
Practical Techniques in Periodontics and Implant Dentistry Edgard El Chaar
Visit to download the full and correct content document: https://ebookmass.com/product/practical-techniques-in-periodontics-and-implant-denti stry-edgard-el-chaar/

More products digital (pdf, epub, mobi) instant download maybe you interests ...
Essential Techniques of Alveolar Bone Augmentation in Implant Dentistry: A Surgical Manual, 2nd Edition Len Tolstunov
https://ebookmass.com/product/essential-techniques-of-alveolarbone-augmentation-in-implant-dentistry-a-surgical-manual-2ndedition-len-tolstunov/

Contemporary Implant Dentistry E Book 3rd Edition, (Ebook PDF)
https://ebookmass.com/product/contemporary-implant-dentistry-ebook-3rd-edition-ebook-pdf/

Lindhe's Clinical Periodontology and Implant Dentistry 7th Edition Niklaus P. Lang
https://ebookmass.com/product/lindhes-clinical-periodontologyand-implant-dentistry-7th-edition-niklaus-p-lang/

Practical Applications of Coaching and Mentoring in Dentistry Janine Brooks
https://ebookmass.com/product/practical-applications-of-coachingand-mentoring-in-dentistry-janine-brooks/
Surgical Essentials of Immediate Implant Dentistry 1st Edition – Ebook PDF Version
https://ebookmass.com/product/surgical-essentials-of-immediateimplant-dentistry-1st-edition-ebook-pdf-version/

Misch's Contemporary Implant Dentistry Randolph R. Resnik Dmd Mds
https://ebookmass.com/product/mischs-contemporary-implantdentistry-randolph-r-resnik-dmd-mds/

Practical Applications of Coaching and Mentoring in Dentistry Helen Caton-Hughes
https://ebookmass.com/product/practical-applications-of-coachingand-mentoring-in-dentistry-helen-caton-hughes/

Digital Communications 1: Fundamentals and Techniques
Safwan El Assad
https://ebookmass.com/product/digitalcommunications-1-fundamentals-and-techniques-safwan-el-assad/

Bone Augmentation in Implant Dentistry: A Step by Step
Guide to Predictable Alveolar Ridge and Sinus Grafting 1st Edition Edition, (Ebook PDF)
https://ebookmass.com/product/bone-augmentation-in-implantdentistry-a-step-by-step-guide-to-predictable-alveolar-ridge-andsinus-grafting-1st-edition-edition-ebook-pdf/
PracticalTechniquesinPeriodonticsandImplantDentistry
PracticalTechniquesinPeriodonticsandImplantDentistry
Editedby
EdgardElChaar,DDS,MS
DepartmentofPeriodontics
UniversityofPennsylvania,DentalMedicine
Philadelphia,PA,USA
Thiseditionfirstpublished2023 ©2023JohnWiley&SonsInc.
Allrightsreserved.Nopartofthispublicationmaybereproduced,storedinaretrievalsystem,ortransmitted,inanyformorbyanymeans, electronic,mechanical,photocopying,recordingorotherwise,exceptaspermittedbylaw.Adviceonhowtoobtainpermissiontoreusematerial fromthistitleisavailableathttp://www.wiley.com/go/permissions.
TherightofEdgardElChaartobeidentifiedastheauthoroftheeditorialmaterialinthisworkhasbeenassertedinaccordancewithlaw.
RegisteredOffice
JohnWiley&Sons,Inc.,111RiverStreet,Hoboken,NJ07030,USA
EditorialOffice 111RiverStreet,Hoboken,NJ07030,USA
Fordetailsofourglobaleditorialoffices,customerservices,andmoreinformationaboutWileyproductsvisitusatwww.wiley.com.
Wileyalsopublishesitsbooksinavarietyofelectronicformatsandbyprint-on-demand.Somecontentthatappearsinstandardprintversionsof thisbookmaynotbeavailableinotherformats.
LimitofLiability/DisclaimerofWarranty
Thecontentsofthisworkareintendedtofurthergeneralscientificresearch,understanding,anddiscussiononlyandarenotintendedand shouldnotberelieduponasrecommendingorpromotingscientificmethod,diagnosis,ortreatmentbyphysiciansforanyparticularpatient. Inviewofongoingresearch,equipmentmodifications,changesingovernmentalregulations,andtheconstantflowofinformationrelatingtothe useofmedicines,equipment,anddevices,thereaderisurgedtoreviewandevaluatetheinformationprovidedinthepackageinsertor instructionsforeachmedicine,equipment,ordevicefor,amongotherthings,anychangesintheinstructionsorindicationofusageandfor addedwarningsandprecautions.Whilethepublisherandauthorshaveusedtheirbesteffortsinpreparingthiswork,theymakeno representationsorwarrantieswithrespecttotheaccuracyorcompletenessofthecontentsofthisworkandspecificallydisclaimallwarranties, includingwithoutlimitationanyimpliedwarrantiesofmerchantabilityorfitnessforaparticularpurpose.Nowarrantymaybecreatedor extendedbysalesrepresentatives,writtensalesmaterialsorpromotionalstatementsforthiswork.Thefactthatanorganization,website,or productisreferredtointhisworkasacitationand/orpotentialsourceoffurtherinformationdoesnotmeanthatthepublisherandauthors endorsetheinformationorservicestheorganization,website,orproductmayprovideorrecommendationsitmaymake.Thisworkissoldwith theunderstandingthatthepublisherisnotengagedinrenderingprofessionalservices.Theadviceandstrategiescontainedhereinmaynotbe suitableforyoursituation.Youshouldconsultwithaspecialistwhereappropriate.Further,readersshouldbeawarethatwebsiteslistedinthis workmayhavechangedordisappearedbetweenwhenthisworkwaswrittenandwhenitisread.Neitherthepublishernorauthorsshallbe liableforanylossofprofitoranyothercommercialdamages,includingbutnotlimitedtospecial,incidental,consequential,orotherdamages.
LibraryofCongressCataloging-in-PublicationDataappliedfor
ISBN:9781119793557(hardback)
CoverDesign:Wiley
CoverImages:CourtesyofEdgardElChaar
Setin9.5/12.5ptSTIXTwoTextbyStraive,Chennai,India
Contents
ListofContributors xiii
Introduction xv
PartIFundamentals 1
1AnatomyandPhysiology 3
EdgardElChaarandThierryAbitbol
OverviewofGingivalTissueandPeriodontium 3
EmbryonicDevelopment 3
FormationoftheEpithelialAttachment 4
FormationoftheCementum,PeriodontalLigament,andAlveolarBone 4
SoftTissuePhysiology 6
Gingiva 6
WidthandThicknessoftheGingiva 6
HistologicalComposition 6
Epithelial–ConnectiveTissueInteraction 7
GingivalFiberGroups 7
AlveolarMucosa 7
JunctionalEpithelium 8
Biotype 8
PeriodontalBiotype 8
AnatomyIsDestiny 9
Anatomy 9
RootSurfaceAnatomy 9
AnteriorTeeth 10
DevelopmentalAnteriorGrooves 10
Premolars 10
TheRootTrunk 11
MaxillaryFirstMolars 11
MandibularFirstMolars 11
CervicalEnamelProjections(CEPs) 12
References 12
FurtherReading 13
2WoundHealing 14
StevenEngebretson
DefinitionsandTermsforClinicalOutcomes 14
InflammatoryPhase 14
ProliferativePhase 14
RemodelingPhase 15
EpitheliumandConnectiveTissueHealing 15
FlapSurgery 15
FreeGraft 15
BoneHealing 15
HealingofExtractionSockets 16
Osseointegration 16
ModifiersofWoundHealing 16
References 17
3DiagnosisandPathologyofPeriodontalDiseases 18
CeciliaWhite
FormulatingaPeriodontalDiagnosis 18
PeriodontalHealthandGingivalHealth 18
Gingivitis:DentalPlaque-Induced 19
NecrotizingPeriodontalDiseases 19
Periodontitis 19
OtherConditionsAffectingthePeriodontium 20
PeriodontalAbscesses 20
Endodontic–PeriodontalLesions 20
