Visit to download the full and correct content document: https://ebookmass.com/product/12-lead-ecg-the-art-of-interpretation-garcia-introducti on-to-12-lead-ecg-ebook-pdf-version/
More products digital (pdf, epub, mobi) instant download maybe you interests ...
Huszar’s ECG and 12-Lead Interpretation 5th Edition
https://ebookmass.com/product/huszars-ecg-and-12-leadinterpretation-5th-edition/
(eTextbook PDF) for Huszar’s ECG and 12-Lead Interpretation 5th Edition
https://ebookmass.com/product/etextbook-pdf-for-huszars-ecgand-12-lead-interpretation-5th-edition/
12-Lead ECG for Acute and Critical Care Providers –Ebook PDF Version
https://ebookmass.com/product/12-lead-ecg-for-acute-and-criticalcare-providers-ebook-pdf-version/
Understanding 12-Lead EKGs (3rd Edition ) 3rd Edition
https://ebookmass.com/product/understanding-12-lead-ekgs-3rdedition-3rd-edition/
Introduction to 80×86 Assembly Language and Computer Architecture – Ebook PDF Version
https://ebookmass.com/product/introduction-to-8086-assemblylanguage-and-computer-architecture-ebook-pdf-version/
The ECG Made Practical 7th Edition John Hampton
https://ebookmass.com/product/the-ecg-made-practical-7th-editionjohn-hampton/
Introduction to Counseling: An Art and Science Perspective – Ebook PDF Version
https://ebookmass.com/product/introduction-to-counseling-an-artand-science-perspective-ebook-pdf-version/
150 ECG Cases (Fifth Edition) John Hampton
https://ebookmass.com/product/150-ecg-cases-fifth-edition-johnhampton/
All Roads Lead to You Jackie Ashenden
https://ebookmass.com/product/all-roads-lead-to-you-jackieashenden-3/
ChapterInReview
Chapter4:TheActualECG:PaperandInk
BoxesandSizes
Calibration
WhereIsEachLeadRepresented?
TemporalRelationshipoftheECG
WhyIsTemporalSpacingImportant?
ChapterInReview
Chapter5:ECGTools
Calipers:TheECGInterpreter’sBestFriend
HowtoUseYourCalipers
ComparingWaveHeights
AddingWaveHeights
ComparingWidths
Axis-WheelRuler
ECGRulers
StraightEdge
Chapter6:TheBasicBeat
IntroductiontoBasicComponents
WaveNomenclature
IndividualComponentsoftheECGComplex
ThePWave
TheTpWave
ThePRSegment
ThePRInterval
TheQRSComplex
TheSTSegment
TheTWave
TheQTInterval
TheUWave
AdditionalIntervals
TheCardiacCycleandComplexFormation
ChapterInReview
Chapter7:TheRate
EstablishingtheRate
NormalandFastRates
BradycardicRates
Let’spracticecalculatingsomerates
Calculatetherates
ChapterInReview
Chapter8:Rhythms
MajorConcepts
General
PWaves
QRSComplexes
IndividualRhythms
SupraventricularRhythms
VentricularRhythms
HeartBlocks
ChapterInReview
PART2:ECGINTERPRETATION
Chapter9:ThePWave
Overview
ECGCaseStudy:PWaveBasics
PWaveMorphology
ECGCaseStudies:PWaveMorphology
AbnormalPWaves
P-mitrale
ECGCaseStudies:P-mitrale
P-pulmonale
ECGCaseStudies:P-pulmonale
IntraatrialConductionDelay(IACD)
ECGCaseStudies:BiphasicPWaves
BiatrialEnlargement
ECGCaseStudies:BiatrialEnlargement
ChapterInReview
Chapter10:ThePRInterval
ConductionOverview
PRDepression
ECGCaseStudy:PRIntervalDepression
MeasuringtheInterval
ShortPRInterval
ECGCaseStudy:ShortPRInterval
Wolff-Parkinson-WhiteSyndrome(WPW)
ECGCaseStudies:WPW
WPWSyndrome AdvancedInformation
ProlongedPRInterval
ECGCaseStudy:ProlongedPRInterval
ChapterInReview
Chapter11:TheQRSComplex
WhattoLookforintheQRSComplex
QRSHeight(Amplitude)
AbnormalAmplitude
ECGCaseStudies:PericardialEffusion
ECGCaseStudy:LargeQRSComplexes
LeftVentricularHypertrophy(LVH)
ElectrocardiogramCriteriaforLeftVentricularHypertrophy
IdentifyingLeftVentricularHypertrophy,StepbyStep
ECGCaseStudies:LeftVentricularHypertrophy
RightVentricularHypertrophy(RVH)
RVHandtheECG
ECGCaseStudies:RightVentricularHypertrophy
QRSDuration
ECGCaseStudies:QRSDuration
TheWide-QRSDifferential,Simplified QRSMorphology
ECGCaseStudies:QRSMorphology
QWaveSignificance
BenignQWaves
RespiratoryVariationofQWaves207
ECGCaseStudies:QWaveSignificance
Significant(Pathological)QWaves
TransitionZone
ECGCaseStudies:TransitionZone
QRSNotching
Osborn(J)Waves
ECGCaseStudies:QRSNotchingandOsbornWaves
ChapterInReview
Chapter12:TheElectricalAxis
HowtoCalculatetheElectricalAxis
IsolatingtheAxis
1
4
5
CausesofAxisDeviation
RightAxisDeviation LeftAxisDeviation
TheZAxis
TheZAxisPrecordialLeadSystem
MoreExamples:AddingtheZAxis
ZAxis:OtherApproaches
ChapterInReview
Chapter13:BundleBranchBlocksandHemiblocks
RightBundleBranchBlock
ECGFindingsinRightBundleBranchBlocks
TheQR′Wave
ECGCaseStudies:RightBundleBranchBlock
LeftBundleBranchBlock
CriteriaforDiagnosingLBBB
ECGCaseStudies:LeftBundleBranchBlock
IntraventricularConductionDelay(IVCD)
SummaryCommentsonBundleBranchBlocks
ECGCaseStudies:IntraventricularConductionDelay Hemiblocks
LeftAnteriorHemiblock
ECGCaseStudies:LeftAnteriorHemiblock
LeftPosteriorHemiblock
ECGCaseStudies:LeftPosteriorHemiblock
BifascicularBlocks
ECGCaseStudies:BifascicularBlock
ChapterInReview
Chapter14:STSegmentandTWaves
Basics
WhereIstheJPoint?
STElevationorDepression
STSegmentShapes
TheTWave
ECGCaseStudies:STSegmentsandTWaves
IschemiaandInjury
ECGCaseStudies:IschemiaandInjury
StrainPattern
RightVentricularStrainPattern
ECGCaseStudies:RightVentricularStrainPattern
LeftVentricularStrainPattern
ECGCaseStudies:LeftVentricularStrainPattern
ECGComparisons:BenignChangesVersusInfarct
PericarditisRevisited
ECGCaseStudies:Pericarditis
STsandTWavesinBlocks
ECGCaseStudies:STsandTsinBlocks
ChapterInReview
Chapter15:AcuteMyocardialInfarction(AMI)
Introduction
ZonesofIschemia,Injury,andInfarction
AcuteCoronarySyndromes
InfarctandQWaves
QWaveInfarct
Non–QWaveInfarct
ECGProgressioninInfarct
ReciprocalChanges
InfarctRegionsontheECG
InfarctRegionsinCombination
AnteriorWallAMI
AnteroseptalMI
ECGCaseStudies:AnteroseptalAMI
AnteroseptalAMIwithLateralExtension
ECGCaseStudies:AnteroseptalAMIwithLateralExtension
LateralWallAMI
ECGCaseStudy:LateralWallAMI
InferiorWallAMI
ECGCaseStudies:InferiorWallAMI
InferolateralAMI
ECGCaseStudies:InferolateralAMI
ApicalAMI
ECGCaseStudies:ApicalAMI
AdditionalECGLeads
PlacingAdditionalRight-SidedLeads
PlacingAdditionalPosteriorLeads
RightVentricularAMI
CriteriaforRightVentricularInfarction
RightVentricularAMI:Summary
ECGCaseStudies:RightVentricularInfarction
PosteriorWallAMI
CarouselPoniesAreBadontheECG
PosteriorWallMI:Summary
ECGCaseStudies:PosteriorWallAMI
ECGCaseStudies:InferoposteriorAMI
ECGCaseStudies:Inferior-RV-PosteriorAMI
Conclusion
ChapterInReview
Chapter16:ElectrolyteandDrugEffects
HyperkalemiaandItsEffects
TheSpectrumofHyperkalemia
TWaveAbnormalitiesinHyperkalemia
ECGCaseStudies:TWaveChangesinHyperkalemia
IVCDandHyperkalemia
PWavesandHyperkalemia
ECGCaseStudies:IVCDandPWavesinHyperkalemia
OtherElectrolyteAbnormalities
Hypokalemia
Hypercalcemia
Hypocalcemia
ECGCaseStudies:OtherElectrolyteAbnormalities
DrugEffects
Digoxin
ECGCaseStudies:DrugEffects
ChapterInReview
Chapter17:PuttingItAllTogether
NewGround
TheQuestionsoftheGram
1.WhatIsMyGeneralImpression?
