Evidence‐Based Neurological Disorders Symptoms, Causes, and Therapy
edited by
Sushil Kumar Upadhyay
Siddhartha Dan
Sheikh Abid Ali
Published by Jenny Stanford Publishing Pte. Ltd.
101 Thomson Road
#06-01, United Square
Singapore 307591
Email: editorial@jennystanford.com
Web: www.jennystanford.com
British Library Cataloguing-in-Publication Data
A catalogue record for this book is available from the British Library.
Evidence-Based Neurological Disorders: Symptoms, Causes, and Therapy
Copyright © 2024 by Jenny Stanford Publishing Pte. Ltd.
All rights reserved. This book, or parts thereof, may not be reproduced in any form or by any means, electronic or mechanical, including photocopying, recording or any information storage and retrieval system now known or to be invented, without written permission from the publisher.
For photocopying of material in this volume, please pay a copying fee through the Copyright Clearance Center, Inc., 222 Rosewood Drive, Danvers, MA 01923, USA. In this case permission to photocopy is not required from the publisher.
ISBN 978-981-5129-18-2 (Hardcover)
ISBN 978-1-003-49634-2 (eBook)
1. An Introduction
Subashani, Vaishnavi Kakkar, Siddhartha Dan, Sushil Kumar Upadhyay, and Anil K. Sharma
Vagus Nerve
1.11.1 Disorders of the Vagus Nerve Accessory Nerve
1.12.1 Disorders of the Accessory Nerve Hypoglossal Nerve
1.13.1 Disorders of the Hypoglossal Nerve Diagnosis of Cranial Nerve Disorders Through Imaging Techniques
1.14.1 Psychiatry
1.14.1.1 Physical symptoms and mental symptoms 1.14.1.2 Psychotherapy as a biological treatment 1.14.1.3 Psychopathology is the fundamental essence of
1.15 the psychiatry
1.14.2 Psychopathology
1.14.2.1 Descriptive psychopathology
1.14.2.2 Clinical psychopathology
1.14.2.3 Theoretical psychopathology
1.14.2.4
2.
Bhawna Paliwal, Siddhartha Dan, Sushil Kumar Upadhyay, and Sunil
3.
2.5 Crucial Benefits of Sleep Diagnosis of Disorder of Consciousness Sleep–Wake Cycle
2.4.1 Rhythmic Eye Motion Sleep and Slow-Wave Sleep
2.4.2
Siddhartha Dan, Ketan D. Kulkarni, Bhawana Paliwal, Mahasweta Mandal, Deepti Sharma, Sushil Kumar Upadhyay, and Vikas Kumar
3.1
3.2 Techniques of Visual Field
3.3
3.4 Visual Input
3.5 Central Visual Pathways
3.5.1 Electrophysiology in Neuroophthalmology
3.5.2 Abnormalities of Optic Disc
3.6 Medicine in Neuro-ophthalmology
3.7 Neuro-ophthalmology of Meningiomas
3.8
3.9
4. Neuro-otology: Dizziness, Vertigo, Imbalance, and
Karishma Sharma, Kartikey Rastogi, Siddhartha Dan, Renu Bansal, and Sushil Kumar Upadhyay
4.4.8 Presyncopal Dizziness 4.4.9
5. Inborn Errors of Metabolism: From Toxic, Metabolic, and Physical Insults to Neurodegenerative Disorders
Rashmi Pandey, Nandini Pharasi, Prasanjeet Kaur, and Lajpreet Kaur
5.3 5.4
5.5
5.15
6.2.3
6.2.2.1
6.2.2.3
6.2.2.4 Huntington’s disease
6.2.2.5 Major depressive disorder
6.2.3.2
6.2.3.3
6.2.3.4
6.3
6.2.4
6.2.3.5 Biogenesis of lncRNA
6.2.3.6 Role of lncRNA in neurological disorders
6.2.5 Regulation of Astrocytic Glutamate Transporters in Brain
6.2.4.1 Presence of glutamate transporters in the brain
Neurodegenerative Disorders and Astrocytic Glutamate Transporter Dysfunction
6.2.5.1
6.2.5.3 Huntington’s disease
6.2.5.4 Epilepsy
6.2.6
Other Molecular Etiology of Neurological Disorders
6.2.6.3 Huntington’s disease
6.2.6.4 Major depressive disorder
6.2.6.5 Amyotrophic lateral sclerosis
6.2.6.6 Autism spectrum disorder
6.2.7 Therapeutics
Immunological Gene Expression in Neurological Disorders
