Senior Managing Editor for Development: Lois Berlowitz
Assistant Editor: Jonathan Cheung
Director of Marketing: David Gesell
Executive Marketing Manager: Katrin Beacom
Marketing Coordinator: Brian Hoehl
Marketing Specialist: Michael Sirinides
Production Manager: Pat Brown
Creative Director: Jayne Conte
Art Director: Laura Gardner
Interior Designer: Carmen DiBartolomeo
Designer: Suzanne Behnke
Composition: Aptara®, Inc./Jogender Taneja
Printing and Binding: Courier/Kendallville
Cover Printer: Lehigh-Phoenix Color/ Hagerstown
Notice: The author and the publisher of this book have taken care to make certain that the information given is correct and compatible with the standards generally accepted at the time of publication. Nevertheless, as new information becomes available, changes in treatment and in the use of equipment and procedures become necessary. The reader is advised to carefully consult the instruction and information material included in each piece of equipment or device before administration. Students are warned that the use of any techniques must be authorized by their medical advisor, where appropriate, in accordance with local laws and regulations. The author and the publisher disclaim any liability, loss, injury, or damage incurred as a consequence, directly or indirectly, of the use and application of any of the contents of this book.
Credits and acknowledgments borrowed from other sources and reproduced, with permission, in this textbook appear on the appropriate page within text.
Cataloging-in-Publication data on file with the Library of Congress.
ISBN 10: 0-13-292106-5
ISBN 13: 978-0-13-292106-0
DEDICATION
This book is dedicated to the memory of a special man who was a revered friend, a mentor, and an enthusiastic educator for Emergency Medical Services.
His passion for quality patient care was a driving force in his role as a physician who helped to develop excellence in EMS education. He was a consummate professional and a wonderful human being.
Dr. Willis D. C. Israel
Dr. I., we miss you!
B. M. B.
CONTENTS
Foreword vii
Preface viii
CHAPTER 1
Key Points to Remember 24
Review Questions 24
CHAPTER 4
THE ANATOMY OF THE HEART (STRUCTURE) 1
THE ELECTRICAL CONDUCTION SYSTEM 26
Objectives 1
Objectives 26
Introduction 1
Introduction 26
Anatomy of the Heart 1
Sinoatrial Node 27
Location, Size, and Shape of the Heart 2
Internodal Pathways 28
Layers of the Heart 3
Valves of the Heart 4
Bachmann’s Bundle, Wenckebach’s Bundle, and Thorel’s Pathway 29
Arteries, Veins, and Capillaries 5
Atrioventricular Node 29
Summary 9
Atrioventricular Junction 29
Key Points to Remember 9
Bundle of His 29
Review Questions 9
CHAPTER 2
Bundle Branches 29
Purkinje’s Network 30
Summary 30
CARDIOVASCULAR PHYSIOLOGY (FUNCTION) 11
Key Points to Remember 30
Review Questions 31
Objectives 11
Introduction 11
CHAPTER 5
Blood Flow through the Heart 11
THE ELECTROCARDIOGRAM 32
Cardiac Cycle 13
Stroke Volume 13
Objectives 32
Cardiac Output 14
Introduction 32
Autonomic Nervous System 14
Electrical Basis of the EKG 32
Receptors and Neurotransmitters 15
EKG Leads 32
Summary 17
EKG Graph Paper 40
Key Points to Remember 17
EKG Waveforms 41
Review Questions 17
CHAPTER 3
BASIC ELECTROPHYSIOLOGY 19
Standard 12-Lead EKG Waveforms 45
Summary 47
Key Points to Remember 47
Review Questions 48
Objectives 19
CHAPTER 6
Introduction 19
INTERPRETATION OF EKG STRIPS 50
Basic Cell Groups 19
Primary Cardiac Cell Characteristics 20
Objectives 50
Major Electrolytes That Affect Cardiac Function 21
Introduction 50
Movement of Ions 21
General Rules 50
Cardiac Depolarization 21
The Five-Step Approach 51
Cardiac Repolarization 22
The 5 + 3 Approach 55
Refractory Periods 23
ST Segment Depression 56
Summary 23
ST Segment Elevation 57
Q Wave 58
Summary 60
Key Points to Remember 60
Review Questions 60
CHAPTER 7
ACUTE MYOCARDIAL INFARCTION 62
Objectives 62
Introduction 62
Coronary Anatomy 62
Pathology 64
Standard Treatment Modalities 67
Noncardiac Causes of Chest Pain 68
Clinical Significance 69
Patient Assessment 69
Summary 70
Key Points to Remember 70
Review Questions 70
CHAPTER
8
MYOCARDIAL ISCHEMIA, INJURY, AND NECROSIS 72
Objectives 72
Introduction 72
Time Is Muscle (Myocardium) 72
Infarct Regions and Definitions 73
Clinical Significance 76
Summary 77
Key Points to Remember 77
Review Questions 77
CHAPTER 9
INTERPRETATION OF INFERIOR MYOCARDIAL INFARCTIONS 79
Objectives 79
Introduction 79
Anatomy and Physiology Review 79
Transmural Versus Subendocardial Infarctions 81
Lead-Specifi c ST Elevation 82
EKG Changes Related to an Inferior Infarction 84
Clinical Significance of Inferior Myocardial Infarctions 85
Summary 87
Key Points to Remember 87
Review Questions 88
CHAPTER 10
INTERPRETATION OF ANTERIOR MYOCARDIAL INFARCTIONS 91
Objectives 91 Introduction 91
Anatomy of the Coronary Arteries 91
”Widowmaker”—Left Anterior Descending Artery 92
Lead-Specifi c ST Segment Elevation 93
EKG Changes Commonly Associated with Anterior Myocardial Infarctions 95
Clinical Significance of Anterior Myocardial Infarctions 95
Summary 98
Key Points to Remember 98
Review Questions 98
CHAPTER 11
INTERPRETATION OF SEPTAL MYOCARDIAL INFARCTIONS 102
Objectives 102
Introduction 102
Anatomy of the Interventricular Septum and the Coronary Arteries 102
Lead-Specifi c ST Segment Elevation 103
EKG Changes Commonly Associated with Septal Myocardial Infarctions 106
Clinical Significance of Septal Myocardial Infarctions 106
Summary 107
Key Points to Remember 107 Review Questions 108