MucogingivalDeformitiesandConditionsAroundtheTeeth 20
TraumaticOcclusalForces 20
ProsthesisandTooth-RelatedFactors 20
References 21
4OralPathologyandOralMedicine 22
EdgardElChaarandArthiM.Kumar
Introduction 22
Non-Dental-BiofilmInducedGingivalDiseases 22
Genetic/DevelopmentalDisorders 22
HereditaryGingivalFibromatosis(HGF) 22
SpecificInfections 22
InfectionsofBacterialOrigin 22
InfectionsofViralOrigin 24
InfectionsofFungalOrigin 25
InflammatoryandImmuneConditions 27
HypersensitivityReactions 27
AutoimmuneDiseasesofSkinandMucousMembranes 27
GranulomatousInflammatoryConditions 30
ReactiveProcesses 31
Epulides 31
Pre-MalignantLesionsandMalignantNeoplasms 32
Endocrine,Nutritional,andMetabolicDiseases 34
TraumaticLesions 34
Physical/MechanicalInsults 34
Chemical/ThermalInsults 36
GingivalPigmentation 36
Endocrine,Nutritional,andMetabolicDiseases 38
GeneticDisorders 38
DiseasesAffectingtheConnectiveTissues 39
AcquiredImmunodeficiencyDiseases 41
InflammatoryDiseases 41
SystemicDisordersthatInfluencethePathogenesisofPeriodontalDisease 41
FurtherReading 44
5PatientExaminationandInitialTherapy 50
ClaireMcCarthy,SteveEngeberston,EdgardElChaar,MeaWeinberg,StuartL.Segelnick,andDenaM.Sapanaro
MedicalHistoryfortheDentalPatient 50
ClinicalandRadiographicalExamination 50
ClinicalExamination 50
RadiographicExamination 51
RadiographicArtifacts 51
OralHygiene 51
Toothbrushing 52
InterproximalCleaning 52
InterproximalBrushes 52
DentalFlossorTape 52
SpecializedOralHygieneAids 53
SingleTuftedBrush 53
BehaviorChangeTechniques 53
Non-surgicalPeriodontalTherapy 54
Benefits 54
Limitations 54
Armamentarium 54
HandInstruments 54
PoweredInstruments 54
Techniques 55
SupragingivalDebridement 55
FundamentalElementsofHandInstrumentation 55
CalculusDetectionTechnique 55
Fulcrums 56
Powered(Ultrasonic)Technique 56
ReevaluationofInitialTherapy 56
OcclusalTherapy 56
MedicationsandImplicationsforPeriodontalTherapy 57
Sedation:MinimalandModerateSedation 57
References 58
FurtherReading 58
PartIIPrinciplesandPracticeofPeriodontalSurgery 61
6SurgicalAnatomyandLocalAnesthesia 63
RoyaAfshar-MohajerandBabakHamidi
AnatomicLandmarks 63
Mandible 63
AnatomicSpaces 65
Maxilla 65
Conclusion 67
PropertiesofLocalAnesthesia 67
PropertiesofIdealAnesthetic 68
TechniquesofLocalAnesthesia 68
MaxillaryAnesthesia 68
MandibularAnesthesia 68
FurtherReading 69
7SuturingTechniques 70
MeaA.Weinberg,StuartL.Segelnick,andEdgardElChaar PrinciplesofSurgicalWoundClosure 70 PropertiesofSutureMaterials 70
SuturingTechniquesandIndicationsforUse 72 References 76
8OsseousSurgery 77 ThierryAbitbol Introduction 77
OsseousSurgery 77
LimitationsandContraindicationstoOsseousResectiveSurgery 78 References 78
9FunctionalCrownLengthening 79 ThierryAbitbol Introduction 79 Checklist 79
OsseousSurgery 80 References 81
10RootAmputation 83
WayneKye Overview 83 Terminology 83
IndicationsandContraindications 84
IndicationsInclude 84
ContraindicationsInclude 84
AdvantagesandDisadvantages 85 Armamentarium 85
SurgicalTechnique 85 Complications 86
OutcomeandFollow-up 86
ImplantsVersusRootResection 87
VitalRootResection 87 References 88 FurtherReading 89
11GuidedTissueRegeneration 90
EdgardElChaarandMichaelBral Overview 90 Indications 91
RepairandRegenerationinPeriodontalDefects 91
GTRforFurcationDefects 91 Technique 91
GTRforPeriodontalIntrabonyandCircumferentialDefects 93
Techniques 94
GTRfortheTreatmentofRecessionDefects 95
Follow-up 97
FurtherReading 97
12EstheticCrownLengthening 98
EdgardElChaar
Overview 98
Etiology 98
Treatment 99
CaseSurgicalDescription 99
Post-ElongationGingivalMarginStability 101
References 101
FurtherReading 102
13SoftTissueManagementinNaturalDentition 103
EdgardElChaar
Overview 103
Classifications 104
DeterminationoftheCEJ 104
DiagnosticandTreatmentConsiderationsBasedonClassificationofPeriodontalBiotypes,
GingivaRecession,andRootSurfaceConditions 106
SurgicalManagementofMucogingivalDeficiencies 106
FreeGingivalGraft(FGG) 106
PedicleSoftTissueGraft 106
CoronallyAdvancedFlap(CAF) 107
Sub-epithelialConnectiveTissueGraft(SCTG) 107
Allograft 108
AcellularDermalMatrix 108
ClinicalStudiesComparingSoftTissueAllografttotheSCTG 109
HistologicalStudiesonSoftTissueAllograft 109
ClinicalCase 109
References 111
FurtherReading 113
PartIIIPrinciplesandPracticeofImplantDentistry 115
14PrinciplesofImplantDentistry 117
EdgardElChaarandAikateriniGeorgantza
Introduction 117
StepsforImplantSuccess 117
FactorsAffectingtheImplantSuccess 118
BoneQualityClassification 118
BonetoImplantContact 118
TransmucosalAttachmentAroundDentalImplants 118
ProbingAroundDentalImplants 118
BiologicalWidthAroundImplants 119
TheMicrogap:InterfaceBetweenImplantandAbutment 119
PlatformSwitching 119
FundamentalCriteriainImplantPlacement:HealedRidges 120
ImplantSurfaceTopography 120
ImplantTopographyonWoundHealing 120
ImplantMaterials 120
BoneHealing 120
PrinciplesofSurfaceTreatment,Topographies,andRoughness 121
ImplantDesign 121
ImplantSurfaceTopography 121
ImplantSurfaceSpecificities:AdvantagesandDisadvantages 121
References 122
FurtherReading 124
15ExaminationandDiagnosis 125
ZahraBagheri
RadiographicExamination 125
ConeBeamComputedTomography 125
ClinicalParameters 125
ClinicalExamination 126
FactorsInfluencingSurgicalManagement 126
FactorsInfluencingProstheticParameters 126
References 127
FurtherReading 127
16ProstheticConsiderations 128
ZahraBagheri
ReviewoftheEstheticParameters 128
TheProstheticSpace 129
Temporization 129
CriticalSpace 129
SubcriticalSpace 130
BuccalContour 130
FinalRestoration 130
AbutmentOptions 130
CementedVersusScrewRetained 130
RestorativeMaterials 130
References 131
17DigitalWorkflowinSurgery 132
EdgardElChaar
IntroductiontoDigitalDentistry 132
Terminology 132
DescriptionofSTL 132
Descriptionof3DVolume 133
ApplicationsofInteractiveSoftware 133
Intra-OralScanners(IOS) 133
VirtualImplantSoftwarePlanning 133
DrillingSurgicalGuide 134
UseofGuidedSurgeryinImmediateImplantPlacement 134
FullArchGuidedSurgery 135
AidinRidgeDeficiencyDiagnosis 135
References 137
FurtherReading 137
18SocketManagement 138
AikateriniGeorgantza
AnatomicalFeaturesoftheAlveolarProcess 138
TheAlveolarProcess 138
TheAlveolarBoneProper 138
AlveolusandExtractionSocket 138
TheAlveolarRidge 138
ClassificationofRemainingBone 138
AlterationsoftheAlveolarProcessFollowingToothExtraction 138
BiologicalEventsandHistologicRidgeAlterations 138
OverviewoftheHistologicSequenceofHealing 139
DimensionalRidgeAlterations 139
ClinicalImplicationsforRidgePreservationandImplantTreatment 139
AtraumaticToothExtraction 140
IndicationsforRidgePreservation 140
ContraindicationsforRidgePreservation 140
RidgePreservationProcedures 140
MaintenanceoftheRootandtheSocketShieldTechnique 140 ForcedEruption 140
