[FREE PDF sample] Chronic total occlusions-a guide to recanalization, 3e (nov 29, 2023)_(1119517273)
Chronic Total Occlusions-A Guide to Recanalization, 3e (Nov 29, 2023)_(1119517273)_(Wiley-Blackwell) Ron Waksman
Visit to download the full and correct content document: https://ebookmass.com/product/chronic-total-occlusions-a-guide-to-recanalization-3enov-29-2023_1119517273_wiley-blackwell-ron-waksman/
More products digital (pdf, epub, mobi) instant download maybe you interests ...
Trapped: Brides of the Kindred Book 29 Faith Anderson
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by law. Advice on how to obtain permission to reuse material from this title is available at http://www.wiley.com/go/permissions.
The right of Ron Waksman and Shigeru Saito to be identified as the authors of the editorial material in this work has been asserted in accordance with law.
Registered Offices
John Wiley & Sons, Inc., 111 River Street, Hoboken, NJ 07030, USA
John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
For details of our global editorial offices, customer services, and more information about Wiley products visit us at www.wiley.com.
Wiley also publishes its books in a variety of electronic formats and by print-on-demand. Some content that appears in standard print versions of this book may not be available in other formats.
Trademarks: Wiley and the Wiley logo are trademarks or registered trademarks of John Wiley & Sons, Inc. and/or its affiliates in the United States and other countries and may not be used without written permission. All other trademarks are the property of their respective owners. John Wiley & Sons, Inc. is not associated with any product or vendor mentioned in this book.
Limit of Liability/Disclaimer of Warranty
The contents of this work are intended to further general scientific research, understanding, and discussion only and are not intended and should not be relied upon as recommending or promoting scientific method, diagnosis, or treatment by physicians for any particular patient. In view of ongoing research, equipment modifications, changes in governmental regulations, and the constant flow of information relating to the use of medicines, equipment, and devices, the reader is urged to review and evaluate the information provided in the package insert or instructions for each medicine, equipment, or device for, among other things, any changes in the instructions or indication of usage and for added warnings and precautions. While the publisher and authors have used their best efforts in preparing this work, they make no representations or warranties with respect to the accuracy or completeness of the contents of this work and specifically disclaim all warranties, including without limitation any implied warranties of merchantability or fitness for a particular purpose. No warranty may be created or extended by sales representatives, written sales materials or promotional statements for this work. This work is sold with the understanding that the publisher is not engaged in rendering professional services. The advice and strategies contained herein may not be suitable for your situation. You should consult with a specialist where appropriate. The fact that an organization, website, or product is referred to in this work as a citation and/or potential source of further information does not mean that the publisher and authors endorse the information or services the organization, website, or product may provide or recommendations it may make. Further, readers should be aware that websites listed in this work may have changed or disappeared between when this work was written and when it is read. Neither the publisher nor authors shall be liable for any loss of profit or any other commercial damages, including but not limited to special, incidental, consequential, or other damages.
Title: Chronic total occlusions : A Guide to Recanalization / edited by Ron Waksman, MedStar Washington Hospital Center, Washington, DC, USA, Shigeru Saito, Shonan Kamakura General Hospital, Kamakura City, Japan.
Description: Third edition. | Hoboken, NJ : Wiley-Blackwell, 2024. | Includes bibliographical references and index.
Identifiers: LCCN 2023021444 (print) | LCCN 2023021445 (ebook) | ISBN 9781119517276 (hardback) | ISBN 9781119517221 (pdf) | ISBN 9781119517313 (epub) | ISBN 9781119517337 (ebook)
Henry Ford Hospital & Health System, Detroit, MI, USA
Wayne State University, Michigan, USA
Salman Allana, MD
Minneapolis Heart Institute and Minneapolis Heart Institute Foundation Minneapolis, MN, USA
Lorenzo Azzalini, MD, PhD, MSc
Division of Cardiology Department of Medicine, University of Washington Seattle, WA, USA
Mir Babar Basir, DO, FACC, FSCAI
Henry Ford Hospital Detroit, MI, USA
Craig Basman, MD
Department of Cardiology, Lenox Hill Hospital New York, NY, USA
Nelson L. Bernardo, MD
Section of Interventional Cardiology
MedStar Washington Hospital Center Washington, DC, USA
Emmanouil S. Brilakis, MD, PhD
Minneapolis Heart Institute and Minneapolis Heart Institute Foundation Minneapolis, MN, USA
Nicholas Burke, MD
Minneapolis Heart Institute and Foundation Minneapolis, MN, USA
Mauro Carlino, MD, PhD, MSc
Division of Interventional Cardiology Cardio-Thoracic-Vascular Department San Raffaele Scientific Institute Milan, Italy
Diljon S. Chahal, MD
University of Maryland School of Medicine Baltimore, MD, USA
Niccolò Ciardetti, MD
Structural Interventional Cardiology Department of Clinical and Experimental Medicine
Careggi University Hospital, Italy
George D. Dangas, MD, PhD
Mount Sinai Medical Center, New York, NY, USA; Cardiovascular Research Foundation, New York, NY, USA
Gabby Elbaz-Greener, MD
Department of Cardiology, Hadassah Medical Center & The Faculty of Medicine, Hebrew University of Jerusalem Jerusalem, Israel
Matthew C. Evans, MD
Medical University of South Carolina Charleston, SC, USA
Aloke V. Finn, MD
CVPath Institute, Gaithersburg, MD, USA; University of Maryland School of Medicine Baltimore, MD, USA
Philippe Généreux, MD
Cardiovascular Research Foundation New York, NY, USA
Luis Gruberg, MD, FACC
Mather Hospital
Donald and Barbara Zucker School of Medicine New York, NY, USA
Ankur Gupta, MD, PhD
Piedmont Heart Institute Atlanta, GA, USA
Hidehiko Hara, MD
Minneapolis Heart Institute and Foundation Minneapolis, MN, USA
Thomas Hovasse, MD
Institut Cardiovasculaire Paris Sud (ICPS) Massy, France
John D. Hung, MBChB, PhD, MRCP
Consultant Cardiologist, Liverpool Heart and Chest Hospital Liverpool University Foundation Trust, UK
Hideaki Kaneda, MD, PhD
Okinaka Memorial Institute for Medical Research Tokyo, Japan
Kathleen E. Kearney, MD
University of Washington Medical Center Seattle, WA, USA
Carson Keck, MD
Medical University of South Carolina Charleston, SC, USA
Michael Kim, MD
Department of Cardiology, Lenox Hill Hospital New York, NY, USA
Chad Kliger, MD
Lenox Hill Hospital/Northwell Health Hofstra School of Medicine, New York, NY, USA
Arber Kodra, MD
Department of Cardiology, Lenox Hill Hospital New York, NY, USA
Takao Konishi, MD
CVPath Institute, Gaithersburg, MD, USA
Selcuk Kucukseymen, MD
Structural Interventional Cardiology Department of Clinical and Experimental Medicine Careggi University Hospital, Italy
Katherine J. Kunkel, MD
HonorHealth Scottsdale Shea Medical Center Scottsdale, AZ, USA
Rahul Kurup, MD, PhD
South West Sydney Local Health District (Campbelltown and Liverpool Hospitals) and Sydney Medical School University of Sydney, NSW, Australia
Tak Kwan, MD
Department of Cardiology, Lenox Hill Hospital New York, NY, USA
Thierry Lefèvre, MD, FESC, FSCAI Institut Cardiovasculaire Paris Sud (ICPS) Massy, France
John R. Lesser, MD
Minneapolis Heart Institute and Foundation Minneapolis, MN, USA
Gabriel Maluenda, MD
MedStar Washington Hospital Center Washington, DC, USA
Anbukarasi Maran, MD
Medical University of South Carolina Charleston, SC, USA
Carlo Di Mario, MD, PhD, FESC, FACC, FSCAI, FRCP
Structural Interventional Cardiology, Department of Clinical and Experimental Medicine Careggi University Hospital, Italy
Francesca Maria Di Muro, MD
Structural Interventional Cardiology, Department of Clinical and Experimental Medicine
Careggi University Hospital, Italy
Alessio Mattesini, MD
Structural Interventional Cardiology, Department of Clinical and Experimental Medicine, Careggi University Hospital, Italy
Michael Megaly, MD, MS
Willis Knighton Heart Institute, Shreveport, LA, USA
Ilan Merdler, MD, MHA
MedStar Washington Hospital Center Washington, DC, USA
Asaad Nakhle, MD
Henry Ford Hospital Detroit, MI, USA
Giulia Nardi, MD
Structural Interventional Cardiology
Department of Clinical and Experimental Medicine Careggi University Hospital, Florence, Italy
William J. Nicholson, MD
Emory Heart and Vascular Center, Division of Cardiology Department of Medicine, Emory University School of Medicine, Atlanta, GA, USA
Atsunori Okamura, MD
Cardiovascular Center, Sakurabashi Watanabe Hospital, Osaka, Japan
Ji Eun Park, MD
University of Maryland School of Medicine Baltimore, MD, USA
Apurva Patel, MD
Department of Cardiology, Lenox Hill Hospital New York, NY, USA
Ashish Pershad, MD, MS
Department of Interventional Cardiology Chandler Regional Medical Center, Gilbert, AZ, USA
Sudhir Rathore, MD
Frimley Health NHS Foundation Trust Surrey, UK
Pavan Reddy, MD
Section of Interventional Cardiology
MedStar Washington Hospital Center Washington, DC, USA
Shigeru Saito, MD, FACC, FSCAI, FJCC
Heart Center, Cardiology & Catheterization Laboratories Shonan Kamakura General Hospital Kamakura city, Japan
Negar Salehi, MD
Mount Sinai Medical Center New York, NY, USA
Pratik B. Sandesara, MD
Emory Heart and Vascular Center, Division of Cardiology Department of Medicine, Emory University School of Medicine, Atlanta, GA, USA
Robert S. Schwartz, MD
Minneapolis Heart Institute and Foundation Minneapolis, MN, USA
James C. Spratt, MD, PhD
Consultant Cardiologist, Professor of Interventional Cardiology, St George’s University Hospitals NHS Foundation Trust, London, UK
Bradley H. Strauss, MD, PhD
Schulich Heart Centre, Sunnybrook Health Sciences Centre University of Toronto, Toronto, ON, Canada
Takahiko Suzuki, MD
Toyohashi Heart Centre, Toyohashi, Japan
Yutaka Tanaka, MD, PhD
Shonan Kamakura General Hospital, Kamakura City, Japan
Jasleen Tiwana, MD
University of Washington Medical Center Seattle, WA, USA
On Topaz, MD, FACC, FACP, FSCAI
Professor of Medicine, Duke University School of Medicine Durham, NC, USA
Etsuo Tsuchikane, MD, PhD
Toyohashi Heart Center, Toyohashi, Japan
Ron Waksman, MD, FACC
Section of Interventional Cardiology MedStar Washington Hospital Center Washington, DC, USA
Luiz Fernando Ybarra, MD
London Health Sciences Centre, Schulich School of Medicine & Dentistry, Western University, London, ON Canada
Foreword
Welcome to the world of chronic total occlusion (CTO) intervention, an exciting and rapidly evolving field within interventional cardiology. This book is the third edition within the last 14 years of the popular Chronic Total Occlusions, a testimonial to the advancement in the field and the interest of interventional cardiologists to win the battle to safely and effectively treat CTOs. The book continues to serve as a comprehensive guide for both novice and experienced practitioners who seek to enhance their understanding and skills in the management of CTOs.