6.3.1 Microglial Dysfunction and Neurological Disorder
6.3.3
6.3.4 Expression of Immunological Genes in Aging Brain
Interplay between Viral Genes in Neurological Disorders
6.3.4.1 Amyotrophic lateral sclerosis
6.3.4.2
6.4
6.3.4.4 Migraine
6.3.4.5 Complex regional pain syndrome 6.3.4.6 Autism spectrum disorder
7. Clinical Perspective and Overview of Spinal Cord Disorders and Cerebellar Ataxias
Shafia Mushtaq, Towfeeq Bilal, Ibraq Khurshid, Wajid Mohammad Sheikh, Aizul Khursheed, Jasmeena Jan, Sheikh Abid Ali, Showket Ul Nabi, Mohd Ashraf Ganie, Showkeen Muzamil, and Shabir Hassan 7.1 Introduction
7.2
7.3 Spinal Cord
7.2.1 Anatomy
7.2.2 Spinal Meninges
7.2.3 Blood Supply
7.2.4 Spinal Cord Tracts
7.2.5 Spinal Nerves
Spinal Cord Disorders: Overview and Clinical Perspective
7.3.1 Classification of Spinal Cord Syndromes
7.3.1.1 Complete (transverse) spinal cord syndrome
7.3.1.2 Incomplete spinal cord lesions
7.3.1.3 Central cord syndrome
7.3.1.4 Brown–Séquard syndrome
7.3.1.5 Anterior cord syndrome
7.3.1.6 Conus medullaris and
cauda equina syndromes
7.3.2 Clinical Features
7.3.3 Diagnostic Features
7.3.4
7.4
7.4.1.1 Multiple sclerosis
7.4.1.2 Transverse myelitis
7.4.1.3 Spinal subarachnoid hemorrhage
7.4.1.4 Syringomyelia
7.4.1.5 Idiopathic spastic paraparesis
7.4.1.6 HIV myelopathy
7.4.1.7 Spinal cord infarction
7.6.4
8. Neuro-oncology, Surgical Oncology, and Chemotherapy: Symptoms, Causes, and Therapy
Ashish Kumar Das, Mudassir Jan Makhdoomi, Zaffer Hamid Bhat, and Sheikh Abid Ali
8.1 Intracranial Tumors
8.2 Pathology of Brain and Spinal Tumors
8.2.1 Intramedullary Tumors
8.2.1.1 Epidermomas
8.2.1.2 Ependymoma
8.2.1.3 Myxopapillary ependymoma
8.2.1.4 Astrocytomas
8.2.2 Intradural-Extramedullary Tumors
8.2.2.1 Meningioma
8.2.2.2 Nerve sheath tumors
8.2.3 Techniques for Detection
8.2.3.1 Magnetic resonance imaging
8.2.3.2 Sample of tissue, biopsies, and surgical excision of a
8.2.3.4 PET or PET–CT scan
8.2.3.5 Biomarker testing of the tumor
8.3
8.6
8.3.1
8.3.2
8.5.1
8.5.2
8.6.1
8.7.2
8.8.1
8.9.1
8.9.2 Spinal Cord Injury
8.9.3 Peripheral Nerve Indulgence Complications with Nervous System from Chemotherapy
8.10.1 Peripheral Neuropathy
8.10.2 Stem Cell Transplantation-Related
9. Neurologic Urology Disorders: Evidence-Based
Rakesh Sahu, Bhaskar Sahu, and Ravindra K. Rawal
11.7 Alternative Silencing Techniques for Neurodegenerative Diseases
11.7.1 Oligonucleotides Antisense 11.7.2 Gene Editing (CRISPR) 11.7.3 AAVs for Nervous
12. Elements of Therapeutic Biomarkers, Prebiotics, Probiotics, and Synbiotics: Current Status and Future Perspectives of Neuro Microbiome
Deeksha Sharma, Ishita Chanana, Usman Umar Zango, Siddhartha Dan, and Sushil Kumar Upadhyay
13. Role of Microbiota in Neuroimmunomodulation: Modern Paradigm Shift toward Therapeutic Approaches of Neurological Disorders
Siddhartha Dan, Subashani, Chandrani Modak, Mansi Srivastava, Raveena, Aditi Aggarwal, Prasanjeet Kaur, and Sushil Kumar Upadhyay
Specific Bacterial Ligands and Related Host Receptors Invade and Adhere to BBB Guarding against Microbial Invasion of CNS through Nasal Cavity Why
Microbiome?
Preface
