Pathology at a Glance, 2e (Sep 7, 2021)_(1119472458)_(Wiley-Blackwell) 2nd Edition Finlayson
Visit to download the full and correct content document: https://ebookmass.com/product/pathology-at-a-glance-2e-sep-7-2021_1119472458_ wiley-blackwell-2nd-edition-finlayson/
More products digital (pdf, epub, mobi) instant download maybe you interests ...
Clinical Nursing Skills at a Glance (At a Glance (Nursing and Healthcare)) (Nov 8, 2021)_(1119035902)_(Wiley-Blackwell) 1st Edition Fordham-Clarke
https://ebookmass.com/product/clinical-nursing-skills-at-aglance-at-a-glance-nursing-and-healthcarenov-8-2021_1119035902_wiley-blackwell-1st-edition-fordham-clarke/
Independent and Supplementary Prescribing At a Glance (At a Glance (Nursing and Healthcare)) (Nov 14, 2022)_(111983791X)_(Wiley-Blackwell) 1st Edition Barry Hill
https://ebookmass.com/product/independent-and-supplementaryprescribing-at-a-glance-at-a-glance-nursing-and-healthcarenov-14-2022_111983791x_wiley-blackwell-1st-edition-barry-hill/
Pain Medicine at a Glance 1st Edition Beth B. Hogans
https://ebookmass.com/product/pain-medicine-at-a-glance-1stedition-beth-b-hogans/
Flow Cytometry of Hematological Malignancies, 2e (Jun 8, 2021)_(1119611253)_(Wiley-Blackwell).pdf Claudio Ortolani
https://ebookmass.com/product/flow-cytometry-of-hematologicalmalignancies-2e-jun-8-2021_1119611253_wiley-blackwell-pdfclaudio-ortolani/
Clinical Pancreatology for Practising
Gastroenterologists and Surgeons, 2e (May 24, 2021)_(1119570077)_(Wiley-Blackwell) Juan Enrique Dominguez Muñoz
https://ebookmass.com/product/clinical-pancreatology-forpractising-gastroenterologists-andsurgeons-2e-may-24-2021_1119570077_wiley-blackwell-juan-enriquedominguez-munoz/
ABC of Clinical Reasoning (ABC Series), 2e (Dec 19, 2022)_(1119871514)_(Wiley-Blackwell) 2nd Edition Nicola Cooper
https://ebookmass.com/product/abc-of-clinical-reasoning-abcseries-2e-dec-19-2022_1119871514_wiley-blackwell-2nd-editionnicola-cooper/
Pulmonary Pathology 2nd Edition Dani S. Zander
https://ebookmass.com/product/pulmonary-pathology-2nd-editiondani-s-zander/
Transplant Pathology 2nd Edition Anthony Chang
https://ebookmass.com/product/transplant-pathology-2nd-editionanthony-chang/
Chronic Total Occlusions-A Guide to Recanalization, 3e (Nov 29, 2023)_(1119517273)_(Wiley-Blackwell) Ron Waksman
https://ebookmass.com/product/chronic-total-occlusions-a-guideto-recanalization-3e-nov-29-2023_1119517273_wiley-blackwell-ronwaksman/
al a Glance Second
PathologyataGlance Pathology ataGlance SecondEdition BarryNewellBSc,MBBS,MRCP,FRCPath
CellularPathologyDepartment
StGeorge’sHospitalMedicalSchool London,UK
AsmaZ.FaruqiMBBS,FRCPath
DepartmentofCellularPathology
BartsHealthNHSTrust London,UK
CarolineFinlaysonMBBS,FRCPath
CellularPathologyDepartment(retired)
StGeorge’sHospitalMedicalSchool London,UK
Thiseditionfirstpublished2022
©2022JohnWiley&SonsLtd
EditionHistory
JohnWiley&SonsLtd(1e,2009)
Allrightsreserved.Nopartofthispublicationmaybereproduced,storedinaretrievalsystem, ortransmitted,inanyformorbyanymeans,electronic,mechanical,photocopying,recording orotherwise,exceptaspermittedbylaw.Adviceonhowtoobtainpermissiontoreusematerial fromthistitleisavailableathttp://www.wiley.com/go/permissions.
TherightofBarryNewell,AsmaZ.FaruqiandCarolineFinlaysontobeidentifiedasthe authorsofthisworkhasbeenassertedinaccordancewithlaw.
RegisteredOffices
JohnWiley&Sons,Inc.,111RiverStreet,Hoboken,NJ07030,USA
JohnWiley&SonsLtd,TheAtrium,SouthernGate,Chichester,WestSussex,PO198SQ,UK
EditorialOffice
9600GarsingtonRoad,Oxford,OX42DQ,UK
Fordetailsofourglobaleditorialoffices,customerservices,andmoreinformationaboutWiley productsvisitusatwww.wiley.com
Wileyalsopublishesitsbooksinavarietyofelectronicformatsandbyprint-on-demand.Some contentthatappearsinstandardprintversionsofthisbookmaynotbeavailableinother formats.
LimitofLiability/DisclaimerofWarranty
Thecontentsofthisworkareintendedtofurthergeneralscientificresearch,understanding,and discussiononlyandarenotintendedandshouldnotberelieduponasrecommendingor promotingscientificmethod,diagnosis,ortreatmentbyphysiciansforanyparticularpatient.In viewofongoingresearch,equipmentmodifications,changesingovernmentalregulations,and theconstantflowofinformationrelatingtotheuseofmedicines,equipment,anddevices,the readerisurgedtoreviewandevaluatetheinformationprovidedinthepackageinsertor instructionsforeachmedicine,equipment,ordevicefor,amongotherthings,anychangesinthe instructionsorindicationofusageandforaddedwarningsandprecautions.Whilethepublisher andauthorshaveusedtheirbesteffortsinpreparingthiswork,theymakenorepresentationsor warrantieswithrespecttotheaccuracyorcompletenessofthecontentsofthisworkand specificallydisclaimallwarranties,includingwithoutlimitationanyimpliedwarrantiesof merchantabilityorfitnessforaparticularpurpose.Nowarrantymaybecreatedorextendedby salesrepresentatives,writtensalesmaterialsorpromotionalstatementsforthiswork.Thefact thatanorganization,website,orproductisreferredtointhisworkasacitationand/orpotential sourceoffurtherinformationdoesnotmeanthatthepublisherandauthorsendorsethe informationorservicestheorganization,website,orproductmayprovideorrecommendations itmaymake.Thisworkissoldwiththeunderstandingthatthepublisherisnotengagedin renderingprofessionalservices.Theadviceandstrategiescontainedhereinmaynotbesuitable foryoursituation.Youshouldconsultwithaspecialistwhereappropriate.Further,readers shouldbeawarethatwebsiteslistedinthisworkmayhavechangedordisappearedbetween whenthisworkwaswrittenandwhenitisread.Neitherthepublishernorauthorsshallbeliable foranylossofprofitoranyothercommercialdamages,includingbutnotlimitedtospecial, incidental,consequential,orotherdamages.
LibraryofCongressCataloging-in-PublicationDataappliedfor PBISBN:9781119472452
CoverDesign:Wiley
CoverImage:©AsmaFaruqi
Setin9/11.5ptTimesNewRomanMTStdbyStraive,Chennai,India
10987654321
Wededicatethisbooktoourlovingandsupportivefamilies.