The presence of CTOs was initially observed during coronary angiography procedures in the mid-20th century. In the early days of percutaneous coronary intervention (PCI), CTOs were considered challenging to treat due to technical difficulties and lack of suitable equipment and often were referred for surgical revascularization or medical treatment. However, the interventional cardiologist was not satisfied with these alternatives to PCI and strongly believed that successful revascularization of CTOs can relieve symptoms, improve cardiac function, and potentially reduce the need for more invasive procedures like coronary artery bypass grafting (CABG). Others questioned the utility of reanalyzing CTO percutaneously and its impact on mortality and quality of life. With the lack of definitive data from randomized clinical trials, the debate was ongoing. But simultaneously skilled operators from around the globe, with industry support, continued to advance the field and reported several important breakthroughs through the past three decades. Among these were the development of specialized guidewires with improved flexibility and penetration power, which allowed for more successful attempts at crossing CTOs.
In the 1990s, the retrograde approach was introduced in the US by Kahn and Hartzler, and in Japan by the co-editor of this book, Dr. Saito. Navigating and crossing the occlusion via native collaterals and saphenous vein grafts expanded the possibilities for CTO intervention and improved success rates. Finally, dedicated devices and tools were developed specifically for crossing and treating these challenging lesions. These devices include CTO-specific guidewires,
microcatheters, and specialized balloon catheters, as well as devices and techniques to seal perforations.
With the advancement of techniques, devices, and operator experience, the success rates of CTO interventions have significantly improved and now stand in the high 90s success rate, with an acceptably low rate of procedural complications.
A key to the success of the procedure is adequate training courses – a dedicated CTO program within the hospital. These programs comprise skilled interventional cardiologists who have extensive experience in performing CTO interventions.
CTO interventions often require a multidisciplinary approach involving collaboration among interventional cardiologists, imaging specialists, and cardiac surgeons. A team-based approach ensures comprehensive evaluation, appropriate patient selection, and optimal treatment strategies for CTO patients.
To stay updated with the latest advancements and techniques in CTO interventions, interventional cardiologists in the USA participate in continuing medical education activities. These include conferences, workshops, case discussions, and comprehensive textbooks, which provide opportunities to learn from experts and share experiences with peers.
It is important to note that the future of CTO interventions is dynamic and subject to ongoing innovation. These potential developments hold the promise of further improving patient outcomes, expanding the eligibility for CTO interventions, and reducing the complexity and invasiveness of procedures.
Advancements in imaging techniques, such as the integration of intravascular ultrasound and optical coherence tomography to enhance lesion visualization and guide treatment strategies, add to this bright future. Furthermore, the development of novel devices and tools, including bioresorbable scaffolds and drugeluting balloons, may further improve outcomes by promoting vessel healing and reducing restenosis rates.
Ongoing innovation in this field is expected to drive these developments. Artificial intelligence (AI) is poised to play a crucial role in improving CTO
interventions. AI algorithms can aid in lesion assessment, procedural planning, and complication management, offering real-time decision support and enhancing procedural precision.
The third edition of this comprehensive CTO intervention guide aims to provide an in-depth exploration of the principles, techniques, and tools employed in the field. Leading experts from around the world have contributed their knowledge and experience to create a resource encompassing the entire spectrum of CTO management. From fundamental physiology and lesion assessment to procedural planning, equipment selection, and complication management, each chapter delves into key aspects of CTO intervention, emphasizing evidence-based practice and innovation within the CTO community.
Our intent is not only to educate and empower interventional cardiologists but also to foster a culture of collaboration and innovation within the CTO community. In this book, you will find invaluable insights and pearls of wisdom gained from years of clinical practice and research. Additionally, we highlight the importance of a multidisciplinary approach, acknowledging the critical role of imaging specialists, nurses,
technicians, and other healthcare professionals in optimizing patient outcomes.
I would like to extend my special thanks to Jason Wermers for his guidance and assistance in the editorial management process of this book. Dr. Saito and I extend our deepest gratitude to all the contributors who generously shared their expertise and experiences, making this book a comprehensive and valuable resource. We hope that it serves as a guide and source of inspiration for healthcare professionals worldwide who are dedicated to improving patient care through the successful management CTOs.
Ron Waksman, MD, FESC,MSCAI, FACC Professor of Medicine (Cardiology), Georgetown University Associate Director, Cardiology Director, Cardiovascular Research and Advanced Education MedStar Heart and Vascular Institute MedStar Washington Hospital Center Washington, DC, USA
Preface
The first therapeutic PCI was performed by Dr. Gruentzig in 1981. The basic idea was to widen a stenotic lesion in a coronary artery by balloon dilation. The key concept at this time was to guide the burstresistant balloon to the lesion site, preceded by a delicate atraumatic guidewire. The structure of PCI balloon catheter consists of several small parts, which is considered both feasible and best in the current technology at the time.
The complex procedure of PCI is first broken down into its component and functional parts. Then, the aggregate of the parts performs the necessary actions on the stenotic lesion to achieve a good overall result. This concept of first breaking it down into parts and then examining the results as an aggregate of parts is very important. Smaller units of functional parts are easier to improve and bring new functionality to. PCI for chronic total occlusions has also become easier with the use of improved combinations of functional components.
The first time I personally performed PCI for a chronic total occlusion was in 1985 or 1986. The patient was a man in his 50s suffering from exertional angina pectoris due to a chronic totally occluded lesion in his right coronary artery. I reported at an academic conference that I had reopened this patient using a Hartzler LPS (ACS) balloon (2.0 mm), and that six months later, the patient was still good on angiography. To my surprise, one of the leading PCI operators at the time stood up and said, “One-vessel occlusion of the right coronary artery does not affect the prognosis in any way, and unnecessary PCI is unacceptable”. At that time, Dr. Gerald Dorros (who was active in Milwaukee at that time), who was invited to the conference at that time, stood up and said in front of everyone, “A young doctor is presenting such a wonderful treatment, and it is unacceptable for a
doctor not to recognize it.” This was the moment when I embarked on the long road of PCI for chronic total occlusion. Looking back, the success of the PCI of the right coronary CTO at that time was because I could use a Hartzler LPS balloon catheter. And what I have learnt from this experiences is that, before opening the door for a new world, there will be many obstacles, and we have to overcome them.
At that time, PCI for CTO was performed using only antegradde approach without contralateral dye injection. However, as the technique was limited to that, the success rate was slow to improve even with the evolution of balloons and wires.
This situation was broken in the 1990s with the introduction of wires with improved torque control and penetrating power, the importance of contralateral dye injection was emphasized. Although the introduction of Intravascular ultrasound (IVUS) in antegrade approach improved the success rate, the wire was advanced into the false lumen and could not enter in the true lumen.
In the 2000s, the retrograde approach was started, and wires and various devices have been developed to make this approach easier. With the introduction of the retrograde approach, more complex CTO lesions were confronted with PCI than ever before. In the 2010s, Complex high-risk indicated percutaneous coronary interventions (CHIP-PCI) were started. PCI for CTO has thus evolved significantly due to (1) technical developments of operators, (2) introduction of more sophisticated and advanced devices, and (3) improved patient’s management strategies This book documents everything of PCI for CTO from the past to the future.
Shigeru Saito, MD, Shonan Kamakura General Hospital.
PART I Pathology, Indications, and Review of Clinical Trials
CHAPTER 1
The Pathobiology of CTO
Gabby Elbaz-Greener1 & Bradley H. Strauss2,*
1 Department of Cardiology, Hadassah Medical Center & The Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel
2 Schulich Heart Centre, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, ON, Canada
* Corresponding author
Introduction
Chronic total occlusions (CTO) are defined by an occlusion age of 3 months or greater, with angiographic thrombolysis in myocardial infarction (TIMI) flow grade 0 or 1 [1]. Our current understanding of CTO development is based on a limited number of autopsy specimens, imaging studies, and animal CTO models. CTO constitute the most challenging lesions in interventional challenge due to the complexity of the composition and the geometric issues, such as CTO entry/exit and the overall occlusion length. In recent years, additional unique features in specific types of CTO, such as occluded native arteries in patients with bypass surgery and stent CTO have been identified. The challenges of CTO PCI have been the impetus for developing unique interventional equipment and strategies, and innovative biologic manipulations [2, 3].
Human coronary CTO studies
Our current understanding of human coronary CTO pathology is based on a small number of autopsy studies. Srivatsa et al. [4, 5] classified angiographic CTOs in 61 patients according to the age of the occlusions (<1 year vs ≥1 year). The main points were: (1) Angiographic occlusion did not necessarily mean histologic occlusion, with 25% of cases demonstrating antegrade continuity and subtotal occlusion (90–95% obstructed). Severe, but not completely obstructive narrowing, may limit contrast reagent penetration into lesions and thereby overestimate the difficulty of a successful guidewire crossing. This was particularly shown in peripheral arterial
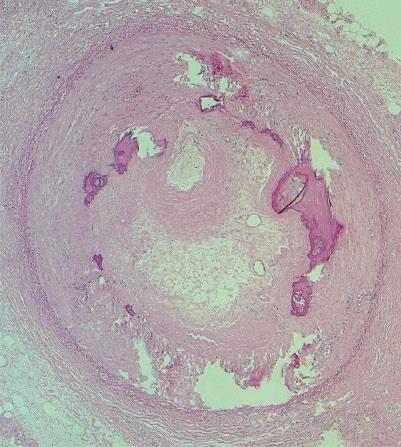
“chronic occlusions” in the lower legs [6], (2) Hard fibrocalcific plaques are a common feature in all CTOs regardless of age, but there is a definite increase in harder plaques in older CTOs, while softer (mainly lipid and loose fibrous tissue) plaques are more likely to be present in CTOs <1 year old, and (3) Recanalization of the CTO intimal plaques by neovascular channels was commonly observed at all time periods, particularly around prominent collections of inflammatory cells (lymphocytes and macrophages) [7] (Figures 1.1A, 1.1B; Figures 1.2A, 1.2B).
