This text is dedicated to my wife, Christina, for supporting my relentless pursuit of knowledge and the translational dynamics that create a physiologic occlusal interface. And to all students of occlusion who strive to understand the science of occlusion and its application for the benefit of patient care and well-being.
Acknowledgements
The American College of Prosthodontists would like to recognize the ACP Task Force on Occlusion Education, led by Dr. Jonathan Wiens, for the time and expertise they devoted to this text; the Whip Mix Corporation, for its support of this project and the advancement of dental education; the many dental and medical professionals who contributed their figures, videos, and other valuable material to this publication; the peer reviewers led by Dr. Nadim Z. Baba and including Dr. John R. Agar, Dr. Lily T. Garcia, and several other prosthodontists; and Mark Heiden and Alethea Gerding, from the ACP staff, for their project management.
Contributors
ACP TASK FORCE ON OCCLUSION EDUCATION
Donald A. Curtis, DMD, FACP
Diplomate, American Board of Prosthodontics
Professor Prevent. and Rest. Dental Sciences
University of California San Francisco San Francisco, California
David P. Donatelli, DDS
Assistant Professor
Department of Restorative Dentistry
Temple University Kornberg School of Dentistry Philadelphia, Pennsylvania
Bryan D. Dye, DDS, MS, FACP
Diplomate, American Board of Prosthodontics
Assistant Professor Department of Restorative Dentistry
West Virginia University
Morgantown, West Virginia
John J. Ference, DMD, MDS, FACP
Diplomate, American Board of Prosthodontics
Assistant Professor of Prosthodontics
University of Pittsburgh School of Dental Med. Pittsburgh, Pennsylvania
Lisa A. Lang, DDS, MS, MBA, FACP
Diplomate, American Board of Prosthodontics
Chair, Associate Professor Department of Comprehensive Care Case Western Res. Univ. School Dental Med. Cleveland, Ohio
Damian J. Lee, DDS, MS
Assistant Professor
Restorative Sciences and Prosthodontics
The Ohio State School of Dentistry Columbus, Ohio
William W. Nagy, DDS, FACP
Diplomate, American Board of Prosthodontics
Professor, Department of Restorative Sciences
Baylor College of Dentistry, Dallas, Texas
Ales Obrez, DMD, PhD
Associate Professor
Department of Restorative Dentistry
University of Illinois-Chicago College of Dentistry Chicago, Illinois
Jennifer L. Wiens Priebe, DDS, MS, FACP
Diplomate, American Board of Prosthodontics
Prosthodontics and Implant Consultants, PC West Bloomfield, Michigan
Rick M. Smith, DDS, MS, FACP
Diplomate, American Board of Prosthodontics
Associate Professor of Prosthodontics
Arizona School of Dentistry and Oral Health
Mesa, Arizona
Daniel F. Tylka, DMD, MS
Clinical Associate Professor
Department of Restorative Dentistry
University of Oklahoma College of Dentistry
Oklahoma City, Oklahoma
Jonathan P. Wiens, DDS, MSD, FACP
Diplomate, American Board of Prosthodontics
Adjunct Clinical Professor
Department of Restorative Dentistry
University of Detroit Mercy School of Dentistry
Detroit, Michigan
CONTRIBUTORS
Peter E. Dawson, DDS
The Dawson Academy
St. Petersburg, Florida
Charles J. Goodacre, DDS, MSD, FACP
Diplomate, American Board of Prosthodontics
Distinguished Professor, Advanced Education Program in Prosthodontics
Loma Linda University School of Dentistry
Loma Linda, California
Niles F. Guichet, DDS, FACP
Diplomate, American Board of Prosthodontics
Providence Prosthodontics
Orange, California
Aldo Leopardi, BDS, DDS, MS
7400 East Crestline Circle
Greenwood Village, CO 80111
Ronald L. Wiens, MA, LSMW, ACSW
Private Consultant
Certified and Licensed Therapist Allen Park, Michigan
The term “occlusion” refers to the manner in which teeth contact in closure and to all functional border movements of the mandible with the teeth in contact. Although many proposals for the specifications of an optimum occlusion have been advanced based on prior training, experience, and literature reviews, none have received universal acceptance.
In studying how best to improve standards for teaching principles of occlusion, it is tempting to get sidetracked into a contest advocating for specific techniques or favored philosophies of treatment. If the goal is to better prepare students for understanding how to treat the many complex problems that will be faced in practice, the educational process should start with the end in mind. Since it is irrational to design treatment that has no specific goal, the starting point should be to learn how the masticatory system works in healthy function so the astute clinician can then understand what is wrong when it isn’t working properly.
To practice intelligently and ethically, every dental graduate must have a sound understanding of occlusion. Graduates cannot claim a workable understanding of occlusion if they are not competent in diagnosing and correcting the routine problems that result from malocclusions. Malocclusion is the condition that exists when the teeth do not come together properly. The effects of malocclusion are many and varied. They are the very effects that every dentist sees and must treat on a daily basis and include excessive wear, sore or sensitive teeth, cracked cusps, and tooth hypermobility. In addition, the effects of malocclusion on the masticatory musculature and as a common causative factor in orofacial pain and craniomandibular disorders are all problems routinely seen in every dental practice. Dentists must assume responsibility for at least recognizing these problems, because dentists are the only health professionals trained in masticatory system disorders including occlusion factors.