2 IsThereAnythingThatSticksOut?
3 WhatIstheRate?
4 WhatAretheIntervals?
5 WhatIstheRhythm?
6.WhatIstheAxis?
7 IsThereAnyHypertrophy?
8 IsThereAnyIschemiaorInfarction?
9 WhatIstheDifferentialDiagnosisoftheAbnormality?
10 HowCanIPutItAllTogetherwiththePatient?
TheBigPicture
PART3:TESTECGS
TestECGs
TestECGAnswers
Acronyms
AdditionalReadings Glossary
AuthorAcknowledgments
IwouldliketobeginbythankingallofthoseeducatorsandclinicianswhospentcountlesshoursteachingthespecificsofmedicineItwasthrough yourhardworkandperseverancethatwelearnhowtotreatpatientsYouallowustheprivilegeofbecominghealersBesecureintheknowledge that,justasripplesflowacrossapond,sotheripplesofknowledgethatyouhaveimpartedtousshallcontinueontheirjourneytolightthewayfor futurecliniciansWehopethatwehaveliveduptoyourexpectationsandhavenotletyoudown
Iwouldalsoliketothankallofthecountlessstudents,residents,paramedics,nurses,EMTs,physicianassistants,andtechniciansthathave askeduscountlessquestionsandcontinuallyquestionedourauthorityItisbyansweringyourquestionsthatwehoneourknowledgeandexpand ourabilitiestoteachYouallowustopassontheknowledgethatwehavelearnedandthisis,inouropinion,ourgreatesthonorAlwayscontinue toquestioneveryoneandchallengethe“standard”thinkingofthetime,becausestagnationistheworstthingthatcouldhappentomedicine
IwouldliketothankJones&BartlettLearningforhavingtheforesighttopublishabookthatdoesnotconformtothe“norm”Iwouldespeciallylike toexpressappreciationandheartfeltgratitudetotheeditorsofthefirstedition:TracyFoss,LorenMarshall,andCynthiaMacielKnowles,andthe editorsofthesecondedition:ChristineEmertonandCarolGuerreroTracy,thanksforbelievinginourproposalandforyoursupportthroughout thefirsteditionCarol,thanksforputtingupwiththedailyphonecallsandtheoccasionaltantrumYourinput,daybyday,moldedthisbookintoa realityLoren,yourinsightsandsuggestionswereappreciatedandinvaluableCynthia,yourhardworkandguidancetransformedthemanuscript intoabook.WethankallofJones&BartlettLearningforyourhardworkandfortheblood,sweat,andtearsthatyouhavepouredintoboth editions.
Finally,IwouldliketothankmyfamilyandfriendswhohavesacrificedtimeawaysothatIcouldaccomplishthisachievement.Iknowthatitistime thatwillneverbereplaced.Someofthepricespaidhavebeenhigh.Hopefully,thelivessavedbecauseoftheinformationpassedonwillbesome consolation.Ithankyou,loveyou,andwillbeforeverinyourdebt.
TomasBGarcia,MD
PublisherAcknowledgments
Jones&BartlettLearningandtheauthorwouldliketothankthefollowingpeopleforreviewingthistext
JohnAmtmann,EdD
Professor AppliedHealthScience MontanaTech
Butte,Montana
ReneeAndreeff,MS,MPAS,PA-C
AcademicCoordinator, ClinicalAssistantProfessor PhysicianAssistantDepartment D’YouvilleCollege Buffalo,NewYork
SteveMBanky,AAS,AAS,EMSI,NREMT-P
StartStateCollege NorthCanton,Ohio
EdwardL.Bays,BS,NREMT-P EMSEducationDirector
MountwestCommunity&TechnicalCollege Huntington,WestVirginia
MichaelABelcher,AAS,BS,MHS,NRP
SouthwesternCommunityCollege Sylva,NorthCarolina
VanessaSmithBester,PA-C,MPAS
MEDEXPhysicianAssistantProgram UniversityofWashington
Tacoma,Washington
JodyBullock,BHS,NREMT-P
CoastalCarolinaCommunityCollege Jacksonville,NorthCarolina
DeniseBuonocore,MSN,ACNPC,CCRN
YaleUniversity
NewHaven,Connecticut
AndrewJ.Burke,EMT-P,EMSI,CICP,CCEMTP
ClevelandClinicEMSAcademy Cleveland,Ohio
RichBurns,NREMT-P,TrainingOfficer
BrunswickCommunityCollege Bolivia,NorthCarolina
CandraCarr,MHS,PA-C
MedexNorthwestPhysician AssistantProgram
Seattle,Washington
EdwardPageChandler,RN,Paramedic,BS ForsythTechnicalCommunityCollege Winston-Salem,NorthCarolina
TedChialtas,BA,EMT-P FireCaptain/Paramedic
SanDiegoFireRescueDepartment ClinicalCoordinator EMSTACollege
Santee,California
TerriAllisonDonaldson,DNP,ACNP-BC AssociateProfessorofNursing
Director,DoctorofNursingPracticeProgram
VanderbiltUniversitySchoolofNursing Nashville,Tennessee
WilliamFaust,MPA,NRP GastonCollege Dallas,NorthCarolina
CarlGarrubba
ChathamUniversityPhysicianAssistantProgram Pittsburgh,Pennsylvania
StevenD.Glow,MSN,FNP,RN,EMT-P
MontanaStateUniversity,CollegeofNursing Missoula,Montana
AnnetteGriffin,MSN,RN,MBA
RhodeIslandCollegeSchoolofNursing Providence,RhodeIsland
ChristopherJ.Hafley,Paramedic,EMSI EMSCoordinator EHOVECareerCenter Milan,Ohio
TonjaHartjes,DNP,ACNP/FNP-BC ClinicalAssociateProfessor
AdultGerontologyAcuteCareARNPProgram CollegeofNursing
UniversityofFlorida Gainesville,Florida
LeslieHernandez,MAEd,LP
UniversityofTexasHealthScienceCenter SanAntonio,Texas
MickeyHouston,APRN,MS,ANP-BC,CCRN NorthernArizonaHealthcare Flagstaff,Arizona
CharleneSJansen,BS,MA,EMT-P MineralAreaCollege ParkHills,Missouri
VirginiaH.Joslin,PA-C,MPH
DepartmentofFamilyandPreventiveMedicine EmoryUniversity Atlanta,Georgia
MelissaLefave,DNP(c),MSN,APRN,CRNA UnionUniversity Jackson,Tennessee
MarkMarchetta,BSN,RN,CEN,NRP AultmanHospital Canton,Ohio
AntoinetteAMelton-Tharrett,RN,EMT-P
RussellCountyAmbulanceService Jamestown,Kentucky
J.CoryMiner,EMTP
UniversityofOregon Eugene,Oregon
DariaNapierkowski,DNP,RN,APN,CNE
WilliamPatersonUniversity Stanhope,NewJersey
MatthewOzanich,BSAS,NREMT-P
Faculty,EMSProgram YoungstownStateUniversity Youngstown,Ohio
BrianMPatten,EMT-PI/C
NorthCentralMichiganCollege Petoskey,Michigan
JoAnneM.Pearce,PhDc,MS,RN DirectorofNursingServices
IdahoStateUniversity,CollegeofTechnology Pocatello,Idaho
KimberlyBuffPrado,DNP,APN
UniversityofMedicineandDentistry Chester,NewJersey
TonyL.Ramsey
DirectorofHealthandPublicSafety DavidsonCountyCommunityCollege
Thomasville,NorthCarolina
DeannaLReising,PhD,RN,ACNS-BC,ANEF
IndianaUniversity
Bloomington,Illinois
KerryS.Risco,PhD,CRNP,NP-C,WCC
DepartmentofNursing
SlipperyRockUniversity SlipperyRock,Pennsylvania
KarlaShort,EMT-P,BBA,MEd
ColumbusDivisionofFire Columbus,Ohio
BrendaSloan,RN,MA
IndianaWesleyanUniversity Marion,Indiana
JohnTodaro,BA,NREMT-P,RN,TNS,NCEE
LowcountryRegionalEMSCouncil NorthCharleston,SouthCarolina
WilliamH.Turner,MS,NRP
ParamedicProgramDirector ShawneeStateUniversity Portsmouth,Ohio
J.KeithWilliams,MPAS,PA-C
AssistantProfessor
PhysicianAssistantDepartment NovaSoutheasternUniversity FortLauderdale,Florida
DavidA.Young,MHS,NREMT-P
WesternPiedmontCommunityCollege Marion,NorthCarolina
JosephR.Yow,MA,EMT-P
GuilfordTechnicalCommunityCollege Jamestown,NorthCarolina
DedicationandBiography
IdedicatethisbooktothetwomostwonderfulandamazingpeopleIknow,myMomandDadThankyouforthelove,understanding,support,and toleranceyouhavegivenmethroughouttheyearsYouhavebeenmyinspirationandmyfoundationinlifeAlsotothelightofmylife,myson DanielYouhaveaddedadepthtomylifethatgoesbeyondmerewordsIloveyouandIamproudtobeyourDadFinally,tomysisterSonia, who,fromthetimeIwasborn,wasalwaysthereforme