Katsuragawa et al. [8] examined autopsy specimens of 10 patients with CTOs, all presumed to be >1 year old. They reported similar findings, namely loose and dense fibrous tissue, atheroma, small recanalization channels, calcification and inflammatory cellular infiltrates, but no fresh thrombus (Figures 1.1A, 1.1B). Small recanalization channels, which traversed the CTO in 4 cases, were correlated with the angiographic appearance of a tapering entrance into the CTO, a well-known favorable sign for successful guidewire crossing [9]. Thus, there is a histologic basis for the presence of softer tissue components and recanalization channels with higher angiographic success rates in guidewire crossing, most frequently evident in CTOs <1-year duration [5].
Recently, additional histology has been published for two specific CTO clinical situations: post bypass and stented coronary lesions.
(1) CTOs in patients with coronary artery bypass graft:
The Canadian CTO Registry reported that > 50% of patients with previous bypass surgery undergoing coronary angiography had a native artery CTO [10]. In fact, the strongest clinical predictor for coronary
Total Occlusions: A Guide to Recanalization, Third Edition. Edited by Ron Waksman and Shigeru Saito.
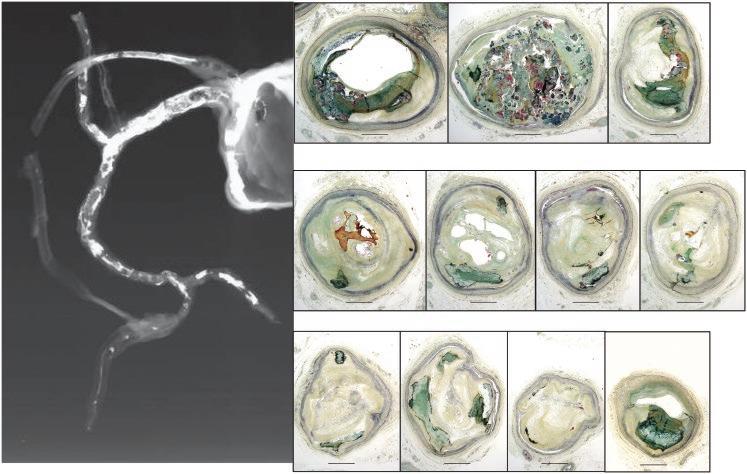
Figure 1.1A Hematoxylin-eosin stained human coronary CTO, demonstrating extensive collagen-rich fibrous tissue, several patches of calcification (Ca), two small microvessels (MV), and a large necrotic area (necrotic). (Courtesy of Dr. Jagdish Butany, University Health Network, Toronto, ON, Canada.)
Figure 1.1B Elastin-trichrome stained human coronary CTO, demonstrating fibrous tissue (lighter staining material inside the lumen), with two distinct areas of calcification (Ca) and two microvessels (MV). M = media. (Courtesy of Dr. Jagdish Butany, University Health Network, Toronto, ON, Canada.)
patients. In 7.5% of patients, the native artery and the graft supplying that territory were both occluded. In particular, a pre-operative proximal stenosis >90% identified the highest risk for a subsequent new CTO. New native artery CTO post bypass had long-term prognostic significance: 21% of these cases had died or experienced nonfatal myocardial infarction or repeated revascularization at a mean of 7.2 years [12].
Sakakura et al. reported on histologic differences in 95 CTOs in patients with and without prior coronary artery bypass grafts (CABG) [13].
In this study, short CTO duration was defined by histology (rather than actual timing), based on organizing thrombi (fibrin) and proteoglycan-rich extracellular matrix, particularly in the middle of the CTO segment (Figure 1.1A). Longer duration (non-bypassed) CTOs in contrast demonstrated more complex features: mainly collagen 1 deposition and moderate calcification (Figure 1.1B). CTOs with bypass grafts were characterized by the heaviest calcification (including the adjacent proximal and distal segments) (Figure 1.2C).
Negative remodeling, defined as reduction in the CTO vessel cross-sectional area relative to the adjacent proximal segment, was least in CTO sections containing organizing thrombus, followed by calcified sections and proteoglycan-rich thrombus sections, but highest in non-calcified CTO sections with collagen type I [13]. This predilection for heavy calcification likely explains the clinical experience of lowest PCI success rates in CTOs which have been previously bypassed [14, 15]. Although bypass surgery is well recognized as the superior revascularization strategy in patients with high SYNTAX score and multivessel disease, there is also a downside of iatrogenic CTO formation, ultimately creating the most technically challenging CTOs for percutaneous revascularization, and a pool of no-option, symptomatic patients.
CTO formation is coronary artery bypass grafting [11]. Angiographic follow-up at one year post coronary artery bypass grafting demonstrated ≥1 new native coronary artery CTO in almost half of the
(2) CTOs in Bare Metal versus Drug Eluting Stents: In-stent occlusion accounts for approximately 12% of all coronary occlusion interventions [16, 17]. The characteristics of chronic stent occlusion (> 3 months post implantation) were described in a detailed pathological analysis of a series of 56 stent occlusions (both bare metal stents [BMS] and drug eluting stent [DES], mainly first generation) [18]. The 5 most common etiologies in order of frequency were (1) acute thrombotic occlusion (>50% of cases), (2) restenosis (>20%, mainly in BMS cases), (3) neoatherosclerosis rupture (10%), and very infrequently, calcified nodules and hypersensitivity reactions. The timing of stent occlusion
relative to stent implantation was 2 years for acute thrombotic, 4.5 years for restenosis and 7.4 years for neoatherosclerosis. The contributing factor most frequently identified was a medial tear (60% of cases), potentially indicative of more aggressive stent sizing. Less frequently, protrusion of a necrotic core, overlapping stents, bifurcation stenting, and stent fracture with complete disruption were also recognized. Neoatherosclerosis (foamy macrophages, necrotic core) was present in 25% of these stent CTO, but neointimal calcification was rarely present, despite a high prevalence of patients with diabetes and renal failure (Figure 1.2D). These findings highlight a number of differences between denovo and stented coronary CTO.
Current paradigm of CTO evolution
The development of CTOs includes several specific stages with unique histologic characteristics present at each stage. The initial acute event leading to the development of a CTO is in many cases a ruptured atherosclerotic plaque with bidirectional thrombus formation [7]. Clinically the arterial occlusion may develop insidiously with minimal symptoms or may present as an acute coronary syndrome. In patients with minimal or no symptoms, the timing of the occlusive event cannot be clearly identified. In fact, the age of approximately 60% of CTO cases cannot be reliably dated by symptoms [10]. In patients with ST segment elevation myocardial infarction (STEMI) not treated with reperfusion therapy, an occluded infarct related artery has been found in 87% of patients within 4 hours, in 65% within 12–24 hours, and in 45% at 1 month [19, 20]. Up to 30% of patients treated with thrombolytic therapy alone have a chronically occluded artery 3–6 months after MI [21]. In patients treated with percutaneous coronary intervention (PCI) during evolving acute myocardial infarction (AMI), approximately 6–11% will have chronic occlusion of an infarct related artery at 6 months, due to either initial treatment failure or late re-occlusion [22].
Characterization of CTO development in human studies is problematic since CTOs are often diagnosed at a very late stage, and data regarding initial stages in their evolution is lacking. Several animal models, particularly rabbit and swine, have been developed to systematically define the development stages of a CTO [10, 23]. However, these models have certain characteristics that could potentially limit their relevance to humans, such as non-coronary location, and
the lack of an underlying atherosclerotic substrate or significant calcification.
Development of CTOs
Acute arterial occlusion due to atherosclerotic plaque rupture with thrombus formation is likely a common initiating event, which then triggers an inflammatory reaction. In a rabbit CTO model, the freshly formed thrombus contains platelets and erythrocytes within a fibrin mesh, which is followed by an invasion of acute inflammatory cells [24]. This early acute inflammatory response (initial 2 weeks) is accompanied by patchy formation of a proteolycan-enriched extracellular matrix and myofibroblast infiltration into the thrombotic occlusion. At the initial part of the intermediate stage (6 weeks), there is marked negative arterial remodeling and disruption of the internal elastic lamina accompanied by intense intraluminal neovascularization and increased CTO perfusion. Total microvessel cross-sectional area increases 2-fold, along with a nearly 3-fold increase in the size of individual intraluminal vessels.
However, by 12 weeks, there is a reduction in both microvessel formation and CTO perfusion, with further declines at the advanced stage (18–24 weeks) This progressive decrease in the CTO perfusion coincides with gradual replacement of proteoglycans by collagen in the extracellular matrix. Human studies have shown collagen and calcium accumulation characterize the later stages of CTO maturation (Figures 1.1 and 1.2). The density of the fibrocalcific tissue is highest at the proximal and distal ends of the lesion compared to the body. Thus, the tissue components of the CTO evolve over time with remarkable spatial variability along the length of the CTO. From a pathobiology standpoint, three specific regions of the CTO have been proposed:
(1) The proximal fibrous cap is a thickened structure at the entrance (the proximal end) of the CTO containing particularly densely packed collagen. It usually contains types I, III, V, and VI of collagen. Type IV collagen has also been observed in calcified tissues [25]. This region represents a distinct physical barrier to crossing into the CTO.
(2) The distal fibrous cap also contains densely packed collagen, but is commonly regarded (although not proven in studies) as a thinner and softer structure compared to the proximal cap. This has been part of the rationale for developing the retrograde approach to cross the CTO.
(3) The main body of CTO
As mentioned earlier, human coronary artery autopsy studies [4, 5, 8] have shown that the lumen of the CTO in some cases contains organized thrombus. Recanalization channels were observed in nearly 60% of lesions. Unlike the preclinical rabbit femoral artery model, the frequency of lumen recanalization and sizes of the channels were similar in different CTO ages. The intimal plaques within the CTO contained collagen, calcium, elastin, cholesterol clefts, foam cells, giant cell atherophagocytes, mononuclear cells (lymphocytes, monocytes), and red blood cells. “Soft” or cholesterol-laden lesions were more prevalent in younger CTOs age (< 1 year); the amount of cholesterol-laden and foam cells declined with advancing CTO age. Older age CTOs typically contained hard fibrocalcific lesions (“hard plaque”).
Extensive recanalization of the intimal plaques by neovascular channels was frequently evident, particularly within and adjacent to the sites infiltrated by inflammatory cells (lymphocytes and macrophages). In some cases, intimal neovascular channels directly communicate with adventitial vasa vasorum. Neovascular channels were also observed in the vascular medial layer; the extent of medial neovascularization was proportional to the cellular inflammation in the intimal plaque. The adventitia of the vessel is usually extensively revascularized in CTOs of all ages. Again, the extent of adventitial neovascularization is correlated to adventitial cellular inflammation. Munce et al. have shown peripheral artery CTO model in a rabbit that a large rise in extravascular vessels surrounding the occluded artery occurred at early time points, which was followed by a significant increase in intravascular vessels within the central body of the occlusion [26]. The temporal and geographic pattern of microvessel formation and the presence of connecting microvessels support the thesis that the extravascular vessels may indeed initiate formation of the intravascular channels within the center of the occlusion. However, as the CTO matures beyond 6 weeks, a reduction in the size and number of central intravascular microchannels was demonstrated, suggesting that many of the vessels in this region become nonfunctional [26].