CHAPTER 12
INTERPRETATION OF LATERAL MYOCARDIAL INFARCTIONS 111
Objectives 111
Introduction 111
Anatomy of the Left Ventricle and the Circumflex Branch of the Left Coronary Artery 111
Lead-Specifi c ST Segment Changes 112
EKG Changes Commonly Associated with Lateral Myocardial Infarctions 114
Clinical Significance of Lateral Myocardial Infarctions 114
Summary 116
Key Points to Remember 116
Review Questions 117
CHAPTER 13
INTERPRETATION OF POSTERIOR MYOCARDIAL INFARCTIONS 120
Objectives 120
Introduction 120
Coronary Artery Anatomy Review 120
Lead-Specifi c ST Segment Changes 121
The Mirror Test 121
Another Trick for Identifying Posterior Myocardial Infarctions 122
Posterior V Leads 122
EKG Changes Related to Posterior Myocardial Infarctions 125
Clinical Significance of Posterior Myocardial Infarctions 126
Summary 128
Key Points to Remember 128 Review Questions 129
CHAPTER 14
AXIS DEVIATION AND BUNDLE BRANCH BLOCKS 131
Objectives 131
Introduction 131
EKG Leads 131
The Hexaxial Reference System 132 Axis Deviation 132
Bundle Branch Blocks 136
Clinical Significance of Bundle Branch Blocks 141
Summary 143
Key Points to Remember 143 Review Questions 144
CHAPTER 15
THERAPEUTIC MODALITIES 146
Objectives 146
Introduction 146
Fibrinolytics 146
Emergency External Cardiac Pacing 150
Defibrillation 152
Cardioversion 155
Summary 157
Key Points to Remember 157
Review Questions 157
CHAPTER 16 CARDIOVASCULAR PHARMACOLOGY 159
Objectives 159
Introduction 159
Oxygen 160
Sympathomimetics 161
Sympatholytics 168
Antidysrhythmics 169
Analgesics 177
Antianginals 178
Alkalinizing Agents 179
Anticoagulants 180
Summary 181
Key Points to Remember 182 Review Questions 182
CHAPTER 17 MORE REVIEW QUESTIONS 184
CHAPTER 18 12-LEAD EKG REVIEW STRIPS 203
Appendix 1 ANSWERS TO REVIEW QUESTIONS 292
Appendix 2 ANSWERS TO REVIEW STRIPS 295
Glossary 313 Index 318
FOREWORD
The value of over 30 years of combined EMS educational experience enables Brenda M. Beasley and Michael West to bring a unique and insightful approach to the topic of 12-lead EKGs and their interpretation. The authors have presented a complex yet vitally important subject in a comprehensive, straightforward, and easy-to-understand format.
The text serves a wide audience of health care providers, including prehospital providers, nurses, physician assistants, respiratory therapists, and anyone requiring a thorough understanding of electrocardiography. I believe that this book fills a void in the subject matter of EKG interpretation. It demonstrates the ability to educate medical personnel who are new to the subject matter while providing a review to those who are more experienced.
Using a reader-friendly writing style, the authors create a text that begins with the basics of EKG interpretation and then introduces a building-block approach to a more detailed discussion of this topic. Many illustrations, tables, and graphs are used to help highlight the important issues of each topic. Also, the reader will fi nd the review questions at the end of each chapter useful in helping to solidify knowledge of salient issues.
Ms. Beasley has played a vital role in EMS education throughout the state of Alabama. She has made a difference in the lives of many people as well as influenced many career decisions. It was her commitment to education in and excitement about emergency medicine that was a significant factor in my choice of medicine as a career and, later, emergency medicine as a profession. The nursing background of both Ms. Beasley and Mr. West and their experience as EMS educators give them the wisdom to continue their roles of educating and influencing others through this text.
The importance of the communication and understanding of EKG changes among all medical personnel cannot be overemphasized. As an emergency medicine physician, I congratulate both Ms. Beasley and Mr. West on a book that provides common ground for physicians, nurses, and prehospital personnel.
Benjamin J. Camp, MD Emergency Medicine Physician
PREFACE
Our purpose in writing the fi rst edition of Understanding 12-Lead EKGs: A Practical Approach was to create a learning resource that was reader-friendly yet comprehensive in its approach to the interpretation of the 12-lead electrocardiogram. Remaining true to that original purpose, we have revised the text in order to update the content as applicable. This text continues to serve as a companion text to the third edition of Understanding EKGs: A Practical Approach
The third edition of this text consists of 18 chapters that are designed to provide the user with a practical approach to the skill of 12-lead EKG interpretation. The original chapters have been updated and new artwork and additional review strips have been added. As from its inception, the goal of this text continues to be to provide a useful and understandable learning tool for health care providers in their provision of optimum patient care.
We continue to believe that an essential prerequisite to understanding 12-lead EKG interpretation is a thorough understanding of basic EKG interpretation. With this thought in mind, we began this book with a series of chapters that review basic dysrhythmia interpretation. This book includes rhythm strip examples within each applicable chapter, as well as an entire chapter devoted to 12-lead EKG review strips. In addition, there are updated chapters devoted to cardiovascular pharmacology, therapeutic modalities, and to incorporating new AHA guidelines.
