NutritionandEyeHealth
JohnG.Lawrenson 1, *andLauraE.Downie 2
1 CentreforAppliedVisionResearch,SchoolofHealthSciences,CityUniversityofLondon, LondonEC1V0HB,UK
2 DepartmentofOptometryandVisionSciences,TheUniversityofMelbourne,Parkville,Victoria3010, Australia
* Correspondence:j.g.lawrenson@city.ac.uk;Tel.: +44-(0)20-7040-4310
Received:2September2019;Accepted:4September2019;Published:6September2019
Dietisakeylifestylefactorthatcanhavelong-termeffectsonocularhealth.ThisSpecialIssue ofNutrientsentitled‘NutritionandEyeHealth’contains12articles,includingreviewsandprimary researchstudies,thatreportonadiverserangeoftopicsrelatingtotheroleofnutritioninmaintaining eyehealth,andthepotentialuseofnutritionalinterventionsforpreventingortreatingoculardisease. Collectively,thesepapersspanaspectrumofocularconditions,includingcornealangiogenesis[1], cataract[2–4],diabeticretinopathy[5],age-relatedmaculardegeneration(AMD)[6,7],andexperimental modelsofretinaldisease[8–10].Inaddition,clinicallyfocussedpapersreportonthevalidationof anovelfoodfrequencyquestionnaireforassessinglong-chainomega-3fattyacidintakeineyecare practice[11],andevidencerelatingtotheapplicabilityofsaffronfortreatingoculardisease[12].
Globally,approximately250millionpeoplesufferfromvaryingdegreesofvisionloss[13].Leading causesincludeseveraleyeconditionsconsideredinthisSpecialIssue,suchascataract,AMD,glaucoma, anddiabeticretinopathy.Theseconditionsdisproportionatelyaffectolderadults,andwithanageing populationthenumberofaffectedindividualsispredictedtoincreaseexponentially[13].Whilstthe aetiologyofage-relatedeyediseaseiscomplexandmultifactorial,oxidativestresshasbeenimplicated asacommoncausativemechanism.Theeyeisparticularlysusceptibletooxidativestressasaresult ofitshighoxygenconsumption,highconcentrationofpolyunsaturatedfattyacidsandcumulative exposuretohigh-energyvisiblelight.Thiscombinationoffactorsleadstothegenerationofreactive oxygenspeciesthatcantriggeroxidativedamagetooculartissues.Consequently,therehasbeen significantresearchinterestintheroleofdietaryantioxidantsandthepotentialtherapeuticbenefits ofantioxidantvitaminandmineralsupplementsasasimpleandcost-effectivestrategyfordisease preventionand/orcontrol[14–17].
AMDischaracterisedbydegenerativechangeswithinthemacula,thecentralareaoftheretina thatisresponsibleforhigh-resolutionvision,inpeopleaged55yearsorolder.AMDisaleadingcause ofseverevisionimpairmentinEuropean-derivedpopulations.IntheUK,thediseaseisresponsiblefor over50%ofcertifiablevisionloss[18].Althoughepidemiologicalstudieshaveprovidedreasonably consistentevidencethatdietisanimportantmodifiableriskfactorforAMD[19],concernshavebeen raisedaboutthevalidityoffindingsfromnon-interventionalstudiesduetothepotentialinfluenceof confoundingfactors.Forexample,peoplewithaparticulardietarypatternmaydifferinotherways (e.g.,theamountofexercisetheyundertake,theirdailyleveloflightexposure)anditisnottypically possibletocontrolforthesedifferences[20].
Intermsofprimaryresearchstudies,thehighestqualityevidencetoevaluatetheefficacyandsafety oftherapeuticinterventionsderivesfromrandomisedcontrolledtrials(RCTs).InRCTs,participants arerandomlyallocatedtoreceiveeithertheinterventionoracomparator(typicallyplaceboorno intervention),whichminimisesthepotentialforbiasintheinterventionassignment[21].There isevidencefromRCTsthatprophylacticantioxidantvitaminormineralsupplementationdoesnot preventthedevelopmentofAMD[22].FivelargeRCTshavecomparedsupplementscontaining
2019, 11,2123
vitaminE,beta-carotene,vitaminC,orantioxidantvitamincombinationswithplaceboinpeoplefrom thegeneralpopulation.Thesetrialsrandomisedmorethan75,000peopleandfollowedtheirclinical outcomesbetween4to10years.Peopletakingthesesupplementswerefoundtohaveasimilarriskof developingAMDtothosenottakingthesupplements[22].
OtherRCTshaveinvestigatedwhetherhigh-doseantioxidantvitaminandmineralsupplements canslowtheprogressionofAMD[23].Mostofthesetrialsrecruitedsmallnumbersofparticipantsand wereofrelativelyshortduration,rangingfrom9monthsto6years.However,onelarge,multi-centre RCTconductedintheUSA,theAge-RelatedEyeDiseaseStudy(AREDS),randomised3640individuals withAMDtotakesupplementformulationscontainingcombinationsofvitaminC,E,beta-carotene, zinc,andcopper,oraplacebo,eachday.AmajorconclusionfromtheAREDSwasthatdaily,long-term supplementationwithvitaminC(500mg),vitaminE(400internationalunits(IU)),beta-carotene (15mg),zinc(80mg,aszincoxide),andcopper(2mg,ascupricoxide)reducedtherelativeriskof progressiontolate-stageAMDfrom28%(observedwithplacebo)to20%at5years,inpeoplewithat leastintermediateAMD.ThismeansthatforpeoplewithintermediateAMD,whoareatthehighestrisk ofprogressiontolateAMD,80fewercaseswouldprogressforevery1000peopletakingthesupplement. However,safetyconcernswereraisedregardinghigh-dosesupplementationofthecarotenoidused intheoriginalAREDSsupplement,beta-carotene,inpeoplewhosmoke[24].Inafollow-upstudy bytheAREDSinvestigators,AREDS2,currentsmokersorthosewhohadceasedsmokingforless than12monthsbeforeenrolmentwerenoteligibletoreceivebeta-carotenesupplementation[25]. TheprimaryanalysisinAREDS2demonstratedthataddingluteinandzeaxanthinand/oromega-3fatty acidstotheAREDSformulawasnotassociatedwithasignificantreductionintheriskofprogression tolate-stageAMDcomparedwiththeoriginalsupplement.Luteinandzeaxanthinarecarotenoidsthat aremajorcomponentsofmaculapigment.Theyareproposedtohaveaprotectiveroleintheretina throughtheirantioxidantpropertiesandabilitytoactasafilterforbluelight[26].Exploratoryanalyses fromAREDS2suggestedthatluteinandzeaxanthinmaybeofvalueforreducingAMDprogression whengivenwithoutbeta-carotene,butthatmoreresearchwasrequiredtotestthishypothesis[27].
Cataractisdefinedasanyvisibleopacitywithintheotherwiseclearcrystallinelensoftheeye. Cataractcanbefurtherclassifiedascortical,nuclear,orposteriorsub-capsular,dependingonthe anatomicallocationoftheopacity.Globally,over60millionpeoplearevisuallyimpairedduetocataract, howevercataract-associatedblindnessshowssignificantgeographicalvariation,accountingforless than22%ofblindnessinhigh-incomecountriescomparedtomorethan44%inSouthEastAsia[13]. Ageisthemostsignificantriskfactorforcataractogenesis.Asthelensages,conformationalchangesto lensproteinsoccurwithsubsequentaggregation,leadingtoaprogressivelossoftransparencyand associatedvisionloss[28].Oxidationreactionswithinthelensarethoughttobeakeyfactorinthis processandtherehasbeenasignificantamountofresearchontheroleofantioxidantnutrientsfor preventingorslowingtheprogressionofcataract[29].Observationaldatasuggestthattheriskof cataractscanbereducedbyadietthatcontainsoptimallevelsofvitaminsCandE,thecarotenoids luteinandzeaxanthin,andthedailyuseofmultivitaminsupplements[29].However,RCTsthathave comparedantioxidantvitaminsupplements(beta-carotene,vitaminsCandE)toaninactiveplaceboor nosupplementhavebeenunabletodetectanyeffectontheincidenceorprogressionofcataract[30]. Thelackofefficacyintheserelativelyshort-termtrialscouldsuggestthatalonger-termintakeora particularcombinationofantioxidantsisrequired.Astudyofbaselinefactorsthatpredictedcataract intheAREDScohortfoundthattheuseofmultivitaminssupplementsreducedtheriskofdeveloping nuclearcataractsoveranapproximate10yearfollow-upperiod[31].
Inconclusion,age-relatedeyediseases,includingcataractandAMD,areofglobalpublichealth concern.Acquiredvisionlossassociatedwiththeseconditionscanbedevastatingtotheindividual throughitsdetrimentalimpactonqualityoflife,andalsoimpartsubstantialsocietalburden.Although thepathogenesisoftheseconditionsisnotfullyunderstood,thereisincreasingevidencethattheirimpact can,tosomeextent,bemitigatedbytargetingmodifiableriskfactors.Sincedietandnutritionhave beenlinkedwiththemostcommondiseasesaffectingtheelderly,dietarymodificationandnutritional
Nutrients 2019, 11,2123
supplementationforthepreventionandtreatmentofthesediseaseshasattractedaconsiderable amountofscientificattention.Asevidencedbythequalityanddiversityofthecontributionsinthis SpecialIssue,theroleofnutritionineyehealthremainsahighlytopicalarea,withscopeforfuture researchtoenhanceourunderstandingoftheroleofnutritionalstrategiesforoptimisingeyehealth.
