(etextbook pdf) for julien’s primer of drug action: a comprehensive guide to the actions, uses, and
(eTextbook PDF) for
Primer
Visit to download the full and correct content document: https://ebookmass.com/product/etextbook-pdf-for-juliens-primer-of-drug-action-a-com prehensive-guide-to-the-actions-uses-and-side-effects-of-psychoactive-drugs-14th-ed itio/
More products digital (pdf, epub, mobi) instant download maybe you interests ...
Drug-Induced Ocular Side Effects: Clinical Ocular Toxicology 8th Edition Frederick T. Fraunfelder
Claire Advokat received her Ph.D. in physiological psychology from Rutgers University, following which she completed an NIH Postdoctoral Fellowship at the College of Physicians and Surgeons of Columbia University in New York City. She then served on the faculty of the Department of Pharmacology at the University of Illinois Health Sciences Center in Chicago. In 1989, she joined the Department of Psychology at Louisiana State University, retiring in 2012 as an emerita professor. Her area of expertise is the neurobiology of psychoactive drugs, including substances of abuse as well as medications developed for the treatment of mental disorders.
Joseph E. Comaty received his M.S. in experimental psychology from Villanova University, his Ph.D. in psychology with a specialization in clinical neuropsychology from the Rosalind Franklin University of Medicine and Science in Illinois, and his postdoctoral Master’s Degree in clinical psychopharmacology from Alliant University/CSPP in California. He retired from his position as chief psychologist, HIPAA privacy officer, and director of the Division of Quality Management of the Louisiana State Office of Behavioral Health, Louisiana Department of Health, in Baton Rouge. He currently serves as a consultant to that agency, conducts forensic fitness for duty evaluations, and has also held an adjunct faculty appointment in the Department of Psychology, Louisiana State University. Dr. Comaty is
a clinical and medical psychologist, licensed to prescribe psychotherapeutic drugs in the state of Louisiana.
Robert M. Julien, M.D., received his M.S. and Ph.D. in pharmacology from the University of Washington and his medical degree from the University of California at Irvine. His many research articles focus on the psychopharmacology of sedative and antiepileptic drugs. Formerly an associate professor of pharmacology and anesthesiology at the Oregon Health Sciences University, Dr. Julien retired as staff anesthesiologist at St. Vincent Hospital and Medical Center in Portland, Oregon. For over three decades, Dr. Julien single-handedly accomplished the herculean task of revising each edition and maintaining a succinct yet comprehensive and clear review of the most up-to-date advances in psychopharmacology. He is also an active consultant and lecturer on pharmacology and anesthesiology.
CONTENTS
Preface
PART 1
Introduction to Psychopharmacology
Biological Basis of Drug Action
1 Pharmacokinetics: How Drugs Are Handled by the Body
Drug Absorption
Drug Distribution
Termination of Drug Action
Time Course of Drug Distribution and Elimination: The Concept of Drug Half-Life
Drug Half-Life, Accumulation, and Steady State
Therapeutic Drug Monitoring
Drug Tolerance and Dependence
2 The Neuron, Synaptic Transmission, and Neurotransmitters
Overall Organization of the Brain
Overview of Synaptic Transmission
Specific Neurotransmitters
Monoaminergic Neurotransmitters
3 Pharmacodynamics: How Drugs Act
Receptors for Drug Action
Dose–Response Relationships
Variability in Drug Responsiveness The Therapeutic Index
PART 2
Pharmacology of Drugs of Abuse
Therapeutic Potential for Drugs of Abuse
4 Epidemiology and Neurobiology of Addiction
Extent of the Drug Problem
Nosology and Psychopathology of Substance Abuse
Neurobiology of Addiction
Pharmacotherapy of Substance Use Disorders
New Directions
5 Ethyl Alcohol and the Inhalants of Abuse
ETHYL ALCOHOL
Pharmacokinetics of Alcohol
Pharmacodynamics
Pharmacological Effects
Psychological Effects
Tolerance, Dependence, and Withdrawal
Toxicity
Teratogenic Effects
Alcoholism and Its Pharmacological Treatment
INHALANTS OF ABUSE
Why Inhalants Are Abused and Who Abuses Them
Consequences of Acute Use of Inhalants
Long-Term Consequences of Chronic Inhalant Abuse
Chapter 5 Appendix: What is a Drink? How Much Alcohol is in Your Drink?
