Professor of Physiology, Anesthesiology, and Cardiopulmonary Science
Louisiana State Universit;, Health Sciences 'Center
New Orleans, Louisiana
Adjunct Professor of l?liysiology and Pediatrics
Tulane University. Meaical Center
New Orleans, Louisiana
Copyright Cl2018 by McGraw-Hill Education. All rights reserved. Except as permitted under the Uoited States Copyright Act of 1976, no part ofthis publication may be reproduced or distributed in any form or by any means, or stored in a database or retrieval system, without the prior written permission of the publisher.
ISBN: 978-1-26-001934-6 MinD: 1-26-001934-9
The IDJlterial in this eBook also appears in the print version of this title: ISBN: 978-1-26-001933-9, MinD: 1-26-001933-0.
eBook conversion by codeMantra Version 1.0
All trademarks are trademarks of their respective owners. Rather than put a trademark symbol after every occurrence of a trademarked name, we use names in an editorial fashion only, and to the benefit ofthe trademark owner, with no intention of infringc::mc::nt of the tradCIDllrk. Where such designations appear in this book, they have been printed with initial caps.
McGraw-Hill Education eBooks are available at special quantity discounts to use as premiums and sales promotions or for use in corporate training programs. To contact a representative, please visit the Contact Us page at www.mhprofessional.com.
Notice
Medicine is an ever-changing science. As new research and clioical c::xpc::rience broaden our knowledge, changes in treatment and drug therapy are required. The authors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of the information contained in this work. Readers are encouraged to confirm the information contained herein with other sources. For example and in particular, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in coonection with new or infrequently used drugs.
TERMS OF USE
This is a copyrighted work and McGraw-Hill Education and its licensors reserve all rights in and to the work. Use of this work is subject to these terms. Except as permitted under the Copyright Act of 1976 and the right to store and retrieve one copy of the work, you may not decompile, disassemble, reverse engineer, reproduce, modify, create derivative works based upon, transmit, distribute, disseroinate, sell, publish or sublicense the work or any part of it without McGraw-Hill Education's prior consent. You may use the work for your own noncommercial and personal use; any other use of the work is strictly prohibited. Your right to use the work may be terminated if you fail to comply with these terms.
THE WORK IS PROVIDED "AS IS." McGRAW-HILL EDUCATION AND ITS UCENSORS MAKE NO GUARANTEES OR WARRANTIES AS TO THE ACCURACY, ADEQUACY OR COMPLETENESS OF OR RESULTS TO BE OBTAINED FROM USING THE WORK, INCLUDING ANY INFORMATION THAT CAN BE ACCESSED 1HROUGH THE WORK VIA HYPERLINK OR OTHERWISE, AND EXPRESSLY DISCLAIM ANY WARRANTY, EXPRESS OR IMPUED, INCLUDING BUT NOT LIMITED TO IMPLIED WARRANTIES OF MERCHANTABILITY OR FITNESS FOR A PARTICULAR PURPOSE. McGraw-Hill Education and its licensors do not warrant or guarantee that the functions contained in the work will meet your requirements or that its operation will be uninterrupted or error free. Neither McGraw-Hill Education nor its licensors shall be liable to you or anyone else for any inaccuracy, error or omission, regardless of cause, in the work or for any damages resulting therefrom. McGraw-Hill Education has no responsibility for the content of any information accessed through the work. Under no circumstances shall McGraw-Hill Education and/or its licensors be liable for any indirect, incidental, special, punitive, consequential or similar damages that result from the use of or inability to use the work, even if any of them has been advised of the possibility of such damages. This limitation of liability shall apply to any claim or cause whatsoever whether such claim or cause arises in contract, tort or otherwise.
Preface
Chapter 1 Function and Structure of the Respiratory System
Functions of the Respiratory System I 1
Structure of the Respiratory System I 4
Key Concepts I 11
Suggested Readings I II
Chapter 2 Mechanics of Breathing
Generation of a Pressure Difference Between Atmosphere and Alveoli
Pressure-Volume Relationships in the Respiratory System I 21
Interaction of Lung and Chest Wall: The Static Pressure-Volume Curve
Airways Resistance I 35
The Work of Breathing I 53
Key Concepts I 55
dinical Problems I 55
Suggested Readings I 58
Chapter 3 Alvw=olar Ventilation
The Lung Volumes I 59
Measurement of the Lung Volumes I 62
Anatomic Dead Space and Alveolar Ventilation I 70
Measurement of Alveolar Ventilation I 72
Alveolar Ventilation and Alveolar Oxygen and Carbon Dioxide Levds I 77
Regional Distribution of Alveolar Ventilation I 81
The Closing Volume I 85
The Effects of Aging I 87
Key Concepts I 89
Clinical Problems I 89
Suggested Readings I 92
Chapter 4 Blood Flow to the Lung
The Bronchial Circulation I 95
The Functional Anatomy of the Pulmonary Circulation I 97
Pulmonary Vascular Resistance I 100
The Regional Distribution of Pulmonary Blood Flow: The Zones of the Lung I 107
Hypoxic Pulmonary Vasoconstriction I 1I4
Effects of Mechanical Ventilation on Pulmonary Blood Flow I 1I6
Pulmonary Edema I 1I7
Key Concepts I 120
dinical Problems I 121
Suggested Readings I 122
Chapter 5 Ventilation-Perfusion Relationships 124
The Concept of Matching Ventilation and Perfusion I 124
Consequences of High and Low VJQ I 125
Testing for Nonuniform Distribution oflnspired Gas and Pulmonary Blood Flow I 127
Regional VJQ Differences and Their Consequences in the Lung I 136
Key Concepts I 139
Clinical Problems I 139
Suggested Readings I 141
Chapter 6 Diffusion of Gases and Interpretation of Pulmonary Function Tests 142
Pick's Law for Diffusion I 143
Limitations of Gas Transfer I 145
Diffusion of Oxygen I 147
Diffusion of Carbon Dioxide I 149
Measurement of Diffusing Capacity I 149
Interpretation of Pulmonary Function Tests I 152
Key Concepts I 154
Clinical Problems I 154
Suggested Readings I 156