The subject neurological disorders and diseases is considered to be essential in various medical and pharma courses, research groups and pharmaceutical formulations. This book provides complete information on every aspect of neorodegenerative disorders and brain injury, including autonomic nervous system, neuro-oncology, cerebellar ataxias, spinal cord disorders, neuro-ophthalmic disorders, and neuro-otology (dizziness, vertigo, imbalance, and hearing) in a concise and informative way. Modern neuroscience has penetrated exciting and diverse frontiers into the causes, diagnosis, and treatment of neurological diseases. Clinical neurology, whilst greatly enhanced by dramatic advances in molecular biology, genetics, neurochemistry, and physiology, remains deeply rooted in practical traditions from collecting history of the disease from the patient to elicitation of physical signs. The synthesis of clinical neurology with translational research provides a fresh perspective that is practical and multidisciplinary. The blend of new science and proven practice underpins this creative approach toward investigating and improving the care of patients suffering from neurological diseases.
This book presents vital and up-to-date information on neurological disorders from the basics to advanced therapeutic approaches in various life-threatening circumstances. It harbors extensive knowledge on the applications as well as effective utilization of advanced personalized medicines, target-based nanoencapsulated phytochemicals, and herbal nanomedicines against neurological diseases, thereby having considerable implications in the field of cancer biology, encompassing pharmaceutical and life science sectors. Moreover, the book provides a strong platform for delineating the complex mechanisms underlying disease therapeutics along with the potential therapies countering the existing menace of drug resistance, especially concerning evidence-based neurological disorders. More so, the book showcases the recent advances in the use of multifaceted and molecular-mediated drug delivery for therapeutic applications. We are sure that the readers will like the
quality text and artwork of this book. The simple and reader-friendly representations of neurological disorders will help them understand the mechanisms of actions. The challenges in neurological disorders with ongoing molecular mechanism and treatment are another highlight of this book.
The chapters in this book cover a spectrum of neurological disorders, addressing the diverse range of symptoms that patients may experience, the multifactorial nature of their causes, and the evidence-supported therapeutic options available. From common conditions such as headaches and epilepsy to more complex disorders like neurodegenerative diseases, each chapter provides a detailed examination of the current state of knowledge.
The lineage and diversity of chapters in the book cover various aspects such as cranial disorders; psychiatry; psychopathology; consciousness and intensive care; neuro-ophthalmic and autonomic neural disorders; neuro-otological disorders like dizziness, vertigo, imbalance, and hearing ailments; inborn neuro-degenerative disorders, molecular and immunological mechanisms of neurological disorders; clinical perspective of spinal disorders; and cerebellar ataxias. Moreover, the book has interesting elements of neurooncology, surgical oncology and chemotherapy, neurologic-urology disorders, evidence-based clinical symptoms, and therapeutic approaches. Some chapters deal with multifaceted therapeutic advances, including neurological rehabilitation, restorative neurology, modern and targeted therapeutic approaches, therapeutic biomarkers, neuro-microbiome, and neuro-immuno modulation.