6 Caffeine and Nicotine
CAFFEINE
Pharmacokinetics
Pharmacological Effects
Mechanism of Action
Reproductive Effects
Tolerance and Dependence
NICOTINE
Epidemiology and Public Policy
Pharmacokinetics
Mechanism of Action
Pharmacological Effects
Tolerance and Dependence
Toxicity
Effects of Passive Smoke
Effects During Pregnancy
Pharmacological Approaches to Nicotine Dependence
7 Cocaine, the Amphetamines, and Other Psychostimulants
COCAINE
History
Forms of Cocaine
Pharmacokinetics
Mechanism of Action
Pharmacological Effects in Human Beings
Comorbidity
Cocaine and Pregnancy
AMPHETAMINES
History
Pharmacokinetics of Amphetamine Compared with Cocaine
Mechanism of Action
Pharmacological Effects
Methamphetamine
Tolerance and Dependence
NONAMPHETAMINE BEHAVIORAL STIMULANTS
Synthetic Cathinones (Bath Salts)
Flakka (α-pyrrolidinovalerophenone)
Pharmacological Treatment of Stimulant Dependency
8 Psychedelic Drugs
Scopolamine: The Prototype Anticholinergic (ACh)
Psychedelic
Monoaminergic Psychedelics
Catecholaminergic Psychedelics
Serotonergic Psychedelics
Glutaminergic NMDA Receptor Antagonists
Salvinorin A
9 Cannabis: A New Look at an Ancient Plant
Epidemiology
History
What Is Cannabis?
Mechanism of Action: Cannabinoid Receptors
Endocannabinoids
Pharmacokinetics
Pharmacological Effects of Cannabis
Synthetic Cannabinoid Agonists of Abuse
Cannabis Tolerance, Withdrawal, Addiction, and Dependence
Treatment Issues
10 Opioid Analgesics
Opioid Misuse and Abuse
Opioid Terminology
History
Pain Signaling
Opioid Receptors
Major Pharmacological Effects of Opiates
Genetic Opioid Metabolic Defects
Tolerance and Dependence
Full Opioid Agonists
Partial Agonists
Mixed Agonist-Antagonist Opioids
Pure Opioid Antagonists
Novel Opioid-Based Compounds Under Development
Future Pharmacotherapy of Opioid Dependence
Illicit Opioids of Abuse
PART 3
Psychotherapeutic Drugs
11 Antipsychotic Drugs
Schizophrenia
Historical Background and Classification of Antipsychotic Drugs
First-Generation Antipsychotics
Second-Generation Antipsychotics
Prominent Side Effects of Second-Generation Antipsychotics
CATIE and CUtLASS Studies
In the Pipeline
Recommendations for the Treatment of Schizophrenia
Additional Applications for Second-Generation Antipsychotics
Additional, Alternative, and Future Approaches to Treatment
Ketamine and Other Glutaminergic Antagonists
Experimental Agents
In the Pipeline
13 Anxiolytics, Sedative Hypnotics, Anesthetics, and Anticonvulsants
Clinical Indications
Historical Background
Sites and Mechanisms of Action
Sedative-Induced Brain Dysfunction
Barbiturates
Nonbarbiturate Sedative-Hypnotic Drugs
Benzodiazepines
Flumazenil: A Benzodiazepine Receptor Antagonist
New Approaches for the Treatment of Anxiety
Drugs Intended for the Treatment of Insomnia
General Anesthetics
Antiepileptic Drugs
14 Drugs Used to Treat Bipolar Disorder
Bipolar Disorder
Diagnostic and Treatment Issues
STEP-BD Study
Mood Stabilizers: Lithium
Mood Stabilizers: Antiepileptic Drugs
Atypical Antipsychotics for Bipolar Disorder
In the Pipeline
Psychotherapeutic and Psychosocial Treatments
PART 4
Special Populations and Integration
15 Child and Adolescent Psychopharmacology
Pregnancy and Psychotropic Drugs
Drugs of Abuse in Children and Adolescents
Antidepressants in Childhood and Adolescence
Antipsychotics in Children and Adolescents
Anxiolytics in Children and Adolescents
Medications for the Treatment of Bipolar Disorder
Medications for Treating Autism Spectrum Disorders
Medications for Treating Behavioral or Aggressive Disorders
Analgesics in Childhood and Adolescence
Attention Deficit/Hyperactivity Disorder
16 Geriatric Psychopharmacology
Inappropriate Drug Use in the Elderly
Control of Agitated and Aggressive Behaviors in the Elderly
Undertreatment of the Elderly: Focus on Depression
Parkinson’s Disease
Alzheimer’s Disease
17 Challenging Times for Mental Health
Epidemiology of Mental Illness
Appendix A: Quick Reference to Psychotropic Medication
Appendix B: Introduction to Epigenetics
Glossary
Index
PREFACE
The fourteenth edition of Julien’s Primer of Drug Action marks over 40 years of continuous publication of this now classic textbook, which has as its goal the documentation of current understanding and advances in the psychopharmacological treatment of mental illness and substance abuse.