TomasBGarcia,MD
DrTomasBGarciareceivedhisundergraduatedegreefromFloridaInternationalUniversityWhileapplyingtomedicalschool,DrGarciawas licensedandpracticedasanEMTinthestateofFloridaDrGarciareceivedhismedicaldegreefromtheUniversityofMiami Hecompletedhis internshipandresidencyatJacksonMemorialHospitalinMiami,FloridaandsubsequentlyreceivedboardcertificationinbothInternalMedicine andEmergencyMedicineDrGarciataughtandpracticedintheEmergencyDepartmentsoftheBrighamandWomen’sHospital/Harvard MedicalSchoolinBoston,MassachusettsandGradyMemorialHospital/EmoryMedicalSchoolinAtlanta,GeorgiaHismainareaofinterestis emergencycardiaccareandhelecturesnationallyontopicsrelatedtotheseissues
Foreword
Electrocardiography:TheArtofInterpretation
Ismedicineanartorascience?ThatquestionhasbeenaskedthousandsoftimesinthepastandcontinuestobeaskedtothisdayIthinkthe answerliessomewhereinthemiddleItisbothanartandascienceWeusesciencetogiveussomeobjectiveanswers,drugs,tools,andto provefactsThescienceofmedicinecanbelearnedbyanyoneandrequiresonlyhardworkandperseveranceItistheartofmedicine,however, whichhastobefelt,loved,nurtured,andfinallyacceptedifwearetobecomegoodclinicians
WhenIteachmedicalstudentsphysicaldiagnosis,theyspendthefirstcoupleofweeksmerelyobservingpatientsfromafarTheyarenottotalkto thepatientsortoexaminethemTheironlydutyistoansweronesimplequestion:Isthepatientsickornotsick?Theyonlyhaveabout10to15 secondstomakeuptheirmindssotheycannotrationalizetoomuchTheirdecisionhastobemadefromthegut,basedoninformationthatthey gainedthroughobservationeitherconsciouslyorunconsciouslyItsoundscomplicatedandyetstudentsamazemewithhowquicklytheylearnthis taskandhoweffectivelytheycanputtheselessonstouseThisinternaldecisionmakerisaninnatepartofusallandwillneversteeryouwrong Allwehavetodoistodevelopit
SowhatdoesthishavetodowithECGs?Simple wearegoingtousethesameapproachtolearnelectrocardiography Theonlywaytolearn electrocardiographyistolookatthousandsofECGsandanswerthequestion,“sickornotsick”MostbooksaboutECGsforgetthisonesimple factandinsteadgoonforpagesandpageswritingabouttheECGsandvariationsthatcanbeseen,followedbyoneexampleECGfindingsare notasuniqueasfingerprints,buttheydovaryfrompersontopersonIfyouonlyseeonesampleECGforeachpathologybutneverseethepicture perfectexampleagaininyourlife,youwillneverbeabletodiagnoseit
ThecomplexlanguagethatisusedinelectrocardiographycanbeconfusingandoverwhelmingMostpeoplebuyanadvancedtextbookon electrocardiography,begintoreadit,andthenquicklygiveupSoundfamiliar?Youhavetobeverycompetentatelectrocardiographytobeable tounderstandthewrittenworddescribingthepossiblevariationsThesimplewaytolearnaboutECGsandonethathasbeenlargely underutilizedistoseevariousexamplesandtodevelopafeelforwhatyouarelookingatAfterawhile,youwillbegintofeelyourguttellingyou whetherthepatientis“sickornotsick”TheprocessoflearningtointerpretECGsisnotunlikelearningtothrowaballYoucanreadaboutthe throw,thetrajectories,thespin,andtheaccuracy,butunlessyouseeafewballsthrownandthrowhundredsorthousandsyourself,youwillnever reallylearnknowhowtothrowaballInthesameway,youneedtoseehundredsofECGsbeforeyoubecomecomfortableBythetimeyoufinish thisbook,youwillfeellikeyouarebeginningtounderstandtheterminologyandtheconceptsAfteryourereadthisbook,youwillfeelvery comfortable
YouneedtorememberthatspecificfindingscanrepresentvariousdiseaseprocessesFromthatlistofpotentialdiseases,youwilldevelopalist ofdifferentialdiagnosesforeachproblemfoundontheECGWewillteachyouhowtodiagnosebiatrialenlargement,rightventricular hypertrophy,andright-sidedstrainWewillgiveyouthebackgroundnecessarytodiagnoseseveremitralstenosis,butitwillbeuptoyoutotalkto thepatientandtoexaminethemtodetermineifthisisanaccuratediagnosisThisisbecauseyouneedreal-timeinterpretationandareallive patienttobecompletelycorrectwhenyouinterpretanECGForexample,itisdifficultsometimestointerpretmildSTsegmentelevationinV1 andV2inapatientwithhypertensionIsitleftventricularhypertrophy(LVH)withstrainorisitaninjury?TherearecertaincriteriaforLVHwith strain,butoccasionallythisisnotasclear-cutasitmayseemWell,theanswerismadesimplerifyouhavethepatientinfrontofyouIfthepatient isvisitingyoubecausetheystubbedtheirtoe,it’sprobablyLVHwithstrainIfthepatientisdiaphoreticandclutchinghischest,thediagnosismost likelywouldbeischemiaandinjuryThiscanalsoworkinreverse,ie,anECGcanguideyourexamanddiagnosisTherehavebeenmanytimes whenIhavebeenshownanECGandIhavetoldthecliniciantogobackandpickupsomeinterestingfindingonphysicalexaminationAgood exampleisaventricularaneurysmTheECGwillinformyouofthepresenceoftheaneurysmandtheaneurysmalheaveonphysicalevidencewill confirmdiagnosis
WhenyouinterpretECGs,youhavetobeabletoputtheknowledgethatyouhavegainedfrominterpretationoftheECGandtranslateittoyour patientAlloftheECGsinthisbookwereobtainedfromrealpatientsTheinterpretationsthatwewillofferaretheinterpretationswemadebythe patients’bedsidesYoucandisagreewithsomeofthemandthat’sokayTherearealotofhardandfastrulesinelectrocardiography,buthowyou interpretanECGwilldependonhowyouweretaughtandyourmoodatthetimeyouinterprettheECGYoucanask20cardiologiststheir opinionsonanECGandyouwouldprobablygetalotofdifferentanswersIfyoushowthemthesameECGthenextday,youwouldprobablyget moredifferentinterpretationsfromthesamegroupWhenitcomestointerpretation,peoplejustdon’tseemtoagreeonmuchThekeyisto understandtheconceptswearetryingtoofferyousothatyoucanusetheminyoureverydaypracticeAnECGwillofferyouawealthof knowledgeaboutapatientItcantellyouabouttheirpastandtheirfuture(prognosis)Itcantellyouabouttheirelectrolyteproblems,systemic illnesses,andtheiranatomyNotbadforasimplebedsidetest
Ihavebeenaskedbyafewhundredstudentstoteachthemwhattheyreallyneedtoknow.Icansumuptheanswerinoneshort,concise statement:YouneedtoknowthechangesthatyourspecificpatientpresentedyouontheirECG!Youneverknowwhatwillbeimportantatanyone pointinyourcareer;anyonefactcancostthepatienttheirlifeandwillcostyoucountlesshoursofguilt,andpossiblymillionsofdollars! ElectrocardiographicinterpretationisthesamewhetheranEMT,paramedic,nurse,resident,attendingphysician,orcardiologistperformsit.You cannotlearnjustenoughtogetby.Doesaparamedicoranurseneedtoknowthechangesofhyperkalemiathatcanleadtoalethalarrhythmia? Doesaresidentneedtoknowthatanaxisshiftcanbeasignificantsignofcardiacdiseaseorofaheartattack?Towhomisitmoreimportantto knowthatanacutebifascicularblockbreaksdownintocompleteheartblockandpossiblyasystoleinthesettingofischemia?Itisimportantto you!