SocketGrafting 140
ManagementofSocketattheEstheticZone 141
ExtractionSocketClassifications 141
TimingofImplantPlacement 142
ImmediateImplantPlacement 142
EarlyImplantPlacementwithPartialBoneHealing(12–16Weeks) 144
LateImplantPlacementCompleteBoneHealing(>6months) 144
References 145
FurtherReading 146
19DeficientRidgesAugmentation 147
EdgardElChaar,AikateriniGeorgantza,andWayneKye CrestalSinusElevation 147
Background 147
Indications 147
Armamentarium 148
SurgicalTechnique 148
Complications 148
Follow-Up 149
LateralSinusFloorElevation 149
Background 149
Indications 149
GraftingMaterials 149
AnatomicalConsiderations 150
Armamentarium 150
SurgicalTechnique 150
Complications 151
PreventionofComplications 151
Follow-up 151
RidgeAugmentation 151
FundamentalsofRidgeAugmentation 151
SurgicalTechniques 152
RidgeClassifications 152
Seibert 152
ExpectationsofRidgeAugmentation 153
HorizontalRidgeAugmentation 153
VerticalRidgeAugmentation 153
FundamentalsofSuccessfulSurgicalTechnique 156
ClinicalCaseofRidgeAugmentation 156
References 158
FurtherReading 159
20SoftTissueAssessmentandEnhancementinImplantDentistry 161
EdgardElChaar
Introduction 161
TechniquestoCreateContour,Thickness,andIncreaseKeratinizedTissue 161
A-FlapManagement 161
RollTechnique 163
AutograftSubepithelialConnectiveTissue(CTG),aFreeGingivalGraft(FGG),orAllograftDermis 165
FreeGingivalGraft(FGG) 165
ConnectiveTissueGrafts(CTG) 166
TechniquesforPapillaManagement 172
RotatedPediculatedMarginalTissue 172
RotatedPediculatedLingualMarginalTissue 172
TechniquesofSoftTissueforExtractionSocketGrafting 173
References 176
FurtherReading 177
21Peri-ImplantDiseases 178
EdgardElChaarandCeciliaWhite
Introduction 178
Prevalence 178
CriteriaforDiagnosisofPeri-implantitis:CaseDefinition 179
RiskFactors 179
HistoryofPeriodontitis 179
ImplantMaintenance 179
NumberofImplants 179
ClinicianExperience 179
ImplantBrand 179
Smoking 179
Microbiota 180
Treatment 180
NonsurgicalTherapy 180
Peri-implantMucositis 180
Peri-implantitis 180
SurgicalTreatment 181
WhatIstheMostPredictableorSuperiorTreatmentModality? 181
ClinicalCasetoIllustratePeri-implantitisTreatment 182
References 184
Index 187
ListofContributors
ThierryAbitbol
ArthurAshmanDepartmentofPeriodonticsandImplant Dentistry
NewYorkUniversity NewYork,NY USA
RoyaAfshar-Mohajer
AshmanDepartmentofPeriodontologyandImplant Dentistry
NewYorkUniversityCollegeofDentistry
NewYork,NY USA
ZahraBagheri
AshmanDepartmentofPeriodontologyandImplant Dentistry
NewYorkUniversityCollegeofDentistry
NewYork,NY USA
MichaelBral DepartmentofPeriodonticsandImplantDentistry
NewYorkUniversityCollegeofDentistry
NewYork,NY USA
EdgardElChaar DepartmentofPeriodontics UniversityofPennsylvania DentalMedicine Philadelphia,PA USA
StevenEngebretson DepartmentofPeriodontologyandImplantDentistry
NewYorkUniversityCollegeofDentistry
NewYork,NY USA
AikateriniGeorgantza
AshmanDepartmentofPeriodontologyandImplant Dentistry
NewYorkUniversityCollegeofDentistry
NewYork,NY USA
BabakHamidi AshmanDepartmentofPeriodontologyandImplant Dentistry
NewYorkUniversityCollegeofDentistry
NewYork,NY USA
ArthiM.Kumar DepartmentofOralandMaxillofacialPathology Radiology&Medicine
NewYorkUniversityCollegeofDentistry
NewYork,NY USA
WayneKye AshmanDepartmentofPeriodontologyandImplant Dentistry
NewYorkUniversityCollegeofDentistry NewYork,NY USA
ClaireMccarthy King’sCollege London UK
DenaM.Sapanaro DepartmentofPediatricDentistry
NewYorkUniversity NewYork,NY USA
StuartL.Segelnick
ArthurAshmanDepartmentofPeriodonticsand ImplantDentistry
NewYorkUniversity
NewYork,NY
USA
MeaA.Weinberg
ArthurAshmanDepartmentofPeriodonticsand ImplantDentistry
NewYorkUniversity
NewYork,NY USA
CeciliaWhite Privatepractice Princeton,NJ USA
Introduction
Inthepast28years,frombeingaresidenttoacademician andclinicalpractitionerinthescienceofPeriodonticsand ImplantDentistry,Ihavewitnessedanexponentialevolutioninthepossibilitiesoftreatments.Consequently,that comeswithawealthofinformationtothepractitioners makingthediscernmentbetweenvalidityoftreatment choicesdifficult.Iworkedthroughouttheyearsonbasing mytreatmentsandmyteachingaroundsolidbiological foundationbecauseIalwaysbelievedthatfundamentals neverchange.Withthatinmind,thepractitionerhasto alwayssetthegoaloftreatmentandthenworkhis/her waybacktoevaluatethestepsittakestoexecuteit.These stepshavetobebasedon,asstatedbefore,solidbiological foundations.
Inordertounderstandthesesolidfoundations,webuilt thismanuscriptinawaytostartwithareviewoffundamentals,mainlythewoundhealing,preparingamorein depthfocusedventedinformationthatthepractitioner canreview.Thesewillbedoneinafacilitatedmanner withoutcompromisingontheneededfundamentals.This manuscriptwillhelpeitherapractitionerinpreparinga surgicaldecision,aresidentpreparingforhis/herboards,
oradentalstudent/surgicalresidentlearningthescience ofPeriodonticsandImplantDentistry.
Iamgratefulformycolleaguesthatcontributedtothis manuscript,withouttheirinvaluableparticipationthis manuscriptwouldhavenotbecomeareality,thusbenefitingtheuserofthiswork.Iwouldliketospecificallythank myoldestdaughter,Lauren,forencouragingmeandhelpingmeinthewritingoftheproposaltothepublisherduring thelockdownfortheCovid-19pandemic.Ihopethatshe, oroneofmyotherchildren,onedayuseitfortheirstudies iftheydecidetotakedentistryastheirvocationalprofessionalcareer.Finally,foryouthereader,Iamhonored andhumbledthatyouchosethisbookinyourendeavor. Periodontology-ImplantDentistryhasbeenagreatjourney formeandIhopeitwillbethesameforyou.Keeplearning andalwaysrememberthreethings:biologyalwayswins, fundamentalsneverchange,setyourgoal,andworkyour wayback.
Sincerely,
EdgardElChaar
Fundamentals
AnatomyandPhysiology
EdgardElChaar 1 andThierryAbitbol 2
1 DepartmentofPeriodontics,UniversityofPennsylvania,DentalMedicine,Philadelphia,PA,USA
2 ArthurAshmanDepartmentofPeriodonticsandImplantDentistry,NewYorkUniversity,NY,USA
OverviewofGingivalTissue andPeriodontium
Macroscopically,thedentalorganappearstobelimited tothedentalcrownsurroundedbysofttissue,whichis scallopedaroundawelldelineatedcircularlinecalledthe cementoenameljunction(CEJ).
Themorphologyofthedentalcrownschangeshape fromthemidlinetotheposteriordentitionandwithit,the functionanddimensionchange.Thesofttissuechanges aswelltoaccommodatethesedifferences.Thatsofttissue willcomprisetwodistinctparts,themucosaandthekeratinizedtissueseparatedbythemucogingivalline(MGL).In thekeratinizedzone,wehavetheattachedgingivaandthe marginalgingiva.Thelatterisanon-attachedtissuethat extendsfewmillimetersfromthemargintothejunctional epithelium(JE),delineatingthesulcusthatisagaponthe innersideofthenon-attachedgingivaaroundtheCEJ.JE isnon-keratinizedepitheliumasitisontheborderofthe attachedandnon-attachedgingiva.