This comprehensive and meticulously researched volume provides a thorough exploration of neurological disorders, offering a reliable resource for healthcare professionals, researchers, and students seeking a deeper understanding of the intricacies surrounding symptoms, causes, and therapeutic interventions at a single platform, making it a valuable and informative resource for graduates of various universities across the globe to understand multifaceted therapeutic applications against life-threatening neurological disorders and diseases. The book is apt to the present needs and well aligned with the offered curricula in universities across the globe for under- and post-graduate as well as PhD
programs, encompassing life sciences as well as medical, paramedical, and pharmaceutical courses. Our goal is to bridge the gap between research and practice, facilitating a seamless integration of evidencebased approaches into clinical decision-making.
We extend our gratitude to the contributors for their dedication and for sharing their expertise to advance the field of neurological research and clinical practice. We sincerely hope that this book will serve as a valuable resource, fostering a deeper appreciation for evidence-based approaches in the understanding and management of neurological disorders. Our special thanks goes to the editorial and production teams of Jenny Stanford Publishing, who were available all the time to impart their valuable input and assistance.
Sushil Kumar Upadhyay Siddhartha Dan Sheikh Abid Ali February 2024
An Introduction to Cranial Nerve Disorders, Psychiatry, and Psychopathology
Subashani,a Vaishnavi Kakkar,a Siddhartha Dan,b
Sushil Kumar Upadhyay,c and Anil K. Sharmac
aDepartment of Biochemistry, School of Life Sciences, Chhatrapati Shahu Ji Maharaj University Kanpur, Uttar Pradesh, India
bDepartment of Biotechnology, Dr. B. R. Ambedkar National Institute of Technology, Jalandhar, Punjab, India
cDepartment of Bio-Sciences and Technology, Maharishi Markandeshwar (Deemed to be University), Mullana-Ambala, Haryana, India sushil.upadhyay@mmumullana.org
The cranial nerves are responsible for providing motor and sensory functions in the body. Peripheral nerves make up 12 pairs of cranial nerves. These nerves have complex anatomy, and studying their structures provides an understanding of the pathology of diseases and disorders associated with cranial nerves. This chapter gives an overview of cranial nerves. The primary goals of psychiatry are the detection and treatment of mental illnesses, while the goal of
Evidence-Based Neurological Disorders: Symptoms, Causes, and Therapy
Edited by Sushil Kumar Upadhyay, Siddhartha Dan, and Sheikh Abid Ali
Copyright © 2024 Jenny Stanford Publishing Pte. Ltd.
ISBN 978-981-5129-18-2 (Hardcover), 978-1-003-49634-2 (eBook) www.jennystanford.com
2 An Introduction to Cranial Nerve Disorders, Psychiatry, and Psychopathology
psychopathology is the exploration of the mind’s abnormal state. Here we discussed the framework of psychiatry and different categories of disorders associated with the mind.
