Small Animal Surgical Emergencies
Second Edition
Edited by Lillian R. Aronson Professor of Surgery School of Veterinary Medicine
University of Pennsylvania Philadelphia, PA, USA
This second edition first published 2022 © 2022 John Wiley & Sons, Inc.
Edition History
John Wiley & Sons, Inc. (1e, 2016)
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by law. Advice on how to obtain permission to reuse material from this title is available at http://www.wiley.com/go/permissions.
The right of Lillian R. Aronson to be identified as the author of the editorial material in this work has been asserted in accordance with law.
Registered Office
John Wiley & Sons, Inc., 111 River Street, Hoboken, NJ 07030, USA
Editorial Office
111 River Street, Hoboken, NJ 07030, USA
For details of our global editorial offices, customer services, and more information about Wiley products visit us at www.wiley.com.
Wiley also publishes its books in a variety of electronic formats and by print-on-demand. Some content that appears in standard print versions of this book may not be available in other formats.
Limit of Liability/Disclaimer of Warranty
The contents of this work are intended to further general scientific research, understanding, and discussion only and are not intended and should not be relied upon as recommending or promoting scientific method, diagnosis, or treatment by physicians for any particular patient. In view of ongoing research, equipment modifications, changes in governmental regulations, and the constant flow of information relating to the use of medicines, equipment, and devices, the reader is urged to review and evaluate the information provided in the package insert or instructions for each medicine, equipment, or device for, among other things, any changes in the instructions or indication of usage and for added warnings and precautions. While the publisher and authors have used their best efforts in preparing this work, they make no representations or warranties with respect to the accuracy or completeness of the contents of this work and specifically disclaim all warranties, including without limitation any implied warranties of merchantability or fitness for a particular purpose. No warranty may be created or extended by sales representatives, written sales materials or promotional statements for this work. The fact that an organization, website, or product is referred to in this work as a citation and/or potential source of further information does not mean that the publisher and authors endorse the information or services the organization, website, or product may provide or recommendations it may make. This work is sold with the understanding that the publisher is not engaged in rendering professional services. The advice and strategies contained herein may not be suitable for your situation. You should consult with a specialist where appropriate. Further, readers should be aware that websites listed in this work may have changed or disappeared between when this work was written and when it is read. Neither the publisher nor authors shall be liable for any loss of profit or any other commercial damages, including but not limited to special, incidental, consequential, or other damages.
Library of Congress Cataloging-in-Publication Data
Names: Aronson, Lillian R., editor.
Title: Small animal surgical emergencies / edited by Lillian R. Aronson.
Description: Second edition. | Hoboken, NJ : Wiley-Blackwell, 2022. | Includes bibliographical references and index.
Identifiers: LCCN 2022000548 (print) | LCCN 2022000549 (ebook) | ISBN 9781119658535 (cloth) | ISBN 9781119658610 (adobe pdf) | ISBN 9781119658627 (epub)
Subjects: MESH: Surgery, Veterinary–methods | Pets–surgery | Emergencies–veterinary | Animal Diseases–surgery | Wounds and Injuries–veterinary
Classification: LCC SF914.3 (print) | LCC SF914.3 (ebook) | NLM SF 914.3 | DDC 636.089/7–dc23/eng/20220209
LC record available at https://lccn.loc.gov/2022000548
LC ebook record available at https://lccn.loc.gov/2022000549
Cover Design: Wiley
Cover Images: Courtesy of Hunter Piegols, Courtesy of Marie Burneko
Set in 9.5/12.5pt STIXTwoText by Straive, Pondicherry, India
March 3, 1963
This textbook is dedicated to my amazing parents, Raphael and Dorothea Aronson. Growing up, my parents created a welcoming home filled with warmth, love, and constant laughter. They stressed the importance of family and community and have always been incredible role models, instilling in me the importance of honesty, respect, to always remain humble and to do the right thing even when it is not popular. From a very young age, my parents supported and encouraged me to follow my passion for veterinary medicine. I wouldn’t be where I am today if it wasn’t for their love and support. I consider myself the luckiest girl in the world, to be their daughter.