Wearegoingtohelpyouunderstandthebasicsofelectrocardiography,thescienceWearegoingtoteachyouusingaprogrammedlearning systemthat,wefeel,willmakeiteasyforyoutolearnatyourownpaceDon’ttrytodoeverythingatonce,becauseitwilloverwhelmyouWhen youarefirststartingout,sticktotheLevel1(blue)material,whichcontainsthebasicteachingpointswrittenforbeginners(seepiv,HowtoUse ThisBook)Asyouadvance,youcangobackandreadthemoreintermediateandadvancedteachingpointsatyourownpaceThisisabook thatismeanttobeusedoverandoveragainuntilyouhaveprogressedthroughallthreelevelsEachtimeyouuseityouwillfindsomeadditional pearls
Inclosing,IwouldliketostatethatyouneedtolookateverythingatyourdisposalandtrustyourselfwhenyouareinterpretinganECG Don’tlet anyonetalkyououtofsomethingthatyouknowistrue JustsmileatthemanddowhatisbestforthepatientYouwillnotgowrong RememberthatanexpertissomeonewhoknowsonemorefactthanyoudoHowever,thatonefactmaynotberelevanttoyourcasesoyoumay bethetrueexpert!
PART1
TheBasics
Part1coversECGbasicsMostoftheboxesarepresentedasLevel1materialAnyonedealingwithECGsshouldbeextremelyfamiliarwiththe informationinthispartIfyouareanexperiencedclinician,youcanskimovertheinformationbutshouldnotskipoveritcompletelyMakesurethat youunderstandthematerialthoroughlybeforegoingontoPart2
NOTE
PediatricelectrocardiographyisnotcoveredinthistextbookduetotheextensiveamountofmaterialrequiredtocoverthistopicThereaderis referredtoatextbookonthespecificsubjectofpediatricelectrocardiography
HowtoReadanECG
ThemajorityofthisbookisgearedtowardbreakingdownthevarioussectionsoftheECGanditscomplexesThechaptersteachyouwhateach partoftheECGrepresentsandtherespectiveabnormalitiesEachsectioncoversthepathologyassociatedwithawaveorintervaloftheECGby usingaproblems-orientedapproachthatconsistsofexaminingthelistofpossiblecausesforapathologicalwaveorintervalanddetermininghow theserelatetotheothercomplexesThislistofpossiblecausesiscalledthedifferentialdiagnosis
AsyoureviewtheECG,lookateachwaveandintervalandcreatelistsofabnormalitiesthatyoufindinthemYouwillthenhaveseverallistsFind outwhatdiseasesorsyndromesarecommontoallofthoselists;thatdiseaseorsyndromewillbe,withalmostcompletecertainty,thediagnosis Beforeyoustartthebook,wewouldliketoofferthefollowingstepstoguideyouinECGinterpretationThesestepswillbecomesecondnature afterreviewanduseDon’tworryifyouareunfamiliarwithsomeoftheterminology youwillbecomefamiliarwithitwhenyoureadthechapters ThemostimportanttasknowistodevelopalogicalapproachtoexaminingandinterpretingtheECGYoucanadjustthissystem,asyouneedto, tomatchyourparticularstyle
1. Getageneralimpressionofwhatisgoingonandkeepitforemostinyourmind.
LookattheECGforafewsecondsandseewhatstrikesyouasthemostimportantdetailIsitischemia,arrhythmia,electrolyteproblems,pacer
problems,orsomethingelse?Don’tletthedetailsoverwhelmyou instead,formthebigpicturefirstandkeepitinyourmindasyoumoveonto interprettheECGEventually,youwilllearnhowtobreakdowntheECGandmethodicallyderiveaninterpretation
2 LookattheECGsequentiallyandinminutedetail
ThisisthesecondconceptthatinvolvesallofthestepsbelowWhenstartingout,trytouseanECGthatcontainsarhythmstripatthebottomthat correlateswiththeleadsabove itwillmakeyourlifemucheasierLookatthebeatsIftheylookdifferent,breakthemdownandfigureoutwhich arethenormalbeatsandwhicharetheabnormalbeatsLookatthenormalbeatsfirsttodetermineyourintervals,axis,blocks,etcThenlookat theabnormalbeatsandfigureoutwhatiscausingthemAretheyPACs,PVCs,aberrantconduction,pacedbeats,orsomethingelse?
3. Whatistherate?
• Isitfastorslow?
• Ifitisirregular,whatistherange?
• Whataretheintervals:PR,QRS,QTc,PP,RR?
• Arethereirregularitiesinanyoftheintervals,forexample,PRdepression?
4 Whatistherhythm?
• Isitfastorslow?
• Regularorirregular?
• Groupedorungrouped?
• CanyouseePwaves?Aretheyallthesame?
• Isthereone-to-oneconductionofthePwavestotheQRScomplexes?
• Wideornarrow?
5 Whatistheaxis?
• Whatquadrantdoesitfallinto?
• Whatistheisoelectriclimblead?
• Whereisthetransitionzoneintheprecordials?
• Calculatetheexactaxis(AdvancedcliniciansshouldalsocalculatetheP,T,andSTaxes)
• Doestheexactaxistellyouanything?
6. Isthereanyevidenceofhypertrophy?
• Leftatrial?
• Rightatrial?
• Biatrial?
• Leftventricular?
• Rightventricular?
• Biventricular?
• Leftorrightstrainpattern?
7. Isthereanyevidenceofischemiaorinfarction?
• ArethereregionalTwaveabnormalities?
• ArethereregionalSTsegmentabnormalities?•ArethereregionalQwaves?
