Patient-Centric Healthcare: Through Institutional Regulation [a chapter from "Healers or predators?: healthcare corruption in India"] Meeta Rajivlochan
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by law. Advice on how to obtain permission to reuse material from this title is available at http://www.wiley.com/go/permissions.
The right of Annie Price, Joseph E. Grey, Girish K. Patel, and Keith G. Harding to be identified as the authors of the editorial material in this work has been asserted in accordance with law.
Registered Office(s)
John Wiley & Sons, Inc., 111 River Street, Hoboken, NJ 07030, USA
John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK
Editorial Office
9600 Garsington Road, Oxford, OX4 2DQ, UK
For details of our global editorial offices, customer services, and more information about Wiley products visit us at www.wiley.com.
Wiley also publishes its books in a variety of electronic formats and by print-on-demand. Some content that appears in standard print versions of this book may not be available in other formats.
Limit of Liability/Disclaimer of Warranty
The contents of this work are intended to further general scientific research, understanding, and discussion only and are not intended and should not be relied upon as recommending or promoting scientific method, diagnosis, or treatment by physicians for any particular patient. In view of ongoing research, equipment modifications, changes in governmental regulations, and the constant flow of information relating to the use of medicines, equipment, and devices, the reader is urged to review and evaluate the information provided in the package insert or instructions for each medicine, equipment, or device for, among other things, any changes in the instructions or indication of usage and for added warnings and precautions. While the publisher and authors have used their best efforts in preparing this work, they make no representations or warranties with respect to the accuracy or completeness of the contents of this work and specifically disclaim all warranties, including without limitation any implied warranties of merchantability or fitness for a particular purpose. No warranty may be created or extended by sales representatives, written sales materials or promotional statements for this work. The fact that an organization, website, or product is referred to in this work as a citation and/or potential source of further information does not mean that the publisher and authors endorse the information or services the organization, website, or product may provide or recommendations it may make. This work is sold with the understanding that the publisher is not engaged in rendering professional services. The advice and strategies contained herein may not be suitable for your situation. You should consult with a specialist where appropriate. Further, readers should be aware that websites listed in this work may have changed or disappeared between when this work was written and when it is read. Neither the publisher nor authors shall be liable for any loss of profit or any other commercial damages, including but not limited to special, incidental, consequential, or other damages.
Library of Congress Cataloging-in-Publication Data
Names: Price, Annie (Of Welsh Wound Innovation (Organization)) editor. | Grey, Joseph E., editor. | Patel, Girish (Of Cardiff University) editor. | Harding, K. G. (Keith G.), editor.
Title: ABC of wound healing / edited by Annie Price, Joseph E. Grey, Girish Patel, Keith G. Harding.
Other titles: ABC series (Malden, Mass.)
Description: Second edition. | Hoboken, NJ : Wiley, 2022. | Series: ABC series
Identifiers: LCCN 2021028004 (print) | LCCN 2021028005 (ebook) | ISBN 9780470658970 (paperback) | ISBN 9781118593844 (adobe pdf) | ISBN 9781118593837 (epub)
Subjects: MESH: Wounds and Injuries–diagnosis | Wounds and Injuries–therapy | Ulcer–therapy | Wound Healing–physiology | Handbook
LC record available at https://lccn.loc.gov/2021028004
LC ebook record available at https://lccn.loc.gov/2021028005
Cover Design: Wiley
Cover Image: Courtesy of Professor Keith G. Harding
Set in 9.25/12pt Minion by Straive, Pondicherry, India
Contents
List of Contributors, vi Foreword, viii
1 Wound Assessment, 1
Joseph E. Grey and Girish K. Patel
2 Traumatic Wounds, 9
Steven L.A. Jeffery and Stuart Enoch
3 Surgical Wounds and Surgical Site Infection, 14
Rhiannon L. Harries, Jared Torkington, and David Leaper
4 Burns, 20
Jonathan J. Cubitt and William A. Dickson
5 Diabetic Foot Ulcers, 26
Michael E. Edmonds and Annie Price
6 Venous and Arterial Leg Ulcers, 34
Joseph E. Grey and Girish K. Patel
7 Pressure Injuries, 41
Joseph E. Grey and Jacqui Fletcher
8 Uncommon Causes of Ulceration, 49
Girish K. Patel and Vincent Piguet
9 Infections, 56
Brendan Healy and Andrew Freedman
10 Lymphoedema and Wounds, 64
Christine Moffatt and Melanie Thomas
11 Nutrition, Skin Care and Continence, 71
Amy Ferris, Joseph E. Grey, and Girish K. Patel
12 Scars, 78
Paul Martin and Duncan A. McGrouther
13 Dressings and Devices, 85
Samantha Holloway, Stuart Enoch, and Joseph E. Grey
14 Drugs and Biological Approaches to Wound Healing, 94
Gregory Schultz and Girish K. Patel Index, 102
List of Contributors
Jonathan J. Cubitt
Consultant Burns and Plastic Surgeon Welsh Centre for Burns and Plastic Surgery
Swansea Bay University Health Board Swansea, UK (Chapter 4)
William A. Dickson MBE
Retired Consultant Burns and Plastic Surgeon Welsh Centre for Burns and Plastic Surgery
Swansea Bay University Health Board Swansea, UK (Chapter 4)
Michael E. Edmonds
Consultant Physician
Diabetic Foot Clinic King’s College Hospital London, UK (Chapter 5)
Stuart Enoch
Professor, Higher Surgical Education Directorate of Education and Research Doctors Academy Group (Intl) (Chapters 2, 13)
Amy Ferris
Consultant Geriatrician
Cardiff and Vale University Health Board
Cardiff, UK (Chapter 11)
Jacqui Fletcher OBE
Senior Clinical Advisor
Stop the Pressure Programme
NHS England and NHS Improvement (Chapter 7)
Andrew Freedman
Reader in Infectious Diseases
Cardiff University School of Medicine
Cardiff, UK
Honorary Consultant Physician
Cardiff and Vale University Health Board
Cardiff, UK (Chapter 9)
Joseph E. Grey
Consultant Physician Department of Gerontology, Cardiff and Vale University Health Board
Cardiff, UK (Chapters 1, 6, 7, 11, 13)
Rhiannon L. Harries
Consultant Colorectal Surgeon
Swansea Bay University Health Board
Swansea, UK (Chapter 3)
Brendan Healy
Consultant in Microbiology and Infectious Diseases
Public Health Wales
Cardiff, UK (Chapter 9)
Samantha Holloway
Reader
Cardiff University School of Medicine
Cardiff, UK (Chapter 13)
Steven L.A. Jeffery
Consultant Burns and Plastic Surgeon
Royal Centre for Defence Medicine
Birmingham, UK
Professor of Wound Study