AuthorContributions: J.G.L.andL.E.D.wrotetheeditorial.
Funding: Thisresearchreceivednoexternalfunding.
ConflictsofInterest: Theauthorsdeclarenoconflictofinterest.
References
1. Estrella-Mendoza,M.F.;Jimenez-Gomez,F.;Lopez-Ornelas,A.;Perez-Gutierrez,R.M.;Flores-Estrada,J. CucurbitaargyrospermaSeedExtractsAttenuateAngiogenesisinaCornealChemicalBurnModel. Nutrients 2019, 11,1184.[CrossRef][PubMed]
2. Braakhuis,A.J.;Donaldson,C.I.;Lim,J.C.;Donaldson,P.J.NutritionalStrategiestoPreventLensCataract: CurrentStatusandFutureStrategies. Nutrients 2019, 11,1186.[CrossRef][PubMed]
3. Lim,V.;Schneider,E.;Wu,H.;Pang,I.H.Cataractpreventiveroleofisolatedphytoconstituents:Findings fromadecadeofresearch. Nutrients 2018, 10,1580.[CrossRef][PubMed]
4. Zych,M.;Wojnar,W.;Dudek,S.;Kaczmarczyk-Sedlak,I.RosmarinicandSinapicAcidsMayIncreasethe ContentofReducedGlutathioneintheLensesofEstrogen-DeficientRats. Nutrients 2019, 11,803.[CrossRef] [PubMed]
5. Rossino,M.G.;Casini,G.Nutraceuticalsforthetreatmentofdiabeticretinopathy. Nutrients 2019, 11,771. [CrossRef]
6. Lawrenson,J.G.;Evans,J.R.;Downie,L.E.ACriticalAppraisalofNationalandInternationalClinical PracticeGuidelinesReportingNutritionalRecommendationsforAge-RelatedMacularDegeneration: AreRecommendationsEvidence-Based? Nutrients 2019, 11,823.[CrossRef][PubMed]
7. Rinninella,E.;Mele,M.C.;Merendino,N.;Cintoni,M.;Anselmi,G.;Caporossi,A.;Gasbarrini,A.; Minnella,A.M.Theroleofdiet,micronutrientsandthegutmicrobiotainage-relatedmaculardegeneration: Newperspectivesfromthegut(-)retinaaxis. Nutrients 2018, 10,1677.[CrossRef]
8. Morita,Y.;Miwa,Y.;Jounai,K.;Fujiwara,D.;Kurihara,T.;Kanauchi,O.LactobacillusparacaseiKW3110 PreventsBlueLight-InducedInflammationandDegenerationintheRetina. Nutrients 2018, 10,1991. [CrossRef]
9. Kang,M.K.;Lee,E.J.;Kim,Y.H.;Kim,D.Y.;Oh,H.;Kim,S.I.;Kang,Y.H.Chrysinamelioratesmalfunction ofretinoidvisualcyclethroughblockingactivationofAGE-RAGE-ERstressinglucose-stimulatedretinal pigmentepithelialcellsanddiabeticeyes. Nutrients 2018, 10,1046.[CrossRef]
10. Yu,M.;Yan,W.;Beight,C.LuteinandZeaxanthinIsomersProtectagainstlight-inducedretinopathyvia decreasingoxidativeandendoplasmicreticulumstressinBALB/cJMice. Nutrients 2018, 10,842.[CrossRef]
11. Zhang,A.C.;Downie,L.E.PreliminaryValidationofaFoodFrequencyQuestionnairetoAssessLong-Chain Omega-3FattyAcidIntakeinEyeCarePractice. Nutrients 2019, 11,817.[CrossRef][PubMed]
12. Heitmar,R.;Brown,J.;Kyrou,I.Saffron(Crocussativus L.)inOcularDiseases:ANarrativeReviewofthe ExistingEvidencefromClinicalStudies. Nutrients 2019, 11,649.[CrossRef][PubMed]
13. Flaxman,S.R.;Bourne,R.R.A.;Resnikoff,S.;Ackland,P.;Braithwaite,T.;Cicinelli,M.V.;Das,A.;Jonas,J.B.; Keeffe,J.;Kempen,J.H.;etal.Globalcausesofblindnessanddistancevisionimpairment1990–2020: Asystematicreviewandmeta-analysis. LancetGlob.Health 2017, 5,e1221–e1234.[CrossRef]
14. Weikel,K.A.;Chiu,C.J.;Taylor,A.Nutritionalmodulationofage-relatedmaculardegeneration. Mol.Asp.Med. 2012, 33,318–375.[CrossRef]
15. Sideri,O.;Tsaousis,K.T.;Li,H.J.;Viskadouraki,M.;Tsinopoulos,I.T.Thepotentialroleofnutritiononlens pathology:Asystematicreviewandmeta-analysis. Surv.Ophthalmol. 2019, 64,668–678.[CrossRef]
16. Loskutova,E.;O’Brien,C.;Loskutov,I.;Loughman,J.Nutritionalsupplementationinthetreatmentof glaucoma:Asystematicreview. Surv.Ophthalmol. 2019, 64,195–216.[CrossRef][PubMed]
17. Li,C.;Miao,X.;Li,F.;Wang,S.;Liu,Q.;Wang,Y.;Sun,J.OxidativeStress-RelatedMechanismsand AntioxidantTherapyinDiabeticRetinopathy. Oxid.Med.Cell.Longev. 2017, 2017,9702820.[CrossRef]
Nutrients 2019, 11,2123
18. Quartilho,A.;Simkiss,P.;Zekite,A.;Xing,W.;Wormald,R.;Bunce,C.Leadingcausesofcertifiablevisual lossinEnglandandWalesduringtheyearending31March2013. Eye 2016, 30,602–607.[CrossRef]
19. Chiu,C.J.;Taylor,A.Nutritionalantioxidantsandage-relatedcataractandmaculopathy. Exp.EyeRes. 2007, 84,229–245.[CrossRef]
20. Downie,L.E.;Keller,P.R.Nutritionandage-relatedmaculardegeneration:Researchevidenceinpractice. Optom.Vis.Sci. 2014, 91,821–831.[CrossRef]
21.Ioannidis,J.P.Implausibleresultsinhumannutritionresearch. BMJ 2013, 347,f6698.[CrossRef][PubMed]
22. Evans,J.R.;Lawrenson,J.G.Antioxidantvitaminandmineralsupplementsforpreventingage-related maculardegeneration. CochraneDatabaseSyst.Rev. 2017, 7,CD000253.[CrossRef][PubMed]
23. Evans,J.R.;Lawrenson,J.G.Antioxidantvitaminandmineralsupplementsforslowingtheprogressionof age-relatedmaculardegeneration. CochraneDatabaseSyst.Rev. 2017, 7,CD000254.[CrossRef][PubMed]
24. Tanvetyanon,T.;Bepler,G.Beta-caroteneinmultivitaminsandthepossibleriskoflungcanceramong smokersversusformersmokers:Ameta-analysisandevaluationofnationalbrands. Cancer 2008, 113, 150–157.[CrossRef][PubMed]
25. Group,A.R.;Chew,E.Y.;Clemons,T.;SanGiovanni,J.P.;Danis,R.;Domalpally,A.;McBee,W.;Sperduto,R.; Ferris,F.L.TheAge-RelatedEyeDiseaseStudy2(AREDS2):Studydesignandbaselinecharacteristics (AREDS2reportnumber1). Ophthalmology 2012, 119,2282–2289.[CrossRef]
26. Arunkumar,R.;Calvo,C.M.;Conrady,C.D.;Bernstein,P.S.Whatdoweknowaboutthemacularpigmentin AMD:Thepast,thepresent,andthefuture. Eye 2018, 32,992–1004.[CrossRef][PubMed]
27. Chew,E.Y.;Clemons,T.E.;Sangiovanni,J.P.;Danis,R.P.;Ferris,F.L.,3rd;Elman,M.J.;Antoszyk,A.N.; Ruby,A.J.;Orth,D.;Fish,G.E.;etal.Secondaryanalysesoftheeffectsoflutein/zeaxanthinonage-related maculardegenerationprogression:AREDS2reportNo.3. JAMAOphthalmol. 2014, 132,142–149.[CrossRef]
28. Michael,R.;Bron,A.J.Theageinglensandcataract:Amodelofnormalandpathologicalageing. Trans.R. Soc.BBiol.Sci. 2011, 366,1278–1292.[CrossRef]
29. Weikel,K.A.;Garber,C.;Baburins,A.;Taylor,A.Nutritionalmodulationofcataract. Nutr.Rev. 2014, 72, 30–47.[CrossRef]
30. Mathew,M.C.;Ervin,A.M.;Tao,J.;Davis,R.M.Antioxidantvitaminsupplementationforpreventingand slowingtheprogressionofage-relatedcataract. CochraneDatabaseSyst.Rev. 2012, 6.[CrossRef]
31. Chang,J.R.;Koo,E.;Agron,E.;Hallak,J.;Clemons,T.;Azar,D.;Sperduto,R.D.;Ferris,F.L.,3rd;Chew,E.Y. Age-RelatedEyeDiseaseStudyGroup.Riskfactorsassociatedwithincidentcataractsandcataractsurgeryin theAge-relatedEyeDiseaseStudy(AREDS):AREDSreportnumber32. Ophthalmology 2011, 118,2113–2119. [CrossRef][PubMed]
© 2019bytheauthors.LicenseeMDPI,Basel,Switzerland.Thisarticleisanopenaccess articledistributedunderthetermsandconditionsoftheCreativeCommonsAttribution (CCBY)license(http://creativecommons.org/licenses/by/4.0/).
