Instant digital products (PDF, ePub, MOBI) ready for you
Download now and discover formats that fit your needs...
Community/Public Health Nursing Practice E Book: Health for Families and Populations (Maurer, Community/ Public Health Nursing Practice) 5th Edition, (Ebook PDF)
Kay J. Cowen received her BSN from East Carolina University in Greenville, North Carolina, and began her career as a staff nurse on the pediatric unit of North Carolina Baptist Hospital in Winston-Salem. She developed a special interest in the psychosocial needs of hospitalized children and preparing them for hospitalization. This led to the focus of her master’s thesis at the University of North Carolina at Greensboro (UNCG) where she received a master of science in nursing education degree with a focus in maternal child nursing.
Mrs. Cowen began her teaching career in 1984 at UNCG where she continues today as clinical professor in the Parent Child Department. Her primary responsibilities include coordinating the pediatric nursing course, teaching classroom content, and supervising a clinical group of students. Mrs. Cowen shared her passion for the psychosocial care of children and the needs of their families through her first experience as an author in the chapter “Hospital Care for Children” in Jackson & Saunders’ Child Health Nursing: A
Comprehensive Approach to the Care of Children and Their Families published in 1993.
In the classroom, Mrs. Cowen realized that students learn through a variety of teaching strategies and became especially interested in the strategy of gaming. She led a research study to evaluate the effectiveness of gaming in the classroom and subsequently continues to incorporate gaming in her teaching. In the clinical setting, Mrs. Cowen teaches her students the skills needed to care for patients and the importance of family-centered care, focusing on not only the physical needs of the child but also the psychosocial needs of the child and family.
During her teaching career, Mrs. Cowen has continued to work part time as a staff nurse: first on the pediatric unit of Moses Cone Hospital in Greensboro and then at Brenner Children’s Hospital in Winston-Salem. In 2006 she became the part-time pediatric nurse educator in Brenner’s Family Resource Center. Through this role she is able to extend her love of teaching to children and families.
Through her role as an author, Mrs. Cowen is able to extend her dedication to pediatric nursing and nursing education. She is married and the mother of twin sons.
We dedicate this book to our partners: ~our families for their unwavering support ~colleagues who have grown and learned with us, and continue to help expand our thinking ~families and children with whom we work, for teaching us the essentials of child health nursing ~students who are our collaborators now and in their future careers as nurses
Thank You
We would like to express our deep gratitude to our colleagues from schools and hospitals across the country for their time over the past 3 years. These individuals assisted us in the revision of this book by contributing and reviewing manuscript chapters and contributing to the supplements that accompany this title. Child Health Nursing: Partnering with Children & Families has benefited immeasurably from your efforts, insights, and willingness to share your expertise as teachers and nurses.
CONtriButOr
Chapter 4: genetics and genomics influence
Linda D. Ward, MN, ARNP
Clinical Assistant Professor Washington State University College of Nursing Spokane, Washington
suPPleMeNtal CONtriButOrs
Jane Brown, MSN, RN Associate Professor Walters State Community College Morristown, Tennessee
Laura L. Brown, RN, MSN, CPN Nursing Instructor Asheville Buncombe Technical Community College Asheville, North Carolina
Pamela P. DiNapoli, PhD, RN Associate Professor University of New Hampshire Durham, New Hampshire
Donna Eberly, RN, MSN Instructor Western Iowa Tech Community College Sioux City, Iowa
reviewers
Mike Aldridge, Concordia University Texas
Kim Amer, DePaul University
Janice Bidwell, San Diego State University
Sharon Koval Falkenstern, PhD, CRNP, PNP-C, CNE
Assistant Professor, Coordinator of NP Option
The Pennsylvania State University University Park, Pennsylvania
Leslie Holmes, RN, BSN, MSN Instructor, Family and Community Nursing Nell Hodgson Woodruff SON Emory University Atlanta, Georgia
Mary Jo Konkloski, RN, MSN, ANP Coordinator, RN Program
Finger Lakes Health College of Nursing Geneva, New York
Patricia Kuster, PhD, RN, CPNP
Assistant Professor
Samuel Merritt College School of Nursing Sacramento, California
Brenda Lykins, RNC-NIC, BSN
Neonatal Outreach Coordinator MultiCare Regional Perinatal Outreach Program Tacoma, Washington
Adelaide R. McCulloch
Patricia Bobbitt, Wake Forest University School of Medicine
Sally Brooks, The University of Louisiana at Monroe
Michael Brown, The University of Texas Health Science Center at Houston
Karyn Casey, The University of Tennessee
Teresa Chase, University of Kentucky
Jennifer Compere, Brenner Children’s Hospital
Joseph De Santis, University of Miami
Linda Esposito, Wake Forest Baptist Medical Center
Melissa Ethington, The University of Texas Health Science Center at Houston
Niki Fogg, Texas Woman’s University
Betty Freund, Kent State University
Julie Garcia, The University of Texas Health Science Center at San Antonio
Carol Hall Grantham, Georgia State University
Debbie Hancock, The University of North Carolina at Greensboro
Kristen Harrison, Wake Forest Baptist Medical Center
Amy Zlomek Hedden, California State University, Bakersfield
Michelle Howell, Wake Forest Baptist Medical Center
Kim Hutchinson, Wake Forest Baptist Medical Center
Arlene Johnson, Clemson University
Eleanor Kehoe, College of Staten Island
Mary Kishman, College of Mount St. Joseph
Julie Kordsmeier, The University of North Carolina at Greensboro
Heidi Krowchuk, The University of North Carolina at Greensboro
Laura Kubin, Texas Woman’s University
Brenda Millet, MSN, RN-BC Staff Development Specialist Children’s National Medical Center Washington, DC
Cheryl Shaffer, RN, MS, PNP, ANP, PhD(c) Associate Professor Suffolk County Community College Selden, New York
Lisa D. South, RN, DSN Assistant Professor
The University of Alabama at Birmingham Birmingham, Alabama
Jane K. Walker, BBA, RN, CLNC, PhD(c)
Associate Professor of Nursing
Walters State Community College Morristown, Tennessee
Jeannie Weston, MS, CNS, BSN
Assistant Clinical Instructor Emory University Atlanta, Georgia
Sarah Kulinski, Lenoir-Rhyne University
Patricia Kuster, Samuel Merritt University
Lin Lin, The University of Texas Health Science Center at Houston
Antoinette McCray, Norfolk State University
Cheryl Mele, Drexel University
Mary Ellen Mitchell-Rosen, Nova Southeastern University
Heidi Monroe, Seattle Pacific University
Brenda Pavill, University of North Carolina Wilmington
Sue Perkins, Washington State University
Kathleen Peterson, The College at Brockport
Janice Pitman, Brenner Children’s Hospital
Kari Crawford Plant, Levine Children’s Hospital
Deborah Roberts, Sonoma State University
T. Kim Rodehorst-Weber, University of Nebraska Medical Center
Carol Rossman, Calvin College
Michele Shaw, Washington State University
Anita Smith, Wake Forest University School of Medicine
Daphnee Stewart, Mercer University
Phyllis Thatcher, Wake Forest Baptist Medical Center
Debra Thomson, Wake Forest Baptist Medical Center
Maureen Tippen, University of Michigan-Flint
Theresa Turick-Gibson, Hartwick College
Diane Van Os, Westminster College
Darla Vogelpohl, University of Toledo
Beverly Bockstruck West, University of Memphis
Melissa Williams, Augusta State University
Cecilia Wilson, Texas Woman’s University
Preface
The world children grow up in today is vastly different from the world we experienced in our early years. Our evolving social environment has resulted in diverse family structures and roles. Multiple racial and ethnic groups now commonly share communities, work environments, and recreation. A variety of technology applications are part of children’s daily routines. Nutritional patterns have changed due to the complexity of daily lives and food marketing, and the environment is identified as an increasing influence on child and adolescent health. The geospatial design elements of communities, including schools, modes of transportation, and safety in neighborhoods, have altered daily behaviors. Life in complex societies offers new challenges to mental health, and homes provide diverse risk and protective factors in managing the health and illness of child family members. New ways of treating diseases, from applications of genomics to a current generation of medications, influence youth health. Healthcare reform, electronic health records, new approaches to chronic and acute condition management, and a focus on prevention have contributed to changes in the information that nurses and other healthcare providers need. We draw heavily upon Healthy People 2020 in this text to guide our suggested interventions and evaluation of goals for health conditions. In addition to an evolution of influences on child health, there have been incredible achievements in nursing education. The American Association of Colleges of Nursing (AACN) published the Essentials of Baccalaureate Education for Professional Nursing Practice in 2008. While we know that many Associate Degree Nursing programs use our books, we also are aware that a number of those programs also use “the Baccalaureate Essentials” in establishing their curricula. We have therefore applied the Essentials throughout the book and cite them in a new feature (see a description later in this preface). In 2009, the “Carnegie Report” on Educating Nurses: A Call for Radical Transformation was published. This long-awaited study emphasized the importance of connecting classroom and clinical learning, focusing on clinical reasoning when working with students, and fostering career ladders and lifelong learning. These recommendations inform our clinical judgment and clinical reasoning features. Finally, in 2010, the Institute of Medicine (IOM) released The Future of Nursing: Leading Change, Advancing Health. The IOM recommended that nurses function to the full extent of their education and training, achieve higher levels of education, be full partners with physicians and other healthcare professionals in the redesign of health care, and work to plan policies that ensure data collection and information infrastructure.
Child Health Nursing: Partnering with Children & Families is a contemporary pediatric nursing textbook. Excellence in pediatric nursing care, whether it is in the acute care setting or in the community, is a challenge and the major objective guiding today’s pediatric nurse. You, as a student, will be challenged to synthesize previous information with new knowledge, apply evidence-based findings, collaborate with other healthcare professionals and families, and integrate current knowledge to use clinical reasoning skills in planning pediatric nursing care. You will be challenged to lead, examining ways in which you can positively influence the health care of children and their families in the challenging times of healthcare reform.
The third edition of Child Health Nursing builds upon the strong foundation and planning of the first two editions and addresses the
need for fresh approaches to child and adolescent health care and nursing education in several ways. Themes in this book include:
■ Partnering with Children and Their Families
■ The Roles and Essential Functions of the Nurse
■ Health Promotion and Health Maintenance
■ Collaboration with Families and Healthcare Providers
■ Evidence-Based Practice
■ Clinical Reasoning
The subtitle, Partnering with Children & Families, reflects the core value of our textbook—emphasizing family-centered care, recognition of the family as the central influence in each child’s life, and respect for families from all cultures. Families are viewed as case managers, as partners with healthcare providers, and as integral participants in care in all pediatric nursing settings. Partnership and interprofessional collaboration are other key concepts of our textbook. In the past, we introduced the BindlerBall Child Healthcare Model as a paradigm with which to view health care of children. This model illustrates an important core value—that all children need health promotion and maintenance interventions, no matter where they seek care or what health conditions they may be experiencing. Families may visit offices or other community settings, specifically to obtain health supervision care; or nurses may integrate health promotion and maintenance into the care for children with acute and chronic illness in a variety of inpatient and outpatient settings. The Bindler-Ball Healthcare Model places health promotion and maintenance at the foundation of a pyramid to demonstrate the need to apply these concepts with all children. See Chapter 1 for an introduction to this model.
what’s New iN this editiON
■ Baccalaureate Essentials Boxes highlight the nine essentials of nursing education identified by the American Association of Colleges of Nursing.
■ NANDA-I 2012-2014 nursing diagnoses for multiple conditions.
■ Updated Healthy People 2020 goals for the pediatric population.
■ More Evidence-Based Practice features emphasize nursing research and offer a critical thinking element.
■ Clinical Judgment speed bumps to encourage critical thinking.