Birmingham City University Birmingham, UK
Honorary Visiting Professor Cardiff University Cardiff, UK (Chapter 2)
David Leaper
Emeritus Professor of Surgery University of Newcastle upon Tyne Newcastle upon Tyne, UK (Chapter 3)
Paul Martin
Professor of Cell Biology
Schools of Biochemistry and Physiology, Pharmacology & Neuroscience University of Bristol Bristol, UK (Chapter 12)
Duncan A. McGrouther
Senior Consultant
Department of Hand and Reconstructive Microsurgery
SingHealth Duke-NUS Academic Medical Centre Singapore (Chapter 12)
Christine Moffatt CBE
International Professor of Clinical Nursing School of Social Sciences
Nottingham Trent University Nottingham, UK (Chapter 10)
Girish K. Patel
Consultant Dermatologist
Welsh Institute of Dermatology Cardiff and Vale University Health Board Cardiff, UK
Honorary Professor Cardiff University School of Biosciences Cardiff, UK (Chapters 1, 6, 8, 11, 14)
Vincent Piguet
Professor and Department Division Director Dermatology, Department of Medicine
University of Toronto Toronto, Canada
Division Head Dermatology
Women’s College Hospital Toronto, Canada (Chapter 8)
Annie Price
Specialist Registrar in Rehabilitation Medicine
Cardiff and Vale University Health Board Cardiff, UK (Chapter 5)
Gregory Schultz
Emeritus Professor University of Florida Gainesville, FL, USA (Chapter 14)
Melanie Thomas MBE
National Clinical Lead for Lymphoedema in Wales Lymphoedema Network Wales
NHS Wales Health Collaborative, UK (Chapter 10)
Jared Torkington
Consultant Colorectal Surgeon Cardiff and Vale University Health Board Cardiff, UK (Chapter 3)
Foreword
The goal of treating wounds is to achieve healing and prevent secondary wound breakdown. Dressings have been used for thousands of years and several notable medical advances have contributed to better wound care. In the 1800s, Lister demonstrated the benefits of antiseptic surgery in reducing infection risk and throughout the 18th and 19th centuries, debridement techniques were developed and advanced by military surgeons. In the late 1800s, sterilised gauze was mass-produced as ready-to-use surgical dressings. George Winter’s observations in 1962, that wounds kept moist healed faster than those kept dry, led to the development of many new materials and advanced wound dressings. Over the past 60 years, there has been an explosion of treatments and current practice involves the use of dressings, devices, drugs, surgical interventions and biologically based treatments to enhance wound healing.
Although a wide range of materials exists, the major benefits of dressings are in managing exudate, minimising leakage and controlling odour and pain. More recently, there has been a rapid increase in the use of devices, from beds and mattresses that aim to prevent and treat pressure injuries, to therapeutic footwear used in diabetic foot disease and negative-pressure devices for a range of wound types. Drugs are often needed to assist in wound healing. The most obvious example is the use of antibiotics for treating wound infection. However, at a time when antimicrobial resistance is seen as a global health challenge, greater understanding and appropriate selection of agents to treat wound infection are urgently needed. Surgery is an essential component for some wound healing problems. This can range from simple draining of an abscess or debridement of unhealthy tissue on the wound surface, through to specialist vascular, orthopaedic or reconstructive procedures. Advances in the understanding of wound healing biology have led to an interest in biological therapies, from platelet concentrate to stem cells.
While treatment advances are rapidly expanding the options for wound care, recent studies have revealed that there are ongoing
problems with wound assessment and diagnosis. Without understanding the cause of the wound and appreciating factors that contribute to delayed or non-healing, successful treatment is less likely. An emphasis on clinical assessment coupled with developments in wound diagnostics may help, but there is also a need for greater engagement of medical specialties and their integration with other members of a multidisciplinary team.
Complete healing of a wound is an obvious measure that should be the goal of care when relevant. However, reduction in wound size, pain, leakage and infection, or improvement in quality of life could also be seen as measures of success in patients who do not have the potential to heal their wounds. Similarly, prevention of recurrence, avoidance of complications and provision of care in dedicated settings should be seen as alternative measures of success. There is a need to capture these factors when evaluating both treatments and services.
Though scientific advances and enhancing the evidence base for existing treatments are important, innovations in service provision and education of healthcare professionals in the management of wounds should not be underestimated. The future for individuals with wound problems requires the ability to access a relevant and capable multidisciplinary team that is appropriate for their needs. Comprehensive, appropriate and patient-centred wound care utilising evidence-based treatments has the potential to benefit many. It is only in recent years that the complexity of the wound healing process and the wide range of factors that can influence healing have been recognised. Greater funding and focus on this subject are essential if the current situation is to be improved.
This new edition of the ABC of Wound Healing aims to take the reader through these issues and provide a ready guide to the recognition, investigation and management of a variety of wound types. It is aimed at ensuring that individuals with wounds receive the standard of care appropriate for modern-day clinical practice.
Professor Keith G. Harding CBE
OVERVIEW
CHAPTER 1
Wound Assessment
Joseph E. Grey1 and Girish K. Patel2,3
1 Department of Clinical Gerontology, Cardiff and Vale University Health Board, Cardiff, UK
2 Welsh Institute of Dermatology, Cardiff and Vale University Health Board, Cardiff, UK
3 Cardiff University School of Biosciences, Cardiff, UK
• Most wounds heal without difficulty, but all wounds have the potential to become chronic.
• The key to successful wound management is diagnosis and treatment of the underlying cause, which requires a detailed history and assessment.
• Certain wound characteristics point to a specific diagnosis and indicate the status of the wound, e.g. infected or clean, healing or non-healing.
• Many local and systemic factors may impede healing; these should be identified and corrected where possible.
• Despite best practice, a small minority of wounds will never heal; improving quality of life and preventing complications are the treatment goals in these cases.