Chapter 7 Transport of Oxygen and Carbon Dioxide in the Blood 157
Transport of Oxygen by the Blood I 157
Hemoglobin and the Physiologic Implications of the Oxyhemoglobin Dissociation Curve I 160
Influences on the Oxyhemoglobin Dissociation Curve I 164
Transport of Carbon Dioxide by the Blood I 171
The Carbon Dioxide Dissociation Curve I 173
The Bohr and Haldane Effects Explained I 174
Key Concepts I 176
dinical Problems I 176
Suggested Readings I 178
Chapter 8 Add-Base Balance 179
The Chemistry of Acids, Bases, and Buffers I 179
Buffer Systems of the Human Body I 182
Acidosis and Alkalosis I 188
Respiratory and Renal Compensatory Mechanisms I 192
Clinical Interpretation of Blood Gases and Acid-Base Status I 194
The Causes of Hypoxia I 197
Key Concepts I 200
Clinical Problems I 20 1
Suggested Readings I 205
Chapter 9 Control of Breathing
The Generation of Spontaneous Rhythmicity I 207
The Medullary Respiratory Center I 209
The Pontine Respiratory Groups I 211
Spinal Pathways I 211
Reflex Mechanisms of Respiratory Control I 212
Influences of Higher Centers I 217
The Response to Carbon Dioxide I 218
The Response to Hydrogen Ions I 226
The Response to Hypoxia I 227
The Response to Exercise I 227
Key Concepts I 231
dinical Problems I 231
Suggested Readings I 233
Chapter 10 Nonrespiratory Functions of the Lung
Pulmonary Defense Mechanisms I 235
Nonrespiratory Functions of the Pulmonary Circulation I 242
Metabolic Functions of the Lung I 244
Key Concepts I 247
Suggested Readings I 249
Chapter 11 The Respiratory System Under Stress
Exercise and the Respiratory System I 250
Altitude and Acclimatization I 257
Diving and the Respiratory System I 264
Sleep and the Respiratory System I 271
Key Concepts I 273
dinical Problems I 273
Suggested Readings I 278
Appendis.:
I. Symbols used in Respiratory Physiology I 294
II. The Laws Governing the Behavior of Gases I 294
III. Frequently used Equations I 295
IY. Table of Normal Respiratory and Circulatory Values I 296
This page intentionally left blank
Preface
The ninth edition of Pulmonary Physiology has been thoroughly updated. New figures and tables have been added and others revised to help students visualize concepts more clearly and learn the material more effectively. New references and clinical correlations have been added to the end of each chapter. It has been more than 3 5 years since Pulmonary Physiology was first published. The book is now older than most of its readers!
Perhaps the greatest pleasure associated with the first eight editions has been receiving the many favorable comments and helpful suggestions from students, readers, and colleagues, and I have used many of these suggestions in the preparation of this new edition.
This book is intended to be used both as an introductory text for beginning students and as a review for residents and fellows in such fields as iaternal medicine, anesthesiology, pediatrics, and pulmonary medicine. Students who have studied the text should be able to review for licensure and certification examinations by concentrating on the figures, key concepts, tables, a cl appendices, which summarize nearly all of the material in the book.
My goal in writing this book is to provide first-year medical students (as well as respiratory therapy, nursing, nurse-anesthesia, and other students) with a solid background on the aspects of pulmonary physiology essential for an understanding of clinical medicine. My approach is to enrn rage self-sufficiency not only in studying pulmonary physiology fo n d i e first time but also in understanding the basic concepts of pulmonary phxsiology wdl enough to apply them with confidence to future patients.
I believe that the ways o aacomplish this are to inform the reader of the goals of each chapter wi cl early stated learning objectives, to give detailed and complete explanations 0f physiologic mechanisms and demonstrate how they apply to pathologic states, a d to give the reader a means of self-testing by providing clinical correlations, problems, and pulmonary function test data to interpret.
The challenge is to write a book that students can read without difficulty in the limited amount of time allocated to pulmonary physiology in the typical curriculum. The material must be presented in a way that discourages memorization without real comprehension, because only those students who understand the basic mechanisms are able to apply them to new situations. The result of this approach should be a book that covers the essentials of the respiratory system as concisely as possible yet raises no questions in students' minds without answering them. I hope that I have achieved these goals in writing this book.
I would like to thank the many people whose comments have helped me revise the various editions of the book, including my colleagues in respiratory physiology and pulmonary medicine, my colleagues at LSU Health Sciences Center and
Tulane University School of Medicine, and my students and readers. I give special thanks to Drs. Andy Pellett and Usa Harrison-Bernard of Louisiana State University Health Sciences Center and Hershel R.aff of the Medical College of Wisconsin I would also like to thank everyone who has helped me prepare the manuscripts, illustrations, and proofs, including my many editors at McGraw-Hill, Betsy Giaimo, and my wife Elizabeth. This book is dedicated in memory ofRoben S. Alexander and Jim Miller.
Levitzky
G.
Function and Structure of the Respiratory System
OBJECTIVES
The reader states the functions of the respiratory system and relates t e stwctural organization of the system to its functions.
Describes the exchange of oxygen and carbon dioxide with the atmosphere and relates gas exchange to the metabolism of the tissues of '/;je body_
Defines the role of the respiratory system in acid-base balance.
Lists the non respiratory functions of the lungs.
Defines and describes the alveolar-capillary umi, tbe site of gas exchange in the lungs.
Describes the transport of gas through the conducting airways to and from the alveoli.
Describes the structural characteris ics olthe airways.