Article
Cucurbitaargyrosperma SeedExtractsAttenuate AngiogenesisinaCornealChemicalBurnModel
MaríaFernandaEstrella-Mendoza 1 ,FranciscoJiménez-Gómez 2 ,AdolfoLópez-Ornelas 2 , RosaMarthaPérez-Gutiérrez 1 andJavierFlores-Estrada 2, *
1 LaboratoriodeInvestigacíondeProductosNaturales,EscueladeIngenieríaQuímicaeIndustrias Extractivas,InstitutoPolitécnicoNacional,UnidadProfesionalAdolfoLópezMateos,Av.Instituto PolitécnicoNacionalS/N,CiudaddeMéxico07708,México;fernandaestrella29@hotmail.com(M.F.E.-M.); rmpg@prodigy.net.mx(R.M.P.-G.)
2 DivisióndeInvestigación,HospitalJuárezdeMéxico,Av.InstitutoPolitécnicoNacional5160,Magdalenade lasSalinas,GustavoA.Madero,CiudaddeMéxico07760,México;microcirugiafco@hotmail.com(F.J.-G.); adolfolopezmd@gmail.com(A.L.-O.)
* Correspondence:javier_70_1999@yahoo.com;Tel.: +52-55-5747-7560(ext.7476)
Received:15April2019;Accepted:17May2019;Published:27May2019
Abstract: Severecornealinflammationproducesopacityorevenperforation,scarring, andangiogenesis,resultinginblindness.Inthisstudy,weusedthecorneatoexaminetheeffectofnew anti-angiogenicchemopreventiveagents.Weresearchedtheanti-angiogeniceffectoftwoextracts, methanol(Met)andhexane(Hex),fromtheseedof Cucurbitaargyrosperma,oninflamedcorneas. ThecorneasofWistarratswerealkali-injuredandtreatedintragastricallyforsevensuccessive days.Weevaluated:opacityscore,cornealneovascularization(CNV)area,re-epithelialization percentage,andhistologicalchanges.Also,weassessedtheinflammatory(cyclooxigenase-2,nuclear factor-kappaB,andinterleukin-1β)andangiogenic(vascularendothelialgrowthfactorA,VEGF-A; -receptor1,VEGFR1;and-receptor2,VEGFR2)markers.Levelsof Cox-2, Il-1β,and Vegf-a mRNA werealsodetermined.Aftertreatment,weobservedareductionincornealedema,withloweropacity scoresandcellinfiltrationcomparedtountreatedrats.Treatmentalsoacceleratedwoundhealing anddecreasedtheCNVarea.Thestainingofinflammatoryandangiogenicfactorswassignificantly decreasedandrelatedtoadown-expressionof Cox-2, Il-1β,and Vegf.Theseresultssuggestthatintake of C.argyrosperma seedhasthepotentialtoattenuatetheangiogenesissecondarytoinflammationin cornealchemicaldamage.
Keywords: Cucurbitaargyrosperma;cornealchemicalburn;angiogenesis;cornealneovascularization (CNV);vascularendothelialgrowthfactor(VEGF);interleukin-1β (IL-1β);cyclooxigenase-2(COX-2); nuclearfactor-kappaB(NF-κB)
1.Introduction
Angiogenesis,inflammation,andoxidativestressareimportantfactorsthatpredisposetoand promotetheprogressionofdegenerativediseases,andcornealdiseasesarenotanexception.Corneal neovascularization(CNV)causedbyviralinfections,autoimmunediseases,andchemicalburnscan progresstocornealulcerationandscaring,potentiallyleadingtoblindness.CNVisalsoassociated withahighrateofcornealallograftrejection[1].Inthiscontext,thenuclearfactor-kappaB(NF-κB) signalingpathwayininflammatory,epithelial,andendothelialcellsisakeystepforthetranscriptional overexpressionofpro-inflammatoryandproangiogenicfactors,includinginterleukin-1β (IL-1β), cyclooxygenase-2(COX-2),andvascularendothelialgrowthfactorA(VEGF-A).Thecyclooxigenase-2 enzymeincreasesthesynthesisofprostaglandinstomodulatecellproliferation,celldeath,andtumor
Nutrients 2019, 11,1184
invasioninmanytypesofcancer.Interleukin-1β,IL-6,andtumornecrosisfactoralpha(TNF-α) regulateCOX-2;therefore,theyareoverexpressedduringinflammation[2–4].
Inanalkali-burncornealinjury,VEGF-Aisanimportantaspectofangiogenesisexpressedin macrophagesandepithelialcells.VascularendothelialgrowthfactorAbindstotwomaintyrosine kinasereceptors,vascularendothelialgrowthfactorreceptor1(VEGFR1)and–receptor2(VEGFR2), onavascularendothelialcelltopromotemigration,proliferation,andneovascularisation,along withmonocyte/macrophagemigrationinthemicroenvironmentinjured[1,5,6].Severaltherapeutic strategiestodecreaseCNVhavebeenused,suchastopicalorsubconjunctivalcorticosteroidsand non-steroidalanti-inflammatoryagents[7].However,thesehavelimiteduseandhaveanumberofside effects[8,9].Anti-VEGFtherapyinchemicallyburnedoculartissuesresultsinasubstantialreduction ofangiogenesisinbothanimalstudiesandclinicaltrials[10,11].However,toestablishitssafetyand efficacy,controlledandrandomizedtrialstojustifytheircontinuedusearerequired.Besides,systemic drugtreatmentisnotrecommendedbecauseofadverseeffects.Therefore,itisimportanttosearchfor newdrugsforthesystemictreatmentofthesedisorders.
CurrentdatainCNVmodelsshowthatnaturalextractsfromplantsorbioactivecompoundsin plantextractshaveangiogenicsuppressingactivity[12–14].Thegenus Cucurbita (pumpkin)belongsto oneofthe300generaoftheCucurbitaceaefamily,anditisoneofthemostpopularvegetableseaten intheworld.Recently,pumpkinwasrecognizedasafunctionalfood,and Cucurbitapepo, Cucurbita maxima, Cucurbitamoschata, Cucurbitaandreana,and Cucurbitaficifolia arethemostcultivatedspecies[15]. Nutritionally,pumpkinseedhasahighamountofpolyunsaturatedfattyacidsaswellasproteins, vitamins,severalminerals,andotherphytochemicals.Theanti-diabetic,antioxidant,anti-carcinogenic, andanti-inflammatorypropertiesofthisseedarestudiedduetoitshighcontentofnaturalbioactive compounds,suchascarotenoids,tocopherols,andsterols[16–19].
Cucurbitaargyrosperma isaneconomicallyimportantspeciescultivatedinMesoamerica.Isozyme, morphological,andecologicalanalysessuggestthatitwasprobablydomesticatedfromtheMexican wildsquash, Cucurbitasororia [20].Theseedisusuallyconsumedasasnackorasaningredientin traditionalstews,althoughthescientificfindingsofitsbeneficialeffectsonhumanhealthhavenot beensufficientlyevidenced,andtheanti-neovasculareffectsofthesecondarymetabolitesremain unknown.However,conceivablyitsphytochemicalcompositioncouldbeliketherelatedspecies, showinganti-inflammatoryeffectsassuggested.Besides,proangiogenicfactorssuchasCOX-2,IL-1β, andVEGF,includingVEGFR1and-R2,inducedbytheinflammatoryagentshavenotbeenstudiedin theseplants.
Theaimofthisstudywastoinvestigatetheeffectoftheseedextractsfrom C.argyrosperma inthe inflammatoryandangiogenicprocessofattenuation.Herein,weshowthathexanicandmethanolic extractsfrom C.argyrosperma seedsignificantlyattenuatetheexpressionofproangiogenicfactors duringinflammationusingaCNVmodel.Also,weobservedbyclinicalmanifestationthatboth extractssignificantlydiminishtheCNVarea.Significantly,cornealre-epithelializationwashigherwith hexane(Hex)extracttreatmentthanmethanol(Met)extract.
2.MaterialsandMethods
2.1.ExtractPreparation
Pumpkinsof C.argyrosperma wereharvestedinanagriculturalfieldofMichoacán,México, andidentifiedbyabotanistintheherbariumoftheNationalPolytechnicInstitute(IPN).Voucher specimennumber4532wasdepositedintheherbariumoftheNationalSchoolofBiologicalSciences ofIPN.Onekilogramofseedwasextractedwith3Lofhexane(50% v/v)andlefttomaceratefor 8daysatroomtemperature.Thecrudeextractwasfilteredforonehourin8 μM-mediumflowfilter paper(Whatman® ,Sigma-Aldrich,Inc.,St.Louis,MO,USA),concentratedusingarotaryvacuum evaporatorandtakentodrynessat60 ◦ Cinavacuumrotatoruntilthecompleteremovalofthesolvent,
2019, 11,1184
obtainingaviscousresidue(8.38g/L).Thesameprocedurewasappliedtotheresidue,usingmethanol forasequentialseparationoftheseedcomponents.Eachextractwasstoredinthedarkat4 ◦ Cuntiluse.
2.2.AnimalModel
Twenty-eightmaleWistarratsweighing200 250g(12weeksold)wereused.Waterandstandard foodwereavailableadlibitum.Thecareandmanagementofexperimentalanimalswereinaccordance withtheguidelinesoftheNationalInstitutesofHealth“GuidefortheCareandUseofLaboratory Animals”,thestandardsdescribedbytheAssociationforResearchinVisionandOphthalmology (ARVO),andOfficialMexicanStandardNOM-062-ZOO-1999.ThestudywasapprovedbytheEthics CommitteeoftheHospitalJuárezdeMéxico(HJM2493/14-B).