The majority of wounds, of whatever aetiology, heal without difficulties (see Chapters 2–4). Some wounds, however, are subject to factors that impede but do not prevent healing if managed appropriately. In contrast, most common chronic wounds do not heal until the underlying disease is adequately treated (see Chapters 5–8). A minority of wounds do not heal despite best practice, where control of symptoms and prevention of complications, rather than healing, become the goals of treatment.
Complications of chronic wounds
• Sinus formation
• Fistula
• Unrecognised malignancy
• Malignant transformation in the ulcer bed (Marjolin ulcer)
• Osteomyelitis
• Contractures and deformity in surrounding joints
• Systemic amyloidosis
• Heterotopic calcification
• Colonisation by multiple drug-resistant pathogens leading to antibiotic resistance
• Anaemia
• Septicaemia
Approach to patients with wounds
In patients with wounds, it is important that the normal processes of developing a diagnostic hypothesis are followed before attempting to treat the wound. A detailed clinical history should be taken, along with an examination of the wound, surrounding skin and (where relevant) the limb, and any appropriate investigations should be performed. Seek to define the cause of the wound and factors that might impede healing. In order to aid management, regular wound assessments are used to monitor progress. A systematic approach to wound assessment is helpful. The following factors should be considered as part of every wound assessment.
Site of the wound
The site of the wound may aid diagnosis; diabetic foot ulcers often arise in areas of abnormal pressure distribution caused by disordered foot architecture. Venous ulcers mostly occur in the gaiter area of the leg. Non-healing ulcers, sometimes in unusual sites, should prompt consideration of malignancy.
Size of the wound
This should be assessed at first presentation and regularly thereafter to monitor response to treatment and provide an indication of healing. The simplest method is using a ruler to measure wound dimensions (longest length and perpendicular width). Wound surface area can be measured using an acetate tracing; the outline of the wound margin is traced onto transparent acetate sheets marked with 1 cm squares and the longest diameter in one plane is multiplied by the longest diameter in the perpendicular plane (for approximately circular wounds) or the number of squares contained within the wound outline are added together (for irregularly shaped wounds). These methods are relatively subjective and can be unreliable; accuracy is also affected by patient positioning, body curvature or tapering of the limbs. More sophisticated methods include using digitised area measurement software or laser techniques, but these require training and specialist equipment. Clinical photography should be carried out whenever possible.
• Limited tissue mobility, e.g. wound tethered by scarring
• Poor surgical apposition
• Wound dehiscence
• Poor venous drainage
• Presence of foreign body and foreign body reactions
• Continued presence of micro-organisms and infection
• Excess local mobility, e.g. over a joint
• Previous radiotherapy
Systemic factors
• Advancing age and general immobility
• Obesity
• Smoking
• Malnutrition
• Deficiency of vitamins and trace elements, e.g. scurvy
• Systemic malignancy and terminal illness
• Shock of any cause
• Chemotherapy
• Immunosuppressant medications, e.g. corticosteroids
• Inherited neutrophil disorders such as leucocyte adhesion deficiency
• Impaired macrophage activity (malacoplakia)
Accurate methods for measuring wound depth are not practical or available in routine clinical practice. However, approximate measurements of greatest depth should be taken to assess the extent of the wound. Undermining of the edge of the wound must be identified by digital examination or use of a probe. The depth and extent of sinuses and fistulae should be identified. Undermining areas and sinuses should be packed with an appropriate dressing to facilitate healing. Undermining wounds and sinuses with narrow necks that are difficult to dress can sometimes be laid open at the
(c)
(d)
Common types of chronic wounds. (a) Venous leg ulcer. (b) Pressure injury. (c) Post-operative wound dehiscence. (d) Diabetic foot ulcer.
Factors that impede wound healing.
bedside to facilitate drainage and dressing. Wounds associated with multiple sinuses or fistulae should be referred for specialist surgical intervention.
Wound edge
Although not diagnostic, examination of the wound edge may help to identify its aetiology in the context of the clinical history. All healing wounds have a thin, shiny, tapered edge. Whereas venous leg ulcers generally have gently sloping edges, arterial ulcers often appear well demarcated and ‘punched out’, and rolled or everted edges should raise the suspicion of malignancy. A biopsy should be taken from the edge of any suspicious wound.
◦ Connective tissue diseases, e.g. rheumatoid arthritis
◦ Varicose veins
◦ Deep venous thrombosis
• Previous venous or arterial surgery
• Smoking
• Medications
• Allergies to drugs and dressings
General principles of wound management
1 Diagnose and treat the underlying cause of the wound
2 Identify and correct factors that impede healing
3 Wash the wound (clean tap water for chronic wounds, sterile water or saline for acute wounds)
4 Remove non-viable tissue and debris
5 Choose a dressing appropriate for the level of wound exudate (see Chapter 13)
Wound bed
Healthy granulation tissue is pink in colour and is an indicator of healing. Unhealthy granulation tissue is dark red in colour, often bleeds on contact and may indicate the presence of wound infection. Excess granulation or overgranulation may also be associated
Laboratory investigations.
Investigation
Haemoglobin
White cell count
Platelet count
Erythrocyte sedimentation rate (ESR); C-reactive protein (CRP)
Urea and creatinine
Albumin
Glucose, haemoglobin A1C
Markers of autoimmune disease, e.g. rheumatoid factor, antinuclear antibodies, anticardiolipin antibodies, lupus anticoagulant
Cryoglobulins, cryofibrinogens, prothrombin time, partial thromboplastin time
Deficiency or defect of antithrombin III, protein C, protein S, factor V Leiden
Rationale
Anaemia may delay healing. May also be an indicator of poor nutrition (e.g. iron, B12 or folate deficiency)
High count may indicate infection
Low count may reflect poor nutrition
Thrombocytopenia may reflect bone marrow suppression and increased risk of bleeding
Thrombocytosis may lead to increased small vessel thrombosis
Non-specific markers of infection/ inflammation. Useful in diagnosis and monitoring treatment of infectious/inflammatory ulceration
High urea impairs wound healing. Renal function important when using antibiotics
Protein loss delays healing
Diabetes mellitus
Indicative of rheumatoid disease, systemic lupus erythematosus and other connective tissue disorders
Haematological disease
Vascular thrombosis
Haemoglobinopathy screen Sickle cell anaemia, thalassaemia HIV status Kaposi sarcoma
Serum protein electrophoresis, Bence-Jones proteins
Urinalysis
Myeloma
Useful in connective tissue disease
Wound swab Not routine. All ulcers colonised (not the same as infection). Swab only when clinical signs of infection
HIV, human immunodeficiency virus.
with infection or non-healing wounds. This can be treated by cautery with silver nitrate or topically applied steroid preparations. The type of tissue at the base of the wound will provide useful information relating to expectation of total healing time and the risk of complications. For example, bone at the base of the wound may suggest a protracted healing time and the possibility of underlying osteomyelitis.