It has been our intent to present the material in a logical order. In order to enable students to work comfortably through the technical information, the content is presented in short, succinct chapters in a building-block format. Students thereby achieve understanding of each chapter before proceeding to the next chapter. At the end of each chapter, we have included the section of multiple-choice questions to be used for self-assessment and review. In addition, we have included practice EKG review strips at the end of the type-specific myocardial infarctions (MI) chapters, as well as Key Points to Remember.
An overview of major updates and additions to this revision may be helpful to you. These changes are summarized in the “What’s New” list below.
WHAT’S NEW IN THE THIRD EDITION
■ Information has been updated to reflect current standards of care.
■ Current treatment regimens for AMI and fibrinolytics (formerly referred to as thrombolytics) and new, updated pharmacologic agents are addressed.
■ Added and enhanced, up-to-date graphics accompany each chapter.
■ Numerous examples of 12-lead EKGs are presented, and new EKG review strips have been added at the end of each applicable chapter.
■ New review strips have been added to Chapter 18.
■ Margin glossaries appear throughout the text.
■ Each chapter features a Summary as a wrap-up of chapter content.
■ The feature Key Points to Remember has been enhanced and revised at the end of each chapter.
■ At the end of each chapter, the authors have provided chapter-specific review questions.
■ Instructor and student resources are available online at Brady’s Resource Central web site.
INSTRUCTOR RESOURCES
This web site contains an array of instructor resources in one location. To access Resource Central, go to www.bradybooks.com and select myemskit/Resource Central. Click on the book cover for this title and follow registration/log-in instructions for Instructors. Your Brady sales representative can offer further assistance.
Once you are logged onto the site, you’ll fi nd the following teaching resources.
■ PowerPoint Slides-updated and revised to include new review strips
■ Lesson Plans
■ Test Bank with more than 250 questions
STUDENT RESOURCES
This web site provides chapter support materials and interactive resources in one location. To access Resource Central, follow directions on the Student Access Code Card provided with the text. If there is no card, go to www.bradybooks.com and select myemskit/Resource Central. Click on the book cover for this title and follow registration/Buy Access/log-in instructions for Students.
Once you are logged onto the site, you will fi nd reinforcement exercises, enrichment activities, and links to additional references and support material.
Since the late 1980s, the use of thrombolytics (now referred to as fibrinolytics) in the treatment of acute myocardial infarctions has become an expanding, dynamic component of the health care profession. The primary goal, however, is the immediate transportation of the patient to a cath lab from either the prehospital arena or the emergency department. As a direct result of this, more and more health care providers are required to interpret, understand, and apply their knowledge of 12-lead EKGs in the clinical settings. We sincerely hope that this logical, comprehensive approach to 12-lead EKG interpretation will provide the student, as well as other health care providers, with a substantial foundation to understand and interpret electrocardiology. Ultimately, it is our wish that your future patients will benefit from the knowledge that you attain from this text.
Brenda M. Beasley e-mail: bjm18@aol.com
Michael C. West e-mail: MWest44266@aol.com
ACKNOWLEDGMENTS
The first edition of Understanding 12-Lead EKGs: A Practical Approach was created as a result of our collective experiences in EMS education as well as in the clinical practice of emergency medicine. As we embarked on the revision of the third edition of this text, we called on the advice of our graduates and colleagues as well as professional reviewers. We wish to recognize the following individuals who were instrumental, each in his or her own unique way, in making this textbook a reality.
We offer our sincere appreciation to the professional and competent team at Brady! The support of Marlene Pratt has been unwavering and much appreciated. Lois Berlowitz (a real angel) has skillfully guided us through completion of this project and has patiently steered us through the tedious process of making the book look good! We would like to recognize Jonathan Cheung who has been involved with every phase of the review process and has done a remarkable job. The numerous demands of production have been in the very competent and effi cient hands of Patrick Walsh, Production Manager; Patricia Gutierrez, Production Liaison; and Pat Brown at Pearson and we are appreciative of their efforts. We also thank Brian Hoehl for marketing expertise during the promotion of this book revision. Many thanks are due to Jogender Taneja and Sanchita Massey at Aptara for expertly guiding us through the copyediting and proofreading of every word in our text!
Thanks are also due to Dr. Ben Camp for writing the Foreword for this book as well as for lending his advice and expertise to us throughout the entire project. Our expert reviewers, listed below, deserve much thanks for providing excellent suggestions and ideas for improving the text.
And last but not least, we gratefully acknowledge our families, friends, and colleagues for their support, encouragement, and acceptance of our long absences during this textbook revision. Without the strength and love we received from each of you this task would have not been possible. Thank you so much for your continuing support.
