Critical Care EEG Basics-Rapid Bedside EEG Reading for Acute Care Providers (Feb 29, 2024)_(1009261169)_(Cambridge University Press) Jadeja
Visit to download the full and correct content document: https://ebookmass.com/product/critical-care-eeg-basics-rapid-bedside-eeg-reading-fo r-acute-care-providers-feb-29-2024_1009261169_cambridge-university-press-jadeja/
More products digital (pdf, epub, mobi) instant download maybe you interests ...
Neuroscience for Neurosurgeons (Feb 29, 2024)_(110883146X)_(Cambridge University Press) 1st Edition Farhana Akter
https://ebookmass.com/product/neuroscience-for-neurosurgeonsfeb-29-2024_110883146x_cambridge-university-press-1st-editionfarhana-akter/
12-Lead ECG for Acute and Critical Care Providers –Ebook PDF Version
https://ebookmass.com/product/12-lead-ecg-for-acute-and-criticalcare-providers-ebook-pdf-version/
Cases in diagnostic reasoning : acute & critical care nurse practitioner Burns
https://ebookmass.com/product/cases-in-diagnostic-reasoningacute-critical-care-nurse-practitioner-burns/
Practical Guide for Clinical Neurophysiologic Testing: EEG
https://ebookmass.com/product/practical-guide-for-clinicalneurophysiologic-testing-eeg/
Edition Hari https://ebookmass.com/product/meg-eeg-primer-2nd-2nd-editionhari/
Neurocritical Care (Pittsburgh Critical Care Medicine) Lori Shutter
https://ebookmass.com/product/neurocritical-care-pittsburghcritical-care-medicine-lori-shutter/
Rowan's Primer of EEG, 2e Second Edition Fields https://ebookmass.com/product/rowans-primer-of-eeg-2e-secondedition-fields/
The Oxford Handbook of EEG Frequency Philip Gable https://ebookmass.com/product/the-oxford-handbook-of-eegfrequency-philip-gable/
Medical-Surgical Nursing: Critical Thinking for Collaborative Care
https://ebookmass.com/product/medical-surgical-nursing-criticalthinking-for-collaborative-care/
CRITICAL CARE EEC BASICS ftipid Eedside EEG Readmg lor Acute Care Pttwiders
CriticalCareEEGBasics NevilleM.Jadeja UniversityofMassachusettsMedicalSchool
KyleC.Rossi
UniversityofMassachusettsMedicalSchool
ShaftesburyRoad,CambridgeCB28EA,UnitedKingdom
OneLibertyPlaza,20thFloor,NewYork,NY10006,USA 477WilliamstownRoad,PortMelbourne,VIC3207,Australia
314–321,3rdFloor,Plot3,SplendorForum,JasolaDistrictCentre,NewDelhi – 110025,India 103PenangRoad,#05-06/07,VisioncrestCommercial,Singapore238467 CambridgeUniversityPressispartofCambridgeUniversityPress&Assessment, adepartmentoftheUniversityofCambridge.
WesharetheUniversity’smissiontocontributetosocietythroughthepursuitof education,learningandresearchatthehighestinternationallevelsofexcellence.
www.cambridge.org
Informationonthistitle: www.cambridge.org/9781009261166
DOI: 10.1017/9781009261159
©NevilleM.JadejaandKyleC.Rossi2024
Thispublicationisincopyright.Subjecttostatutoryexceptionandtotheprovisions ofrelevantcollectivelicensingagreements,noreproductionofanypartmaytake placewithoutthewrittenpermissionofCambridgeUniversityPress&Assessment. Firstpublished2024
AcataloguerecordforthispublicationisavailablefromtheBritishLibrary.
LibraryofCongressCataloging-in-PublicationData
Names:Jadeja,NevilleM.,1986-author.|Rossi,KyleC.,author. Title:CriticalcareEEGbasics:rapidbedsideEEGreadingforacutecareproviders/ NevilleM.Jadeja,UniversityofMassachusettsMedicalSchool,Massachusetts, KyleC.Rossi,UniversityofMassachusettsMedicalSchool,Massachusetts. Description:Cambridge,UnitedKingdom;NewYork,NY:CambridgeUniversity Press,2023.|Includesbibliographicalreferencesandindex. Identifiers:LCCN2023031153(print)|LCCN2023031154(ebook)| ISBN9781009261166(paperback)|ISBN9781009261159(ebook)
Subjects:LCSH:Electroencephalography.|Criticalcaremedicine. Classification:LCCRC386.6.E43J332023(print)|LCCRC386.6.E43(ebook)| DDC616.8/047547–dc23/eng/20230817
LCrecordavailableat https://lccn.loc.gov/2023031153
LCebookrecordavailableat https://lccn.loc.gov/2023031154
ISBN978-1-009-26116-6Paperback
CambridgeUniversityPress&Assessmenthasnoresponsibilityforthepersistence oraccuracyofURLsforexternalorthird-partyinternetwebsitesreferredtointhis publicationanddoesnotguaranteethatanycontentonsuchwebsitesis,orwill remain,accurateorappropriate.
Everyefforthasbeenmadeinpreparingthisbooktoprovideaccurateandup-to-date informationthatisinaccordwithacceptedstandardsandpracticeatthetimeofpublication.Althoughcasehistoriesaredrawnfromactualcases,everyefforthasbeenmadeto disguisetheidentitiesoftheindividualsinvolved.Nevertheless,theauthors,editors,and publisherscanmakenowarrantiesthattheinformationcontainedhereinistotallyfree fromerror,notleastbecauseclinicalstandardsareconstantlychangingthroughresearch andregulation.Theauthors,editors,andpublishersthereforedisclaimallliabilityfordirect orconsequentialdamagesresultingfromtheuseofmaterialcontainedinthisbook.Readers arestronglyadvisedtopaycarefulattentiontoinformationprovidedbythemanufacturer ofanydrugsorequipmentthattheyplantouse.
NMJdedicatesthisbooktoShilpaDeshmukh.
KCRdedicatesthisbooktoMeganRossi.
Foreword TheEEG,oneoftheoldestdiagnostictoolsforevaluatingbrainfunction,has nowbeeninusefor100yearssinceitsinventionbyHansBerger.Therehas beenarenaissanceinEEGuseasameansofevaluatingandmonitoring criticallyillpatientsinthepast20years,madepossiblebyadvancesin computingandvisualizationtechnologies.Therefore,althoughEEGisarelativelyancienttool,itissimultaneouslyayoungfield.Inparticular,continuous EEGmonitoringintheICUhasmarkedlyimprovedthemanagementof neurocriticallyillpatients.
Thereareseveralcomprehensivetextbooks,handbooks,andatlasesdedicatedtocriticalcareEEGmonitoring,aswellasnewchaptersinclassicalEEG tomes.Thiscanbeparticularlyintimidatingtomedicalprofessionalswhose backgroundsarenotinclinicalneurophysiologyorepilepsy,butwhoare nonethelessexpectedtoutilizethesetoolsineverydaypractice.Practitioners maynotevenhavemorethanapassingfamiliaritywithEEGsthemselves.This iswherethenewbookbyNevilleJadejaandKyleRossibecomesavaluable assetinlearningcriticalcareEEGthatisbothefficientandpractical.
Thebookisshortenoughthatitcanbereadcover-to-coverwithinacouple ofdaysofconcertedeffort,evenlesswithsomefamiliaritywithEEGs. Nonetheless,itiscomprehensiveenoughthatitshouldcovermostofthe commonscenariosencounteredbycaretakersofthecriticallyillpatients.The bookintroducesthebasicsofEEGrecordings,whenandhowtoorderanEEG, andtheimportanceofrecognizingandaccountingforrecordingartifactsand medicationeffects.ThecoreprinciplesofcriticalcareEEGs – rangingfrom interictalepileptiformdischargestorhythmicandperiodicdischarges,the ictal–interictalcontinuum,seizures,andstatusepilepticus – arewellcovered. Aspecialemphasisisplacedonpost-cardiac-arrestEEGs,whicharedistinct frommostothercriticalcareEEGs,andencephalopathy,whichisencountered inthemajorityofpatientsundergoingcriticalcareEEGs.AsallmodernEEG systemshavequantitativeEEGtools,thistopic,too,isgivenspecialconsideration,ratherthandetailedanalysis,whichcanonlybeseenunderscrutinyin retrospect.