Necrotic tissue, slough and eschar
The wound bed may be covered with non-viable, unhealthy tissue, which can be classified as necrotic (dead) tissue, slough (immune cells and debris, usually cream or yellow in colour) or eschar (dry, black, hard necrotic tissue). The amount of necrosis and slough in the wound is an indicator of the wound status. Necrotic tissue and slough may be quantified as excessive (+++), moderate (++), minimal (+) or absent (−). Since non-viable tissue can harbour pathogenic organisms and delay normal healing, it should be removed; this is termed debridement.
Surrounding skin
The surrounding skin may provide diagnostic clues as to the aetiology of the wound; for example, the characteristic signs of chronic venous insufficiency (see Chapter 6). Cellulitis associated with wounds should be treated with systemic antibiotics. Eczematous changes may need treatment with potent topical steroid preparations. Maceration of the surrounding skin is often a sign of the inability of the dressing to control the wound exudate, which may respond to more frequent dressing changes or change in dressing type. Callus (hardened skin) surrounding and sometimes covering neuropathic foot ulcers (e.g. in diabetes) must be debrided (see Chapter 5).
Infection
All open wounds are colonised with bacteria. Bacteriological culture should be performed only if clinical signs of infection are present or if there are issues of infection control to be considered (e.g. methicillin-resistant Staphylococcus aureus [MRSA], Panton Valentine Leukocidin [PVL]-secreting Staph. aureus). The classic signs of infection are heat, redness, swelling and pain. Additional signs of wound infection include increased exudate, delayed healing, contact bleeding and abnormal granulation tissue. Treatment with antimicrobial therapy should be guided by microbiological results and local resistance patterns (see Chapter 9).
Sun-exposed areas Basal cell carcinoma, squamous cell carcinoma
Wound exudate
Loss of the epidermal barrier results in water loss presenting as exudate. The quantity of exudate is usually classified as heavy (dressing soaked; +++), medium (dressing wet; ++) or minimal (dressing dry; +). A moist (versus dry) wound environment promotes healing, but excessive exudate may be due to wound infection or oedema in the wound area and can delay healing. It can also macerate the surrounding skin, leading to further breakdown. Exudate should be controlled using dressings appropriate for the level of moisture, and any infection should be treated. Barrier films applied to the surrounding skin help prevent further maceration. The oedematous leg should be elevated when seated.
Squamous cell carcinoma on the medial aspect of the knee – an unusual location for a chronic leg ulcer.
Methods of wound measurement. (a) Wound measurement using a ruler. (b) Wound measurement using acetate tracing.
Odour
Malodour can be caused by infection, necrotic tissue and saturated dressings. As well as treating the cause of malodour (e.g. debriding necrotic tissue, treating infection), superabsorbent dressings or charcoal dressings may be useful to control odour. Topical metronidazole is useful for malodour associated with fungating tumours.
Pain
Pain is a characteristic feature of many healing and non-healing wounds. Pain can be caused by both nociceptive and neuropathic stimuli. Intermittent pain is often related to dressing removal or recent application of new dressings and may necessitate the use of analgesia prior to dressing change. Constant pain may arise as a result of the underlying condition, including ischaemia, neuropathy,
Edges Type of ulcer
Transparent Epithelialising
White Macerated
Sloping Venous ulcer
Punched out Arterial/vasculitic ulcer
Rolled Basal cell carcinoma
Raised/thickened Squamous cell carcinoma
Undermining Pressure injury and ulceration, tuberculosis, syphilis
Purple ± ragged edge Pyoderma gangrenosum or other inflammatory disease (e.g. vasculitis)
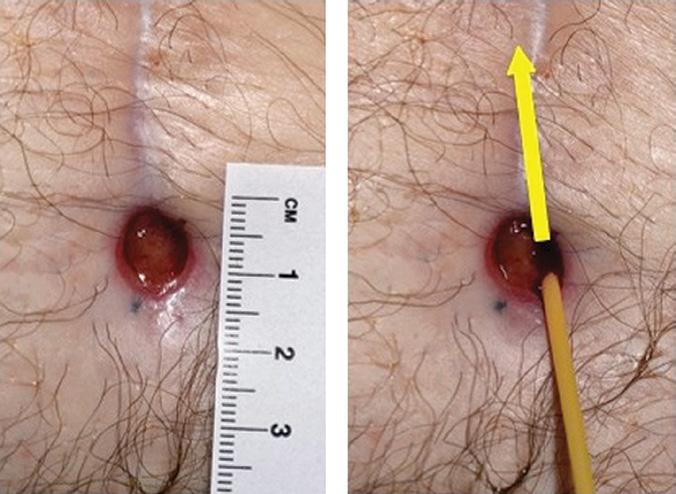
(a)
(b)
The importance of probing a wound. (a) A small abdominal wound. (b) On examination with a probe, the wound is actually undermining by 2.5 cm in a cranial direction.
Wound edge characteristics.
Communication between pilonidal sinus wounds.
Healing edge of an abdominal wound. The size of the original wound is evident by the amount of newly formed scar tissue present.
tissue oedema, chronic tissue damage (e.g. lipodermatosclerosis), infection or scarring (e.g. atrophie blanche). The nature and type of pain should be identified and treated appropriately. Various pain assessment tools are available to help assess the nature and severity of pain. Patients with recalcitrant or difficult-to-control pain may benefit from referral to a local pain team.
Non-healing wounds
Non-healing wounds have traditionally been defined as those that fail to progress through an orderly sequence of repair in a timely fashion. Such wounds are sometimes thought of as being caused by neglect, incompetence, misdiagnosis or inappropriate treatment
strategies. However, it is important to appreciate and acknowledge that some wounds are resistant to all efforts of treatment aimed at healing and alternative endpoints should be considered. Measures aimed at improving quality of life are paramount in these instances.