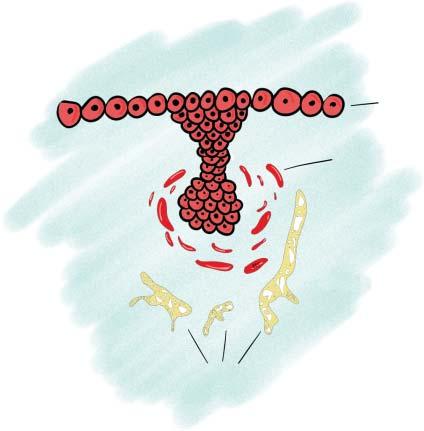
Inamicroscopiccross-sectionalview,wecanappreciatethedifferentpartsofhardandsofttissueinteracting togethermakingtheperiodontiumofthedentalorgan fromitsincisaltipapically(Figure1.1).Thisfigureshows theintricatecomponentsofthedentalorganandthe harmonyneededtomakethisinteractionworkreminding usofawell-tunedopera.Allofthishardandsofttissue requiresirrigationfromperfectlylinedupbloodcirculation,whichoriginatesfromanalveolararterydividing itselfinaperiodontalligament(PDL)branch,dental branch,andanintra-marrowbranch.Insidethemucosa, anintricatecircularsystemleadstoasupra-periosteal arterycrossingintothekeratinizedgingivainalinearmanneruptothegingivalcollarinwhichthethreearteries,
PDL,intra-marrow,andsupra-periostealformthegingival crevicularplexus(Figure1.2).
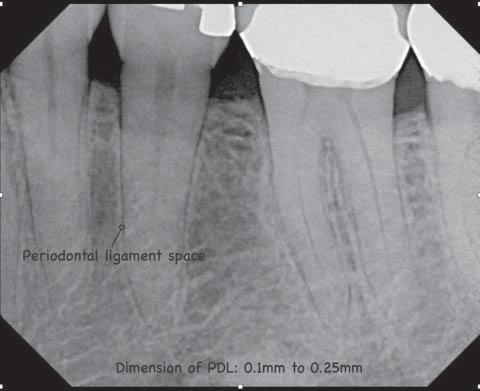
Radiographically,thePDLspacecanbeobservedandits widthrangesbetween0.1and0.25mm(Figure1.3).Any wideningbeyondthesemarginsisconsidereda“widening oftheperiodontalligament,”whichcanbeasignofinflammationeitherfromanearlyperiodontaldiseaseatthecoronallevelorexcessiveocclusaltrauma.
Thisharmoniousintricatesystemcalledthedentalperiodontiumwillbereviewedinthismanual,wishingyou greatreadingandenjoyment.
EmbryonicDevelopment
Atapproximatelyfourtofiveweeksintoembryonicdevelopment,thereisdowngrowthoftheectodermofthe primitiveoralstomatodeumintotheunderlyingectomesenchyme.Attheterminalendofthisdowngrowth,thecells formaknoblikestructureorbud.Cellsinthesurrounding ectomesenchymebegintoconcentratearoundthisbud.
Severalweekslater,thisectodermalbudhasdevelopedintoacuplikestructurewithfourdistinctlayers: anouterenamelepithelium(OEE),aninnerenamel epithelium(IEE),astellatereticulum(SR),andastratum intermedium(SI).DirectlybeneaththeIEE,cellsofthe underlyingectomesenchymehavecondensedintoadental papilla(DP).Surroundingthesetwostructuresisathird condensation,thedentalfollicle(DF),whichwillgive risetomostofthecementum,periodontalligament,and alveolarbone.
Attheapicalextentoftheroot,theIEEandOEEhave fusedtoformHertwig’sepithelialrootsheath(HES).More coronally,thisrootsheathbreaksdowntoformislandsof
Crevicular epithelium
Junctional epithelium
Periodontal ligament
Mucogingival junction
Alveolar bone
Alveolar mucosa
Cementum

Differentcomponentsoftheperiodontiuminacross section.
epithelialcellsinthedevelopingPDLspace,theepithelial restsofMalassez(ERM).Thebreakdownoftherootsheath andsubsequentexposureofthedentin(D)totheDFallows cellsintheDFnearestthedevelopingrootsurfacetodifferentiateintocementoblasts(CB)andlaydownthefirst cementummatrix(CM).Furtherawayfromthetoothfollicle,cellsdifferentiateintofibroblastsandlaydownthefirst bundlesofcollageninthePDL(Figures1.3–1.6).

to 5 weeks
FormationoftheEpithelialAttachment
Afterformed,theenameliscoveredbyanepithelium calledthereduceddentalepithelium(RED)extending
toCEJ.Duringeruption,thetipofthetoothapproaches theoralmucosaleadingtoafusionoftheREDwithoral epithelium(OE).Oncethetipemerges,theREDistermed EpithelialAttachment.Asthetootherupts,theattached epitheliumgraduallyseparatesfromitssurfacecreatinga groovecalledtheGingivalSulcus.
FormationoftheCementum,PeriodontalLigament, andAlveolarBone
ThedepositionofcementumontherootsurfacethatgraduallythickenstowardthePDLspaceissomewhatsimilar

Figure1.5 Bellstageinembryologicformation.(OEE:outer enamelepithelium;IEE:innerenamelepithelium;SR:stellate reticulum;SI:stratumintermedium;DF:dentalfollicle;DP: dentalpapilla).

Cementum matrix Cementoblast
periodontal ligaments Bone
Figure1.6 Apicalformationofthedifferentperiodontal ligament.ERM,epithelialrestofmalassez;HES,Hertwig’s epithelialrootsheath.
tothedepositionofalveolarbonethatthickensthealveolarbonesupportfromtheoppositesideoftheligament space.Asaresult,thecementumdoeshavesomestructural andbiochemicalsimilarities(aswellassomecriticaldifferences)withalveolarbone.
Aswiththedevelopmentofthealveolarboneproper, anorganicmatrixofcementumcomposedprimarilyof typeIandtypeIIIcollagenissecretedbyalayerofformativecells(thecementoblasts)overthethinhyaline-like
layersecretedbyHEScoveringtherootdentin.Thisfine fibrillarmatrixcalcifiestoformarelativelyuniformand well-organizedlayerofcementumfreeofcellularelementscalledprimaryacellularcementum.Thisfirstthin layerofmineralizedcementumcontainsonlythefibrillar matrixfromthecementoblaststhemselves.Thesefibers arethereforecalledintrinsicfibersofcementum.
Asthecementumcontinuestothickenbyapposition ofcementumbythecementoblastlayers,thisthickening cementumwillencounterandincorporatebundlesofthe formingperiodontalligament.Theseligamentbundles incorporatedintothecementumsurfacewillcalcifyalong withthesurroundingintrinsicfiberstoformasignificant portionofthemoresuperficiallayersofthecementum. Theseinsertionsofcalcifiedligamentfibersaretermed extrinsicfibersofthecementum.Asimilarentrapment andcalcificationprocessoccursontheformingalveolar boneside.Thegeneraltermforthesecalcifiedinsertionsof bundlesofligamentfibersintothecementumandboneare Sharpey’sfibers.Onthecementumside,theseSharpey’s fibersaremuchthinnerindiameterandinsertatcloser intervalswhencomparedwiththealveolarboneside.
Thesedifferencesinthepatternofinsertionhaveclinical importanceinthedistributionofforcesthataregeneratedwithinthePDLduringocclusion,toothmovement, andtraumaticforces.Specifically,theseforcesaremore evenlydistributedalongthecementumsurfaceandare moreconcentratedalongthemorewidelyspacedinsertionsonthealveolarboneside.Asaresult,inresponse tomechanicalforces,thereisgenerallyaremodelingof theperiodontalhousingonthealveolarbonesideandnot onthecementumside.Thispreventsthepossibilityof significantcementumandrootresorption.Inaddition,the rootcementumisprotectedfromthisrelativelyextensive remodelingbecauseitisavascular,andthereforenotas exposedtoosteoclast-likeprecursorcellsinthecirculation. Althoughsmallareasofmicroscopiccementumresorption andrepairhavebeenfrequentlyobservedinhistologic sections,moreextensiveresorptionofcementumisusually notseenunlessthereisaforceonthetoothofahigh enoughmagnitude,orduration,orboth,thatcannotbe accommodatedbytheremodelingofthealveolarbone.
Asthetoothcompletesactivelyeruptingintotheoral cavityandmeetsitsopposingtoothintheotherarch, theformationofcementumbecomessomewhatlessregularandorganized.Thistypeofcementumformation thatoccursoverthemoreorganizedprimarycementumis calledsecondarycementum.Itoccursmainlyalongtheapicalonethirdoftheroot.Duringtheformationofsecondary cementum,cellsinthelayerofsecretingcementoblastswill oftenbecomeentrappedwithintheCM.Theseentrapped cementoblastsbecomecementocytessimilarinappearance
totheentrappedosteoblaststhatbecomeosteocytesonthe alveolarboneside.Theseareasofcementumthatcontain cementocytesarecalledcellularcementum.Layersof cellularcementumaregenerallyseenintheapicalone thirdoftherootsurface.Insecondarycementum,these layersofcellularcementumoftenalternatewithlayersof acellularcementum.