Thereisaverylargeaudiencewhowouldbenefitfromreadingthisbook: theEEGtechnologists,nurses,advancedpracticeproviders,non-neurology criticalcarephysicians,andevenneurocriticalcarephysicianswithoutspecializedtraininginclinicalneurophysiology.Oneofthekeystrengthsofthisbook liesinitscomprehensivecoverageofthelateststandardterminologyasestablishedbytheAmericanClinicalNeurophysiologySociety.Thisterminologyis nowacornerstoneinthefield,adoptedbynearlyallcontemporaryclinical
neurophysiologists.Additionally,thebookdescribesthestructureofthereports generatedinthisdiscipline,enhancingthecommunicationbetweenthecare teamandtheclinicalneurophysiologist.Thisensuresamorestreamlinedand effectiveexchangeofinformation,crucialforoptimalpatientcare.Icannot emphasizehowcriticalthiscommunicationisinthecareofthesepatients,and Icanthinkofnobetterwaytoquicklylearnthislanguagethanthroughthis veryuseful,readable,well-illustratedbook.IwarmlycongratulateDrsJadeja andRossionproducingthisoutstandingwork.
JongWooLee,MD,PhD
AssociateProfessorofNeurology,HarvardMedicalSchool DepartmentofNeurology,BrighamandWomen’sHospital
Preface Electroencephalograms(EEG)arecommonplaceinacutecareenvironments suchasemergencyrooms,intensivecareunits,andhospitalfloors.Criticallyill patientswithalteredmentalstatusareatahighriskofseizures,whichmay occurwithoutclinicallyapparentconvulsions(nonconvulsiveseizures)and thereforecanonlybediagnosedonEEG.Delayinthedetectionandtreatment ofcontinuousseizures(statusepilepticus)isassociatedwithrefractorinessto therapyandsecondaryneurologicalinjury.Additionally,theEEGmayhelp confirmencephalopathy,gradeitsseverity,characterizeparoxysmalevents, andtitrateanestheticsandsedation,amongotherindications,incriticallyill patients.
However,mostacutecareproviders(includingmanyneurologists)are unfamiliarwithcriticalcareEEGdespiteeasyavailabilityandwidespreaduse. WithoutconfidentbedsideEEGreadingskills,theyaredependentonofficial reportsorremoteinterpretations,whichcanbedifficulttounderstandornot immediatelyavailableforreview.Thispocketbookintroducesthereadertothe basicsofcriticalcareEEGwithanemphasison real-timebedsideEEGreading
TailoredspecificallyforacutecareproviderswithoutanEEGbackground, thisbookallowsreadersofallskilllevelstobecomefamiliarwithcommon criticalcareEEGpatternsandwhattheymeanandwhattodoaboutthem. Withpractice,quickandeasybedsideEEGreadingwillbecomeapowerful extensiontoyourneurologicalassessment.Wehopethatthisuniquebook, whichiseasytounderstandandheavilyillustrated,willhelpyoutoharnessthe immensepotentialofthisfascinatingtestinordertobesthelpyourpatients.
Acknowledgments ThisapproachborrowsheavilyfromthoseofourteachersattheBrighamand Women’sHospitalandBethIsraelDeaconessMedicalCenter,Harvard MedicalSchool.WealsogratefullyacknowledgeourcolleaguesatUMass MemorialMedicalCenter,UMassChanMedicalSchool,includingDon Chin;FeliciaChu,MD;IkaNoviawaty,MD;MugdhaMohanty,MD;and BrianSilver,MD.Lastbutnotleast,wethankCatherineBarnes,Kim Ingram,BethSexton,RuthSwan,MarijasinthaSrinivasan,andtheteamat CambridgeUniversityPressformakingthisworkpossible.
HowtoReadThisBook Thisbookhastwopartsthatshouldbereadsequentially:
PartI(Introduction) describesthebasicsofEEG(emphasizingcriticalcare EEG).Additionally,itincludesclinicalindicationsforEEG,anapproachto rapidbedsideEEGreading,howtorecognizeartifactandmedicationeffects, howtoexplainrhythmicorperiodicpatterns,andtheincreasinglyrelevant conceptoftheictal-interictalcontinuum(IIC).Italsodescribeshowto diagnoseseizuresandstatusepilepticusaswellaspost–cardiacarrestpatterns andquantitativeEEG.
PartII(Case-BasedApproachtoSpecificConditions) describesanapproach tospecificcommonlyencounteredICUconditionsusingcase-basedclinical reasoning.Eachcaseconsistsofashortclinicalvignettethatincludesabrief clinicaldescription,sampleEEG,andwhattodonextwithrelevantclinical reasoning.Thisprovidesadirectpracticalapproachtocommoncriticalcare EEGpatterns.
Finally,thereisanappendixaboutunderstandingEEGreports.Thisexplains thecommonpresentationandmeaningoftermsusedinanEEGreportfor acutecareprovidersofallspecialties.
EEGBasics Chapter 1 Introduction ◾ HowEEGsarerecorded
◾ Threerulesofpolarity
◾ PartsofanEEGmachine
◾ Electrodes
◾ Montagesandlocalization
◾ Display
◾ Frequency
◾ Rhythm
◾ NormaladultEEG
◾ StrengthsandlimitationsofEEG
Thischapterintroducesthebasicconceptsofelectroencephalography(EEG) recording,withwhichreadersneedtobefamiliarbeforeadvancing.Specifically tailoredtoacutecareproviders,itassumesthatmostreadersdonothaveprior EEGreadingexperience.Therefore,theneurophysiologyhasbeensimplifiedto the “barebasics.” Thischapterisintendedasafoundationtounderstand furtherconceptsdescribedinthisbook;itcannotserveasadetailedreference, forwhichmanyexcellenttextbooksareavailable.
HowEEGsAreRecorded Electroencephalographs(EEGs)aregraphicalrepresentationsofcontinuous synapticactivityofthe pyramidalneurons inthesuperficialcortex.These neuronsarearrangedradially,likespokesofawheel,withtheirsuperficial endstowardsthecorticalsurface.Eachneuronalsofunctionsasadipole,with eachofitstwoendscarryingasmallbutopposingcharge.Summationsoftiny superficialchargesformcorticalpotentials.Electrodesplacedonthescalpcan measurethepotentialoftheunderlyingcorticalregion.
Whenelectrodesarepaired,thepotentialdifferencebetweentwo electrodes(V)causesasmallcurrent(I)tomoveacrosstheresistanceof thecircuit(R)governedby Ohm’slaw (V=I×R).Thestrengthand directionofthecurrentarecomputedbytheEEGmachineanddisplayed asawaveformovertime.Inputsfro mdeeperstructures,suchasthe thalamus,synchronizecorticalneuronalactivitytogeneratepatternsof electrographicactivitycalledrhythms.
Sincesynaptictransmissionoccursconstantly,thenormalEEGisalways continuous.Disruptionstoneuronalfunctionandsynaptictransmissionwill
leadtobreaksintherecording(discontinuity).Therefore,discontinuityindicatescorticalneuronaldysfunction.
ThreeRulesofPolarity TheEEGscreenshowsanarrangementofchannels,eachshowingalinewith waveforms.Each channel consistsoftwoelectrodesthatrecordtheelectrical potentialfromtheirunderlyingregionofcortex.TheEEGmachinethen computesthepotentialdifferencebetweenthosetwoelectrodesanddisplays itasawaveform.