Lists the components of the ches wall an relates the functions of the muscles of respiration to the movement of air into and out of the alveoli.
Describes the central nervous system initiation of breathing and the innervation of the respiratory muscles.
The main fu nctions of the respiratory system are to obtain oxygen from th'.e external environment and supply it to the cells and to remove from the boay; the carbon dioxide produced by cellular metabolism.
The respiratory system is composed of the lungs, the conducting airways, the parts of the central nervous system concerned with the control of the muscles of respiration, and the chest wall. The chest wall consists of the muscles of respirationsuch as the diaphragm, the intercostal muscles, and the abdominal muscles-and the rib cage.
FUNCTIONS OF THE RESPIRATORY SYSTEM
The functions of the respiratory system include gas exchange, acid-base balance, phonation, pulmonary defense and metabolism, and the handling of bioactive materials.
Gas Exchange
Oxygen from the ambient air is exchanged for carbon dioxide produced by the cells of the body in the alveoli of the lungs. Fresh air, containing oxygen, is inspired into the lungs through the conducting airways. The forces causing the air to flow are generated by the respiratory muscles, acting on commands initiated by the central nervous system. At the same time, venous blood returning from the various body tissues is pumped into the lungs by the right ventricle of the heart. This mixed venous blood has a high carbon dioxide content and a low oxygen content. In the pulmonary capillaries, carbon dioxide is exchanged for oxygen from the alveoli. The blood leaving the lungs, which now has a high oxygen content and a relatively low carbon dioxide content, is distributed to the tissues of the body by the left side of the heart. During expiration, gas with a high concentration of carbon dioxide is expelled from the body. A schematic diagram of the gas exchange function of the respiratory system is shown in Figure 1-1.
Other Functions
ACID-BASE BALANCE
In the body, increases in carbon dioxide lead to increases in hydrogen ion concentration (and vice versa) because of the following reaction:
The respiratory system can therefore participate in base balance by ing C02 from the body. The central nervous system has sensors for the C02 and the hydrogen ion levels in the arterial blood and in the cerebrospinal fluid that send information to the controllers of breathing. balance is discussed in greater detail in Chapter 8; the control of breathing is discussed in Chapter 9.
PHONATION
Phonation is the production of sounds by the movement of air through the vocal cords. Speech, singing, and other sounds are produced by the actions of the central nervous system controllers on the muscles of respiration, causing air to flow through the vocal cords and the mouth. Phonation will not be discussed in detail in this book.
PULMONARY DEFENSE MECHANISMS
Each breath brings into the lungs a small sample of the local atmospheric environment. This may include microorganisms such as bacteria, dust, particles of silica or asbestos, toxic gases, smoke (cigarette and other types), and other pollutants. In addition, the temperature and humidity of the local atmosphere vary tremendously. The mechanisms by which the lungs are protected from these environmental assaults are discussed in Chapter 10.
conductlng airways
Pulmonary artery Veins
High C02 + Right ventricle +Right atrium
Exttlrnal environment
Alveoli
Pulmonary capillaries
High 0 2 Low C02 h eft atrium t Lett vent ride Low C02
Pul monary veins A orta
Systemic capillaries
Metabolizing tissues
Figure 7-J. Schematic representation of gas exchange between the tissues of the body and the environment.
PULMONARY METABOLISM AND THE HANDLING OF BIOACTIVE MATERIALS
The cells of the lung must metabolize substrates to supply energy and nutrients for their own maintenance. Some specialized pulmonary cells also produce substances necessary for normal pulmonary function. In addition, the pulmonary capillary endothdium contains a great number of enzymes that can produce, metabolize, or
modify naturally occurring vasoactive substances. These metabolic functions of the respiratory system are discussed in Chapter 10.
STRUCTURE OF THE RESPIRATORY SYSTEM
Air enters the respiratory system through the nose or mouth. Air entering through the nose is Slrered, heated to body temperature, and humidifled as it passes through the nose and nasal turbinates. These protective mechanisms are discussed in Chapter 10. The upper airways are shown in Figure 10--1. Air breathed through the nose enters the airways via the nasopharynx and through the mouth via the oropharynx. It then passes through the glottis and the larynx and enters the tracheobronchial tree. After passing through the conducting airways, the inspired air enters the alveoli, where it comes into contact with the mixed venous blood in the pulmonary capillaries.
The Airways
After passing through the nose or mouth, the pharynx, and the larynx upper airways), air enters the tracheobronchial tree. Starting with the trachea, the air may pass through as few as 10 or as many as 23 generations, or branchings, on its way to the alveoli. The branchings of the tracheobronchial tree and its nomenclature are shown in Figure 1-2. Alveolar gas exchange units are denoted by the U-shaped sacs.
Figure 1-2. Schematic representation of airway branching in the human lung with approximate dimensions. (Reproduced with permission from Weibel ER: Morphometry of the Human Lung. Berlin: Springer-Verlag; 1963. Data from Bouhuys A: The Physiology of Breathing. New York: Grune & Stratton; 1977.)
The first 16 generations of airways, the conducting zone, contain no alveoli and thus are anatomically incapable of gas exchange with the venous blood. They constitute the anatomic tkad space, which is discussed in Chapter 3. Alveoli start to appear at the 17th through the 19th generations, in the respiratory bronchioles, which constitute the transitional zone. The 20th to 22nd generations are lined with alveoli. These alveolar ducts and the alveolar sacs, which terminate the tracheobronchial tree, are referred to as the respiratory zone.
Respiratory bronchioles have some alveoli, as shown in Figure 1-2. Each respiratory bronchiole branches into about 100 alveolar ducts and 2000 alveoli in the adult human lung. An acinus contains 10 to 12 of these respiratory bronchioles and their branches; they are called terminal respiratory units. All of the airways of an acinus participate in gas exchange. The numerous branchings of the airways result in a tremendous total cross-sectional area of the distal portions of the tracheobronchial tree, even though the diameters of the individual airways are quite small. This can be seen in the table within Figure 1-2.