These microvessels generally range in size from 100 to 200 µm, but can be as large as 500 µm [5]. In contrast to the vasa vasorum which run in radial direction,
these intimal microvessels run within and parallel to the thrombosed parent vessel [27], and therefore have particular relevance for crossing of CTOs as a pathway for guidewire crossing.
Calcification
Calcification, a major predictor of procedure failure [28–30], seems to be particularly determined by coronary occlusion duration. In short duration coronary occlusions (≤3 months), intimal plaque calcification was present in 54% of coronary occlusions, but reached 100% in CTO of >5 years duration [5] (Figure 1.2C). In contrast, insulin-dependent diabetes mellitus was more frequently observed in patients with predominantly cholesterol laden or mixed CTOs than in those with fibrocalcific CTOs [5].
Calcification changes range from crystal formation to tissue that is histomorphologically indistinguishable from bone. Calcification is correlated with chronic kidney disease, diabetes mellitus, and is a consequence of aging. Our understanding of the balance between promotion and inhibition of calcification in the CTO is much more limited.
The process of the CTO calcification is usually simplified into two mechanisms:
(1) Passive process: This requires high concentrations of tissue calcium and phosphate but is recognized as a regulated process [31–34]. It was initially considered that calcium precipitation occurred when apoptotic cell fragments and cholesterol crystals served as a crystallization nidus and the calcium and phosphate concentration approached the salt solubility product in the presence of a lower concentration of local calcium-chelating molecules. The formation of hydroxyapatite crystals in this way is now regarded as a semi-regulated process, and the high phosphate levels might induce vascular smooth muscle cells to differentiate into an osteoblastic phenotype resulting in bone formation.
(2) Active osseous process: This requires recruitment of osteoblasts and osteoclast-like cells into the atherosclerotic plaque. This process can be triggered by immunomodulating cytokines, causing local production of ossification factors such as BMP-2 [34–36], culminating in producing extra osseous bone tissue inside the media and lumen of CTO. Similar to skeletal bone, these bone/cartilage-like structures are subject to resorption by osteoclastlike cells.
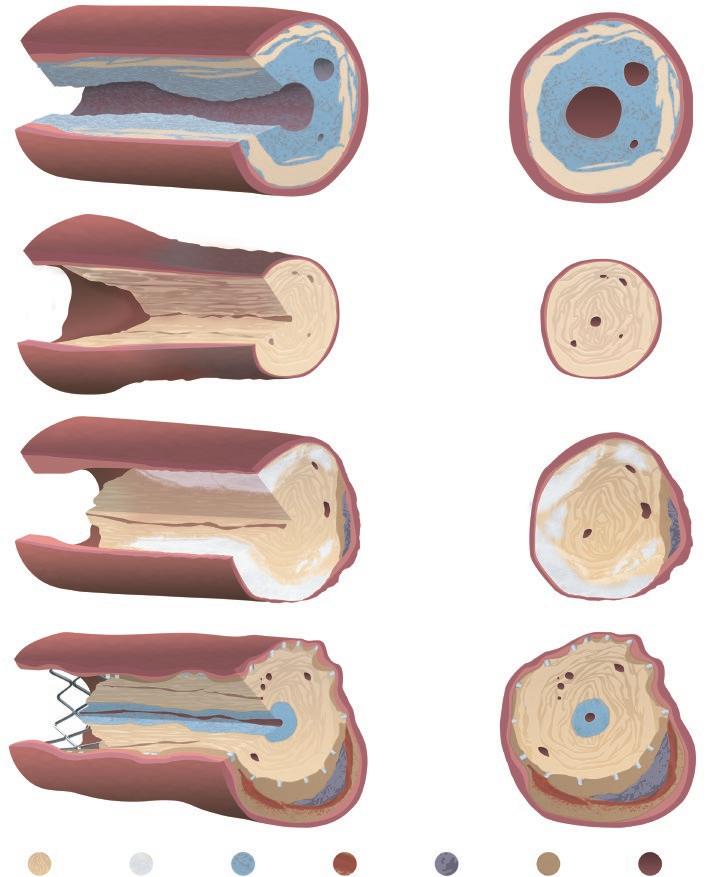
A. CTO<1 year: Proteoglycan-enriched tissue with abundant microvessels near center of CTO, surrounded by recently formed collagen.
B. CTO>1 year: Dense fibrosis tissue, predominantly collagen, with a few microvessels. Prominent negative remodeling in the occluded segment relative to adjacent, non-occluded segment.
C. Calcified CTO: Particularly common in long-standing CTOs in previous bypassed arteries. Collagen and heavy calcification are evident throughout, with calcification
Summary
In this chapter we have summarized the key components of CTOs and suggested an impact of each on
particularly evident in the deeper vessel layers. Atherosclerotic plaques with necrotic core are present at the periphery of artery.
D. In-stent CTO: Small rim of proteoglycan-enriched tissue and microvessels located within the most inner layer of the CTO. Dense surrounding collagen is main constituent, both inside and outside stent struts. Cholesterol plaques also present in deeper vessel layers outside the stent struts. Fibrin deposits may be present around the stent struts and occasionally in center of CTO. The medial layer is compressed by stent struts.
guidewire crossing. Better understanding of the CTO structure incorporating the imaging techniques with advances in guidewires and other plaque modification strategies may enable significant improvements
D. In-stent CTO
C. Calcified CTO
B. CTO >1 year
A. CTO <1 year
in CTO revascularization. The pathophysiology of collagen accumulation and calcification in CTO is now at the frontier of CTO translational to clinical research. A biologic approach using locally delivered collagenase to target matrix collagen within CTOs to enhance guidewire crossing successes with softer guidewires has encouraging results in initial clinical trials [2, 3, 37]. These efforts will hopefully contribute to higher CTO revascularization success rates and a wider application of percutaneous revascularization for appropriate cases in the near future.
References
1 Galassi AR, Brilakis ES, Boukhris M, Tomasello SD, Sianos G, Karmpaliotis D, Di Mario C, Strauss BH, Rinfret S, Yamane M, Katoh O, Werner GS, Reifart N. Appropriateness of percutaneous revascularization of coronary chronic total occlusions: an overview. Eur Heart J 2016; 37: 2692–2700.
2 Strauss BH, Goldman L, Qiang B, Nili N, Segev A, Butany J, Sparkes JD, Jackson ZS, Eskandarian MR, Virmani R. Collagenase plaque digestion for facilitating guide wire crossing in chronic total occlusions. Circulation 2003; 108: 1259–1262.
3 Strauss BH, Osherov AB, Radhakrishnan S, Mancini GB, Manners A, Sparkes JD, Chisholm RJ. Collagenase Total Occlusion-1 (CTO-1) trial: a phase I, dose-escalation, safety study. Circulation 2012; 125: 522–528.
4 Srivatsa S, Holmes D, Jr. The histopathology of angiographic chronic total coronary artery occlusions N changes in neovascular pattern and intimal plaque composition associated with progressive occlusion duration. J Invasive Cardiol 1997; 9: 294–301.
5 Srivatsa SS, Edwards WD, Boos CM, Grill DE, Sangiorgi GM, Garratt KN, Schwartz RS, Holmes DR, Jr. Histologic correlates of angiographic chronic total coronary artery occlusions: influence of occlusion duration on neovascular channel patterns and intimal plaque composition. J Am Coll Cardiol 1997; 29: 955–963.
6 Roy T, Liu G, Shaikh N, Dueck AD, Wright GA. Puncturing Plaques. J Endovasc Ther 2017; 24(1): 35–46.
7 Stone GW, Kandzari DE, Mehran R, Colombo A, Schwartz RS, Bailey S, Moussa I, Teirstein PS, Dangas G, Baim DS, Selmon M, Strauss BH, Tamai H, Suzuki T, Mitsudo K, Katoh O, Cox DA, Hoye A, Mintz GS, Grube E, Cannon LA, Reifart NJ, Reisman M, Abizaid A, Moses JW, Leon MB, Serruys PW. Percutaneous recanalization of chronically occluded coronary arteries: a consensus document: part I. Circulation 2005; 112: 2364–2372.
8 Katsuragawa M, Fujiwara H, Miyamae M, Sasayama S. Histologic studies in percutaneous transluminal coronary angioplasty for chronic total occlusion: comparison of tapering and abrupt types of occlusion and short and long occluded segments. J Am Coll Cardiol 1993; 21: 604–611.
larization of chronic coronary occlusions: an overview. J Am Coll Cardiol 1995; 26: 1–11.
10 Fefer P, Knudtson ML, Cheema AN, Galbraith PD, Osherov AB, Yalonetsky S, Gannot S, Samuel M, Weisbrod M, Bierstone D, Sparkes JD, Wright GA, Strauss BH. Current perspectives on coronary chronic total occlusions: the Canadian Multicenter Chronic Total Occlusions Registry. J Am Coll Cardiol 2012; 59: 991–997.
11 Pereg D, Fefer P, Samuel M, Wolff R, Czarnecki A, Deb S, Sparkes JD, Fremes SE, Strauss BH. Native coronary artery patency after coronary artery bypass surgery. JACC Cardiovasc Interv 2014; 7: 761–767.
12 Pereg D, Fefer P, Samuel M, Shuvy M, Deb S, Sparkes JD, Fremes SE, Strauss BH. Long-term follow-up of coronary artery bypass patients with preoperative and new postoperative native coronary artery chronic total occlusion. Can J Cardiol 2016; 32: 1326–1331.
13 Sakakura K, Nakano M, Otsuka F, Yahagi K, Kutys R, Ladich E, Finn AV, Kolodgie FD, Virmani R. Comparison of pathology of chronic total occlusion with and without coronary artery bypass graft. Eur Heart J 2014; 35: 1683–1693.
14 Michael TT, Karmpaliotis D, Brilakis ES, Abdullah SM, Kirkland BL, Mishoe KL, Lembo N, Kalynych A, Carlson H, Banerjee S, Lombardi W, Kandzari DE. Impact of prior coronary artery bypass graft surgery on chronic total occlusion revascularisation: insights from a multicentre US registry. Heart 2013; 99: 1515–1518.
15 Teramoto T, Tsuchikane E, Matsuo H, Suzuki Y, Ito T, Ito T, Habara M, Nasu K, Kimura M, Kinoshita Y, Terashima M, Asakura Y, Matsubara T, Suzuki T. Initial success rate of percutaneous coronary intervention for chronic total occlusion in a native coronary artery is decreased in patients who underwent previous coronary artery bypass graft surgery. JACC Cardiovasc Interv 2014; 7: 39–46.