Threesimplerulesofpolaritygoverntheappearanceofeachwaveform. Consider,forexample,asingleEEGchannel,sayD1-D2.Thisiscomposed ofscalpelectrodesD1andD2,eachsamplinganareaofunderlyingcortex. Dependingontheirarrangement,theymaylieadjacenttoordistantfrom another.TheappearanceofawaveforminchannelD1-D2willdependonthe relativedifferenceinelectricalpotentialsatelectrodeD1andelectrodeD2(i.e., D1 D2).Thegreaterthedifference,thehighertheamplitude(voltage). Further,thedirection(polarity)ofthewaveisdeterminedasfollows:
• Rule1:IfpotentialatD1islessthanD2(i.e.,D1 < D2orD1isrelatively negative),theirdifferenceisnegative – reflectingasanupwarddeflection.
• Rule2:IfpotentialatD1isgreaterthanD2(i.e.,D1 > D2orD2isrelatively negative),theirdifferenceispositive – reflectingasadownwarddeflection.
• Rule3:IfbothD1andD2areequipotentialorinactive,thentheirdifference isneutral – thereisnodeflection.
Asyoucansee,thepointersimplydeflectstotherelativelysmaller(i.e.,more negative,orlesspositive)electrodepotentialasshownin Figure1.1.
PartsofanEEGMachine AtypicalEEGrecordingconsistsofelectrodes(fixedtothepatient’sscalp), eachofwhichisconnectedbywiretoaheadbox.Theheadboxispluggedinto aportablecomputerwithadisplayscreen.Itcanbeeasilyunpluggedto temporarilydisconnecttherecordingfortransport.
Electrodes Thesearesmall,circular,dome-shapedmetallicdiscsperforatedbyasmallhole ontheirtop.Theyareappliedtothescalpusingglueorcollodion.Collodionis extremelyflammableandemitsanoxiousodor,butformsstrong,sweatresistant,anddurableconnections,usefulforcontinuousEEG.
Electrodesaremadeofparamagneticmaterialssuchasstainlesssteelortin andcoatedwithsilverorsilverchloride.MRIconditionalelectrodesare alsoavailable.
Singleuseelectrodesshouldbeusedinpatientswithsuspectedprion disease(e.g.,Jakob–CreutzfeldtDisease)[1].
ApplicationofElectrodes First,theelectrodeisdippedinanadhesivepasteandthenplacedonprepared skin.Next,agauzesoakedincollodionisplacedovertheelectrodeandair driedtoformdurableconnections.Finally,eachelectrodeisfilledwithelectroconductivegelthroughthesmallholeonthetopofitsdomeusingablunt needleandsyringe.Thisensuresanadhesiveelectricalconnection.
PlacementofElectrodes Electrodesareplacedusingthe standardizedinternational10–20system.This systemusesthreebonyanatomicallandmarksofthescalptoformaflexible map.Theseincludethenasion(centerofthenosebridge),inion(centerofthe occipitalprominence),andpreauricularpoint(justinfrontofthetragus). Pointsforelectrodeplacementareselectedatapproximationsofeither10% or20%ofthedistancebetweenthelandmarksasshownbelow.
Eachelectrodeisreferencedbyaletterrepresentingtheunderlyingregion ofcortex(e.g.,frontopolar(Fp),frontal(F),temporal(T),parietal(P),occipital (O),orcentral(C)),andanumber – even(2,4,6,8)forright,odd(1,3,5,7) forleft,andZforthemidline(Fz,Cz,andPz).Forexample,Fp1isfortheleft frontopolarelectrode,etc.
Acommonadaptationcalledthemodifiedcombinatorialnomenclature usesT7forT3,T8forT4,P7forT5,andP8forT6[2].Thisbringsthenames oftheseelectrodesinlinewiththemoreextensive10–10system,whichusesfar moreelectrodes. Figures1.2(a) and 1.2(b) showtheplacementofelectrodes usingtheinternational10–20system.
Figure1.2(a) International10–20system; topview.
MontagesandLocalization Montages Figure1.2(b) International10–20system; sideview.
Channels(electrodepairs)aredisplayedontheEEGscreenusingspecific arrangements.Thesespecificarrangementsarecalled montages. Therearemanydifferenttypesofmontages,detaileddescriptionsofwhich arebeyondthescopeofthisbook.However,acutecareprovidersshouldbe familiarwithusingalongitudinalbipolar(doublebanana)montage,asthisisa commondefaultmontageandeasytouseatthebedside.AllEEGexamplesin thisbookusethismontage.
Eachchannelofalongitudinalbipolarmontageshowsthepotentialdifferencebetweentwoadjacentelectrodesonthescalp,andisconnectedtoother channelsinlongitudinal(fronttoback)chainsasshownbelow[3].
Figure1.3(a) showsanexampleofthelongitudinalbipolarmontage,while Figure1.3(b) showsaschematicrepresentationofitselectrodechains.
Localization Thisistheartofapproximatingthelocation(origin)ofawaveformonthe corticalsurface.
Ideally,differenttypesofmontagesshouldbeusedtogetherduringlocalization,butthiscanbechallengingatthebedside.Therefore,welimitourselves heretousingthelongitudinalbipolarmontage.
Thekeytolocalizationisanelectrographicprinciplecalleda phasereversal. ThisisasimultaneousbutoppositedeflectionintwoadjacentEEGchannels containingacommonelectrode.Aphasereversalimpliesthatthecortical potentialismaximalatthelocationofthecommonelectrode.
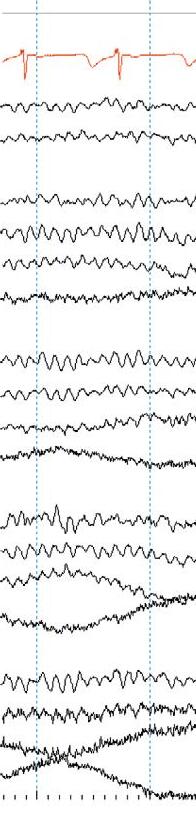
Mostphasereversalsarenegative(><),thoughrarelypositivephase reversals(<>)mayoccur. Figure1.4 showsanexampleoflocalizingafocal sharpwave.
Left temporalchain Right temporalchain Left parasagittalchain Right parasagittalchain Midlinechain ECG
Figure1.3(a) EEGinlongitudinalbipolarmontage.
nasion inion LEFT RIGHT A1 A2 Figure1.3(b) Longitudinalbipolarmontageelectrodechains.
Display(Parameters) Atypicalbedsidedisplayusingalongitudinalbipolarmontageisshownin Figure1.3(a). Variationstothisformatexist.Commonly,theleftandtheright temporalchainsarestackedtogetherfollowedbytheleftandrightparasagittal chains.Thismakesiteasytocomparethetemporalandparasagittalregionsof bothhemispheresforasymmetry.Readersshouldknowthatthetemporal regionsarealsothemostepileptogenicsofocusingonthesechannelsyields results!Thetopbarofarecordingshowsthesensitivity,filtersettings,and timebase.
Sensitivity (µV/mm)isthemagnificationofEEGactivity.Thelowerthe value,thehighertheamplitudeofthewaveformonthescreen.MostEEGsare displayedatasensitivityof7µV/mmasadefaultsetting.
Frequencyfilters aimtoreduceartifactornoise.Thethreecommontypes offiltersarehighfrequencyfilter(HFF),lowfrequencyfilter(LFF),andnotch filter(60Hz).
◾ Highfrequencyfilters(HFF)screenoutfrequenciesgreaterthantheir settingandallowlowerfrequenciestopass(lowpass).Theyare particularlyusefultofilteroutmyo genic(muscle)artifactbutmayalter theunderlyingactivitytolookfalselysharper.TheHFFisusuallyset at70Hz.
◾ Lowfrequencyfilters(LFF)screenoutfrequencieslowerthantheirsetting andallowhigherfrequenciestopass(highpass).
◾ Notchfiltersarespecifictoscreenout60Hzartifact.