STRUCTURE OF THE AIRWAYS
The structure of the airways varies considerably, depending on their location in the tracheobronchial tree. The trachea is a fibromuscular tube supported ventrolaterally by Cshaped cartilage and completed dorsally by smooth muscle. The cartilage of the large bronchi is semicircular, like that of the trachea, but as the bronchi enter the lungs, the cartilage rings disappear and are replaced by irregularly shaped cartilage plates. They completely surround the bronchi and give the intrapulmonary bronchi their cylindrical shape. These plates, which help support the larger airways, diminish progressively in the distal airways and disappear in airways about 1 mm in diameter. By deflnition, airways with no cartilage are termed bronchioles. Because the bronchioles and alveolar ducts contain no cartilage support, they are subject to collapse when compressed. This tendency is partly opposed by the attachment of the alveolar septa, containing elastic tissue, to their walls, as seen in Figure 1-3 and shown schematically in Figure 2-18. As the cartilage plates become irregularly distributed around distal airways, the muscular layer completely surrounds these airways. The muscular layer is intermingled with elastic fibers. As the bronchioles proceed toward the alveoli, the muscle layer becomes thinner, although smooth muscle can even be found in the walls of the alveolar ducts. The outermost layer of the bronchiolar wall is surrounded by dense connective tissue with many elastic fibers.
THE LINING OF THE AIRWAYS
The entire respiratory tract, except for part of the pharynx, the anterior third of the nose, and the respiratory units distal to the terminal bronchioles, is lined with ciliated cells interspersed with mucus-secreting goblet cells and other secretory cells. The ciliated cells are pseudostratified columnar cells in the larger airways and become cuboidal in the bronchioles. In the bronchioles, the goblet cells become less frequent and are replaced by another type of secretory cell, the Club cell. dub cells,
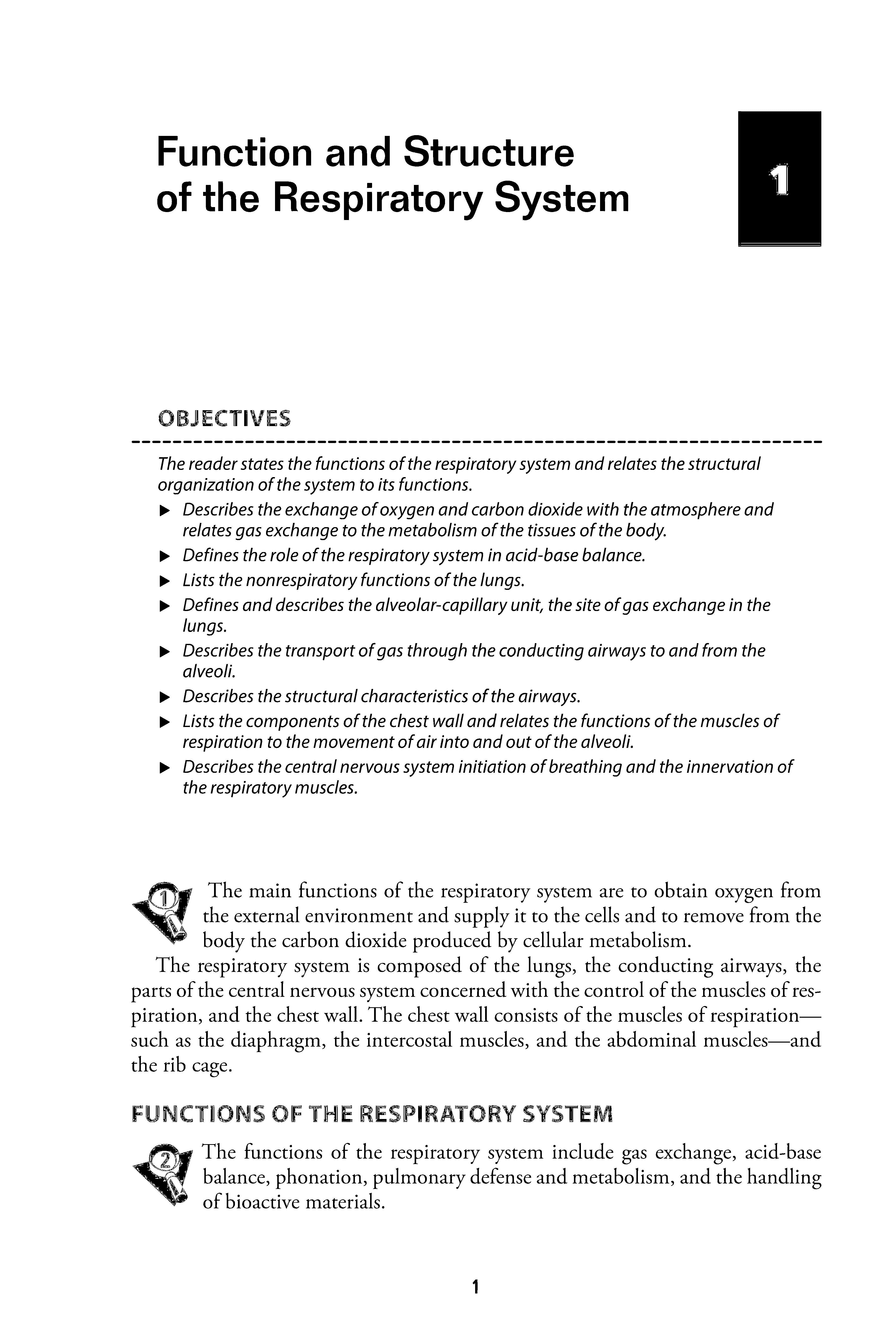
Figure 1-3. Scanning electron micrograph of human lung parenchyma. A = alveolus; S= alveolar septa; D =alveolar duct; PK = pore of Kohn; PA = small branch of the pulmonary artery. (Reproduced with permission from Fishman AP. Kaiser LR, Fishman JA.et al: Pulmonary Diseases and Disorders, 3rd ed. New York: McGraw-Hill; 1998.)