A literature review reveals why there is so much confusion regarding the role of malocclusion as a factor in masticatory system pain and dysfunction.1 Investigators found that in a 25-year period (1969-1994) 75% of the articles published supported the position that malocclusion was not a factor in the etiology of craniomandibular disorders (CMD). One study reported that most patients who availed themselves of occlusal equilibration to correct malocclusion had more symptoms after treatments than before and wished they had never had the service. In consideration of these reports, plus the added requirements to teach new techniques, materials, and implant placement and the impact of digital advancements, interest in occlusion waned, and curriculum time for occlusion was significantly reduced. Some dental educators were asking “Is occlusion important, and if it is, what do we teach?”
An analysis of the literature minimizing the importance of occlusion clarifies why the opinions expressed are varied among the many dentists who support the position that effective occlusion diagnostic and treatment skills are absolutely necessary for managing dentally related masticatory system disorders, including problems of orofacial pain and CMDs. In revisiting the negative admonitions in the literature, it is apparent that not a single study followed the clinical guidelines that knowledgeable clinicians agree are essential for successful occlusal treatment.
In response to the serious need to elevate the teaching of occlusion as an essential need in every dental curriculum, the American College of Prosthodontists (ACP) established an Occlusion Task Force to revisit the evidence and make recommendations for an occlusion curriculum overhaul at all levels in dental education. This task force, operating under the auspices of two consecutive presidents, Dr. Lyndon Cooper and Dr. Jonathan Wiens, recruited 130 educators representing all the dental schools in the USA and Canada to participate in this effort.
This text is the first of a series of advancements planned by the ACP to established evidence-based standards for occlusion education, diagnosis, treatment, research –and perhaps in the future – insurance reimbursement for diagnosis and treatment of occlusion related CMDs as a dentally related medical problem.
The premise that drives the ACP to improve protocols for teaching principles of occlusion is straightforward. Graduates who have not learned how to recognize and treat problems of occlusion will not know how to prevent them, causing problematic disharmonies in the dental treatment they perform on their patients.
There are many excellent, well-known textbooks on occlusion, such as Functional Occlusion by Dr. Peter E. Dawson and the Management of Temporomandibular Disorders and Occlusion by Dr. Jeffrey P. Okeson, yet a need to establish a fundamental knowledge reference base remains. Recognizing this need, the American College of Prosthodontists (ACP) appointed a Task Force on Occlusion Education to develop a resource.
The goal of this text is to develop concepts of occlusion based upon the best available science combined with a consensus of the best clinical practices by leading prosthodontic educators and practitioners. This combination provides clarity and understanding to enable students of occlusion to begin their journey of discovery with a sound foundation. Drs. Niles Guichet and Pete Dawson, pioneers in occlusal studies, provided valuable guidance and counsel in the development of this text. Their contributions to the literature and continuing dental education are noteworthy.
This enhanced book is designed to be a quick reference “bluebook” with universal appeal. It is intended to be a uniquely interactive learning experience, as the reader will be able to intuitively explore the galleries of videos, images, presentations, and track progress with the Q&A reviews at the end of each chapter. Beginning undergraduate and postgraduate dental students, dental hygienists, assistants, and technicians will find this publication an invaluable source of information on dental occlusion.
This text consists of ten chapters followed by review questions and answers. The first chapter begins with a glossary, as learning occlusal terminology will facilitate a better understanding of the text that follows. Rather than an alphabetical listing, these occlusal terms have been reorganized under five headings (Parametrics, Articulation, Mandibular Movements, Occlusal Instruments, and Temporomandibular Joint) for comparison and contrast. The ACP acknowledges the Academy of Prosthodontics for their willingness to share the Glossary of Prosthodontic Terms
The next three chapters include anatomy and physiology, occlusal instruments, occlusal disorders, and equilibration methodology. These sections are designed to teach students how to analyze the various skeletal and dental morphologies that impact the occlusal interface, as well as the dynamics of the range of mandibular motion and the various instruments used to measure, record, and recreate a stable occlusal interface.
A text on occlusion would be incomplete without a chapter on temporomandibular disorders (TMD), as the TM joints and associated neuromusculature provide an overriding influence on the occlusal interface. The objective of this section is to help the reader to recognize normal to simple TMD and/or neuromuscular disorders, and how to manage joint instability and achieve neuromuscular release prior to restoring the occlusion.
Arriving at a diagnosis and treatment plan is critical in the management of occlusal and temporomandibular disorders as well as when planning how best to restore the occlusion. Various diagnoses and related treatment plans are outlined. The occlusal prerequisites for various types of treatment in managing partial and complete edentulism follow. The occlusal interface for fixed, removable, and implant prosthodontics may be managed differently depending upon patient parameters and is described. The last section on advanced occlusal concepts delves into more complex diagnoses and treatment, and directs the reader to other sources of information for further study and investigation.
The ACP recognizes the members of the Task Force on Occlusion Education for their valuable time and effort. Without question this work could never have been published without the help of the Whip Mix Corporation, which provided graphics and an unrestricted educational grant to help produce this text.
The following occlusal terminology was primarily derived from the GPT-8, and was reorganized into groups. The regrouping of terms is believed to be beneficial for better comprehension and retention. The reader is encouraged to review the complete Glossary for other prosthodontic terms. In addition, the Glossary is searchable for other related terms.