2.3.ExperimentalDesign
Animalswereintraperitoneallyanesthetizedwithpentobarbitalsodium(0.5mg/kg),inhaled sevoflurane,andonedropofophthalmictetracaine,toperformthechemicalcauterizationofthecornea. Centralcorneasfromtherighteyeswereburnedbyapplying3-mm-diameterfilterpapersaturated with1MNaOHsolutionfor30s,withimmediatewashingwith10mLofsalinesolution.Toavoid infection,adropofophthalmicciprofloxacinwasappliedevery24huntiltheendofthestudy[21]. EachextractwasdissolvedinwaterandTween-80(20%)(Veh).Ratswererandomlydividedinto fourgroups(n = 7each)[21,22]:non-chemicallyburnedhealthycorneas(non-CB)treatedonlywith thevehicle;chemicallyburned(CB)corneastreatedwiththevehicle(CB-Veh);CBcorneastreated withhexanicextract(CB-Hex);andCBcorneastreatedwithmethanolicextract(CB-Met).Allgroups received400mg/kg/7daysofHex/Metextractsorthevehicleinasingledose(0.5mL)byoralgavage, atthesametimedaily(10:00h).Animalswereeuthanizedwithanoverdoseofpentobarbital.
2.4.ClinicalManifestation
Cornealopacity,epithelialdefects,andtheCNVareawereevaluatedeightdaysafterCB.Corneal opacitywasscoredusingascalingsystemfrom0to4:0 = noopacity,completelyclearcornea; 1 = slightlyhazy,irisandlensvisible;2 = moderatelyopaque,irisandlensstillvisible;3 = severely opaque,irisandlenshardlyvisible;and4 = completelyopaque,withnovisibilityoftheirisand lens[23].
ThemeasurementoftheCNVarea(mm2 )wasperformed invivo usingarulerunderamicroscope andphotographed.ThesoftwareprogramImage-ProPlusversion6.0software(byMediaCybernetics, Inc.,Rockville,MD,USA)wasused.Inferonasalquadrantwasselectedtocalculatetheneovascularized area,accordingtoapreviousreport[24].
Toevaluatecornealwoundre-epithelialization,weusedcornealfluoresceinstaining.Briefly, fluoresceinsodiumophthalmicstripwasinstilledintothelowerconjunctivalsacandthecorneawas examinedusingaslitlampbiomicroscopewithcobaltbluelight.Injuredepithelialtissuesretainthe fluoresceinstaining,whereasthelackofstainindicatesre-epithelialization.There-epithelialization percentagewasevaluatedintheCBcorneas,consideringthatatotalareaofapproximately7mm2 was 100percent(a3-mmdiscsaturatedwith1MNaOH).
2.5.HistologicalEvaluation
Enucleatedeyes(n = 4pergroup)wereimmediatelyfixedinneutralformalin.Cuttissueslides (3–5mm)weremade(anteroposterior)andincludedtheopticnerve.Slidesweredehydratedingraded alcoholsandembeddedinparaffin.Histologicalsectionsof2 μmwereprocessedandstainedwith hematoxylin–eosin(HE).Wemeasuredthecornealthicknessandcellinfiltrationintheperipheral region(500 μmbeyondthelimbus)usinglightmicroscopy(axioscope2plus,CarlZeiss,Göttingen, Germany).Thepercentageoftheinfiltrationwascalculatedinamaskedfashionbasedonthedensity inthecornealstromaoftheCB-Vehgroup.
Nutrients 2019, 11,1184
Other2-μm-sectionsweredewaxedandrehydratedwithantigenrecoverysolution(ImmunoDNA Retriever20× withCitrate;BioSB,SantaBarbara,CA,USA).SlideswerethenloadedintoaShandon Sequenzachamber(ThermoShandon,Cheshire,UnitedKingdom).Weusedtheproceduredescribed forthepolymer-basedimmunodetectionsystem(PolyVue® mouse/rabbit3,3 -Diaminobenzidine,DAB, detectionsystem,DiagnosticBioSystems,Pleasanton,CA,USA).Weapplied100 μLofIL-1β (Cat. No.sc-7884),NF-κBp65(sc-8008),COX-2(sc-1746),VEGF-A(sc-7269),andVEGFR1(sc-31173).All antibodieswerepurchasedfromSantaCruzBiotechnology,Inc.(SantaCruz,CA,USA).TheVEGFR2 antibody(MAB3571)waspurchasedfromR&DSystems,Inc.(Minneapolis,MN,USA).Alldilutions wereat1:200andincubatedovernightat4 ◦ C.Later,theenhancersPolyvuePlusandHRPwereadded andincubatedwithDABplus/chromogensubstrateandcounterstainedwithhematoxylin.AnAxio Imager.A2microscopewithanintegratedcamera,AxiocamICc5,(CarlZeissMicroscopyGmbH,Jena, Germany)wasusedforhistologicalobservationandimagecapture.Micrographsoftheperipheral regionofthecornea(threefieldspersideat200× magnification)weretakentomeasurethemean stainingintensityofthesemarkers.ImageswereanalyzedwiththeImage-ProPlussoftwareversion 6.0(MediaCybernetics,Inc.,Rockville,MD,USA).
2.6.QuantitativeReverse-TranscriptionPolymeraseChainReaction(qRT-PCR)
TotalRNAwasisolatedfromcornealtissueusingTRIzol™ Reagent(Invitrogen,Boston,MA,USA)(n = 3pergroup).OnemicrogramofDNaseI-treatedRNA(RocheAppliedScience,Mannheim,Germany)was reversetranscribedwithSuperScript® IIReverseTranscriptasesystem(LifeTechnologiesCorp.,Carlsbad, CA,USA).QuantificationofmRNAwascarriedoutusingqPCRwithSYBRgreenandthefollowing primers: Cox-2 (5 -CTGAGGGGTTACCACTTCCA-3 ;and5 -CTTGAACACGGACTTGCTCA-3 ); Il-1β(5 -AGGCTTCCTTGTGCAAGTGT-3 and5 -TGAGTGACACTGCCTTCCTG-3 ); Vegf-a (5GCCCATGAAGTGGTGAAGTT-3 and5 -ACTCCAGGGCTTCATCATTG-3 );and Gapdh (5CTCATGACCACAGTCCATGC-3 and5 -TTCAGCTCTGGGATGACCTT-3 ).Thecyclingprotocol wasasfollows:denaturation(95 ◦ Cfor10min),45cyclesofamplification(95 ◦ Cfor15s,59 ◦ Cfor15 s,and72 ◦ Cfor20s),andafinalextensionat72 ◦ C.Ameltingcurveanalysiswasalsoperformedto ascertainthespecificityoftheamplifiedproduct.Theexpressionforeachgenewasnormalizedto Gapdh Expressionwasquantifiedasfold-changeusingthe ΔΔCtmethod.
2.7.StatisticalAnalysis
WeusedGraphPadPrismsoftware(LaJolla,CA,USA)(version5.0).Valuesaremeanwith standarddeviation(mean ± SD).Inallcases,weusedunifactorialanalysisofvariancefollowedby Tukey’spost-hocanalysis.
3.Results
3.1.AmeliorationofCornealWoundRepair
Weevaluatedcornealwoundhealingmediatedbytheextractsinthealkali-burncornealmodel. Figure 1ashowsthatthetreatedgroupshadasignificantreductionincornealopacityscoreandCNV areacomparedtotheCB-Veh(p < 0.05and p < 0.001,respectively).However,CNVintheCB-Met treatedgroupwaslowerthantheCB-Hexgroup(p < 0.05)andfurthermoredidnotshowasignificant increaseinthepercentageofre-epithelialization(Figure 1b).
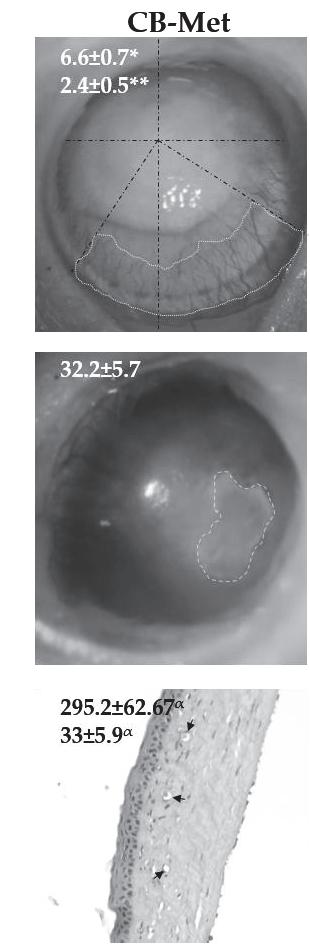
UsingHE-stainedslides(Figure 1c),thenon-CBgrouphadanaveragecornealthicknessof336.7 ± 39.5 μm,withanintactepithelialandstromallayer.Therewereneitherinflammatorycellsnorblood vessels.Conversely,cornealintegrityintheCB-Vehgroupwasseverelyimpaired,withalossofthe epithelialcelllayersanddisruptionofstromalcollagenfibers.Thecornealthicknessinthisgroupwas 592.3 ± 112.1 μm,withanaveragecellinfiltrationof81 ± 11.9%.CornealthicknessintheCB-Hexgroup was427.2 ± 113.7 μm,whichwassignificantlyreducedcomparedtotheCB-Veh),withareductionin cellinfiltration(40 ± 8.1%).Similarly,theCB-Metgroupshowedadecreaseincellinfiltration(33.2 ±
2019, 11,1184
5.9%)andcornealthickness(295.2 ± 62.67 μm)(p < 0.001)comparedtoCB-Veh.Cornealthicknessin theCB-Metgroupwasnotsignificantlydifferentfromthatofthenon-CBgroup.