Contents
Contributors xii
Preface xvii
Acknowledgements xviii
About the Companion Website xix
Daisy’s Story xx
1 Triage and Initial Stabilization of the Emergency Small Animal Surgical Patient 1
Dana Clarke
2 Operating Room Nursing Tips for Emergency Surgical Procedures 20
Cami Elliott, Michelle Capps, and Michael McCallum
Section I Gastrointestinal System 49
3 Emergency Stabilization of the Acute Abdomen Patient 51
Nyssa Levy and Matthew Beal
4 Esophageal Foreign Bodies 58
Ivan Doran
5 Gastrointestinal Foreign Bodies 70
Amie Koenig and Mandy L. Wallace
6 Intussusception 81
Janet Kovak McClaran and Yekaterina Buriko
7 Rectal Prolapse 88
Jennifer L. Huck
8 Gastric Dilatation and Volvulus 93
Michael S. Tivers and Sophie Adamantos
9 Intestinal Volvulus 108
Elizabeth LaFond and Kristina Kiefer
10 Colonic Torsion 115
Chloe Wormser
11 Peritonitis 119
Adrienne Bentley and Anusha Balakrishnan
12 Surgical Intervention Post-Celiotomy 141
Michael B. Mison
13 Biliary Emergencies 146
Lori Ludwig and Sean Smarick
14 Hemoperitoneum 164
Cassie N. Lux, William T. N. Culp and Steven E. Epstein
15 True Abdominal Hernias 178
Daniel D. Smeak
16 Traumatic and Incisional Hernias 190
Todd Hamilton
17 Perineal Hernias 199
Karen M. Tobias
18 Pancreatic Abscessation 216
F. A. (Tony) Mann
19 Hepatic Emergencies 226
James A. Perry, Steven E. Epstein, and William T. N. Culp
20 Bleeding Gastrointestinal Ulcers 238
Yekaterina Buriko, David Holt, Laura Ateca, and Lesley King
21 Enteral Feeding Tubes 251
Aarti Kathrani
Section II Urinary System 263
22 Stabilization of the Uremic Patient 265
Kari Beer and Kenneth Drobatz
Section IIa Urinary System - Urinary Tract Trauma 277
23 Renal and Ureteral Injury 279
Dan Degner and Chloe Wormser
24 Approach to the Uroabdomen 285
Sara Colopy, Adam Townsend, and Dale Bjorling
25 Urethral Injury 297
Sara Colopy, Adam Townsend, and Dale Bjorling
Section IIb Urinary System – Urinary Obstruction 311
26 Ureteral Obstruction 313
Daniel Degner, Dana Clarke, and Chloe Wormser
27 Urethral Obstruction 331
Heidi Phillips and Sara Colopy
Section III Respiratory System 351
Section IIIa Respiratory System – Upper Airway Disease 353
28 Stabilization Techniques for Patients with an Upper Respiratory Obstruction 355
Meredith Maczuzak and Deborah C. Silverstein
29 Tracheostomy 364
Nathaniel Lam
30 Brachycephalic Airway Syndrome 372
Mike Schlicksup
31 Laryngeal Paralysis 383
Georga T. Karbe
32 Laryngeal Trauma 391
Eric Monnet
33 Tracheal Collapse 395
William T. N. Culp and Matthew D. O’Donnell
Section IIIb Respiratory System – Pleural Space Disease 405
34 Stabilization Techniques for Patients with Pleural Space Disease 407
Erica Reineke and Jen Savini
35 Diaphragmatic Hernia 417
MaryAnn Radlinsky
36 Pyothorax 425
Lori S. Waddell and David A. Puerto
37 Hemothorax 433
Chad W. Schmiedt and Benjamin M. Brainard
38 Pneumothorax 441
David A. Puerto and Lori S. Waddell
39 Lung Lobe Torsion 451
Jacob A. Rubin and Jaime Green
40 Surgical Approach to the Thoracic Cavity 459
David A. Puerto and Jacob A. Rubin
Section IIIc Respiratory System – Chest Wall Disease 467
41 Stabilization Techniques for Patients with Chest Wall Disease 469
Nolan Chalifoux and Deborah Silverstein
42 Pectus Excavatum 475
Krista N. Adamovich-Rippe and William T. N. Culp
43 Flail Chest 483
Eric Monnet
Section IV Cardiovascular System 487
44 Pacemaker Therapy 489
Caryn Reynolds and Katrine Saile
45 Pericardial Effusion 501
Augusta Pelosi and Amy Koenigshof
46 Open-Chest Cardiopulmonary Resuscitation 514
Jasper Burke and Deborah Silverstein
Section V Reproductive System 525
47 Cesarean Section 527
Stephen D. Gilson
48 Pyometra 534
Jacqueline Davidson and Dorothy Black
49 Penile and Testicular Emergencies 541
Susan P. Gregory
50 Prostatic Abscessation 553
Richard A. S. White
51 Uterine and Vaginal Prolapse 565
Pieter Nelissen
Section VI Wound Management 573
52 Bite Wounds 575
David Holt and Vincent Thawley
53 Burn Injury 586
Caroline Garzotto and Dana Clarke
54 Penetrating Injury in the Dog and Cat 600
Steve J. Mehler
55 Necrotizing Fasciitis 613
Karol A. Mathews and Ameet Singh
56 Degloving and Shear Injuries 626
Bryden J. Stanley and Susan W. Volk
57 Skin Flaps and Grafts: Managing Complications 645
Michael B. Mison
58 Incisional Infections 652
Brandy A. Burgess
Section VII Ocular Emergencies 659
59 Ocular Emergencies 661
Deborah C. Mandell and Rosalie M. Atkins
Section VIII Oral Surgical Emergencies 685
60 Oral Surgical Emergencies 687
Alexander M. Reiter
Section IX Orthopedic Emergencies 701
61 Approach to the Septic Joint 703
Samuel P. Franklin
62 Surgical Management of Open Fractures 715
Kimberly Agnello
63 Traumatic Joint Luxation and Reduction 725
Anna Massie and Po-Yen Chou
Index 739
Contributors
Sophie Adamantos BVSc CertVA DACVECC DECVCC
MRCVS FHEA
Clinical Director
Paragon Veterinary Referrals Wakefield, UK
Krista N. Adamovich-Rippe DVM DACVS
Associate Surgeon Central Texas Veterinary Specialty and Emergency Hospital Austin, TX, USA
Kimberly Agnello DVM DACVS