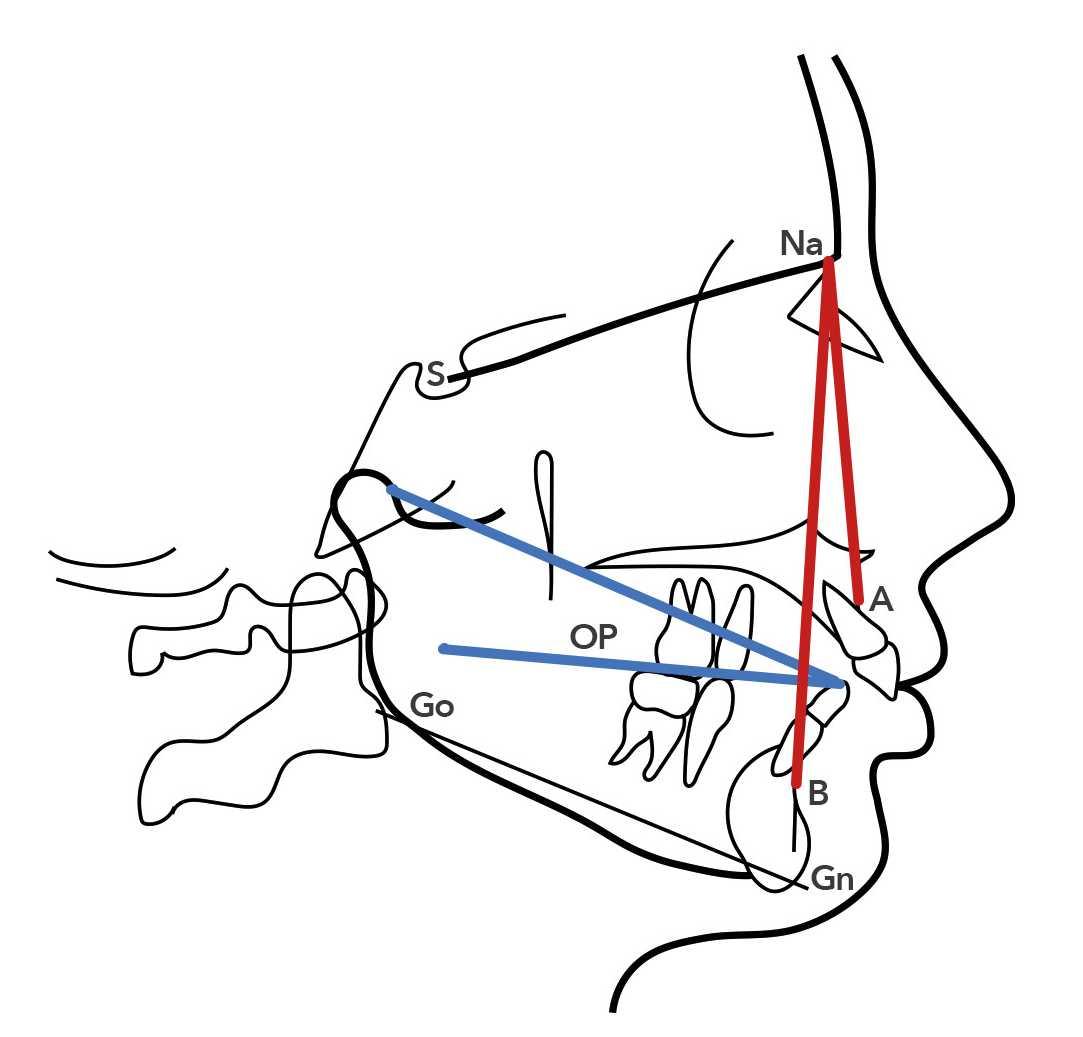
ANB angle (ANB): in cephalometric analysis, the angle formed between the nasion point A line and the nasion point B line.
Balkwill angle: eponym for the angle bounded by lines connecting the mandibular central incisor’s incisal edge to each condyle and the angle created with the occlusal plane. (Not in GPT).
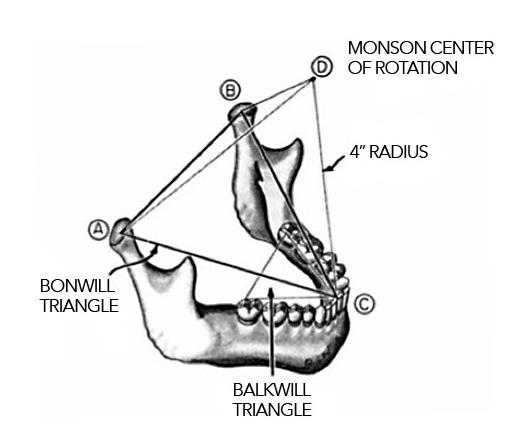
Bonwill triangle: eponym for a 4-inch equilateral triangle bounded by lines connecting the contact points of the mandibular central incisor’s incisal edge (or the mid-line of the mandibular residual ridge) to each condyle (usually its mid point) and from one condyle to the other.