Contents Preface, 8
Abbreviations, 9
Introduction
1Thenormalhumancell, 14
2Fluiddynamics, 18
Tissuedamage
3Tissuetypesandtheeffectoftissuedamage, 22
4Celldeath, 26
5Harmfulagentsintheenvironment, 28
6Theeffectsoftobacco,alcoholandotherdrugs, 32
7Nutritionaldisorders, 36
Inflammationandimmunity
8Thebody’snaturaldefences, 40
9Bcellsandimmunoglobulins, 44
10TcellsandtheTCR, 46
11Themajorhistocompatibilitycomplex, 50
12Primaryandsecondarylymphoidorgansandthe monocyte–macrophage(reticuloendothelial)system, 52
13Acuteinflammation, 56
14Chronicinflammation, 60
15Woundhealingandrepair, 62
16Infectionandimmunodeficiency, 64
17Shock, 68
18Toleranceandautoimmunedisease, 72
19Hypersensitivityreactions, 76
20Overviewofinflammationandimmunity, 80
Genetics
21Celldivision, 84
22Geneticdisease, 86
Neoplasia
23Disorderedcellgrowth, 92
24Basicconceptsinneoplasia, 96
25Tumorigenesisandoncogenesis, 100
26Oncogenesandtumoursuppressorgenes, 102
27Commoncarcinomahistologicalsubtypes, 106
28Tumourprognosisandtreatment, 108
Methodsinhistocytopathology
29Basictechniquesinhistopathology, 112
30Cytopathology, 116
31Molecularpathology, 118
Multisystemsdisease
32Sarcoidosisandsyphilis, 122
33Wilson’sdiseaseandhaemochromatosis, 124
34Systemicvasculitis, 126
Cardiovasculardisease
35Normalbloodvesselsandtypesofaneurysm, 130
36Congenitalheartdisease, 134
37Systemichypertension, 136
38Atherosclerosis, 138
39Coronaryheartdisease, 142
40Thrombosis, 146
41Embolismanddisseminatedintravascularcoagulation, 150
42Cardiacvalvulardisease, 154
43Myocardialandpericardialdisease, 156
Respiratorydisease
44Pulmonaryvasculardisorders, 160
45Pneumonia, 162
46Bronchiectasis, 164
47Tuberculosis, 166
48Chronicobstructivepulmonarydisease, 170
49Fibrosingalveolitis, 172
50Primarylungcarcinoma, 174
51Othertumoursofthelungandpleura, 176
Gastrointestinaltractdisease
52Malabsorption, 180
53Pepticulcerationand Helicobacterpylori, 184
54Oesophagealdisease, 188
55Tumoursofthestomachandsmallintestine, 192
56Mechanicaldiseaseofthegastrointestinaltract, 196
57Inflammatoryboweldisease:ulcerativecolitisandCrohn’s disease, 198
58Colorectalpolyps,colorectalcancerandanalcarcinoma, 202
Hepaticandpancreaticobiliarydisease
59Normalliverandtheeffectsofliverdamage, 208
60Jaundice,gallstonesandcarcinomaofthegallbladder, 210
61Fattyliverdisease:alcoholicandnon-alcoholic, 212
62Autoimmuneliverdisease:AIH,PBC,PSC, 216
63Viralhepatitis, 220
64Cirrhosis, 224
65Acuteandchronicpancreatitis, 228
66Tumoursoftheliver,biliarytreeandpancreas, 232
Genitourinarytractdisease
67Congenitalandinheritedabnormalitiesofthekidneyand urinarytract, 236
68Thenephronandrenalaspectsofhypertension, 240
69Glomerulonephritis, 242
70Importanttypesofglomerulonephritis, 244
71Tubulointerstitialdiseases, 248
72Renalneoplasms, 252
73Bladdertumours, 254
74Testicularcancer, 256
75Prostaticdisease, 258
Gynaecologicalandobstetricdisease
76Vulvalandvaginalpathology, 262
77Cervicalcancer, 266
78Benignuterineconditions, 270
79Uterinemalignancies, 272
80Ovarianneoplasia:partone, 274
81Ovarianneoplasia:parttwo, 278
82Obstetricpathology, 280
83Paediatrictumours, 284
Nervoussystemdisease
84Cerebrovascularaccidents, 288
85Cerebrovascularaccidentsyndromes, 290
86Raisedintracranialpressure, 292
87Traumaticinjuryandintracranialhaemorrhage, 294
88Centralnervoussystemtumours, 296
89Infectionsofthenervoussystem, 298
90Movementdisorders, 300
91Acquireddisordersofmyelination, 304
92Dementia, 306
Endocrinedisease
93Pituitarypathology, 310
94Non-neoplasticpathologyofthethyroid, 312
95Thyroidneoplasms, 314
96Parathyroidglandpathology, 316
97Adrenalpathology, 318
98Diabetesmellitus, 320
Headandneckpathology
99Headandneckpathology, 324
Lymphoreticulardisease
100Assortedhaematologicalconditions, 328 101Leukaemia, 330 102Lymphoma, 332
103Myeloma, 336
104Myeloproliferativedisorders, 338
Musculoskeletaldisease
105Muscledisorders, 342
106Arthritis, 344
107Miscellaneousnon-neoplasticosteoarticularpathology, 348 108Bonetumours, 352
Skindisease
109Inflammatorydermatoses, 356
110Benignskintumours, 358
111Malignantskintumours, 360
Breastdisease
112Benignbreastdisease, 364 113Breastcarcinoma, 366
Casestudiesandquestions, 368 Answers, 373 Glossary, 378 Referenceranges, 380 Index, 381
Preface Wehavegreatlyappreciatedthefeedbackandcommentsreceived regardingthefirsteditionof PathologyataGlance.Itishearteningtoknowthatthisguidetopathology,whichaimstohighlight thefundamentalaspectsofparticulartopicsinthemannerofa low-scaleroadmap,hasbeenusefultohealthcareprofessionalsat allstagesoftheircareers.
Pathologyisfundamentaltomedicine,andagoodcoreknowledgehelpsimmenselytounitetheapparentlydisparatecollections ofsigns,symptomsandfactsencounteredinthestudyofothermedicalandsurgicaldisciplines.
Students,facedwithlimitlesslayersofinformationindetailed textbooksandonlinelearningplatforms,foundthisbookgave abalancedoverviewandaframeworkontowhichinformation gleanedfromothersourcescouldbeadded.Doctorsfromhouse officertoconsultanthavethankedusforsimplifyingtheirstarting pointforthepreparationofpresentations. PathologyataGlance is alsoapopularrevisionaid.
Acknowledgements Weareindebtedtothosewhoseexpertisecontributedtothefirst editionandseveralpeoplewhokindlypointedouterrorsorareas
inwhichnewinformationhassupervened,inparticularDrJoe Houghton.
DrKateWheeler,ConsultantinPaediatricOncology,gaveus invaluablehelpwiththechapteronpaediatrictumoursinthesecondedition.MrColinJardine-Brown’smotivationalskillsand expertadvicearealsomuchappreciated(C.J.F.).
ThehelpgiveninthefirsteditionbyDrJenniferElse(renal overview),ProfessorNeilShepherd(Helicobacterpylori),DrDavid Bevan(haemostasis),ProfessorPhilipButcher(tuberculosis),ProfessorPeterMcCrorie(hypertension)andDrJonathanWilliams (breastdisease)continuestobegreatlyappreciatedinthesecond editionof PathologyataGlance
Ourthanksgoalsototheeditorialstafffortheirpatienceand encouragement.
BarryNewell
AsmaZ.Faruqi
CarolineFinlayson
Abbreviations ACalternatingcurrent
ACEangiotensin-convertingenzyme
ACSacutecoronarysyndromes
ACTHadrenocorticotrophichormone
ADHantidiuretichormone
ADPKDautosomaldominantpolycystickidneydisease
AFPalpha-fetoprotein
AIDSacquiredimmunedeficiencysyndrome
AIHautoimmunehepatitis
AINanalintraepithelialneoplasia;acuteinterstitial nephritis
ALDalcoholicliverdisease
ALLacutelymphoblasticleukaemia
ALPalkalinephosphatase
ALTalanineaminotransferase
AMIacutemyocardialinfarction
AMLacutemyeloblasticleukaemia
ANCAantineutrophilcytoplasmicantibody
APCadenomatouspolyposiscoli
APTTactivatedpartialthromboplastintime
ARDSadultrespiratorydistresssyndrome
ASHalcoholicsteatohepatitis
ASTaspartateaminotransferase
ATNacutetubularnecrosis
ATPadenosinetriphosphate
AVatrioventricular
BALbronchoalveolarlavage
BCCbasalcellcarcinoma
BCGbacilleCalmette–Guérin
BCRBcellreceptor
BEBarrett’soesophagus
BMIbodymassindex
CAcoronaryartery
cAMPcyclicadenosinemonophosphate
CARScompensatoryanti-inflammatoryresponsesyndrome
CBDcommonbileduct
CCAcholangiocarcinoma
CCKcholecystokinin
CDclusterofdifferentiation;coeliacdisease
CFcysticfibrosis
CFAcryptogenicfibrosingalveolitis
CFTRcysticfibrosistransmembraneconductanceregulator
CFUcolonyformingunit
CGINcervicalglandularintraepithelialneoplasia
CHDcoronaryheartdisease
CINcervicalintraepithelialneoplasia
CJDCreutzfeldt–Jakobdisease
CLLchroniclymphocyticleukaemia
CMLchronicmyeloidleukaemia
CMVcytomegalovirus
CNScentralnervoussystem
COcarbonmonoxide
COPDchronicobstructivepulmonarydisease
CRCcolorectalcarcinoma
CrDCrohn’sdisease
CRPC-reactiveprotein
CSFcerebrospinalfluid
CTcomputedtomography
CVAcerebrovascularaccident
DADdiffusealveolardamage
DAIdiffuseaxonalinjury
DAMPdamage-associatedmolecularpattern
DCdirectcurrent
DCCdeletedincoloncancer
DCISductalcarcinomainsitu
DICdisseminatedintravascularcoagulation
DIPdesquamativeinterstitialpneumonia
DMdiabetesmellitus
DNAdeoxyribonucleicacid
DPASdiastasePAS
DUduodenalpepticulcer
dVINdifferentiatedvulvalintraepithelialneoplasia
DVTdeepvenousthrombosis
EATCLenteropathy-associatedT-celllymphoma
EBUSendobronchialultrasound
EBVEpstein–Barrvirus
EGFepidermalgrowthfactor
EGFRepidermalgrowthfactorreceptor
ENaCepithelialsodiumchannel
ENTear,noseandthroat
ERendoplasmicreticulum