Associate Professor of Surgery University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Laura Ateca VMD DACVECC
Attending Criticalist Emergency and Critical Care Service, Guardian Veterinary Specialists Brewster, NY, USA
Rosalie M. Atkins DVM DACVO VCA Northwest Veterinary Specialists, Clackamas, OR, USA
Anusha Balakrishnan BVSc DACVECC Triangle Veterinary Referral Hospital, Durham, NC, USA
Matthew Beal DVM DACVECC
Head of Interventional Radiology Services, Head of Emergency and Critical Care Medical Services Department of Small Animal Clinical Sciences Michigan State University, College of Veterinary Medicine East Lansing, MI, USA
Kari Santoro Beer DVM DACVECC Emergency and Critical Care Specialist Oakland Veterinary Referral Services Bloomfield Hills, MI, USA
Adrienne Bentley DVM DACVS Staff Surgeon
Cornell University Veterinary Specialists Stamford, CT, USA
Dale Bjorling DVM DACVS Professor of Small Animal Surgery University of Wisconsin-Madison School of Veterinary Medicine Madison, WI, USA
Dorothy Black DVM MPVM DACVECC Criticalist and Owner Rex Vet, Inc., San Mateo, CA, USA
Ben Brainard VMD DACVAA DACVECC
Professor of Small Animal Critical Care Director of Clinical Research Department of Small Animal Medicine and Surgery University of Georgia, College of Veterinary Medicine Athens, GA, USA
Brandy A. Burgess DVM MSc PhD DACVIM-LA DACVPM
Associate Professor, Director of Infection Control University of Georgia, College of Veterinary Medicine Athens, GA, USA
Kate Buriko DVM DACVECC
Assistant Professor, Emergency and Critical Care University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Jasper Burke VMD
Resident in Emergency and Critical Care University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Michelle Capps CVT
Surgical Nursing Staff Supervisor University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Nolan Chalifoux DVM
Resident in Emergency and Critical Care
University of Pennsylvania, School of Veterinary Medicine
Philadelphia, PA, USA
Po-Yen Chou BVM MVM DACVS
Assistant Professor of Small Animal Orthopedic Surgery
Department of Surgical and Radiological Sciences
University of California-Davis, School of Veterinary Medicine
Davis, CA, USA
Dana Clarke DVM DACVECC
Assistant Professor, Interventional Radiology and Critical Care
University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Sara Colopy DVM, PhD, DACVS
Clinical Assistant Professor, Small Animal Surgery
University of Wisconsin, School of Veterinary Medicine Madison WI, USA
William T.N. Culp VMD DACVS
Professor of Small Animal Surgery
Department of Surgical and Radiological Sciences
University of California-Davis, School of Veterinary Medicine
Davis, CA, USA
Jacqueline Davidson DVM MS
Clinical Professor
Veterinary Medical Teaching Hospital, Texas A and M College Station, TX, USA
Daniel Degner DVM DACVS
Animal Surgical Center of Michigan Burton, MI, USA
Ivan Doran BVSc CertSAS DSAS(Soft Tissue) MRCVS
RCVS Specialist in Small Animal Soft Tissue Surgery
Highcroft Veterinary Referrals Bristol, UK
Kenneth Drobatz DVM DACVECC
Professor of Small Animal Emergency and Critical Care
University of Pennsylvania, School of Veterinary Medicine
Philadelphia, PA, USA
Cami Elliot CVT
Nashville Veterinary Specialists and Animal Emergency
Nashville, TN, USA
Steven E. Epstein DVM DACVECC
Professor of Emergency and Critical Care
Department of Surgical and Radiological Sciences
University of California-Davis, School of Veterinary Medicine Davis, CA, USA
Samuel P. Franklin DVM MS PhD DACVS DACVSMR
ACVS Founding Fellow, Minimally Invasive Surgery, Small Animal Orthopedics
Kansas City Canine Orthopedics, Kansas City, KS, USA
Caroline Garzotto VMD DACVS
Staff Surgeon
Mount Laurel Animal Hospital Mount Laurel, NJ, USA
Stephen D. Gilson DVM DACVS
ACVS Founding Fellow in Surgical Oncology
Indigo Veterinary Specialists Phoenix, AZ, USA
Jaime Green DVM, DACVS
Maine Veterinary Medical Center Scarborough, ME, USA
Susan P. Gregory BVetMed PhD DVR DSAS (Soft Tissue)
FHEA MRCVS
Professor of Veterinary Nursing (retired)
Royal Veterinary College, Department of Clinical Science and Services
North Mymms, Hatfield, Hertfordshire, UK
Todd Hamilton VMD DACVS
Maine Veterinary Medical Center Scarborough, ME, USA
David Holt BVSc DACVS
Professor of Small Animal Surgery
University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Jennifer L. Huck DVM DACVS
Assistant Professor of Surgery
University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Georga T. Karbe Dr Med Vet MRCVS DACVS Department Head: Soft Tissue Surgery University of Veterinary Medicine Hannover, Hannover, Germany
Aarti Kathrani BVetMed PhD DACVIM DACVN FHEA MRCVS
Senior Lecturer in Small Animal Internal Medicine Royal Veterinary College, Clinical Science and Services Department Hatfield, Hertfordshire, UK
Kristina Kiefer DVM PhD CCRP DACVSMR Surgical Coach VetSSMART LLC St Paul, MN, USA
Amie Koenig DVM, DACVIM DACVECC Professor of Emergency and Critical Care Department of Small Animal Medicine and Surgery University of Georgia, College of Veterinary Medicine Athens, GA, USA