1.1 Introduction to Cranial Nerves
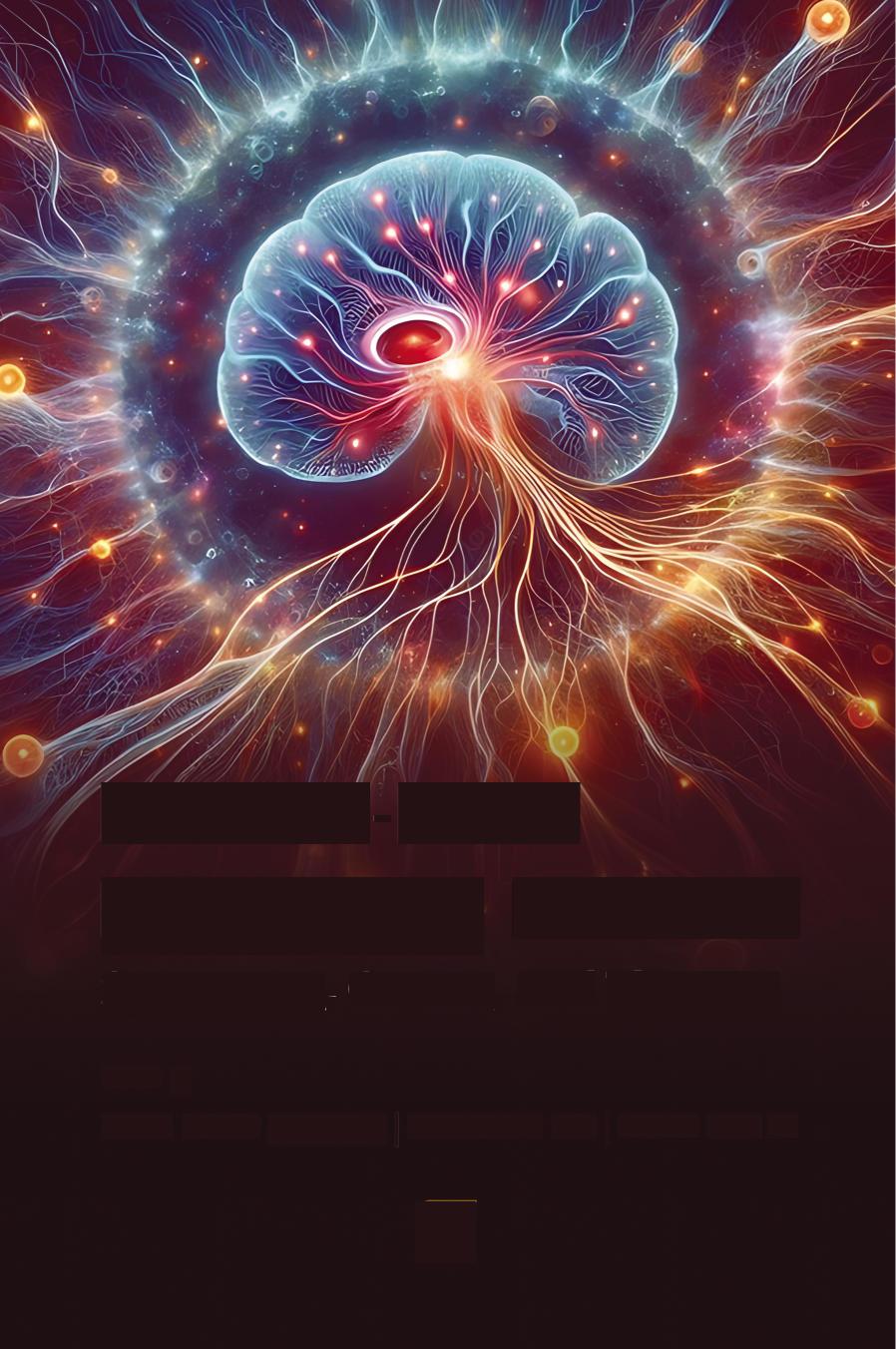
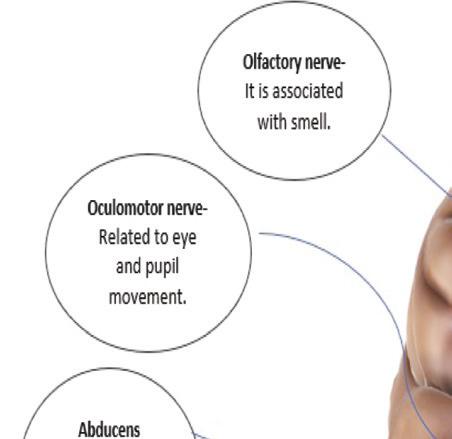
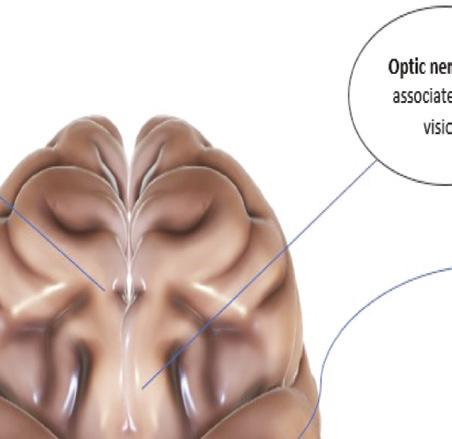
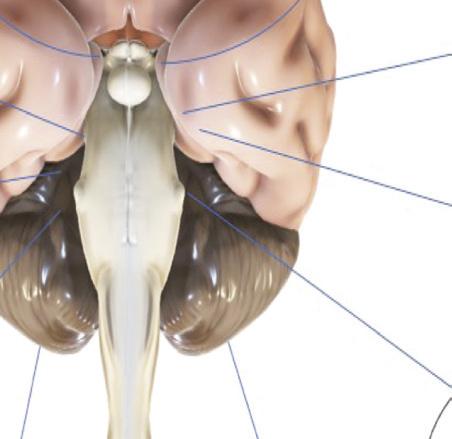
The cranial nerves in the human body control motor and sensory functions throughout the body (Fig. 1.1). It is crucial to comprehend the cranial nerve structure in order to recognize pathological alterations in situations of nervous disorders. It is, therefore, important to recognize and understand the most common symptoms and disorders associated with each cranial nerve. Dysfunctions of the cranial nerves may be brought on by illnesses, inflammation, tumors, infectious illnesses, or severe injuries to surrounding structures [1].
Olafactory nerveIt is associated with smell.
Oculomotor nerveRelated to eye and pupil movement.
Abducens nerve-Related to eye movement.
Facial nerveRelated to face movement & taste.
Optic nerveIt is associated with vision.
Trochlear nerve-Related to eye movement.
Vagus nerveRelated to movement, sensation & abdominal organs
Hypoglossal nerve-Similar functions as vagus
Accessory nerve-Related to neck movement
Trigeminal nerveRelated to face sensation.
Vestibulocochlear nerveRelated to hearing.
Glosspharyngeal nerve-Related to swallowing & taste
Figure 1.1 Diagrammatic representation of cranial nerves.
1.2 Olfactory Nerve
Our sense of smell is tied to the first cranial nerve (CN I), also known as the olfactory nerve. The olfactory nerve is paired and contains exclusively afferent sensory nerve fibers, like all cranial nerves. The olfactory nerve, along with the optic nerve, is the shortest cranial nerve and does not connect to the brainstem. Since the olfactory nerve develops from the forebrain throughout development, it is regarded as a part of the central nervous system. Olfactory glia coats the olfactory nerves instead of being myelinated by Schwann cells. The upper region of the superior turbinate, the septum, and the posterior upper aspect of both nasal cavities are lined by the olfactory epithelium, a specialized epithelial tissue. Bipolar olfactory neurons are located within this specialized epithelium, and their olfactory nerve fibers travel through the tips of these neurons. Each human nostril has 6–10 million olfactory neurons spread over an area of 2.5 cm² [2].