Figure1. Methanol(Met)andhexane(Hex)extractsof Cucurbitaargyrosperma seedinchemicallyburned corneas(CB)comparedtotheuntreatedgroup(CBcorneastreatedwiththevehicle,CB-Veh).(a)Average ofopacityscore(OPA)andcornealneovascularizationarea(CNV)inmm2 .(b)Re-epithelialization percentage(RE).(c)Cornealthicknessinmicrons(THK)andinfiltrationcellpercentage(INF).Average value ± SD;* p < 0.05;** p < 0.01,and α p < 0.001comparedtoCB-Veh. @ p < 0.05comparedtoCB-Met. Graydottedlinesshowstudiedarea,andblacklinesarethegeometricalaxis.CB-Hex:CBcorneas treatedwithhexanicextract;CB-Met:CBcorneastreatedwithmethanolicextract.Arrowsindicatethe lumenofstromalbloodvessels.(Scalebar = 100 μm).
3.2.Anti-inflammatoryEffect
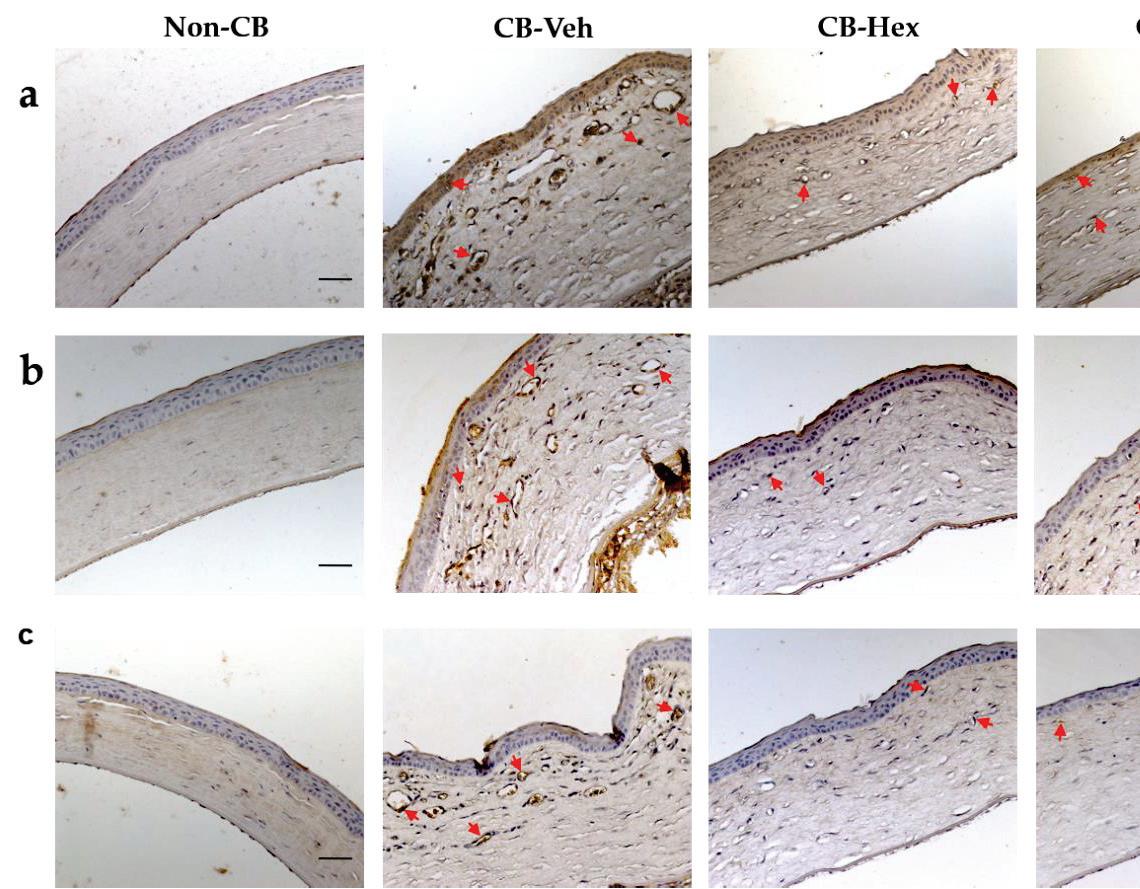
Severalinflammatorycytokinesimplicatedinalkali-inducedcornealinjuryareregulatedbythe nuclearinternalizationofactiveNF-κB.Hence,welookedforthestaininglocationofNF-κBinthe corneallesions.Inthenon-CBgroup,NF-κBwasrestrictedtothecytoplasmofepithelialcellsinthe basallayer(Figure 2a).IntheCB-Vehandbothextract-treatedgroups,NF-κBwasdistributedinthe nuclearcompartmentofendothelialandinflammatorycells.However,stainingdensitydecreasedin theCB-Hex(41.13 ± 9.6)andtheCB-Met(32.73 ± 8.1)comparedtotheCB-Veh(73.31 ± 10.4; p < 0.0001 both).Additionally,weperformedmeasurementsofthestainingintensityforIL-1β (Figure 2b)and COX-2(Figure 2c).Inthenon-CB,therewasalowstainingintensityforIL-1β (9.28 ± 2.6)comparedto CB-Veh(75.95 ± 12.16; p < 0.0001),showingadistributionalongwiththecornealstromaaswellas endothelialcells.Meanwhile,theintensitiesintheCB-Hex(42.16 ± 9.14)andtheCB-Met(38.21 ± 7.9) werelowerthantheCB-Vehgroup(p < 0.0001).StainingintensityforIL-1β betweentheCB-Met andtheCB-Hexshowednodifferences(p >0.05).Likewise,theintensityforCOX-2wassignificantly differentwhencomparingtheCB-Veh(102.6 ± 13.08)totheCB-Hex(68.79 ± 10.73)andtheCB-Met (37.15 ± 7.18)(p < 0.0001)groups.Thenon-CBhadadetectableexpressionof7.49 ± 3.48.Staining
Nutrients 2019, 11,1184
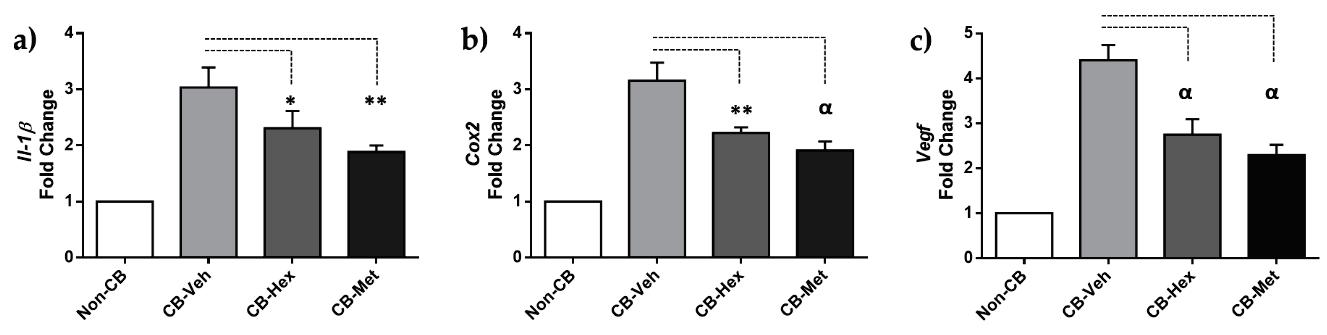
intensityforIL-1β andCOX-2inthecorneawasalsoconfirmedatthelevelofmRNA(Figure 3): Il-1β expressionfortheCB-Met(2.31 ± 0.30)andtheCB-Hex(1.89 ± 0.11)groupswasdecreasedcompared totheCB-Vehgroup(3.03 ± 0.35; p < 0.05and p < 0.01,respectively)(Figure 3a).The Cox-2 inthe CB-Hex(2.22 ± 0.10)andtheCB-Met(1.91 ± 0.15)wasalsodiminishedcomparedtotheVehgroup (3.15 ± 0.31; p < 0.01)(Figure 3b).The Il-1ß expressionshowednodifferencebetweentheCB-Metand theCB-Hexgroups(p > 0.05);ontheotherhand,thereweredifferencesfor Cox-2 (p < 0.05).
