ContEnts
preface xix
Part o n E drugs in society/ drugs in our Lives 1
Chapter 1
Drugs and Behavior today 1
By the Numbers . . . 2
Social Messages About Drug Use 3
Two Ways of Looking at Drugs and Behavior 4
A Matter of Definition: What Is a Drug? 5
■ hE a L th Lin E : Defining Drugs: Olive Oil, Curry Powder, and a Little Grapefruit? 6
Instrumental Drug Use/Recreational Drug Use 6
Drug Misuse or Drug Abuse? 7
■ d rugs . . in f o C us: Drug Abuse and the College Student: An Assessment Tool 8
Drugs in Early Times 9
Drugs in the Nineteenth Century 10
Drugs and Behavior in the Twentieth Century 11
Drugs and Behavior from 1945 to 1960 12
Drugs and Behavior after 1960 12
■ Qui C k Con CEP t Ch EC k 1.1: Understanding the History of Drugs and Behavior 13
Present-Day Attitudes toward Drugs 14
Patterns of Drug Use in the United States 14
Illicit Drug Use among High School Seniors 15
Illicit Drug Use among Eighth Graders and Tenth Graders 16
Illicit Drug Use among College Students 16
Alcohol Use among High School and College Students 16
Tobacco Use among High School and College Students 17
Drug Use and Drug Perceptions 17
Illicit Drug Use among Adults Aged Twenty-Six and Older 18
Making the Decision to Use Drugs 19
■ Qui C k Con CEP t Ch EC k 1.2: Understanding Present-Day Drug Use in the United States 19
Specific Risk Factors 19
Specific Protective Factors 21
Present-day Concerns 21
Club Drugs 21
Nonmedical Use of Prescription Pain Relievers 21
■ d rugs . . . in f o C us: Facts about Club Drugs 22
Nonmedical Use of Prescription Stimulant Medications 23
Nonmedical Use of Over-the-Counter Cough-and-Cold Medications 23 Why Drugs? 23
■ Portrait: From Oxy to Heroin— The Life and Death of Erik 24
Summary 24 / Key Terms 25 / Endnotes 26
Chap t er 2
Drug-taking Behavior: personal and social issues 28
By the Numbers . . . 29 Drug Toxicity 30
■ d rugs . . in f o C us: Acute Toxicity in the News: Drug-Related Deaths 32
■ Qui C k Con CEP t Ch EC k 2.1: Understanding Dose-Response Curves 33 The DAWN Reports 33 Emergencies Related to Illicit Drugs 34 Drug-Related Deaths 34 Judging Drug Toxicity from Drug-Related Deaths 35 Demographics and Trends 35 From Acute Toxicity to Chronic Toxicity 36 Behavioral Tolerance and Drug Overdose 37
■ Qui C k Con CEP t Ch EC k 2.2: Understanding Behavioral Tolerance through Conditioning 38
Physical and Psychological Dependence 39 Physical Dependence 39 Psychological Dependence 39
Diagnosing Drug-Related Problems: The Health Professional’s Perspective 41
Special Circumstances in Drug Abuse 43
Drug Abuse in Pregnancy 43
Drug Abuse and HIV Infection 43
■ hE a L th Lin E : Effects of Psychoactive Drugs on Pregnant Women and Newborns 44 Drugs, Violence, and Crime 45 Pharmacological Violence 45
Economically Compulsive Violence 46 Systemic Violence 47
Governmental Policy, Regulation, and Laws 48 Efforts to Regulate Drugs, 1900–1970 48
Rethinking the Approach toward Drug Regulation, 1970–Present 49
Drug Law Enforcement and Global Politics 50
■ Portrait: Pablo Escobar—Formerly Known as the Colombian King of Cocaine 51
■ hE a L th Lin E : Harm Reduction as a National Drug-Abuse Policy 53
Summary 54 / Key Terms 55 / Endnotes 55
■ Point/Count E r P oint i : Should We Legalize Drugs in General? 58
Chapter 3
how Drugs Work in the Body and on the Mind 60
By the Numbers . . . 61
How Drugs Enter the Body 61
Oral Administration 61
Injection 62
Inhalation 63
Absorption through the Skin or Membranes 63 How Drugs Exit the Body 64
■ d rugs . . . in f o C us: Ways to Take Drugs: Routes of Administration 65
Factors Determining the Behavioral Impact of Drugs 66 Timing 66
Drug Interactions 67
Cross-Tolerance and Cross-Dependence 67
■ Qui C k Con CEP t Ch EC k 3.1: Understanding Drug Interactions 67
■ hE a L th aLE rt: Adverse Effects of Drug–Drug and Food–Drug Combinations 68
Individual Differences 69
Introducing the Nervous System 69
The Peripheral Nervous System 70
Sympathetic and Parasympathetic Responses 70
The Central Nervous System 71
Understanding the Brain 72
The Hindbrain 73
The Midbrain 73
The Forebrain 73
■ Qui C k Con CEP t Ch EC k 3.2: Understanding Drugs and Brain Functioning 74
Understanding the Neurochemistry of Psychoactive Drugs 74
Introducing Neurons 74
Neuronal Communication 75
Drug Influences on Neuronal Communication 76
The Major Neurotransmitters in Brief: The Big Seven 76
Physiological Aspects of Drug-Taking Behavior 78
The Blood–Brain Barrier 78
■ d rugs . . in f o C us: Endorphins, Endocannabinoids, and the “Runner’s High” 79
Biochemical Processes Underlying Drug Tolerance 80
■ Qui C k Con CEP t Ch EC k 3.3: Understanding Cross-Tolerance and Cross-Dependence 80
Physiological Factors in Psychological Dependence 81
■ hE a L th Lin E : Drug Craving and the Insula of the Brain 82
Psychological Factors in Drug-Taking Behavior 82 Expectation Effects 83
■ Portrait: Nora D. Volkow—A ScientistGeneral in the War on Drugs 84 Drug Research Procedures 85
Summary 85 / Key Terms 86 / Endnotes 86
Part two Legally restricted drugs in our society 89
Chapter 4 the Major stimulants: Cocaine and amphetamines 89
By the Numbers . . . 90
The History of Cocaine 90 Cocaine in Nineteenth-Century Life 91
■ hE a L th aLE rt: Cocaine after Alcohol: The Risk of Cocaethylene Toxicity 91
Freud and Cocaine 92
■ d rugs . . . in f o C us: What Happened to the Coca in Coca-Cola? 93
■ Qui C k Con CEP t Ch EC k 4.1: Understanding the History of Cocaine 94
Acute Effects of Cocaine 94
Chronic Effects of Cocaine 95
■ hE a L th aLE rt: The Physical Signs of Possible Cocaine Abuse 95
Medical Uses of Cocaine 96
How Cocaine Works in the Brain 96
Present-Day Cocaine Abuse 96
From Coca to Cocaine 97 From Cocaine to Crack 97
■ d rugs . . . in f o C us: Crack Babies
Revisited: What Are the Effects? 99
Patterns of Cocaine Abuse 100
Treatment Programs for Cocaine Abuse 100
■ d rugs . . in f o C us: Paco: A Cheap Form of Cocaine Floods Argentine Slums and Beyond 100
■ Portrait: Robert Downey Jr. and Others—Cleaning Up after Cocaine 101
Amphetamines 103
The Different Forms of Amphetamines 103
The History of Amphetamines 104
How Amphetamines Work in the Brain 104
Acute Effects of Amphetamines 104
Chronic Effects of Amphetamines 105 Methamphetamine Abuse 105
Present-Day Patterns of Methamphetamine Abuse 105
■ d rugs . . in f o C us: Methamphetamine and the Heartland of America 107
Methamphetamine-Abuse Treatment 107
■ Qui C k Con CEP t Ch EC k 4.2: Understanding Patterns of Cocaine and Methamphetamine Abuse 108
Medical Uses for Amphetamines and Similar Stimulant Drugs 108
■ hE a L th Lin E : “Bath Salts” as a New Form of Stimulant Abuse 109
Stimulant Medications for ADHD 109
Other Medical Applications 110
Stimulant Medication and Cognitive Enhancement 111