8 HowcanIputitalltogether?
ThinkofallthefindingsandtrytocomeupwithacommonthemetothedifferentialdiagnosisthatyouhavedevelopedThinkofeverythingand overlooknothingBesuretoconsidertherate,rhythm,axis,hypertrophy,intervalabnormalities,blocks,andSTandTwaveabnormalities
9. CanIputitalltogetherwithmypatient’ssignsandsymptoms?
DothediagnosisandfindingsontheECGmakesensewiththepatient’spresentingsignsandsymptoms?CantheECGbeapresentationofa problemorthecauseofsomepre-existingcondition?Askyourself,“HowcanIusetheinformationtoadequatelytreatthepatient?”
10 Whatismyfinaldiagnosis?
Listyourfinalsinglediagnosisoryourabbreviatedlistofdifferentialdiagnoses
Inclosing,don’tforgetthatittakestimetolearntointerpretECGsSomeoftheconceptswementioninthelistabovemaybeaboveyourlevel now,butnotforlong!Themoreyouusethebook,thebetteryouwillbecomeLastly,havefun!Lifeisshort
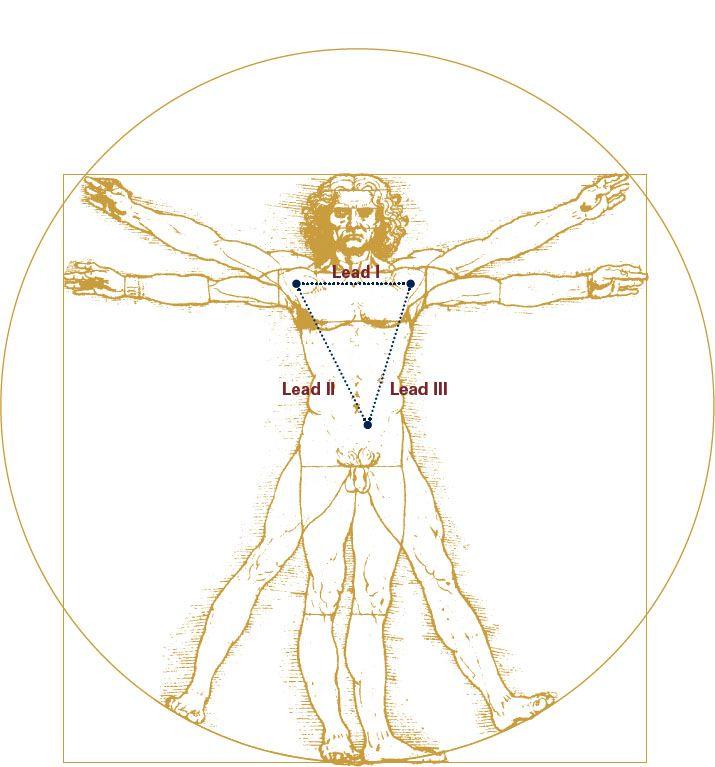
GrossAnatomy
SinceyouarelearningECGinterpretationyoulikelyarealreadyfamiliarwithbasicanatomyHowever,areviewisneverabadthing,soweare goingtocoverthebasicanatomyoftheheartandthenconcentrateontheelectricalconductionsystem
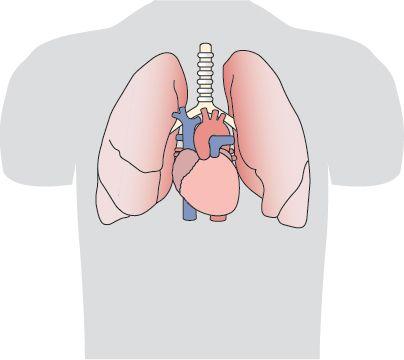
Theheartsitsinthemiddleofthechestataslightanglepointingdownward,totheleft,andslightlyanteriorTakealookatFigure1-1
Now,let’slookattheheartitselfFirst,fromananteriorview,andthenincross-section
Figure1-1:Locationoftheheartinthechestcavity
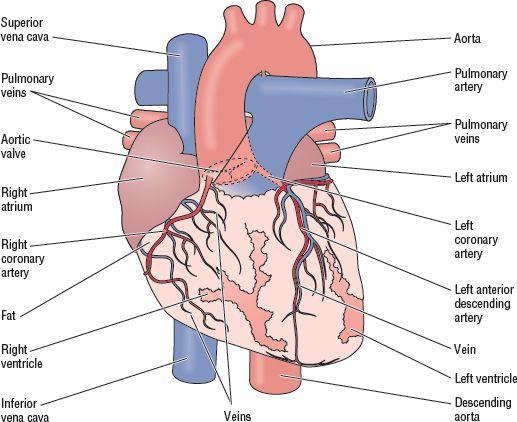
AnteriorView
Therightventricle(RV)dominatestheanteriorview.MostoftheanteriorsurfaceoftheventriclesconsistsoftheRVsurface.Akeypointto rememberisthat,thoughtheRVdominatesthisvisualview,theleftventricle(LV)dominatestheelectricalview.Wewillreviewthisinmoredetail inthechapter,IndividualVectors,whenwediscussvectors
Figure1-2:Anteriorviewoftheheart
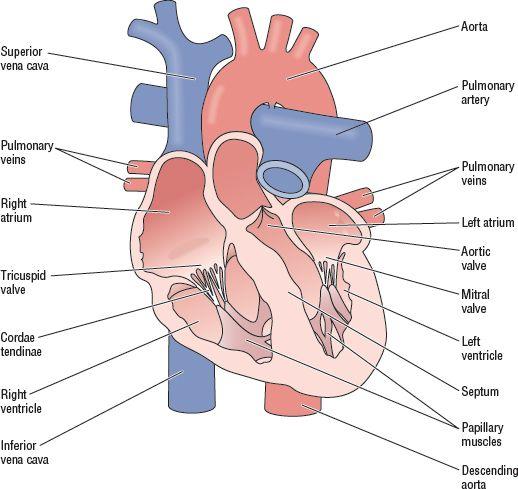
TheHeartinCrossSection
Hereisacross-sectionalviewoftheheart(Figure1-3)Inthefollowingsections,wewillcoverthefunctionoftheheartasapumpandreviewthe electricalconductionsystemingreaterdetail
Figure1-3:Cross-sectionalviewoftheheart
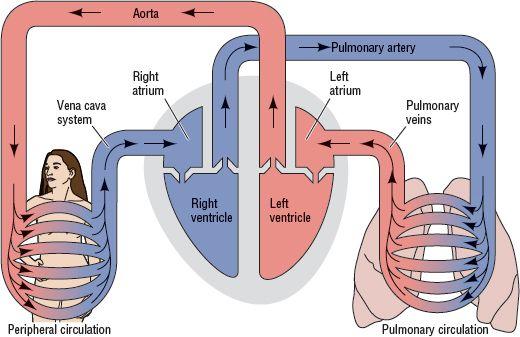
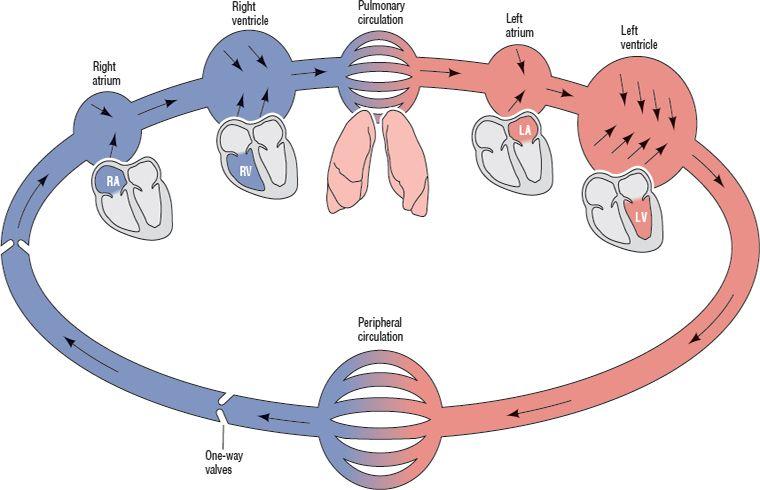
TheHeartasaPump
Theheartconsistsoffourmainchambers:thetwoatriaandthetwoventriclesTheatriaemptyintotheircorrespondingventriclesTheleft ventricleemptiesintotheperipheralcirculatorysystem,andtherightventricleemptiesintothepulmonarysystemVeinsbringbloodtotheheart, whilearteriestakebloodawayfromtheheartAsFigure1-4shows,thisisaclosedsystemBloodcirculatesinsidethisclosedsystemoverand over,takingupoxygeninthelungsandgivingituptotheperipheraltissuesThisisasimplisticexplanationofaverycomplicatedsystem,butit willsufficeforourpurposesatthistime
Figure1-4:Theheartasapump
PumpFunctionSimplified
Itissimplesttothinkofthecirculatorysystemasanengineerwould:asystemofinterconnectedpumpsandpipes
TakealookatFigure1-5
WeseethattherearefourpumpsinsequenceThetwosmallprimerpumpsaretheatria,whosesolepurposeistopushasmallamountofblood intothetwolargerones,theventriclesTheventriclesdifferinsizeandintheamountofpressurethattheycangenerateBecauseoftheone-way valvesfoundinthevenoussystem,bloodcanonlyflowforward
Figure1-5:Simplifiedpumpfunctionofthecirculatorysystem(Bluerepresentsdeoxygenatedblood;redrepresentsoxygenatedblood)
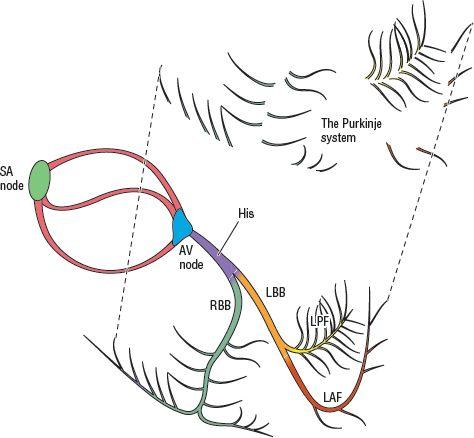
TheElectricalConductionSystem