also knmvn as bronchiolar exocrine cells, were called ClaJ:a cells until recendy, when the name was changed because Max Clara, who first characteriz.ed them in 1937, was a member of the Naz.i Party and used tissue from c:n:cuted people in his studies. Oub cdis secrete proteins (including surfactant apoproteins SpA, SpB, and SpDsee Chapter 2), lipids, glycoproteins, and modulators of inflammation. They also
act as progenitor cells for Club cells and for ciliated epithelial cells, metabolize some foreign material, and participate in airway fluid balance. The ciliated epithelium, along with mucus secreted by glands along the airways and the goblet cdls and the secretory products of the dub cells, constitutes an important mechanism for the protection of the lung. This mechanism is discussed in detail in Chapter 10.
Mast celis are also found in the airways. They contain membrane-bound secretory granules that consist of many inflanunatory mediators, including histamine, proteoglycans, lysosomal enzymes, and metabolites of arachidonic acid that can induce bronchoconstriction, stimulate mucus secretion, and induce mucosal edema by increasing permeability of bronchial vessels.
The Alveolar-Capillary Unit
The alveolar-capillary unit is the site of gas exchange in the lung. The alveoli, traditionally estimated to number about 300 million in the adult (a more recent study calculated the mean number of alveoli to be 480 million), are almost completely enveloped in pulmonary capillaries. There may be as many as 280 billion pulmonary capillaries, or approximatdy 500 to 1000 pulmonary capillaries per alveolus. These staggering numbers of alveoli and pulmonary capillaries result in a vast area of contact between alveoli and pulmonary capillaries-probably 50 to 100 m 2 of surface area available for gas exchange by diffusion. The alveoli are about 200 to 250 IJ.m in diameter.
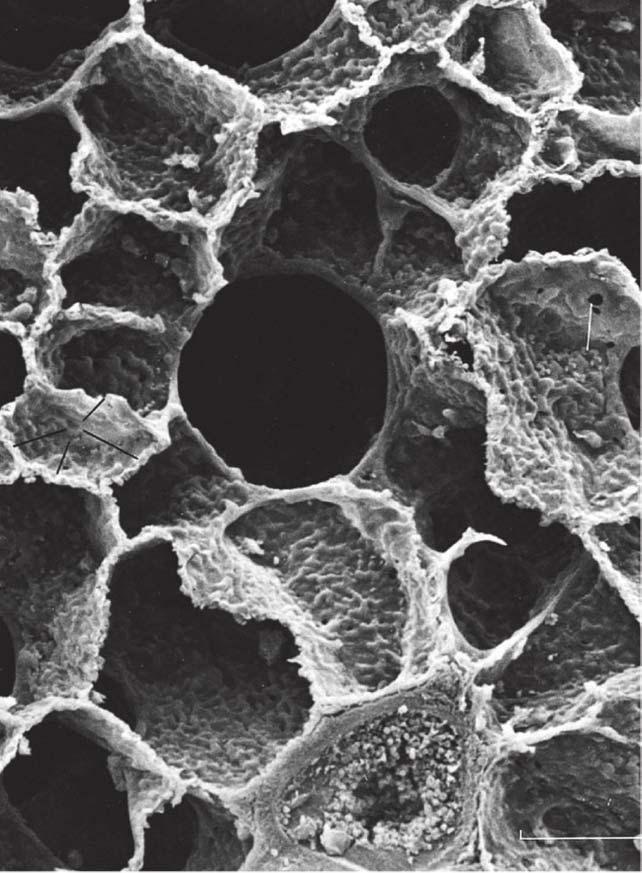
Figure 1-3 is a scanning electron micrograph of the alveolar-capillary surface. Figure 1--4 shows an even greater magnification of the site of gas exchange.
In Figure 1--4 the alveolar septum appears to be almost entirely composed of pulmonary capillaries. Red blood cells (erythrocytes) can be seen inside the capillaries at the point of section. Elastic and connective tissue fibers, not visible in the figure, are found between the capillaries in the alveolar septa. Also shown in these figures are the pores of Kahn or interalveolar communications.
THE ALVEOLAR SURFACE
The alveolar surface is mainly composed of a thin layer of squamous epithelial cells, the type I alveolar cells. Interspersed among these are the cuboidal type II alveolar cells, which produce the fluid layer that lines the alveoli. Although there are about twice as many type II cells as there are type I cdls in the human lung, type I cells cover 90% to 95% of the alveolar surface because the average type I cell has a much larger surface area than the average type II cell does. The thin-walled type I cdls allow most of the gas exchange between the alveolar air and the pulmonary capillary blood; type I alveolar epithelial cells may also help remove liquid from the alveolar surface by actively pumping sodium and water from the alveolar surface into the interstitium.
The alveolar surface fluid layer is discussed in detail in Chapter 2. A third cell type, the free-ranging phagocytic alveolar macrophage, is found in varying numbers in the extracellular lining of the alveolar surface. These cells patrol the alveolar surface and phagocytize inspired particles such as bacteria. Their function is discussed in Chapter 10.
Rgure 7-4. Scanning electron micrograph of the surface and cross section of an alveolar septum. Capillaries (Q are sectioned In the foreground, with erythrocytes (EQ within them. A= alveolus; D =alveolar duct; PK = pore ofKohn; AR =alveolar entrance to duct; • =connective Ussue fibers. The encTrcled asterisk Is at aJunction of 3 septa. The arrows Indicate the edges of a type I alveolar epithelial cell. (Reproduced with permission from Fishman AP, Kaiser LR, Fishman JA,et al: Pulmonary Diseases and Disorders, 3rd ed. New York: McGraw-Hill; 1998.)
