience.Creatingthecontextfor thedynamicsof innovationisnow acentral roleofleadershipcapacityandisessential totheabilityto besustainedandtothrive.
Coachingpeopleintothefuturetheymustliveinrequiresspecial skills.Unlikein thepast,leaderscannotsimplyforcepeopleintoamoldor intocompliancewith demandsthattheyplayednopartinsetting.Allowingpeopletobeinvestors,partners, andstakeholdersintheir ownprocessesisatalentnecessaryinthenew leader.Leading workersoutofatoxicandperenniallysickor stuckworkenvironmentisapartofthis process.Itrequirestheleader tounderstandthecharacteristicsofneuroticand pathological organizationsandthosebehaviorsthatpreventpeopleandtheir organizationsfromembracingthechangestheymustadapttoinorder tothriveinthe new worldofhealthcare.
Finally,leadersmustfocusontheenergyandspiritwithintobeinnovativeandgrow andtherebyactasmodelsfor othersintheir ownsearchfor meaningandvalueinwhat theydo.Buttheabilitytoexhibitcreativity,self-understanding,andpersonal growthis notobtainedaccidentallyor withouteffort;itrequiresregular mental andspiritual exercise,includingperiodsofreflection,torefineit.Inthefuture,leaders,tosustain their effectivenessintheleadershiprole,will needtoengageinreflectivepersonal workandincreasetheir level ofcreativity.
Likeothersofitskind,thisbookisalwaysaworkinprogress.Itisnecessarilyand forever incomplete.Thereisalreadyahostofgoodbooksoncontemporaryleadership, withmorearrivingonthebookshelveseveryday.Theytooareincomplete.What individualswhowanttolearnaboutleadershipmustdoisseethemyriadavailable resourcesonthetopicasmakingupasingledynamicandgrowingbodyofknowledge. Thus,iftheywanttoimprovetheir leadershipskills,theyshouldusethisbookasone resourcealongwithothers,understandingatthesametimethatthetheoriesof leadershipandtheir applicationwill advanceasmoreinformationbecomesavailable.
Wehopethatthecontentsofthisfourtheditionof Quantum Leadership stimulate reflectionanddiscussion.Webelievethatthisbookextrapolates,inadefensible manner,fromcurrentresearchandpracticesnewer waysofconceivingandexercising theleadershiprole.Atthistime,leadersarechallengedtotakethenextstepinthe journeytowardbetter andmorerelevantmethodsofleadership.Thosewhoselivesthey affecthavearighttoexpectthebestthattheleadershavetooffer,especiallyasmoreis demandedofprofessionalsthanever before.Wehopethisfourtheditionplayssome small roleinensuringthatthosewhoprovidehealthcareservicesgetfromtheir leaders whattheyhaveeveryrighttoexpectandasaresultthehealthofour nationisadvanced.
TimPorter-O’GradyandKathyMalloch ACKNOWLEDGMENTS Wewishtoacknowledgeandthankour leadershipcolleagueJaynelleStichler,DNSc, RN,FAAN,for her excellentcontributionofchapter-basedcasestudiesfor eachofthe topical chaptersinthistext.Dr.Stichler servesasanexemplar ofnursingleadership andleadershippracticeexcellence,asclearlydemonstratedinthequalityofcases containedinthistext.
Thisfourtheditionof Quantum Leadership couldnothavebeencompletedwithoutthe supportofagoodnumber ofpeople.First,Ithankmycoauthor,KathyMalloch,who committedfull timeandenergytothisbookandwhosecollaborationcontinually encouragesme.Ialsoacknowledgethemanycolleaguesinnursingandhealthcarewho wereboththesubjectsourceandthemotivationfor thisbookandhavemuchtodowith itscontent.Their encouragementkeptusfocusedonwritingatextthatisbothrelevant anduseful.Finally,IthankMarkPonder,RN,for his38yearsofsupportand partnership,andfor beingasigntomethatcaring,loving,andnursinghavenothingto dowithgender.
TimPorter-O’Grady
Thefourtheditionof Quantum Leadership istheresultofinsightsgarneredfromour manydedicatedreaders,andfor thiswearegrateful.Weacknowledgeandthankour colleaguesfor their undyingdedicationtolifelonglearningsotheycaninfluenceand empower otherstobethebesttheycanbe.