Summary 111 / Key Terms 112 / Endnotes 112
■ Point/Count E r P oint ii : Should Cognitive Performance-Enhancing Drugs Be Used by Healthy People? 116
Chapter 5
Opioids: Opium, heroin, and Opioid pain Medications 118
By the Numbers . . . 119
Opium in History 119
The Opium War 121
Opium in Britain and the United States 122
Morphine and the Advent of Heroin 123
Opioids in American Society 124
Opioid Use and Heroin Abuse after 1914 124
Heroin Abuse in the 1960s and 1970s 125
Heroin and Other Opioids since the 1980s 126
■ Qui C k Con CEP t Ch EC k 5.1: Understanding the History of Opium and Opioids 127
Effects on the Mind and the Body 127
How Opioids Work in the Brain 128
Patterns of Heroin Abuse 129
Tolerance and Withdrawal Symptoms 130
The Lethality of Heroin Abuse 130
■ Qui C k Con CEP t Ch EC k 5.2: Understanding the Effects of Administering and Withdrawing Heroin 131
Heroin Abuse and Society 132
Treatment for Heroin Abuse 132
Heroin Detoxification 132
Methadone Maintenance 133
Alternative Maintenance Programs 134
Behavioral and Social-Community Programs 134
Medical Uses of Opioid Drugs 134
■ hE a L th aLE rt: Sustained-Release Buprenorphine: A New Era in Heroin-Abuse Treatment 135
Beneficial Effects 135
Prescription Pain Medication Misuse and Abuse 137
OxyContin Abuse 137
Responses to OxyContin Abuse 137
■ Portrait: David Laffer—Pharmacy Robber and Killer of Four 138
Abuse of Other Opioids Pain Medications 138
Prevalence of Nonmedical Use of Opioid Pain Medications 138
Summary 139 / Key Terms 140 / Endnotes 140
Chapter 6
lsD and Other hallucinogens 143
By the Numbers . . . 144
A Matter of Definition 144
Classifying Hallucinogens 145
Lysergic Acid Diethylamide (LSD) 146
■ d rugs . . in f o C us: Strange Days in Salem: Witchcraft or Hallucinogens? 147
The Beginning of the Psychedelic Era 147
■ Portrait: Timothy Leary—Nutty Professor or Psychedelic Visionary? 149
Acute Effects of LSD 149 Effects of LSD on the Brain 150
Patterns of LSD Use 151
Facts and Fiction about LSD 151
Will LSD Produce Substance Dependence? 151
Will LSD Produce a Panic Attack or Psychotic Behavior? 151
Will LSD Increase Your Creativity? 152
Will LSD Damage Your Chromosomes? 152
■ hE a L th aLE rt: Emergency Guidelines for a Bad Trip on LSD 152
Will LSD Have Residual (Flashback) Effects? 153
Will LSD Increase Criminal or Violent Behavior? 153
Psilocybin and Other Hallucinogens Related to Serotonin 154
Lysergic Acid Amide (LAA) 154
■ hE a L th Lin E : Bufotenine and the Bufo Toad 155
Dimethyltryptamine (DMT) 155
Harmine 156
Hallucinogens Related to Norepinephrine 156
Mescaline 156
DOM 156
■ d rugs . . . in f o C us: Present-Day
Peyotism and the Native American Church 157
MDMA (Ecstasy) 157
■ hE a L th aLE rt: MDMA Toxicity: The Other Side of Ecstasy 158
Hallucinogens Related to Acetylcholine 159
Amanita muscaria 159
The Hexing Drugs and Witchcraft 159
Miscellaneous Hallucinogens 160
Phencyclidine (PCP) 161
Acute Effects of PCP 161
■ Qui C k Con CEP t Ch EC k 6.1: Understanding the Diversity of Hallucinogens 161
Patterns of PCP Abuse 162
Ketamine 162
■ Qui C k Con CEP t Ch EC k 6.2: Understanding PCP 163
Salvia divinorum 163
Summary 163 / Key Terms 165 / Endnotes 165
Chapter 7
Marijuana
167
By the Numbers . . . 168
A Matter of Terminology 168
The History of Marijuana and Hashish 170
Hashish in the Nineteenth Century 170
Marijuana and Hashish in the Twentieth Century 170
The Anti-Marijuana Crusade 171
Challenging Old Ideas about Marijuana 172
Acute Effects of Marijuana 172
Acute Physiological Effects 173
Acute Psychological and Behavioral Effects 173
■ Qui C k Con CEP t Ch EC k 7.1: Understanding the Effects of Marijuana 174
■ d rugs . . in f o C us: The Neurochemical “Yin and Yang” of Cannabis 175
Effects of Marijuana on the Brain 175
Chronic Effects of Marijuana 176
Tolerance 176
Withdrawal and Dependence 176
Cardiovascular Effects 177
Respiratory Effects and the Risk of Cancer 177
Effects on the Immune System 178
Effects on Sexual Functioning and Reproduction 178
Long-Term Cognitive Effects and the Amotivational Syndrome 178
The Gateway Hypothesis 179
The Sequencing Question 179
The Association Question 180
The Causation Question 180
■ Qui C k Con CEP t Ch EC k 7.2:
Understanding the Adverse Effects of Chronic Marijuana Abuse 181
Patterns of Marijuana Smoking 181
Causes for Concern 182
■ hE a L th aLE rt: A Synthetic Marijuana called Spice 182
Medical Marijuana 183
Muscle Spasticity and Chronic Pain 183
■ Portrait: Marcy Dolin—Marijuana
Self-Medicator 183
Nausea and Weight Loss 184
The Medical Marijuana Controversy 184
The Issues of Decriminalization and Legalization 185
Summary 186 / Key Terms 187 / Endnotes 187
Part thr EE Legal drugs in our society 191
Chapter 8
alcohol: social Beverage/social Drug 191
By the Numbers . . . 192
What Makes an Alcoholic Beverage? 192
Alcohol Use through History 194
Alcohol in Nineteenth-Century America 194
The Rise of the Temperance Movement 195
The Road to National Prohibition 196
The Beginning and Ending of a “Noble Experiment” 196
Present-Day Alcohol Regulation by Taxation 196
Patterns of Alcohol Consumption Today 197
Overall Patterns of Alcohol Consumption 197
■ hE a L th Lin E : Multiple Ways of Getting a Standard Drink 198
■ d rugs . . . in f o C us: Visualizing the Pattern of Alcohol Consumption in the United States 199
Problematic Alcohol Consumption among College Students 200
Alcohol Consumption among Adolescents 200
■ Qui C k Con CEP t Ch EC k 8.1:
Understanding Alcoholic Beverages 201
The Pharmacology of Alcohol 201
The Breakdown and Elimination of Alcohol 201
Measuring Alcohol in the Blood 202
■ hE a L th Lin E : Gender, Race, and Medication: Factors in Alcohol Metabolism 203
Effects of Alcohol on the Brain 204
Acute Physiological Effects 204
Toxic Reactions 205
Heat Loss and the Saint Bernard Myth 205
■ hE a L th aLE rt: Emergency Signs and Procedures in Acute Alcohol Intoxication 205
Diuretic Effects 206
Effects on Sleep 206
Effects on Pregnancy 206
Interactions with Other Drugs 206
Hangovers 206
Acute Behavioral Effects 207
Blackouts 208
Driving Skills 208
Preventing Alcohol-Related Traffic Fatalities among Young People 209
■ Portrait: Candace Lightner—Founder of MADD 209
Alcohol, Violence, and Aggression 210
■ d rugs . . in f o C us: Alcohol, Security, and Spectator Sports 211
■ d rugs . . . in f o C us: Caffeine, Alcohol, and the Dangers of Caffeinated Alcoholic Drinks 212 Sex and Sexual Desire 212
Alcohol and Health Benefits 212
■ Qui C k Con CEP t Ch EC k 8.2: Understanding the Data from Balanced Placebo Designs 213
■ hE a L th aLE rt: Guidelines for Responsible Drinking 214
Strategies for Responsible Drinking 215
Summary 215 / Key Terms 216 / Endnotes 216
Chapter 9