THE CAPIUARY' ENDOnfEUUM
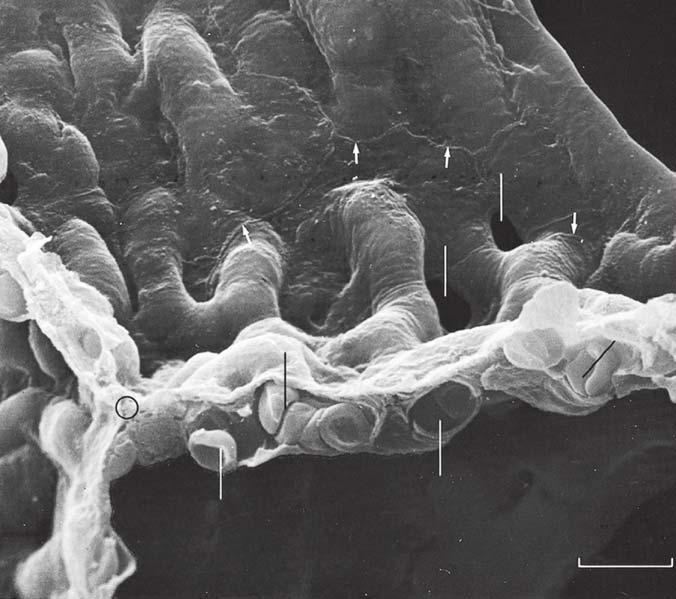
A cross section of a pulmonary capillary is shown in the transmission dcctton micrograph in Figure 1-5. An erythrocyte is seen in cross section in the lumen of the capillary. Capill.aries aze formed by a single layer of squamous epithdial cdls that are aligned to form tubes. The nucleus of one of the capillary endothelial cdls can be seen in the micrograph.
The barrier to gas c:xch.ange between the alveoli and pulmonary capill.aries can also be seen in Figure 1-5. It consists of the alveolar epithelium, the capillary endo· thelium, and the interstitial space between them. Gases must also pass through the fluid lining the alveolar surf.tce (not visible in Figure 1-5) and the plasma in the capillary. The barrier to diffusion is normally 0.2· to 0.5"f.UD. thick. Gas c:u:h.ange by diffusion is discussed in Chapter 6.
Rgure 7-5. Transmission electron micrograph of a cross section of a pulmonary capillary. An eryttlrocyte (EC} is seen within the capillary. C =capillary; EN = capillary endothelial cell (note its large nudeus); EP =alveolar epithelial IN =interstitial space; BM =basement membrane; FB =fibroblast processesi 2, 3,4 =diffusion pathway through the alveolarcapillary banier, the plasma, and the erythrocyte. respectively. Note that the alveolar-capillary barrier appears to have a thin side and a thick side that has a greater interstitial space and more connective tiSji;Ue. (Reproduced with permission from Weibel ER. Morphometric estimation of pulmonary diffusion capadty, I. Model and method. Resplr Physlol. 1970;11 :54-75J
The Muscles of Respiration and the Chest Wall
The muscles of respiration and the chest wall are essential components of the respi· ratory system. The lungs are not capable of inflating themselves-the fura: for this inflation must be supplied by the muscles of respiration. The chest wall must be int:act and able to expand if air is to enter the alveoli normally. The interactions among the muscles of respiration and the chest wall and the lungs are discussed in detail in the nat cb.aptl:r.
Parietal pleura
pleura
Diaphragm
Costodiaphragmatic recess
Figure J-6. The primary components ofthe chest wall. (Reproduced with permission from Fishman AP, Kaiser LR, Fishman JA,et al: Pulmonary Diseases and Disorders, 3rd ed. New York: McGraw-Hill; 1998.)
The primary components ofthe chest wall are shown schematically in Figure 1-6. These include the rib cage; the external and internal intercostal muscles and the diaphragm, which are the main muscles of respiration; and the lining of the chest wall, the visceral and parietal pleura. Other muscles of respiration include the abdominal muscles, including the rectus abdominis; the parasternal intercartilaginous muscles; and the sternocleidomastoid and scalene muscles.
The Central Nervous System and the Neural Pathways
Another important component of the respiratory system is the central nervous system. Unlike cardiac muscle, the muscles of respiration do not contract spontaneously. Each breath is initiated in the brain, and this message is carried to the respiratory muscles via the spinal cord and the nerves innervating the respiratory muscles.
Spontaneous automatic breathing is generated by groups of neurons located in the medulla. This medullary respiratory center is also the final integration point for influences from higher brain centers; for information from chemoreceptors in the blood and cerebrospinal fluid; and for afferent information from neural receptors in the airways, joints, muscles, skin, and dsewhere in the body. The control of breathing is discussed in Chapter 9.
KEY CONCEPTS
The main function of the respiratory system is the exchange of oxygen from the atmosphere for carbon dioxide produced by the cells of the body.
Other functions of the respiratory system include participation in the acid-base balance of the body, phonation, pulmonary defense, and metabolism.
SUGGESTED READINGS
Albertine KH. Anatomy of the lungs. In: Mason RJ, Broaddus VC, Martin TR, et al., eds. Murray & Nwl's Tatboolt ofRlspirrztory Medu:ine. 5th ed. Philadelphia, PA: WB Saunders and Company; 2010:3--25. Bouhuys A TIH Physiology ofBmnhing. New York. NY: Grone & Stratton; 1977:26--42.
Netter FH. The Ciba Coll«#on of MediCid Illustrations, WI/ 7: &spiratory System. Summit, NJ: Ciba; 1979:3--43.