INSTRUCTOR REVIEWERS
Tera Barnes, RN, EMT-P
Paramedic Program Director
EMS Department Chair
Indian River State College
Ft. Pierce, FL
Cornelia A. Bryan, MHHS, NREMT-P
Adjunct Faculty
Youngstown State University
Youngstown, OH
Deborah K. Drummonds, RN, MN, CCRN, CEN
Assistant Professor: School of Nursing and Health Sciences
Abraham Baldwin College: School of Nursing and Health Sciences
Tifton, GA
Nancy Faber, NREMT-P, CCEMT-P
Lead EMS Instructor, Course Coordinator
Southern Fox Valley EMS System Delnor Hospital Geneva, IL
Eric M. Greenfield, D.O., NREMT-P Medical Director, Calhoun Community College Decatur, AL
Attending Emergency Physician, Huntsville Hospital Huntsville, AL
Rosemary Smith Harrell, RN, BSN, CEN, CCEMTP Clinical Coordinator Paramedic Program Trident Technical College Charleston, SC
David James Newton, MPH, NREMT-P EMS Instructor and Clinical Coordinator Gwinnett Technical College Lawrenceville, GA
David Pierce, BA, NREMT-P
EMS Faculty
Century College
White Bear Lake, MN
Brittany Ann Williams, MHSc, BSRT-NPS, NREMT-P Associate Professor EMS
Santa Fe College
Gainesville, FL
Randy Williams, NREMT-P Instructor of Paramedic Technology/EMS Programs Coordinator
Bainbridge College
Bainbridge, GA
This page intentionally left blank
THE ANATOMY OF THE HEART
(STRUCTURE)
INTRODUCTION
It is our belief that in order to properly master the art of 12-lead EKG interpretation, you must first have a thorough understanding of the structure of the heart. Therefore, this chapter provides you with a foundation upon which to review the fundamental knowledge of basic dysrhythmia interpretation. The focus of this chapter is thus to provide you with a simple yet comprehensive reassessment of cardiac anatomy. After you have reviewed the knowledge of basic cardiac anatomy (structure), you will be prepared to move to the next chapter, which reexamines the basic physiology (function) of the heart.
ANATOMY OF THE HEART
First you must realize that the heart is a muscle. Although we do not usually think of exercising our heart muscle when we go to the gym, the fact is that the heart muscle (myocardium) is constantly in the exercise mode. At times of rest, the exercise is more sedate. However, think of the vigor with which your heart muscle must exercise when you walk (or run) up six flights of stairs. Now as you feel your heart pumping, you can easily understand that your heart muscle is indeed exercising.
We often hear the heart referred to as a two-sided pump. This analogy works well in our understanding of the basics of cardiac anatomy. Indeed, one can visualize this pump as having a right side and a left side. On each side of the pump, there is an upper chamber, which is referred to as the atrium (atria, plural) and a lower chamber known as the ventricle (Figure 1–1). There is a total of four hollow chambers in the normal heart. Again, the two upper chambers of the heart are called atria and the two lower chambers are called ventricles. The interatrial septum separates the upper chambers, and the interventricular septum separates the lower, inferior chambers. Externally, the atrioventricular groove, known as the coronary sulcus, surrounds the outside of the heart and divides the atria from the ventricles. The anterior and posterior interventricular grooves separate the ventricles externally. The muscle fibers of the ventricles are continuous, as are the atrial muscle fibers.
1
OBJECTIVES
Upon completion of this chapter, you will be able to:
■ Identify the location, shape, and size of the heart
■ Describe the chambers of the heart
a. Atria
b. Ventricles
■ Name and locate the layers of the heart
■ Name and locate the valves of the heart
■ Describe the structure and function of the blood vessels
a. Arteries
b. Coronary arteries
c. Veins
d. Capillaries
dysrhythmia abnormal rhythm atrium upper chamber of the heart
ventricle lower chamber of the heart
Right atrium
Right ventricle
Figure 1–1. The chambers of the heart
Interatrial septum
Left atrium
Left ventricle
Interventricular septum
mediastinum central section of the thorax (chest cavity)
The two upper chambers of the heart are located at the base, or top, of the heart whereas the lower chambers are located at the bottom, or apex of the heart. The upper chambers of the heart are thin-walled and receive blood as it returns to the heart. The lower chambers of the heart have thicker walls and pump blood away from the heart. The right ventricle pumps blood to the pulmonary circulation and the left ventricle pumps blood throughout the systemic circulation.
LOCATION, SIZE, AND SHAPE OF THE HEART
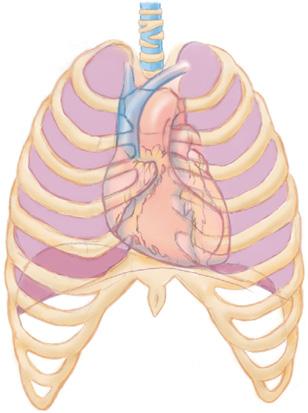
It is important for you to understand the location of the heart in that the effectiveness of one of our most basic yet most important skills—namely, CPR—depends on reasonable knowledge of this position. The proper placement of electrodes to record an electrocardiogram, either 3-lead or 12-lead, depends upon the proper understanding of the location of the heart. The central section of the thorax (chest cavity) is called the mediastinum. It is in this area that the heart is housed, lying in front of the spinal column, behind the sternum and between the lungs (Figures 1–2 and 1–3). When thinking of the heart muscle in terms of its
Trachea
Figure 1–2. Location of the heart within the chest
Mediastinum
Right Lung
Right pleural cavity
Left Lung
Pericardial cavity Heart
Figure 1–3. Anatomical relationships in the thoracic cavity
Visceral pleura
Parietal pleura
Left pleural cavity
mass, one should realize that two-thirds of the heart lies to the left of the midline. The apex of the heart lies just above the diaphragm, and the base of the heart lies at approximately the level of the third rib.
The exact size of the heart varies somewhat among individuals; but on average, it is approximately 5 inches (10 to 12 centimeters) in length and 3 inches (9 centimeters) wide. The shape of the heart is somewhat cone-like in appearance. It is appropriate to visualize the heart as approximately the size of the owner’s closed fist.
LAYERS OF THE HEART
Pericardium
Surrounding the heart is a closed, two-layered sac referred to as the pericardium, also known as the pericardial sac. In direct contact with the pleura is the outer layer or the parietal pericardium. This layer consists of tough, nonelastic, fibrous connective tissue and serves to prevent overdistention of the heart. The thin, serous inner layer of the pericardium is called the visceral pericardium and is contiguous with the epicardium, which surrounds the heart. A space filled with a scant amount of fluid (approximately 10 cubic centimeters [cc]) separates the two pericardial layers. This fluid helps to reduce friction as the heart moves within the pericardial sac by acting as a lubricant.