ERCPendoscopicretrogradecholangiopancreatography
ESRerythrocytesedimentationrate
ESSendometrialstromalsarcoma
ETendothelin
FAPfamilialadenomatouspolyposis
FDCfollicledendriticcell
FEV1 forcedexpiratoryvolumein1second
FFAfreefattyacid
FFPEformalin-fixed,paraffin-embedded
FGFfibroblastgrowthfactor
FNAfineneedleaspiration
FOBfaecaloccultblood(test)
FSHfollicle-stimulatinghormone
FVCforcedvitalcapacity
G6PDglucose-6-phosphatedehydrogenase
GABAgamma-aminobutyricacid
GALTgut-associatedlymphoidtissue
GBMglomerularbasementmembrane
GCgastriccancer
GDPguanosinediphosphate
GFDgluten-freediet
GFRglomerularfiltrationrate
GGTgamma-glutamyltransferase
GHgrowthhormone
GIgastrointestinal
GNglomerulonephritis
GORDgastro-oesophagealrefluxdisease
GPgeneralpractitioner
GTNglyceryltrinitrate
GTPguanosinetriphosphate
HAARThighlyactiveantiretroviraltherapy
HAVhepatitisAvirus
Hbhaemoglobin
HBcAghepatitisBcoreantigen
HBeAghepatitisBeantigen
HBOChereditarybreastandovariancancer(syndrome)
HBsAghepatitisBsurfaceantigen
HBVhepatitisBvirus
HCChepatocellularcarcinoma
HCGhumanchorionicgonadotrophin
HCVhepatitisCvirus
HDLhighdensitylipoprotein
HDVhepatitisDvirus
H&Ehaematoxylinandeosin
HEVhepatitisEvirus;highendothelialvenules
HGOChigh-gradeovarianserouscarcinoma
HIAAhydroxyindoleaceticacid
HIVhumanimmunodeficiencyvirus
HLAhumanleucocyteantigen
HNPCChereditarynon-polyposiscolorectalcarcinoma
H2 O2 hydrogenperoxide
HP Helicobacterpylori;hydrostaticpressure
HPVhumanpapillomavirus
HRSCHodgkin–Reed–Sternbergcell
HSILhigh-gradesquamousintraepitheliallesion hspheatshockprotein
5HTserotonin/5-hydroxytryptamine
IBDinflammatoryboweldisease
ICAMintercellularadhesionmolecule
IDCinvasiveductalcarcinoma
IFNinterferon
Igimmunoglobulin
IHCimmunohistochemistry
ILinterleukin
INRinternationalnormalisedratio
ISLNin-situlobularneoplasia
IUDintrauterinedevice
IVCinferiorvenacava
JGAjuxtaglomerularapparatus
LAKlymphokine-activatedkiller
LDHlactatedehydrogenase
LDLlowdensitylipoprotein
LHluteinisinghormone
LSILlow-gradesquamousintraepitheliallesion
MALTmucosa-associatedlymphoidtissue
MCHCmeancorpuscularhaemoglobinconcentration
MCVmeancorpuscularvolume
MENmultipleendocrineneoplasia
MGUSmonoclonalgammopathyofuncertainsignificance
MHCmajorhistocompatibilitycomplex;mean haemoglobinconcentration
MImyocardialinfarction
MMRmismatchrepair(enzymes)
MPDmyeloproliferativedisease
MPTP1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine
MRCPmagneticresonancecholangiopancreatography
mRNAmessengerRNA
MSImicrosatelliteinstability
NADPnicotinamide-adenine-dinucleotidephosphate
NADPHreducedNADP
NAFLDnon-alcoholicfattyliverdisease
NASHnon-alcoholicsteatohepatitis
NETneutrophilextracellulartrap
NHLnon-Hodgkinlymphoma
NKnaturalkiller(cell)
NLPHLnodularlymphocytepredominantHodgkin lymphoma
NMDA N-methyl-D-aspartate
NOnitricoxide
NOSnototherwisespecified
NSAIDnon-steroidalanti-inflammatorydrug
NSGCTnon-seminomatousgermcelltumour
NSTEMInon-ST-elevatedmyocardialinfarction
PAFplateletactivatingfactor
PAHpolycyclicaromatichydrocarbon
PAMPpathogen-associatedmolecularpattern
PANpolyarteritisnodosa
PASperiodicacid–Schiff
PBCprimarybiliarycholangitis
PEpulmonaryembolism
PEG-IFNpegylatedinterferon
PGEprostaglandinE
PHTportalhypertension
PKDpolycystickidneydisease
PMNpolymorphonuclearneutrophil
PNETprimitiveneuroectodermaltumour
POPplasmaoncoticpressure
PRRpatternrecognitionsensor
PSAprostate-specificantigen
PSCprimarysclerosingcholangitis
PTHparathyroidhormone
PVCpolyvinylchloride
RArheumatoidarthritis
RFrheumatoidfactor
RNAribonucleicacid
ROSreactiveoxygenspecies
SAsinoatrial
SAMEsyndromeofapparentmineralocorticoidexcess
SBPspontaneousbacterialperitonitis
SCCsquamouscellcarcinoma
SCFAshort-chainfattyacids
SCIDseverecombinedimmunodeficiency
SIADHsyndromeofinappropriateantidiuretichormone secretion
SIRSsystemicinflammatoryresponsesyndrome
SLEsystemiclupuserythematosus
SMAsuperiormesentericartery
SMCsmoothmusclecell
SRBCTsmallroundbluecelltumour
SSLsessileserratedlesion
STEMIST-elevatedmyocardialinfarction
T4thyroxine
TBtuberculosis
TcTcytotoxic(cell)
TCRTcellreceptor
T2DMtype2diabetesmellitus
TFtissuefactor
TDLUterminalductlobularunit
TGFtransforminggrowthfactor
ThThelper(cell)
TLRToll-likereceptor
TNFtumournecrosisfactor
TSAtraditionalserratedadenoma
TSGtumoursuppressorgene
TSHthyroid-stimulatinghormone
TTthrombintime
UCulcerativecolitis
UDCAursodeoxycholicacid
UIPusualinterstitialpneumonia
UTIurinarytractinfection
uVINusualvulvalintraepithelialneoplasia
VEGFvascularendothelialgrowthfactor
VLDLverylowdensitylipoprotein
VOCvolatileorganiccompound
VSDventricularseptaldefect
vWFvonWillebrandfactor
WCCwhitecellcount
WHOWorldHealthOrganisation
WHRwaist/hipratio
5YSRfive-yearsurvivalrate
Generalpathology Introduction • 1 Thenormalhumancell Overview of the structure of normal human cells
Controlling the intracellular environment: cell membrane and ion pumps
Phospholipid bilayer: hydrophilic ends on outer and inner aspects. Hydrophobic ends inside membrane, stabilised by cholesterol
Na/Cl pump
Calcium channel
Receiving signals
Cell surface receptors and second messengers
Intracellular transport, cell movement and mitosis
Centriole: spindle formation (cell division)
Cytoskeletal components: microtubules and filaments
Degradation/destruction
Lysosome
Peroxisome
Cell membrane: a phospholipid bilayer,containing ion channels and receptor molecules
Receptor binding site
Signalling molecules transmit signal to nucleus
Protein production and secretion
Nucleus
Ribosome and newly producedpeptide
Rough (with ribosomes) and smooth endoplasmic reticulum
Golgi apparatus: protein modification (folding and addition of carbohydrate)
Secretory vesicle containing protein/glycoprotein product
Proteosome: degrades defective protein
Energy production
Mitochondrion
Cytosol
Theimportantfunctionsofthecellare:manufactureofproteins forlocalordistantuse,energygeneration,functionsappropriateto tissuetypeandreplication.
Themainelementsarethenucleus,thecytoplasm(cytosol),the cytoskeletonandthesubcellularorganelles,allboundbymembranes.
Nucleus Thenuclearmembranecontainsporestopermitmetabolites,RNA andribosomalsubunitsinorout.Itcontains: •DNA,thenuclearchromatin,whichonlyformsabout20%ofthe nuclearmass.
•Nucleoli–ribosomalRNAsynthesisandribosomesubunit assembly.
•Nucleoprotein,e.g.syntheticenzymesforDNA,RNAandregulatoryproteins,allmadeinthecytoplasmandimportedintothe nucleus.
•Messenger,transferandribosomalRNAenrouteforthe cytoplasm.
Cytosol
Thenutritiousfluidmediumthatbathesandsupportsthe organelles,throughwhichthecytoskeletonramifies.Manyreactionstakeplacehere.
Cytoskeleton
•Microtubules:organellessuchassecretoryvesiclesorinternalised receptorscanbetransportedthroughthecellviathecytoskeleton.
•Microfilaments(actin,myosin):thesestabilisecellshapeandact ascontractileproteinsinmuscle.
•Intermediatefilaments,e.g.cytokeratin,desmin,neurofilament proteinsandglialfibrillaryacidicprotein(thetypesdifferbetween tissuesandallarestructural).
Organelles
Mitochondria
ThesearethemainATP/energy-generatingorganellesandhouse theKrebscycleandoxidativephosphorylation.Theyhavetheir ownssDNA(maternallyderived)whichcodesaminorityoftheir proteins.Aporousoutermembraneandfoldedinnermembraneare present.
Ribosomes
Nucleolus-producedribosomalsubunitsaggregateinthecytosol andattachtotheendoplasmicreticulumorlielooseinthecytosol, dependingonthedestinationoftheproteintobemade(freeribosomesmakeproteinsforinsidethecellitself).Ribosomestranslate RNAstrandsintoacorrectlyassembledaminoacidsequence(peptidemolecule).
Endoplasmicreticulum (ER)
TheERisanirregularmazeofmembrane-boundtubules,saccules andcisternswhichramifiesthroughthecell.
• RoughER isstuddedwithribosomes.Proteinsmadebytherough ERpassintotheroughERcisternaeandundergosecondaryfoldingandearlyglycosylationbeforebeingincorporatedintomembranesforexportfromthecell,receptormoleculesonthecell,or componentssuchaslysosomeswithinthecell.
• SmoothER:thereisafurtheradditionofcarbohydratemoieties toprotein,foldingtoachievetertiarystructure.
Golgi apparatus –seediagram.
Secretoryvesicles
Thesemembrane-boundpacketsaremovedviathecytoskeletonto fusewiththecellmembranetoexpeltheircontentsoutside.