■ Clinical Reasoning section at the end of chapter to help with application of concepts and synthesis.
■ New statistics, and integration of current health care implications and environmental considerations.
OrgaNizatiON
The six units in this textbook have a unifying theme. The first unit, Nurses, Children, and Families, lays the foundation for a thorough understanding of pediatric nursing in today’s world. It discusses the nurse’s roles in caring for children in the hospital, community, and home, as well as the concepts of family-centered care and cultural considerations.
The second unit focuses on Child Concepts and Application, melding theory with application so that concepts can be applied to pediatric nursing care in a variety of settings. Genetics and genomics are current concepts that will be increasingly employed in future health care. We describe concepts of growth and development and child/family
communication in separate chapters, and examine applications to pediatric nursing. The pediatric assessment chapter provides basic and detailed information that will be applied in all pediatric healthcare settings.
The third unit focuses on Health Promotion and Maintenance Through Childhood. The first chapter introduces basic concepts, and each of the remaining five chapters applies health promotion and maintenance concepts with specific approaches for children at each developmental stage from newborn through adolescence. Nurses assess children thoroughly, establish goals in partnership with the family, intervene to promote and maintain health and foster development, and evaluate the outcomes of care. This unique approach minimizes repetition throughout the book, and underscores the need for all children to receive routine health promotion and health maintenance to achieve optimal health.
The fourth unit, Child Healthcare Settings and Considerations, explores the various settings in which care occurs. In addition to the hospital, nurses and nursing students are likely to provide care in community settings, such as health centers, schools, and homes, where health promotion and maintenance activities predominate. Special considerations for the care of children during disasters are also discussed. Shorter hospitalizations have become the norm, thereby increasing the need for more comprehensive care in community settings, such as specialty outpatient centers where nurses coordinate care for children with various health conditions. Children need special attention when they have chronic health conditions, when they have lifethreatening illnesses or injuries, or when they need end-of-life care.
The fifth unit discusses Nursing Care for Common Health Conditions. The unit begins with a chapter on infant, child, and adolescent nutrition, which discusses both nutritional requirements for health and some common nutritional disruptions. A chapter on social and environmental influences addresses topics pertinent to children and
Visuals That Teach
The art program of this book continues to use a thoroughly integrated approach, beginning with the cover and carried through the interior of the textbook. The cover of Child Health Nursing features hand-painted tiles from Rydal Elementary School in Abington, Pennsylvania. Art is both a method of expression and a healing modality, and the feelings, design, and colors of the tiles integrated throughout this book will help you identify with children and their families, and understand their experiences.
their families in today’s world, such as violence and substance use. A chapter on pediatric pain assessment and management provides general nursing care concepts that are woven through the remainder of the book. Another chapter focuses on the prevention and treatment of infectious and communicable diseases, a significant role in pediatric nursing care.
The sixth unit consists of 14 chapters that address Nursing Care of Specific Health Conditions. Information about health conditions, including both illnesses and injuries, is grouped by body systems, eliminating the need for duplication at various places in the text. This streamlined approach builds on previous concepts rather than repeating them, integrating a developmental approach with pertinent conditions affecting all age groups from newborn to adolescent.
The chapters fully describe diseases and injuries beginning with an anatomic and physiologic overview, pediatric differences, and system-specific assessment guidelines. This is followed by a discussion of the etiology, pathophysiology, clinical manifestations, and collaborative care, including diagnostics and clinical therapy sections for each of the major conditions. Nursing management of major conditions contains detailed sections on assessment and diagnosis, planning and intervention, and evaluation of care. The book is readable and understandable, taking the student from present knowledge level to mastery of new material. The many features further enhance the readability of the material for students coming from various backgrounds and nursing programs and curricula.
Sample nursing care plans will assist you in applying developmental, psychosocial, and physiologic concepts to the care of children with specific conditions. North American Nursing Diagnosis Association (NANDA International) diagnoses are used, as well as the current Nursing Intervention Classifications (NIC) and Nursing Outcomes Classifications (NOC).
Gorges has very broad responsibilities for maintaining the health of all the children
A Day in the Life of a Nurse helps identify the roles and focus of nursing care in each of three settings: the hospital, the healthcare center, and the school setting.
PHOTO STORY. . .
MANAGING MYELODYSPLASIA
Daily exercise using crutches is
Tests for Short Stature PURPOSE RELATED TO SHORT STATURE
Screens for growth hormone deficiency
Detects pituitary malformation or tumor
testing
Tests for growth hormone deficiency
Identifies other potential causes of delayed growth
Screens for inflammatory bowel disease with anemia
Screens for celiac disease
Felner, E. I. (2011). Hypopituitarism. In R. M. Kliegman, B. F. Schor, & R. E. Behrman, Nelson textbook of pediatrics (19th ed., Saunders Elsevier; Cooke, D. W., Divall, S. A., & Radovick, S. In S. Melmed, K. S. Polonsky, P. R. Larsen, & H. M. Kronenberg, (12th ed., pp. 935–1053). Philadelphia, PA: Saunders Elsevier.
clonidine, glucagon, insulin, L-dopa) are adrelease of growth hormone, may be used to hormone deficiency. Confirmation of the disorder demonstrate a growth hormone response (with 10 ng/mL) after presentastimuli as previously menendocrinologists believe than other tests, such as low hormone deficiency may ocmore other pituitary hormay be total deficiency (no produced) or partial deficiency produced, but not enough growth).
■ Growth hormone deficiency
■ Renal failure
■ Turner syndrome
■ Noonan syndrome
■ Short stature from Prader-Willi syndrome (PWS)
■ Children with a history of intrauterine growth retardation
■ Idiopathic short stature
Source: Data from Cooke, D. W., Divall, S. A., & Radovick, S. (2011). Normal and aberrant growth. In S. Melmed, K. S. Polonsky, P. R. Larsen, & H. M. Kronenberg, Williams textbook of endocrinology (12th ed., pp. 935–1053). Philadelphia, PA: Saunders Elsevier; Ferguson, L. A. (2011). Growth hormone use in children: Necessary or designer therapy? Journal of Pediatric Health Care, 25(1), 24–30; Sperling, M. A. (2010). Treatment of short children with GH plus IGF-1: Are two hormones better than one? Infectious Diseases in Children, 23(1), 46–48.
The photographs and drawings throughout the textbook do more than illustrate concepts and examples. You will find critical thinking opportunities among the figure captions. These unique highlights, also appearing in the text itself, encourage you to apply information and analyze the nursing implications needed to provide care for children and their families, thus adding true learning value to the visuals.
Photo Stories help bring information and concepts “alive” to develop a deeper understanding about the effect of a specific condition on the child and family. These stories include photographs of a child or situation to demonstrate the challenges a child and family may face in managing the condition.
treatment are important maximum adult height estimation of skeletal maevaluate the child with a growth used to predict final height. the hand or wrist bone is stage of bone ossification and child. Using standardized ossification, radiologists can dechronologic and bone ages delayed (less than the child’s (greater than the child’s age) indicative of a systemic chronic abnormality requiring inves-
deficiency, replacement theradministered to promote growth Growth hormone replacement
requires subcutaneous injections 6 to 7 times per week and generally continues for several years until growth is complete. The pediatric endocrinologist adjusts the dosage based on response to treatment (Ferguson, 2011). See Box 32–2 The child usually experiences increased growth velocity for the first year of treatment, followed by a gradual decrease in growth for subsequent months or years. Growth should progress at least at the normal growth rate for age while the child is continued on growth hormone treatment. If growth is slower than anticipated, compliance to therapy must be considered before the dosage is increased. Replacement therapy is continued until either the child achieves an acceptable height or growth velocity drops to less than 2 cm (1 in.)
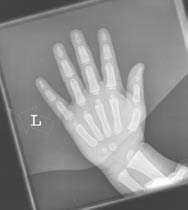
As They Grow Bone Age
FIGURE 32–4 ■ The radiograph of the hand and wrist of a 3-year-old and 13-year-old girl reveal significant differences in skeletal maturation that are closely tied to physiologic maturation. The 3-year-old has many bones in the hand and wrist that have not fully developed. The secretion of estrogen during puberty has resulted in the development and calcification of secondary ossification centers of most of the bones in the hand and wrist of the 13-year-old.
Source: Courtesy of Dorothy Bulas, M.D., Children’s National Medical Center.
As They Grow illustrations help you visualize the important anatomic and physiologic differences between a child and an adult. These features illustrate the important ways that a child’s development influences healthcare needs and how the child progresses through developmental stages.
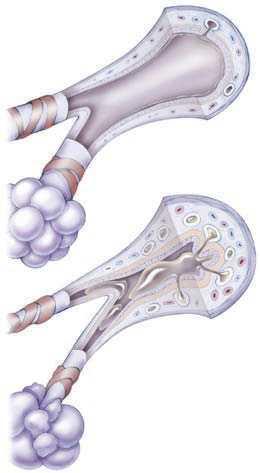
The text explains in-depth pathophysiology of pediatric conditions, and accompanying Pathophysiology Illustrated figures allow you to see into the body to visualize the causes and effects of conditions on children. These elaborate drawings illustrate conditions on a cellular or organ level, and may also portray the step-by-step process of a disease. Drawings or photos with artistic overlays relate disease to its anatomic location and action.
Pathophysiolog y Illustrated Asthmatic Episode
BOX 32–2
FDA-Approved Uses of Growth Hormone in Children
arterial exists, the oxygen
impulses, continues to increase until approximately 4 years of age. Brain growth results in the increasing head circumference in infants and toddlers. Brain growth continues until the child is 12 to 15 years of age.
TABLE 32–9 Laboratory Findings in the Child with Diabetic Ketoacidosis
Respirator y Distress and Respirator y Failure 747
come damaged in a very short time Because the nervous system helps to control and coordinate many body functions, alterations in neurologic function can have widespre ad effects on the body’s metabolism.
NEUROLOGIC ASSESSMENT
Nursing Assessment and Diagnosis
Features That Help You Use This Book Successfully
LABORATORY STUDY RESULTS
Serum glucose Greater than 200 mg/dL
cricoid cartilage, is often performed if long-term airway management is needed.
Serum ketones Positive
Myelination, the progressive covering of axons with layers of myelin or a lipid protein sheath, is also incomplete at birth. Lack of myelination is associated with the presence of primitive reflexes. As the myelination progresses, the primitive reflexes disappear. See Table 7–19 8 for the expected appearance and disappearance of primitive reflexes during early infancy This process continues throughout childhood, proceeding in a cephalocaudal direction. The myelination process accounts for the progressive acquisition of fine and gross motor skills and coordination during early childhood, and it is ultimately responsible for the speed and accuracy of nerve impulses.
Arterial blood gas pH Acidotic—pH less than 7.3 and bicarbonate less than 15 mEq/L
Urine Positive for ketones (ketonuria)
Assisted ventilation must be provided until the child breathes spontaneously or until mechani cal ventilation is initiated Children are often sedated to optimize ventilation. Continuous positive airway pressure (CPAP) is one form of PEEP used to improve oxygenation and lung compliance When respirator y failure cannot be managed, it results in cardiopulmonar y arrest.
Serum potassium Elevated, decreased, or normal
In infants and young children the vertebral bodies are wedge shaped, the ligaments permit more movement, and the articulating facets at C1 and C2 permit more sliding in cases of injury. The child’s spinal cord attains adult characteristics after 10 ye ars of age when the vertebral body loses its wedge shape and the facets become more vertically aligned (Mathison, Kadom, & Krug, 2008).
Serum chloride Elevated
Serum sodium Decreased
Continuously monitor the child’s vital signs, respiratory status, perfusion, and mental status. Assess for changes in neurologic status, respiratory pattern, blood pressure, and heart rate. Monitor for cardiac arrhythmias associated with hypokalemia. Assess for signs of dehydration, including dry skin and mucous membranes, and depressed fontanels in infants.