Historical discoveries that certain chemical compounds could help people who suffer from psychosis, depression, anxiety, mania, and other neurological and psychological conditions led to the development of medications that greatly improved the treatment of these devastating disorders. And similarly, during this time, there has been a corresponding explosion in our knowledge of the neurological substrates, the receptors, and enzymes that are affected by these drugs (discussed in Chapter 3), and an appreciation that they can be most effective when integrated with appropriate behavioral therapy. Unfortunately, progress in the basic science of psychopharmacology has not yet produced corresponding clinical improvements.
As with each of the prior editions, we strive in the fourteenth edition to present the information in a clear, concise, and timely manner, describing the general principles of each class of psychoactive drugs, as well as providing specific information about the individual agents. Each chapter includes an overview of the
current models of the disorders, background and mechanisms of action of the drugs, and rationales for drug treatment. Chapters on drugs of abuse provide historical context and epidemiological updates, discussions of the classic agents, and descriptions of the most recent drugs of concern, as well as the latest developments in regard to pharmacological treatments of these disorders.
As in earlier editions, each chapter of the fourteenth edition has been revised to reflect the latest developments in the field. A broad overview of these changes since the last edition suggests the following prominent themes.
First, there has been continued expansion of the clinical indications for the major therapeutic drug classes. These ongoing changes reflect efforts on the part of the pharmaceutical companies to expand the use of their products to a broader array of behavioral health conditions.
Second, the rate of drug development for the treatment of behavioral health disorders has slowed. Although a few new agents have been brought to market since the last edition of this book, most of these agents are so-called “me too” drugs that are similar to those already on the market. In addition, the newer medications, referred to as “second generation” or even “third generation,” have not been shown to produce better outcomes compared to what are referred to as “first generation” drugs originally marketed in the mid to late 1950s. The differences among these drugs are more a reflection of
differing side effect profiles. This understanding has revived interest in the original agents and in comparisons of therapeutic effectiveness, not only among psychiatric medications, but also between pharmacological and nonpharmacological treatments. Accordingly, the discussion of antipsychotic drugs (Chapter 11) has been completely revised and updated to reflect current concepts of psychopharmacological mechanisms of action.
Third, one practical effect of this pessimistic view is a decrease in current pharmaceutical investment into research and development of new psychotropic medications—but with two exceptions. The first is the ongoing research, so far unsuccessful, for treatments of Alzheimer’s disease (Chapter 16). The second major area of current psychiatric drug research involves an old drug, ketamine. This anesthetic agent has recently been shown to be a rapid-acting and effective antidepressant drug. Due to safety concerns and its short duration of action, ketamine itself cannot yet be used for routine clinical applications. Nevertheless, this finding has generated new interest in developing agents that have the same efficacy without the attendant risks (Chapter 12).
Fourth, although drug development may be undergoing a hiatus, there has been continuing interest in understanding the genetic basis of the disorders, drug effects, and interactions. Increased knowledge of how the environment interacts with our genetic substrate is having a profound effect on all aspects of medicine and in our context, especially on theories of addiction and how genetic susceptibility is
involved in the etiology of substance abuse. In this edition, we have expanded the section on epigenetics with a summary of the CRISPRCas9 gene editing tool (Appendix B).
Fifth, there is increasing overlap between the therapeutic and addictive effects of drugs. Many therapeutic drugs, such as the stimulants (Chapters 6 and 7) and especially the opiates (Chapter 10), are involved in the ongoing epidemic of abuse and overdose deaths. Extraordinary efforts are being made to develop products that are resistant to misuse and diversion. At the same time, research on substances primarily considered to be drugs of abuse, such as hallucinogens (Chapter 8) and cannabis (Chapter 9), is revealing new therapeutic possibilities. As always, we are optimistic that scientific investigation will result in new insights into the etiology of mental illness and addiction and that the future will bring more effective treatments for these devastating disorders.