Amy Koenigshof DVM MS DACVECC Two by Two Animal Hospital Berrien Springs, MI, USA
Janet J Kovak McClaren DVM DACVS DECVS MRCVS Staff Doctor London Veterinary Specialists London, UK
Elizabeth LaFond DVM DACVS DACVSMR Veterinary Specialists of Sydney Miranda, NSW, Australia
Nathaniel Lam DVM DACVS Chief of Surgery VCA Oahu Veterinary Specialty Center Pearl City, HI, USA
Nyssa Levy DVM MS DACVECC Assistant Professor, Emergency and Critical Care Medicine Department of Small Animal Clinical Sciences Michigan State University, College of Veterinary Medicine East Lansing, MI, USA
Lori Ludwig VMD MS DACVS Mobile Veterinary Surgery Charleston, SC, USA
Cassie N. Lux DVM DACVS
Associate Professor of Surgery Department of Small Animal Clinical Sciences College of Veterinary Medicine, University of Tennessee Knoxville, TN, USA
Mike McCallum CVT Director of Operations
University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Meredith Maczuzak DVM DACVECC Emergency Medicine Specialist Pittsburgh Veterinary Specialty and Emergency Center – BluePearl South Hills, PA, USA
Deborah C. Mandell VMD DACVECC Professor, Clinical Emergency and Critical Care University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
F.A. (Tony) Mann DVM MS DACVS DACVECC Professor and Small Animal Soft Tissue Surgeon Director of Small Animal Emergency and Critical Care Services
University of Missouri-Veterinary Medical Teaching Hospital Columbia, MO, USA
Anna Massie DVM DACVS Assistant Professor of Surgery University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Karol A. Mathews DVM DVSc DACVECC
Professor Emeritus of Emergency and Critical Care
Ontario Veterinary College, University of Guelph Guelph, ON, Canada
Steve J. Mehler DVM DACVS Main Line Veterinary Specialists Devon, PA, USA
Michael B. Mison DVM DACVS Surgery – MedVet Salt Lake City Salt Lake City, UT, USA
Eric Monnet DVM PhD FAHA DACVS ECVS Professor of Surgery Department of Clinical Sciences
College of Veterinary Medicine and Clinical Sciences
Colorado State University Fort Collins, CO, USA
Pieter Nelissen DVM CertSAS DECVS MRCVS
European Specialist in Small Animal Surgery, RCVS
Recognized Specialist in Small Animal Surgery (Soft Tissue), Founder and Director, Department Head of Surgery
Frontier Veterinary Specialists Munich, Germany
Matthew D. O’Donnell DVM DACVS
Central Texas Veterinary Specialty and Emergency Hospital
Austin, TX, USA
Augusta Pelosi DVM DACVS DACVIM (Cardiology)
Cardiologist
Veterinary Heart Institute Boca Raton, FL, USA
James A. Perry DVM PhD DACVIM (Oncology) DACVS
Veterinary Cancer and Surgery Specialists Milwaukie, OR, USA
Heidi Phillips VMD DACVS
Associate Professor of Small Animal Surgery University of Illinois, College of Veterinary Medicine Urbana, IL, USA
David A. Puerto DVM DACVS
Center for Animal Referral and Emergency Services Langhorne, PA, USA
MaryAnn Radlinsky DVM MS DACVS
Founding Fellow, Minimally Invasive Surgery
Small Animal Soft Tissue
Salt River Veterinary Specialists Scottsdale, AZ, USA
Erica Reineke VMD DACVECC
Associate Professor of Emergency and Critical Care University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Alexander M. Reiter Dipl Tzt Dr med vet DAVDC DEVDC
FF-AVDC-OMFS
Professor of Dentistry and Oral Surgery
University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Caryn Reynolds DVM DACVIM (Cardiology)
Cardiologist
Dove Lewis Emergency Hospital Portland, OR, USA
Jacob Rubin DVM DACVS
Maine Veterinary Medical Center Scarborough, ME, USA
Katrine Saile DVM, MS, DACVS
Associate Surgeon
Blue Pearl Pittsburgh Veterinary Specialty and Emergency Center Pittsburgh, PA, USA
Jennifer Savini DVM DACVECC
Emergency and Critical Care Specialist
VRC Specialty Hospital Malvern, PA, USA
Mike Schlicksup DVM DACVS
Columbia Veterinary Emergency Trauma and Specialty Columbia, SC, USA
Chad Schmeidt DVM DACVS
Professor of Small Animal Surgery University of Georgia, College of Veterinary Medicine Athens, GA, USA
Deborah Silverstein DVM DACVECC
Professor of Critical Care University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Ameet Singh BSc DVM DVSc DACVS
Associate Professor of Surgery Ontario Veterinary College, University of Guelph Guelph, ON, Canada
Sean Smarick DVM DACVECC Independent Consultant North Huntingdon, PA, USA
Daniel D. Smeak DVM DACVS
Vice President, Surgical Models, Inotiv; Fort Collins
Emeritus Professor of Surgery Colorado State University Fort Collins, CO, USA
Bryden J. Stanley BSc BVMS MACVSc MVetSc DACVS
Emeritus Professor Michigan State University, College of Veterinary Medicine East Lansing, MI, USA
Vincent Thawley VMD, DACVECC
Assistant Professor, Clinical Emergency and Critical Care University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Michael S. Tivers BVSc PhD CertSAS DECVS MRCVS
Head of Surgery
Paragon Veterinary Referrals Wakefield, UK
Karen M. Tobias DVM MS DACVS
Institute Professor, Department of Small Animal Clinical Science
University of Tennessee, College of Veterinary Medicine Knoxville, TN, USA
Adam Townsend DVM Resident, Small Animal Surgery University of Wisconsin-Madison, School of Veterinary Medicine Madison, WI, USA