Performing a nursing assessment of the child with a potential or actual neurologic condition involves a careful review of the signs and symptoms in many body systems and analysis of their relationship to neurologic functioning. Use the guidelines in Table 33–3 to perform a comprehensive assessment of a child with a neurologic condition. Numerous diagnostic procedures and laboratory tests are used for the diagnosis of neurologic conditions (Table 33–4). Additional information about these diagnostic procedures and laboratory tests can be found in Appendixes D and E 8
Nursing students face challenges in their education—managing demands on their time, applying research findings, evaluating components of evidence-based practice, and developing their critical thinking skills. Thus instructors and students alike value the in-text learning aids that we include in our textbooks to meet the challenges of pediatric nursing in today’s world. We developed a textbook that is easy to learn from and easy to use as a professional reference. The following guide will help you use the features and resources from Child Health Nursing to succeed in the classroom, in the clinical setting, on the NCLEX-RN® examination, and in nursing practice.
Nursing diagnoses that apply to the child with diabetic ketoacidosis may include:
ALTERED STATES OF CONSCIOUSNESS
■ Injury, Risk for related to altered cerebral function
The brain depends on a continuous blood flow to meet its high demands for oxygen. Through an autoregulatory process, the cerebral blood vessels dilate to maintain the cerebral blood flow in response
Serum phosphate Decreased
Serum osmolality Elevated
When acute respirator y failure becomes life threatening, extracorporeal membrane oxygenation (ECMO) may be initiated (Ayad, Dietrich, & Mihalov, 2008). ECMO is a cardiopulmonar y bypass system with external oxygenation and a pump mechanism that provides respirator y and hemodynamic support. It allows the lungs to rest and heal However, several significant complications may result from its use, such as bleeding, stroke, renal insufficiency, hypertension, seizures, electrolyte abnormalities, pneumothorax, cardiac dysfunction, and infection (Ayad et al., 2008). This is a complex and expensive treatment available in special centers, so the child may have to be transferred to anot her hospital to re ceive this therapy.
■ Fluid Volume: Deficient related to osmotic diuresis
Level of consciousness (LOC) is perhaps the most important indicator of neurologic dysfunction. Consciousness, the responsiveness or awareness of the mind to sensory stimuli, has two components: (1) Alertness, or arousal, the ability to react to stimuli, is controlled
■ Nutrition, Imbalanced: Less than Body Requirements related to catabolism of protein and fat for fuel
TABLE 33–3 Assessment Guidelines for the Child with a Neurologic Condition
■ Knowledge, Deficient related to recognition, treatment, and prevention of diabetic ketoacidosis
Source: Data from Cooke, D. W., & Plotnick, L. (2008b). Management of diabetic ketoacidosis in children and adolescents. Pediatrics in Review, 29, 431–436; Jerreat, L. (2010). Managing diabetic ketoacidosis. Nursing Standard, 24(34), 49–55; McFarlane, K. (2011). An overview of diabetic ketoacidosis in children. Paediatric Nursing, 23(1), 14–19.
Assessment Guidelines for the Child tables in each of the systems chapters provide an overview of the key aspects of an integrated assessment for conditions within the body system.
Collaborative Care
Nursing Management
Level of consciousness
■ Is the infant or child difficult to arouse?
Planning and Implementation
■ Is the infant or child irritable or difficult to calm or console?
■ Is the child oriented? Can the child tell the examiner his or her name and age?
■ What is the child’s ability to concentrate? Can the young child name pictures of animals? Can the older child answer simple math questions or spell words?
■ The Glasgow Coma Scale provides a numeric score for future comparison. See Table 33–5
Cranial nerves
Fontanels and sutures
Cognitive function
Pupils
TABLE 33–6 Assessment of Cranial Ner ves in the Unconscious Child
■ Assess the cranial nerves. See Table 7–18 8 8 See Table 33–6 for methods to indirectly assess cranial nerves in the unconscious child.
■ Palpate fontanels and suture lines on the infant’s scalp.
The immediate goal of collaborative care is to normalize the pH level, restore blood glucose to target level, and correct fluid and electrolyte imbalance. The long-term goal of management includes preventive education to reduce the risk of further diabetic ketoacidosis episodes.
Vital signs
■ Are the child’s verbal skills developmentally appropriate for age?
■ Does the child follow directions and respond appropriately?
■ Check the pupils for size and reaction to light and accommodation. See Figure 33–4 on page 1154
Nursing care is focused on the recognition of progression from respiratory distress to respirator y failure and supportive care to the child and family
■ Assess heart rate, respiratory rate, and blood pressure.
Intravenous fluids are given in boluses of 10 to 20 mL/kg rapidly over 5 minutes if the child is in hypovolemic shock. Adequate fluids are given to reverse the fluid deficit. The insulin infusion must be carefully titrated to control the gradual reduction in hyperglycemia. Monitor blood glucose levels hourly or as indicated. Frequently monitor the electrolytes and acid–base status, as well as urine glucose and ketone levels as indicated. Intake and output are monitored hourly. Assess for signs of hypoglycemia which may occur during insulin infusion.
CRANIAL NERVES AND REFLEX
Diagnostic Tests
REFLEX ASSESSMENT PROCEDURE AND NORMAL FINDINGS
Posture and movement
Nursing Assessment and Diagnosis
II, III
Pupillar y Shine a light source in the eye.
II, IV, VI
Clinical Therapy
Oculocephalic
red simularbia in the emia unrefailure. spirator y mechani cal increase the pedionsiveness decreases. endotracheal protected monitorthat the hea. See eation of neck at the
See Table 32–9 for laboratory findings in diabetic ketoacidosis. CT scan of the brain and possible intubation and implementation of intracranial pressure (ICP) lowering strategies will be required.
Practice Alert
■ Inspect the infant’s posture and movement by using the primitive reflexes. See Table 7–19 8
■ Observe the child’s play or other spontaneous activity to assess strength as well as symmetry and smoothness of movements.
Monitor the child for changes in vital signs, respirator y status, and level of responsiveness. Perform the respirator y assessment using guidelines in Table 25–1 Signs and symptoms of respirator y compromise may progress rapidly. Detection of earlier subtle signs is important so interventions can be initiated to prevent progression to respirator y failure. Attach a cardiorespirator y monitor and pulse oximeter. S erial blood gases may be needed to monitor the child.
Practice Alert
III, VIII
Oculovestibular
Rapid, concentrically constricting pupils indicate intact cranial ner ves II, III.
Neck stiffness
Pain
Family history
with a demonstrates interpreting the and the pH 90 mmHg or less. than indicate oxygen to left, and the tisand the Altered States of Consciousness 1155
■ Monitor for an increased systolic blood pressure, a widened pulse pressure, bradycardia, and irregular respirations (late signs of increased intracranial pressure).
Only regular insulin is administered intravenously for treatment of hyperglycemia or diabetic ketoacidosis. Do not use other insulin types as they may lower the blood glucose too rapidly or too slowly.
■ Evaluate muscle strength and tone, comparing side to side. Is any weakness present?
■ Test the child’s coordination for smoothness and symmetry of response.
Perform with eyes held open (doll’s eyes) and head moved horizontally or vertically
■ Are the child’s motor skills developmentally appropriate for age? Were motor skills acquired at the appropriate age? Has the child lost a previously acquired skill?
The child with ketoacidosis is hospitalized. Medical management includes isotonic intravenous fluids and electrolytes for dehydration and acidosis. Short-acting insulin (0.1 unit/kg per hour) is administered by continuous intravenous infusion pump to decrease the serum glucose level at a rate not to exceed 100 mg/dL/hr. Faster reduction of hyperglycemia and serum osmolality increases the risk for cerebral edema. When glucose is lowered too rapidly, water is freed and attracted to the glucose, which has accumulated in large quantities in the brain. Bicarbonate is not routinely used for treatment of DKA as it places the child at increased risk for hypokalemia, acidosis, and cerebral edema (Cooke & Plotnick, 2008b). As insulin is administered, potassium shifts to the cells, resulting in hypokalemia. Potassium supplementation is given only after confirmation of renal function.
■ Assess deep tendon reflexes for smoothness and symmetry of response. See Table 7–20 8
intubation is performed. A tracheostomy may be performed for longterm airway management. Frequent suctioning may be required Keep suction apparatus with catheters at the bedside along with oxygen, resuscitation bag and mask, and extra endotracheal or tracheostomy tubes (if applicable). Pulse oximetry or arterial blood gas analysis is performed at regular intervals to ensure that gas exchange is adequate Assisted ventilation may be required (refer to the Skills Manual ). Anticipate that seizures may occur. Pad the side rails to protect the child from injury
■ Assess for neck stiffness (nuchal rigidity).
When head is turned suddenly to the right, the eyes of an infant or comatose patient look to the left, and similarly look to the right when the head is turned to the left. Absence of this reflex suggests brainstem dysfunction in comatose patients.
■ Assess level of pain when present.
Perform Routine Nursing Care
■ Is there a family history of headaches, seizures, neurofibromatosis, or other neurologic condition?
Precaution: Cer vical spine injur y must be ruled out before this assessment is performed.
Place the head in a midline and slightly elevated position. Inject ice water into the ear canal.
When the child has a chronic respiratory or neuromuscular condition, development of respiratory failure may be gradual as muscles associated with breathing may be weakened. Signs will be subtle. Be particularly alert to behavior changes in addition to respiratory signs. Pulse oximetr y and serial blood gases may be needed to monitor the child.
Eyes deviating toward the irrigated ear indicate intact cranial ner ves III, VIII.
Precaution: Ensure that the tympanic membrane is intact to keep fluid from entering the middle ear
Note: A physician usually performs this assessment.
V, VII Corneal Gently touch the cornea with a sterile cotton swab.
If the corneal reflex is absent, place artificial tears in the eyes and cover with gauze, taping over so they remain closed Perform routine mouth care by brushing the teeth and using swabs with water. Gently clean the oral mucosa in newborns and keep secretions from accumulating
The child is tapered off intravenous insulin and transitioned to subcutaneous insulin when clinically stable. Oral feedings are reintroduced when the child is alert enough and the glucose level is stabilized. This plan varies according to the primary healthcare provider or endocrinologist.
Clinical Tip
Provide adequate nutrition. Initially, nutrients may be supplied intravenously. A nasogastric or transpyloric tube may be inserted if the infant or child remains unconscious or is not alert enough to take food by mouth. A gastrostomy tube may be inserted if it is anticipated that enteral feeds will be needed for longer than 3 months. (S ee the Skills Manual .)
Insulin binds to IV tubing. Run 50 to 100 mL of insulin through the new IV tubing to saturate all the binding sites. This ensures that the full dose of insulin reaches the child from the outset.
If the child has an endotrache al tube or tracheostomy tube, assess for secretions that may further obstruct the airway Examples of nursing diagnoses associated with respirator y failure include:
Practice Alerts warn you of safety precautions and other nursing alerts to consider in providing safe care.
Cerebral edema is the most common cause of DKA-related deaths. Mannitol is kept on standby for treatment of neurologic symptoms secondary to cerebral edema (Cooke & Plotnik, 2008b).
A blink indicates intact cranial ner ves V, VII.
IX, X Gag Irritate the phar ynx with a tongue depressor or cotton swab.
See Chapter 33 8 for information about cerebral edema.
■ Breathing Pattern, Ineffective associ ated with prolonged tachypnea and muscle fatigue
A gagging response indicates intact cranial ner ves IX, X.
Nursing Management
■ Airway Clearance, Ineffective related to sedation and loss of protective cough reflex
Clinical Judgment
■ Communication: Verbal, Impaired related to artificial ai rway
Prevent complications associated with immobility (muscle atrophy, contractures, and skin breakdown) as described in Box 33–2 Nurses support physical therapy efforts with extra passive range of motion exercises.