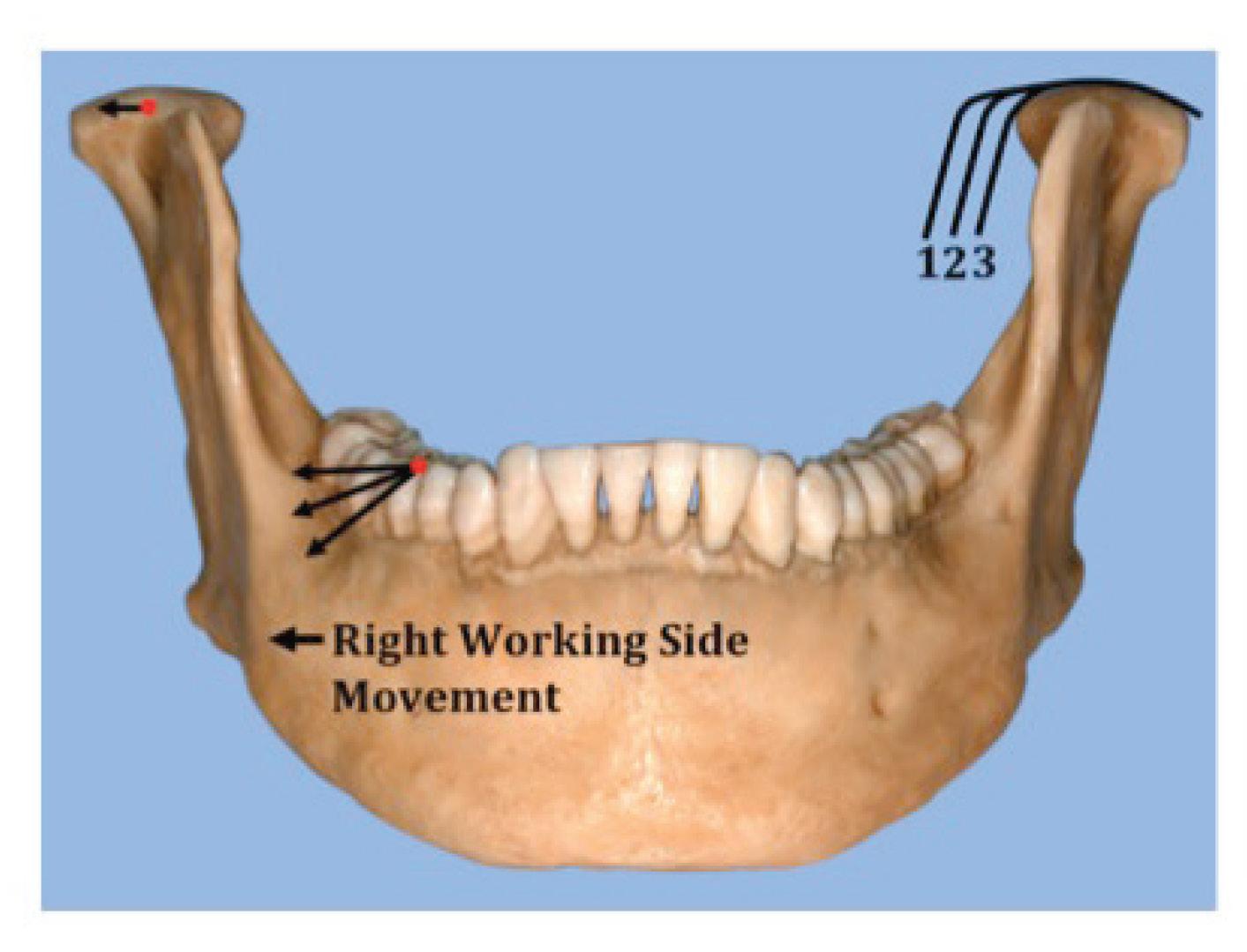
Bennett angle: the angle formed between the sagittal plane and the average path of the advancing condyle as viewed in the horizontal plane during lateral mandibular movements.
cusp angle: the angle made by the average slope of a cusp with the cusp plane measured mesiodistal or buccolingually.
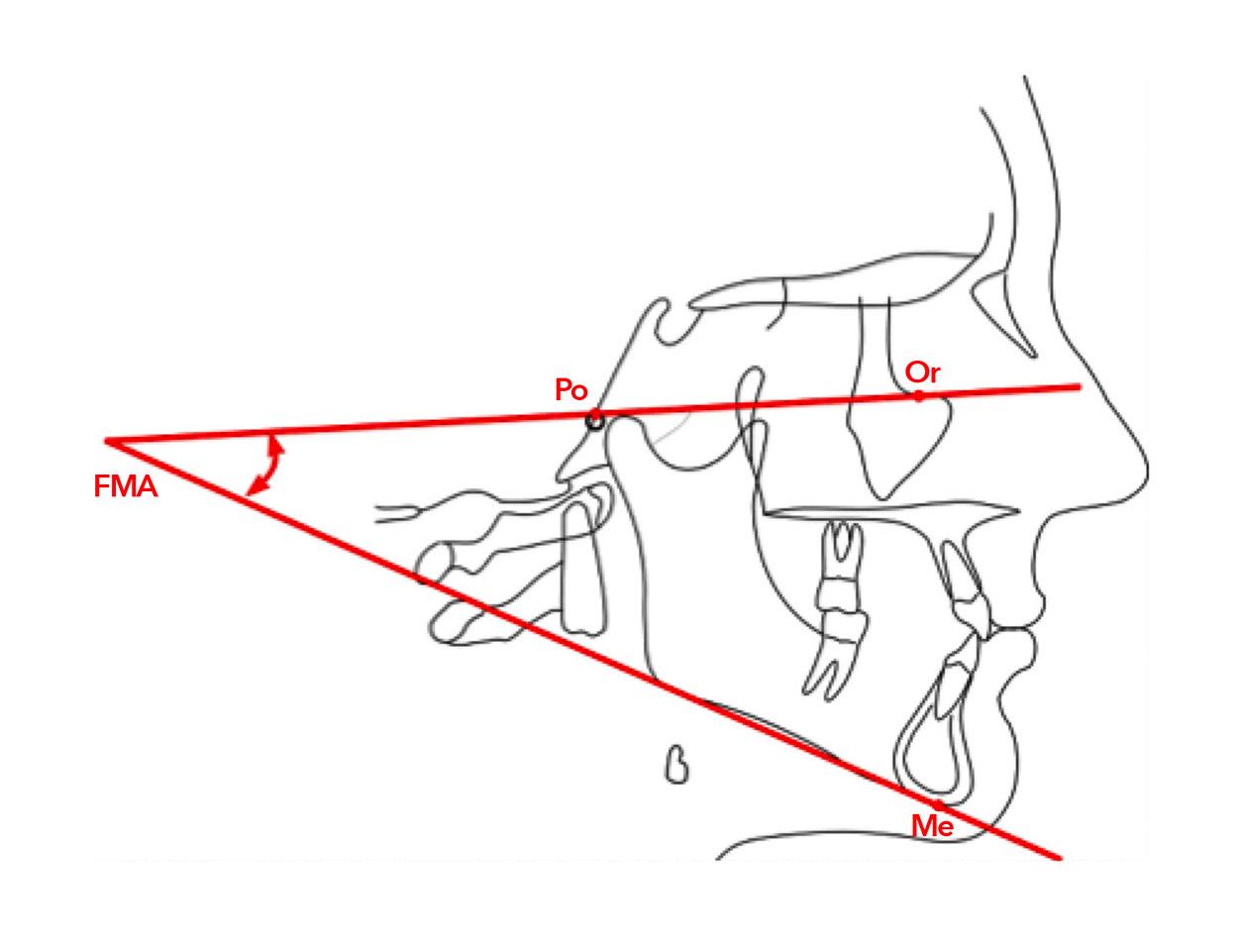
Frankfort mandibular plane angle: eponym for the angle formed by the intersection of the Frankfort horizontal plane with the mandibular plane.
Fischer’s angle: eponym for the angle formed by the intersection of the protrusive and nonworking side condylar paths as viewed in the sagittal plane.
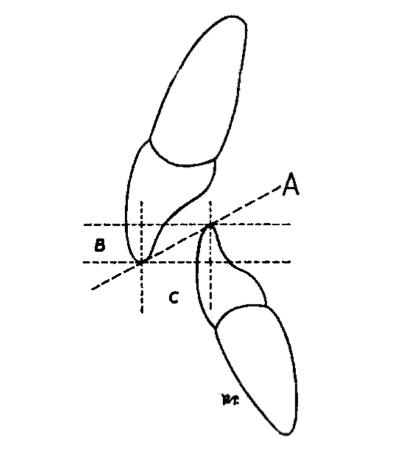
incisal guide angle: anatomically, the angle formed by the intersection of the plane of occlusion and a line within the sagittal plane determined by the incisal edges of the maxillary and mandibular central incisors when the teeth are in maximum intercuspation on an articulator, that angle formed, in the sagittal plane, between the plane of reference and the slope of the anterior guide table, as viewed in the sagittal plane.
A. The ANB angle is noted in red, subspinale to nasion to supramentale. The Balkwill angle is noted in blue, condyle to median incisor midpoint to occlusal plane.
FIGURE
B. The A and B represent the condyles, while the median incisor C represents the third point of Bonwill’s 100 mm equilateral triangle. Point D represents Monson’s proposed Center of Rotation approximately located in the glabella or crista galli. The Balkwill triangle or angle is represented by the angle created between the Bonwill Triangle and the Occlusal Plane.66
FIGURE
C. The Bennett angle is represented by the morphological shape of the medial wall of the glenoid fossa and is numbered above as 1,2,3. In the above illustration the patient’s left condyle will move downward and forward, which is known as left mediotrusion. Note that angle #1 has more immediate translation (sideways movement) than #3.
FIGURE 1.1 C
D. The Frankfort mandibular plane angle is formed by the porion-orbitale plane and the menton-gonial plane.
FIGURE 1.1 D
FIGURE 1.1 E & F VERTICAL AND HORIZONTAL OVERLAP
E. Vertical overlap of the incisors measures 7 mm for this patient.
F. Horizontal overlap of the incisors measures 6 mm for this patient. The combined vertical overlap of 7 mm and horizontal overlap of 6 mm results in an incisal angle of more than 45 degrees.