It is unrealistic to expect practitioners to read and analyze the field critically. Prescribers rely on sources of information that can be presented in compact formats or review articles that provide an informed, comprehensive summary of the important topics. Such resources include publications such as the Carlat Psychiatry Report, which does not accept any advertisements or drug company money, studies funded by government agencies such as the National Institute of Mental Health (NIMH), reviews of information by the Agency for Healthcare Research and Quality (AHRQ), and the Cochrane Library reviews. None of the authors of this book have financial ties with the
pharmaceutical industry and we strive to ensure that the information we provide is as objective and unbiased as possible.
Finally, we appreciate that keeping current with medical literature is a daunting task. Even the most dedicated authors of textbooks on psychopharmacology too often miss some important developments. We also acknowledge that in order to be as succinct as possible, while remaining comprehensive, clinical data receive greater attention than preclinical results. We made this decision because it is difficult to predict whether or which preclinical outcomes will produce clinical breakthroughs. We accept the risk that by doing so, we may miss some important subsequent developments.
We are indebted to our colleagues, who review each edition and offer valuable criticism and suggestions for improvement. Their input is very much appreciated and we have attempted to incorporate their recommendations as much as possible. While making every effort to accommodate many of their proposals, we acknowledge and regret that we may have fallen short in some instances.
Dedication
Robert M. Julien, MD, Ph.D., was solely responsible for originally authoring and regularly updating this well-known book for over 30 years, beginning with the first edition in 1975. Dr. Julien’s unique achievement was to author a text that has served for decades to make the immense amount of information accessible and timely to all those interested in understanding this important area of study. It is a testament to his expertise and dedication that the Primer of Drug Action has through the years attained and maintained its reputation as a resource that is always relevant, accurate, and remarkably up to date. Beginning with the eleventh edition, published in 2008, we have been honored to have been selected by Bob to join him in contributing to this stellar work. Only by being involved as authors over the last three editions and now the current one have we fully appreciated what a tremendous accomplishment it is for one person to have done what Bob has accomplished. And on top of his immense scholarship, integrity, and generosity, Bob is a wonderful person who is a delight to work with and who we are grateful to call our friend and colleague. So, it is a great honor to dedicate this fourteenth edition of Julien’s Primer of Drug Action to Dr. Robert Julien on the occasion of his seventy-fifth birthday. Happy Birthday, Bob!
Claire D. Advokat, Ph.D.
Joseph E. Comaty, Ph.D., M.P.
Introduction to Psychopharmacology
BIOLOGICAL BASIS OF DRUG ACTION
Pharmacology is the science of how drugs affect the body. Psychopharmacology, a subdivision of pharmacology, is the study of how drugs specifically affect the brain and behavior. To understand the actions, behavioral uses, therapeutic uses, and abuse potentials of psychoactive drugs, we need to know how the body responds when we take such drugs. This understanding involves some knowledge of brain anatomy, the basic principles of drug absorption, distribution, metabolism, and excretion (collectively termed pharmacokinetics), as well as the interactions of a drug with its “receptor,” or the structure with which the drug interacts to produce its effects (the area of study termed pharmacodynamics).
This book specifically concerns drugs that affect the brain and behavior. It is an introduction to psychopharmacology, presenting not only drugs useful in treating psychological disorders, but also drugs prone to compulsive use and abuse. The book begins with three chapters devoted to the fundamentals of drug action.
Chapter 1 explores the area of pharmacokinetics, the movement of drug molecules into, through, and out of the body. It addresses such questions as: What are the ways by which drugs get into the body and how does that relate to their actions? Once in the body, how do drugs get to the sites at which they produce their effects? Once a drug exerts its effect, how is that action terminated? Finally, how does the body eventually get rid of the drug?
For readers without a background in neuroscience, Chapter 2 introduces the structure and function of the nervous system and the neuron, because this is where psychoactive drugs produce their effects. We focus on the connection between two different neurons, the synapse, and the chemical substances through which neurons communicate, the neurotransmitters. By studying the process of synaptic transmission, we begin to understand the mode of action of psychoactive drugs. The phenomenon of synaptic transmission is not static; rather, neurons have the ability to remodel themselves continually, a process called synaptic plasticity, which mediates learning and memory as well as such disorders as anxiety, depression, and addiction. A healthy, functioning brain is one that through this process of synaptic plasticity is continually remodeling itself in response to the environment. Healthy neurons continually form new synaptic contacts, maintaining the beautiful architecture that exists through normal interactions with millions of other neurons.