Quality of life
Several studies have shown that individuals with non-healing wounds have a decreased quality of life. This is due to a multitude of factors, including the frequency and regularity of dressing changes, which cause disruption to daily routine, lack of sleep, restricted mobility, pain, odour, wound infection and the physical and psychological effects of polypharmacy. The loss of independence associated with functional decline can lead to changes, sometimes subtle, in
(a)
(b)
Examination of the wound bed. (a) Healthy granulation tissue in a hidradenitis suppurativa excision. (b) Unhealthy granulation tissue in a diabetic foot ulcer.
Dead tendon in the base of the wound (indicated by arrow).
Squamous cell carcinoma with raised edges.
Types of wound debridement
1 Sharp – using a scalpel or curette at the bedside
2 Surgical – in the operating theatre using sharp or hydrosurgical (high-powered water jet) methods
3 Autolytic – facilitation of the body’s own mechanism of debridement with moisture-donating dressings
4 Biological – larval (maggot) therapy
5 Enzymatic – not widely used; paw-paw or banana skin used in developing countries
6 Mechanical – wet-to-dry dressings or debridement pads or wipes
7 Ultrasonic – low-frequency ultrasound applied to wound bed
overall health and well-being. These changes include altered eating habits, depression, social isolation and a gradual reduction in activity levels. Many individuals with non-healing wounds complain of difficulties with emotions, finances, physical health, daily activities, friendships and leisure pursuits.
Quality of life is not always related to ulcer healing. Patients’ concerns and goals of treatment should be taken into consideration. Control of odour, exudate and pain may improve an individual’s quality of life. Additionally, optimisation of chronic wound management will lead to a reduction in the frequency of dressing changes, further enhancing quality of life. In a minority of instances, seemingly drastic measures such as amputation in a person with chronic leg ulceration may need to be considered where the quality of life is severely affected by the non-healing wound and its complications.
(a) (b)
(c) (d)
Examination of the wound bed. (a) Necrotic tissue. (b) Slough. (c) Fibrin (scar tissue). (d) Eschar.
(a) Pressure injury with extensive callus build-up before debridement. (b) Sharp debridement using a ring curette at the bedside. (c) All callus has been removed and healthy bleeding tissue is visible.
Maceration of surrounding skin.
A non-healing wound; this venous leg ulcer has been present for over 10 years and has not healed despite optimal treatment.
Common features of non-healing wounds
• Absence of healthy granulation tissue
• Presence of necrotic and unhealthy tissue in the wound bed
• Excess exudate and slough
• Lack of adequate blood supply
• Failure of re-epithelialisation
• Cyclical or persistent pain
• Recurrent wound breakdown
• Clinical or subclinical infection
Further reading
Falanga, V., Lindholm, C., Carson, P.A. et al. (eds.) (2012). Text Atlas of Wound Management, 2e. London: Informa Healthcare.
Frykberg, R.G. and Banks, J. (2015). Challenges in the treatment of chronic wounds. Advances in Wound Care 4 (9): 560–582.
Leaper, D.J., Schultz, G., Carville, K. et al. (2012). Extending the TIME concept: what have we learned in the past 10 years? International Wound Journal 9 (Suppl.2): 1–19.
Wounds UK (2018). Best Practice Statement: Improving Holistic Assessment of Chronic Wounds. London: Wounds UK.
Larval debridement of a pressure injury.
OVERVIEW
CHAPTER 2
Traumatic Wounds
Steven
L.A. Jeffery1,2,3 and Stuart Enoch4
1 Royal Centre for Defence Medicine, Birmingham, UK
2 Birmingham City University, Birmingham, UK
3 Cardiff University, Cardiff, UK
4 Directorate of Education and Research, Doctors Academy Group (Intl)
• Traumatic wounds are common and range from minor epithelial loss that will heal spontaneously within a few days to extensive tissue necrosis and degloving that require complex surgical treatment.
• Understanding the mechanism of injury helps guide wound management.
• All traumatic wounds are contaminated to some degree; the risk of infection is reduced by adequate cleaning and debridement.
• The reconstructive ladder is a useful framework for considering methods of wound closure.
Since the evolution of our species, humans have been sustaining traumatic injuries. In the fifth century BC, Hippocrates advocated that wounds be bathed in water or wine, and that a suppurating wound was a healing wound. In the early fourteenth century, Guy de Chauliac proposed five wound management principles that have stood the test of time.
Wound management principles
Removal of foreign bodies
Rejoining of severed tissues
Maintenance of tissue continuity
Preservation of organ substance
Prevention of complications
Mechanisms of injury
Traumatic wounds usually involve some loss or damage to an epithelial surface (usually skin) but may also involve the underlying connective tissue, with or without epithelial loss (e.g. contusion, degloving or crush injury). Understanding the mechanism of injury helps guide wound management. Traumatic wounds may be classified as superficial or deep, tidy or untidy, contaminated or not contaminated. They may be categorised as follows.
Abrasions are superficial epithelial wounds caused by frictional scraping forces. When extensive, they may be associated with fluid loss. Such wounds should be cleansed to minimise the risk of infection and remove superficial foreign bodies (which can result in unsightly ‘tattooing’). Abrasions can be covered with a simple non-adhesive dressing, if required, and are best left to heal by re-epithelialisation.
Lacerations occur when trauma exceeds the intrinsic tissue strength, for example, when the skin is torn by blunt injury over a bony prominence such as the elbow or the knee. The edges will be irregular. Minimal tissue damage may be amenable to primary suturing. Closure with adhesive strips (e.g. Steri-Strips™) may be appropriate in some circumstances, for example, simple linear lacerations or a pretibial laceration. If post-injury oedema is anticipated, primary suturing of the wound is not advisable since this causes increased tissue tension and consequently risks wound breakdown.
Penetrating trauma by a sharp point (e.g. a nail, bullet) may result in minimal damage to skin and connective tissue but cause deeper damage to vessels, nerves and/or internal organs. The visible skin wound may be deceptive and hence a full exploration of the wound is advisable. Penetration may carry dirty tissue deep into the wound. In gunshot wounds, an exit wound may be present. Contusions are caused by more extensive tissue trauma following severe blunt or blast trauma. The overlying skin may appear to be intact but later become non-viable. Large haematomas under skin or in muscle may be present. If superficial and fluctuant, they can be evacuated with overlying necrotic tissues. Ultrasound or magnetic resonance imaging scans may help to define a haematoma amenable for evacuation. Extensive contusion risks infection (antibiotic prophylaxis should be considered in open wounds) and compartment syndrome (fasciotomy will be needed to preserve the limb).