G. The relative incisal guide angle “A” may be determined by measuring the vertical overlap “B” and horizontal overlap “C.” The red arrow represents the incisal guidance angle, from Trapozzano VR: Laws of articulation.67
FIGURE 1.1
1.1 Parametrics
1.1.2
AXES
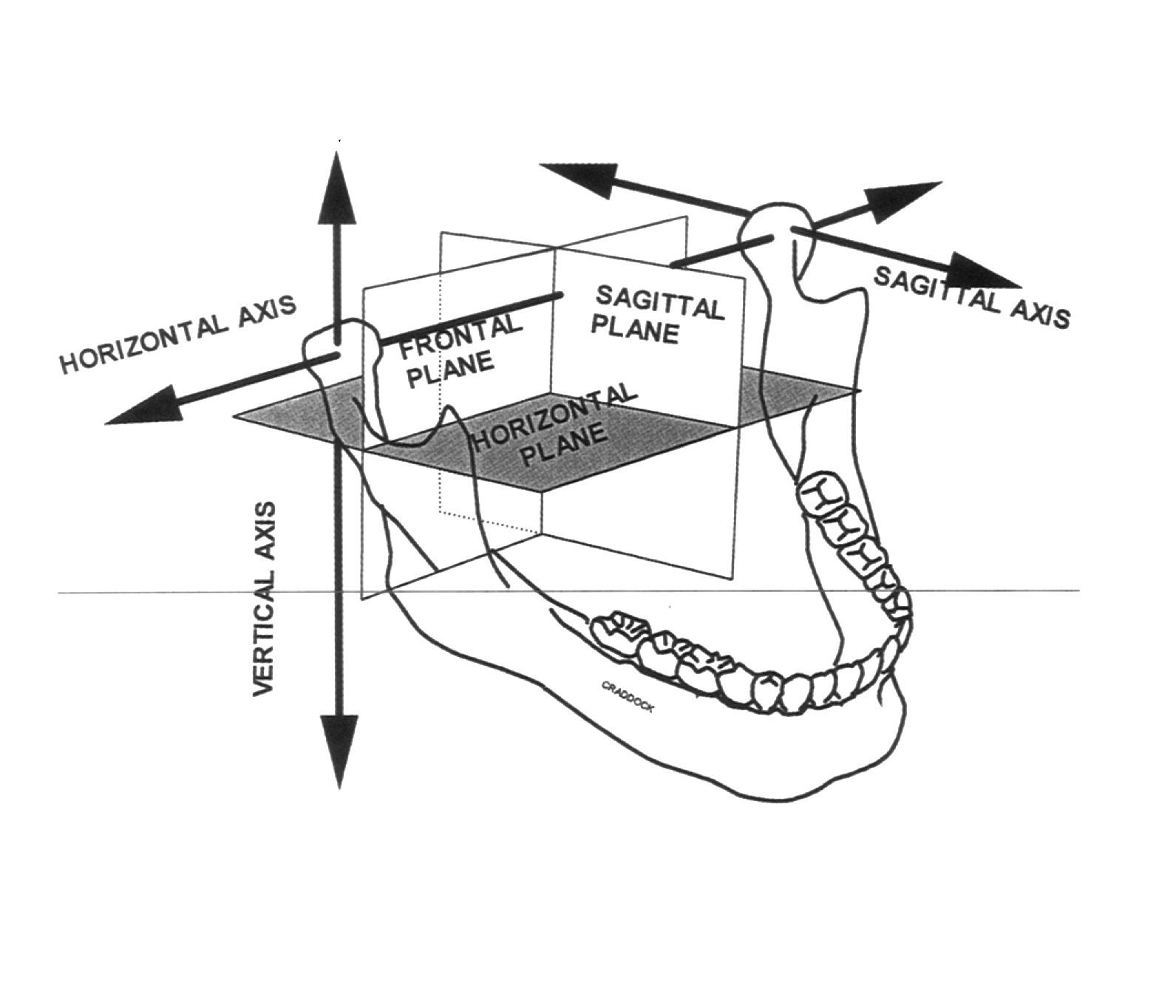
sagittal axis: an imaginary anteroposterior line around which the mandible may rotate when viewed in the frontal plane.
vertical axis of the mandible: an imaginary line around which the mandible may rotate through the horizontal plane.
transverse horizontal axis (THA): an imaginary line around which the mandible may rotate within the sagittal plane.
Bergstrom point (axis): A point measured 10 mm anterior and 7 mm inferior along the tragus-orbitale line representing the approximate location of the transverse horizontal axis.
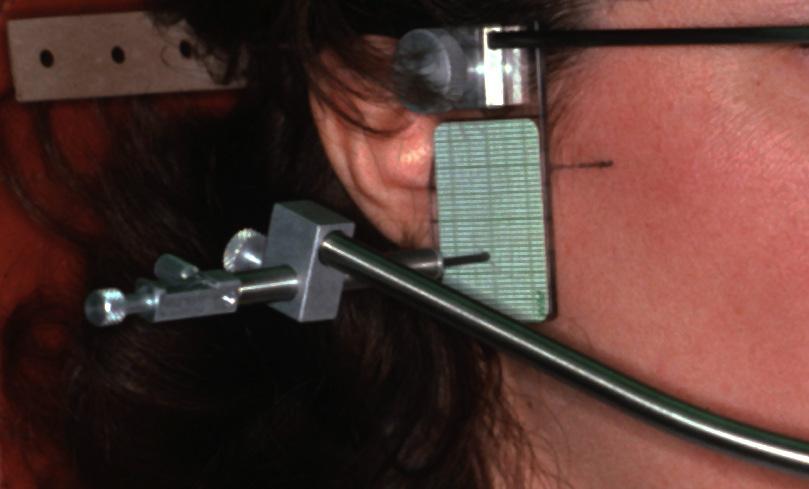
INTERACTIVE 1.1 TRANSVERSE HORIZONTAL AXIS
Using a kinematic facebow the transverse horizontal axis (THA) may be located. As the mandible is positioned in centric relation (CR), pure rotation may occur, designating the THA position. Tip: tap pause to read longer slides.