An inflammation of the serous pericardium is called pericarditis. Although the cause of this disease is frequently unknown, it may result from infection or disease of the connective tissue. This disease can cause severe pain, which may be confused with the pain of myocardial infarction. Pericarditis can cause changes in the 12-lead EKG and can mimic an acute myocardial infarction, which will be addressed later in Chapter 7. This can make physical assessment of the cardiac patient a real challenge for the clinician.
An excess accumulation of fluid in the pericardial sac is called cardiac tamponade. This condition is an extreme emergency and must be detected and treated expeditiously.
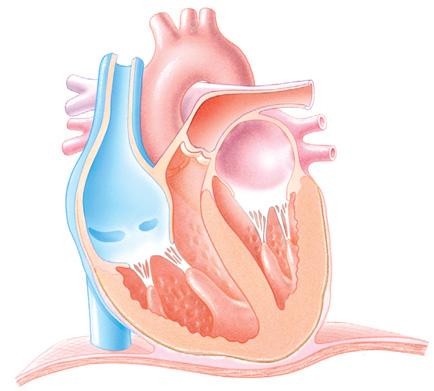
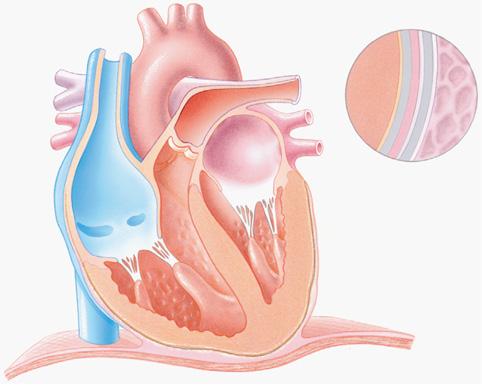
The heart wall
Three layers of tissue compose the heart wall: the epicardium, myocardium, and endocardium (Figure 1–4). This specialized cardiac muscle tissue is unique to the heart. The epicardium accounts for the smooth outer surface of the heart. The main coronary arteries are located on the surface of the heart. The thick, middle layer of the heart is called the
pericardium closed, two-layered sac that surrounds the heart. Also called pericardial sac
pericarditis inflammation of the serous pericardium cardiac tamponade excess accumulation of fluid in the pericardial sac
epicardium smooth outer surface of the heart
myocardium thick middle layer of the heart composed primarily of cardiac muscle cells; responsible for the heart’s ability to contract endocardium innermost layer of the heart; composed of thin connective tissue
atrioventricular (AV) valves the valves through which the blood passes from the atria to the ventricles
tricuspid valve named for its three cusps; located between the right atrium and right ventricle
chordae tendineae fine chords of dense connective tissue that attach to papillary muscles in the wall of the ventricles
mitral valve similar in structure to the tricuspid valve but has only two cusps; located between the left atrium and the left ventricle. Also called bicuspid valve semilunar valves prevent the backflow of blood into the ventricles; each valve contains three semilunar (or moonshaped) cusps
Myocardium
Epicardium
Pericardial cavity
Lung
Parietal pericardium
Pleural cavity
Pleura
Endocardium
Diaphragm
myocardium and is the thickest of the three layers of the heart wall. The myocardium is composed primarily of cardiac muscle cells and is responsible for the heart’s ability to contract. The innermost layer, the endocardium, is composed of thin connective tissue. This smooth inner surface of the heart and heart valves serves to allow blood to flow more easily throughout the heart.
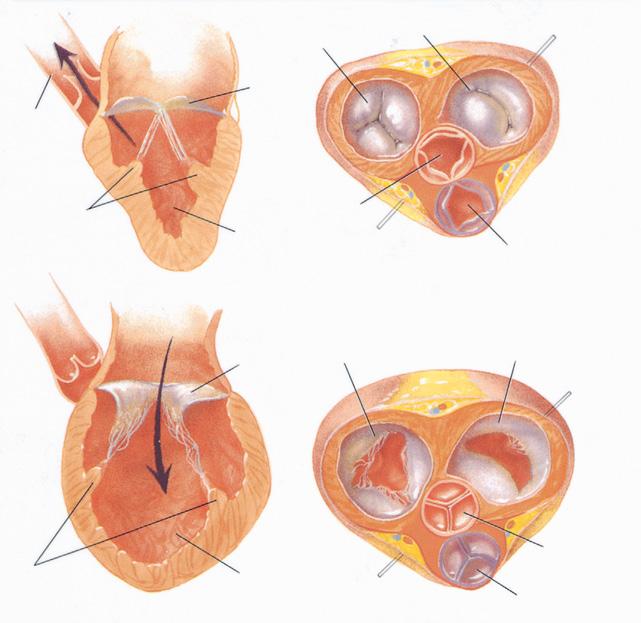
VALVES OF THE HEART
The four valves of the heart allow blood to flow in only one direction. There are two sets of valves: the atrioventricular valves and the semilunar valves (Figure 1–5).
Atrioventricular valves
As indicated by the name, the atrioventricular (AV) valves are located between the atria and the ventricles. These valves allow blood to flow from the atria into the ventricles. They are also effective in preventing the blood from flowing backward from the ventricles into the atria. The tricuspid valve is named for its three cusps and is located between the right atrium and the right ventricle. Free edges of each of the three cusps extend into the ventricles where they attach to the chordae tendineae. Chordae tendineae are fine chords of dense connective tissue that attach to papillary muscles in the wall of the ventricles. Chordae tendineae and papillary muscles work in concert to prevent the cusps from fluttering back into the atrium, allowing disruption of blood flow through the heart. The mitral valve (or bicuspid valve) is similar in structure to the tricuspid valve, but has only two cusps. The mitral valve is located between the left atrium and the left ventricle.