Bite wounds need special, urgent consideration because of the degree of contamination and high risk of infection. The skin injury could be a puncture wound, a laceration or an abrasion, or a combination of these. There may also be deeper damage from a crush injury. Humans and animals have high numbers of
pathogenic bacteria in their mouths and therefore human and animal bites carry a high risk of infection. Special attention should be given to cleaning, irrigating and debriding these wounds. Because of the risk of infection, there is concern about when it is safe to primarily close these injuries and when they should be left open. Nowadays it is thought to be relatively safe to close bite wounds that are not deep, less than 24 hours old and with little contamination. Human bites also carry the risk of viral transmission, e.g. hepatitis B or C. Antibiotics should be prescribed for 1 week. The tetanus status of the patient should be determined and prophylaxis provided if needed.
Avulsion injuries and degloving: as with wounds from a blast injury, these wounds are characterised by shearing of the skin and subcutaneous tissues from the underlying fascia and muscle, with disruption of the blood vessels where they perforate the fascia before supplying the skin. The viability of the tissue should be assessed, and non-viable tissue excised. It is important not to close these wounds under tension, as this will further reduce the
Management of bite wounds.
Safe to close Leave open after exploration and debridement
• <24 h old
• No signs of infection
• Superficial
• Light contamination
• >24 h old
• Already showing signs of infection
• Deep puncture wound
• Heavy contamination
• Crush injury
• Bites to the limbs, hands or feet
blood supply to the skin. Rather, such wounds should be left open. Negative-pressure wound therapy should be considered (see Chapter 13).
Surgical incisions cause minimal tissue damage since they are usually made with precision and in an environment with appropriate aseptic precautions. Controlled haemostasis and asepsis reduce the risk of infection, leading to improved wound healing. Large surgical wounds may be left open to heal by secondary intention or with delayed skin grafting, depending on the extent of the residual defect.
Management
Triage and resuscitation may be needed before definitive wound management; this should be done according to the Advanced Trauma Life Support® guidelines. Arterial bleeding is easy to recognise (pulsatile and bright red) provided it is overt, but if it is hidden from view, e.g. following penetrating injury to the aorta, it can lead to profound unexpected haemorrhagic shock. Early exploration and repair or ligation of blood vessels may be required. Venous haemorrhage is flowing and dark red, and can usually be controlled by adequate direct pressure. Capillary bleeding oozes and is bright red; it can lead to shock if the injury is extensive and should not be underestimated. All penetrating and traumatic wounds should be explored if there is suspicion of blood vessel, nerve or organ damage. Attention to fractures, debridement of devascularised tissue and removal of foreign material may be required.
Pretibial laceration closed with adhesive strips.
Fasciotomy wound.
Degloving injury – avulsion of the skin from underlying tissue.
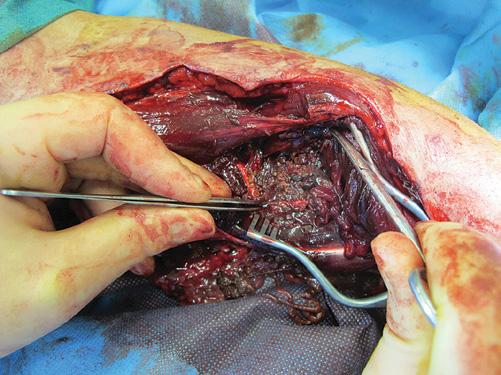
Contamination and debridement of traumatic wounds
All traumatic wounds are contaminated and will contain a variable amount of foreign material or dirt, depending on where and how the wound was sustained. A knife wound may produce relatively little wound contamination, whereas wounds sustained on the battlefield or in the farmyard will inevitably be heavily contaminated. Patients with tetanus-prone wounds should receive tetanus toxoid vaccination +/– immunoglobulin. Patients with severely contaminated wounds should receive prophylactic broad-spectrum antibiotics. Prior to wound debridement, all wounds should be cleaned of particulate matter using soap and water.
The degree of debridement will depend on the extent of contamination and the resources available. Large wounds should be assessed and debrided under general anaesthetic. Photographs should be taken in theatre to allow planning of further management without the need for dressings to be taken down. 3D photography is particularly
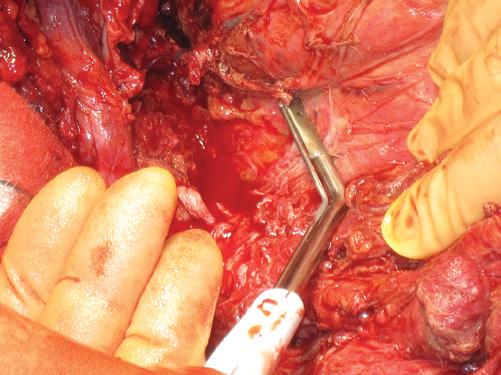
useful in recording complicated wounds. In limb wounds, tourniquet control facilitates a bloodless field and effective excision of necrotic and contaminating material.
Debridement should be performed systematically in layers: ‘Start at the skin and work your way in’. The skin edges are best excised using a scalpel. More mobile tissues, such as fat and muscle, are best debrided using scissors. Debridement of material that is difficult to pick up with forceps, such as sand or adventitial tissue, is best carried out by hydrosurgical means.
Larger complex wounds are often uneven and contain numerous pockets of foreign contaminated material, which may be forced deep between tissue planes. Every such pocket must be explored and included in the debridement. Once debridement is complete, irrigation with at least 3 litres of warm saline should be performed, prior to application of a dressing. High-pressure irrigation is contraindicated as it further damages the tissues and drives foreign material deeper.
Heavily contaminated traumatic wound.
Arm wound with tourniquet in place prior to debridement.