16 Azzalini L, Dautov R, Ojeda S, Benincasa S, Bellini B, Giannini F, Chavarria J, Pan M, Carlino M, Colombo A, Rinfret S. Procedural and long-term outcomes of percutaneous coronary intervention for in-stent chronic total occlusion. JACC Cardiovasc Interv 2017; 10: 892–902.
17 Lamelas P, Padilla L, Abud M, Cigalini I, Vaca I, Ordonez S, Santiago R, Tinoco de Paula JE, Ybarra LF, Botelho Da Silva AC, Campos C, Piccaro de Oliveira P, Belli KC, de Quadros AS. In-stent chronic total occlusion angioplasty in the LATAM-CTO registry. Catheter Cardiovasc Interv 2021; 97: E34–E39.
18 Mori H, Lutter C, Yahagi K, Harari E, Kutys R, Fowler DR, Ladich E, Joner M, Virmani R, Finn AV. Pathology of chronic total occlusion in bare-metal versus drug-eluting stents: implications for revascularization. JACC Cardiovasc Interv 2017; 10: 367–378.
19 DeWood MA, Spores J, Notske R, Mouser LT, Burroughs R, Golden MS, Lang HT. Prevalence of total coronary occlusion during the early hours of transmural myocardial infarction. N Engl J Med 1980; 303: 897–902.
20 Betriu A, Castaner A, Sanz GA, Pare JC, Roig E, Coll S, Magrina J, Navarro-Lopez F. Angiographic findings 1 month after myocardial infarction: a prospective study of 259 survivors. Circulation 1982; 65: 1099–1105.
21 Veen G, Meyer A, Verheugt FW, Werter CJ, de Swart H, Lie KI, van der Pol JM, Michels HR, van Eenige MJ. Culprit lesion morphology and stenosis severity in the prediction of reocclusion after coronary thrombolysis: angiographic results of the APRICOT study. Antithrombotics in the Prevention of Reocclusion in Coronary Thrombolysis. J Am Coll Cardiol 1993; 22: 1755–1762.
22 Stone GW, Grines CL, Cox DA, Garcia E, Tcheng JE, Griffin JJ, Guagliumi G, Stuckey T, Turco M, Carroll JD, Rutherford BD, Lansky AJ, Controlled A and Device Investigation to Lower Late Angioplasty Complications I. Comparison of angioplasty with stenting, with or without abciximab, in acute myocardial infarction. N Engl J Med 2002; 346: 957–966.
23 Fefer P, Robert N, Qiang B, Liu G, Munce N, Anderson K, Osherov AB, Ladouceur-Wodzak M, Qi X, Dick A, Weisbrod M, Samuel M, Butany J, Wright G, Strauss BH. Characterisation of a novel porcine coronary artery CTO model. EuroIntervention 2012; 7: 1444–1452.
24 Jaffe R, Leung G, Munce NR, Thind AS, Leong-Poi H, Anderson KJ, Qi X, Trogadis J, Nadler A, Shiff D, Saperia J, Lockwood J, Jacobs C, Qiang B, Teitelbaum A, Dick AJ, Sparkes JD, Butany J, Wright GA, Strauss BH. Natural history of experimental arterial chronic total occlusions. J Am Coll Cardiol 2009; 53: 1148–1158.
25 Katsuda S, Okada Y, Minamoto T, Oda Y, Matsui Y, Nakanishi I. Collagens in human atherosclerosis. Immunohistochemical analysis using collagen type-specific antibodies. Arterioscler Thromb 1992; 12: 494–502.
26 Munce NR, Strauss BH, Qi X, Weisbrod MJ, Anderson KJ, Leung G, Sparkes JD, Lockwood J, Jaffe R, Butany J, Teitelbaum AA, Qiang B, Dick AJ, Wright GA. Intravascular and extravascular microvessel formation in chronic total occlusions a micro-CT imaging study. JACC Cardiovasc Imaging 2010; 3: 797–805.
27 Dible JH. Organisation and canalisation in arterial thrombosis. J Pathol Bacteriol 1958; 75: 1–7.
28 Galassi AR, Tomasello SD, Reifart N, Werner GS, Sianos G, Bonnier H, Sievert H, Ehladad S, Bufe A, Shofer J, Gershlick A, Hildick-Smith D, Escaned J, Erglis A, Sheiban I, Thuesen L, Serra A, Christiansen E, Buettner A, Costanzo L, Barrano G, Di Mario C. In-hospital outcomes of percutaneous coronary intervention in patients with chronic total occlusion: insights from the ERCTO (European Registry of Chronic Total Occlusion) registry. EuroIntervention 2011; 7: 472–479.
29 Morino Y, Abe M, Morimoto T, Kimura T, Hayashi Y, Muramatsu T, Ochiai M, Noguchi Y, Kato K, Shibata Y, Hiasa Y, Doi O, Yamashita T, Hinohara T, Tanaka
H, Mitsudo K, Investigators JCR. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv 2011; 4: 213–221.
30 Tajti P, Karmpaliotis D, Alaswad K, Jaffer FA, Yeh RW, Patel M, Mahmud E, Choi JW, Burke MN, Doing AH, Dattilo P, Toma C, Smith AJC, Uretsky B, Holper E, Wyman RM, Kandzari DE, Garcia S, Krestyaninov O, Khelimskii D, Koutouzis M, Tsiafoutis I, Moses JW, Lembo NJ, Parikh M, Kirtane AJ, Ali ZA, Doshi D, Rangan BV, Ungi I, Banerjee S, Brilakis ES. The hybrid approach to chronic total occlusion percutaneous coronary intervention: update from the PROGRESS CTO registry. JACC Cardiovasc Interv 2018; 11: 1325–1335.
31 Hunt JL, Fairman R, Mitchell ME, Carpenter JP, Golden M, Khalapyan T, Wolfe M, Neschis D, Milner R, Scoll B, Cusack A, Mohler ER, 3rd. Bone formation in carotid plaques: a clinicopathological study. Stroke 2002; 33: 1214–1219.
32 Doherty TM, Asotra K, Fitzpatrick LA, Qiao JH, Wilkin DJ, Detrano RC, Dunstan CR, Shah PK, Rajavashisth TB. Calcification in atherosclerosis: bone biology and chronic inflammation at the arterial crossroads. Proc Natl Acad Sci U S A 2003; 100: 11201–11206.
33 Johnson RC, Leopold JA, Loscalzo J. Vascular calcification: pathobiological mechanisms and clinical implications. Circ Res 2006; 99: 1044–1059.
35 Hosseinkhani H, Hosseinkhani M, Khademhosseini A, Kobayashi H. Bone regeneration through controlled release of bone morphogenetic protein-2 from 3-D tissue engineered nano-scaffold. J Control Release 2007; 117: 380–386.
36 Zheng LW, Cheung LK. Effect of recombinant human bone morphogenetic protein-2 on mandibular distraction at different rates in a rabbit model. Tissue Eng 2006; 12: 3181–3188.
37 Graham JJ, Bagai A, Wijeysundera H, Weisz G, Rinfret S, Dick A, Jolly SS, Schaempert E, Mansour S, Dzavik V, Henriques JPS, Elbarouni B, Vo MN, Teefy P, Goodhart D, Mancini GBJ, Strauss BH, Buller CE. Collagenase to facilitate guidewire crossing in chronic total occlusion PCI-The Total Occlusion Study in Coronary Arteries-5 (TOSCA-5) trial. Catheter Cardiovasc Interv 2022; 99: 1065–1073.
CHAPTER 2
Pathology of Chronic Total Occlusions: Implications for Revascularization
Takao Konishi
Aloke V. Finn
1, Ji Eun Park2,
Diljon S. Chahal
2 &
1,2,*
1 CVPath Institute, Gaithersburg, MD, USA
2 University of Maryland School of Medicine Baltimore, MD, USA
* Corresponding author
Introduction
Chronic total occlusions (CTO) are commonly observed in daily coronary angiography (CAG), occurring in 18–31 % of patients with significant coronary artery disease (CAD) undergoing CAG [1, 2]. Percutaneous coronary intervention (PCI) of CTOs remains challenging, with lower success rates and higher rates of restenosis, as compared to non-occluded lesions [3, 4]. New techniques, device-based innovations, increasing operator experience, and an algorithmic approach has led to increased success rates with CTO-PCI, with current success rates approaching 85–94 % in experienced centers [5, 6]. Incomplete revascularization for CTOs is associated with higher rates of death and worse major adverse cardiac events as compared to complete revascularization in patients with multivessel coronary artery disease [3, 4, 7]. Understanding the pathology of CTOs can be useful for the CTO-PCI strategy and planning, which can facilitate the increased success of CTO-PCI. In this chapter, we will explore the pathological findings of CTOs as they may pertain to successful procedural outcomes.
Histopathology of chronic total occlusions, with and without prior coronary artery bypass grafts
Chronic total occlusions are composed of atherosclerotic and/or thrombotic components that can be composed of multiple layers of different tissues. Angiographic total occlusions are not always consistent with histologic total occlusions, with one study showing that only 22 % of all angiographic CTOs correlated to a 100 % occlusion on histopathology [8]. This is probably expected given the superior resolution of histopathology compared to angiography.
In a previous report, we defined CTOs pathologically as lesions where the lumen area was occupied by proteoglycan and/or collagen with or without neovascularization and chronic inflammation [9].The long-duration CTO (LD-CTO) was defined as a lesion that has a matrix consisting predominantly of collagen without fibrin in any section of CTOs. The short-duration CTO (SD-CTO) was defined as a lesion that has a matrix consisting predominantly of proteoglycan with fibrin. The pathological characteristics of the LD-CTO and the SD-CTO are compared in Figure 2.1 [10].