Provide Sensory Stimulation
Electrolytes are replaced as needed. Potassium is not administered until the child has voided to confirm renal function. Monitor for signs and symptoms of hypokalemia, including hypotension, weak pulse, shallow respirations, and muscle weakness. Continuous cardiac monitoring is performed to detect cardiac conduction changes related to hypokalemia. Weigh the child daily. Provide emotional care and support to the child and family.
Clinical Tips are “pearls” from clinical nursing experts embedded throughout the textbook.
Care in the Community
Some signs of the intact neurologic status of an infant (newborn to 2 months of age) are a cr y with a loud and energetic quality, a strong suck, and suck-swallowing coordination. What is one additional sign?
■ Family Processes, Interrupted related to child’s life-threatening illness
Nursing care focuses on administering insulin, fluids, and electrolytes, and monitoring the child for signs and symptoms of associated complications. Once the child is stabilized, the focus of care shifts to educating the child and family on methods to prevent further episodes of diabetic ketoacidosis.
Planning and Implementation
Following are nursing diagnoses that may be appropriate for the child with an altered level of consciousness:
Position the child with respirator y distress in an upright position (by elevating the head of the bed) with the head in midline to help maintain the airway Administer oxygen as ordered (Figure 25–9 ■).
■ Breathing Pattern, Ineffective related to neuromuscular dysfunction associated with increased intracranial pressure
■ Aspiration, Risk for related to poor control of secretions with decreased level of consciousness
■ Skin Integrity, Risk for Impaired related to agitation and skin rubbing against bedding
■ Communication: Verbal, Impaired related to physiologic con-
Because the child with a severely altered level of consciousness may still be able to he ar, talking to him or her may be beneficial. Listening to music or tapes of family members talking or reading can soothe a child when family members cannot be present. Explain all procedures and actions to the parents and child. Encourage the parents to stroke and touch the child in a soothing manner
When the child becomes more alert, gradually and repeatedly orient the child to time, place, and person, depending on his or her age and level of understanding. Encourage parents to bring objects or toys from home to make the environment more familiar and promote a feeling of security
The prevention of future episodes of diabetic ketoacidosis is important. Partner with the child and family to ensure they learn strategies to keep hyperglycemic episodes from progressing to diabetic ketoacidosis. (See Partnering with Families: Preventing DKA.) Parents should have specific instructions on how often to check the blood glucose and when to check the urine for ketones when the child is
NEW! Clinical Judgment speed bumps appear when an opportunity for critical thinking arises.
Provide Emotional Support
Explain the child’s condition to the family in simple terms. Encourage parents to take part in the child’s care and therapy as much as possible
related to
term and emotional health of diagnosed provide home hool nursher facilities grows; this family, and ew on page ies to mainneeded (see re). ons are peror respirags may be of infancy with fluids, and ensure erform range of y. Physical ractures. It is keeping the Splints may provide parents
Arrange a the child’s determine educaestablished. mputers if ention proas possible not ask the g books to fer the child contributes needs. Surger y, of the child ily care are providing a members, and creates a family to respite ther a famcoordinate ce and supAsk what and family
Case Scenarios and photos at the beginning of the chapter engage you with a child’s real-life experience with a specific health challenge. Additional information about the child and family appears throughout the chapter to illustrate application of nursing care. Use the questions embedded in each scenario to apply pathophysiologic, psychosocial, family, culture, developmental, or nursing process considerations. At the end of the chapter, a detailed Clinical Reasoning in Action exercise picks up the opening scenario and asks you to apply what you have read.
Legal and Ethical Considerations Muscular Dystrophy Care
6. Integrate
ASSESSMENT FOCUS ASSESSMENT GUIDELINE
7. Summarize strategies for preparing children and families for discharge from the hospital setting.
Growth
8. Evaluate the effectiveness of teaching strategies used with the hospitalized child and his or her family
■ Carefully measure weight, length, or height and plot on a growth curve.
■ Compare measurements at different ages to assess the growth pattern over time and to assess the growth velocity.
Blood pressure/pulse
“Why
do
they need to take my tonsils out? They’re fine where they are!”
—Tiona, age 5
Anterior pituitary
Growth
The child with muscular dystrophy has a shortened life span. Parents provide comprehensive care and require support both physically and emotionally as the child’s condition progresses. The child continues to develop in many ways, especially cognitively, as the years pass. Therefore, the needs for explanation and ability to understand the diagnosis change for the child over time. Parents may have difficulty initiating discussions with the growing child about desire for end-of-life care (Penner, Cantor, & Siegel, 2010). An ethical approach to care demands that such a complex chronic disease be managed by an interdisciplinar y team that collaborates on a regular basis. The child, family, and a variety of health, social, and educational professionals should all be part of the team. The plan of care will include physical, emotional, cognitive, and palliative care; it will evolve and change as the child grows older Nurses are essential members of the team and may work with families as team managers.
Facial characteristics
Neck
Muscles
Genitalia and secondary sexual characteristics
■ Assess blood pressure and compare to expected norms for age. See Appendix B 8
■ Inspect the face for unusual features such as a protuberant tongue, protuberant eyes, or moon face.
Five-year-old Tiona Lewallen has a histor y of frequent tonsillitis and is scheduled for a tonsillectomy and adenoidectomy in the morning. Her mother has brought her in today for preoperative evaluation and instruction. Tiona has no other health problems. Her experience with health care is limited to well-child checkups and immunizations as well as several visits to the otolar yngologist in the past year She has no prior hospitalizations. Tiona will return at 6:30 a.m. for surger y. She will be admitted to the pediatric day short-stay unit for a few hours following surger y and will then be discharged home as long as she is able to drink fluids and take oral pain medication. How should the nurse assess what Tiona knows about her surger y? What techniques should be used to teach Tiona about the surger y? What instructions should Tiona’s mother receive from the nurse in the preoperative clinic related to care prior to surgery?
Clinical Re asoning in Action
INTRODUCTION
Body odor
Skin
Recall Tiona, the child described in the beginning of the chapter She is a 5-yearold girl who was admitted to the hospital for a tonsillectomy and adenoidectomy (T&A).
DESCRIPTION
Parents may exhibit feelings of guilt and hopelessness. The mother who learns she has carried the gene that affects her son can be devastated. Encourage parents to express their feelings. Genetic counseling is recommended for the entire family, and it is especially important to identify women who are carriers of one of the X-linked disorders. Siblings may feel neglected because their brother or sister is receiving so much attention. They may be concerned that they will develop the disease. Sometimes multiple children in a family are affected with the condition and as one child worsens, the effect on siblin gs is profound On the other hand, siblings without the disease may feel guilty for their good health. Encourage the parents to involve siblings in the affected child’s care to reassure them of their importance (See Chapter 16 8 for ideas about involvement of siblings in care.)
■ Palpate the neck for an enlarged thyroid or goiter.
■ Assess strength and muscle tone.
■ Assess external genitalia for signs of ambiguous genitalia, or inappropriate size for age.
■ Determine the child’s stage of development for each characteristic (breast and pubic hair for girls, genital and pubic hair for boys) by comparing to the images in Figures 7–43, 7–44, and 7–45 8 8
■ Assess the sexual maturity rating with information in Figure 7–46 8 Compare the stage of development to the age of the boy or girl to determine early or delayed onset of puberty.
■ Assess body odor for unusual smell (e.g., sweet, musty, cheesy, sweaty feet).
2. As Tiona and her mother are preparing to leave the hospital, Tiona says, “I am going to be good so I do not have to come to the hospital anymore!” How should the nurse respond?
■ Assess skin color, noting areas of unusual pigmentation.
Mental status ■ Note affect. Assess for anxiety, irritability, or lethargy.
Following Tiona’s operation, she refused to drink liquids because it hurt when she swallowed. After receiving intravenous pain medication, Tiona realized that she could swallow without too much pain and began to eat Popsicles and drink liquids. She was then switched to oral pain medication. Later in the day, Tiona was drinking liquids well enough to be discharged home.
DISCUSSION
3. Tiona’s mother states that she is worried that her daughter will not drink enough at home. What can the nurse suggest to Tiona’s mother to encourage her to drink fluids? What are the symptoms of dehydration that Tiona’s mother should watch for over the next few days?
Family history ■ Assess for family history of metabolic or endocrine disorders.
4. Children Tiona’s age have many fears and stressors related to hospitalization and surgery. How can her mother assist Tiona to express her feelings about the hospital experience once she is home?
Note: *Refer to Chapter 7 8 for the actual techniques of assessment mentioned in this table.
1. What information should the nurse include in the discharge teaching plan for Tiona’s mother?
NCLEX-RN® Review
FIGURE 32–2 ■ Feedback mechanism in hormonal stimulation of the gonads during puberty.
The anterior pituitary gland is considered to be the “master gland” of the body. The major function of the anterior pituitary gland is the production and release of thyroid-stimulating hormone (TSH), adrenocorticotropic hormone (ACTH), luteinizing hormone (LH), follicle-stimulating hormone (FSH), growth hormone (GH), and
1. The nurse is caring for a female child who is recovering from a motor vehicle accident. The child’s parents ask if it is okay to bring the child’s siblings to visit. What is the most appropriate response by the nurse?
1. “No, it would not be good for your child to see her siblings as it may make her worse.”
3. Which behavior by a child’s parents is the best indicator that they understand how to administer medication to the child at home following surgery?
1. The parents sign the written discharge instruction verifying understanding of the instructions.
As the child’s condition weakens, the family again needs additional support. They experience grieving, each person in their own way. They have lived with chronic sorrow and now need to prepare for the child’s death. The child is usually old enough to recognize the deteriorating condition. See Chapter 18 8 for further discussion of bereavement and end-of-life care
2. “No, it would be very upsetting for your child’s siblings to see her this way.”
Tables of Diagnostic Procedures and Laboratory Tests pertinent to the specific systems assist you in clinical when you need the information.
Inborn errors of metabolism (inherited biochemical abnormalities of the urea cycle and amino acid and organic acid metabolism) often have a significant impact on the endocrine system’s ability to support growth and development. Some chromosomal abnormalities also result in disturbances in growth and sexual development. These disorders are discussed on page 1141
TABLE 32–3 Diagnostic Procedures and Laboratory Tests for the Endocrine System*
3. “Yes, it is okay to bring your child’s siblings to see her as long as you bring someone to watch them.”
2. The parents give the medication to the child using the appropriate technique in the nurse’s presence.
DIAGNOSTIC PROCEDURES LABORATORY TESTS
4. “Yes, it is okay to bring your child’s siblings for a visit as long as we educate them on what to expect when they visit.
ACTH stimulation test
2. How can the nurse best limit the amount of separation anxiety that the hospitalized toddler will experience?
3. The parents state they understand how to administer the medication and deny questions.
Fasting plasma glucose
4. The parents state they can give the medication to the child using appropriate technique.
Adrenal (ACTH) suppression test
Bone age
1. Reduce the amount of time spent with the child when the parents are not present.
Computed tomography (CT)
2. Discourage the amount of time the parents hold their child while hospitalized.
Hemoglobin A1c
Hormone levels
4. The nurse is caring for a 5-year-old male child who will be having a tonsillectomy performed. What teaching method is most appropriate for this child prior to the surgical procedure?
1. Provide the child’s mother with brochure about the procedure.
Insulin-like growth factor (IGF-1) and Insulin-like growth factor-binding protein
Evaluation
3. Encourage the parents to leave the child’s room when care is being provided.
DISORDERS OF PITUITARY FUNCTION
Expected outcomes of nursing care for the child with muscular dystrophy include maintenance of optimal mobility and development, positive self-image for the affected child, and positive management of the emotional challe nges by all family memb ers.