Susan W. Volk VMD PhD DACVS
Associate Professor, Small Animal Surgery University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Lori S. Wadell DVM DACVECC
Professor of Clinical Critical Care Medicine
University of Pennsylvania, School of Veterinary Medicine Philadelphia, PA, USA
Mandy L. Wallace DVM MS DACVS Assistant Professor University of Georgia, College of Veterinary Medicine Athens, GA, USA
Richard A.S. White BVetMed PhD DSAS DVR FRCVS
DACVS ECVS
European and RCVS Specialist in Small Animal Surgery, RCVS Specialist in Veterinary Oncology, ACVS Founding Fellow, Surgical Oncology
Clinical Director, Smart Paws GmbH
Special Professor of Small Animal Surgery
University of Nottingham, Nottingham, UK
Chloe Wormser VMD DACVS
Elite Veterinary Surgery
Northway Animal Emergency Clinic
Gansevoort, NY, USA
Preface
As the management of small animal surgical emergencies is constantly evolving, the purpose for writing this second edition is to have an up-to-date resource for the veterinary surgeon, critical care specialist, and general practitioner that builds on information presented in the first edition and provides updated information on preoperative stabilization, new and innovative treatment options and aftercare. Similar to the first edition, the majority of chapters are authored by two, and occasionally three, specialists in the fields of both surgery and emergency/ critical care to combine the expertise of individuals from these two disciplines. In addition to approximately 70 authors who contributed to the first edition, 18 new authors have agreed to share their knowledge and expertise with the reader. The layout of the second edition is similar to the first edition, with many of the chapters covering step-bystep information on emergency stabilization, diagnostic approach, operative techniques, postoperative care, common complications encountered, and how to troubleshoot such complications should they occur. Relevant anatomy, imaging and full color illustrations and drawings have been incorporated into each chapter to support the text. Case presentations have also been included when appropriate.
To strive to enhance the content of the first edition, nine new chapters have been added based on advice received from respected colleagues. Following the introductory chapter, Triage and Initial Stabilization of the Emergency Small Animal Surgical Patient, a new chapter, Operating Room Nursing Tips for Emergency Surgical Procedures, has been added to the beginning of the book to assist veterinary nurses and operating room technicians who may be working with these critical patients. This chapter provides
information on patient positioning and preparation in the operating room, essential equipment, and appropriate sterilization techniques. For the section on the gastrointestinal system, four new chapters have been added, including Rectal Prolapse, Colonic Torsion, Surgical Intervention Post-Celiotomy, and a chapter on Enteral Feeding Tubes. Including the chapter on nutritional support reiterates the importance of appropriate stabilization and aftercare to the ultimate success of the emergency surgical patient. In the cardiovascular system section, a chapter has been added on Open-Chest Cardiopulmonary Resuscitation, and in the section on wound management, two new chapters have been added, including The Failed Flap and Incisional Infections. Finally, for the section on orthopedic emergencies, in addition to updating chapters from the first edition on the Approach to the Septic Joint and the Surgical Management of Open Fractures, a chapter on Traumatic Joint luxation and Reduction has been added to provide a comprehensive resource when faced with an orthopedic emergency.
Although there are veterinary textbooks that focus on small animal surgery and those that focus on critical care medicine, this is the only book that focuses on the combination of these two disciplines, filling a niche currently vacant in the veterinary literature. Additionally, this book is unique in that the majority of the chapters are co-authored by experts in both fields. Because surgical emergencies are common in veterinary medicine, this textbook should have a wide audience, including surgical and critical care residents in training, veterinary surgeons and criticalists, and veterinary practitioners who work in emergency medicine or those who have an interest in surgery.
Acknowledgements
I would like to thank the staff at Wiley, with special thanks to Meryl Le Roux and Erica Judisch, for all their help and encouragement throughout this process. Without their support and guidance, completion of this project would not have been possible.
The impact of Covid-19 on many of the authors who contributed to this textbook cannot be overstated. The disruption in normal work, family routine, health issues, and economic hardship resulted in significant fear and anxiety. I truly want to thank all the authors for their dedication and commitment to this project – I know it wasn’t easy.