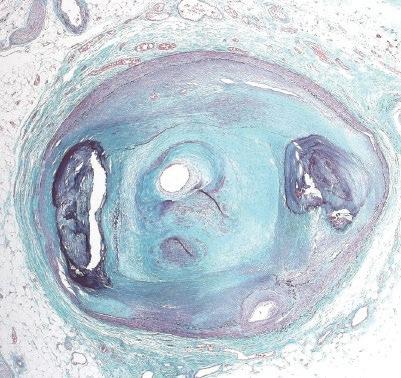
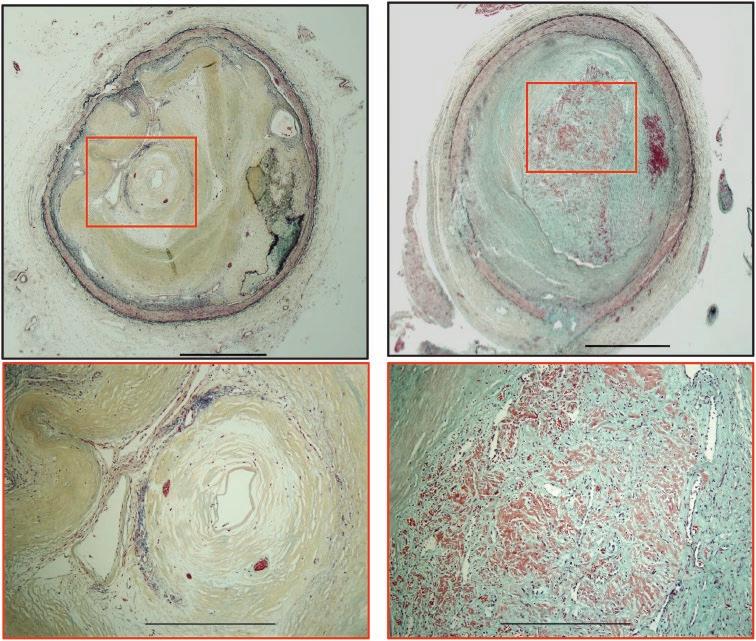
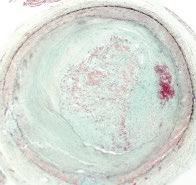
Figure 2.1 Representative images of long-duration CTO and short-duration CTO without coronary artery bypass graft. (A and C) Low-power images of long-duration and shortduration CTO without coronary artery bypass graft. (B and D) High-power images of boxed areas in (A) and (C), respectively.
The matrix is predominantly composed of collagen type I in (B). The matrix predominantly consists of proteoglycan and fibrin in (D). CTO, chronic total occlusion. All sections are stained by Movat Pentachrome. Reproduced with permission from Sakakura et.al., 2014 / Oxford University Press.
Additionally, we classified CTOs into three groups: (1) CTO with coronary artery bypass graft (CABG), defined as having an arterial or venous bypass graft anastomosed distal to the CTO with a duration over 2 years, (2) LD-CTO without previous CABG, (3) SD-CTO without previous CABG (Figures 2.1 and 2.2) [10].Morphologically, CTOs with CABG and SD-CTO tended to be located in the proximal segment of the artery, whereas only half of LD-CTOs were located in the proximal vessel. A histologic comparison of plaque components showed that both the area of organized thrombus and of necrosis were greatest in SD-CTO, followed by LD-CTO, and CTO with CABG. In contrast, calcification area was highest in CTO with CABG, followed by LD-CTO, and SD-CTO. Arterial remodeling was evaluated using remodeling index [ratio of the internal elastic lamina (IEL) area in CTO divided by the largest IEL area in one of the proximal reference sections]. The
remodeling index was the lowest (indicating negative remodeling) in LD-CTO, followed by CTO with CABG, and SD-CTO. To summarize, CTOs with CABG are characterized by calcified plaque and moderate negative remodeling, while LD-CTOs are characterized by severe negative remodeling and moderate calcification (Figure 2.3). SD-CTOs are characterized by abundant organizing thrombi and necrotic cores, with the least negative remodeling. These pathological differences between groups are useful for stratifying the technical difficulty of CTO lesions, which may aid in patient selection and strategic approaches to CTO PCI (Figure 2.3).
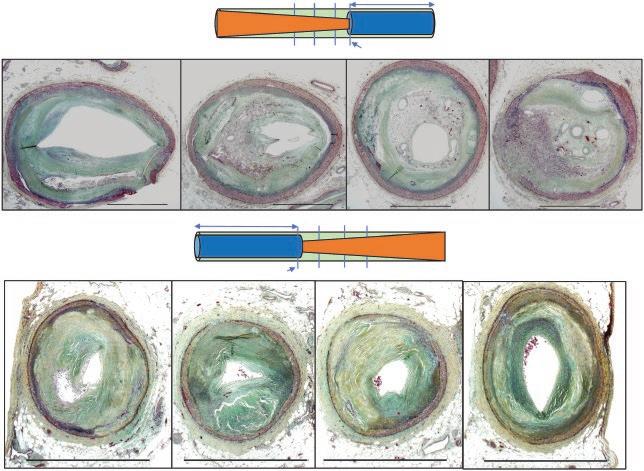
In addition, the lumen pattern was classified as abrupt versus tapered, depending on the degree of narrowing prior to or after the occluded segment (Figure 2.4). Although there was no statistical difference in the prevalence of the lumen pattern between the groups, the abrupt pattern was more
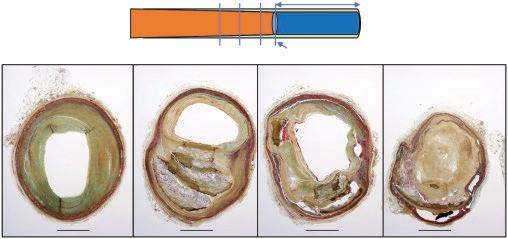
Figure 2.2 A representative case of chronic total occlusion with coronary artery bypass graft. The radiograph (left) shows severe calcification of the vein graft as well as a right coronary artery. P-1 is a proximal segment, and D-1 is the distal segment. Serial CTO images show severe calcification. Note: Percent area calcification in CTO-1 is 70 % and CTO-5 shows five microchannels >200 mm in size. The proximal and
distal sections to CTO show 54 and 48 % area calcification, respectively. CTO, chronic total occlusion; PRC, proximal right coronary artery; MRC, middle right coronary artery; RMB, right marginal branch; DRC, distal right coronary artery; PD, posterior descending artery; P-1, proximal first section; D-1, distal first section. Reproduced with permission from Sakakura et.al., 2014 / Oxford University Press.
Cholesterol clefts
Necrotic core
Calci ed plaque
Fibrin
Collagen Angiogenesis
Healed thrombus
Lesion dif culty
Figure 2.3 Lesion characteristics of three types of CTO lesions. CTO with CABG lesions showed moderate negative remodeling and severe calcification. LD-CTO is characterized by collagen rich plaque with severe negative remodeling and moderate calcification. SD-CTO is
characterized by organized thrombus and fibrin with less negative remodeling and less calcification in the plaque. In summary, CTO with CABG is considered the most challenging lesions, followed by LD-CTO, and SD-CTO in PCI. Adapted from Sakakura et al,2014.
Graft
Abrupt Pattern Morphology
Tapered Pattern Morphology
Figure 2.4 (A) Representative images of the abrupt lumen pattern. Adjacent proximal segment and CTO segment of mid-left anterior descending. Percent stenosis in P-3, P-2, and P-1 is 71, 80, and 71 %, respectively, and was assigned to the abrupt lumen pattern. (B) Representative images of the tapered lumen pattern. Upper panels: adjacent proximal segment and CTO segment of mid-right coronary artery. Percent stenosis in P-3, P-2, and P-1 is 70, 91, and 90 %, respectively; this case
frequently seen in the proximal lumen of the CTO, compared with the distal lumen, which may explain the recent increase in procedural success with the retrograde approach which may be more fruitful in cases of proximal versus distal lumen occlusion. Microchannels over 200µm in diameter were rarely observed in all three groups, which may indicate more favorable CTO crossing with coronary guidewires with tapered tip diameters <0.014� (360 uM) [11].
was assigned as the tapered lumen pattern, because of the gradual opening of the lumen. Lower panels: the adjacent distal segment and CTO segment of mid-left anterior descending. Percent stenosis in D-3, D-2, and D-1 is 85, 91, and 95 %, respectively; this case was assigned as the tapered lumen pattern because of the gradual opening of the lumen. CTO, chronic total occlusion. Reproduced with permission from Sakakura et.al., 2014 / Oxford University Press.
Pathology of in-stent chronic total occlusion and its difference from native CTO
In-stent chronic total occlusions (IS-CTO) are also not uncommonly observed in PCI. The prevalence of IS-CTO is estimated to be 5–13 % of all CTOs [12–14]. The major etiologies of IS-CTO are acute thrombotic occlusion, restenosis, and plaque rupture from neoatherosclerosis [15].A representative
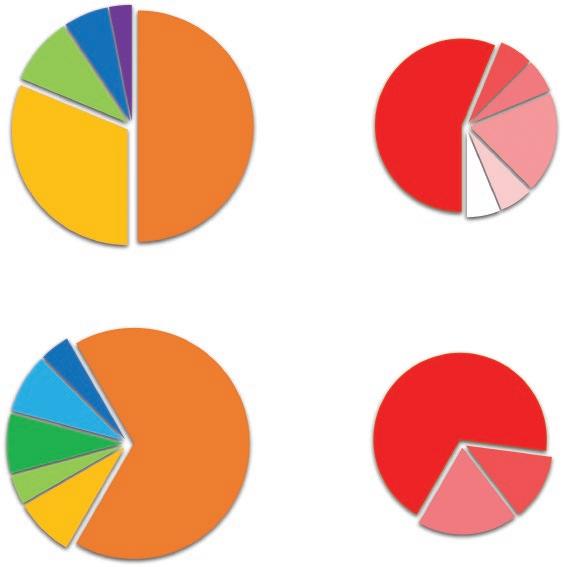
case study for each etiology of IS-CTO for bare metal stent (BMS) and a drug-eluting stent (DES) is depicted in Figures 2.5–2.7. The frequency of each etiology of IS-CTO and the major contributing risk factor for acute thrombotic occlusion are shown in Figure 2.8. Acute thrombotic occlusion was the most frequent cause of IS-CTO in both BMS (50 %) and DES (67 %), with medial tear being the major contributing risk factor for both BMS and DES (56 % and 69 %, respectively). The second most frequent cause was restenosis (31 % of BMS; 8 % of DES; p=0.08). Plaque rupture from neoatherosclerosis was seen in 9 % of BMS and 4 % of DES. Overall, neointi-
mal calcification was minimal in IS-CTO. However, in BMS, neointimal calcification was observed in 3 lesions with in-stent neoatherosclerotic rupture and one lesion involving an in-stent calcified nodule. In the cases with etiologies of acute thrombotic occlusion, restenosis, neointimal erosion, and hypersensitivity, neointimal calcification were not observed. Thus, it can be said that IS-CTOs differ from native CTOs, especially in terms of intimal calcification, which is seen more frequently in native CTO, presumably due to a higher prevalence of acute thrombotic occlusion in IS-CTO. In addition, there was a tendency toward longer length of collagen
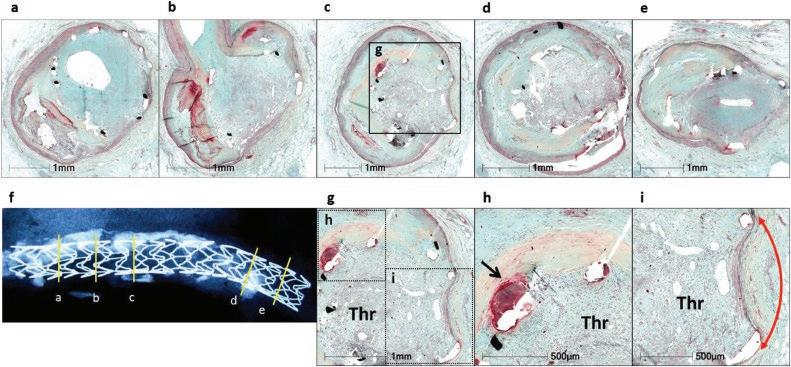
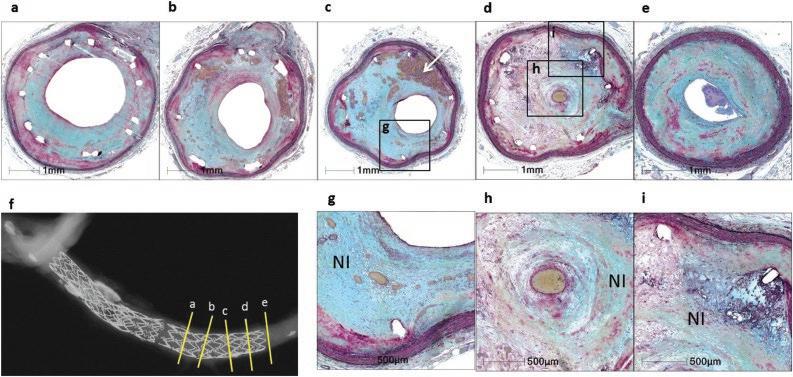
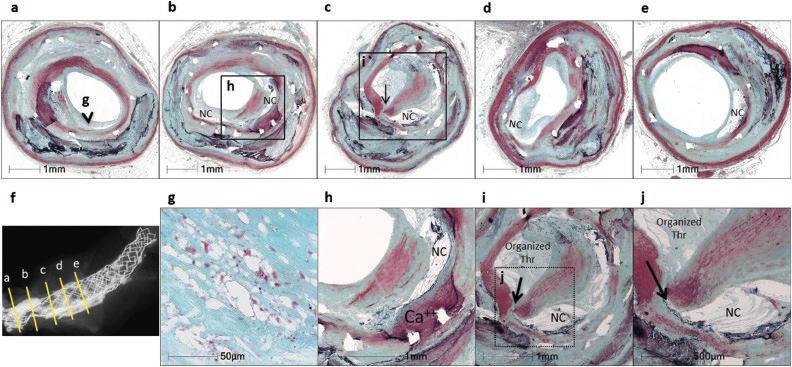
Figure 2.5 In-stent CTO due to acute thrombotic occlusion. Serial cross-sections of BMS (A, a to c are from the proximal segment, and d and e are from the distal stent) and zotarolimus-eluting stent (B, a to e), and corresponding radiographs (f) illustrating the site of the sectioning, whereas high-power images are shown in g to i. Both stents had been implanted for 2 years in 2 different patients. Organized thrombus is in direct
contact with the stent struts. Red arrows indicate the extent of medial tear (in i in A and g to i in B). Black arrow in h in A indicates persistent fibrin. (All sections stained by Movat pentachrome.) Thr, organized thrombus in A and organized and organizing thrombus in B; BMS, bare-metal stent. Reproduced with permission from Mori et.al., 2017 / American College of Cardiology Foundation.