Ocbs M, Nyengaani JR, Jung A, er al. The number of alveoli in the human lung. Am] &spir Crit Med.. 2004;169:120--124.
Ocbs M, Weibel ER. Functional design of the human lung for gas exchange. In: Fishman AP, Flias JA., Fishman JA., Grippi MA. Senior RM, Pack AI, eds. Fislmum} Pulmonary Diseases anti Disorrl=. 4th ed. New York, NY: McGraw-Hill; 2008:23--69.
Ocbs M, Weibel ER. Functional design of the human lung for gas exchange. In: Grippi MA. Elias JA., Fishman JA, Kotloff RM, Pack AI, Senior RM, Siegel MD, eds. Fislmum's Pulmonary Diseaser anti Duordm. 5th ed. New York, NY: McGraw-Hill; 2015:20--62.
Weibel ER. Morphometry ofthe Human Lung. Berlin, Germany: Springer-Verlag; 1963.
Weibel ER. Morphomettic estimation of pulmonary diffusion capacity, I. Model and method. &spir PhyswL 1970;11:54--75.
Weibel ER. lr t:al= more than cells to make a good lung. Am] &spir Grit Qm Med.. 2013;187:342-346.
Weibel ER, Taylor CR. Functional design of the human lung for gas achange. In Fishman AP, Kaiser I.R, Fishman JA, Grippi MA, Senior RM, eds. Pulmonary Diseaser and Disorrl=. 3rd ed. New York, NY: McGraw-Hill; 1998:21--61.
Mechanics of Breathing
OBJECTIVES
The reader understands the mechanical properties of the lung and the chest wall during breathing.
IJJ. Describes the generation of a pressure gradient between the atmosphere and the alveoli.
IJJ. Describes the passive expansion and recoil ofthe alveoli.
IJJ. Defines the mechanical interaction of the lung and the chest wall, and relates this concept to the negative intrapleural pressure.
IJJ. Describes the pressure-volume characteristics of the lung and the chest wall, and predicts changes in the compliance of the lung and the chest wall in different physiologic and pathologic conditions.
IJJ. States the roles ofpulmonary surfactant and alveolar interdependence in the recoil and expansion of the lung.
IJJ. Defines the functional residual capacity (FRO, and uses his or her understanding of lung-chest wall interactions to predict changes in FRC in different physiologic and pathologic conditions.
IJJ. Defines airways resistance and lists the factors that contribute to or alter the resistance to airflow.
IJJ. Describes the dynamic compression ofairways during a forced expiration.
IJJ. Relates changes in the dynamic compliance of the lung to alterations in airways resistance.
IJJ. Lists the factors that contribute to the work of breathing.
IJJ. Predicts alterations in the work of breathing in different physiologic and pathologic states.
Air, like other fluids, moves a region of _higher pressure to one of lower pressure. Therefore, for arr to be moved mto or out of the lungs, a pressure difference between the atmosphere and the alveoli must be established. If there is no pressure difference, no airflow will occur.
Under normal circumstances, inspiration is accomplished by causing alveolar pressure to fall bdow atmospheric pressure. When the mechanics of breathing are being discussed, atmospheric pressure is conventionally referred to as 0 em H 20, so lowering alveolar pressure bdow atmospheric pressure is known as negative-pressure breathing. As soon as a pressure difference sufficient to overcome the resistance to
airflow offered by the conducting airways is established between the atmosphere and the alveoli, air flows into the lungs. It is also possible to cause air to flow into the lungs by raising the pressure at the nose and mouth above alveolar pressure. This positive-pressure ventilation is generally used on patients unable to generate a sufficient pressure difference between the atmosphere and the alveoli by normal negative-pressure breathing. Air flows out of the lungs when alveolar pressure is sufficiendy greater than atmospheric pressure to overcome the resistance to airflow offered by the conducting airways.
GENERATION OF A PRESSURE DIFFERENCE BETWEEN ATMOSPHERE AND ALVEOLI
During normal negative-pressure breathing. alveolar pressure is made lower than atmospheric pressure. This is accomplished by causing the muscles of inspiration to contract, which increases the volume of the alveoli, thus lowering the alveolar pressure according to Boyle's law. (See Appendix II: The Laws Governing the Behavior of Gases.)
Passive Expansion of Alveoli
The alveoli are not capable of expanding themselves. They only expand passively in response to an increased distending pressure across the alveolar wall. This increased transmuralpressure diffirence, generated by the muscles of inspiration, further opens the highly distensible alveoli, and thus lowers the alveolar pressure. The transmural pressure difference is conventionally calculated by subtracting the outside pressure (in this case, the intrapleural pressure) from the inside pressure (in this case, the alveolar pressure).
Negative Intrapleural Pressure
The pressure in the thin space between the visceral and parietal pleura is normally slighdy subatmospheric, even when no inspiratory muscles are contracting. This negatiVI! intrapleural pressure (sometimes also referred to as negative intrathoracic pressure) of -3 to -5 em H 20 is mainly caused by the mechanical interaction between the lung and the chest wall. At the end of expiration, when all the respiratory muscles are relaxed, the lung and the chest wall are acting on each 8;1 other in opposite directions. The lung is tending to decrease its volume because of the inward elastic recoil of the distended alveolar walls; the chest wall is tending to increase its volume because of its outward elastic recoil. Thus, the chest wall is acting to hold the alveoli open in opposition to their elastic recoil. Similarly, the lung is acting by its elastic recoil to hold the chest wall in. Because of this interaction, the pressure is negative at the surface of the 8J very thin (about 10-30 thickness at normal lung volumes), fluidfilled pleural space, as seen on the left in Figure 2-1. There is normally no gas in the intrapleural space, and the lung is held against the chest wall by the thin layer of serous intrapleural liquid, estimated to have a total volume of about 15 to 25 rnL in an average adult.