Lysosomes
Theseareintracellularmembrane-boundvesicles,containing destructivechemicalsandenzymes,whichfusewithphagosomes toreleasetheircontentsintothephagolysosomeanddestroy pathogens.Lysosomesalsodegradeworn-outcellorganelles (autophagy).
Peroxisomes
Thesesmallmembrane-boundgranulescontainoxidativeenzymes whichmakehydrogenperoxideplusitsregulatorcatalase.
Proteasomes Theseidentifydefectiveproteinsanddegradethemintotheircomponentpeptidesandaminoacidsforreusebythecell.Portionsof broken-downproteinareboundbyMHCclassImoleculesanddisplayedonthecellsurfacetoTccells.
Centrosome Thiscontainsthetwolinkedcentrioles,fromwhichmicrotubules radiateintothecell.Thecentriolesduplicateandmigratetooppositeendsofthecellduringcelldivision,separatingtheduplicated chromosomes.
Membranes
Membranesarephospholipidbarrierssurroundingthecellitself andcertainorganelles.Theyisolateportionsofthecellandpermitseveral,oftenincompatible,metabolicprocessestotakeplace simultaneously.
Thecell membrane
Thisphospholipidbilayerinteractswiththeextracellularworldby assortedsurfacemolecules.Thecentreislipophilicandthesurfaces hydrophilic,withcholesterolasastabilising‘spacer’betweenthem. The‘rafttheory’suggeststhatintramembranestructurescanfloat andbecross-linkedaroundtheperimeterofthecell.
Membraneproteins:proteinsthatprojectthroughthemembrane outsidethecellusuallyhaveattachedcarbohydrates.Glycolipids arecarbohydratesattachedtothelipidmembraneandareimportantincellrecognition,cell–cellbondsandadsorbingmolecules. Sometissueshaveaprotectiveglycocalyx.
Transportthroughthecellmembrane:themainmechanismsareas follows.
•Passivediffusion(needsonlyaconcentrationgradient),e.g.lipids andlipid-solubleagentslikeethanol.
•Facilitateddiffusion:thebindingofamoleculetriggersaconformationalchangewhichmovesthemoleculeacrossthemembrane.
•Activetransport:againstaconcentrationgradienttomaintainionconcentrationswithinthecell,e.g.theNa+ /K+ -ATPase complex.
•Bulktransport: endocytosis, transcytosis and exocytosis.Endocytosisincludes receptor-mediatedendocytosis (ligandsorviral
particles)and phagocytosis (engulfingofparticles). Pinocytosis,the samplingofsmallquantitiesofextracellularfluid,isnotreceptor mediated.
Transmissionofmessagesacrossthecellmembrane
•Lipid-solubleagents(e.g.steroids)diffusedirectlyacrosscell membranes.
•Receptorbindingandactivationofsecondarymessengers: appliestoproteinmessengermolecules,whichbindtoaspecific
cellsurfacereceptor(ligand),resultinginactivetransportofthe moleculethroughthemembraneorthetriggeringofintracellular cascadereactions.
Neurotransmitters:thesearechemicalmessengersforneurones ormyocytesthatcauseanelectricalresponseinthetargetby receptor-mediatedopeningofanionchannel.
• 2 Fluiddynamics Lymphatic drainage
Lymph exits via efferent lymphatic B
Thoracic duct returns lymph to venous system
Compartmentalisation within the body
Plasma protein
Fluid and electrolytes
Lymph carries fluid, cells, complement and other particles, e.g. bacteria to the lymph node
Fenestrated lymphatic endothelium lines blind-ended tubes which collect interstitial fluid
Vascular compartment
Fluid moves freely between the vascular and interstitial compartments, via the permeable capillary bed
Protein is retained within the vascular compartment by its large size and negative charge
Cell
Low Ca2+
High K+
Cell Interstitial compartment
High H2O and Na+
Cellular compartment
Cell membranes tightly regulate their electrolyte contents using Na/K exchange and calcium pumps
Normal fluid movement
Arterial side: hydrostatic pressure (HP) forces plasma out of fenestrated capillary endothelium
HP
Pre-capillary sphincter under sympathetic controlCapillary bed
Post-capillary venule reacts to vasoactive mediators
Venous side: hydrostatic pressure low
Valve
Plasma protein exerts oncotic pressure (POP) on fluid to remain in or return to vessel
Transudate
Normal specific gravity of <1.015
Excess plasma fluid without protein
Fluid accumulates in tissues, exceeding capacity of lymphatics to drain it, causing ‘pitting’ oedema caused when:
The plasma oncotic pressure drops, e.g. decreased protein production by the liver in chronic liver disease, or protein loss via the kidneys in nephrotic syndrome
Plasma protein retained in vessels, fluid is pressed out of vessels into the interstitium Oedema occurs if lymphatic drainage cannot meet demand
Fluid, without cells or plasma proteins
The hydrostatic pressure increases, e.g. back-pressure due to congestive cardiac failure
Specific gravity > 1.015
Lymphatics collect surplus interstitial fluid
Excess plasma fluid with protein
Example: inflammation, vascular response to inflammatory mediators:
Constriction of post-capillary venules increases hydrostatic pressure
Endothelial cells contract, enlarging the space between cells
Both fluid and plasma proteins move out of capillaries into the interstitium
Loss of plasma proteins reduces the osmotic pull on fluid to return to the blood vessels
Increased quantities of fluid, plus any cells, complement proteins or micro-organisms enter the lymph, but drainage cannot meet demand and fluid remains in the interstitium
Exudate
Approximately70%ofthebodyiscomposedofwater.Waterprovidestheessenceofthefluidmediumforthetransportofcells, nutrientsandwasteproductsbetweenorgans,providessubstance forcellularcytosolandisthesolventinwhichnumerouschemical reactionsoccur.Disruptionsofthequantityofwaterinthebody anditsdistributioncanhaveseriousconsequences.
Discussionsoffluidbalancetendtorevolvearoundacompartmentalmodeloffluiddistribution.Threemaincompartmentsare described:theintracellular(66%),interstitial/intercellular(25%) andintravascular(7%).Afourthcompartmentofspecialisedfluids (2%)canalsobeconsideredandincludessecretionsofthegastrointestinal(GI)tract,peritonealandpleuralfluids,cerebrospinalfluid, synovialfluid,intraocularfluidandthevestibulocochlearfluids. Thefourthcompartmentisoftenamalgamatedintotheinterstitial.
Fluidmovementisdynamicbetweenallofthecompartmentsand tendstofollowpassiveosmoticandhydrostaticgradients,provided thatthemembraneseparatingthecompartmentsiswaterpermeable.Ifwatermovementbetweenbodycompartmentsisrequired, manipulationofthesegradientsistypicallythemethodbywhich thisisaccomplished.Forexample,thesecretionofsweatinvolves thepumpingofsodiumandchlorideionsintothelumenofthe sweatduct.Waterthenfollowspassivelythroughmembranepores andintercellularjunctions.
Electrolytes Electrolytesareoneofthemainclassesofsolutewithinbodywater. Thechiefintracellularcationispotassiumandtheprincipalextracellularcationissodium.Thisdifferentialdistributionofsodium andpotassiumismaintainedbytheNa+ /K+ -ATPasethatispresent oneffectivelyallcells.Itisthebasisfortheelectricalactivityof neurones,skeletalmuscleandcardiacmuscle.Alterationsinthe extracellularconcentrationofeitherpotassiumorsodiumcan destabilisetheelectricallyexcitablemembranesofthesecells,generatingaberrantelectricalactivitysuchasseizures,arrhythmiasor muscleweakness.
Electrolyteconcentrationsarealsovitalinmaintainingturgor withincells.Iftheosmolarityofextracellularfluidisdisturbed, waterwillmoveinoroutofcellsaccordingly,resultingincell swelling(andultimatelyrupture)orshrinkage.Sucharethepotentiallycatastrophiceffectsofthisinappropriatemovementofwater thatbodyosmolarityisextremelytightlyregulatedbytheantidiuretichormone(ADH)system.Inextremesituations,homeostaticmechanismswillstrivetopreservebloodosmolarity(which isinequilibriumwiththatoftheothercompartments)evenatthe expenseofelectrolytelevelsandotherparameters.
Bloodandbloodfiltration Thevascularcompartmentcontains70mLofbloodperkilogram bodyweight(hence4900mLfora70-kgman).Cellularconstituents (erythrocytes,leucocytesandplatelets)comprise40%ofthisvolume,whiletheremaining60%isplasma.Plasmaiswaterinwhich electrolytes,numeroustypesofproteinsandlipoproteinsaredissolved.Bloodservesasatransportmediumtodelivernutrientsto thetissuesandtoremovewasteproductsfromthem.Thismovementofnutrientsandmetabolitesoccursatthecapillarylevel.
Whenbloodreachesthecapillaries,fluidandelectrolytescan passeasilythroughthegapsbetweenendothelialcells,butcells andlargermolecules(proteins)cannot.Thismovementisbidirectionalandthedirectionthatdominatesisregulatedbythebalance betweenthehydrostaticpressure(HP)exertedbythebloodpressure generatedbytheheartandtransmittedthroughthevasculartree andtheplasmaoncoticpressure(POP)generatedbyplasmaproteins.TheHPdriveswaterfromthebloodintothetissueswhereas thePOPprovidesagradientthatdrawsfluidbackintotheblood fromtheextracellularspace.