Semilunar valves
In much the same manner as the AV valves prevent backflow of blood into the atria, the semilunar valves serve to prevent the backflow of blood into the ventricles. Each semilunar valve contains three semilunar (or moon-shaped) cusps. The semilunar valves are the pulmonic and aortic valves. The semilunar valve located between the right ventricle and the
Figure 1–4. Layers of the heart
Tricuspid (right AV) valve closed
Left atrium
Aorta
Papillary muscles tense
Mitral (left AV) valve closed
Mitral valve closed
Aortic semilunar valve open
Left ventricle contracted
(a) SYSTOLE
Tricuspid valve open
Mitral valve open
Pulmonary semilunar valve open
Mitral valve open
Papillary muscles relaxed
Left ventricle dilated
(b) DIASTOLE
Aortic valve closed
Pulmonary semilunar valve closed
pulmonary artery is called the pulmonic valve. The semilunar valve located between the left ventricle and the trunk of the aorta is called the aortic valve. Changes in chamber pressure govern the opening and closing of the heart valves. During ventricular systole (contraction of the ventricles), the AV valves close and the semilunar valves open. During ventricular diastole (relaxation of the ventricles), the aortic and pulmonic valves are closed and the mitral and tricuspid valves are open. Passive filling of the coronary arteries occurs during ventricular diastole.
ARTERIES, VEINS, AND CAPILLARIES
Because we tend to refer to the heart as the body’s pump, we can similarly consider the vasculature, or the blood vessels, as the container for the fluid, or blood. When considering the purpose of this text, it is appropriate to discuss three commonly accepted groups of blood vessels: arteries, veins, and capillaries.
Arteries
Arteries, by virtue of their primary function, are relatively thick-walled and muscular. These blood vessels function under high pressure in order to convey blood from the heart out to the rest of the body. One definition of the prefix a is away from, so a helpful hint is to remember that the word artery also begins with the letter a, and thus arteries carry blood away from the heart. The larger arterial blood vessels are called arteries, which branch off into smaller blood vessels known as arterioles. Arteries carry oxygenated blood, with the exception of the pulmonary and umbilical arteries.
pulmonic valve
semilunar valve located between the right ventricle and the pulmonary artery
aortic valve semilunar valve located between the left ventricle and the trunk of the aorta
arteries thick-walled and muscular blood vessels that func tion under high pressure to convey blood from the heart out to the rest of the body
Figure 1–5. Valves of the heart
Typical vein
Lumen
Tunica intima
Tunica media
Tunica adventitia
Typical capillary
Typical artery
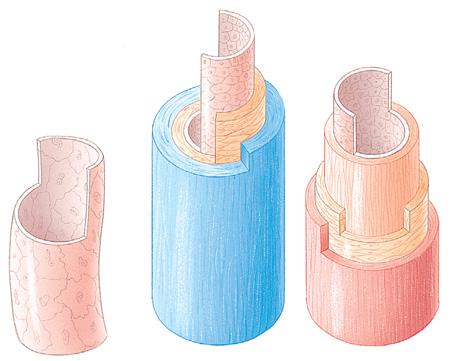
Figure 1–6. Arterial wall layers
Lumen
Tunica intima
Elastic membrane
Tunica media
Muscle
Tunica adventitia
coronary arteries the two arteries— right and left—that supply blood to the myocardium
Arteries also operate in the regulation of blood pressure through functional changes in peripheral vascular resistance (the amount of opposition to blood flow offered by the arterioles). Arterial walls consist of three distinct layers: the intima, media, and adventitia (Figure 1–6). These layers are also called tunics (coats or coverings). The tunica intima is the innermost layer and consists of endothelium and an inner elastic membrane. This inner elastic membrane separates the intimal layer from the next layer, the tunica media. The tunica media is the middle layer and consists of smooth muscle cells. In this middle layer, blood flow through the vessel is regulated by constriction or dilation. Vasoconstriction, or a decrease in the diameter of the blood vessel, produces a decrease in blood flow. In contrast, vasodilation, or an increase in the diameter of the blood vessel, produces an increase in blood flow. The tunica adventitia, or outermost layer, is composed of various connective tissues that anchor the blood vessels to adjacent tissues. (See Table 1–1.)
Coronary
arteries and the coronary sinus
The primary structures of importance in this section are the coronary arteries and the coronary sinus.
Two Main Coronary Arteries The two main coronary arteries, the right and left, arise from the trunk of the aorta and function to carry oxygenated blood throughout the myocardium. These arteries branch off into smaller vessels to supply the heart with oxygen. Because the left side of the heart is more muscular than the right side, the left coronary artery branches are more muscular than the right coronary artery branches. Oxygenated blood is distributed throughout the heart muscle through the process known as coronary circulation (discussed in detail in Chapter 7).