Thankyou,Tim,for your friendshipandunquestionablesupport youareonevery special person: aleader,ahealer,athinker,avisionary,andagreatcolleague.Finally, mygreatestthanksandrecognitiongotomyhusband,Bryan“Mallotchi,”myverybest friendandconfidant,alwaysencouragingmeandtoleratingmyinconsistencies.Without hisunconditional support,myworkasaleadershipadvocateandhealer wouldnotbe nearlyasmeaningful.
KathyMalloch
CASESTUDYINSTRUCTIONS Theuseofcasestudiesineducationprovidesarichopportunityfor studentstoemploy situatedcognitionintheapplicationofnew knowledgewhenanalyzingthecase situationsinalowstakesenvironment.Casestudyanalysisasateachingmethoduses abstractconceptualizationwithactiveparticipationandexperimentationasthestudents reflectoneachcasescenario,applyingexperiential knowledgelearnedfrompersonal experienceandthenew cognitiveknowledgefromcontentreadinthetextbookchapters (Kolb,Boyatzis,&Mainemelis,2000).
Ineachchapter,twocasestudiesrelatedtothematerial areprovided.Thesecanbe usedtofacilitateclassroomdiscussionor canbeassignedfor individual student learningbeyondreadingthechapter content.Eachcasestudypresentsreal-life situations,completewithcomplexity,structuredcontroversy,extraneousandpertinent information,emotion,anddecisionsthatneedtobemadebyweighingall possible optionsandusingthenew knowledgegainedfromreadingthechapter.
Inreviewingeachcase,studentsshouldusecritical thinkingandproblem-solving skillstoanalyzethecase.Theycanapplyprinciplesfromthechapter contenttoidentify possiblemethodstoresolvethecaseor toreflectonpersonal insightstoenrichclass discussion.
Studentsshouldbeencouragedto(1) identifythestakeholdersineachcase;(2) describethecasesituationfromtheperspectiveofeachstakeholder;(3) applythe chapter’scontentasaframeworkfor analyzingthecase;and(4) determineacourseof actiontoresolvethecase,recognizingthatthereisnotonecorrectanswer or bestway toresolveeachcase.
Thecasestudiescanbeassignedasreflectiveessaysor theycanbeappliedasa frameworkthatstudentscanusetowriteacasefromtheir ownexperience.Theycan presenttheir casestotheclassor demonstrateknowledgeandapplicationofthe chapter’scontentinclassdiscussion.
Thecasestudyanalysesamplifythechapter contentandengagestudentsinapplying theprinciplestoreal organizational situations.
References
Kolb,D.A.,Boyatzis,R.E.,&Mainemelis,C.(2000).Experiential learningtheory: Previousresearchandnew directions.InR.J.Sternberg&L.F.Zhang(Eds.),
Perspectives on cognitive, learning and thinking styles.Hillsdale,NJ: Erlbaum.
CHAPTERONE ANewVesselforLeadership:Changingthe HealthLandscapeinanAgeofReform Thehardestthingisnottogetpeopletoacceptnew ideas;itistogetthemtoforget oldones.
John Maynard Keynes
ChapterObjectives At the completion of this chapter, the reader will be able to
• Compare the characteristics of the IndustrialAge withthose of the twenty-firstcentury.
• Enumerate the elements of quantumthinkingandexplainhow quantumthinkinghas influencedthe journeyinto the Age of Technologyandthe Age of HealthReform.
• Assess the impactof quantumscience andrecentadvances intechnologyonhealthcare andclinicalpractice.
• Describe the implications of Age of Technologythinkingonthe exercise of leadershipina time of reformatting healthcare.
• Identifythe differentskillsets for leaders incontemporarycomplexorganizations.
Transformationcontinuestobethecenterpieceofthefutureofhealthcare.Oursisan ever-evolvingtransformativeage,filledwithahostofinspiringandchallenging opportunitiesthat,justadecadeago,werethestuffofsciencefiction.Whowouldhave thoughtthatthisgenerationwouldseetheadventoffiber optics,satellite-based universities,cloning,customizedDNA-basedtreatmentmodalities,genomics,lasers, andamyriadoftechnological innovationsthatbogglethemindandenthrall the imagination?Andwhocouldhaveimaginedthat,after anintense,decades-longpolitical andsocial debate,wewouldbeconfrontingthevagariesandchallengesof implementingsignificantnational healthreform?
Alongwiththesemanyinnovationscomethechallengingadjustmentswemustmake toliveinthisincreasinglydigital universe.Instantcommunication,boundary-less relationships,theglobalizationofeconomicsandpolitics,Internetinteraction,virtual communication,knowledgethatexceedsour capacitytoassimilateit all havea dramaticimpactonour abilitytothriveinthetwenty-firstcentury.For mostofus,the changeshavecomesofastthatwedon’tfullycomprehendhow theywill affectus,and wearehardpressedtocopewiththeir implications.