SoftTissuePhysiology
Gingiva
Thegingivaconsistsoffreeandattachedtissue.The attachedgingivaistheportionofthegingivathatisfirm, dense,stippled,andtightlyboundtotheunderlyingperiodontium,tooth,andbone.Thefreegingivalmarginis definedasthecoronalborderofthefreegingivathatsurroundsthetoothandisnotdirectlyattachedtothetooth surface.Thefreegingivalmargingenerallycorresponds tothebaseofthegingivalsulcus.Itispresentin30–40% ofadultsandmostfrequentlyoccursinthemandibular premolarandincisorregions.Themucogingivaljunction(MGJ)representsthejunctionbetweenthegingiva (keratinized)andalveolarmucosa(non-keratinized) (Lindhe1983).
WidthandThicknessoftheGingiva
Bowers(1963)measuredthewidthsofthefacialattached gingivaintheprimaryandpermanentdentitionsof240 subjects.Thewidthofattachedgingivarangedfrom1to 9mm.Valuesweregreatestintheincisorregions(especiallythelateralincisor)andtheleastinthecanineand firstpremolarsites.Themaxillausuallyexhibitedabroader zoneoftheattachedgingivathanthemandible.Clinically healthygingivawasnotedinsubjectswithlessthan1mm oftheattachedgingiva,butthetissuewasusuallyinflamed inareasofnoattachedgingiva.Buccal–lingualtoothpositionaffectedtheamountoftheattachedgingivapresent, andhighfrenumandmuscleattachmentsweregenerally associatedwithnarrowzonesofattachedgingiva.Facially positionedteethhadnarrowerzonesofattachedandkeratinizedtissuethanwell-alignedorlinguallypositioned teeth.Asteethmovedlingually,anincreaseinthewidth ofattachedandkeratinizedtissueandaslightdecreasein clinicalcrownheightwereobserved.Teethmovingfacially hadadecreaseinthewidthoftheattachedandkeratinized tissue.
Voigtetal.(1978)measuredthewidthoflingualattached gingivainthemandible.Thekeratinizedtissuerangedfrom
1to8mm.Greatestwidthswererecordedonthefirstand secondmolars(4.7mm),decreasingatpremolarandthird molarsites.Thesmallestwidthswereobservedonthe incisorsandcanines(1.9mm).
Goaslindetal.(1977)measuredthethicknessofthefree andattachedfacialgingivainapopulationconsistingof 10males(ages25–36).Resultsdemonstratedconsiderablevariationofgingivalthicknessamongsubjectsand amongareaswithinindividualsubjects.Freegingival thicknessaveraged1.56–0.39mm,increasedfromanterior toposteriorandwasdirectlyproportionaltosulcusdepth. Thicknessoftheattachedgingivaaveraged1.25–0.42mm, increasedfromanteriortoposteriorinthemandibulararch, remainedrelativelyconstantinthemaxillaryanterior,and wasinverselyproportionaltoattachedgingivalwidth.The overallmeanthicknessforallareaswas1.41mm.
HistologicalComposition
Asdiscussedinthetoothdevelopmentsection,whiletooth emergesanderuptioncontinues,threedistinctzonesof epitheliumform:outerepithelium,crevicularepithelium, andtheJE.Eachisdifferentinstratification,organization, andfunction.
Liketheepidermis,theOEhasmultiplelayers:
1. Stratumbasale:onetotwolayerofcuboidal-shaped cellsthatdivideandmigratetothesuperficiallayers
2. Stratumspinosumorpricklecelllayer:spinousshapedcellswithlargeintercellularspaces
3. Stratumgranulosum:flattenedgranularcellswithflattenedandcondensednuclei,increasedaccumulationof keratohyalingranules,andintracellularandextracellular membrane-coatedgranules
4. Stratumcorneum:flattenedcellspackedwithkeratin; nucleimaybeundiscernibleknownasorthokeratinized ormayhavevisibledensenucleicalledparakeratinized; cellsshedandarereplacedbycellsfromthedeeperlayers migratingupward.
Inboththebasalandpricklecelllayersconnecttoeach otherviadesmosomes,whichappearmicroscopicallyasa thickening.Eachhalfismadeofahemi-desmosomethat attachtounderlyingcellthroughintermediatefilaments. Withintheoralgingivalepithelium,thereareseveral othercellsnotderivedfromkeratinocytes.Theseinclude melanocytesthattransfermelaninpigmentgranulesto thesurroundingbasallayerofkeratinocytes,Langerhans cellsthatarepartofthereticulo-endotheliumsystem andareresponsibleforprocessingandpresentingforeignantigenstotheimmunesystem,andMerkelcells
thatmayberesponsibleforperceptionofsensationinthe gingiva.
Ontheouterlayer,in45%ofthepatient,stipplingis noticed.Itusedtobethoughtthatitspresenceisasignof healthbutlateritwasrefuted.BasedonKarringandLoe (1970),thestipplingcoincideswiththeintersectionwith epithelialridges.Epithelial(rete)ridgesrepresentareas ofepithelialproliferationintotheunderlyingconnective tissue(CT).Thesearebelievedtopromoteanchoringof epitheliumtotheCTbyincreasingthesurfaceareaof attachment.Theyaremorepronouncedinthegingivathan inthealveolarmucosa.
TheCTofthegingivaconsistsofcells,fibers,andground substance(proteoglycans[PGs]andglycoproteins[GPs]). Cellsconstituteabout5%oftheCTandincludefibroblasts (65%),mastcells,PMNs,macrophages,lymphocytes,and plasmacells.Fibersaccountforapproximately60–65%of theCT,withcollagenpredominatingreticulinandelastic fibers.Groundsubstancecomprises35%oftheCTand consistsofprotein-polysaccharidemacro-moleculesmade upofPGsandGPs.ThePGscontainglycosaminoglycans (GAGs)asthepolysaccharideunitsthatarecovalently bondedtooneormoreproteinchains.PGsareusually largemoleculesinthegroundsubstancethatfunction toregulatediffusionandfluidflowthroughthematrix, actingasmolecularfilters.GPsfunctionincell-to-cell andcell-to-matrixinteractions.Fibronectin(FN)isthe principalGPinCT,servingtoorientfibroblaststocollagen andprovideproteinattachmentforcell–matrixadhesions. FNmayinfluencethemigrationoffibroblastsandplay acrucialroleinmaintainingstructuralintegrityofCT. Laminin(LN)istheattachmentGPforepithelialcells, whichmediatesattachmentofthesecellstothebasement membraneandpreferentiallybindstypeIVcollagen.
Epithelial–ConnectiveTissueInteraction
Karringetal.(1975)examinedtheroleofCTindeterminingdifferentiationoftheepitheliumbyimplanting CTfromthepalatesofmonkeys(withtheepithelium removed)intopouchescreatedinthebuccalalveolarmucosa.Threetofourweekslater,thegraftswere exposedandallowedtore-epithelializefromsurrounding non-keratinizedalveolarmucosa.ThesiteswithCTtransplantsfromthepalatehealedwithakeratinizedsurface displayingthesamecharacteristicsasnormalgingival epithelium.Theresultsofthisstudydemonstratedconclusivelythatthedeterminantforepithelialdifferentiation (keratinizationornon-keratinization)istheunderlyingCTandisnotthefunctionalstimuliaspreviously thought.
GingivalFiberGroups
Hassell(2000),describedthegingivalcollagenfibersand dividedthemintofiveprincipalandsixminorgroupings.
Theprincipalgroupings:
a.Dentogingival
b.Alveolo-gingival
c.Dento-periosteal
d.Circular
e.Transseptal
Thesecondarygrouping:
a.Periosteogingival
b.Interpapillary
c.Transgingival
d.Intercircular
e.Intergingival
f.Semicircular
Thedentogingivalfibersextendfromthecementuminto thelaminaproprialaterally.Alveolo-gingivalfibers“fan” coronallyintothelaminapropriafromtheperiosteumat thealveolarcrest.Thedento-periostealfibersextendfrom thecementum(closetoCEJ)intotheperiosteumatthe alveolarcrest.Circularfiberscircumscribethetoothand arepresentintheattachedgingivalcoronaltothealveolar crestandinthefreemarginalgingiva.Thetransseptalfibers extendmesiallyanddistally,insertingintothecementum oftheadjacentteethcoronaltothealveolarcrest.
AlveolarMucosa
Thealveolarmucosacoversthebasalpartofthealveolarprocessandcontinueswithoutdemarcationintothe vestibularfornixandthefloorofthemouth.Itismovable andlooselyattachedtotheperiosteum.