TheelectricalconductionsystemoftheheartismadeupofspecializedcellsSomeofthesearespecializedforpacemakingfunctionsandsome forthetransmissionoftheimpulsesthattravelthroughthemWewillbreakdownthesysteminthefollowingparagraphsanddescribethe functionsofeachofthepartsingreaterdetail
ThemainfunctionofthesystemistocreateanelectricalimpulseandtransmititinanorganizedmannertotherestofthemyocardiumThisisan electrochemicalprocessthatcreateselectricalenergythatispickedupbytheelectrodeswhenweperformanelectrocardiogram(ECG)(More onthisinthechapter,IndividualVectors)
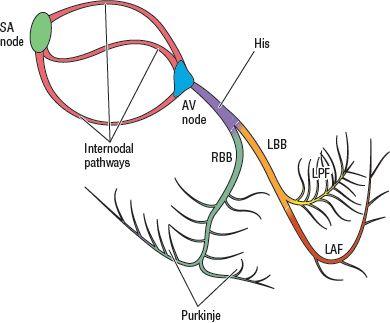
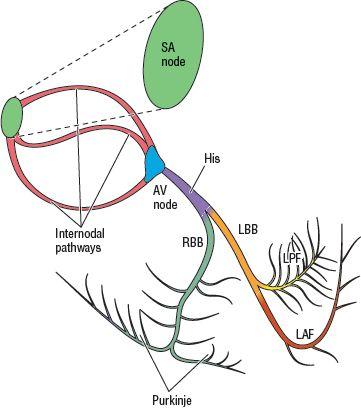
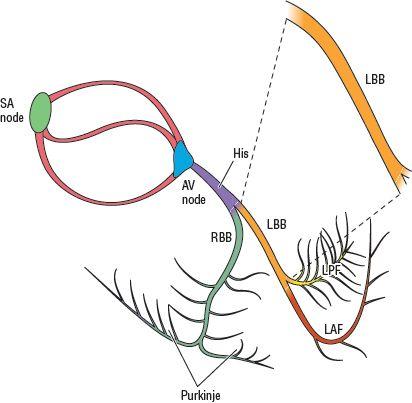
Figure1-6:Theelectricalconductionsystem
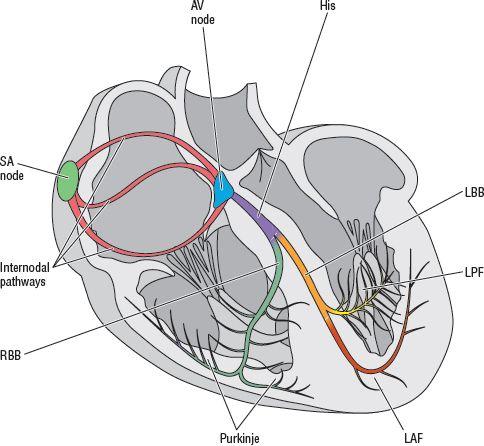
Thespecializedconductionsystemisinterwovenwiththemyocardialtissueitselfandisonlydistinguishablewithcertainstainsundera microscopeSoinlookingatFigure1-7,keepinmindthatthesystemisactuallyintheheartwallsTheatrialmyocytesareinnervatedbydirect contactfromonecelltoanother;thefirstcellinnervatesthesecond,thesecondinnervatesthethird,andsoonTheinternodalpathwaystransmit theimpulsefromthesino-atrial(SA)nodetotheAVnodeThePurkinjesystemencirclestheentireventricles,justundertheendocardium,andis thefinalcomponentoftheconductionsystemThePurkinjecellsinnervatethemyocardialcellsthemselves
Figure1-7:Theelectricalconductionsystemoftheheart
PacemakerFunction
Whatisthepacemakerfunctionoftheheart,andwhydoweneedit?Thepacemakerdictatestherateatwhichtheheartwillcyclethroughits pumpingactiontocirculatethebloodThepacemakercreatesanorganizedbeatingofallofthecardiaccells,inaspecializedsequence,to produceeffectivepumpingactionItsetsthepacethatalloftheothercellswillfollowLet’slookatananalogy
ImaginethateachcelloftheheartrepresentsasinglemusicianWhenwehaveafewdozenofthesemusicians,wehaveanorchestra the heartNow,ifeachmusiciandecidestoplaywheneverheorshewantsto,theywouldmakeanunrecognizablejumbleofsoundThemusicians needabeatorsignaltocuethemwhentostarttoplay,directthemwhentocomeintothepieceandwhentoleave,andcoordinatetheiractionsto createabeautifulmelodyInmusic,thatpacemakeristheunderlyingbeatkeptbythedrummerortheconductorInsectionsthatareswift,the beatincreasesInsectionsthatareslowandsoft,thebeatdecreasesThesamethinghappensintheheart;duringexercisethepacespeedsup, andduringrestitslows
Aswehavementioned,therearespecializedcellswhosefunctionistocreateanelectricalimpulseandactastheheart’spacemakerThemain areathatfillsthisimportantfunctionistheSAnode,foundinthemuscleoftherightatriumThisarearespondstotheneedsofthebody, controllingthebeatbasedoninformationitreceivesfromthenervous,circulatory,andendocrinesystemsThemainpacemakerpacesatarate of60to100beatsperminute(BPM),withanaverageof70
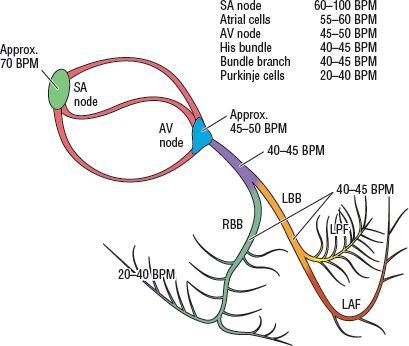
PacemakerSettings
Onethingweknowaboutthebodyisthateverythinghasabackup.Everycellintheconductionsystemiscapableofsettingthepace.However, theintrinsicrateofeachtypeofcellisslowerthanthecellsthatprecedeit.ThismeansthatthefastestpaceristheSAnode,thenextfastestisthe AVnode,andsoon.Thefastestpacersetsthepacebecauseitcausesalltheonesthatcomeafterittoresetaftereachbeat.Inthisway,the slowerpacerswillneverfire.Ifthefasterpacerdoesn’tfireforsomereason,thenextfastestwillbethereasabackuptoensurefunctionthatisas closetonormalaspossible.