KeyPoint Communicationtechnologyhascreatedaworldwithoutboundaries.Wenow must createour ownboundariesinawaythatproducesabalanceamongtheconflicting demandsofour lives.
Thepaceofchangealone apacesimplyunheardofinthelastcentury isenough tooverwhelmeventhemostenergized.Assoonaswehavethetimetoconsider the particularsofthemostrecentchanges,new changesareuponusandinsinuating themselvesintoour culture.Wedonotevenhavetheluxuryofidentifyingtheir advantagesanddisadvantagesandofconsideringtheir potential influenceonour lives.
Our society,for instance,isjustbeginningtounderstandtheimpacttheWebhashad andwill continuetohaveoncommunication,business,andpolitics.Further,new elementsoftheInternetalreadyalter how weliveour livesandchangethequestionswe askaboutwhatispassingbeforeour veryeyes.Yesterday’squestionswill notbe answeredbecausetomorrow hasbecometodaysooner thanweever couldhave imagined.
LeadinginaFluidWorld Fluidityhasbecomeacharacteristicofdoingbusinessandmanaginglifeineveryhuman arena.Becauseoftheprevalenceofaccommodatingchangeinitiatives,theabilityto adjustcoursehasbecomeanecessity.Inthiscontext,leadershipcannotbethesame.Just astheunderpinningsofour society,includinghow wedeliver healthcare,arebeing radicallytransformed,somusttheleadershipnecessarytoguidepeoplethroughlife. Theoldmodelsofleadershiparenolonger adequatetomeetthedemandsofthetimes. Whentheworldwasslower pacedandsystemstheory,complexitytheory,andquantum theorywerenotaswell formedor asinfluential,thenatureandroleofleadershipwere different.Eventheoperational realitiesoftheworkplacehavechangedtothepointthat workitselfrequiresdifferentskillsandadifferentethos(Exhibit 1-1).
Exhibit1-1New Versus OldSkillSets
Knowledge Worker
• Conceptualsynthesis
• Competentcare
• Multiple “intelligences”
• Mobile skillset
Employee (FormerType)
• Functionalanalysis
• Manualdexterity
• Fixedskillset
• Process value
• Outcome practice
• Teamperformance
• Process practice
• Unilateralperformance
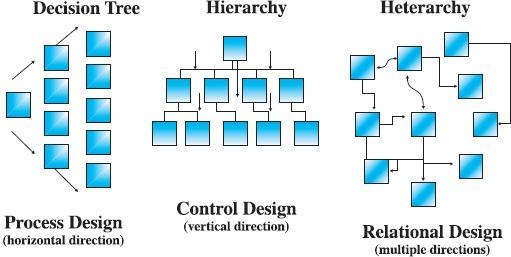
Thestableinstitutionsofthetwentiethcenturyhavebeensupplantedaswemore deeplyunderstandtheframeworkfor thetwenty-firstcentury.Thebrick-and-mortar empiresofthepastarebreakingup,replacedbyagrowingdigital architectureaswork movesawayfrominstitutionsaltogether.Theinfrastructureofsocietyisbecomingless institutional andmoreinformationbased,andthearchitectureofour placesofwork, service,andbusinessischangingdramatically.Informationstructuresareprimarily relational andfunctioncollaterallyandinmultimodal ways,whereasmostofour businessstructureshavehistoricallyfunctionedvertically.Leadinginacomplex multimodal workcultureisradicallydifferentfromleadinginapredominantlyvertical or linear workculture.
IntheIndustrial Age,organizationswereprimarilyfixed,finite,andfunctional. WorkintheIndustrial AgewasbasedonNewtonianprinciples,andfromthebeginning ofthetwentiethcentury,whenFrederickTaylor laiddownthefoundationsofscientific management,tothelate1960s,businessorganizationswerestructuredmechanistically andhierarchically.Eventhemanagementtheoristsofthe1930s,1940s,and1950sdid notradicallyalter basicorganizational design.Historically,theworker hasmostlybeen consideredasubsetofthework.Mosttrainingwasgainedonthejob,andthe apprenticeshipmodel usedfor trainingwasessentiallyhierarchical aswell.The organizationownedtheworkandsettherules.Communicationanddecisionmaking traveledupanddownthecorporateladder: Thehigher uptheladder,thegreater a person’sauthorityandautonomy.Atthebottomweretheworkerswhoperformedmost ofthefunctions under thecontrol ofthosewhohadmoved“upward.”Although attentionwaspaidtoboththeworkandtheworker,thisattentionwasbarelyreflectedin themanagementstructureandtheapplicationofleadershipinorganizations.