Themaindifferencewiththegingivaisthevascular networkdistributedwithintheperiosteumofthealveolar mucosa.Itisdenselyarranged,consistingofarterioles, venules,andalargenumberofcapillaries.Thisdifference indistributionofvesselsisconsideredtoreflectthehistologicaldifference.Intheattachedgingiva,theCTisfirmly attachedtothealveolarprocessandthatismainlydueto itsfunctionwhichistoresistthecompressionandfriction ofmastication(SquierandHill1985).Incontrast,the laminapropriaandsubmucosaltissuebeneaththealveolarmucosahaveafibrousstructureconsistingofmany elasticfibersthatarelooselyattachedtotheperiosteum tohandlethevascularmeshworkthatismainlycircular andstacked.AccordingtoLozdanandSquier(1969),the
markeddifferenceinelastictissuecontentbetweenthe gingivaandalveolarmucosawasusedasareferenceto definethistransitionandthepositionoftheMGJ.
JunctionalEpithelium
Asdiscussedearlierinthetoothdevelopment,withthe tootheruption,theOEandthereducedenamelepithelium(REE)fuseandtheJEisformed.Inperiodontal healththeJEconsistsofasingleormultiplelayersof non-keratinizingcellsadheringtothetoothsurfaceand functionsasasecurityseal-barrieratthebaseofthesulcus.
SabagandSaglie(1981)describedtheattachmentof epitheliumtothecementumrootsurfacetobemediatedby fourtoeighthemidesmosomespermicronatthecoronal zoneofepithelialattachmentandtwohemidesmosomes permicronintheapicalzone.Becauseofthisarrangement,theauthorssuggestedthatthecoronalzoneof thecementalsurfacemayexhibitenhancedadhesionof epithelialattachmentwhencomparedwiththeapical zoneGargiuloetal.(1961)studiedthedimensionsand relationsofthedento-gingivaljunctioninman.Themean averagelengthoftheepithelialattachment(phasesI–IV) was0.97mmwitharangeof0.71–1.35mmmeanaverage.
Histologically,TenCate(1989)foundthattheimmature characteroftheJEwascharacterizedbythepresence ofhemidesmosomesthatarenecessaryforepithelial attachmentbutarenotseeningingivalandsulcular epithelium.
Biotype
Theperiodontalbiotypeanditsclinicalsignificancehave fascinatedcliniciansandresearcherssincetheearlytwentiethcentury.Asearlyas1923,Hirschfeldconductedan anthropometricstudyonhumanskulls,inwhichhenoted theexistenceofathinalveolarcontour.Hepostulatedthat suchathinbonycontourwaslikelyaccompaniedbya thingingivalform.Lateron,in1969,OschenbeinandRoss classifiedthegingivalanatomyaseitherflatorpronounced scalloped.Theysuggestedthatflatgingivawasrelatedto squaretoothformsandpronouncedscallopedgingivawas relatedtotaperedtoothforms.In1977,Weisgoldasserted thatathin,scallopedgingivalarchitecturehasanincreased susceptibilitytorecession.
Laterin2009,DeRoucketal.illustratedthepresenceoftwodistinctgingivalbiotypes.Thefirsttypewas thin-scalloped,makingupone-thirdofthestudypopulation.Thesesubjectstypicallyhadaslendertoothform,a narrowzoneofkeratinizedtissue,andtendedtobefemales. Thesecondtypewasdescribedasthick-flat,occurringin
two-thirdsofthestudypopulation.Thesecaseswere comprisedofamoresquaretoothform,abroadzoneof keratinizedtissue,andweretypicallyfoundinmales.
Ina2010systematicreview,Fuetal.detailedthedifferentclinicalmethodsofdiagnosingbiotypeandthedifferencesnotedbetweenthetwo,asillustratedinthefollowing table:
CharacteristicsThinThick
ProfileHighlyscalloped softtissueand bonecontours
Softtissue texture
Widthof keratinizedand attached gingiva
Relativelyflatsoft tissueandbone contours
Delicate,friableDense,fibrotic
NarrowWide
BonethicknessThin;presence ofbony dehiscencesand fenestrations
Thick;presenceof ledges
Reactionto insults Reactsreadily withrecession Relatively resistantto gingival recessions;reacts withpocket formationor intrabonydefects
PeriodontalBiotype
Onewaytodescribeindividualdifferencesastheyrelateto thefocusofthisreviewistheperiodontal“biotype.”The biotypehasbeenlabeledbydifferentauthorsasgingival orperiodontalbiotype,morphotype,orphenotype.In thisreview,itwillbereferredtoasperiodontalbiotype. Theassessmentofperiodontalbiotypeisconsideredrelevantforoutcomeassessmentoftherapyinseveraldental disciplines,includingperiodontalandimplanttherapy, prosthodontics,andorthodontics.Overall,thedistinctionamongdifferentbiotypesisbaseduponamultitude ofanatomiccharacteristicsofthecomponentsofthe masticatorycomplex,including:
1. Gingivalbiotype,whichincludesinitsdefinitiongingival thickness(GT)andkeratinizedtissuewidth(KTW)
2. Bonemorphotype(BM)
3. Toothdimension
ArecentsystematicreviewZweersetal.(2014),usingthe parametersreportedpreviously,classifiedthebiotypesin threecategories:
BiotypeCrownformCervicalconvexitiesLocationofcontactsZoneofKTTissuequalityAlveolarbonequality ThinscallopedSlender,TriangularSubtleIncisalNarrowClear,thinThin ThickflatSquarePronouncedCervicalBroadThick,fibroticThick ThickScallopedSlenderVariableVariableNarrowThick,fibroticVariable
Thestrongestassociationwithinthedifferentparametersusedtoidentifythedifferentbiotypesisfoundamong GT,KTW,andBM.Theseparametershavebeenreported tobefrequentlyassociatedwiththedevelopmentorprogressionofmucogingivaldefects,gingivalrecessioninparticular.Keratinizedtissuewidthrangesinathinbiotype from2.75(0.48)mmto5.44(0.88)mmandinathickbiotypefrom5.09(1.00)mmto6.65(1.00)mm.Thecalculated weightedmeanforthethickbiotypewas5.72(0.95)mm (95%CI5.20;6.24)and4.15(0.74)mm(95%CI3.75;4.55) forthethinbiotype.Gingivalthicknessrangesfrom0.63 (0.11)mmto1.79(0.31)mm.AnoverallthinnerGTwas observedwithcanineteethandrangedfrom0.63(0.11)mm to1.24(0.35)mm,withaweightedmean(thin)of0.80mm (0.19).
Whendiscriminatingbetweeneitherathinorthick periodontalbiotype,ingeneral,athinnerGTcanbefound inathinbiotypepopulationregardlessoftheselected study.Bonemorphotype(BM)resultedinameanbuccal bonethicknessof0.343(0.135)mmforthinbiotypeand 0.754(0.128)mmforthick/averagebiotype.BMshavebeen radiographicallymeasuredwithcone-beamcomputed tomography(CBCT).
AnatomyIsDestiny
Anatomy
Ahealthyperiodontiumislargelyderivedfromaphysiologicequilibriumamongessentialelementsconducivetoa stableenvironmentagainstchronicdeterioration.Asatherapeuticobjectiveitisinfactthesecomponentsthat,once identified,arerecreatedsurgicallyornon-surgically.
Tothatendosseoussurgery,forexample,resultsideally intheartificialrecreationofaphysiologicarchitectureof boneanditsrelationtotheoverlyingsofttissue.Asurgicallyrecreatedperiodontalenvironmentiswherepresumablyhealthmaybemaintainedwithareasonableregimen ofhomecareandofficehygienevisits.
Ofthecomponentsthatmustbegivendueattentionin theunderstandingofperiodontalhealthdiseaseandsubsequenttreatment,theanatomyofthenaturaldentitionis akey.
Athoroughstudentofthefundamentalsofperiodontics cannotescapetheuncannynearmathematicalsystem,
whichexistsandbindsbasicdentalanatomyasitsmost recurrentvariationsarticulateandcoexistwiththeelementsoftheperiodontium,namely,softtissueandbone. Tothatendwewillconcentrateprimarilyontheradicular anatomyofthepermanenthumandentitionandsome relevantaspectsofcoronalanatomyaswell.
Understanding“thesystem”isonewaytoseeclearly throughthemazethatrepresentsperiodontalhealthand restingequilibrium,disease,andtherecreationofaremissivestatethroughtreatment.Thischapterisanattemptto reviewsomeofthemoresalientfeaturesofdentalanatomy astheyrelatetoperiodontalparameters.