A. Note the designations of the three planes: horizontal, sagittal, and frontal planes. Mandibular movement can occur around all three axes and in all three planes, Craddock MR, Parker MH, Cameron S, et al: Artifacts in recording immediate mandibular translation: A laboratory investigation. J Prosthet Dent 1997;78:172-178.68
B. The red dot marks the transverse horizontal axis with rotation occurring in the sagittal plane as determined by the kinematic facebow.
C. Bergstrom Point: The tragus of the ear is outlined in green, the orbitale point in red, and the Bergstrom point in blue. This represents the mathematical approximate location of the kinematic THA – 10 mm anterior to tragus and 7 mm inferior to the tragus-orbitale line.
1.1 Parametrics
1.1.3 CURVES
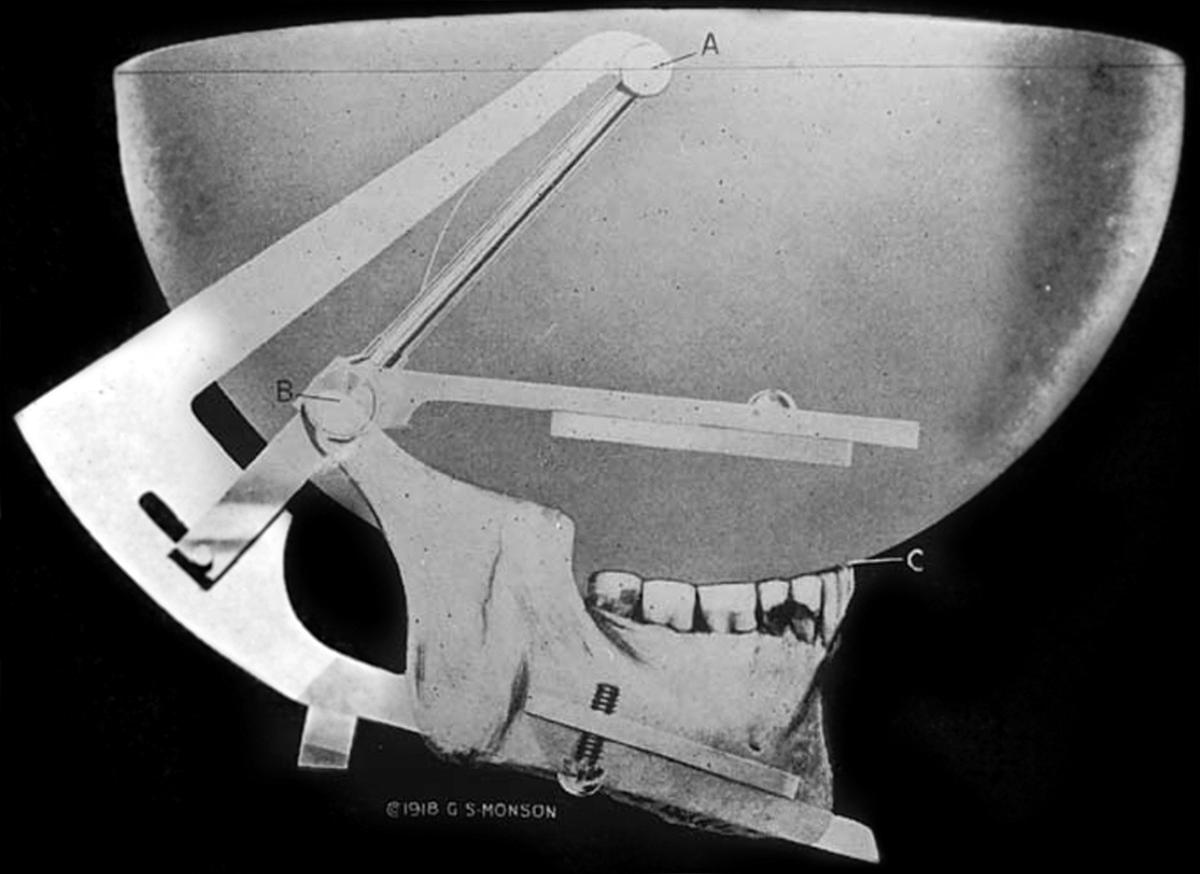
Monson curve: eponym for a proposed ideal curve of occlusion in which each cusp and incisal edge touches or conforms to a segment of the surface of a sphere 8 inches in diameter with its center in the region of the glabella.
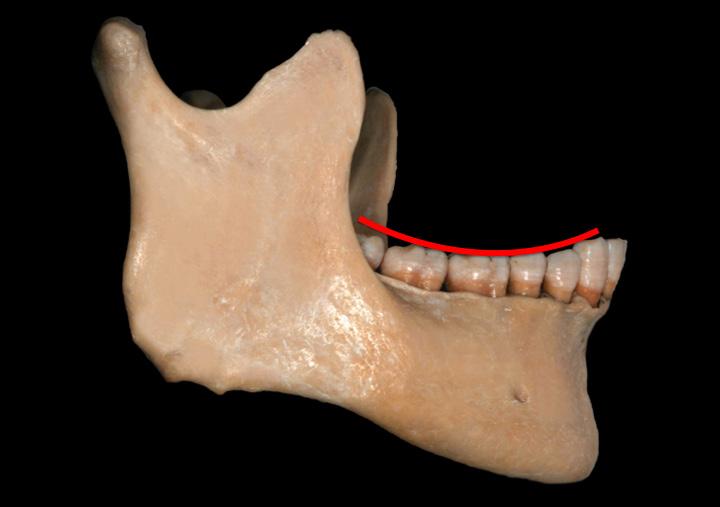
Spee curve: eponym for ANTEROPOSTERIOR CURVE – the anatomic curve established by the occlusal alignment of the teeth, as projected onto the median plane, beginning with the cusp tip of the mandibular canine and following the buccal cusp tips of the premolar and molar teeth, continuing through the anterior border of the mandibular ramus, ending with the anterior-most portion of the mandibular condyle.