Wound closure
The ‘reconstructive ladder’ is a useful way of thinking about how to close wounds. The simpler techniques are safest but may not give the best result. Each rung of the ladder represents a more complex type of wound closure. More complicated techniques may give a better result, but the higher up the ladder, the worse the risk of failure. Decisions about wound management should take into account local factors such as the location and size of the wound and mechanism of injury, and patient factors such as comorbidities, expected functional outcome, occupational circumstances and likely period of time off work. Alternative treatments such as negative-pressure wound therapy and dermal matrices also have a role in reconstructing defects (see Chapter 14).
Timing of wound closure Clean, tidy wounds may be safely closed within 6 hours of the injury. With the exception of the face, hands and perineum, all other contaminated wounds should be left open initially.
Healing by secondary intention Some wounds may be left open to heal by secondary intention, i.e. by formation of granulation tissue, re-epithelialisation and wound contraction. Dressings are used as a barrier and to optimise the environment for healing (e.g. by absorbing excess exudate). This process is slow and can lead to scarring and contractures.
Primary wound closure Primary wound closure (approximation of wound edges) can be achieved by the following methods. • Adhesive strips are useful in closing superficial wounds. They allow for wound swelling and are associated with low infection rates.
Dirt identified in bloodless field.
Hydrosurgical debridement.
‘The solution to pollution is dilution’ – following debridement, wounds should be irrigated thoroughly with warm saline.
Debrided wound ready for dressing application.
Free tissue transfers
Distant tissue transfers
Local tissue transfers Direct tissue closure
Skin graft
Allow wound to heal by secondary intention
The reconstructive ladder.
Failed healing of donor site after harvesting of split-thickness skin graft.
• Methacrylate ‘super-glues’ are widely used for skin closure, particularly for the scalp. They can also be placed over the wound edges following subcuticular suturing. They are usually contraindicated in wounds with uneven edges, deep wounds and infected wounds or bites.
• Metal clips and staples are alternatives to conventional suturing. Despite their need for removal, they are associated with good cosmetic results and low infection rates. Disposable applicators
are expensive but allow rapid closure of long wounds after prolonged surgical procedures.
• Sutures are used to bring tissues together and to aid optimal wound healing. The three important considerations for primary closure are the suture material, type of needle or appliance, and the technique of closure (see Chapter 3). An adhesive polyurethane film dressing can be applied over sutured wounds to provide a barrier to infection.
Skin grafts Where skin defects are too large for primary skin apposition, and healing by secondary intention is inappropriate, skin grafts may be used. Free skin grafts are taken from another part of the body and rely on revascularisation from a healthy, wellvascularised recipient wound bed. Split-thickness skin grafts consist of epidermis and a variable amount of dermis; the donor site is left to heal by re-epithelialisation. Full-thickness skin grafts consist of epidermis and dermis, with the donor site requiring primary closure, thereby limiting the size of graft that can be taken.
Skin flaps Many wounds, such as fracture sites and exposed bone or tendon, are not suitable for grafting, and techniques further up the reconstructive ladder, such as a flap reconstruction must be used. A flap is a unit of tissue that can be moved to cover a wound while surviving on its own vascular supply. It may consist of different tissue types, including skin, muscle, fat or bone. Local flaps are moved (e.g. rotated or advanced) from an area adjacent to the defect. Distant flaps can be pedicled (transferred whilst maintaining its blood supply via one or more named blood vessels) or free (detatched from its blood supply and reattached to vessels at the recipient site using microsurgical techniques).
Both skin grafts and skin flaps require donor tissue, with the additional risk of donor site complications such as infection, nonhealing or scarring. Allografts (from cadaveric or living donors) or xenografts (from animals, usually porcine) can be used when there is not enough autologous tissue available, such as in severe burns. These will usually be rejected by the host immune system but are useful as a temporary cover.
Further reading
Clasper, J.C., Standley, D., Heppell, S. et al. (2009). Limb compartment syndrome and fasciotomy. Journal of the Royal Army Medical Corps 155: 298–301.
Jeffery, S.L.A. (2009). Advanced wound therapies in the management of severe military lower limb trauma: a new perspective. Eplasty 21: e28.
Jeffery, S.L.A. (2016). The management of combat wounds: the British military experience. Advances in Wound Care 5 (10): 464–473.
Savage, J.M. and Jeffery, S.L.A. (2013). Use of 3D photography in complexwound assessment. Journal of Wound Care 22 (3): 156–160.
Taylor, C.J. and Jeffery, S.L.A. (2009). Management of military wounds in the modern era. Wounds UK 5 (4): 50–58.
Surgical Wounds and Surgical Site Infection
Rhiannon L. Harries1, Jared Torkington2, and David Leaper3
1 Department of Colorectal Surgery, Swansea Bay University Health Board, Swansea, UK
2 Department of Colorectal Surgery, Cardiff and Vale University Health Board, Cardiff, UK
3 University of Newcastle upon Tyne, Newcastle upon Tyne, UK
OVERVIEW
• Surgical wounds are made in a sterile environment after preparation of the skin using an antiseptic agent in order to facilitate a surgical procedure.
• Varying methods of wound closure are available; there are many factors to consider, including the site of the wound, the size of the defect, the degree of contamination, etc.
• Surgical site infections (SSIs) are caused by many, often resistant, organisms, usually derived from the patients themselves and related to the site of surgery.
• Most SSIs are superficial but deeper infections can be lifethreatening.
• There is a focus on prevention of SSIs by identifying and addressing risk factors.
A surgical wound is a cut or incision made to facilitate a surgical procedure by using a cutting instrument such as a scalpel or dia thermy. The size and location of the incision will be determined by the source of the disease or injury being surgically treated, and con sideration is given to the cosmetic outcome by favouring Langer’s lines (corresponding to the natural orientation of collagen fibres in the dermis), where possible.
Requirements for successful postoperative wound healing
Postoperative wound healing occurs only if certain principles are followed:
• Absence of haematoma
• Absence of infection
• Accurate skin apposition
• Tension-free apposition
Classification
Surgical incisions are made in a sterile environment after prepara tion using an antiseptic agent (e.g. chlorhexidine, povidone‑iodine) immediately prior to incision, in order to minimise infections. Surgical wounds can be classified according to the degree of con tamination, which helps predict the risk of subsequent infection and its effect on wound healing.
Clean: clean surgical wounds with no evidence of inflammation or infection. Also includes surgery involving the insertion of a pros thesis. Examples include inguinal hernia repair, mastectomy, cataract operation and thyroidectomy. Operations involving the gastrointestinal, genitourinary and respiratory tracts are excluded due to a higher risk of infection.