Atmospheric pressure: 0 em H2 0
No air flow: atmospheric pressure = alveolar pressure
Intrapleural pressure: -Scm H20
Alveolar pressure: Ocm H2 0
Atmospheric pressure: 0 em H20
Air flows In :atmospheric pressure> alveolar pressure ........._
Outward recoilof chest wall
Alveolar pressure: -1 em H2 0
Force generated by / inspiratory muscles
Intrapleural pressure: -8cmH2 0
Transmural pressure = Ocm H20-(-5 em H20) = +5 em H20
End expiration
Transmural pressure= -1 em H20-{-8 em H20) =+ 7 em H2 0
During Inspiration
Figure 2-1. Representation of the interaction of the lung and chest wall. Left: At end expiration, the muscles of respiration are relaxed. The inward elastic recoil of the lung is balanced by the outward elastic recoil of the chest wall. Intrapleural pressure is -5 em Hp; alveolar pressure is 0. The transmural pressure difference across the alveolus is therefore 0 em Hp -{-5 em Hp}, or 5 em Hp. Since alveolar pressure is equal to atmospheric pressure, no airflow occurs. Right: During inspiration, contraction of the muscles of inspiration causes intrapleural pressure to become more negative. The transmural pressure difference increases and the alveoli are distended, decreasing alveolar pressure below atmospheric pressure, which causes air to flow into the alveoli.
Initially, before any airflow occu.rs, the pressure inside the alveoli is the same as atmospheric pressure-by convention 0 em H 2 0. Alveolar pressure is greater than intrapleural pressure because it represents the sum of the intrapleural pressure plus the alveolar elastic recoil pressure:
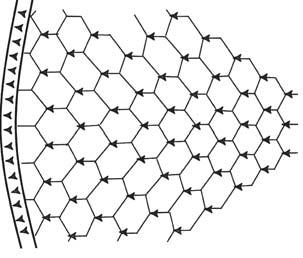
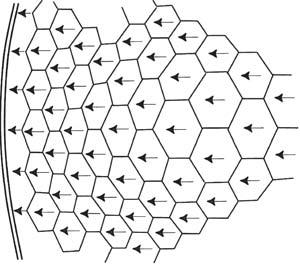
The muscles of inspiration act to increase the volume of the thoracic cavity. The outside of the lung (the visceral pleura) adheres to the inside of the chest wall (the parietal pleura). As the inspiratory muscles contract, expanding the thoracic volume and increasing the outward stress on the lung, the intrapleural pressure becomes more Therefore, the transmural pressure difference tending to distend the alveolar wall (sometimes called the transpulmonary pressure) increases as shown in Figure 2-1, and the alveoli enlarge passivdy. Increasing alveolar volume lowers alveolar pressure and establishes the pressure difference for airflow into the lung. In reality; only a small percentage of the total number of alveoli are directly exposed to the intrapleural surface pressure, and at flrst thought, it is difficult to see how alveoli located centrally in the lung could be expanded by a more negative intrapleural pressure. However, analysis has shown that the pressure at the pleural surface is transmitted through the alveolar walls to more centrally located alveoli and small airways. This structural interdependence of alveolar units is depicted in Figure 2-2.
Note that in Figure 2-1, the inward alveolar elastic recoil calculated by the equation above is equal to the transmural pressure difference. This is true under static conditions, but they may differ slightly during a breath as the alveoli are stretched.
The Muscles of Respiration
INSPIRATORY MUSCLES
The muscles of inspiration include the diaphragm, the external intercostals, and the accessory muscles of inspiration, which include the sternocleidomastoid, the trapezius, and the muscles of the vertebral column.
The Diaphragm-The diaphragm is a large (about 250 cm2 in surface area) domeshaped muscle that separates the thorax from the abdominal cavity. As mentioned in Chapter 1, the diaphragm is considered to be an integral part of the chest wall and must always be considered in the analysis of chest wall mechanics.
The diaphragm is the primary muscle of inspiration. When a person is in the supine position, the diaphragm is responsible for about two-thirds of the air that enters the lungs during normal quiet breathing (which is called eupnea). (When a person is standing or seated in an upright posture, the diaphragm is responsible for only about one-third to one-half of the tidal volume.) It is innervated by the two phrenic nerves, which leave the spinal cord at the third through the fifth cervical segments.
The muscle fibers of the diaphragm are inserted into the sternum and the six lower ribs and into the vertebral column by the two crura. The other ends of these muscle fibers converge to attach to the fibrous cmtra.l tendon, which is also attached
Negative pressure breathing
Positive pressure ventilation (B)
Figure 2-2. Structural Interdependence of alveolar units. The pressure difference across the outermost alveoli is transmitted mechanically through the lung via the alveolar septa. The insets show the author's idea of what might happen in negativepressure breathing and positive-pressure ventilation. In negative-pressure breathing (Inset A) the mechanical stress would likely be transmitted from the more exterior alveoli (those closest to the chest waiD to more interior alveoli, so the exterior alveoli might be more distended. In positive-pressure ventilation (Inset B) the lungs must push against the diaphragm and rib cage to move them. The outermost alveoli might be more compressed than those located more Interiorly.
to the pericardium on its upper surface (Figure During nonnal quiet breathing, contraction of the d.iaplu:agm causes its dome to descend 1 to 2 c.m into the abdominal avity, with little change in its shape. This elongates the thotax: and increases its volume. These small downward movements of the diaphragm are possible beause the abdominal viscera can push out against the relatively compliant abdominal wall. During a deep inspiration, the diaphragm an descend as much as 10 em. With such a deep inspiration, the limit of the compliance of the abdominal wall is reached, abdominal pressure increases, and the indisten.sible central tendon becomes 6.ud against the abdominal contents. After this point, contraction of the d.iaplu:agm against the fixed central tendon elevates the lower ribs (Figure 2-3).