Chronic
alcohol abuse and alcoholism 220
Alcoholism: Stereotypes, Definitions, and Life Problems 221
By the Numbers . 221
Problems Associated with a Preoccupation with Drinking 221
Emotional Problems 223
Vocational, Social, and Family Problems 223
Physical Problems 223
■ hE a L th Lin E : A Self-Administered Short Michigan Alcoholism Screening Test (SMAST) 224
Hiding the Problems: Denial and Enabling 224
■ Qui C k Con CEP t Ch EC k 9.1: Understanding the Psychology of Alcoholism 225
Alcohol Abuse and Alcohol Dependence: The Health Professional’s Perspective 225
Physiological Effects of Chronic Alcohol Use 226
Tolerance and Withdrawal 226
Liver Disease 226
Cardiovascular Problems 227
Cancer 227
Dementia and Wernicke-Korsakoff Syndrome 228
Fetal Alcohol Syndrome (FAS) 228
■ hE a L th Lin E : Alcoholism Screening Instruments in Professional Use 230
Patterns of Chronic Alcohol Abuse 230
Gender Differences in Chronic Alcohol Use 231
Alcohol Abuse among the Elderly 231
The Family Dynamics of Alcoholism: A Systems Approach 232
Children of an Alcoholic Parent or Parents 232
The Genetics of Alcoholism 233
The Concept of Alcoholism as a Disease 234
Approaches to Treatment for Alcoholism 235
Biologically Based Treatments 235
■ Portrait: Bill W. and Dr. Bob—Founders of Alcoholics Anonymous 237
Alcoholics Anonymous 237
■ hE a L th Lin E : Is Controlled Drinking Possible for Alcoholics? 238
■ d rugs . . in f o C us: The Non-Disease Model of Alcoholism and Other Patterns of Substance Abuse 239
■ Qui C k Con CEP t Ch EC k 9.2: Understanding Alcoholics Anonymous 240 SMART Recovery 240
Chronic Alcohol Abuse and Alcoholism in the Workplace 240
Summary 241 / Key Terms 242 / Endnotes 242
■ Point/Count E r P oint iii : Should Alcoholism Be Viewed as a Disease? 246
Chapter 10
nicotine and tobacco Use 248
By the Numbers . . . 249
Tobacco Use through History 249
Politics, Economics, and Tobacco 250
Snuffing and Chewing 250
Cigars and Cigarettes 250
Tobacco in the Twentieth Century 251
Health Concerns and Smoking Behavior 252
■ hE a L th Lin E : African Americans, Smoking, and Mentholated Cigarettes 252
The Tobacco Industry Today 253
The Tobacco Settlement of 1998 254
The Tobacco Control Act of 2009 254
Tobacco Regulation and Global Economics 254 What’s in Tobacco? 254
Carbon Monoxide 255
Tar 255
Nicotine 256
The Dependence Potential of Nicotine 256
The Titration Hypothesis of Nicotine Dependence 256
Tolerance and Withdrawal 257
Health Consequences of Tobacco Use 257
■ hE a L th Lin E : Visualizing 400,000 to 440,000 Annual Tobacco-Related Deaths 257
Cardiovascular Disease 257
Respiratory Diseases 258
Lung Cancer 259
Other Cancers 259
Special Health Concerns for Women 260
The Hazards of Environmental Smoke 260
■ hE a L th aLE rt: Signs of Trouble from Smokeless Tobacco 261
Patterns of Smoking Behavior and Use of Smokeless Tobacco 261
■ Qui C k Con CEP t Ch EC k 10.1: Understanding the Effects of Tobacco Smoking 262 The Youngest Smokers 262
Attitudes toward Smoking among Young People 262
Smokeless Tobacco 263
Cigars 264
Tobacco Use around the World 264
■ Portrait: Sigmund Freud—Nicotine
Dependence, Cigars, and Cancer 265
Quitting Smoking: The Good News and the Bad 265
The Good News: Undoing the Damage 266
The Bad News: How Hard It Is to Quit 266
■ hE a L th Lin E : How to Succeed in Quitting Smoking—By Really Trying 268
Nicotine Gums, Patches, Sprays, and Inhalers 268
The Role of Physicians in Smoking Cessation 268
A Final Word 269
Summary 270 / Key Terms 271 / Endnotes 271
Chapter 11
275
Coffee 276
By the Numbers . . . 276
Coffee in Britain and North America 276
Major Sources of Coffee 277
The Caffeine Content in Coffee 277
■ d rugs . . in f o C us: Why There Are No (Live) Flies in Your Coffee 278
Tea 278
Tea in Britain and North America 278
The Chemical Content in Tea 279
Chocolate 279
How Chocolate Is Made 280
The Chocolate Industry Today 280
The Xanthine Content in Chocolate 280
■ hE a L th Lin E : Chocolate, Flavanols, and Cardiovascular Health 281
Soft Drinks 281
Caffeine from OTC Drugs and Other Products 281
■ Portrait: Milton S. Hershey and the Town Built on Chocolate 282
Caffeine as a Drug 282
■ Qui C k Con CEP t Ch EC k 11.1: Understanding Caffeine Levels in Foods and Beverages 283
Effects of Caffeine on the Body 283
Effects of Caffeine on Behavior 283
Potential Health Benefits 284
Potential Health Risks 285
Cardiovascular Effects 285
Osteoporosis and Bone Fractures 285
■ hE a L th Lin E : Coffee, Genes, and Heart Attacks 286
Breast Disease 286
Effects during Pregnancy and Breastfeeding 286
Panic Attacks 286
Dependence, Acute Toxicity, and Medical Applications 287
Tolerance 287
Withdrawal 287
Craving 287
Acute Toxicity of Caffeine 287
Prescription Drugs Based on Xanthines 288
Caffeine and Young People: A Special Concern 288
■ d rugs . . . in f o C us: Energy Shots 289
Summary 289 / Key Terms 290 / Endnotes 290
Part four Enhancers and depressants 293
Chapter 12 performance-enhancing Drugs and Drug testing in sports 293
Drug-Taking Behavior in Sports 294 By the Numbers . . . 294
What Are Anabolic Steroids? 294
Anabolic Steroids at the Modern Olympic Games 295
■ Portrait: Lance Armstrong: From Honor to Dishonor 297
Anabolic Steroids in Professional and Collegiate Sports 297
Performance-Enhancing Drug Abuse and Baseball 297
■ d rugs . . . in f o C us: Suspension
Penalties for Performance-Enhancing Drug Use in Sports 298
The Hazards of Anabolic Steroids 299
Effects on Hormonal Systems 299
Effects on Other Systems of the Body 300
Psychological Problems 300
Special Problems for Adolescents 301
■ Qui C k Con CEP t Ch EC k 12.1: Understanding the Effects of Anabolic Steroids 301
Caffeine
Patterns of Anabolic Steroid Abuse 301
The Potential for Steroid Dependence 302 Counterfeit Steroids and the Placebo Effect 303
■ hE a L th aLE rt: The Symptoms of Steroid Abuse 304
Nonsteroid Hormones and Performance-Enhancing Supplements 304
Human Growth Hormone 304
Dietary Supplements as Performance-Enhancing Aids 305
Nonmedical Use of Stimulant Medication in Baseball 306
Current Drug-Testing Procedures and Policies 306
The Forensics of Drug Testing 306
■ d rugs . . . in f o C us: Pharmaceutical Companies and Anti-Doping Authorities: A New Alliance 307
Sensitivity and Specificity 308
Masking Drugs and Chemical Manipulations 308
Pinpointing the Time of Drug Use 309
■ Qui C k Con CEP t Ch EC k 12.2: Understanding Drug Testing 310
The Social Context of Performance-Enhancing Drugs 310
Summary 311 / Key Terms 312 / Endnotes 312
Chapter 13
Depressants and inhalants 315
By the Numbers . . . 316
Barbiturates 316
Categories of Barbiturates 317
Acute Effects of Barbiturates 317
■ d rugs . . in f o C us: Is There Any Truth in “Truth Serum”? 318