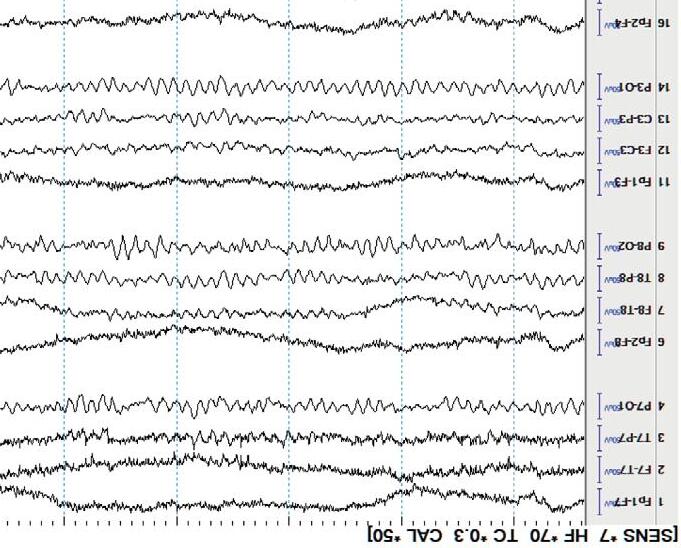
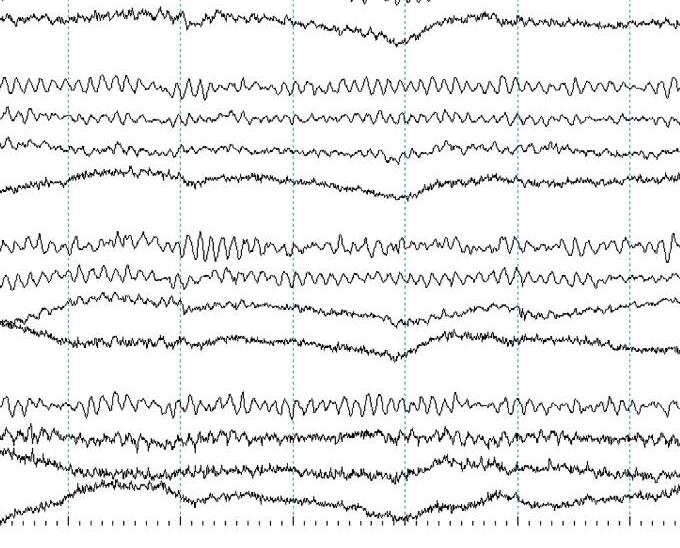
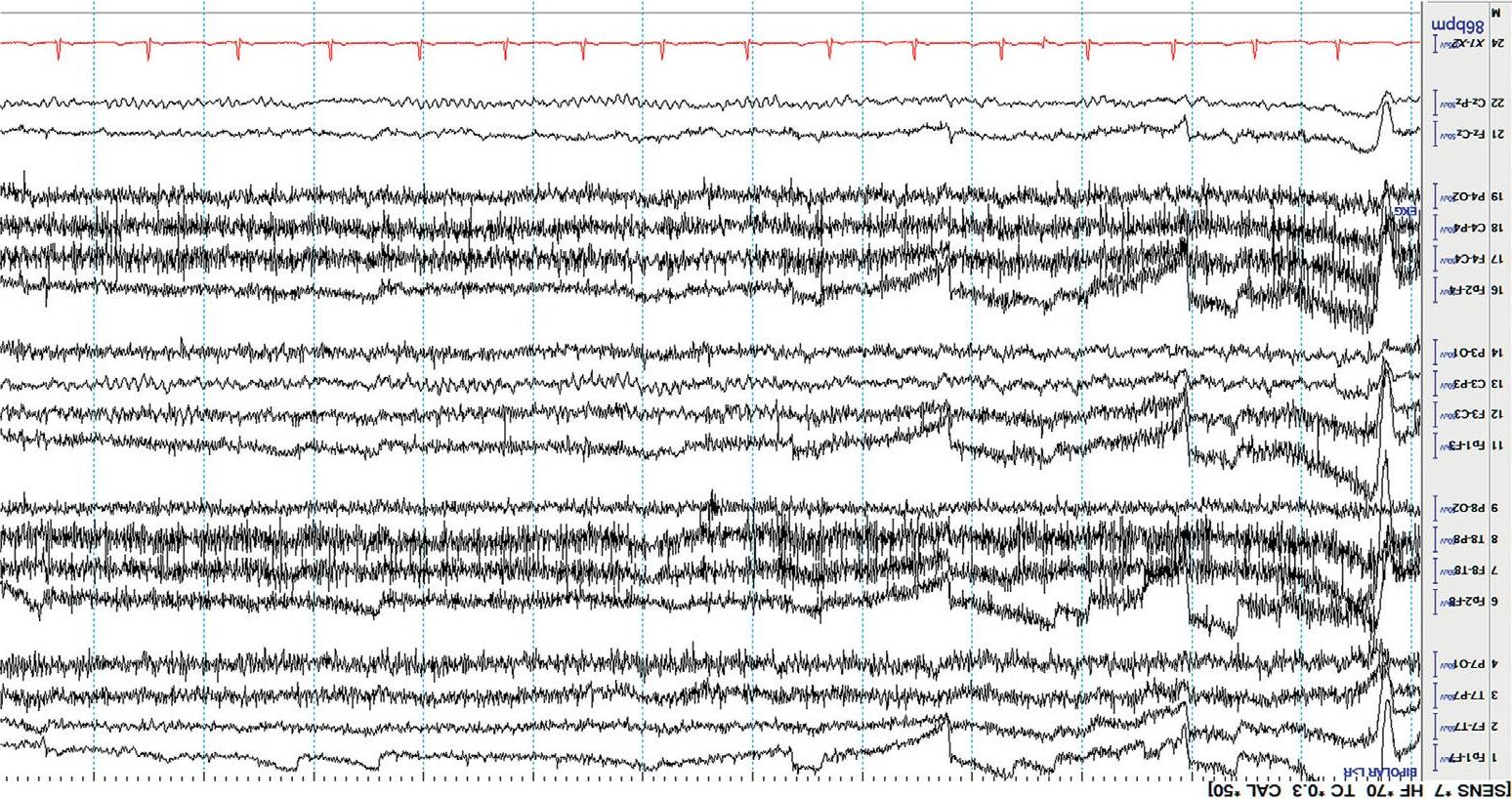
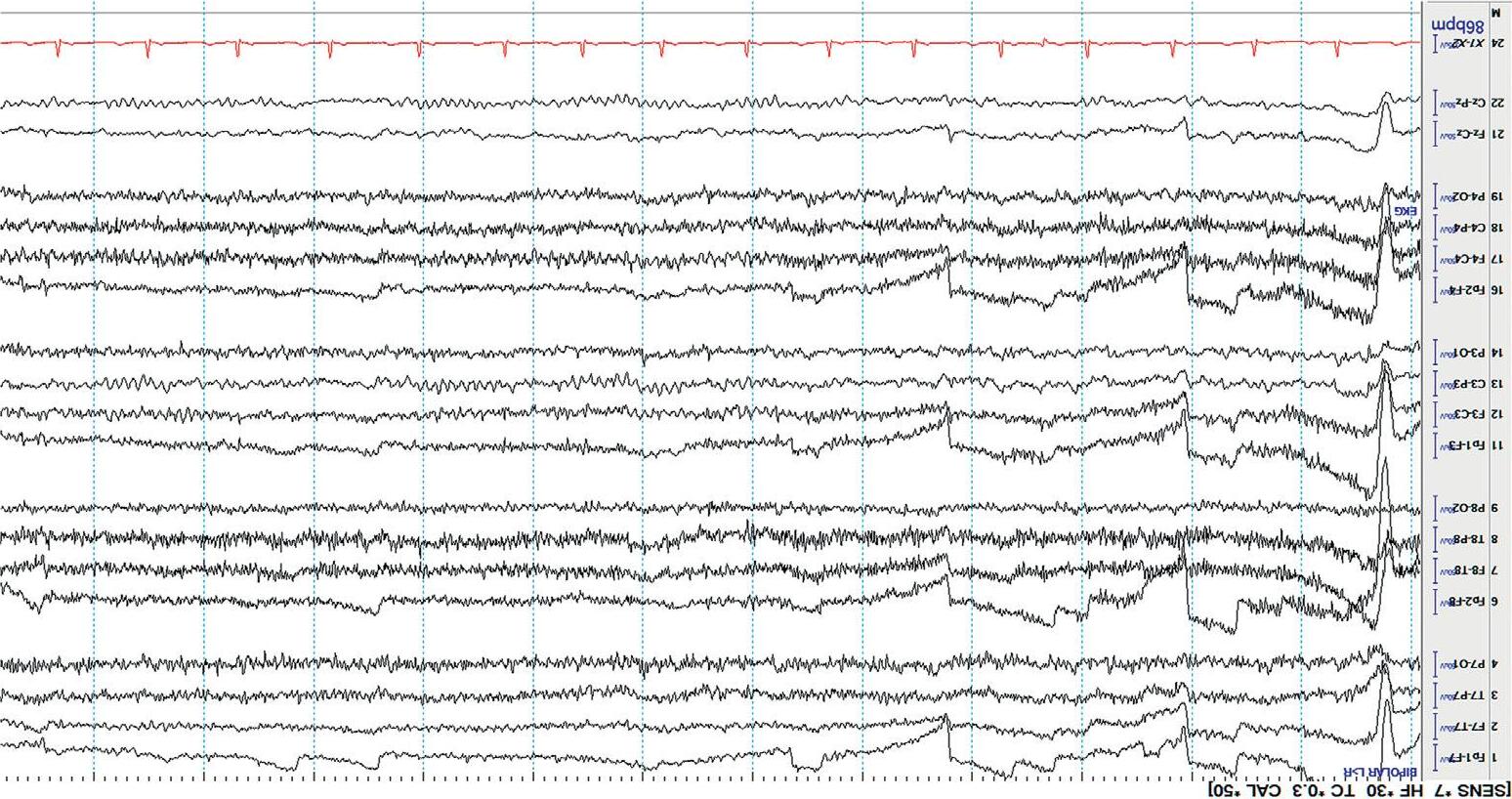
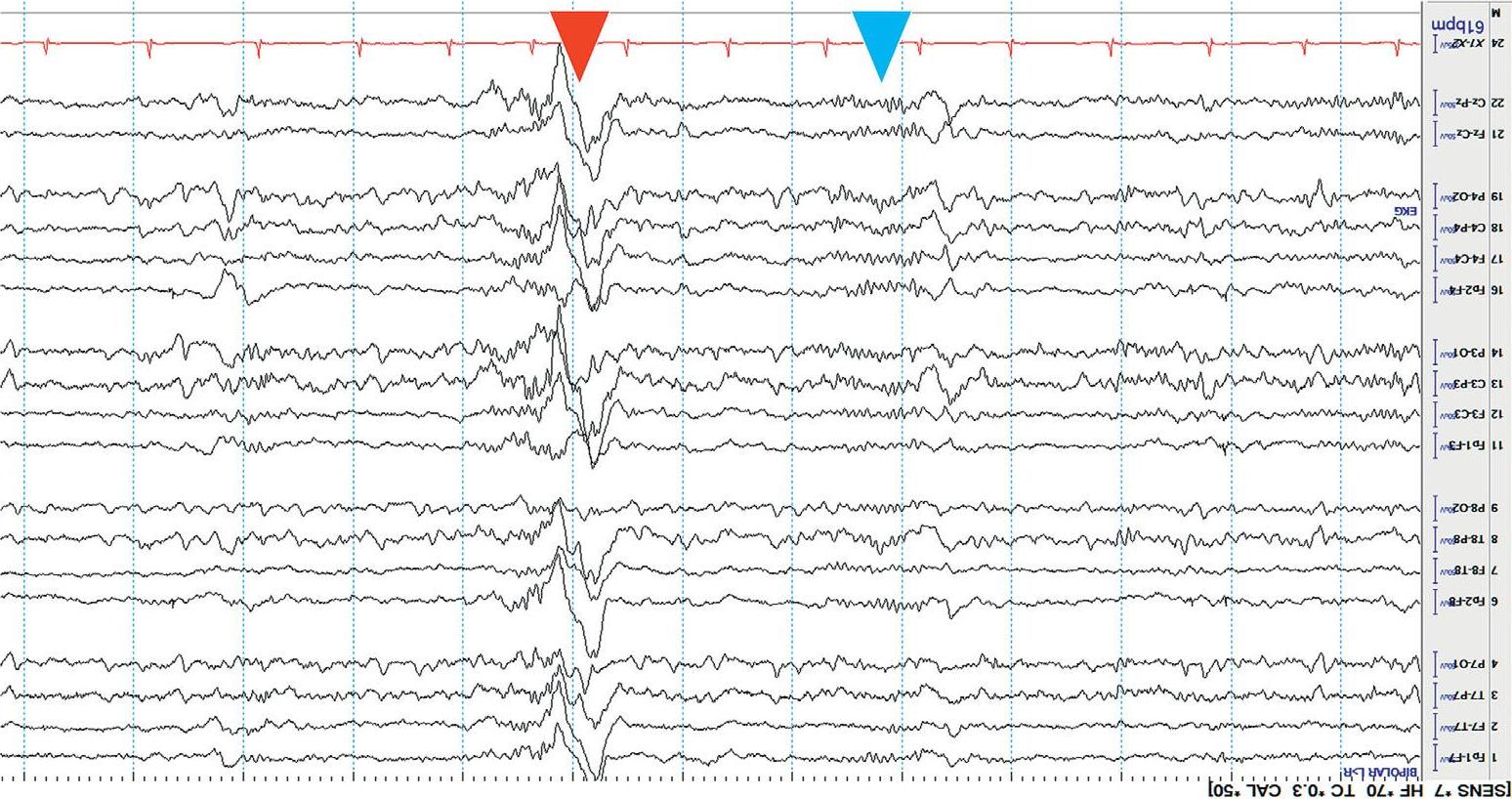