Figure1-8:Intrinsicratesofpacingcells
TheSinoatrial(SA)Node
TheSAnode,theheart’smainpacemaker,isfoundinthewalloftherightatriumatitsjunctionwiththesuperiorvenacavaItsbloodsupplycomes
fromtherightcoronaryarteryin59%ofcasesIn38%,thebloodsupplyoriginatesfromtheleftcoronaryartery,andinthelast3%,itarisesfrom both
Figure1-9:SAnode
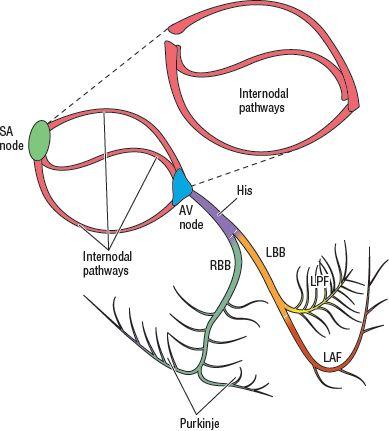
TheInternodalPathways
Therearethreeinternodalpathways:anterior,middle,andposterior.TheirmainpurposeistotransmitthepacingimpulsefromtheSAnodeto theAVnode.Inaddition,thereisasmalltractofspecializedcellsknownastheBachmannbundlethattransmitstheimpulsesthroughtheinteratrialseptumAllofthesepathwaysarefoundinthewallsoftherightatriumandtheinter-atrialseptum
Figure1-10:Internodalpathways
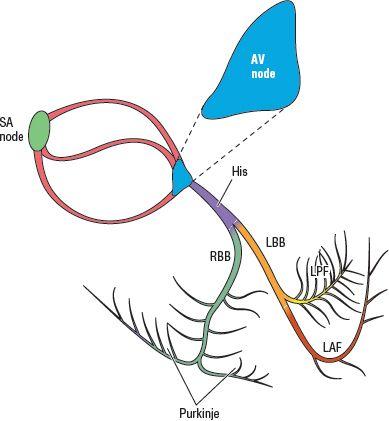
TheAtrioventricular(AV)Node
TheAVnodeislocatedinthewalloftherightatriumjustnexttotheopeningofthecoronarysinus,thelargestveinoftheheart,andtheseptal leafletofthetricuspidvalveItisresponsibleforslowingdownconductionfromtheatriatotheventriclesjustlongenoughforatrialcontractionto occurThisslowingallowstheatriato“overfill”theventriclesandhelpsmaintaintheoutputoftheheartatamaximumlevelTheAVnodeisalways suppliedbytherightcoronaryartery
AVnode
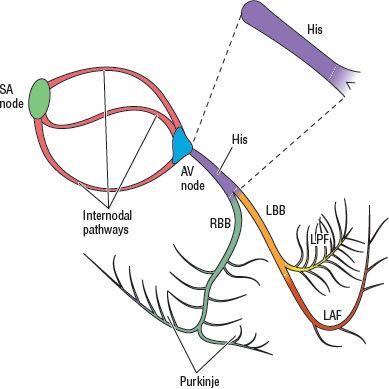
TheBundleofHis
TheBundleofHisstartsattheAVnodeandeventuallygivesrisetoboththerightandleftbundlebranchesItisfoundpartiallyinthewallsofthe rightatrium,andintheinterventricularseptumTheHisbundleistheonlyrouteofcommunicationbetweentheatriaandtheventricles
Figure1-12:BundleofHis
TheLeftBundleBranch(LBB)
TheleftbundlebeginsattheendoftheHisbundleandtravelsthroughtheinterventricularseptumTheleftbundlegivesrisetothefibersthatwill innervatetheLVandtheleftfaceoftheinterventricularseptumItfirstconnectstoasmallsetoffibersthatinnervatetheuppersegmentofthe interventricularseptumThiswillbethefirstareatodepolarize,meaningthattheheart’scellsfireTheleftbundleendsatthebeginningoftheleft anterior(LAF)andleftposteriorfascicles(LPF)
Figure1-11:
Figure1-13:Leftbundlebranch(LBB)
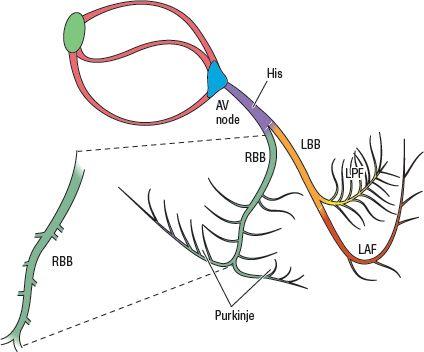
TheRightBundleBranch(RBB)
Therightbundle,whichalsostartsattheHisbundle,givesrisetothefibersthatwillinnervatetheRVandtherightfaceoftheinterventricular septumItterminatesinthePurkinjefibersassociatedwithit
Figure1-14:Rightbundlebranch(RBB)
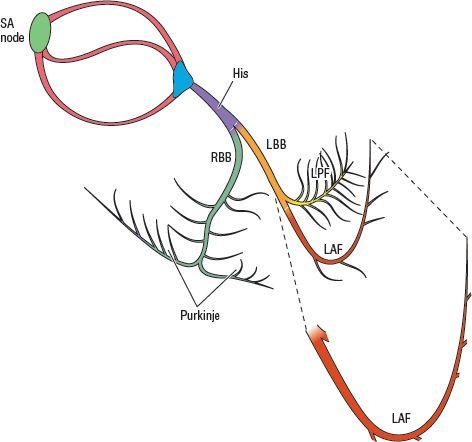
TheLeftAnteriorFascicle(LAF)
TheLAF,alsoknownastheleftanteriorsuperiorfascicle,travelsthroughtheleftventricletothePurkinjecellsthatinnervatetheanteriorand superioraspectsoftheleftventricleItisasingle-strandedfascicle,incomparisontotheLPF
Figure1-15:Leftanteriorfascicle(LAF)
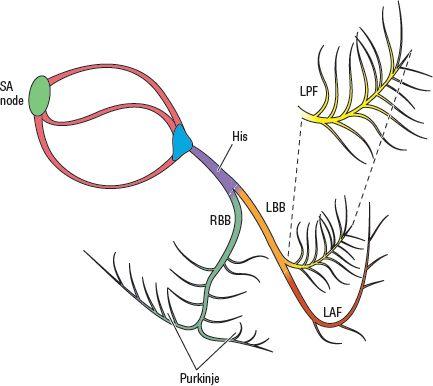
TheLeftPosteriorFascicle(LPF)
TheLPFisafan-likestructureleadingtothePurkinjecellsthatwillinnervatetheposteriorandinferioraspectsoftheleftventricle.Itisverydifficult toblockthisfasciclebecauseitissowidelydistributed,ratherthanbeingjustonestrand.
Figure1-16:Leftposteriorfascicle(LPF)
ThePurkinjeSystem
ThePurkinjesystemismadeupofindividualcellsjustbeneaththeendocardium.Theyarethecellsthatdirectlyinnervatethemyocardialcellsand initiatetheventriculardepolarizationcycle.
Figure1-17:Purkinjesystem.