Intheproximalcapillarybed,HPexceedsPOPandthereisa netmovementoffluidfromthebloodintotheextracellularspace. Theinterstitialfluidisinequilibriumwiththeintercellularfluid andthereisreadymovementofnutrientsandmetabolitesbetween thesetwocompartments.However,theHPfallsacrossthecapillary bedandonthedistalsideisoverpoweredbytheoncoticpressure, causinganetmovementoffluidanditsaccompanyingsolutesback intotheblood.Nevertheless,theactionofthePOPisnotcomplete andasmallquantityoffluidremainsintheextracellularspace.This islymphandishandledbythelymphaticdrainagesystem.
Lymphaticsystem Lymphaticvesselscommenceinthetissuesasblind-endedtubes linedbyfenestratedendothelium.Thelymphismassagedthrough progressivelylargerandmorevalve-bearing,muscularised(nonleaky)vesselstothethoracicduct,whichemptiesintothevenous systemviathesuperiorvenacava,returningthefluidtothecirculation.Enroute,lymphissievedthroughlymphnodesandthus lymphhasavitalroleinpresentingextracellularmaterialtothe immunesystem.
Transudates Atransudateisanabnormalaccumulationoffluidthathasalow concentrationofprotein(typicallydefinedaslessthanbloodalbumin).Transudatesmayoccurinnumerouslocations,includingthe pleuralandperitonealcavities,andariseforoneoftworeasons.
1 Increasedhydrostaticpressure,typicallybackpressurewithinthe venoussystemduetoinadequatecardiacfunction.Fluidaccumulatesintheextracellularcompartmentandyields‘pitting’oedema oftheskin.Pleuraleffusionsmayalsobeseen.
2 The plasmaoncoticpressuredrops duetoeitherdecreasedhepatic proteinsynthesis(asincirrhosis)orexcessiveproteinlossviathe kidneys(nephroticsyndrome).Aswellaspittingoedema,ascites andpleuraleffusionsarecommon.
Exudate Anexudateisanabnormalcollectionoffluidthathasahighprotein concentration,typicallygreaterthanplasmaalbumin.Exudatesare causedbyinflammatoryprocessesthatmarkedlyincreasetheleakinessofthecapillarybedsuchthatproteinsthatwouldnotnormally beabletoleavethecirculationarenowableto.Constrictionof post-capillaryvenulesraisesthehydrostaticpressureandalsocontributestoexudateformation.
Tissuedamage • 3 Tissuetypesandtheeffectoftissuedamage Tissue replacement by stem cells, e.g. colon
Epithelium
Mucosa with straight-sided crypts
Stem cell at crypt base divides to supply new cells for surface and self-renews
M. mucosae
Submucosa
M. propria
Subserosal fat
The effects of damage depends on the tissue type affected and the type of damaging agent
Labile cells
Constantly self-renewing, e.g. bone marrow derived cells, epithelium: generally have short lifespan, high turnover; are quick to regenerate following trauma. Liable to damage by radiation or chemotherapeutic drugs,which affect cells undergoing mitosis
Stable cells
Self-renew as required, from stem cells or mature cells. May divide in limited fashion. Long lifespan tissues, e.g. liver, regenerate effectively following injury if sufficient normal liver remains.
Fibroblast and endothelial cell proliferation is essential for healing and repair in many tissues
Permanent cells
Long lifespan, little or no capacity to self-renew, e.g. brain, cardiac muscle. Damage causes tissue loss: in the heart, scar tissue forms; in the brain the tissue liquefies
Cell types
Epithelium:
Covers surfaces, cells bind each other to form an impermeable barrier. Specialised to local needs
Neuroectoderm: Neurons, melanocytes and neuroendocrine cells
Connective (‘soft’) tissue:
Supporting tissues, e.g. fat, bone, fibrous tissue, nerve insulation, cartilage, muscle (smooth, striated, cardiac)
Endothelium lines vascular system
Haemopoeiticand lymphoreticular
Bone marrow-derived cells and their precursors. Mature cells are mobile, many circulate
Germ cells:
Haploid generative cells in testis and ovary
Placenta Trophoblast
Most damaging agents affect tissues directly, but watershed zone infarction can occur as an indirect consequence of diminished blood flow at the ‘watershed’ between zones supplied by end-arteries
The two main types of cell death, coagulative and liquefactive necrosis, and distinctive histological subtypes: fibrinoid, caseous and fat necrosis. The clinical observation of “gangrenous necrosis” refers to blackened, ischaemic extremities: dry gangrene is due to infarction (coagulative necrosis) and wet gangrene has superadded infection, causing liquefaction
Normal tissue:
Cells have nuclei and distinct cell outlines
Coagulative necrosis
Example, renal infarct: cell outline preserved but cell contents degenerate
Liquefactive necrosis
Necrotic material
liquefies, e.g. brain, abscess contents
Fibrinoid necrosis
Blood vessel destruction by eosinophilic ‘fibrinoid’ material, e.g. vasculitis.
Caseous necrosis
Tuberculosis –crumbly necrotic debris, combining coagulative and liquefactive features: granulomatous reaction
Fat necrosis
Follows trauma and forms hard nodule which can be mistaken for tumour (e.g. in breast)
Normaltissuetypes Epithelium
Epithelium,derivedfromembryonalectoderm*,linesthebody’s surfaces.Itconstantlyregeneratesandhealsquickly.Thethreemain epithelialsubtypesare:
1Squamous:functionsasabarrierandprotectsagainstfriction.
a. Stratifiedsquamous:coversskin,pharynx,tongue,oesophagus,anus,vagina,externalauditorycanal;keratinisationisonly normallyseenintheskin.
b. Simplesquamous:formsmesotheliumliningthepleuraland peritonealcavities.Pathologistsregardendotheliumasaseparate entityfromsimplesquamousepithelium(SeeNotebelow).
2Glandular:linesallsecretoryorgans.Itsfunctionsinclude:
a. Secretion:
•Non-specialised,e.g.mucin,totrapbacteriainthenoseor assistfoodtransitingut.
•Specialised,e.g.hormoneoracidsecretion(gastricparietal) orabsorption(gut,renaltubules).
b. Iontransfer:renaltubules.
c. Clearance:ciliatedbronchialcellsremoveinhaledparticles stuckinmucin(mucociliaryescalator).
3Urothelial(formerly‘transitional’):this‘pseudostratified’epitheliumlinestheurinarytract.Itcontains umbrella cellsthatmaintain theintegrityofthesurfaceonstretchingtoaccommodateurine.
Note: Mesothelialcells,thesingle-layedsimpleepitheliumlining thepleuralandperitonealcavities,arederivedfrommesoderm, butcontainkeratins.Endothelium(seelater)isoftendescribedby non-pathologistsasasimplesquamousepithelium,butendothelial cellsdonotcontainkeratinfibres,adefiningfeatureofepithelium (theyaresupportedbyvimentinfibres).Notethatsynovialcavities arenotlinedbyepithelialcells,butbytwocelltypes,derivedfrom fibroblastsandmacrophages.
Neuroectodermal-derivedtissue
Thisformsthecentralandperipheralnervoussystem.Scatteredneuroendocrinecellspopulatevariousepitheliaandsecrete site-specificsubstances,e.g.skinmelanocytes,guthormonesecretingcellsandinthebronchus(wheretheyarethoughttogive risetopulmonarysmallcellcarcinoma).
Connectivetissue
Thisformsstructuraltissues.
• Fat (adipo-)storeslipid,canregenerateandmaysecreteor respondtocytokines.Adipokinescandriveinflammation.
• Bone (osteo-)consistsmainlyofmatrix-containingsparseosteocytesandisconstantlyremodelledbyosteoblasts,whichlaydown matrix,andosteoclasts,whichresorbit,inresponsetophysical stressesandhormones(e.g.parathyroidhormoneorcalcitonin).It healsexcellently.
• Fibroustissue (fibro-),suchastendon,whichconsistsmainlyof acellularandavascularcollagenoustissueandhealspoorly.
• Cartilage (chondro-)consistsmainlyofavascularmatrix,in whichafewchondrocytesareembedded;ithealspoorly.
• Nervesheath (neurofibro-)thereareseveralnervesheathcomponents,whichmayundergobenignproliferation,e.g.afteramputation,orformmalignanttumours.MyelinismadebySchwanncells, whichcanformschwannomas.
• Smoothmuscle (leio-)formsthewallsofmedium-sizedandlarge bloodvesselsandlymphatics,theuterinemyometrium,thevaginal wallandthemuscularlayersoftheGI,respiratoryandurological tracts.Itcanregeneratebutoftenhealsbyscarring.
• Striatedmuscle ((rhabdo)myo-)formsvoluntarymuscle.Regenerationislimited.
• Cardiacmuscle:myocardiumonly;doesnotregenerate.
• Endothelium arisesfrom‘bloodislands’oftheembryonalmesoderm.Differenttypeslinethebloodvessels,lymphaticsandthe hepaticandsplenicsinusoids.Endotheliumreadilyregenerates.
Haemopoietic andlymphoreticulartissue Thesetissuesgeneratebloodcellsandformtheimmunesystem. TheyarediscussedinChapters8–12.
Germ cells
Thesearetheovarianandtesticularreproductivecells.Theyare constantlyproducedbythetestis;theovarycontainsafinitenumberfrombirth.
Proliferativeandregenerativecapacity • Labiletissues readilyregenerateandconstantlyproliferateinlife, e.g.theepitheliaoftheskin,gastrointestinaltract,bronchus.