Chronic Effects of Barbiturates 319
Current Medical Uses of Barbiturates 319 Patterns of Barbiturate Abuse 319
Nonbarbiturate Sedative-Hypnotics 320
The Development of Antianxiety Drugs 320
Benzodiazepines 321
Medical Uses of Benzodiazepines 321
Acute Effects of Benzodiazepines 322
Chronic Effects of Benzodiazepines 322
How Benzodiazepines Work in the Brain 323 Patterns of Benzodiazepine Misuse and Abuse 323
Nonbenzodiazepine Depressants 324
■ hE a L th aLE rt: The Dangers of Rohypnol as a Date-Rape Drug 324
Zolpidem and Eszopiclone 325
Buspirone 325
Beta Blockers 325
Antidepressants 325
■ Qui C k Con CEP t Ch EC k 13.1: Understanding the Abuse Potential in Drugs 326
A Special Alert: The Risks of GHB 326
Acute Effects 326
Protective Strategies for Women 326
■ Portrait: Patricia White, GHB, and the “Perfect” Crime 326
Inhalants through History 327
Nitrous Oxide 328
Ether 329
Glue, Solvent, and Aerosol Inhalation 329
The Abuse Potential of Inhalants 329
Acute Effects of Glues, Solvents, and Aerosols 330
The Dangers of Inhalant Abuse 330
■ hE a L th aLE rt: The Signs of Possible Inhalant Abuse 330 Patterns of Inhalant Abuse 331
■ d rugs . . in f o C us: Resistol and Resistoleros in Latin America 332
The Dependence Potential of Chronic Inhalant Abuse 333
Responses of Society to Inhalant Abuse 333
■ Qui C k Con CEP t Ch EC k 13.2: Understanding the History of Inhalants 334
Summary 334 / Key Terms 335 / Endnotes 336
Part five Medicinal drugs 339
Chapter 14
prescription Drugs, Over-theCounter Drugs, and Dietary supplements 339
By the Numbers . . . 340
The History of Prescription Drug Regulations 341 Procedures for Approving Prescription Drugs 342
Phases of Clinical Testing for Prescription Drugs 342
Patents and Generic Forms of Prescription Drugs 344
Speeding Up the FDA Approval Process 344
Procedures for Approving OTC Drugs 345
Are FDA-Approved Drugs Safe? 346
■ Qui C k Con CEP t Ch EC k 14.1: Understanding the FDA Approval Process 346
The Issue of Speed versus Caution 346 Patterns of Prescription Drug Misuse 347
Unintentional Drug Misuse through Prescription Errors 347
■ hE a L th Lin E : The Potential for Death by Prescription Error 348
■ hE a L th Lin E : Doctor Shopping for Prescription Drugs 349 Patterns of Prescription Drug Abuse 349
Major OTC Analgesic Drugs 349
Aspirin 350
Acetaminophen 351
Ibuprofen 351
Naproxen 352
OTC Analgesic Drugs and Attempted Suicide 352
■ Qui C k Con CEP t Ch EC k 14.2: Understanding OTC Analgesic Drugs 352
Other Major Classes of OTC Drugs 352 Sleep Aids 352
Cough-and-Cold Remedies 353
The Pharmaceutical Industry Today 353
■ Portrait: Ryan Haight and the Ryan Haight Act of 2008 354
Dietary Supplements 355
■ d rugs . . in f o C us: What We Know about Nine Herbal Supplements 356 Summary 357 / Key Terms 358 / Endnotes 358
■ Point/Count E r P oint iv : Should Prescription Drugs Be Advertised to the General Public? 360
Chapter 15
Drugs for treating schizophrenia and Mood Disorders 362
The Biomedical Model 363
By the Numbers . . . 363
Antipsychotic Drugs and Schizophrenia 364
The Symptoms of Schizophrenia 364 The Early Days of Antipsychotic Drug Treatment 364
■ hE a L th Lin E : Mercury Poisoning: On Being Mad As a Hatter 365
Antipsychotic Drug Treatment 365
First-Generation Antipsychotic Drugs 365
Second-Generation Antipsychotic Drugs 366
Third-Generation Antipsychotic Drugs 367 Effects of Antipsychotic Drugs on the Brain 367 Drugs Used to Treat Depression 368
■ Portrait: The Melancholy President— Abraham Lincoln, Depression, and Those “Little Blue Pills” 369
First-Generation Antidepressant Drugs 369
Second-Generation Antidepressant Drugs 370
Third-Generation Antidepressant Drugs 370
■ hE a L th aLE rt: SSRI Antidepressants and Elevated Risk of Suicide among Children and Adolescents 371
Effects of Antidepressant Drugs on the Brain 371 The Effectiveness of Specific Antidepressant Drugs 372 Drugs for Other Types of Mental Disorders 372 Mania and Bipolar Disorder 372
■ Qui C k Con CEP t Ch EC k 15.1: Understanding the Biochemistry of Mental Illness 373 Autism 373
Off-Label Usage of Psychotropic Medications 374 Psychiatric Drugs, Social Policy, and Deinstitutionalization 374
■ d rugs . . in f o C us: Psychiatric Drugs and the Civil Liberties Debate 375 Summary 375 / Key Terms 376 / Endnotes 376
Part s ix Prevention and treatment 379 Chapter 16
By the Numbers . . . 380 Levels of Intervention in Substance-Abuse Prevention 380
■ Qui C k Con CEP t Ch EC k 16.1: Understanding Levels of Intervention in SubstanceAbuse Prevention Programs 381 Strategies for Substance-Abuse Prevention 381 Resilience and Primary Prevention Efforts 382
Measuring Success in a Substance-Abuse Prevention Program 382
A Matter of Public Health 382
■ hE a L th Lin E : The Public Health Model and the Analogy of Infectious Disease Control 383
■ Portrait: Dr. A. Thomas McLellan Goes to Washington (Briefly) 384
Lessons from the Past: Prevention Approaches That Have Failed 384
Reducing the Availability of Drugs 384
Punitive Measures 385
Scare Tactics and Negative Education 385
Objective Information Approaches 386
Magic Bullets and Promotional Campaigns 386
Self-Esteem Enhancement and Affective Education 386
Hope and Promise: Components of Effective School-Based Prevention Programs 387
Peer-Refusal Skills 387
Anxiety and Stress Reduction 387
Social Skills and Personal Decision Making 387
An Example of an Effective School-Based Prevention Program 387
■ hE a L th Lin E : Peer-Refusal Skills: Ten Ways to Make It Easier to Say No 388
Drug Abuse Resistance Education (D.A.R.E.) 389
■ Qui C k Con CEP t Ch EC k 16.2:
Understanding Primary Prevention and Education 389
Community-Based Prevention Programs 390
Components of an Effective Community-Based Program 390
Alternative-Behavior Programming 391
The Influence of Media 391
An Example of an Effective Community-Based Prevention Program 391
Family Systems in Primary and Secondary Prevention 392
Special Role Models in Substance-Abuse Prevention 392
■ d rugs . . in f o C us: Substance Use and Abuse among Young Mothers 393
Parental Communication in Substance-Abuse Prevention 393
The Triple Threat: Stress, Boredom, and Spending Money 394
Multicultural Issues in Primary and Secondary Prevention 394
Prevention Approaches in Latino Communities 394
Prevention Approaches in African American Communities 395
Substance-Abuse Prevention in the Workplace 395
The Economic Costs of Substance Abuse in the Workplace 396
Drug Testing in the Workplace 396
The Impact of Drug-Free Workplace Policies 397
Yes, You: Substance-Abuse Prevention and the College Student 397
Changing the Culture of Alcohol and Other Drug Use in College 398
Substance-Abuse Prevention on College Campuses 398