Table 1–1 ■ Arterial Wall Layers
Name
Tunica intima Innermost Connective and elastic
Tunica media Middle Smooth muscle, elastic, and collagen
Tunica adventitia Outermost Connective
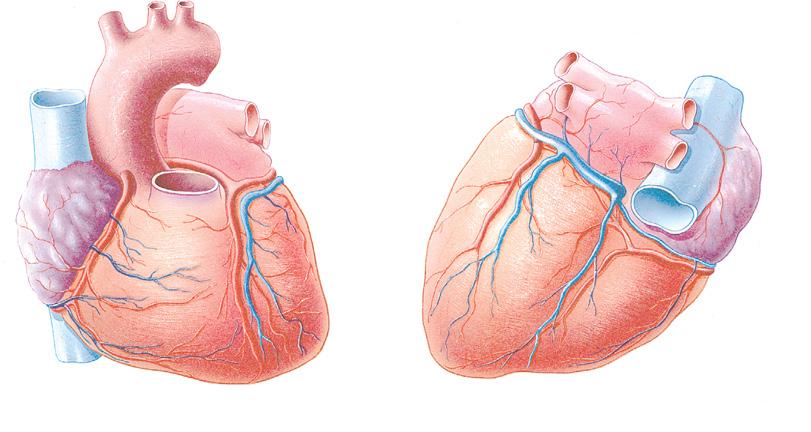
As the left coronary artery leaves the aorta, it immediately divides into the left anterior descending artery and the circumflex artery. The anterior descending artery is the major branch of the left coronary artery and supplies blood to most of the anterior part of the heart. A marginal branch of the left coronary artery supplies blood to the lateral wall of the left ventricle. The circumflex branch of the left coronary artery extends around to the posterior side of the heart, and its branches supply blood to much of the posterior wall of the heart. Each of these divisions has numerous branches that form a network of blood vessels, which in turn serve to provide oxygenation of designated portions of the myocardium.
The right coronary artery extends from the aorta around to the posterior portion of the heart. Branches of the right coronary artery supply blood to the lateral wall of the right ventricle. A branch of the right coronary artery called the posterior interventricular artery or posterior descending artery lies in the posterior interventricular region and supplies blood to the posterior and inferior part of the heart’s left ventricle. The right coronary artery branches also supply oxygen-rich blood to a portion of the electrical conduction system.
Coronary Sinus The coronary sinus is a short trunk that serves to receive deoxygenated blood from the veins of the myocardium. This trunk empties into the right atrium. (See Figure 1–7.)
Veins
Veins are blood vessels that carry blood back to the heart. Veins branch off into smaller vessels known as venules. With the exception of venules, veins are structurally similar to arteries in that they also have three layers. Unlike arteries, however, veins operate under low pressure, and are relatively thin-walled and contain one-way valves. With the exception of the pulmonary vein, the veins convey deoxygenated blood. The larger veins of the body ultimately empty into the two largest veins, the superior vena cava and the inferior vena cava, which empty deoxygenated blood into the heart’s right atrium. The superior vena cava drains blood from the head and neck, while the inferior vena cava collects blood from the rest of the body.
coronary sinus passage that receives deoxygenated blood from the veins of the myocardium veins blood vessels that carry blood back to the heart, operate under low pressure, and are relatively thin-walled superior vena cava drains blood from the head and neck inferior vena cava collects blood from the lower portion of the body
Coronary sinus
Figure 1–7. Coronary circulation
capillaries tiny blood vessels that allow for the exchange of oxygen, nutrients, and waste products between the blood and body tissues; connectors between arteries and veins
Capillaries
Capillaries are tiny blood vessels whose walls are the thinnest of all blood vessels. There is a greater number of capillaries in the human body than any other blood vessel. Capillaries are so tiny that red blood cells must pass through them in single file. From the arterioles, blood flows into the capillaries, where the vast majority of gas exchange occurs.
In summary, arterioles transport oxygenated blood into the capillaries. Capillaries allow for the exchange of oxygen, nutrients, and waste products between the blood and body tissues and are viewed as “connectors” between arteries and veins. The smallest of the veins, the venules, then receive the deoxygenated blood, which travels back to the heart via the venous system. (Refer to Figure 1–8 for the major veins and arteries of the circulatory system.)
Pulmonary vein
Superior vena cava
Pulmonary artery
Aorta
Inferior vena cava
Posterior tibial
Dorsal pedis
MAJOR ARTERIES
MAJOR VEINS
Carotid
Brachial
Femoral
Radial
Capillary bed
VeinArtery
Arterioles
Venules
Valve
Figure 1–8. Circulatory system
Summary
CHAPTER 1
This chapter has provided you the student with a simple yet comprehensive look at cardiac anatomy. A thorough understanding of cardiovascular anatomy is integral to appropriate dysrhythmia recognition.
Key Points to Remember
CHAPTER 1
1. The heart is located in the mediastinum.
2. The heart lies in front of the spinal column behind the sternum and between the lungs.
3. The apex (bottom) of the heart lies just above the diaphragm; the base of the heart lies at approximately the level of the third rib.
4. There are a total of four hollow chambers in the normal heart; on each side of the heart, there is an upper chamber, which is referred to as the atrium (atria, plural) and a lower chamber known as the ventricle.
5. Surrounding the heart is a closed, two-layered sac referred to as the pericardium, which is also known as the pericardial sac.
6. The epicardium accounts for the smooth outer surface of the heart.
7. The thick, middle layer of the heart is the myocardium and is the thickest of the three layers of the heart wall.
8. The innermost layer, the endocardium, is composed of thin connective tissue.
Review Questions
CHAPTER 1
1. When reviewing the layers of the heart, you will recall that the fibrous sac covering the heart, which is in contact with the pleura, is called the: a. epicardium. c. pericardium. b. myocardium. d. endocardium.
2. The heart chamber with the thickest myocardium is the:
a. right ventricle. c. right atrium. b. left ventricle. d. left atrium.
3. The pulmonic and aortic valves are open during: a. systole. c. cardiac cycle. b. diastole. d. systole and diastole.
9. The four valves of the heart allow blood to flow in only one direction.
10. The AV valves are located between the atria and the ventricles.
11. The AV valves allow blood to flow from the atria into the ventricles.
12. The semilunar valves serve to prevent the backflow of blood into the ventricles.
13. Arteries are relatively thick-walled and muscular in structure and function under high pressure in order to convey blood from the heart out to the rest of the body.