Fluid deprivation test
Karyotype
4. Encourage parental involvement in the child’s care and suggest rooming in if possible.
The pituitary gland consists of two lobes, an anterior lobe and a posterior lobe. The functions of the posterior pituitary gland include regulation of fluid balance through release of antidiuretic hormone (ADH), which is stored in the hypothalamus; and production of oxytocin, which is also stored in the hypothalamus.
Refe rences
Bind ler, R. C., Ball J. W., Lade wig, P. W., & London M. L. (2011). Clinical skills manual for maternal & child nursing care (3rd ed p. 110). Upp er Saddle
River, NJ: Pe arson.
Complementar y Therapy Muscular Dystrophy
Brain Injury Association of America. (2011). A guide to selecting and monitoring brain injury rehabilitation services Retrieved from http://www.biausa.org/Default aspx?SiteSearchID 1192&ID /search-results.htm
Chahal, N., Manlhiot, C., Colapinto, K., Alphen, J. V., McCrindle, B. W & Rush, J. (2009). Association between parental anxiety and compliance with preoperative requirements for pediatric outpatient surgery. Journal of Pediatric Health Care, 25(6), 372–377.
Many families who have a child with muscular dystrophy use different types of complementar y care. The nurse always assesses for such approaches, provides information as needed by the family, makes recommendations for complementary therapies that may be helpful, and cautions against those that could be harmful due to interactions with medications or other problems. Common complementar y care used in muscular dystrophy includes dietar y enhancement. This enhancement includes vitamins A, C, E, D, and B-complex; minerals such as calcium, magnesium, zinc, and selenium; probiotic supplement; omega-3 fatty acids; herbal remedies such as green and rhodiola rosea teas; muscular and immunologic enzymes such as coenzyme Q10, N-acetyl cysteine, acetyl-L-carnitine, creatine, and L-theanine; melatonin to promote sleep; and massage to assist with reduction of muscle spasms (University of Mar yland Medical Center, 2011).
2. Sit with the child while he watches a video about the procedure.
3 IGFBP-3
3. Use dolls to teach the child about the procedure.
Magnetic resonance imaging (MRI)
See Appendix I 8 8 for answers.
Thyroid radioactive iodine uptake (RAIU) scan
Newborn metabolic screening
4. Allow the child to talk to other children who have had the procedure.
Provocative growth hormone testing
Thyroid antibodies
Note: *See Appendixes D and E 8 for information about these diagnostic procedures and for expected laboratory tests values.
Crenshaw J. T., & Winslow, E. H. (2008). Preoperative fasting and medication instruction: Are we improving? AORN Journal, 88(6), 963–976.
Disch, J Dreher M., Davidson, P Sinioris, M., & Wainio, J. A. (2011). The role of the chief nurse officer in ensuring patient safety and quality. Journal of Nursing Administration, 41(4), 179–185.
Fisher M. J & Broome, M. E. (2011). Parent-provider communication during hospitalization. Journal of Pediatric Nursing, 26(1), 58–69.
Forsner, M., Jansson, L., & Söderberg, A. (2009). Afraid of medical care: School-aged children’s narratives about medical fear Journal of Pediatric Nursing, 24(6), 519–528. Frisch, A. M., Johnson, A., Timmons, S., & Weatherford, C. (2010). Nurse practitioner role in preparing families for pediatric outpatient surgery. Pediatric Nursing, 36(1), 41–47.
Drahota, A., & Malcarne, V. L. (2008). Concepts of illness in children: A comparison between children with and without intellectual disability Intellectual and Developmental Disabilities, 46(1), 44–53. Emergency Nurses Association. (2009). Emergency nursing resource: Family presence during invasive procedures and resuscitation in the emergency department Retrieved from http://www.ena.org/IENR/ENR/Documents/ FamilyPresenceENR.pdf
Complementary Therapy boxes present approaches other than traditional medical prescriptions that may be used by children and families to maintain health or treat diseases. These boxes discuss research when it is present to support or refute the efficacy of these modalities. At other times, they alert you about information to gather from the family and to consider when planning care.
are in similar over time or if body prophysician, nurse channel to anin the 25th percentile performed clues to nudietary insuggest specific
a description of activities in the last day. Then start with the most recent event and move backwards, integrating food intake into the daily schedule. For example, you might begin by saying, “You mentioned you got up early to come to the clinic today. What did Sam eat at home before you left? Did he have a snack as you traveled here or
■ Promotes a healthy school environment by ensuring immunization compliance, monitoring playground equipment safety, promoting infection control, and implementing programs for bullying and violence prevention
■ Educates students about healthy lifestyles, good nutrition, exercise, oral health, smoking cessation, sexually transmitted infections, and pregnancy prevention
■ Manages students with chronic conditions, administers medications, and participates in the development of individualized health plans (IHPs) and individualized education plans (IEPs) for those with disabilities
Developing Cultural Competence Growth Grids
■ Refers students’ families to healthcare providers and insurance programs and connects students with needed services (e.g., for substance abuse treatment, behavioral and mental health, and reproductive health)
■ Serves as a leader in the preparation of policies for school-wide emergencies, school health programs, mental health intervention, and student and faculty health emergencies
The growth grids now in use were standardized using a cross section of the U.S. population and are generally reflective of most children. However, children from some other countries or cultures may fall outside these curves. For example, new immigrants or adoptees may be in lower percentiles, and catch up over several months or years. Children of immigrants from developing countries tend to be larger than their parents. Even when small, children should follow normal growth patterns. For example, a child may remain at the 10th or 25th percentile for height, but continue to slowly grow and not fall to a lower percentile.
■ Identifies and reports clusters of symptoms that may indicate an epidemic
Source: Data from American Academy of Pediatrics Council on School Health. (2008). Role of the school nurse in providing school health services. Pediatrics, 121(5), 1052–1056; Robert Wood Johnson Foundation. (2010). Unlocking the potential of school nursing: Keeping children healthy, in school, and ready to learn. Retrieved from http://www.rwjf.org/files/research/cnf14.pdf
Developing Cultural Competence boxes challenge you to explore differences among racial, ethnic, and social groups, and to plan nursing care that addresses the issues of health disparity.
date grades for screening and selected children who must be screened for conditions such as visual or hearing problems, and scoliosis screening in public schools. B, The school nurse treats this child with a nebulizer to determine if the asthma episode can be controlled before calling the parent to come and pick up the child and seek care from the primary care provider. The parent should be informed of nebulizer treatment provided in case the child’s asthma episode continues and additional treatment is needed.
Legal and Ethical Considerations Child Nutrition Reauthorization Act
The Child Nutrition Reauthorization Act of 2010, titled the Healthy, Hunger-Free Kids Act of 2010, continues the federal school meal programs (breakfast, lunch, after-school snack, and summer food service) for low-income children and increases access to nutritional foods. The program also has goals for nutrition education and physical activity in an effort to address childhood obesity. School nurses may work with food service personnel in the nutrition programs for healthy eating and in creating a nutrition education program for students (Sherry, 2008). See Chapter 19 8 8
Legal and Ethical Considerations boxes identify laws and ethical issues pertinent to pediatric nursing topics.
Medications Used to Treat boxes list the actions, indications, and important nursing implications for medications.
778 Unit VI | Chapter 25 | Alterations in Respiratory Function
Medications Used to Treat Asthma
QUICK-RELIEF MEDICATION ACTION/INDICATION
Short-Acting Beta2-Agonists (SABA)
Albuterol
Levalbuterol
Pirbuterol:
Metered dose inhaler (MDI) or nebulizer
Corticosteroids
Methylprednisolone
Prednisone
Prednisolone: Oral
Anticholinergic
Ipratropium: Metered dose inhaler (MDI) or nebulizer
Relaxes smooth muscle in airway leading to rapid bronchodilation (within 5–10 minutes) and mucus clearing
Drug of choice for acute therapy and for prevention of exercise-induced bronchospasm
NURSING MANAGEMENT
■ Use this rescue medication before inhaled steroid, wait 1–2 minutes between puffs, wait 15 minutes to give inhaled steroid. Child should hold breath 10 seconds after inspiring. Then rinse mouth and avoid swallowing medication. Use a spacer
■ Differences in potency exist, but all products are comparable on a per puff basis.
■ Some dose-related side effects include tachycardia, nervousness, nausea and vomiting, and headaches.
■ Regular use more than 2 days a week for symptom control indicates a loss of control and need for additional therapy
Diminishes airway inflammation, secretions, and obstruction, enhances bronchodilating effect of beta2-agonists
Used for acute asthma episodes that are not completely responsive to beta2-agonists; helps reduce rate of hospitalization
Inhibits bronchoconstriction and decreases mucus production with an onset of action in 30–90 minutes
DAILY CONTROL MEDICATIONS ACTION/INDICATION
Long-Acting Beta2-Agonists (LABA)
Salmeterol
Formoterol:
Dry powder inhaler (DPI)
Inhaled Corticosteroids (ICS)
Beclomethasone
Evidence-Based Practice boxes further enhance the approach to research. We describe a particular nursing problem and investigate the evidence from several studies that explore solutions to the problem. We emphasize nursing research, provide an interpretation explaining the implications of the studies, and then invite you to apply critical thinking skills to further identify nursing care approaches.
Budesonide
Flunisolide
Fluticasone
Mometasone
Triamcinolone:
Metered dose inhaler (MDI) or nebulizer
Methylxanthines
Theophylline: Oral
Mast-Cell Inhibitors
Cromolyn sodium Nedocromil:
Metered dose inhaler (MDI) or nebulizer
Relaxes smooth muscles in airway, used for nocturnal symptoms and prevention of exercise-induced bronchospasm.
These medications should not be used as single therapy for asthma in children, but prescribed in combination with corticosteroids (U.S. Food and Drug Administration, 2010).
■ Short-term therapy should continue until child achieves 80% peak expiratory flow rate personal best or symptoms resolve.
■ Give with food to reduce gastric irritation.
■ Give oral dose in early morning to mimic normal peak corticosteroid blood level.
■ Assess for potential adverse effects of long-term therapy: decreased growth, unstable blood sugar, and immunosuppression.
■ Do not use for primary emergency treatment because of delayed onset.
■ Rinse mouth afterward to get rid of bitter taste.
■ Side effects include increased wheezing, cough, nervousness, dry mouth, tachycardia, dizziness, headache, and palpitations.
■ Prevent medication contact with eyes.
NURSING MANAGEMENT
■ Do not use for acute asthma episode.
■ Take pre-exercise dose 30–60 minutes before activity Do not use additional dose before exercise if already using twice-daily doses which should be 12 hours apart.
■ Caution against overdosage as side effects such as tachycardia, tremor, irritability, and insomnia will last 8–12 hours.
Practice Care Coordination for Children with Special Healthcare Needs
Anti-inflammatory, controls seasonal, allergic, and exercise-induced asthma
Effectively reduces mucosal edema in airways
■ Report failure to respond to usual dose as this may indicate a need for stepped-up therapy
■ Administer with spacer or holding chamber
PROBLEM Children with special healthcare needs require assistance from a variety of programs and services to maximize their potential. Fragmentation of care may result in the child’s needs being unmet.
EVIDENCE
■ Separate parts and clean inhaler daily
■ Rinse mouth and gargle following treatment to remove drug from oropharynx to reduce chance of cough, thrush, and dysphonia.
coordination by nurses as an integral aspect of each visit decreased the number of visits to the primary care provider and to the emergency department Antonelli, Stille, & Antonelli, 2008).
A longitudinal study compared the use of pediatric practice-based
■ Monitor growth; however recommended doses do not have long-term or irreversible effects on vertical growth (Fong & Levin, 2007).