■ hE a L th Lin E : Alcohol 101 on College Campuses 399
Substance-Abuse Prevention Information 399
Summary 400 / Key Terms 401 / Endnotes 401
■ Point/Count E r P oint v : Should We Continue to D.A.R.E. or Should We Give it up? 405
Chapter 17
substance-abuse treatment: strategies for Change 407
By the Numbers . . . 408
Designing Effective Substance-Abuse Treatment Programs 409
The Biopsychosocial Model for Substance-Abuse Treatment 409
Intervention through Incarceration and Other Punitive Measures 409
Substance-Abuse Treatment and Law Enforcement 410
■ d rugs . . in f o C us: Penalties for Crack versus Penalties for Powder Cocaine: Correcting an Injustice 413
Prison-Alternative Treatment Programs 414 Drug Courts 414
■ Portrait: Monsignor William O’Brien— Founder of Daytop Village 415
Prison-Based Treatment Programs 416
Substance-Abuse Treatment in the Workplace 416
The Personal Journey to Treatment and Recovery 417 Rehabilitation and the Stages of Change 417
Stages of Change and Other Problems in Life 418
■ Qui C k Con CEP t Ch EC k 17.1: Understanding the Stages of Change in SubstanceAbuse Treatment 419
The Impact of Family Systems on Treatment and Recovery 419
Family Dynamics in Drug Abuse 419
Enabling Behaviors as Obstacles to Rehabilitation 420
Survival Roles and Coping Mechanisms 421 Resistance at the Beginning, Support along the Way 421
Finding the Right Substance-Abuse Treatment Program 421
Judging the Quality of the Treatment Facility 422
Principles to Maximize the Chances of Successful Treatment 423
Needing versus Receiving Substance-Abuse Treatment 423
A Final Note: For Those Who Need Help . . . 424
Summary 425 / Key Terms 426 / Endnotes 426
Credits 429 index 433
This page intentionally left blank
In today’s world, drugs and their use have the potential for good and for bad. As a society and as individuals, we can be the beneficiaries of drugs—or their victims. This perspective continues to be the message of Drugs, Behavior, and Modern Society, Eighth Edition. As has been the case since the first edition, this book introduces the basic facts and major issues concerning drug-taking behavior in a straightforward, comprehensive, and reader-friendly manner. A background in biology, sociology, psychology, or chemistry is not necessary. The only requirement is a sense of curiosity about the range of chemical substances that affect our minds and our bodies and an interest in the challenges these substances bring to our society and our daily lives. These challenges can be framed in terms of three fundamental themes.
The role of drug-taking behavior throughout history
First of all, present-day issues concerning drug misuse and abuse are issues that society has confronted for a long time. Drugs and drug-taking behavior are consequences of a particularly human need to feel stronger, more alert, calmer, more distant and dissociated from our surroundings, or simply good. It is the misuse and abuse of chemical substances to achieve these ends that have resulted in major problems in the United States and around the world.
The diversity in psychoactive drugs in our society
There is an enormous diversity among drugs that affect the mind and the body. We need to educate ourselves not only about illicit drugs such as cocaine, amphetamines, heroin, hallucinogens, and marijuana but also about legally available drugs such as alcohol, nicotine, and caffeine. Drugs, Behavior, and Modern Society has been designed as a comprehensive survey of all types of psychoactive drugs, addressing the issues of drug-taking behavior from a combination of psychological, biological, and sociological perspectives. The personal impact of drug-related issues in our lives Finally, we need to recognize that, like it or not, the decision to use drugs is one of life’s choices in contemporary society, regardless of our racial, ethnic, or religious background, how much money we have, where we live, how much education we have acquired, whether we are male or female, and whether we are young or old. The potential for misuse and abuse is a problem facing all of us.
new to this edition
The Eighth Edition of Drugs, Behavior, and Modern Society is divided into six sections:
Part One (Chapters 1–3): Drugs in Society/Drugs in Our Lives
Part Two (Chapters 4–7): Legally Restricted Drugs in Our Society
Part Three (Chapters 8–11): Legal Drugs in Our Society
Part Four (Chapters 12 and 13): Enhancers and Depressants
Part Five (Chapters 14 and 15): Medicinal Drugs
Part Six (Chapters 16 and 17): Prevention and Treatment
As you will see, chapters about particular drugs have been grouped not in terms of their pharmacological or chemical characteristics but, rather, in terms of how readily accessible they are to the general public and today’s societal attitudes toward their use. The last section of the book concerns itself with prevention and treatment. In addition, several special features throughout the book will enhance your experience as a reader and serve as learning aids.
This text is available in a variety of formats—digital and print. To learn more about our programs, pricing options, and customization, visit www.pearsonhighered .com
By the numbers . . .
At the beginning of each chapter, a feature called By the Numbers . . . provides an often surprising and provocative insight into current viewpoints and research. It is presented in a brief, quantitative format that draws you into the chapter and sets the stage for further exploration.
Quick Concept Checks
Sometimes, when the material gets complicated, it is good to have a quick way of finding out whether you understand the basic concepts being explained. Each chapter of this book includes, from time to time, a Quick Concept Check, where you can see in a minute
or two where you stand. Some of the Checks are in a matching format; others involve interpreting a graph or diagram. In some cases, you will be asked to apply the principles you have learned to a real-world situation.
portraits
Seventeen Portrait features, one in each chapter, take you into the lives of individuals who either have influenced our thinking about drugs in our society or have been affected by drug use or abuse. Some of these people are known to the public at large, but many are not. The subjects of these Portraits include a brutal drug trafficker (Pablo Escobar, Chapter 2), a movie star (Robert Downey Jr., Chapter 4), a convicted killer (David Laffer, Chapter 5), a cultural icon (Timothy Leary, Chapter 6), and a depressive U.S. President (Abraham Lincoln, Chapter 13). All the Portraits put a human face on discussions of drugs and behavior. They remind us that we are dealing with issues that affect real people in all walks of life, now and in the past.