14. Veins are defined as blood vessels that carry blood back to the heart, operate under low pressure, are relatively thin-walled, and contain one-way valves.
15. Capillaries are tiny blood vessels whose walls are the thinnest of all blood vessels; they allow for the exchange of oxygen, nutrients, and waste products between the blood and body tissues. Capillaries are viewed as connectors between arteries and veins.
4. The large blood vessel that returns unoxygenated blood from the head and neck to the right atrium is called the:
a. jugular vein. c. superior vena cava. b. carotid artery. d. inferior vena cava.
5. The innermost layer of the arterial wall is called the: a. tunica intima. c. myocardium. b. tunica media. d. tunica adventitia.
6. The most numerous blood vessels in the body are the:
a. arteries. c. venules. b. capillaries. d. veins.
7. Blood flow between the heart and lungs comprises the:
a. systemic circulation.
b. venous circulation.
c. myocardial circulation.
d. pulmonary circulation.
8. Blood vessels that function under high pressure in order to convey blood from the heart out to the rest of the body are called:
a. venules. c. arteries.
b. veins. d. capillaries.
9. The blood vessel that returns unoxygenated blood from the myocardium to the right atrium is called the great cardiac vein or the:
a. jugular vein. c. coronary sinus.
b. carotid artery. d. inferior vena cava.
10. are fine chords of dense connective tissue that attach to papillary muscles in the wall of the ventricles.
a. Coronary arteries c. Chordae tendineae
b. Coronary sinuses d. Purkinje fibers
11. The right and left coronary arteries branch off of the:
a. coronary sinus.
b. right atrium.
c. left atrium.
d. trunk of the aorta.
12. The central section of the thorax is called the:
a. costal margin. c. diaphragm.
b. mediastinum. d. xiphoid.
13. The smooth outer surface of the heart is called the:
a. myocardium. c. endocardium.
b. epicardium. d. pericardium.
14. An inflammation of the serous pericardium is called:
a. myocarditis. c. pulmonitis.
b. pericarditis. d. tendonitis.
15. The coronary _______ is the short trunk that serves to receive deoxygenated blood from the veins of the myocardium.
a. artery c. sinus
b. fiber d. tissue
CARDIOVASCULAR PHYSIOLOGY (FUNCTION)
INTRODUCTION
Now that you have reviewed the structure of the heart, it is time to address the basic function (or physiology) of the cardiovascular system. The focus of this chapter is to provide you with an uncomplicated yet inclusive review of cardiac physiology. After you have mastered it, you will be prepared to move to the next chapter, which addresses the basic electrophysiology of the heart.
NOTE: Now is the perfect time to look back at the review questions from Chapter 1. Then proceed on through the objectives and contents of this chapter.
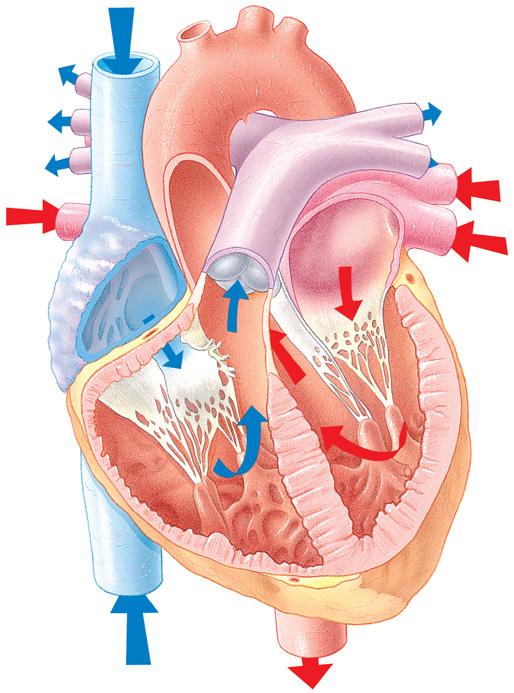
BLOOD FLOW THROUGH THE HEART
The path of blood flow through the heart is our first consideration in reviewing the knowledge of the physiology of circulation ( Figure 2–1 ). Imagine that the right atrium is a receptacle that functions, in part, to receive unoxygenated blood from the head, neck, and trunk. The right ventricle receives blood from the right atrium and pumps it to the pulmonary system. The left atrium receives oxygenated blood from the pulmonary system. The left ventricle receives this oxygenated blood from the left atrium and pumps it to the body system.
In order to simplify the route of circulation, you may choose to divide this concept into three components. The first component would consist of blood flow through the right heart. That is, unoxygenated blood flows from the inferior and superior vena cavae into the:
Right atrium Through the Into the right Through the tricuspid Ventricle pulmonic valve valve
2
OBJECTIVES
Upon completion of this chapter, you will be able to:
■ Describe the sequence of blood flow through the heart
■ Describe the cardiac cycle, including a. Definition b. Systole c. Diastole
■ Discuss the term stroke volume
■ Discuss cardiac output, preload, Starling’s Law, and afterload
■ Describe the autonomic nervous system
■ Discuss the two major divisions of the autonomic nervous system
Right atrium
Tricuspid valve
Right ventricle
Aorta
Pulmonary trunk
Left pulmonary arteries
Left pulmonary veins
Left atrium
Pulmonary valve
Mitral valve
Left ventricle
The second component of blood flow through the pulmonary circulation continues when the blood travels from the pulmonic valve into the:
Pulmonary Into the lungs Through the Into the arteries pulmonary Pulmonary alveolar-capillary Veins network
The third and final component of blood flow through the pulmonary circulation continues when the blood travels from the pulmonary veins into the:
Left atrium Through the Into the left Through the mitral valve ventricles aortic valve into the aorta and out to the systemic circulation