PointtoPonder Theworker isincreasinglyincontrol.Theknowledgenecessarytogetworkdoneis now mostlyinthehandsofthosewhodothework.Becausetheworkplaceis becomingmoredependentonknowledgeableworkers,amajor shiftinpower and control hasoccurred,andtheoldstructuresarenow inconflictwiththisnew typeof worker.
Butthisisnolonger thecaseincontemporaryworksystems.Inthecurrentworldof
work,itisnottheorganizationbuttheworker whoownsthework.Thecharacter of workchangedsubstantiallyattheendofthetwentiethcentury itbecameincreasingly technical andcomplex,oftencalled“knowledgework” andnow individualsusually needtobetrainedfor jobsbeforetheybecomeeligiblefor them.Indeed,theyare expectedtoarrive“ontherun”andstartcontributingfromtheoutset.Further, organizations’increaseddependenceonknowledgeworkershascreatedanew power equation,shiftingthelocusofcontrol fromtheorganizationtotheworker.
IntheIndustrial Age,leadership(Murphy&Riggio,2003) meantbeingagood manager,guidingone’ssubordinateslikeagoodparent,anddirectingtheir activitiesin theinterestsoftheorganization.Thecritical skillswerethoserequiredfor planning, organizing,leading,implementing,controlling,andevaluating(notetheacronym constructedfromthesesixwords: POLICE).Theabilitytofunctionwell andundertake well-definedprocesseswasthebasisofeveryrole.Goodperformanceandasenseof responsibilitywerehighlyvalued,stronglyencouraged,andheavilyrewarded.
Exhibit1-2WorkLife RealityShift
OldReality
• Scriptedlives
• Unlimitedresources
• Fixedfunctions
• Employee
• Fixedjobs
• Promotion
NewReality
• Ownyour script
• Finite resources
• Tightness of fit
• Stakeholder/member
• Fluidroles
• Mobility
Sowascompliancewiththeexpectationsoftheworkplace.Organizational leaders usedvertical communicationandcommandstrategiesexclusivelytoensurethatthe workplacestayedfocusedandorderlyandthattheworkwasperformedefficiently. Theyalsorefinedhierarchical mechanismsandfosteredcongruenceofworkplace behavior inwhatever waytheycould.
Inthisindustrial contextthefirstcontemporarynotionsofleadershipdeveloped.A wholehostofapproachestounderstandingleadershipandactingasaleader emerged duringthepastcentury,andeachonereflectedprevailingnotionsofworkand workplaceorganization(Exhibit 1-2).Thesevariousapproacheshelpedtocreatethe currentframeworkfor leadership,bothintherealmsofactionanddecisionmaking.
NewtonandOrganizationalDesign Newtonianmechanicshadatremendousinfluenceontwentieth-centuryscienceand
business.Inparticular,Newton’smodel ofthephysical universeinfluencedsocial theoriststoview social relationships,roles,andworkashighlymechanistic.Thereason thatthismechanisticframeworkwassopervasivewasitsclarityandsimplicity,linear structureandcoherence,anditsgeneralizedagreementwithpeople’snotionsofcommon sense.Especiallyappealingwasitsdependenceonreductionism,thetenetthatany complexphenomenoncouldbeunderstoodsimplybyreducingittoitssmallest componentsandanalyzingitcompartmentally.Thislinear simplicitywasespecially appealingtobusinessandorganizational leadersandwasembracedbythemwithgreat veracityinwaysthatwoulddefinethestructureofworktothisveryday.Asaresult, entrepreneursandorganizational gurusconstructedmodelsofworkinwhichwork activitieswerehighlycompartmentalized,andtheysucceededinspreadingtheuseof thesemodelsthroughouttheworld.Subsequently,workwasgenerallydesignedwith efficiencyandeffectivenessinmind,andspecial attentionwaspaidtoindividual performanceasameansofensuringthattheworkwasdoneasplanned.
KeyPoint Inthetwentiethcenturythefocusofworkwasonperformingtherightprocesses.In thetwenty-firstcenturythefocusisonobtainingtherightoutcomes.