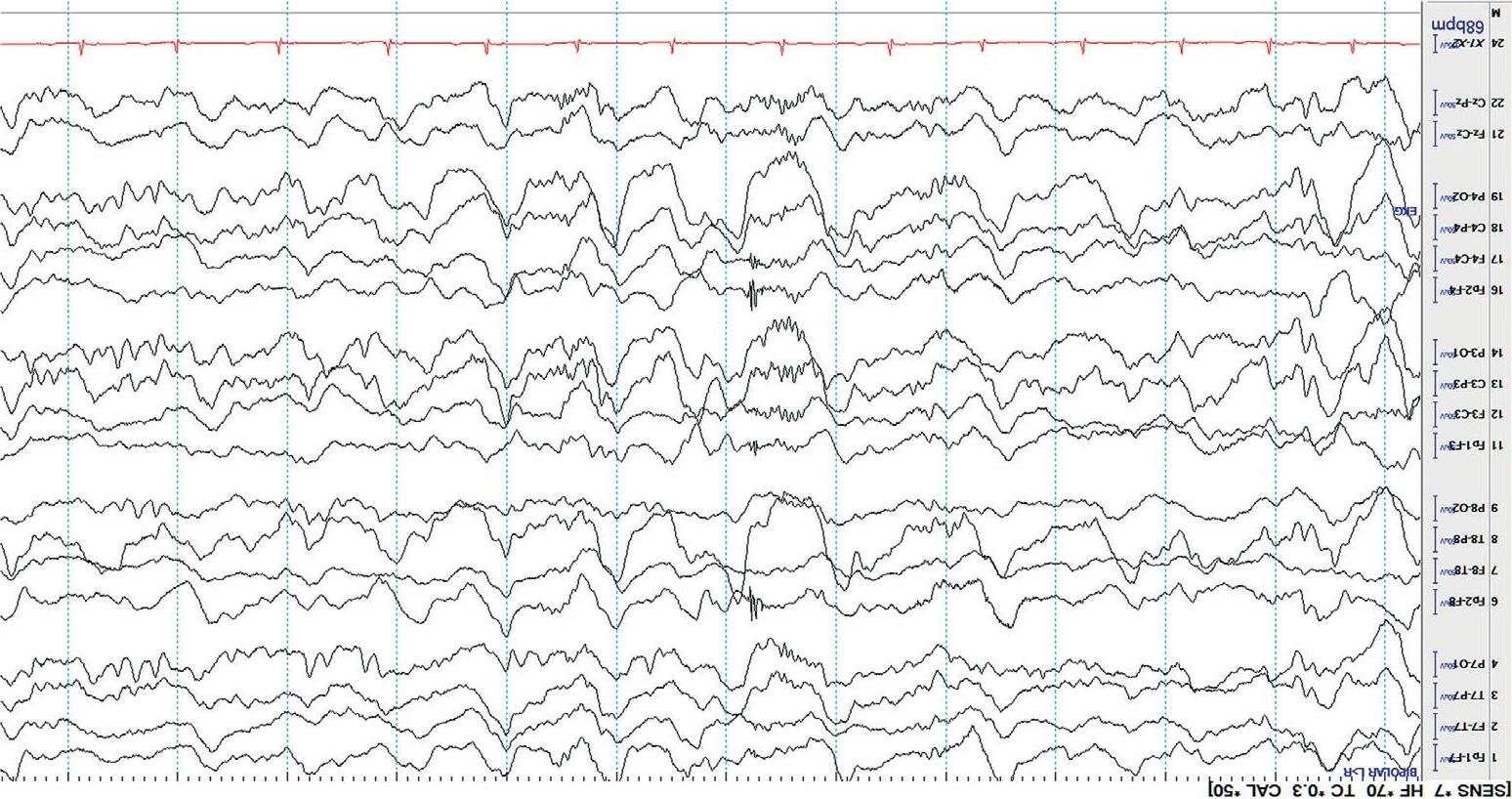
Mostdisplaysshow10or15secondsperpageofEEG. Figure1.5 showsa typicaldisplayusingthelongitudinalbipolarmontagewithexcessivemuscle artifactbefore(a)andafter(b)applicationof30Hzhighfrequencyfilter.