Wilson curve: 1: eponym for the MEDIOLATERAL CURVE 2: in the theory that occlusion should be spherical, the curvature of the cusps as projected on the frontal plane expressed in both arches; the curve in the lower arch being concave and the one in the upper arch being convex. The curvature in the lower arch is affected by an equal lingual inclination of the right and left molars so that the tip points of the corresponding crossaligned cusps can be placed into the circumferences of a circle. The transverse cuspal curvature of the upper teeth is affected by the equal buccal inclinations of their long axes.
compensating curve (CC): 1: the anteroposterior curving (in the median plane) and the mediolateral curving (in the frontal plane) within the alignment of the occluding surfaces and incisal edges of artificial teeth that is used to develop balanced occlusion. 2: the arc introduced in the construction of complete removable dental prostheses to compensate for the opening influences produced by the condylar and incisal guidances during lateral and protrusive mandibular excursive movements.
1.3 A CURVES
A. Curve of Monson – a 4-inch (100 mm) radius sphere that determines the occlusal curve “C,” the center of rotation is in the glabella “A,” from Monson GS: Occlusion as applied to crown and bridge work. 69 FIGURE
B. Curve of Spee – the anteroposterior occlusal curve (sagittal view).
FIGURE 1.3 B & C CURVES
C. Curve of Wilson – the mediolateral occlusal curve (frontal view).
1.1 Parametrics
1.1.4 PLANES
ala-tragus plane: a line running from the inferior border of the ala of the nose to some defined point on the tragus of the ear, usually considered to be the tip of the tragus. It is frequently used, with a third point on the opposing tragus, for the purpose of establishing the ala tragus plane. Ideally the ala-tragus plane is considered to be parallel to the occlusal plane. The occlusal plane is at an angle of approximately 10 degrees relative to the Frankfort horizontal plane, when viewed in the mid sagittal plane.
axis-orbital plane: the horizontal plane established by the transverse horizontal axis of the mandible with a point on the inferior border of the right or left bony orbit (orbitale). This plane can be used as a horizontal reference point.
Frankfort horizontal plane (FHP): eponym for a plane established by the lowest point on the margin of the right or left bony orbit and the highest point on the margin of the right or left bony auditory meatus.
frontal plane: any plane parallel with the long axis of the body and at right angles to the median plane, thus dividing the body into front and back parts. So called because this plane roughly parallels the frontal suture of the skull.
horizontal plane: any plane passing through the body at right angles to both the median and frontal planes, thus dividing the body into upper and lower parts; in dentistry, the plane passing through a tooth at right angles to its long axis.
mandibular plane (MP): in cephalometrics, a plane that passes through the inferior border of the mandible.
occlusal plane (OP): the average plane established by the incisal and occlusal surfaces of the teeth. Generally, it is not a plane but represents the planar mean of the curvature of these surfaces.
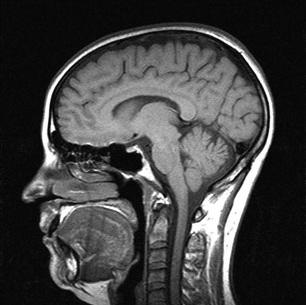
sagittal plane: any vertical plane or section parallel to the median plane of the body that divides a body into right and left portions.
A. Sagittal plane.
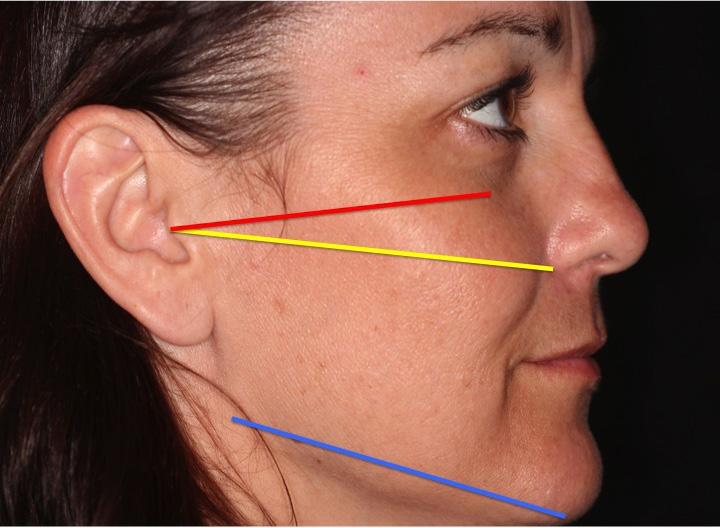
FIGURE 1.4 B PLANES
B. The red line represents the Frankfort horizontal plane, the yellow line represents Camper’s plane, and the blue line represents the mandibular plane – sagittal view.