Also,twentieth-centuryorganizationsfocusedontheassumptionthatbyconstructing workprocessesproperly,theywouldproduceproductsandservicesofconsistently goodquality.Hereagain,theorganizational literatureofthetimereflectedareductionist model.Theorganizational gurusviewedorganizationsasbeingessentiallythesameas always,althoughdifferinginstructureinminor waysandcharacterizedbyanincreased degreeofcontrol over employees.AsPeter Drucker pointedout,thecornerstoneof mosttwentieth-centuryorganizationswascontrol,asindicatedbythe“lineandbox” approachtoconfiguringtheworkplace(Edersheim&Drucker,2007) (seeFigure 1-1).
Figure1-1ChangingOrganizational Models.
GroupDiscussion Wearelivingonthecuspofthetransitionbetweentwohealthsystems,andlifeinthe AgeofHealthReformwill differ substantiallyfromlifeinthetraditional tertiary caresystem.Thechangesthatwill occur includechangesinclinical workand leadership.Brainstormatleast10changesthatwill occur inhealthreform(under the PatientProtectionandAffordableCareAct[PPACA]) over thisnextdecadeand discusstheir implicationsfor leaders.
EclipsingtheIndustrialAge For thepast30yearsor so,thestandardmodelsofworkandtheunderpinningsof societyhavebeenshiftingradically.Theimpactofour burgeoningtechnologyhas broughtaboutanew constructfor social structuresandrelationshipsacrossthewhole humanlandscape.Quantumtheory,refinedandappliedsincethemiddleofthetwentieth century,hashelpedtocreatenewer technologiesthataffectlifefromthemolecular to theglobal levels(Sreekantan&National InstituteofAdvancedStudies,2009).
Exhibit1-3ConceptualFoundations
Newtonian
• Mass production
• Compartmentalism Quantum
• Envisionthe whole
• Integration
• Reductionism
• Analysis
• Discrete action
• Synthesis
• Relatedness
• Teamaction
For example,consider thecomputer chip,whichhassingle-handedlyalteredhuman experienceforever.Amongother things,itbroughtaboutawholenew understandingof quantumprinciplesandchangedtheveryfoundationsofsocial lifebyconnectingpeople inanew way.Further,wenow livewiththeknowledgethateverythingislinkedand thateventsinonepartoftheuniversehavesomekindofimpactoneventsinother parts. Our understandingofthelinkagesamongall experiencesisthebasisfor complexity scienceandhasledtochangesintheconceptual foundationsofthesciencesandtheir social application(Exhibit 1-3).
Inturn,thesechangeshaveraisedthelevel ofconflictsurroundingbasicissues, rangingfromtheexistenceandnatureofGodtoethical andsocial norms.Claimsthat onceseemedbeyondquestionarenow opentoinvestigationandcontinuouschallenge. New scientificdiscoverieshavesubstantial religious,philosophical,andethical implicationsandhavecausedsocial discomfortamongthoseholdingmoretraditional beliefs(Volti,2010).
Itisintothisequationthatorganizational leadersarenow thrust.Theproblemisthat theytooareexperiencingtheconflictendemictothetimes.Mostleadershavespentthe majorityoftheir livesleadinginIndustrial Agemodels,justaseveryoneelsehas.They tooareconfrontingnewer realitieswithbeliefsandpracticesacquiredinthepast.They tooarestrugglingtomakesenseofthechangesoccurringglobally.Asanadditional challengetoadaptingtothesechanges,theymustalsoleadotherstoadaptsuccessfully toawholenew model guidinghumanorganization,relationship,andbehavior. Furthermore,therelateddiscoveriesandinnovationsareoccurringfaster thantherateof adaptation.Assoonasonechangeisaccommodated,another occurs,requiringa differentresponse(Nickerson,2010).
GroupDiscussion HealthcareprovidersatthebeginningoftheAgeofHealthReform(PPACA) mustbe willingtoleavesomethingsbehind(becausetheywill ceasetohavevalue) andto takeonsomenew things.Listsomeofthepractices,habits,rituals,or routinesthat needtobeleftbehind,anddiscusssymbolicactsor eventsthatcouldbeusedtohelp letgooftheseformally.Whatreplacessomeofthese“old”practices?
ChangeIs Quantumtheoryhastaughtusthatchangeisnotathingor aneventbutrather adynamic thatisconstitutiveoftheuniverse.Changecannotbeavoidedbecauseitiseverywhere, butwecaninfluenceitscircumstancesandconsequences.Inshort,wecangiveit direction.Thisnotionofconstantchangereflectsfoundationsinquantummechanicsthat suggestthatmatter isconstantlymovingintheuniverseandcanevenbeinmorethanone placeatonetimewhiletakingdifferentforms.Quantumnessisalmostcounterintuitive andreflectscharacteristicsanddynamicsofmatter andenergythatdon’tfitanylogical, ordered,structuredunderstandingofthem.