Frequency Thisreferstothenumberofwavesoccurringpersecond.Itismeasuredin hertz(Hz).Forexample,ifarhythmicwavepatternoccurseverysecond,its frequencyis1Hz.
Activitycanbeeasilydescribedbasedonincreasingorderoffrequencyas follows:
◾ Deltarange(1–4Hz)
◾ Thetarange(5–7Hz)
◾ Alpharange(8–13Hz)
◾ Betarange(>13Hz).
Rhythm Thisreferstoanelectrographicpatternthatnotonlyhasaregularfrequency,butalsoaspecificshapeandlocation.Whilefrequencyismerelya descriptiveterm,rhythmsindicatenormalorpathologicalsignificance – i.e., isitanormalorabnormalpattern?
Forexample,the “alpharhythm” (a.k.a.posteriordominantrhythm)isan electrographichallmarkofnormalwakefulness.
NormalAdultEEG Thenormalbackgrounddependsonthephysiologicalstate:awake,drowsy, orasleep.
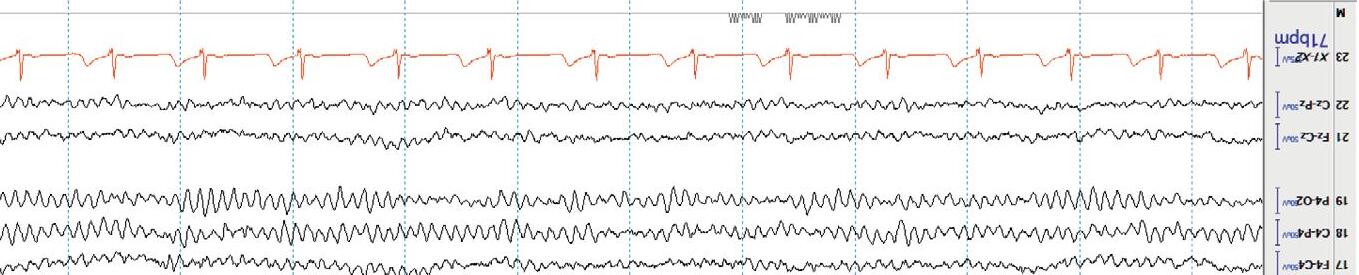
Awake Lookforthe alpharhythm(posteriordominantrhythm,PDR).Thisisthe 8.5 – 13Hz(alpharange)rhythm,maximalintheposteriorheadregions, thatattenuateswitheyeopening(anindicationofreactivity).Thealpha rhythmisanobviousfeatureofnormalwakefulnessandisbestobserved aftereyeclosureintheoccipitalchannels(O).Loweramplitude beta activity occursanteriorly.Anyintrusionofthetaordeltaactivityduringfull wakefulnessisusuallyindicativeof anabnormality.Furthermore,theamplitudeofthebackgroundactivityshouldnormallydecreasefromposterior (O)toanterior(Fp).Thisiscalledthenormal anterior –posterior(AP) gradient .Additionally,therewillbeartifactfrom eyeblinks and muscle activityinthefrontalisandtemporalismuscles. Figure1.6 showsanEEG duringnormalwakefulness.
Figure1.4 Localizingasharpwave(blackarrow)throughphasereversaltoelectrodeP8(blackcircle).
Figure1.5(a) EEGwithHFFsetto70Hz.
Figure1.5(b) ThesameEEGwithHFFsetto30Hz.
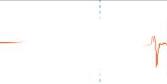
Drowsy Asthepatientbecomesdrowsy(N1sleep),the alpharhythmscanslowand becomemoreintermittent,thebackground amplitudedecreases,the frequencyslows,and slowlateral(“ roving ”)eyemovements canappear. Eyeblinksandmuscleartifactdisappear. Figure1.7 showstheEEG duringdrowsiness.
Sleep
Lightsleepshowsfurtherslowingofthebackgroundfrequencies. StageN2 sleep isidentifiedbythepresenceof sleepspindles and K-complexes.Sleep spindlesaretransient,frontocentralpredominant,spindle-shapedburstsof 12– 16Hzactivity,whileK-complexesarecomposedofahighamplitude, centrallypredominant,generalizedwave,oftenfollowedbyabriefburstof spindleactivity. Figure1.8(a) showsstageN2sleep.
StageN3or slowwavesleep ischaracterizedbyhighamplitude,generalized,semirhythmicdeltaslowing[ 4].Rapideyemovement(REM)sleepis seldomseenintheICU. Figure1.8(b) showsstageN3orslowwavesleep.
StrengthsandLimitationsofEEG Strengths TheEEGisanoninvasiveandeasilyavailabletesttoevaluatecorticalfunction.Further,ithasexcellenttemporal(time)resolution.Thismeansthat thoughitisnotnearlyasgoodasneuroimaginginpointingtothelocationof problems(lowspatialresolution),itcanalmostimmediately(inmilliseconds) detectanyalterationofcorticalfunction.
Additionally,EEGaccompaniedbyvideorecordingremainsthegold standardtestforthediagnosisofseizures.
Limitations Relativelylowspatialresolutionaside,EEGhasotherlimitations.Ithaspoor resolutionforneuronalactivitiesthatarisefromdeeperstructuresofthe brainsuchasthesulcaldepths,theinsulae,aswellasbasalandmesial structures.Remember,thecortexisdeeplyenfoldedandmostofitdoesnot lieonthesurface!