Relaxes muscle bundles that constrict airways; dilates airway; provides continuous airway relaxation; sustained release for prevention of nocturnal symptoms
Data were analyzed from the 2005–2006 National Survey of Children with Special Healthcare Needs to determine the association between receiving adequate care coordination, family–provider relations, and outcomes in the child and family Data indicated that 68.2% of the families reported receiving some type of assistance with care coordination. Of these, 59.2% indicated they received adequate help, and 40.8% indicated the assistance was inadequate. Adequate care coordination was associated with family-centered care, satisfaction with care received, and a partnership with healthcare professionals. Families who reported receiving adequate care coordination were less likely to have problems with specialty referrals, family financial burden, and reduction in work hours. These families also had less out-of-pocket expenses, fewer visits to the emergency department per month, and fewer missed days of school for the CSHCN than families who reported receiving inadequate assistance with care coordination Turchi, Berhane, Bethell, et al., 2009).
■ Prevent eye exposure through proper MDI, nebulizer, or DPI administration.
■ Monitor for headache, gastrointestinal upset, dizziness, and infection.
■ Use exactly as prescribed.
■ Tablet should not be crushed or chewed.
■ Use for long-term control. Works best when a therapeutic serum level (10–20 mcg/L) is maintained; give same time each day
■ Requires serum level monitoring and dose adjustment.
■ Limit caffeine intake.
Anti-inflammatory, inhibits early and late phase asthma response to allergens and exercise-induced bronchospasm; may be used for unavoidable allergen exposure.
A descriptive study of six pediatric primary care practices was conducted to evaluate the effectiveness of a care coordination measurement tool. Other purposes of the study were to describe care coordination activities that occurred in a pediatric primary care setting, to assess the relationship of care coordination activities in this setting to outcomes related to the use of resources, and to measure personnel costs related to care coordination activities. The study found that care coordination activities were used by patients at all levels of acuity, including children and youth with special healthcare needs; the care coordination tool was used effectively in the pediatric primary care setting; care coordination provided by nurses instead of physicians in this setting decreased costs; and care
May be used as a substitute for inhaled corticoste-
■ Side effects include tachycardia, dysrhythmias, restlessness, tremors, seizures, insomnia, hypotension, severe headaches, vomiting, and diarrhea.
■ Do not use at time of symptom development or acute exacerbation.
■ The patient must use up to 4 times a day to be effective.
■ Therapeutic response is seen in 2 weeks; maximum benefit may not be seen for 4–6 weeks.
for hospitalfor hospito answer
emotional risk for follow fibrosis or lessness. hospital admisvironment, responses, anticipated s care. Give ncerns. Refer to t is needed
■ General pediatric unit
■ Short-stay unit, outpatient unit, or ambulatory surgical unit
■ Emergenc y department
■ Neonatal intensive care unit (NICU) or pediatric intensive care unit (PICU)
A randomized controlled trial measured how monitoring and discussing healthrelated quality of life (HRQoL) improved psychosocial well-being in adolescents with type 1 diabetes. Ninety-one adolescents between the ages of 13 and 17 with type 1 diabetes participated in the study and were randomly assigned to the HRQoL intervention group or the control group. During a 12-month period, all participants had 3 scheduled visits for routine diabetes care at 3-month intervals. The intervention group completed the Pediatric Quality of Life Inventory on a computer at each visit prior to being seen by the healthcare provider. The results were discussed with the adolescent during the visit. Over the 12-month period, mean scores for psychosocial health, behavior, mental health, and family activities improved in the intervention group except for those adolescents with the highest hemoglobin A1c values. Adolescents in the intervention group demonstrated higher self-esteem at follow-up visits and were more satisfied with care than those in the control group (de Wit, Delemarre-van de Waal, Bokma, et al., 2008).
Baccalaureate Essential II Basic Organizational and Systems Leadership for Quality Care and Patient Safety
A cross-sectional design was utilized to determine the impact of family support and environment on quality of life, adherence to treatment, and metabolic control in 157 adolescents ages 10 to 18 with type 1 diabetes. Four instruments were used in the study: a self-report questionnaire on adherence, Diabetes Family Behavior Scale, Family Environment Scale, and Diabetes Quality of Life. Results of the study indicated that increased family support predicted a better quality of life in both males and females, and higher family conflict predicted a lower quality of life. Increased family support also predicted an increase in adherence in females. Additionally, the study found that the longer the teen had been diagnosed with diabetes, the less likely he or she was to be adherent to a management plan and to have good metabolic control. Results
Quality improvement and safety is a priority for healthcare organizations. Nurses at the bedside have a major influence on the quality of care provided and the safety of the patient; however, it is the responsibility of the organization’s leadership to provide the staffing and resources so that safe and quality care can be provided (Disch, Dreher, Davidson, et al., 2011). Healthcare providers must advocate for best practices that focus on risks unique to children. Children in the healthcare setting are at risk for harm related to misidentification, adverse effects from high-alert medications, and healthcare-acquired or associated infection (Steering Committee on Quality Improvement and Management & Committee on Hospital Care, 2011). Young children are especially vulnerable to injur y because of their developmental immaturity, including the inability to recognize safety risks. It is essential that the hospital environment be free of hazards that pose risks for children.
RESEARCH boxes focus on relevant research studies to give students additional information and background information.
Partnering with Families boxes help you to apply the concepts of family-centered nursing care by providing approaches and teaching in a format directly applicable when you work with families.
necessary for home management, including insulin administration, blood glucose testing, meal planning, and the recognition and treatment of both hypoglycemia and hyperglycemia. Partner with the child and family to identify barriers to management.
Explain the goals of insulin therapy. Teach the parents and child (if age appropriate) how to draw up and administer insulin or how to use an insulin pen. Insulin pens might be accepted more readily than the traditional syringe and vial method; they are easier to transport, they provide more accurate dosing, and they decrease
BOX 32–6
can Americans scored significantly higher than Caucasians on both measures. Participants who lived in single-parent homes had poorer diabetic control, as indicated by a higher hemoglobin A1c, but had higher scores in resilience (Winsett, Stender, Gower, et al., 2010).
IMPLICATIONS
Developmental tasks of adolescents focus on development of self-concept and self-esteem. Adolescents with type 1 diabetes must also cope with the increasing responsibility for complex self-management, including insulin administration, blood glucose testing, exercise, and nutrition. Self-esteem and self-concept often become linked with the disease as peers react to the differences noted. Life satisfaction, perceived control, and worries associated with having diabetes are important considerations when counseling the teenager and family about the management of diabetes. Additionally, it is important to know that adolescents value parental involvement and care rather than perceiving it as a reason for conflict. Parental involvement and supervision is important in helping adolescents transition successfully to self-management of their disease. Peers are also very important to adolescents with diabetes. Continued involvement in school activities and summer camps provide excellent avenues for friendship and promote a positive quality of life.
NEW! Baccalaureate Essentials boxes focus on the nine essentials of nursing education identified by the American Association of Colleges of Nursing.
CRITICAL THINKING APPLICATION
What questions can be used to explore an adolescent’s perceptions of family involvement, care, and control? How can you address quality of life issues in adolescents with diabetes? What questions can be asked to determine the adolescent’s self-efficacy and resilience?
anxiety associated with needles and insulin administration in public (Hanas, de Beaufort, Hoey, et al., 2011). Rotating the injection sites is important to decrease the chances of lipoatrophy, loss of subcutaneous tissue, or hypertrophy, in which collagen is replaced by fat cells (Figure 32–10 ■). The absorption rate of insulin varies by the site used. Insulin is usually absorbed most rapidly from the abdomen; however, insulin absorption is increased in the extremities with exercise. An understanding of the different types of insulin and their actions is essential.
Research: Communication Between Adolescents with Type 1 Diabetes and Their Parents
Transcripts of interactions between adolescents ages 11 to 15 years with type 1 diabetes and their parents were analyzed. Participation in the study required that the adolescent had been diagnosed with type 1 diabetes for at least a year and have no other chronic illness, psychologic problems, or learning disability Transcripts were based on a 10-minute interaction between the adolescent and his or her parents in which a diabetes management task, identified by the teen as a source of disagreement, was discussed.
Five themes were identified from the transcripts: fear, frustration, discounting, normalizing, and trusting. Parents demonstrated frustration, fear and difficulty in trusting the child with the daily management of diabetes. Parents were also fearful of long-term complications. Adolescents demonstrated frustration because they did
not feel their parents recognized their successes in their diabetes management. Discounting was noted in statements by parents that showed a lack of respect for the adolescents’ opinions and failure to include the adolescents in decisions related to their care. These statements further added to the child’s frustration. The theme of normalizing was noted in only a few families and included statements indicating that the family was attempting to view diabetes as a normal aspect of the adolescent’s life. The other themes of fear, frustration, trust, and discounting were cited as barriers to achieving the goal of normalcy
The study concluded that effective communication between parents and adolescents with type 1 diabetes is essential and that nurses should work with families to facilitate communication related to diabetes management (Ivey, Wright, & Dashiff, 2009). EVIDENCE
Partnering with Families
Helping the Infant Sleep
Video
Helping the Infant Sleep
Helping an infant to self-regulate and be able to sleep for longer periods is often a stressful challenge for families. Parents need to have substantial sleep periods themselves to be refreshed and able to deal with daily life. When up several times during the night with a baby, parents may become irritable and fatigued. Question the family about the baby’s sleep routine. The infant passes into light sleep several times at night and may awaken; self-regulation will assist in helping the infant get back to sleep. Suggestions helpful for the family are as follows:
■ Place the baby to sleep in a quiet and darkened room, a “sleep friendly” environment.
■ Establish a consistent sleep routine and time; the routine may involve some cuddling and rocking time but should not be vigorous, stimulating play
and psychologic health are closely related to these factors. For many parents, membership in a faith-based congregation provides spiritual sustenance and an important sense of belonging. This group may also provide food, clothing, and care for the new infant. Sometimes parents who have not attended institutionalized services will choose to do so to offer a significan t spiritual home for their new child. Services such as christening and blessing an infant welcome the child formally into the family and provide meaning to parents and extended family members. Having a baby often helps parents to feel that they have an important meaning and purpose in life, regardless of a faith-based membership An atmosphere where the infant is valued and offers
■ Provide a consistent transitional object, such as a favorite blanket each night.
■ Put the baby to bed while still awake but drowsy rather than after falling asleep, so the infant learns self-soothing skills.
■ Do not tr y to awaken the baby in non-rapid eye movement (NREM or quiet) sleep.
■ For the baby who has trouble going to sleep, remain in the room for a few minutes but do not establish eye contact; place a hand on the abdomen or chest or gently hold flailing arms and legs.
Source: Data from National Sleep Foundation. (2011). Sleep, infants, and parents. Retrieved from http://www.sleepfoundation.org/articles/ask-the-expert/sleep-infants-and-parents
cues related to hunger or discomfort, the nurse plans interventions to help prevent further problems. Teaching, demonstrations, and acknowledging parent success are all health maintenance actions. An expected outcome for these activities is the reestablishment of expected growth and development, and age-appropriate interactions of the infant with others.
The infant’s social interactions, both within and outside the family,
284 Unit III | Chapter 10 | Health Promotion and Maintenance of the Infant
of otitis media. The major risk factor for frequent otitis media is low socioeconomic status, regardless of ethnicity ( Smith & Boss, 2010). Be alert for risk factors, plan prevention programs, and ensure prompt care and teaching about treatments for families of children affected. What prevention measures would you emphasize for families? See the nursing management section on otitis media for suggestions of preventive approaches.
of ear pain (F
24–9 ■ ). Diarrhe a, vomiting, and fever are typical of otitis media. Irritability and “acting out” may be signs of a related hearing impairment. The child with otitis media often has night awakenings with cr ying due to increased pressure when prone or supine. See the Clinical Manifestations table for further detail.