(B)
(A)
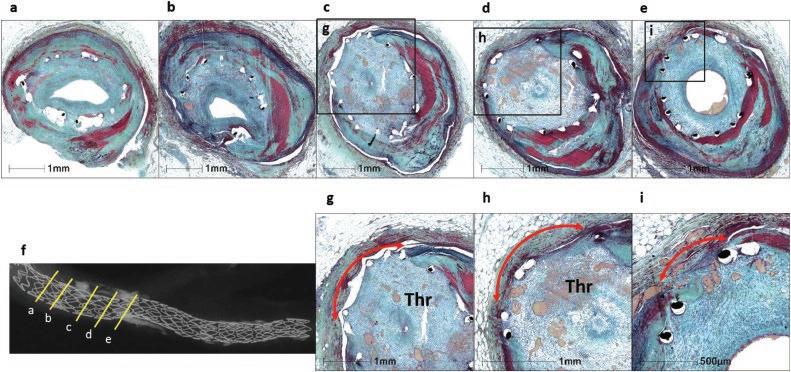
Figure 2.6 Restenosis. Cross-sectional histology of BMS (A) implanted for 4 years and sirolimus-eluting stent (B) implanted for 2 years in 2 different patients. Note the in-stent region in both cases is predominantly occupied by excessive neointimal formation. In a and g in A, the neointima is rich in elastic tissue (white arrow) close to the lumen (illustrated at high power in g) whereas the peristrut region shows some angiogenesis (asterisk) (g); whereas c and d show neointimal tissue rich in smooth muscle cells and proteoglycans and collagen (high-power
and smooth muscle cell-rich tissue in the proximal and distal fibrous caps of the BMS CTOs than in DES. These findings suggest a similar approach to IS-CTO as native CTO-PCI, with special attention to BMS lesions, which may require stiffer wires than DES lesions. This also suggests that DES when they occlude may have delayed thrombus organization.
images shown in h and i). B shows restenotic sirolimuseluting stent. The lesion consists of smooth muscle cells in a proteoglycan-rich matrix with interspersed fibrin (white arrow in c). Total occlusion (defined by 99 % luminal narrowing) is observed in section d and high-power images of boxed areas in c and d are shown in g to i. (All sections stained by Movat pentachrome.) BMS, bare-metal stent; NI, neointima. Reproduced with permission from Mori et.al., 2017 / American College of Cardiology Foundation.
Clinical implications from a pathological point of view
These histopathologic data suggest that CTOs with previous CABG are likely the most challenging lesions mainly because of the severe calcification, compared to the other types of CTOs, including
(B)
(A)
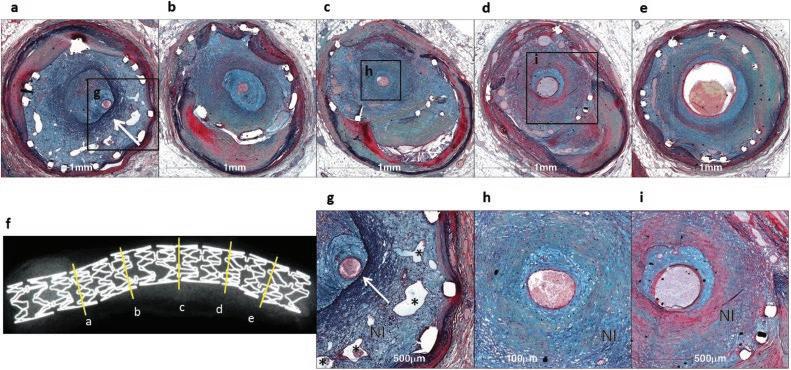
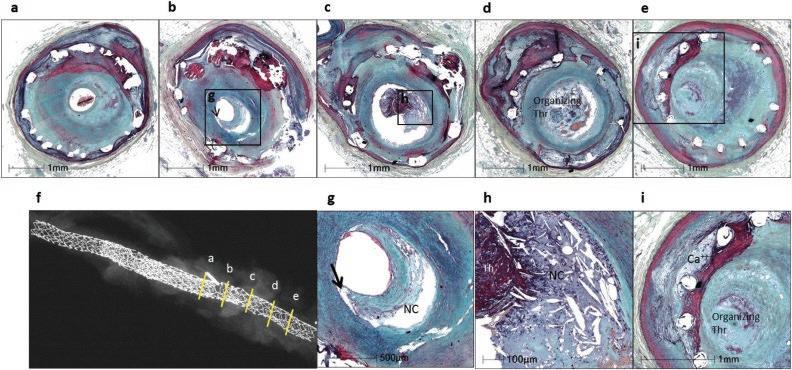
Figure 2.7 Neoatherosclerotic rupture. Cross-sectional histology of BMS (A) implanted for 8 years and paclitaxeleluting stent (PES) implanted for 5 years (B) in 2 different patients. (A) The site of serial sections (a to e) are taken from the proximal region of the stent as seen in the radiograph in f. All serial sections in a–e show presence of in-stent neoatherosclerosis. Note rupture site in c (see arrow) and corresponding high-power images in g to j. The arrowhead in a points to the site of foamy macrophage infiltration, which is highlighted in g, whereas necrotic core (NC) is observed in b to e. Black arrow indicates rupture site in c, i, and j. The lumen is occupied by a NC and calcified (Ca++) plaque (c and i). An organized thrombus is observed
IS-CTO, when considering complete revascularization by PCI. Clinically, the procedural success rate of CTO PCI is lower in patients with prior CABG, compared to patients without prior CABG [16, 17]. Azzalini et al. showed that the procedural success was lower in patients who had undergone CABG (81 % vs 87 %; P = 0.001) [16],and Tajti et al. showed that prior CABG patients had lower procedural success (82 %
in the lumen in c, i, and j. (B) Serial sections (a to e) are taken from distal portion of PES, shown in the radiograph in f. Note IS-neoatherosclerosis is observed in b and c. A necrotic core with a thin cap (arrow) is shown at high power in g, which is highlighted from boxed area in b. Similarly, the boxed area from c is shown at high power in h and highlights the rupture site of the necrotic core with overlying thrombus (Thr). Neointimal calcification (Ca++) around stent struts is observed in a to e and can be appreciated at high power in i. (All sections stained by Movat pentachrome.) BMS, bare-metal stent. Reproduced with permission from Mori et.al., 2017 / American College of Cardiology Foundation.
versus 87 %, P<0.001) [17].This is probably because of lesion calcification and negative remodeling, which have been previously associated with higher incidence of CTO PCI failure [17, 18] and are frequently seen in CTOs with CABG [10].LD-CTOs are characterized by severe negative remodeling and moderate calcification, which increase the complexity of PCI. SD-CTOs are characterized by abundant organizing
(B)
(A)
P=0.13
Etiology of In-stent CTO
Major Contributing Risk Factor In Acute Thrombotic Occlusion
Figure 2.8 The frequency of each etiology for IS-CTO and the major contributing risk factor for acute thrombotic occlusion. Pie chart on the left illustrates the etiology of in-stent CTO (upper BMS, lower DES), and the pie charts on the right illustrate the major contributing risk factor for acute thrombotic occlusion. There were more frequent
thrombi and necrotic cores, and the least negative remodeling and calcification. SD-CTOs should be attempted via the antegrade approach because the components of such lesions are loose tissue and easier to penetrate (Figure 2.3). Since the major etiology of IS-CTO is thrombotic occlusion (Figure 2.8), an antegrade approach using direction-controlled wiring technique can be effective. Because the abrupt lumen pattern was more frequently observed in the proximal lumen, compared to the distal lumen in CTOs, switching the strategy from the antegrade approach to the retrograde approach when progress is not made using antegrade approach may facilitate crossing. Careful review of angiography and coronary computed tomography, with intravascular imaging when necessary, is important to predict the components of plaque in CTOs to aid in determining lesion complexity and strategy to facilitate crossing.