• Stabletissues includetheliverandkidney,andcan,ifnecessary,regeneratebutusuallyshowonlyverylimitedcellturnover. Theliverhashugeregenerativecapacity:overhalfcanberemoved yettheremaindercanundergocompensatoryregeneration.Renal tubulesarequicktoregeneratefollowingdamagesuchastransient ischaemia.
• Permanenttissues showlittletonoregenerationsocelldeathcan becatastrophic(e.g.cardiacmyocytes,neurones).
Stemcells areprogenitorcellsthatcanpotentiallyformanytissue butrespondtolocalhormonesandcytokinestoyieldcellsappropriatetotheplaceinwhichtheyaregenerated.Stemcellsdivide toformacopyofthemselves(andarethusimmortal)plusapopulationof‘committed’progenitorcells.Thesedivideinto‘transit amplifyingcells’andafterseveralcelldivisionsyieldterminallydifferentiatedcellswhichdieoncetheirlifespanisover,tobereplaced byfurtherstemcellprogeny.
Cellreplacementintissueswithahighturnoverisbystemcells. Intissuessuchasliver,withalowcellturnover,replacementof individuallydamagedcellsisbydivisionofadjacentcells,butlarger amountsofhepatocytelossrequiresstemcellsforreplacement. Eachtissuehasacompartmentcontainingitsownstemcell.
Tissuenecrosis Necrosisisaformofunregulatedcelldeathwhichhasavarietyof causes,chieflyphysicaltrauma,infarction,infectionorchemicals. Theappearanceofnecrosisvariesaccordingtothestimulusandthe tissue.Themajortypesareasfollows.
• Coagulativenecrosis duetoischaemiaiscommonestandusually appearsasafirm,pale,wedge-shapedregionoftissuereflectingthe territorysuppliedbyanoccludedarteriole.Thecellsretaintheir shapebutlosetheirnucleiandareknownas‘ghostcells’.
• Liquefactivenecrosis typicallyaffectsthecentralnervoussystem (CNS),oftenafterastroke.Oncethedamagedtissuehasbeen clearedthereisnohealingandnoscar,andonlyacysticspace remains;themechanismisnotwellunderstood.Abscessesalso
showliquefactivenecrosis,duetoenzymicdigestionoftissuesby theinfectingorganism.
• Caseation isawhite,crumbly,cottagecheese-likeappearance foundintuberculosisandsomefungalinfections.Itisamixture ofcoagulativeandliquefactivenecrosis.
• Fatnecrosis:hard,brightyellownodulesoffatnecrosisoccur, possiblysecondarytotraumaandmaybecomecalcifiedandresembletumourclinically.Digestionoffatbypancreaticenzymeswith fatnecrosisandcalcificationiscommonlyseeninacuteandchronic pancreatitis.
Typesofinfarction Infarctionisnecrosisofatissueororganduetodisruptionofits bloodsupply.In arterial infarctionthereisinadequateflowinto theorgan.In venous infarctiontheoutflowisobstructed,preventingflowthroughtheorganandcausingcongestionandstagnation.Arterialinfarctionistypicallyduetoocclusionofthevessel byathrombusorembolus;externalcompressionisrare.Venous infarctionoftenreflectscompressionoftheveins,asoccursinstrangulationofahernia. Watershedzone infarctionsareillustrated opposite.
• 4 Celldeath Initiation of apoptosis may be via extrinsic or intrinsic pathways.
Caspases are central to apoptosis; so far 14 have been described
Effector caspases are enzymes which cleave proteins in membranes, the nucleus and the cytoskeleton and activate nuclear DNAase
Cytochrome-c release from mitochondrial membrane
Initiator caspases activate effectors
Mitochondrion
Anti-apoptosis
Bcl-2 blocks release of cytochrome-c, and may modulate Ca ion flux.
Bcl-xL stabilises the mitochondrial membrane and neutralises proapoptotic molecules by binding
Pro-apoptosis
Bad, Bax and Bim proteins activate apoptosis. They displace Bcl-2 and Bcl-xL
Bid, once activated, induces cytochrome-c release
Cascade of effector caspase activation
Extrinsic ‘death receptor’ pathway stimulated by cross-linking receptors, e.g. TNFR1, Fas. Example: TNF secretion by immune cells
Direct activation
Example: Granzyme B injected into cells by Tc cells through holes in membranes made by perforin
Intrinsic activation
Main pathway is by mitochondrial membrane release of cytochrome c and other pro-apoptotic molecules, influenced by Bcl-2 family members
Example: growth factor blockage/ withdrawal
Can be stimulated by autophagic or necrotic mechanisms which increase Ca++ levels in cytosol DNA damage via p53 stimulates caspases directly or through the synthesis of Bax and Bak
Fragments bud off the cell surface and express new ligands. The cell shrinks
Macrophages and some adjacent epithelial cells attach to the ligands and engulf the debris, digesting it in phagolysosomes.
There is no acute inflammation
Necrosis
Agents which cause necrosis fall into the following main categories:
Ischaemia, hypoxia or re-perfusion, e.g. myocardial infarction
Infection, e.g. bacterial, viral, fungal
Immune-mediated, e.g. cross-reacting antibodies
Physical agents, e.g. extreme heat or cold, electrocution, irradiation
Chemical agents, e.g. strong acid or alkali, drugs which bind DNA
Nutritional, e.g. folic acid/B12 deficiency
The generation of free radicals is a common effector pathway (oxidative stress occurs when there is more generation of reactive oxygen species (free radicals) than can be cleared by the available scavenging systems)
Surplus or worn-out material from intracellular protein production
Formation of autophagosome
Portion of cytoplasm enveloped in double lipid membrane Fusion with lysosome
Autophagolysosome
Storage of indigestible remnants
Degradation and recycling of protein and other elements
Na/K pump in the cell membrane fails, e.g. loss of ATP production by mitochondria. Lactic acid may accumulate
Na+ enters the cell, passively accompanied by water. The cell swells
Ca/Mg pump fails: excess cytosol Ca++ activates enzymes which deplete ATP
The membranes bleb and ribosomes dissociate from endoplasmic reticulum, cytoskeletal components clump
The situation is still reversible
Enzymes activated by Ca++ digest the cell membrane, cytoskeleton and the nuclear chromatin
The damage is irreversible
Various nuclear changes may occur: it may shrink and get darker (pyknosis), fade away (karyolysis) or fragment (karyorrhexis). Similar nuclear changes are seen in apoptosis, particularly karyorrhexis. Some claim that this appearance is unique to apoptosis but it is disputed
Release of cell contents stimulates acute inflammation. This adds to the damage by releasing further digestive enzymes and free radicals into the tissue
If proteolytic digestion predominates there is less inflammation and the result is coagulative necrosis
If hydrolytic enzyme digestion predominates, the tissue undergoes liquefaction
Inthelivingperson,celldeathoccursallthetimeandisoftena necessaryprocess.Thetwomechanismsthatproducecelldeathare apoptosisandnecrosis.Itisbecomingclearthattheseentitiesare notalwaysdistinct,butgeneralisationsaremadebelow.
Apoptosis Apoptosis,oftencalled‘programmedcelldeath’,occursduringembryologicaldevelopment,asnewtissuesareformedand remodelled,orinphysiologicalcyclessuchasthemenstrualcycle. Apoptosisischaracterisedbytheorderlybreakdownofcellular constituents,whicharepackagedintomembrane-boundvesicles andtaggedforcollectionbyphagocytes.Thisrequiresenergy.
Theinitiationofapoptosisisasfollows.
1 Bindingofa‘deathligand’(e.g.TNFR1orFas)onthecell surface,e.g.directbindingbyTcellsorNKcells,ortumournecrosis factor(TNF)secretionbyimmunecells.
2 Membranedisruptionbyperforin,thenintracellularinjectionof granzymeBbyacytotoxicTcell(Chapter10).
3 Releaseofpro-apoptoticproteins,e.g.cytochrome c,fromleaky mitochondrialmembranes,aprocesslargelyregulatedbypro-and anti-apoptoticproteinsoftheBcl-2family.
4 TP53,a‘gatekeeper’geneinthecellcycle.p53proteininstigates apoptosisifthereisafailuretorepairDNAdamage(Chapter26).
Oncestarted,apoptosisisgenerallyirreversible,involvingafinal commonpathwayofanintracellularcascadeofcaspases.Proteolyticcleavageofcellcontentsandwaterlosscausescellshrinkage. Fragmentsbudoff,envelopedbycellmembrane,whichexpresses newligands.Apoptosisdoesnotstimulateanacuteinflammatory response;instead,macrophagesandadjacentcellsbindthenewligandsandphagocytosethefragments.
Necrosis Thedeathofagroupofcellsduetoanoxiousstimulusisreferred toasnecrosis.Necrosisiscausedbymanyphysicalandchemical agents,amongstthemostcommonofwhichareischaemia,infectionanddrugs(e.g.chemotherapy).Necroticcellulardebrisstimulatesanacuteinflammatoryresponsewhichmayincreasethearea oftissuedamagedduetotheleakageoflysosomalenzymesfrom polymorphsandmacrophages.
Ithasbeensuggestedthatnecrosisiswhathappensaftercell death(i.e.irreversibledamage)andthatchangesuptothispoint, whichcanbereversed,shouldbeclassedascelldamage.Thepoint ofnoreturnisbestrecognisedwhenthereisalossofmembrane integrityandinfluxofcalciumintothecytosolfromtheinterstitial fluidorfromtheendoplasmicreticulum.