Chapter 3 explores the area of pharmacodynamics. It examines the
interaction between drugs and the receptors to which the drugs attach and through which they produce their effects. Receptors are described both structurally and functionally, and how drugs alter receptor structure and function is discussed. Finally, we summarize the ways in which such actions underlie the therapeutic effects and the side effects of drugs. These three chapters provide the basic foundation for understanding more specific information in subsequent chapters.
Pharmacokinetics: How Drugs Are Handled by the Body
When we have a headache, we take it for granted that after taking some aspirin our headache will probably disappear within 15 to 30 minutes. We also take it for granted that, unless we take more aspirin later, the headache may recur within 3 or 4 hours. This familiar scenario illustrates four basic processes in the branch of pharmacology called pharmacokinetics. Using the aspirin example, the four processes are as follows:
1. Absorption of the aspirin into the body from the swallowed tablet
2. Distribution of the aspirin throughout the body, including into a fetus if a female is pregnant at the time the drug is taken
3. Metabolism (detoxification or breakdown) of the drug as the aspirin that has exerted its analgesic effect is broken down into metabolites (by-products or waste products) that no longer exert any effect
4. Elimination of the metabolic waste products, usually in the urine
These four processes are sometimes abbreviated as ADME. In concert, they determine the bioavailability of a drug, that is, how much of the drug that is administered actually reaches its target.
The goal of this chapter is to introduce these pharmacokinetic processes. Because many drugs need to be taken chronically and for various periods of time, the chapter also explores the steady-state maintenance of therapeutic blood levels of drugs in the body and the usefulness of therapeutic drug monitoring. Finally, the chapter introduces the concepts of drug tolerance and drug dependence.
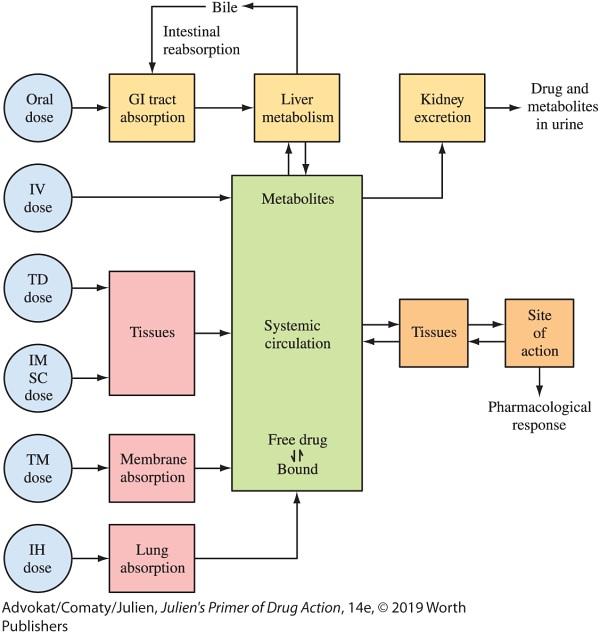
In its simplest form, pharmacokinetics describes the time course of a particular drug’s actions the time to onset and the duration of effect. Usually, the time course simply reflects the amount of time required for the rise and fall of the drug’s concentration at the target site. Figure 1.1 summarizes drug movement through the body and its equilibrium at its site of action.
FIGURE 1.1 Schematic representation of the fate of a drug in the body IM = intramuscular; IV = intravenous; TM = transmembrane; SC = subcutaneous; TD = transdermal; IH = inhalational.
The root kinetics in the word pharmacokinetics implies movement and time. Knowledge of movement and time offers significant insight into the action of a drug. At the very least, it helps distinguish a
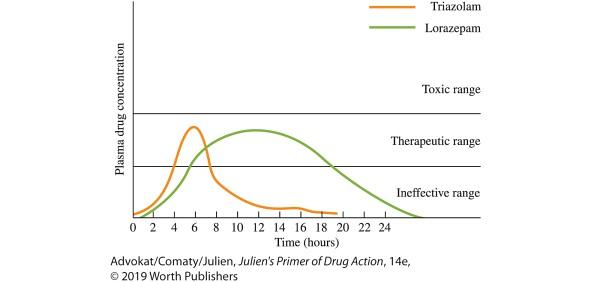
particular drug from other related drugs. For example, the main difference between the two benzodiazepines (see Chapter 13) lorazepam (Ativan) and triazolam (Halcion) is in their pharmacokinetics. Both these drugs depress the functioning of the brain, causing sedative and antianxiety effects. Lorazepam, however, persists for at least 24 hours in the body, while triazolam persists for only about 6 to 8 hours. If lorazepam is administered at bedtime for treatment of insomnia, daytime sedation the next day can be a problem, because lorazepam persists in the body through the next day. But for a longer, steady action, as might be useful in treating anxiety, lorazepam would be the superior agent to use.