Finally, since the publication of the first edition, many of us lost a dear friend and colleague, Dr. Lesley King. Lesley was a Professor of Critical Care at the University of Pennsylvania and was instrumental in the development of intensive care as a veterinary specialty. Lesley made significant contributions to the veterinary literature including as a contributor to the first edition of this textbook. Lesley was not only a colleague, but also a good friend, and will be dearly missed.
About the Companion Website
This book is accompanied by a companion website: www.wiley.com/go/aronson/surgical
The website includes:
● Case Studies
● Video clips
● References
Daisy’s story can be found in Chapter 54 (Case Report 54.2). After an encounter with a porcupine, Daisy underwent two major surgeries and spent weeks in our
ICU recovering. During times of COVID-19, a new normal developed and owners were unable to visit their pets during their hospital stay. Daisy’s owners decided on the next best thing – Facetime! Here she is being read a story during one of her virtual visits with Mom and Dad.
Daisy’s Story
Triage and Initial Stabilization of the Emergency Small Animal Surgical Patient
Dana Clarke
University of Pennsylvania, School of Veterinary Medicine, Philadephia, PA, USA
Introduction
One of the most challenging aspects of emergency medicine is being presented with patients who have a variety of clinical signs and disease severities to assess, prioritize, stabilize, and provide with definitive care. The veterinary clinician is reliant on information provided by the client, their physical assessment, and initial diagnostics to determine severity of illness and injury, and therefore, urgency of care. Efficient identification and treatment of respiratory, cardiovascular, urinary, and neurologic derangements is essential for successful patient outcomes. When emergency surgical intervention is required, it is crucial to appropriately stabilize the patient for anesthesia without unduly delaying surgical care.
Triage and Initial Assessment
Triage is an essential tool in the setting of emergency medicine to assess and prioritize critically ill patients [1, 2]. This is particularly true of patients that may require emergency surgical intervention, as the time to provide appropriate stabilizing care and definitive surgical therapy likely impacts patient outcome.
In many veterinary hospitals, nurses obtain pertinent historical information and perform a basic assessment to determine whether the patient needs immediate further evaluation or is stable enough to be seen in turn. In general, over-triage is preferred to under-triage in veterinary medicine, as the severity of signs presented by the patient and observed by the pet owner may not be fully appreciated by untrained individuals. Triage and training systems in patient assessment are used routinely in human emergency medicine. A variety of triage systems exist for human patients,
which when combined with education of the medical staff on the system’s guidelines for prioritizing medical care, reduces inconsistencies in decision-making [3]. In veterinary medicine, no uniformly accepted triage system exists. Veterinary healthcare professionals therefore use historical information and intuition to make rapid decisions regarding the need for immediate care and order in which patients will be seen. The animal trauma triage (ATT) score was developed retrospectively and assessed prospectively to help to classify and prognosticate for a heterogenous patient group. For each patient, six categories are assessed (perfusion, cardiac, respiratory, skeletal, neurologic, and eye/muscle/integument) and scored from 0 to 3, with 0 being unaffected or only slightly affected to 3 indicating severe injury. The six scores are added together with a maximum possible score of 18. In both the retrospective and prospective populations, the mean ATT score of survivors was significantly lower than non-survivors and for each one-point increase in ATT, the likelihood of survival decreased 2.3–2.6 times [4]. Another veterinary triage system, adapted from the Manchester triage system, uses a five-category system using color-coding to indicate urgency. Examples of “red” emergencies (those which need to be seen immediately) include severe respiratory distress, decompensated shock, lifethreatening hemorrhage, and active seizures. Very urgent emergencies, including moderate respiratory distress, evidence of aortic thromboembolism, and urethral obstruction, were classified as “orange.” Urgent emergencies, such as mild hemorrhage, moderate dehydration and open fracture were classified as “yellow,” while non-urgent disease processes such as localized inflammation, soft-tissue swelling, stranguria and recent isolated seizure were classified as “green” [5]. The study determined that the use of a veterinary triage list by nurses upon triage corresponded better to retrospectively reviewed patient status than when individual
judgment and intuition upon triage were employed [5]. Multicenter, prospective evaluation of this veterinary triage list is warranted to determine whether patient care is improved and time to be seen can be better estimated.
Irrespective of the need for a formal veterinary triage system, a brief, but thorough physical exam remains the gold standard for recognizing critical patient status. The initial triage assessment includes visual examination and assessment of four key body systems: cardiovascular, respiratory, neurologic, and urinary [6, 7]. Information regarding the patient’s mentation and responsiveness, as well as respiratory rate and effort, are obtained quickly on brief visual exam, often before performing any parts of a physical examination. Thoracic and cardiac auscultation with concurrent pulse palpation and a more thorough assessment of neurologic status, if indicated, follows visual examination. After cardiovascular, respiratory, and neurologic status is determined, if the patient is stable enough for further evaluation, urinary triage can be performed. Any significant pain must be addressed urgently to improve patient comfort and so that the effects of pain do not alter interpretation of cardiovascular and respiratory findings. Additionally, aggression should not be considered a sign of patient stability, as many scared and stressed patients will be aggressive in the face of severe shock.