Factorsthatinfluencewhetherthedamageisreversibleinclude:
• Thedurationofthestimulus,e.g.ischaemiaduetocoronaryartery thrombosiswillcausemyocardialinfarction,butiftheocclusionis rapidlyclearedtheareaofcardiacmusclethatdieswillbereduced (Chapter36).Reperfusionmaycauseproblemsduetotherelease offreeradicalsinthereperfusedterritory.
• Thedoseofachemicalagent:whatcancausecelldeathinsome people,doesnotinothersduetogeneticpolymorphism(variation ininheritedgenesencodingtheliverenzymesthatmetabolisethe drugs).
• Thetissuetypeanditsmetabolicactivity:theneuronesofthebrain andcardiacmusclecellsarehighlymetabolicallyactive.Energyproductionfromglycolysisviaanaerobicpathwaysisavailableforliver
ormuscle(whichstorestarch)butproducestoxiclacticacidwithin thecell.Damagebeginswithinminutesinthebrain,butlimbstriatedmusclescanbedeprivedofoxygenforseveralhours.Cooling oftissuesreducestheirmetabolismandincreasessurvivaltime.
• Thestateofhealthoftheexistingtissue,e.g.ironoverloadin haemochromatosisrendersthelivermoresusceptibletodamageby othertoxins,likealcohol.
Autophagy Thebodyattemptstopreservecellsthroughtimesofadversity byundergoingautophagy,aparticulartypeofcellularadaptation commonlyseeninstarvationandalsoininfection.Itisalsoinitiated bygrowthfactordeprivation.
Portionsofcytoplasmareboundbymembranestoformavesicle (autophagosome),whichfuseswithalysosomeanditscontents, oncedegradedbyhydrolaseenzymes,arethenrecycled.Theprocess islikehibernationandcanbereversedoncetheleantimespass,but iftakentoextremesbecausethestimuluspersists,thecelldieseither byapoptosisornecrosis.
Pathologicalexamplesofdiseasesinwhichautophagyplays animportantroleincludeneurodegenerativediseasessuchas Alzheimer’s,Parkinson’sandHuntington’sdiseases.Muchinterest hasrecentlydevelopedintheroleplayedbyautophagyincancer.
Freeradicals Freeradicalsarehighlyreactiveanionswithanunpairedouter orbitalelectron.Theyreactwithinorganicororganicchemicalsto formfurtherfreeradicals.Importantexamplesare:
•Reactiveoxygenspecies(ROS):hydrogenperoxide(H2 O2 ),superoxideanionradical(O2 ⋅)andhydroxylradical(⋅OH).
•Nitricoxide(NO)madebyendothelium,macrophages,neurones andothercells.
Formation •Duringnormalcellularenergygenerationbyoxygenreduction andelectrontransfer.
•Killingofpathogensbyphagocytes:ROSarepreformedina membranecomplex.
•Unwantedby-productofintracellularoxidasereactions.
•Radiation(generateshydroxylandhydrogenfreeradicalsbyionisingwater).
•Toxicby-productofdrug/chemicalmetabolismbycellular enzymes,e.g.intheliver.
Harmfuleffects •Lipidmembranedamagebyperoxidation(affectsthecellmembraneandthemembranesoforganelles).
•Proteindamagebyaminoacidoxidation,cross-linkagesorproteinbreakdown,e.g.microtubuleaggregation.
•DNAdamagecancausemutationsandcancer.
Protection •NaturaldecaytooxygenandH2 O2 .
•Antioxidants,e.g.glutathioneandvitaminsA,CandE.
•Bindingofcopperandirontotransportproteins.
•ScavengingenzymesthatbreakdownH2 O2 andsuperoxide anion,e.g.catalase,superoxidedismutasesorglutathione peroxidase.
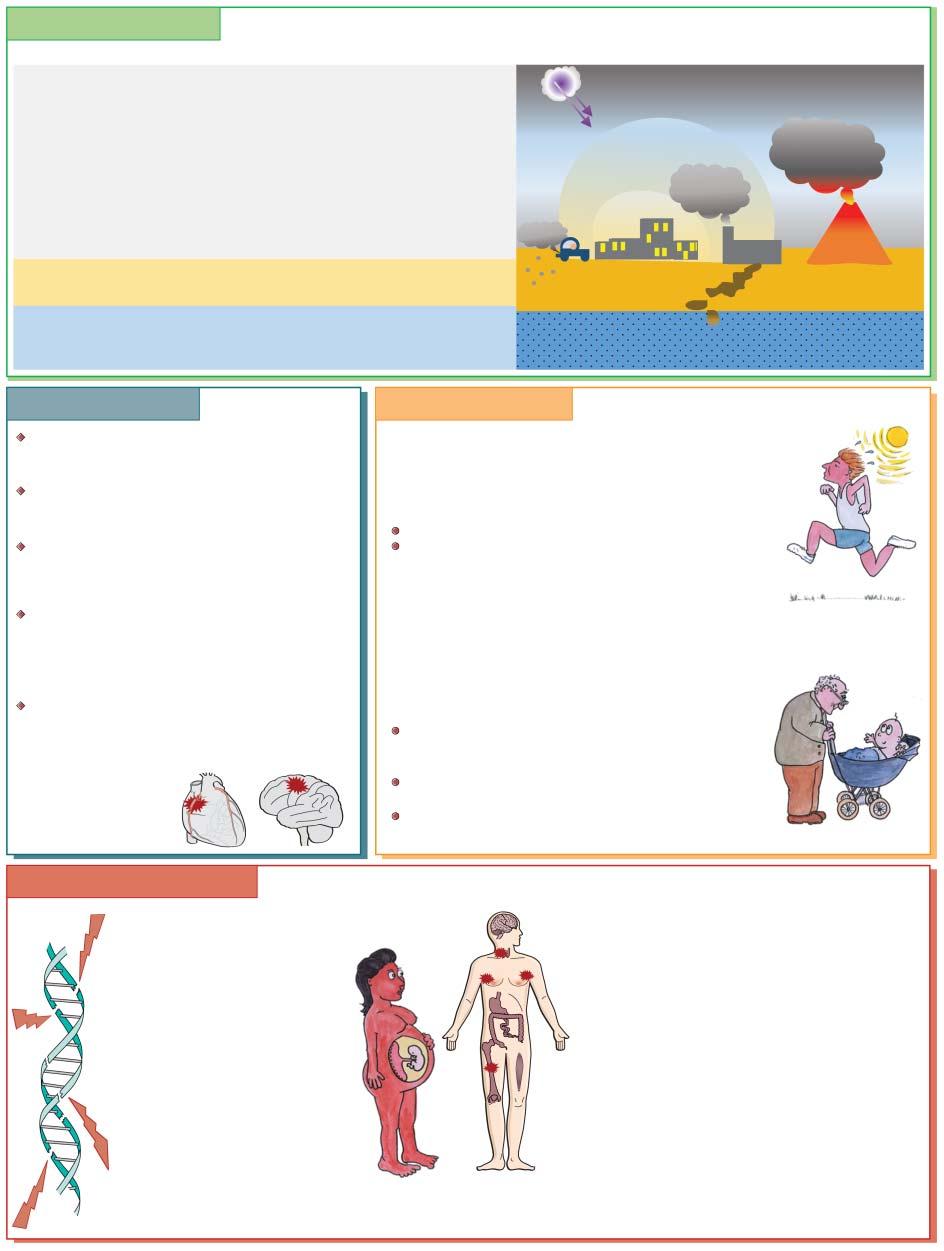
• 5 Harmfulagentsintheenvironment Environmental pollution AIR
Air pollution alone is estimated to cause >6 million deaths annually in the world, a number similar to tobacco smoking. The effects on humans of air pollution include: asthma, COPD, lung cancer, MI, stroke, neurodegenerative and skin disorders.
Increased UV light penetration via stratospheric ozone (O3) deficiencies
Particulate matter, small worst (PM10, PM2.5): e.g. smog, soot, tobacco smoke
Organisms: bacteria and their spores, viruses
Dust: “atmospheric, heavy or settling,” e.g. derived from industry, incineration of waste, natural phenomena such as volcanic eruption
Gases:eg CO2 /CO, sulphates, nitrous compounds, PAH , VOC.
Increased O3 at ground level
Heavy metals, e.g. lead
Noise pollution
Radioactive waste
LAND
Chemical/radioactive waste e.g. heavy metals, hydrocarbons or pesticides
WATER
Chemical waste, soil waste, air pollution washed into water by rain, alteration in organisms (e.g. algal bloom in sea), plastics. Radioactive waste
Cold-induced damageHeat-induced damage Hypothermia occurs when the core temperature is <35C. Frostbite is localised freezing of exposed peripheries, e.g. nose, fingers
The problems which affect resuscitation efforts are those of plasma volume depletion and alterations in ion concentration
A cold-induced diuresis increases plasma viscosity and the blood becomes hyper-coagulable, increasing the risk of myocardial infarction and stroke on resuscitation
Leakage of plasma occurs across damaged capillary endothelium. Hypovolaemia may cause shock if a patient is warmed suddenly, without careful monitoring and fluid and electrolyte correction
Plasma K+ levels rise because of the loss of integrity of the cellular Na+/K+ pump - this normally functions to keep intracellular K+ levels high and Na+ low, while the reverse is true in the extracellular fluid.