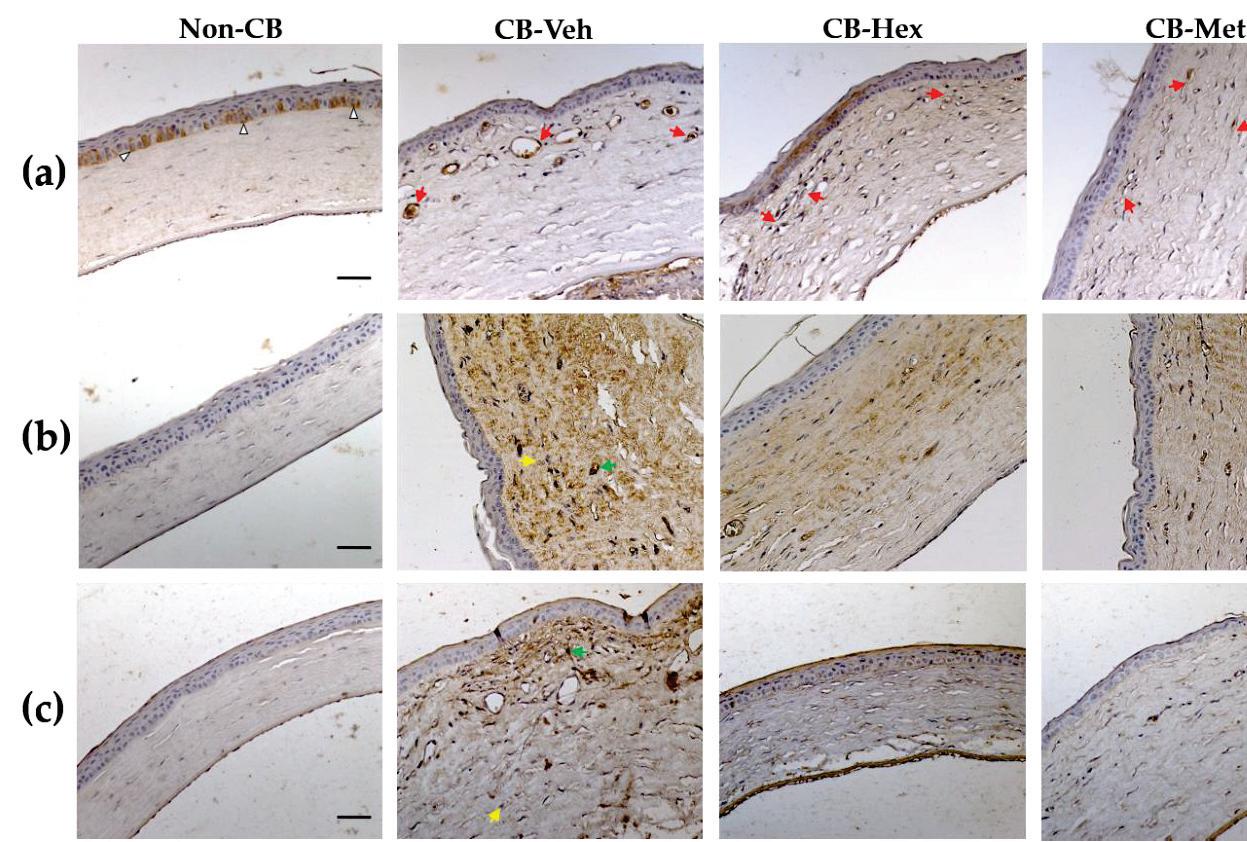

Figure2. MicrographofMetandHexextractsof C.argyrosperma seedintheCBcomparedtothe non-CBandCB-Vehgroups.(a)Nucleistainedwithanti-NF-κBp65(redarrows).(b)Stainingintensity forinterleukin-1β (IL-1β)alongwiththecornealthickness.(c)Cyclooxigenase-2(COX-2)staining inthestudiedgroups.ArrowheadsindicatethecytoplasmicdistributionofNF-κBp65.Yellowand greenarrowsrepresenttheminimumandmaximumstainingintensity,respectively,consideredfor softwareanalysis.(Scalebar = 100 μm).CB:chemicallyburnedcorneas;CB-Veh:CBcorneastreated withthevehicle;CB-Hex:CBcorneastreatedwithhexanicextract;CB-Met:CBcorneastreatedwith methanolicextract.
Figure3. (a)qRT-PCRfor Il-1β,(b) Cox-2,and(c) Vegf-a.Barsaretheexpressionlevelsineachgroup. * p ≤ 0.05,** p ≤ 0.01,and α p ≤ 0.001comparedtotheCB-Vehgroup.CB:chemicallyburnedcorneas; CB-Veh:CBcorneastreatedwiththevehicle;CB-Hex:CBcorneastreatedwithhexanicextract;CB-Met: CBcorneastreatedwithmethanolicextract.
2019, 11,1184
3.3.Anti-AngiogenicEffect
Duetotheanti-inflammatoryeffectintheCB-HexandtheCB-Met,weassessedwhetheritwas relatedtoanattenuationofCNV,bydeterminingthestainingintensityofVEGF-Aanditsreceptors (Figure 4).IntheCB-Veh,VEGF-Awasinthecytoplasmandnucleusoftheepithelial,endothelial, andotherinfiltratedcellswithanintensityof102.02 ± 14.04.AdecreaseinVEGF-Aintensitieswas observedfortheCB-Hex(71 ± 9.11)andCB-Met(61.3 ± 9.59)(p < 0.001)groups.Besides,staining intensitybetweenVEGF-AintheCB-MetandCB-Hexgroupsshoweddifferences(p < 0.05),andin thenon-CBgroupitwasabout16.25 ± 5.25(Figure 4a).The Vegf-a expressionwasalsoconfirmed (Figure 3c).The Vegf-a fortheCB-Hex(2.74 ± 0.34)andCB-Met(2.29 ± 0.23)groupsdecreasedcompared totheCB-Veh(4.40 ± 0.34; p < 0.05and p < 0.01,respectively).
Relevantly,stainingforVEGFR1wasdistributedinendothelialandinflammatorycellsofthe CB-Vehcorneas(54.4 ± 6.8)andwashigherwhencomparedtotheCB-Hex(33.13 ± 5.8; p < 0.0001) andCB-Met(25.47 ± 3.7; p < 0.0001)groups(Figure 4b).Vascularendothelialgrowthfactorreceptor 2immunostainingwaslocalizedinthemembraneregioninendothelialcells,andintheCB-Veh (23.06 ± 3.5)itwashighercomparedtotheCB-Hex(15.67 ± 2.6; p < 0.0001)andtheCB-Met(10.95 ± 2.1; p < 0.0001)groups(Figure 4c).
Figure4. ImmunolocalizationofvascularendothelialgrowthfactorA(VEGF-A)anditsreceptors, (vascularendothelialgrowthfactorreceptor1,VEGFR1,and-receptor2,VEGFR2),inthetreated groups.(a)StainingintensitiesforVEGF-A.(b)and(c)Membranousstaininginendothelialcellsfor VEGFR1andVEGFR2,respectively(redarrows).Redarrowsrepresentstainingintensityconsidered forsoftwareanalysis.(Scalebar = 100 μm).CB:chemicallyburnedcorneas;CB-Veh:CBcorneastreated withthevehicle;CB-Hex:CBcorneastreatedwithhexanicextract;CB-Met:CBcorneastreatedwith methanolicextract.
4.Discussion
Thecorneaisatransparent,avascular,andimmune-privilegedtissue.However,theinflammatory responseandgrowthofnewvesselsinducedbyinfections,autoimmunity,andchemicalburnsmaycause
Nutrients 2019, 11,1184
visionlossandahighrejectionrateofcornealallograftsifnottreatedeffectively[1,25].Recently,ithas beendemonstratedbyhistopathologicalandclinicalobservationinanimalmodelsthatanti-neovascular topicaltreatmentsaresuccessfulatavoidingCNV[8,26].Toexaminethisphenomenon,experimental modelscombinedwithnewtherapeuticstrategieshavebeenused,primarilyaimedatpreserving cornealtransparencythroughbyattenuatingtheinflammatoryandneovascularizationresponses.
Chemicallyburnedcorneashavelongbeenusedforthispurposebecausetheyareaccompanied bytherecruitment/migrationofneutrophilsandmacrophageswithresultantdamagetothe normaltissuestructure.Furthermore,thereleaseofoxidativederivatives,cytokines,chemokines, matrixmetalloproteinases(MMPs),andgrowthfactorsincludingVEGFcaninfluencecorneal angiogenesis [21,27,28].TopicaltreatmentswithmonoclonalantibodiestoVEGF-Aoritsreceptor VEGFR2suppressthemechanismofactionofVEGFinendothelialcells,whereasdexamethasone inhibitsCNVmediatedbysuppressingtheactivityofNF-κB,anddecreasingtheexpressionofIL-1β, COX-2,andVEGF[7,29].Inthesameway,treatmentswithextractsofpropolisand Diospyroskaki, aswellasotherpurifiedphytochemicals(naringeninand( )-Epigallocatechingallate),haveshown adecreaseinCNVthroughdown-regulationofVEGF-A,IL-1β,IL-6,andmetalloproteases,promoting thehealingofcornealwounds[12–14].