Clean-contaminated: clean surgical wounds with a higher risk of infection. These include operations involving controlled entry into the gastrointestinal, genitourinary or respiratory tract (with out spillage) and also aural or gynaecological surgery. Examples include cholecystectomy (without spillage of bile), hysterectomy and the insertion of grommets.
Contaminated: contaminated surgical wounds such as spillage from the gastrointestinal tract or entrance into an infected genitouri nary or biliary tract. Fresh traumatic wounds from a clean source are included. Examples include colectomy and appendicectomy for an inflamed appendix.
Dirty: dirty surgical wounds such as those with faecal contamination, the presence of foreign bodies, devitalised tissue, bacterial inflam mation or perforated viscus. Traumatic wounds either from a dirty source or non‑acute (>24 hours old) are included. Examples include abscess drainage and laparotomy for faecal peritonitis. The risk of wound infection varies from 0.5–2% for clean cases to up to 40% for dirty cases. Prophylactic antibiotic administration is recommended for contaminated and dirty cases. Antibiotic usage is at the discretion of the surgeon for clean operations but it may be indicated for certain cases, such as implant insertion. Antibiotics must be administered 30 minutes prior to induction of anaesthesia
for maximal benefit. Antibiotic choice should be based on the organism most likely to be the cause of a wound infection related to the type of operation.
Wound closure
Surgical wounds can be closed by either primary or secondary intention.
Primary intention: a wound closed by approximation of the wound edges or by placement of a skin graft or flap in order to facilitate the biological event of healing, by joining together the wound
edges and eliminating the dead space. Careful epidermal align ment and eversion of the edges reduce scar formation. Primary closure of a wound is suitable for acute (less than 24 hours dura tion) clean wounds with tension‑free, well‑vascularised wound edges.
Secondary intention: a wound left open to close via epithelialisation and contraction. Secondary closure of a wound is advocated for management of contaminated or infected wounds, or where wound edges may be under tension if approximated. A contaminated wound may be closed at 48 hours if there is no ongoing evidence of infection (termed delayed primary closure).
Sutures
Primary closure is often performed using sutures, and can be achieved by a variety of different suture materials and suturing techniques. The ideal suture material needs a high breaking strength, to be handled comfortably and to knot securely, with min imal tissue reaction and bacterial growth. Suture choice is decided based on both suture properties and patient factors. Sutures can be either absorbable (e.g. polydioxane, polyglactin, poliglecaprone) or non‑absorbable (e.g. nylon, polypropylene). Absorbable sutures provide temporary support and thereafter are absorbed at varying rates. They are often used internally but do have an advantage for skin closure in certain patients such as
Site of sutures
Scalp and face
Upper limb
Number of days
3–4
7
Lower limb 7–10
Over a joint 14 Trunk 10–14
children, as they do not require removal. Non‑absorbable sutures require removal; the duration is dependent on the location of the incision. While they do not absorb, some lose tensile strength over time. Sutures should be removed using a method that prevents the external part of the suture passing through the suture tracts to avoid the introduction of infection.
Sutures are either monofilament or braided. Monofilament sutures are made of a single strand, resist colonisation by micro‑ organisms and cause less tissue reaction compared to braided sutures. Braided sutures are made of multiple strands braided or twisted together and are easier to handle than monofilament sutures. Antibacterial impregnated sutures are also commercially available.
Size of suture thread is classified as a fraction of gauge 0. Thinner sutures (e.g. 5/0) are used for skin closure on the face and thicker sutures (e.g. 2/0) can be used for skin closure on the trunk.
Thinnest Thickest 8/0 6/0 4/0 2/0 02
Sizes of suture thread, classified as a fraction of gauge 0.
Needles are classified according to their type and shape, and their choice is dependent on the tissue being sutured, gauge of needle
Primary closure using interrupted sutures.
Groin wound left open to heal by secondary intention.
Timings for removal of non-absorbable sutures.
Examples of suture materials.
Suture Material
Monocryl® Poliglecaprone
Vicryl® Polyglactin 910
PDS® Polydioxanone
Synthetic/natural
Synthetic
Synthetic
Synthetic
Sofsilk™ Silkworm cocoons Natural
Surgipro™ Polypropylene Synthetic
Ethilon® Nylon-polyamide Synthetic
Cutting needles for stitching skin
Braided/monofilament
Absorbable/non-absorbable
Monofilament Absorption 90–120 d
Braided Absorption 56–70 d
Monofilament Absorption 180–210 d
Braided Absorption 2 yr
Monofilament Non-absorbable
Monofilament Non-absorbable
Round bodled needles for peritoneum, muscles, and fat
Cutting needles for aponeurosis
Needles used for suturing the abdominal wall
Needles used for suturing the bowel
The threads are swaged into the needles
Types of needles used for different surgical procedures. Straight needles and hand needles are rarely used due to the added risk of needlestick injury. A cutting needle has three edges with the cutting edge on the concave surface; it is suitable for tissue penetration and should be chosen for suturing skin. A reverse cutting needle has the cutting edge on the inferior aspect of the needle. A round-bodied, or tapercut, needle is shaped so the tip pierces and the needle then separates the tissues and should be used for anastomosis. A blunt needle has a rounded end to avoid splitting tissues and is used for fascial closure.
of needles used in wound closure.
used, operative accessibility and surgeon preference. The needle type is based on the cross‑sectional appearance. A number of suturing techniques exist, and are dependent on location of the incision, patient factors and surgeon choice. Knots should be tied snug but not too tight as the skin is likely to swell as a result of inflammation.
Other methods of primary closure
Primary closure may also be achieved by other methods includ ing surgical staples, adhesive strips or adhesive glue. Surgical staplers allow rapid closure of long wounds (e.g. laparotomy incisions), but they require subsequent removal. Other forms of surgical staples are also commonly used for bowel anastomosis and gastric and lung resections. Skin adhesives (e.g. cyanoacr ylate) are topically applied to easily approximated skin edges where haemostasis is already achieved. The adhesive remains liquid until exposed to water or water‑containing tissues, when it polymerises and forms a bond. The skin adhesive acts as a barrier to microbial penetration. Adhesive strips are useful for closure of small superficial wounds and are applied across the wound in a manner that brings the skin on either side of the wound together. Durability of the adhesive strips can be