The high plasma K+ levels may cause cardiac arrhythmias
Radiation-associated disease Exogenous: high ambient temperatures and excessive exercise may cause fluid and electrolyte loss and dehydration
Treatment is by cooling and fluid and electrolyte replacement
Mixed exogenous/endogenous: high ambient temperatures and impaired heat-losing mechanisms cause heat stroke
Example: athletes exercising in extremely hot environments
Infants, children and the elderly, especially those taking medication such as diuretics or tranquilisers
Treatment is with cooling, fluid and electrolyte replacement –antipyretics are ineffective
Many patients develop lactic acidosis, hypocalcaemia, muscle fibre damage and myoglobinuria, which may damage renal tubules
Endogenous:
Infections cause fever due to the release of cytokines, e.g. IL-1 and TNF, which affect the temperature control centre in the hypothalamus
Example: the drenching sweats and high fevers seen in tuberculosis and some lymphoma patients (though why this is typically at night is not clear)
Febrile convulsions are common in children with high temperatures
An aberrant response to anaesthetic may cause ‘malignant hyperthermia’
Radiation effects Ionizing radiation causes DNA breakages and cross-linkage.
Rapidly dividing tissues (bone marrow, gut, skin, bronchus, urinary tract) are particularly susceptible
Effects vary depending on type (α, β particles or γ , X-rays), depth of penetration, dose and host factors
Therapeutic deep X-ray radiotherapy (DXT) works because tumour cells tend to divide more rapidly than normal tissue
Radiation effects are cumulative.
Delivering divided doses (fractionating) and converging on tumour from different angles, DXT to tumour is maximised, but normal tissue damage is minimised
Immediate : High doses (e.g. 2000 rads) cause convulsion, coma and death within 1 day
Acute/subacute (hours /days-weeks)
Cerebral oedema, diarrhoea, dehydration, septicaemia (from gut breakdown), bone marrow failure
Long-term (months/years/decades) effects.
Fibrosis: strictures of small bowel, pericardial fibrosis, interstitial fibrosis of lung or kidney, spinal cord damage.
Mutation: Cancers: carcinoma (e.g. breast or thyroid), bone marrow derived cells (e.g. leukaemia, lymphoma), soft tissue (sarcomas)
Pregnancy:
In utero exposure: may cause fetal growth/mental retardation, microcephaly or hydrocephaly.
Future pregnancies in survivors: no radiation effects found
Environmentalpollution Air,soilandwaterareallliabletocontamination(seediagram). Airpollutionisamajorcauseofmortalityandmorbiditydue toasthma,chronicobstructivepulmonarydisease(COPD),lung cancer,myocardialinfarction(MI),stroke,andneurodegenerative andskindisorders.Globally,morethan6millionannualdeathsare attributedtoairpollution.
Physicalagents Electrocution
ElectrocutionbylightningorcontactwithDCorACcurrentsfrom thedomesticelectricitysupplyoftencausescharringoftheskinat theentry(e.g.handorhead)andexit(e.g.foot)points.Thedamage isrelatedtothetypeofshockandtheresistanceofthetissue.Muscle tetanymayrenderthesubjectunabletoletgoofafaultyelectrical wireorsocket.Electricalcurrentsareconductedthroughthebody bestbyfluidswithhighioncontent,i.e.blood,nervesandtissue fluids.Inelectricallyresistanttissue,suchasfat,boneortendon,the heatgeneratedcancausesevereburnsandjointsareoftendamaged. CNSinjuryislikelyiftheheadisstruckbylightningforexample,or currentpassingacrossthebodymaycausecardiacarrhythmiasand suddendeath.Electrocutioncancauserespiratoryarrest,seizures andrhabdomyolysis.Therapeutically,aDCshockappliedtothe praecordiumtotreatventricularfibrillationduringcardiacarrest mayshocktheheartbackintosinusrhythm.
Extremes oftemperature
Cellularhomeostasisdependsontemperature-sensitiveenzyme reactionsandthemaintenanceofionconcentrationswithinafairly narrowrangeofnormalvalues.Thenormalcoretemperatureis maintainedbythehypothalamusandisregulatedbyinterleukin (IL)-1releasefrommacrophagesandlocalprostaglandinproduction.Heatisgeneratedbymuscleandmetabolicactivitywithinthe bodyandislostthroughtheskin,sweatandbreath.
Excessheat:Heatexhaustion(coretemperature37–40∘ Cwith dizziness,headache,thirst,malaiseandnausea)requiresrehydrationandcooling.Leftuntreateditmayprogresstoamedical emergency, heatstroke (coretemperature40–42∘ Cwithsevereconfusion,problemswithcardiacfunctionandrespiration);42.5∘ C isvirtuallyalwaysfatal.Thecausemaybeincreasedheatgeneration(e.g.exercise),aninabilitytoloseheat(e.g.clothingor medication)oradisturbanceofhypothalamicthermalregulatory mechanisms.Thebodyrespondsbyprofoundvasodilatation.
Burns:Causedamagebycoagulatingtheskinandvariableamounts ofsubcutaneoustissue.Lipidmembranesmelt,enzymesdenature andproteinsprecipitate.Burnsareclassifiedasfirst,secondor thirddegreeaccordingtothedepthoftissuedamagedandthe surfaceareaofthebodyaffected.Plasmaandtissuefluidleak fromthesurfacesoftheburnedareasandmaycausehypovolaemic shockif >70%ofthebodysurfaceisinvolvedwiththird-degree burns.Thelossofvitalproteinmoleculesintheexudateimpairs theacuteinflammatoryresponseandhealing.Inhalationoffireand smokedamagestherespiratorytractmucosaandthealveolarwalls, causingacuterespiratorydistresssyndrome.Thedamagingeffectof heatisutilisedinradiofrequencyablation.
Cold:Hypothermiaoccurswhenthecoretemperaturedropsto 35∘ C.Ifshiveringandincreasedmuscleactivityfailtohaltthefall intemperature,respirationrate,pulse,bloodoxygenationandtissue perfusiondecreases.Bloodsludgesasplasmaislostbycold-induced diuresisandleakyendothelium.Thepatientbecomesconfused, thendeeplyunconscious.Deathisusualby28∘ C.
Suddenexposuretoextremecold,asseeninfrostbite,causes hypothermicdamagetoexposedorlesswell-perfusedparts,such asfingers,noseortoes.Thefluidinthecapillaries,cellsandtissues freezesandtherebyincreasesthevolumeofthecells.Theplasma membranesrupture,asdothoseoftheorganelles.Thereisgangrenousischaemicnecrosisoftheextremities.Treatmentisbygradualwarming.Oftentheextentofthedamageislessthaninitially feared,sodelayhastyamputation.
Perfusionwithcooledbloodreducesmetabolicdemandsand complicationsduringcardiactransplantsurgery.Thetransplanted heartwillhavebeentransportedtothedonor’shospitalinasupercooledstatetoreducetissuedeterioration.
Radiation Radiationcausesionisationofmoleculesintissuefluid,forming freeoxygenradicals(reactiveoxygenspecies)whichdamagetissues. Risksarerelatedtothetype,extentandcumulativedoseofradiationandthetissuesexposedtoit(seediagram).
Chemicalagents Exposuretostrongacidoralkalirupturescellmembranes,producingcellandtissuenecrosisandcapillarydamagewithleakageof bloodintotissues.Theeffectscanmimicburns.Healingofextensive woundsisoftenbyscarring.
Manyindustriesgenerateharmfulsubstancesasby-products. Somechemicalsreactwithcellularconstituentsorarealtered bynormalmetabolicpathwaystocreatetoxicmetabolites,for example:
•Conjugationwithglucuronidemayrenderamoleculesafeuntil itisexcretedbythekidney,whentheglucuronideisconservedand theurinaryepitheliumisexposedtothetoxicmetabolite.
•Volatileorganiccompounds(VOCs),e.g.polycyclicaromatic hydrocarbons(PAHs),aregeneratedbythepetrochemicalindustryorbycombustionoftars(e.g.soot)andalsofoundincigarette smoke.WhenconvertedtoepoxidesbycytochromeP450theycan bindandmutateDNA.SootwaslinkedtoscrotalcancerinchimneysweepsbyPercivalPottin1775.Smoking-relatedPAHsare stronglylinkedtothedevelopmentoflungcancer.
•Vinylchloridemonomers,producedduringPVCmanufacture, maygeneratechloracetaldehydewhenmetabolisedbyhepatic cytochromeP450;thiscanbindandmutateDNA.
CancertreatmentemploysdrugsthatinterferewithDNAreplicationtoattackdividingcells,workingonthepremisethatmore tumourthannormalcellsareusuallyproliferatingatanyone time,e.g.cyclophosphamidealkylatesDNAandcausesnonsense mutations.
Water Deathbydrowningisduetoasphyxia.Diatomsfromthewater enterthebloodandtissues.Deathisfourtofivetimesfaster infreshwaterthansaltwaterbecausethehypotonicfresh-water
solutionthatentersthebloodviathepulmonarycapillarybed causeshaemodilution,withlowchlorideandpotassiumlevels,and laterhyperkalaemiaduetoredcelllysis.Seawatermaybealmost isotonic,althoughusuallyitishypertonicandthebloodchloride levelisincreased,buthaemolysisdoesnotoccur,andthusresuscitationeffortshavemorechanceofsuccessinpeoplerescuedfromthe
sea.Peoplewhosurvivenear-drowningmaydeveloppneumonitis fromorganismsindirtywater.
Infectiousagents Inordertocausedamage,organismsmustevadethebody’sprimary defencesandenterthetissues(seeChapter16).