RootSurfaceAnatomy
Facialandpalatalorlingualrootsurfacesareforthemost partconvextoflat.Therelativepositionoftheserootsurfacesaswellastheirinherentgeometrymakethesesurfacesmoreaccessibleandlesspronetotheaccumulationof biofilm,presumablywithadequatehomecareandhygiene. Interproximalandinterradicularrootsurfacesareprimarilyconcavetoflat;thesesurfacesontheotherhand,because oftheirrelativepositioninthearchandbecauseoftheir shapearemorelikelytobesusceptibletoperiodontalbreakdown.
Proximalandinterradicularsurfaceshoweverbecauseof theiroutline,whichisgenerallyconcave,andtheirinter proximalorinterradicularpositionareinfactlessamenable tomaintenanceandmorepronetoperiodontalbreakdown thanfacialorlingualsurfaces.
Thispatterntendstoworsenanteroposteriorforatleast tworeasons:
Anteriorteethareinherentlyaccessibleforhygiene, whereasposteriorteethwouldbemoreproblematicin thatrespect.Interproximalcontactsandcorresponding septaarealsogenerallybroaderfromtheanteriorpart ofthearchback.Thisparticularanatomymakesthe posteriorcontactarea,theareainitiallysusceptibletoan etiologicalinsultandlesionmoredifficulttoaccess. Alsoasperiodontaldiseaseprogresses,theformationof osseouscratersorforthatmatteranytypeofintrabony lesionisnowmorelikelytoformwherebroadposteriorseptaareinitiallypresent.Thisaddstotheoverall inaccessibilityoftheseareas.Againthereasonswhy craterformationismoreprobablewithbroadersepta
isthepurposeofasubsequentpartofthebookwhere thebiologicfundamentalsofdiseaseprogressionand healingwillbeentertained.
AnteriorTeeth
Weknowanteriorteethforthemostparttobesinglerooted withamostlyconicalradicularshapeapico-coronally.They arerelativelyaccessiblefordebridementbecauseoftheir forwardpositioninthearch.Fromthepointofviewofa periodontistthefactthatanteriorteethhaveconicalroots impliesthefollowing:
Verticallossofattachmentbecomesexponentiallymore severeasitprogressesapicallyonanincreasinglyfluted radiculararea.Also,asperiodontaldiseaseincreasesin severity,thesemaybecomemoredifficulttorestoreand recreateanestheticoutcome,particularlyinthemaxillaryanteriorsegmentwherefluteddivergentrootslead toblackinterproximaltriangleswitharecededperiodontium.Anteriorteethwithanaccentuatedfacialor buccalparaboliccontoursaremoredifficulttorestoreas opposedtoteethwithaflatterprofile.Coronalanatomy ofanteriorteethisusuallydescribedassquare,ovoid, ortapered/triangle.Squarecrownsareusuallyassociatedwithrelativelybroadinterproximalcontactareasin allthreedimensions.Forthisparticularanteriortooth morphologythesofttissuebiotypeisusuallythick.
Squarecrownsaremoreoftenshortapico-coronally. Thesemaybeindicativeofalteredpassiveeruption,a conditionwhereadultteeththatarefullyeruptedhavea softtissuemarginpositionedmorecoronalthanthenorm. Thesesquareshapedteethtendtobeassociatedwith broadinterproximalseptaewhereinterproximalcraters aremorelikelytoform.Estheticsareaconsiderationwhen periodontaldiseaseispresentandresectiveperiodontal surgicaltreatmentisnotplannedunlessaprostheticcommitmentissecuredtoaddresscontingentissue,usuallyof anestheticnature.
Ovoidortriangularshapedanteriorteethcoronally presentwithacontactthatismorepointthanarea.These areassociatedwithcorrespondingthinnerinterproximal septae.
Asaresultinterproximalcratersarenotasprobableas withsquareshapedcrowns.Alsowithmoreovoidshaped teeth,thetissuebiotypeandthealveolustendtobethinner;softtissuerecessionsarethereforelikelywitheither periodontaldiseaseortreatment.
Mandibularanteriorteethhaverelativelysmallcontact points.Theseteeth,whicharetypicallyshortandsquarish haveathinnerosseousseptumandthinalveolarboneas wellasathinsofttissuebiotype;asaresult,theseteethare pronetorecessions.Mandibularanteriorteethhoweverare
notintheestheticzoneandthusmarginalsofttissuerecessionsmaynotbecritical(Glickman1953).
DevelopmentalAnteriorGrooves
Maxillaryincisorswillsometimespresentwithafaciogingivaldevelopmentalgroove.
Althoughthisconditionismorefrequentlyfoundonthe palatalsurfaceofmaxillaryincisors,ithassometimesbeen observedonthefacialaspectoftheseteeth.Theseusually presentasanarrowdevelopmentalgroovethatcoursesover thecingulumareafromapointcoronally.
Thegrooveitselfisanatomicallypronetolocalizedperiodontalbreakdown.Prognosisandtreatmentalternatives dependlargelyontheseverityandthegeometry,thenumberofbonywallsforexample,ofthelesionassociatedwith theanatomicalgroove.
Canineshavebulbousprominentrootsbothmandibular andmaxillary.Asaresultthealveolarboneisthinandthe biotypeassociatedwiththeseisrelativelythinalveolusand softtissuebiotype.Thesefactshaveanimpactoftreatment approachandshouldbeaddressedwithcautionastissue manipulationmayresultinrecessionsfromfenestrations anddehiscencelikelytobepresentwithathinbuccalwall. Conebeamimagerymaybeusefulinarrivingatthecorrectdiagnosis(LeeandLee1968;EverettandKramer1972; Kogon1986;Avitaletal.1988).
Premolars
Premolarsarerelativelysmallteethcoronallyandmay deceivinglyappear,perhapsasaresultoftheirrelativesize coronallytobesinglerooted.
Themaxillaryfirstpremolaristheclassicexampleas towhythatisnotthecase.Inthemajorityofcases,the firstpremolarisbifurcated,hastworootsassociatedwitha shortroottrunkor,intheleast,adeepmesialgroove.With thatinmind,assumptionsshouldnotbemaderegarding theanatomyofpremolarsrathertheyshouldbelookedat individuallywithnopreconceivednotion(Dababnehand Rodan2013).
Forthepurposeofdiagnosis,prognosis,andtreatment, furcationinvolvementshavebeenclassifiedandcategorizedaccordingtheirdegreeofseverityitselfameasureof theclinicalpenetrabilityofacalibratedperiodontalprobe.
Forthemostpartitisthehorizontalinvolvementthat hasbeenusedasameasureofprognosisandtreatment potential.Inoneparticularpublicationhowevertheverticalcomponentofthefurcationinvolvementwasaddressed intermsofseverityandpotentialfortreatment.Againin subsequentchapters,theissueoffurcationinvolvement willberevisitedasitisrelatedtoperiodontaldisease,
prognosis,andtreatmentalternatives(Hampetal.1975; TarnowandFletcher1984).
TheRootTrunk
Theroottrunkisessentiallyameasureofthedistance betweentheCEJtotheanatomicalroofofafurcation area.Itisalsoanestimateoftheanatomicalpotentialof afurcatedmultirootedtoothtoperiodontalbreakdown. Ashortroottrunkismoresusceptibletoafurcation involvementthanalongroottrunk;ineffect,thelatter providesmoreleewayinthefaceofperiodontalbreakdown.Whenatoothwithalongroottrunkisaffected withafurcationinvolvement,thatisindicativeofasevere periodontalconditionandanunfavorableprognosis.Once ananatomicalfurcationbecomesclinicallydetectable,this representsasignificantprognosisdownturnforthegiven tooth.Treatmentoptionsandtreatmentoutcomesare,as wewillseeinnsubsequentchaptersofthisbook,severely compromisedandwilldependastheliteraturesupportsit, ontheseverityofthelesionGargulio(1961).
MaxillaryFirstMolars
Asisthecaseingeneralformolarteeth,theiranatomyhas beenreportedandisdescribedintermsofthefirstmolar. Thisincludesthefirstmaxillarymolar.
Thefirstmaxillarymolartypicallyhasthreeroots,a mesiobuccal,adistobuccal,andapalatal.
Assuch,threeanatomicalfurcationsarepresent:abuccal,amesial,andadistal.
Iftheroottrunkofthemaxillaryfirstmolarismeasured fromtheCEJtotheroofofeachanatomicalfurcation,the literatureindicatesthatthebuccalroottrunkistheshortest followedbythemesialandthedistal,respectively.One shouldnotehoweverthatthefurcationonthebuccalis midwayfrommesialtodistal;thedistalfurcationisdirectly belowthecontactareasomidwaybucco-palatally,whereas themesialfurcationisslightlyoffcenter.Theseallhave significantimplicationswithrespectthesusceptibilityto periodontaldiseaseaswellastreatmentimplications.