Weaimtoevidencetheabilityofthehexaneandmethanolextractsof C.argyrosperma seedto reduceCNVafteraninflammatorystimulusinducedbyachemicalburninratcornea.Tothisend, weexaminedthenuclearlocalizationofNF-κBp65,animportantmarkerfortheoverexpression ofVEGF-A,IL-1β,andCOX-2indamagedcorneas.ThereceptorVEGFR2intheendothelialcells ofcornealstromalneovesselsasanactivemarkerofangiogenesiswasstudied.Angiogenesisis initiatedwhenVEGFR2isactivatedbytyrosinephosphorylationbyVEGF-Abinding.Consecutively, downstreampathwaysareactivated,suchasp38MAPKandERK1/2,producingastrongmitogenic andsurvivalprocess[30,31].Incontrast,suchamitogenicsignalisnotequallyinducedbyVEGFR1. AlthoughVEGFR1bindstoVEGF-AwithahigheraffinitythanVEGFR2,theinductionofVEGFR1 phosphorylationislowanditsdownstreamsignalingisstillpoorlyexplored[32].Vascularendothelial growthfactorreceptor1possessesanti-angiogenicactivitybyavoidingtheunionbetweenVEGF-A andVEGR2.CornealstudiesshowthattheproteolyticenzymeMMP14canshavetheextracellular domainofVEGFR1,convertingitintoasolublereceptor(sVEGFR)thatactsasadecoyforVEGF-A[33]. Nevertheless,VEGFR1indirectlyinducesangiogenesisbystimulatingthemigrationofmonocytes andmacrophagesdirectedtowardsthedamagedmicroenvironment.Forthesereasons,thisstudy evaluatesbothreceptorsbecausetheyareexpressedpredominantlyinendothelialcellsintheangiogenic environment:(1)VEGFR1asamarkerintheinfiltrationofmonocytesandneovessels;and(2)VEGFR2 asanactivemarkerofangiogenesis.Ourresultsshowthatthestainingintensityandexpressionof Vegf-a decreasedalongwiththestainingofVEGFR2andVEGFR1inendothelialcellsofextract-treated corneas.Additionally,decreasesin Il-1β and Cox-2 expressionswerealsoobserved,suggestingthat hexanic-andmethanolic-extractcomponentscanattenuatethesepro-angiogenicfactors,likelythrough alackofnuclearactivationofNF-κB,whichwasalsoobserved.
Treatmentwithhexanolicextractof C.argyrosperma seedshowsarepairingofthecornealdamage associatedwithadecreaseintheexpressionofinflammatoryandangiogenicfactors. Cucurbitapepo seedextracts,containingmainlyalpha-linoleic(ALA),linolenicacids(LA),tocopherols,andsterols, showedeffectivehealingofskinwoundswithacompletere-epithelialization,organizationofcollagen fibers,andabsenceofinflammatorycells[18].Particularly,treatmentwithALAinculturesofcorneal epithelialcellsandwhenitistopicallyappliedtoadryeyeanimalmodelhasanti-inflammatory activity,decreasingthereleaseandexpressionofinflammatoryfactors(TNF-a,IL-6,IL-1β,andIL-8) regulatedbytheNF-κBpathway[34,35].Inaddition,LAdecreasedcornealfluoresceinstainingand wasassociatedwithasignificantdecreaseinthenumberofCD11b(+)cells[36].
Althoughwearestillcharacterizingthebioactivecompoundsinthemethanolicextract,we canspeculatethatthecontentofphytochemicalsissimilartothe C.pepo seed[16].Someofthese componentsincludeflavonoidssuchasquercetin,luteolin,andapigenin,whichatlowconcentration
2019, 11,1184
intakeshaveprotectiveanti-inflammatoryeffectsonhumanretinalpigmentepithelialdamageby hypoxia,inhibitingVEGFandfactorsrelatedtoitsactivation[37].Forexample,quercetininhibitsthe productionofinflammatoryfactorsinVEGF-stimulatedretinalphotoreceptorcells,associatedwith inactivationofNF-κBasaconsequenceoftheblockageofmitogen-activatedproteinkinases(MAPK) andproteinkinaseB(Akt)phosphorylation[38].Nonetheless, C.argyrosperma maydifferinthecontent andtypesofflavonoidsfrom C.pepo.Thiswouldbringusclosertoabetterunderstandingofthe mechanismsofattenuatedangiogenesisbythephytochemicalscontainedinthemethanolextract, whichinturncouldactsynergistically,eitherdirectlyorindirectly,inVEGF-Aregulation.
CornealinflammationeventuallycausesvisionlossduetoCNV.Cornealalkali-injurynot onlyupregulatedNF-κB,IL-1β,andCOX-2expression,italsosignificantlyincreasedVEGFandits receptorsVEGFR1andVEGFR2inendothelialcells.Thisworkdemonstratesforthefirsttime,that methanolicorhexanicextractsof C.argyrosperma seed(400mg/kg/7days)improvethehealingof cornealwoundscausedbyachemicalagentandmaycontributetotheanti-inflammatorypropertiesof thephytochemicalsinitscomposition.Inaddition,asignificantreductionoftheCNVwasrelatedto theattenuationofproangiogenicfactors.Significantly,ourresultsindicatethat C argyrosperma Hex extractisbetterthanMetextractatreducingcornealre-epithelializationtime,improvingthehealing processandthuspreventingtheentranceofmicroorganismsandinflammatorymediatorsintothe deeperlayers,probablythroughtheinhibitionoftheNF-κBpathwayforatleastsevendaysafter cornealalkaliburn.
5.Conclusions
Intakeof Cucurbitaargyrosperma seedmaybeanoptionforpreventingcornealangiogenesis. Inaddition,itmightbenefitwoundhealingorinhibitneovascularizationinotherdegenerative pathologies.Furtherpharmacologicalandphytochemicalstudiesarerequiredtoidentifytheir constituentsandaccuratelyassessthisactivity.
AuthorContributions: Conceptualization,R.M.P.-G.;Formalanalysis,J.F.-E.;Investigation,M.F.E.-M.,F.J.-G., R.M.P.-G.andJ.F.-E.;Methodology,M.F.E.-M.,F.J.-G.,andR.M.P.-G.;Projectadministration,J.F.-E.;Resources, F.J.-G.andR.M.P.-G.;Supervision,J.F.-E.;Visualization,A.L.-O.andJ.F.-E.;Writing—originaldraft,A.L.-O.and J.F.-E.;Writing—reviewandediting,A.L.-O.andJ.F.-E.
Funding: ThisresearchwassupportedbytheHospitalJuárezdeMéxicoandSchoolofChemicalEngineeringand ExtractiveIndustriesfromtheNationalPolytechnicInstitute.
Acknowledgments: WethankJuliaD.Toscano-Garibayforhernumerouscommentsonthemanuscript.
ConflictsofInterest: Theauthorsdeclarenoconflictofinterest.
References
1. Azar,D.T.Cornealangiogenicprivilege:Angiogenicandantiangiogenicfactorsincornealavascularity, vasculogenesis,andwoundhealing(anAmericanOphthalmologicalSocietythesis). Trans.Am.Ophthalmol.Soc. 2006, 104,264–302.
2. Kuwano,T.;Nakao,S.;Yamamoto,H.;Tsuneyoshi,M.;Yamamoto,T.;Kuwano,M.;Ono,M.Cyclooxygenase 2isakeyenzymeforinflammatorycytokine-inducedangiogenesis. FASEBJ. 2004, 18,300–310.[CrossRef]
3. Nakao,S.;Kuwano,T.;Tsutsumi-Miyahara,C.;Ueda,S.;Kimura,Y.N.;Hamano,S.;Sonoda,K.H.;Saijo,Y.; Nukiwa,T.;Strieter,R.M.;etal.InfiltrationofCOX-2-expressingmacrophagesisaprerequisiteforIL-1 beta-inducedneovascularizationandtumorgrowth. J.Clin.Investig. 2005, 115,2979–2991.[CrossRef]
4. Sobolewski,C.;Cerella,C.;Dicato,M.;Ghibelli,L.;Diederich,M.Theroleofcyclooxygenase-2incell proliferationandcelldeathinhumanmalignancies. Int.J.CellBiol. 2010, 2010,215158.[CrossRef]
5. Cursiefen,C.;Chen,L.;Borges,L.P.;Jackson,D.;Cao,J.;Radziejewski,C.;D’Amore,P.A.;Dana,M.R.; Wiegand,S.J.;Streilein,J.W.VEGF-Astimulateslymphangiogenesisandhemangiogenesisininflammatory neovascularizationviamacrophagerecruitment. J.Clin.Investig. 2004, 113,1040–1050.[CrossRef][PubMed]
Nutrients 2019, 11,1184
6. Sivak,J.M.;Ostriker,A.C.;Woolfenden,A.;Demirs,J.;Cepeda,R.;Long,D.;Anderson,K.;Jaffee,B. Pharmacologicuncouplingofangiogenesisandinflammationduringinitiationofpathologicalcorneal neovascularization. J.Biol.Chem. 2011, 286,44965–44975.[CrossRef]