Clinical Manifestations Acute Otitis Media and Otitis Media with Effusion
ETIOLOGY
Acute otitis media—bacterial infection in the middle ear from pathogens transferred from the nasophar ynx; most common infectious agents are S. pneumoniae, H. influenzae, M. catarrhalis
Otitis media with effusion collection of fluid in the middle ear behind the tympanic membrane which is not infected with bacteria.
Examination—bulging tympanic membrane, air or fluid bubbles present behind tympanic membrane; immobile or poorly mobile tympanic membrane, red (or other color change such as white, gray, or yellow as long as bulging is present) tympanic membrane, reduced visibility of tympanic membrane landmarks with displaced light reflex.
Behavioral—difficulty hearing or responding as expected to sounds.
Examination—signs of acute inflammation are NOT present; tympanic membrane is retracted or neutral; immobile or partly mobile tympanic membrane; yellow or gray tympanic membrane; opaque or thickened tympanic membrane with visibility of landmarks reduced.
Nursing Care Plans are present in every chapter dealing with health conditions. They illustrate the conceptual approach that nurses need in caring for children, including assessment, NANDA nursing diagnoses, goals, plans, interventions (with NIC), and evaluation (with NOC).
CLINICAL THERAPY
Treat ear pain with anesthetic eardrops, herbal pain products instilled into the auditor y canal, or systemic acetaminophen or ibuprofen.
Verify that the tympanic membrane is intact before inserting eardrops. Obser ve the child’s condition for 48–72 hours and if not improved, treat with course of antibiotics.
Provide symptomatic treatment of pain. Carefully assess hearing acuity over several months. Assess speech if loss of hearing acuity occurs. Assess development.
Clinical Manifestations boxes link etiology, clinical manifestations, and clinical therapy for specific conditions.
about age-appropriate foods. Since appetite may be impaired during periods of treatment, the child may be lacking fruits, vegetables, or other foods, as well as the nutrients they include. Encourage parents to be sure the child has a well-balanced diet during periods of remission.
■ Perform developmental screening of young children. Provide suggestions for parents about the stimulation that is appropriate for the child’s age. Include quiet activities that can be used when the child is fatigued or receiving therapy These might include reading books, listening to music, and working on a computer Have the parent plan for these activities on days that the child goes for chemotherapy or other treatment.
■ Ask about the school-age child’s progress in school. Performance may be altered due to neurologic effects of treatment as well as missing school. Plan for the family to partner with the school personnel for provision of tutors, computer programs, or other needed assistance.
■ Encourage continued social contact with peers when blood counts are adequate to prevent infection.
PHYSICAL ASSESSMENT AND SCREENING
■ Careful physical assessments are performed to identify any abnormalities that may result from cancer or its treatment. Be alert for signs of anemia, neutropenia, and thrombocytopenia; refer for treatment and suggest preventive measures such as infection control for neutropenia.
Cardiopulmonary and neuromuscular assessments are particularly important. Vision and hearing should be assessed prior to treatment and periodically throughout. Include measurements of fine and gross motor activity
ELIMINATION
■ Toddlers may have an interruption in toilet training during periods when they do not feel well. Help parents to understand this regression, and encourage them to start again when the child is feeling better
■ Some medications cause diarrhea or constipation, so evaluate bowel patterns and provide guidance as needed. Skin care instruction may be needed if the child has diarrhea and is relatively immobile. Increasing fluids and fiber foods may be needed for constipation.
■ Evaluate urinary output since many medications have effects on kidney function. Encourage adequate fluids
Health Promotion & Maintenance Overviews summarize the needs of children with specific chronic conditions, such as asthma or diabetes. These overviews teach you to look at the child who has a chronic illness like any other child, with health maintenance needs for prevention, education, and basic care.
End-of-Chapter Review
Chapter Highlights summarize key points of the chapter.
Clinical Reasoning in Action refers back to the chapter-opening scenario and asks critical thinking questions to help students apply knowledge to real patient care.
NCLEX-RN® Review prepares students for course exams on chapter content and gives exposure to all formats of NCLEX®-style questions.
Detailed References provide the basis for evidence-based nursing care and support the currency and accuracy of the textbook.
saline. Contemporary Pediatrics, 28(2), 30–38. American Academy of Allergy Asthma, and Immunology (AAAAI). (2013). What is a peak flow meter? Retrieved from http://www.aaaai.org/ American Academy of Pediatrics (AAP). (2012). Red book: 2012 Report of the Committee on Infectious Diseases (29th ed.). Elk Grove Village, IL: Author American Academy of Pediatrics (AAP) Committee on Infectious Disease. (2009). Policy statement—Modified recommendations for use of palivizumab for prevention of respiratory syncytial virus infections. Amirav I. (2010). To inhale or not to inhale: Is that the question? A simple method of DPI instruction. Journal of Pediatrics, 156(2), 339–339e1. Antoon, A. Y & Donovan, M. K. (2007). Burn in uries. In R. M. Kliegman, R. E. Behrman, H. B. Jenson, & B. F. Stanton, Nelson textbook of pediatrics (18th ed pp. 450–458). Philadelphia, PA: Elsevier Saunders. Askin, D. F & Diehl-Jones, W. (2009). Pathogenesis and prevention of chronic lung disease in the neonate. Critical Care Nursing Clinics of North America, 21 11–25. Asthma Initiative of Michigan for Healthy Lungs. (2011).
Emergency Medical Clinics of North America, 26 953–959. Baker, L. K., & Denyes, M. J. (2008). Predictors of self-care in adolescents with cystic fibrosis: A test of Orem’s theories
Bonkowsky, J. L., & Tieder J. S. (2009). A pragmatic approach to ALTEs. Contemporary Pediatrics, 26(11), 54–63. Brashers, V. L. (2010a). Alterations in pulmonary function. In K. L. McCance, S. E. Huether, V. L. Brashers, & N. S. Rote, Pathophysiology: The biologic basis for disease in adults and children (6th ed pp 1266–1309). St. Louis, MO: Mosby Elsevier Brashers, V. L. (2010b). Structure and function of the pulmonary system. In K. L. McCance, S. E. Huether, V. L. Brashers, & N. R. Rote, Pathophysiology: The biologic basis for disease in adults and children (6th ed pp 1242–1265). St. Louis, MO: Mosby Elsevier Busse, W. W Morgan, W. J Gergen, P. Mitchell, H. E., Gern, J. E., Liu, A. H., Sorkness, C. A. (2011). Randomized trial of omalizumab (Anti-IgE) for asthma in inner-city children. New England Journal of Medicine, 364(11), 1005–1015. Callahan, K. A., Panter T. M., Hall T. M., & Slemmons, M. (2010). Peak flow monitoring in pediatric asthma management: A clinical practice column submission. Journal of Pediatric Nursing 25 12–17. Camargo, C. A., Rachelefsky, G., & Schatz, M. (2009). Managing asthma exacerbations in the emergency department: Summary of the National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the management of asthma exacerbations. Journal of Allergy and Clinical Immunology 124 S5–S14. Carbajal R Biran, V Lenclen, R Epaud, R Cimerman, P Thibau t, P Fauroux, B. (2008). EMLA cream and nitrous oxide to alleviate pain induced by palivizumab (Synagis) intramuscular injections in infants and young children. Pediatrics, 121(6), e1591–e1598. Carrier C. T. (2009). Back to sleep: A culture change to improve practice Newborn & Infant Nursing Reviews, 9(3), 163–168.
Centers for Disease Contro and Prevention (CDC). (2008). Initiating change: Creating an asthmafriendly school Retrieved from http://www.cdc.gov/ HealthyYouth/asthma/creatingafs/index.htm
Centers for Disease Contro and Prevention (CDC). (2011a). Trends in tuberculosis—United States, 2010. Morbidity and Mortality Weekly Report 60(11), 333–337. Centers for Disease Contro and Prevention (CDC). (2011b). Vital signs: Asthma prevalence disease characeristics, and self-managemen education—United States, 2001–2009. Morbidity and Mortality Weekly Report 60(17), 547–552. Chipps, B Zeiger R. S., Murphy K., Mellon, M., Schatz, M., Kosinski M., Ramachandran, S. (2011). Longitudinal validation of the Test for Respiratory Asthma Contro in Kids in pediatric practices. Pediatrics, 127(3), e737–e747.
Clark, A. P., Giuliano K., & Chen, H. (2006). Pulse oximetry revisited: “But his O2 was normal!” Clinical Nurse Specialist, 20(6), 268–272. Coffman, S. (2009). Late preterm infants and risk for RSV Maternal and Child Nursing, 34(6), 378–384.
bandage is prepared. This action prevents more air from entering the chest. For a closed pneumothorax, a needle or tube thoracostomy is performed rapidly to relieve the pressure in the chest. This is usually performed before a chest radiograph that often reveals air in the chest. A chest tube is inserted and a closed drain-
Chapter Highlights
■ Respiratory conditions are the most common cause of hospitalization in children between 1 and 9 years of age and a leading cause in children between 10 and 19 years of age.
■ The child’s airway is shorter and narrower than an adult’s. These differences create a greater potential for obstruction. The lungs have no muscles of their own, so respiration is powered by the diaphragm and intercostal muscles.
■ Children under 2 years have an increased risk of developing tuberculosis, and if untreated have a greater chance of progressing to active TB and spreading beyond the lungs (e.g., meningitis and disseminated TB).
■ Foreign body aspiration is most often caused by small objects that make their way into the child’s mouth, such as foods, small toy parts, or household objects like beads, safety pins, coins, or buttons. The increasing mobility and tendency to put small objects in the mouth makes this a major health problem for infants and toddlers.
■ Asthma is one of the most common chronic respiratory disorders in childhood. The respiratory difficulties of an acute asthma episode result from inflammation that causes the normal protective mechanisms of the lungs (mucous formation, mucosal swelling, and airway muscle contraction) to overreact in response to a stimulus and cause airway obstruction.
■ Signs of impending respiratory failure in infants and children include worsening respiratory distress, irritability lethargy mottled color or cyanosis, diaphoresis, and increased respiratory effort such as dyspnea (difficulty breathing), tachypnea (increased respiratory rate), nasal flaring, grunting, and retractions.
■ Bronchopulmonary dysplasia (BPD) usually develops in neonates with a birth weight of 1000 g or less and a gestational age at birth of less than 28 weeks who are treated with oxygen and positive-pressure ventilation for respiratory failure or respiratory distress syndrome. Treatment leads to inflammation and damage to the bronchioles, resulting in fibrosis, edema of the bronchioles, and smooth muscle hypertrophy
■ Sudden infant death syndrome (SIDS) is a leading cause of death in infants. Onset of the fatal episode occurs during sleep and remains unexplained after a thorough investigation, including an autopsy, a review of the circumstances of death, and the clinical history.
Signs of smoke inhalation injury in children include burns of the face and neck, singed nasal hairs, soot around the mouth or nose, and hoarseness with stridor or voice change.
■ Apnea is cessation of respiration lasting longer than 20 seconds, or any pause in respiration associated with cyanosis, marked pallor, hypotonia, or bradycardia.
■ Pulmonary contusion occurs in association with blunt chest trauma. The energy from the injury often bruises the lung tissue in the absence of rib fractures. Although the child may appear initially asymptomatic, respiratory distress often develops within a few hours.
■ Three types of apnea are noted in neonates: central apnea, in which there is complete cessation of breathing; obstructive apnea, in which there is an absence of nasal airflow when respiratory efforts are present; and mixed apnea, in which a central respiratory pause either precedes or follows airway obstruction.
■ A pneumothorax may become life threatening if internal pressure from a closed pneumothorax is not vented. Air leaking into the chest cavity during inspiration cannot escape during expiration, increasing compression. Venous blood return to the heart is impaired as the mediastinum shifts toward the unaffected lung.