Respiratory Assessment
Before any physical examination, all patients should have their respiratory rate, effort, noise, and pattern observed from afar. If a patient is showing any changes in respiratory pattern or effort, oxygen supplementation should be provided immediately. If there is any respiratory compromise, the patient should be presumed to be in hypoxemic shock until proven otherwise and oxygen supplementation should be provided. Further respiratory triage involves auscultation of the upper airway, trachea, and thorax. During abbreviated thoracic auscultation, emphasis should be placed on determining heart rate, rhythm, the presence of murmur(s) or arrhythmia(s), and lung sounds in all lung fields. Visual and auditory assessment of respiratory pattern and noise combined with thoracic auscultation should help localize the anatomic origin of the respiratory distress. The impact of pain, stress, and anxiety on respiratory rate and effort should not be underestimated (Figure 1.1).
If respiratory noise is localized to the upper airway, diseases associated with an upper airway obstruction, including laryngeal paralysis, laryngeal collapse, brachycephalic airway disease, tracheal collapse, the presence of a tracheal, laryngeal, or pharyngeal mass, and the presence of a

foreign body should be ruled out. See Chapter 28 for stabilization of the patient with upper airway obstruction. If decreased lung sounds relative to respiratory effort are heard dorsally, pneumothorax should be suspected. However, if decreased lung sounds are heard ventrally, pleural effusion should be considered. Lung sounds may not be completely absent in the presence of pleural effusion or pneumothorax, they may be reduced relative to the other lung fields but still present. See Chapter 34 for stabilization of the patient with pleural space disease. Diseases of the chest wall such as masses, rib fractures, and flail segments may also result in abnormal auscultation of the pulmonary parenchyma. For more information on chest wall disease, see Chapter 41.
For patients in respiratory distress with a heart murmur, arrhythmia, pleural effusion, or pulmonary crackles present on auscultation, cardiogenic and hypoxemic shock should be considered as possible differentials. This is particularly important since fluid therapy is often contraindicated in most patients with cardiac dysfunction or failure and must be ruled out, to the best of the clinician’s ability on triage, prior to administering intravenous (IV) fluid therapy.
Hypoxemic Shock
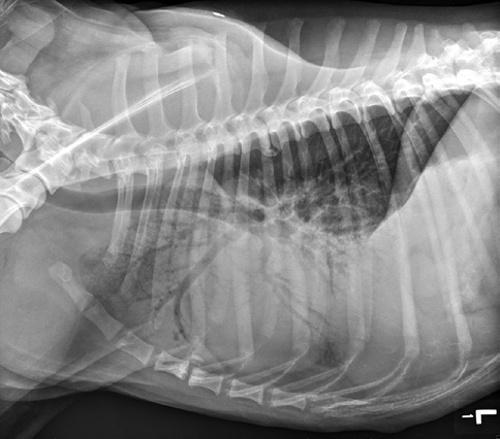
Hypoxemic shock occurs secondary to decreased arterial blood oxygen content. Common causes of hypoxemic shock include pulmonary parenchymal disease, such as pneumonia, severe anemia, and hypoventilation (Figure 1.2). Many veterinary patients in hypoxemic shock are at the limits of their physiologic reserves, and are intolerant of excessive handling, restraint, and manipulation; they should be handled carefully. Clinical signs include weakness, mental
Figure 1.1 Cat with open mouth breathing secondary to the pain associated with an aortic thromboembolism.
Figure 1.2 Lateral thoracic radiograph showing cranioventral pulmonary infiltrates creating an alveolar pattern consistent with aspiration pneumonia.
depression, pale mucous membranes, dyspnea, crackles or increased bronchovesicular lung sounds, or decreased lung sounds ventrally (pleural effusion) or dorsally (pneumothorax), and cyanosis. Patients with diaphragmatic hernia may have decreased lung sounds dorsally or ventrally. Cyanosis is only seen with severe hypoxemia (at least 5 g/dl of deoxygenated hemoglobin), and thus the absence of cyanosis absolutely does not rule out hypoxemia. In anemic animals, cyanosis is unlikely to be detected due to decreased hemoglobin concentration, and therefore should not be relied upon to diagnose hypoxemia [8].
In any patient with suspected hypoxemic shock, supplemental oxygen should be provided until the ability to adequately oxygenate is confirmed. Diagnostics that can be helpful for the patient in hypoxemic shock include pulse oximetry (peripheral capillary oxygen saturation, SpO2), arterial blood gas analysis, thoracic radiographs, thoracic/trauma computed tomography (CT), and thoracic ultrasound. SpO2 may be less effective with bright lighting, poor perfusion, high motion, and pigmentation of the skin. It is convenient since it can noninvasively determine percentage of oxygenated hemoglobin, and, for sedentary patients, can be left in place for continuous monitoring (Figure 1.3). Many patients in respiratory distress will not tolerate the restraint necessary for arterial blood gas collection and thoracic radiographs, especially on presentation. If obtaining an arterial blood gas is feasible, findings may include decreased SpO2, decreased partial pressure of carbon dioxide (PaCO2) consistent with hyperventilation, increased PaCO2 consistent with hypoventilation, decreased partial pressure of oxygen

Figure 1.3 Continuous pulse oximetry assessment in a laterally recumbent dog receiving oxygen supplementation via nasal prongs.