Schrödinger,amid-twentieth-centuryphysicist,usedhisfamous“Schrödinger’s Box”thoughtexperimenttoshow twoprevailingrealitiesoperatingatanygiventime, actual realityandpotential reality.Actual realityisthatwhichcurrentlyoccupiesour immediateattention.Potential reality,ontheother hand,althoughcurrentandpresent,is notyetexperienced.Beingstill potential,itiswaitingfor therightmomenttobecome expressedandthusactual.
Potential realityistherealminwhichleadershiptakesform.Theleader’sroleisto engagewiththeunfoldingreality,perceiveit,evenpredictit,noteitsdemandsand implications,translateitfor others,andfinallyguideothersintoactionstomeetthe demandsofarealitynotquitepresent.Thisleader mustbecomfortablewiththe ambiguityofthe“inbetween,”thatis,livingintworealities,thatwhichisendingand thatwhichisemerging.Demonstratingthiscomfortwiththejourneyprovidesaframe for leadingothersthroughthechaosanduncertaintyofconstantchange.
PointtoPonder Astopsigncanbeusedtoillustratepotential reality.Whenfirstseen,itnotifiesa driver tostop butnotimmediately.Thesignisareal object,areality,anditdoes requireareal response.Thedriver’spreparationtostopisthefirstinthechainof actions,anditisthisactionthatlinkstheactual tothepotential.
Inthistransformational timebetweentwoparadigms,theleader’sprimaryroleisto livefullyintherealmofpotential reality.Theleader isnotsomuchanoperational expertandproblemsolver asagood“signpostreader.”Tobeeffective,theleader must anticipatethepathofchangeandthenspell itoutfor thosewhoaremovingtheir own activities,knowinglyor unknowingly,inthesamedirectionasthechangeistakingform (Yang&Shan,2008).
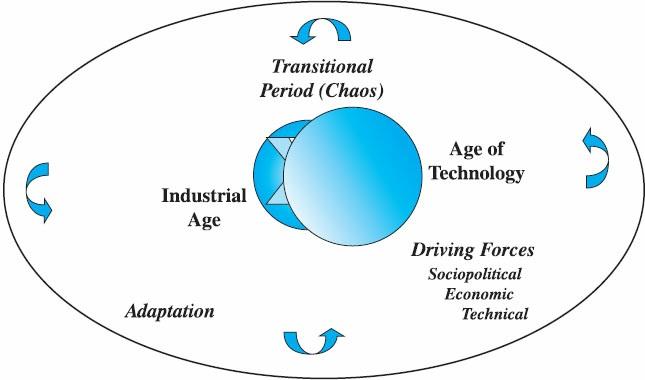
TheTransitionBetweenAges Agechangesdonotoccur quickly.Suchchangesgenerallyoccur over twoor three decades.Thechallengeisnottobecome“stuck”intheno-man’s-landbetweenan extinguishinglifescriptandanemergingone.Thedynamicsofasubstantivechangeare movinginconcerttocreatetheunderpinningsfor acomprehensivetransition(Bridges, 2002) fromonewayoflivingtoanother.Thishasoccurredseveral timesinhuman history.FromtheMiddleAgesthroughtheAgeofEnlightenmentandtheIndustrial Age anduptothecurrentera,whichwemightdubtheDigital Age(or theInformationAge), historicindicatorshavepresagedmajor shiftsinhumanexperience(Figure 1-2).
Figure1-2TheUniversal CycleofTransformation.
Thereisanimportantdifference,though,betweenpreviousshiftsandtheonethatis now occurring.Inhindsight,thesignificanceofpreviousshiftsquicklybecameclear, evenifitwasrarelyapparentduringthecritical transitionpoints.Today,ontheother hand,theperiodbetweenpredictingfuturechangesandconfrontingtheir unfoldingistoo brieftoallow planstobemadetoaccommodatethem.Indeed,today’sleadersactas agentsofchange,but,likeeveryoneelse,theymustalsoundergothechangesthemselves virtuallyatthesametimeastheyperceivethem.Whollynew leadershipskillsare requiredtomanageinthiskindofaworld.
Thinkfor amomentaboutsomeofthewaysinwhichthescriptoflifeisbeing
rewrittenfor all ofus:
• TheWebisnow aprimarybusinesstool,anditisfundamentallyalteringhow businessgetsdone.