Further,corticalpotentialsmeasuredatthescalparetiny(oftenonlya fewmicrovolts)duetothedampeningeffectofthickskullbones,fluid,and fascia.Therefore,asizeableregionofcortexmustbeinvolvedtoproduce scalpsignals(bysomeestimates,around6 – 10cm2 ).Forthisreason,smaller
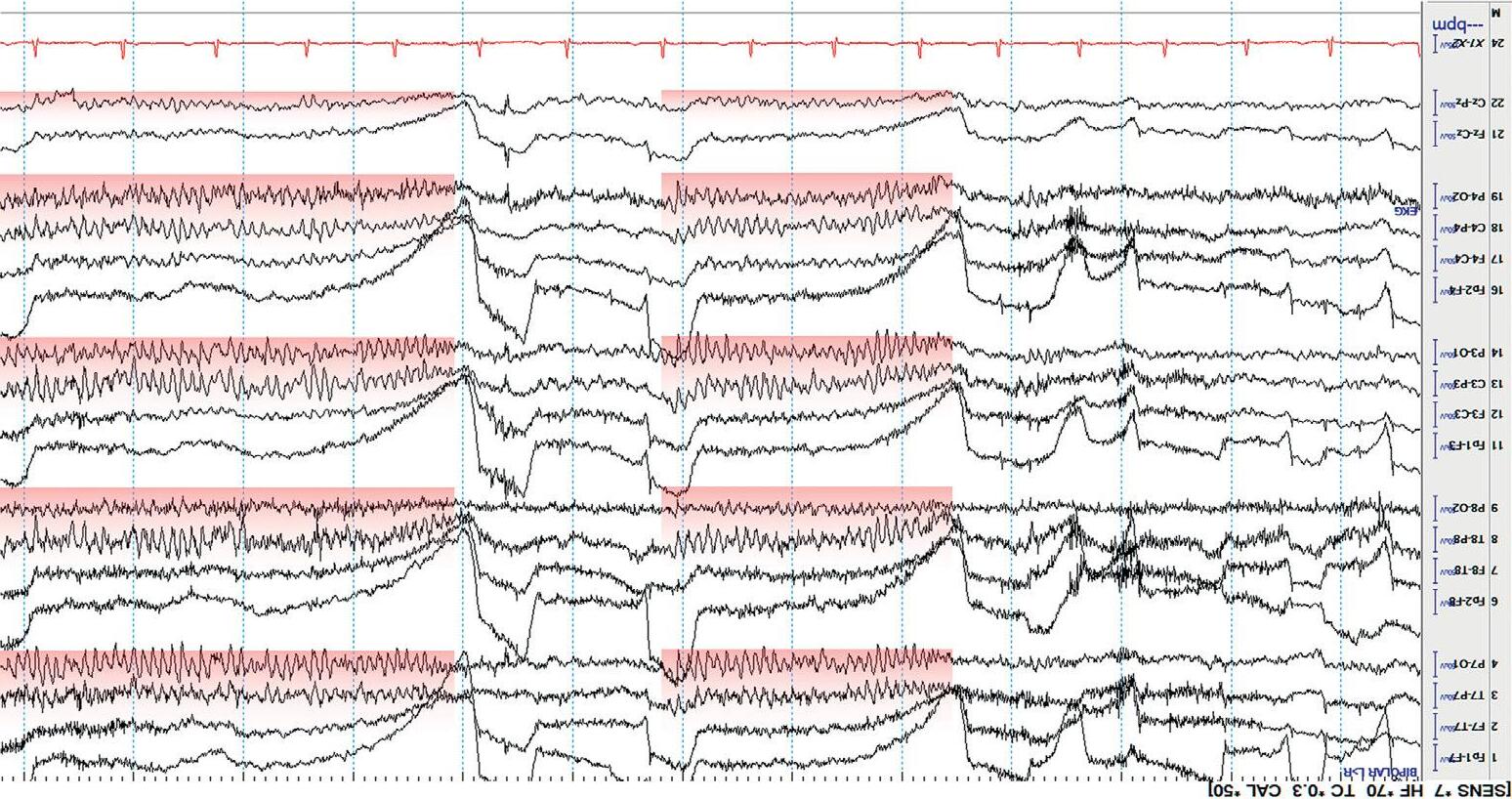
Figure1.6 NormalawakeEEG;thePDRishighlightedinred.
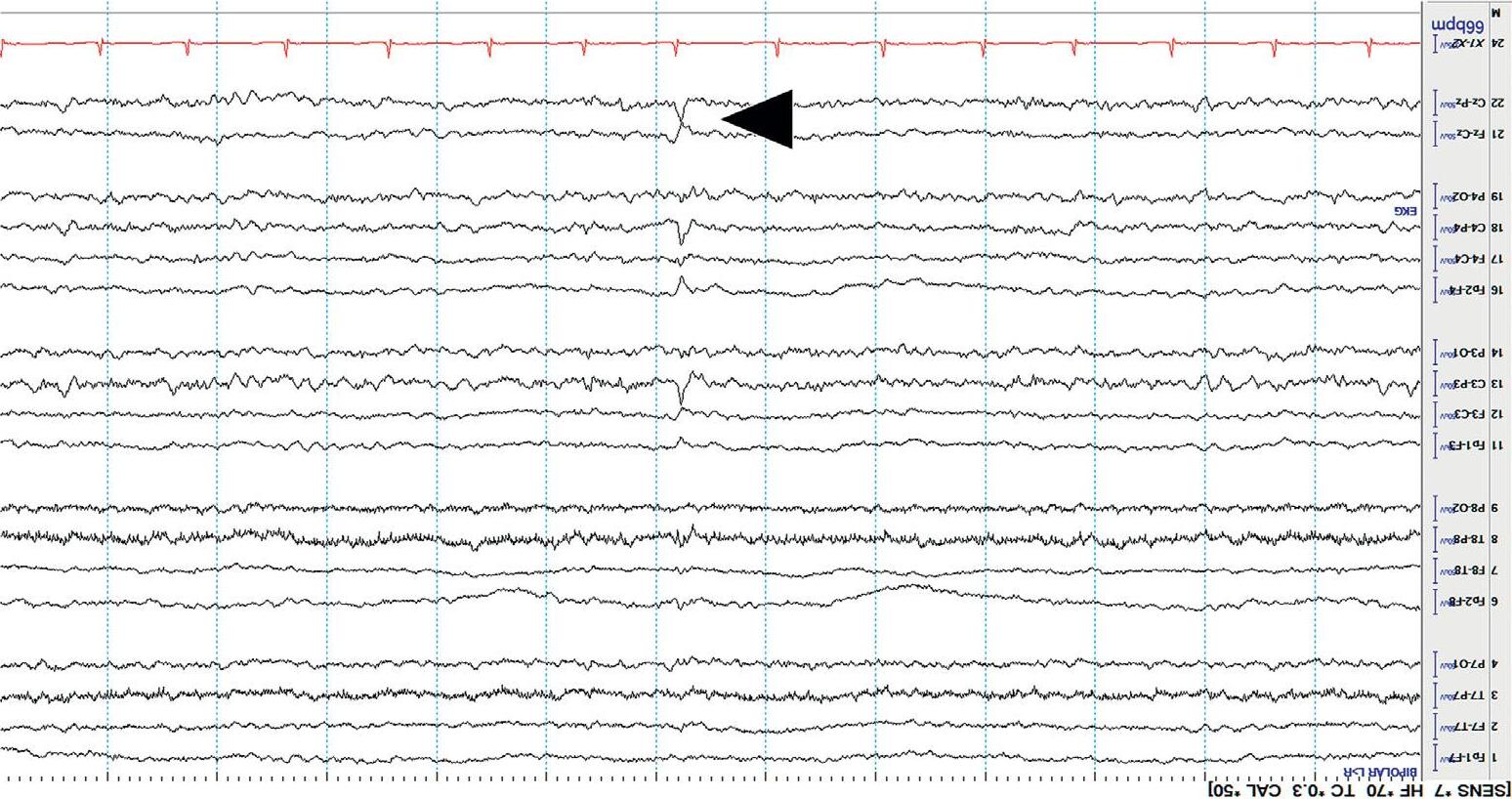
Figure1.7 NormaldrowsyEEG;blackarrowmarksanormal “vertexwave.”
Figure1.8(a) NormalstageN2sleep;thebluearrowmarksanormalsleepspindle,andtheredarrowmarksanormalK-complex.
Figure1.8(b) NormalstageN3sleep(slowwavesleep).
fociofactivity,suchasseizureonsets,maynotalwaysbedetectedonscalp recordings.However,theymaystillleadtoclinicalmanifestationssuchas epilepticauraorfocalmotorseizures.Generally, ifawarenessisimpaired (e.g.,unresponsivenessduringa seizure),thentheEEGisabnormal .Thisis likelybecausealargeregionofcorticaldysfunctionisrequiredforan impairmentofawareness.