REMINDER
Sothatthepathologythatwewillpresentintherestofthebookcanbeunderstood,itiscriticaltounderstandtheheart’selectricalconduction systemThispathologycoversaberrantlytransmittedbeats,bundleblocks,fascicularblocks,AVblocks,andrhythmdisturbancesWesuggestat thispointthatyougobackoverthesystemafewtimesuntilyouarefamiliarwithitscomponentsandthewaythatthepacedelectricalimpulse travelsthroughtheheart
ThisismeanttobeacursoryreviewofcardiacandconductionsystemanatomyWewillspendmoretimeonvariousaspectsofthesystemaswe discusstheindividualpathologicstatesForamoreextensivereviewofthesubject,trythebooksmentionedintheAdditionalReadingssection
CHAPTERINREVIEW
1. Visually,therightventricledominatestheanteriorviewoftheheart.TrueorFalse.
2 TherightventriclepumpsthebloodthroughtheperipheralcirculationTrueorFalse
3. Whichofthestatementsbelowisincorrect:
A Theelectricalconductionsystemoftheheartismadeupofspecializedcells
B. Theconductionsystemisinterwovenintothemyocardialtissue
C. Theconductionsystemisvisibleunderthemicroscopewithoutspecialstains
D TheinternodalpathwaystransmittheimpulsebetweentheSAnodeandtheAVnode
Matchthefollowingcorrectly:
4. SAnode
5 Atrialcells
6. AVnode
7. Hisbundle
8. Purkinjecells
9. Myocardialcells
10. TheAVnodeisalwayssuppliedby:
A Theleftanteriordescendingartery
B. Theposteriordescendingartery
C Therightcoronaryartery
D. Theleftcircumflexartery
E. Thefirstdiagonalartery
40–45BPM
30–35BPM
60–100BPM
20–40BPM
55–60BPM
45–50BPM
Whydoyouneedtoknowaboutthegenerationofelectricalactivityinacellandtheeffectofelectrolytesontheelectrocardiogram(ECG)?
BecausebeforeyoucanunderstandwhatanECGdoes,youneedtoknowhowitgetsitsinformationElectrolytesarethemeansbywhichthecell develops“electricity”Youalsoneedtoknowaboutelectrolytesbecauseimbalancescancauselife-threateningproblemsForexample,ifyou knewthatpeaked,sharpTwaveswereasignofhyperkalemia(elevatedpotassium),orthataprolongedQTintervalcouldbeasignof hypocalcemiaorhypomagnesemia,youmightavertaseriousarrhythmiaIttakesonlyminutesinsomecasestogofrompeakedTwavesto asystole(Bytheway,pacersdonotworkinhyperkalemia!)AlittleknowledgeaboutelectrolytesandtheireffectsontheECGpatternscansave thepatient andyou
TounderstandwhytheECGisalteredbyanelectrolyteabnormality,wewillreviewthewayinwhichthemyocardialcellbecomespolarizedand depolarized,andthebiochemicalmechanismsthatallowthecelltocontractWewilltrytomaketheconceptsaspainlessaspossible,sobear withusThisisintendedtobeonlyaverybasicdiscussionofthetopic,whichyoucansupplementwithagoodphysiologytextbookasneeded
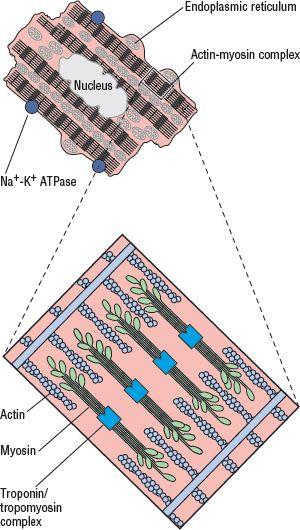
MechanicsofContraction
Imaginethattheheartismadeupofaseriesofsmallbarrelsorcells(Figure2-1)Eachofthesebarrelsismadeupoftwohalvesthatslideover eachotherandareheldtogetherbyinterlockingpieces(actinandmyosinproteins)Theactinmoleculesareattachedtotheoutsideedgesofthe barrelwall,andthemyosinmoleculesareinterspersedbetweentheactinmolecules
Figure2-1:Myocardialcell(myocyte)
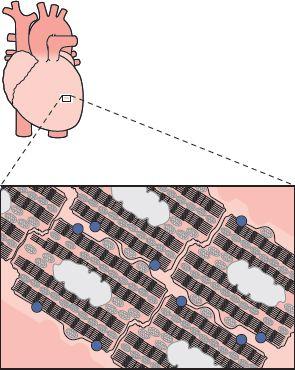
Theoutsidesofthebarrels(cells)arefusedtogethertoformlongbands,ormyofibrils(Figure2-2)Thesebands,inturn,areheldtogetherside-tosidebywire(connectivetissue)toformsheets,whicharecoveredwithfluid(extracellularfluid)Themainfunctionofthebandsistocontractand expandWhenoneofthebarrelscontracts,thewholesheetshortensbyasmallamountWhenallofthebarrelscontract,thewholesheetshortens significantlyThesheetreturnstoitsstartingsizeasallofthebarrelsrelaxThesheetsarearrangedtoformthefoursacsthatconstitutetheheart: twosmall,thinonesontop(theatria)andtwolarge,thickonesonbottom(theventricles)
Figure2-2:Barrelsareheldtogether,formingmyofibrilsandsheets
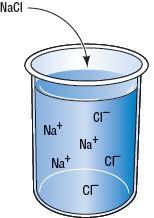
IonMovementandPolarity
Thefluidinsideandoutsideofthebarrelcontainswater,salts,andproteinsThefluidsarenotthesame,however;theconcentrationsofsalt moleculesandproteinsaredifferentineachoneInliquids,saltsbreakdownintopositivelyandnegativelychargedparticlesknownasions (Figure2-3)Inotherwords,anionisapositivelyornegativelychargedparticleinasolutionInthebody,themainpositivelychargedionsare sodium(Na+),potassium(K+),andcalcium(Ca++)Chloride(Cl)isthemainnegativelychargedion
Figure2-3:Saltsinaliquidmediumturnintopositivelyandnegativelychargedions
Ifthecellwerenotalive,theconcentrationsofalloftheionsandchargeswouldbethesameonbothsidesofthebarrelwall(thecellmembrane) However,alivecellmaintainsdifferencesintheseconcentrationsacrossthecellmembrane(Figure2-4)Theinsideofthecellhasahigher potassiumconcentration,whereastheoutsidehasahigherconcentrationofsodiumThehigherpositivechargeoutsidethecellthuscauses relativelymorenegativechargeinsidethecellTheoutsideofthecellwallalsohasmorecalcium,whichaddstothegreaterpositivecharge outsidethecellThisdifferencebetweenthechargesoutsideandinsideofthecellwallisknownasitselectricalpotential
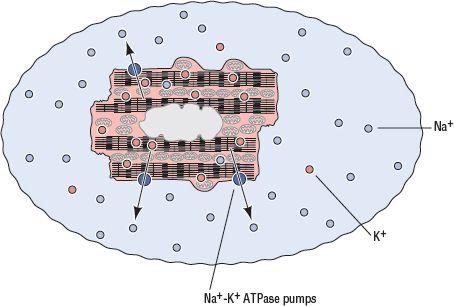
ChargesandionsnaturallywanttocancelthemselvesoutandmaintainneutralityThecellwallisnotacompletelyimpermeablemembraneItis semi-permeable,becauseitcontainssmallleaksthatletsomeoftheionsintoandoutofthecellThenaturaltendencyisforsodiumtoenterand potassiumtoexitTomaintainanelectricalpotential,thecellmusthavesomewayofpushingtheionsaroundagainsttheirwishesEnterthe sodium-potassiumATPasepumps(bluedotsinfigures)Thepumpsactivelymoveionsaroundtomaintaintherestingconcentrationandcharge ofthecellNow,howdoesthepumpdothat?ThepumpusesATP,thebody’sfuelpellet,topushoutthreesodiumions(threepositivecharges) andbringintwopotassiumions(twopositivecharges)TheresultisagreaternumberofpositivechargesoutsidethebarrelthaninsideInother words,theoutsidesolutionhasapositivecharge,whiletheinnersolutionhasamorenegativechargeBecauseofthispumpingaction,the electricalpotentialoftherestingmyocyteisapproximately 70to 90mV