Drugs . . . in Focus
There are many fascinating stories to tell about the role of drugs in our history and our present-day culture, along with important facts and serious issues surrounding drug use. A total of 26 Drugs . . . in Focus features are presented in the Eighth Edition. The topics of these features cover a wide range, from questions about the origins of the word coca in Coca-Cola (Chapter 4) and possible hallucinogenic witchcraft in seventeenth century Salem, Massachusetts, (Chapter 6), to future possibilities of gene doping in the Olympics (Chapter 12) and the present-day use of “truth serum” in terrorist interrogations (Chapter 13).
health line
Helpful information regarding the effectiveness and safety aspects of particular drugs, specific aspects of drug-taking behavior, and new medical applications can be found in 22 Health Line features throughout the book. Health Line topics include understanding the neurological basis for drug craving (Chapter 3), the controversy over the use of stimulant medications as “smart pills” (Chapter 4), concerns over a new synthetic marijuana called Spice (Chapter 7), the risks of smoking mentholated cigarettes among African Americans (Chapter 10), “doctor-shopping” and prescription pain medications (Chapter 14), and alcohol prevention programs like Alcohol 101 on college campuses (Chapter 16), to name a few.
health alert
Information of a more urgent nature is provided in 14 Health Alert features. You will find important facts that you can use to recognize the signs of drug misuse or abuse and ways in which you can respond to emergency drug-taking situations, as well as useful Internet links where you can go for assistance. Health Alert topics in the Eighth Edition include strategies to avoid adverse effects of drug-drug and food-drug combinations (Chapter 3), the risks of cocaine combined with alcohol (Chapter 4), emergency guidelines for adverse reactions to LSD (Chapter 6) or alcohol (Chap ter 8), and the dangers of Rohypnol as a date-rape drug (Chapter 13).
point/Counterpoint Debates
Drug issues are seldom black or white, right or wrong. Some of the most hotly debated questions of our day concern the use, misuse, and abuse of drugs. These issues deserve a good deal of critical thought. This is why at specific locations in this book, I have taken five important controversies concerning drugs, collected the key viewpoints pro and con, and created a Point/ Counterpoint debate based on a simulated conversation that two hypothetical people might have on that question. The Point/Counterpoint features appear at the end of the chapter that deal specifically with the controversy addressed in the debate. I invite you to read these debates carefully and try to arrive at your own position, as an exercise in critical thinking. Along with considering the critical thinking questions for further discussion that follow each Point/Counterpoint feature, you may wish to continue the debate in your class.
supplements
Pearson Education is pleased to offer the following supplements to qualified adopters.
instructor’s Manual and test Bank
(0-205-04839-0)
This Instructor’s Manual and Test Bank provides instructors with support material, classroom enrichment information, and wealth of assessment questions. Corresponding to the chapters in the text, each of the manual’s 17 chapters contains discussion questions, lecture outlines, video suggestions, and a test bank, which
includes an extensive set of multiple choice, true/false and essay questions.
Mytest test Bank (0-205-04837-4)
This test bank is available in computerized format, which allows instructors to easily create and print quizzes and exams. Questions and tests can be authored online, allowing instructors ultimate flexibility and the ability to efficiently manage assessments anytime, anywhere. Instructors can easily access existing questions, edit, create, and store using simple drag and drop Word-like controls. For more information, go to www.PearsonMyTest.com.
powerpoint presentation (0-205-04836-6)
The PowerPoint Presentation is an exciting interactive tool for use in the classroom. Each chapter pairs key concepts with images from the textbook to reinforce student learning.
Mypsychlab (www.mypsychlab.com)
This online study resource offers a wealth of animations and practice tests, plus additional study and research tools. With this edition, there are now new assessments, web and video/media links, and flash cards. www.pearsonhighered.com
an invitation to readers
I welcome your reactions to Drugs, Behavior, and Modern Society, Eighth Edition. Please send any comments or questions to the following address: Dr. Charles F. Levinthal, Department of Psychology, 135 Hofstra University, Hempstead, NY 11549. You can also communicate by fax at 516 463-6052 or at the following email address: charles.f.levinthal@hofstra.edu. I look forward to hearing from you.
acknowledgments
In the course of writing the Eighth Edition, I have received much encouragement, assistance, and expert advice from a number of people. I have benefited from their generous
sharing of materials, knowledge, and insights. I am particularly indebted to Dr. Elizabeth Crane, Substance Abuse and Mental Health Services Administration, U.S. Department of Health and Human Services; Charles F. Miller, Office of Policy and Interagency Affairs, National Drug Intelligence Center, U.S. Department of Justice; Dr. Patrick M. O’Malley, Institute for Social Research, The University of Michigan, Ann Arbor; and Lawrence Payne, Office of Public Affairs, Drug Enforcement Administration, U.S. Department of Justice.
I am fortunate to have worked with a superb team at Pearson. I am especially indebted to my editor, Susan Hartman, my program manager, Reena Dalal, and my senior project manager, Revathi Viswanathan. Their professionalism and talents contributed so much to the production quality of this book and are greatly appreciated. A number of manuscript reviewers made invaluable suggestions as I worked on the Eighth Edition. I thank all of them for their help: Marge MurrayDavis, Minnesota State University; Philip Langlais, Old Dominion University; Robin Joynes, Kent State University; Chris Jones-Cage, College of the Desert; Susan Fellows, California State University, Dominguez Hills; Toni Watt, Texas State University; Larry Ashley, University of Nevada; Frank White, University of North Dakota; Jennifer Graham, Penn State University; Christopher Goode, Georgia State University; Andy Harcrow, The University of Alabama; Robert Carr, University of South Dakota; John Gampher, University of Alabama at Birmingham; Bengie Cravey, Darton State College; Lee Ancona, University of North Texas; Sidney Auerbach, Rutgers University; Christopher Correia, Auburn University; Perry Fuchs, UT Arlington; Edith Ellis, College of Charleston; Neil Rowland, University of Florida; William Cabin, Richard Stockton College.
On a more personal note, there are others who have given me their support over the years and to whom my appreciation goes beyond words. As always, I thank my mother-in-law, Selma Kuby, for her encouragement and love.
Above all, my family has been a continuing source of strength. I will always be grateful to my sons David and Brian, and to my daughters-in-law Sarah and Karen, for their love and understanding. I am especially grateful to my wife, Beth, for her abiding love, support, and complete faith in my abilities. The Eighth Edition is dedicated to my grandsons, Aaron Matthew Levinthal and Michael Samuel Levinthal.
Charles F. Levinthal
This page intentionally left blank
Drugs . . . in Focus
Drug Abuse and the College Student: An Assessment Tool
In a research study conducted at Rutgers University, a cutoff score of five or more “yes” responses to the following twentyfive questions in the Rutgers Collegiate Substance Abuse Screening Test (RCSAST) was found effective in correctly classifying 94 percent of young adults in a clinical sample as problem users and 89 percent of control individuals as nonproblem users. It is important, however, to remember that the RCSAST does not by itself determine the presence of substance abuse or dependence (see Chapter 2). The RCSAST is designed to be used as one part of a larger assessment battery aimed at identifying which young adults experience problems due to substance use and specifically what types of problems a particular individual is experiencing. Here are the questions:
1. Have you gotten into financial trouble as a result of drinking or other drug use?
2. Is alcohol or other drug use making your college life unhappy?
3. Do you use alcohol or other drugs because you are shy with other people?
4. Has drinking alcohol or using other drugs ever caused conflicts with close friends of the opposite sex?
5. Has drinking alcohol or using other drugs ever caused conflicts with close friends of the same sex?
6. Has drinking alcohol or using other drugs ever damaged other friendships?
7. Has drinking alcohol or using other drugs ever been behind your losing a job (or the direct reason for it)?
8. Do you lose time from school due to drinking and/or other drug use?
9. Has drinking alcohol or using other drugs ever interfered with your preparations for exams?
10. Has your efficiency decreased since drinking and/or using other drugs?
11. Do you drink alcohol or use other drugs to escape from worries or troubles?
12. Is your drinking and/or using other drugs jeopardizing your academic performance?
13. Do you drink or use other drugs to build up your self-confidence?
14. Has your ambition decreased since drinking and/or drug using?
15. Does drinking or using other drugs cause you to have difficulty sleeping?
16. Have you ever felt remorse after drinking and/or using other drugs?
17. Do you drink or use drugs alone?
18. Do you crave a drink or other drug at a definite time daily?
19. Do you want a drink or other drug the next morning?
20. Have you ever had a complete or partial loss of memory as a result of drinking or using other drugs?
21. Is drinking or using other drugs affecting your reputation?
22. Does your drinking and/or using other drugs make you careless of your family’s welfare?
23. Do you seek out drinking/drugging companions and drinking/drugging environments?
24. Has your physician ever treated you for drinking and/ or other drug use?
25. Have you ever been to a hospital or institution on account of drinking or other drug use?
Source: Bennett, M. E.; McCrady, B. S.; Frankenstein, W.; Laitman, L. A.; Van Horn, D. H. A.; and Keller, D. S. (1993). Identifying young adult substance abusers: The Rutgers Collegiate Substance Abuse Screening Test. Journal of Studies in Alcohol, 54, 522–527. Reprinted with permission of the authors of the RCSAST.
large number of separate medications. This population is especially vulnerable to the hazards of drug misuse.