7. Nakao,S.;Hata,Y.;Miura,M.;Noda,K.;Kimura,Y.N.;Kawahara,S.;Kita,T.;Hisatomi,T.;Nakazawa,T.; Jin,Y.;etal.Dexamethasoneinhibitsinterleukin-1beta-inducedcornealneovascularization:Roleofnuclear factor-kappaB-activatedstromalcellsininflammatoryangiogenesis. Am.J.Pathol. 2007, 171,1058–1065. [CrossRef][PubMed]
8. Gupta,D.;Illingworth,C.Treatmentsforcornealneovascularization:Areview. Cornea 2011, 30,927–938. [CrossRef]
9. Sheppard,J.D.;Comstock,T.L.;Cavet,M.E.ImpactoftheTopicalOphthalmicCorticosteroidLoteprednol EtabonateonIntraocularPressure. Adv.Ther. 2016, 33,532–552.[CrossRef][PubMed]
10. Al-Debasi,T.;Al-Bekairy,A.;Al-Katheri,A.;AlHarbi,S.;Mansour,M.Topicalversussubconjunctival anti-vascularendothelialgrowthfactortherapy(Bevacizumab,RanibizumabandAflibercept)fortreatment ofcornealneovascularization. SaudiJ.Ophthalmol. 2017, 31,99–105.[CrossRef][PubMed]
11. Zhou,C.;Robert,M.C.;Kapoulea,V.;Lei,F.;Stagner,A.M.;Jakobiec,F.A.;Dohlman,C.H.;Paschalis,E.I. SustainedSubconjunctivalDeliveryofInfliximabProtectstheCorneaandRetinaFollowingAlkaliBurnto theEye. Investig.Ophthalmol.Vis.Sci. 2017, 58,96–105.[CrossRef]
12. Keshavarz,M.;Mostafaie,A.;Mansouri,K.;Shakiba,Y.;Motlagh,H.R.Inhibitionofcornealneovascularization withpropolisextract. Arch.Med.Res. 2009, 40,59–61.[CrossRef][PubMed]
13. Oguido,A.;Hohmann,M.S.N.;Pinho-Ribeiro,F.A.;Crespigio,J.;Domiciano,T.P.;Verri,W.A.,Jr.; Casella,A.M.B.NaringeninEyeDropsInhibitCornealNeovascularizationbyAnti-Inflammatoryand AntioxidantMechanisms. Investig.Ophthalmol.Vis.Sci. 2017, 58,5764–5776.[CrossRef][PubMed]
14. Yang,S.J.;Jo,H.;Kim,K.A.;Ahn,H.R.;Kang,S.W.;Jung,S.H.DiospyroskakiExtractInhibitsAlkali Burn-InducedCornealNeovascularization. J.Med.Food 2016, 19,106–109.[CrossRef]
15. Kocyan,A.;Zhang,L.B.;Schaefer,H.;Renner,S.S.Amulti-locuschloroplastphylogenyfortheCucurbitaceae anditsimplicationsforcharacterevolutionandclassification. Mol.Phylogenet.Evol. 2007, 44,553–577. [CrossRef]
16. Akomolafe,S.F.;Oboh,G.;Oyeleye,S.I.;Molehin,O.R.;Ogunsuyi,O.B.PhenolicCompositionandInhibitory AbilityofMethanolicExtractfromPumpkin(Cucurbitapepo L)SeedsonFe-inducedThiobarbituricacid reactivespeciesinAlbinoRat’sTesticularTissueIn-Vitro. J.Appl.Pharm.Sci. 2016, 6,115–120.[CrossRef]
17. Yadav,M.;Jain,S.;Tomar,R.;Prasad,G.B.;Yadav,H.Medicinalandbiologicalpotentialofpumpkin: Anupdatedreview. Nutr.Res.Rev. 2010, 23,184–190.[CrossRef]
18. Bardaa,S.;BenHalima,N.;Aloui,F.;BenMansour,R.;Jabeur,H.;Bouaziz,M.;Sahnoun,Z.Oilfrompumpkin (Cucurbitapepo L.)seeds:Evaluationofitsfunctionalpropertiesonwoundhealinginrats. LipidsHealthDis. 2016, 15,73.[CrossRef][PubMed]
19. Medjakovic,S.;Hobiger,S.;Ardjomand-Woelkart,K.;Bucar,F.;Jungbauer,A.Pumpkinseedextract:Cell growthinhibitionofhyperplasticandcancercells,independentofsteroidhormonereceptors. Fitoterapia 2016, 110,150–156.[CrossRef]
20. Sanchez-delaVega,G.;Castellanos-Morales,G.;Gamez,N.;Hernandez-Rosales,H.S.;Vazquez-Lobo,A.; Aguirre-Planter,E.;Jaramillo-Correa,J.P.;Montes-Hernandez,S.;Lira-Saade,R.;Eguiarte,L.E.Genetic Resourcesinthe“CalabazaPipiana”Squash(Cucurbitaargyrosperma)inMexico:GeneticDiversity,Genetic DifferentiationandDistributionModels. Front.Plant.Sci. 2018, 9,400.[CrossRef]
21. Choi,H.;Phillips,C.;Oh,J.Y.;Stock,E.M.;Kim,D.K.;Won,J.K.;Fulcher,S.ComprehensiveModelingof CornealAlkaliInjuryintheRatEye. Curr.EyeRes. 2017, 42,1348–1357.[CrossRef]
22. Atiba,A.;Wasfy,T.;Abdo,W.;Ghoneim,A.;Kamal,T.;Shukry,M.Aloeveragelfacilitatesre-epithelialization ofcornealalkaliburninnormalanddiabeticrats. Clin.Ophthalmol. 2015, 9,2019–2026.[CrossRef][PubMed]
23. Yoeruek,E.;Ziemssen,F.;Henke-Fahle,S.;Tatar,O.;Tura,A.;Grisanti,S.;Bartz-Schmidt,K.U.;Szurman,P. Safety,penetrationandefficacyoftopicallyappliedbevacizumab:Evaluationofeyedropsincorneal neovascularizationafterchemicalburn. ActaOphthalmol. 2008, 86,322–328.[CrossRef][PubMed]
24. Rogers,M.S.;Birsner,A.E.;D’Amato,R.J.Themousecorneamicropocketangiogenesisassay. Nat.Protoc 2007, 2,2545–2550.[CrossRef][PubMed]
25. Dana,M.R.;Streilein,J.W.Lossandrestorationofimmuneprivilegeineyeswithcornealneovascularization. Investig.Ophthalmol.Vis.Sci. 1996, 37,2485–2494.
2019, 11,1184
26. Roshandel,D.;Eslani,M.;Baradaran-Rafii,A.;Cheung,A.Y.;Kurji,K.;Jabbehdari,S.;Maiz,A.;Jalali,S.; Djalilian,A.R.;Holland,E.J.Currentandemergingtherapiesforcornealneovascularization. Ocul.Surf. 2018, 16,398–414.[CrossRef][PubMed]
27. Shakiba,Y.;Mansouri,K.;Arshadi,D.;Rezaei,N.Cornealneovascularization:Moleculareventsand therapeuticoptions. RecentPat.Inflamm.AllergyDrugDiscov. 2009, 3,221–231.[CrossRef][PubMed]
28. Edelman,J.L.;Castro,M.R.;Wen,Y.CorrelationofVEGFexpressionbyleukocyteswiththegrowthand regressionofbloodvesselsintheratcornea. Investig.Ophthalmol.Vis.Sci. 1999, 40,1112–1123.
29. Nakao,S.;Zandi,S.;Lara-Castillo,N.;Taher,M.;Ishibashi,T.;Hafezi-Moghadam,A.Largertherapeutic windowforsteroidversusVEGF-Ainhibitorininflammatoryangiogenesis:Surprisinglysimilarimpacton leukocyteinfiltration. Investig.Ophthalmol.Vis.Sci. 2012, 53,3296–3302.[CrossRef][PubMed]
30. Kim,Y.M.;Hwang,S.;Kim,Y.M.;Pyun,B.J.;Kim,T.Y.;Lee,S.T.;Gho,Y.S.;Kwon,Y.G.Endostatinblocks vascularendothelialgrowthfactor-mediatedsignalingviadirectinteractionwithKDR/Flk-1. J.Biol.Chem. 2002, 277,27872–27879.[CrossRef]
31. Gee,E.;Milkiewicz,M.;Haas,T.L.p38MAPKactivityisstimulatedbyvascularendothelialgrowthfactor receptor2activationandisessentialforshearstress-inducedangiogenesis. J.CellPhysiol. 2010, 222,120–126. [CrossRef]
32. Koch,S.;Claesson-Welsh,L.Signaltransductionbyvascularendothelialgrowthfactorreceptors. ColdSpring Harb.Perspect.Med. 2012, 2,a006502.[CrossRef]
33. Han,K.Y.;Chang,J.H.;Lee,H.;Azar,D.T.ProangiogenicInteractionsofVascularEndothelialMMP14 WithVEGFReceptor1inVEGFA-MediatedCornealAngiogenesis. Invest.Ophthalmol.Vis.Sci. 2016, 57, 3313–3322.[CrossRef]
34. Erdinest,N.;Shmueli,O.;Grossman,Y.;Ovadia,H.;Solomon,A.Anti-inflammatoryeffectsofalphalinolenic acidonhumancornealepithelialcells. Investig.Ophthalmol.Vis.Sci. 2012, 53,4396–4406.[CrossRef]
35. Erdinest,N.;Shohat,N.;Moallem,E.;Yahalom,C.;Mechoulam,H.;Anteby,I.;Ovadia,H.;Solomon,A. Nitricoxidesecretioninhumanconjunctivalfibroblastsisinhibitedbyalphalinolenicacid. J.Inflamm. 2015, 12,59.[CrossRef]
36. Rashid,S.;Jin,Y.;Ecoiffier,T.;Barabino,S.;Schaumberg,D.A.;Dana,M.R.Topicalomega-3andomega-6 fattyacidsfortreatmentofdryeye. Arch.Ophthalmol. 2008, 126,219–225.[CrossRef]
37. Chen,R.;Hollborn,M.;Grosche,A.;Reichenbach,A.;Wiedemann,P.;Bringmann,A.;Kohen,L.Effectsof thevegetablepolyphenolsepigallocatechin-3-gallate,luteolin,apigenin,myricetin,quercetin,andcyanidin inprimaryculturesofhumanretinalpigmentepithelialcells. Mol.Vis. 2014, 20,242–258.[PubMed]
38. Lee,M.;Yun,S.;Lee,H.;Yang,J.QuercetinMitigatesInflammatoryResponsesInducedbyVascular EndothelialGrowthFactorinMouseRetinalPhotoreceptorCellsthroughSuppressionofNuclearFactor KappaB. Int.J.Mol.Sci. 2017, 18,2497.[CrossRef]
© 2019bytheauthors.LicenseeMDPI,Basel,Switzerland.Thisarticleisanopenaccess articledistributedunderthetermsandconditionsoftheCreativeCommonsAttribution (CCBY)license(http://creativecommons.org/licenses/by/4.0/).