• Fiber optics,inconjunctionwithsatellitetechnology,hasconnectedtheworld intoaseamlesscommunicationsnetworkinwhichinformationcanbetransmitted instantlyfromanyplaceontheglobetoanyother place.
• Informationhasthusbecomehighlyportable,and,giventhedevelopmentsin shipping,everyonehasaccesstoalmostanythingtheywantor needfrom anywhereintheworld.
• Technologyhasenabledcommunicationandinteractiontobecomeincreasingly moreportableaschipshavebecomesmaller anddigital deviceshavebecome packedwithtechnologyandapplicationsinlighter,smaller,moreportable hardware.
• Eachpersonhascontrol over anyrelationship,personal or business,andcan personalizeanyinteractionwithinanycontextatanytimeandinanywayheor shedesires.
• Miniaturizationhasmadeitpossiblefor peopletobemobileandstill remain connectedtoeverythingandeveryone.Furthermore,ithasmadeinnovationsin service,communication,information,andhealthcarefaster,easier,andless expensivetoimplementthanever before.
• Globalizationhascreatedaworldcommunityandremovedtraditional boundariesbetweenpeople,betheypolitical,social,or physical.The recognitionofthemobilityofhumanexperienceandofworkhascreatedanew virtual andglobal landscapefor humanaction.
Thesearejustaverysmall sampleofthetransformationsthatareoccurring.And thesetransformationsareonlythebeginning.Evenso,theyhaveamajor impactonour understanding,onthewayweliveandrelate,and,ofcourse,onthewaywework.
Imaginethelivesofour great-grandparentsor evenour grandparentsandhow differentour livesarefromtheirsasaresultofthesetechnologies(keepinmind,for example,therewerenocell phonesbefore1986).Then,consider thepossibilitythatthe childrenofcurrentteenagersmightnever writeor readaswehave,interactandplayas wehave,relatetoeachother or travel aswehave.Andremember,thisgenerationis currentlyusheringinanew wayoflivingandworkingasthebabyboomgeneration beginstoretire.
Inshort,our generationisatransitional generation thelastgenerationofthe Industrial AgeandthegenerationonthecuspoftheDigital Age.Weareinessencethe bridgebetweentwowaysofexperiencingtheworld(comparedigital immigrantsto
digital natives).Whatwedonow laysthegroundworkfor afuturethatwill looknothing liketheworldmostofushaveknown.
GroupDiscussion Listdramaticdiscoveriesandinventionsthatoccurredduringthepastcenturyand comparethewaylifechangedasaconsequencewiththewaylifechangedduringthe precedingmillennium.Then,discussthetechnological changesoccurringinthefirst decadesofthetwenty-firstcenturythataffectthefutureofhealthreformandcare delivery.
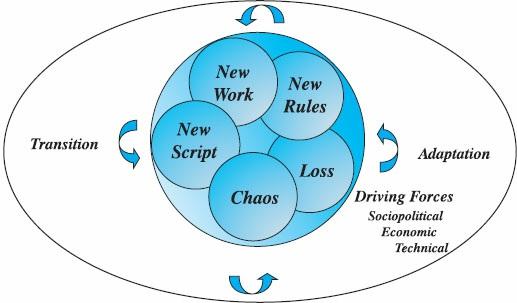
LeadingChange Itisimportantthatleadersbeawareofthetransformativeworkthatdefinestheir role. TheDigital Agenow callsfor leaderstoperceivetheir roledifferentlyandtoexpressit inwaysthatbestfitthecharacteristicsofemergingsociotechnical culture(Figure 1-3). Theroleoftoday’sleadersistoencouragethistransformation.Indeed,theymust makeacommitmenttothejourneyandworkhardtoincorporatethechangesintheir livesinaverypersonal way.Inother words,rather thansimplysuggestingthateveryone andeverythingmustchange,theymustleadbyexample.Theymustserveaswitnessesto thechangesandshow othershow toadapttothechangesintheir ownlives.
Figure1-3Universal DynamicsofTransformation.
PointtoPonder Thebehavior ofleadersmustexemplifytheir commitmenttosustaintheir own journeyandtocoordinateandfacilitatetheeffortsofotherstobuildadesiredfuture.
Intheinitial stageofthistransformation,leadersmustbeabletoshow thatthe comingchangesrepresentacritical shiftandmust,throughtheir passionfor movement, inspireresponsesfromothers.Thisisnotthetimefor complacencybutfor truthtelling andconfrontation.Inshort,itisatimetoinformpeoplehow thechangesmakea substantial differenceintheir livesandintheir work.Advancingpeople’sawarenessof thisrequiresalevel ofhonestyanddirectnessoncethoughttobeconfrontational.