In contrast, drug abuse is typically applied to cases in which a licit or illicit drug is used in ways that produce some form of physical, mental, or social impairment (See Drug in Focus on p. 8). The primary motivation for individuals involved in drug abuse is recreational. Drugs with abuse potential include not only the common street drugs but also legally available psychoactive substances, such as caffeine and nicotine (stimulants), alcohol and inhaled solvents (depressants), and a number of prescription or OTC medications designated for medical purposes but used by some individuals exclusively on a recreational basis. In Chapter 5, we will examine concerns about the abuse of opioid pain medications such as Vicodin, OxyContin, and Percocet, among others. In these particular cases, the distinction between drug misuse and drug abuse is particularly blurry. When there is no intent to make a value judgment about the motivation or consequences of a particular type of drug-taking behavior, we will refer to the behavior simply as drug use.
Before examining the major role that drugs and drug-taking behavior play in our lives today, however, it is important to examine the historical foundations of drug use. We need to understand why drug-taking behavior has been so pervasive over the many centuries of human history, and why drug-taking behavior remains so compelling for us in our contemporary society. We also need to understand the ways in which our society has responded to problems associated with drug use. How have our attitudes toward drugs changed over time? How did people feel about drugs and drug-taking behavior one hundred years ago, fifty years ago, twenty years ago, or even ten years ago? These are questions that we will now address.
Drugs in Early Times
Try to imagine the accidental circumstances under which a psychoactive drug might have been discovered. Thousands of years ago, perhaps a hundred thousand years ago, the process of discovery would have been as natural as eating, and the motivation as basic as simple curiosity. In cool climates, next to a cave dwelling may have grown a profusion of blue morning glories or brightly colored mushrooms, plants that produce hallucinogens similar to LSD. In desert regions, yelloworange fruits grew on certain cacti, the source of the hallucinogenic drug peyote. Elsewhere, poppy plants, the source of opium, covered acres of open fields. Coca leaves, from which cocaine is made, grew on shrubs along the mountain valleys throughout Central and
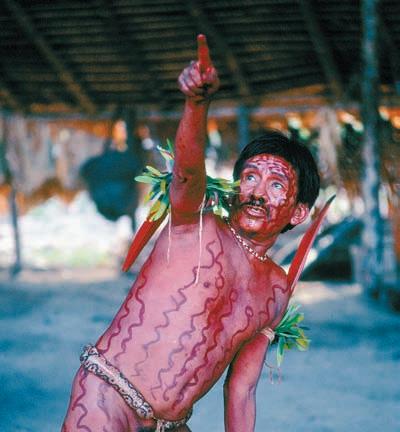
In a wide range of world cultures throughout history, hallucinogens have been regarded as having deeply spiritual powers. Under the influence of drugs, this modern-day shaman communicates with the spirit world.
South America. The hardy cannabis plant, the source of marijuana, grew practically everywhere.
Some of this curiosity may have been sparked by observing the unusual behavior of animals as they fed on these plants. Within their own experience, people made the connection, somewhere along the line, between the chewing of willow bark (the source of modern-day aspirin) and the relief of a headache or between the eating of the senna plant (a natural laxative) and the relief of constipation.9
Of course, some of these plants made people sick, and many of them were poisonous and caused death. However, it is likely that the plants that had the strangest impact on humans were the ones that produced hallucinations. Having a sudden vision of something totally alien to everyday life must have been overwhelming, like a visit to another world. Individuals with prior knowledge about such plants, as well as about plants with therapeutic powers, would eventually acquire great power over others in the community.
The accumulation of knowledge about consciousness-altering substances would mark the beginning of shamanism, a practice among primitive societies, dating back by some estimates more than forty thousand
shamanism: The philosophy and practice of healing in which diagnosis or treatment is based on trancelike states, on the part of either the healer (shaman) or the patient.
years, in which an individual called a shaman acts as a healer through a combination of trances and plantbased medicines, usually in the context of a local religious rite. Shamans still function today in remote areas of the world, often alongside practitioners of modern medicine. As we will see in Chapter 6, hallucinationproducing plants of various kinds play a major role in present-day shamanic healing.
With the development of centralized religions in Egyptian and Babylonian societies, the influence of shamanism gradually declined. The power to heal through one’s knowledge of drugs passed into the hands of the priesthood, which placed greater emphasis on formal rituals and rules than on hallucinations and trances.
The most dramatic testament to the development of priestly healing during this period is a 65-foot-long Egyptian scroll known as the Ebers Papyrus , named after a British Egyptologist who acquired it in 1872. This mammoth document, dating from 1500 b.c ., contains more than eight hundred prescriptions for practically every ailment imaginable, including simple wasp stings and crocodile bites, baldness, constipation, headaches, enlarged prostate glands, sweaty feet, arthritis, inflammations of all types, heart disease, and cancer. More than a hundred of the preparations contained castor oil as a natural laxative; some contained “the berry of the poppy,” which we now recognize as the Egyptian reference to opium. Other ingredients were quite bizarre: lizard’s blood, the teeth of swine, the oil of worms, the hoof of an ass, putrid meat with fly specks, and crocodile dung (excrement of all types being highly favored for its ability to frighten off the evil spirits of disease).10
How successful were these strange remedies? It is impossible to know because no records were kept on what happened to the patients. Although some of the ingredients (such as opium and castor oil) had true medicinal value, much of the improvement from these concoctions may have been psychological rather than physiological. In other words, improvements in the patient’s condition resulted from the patient’s belief that he or she would be helped—a phenomenon known as the placebo effect. Psychological factors have played a critical role throughout the history of drugs. The importance of the placebo effect as an explanation of some drug effects will be examined in Chapter 3.
Along with substances that had genuine healing properties, some psychoactive drugs were put to less positive use. In the early Middle Ages, Viking warriors ate the mushroom Amanita muscaria, known as fly agaric, and experienced a tremendous increase in energy, which resulted in wild behavior in battle. They were called Berserkers because of the bear skins they wore, but this is
the origin of the word “berserk” as a reference to reckless and violent behavior. At about the same time, witches operating on the periphery of European society created “witch’s brews,” mixtures made of various plants such as mandrake, henbane, and belladonna, creating strange hallucinations and a sensation of flying. The toads that they included in their recipes didn’t hurt either: We know now that the sweat glands of certain toads contain a chemical related to dimethyltryptamine (DMT), a powerful hallucinogenic drug (see Chapter 6).11
Drugs in the Nineteenth Century
By the end of the nineteenth century, the medical profession had made significant strides with respect to medicinal healing. Morphine was identified as the active ingredient in opium, a drug that had been in use for at least three thousand years and had become the physician’s most reliable prescription for the control of pain due to disease and injury. The invention of the syringe made it possible to deliver the morphine directly and speedily into the bloodstream. Cocaine, having been extracted from coca leaves, was used as a stimulant and antidepressant. Sedative powers to calm the mind or induce sleep had been discovered in bromides and chloral hydrate.