P=0.11
acute thrombotic occlusion lesions in DES versus BMS, whereas restenosis was a more frequent cause of CTO in BMS versus DES. All other causes were observed in <10 % of lesions, and the differences did not reach significance. BMS, bare-metal stent; CTO, chronic total occlusion; DES, drug-eluting stent.
Conclusions
The detailed understanding of pathological characteristics of CTOs can be useful for the procedural success of CTO-PCI. There are several differences between the types of CTO lesions in terms of plaque morphologic characteristics, including thrombotic and calcific components, which can be affected by the presence of coronary artery bypass grafts, or bare metal versus drugeluting stents. This in turn can influence the PCI strategies used. Furthermore, an abrupt pattern in the proximal lumen and tapered pattern in the distal lumen may indicate a favorable retrograde approach to crossing for CTO-PCI. Further research into the pathological correlates to CTOPCI will hopefully continue to lead to higher procedural success rates.
References
1 Fefer P, Knudtson ML, Cheema AN, Galbraith PD, Osherov AB, Yalonetsky S, Gannot S, Samuel M, Weisbrod M, Bierstone D et al. Current perspectives on coronary chronic total occlusions: the Canadian Multicenter Chronic Total Occlusions Registry. J Am Coll Cardiol 2012; 59: 991–997. doi: 10.1016/j.jacc.2011.12.007.
2 Jeroudi OM, Alomar ME, Michael TT, El Sabbagh A, Patel VG, Mogabgab O, Fuh E, Sherbet D, Lo N, Roesle M et al. Prevalence and management of coronary chronic total occlusions in a tertiary Veterans Affairs hospital. Catheter Cardiovasc Interv 2014; 84: 637–643. doi: 10.1002/ccd.25264.
3 Farooq V, Serruys PW, Garcia-Garcia HM, Zhang Y, Bourantas CV, Holmes DR, Mack M, Feldman T, Morice MC, Stahle E et al. The negative impact of incomplete angiographic revascularization on clinical outcomes and its association with total occlusions: the SYNTAX (Synergy Between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery) trial. J Am Coll Cardiol 2013; 61: 282–294. doi: 10.1016/j.jacc.2012.10.017.
4 Hwang D, Park J, Yang HM, Yang S, Kang J, Han JK, Park KW, Kang HJ, Koo BK, Kim HS. Angiographic complete revascularization versus incomplete revascularization in patients with diabetes mellitus. Cardiovasc Diabetol 2022; 21: 56. doi: 10.1186/s12933-022-01488-7.
5 Maeremans J, Walsh S, Knaapen P, Spratt JC, Avran A, Hanratty CG, Faurie B, Agostoni P, Bressollette E, Kayaert P et al. The hybrid algorithm for treating chronic total occlusions in Europe: the RECHARGE registry. J Am Coll Cardiol 2016; 68: 1958–1970. doi: 10.1016/j.jacc.2016.08.034.
6 Wu EB, Brilakis ES, Mashayekhi K, Tsuchikane E, Alaswad K, Araya M, Avran A, Azzalini L, Babunashvili AM, Bayani B et al. Global chronic total occlusion crossing algorithm: JACC state-of-the-art review. J Am Coll Cardiol 2021; 78: 840–853. doi: 10.1016/j.jacc.2021.05.055.
7 Nagaraja V, Ooi SY, Nolan J, Large A, De Belder M, Ludman P, Bagur R, Curzen N, Matsukage T, Yoshimachi F et al. Impact of incomplete percutaneous revascularization in patients with multivessel coronary artery disease: a systematic review and meta-analysis. J Am Heart Assoc 2016; 5. doi: 10.1161/JAHA.116.004598.
8 Srivatsa SS, Edwards WD, Boos CM, Grill DE, Sangiorgi GM, Garratt KN, Schwartz RS, Holmes DR, Jr. Histologic correlates of angiographic chronic total coronary artery occlusions: influence of occlusion duration on neovascular channel patterns and intimal plaque composition. J Am Coll Cardiol 1997; 29: 955–963. doi: 10.1016/ s0735-1097(97)00035-1.
9 Yahagi K, Kolodgie FD, Otsuka F, Finn AV, Davis HR, Joner M, Virmani R. Pathophysiology of native coronary, vein graft, and in-stent atherosclerosis. Nat Rev Cardiol 2016; 13: 79–98. doi: 10.1038/nrcardio.2015.164.
10 Sakakura K, Nakano M, Otsuka F, Yahagi K, Kutys R, Ladich E, Finn AV, Kolodgie FD, Virmani R. Comparison of pathology of chronic total occlusion with and without coronary artery bypass graft. Eur Heart J 2014; 35: 1683–1693. doi: 10.1093/eurheartj/eht422.
11 Rossi JE, Nair R, Ellis SG, Kapadia SR, Khatri JJ. Use of polymer-jacketed, tapered-tip, low-force guidewires with composite-core, dual-coil design as part of the antegrade approach to coronary chronic total occlusions. J Invasive Cardiol 2020; 32: 161–168.
12 Werner GS, Moehlis H, Tischer K. Management of total restenotic occlusions. EuroIntervention 2009; 5(Suppl D): D79–83.
13 Azzalini L, Dautov R, Ojeda S, Benincasa S, Bellini B, Giannini F, Chavarria J, Pan M, Carlino M, Colombo A et al. Procedural and long-term outcomes of percutaneous coronary intervention for in-stent chronic total occlusion. JACC Cardiovasc Interv 2017; 10: 892–902. doi: 10.1016/j.jcin.2017.01.047.
14 Miura K, Tanaka H, Kishi K, Muramatsu T, Okada H, Oikawa Y, Kawasaki T, Yoshikawa R, Okamura A, Tsuchikane E. Impact of timing and treatment strategy on coronary perforation during percutaneous coronary intervention for chronic total occlusion. Am J Cardiol 2022; 172: 26–34. doi: 10.1016/j.amjcard. 2022.02.019.
15 Mori H, Lutter C, Yahagi K, Harari E, Kutys R, Fowler DR, Ladich E, Joner M, Virmani R, Finn AV. Pathology of chronic total occlusion in bare-metal versus drugeluting stents: implications for revascularization. JACC Cardiovasc Interv 2017; 10: 367–378. doi: 10.1016/j. jcin.2016.11.005.
16 Azzalini L, Ojeda S, Karatasakis A, Maeremans J, Tanabe M, La Manna A, Dautov R, Ybarra LF, Benincasa S, Bellini B et al. Long-term outcomes of percutaneous coronary intervention for chronic total occlusion in patients who have undergone coronary artery bypass grafting vs those who have not. Can J Cardiol 2018; 34: 310–318. doi: 10.1016/j.cjca.2017.12.016.
17 Tajti P, Karmpaliotis D, Alaswad K, Jaffer FA, Yeh RW, Patel M, Mahmud E, Choi JW, Burke MN, Doing AH et al. In-hospital outcomes of chronic total occlusion percutaneous coronary interventions in patients with prior coronary artery bypass graft surgery. Circ Cardiovasc Interv 2019; 12: e007338. doi: 10.1161/ CIRCINTERVENTIONS.118.007338.
18 Brilakis ES, Mashayekhi K, Tsuchikane E, Abi Rafeh N, Alaswad K, Araya M, Avran A, Azzalini L, Babunashvili AM, Bayani B et al . Guiding principles for chronic total occlusion percutaneous coronary intervention. Circulation 2019; 140 : 420–433. doi: 10.1161/CIRCULATIONAHA.119.039797.
CHAPTER 3
Indications and Guidelines of PCI for CTO
Ilan Merdler, Gabriel Maluenda & Ron Waksman*
MedStar Washington Hospital Center, Washington, DC, USA
* Corresponding
author
Introduction
Chronic total occlusions (CTOs) are completely occluded coronary arteries with no flow and an estimated duration of at least 3 months. They are found in about one-quarter of patients undergoing coronary angiography [1, 2]. In recent years, CTO percutaneous coronary intervention (PCI) has seen the development of enhanced techniques, along with greater equipment and operator experience, and success rates of 80% have been reported [3]. However, a 30-day mortality rate of over 1% and an almost 5% rate of perforations were also reported [4]. There are 7 widely accepted principles [5] for CTO-PCI: ischemic symptom improvement as the primary indication, in-depth planning, microcatheters for optimal manipulation, combination of antegrade and retrograde approaches, efficient change of technique, specific CTO-PCI expertise, and optimum stent expansion. In this chapter, we will discuss the indications and guidelines of CTO-PCI and the relevant evidence.
Outcome
benefits associated with CTO-PCI
Symptom improvement is the primary indication for CTO-PCI. Two randomized control trials [6, 7] (Table 3.1) and several observational trials [3] have shown improvement in symptoms in these patients. However, randomized trials have not succeeded in demonstrating the efficacy of CTO revascularization for hard endpoints such as mortality, myocardial infarction, stroke, or heart failure [8]. Thus, the main indication for CTO-PCI currently is symptom control.
Symptom relief
Successful PCI of CTO has been associated with important symptomatic relief when compared to failed procedures. In the TOAST-GISE (Total Occlusion Angioplasty Study-Societa Italiana di Cardiologia Invasiva) multi-center study conducted on 369 patients with CTOs > 30 days of duration, patients with successful CTO-PCI were more frequently free of angina (88.7%) compared to patients who had an unsuccessful procedure (75%) at 1-year follow-up (p = 0.008) [9]. The results of the FACTOR trial (FlowCardia’s Approach to Chronic Total Occlusion Recanalization), conducted in 125 patients and based on the Seattle Angina Questionnaire (SAQ) performed at baseline and 1 month after CTO-PCI, showed that procedural success was independently associated with angina relief (SAQ delta among successful and unsuccessful PCI = 9.5 points, p = 0.019), improved physical activity (SAQ delta = 13.1 points, p = 0.001), and enhanced quality of life (SAQ delta = 20.3 points, p < 0.001), which was greater in symptomatic patients than in asymptomatic patients [10]. The EuroCTO multicenter trial randomly assigned 396 patients to CTO-PCI versus optimal medical therapy alone. At 1 year, in comparison with patients randomly assigned to medical therapy only, CTO-PCI patients had greater improvement in angina frequency (subscale change difference, 5.23; 95% CI, 1.75–8.71; P = 0.003) and quality of life (subscale change difference, 6.62; 95% CI, 1.78–11.46; P = 0.007), as assessed with the SAQ [6]. The IMPACTOR-CTO trial (Impact on Inducible Myocardial Ischemia of Percutaneous Coronary Intervention versus Optimal Medical Therapy in
Chronic Total Occlusions: A Guide to Recanalization, Third Edition. Edited by Ron Waksman and Shigeru Saito.