The basal projections of olfactory sense neurons ascend and pass the ethmoid plate as myelinated axons gathered into tiny nerve bundles known as olfactory filaments. There are between 15 and 20 of these tiny nerve bundles on either side of the nasal cavity, and they together make up an olfactory nerve. A place that could sustain injury from trauma or infection is where the olfactory nerve crosses the bony sieve plate. The cribriform pore makes it simple for infections to enter the cranial cavity and makes it easier for the olfactory nerve to be sheared during trauma. The olfactory phyla enter the olfactory bulb ventrally after passing via the subarachnoid space and cribriform plate. The dura, which covers the cerebral surface of the cribriform plate, is continuous with the foundation membrane of the olfactory epithelium, which escapes through the holes. Although the ventral surface of the olfactory bulb resides in the back third of the sieve plate, its dorsal surface lies below the inferior surface of the frontal lobes, specifically the orbital and rectus gyri. In addition to relaying signals between the primary olfactory cortex and the olfactory epithelium, the olfactory bulb is also responsible for receiving signals. Olfactory nerve testing is simple and intuitive. For the right testing, a patient must be willing, awake, and have a completely higher cognitive function, as well as an unobstructed airway and unblocked nostrils [2].
1.2.1 Disorders of the First Cranial Nerve
1.2.1.1 Congenital anosmia
Congenital anosmia is an uncommon condition defined by the lost ability to smell, with no concomitant inherited anatomical or metabolic problems. It is inherited in an autosomal dominant manner. Anosmia can occur on its own, but it can also be a sign of another disorder since birth, called the Kallman syndrome. Due to the additional and distinctive symptoms of anosmia, the Kallman syndrome is a type of hypogonadotropic hypogonadism that can be recognized from other types. During the embryonic growth of the olfaction system, neurons that synthesize the gonadotropinreleasing hormone are stopped from migrating from the olfactory epithelial surface to a region of the hypothalamus, which results in a disorder termed the Kallman syndrome. Olfactory bulbs exhibit aplasia or hypoplasia due to improper projections of olfactory neurons to the olfactory bulb from the olfactory placode [3–5].
1.2.1.2 Olfaction and tumors
Meningiomas are the most frequent cause of olfactory bulb and tract compression and bulk effects. Tumors of the front skull base can impair smell perception and can covertly manifest as anosmia. The neuroepithelium of the cribriform plate, the medium turbinate, the superior portion of the nasal septum, and the superior turbinate are the origins of the malignant tumor known as esthesioneuroblastoma (ENB). These tumors frequently develop along the cranial nerves as they pass through the skull’s bottom and enter the frontal skull base. The olfactory nerve, olfactory tract, and olfactory bulb are frequently affected by this form of malignancy. Such unique malignancies like primitive neuroectodermal tumors and olfactory ensheathing cell tumors are virtually often observed in youngsters [5, 6].
1.2.1.3 Post-trauma
anosmia
In the modern world, olfactory impairment is frequently brought on by head trauma, which can happen through a variety of causes. Three mechanisms—disturbance of the sinus or nasal passageways, tearing of the olfactory nerve fibers at the cribriform plate, and
localized hemorrhage or injury in the main olfactory cortex or olfactory bulb—are often to blame for post-traumatic olfactory impairment [7].
1.3 Optic Nerve
Vision is essential to human life since it is a powerful tool for information transmission and a source of enjoyment. The light that enters the eye passes to the receptor layer of the rods and cones in the retina, where they are, respectively, color sensitive and insensitive to light. The bipolar cells, which myelinate the ganglion cells and join them to form the optic nerve, receive impulses from these receptors. In contrast to the other cranial nerves, the optic nerve is a real part of the central nervous system, and the glial cells that are found between its fibers are made of oligodendrocytes rather than Schwann cells. A disorder that affects glial cells in the central nervous system, such as childhood-onset metabolic storage disorders, migraine, and multiple sclerosis, can therefore affect the optic nerve, while a disease that affects Schwann cells (such as the Guillain–Barre syndrome) cannot. The internal carotid artery’s ophthalmic branch nourishes the optic nerve.