There were also new drugs for specific purposes or particular diseases. Anesthetic drugs were discovered that made surgery painless for the first time in history. Some diseases could actually be prevented through the administration of vaccines, such as the vaccine against smallpox introduced by Edward Jenner in 1796 and the vaccine against rabies introduced by Louis Pasteur in 1885. The discovery of new pharmaceutical products marked the modern era in the history of healing.12
The social picture of drug-taking behavior during this time, however, was more complicated. By the 1890s, prominent leaders in the medical profession and social reformers had begun to call attention to societal problems resulting from the widespread and uncontrolled access to psychoactive drugs. Remedies called
shaman (SHAH-men): A healer whose diagnosis or treatment of patients is based at least in part on trances. These trances are frequently induced by hallucinogenic drugs.
ebers Papyrus: An Egyptian document, dated approximately 1500 b c., containing more than eight hundred prescriptions for common ailments and diseases.
placebo (pla-Cee-bo) effect: Any change in a person’s condition after taking a drug, based solely on that person’s beliefs about the drug rather than on any physical effects of the drug.
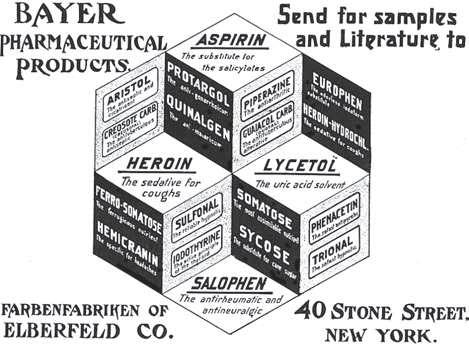
Around 1900, heroin was advertised as a completely safe remedy for common ailments, along with aspirin. No one knows how many people became dependent on heroin as a result.
patent medicines , sold through advertisements, peddlers, or general stores, contained opium, alcohol, and cocaine and were promoted as answers to virtually all common medical and nonmedical complaints.
Opium itself was cheap, easily available, and completely legal. Most people, from newborn infants to the elderly, in the United States and Europe “took opium” during their lives. The way in which they took it, however, was a critical social factor. The respectable way was to drink it, usually in a liquid form called laudanum. By contrast, the smoking of opium, as introduced by Chinese immigrants imported for manual labor in the American West, was considered degrading and immoral. Laws prohibiting opium smoking began to be enacted in 1875. In light of the tolerant attitude toward opium drinking, the strong emotional opposition to opium smoking may be viewed as more anti-Chinese than anti-opium.13
Like opium, cocaine was in widespread use and was taken quite casually in a variety of forms during this period. The original formula for Coca-Cola, as the name suggests, contained cocaine until 1903 (see Chapter 4), as did Dr. Agnew’s Catarrh Powder, a popular remedy for chest colds. In the mid-1880s, Parke, Davis, and Company (since 2002, merged with Pfizer, Inc.) was selling cocaine and its botanical source, coca, in more than a dozen forms, including coca-leaf cigarettes and cigars, cocaine inhalants, a coca cordial, and an injectable cocaine solution.14
A Viennese doctor named Sigmund Freud, who was later to gain a greater reputation for his psychoanalytic theories than for his ideas concerning psychoactive drugs, promoted cocaine as a “magical drug.” In an influential paper published in 1884, Freud recommended cocaine as a safe and effective treatment for morphine addiction. When a friend and colleague became heavily
addicted to cocaine, Freud quickly reversed his position, regretting for the rest of his life that he had been initially so enthusiastic in recommending its use (see Chapter 4).15
Drugs and Behavior in the Twentieth Century
By 1900, the promise of medical advances in the area of drugs was beginning to be matched by concern about the dependence that some of these drugs could produce. For a short while after its introduction in 1898, heroin (a derivative of morphine) was completely legal and considered safe. Physicians were impressed with its effectiveness in the treatment of coughs, chest pains, and the respiratory difficulties associated with pneumonia and tuberculosis. This was an era in which antibiotic drugs were unavailable, and pneumonia and tuberculosis were among the leading causes of death.16
Some physicians even recommended heroin as a treatment for morphine addiction. Its powerful addictive properties, however, soon became evident. The enactment of laws restricting access to heroin and certain other psychoactive drugs, including marijuana, would eventually follow in later years, a topic discussed further in Chapter 2.
At the beginning of the twentieth century, neither the general public nor the government considered alcohol a drug. Nonetheless, the American temperance movement dedicated to the prohibition of alcohol consumption, led by the Women’s Christian Temperance Union and the Anti-Saloon League, was a formidable political force. In 1920, the Eighteenth Amendment to the U.S. Constitution took effect, ushering in the era of national Prohibition, which lasted for thirteen years.
Although successful in substantially reducing the rates of alcohol consumption in the United States, as well as the number of deaths from alcohol-related diseases, Prohibition also succeeded in establishing a nationwide alcohol distribution network dominated by sophisticated criminal organizations. 17 Violent gang wars arose in major American cities as one group battled another for control of the liquor trade.
By the early 1930s, whatever desirable healthrelated effects Prohibition may have brought were perceived to be overshadowed by the undesirable social changes that had come along with it. Since its end in 1933, the social problems associated with the era
patent medicine: Historically, a drug or combination of drugs sold through peddlers, shops, or mail-order advertisements.
of Prohibition have often been cited as an argument against the continuing restriction of psychoactive drugs in general.
Drugs and Behavior from 1945 to 1960
In the years following World War II, for the first time, physicians were able to control bacteria-borne infectious diseases through the administration of antibiotic drugs. Although penicillin had been discovered in a particular species of mold by Alexander Fleming in 1928, techniques for extracting large amounts from the mold were not perfected until the 1940s. Also during that time, Selman Waksman found that a species of fungus had powerful antibacterial effects; it was later to be the source of the drug streptomycin.
In the field of psychiatry, advances in therapeutic drugs did not occur until the early 1950s, when quite accidentally a group of psychoactive drugs were discovered that relieved schizophrenic symptoms without producing heavy sedation. The first of these, chlorpromazine (brand name: Thorazine), reduced the hallucinations, agitation, and disordered thinking common to schizophrenia. Soon after, there was a torrent of new drugs, forming the basis not only for the treatment of schizophrenia but also the
chlorpromazine (chlor-PrO-mah-zeen): An antipsychotic (antischizophrenia) drug. Brand name is Thorazine (THOR-a-zeen).
treatment of mental illness in general. It was a revolution in psychiatric care, equivalent to the impact of antibiotics in medical care a decade earlier.
In the recreational drug scene of post–World War II America, a number of features stand out. Smoking was considered romantic and sexy, and smoking was commonplace. In 1955, regular cigarette smoking involved more than half of all male adults and more than one-quarter of all female adults in the United States. It was the era of the two-martini lunch; social drinking was at the height of its popularity and acceptance. Cocktail parties dominated the social scene. There was little or no public awareness that alcohol or tobacco use constituted drug-taking behavior. In contrast, the general perception of certain drugs such as heroin, marijuana, and cocaine was simple and negative: They were considered bad, they were illegal, and “no one you knew” had anything to do with them. Illicit drugs were seen as the province of criminals, the urban poor, and nonwhites.18 The point is that an entire class of drugs were, during this period, outside the mainstream of American life. Furthermore, an atmosphere of fear and suspicion surrounded people who took such drugs. Nonetheless, for the vast majority of Americans, drugs were not considered an issue in their lives.
Drugs and Behavior after 1960
During the 1960s, basic premises of American life—the beliefs that working hard and living a good life would
The famous Woodstock Festival concert drew an estimated 500,000 people to a farm in upstate New York in the summer of 1969. According to historian David Musto, the peacefulness of such a gigantic gathering is considered to have been due, at least in part, to the widespread use of marijuana, as opposed to alcohol.