Thesurfaceareaofeachofthethreemaxillaryfirstmolar rootshasbeenreportedwiththemesiobuccal,thepalatal, andthedistobuccalrootsusuallyinthatorderofdecreasingsize.
Aswithanyfurcatedormultirootedteethintraradicularrootconcavitiesarepresentwithmaxillarymolars. Becauseofthethreerootshereasopposedtothetworoots formandibularmolars,furcationinvolvementstendto beunidirectionalformandibularmolars.Formaxillary molarshowever,thepresenceofthreefurcationsmeans thatthesecanbeaffectedinternallyratherthansimply
fromthefurcationentrance.Thisaddstothepotentialon prognosisandtheabilitytotreatormaintaintheseareas. Oneshouldnotethatrootanatomyshouldbeseennot onlyasitrelatestoeachindividualtoothinisolationbut alsowithrespecttotheirrelativepositioninthearch.For example,themaxillaryfirstmolaroftenpresentswithadistobuccalrootthatanglesdistallyandbuccally.Thatmay leadtoathinalveolarbuccalhousingwhereafenestration ordehiscencearetobeconsidered.Alsothedistaldivergenceofthedistobuccalrootoftenresultsinathininterdentalseptumwiththeadjacentsecondmolar.Thishas significantimplicationsintermsofdiseaseprogressionand treatmentalternatives.Suchanatomicalrelationshipsmay potentiallyfoundanywhereinthearch(Hermanetal.1983; GherandDunlap1985;Roussa1998).
MandibularFirstMolars
Firstmolarsrepresenttheclassicanatomyformandibular molarswithvariationsexpectedforsecondmolarsandparticularlythirdmolars.
Themandibularfirstmolartypicallyhastworoots,a mesialandabuccal,withtwocorrespondinganatomicalfurcations,abuccalandalingual.Theroottrunk, measuredfromtheCEJtotheroofofthefurcation,is shorteronthebuccalthenonthelingualthenonthe buccal.Roottrunklengthhasimplicationsbothinterms ofprognosisandtreatment.Whenfurcationinvolvements arediagnosedasopposedtoshorterroottrunk,thatis indicativeofmorelossofattachmentandthereforeamore unfavorableprognosisintermsoftreatment.Ashorter furcationhowevercanbemoreofapotentialchallenge withrespectivetoanytypeofresectiveosseoussurgery wheretheanatomicalfurcalentranceisclosertotheCEJ apicoronally.Thisconstitutesaphysicallimittotheapical positioningofthealveolarmargin.Thiswouldincludea crownlengtheningforexamplewheretheestablishmentof thebiologicwidthmaybetheintendedobjectivebutwhere thelengthoftheroottrunkmayrepresentalimitingfactor.
Thefurcalentranceisusuallywideronthebuccalthan onthelingualalthoughtheliteratureindicatesthatin mostinstancesthefurcalentranceisnarrowerindiameter theninstrumentsusedfordebridement.Bothrootsofthe mandibularmolarareusuallykidneyshapedinahorizontalcrosswiththeinterproximalandintraradicularroot surfacesbeingmoreconcaveonthemesialthenthedistal root.Becausebothrootsareconcaveonthefurcalaspect, thisaccessfordebridementischallengingendeavor.Also thefactthemesialrootismorekidneyshapedhasoften ledclinicianstofavorthedistalrootoverthemesialroot inrootresectionproceduresbecauseitiscomprehensively moretreatableperiodontallyandrestoratively.Insome
instancesandwithgoodjudgement,rootsurfacesmaybe reshapedwithfinediamondstomodifytheiranatomytoa moretreatableormaintainableone.
Oneadditionalimportantaspectofintrafurcalroot anatomyistheintermediatebifurcationalridge,which runsinamesiodistaldirection.Itspositionwithinthe furcationcanpotentiallyinterferewithanaccurateclinical estimateofagivenfurcationinvolvement(Everettetal. 1958;Bower1979a,b;GherandVernino1980).
CervicalEnamelProjections(CEPs)
CEPsmaybedescribedasfingerlikeextensionsofenamel fromthecoronalportionofthetoothatvariousdepths beyondtheCEJ.BecausetheyareenamelintheircompositiontheirsofttissueinterfaceisnotaCTattachment butalongJE.Assuchtheyareoftenthefocusoflocalized periodontalbreakdown.CEPsareclassifiedaccordingtheir proximitytothefurcationarea,themostseverebeingone thatisactuallywithinafurcation.
References
Avital,K.,Tal,H.,Yechenskhy,N.,andMazei,O. (1988).Faciallingualgrooves. J.Periodontol. 59: 615–617.
Bower,R.C.(1979a).Furcationmorphologyrelativeto periodontaltreatment.Furcationrootsurfaceanatomy. J.Periodontol. 50:366–374.
Bower,R.C.(1979b).Furcationmorphologyrelativeto periodontaltreatmentfurcationentrancearchitecture. J.Periodontol. 50:23–27.
Bowers,G.M.(1963).Astudyofthewidthoftheattached gingiva. J.Periodontol. 34:201–209.
Dababneh,R.andRodan,R.(2013).Anatomicallandmarksof maxillarybifurcatedfirstpremolarandtheirinfluenceon periodontaldiseaseandtreatment. J.Int.Acad.Periodontol. 15:8–15.
DeRouck,T.,Eghbali,R.,Collys,K.etal.(2009).Thegingival biotyperevisited:transparencyoftheperiodontalprobe throughthegingivalmarginasamethodtodiscriminate thinfromthickgingiva. J.Clin.Periodontol. 36(5): 428–433.
Everett,F.G.andKramer,G.M.(1972).TheDistoLingala Grooveinthemaxillarylateralincisors.aperiodontal hazard. J.Periodontol. 43:352–361.
Everett,F.G.,Jump,E.B.,Holder,T.D.,andWilliams,G.C. (1958).Theintermediatebifurcationalridge:astudyofthe morphologyofthebifurcationofthelowerfirstmolars. J.Dent.Res. 37:162–169.
IntermediateCEPsarefoundmostcommonlyonthe buccalaspectofmandibularsecondmolarsmostlyasclass IIprojections.
Cementiclesandenamelpearlsareusuallysmallisolated globulesmadeofcementumorenamelrespectively.They canbedetectedusuallywithinthebodyofthePDLandare oflittleknownsignificance.Accessorycanalshavebeen describedcoursinglaterallytotheperiodontalligament. Thepotentialfortheseaspathwaysforcrosscontaminationisnotclearfromtheavailableliterature(Swanand Hurt1976;MastersandHoskins1984;YouandTsai1987; MoskowandCanut1990).
Itmaybeimportanttonotethefollowingasfarthe enamelrelatestothecementumattheCEJ:sixtypercent ofthecementumandenameloverlap;thirtypercentform abuttjoint;tenpercentareseparatedbyagap(Gutman 1978).
Fu,Jia-Hui,Chu-YuanYeh,Hsun-LiangChan,etal. Tissuebiotypeanditsrelationtotheunderlyingbone morphology. J.Periodontol. 2010;81(4):569–574.
Gargiulo,A.W.,Wentz,F.M.,andOrban,B.(1961). Dimensionsandrelationsofthedentogingivaljunctionin humans. J.Periodontol. 32:261–267.
Gargulio,A.W.(1961).Dimensionsandrelationsofthe dentogingivaljunctioninhumans. J.Periodontol. 32: 261–267.
Gher,M.E.andDunlap,R.M.(1985).Linearvariationsofthe rootsurfaceofthemaxillaryfirstmolar. J.Periodontol. 56: 39–43.
Gher,M.E.andVernino,A.R.(1980).Clinicalsignificancein thepathogenesisandtreatmentofperiodontaldisease. J.Am.Dent.Assoc. 101(4):6227–6263.
Glickman,I.(1953). ClinicalPeriodontology:ThePeriodontum inHealthandDisease:DiagnosisandTreatmentof PeriodontalDiseaseinthePracticeofGeneralDentistry Philadelphia:Saunders. Goaslind,G.D.,Robertson,P.B.,Mahan,C.J.etal.(1977). Thicknessoffacialgingiva. J.Periodontol. 48:768–771. Gutman,J.L.(1978).Prevalence,location,andpatencyof accessorycanalsinthefurcationregionoffthepermanent molars. J.Periodontol. 49:21–26.
Hamp,S.E.,Nyman,S.,andLindhe,J.(1975).Periodontal treatmentofthemultirootedteeth.Resultsafterfiveyears. J.Clin.Periodontol. 2:126–135.