The optic nerve (or second cranial nerve, CN II) is formed from the vision receptors of the retina. The bulk of the optic nerve fibers, but not all of them, crosses at the optic chiasm. The internal capsule then allows the optic tract to transfer the post-synaptic fibers from the lateral geniculate ganglion inside the thalamus to the calcarine cortex of the occipital lobe [8]. The visual field of only one eye, but some information from both eyes, is sent to each lateral geniculate ganglion. Other systems, like the auditory system, provide information to the geniculate ganglion, and this information aids the visual system in focusing on the appropriate region of the visual field [9, 10].
1.3.1 Retinal and Optic Nerve Disorders
1.3.1.1 Macular degeneration
The pigmented epithelium of the retina degenerates in at least 25% of Americans over the age of 65; regrettably, this occasionally
affects the maculae. The central vision is lost as a result. Although the peripheral vision is initially intact, it gradually deteriorates over time. Macular degeneration patients can also have complicated visual hallucinations, just like other blind people. Additionally typical of macular degeneration, depression plays a significant role in the overall disability [11, 12].
1.3.1.2 Occlusion
of the central retinal artery
The central fovea is abnormally prominent, and the retina is diffusely pale with central retinal artery blockage (cherry red). The main symptom of central retinal artery occlusion is a sudden, painfree impairment in the affected eye. Although temporal arteritis is a possibility, an embolism is typically the cause [8].
1.3.1.3 Illusions
of vision (metamorphopsias)
Form, size, movement, and color aberrations can all be signs of a visual illusion. Additionally, visual images may separate from visual memories, creating a strange feeling or déjà vu, like temporal lobe epilepsy. Micropsia, macropsia, and the perception that the object is approaching the patient are examples of visual illusions. In cases where the vestibular system is also involved, objects may also appear to invert, lose color, or shift their orientation in space. These forms of illusions are more common in the right hemisphere and are associated with lesions in the occipital, occipitoparietal, or occipitotemporal areas. They frequently come along with problems with the visual field [13].
1.3.1.4 Occlusion
of the central retinal vein
The optic disc is severely enlarged with central retinal vein blockage, along with diffuse hemorrhages and “cotton-wool” patches. The start of central venous blockage is similarly rather quick; it gets worse over a few days, and it normally does not hurt. It typically has an arteriosclerosis connection, presumably because the thicker arteriole within the adventitial envelope that both veins share at the crossing point compresses the vein [8].
1.3.1.5 Hallucinations with complex visual content and corticothalamic processes
The visual association cortex’s inhibition may have been released, or the brain may have been directly stimulated, which is what causes visual hallucinations. Visual hallucinations are primarily produced by the actions of serotonin and acetylcholine. The raphe lesion of peduncular hallucinosis (serotonin site), which causes the creation of visual hallucinations in the cortex, excites the dorsal lateral geniculate nucleus and its connections to the optical association cortex [8].
1.3.1.6 Retro-bulbar neuropathy
Retrobulbar neuropathy, which can damage the eyes either concurrently or consecutively, might happen suddenly. The optic disc may seem normal, but the vision quickly deteriorates. The eye hurts when it moves and is delicate to pressure. Usually, demyelination processes are the culprit [11].
1.3.1.7 Blind people with visual hallucinations: Bonnet syndrome
Complex visual hallucinations are most frequent in macular degeneration patients who are experiencing vision loss [14]. The 10% of people who suffer from severe visual loss experience hallucinations. These hallucinations are not stereotypical; instead, they frequently involve vivid images of people and animals that endure for hours when drowsy or only a short while when awake [15]. With eyes open, they frequently happen in the evening. Most people have insight and are not bothered by these hallucinations (unless they also have dementia) [16].
1.3.1.8 Defects in the visual system in schizophrenia
Nystagmus is one of the neurological “soft symptoms” of schizophrenia. Furthermore, schizophrenia patients may show anomalies in higher-order visual information processing [17], as well as a problem with encoding while processing faces in the right fusiform facial region of the brain (a portion of the brain that is also impacted in autism) [18].