Inthecaseofhealthcare,themajor reformsunder waywill leadtotheendofthe hospital-basedsickness-orientedmodel ofservicedelivery.Our technologiesenableus totreatillnessesatanearlier stageandreducetheneedfor costlysurgical interventions. Asaconsequence,notonlyphysiciansbutalsonursesandother healthprofessionals mustmakesubstantial changesinthewaytheypracticetheir professionsandprovide services.Theintroductionofvalue-drivenapproachesthatfocusonearlyengagement, attainingthehighestlevel ofpersonal health,preventionrather thantreatment,and designingthesystemtoprovideacontinuumofhealthservicesrepresentsaneffective model ofhealthservice(Birk,2013).
Leadersinhealthcaremusthelppeoplesever their attachmenttothekindof healthcaresystemwithwhichtheyhavebecomecomfortable.Healthreformcallsusall tofocusonaccountability,earlyengagement,prevention,cost-effectiveness,anda higher level ofaggregatehealthfor all citizens.Somanyhealthprofessionalsare mourningthelossofwhatispassingawayor haspassedaway.Insomecases,their senseoflossisunderstandable,butmostofwhattheymournfor should not beretained or broughtback.Thatwasthen;thisisnow.Someofthefactorsthatattractedmanyofus tohealthcarehavevanishedfor good.Thequestionisnotwhether theywill return,but how toadapttothenew circumstancesandnew modelsofhealthservice.
Healthcareleadersmusttrytoengageothersintheprocessofmakingtheir own changes.Theymusttakewhatever actionisnecessarytoimpressuponhealth professionalsthatthisisatimeofgreatmobilityandofshiftingfoundations.In particular,theymustcall all stakeholderstothetabletoworkoutwhatmustbealtered andwhatmustbeintroducedtofashionanew healthcaredeliverysystem.Agreat tragedywill occur ifhealthcareleadersareunsuccessful inthistaskandallow stakeholderssimplytoreacttochangeslongsincepast.Complacencyguarantees failure.
Leadersmaybevictimsoftheir owninsightsandpastsuccesses,whichcancause themtouseanoutdatedrecipefor successaswell asmisleadingmeasuresofsuccess. Theymustseetheapproachingchallengeswithinthecontextoftheir becoming,not throughtheeyesofpasttriumphs.
Notonlymustleadersclosethedoor ontheoldmodelsofhealthdeliveryand clinical work,buttheymustturnaroundandfacethefuture,viewingtheentire landscapetodevelopaworkablevision.Often,healthcareleadersaretooshortsighted, andtheir visiontootenuous.Theconditionsthatdeterminethefutureofhealthcareare vastlydifferentfromanythingthatwehaveexperiencedtodate,andthusleadersmust constructaradical visionofhow serviceswill beprovidedinthenew healthcare landscape.Theimpactofmicronization,genomics,biotherapeutics,chemotherapeutics, andnew economicandservicedeliverymodelsisforever alteringWesternmedicine (Exhibit 1-4),andsothestructuresthatsupporttheprovisionofWesternmedicinealso needtochange.Thebrick-and-mortar infrastructureandthecurrentadministrativeand operational frameworksarenolonger entirelyrelevant,andtheymustbeadjustedin responsetofinancial,political,andtechnological pressuresofachanginghealthcare system.Imaginehow painful thatmessageisfor theseriousandtalentedmenand womenwhohavedevotedtheir livestobuildingtheir imageofthehealthcaresystem. Therequirementtotear itapartandbeginanew isoverwhelmingtothem,buttheyare calledtothistaskbythechangesthathavealreadyoccurredandthoseanticipatedaswe refineandunfoldhealthreformover thenexttwodecades.
KeyPoint Movingintoareformedhealthsystemdoesnotmeanleavingeverythingbehind.It doesmeanthinkingaboutwhatneedstobeleftbehindandreflectingonwhatshould gowithusaswemoveintoanagewithadifferentsetofparameters.
Exhibit1-4ChangingMedicalTherapies
OldTherapies
• Surgery
• Salves andcreams,drugs
• Accommodation
• Nothingcanbe done
• Treatments
• Enemas
• Bloodletting
• Generalsupplements
NewTherapies
• Lasers
• Microsurgery
• Genomics
• Pharmaceuticals
• Chemotherapy
• Radiotherapy
• Synthetic products
• Specifiedsupplements