References
1.EggenbergerE.Priondisease. NeurologicClinics. 2007Aug1;25(3):833–42.
2.AcharyaJN,HaniAJ,CheekJ,Thirum alaP,TsuchidaTN.AmericanClinical NeurophysiologySocietyGuideline2:GuidelinesforStandardElectrodePosition Nomenclature. TheNeurodiagnosticJournal. 2016Oct1;56(4):245– 52.
3.AcharyaJN,HaniAJ,ThirumalaP,TsuchidaTN.AmericanClinical NeurophysiologySocietyGuideline3:AProposalforStandardMontagesto BeUsedinClinicalEEG. TheNeurodiagnosticJournal. 2016Oct1;56(4):253– 60.
4.TatumIVWO,HusainAM,BenbadisSR,KaplanPW.NormaladultEEGand patternsofuncertainsignificance. JournalofClinicalNeurophysiology. 2006Jun 1;23(3):194 – 207.
PartI Chapter 2 Introduction Indications ◾ WhentorequestanEEG
◾ LimitationsofcriticalcareEEG
◾ Continuousvs.routineEEG
◾ Durationofmonitoring
◾ AdvantagesofbedsideEEGreading
ThemostimportantindicationforEEGincriticallyillpatientsistoevaluate fluctuatingorpersistentlyabnormalmentalstatus(orotherfocalneurological deficits)thatcannototherwisebeexplained.Commonly,thesesymptomsarea manifestationofphysiologicaldiffusecerebraldysfunction(encephalopathy), ortheymaybeduetoseizureactivitywithoutapparentclinicalmanifestations. Such “nonconvulsive” seizures(NCS),thatmayonlybedetectedbyEEG,occur inatleast8–10%ofcriticallyillpatients[1].ContinuousorfrequentNCSare callednonconvulsivestatusepilepticus(NCSE)andmayresultinsecondary neurologicalinjury,includingneuronaldeathoralterationofneuronalnetworks[2].Leftuntreated,NCSEcanbecomerefractorytotreatment[3]. Further,delaysindiagnosisandlongerdurationofNCSEareassociatedwith pooroutcomes,increasedmortality,andchronicsequelaesuchascognitive impairmentandepilepsy[4,5].Therefore,timelyEEGisessentialforearly detectionandtreatment[6].
WhentoRequestanEEG ◾ Acutebraininjuries
◾ Alteredmentalstatus(withoutacutebraininjury)
◾ Afterconvulsivestatusepilepticus(CSE)
◾ Generalizedtonicclonicseizures(GTC),withoutreturntobaseline
◾ Managementofrefractorystatusepilepticus
◾ Monitoringdepthofanesthesia/sedation
◾ Paroxysmalclinicaleventsconcerningforseizure
◾ Pharmacologicalparalysis
◾ Postcardiacarrest
◾ Braindeathevaluation
AcuteBrainInjuries(e.g.,Trauma,Hemorrhage,Ischemia,andEncephalitis)
NCS/SEiscommonafteracutebraininjuries.Severeinjuriesresultingreater seizurerisk.Empiricantiseizuredrugprophylaxismaynotbeadequatefor seizureprevention.Additionally,EEGmonitoringmaybeusefultodetect delayedcerebralischemia(DCI)andaidinprognostication[6,7].
AlteredMentalStatus(withoutAcuteBrainInjury) NCS/SEisariskincriticallyillpatientswithalteredmentation,evenifthereis nopriorhistoryofbraininjuryorepilepsy.Theelderlyandthosewithsevere sepsis,hepaticencephalopathy,anduremicencephalopathyareespeciallyvulnerable.Additionally,EEGcanconfirmencephalopathy,gradeitsseverity, suggestpotentialetiologies,andestimateprognosis.Unexpectedlynormal EEGincomamaysuggestlocked-insyndrome,catatonia,orpsychogenic coma[6,7].
AfterConvulsiveStatusEpilepticus(CSE)orGeneralizedTonicClonic(GTC)
SeizureswithoutReturntoBaseline
ContinuousorfrequentconvulsionswithoutrecoveryaretermedCSE.CSEisa clinicaldiagnosisthatdoesnotrequireEEG.Infact,therecordisobscuredby muscleartifact.However,EEGiscrucialinthosewhodonotrecoverimmediatelyaftercessationofmotoractivity.ThisisbecauseNCS/SEiscommonafter CSEwithonestudyreportingNCSin48%andNCSEin14%inthefirst 24hoursafterCSE[8].Additionally,EEGisusefultodistinguishNCS/SEfrom prolongedpostictalencephalopathyorsedativeeffect.Anunexpectedlynormal recordduringconvulsionsmaysuggestfunctional/psychogenicSE[6,7].
ManagementofRefractoryStatusEpilepticus(RSE) RSEisthetermforpersistentseizuresdespitefirstlinetherapywitha benzodiazepineandatleastoneacceptableantiseizuremedication(ASM); seizuresoccurringorrecurringdespiteanesthesia/sedationissuper-refractory SE(SRSE).Sinceseizureactivityintheseconditionsisusuallynonconvulsive, theEEGisnecessaryformanagement.Thisincludesmonitoringresponses toantiseizuretherapies,titrationofanesthesia/sedation,trendingrhythmic andperiodicpatterns,confirmingseizuretermination,anddetecting recurrence[6,7].
MonitoringDepthofAnesthesia/Sedation TheEEGcanaugmentabedsideassessmentofconsciousnessduringanesthesia/sedation.Itcandetermineadequacyofburstsuppression(adepthof sedationoftennecessaryforRSE)orcompletesuppressioninmedically inducedcoma(e.g.,pentobarbitalcoma)[6,7].
ParoxysmalClinicalEventsConcerningforSeizure Paroxysmssuchasabnormalmovements(e.g.,eyelidflutter,nystagmus, chewing,myoclonus,twitches,tremors,rigors,andposturing),dysautonomia spells(e.g.,apnea,heartrate,andbloodpressurechanges),orunexplained elevationsinintracranialpressurearecommonincriticallyillpatients.EEGis usefulfordetectingiftheseareduetoseizure[6].
PharmacologicalParalysis TheEEGisusefulfordetectingseizuresduringperiodsofneuromuscular blockade(e.g.,duringextracorporealmembraneoxygenation(ECMO)or therapeutichypothermia(TH)),asmotoractivityissuppressed[6].
PostCardiacArrest(CA) Seizures(usuallynonconvulsive)occurinathirdofcomatosepatientsafter cardiacarrest.EEGisrecommendedduringperiodsofTHandrewarming. Additionally,EEGcandistinguishcorticalfromsubcorticalmyoclonusandaid inneurologicalprognostication[6,7].
BrainDeath(DeathbyNeurologicalCriteria) TheEEGmaybeusedasasupplementarytooltoconfirmadiagnosisofbrain death.Importantly,theEEGshouldnotbeusedalonetodeterminebrain death[9].
LimitationsofCriticalCareEEG Comparedtothecontrolledenvironmentofaneurophysiologylaboratory, recordingEEGsincriticalcaresettings(e.g.,ICUs,emergencyrooms,step downunits,andhospitalfloors)presentschallenges:
1. Artifact canoftenariseduetocontaminationfromelectricalnoisecoming fromvariousdevicesinthepatient’sroom(e.g.,IVpumps,dialysis machines,andeventhebed!).Criticalcaresettingsarealsobusyplaceswith frequentmovementofequipment,patients,andstaff,makingtherecord pronetovariousotherartifacts.
2. Electrodeplacement ishamperedbyscalplesions(e.g.,hematomas, infections,orswellings)andsurgicalwoundsanddressings(e.g., craniotomy).Electrodesbecomecontaminatedbybloodordischarge.Even sweatyskincausesartifact.
3. Patientmovements (e.g.,duringpersonalcare,transfers,orvolitional)can disruptrecordingsandintroduceartifact.Thecriticallyillarepronetomany abnormalmovementsorparoxysmsthatcanmimicseizures.Agitatedor deliriouspatientsmaypullofftheirelectrodesorself-disconnectthe recordingentirely.