2
The kinetic differences between lorazepam and triazolam are illustrated in Figure 1.2, which shows three ranges in the blood plasma: an ineffective range (where not enough drug is present to produce either sedative or antianxiety effect), a therapeutic range, and a toxic range (where sedation becomes excessive). Triazolam reaches peak blood level rapidly and is of short duration. Lorazepam, on the other hand, reaches peak blood level later and persists longer in the therapeutic range. In essence, pharmacokinetic differences account for these results and allow two similar drugs to be used to achieve different therapeutic goals.
FIGURE 1.2 Theoretical blood levels of triazolam (a short-acting benzodiazepine) and lorazepam (a longer-acting benzodiazepine) over time following oral administration. Approximations for ineffective, therapeutic, and toxic blood levels are shown
DRUG ABSORPTION
The term drug absorption refers to processes and mechanisms by which drugs pass from the external world into the bloodstream. For any drug, a route of administration, a dose of the drug, and a dosage form (liquid, tablet, capsule, injection, patch, spray, or gum) must be selected that will both place the drug at its site of action in a pharmacologically effective concentration and maintain the concentration for an adequate period of time. Drugs are most commonly administered in one of six ways, which may be divided into two categories:
1. Enteral routes refer to administration involving the gastrointestinal (GI) tract:
a. Orally (swallowed when taken by mouth)
b. Rectally (embedded in a suppository, which is placed in the rectum)
2. Parenteral routes refer to administration that does not involve the GI tract:
a. Injected (given in liquid form with a needle and syringe)
b. Inhaled through the lungs as gases, as vapors, or as particles carried in smoke or in an aerosol
c. Absorbed through the skin (usually as a drug-containing skin patch)
d. Absorbed through mucous membranes (from “snorting,” or sniffing, the drug, with the drug depositing on the oral or nasal mucosa; termed insufflation)
Oral Administration
To be effective when administered orally, a drug must be soluble (able to dissolve) and stable in stomach fluid (not destroyed by gastric acids), enter the intestine, penetrate the lining of the stomach or intestine, and pass into the bloodstream. Because they are already in solution, drugs that are administered in liquid form tend to be absorbed more rapidly than those given in tablet or capsule form. When a drug is taken in solid form, both the rate at which it dissolves and its chemistry limit the rate of absorption. Food in the stomach may either increase or decrease the rate of absorption; carbonation may speed up absorption. As an example, absorption of the antipsychotic drug ziprasidone (Geodon) is cut in half if taken without food (Carlat, 2011). In some cases, rather than the active drug itself, the oral formulation contains a precursor (forerunner) of a drug, called a prodrug. A prodrug must undergo chemical conversion by metabolic processes before becoming an active pharmacological agent. An example of this type of medication is the drug lisdexamfetamine (Vyvanse), approved for the treatment of attention deficit/hyperactivity disorder (ADHD; see Chapter 15).
After a tablet dissolves, the drug molecules contained within it are carried into the upper intestine, where they are absorbed across the intestinal mucosa by a process of passive diffusion, passing from an area of high concentration into an area of lower concentration. This process necessitates that the drug molecules, at least to some degree,
be soluble in fat (be lipid soluble). In reality, even a small amount of lipid solubility allows for absorption after oral administration; the most lipid-soluble drugs are merely absorbed faster than less lipidsoluble drugs. In general, most psychoactive drugs have good solubility in the lipid linings of the stomach and intestine; therefore, about 75 percent (or more) of the amount of an orally administered psychoactive drug is absorbed into the bloodstream within about 1 to 3 hours after its administration.
As illustrated in Figure 1.3, the digested nutrients from the small intestine (and most of the colon—the large intestine) flow into veins, which collect into the hepatic portal vein. Through the hepatic portal vein, nutrients and other products involved in digestion are transported to the liver as a first stop before going to other organs. This occurs before general circulation of the blood to the rest of the body. As described later in this chapter, a significant amount of drug metabolism takes place in the liver during this process, which is accordingly termed first-pass metabolism.