(PaO2) consistent with hypoxemia, and an increased partial pressure of alveolar–arterial oxygen gradient P(A–a) O2). Calculation of the P(A–a)O2 gradient provides objective information on pulmonary function by removing the influence of ventilation on PaO2. When a patient is breathing 21% oxygen, the P(A–a)O2 should be less than 10–15 mmHg. When a patient is breathing 100% oxygen, the P(A–a)O2 should be less than 150 mmHg. If the P(A–a)O2 gradient is greater than 15 mmHg while breathing 21% oxygen, it is consistent with pulmonary dysfunction. For A–a gradient calculation, see the formula in Box 1.1.
Preliminary evaluation of the ratio of SpO2 to fraction of inspired oxygen (FiO2) to the partial pressure of oxygen in arterial blood to FiO2 (PaO2/FiO2) showed good correlation between the two values in dogs. It is possible that with further investigation, the SpO2/FiO2 may become a reliable, less invasive alternative to determining PaO2/FiO2 [9].
Thoracic radiographs may show pulmonary parenchymal infiltrates ventrally consistent with pneumonia, caudodorsally consistent with non- cardiogenic pulmonary edema, and in the perihilar region consistent with congestive heart failure. In the trauma patient,
Box 1.1 Formula Used for A–a Gradient Calculation
The partial pressure of alveolar–arterial oxygen (P(A–a)O2) gradient provides objective information on pulmonary function by removing the influence of ventilation on PaO2.
PA-a OP OP 22AaO2
PO FO2P PP CO R Ai atmH 22Oa 2 /
PAO2 = alveolar gas equation
FiO2 = percentage of inspired O2
Patm = atmospheric pressure (760 mmHg used at sea level)
PH2O = water vapor pressure (53 mmHg 39°C for dogs/ cats; 47 mmHg at 37°C in humans)
R = respiratory quotient (approximately 0.8–0.9)
Example Blood Gas
PaCO2 = 24.2
PaO2 = 59.5
PAO2 = (0.21 × (760 – 53)) – (24.2/0.9)
PAO2 = 121.6
P(A–a)O2 = 121.6–59.5
P(A–a)O2 = 62.1 (indicates hypoxemia is due to pulmonary dysfunction)
pulmonary contusions, which can be present in any lung field(s), may not become radiographically apparent for up to 48 hours, although peak opacification has been shown to occur at 6 hours in human trauma patients [10].
Additionally, up to 30% of human trauma patients do not have radiographic evidence of contusions on initial thoracic radiographs, which is why CT is often proposed as the preferred method of thoracic imaging [10–12]. In a study of dogs that had succumb to vehicular trauma, thoracic radiographs underestimated the presence of contusions, while also overestimating their severity. The same study also noted that thoracic radiographs were less sensitive than CT for detecting rib fractures [13]. Initial investigation in the use of thoracic ultrasound for detection of pulmonary contusions in dogs with vehicular trauma showed a high sensitivity for diagnosing contusions compared with CT, and even noted improved sensitivity compared with thoracic radiographs [14]. Therefore, cautious respiratory monitoring and repeat thoracic imaging may be indicated in any patient with a history of known or suspected trauma.
Thoracic ultrasound, also known as thoracic focused assessment with sonography for trauma, triage, and tracking (TFAST), allows clinicians to assess for pleural
and pericardial effusion, pneumothorax, and pulmonary parenchymal infiltrates [15–20]. It is particularly useful in patients that are not stable enough for thoracic radiographs, as well as a monitoring tool to assess for response to therapy. Thoracic ultrasound may be performed with the patient in sternal or lateral recumbency. Pleural effusion is generally visible in the cranial and/or caudoventral pleural space. Ultrasound guidance to localized fluid pockets can be helpful to guide thoracocentesis. When evaluating for the presence of pneumothorax, the caudodorsal thorax is evaluated for the lack of a “glide” sign, which is diagnostic for pneumothorax. A glide sign is created by the normal back and forth respiratory motion of the interface between the visceral and parietal pleura (Video 1.1). Free air in the thoracic cavity obliterates the glide sign [15–17]. Cellular or fluid infiltrate into the pulmonary parenchyma, as with edema, hemorrhage, and pneumonia can be assessed using ultrasound in four windows in each hemithorax (caudodorsal, cranial, middle lung lobe regions, and perihilar) for the presence of increased penetration of ultrasound, which manifest as hyperechoic lines (B-lines) in parallel with the ultrasound beam, that can be individual or coalescing (Figure 1.4 and Video 1.2) [18–22].
Video 1.1 TFAST showing a normal glide sign, which is created by the respiratory motion of the visceral and parietal pleural interface sliding back and forth.
Video 1.2 TFAST showing coalescing B-lines created by marked pulmonary infiltrates allowing ultrasound penetration into the pulmonary parenchyma.
Figure 1.4 TFAST ultrasonographic appearance (still image) of a B-line, which is created by increased infiltrates in the pulmonary parenchyma allowing ultrasound penetration.