Clinical Re asoning in Action
■ Obstructive sleep apnea syndrome is a disorder of breathing during sleep that in children is commonly caused by enlarged tonsils and adenoids. Children have symptoms of sleep deprivation such as daytime sleepiness, poor attention, increased activity aggression or acting-out behavior and poor school performance.
DISCUSSION
INTRODUCTION
Return to the scenario at the beginning of the chapter Hannah and her mother are learning more about asthma management during a health center visit with the nurse practitioner She has no asthma symptoms during today’s visit, and has taken all medications prescribed since her recent hospitalization.
DESCRIPTION Prior to the acute asthma episode that occurred at school, Hannah had used only short-acting beta2-agonists for symptoms, about once a week. During her hospitalization she needed systemic corticosteroids and was sent home with oral corticosteroids that were tapered and discontinued 3 days ago. Because of the severity of her asthma episode, Hannah’s daily treatment will be changed from step 1 for intermittent asthma to step 2 for mild persistent asthma.
Coleman-Phox, K., Odouli R., & De-Jun, L. (2008). Use of a fan during sleep and risk of sudden infant death syndrome. Archives of Pediatrics and Adolescent Medicine, 162(10), 963–968. Cruz, A. T & Starke, J. R. (2010). Pediatric tuberculosis. Pediatrics in Review 31(1), 13–25. Cuff S., & Loud, K. (2008). Exercise-induced bronchospasm. Contemporary Pediatrics, 25(9), 88–95. Cystic Fibrosis Foundation. (2011a). About cystic fibrosis: What you need to know Retrieved from http://www.cff.org/AboutCF/ Cystic Fibrosis Foundation. (2011b). About cystic fibrosis: Frequently asked questions Retrieved from http:// www.cff. org/AboutCF/Faqs/ Cystic Fibrosis Foundation. (2011c). Screening for cystic fibrosis Retrieved from http://www.cff.org/ AboutCF/Testing/NewbornScreening/ScreeningforCF/ Cystic Fibrosis Foundation. (2011d). Airway clearance techniques Retrieved fromhttp://www.cff.org/ treatments/Therapies/Respiratory/AirwayClearance/ D’Agustino J. (2010). Pediatric airway nightmares. Emergency Medical Clinics of North America, 28 119–126. Davis, P. G., Schmidt, B Roberts, R. S., Doyle, L. W Asztalos, E., Haslam, R Tin, W. (2010). Caffeine for apnea of prematurity trial: Benefits may vary in subgroups. Journal of Pediatrics, 156(3), 382–387. Dukhovny D Lorch, S. A., Schmidt, B Doyle, L. W Kok, J. H., Roberts, R. S., Zupancic, J. A. F. (2011). Economic evaluation of caffeine for apnea of prematurity Pediatrics, 127(1), e146–e155. Duncan, J. R Paterson, D. S., Hoffman, J. M., Mokler D. J Borenstein, N. S., Belliveau, R. A., Kinney H. C. (2010). Brainstem serotonergic deficiency in sudden infant death syndrome.Journal of the American Medical Association, 303(5), 430–437. Durbin, W. ., & Stille, C. (2008). Pneumonia. Pediatrics in Review, 29(5), 147–158. Everard, M. L. (2006). Aerosol delivery to children. Pediatric Annals, 35(9), 630–636. Fakhoury K. F Sellers, C., Smith, E. O Rama, J. A., & Fan, L. L. (2010). Serial measurements of lung function in a cohort of young children with bronchopulmonary dysplasia. Pediatrics, 125(6), e1441–e1447.
Flume, P. A., O’Sullivan, B. P Robinson, K. A., Goss, C. H., Mogayzel P. J Willey-Courand, D. B Cystic Fibrosis Foundation, Pulmonary Therapies Committee (2007). Cystic fibrosis pulmonary guidelines: Chronic medications for maintenance of lung health. American Journal of Respiratory and Critical Care Medicine, 176 957–969. Fong E. W & Levin, R. H. (2007). Inhaled corticosteroids for asthma. Pediatrics in Review, 28(6), e30–e35. Fu L. Y Colson, E. R Corwin, M. J & Moon, R. Y. (2008). Infant sleep location: Associated maternal and infant characteristics with sudden infant death syndrome prevention recommendations. Journal of Pediatrics, 153(4), 503–508. Geary, C., Caskey M., Fonseca, R & Malloy M. (2008). Decreased incidence of bronchopulmonary dysplasia after early management changes, including surfactant and nasa continuous positive airway pressure treatment at delivery lowered oxygen saturation goals, and early
Review
1. Describe the signs and symptoms that would indicate that Hannah’s asthma is progressing in severity Develop an asthma action plan that provides guidance for daily management as well as managing asthma symptoms to
2. Identify information about the family’s lifestyle and home environment that could be potential triggers for Hannah’s asthma.
3. Develop an asthma education plan that corresponds to Hannah’s stage of development, and identify appropriate self-care responsibilities to begin teaching her
4. Describe the essential elements of an individualized health plan for Hannah and the actions that must be taken to have one developed in collaboration with the school nurse.
3. An 8-year-old
is diagnosed with viral pneumonia and sent home from the clinic without an antibiotic prescription. The symptoms worsen, and the child returns to the clinic a week later with signs of a higher fever listlessness, and a harsh, productive cough. The child’s mother states, “I knew a prescription for antibiotics was needed.” Which indicates the nurse’s most appropriate response?
1. “It is better to wait to make sure so we don’t use antibiotics unnecessarily This approach also saves healthcare dollars.”
2. “Sometimes we just do not know. I’m glad you came back in.”
Acknowledgments
It is both challenging and a significant responsibility to write a pediatric textbook. Pediatric nursing is constantly changing due to new knowledge and technologies. It is inspiring to observe this evolution of pediatric nursing practice and to have the opportunity to share with nursing students much of our enthusiasm for working with children and their families. We appreciate the opportunity to contribute to the education of a new generation of nurses.
This edition of the textbook used the strong foundation of the first edition and integrated some new features. The production of a textbook requires a team that is fully committed to the vision from the beginning of the revision through the final production process. We were fortunate to have a close collaborative relationship with our publishing company, Pearson. Kim Norbuta, our nursing editor, infused new ideas and approaches into the textbook and accompanying learning aids. We are excited about the coming application of simulations as methods of expanding understanding of pediatric nursing for the student. Julie Alexander, vice president and publisher, has once again enthusiastically supported this venture on behalf of Pearson.
Our developmental editor, Kim Wyatt, has worked with us for several books; she is a cheerleader and a friend, and she has an exquisite eye for detail. She worked side by side with a new editor, Mary Cook, to ensure the quality and timeliness of the present edition. Mary was essential in cultivating our relationship with reviewers— her pleasant and competent manner was outstanding. We thank Maria Reyes, production editor; Patrick Walsh, production managing editor; and editorial assistant Erin Rafferty, for their expertise and valuable contributions. Our thanks also go to Mary Siener for
the textbook design. At S4Carlisle Publishing Services, we thank Lynn Steines for coordinating production, and Joan Lyon for her copyediting skills.
George Dodson took many of the photos in this book. We sincerely thank the children, families, and nurses who allowed us to illustrate development, pediatric healthcare conditions, and nursing care of children in hospital, home, and community settings.
One chapter in the book was written by an expert in a specialized field. We particularly thank Linda Ward for her contributions on genetics and genomics. She is a participant in the National Institutes of Health Summer Genetics Institute and a researcher in education of nurses on these important topics, and we could have no better contributor. We would also like to acknowledge the academic- and clinical-based pediatric nurses who served as reviewers and consultants. Their valuable feedback enabled us to more appropriately focus our chapters for today’s student nurses and the practice of pediatric nursing.
This book emphasizes partnering with families to provide comprehensive care for children. Our own families are also critically important to our lives. Without them we could not reach our own personal and professional goals, and we depend on them every day for support, love, and caring. We thank them for their enduring partnerships and contributions that made this book a reality.
Jane W. Ball
Ruth C. Bindler
Kay J. Cowen
UNIT I
Nurses, Children, and Families 1
Chapter 1
Child Health Nursing: Concepts, Roles, and Issues 2
Overview of Pediatric Health Care 3
Role of the Nurse in the Care of Children 3
Direct Care Provider 3
Patient Educator 5
Patient Advocacy 6
Case Manager 6
Research 6
History of Child Health Care 7
The Beginnings of Child Health Nursing 7
Historic Legislation 8
Other Advances in Child Health Care 8
Nursing Process in Pediatric Care 9
Clinical Reasoning 9
Evidence-Based Practice 9
Assessing Quality of Health Care 10
Contemporary Climate for Pediatric Nursing Care 11
Partnering with Families:
Family-Centered Care 11
Culturally Competent Care 11
Pediatric Health Statistics 12
Infant Mortality 12, Child Mortality 13
Healthy People 2020 14
Morbidity and Hospitalization 14
Healthcare Financing 14
Health Benefits 15
Healthcare Technology 16
Legal and Ethical Concepts and Responsibilities 16
Informed Consent 19, Child Participation in Healthcare Decisions 20, Child’s Rights Versus Parents’ Rights 20, Confidentiality 21, Patient
Self-Determination Act 21
Ethical Concepts and Issues 22
Withholding or Withdrawing Medical Treatment 22, Genetic Testing of Children 23, Organ Transplantation Issues 23
Partnering with Children and Their Families 24
Chapter 2
Family-Centered Care: Theory and Application 28
Family Roles 29
Family-Centered Care 29
History of Family-Centered Care 29
Promoting Family-Centered Care 30
Family Composition 32
Nuclear Family 32
Blended or Reconstituted Family 32
Extended Family 33
Single-Parent Family 33
Binuclear Family 33
Heterosexual Cohabiting Family 34
Gay and Lesbian Family 34
Family Functioning 34
Transition to Parenthood 34
Parental Influences on the Child 35
Family Size 35
Sibling Relationships 35
Parenting 35
Authoritarian Parents 36
Authoritative Parents 36
Permissive Parents 36
Indifferent Parents 36
Parent Adaptability 36
Assessing Parenting Styles 37
Discipline and Limit Setting 38
Special Family Considerations 39
Divorce and Its Effects on Children 39
Stepparenting 39
Foster Care 40
Foster Parenting 41
Health Status of Foster Children 41
Transition to Permanent Placement 41
Adoption 42
Legal Aspects of Adoption 42
Preparation for Adoption 42
International Adoptions 43
Family Theories 43
Family Development Theory 44
Family Systems Theory 44
Family Stress Theory 45
Family Assessment 45
Family Stressors 45
Family Strengths 45
Collecting Data for Family Assessment 46
Family Assessment Tools 46
Genogram 47, Family Ecomap 47, Family APGAR 47, Home Observation for Measurement of the Environment 47, Friedman Family Assessment Model 48, Calgary Family Assessment Model 48
Family Support Services 50
Nursing Management 50
Chapter 3
Cultural Influences 55
Culture—Definitions and Basic Concepts 56
Culture and Nurse Theorists 56
Application of Cultural Theories 58
Definitions Related to Culture 58
Demographics and Cultural Diversity in the United States 59
Cultural Competence in Nursing 59
Health Care and Culture 60
Disparities in Health and Barriers to Health Care 60
Access and Barriers 60, Biological Differences 62, Environmental Differences 63
Cultural Practices That Influence Health Care 63
Family Roles and Organization 63, Communication 64, Time Orientation 65, Nutrition 66
Health Beliefs, Approaches, and Practices 66
Health Beliefs 66, Health Approaches and Practices 67
Nursing Management 71
UNIT II
Child Concepts and Application 77
Chapter 4
Genetic and Genomic Influences 78
Partnering with Families: Meeting the Standard of Genetic Nursing Care Delivery 79
Impact of Genetic Advances on Health Promotion and Health Maintenance 80
Genetic Basics 82
Cell Division 82
Chromosomal Alterations 83
Alterations in Chromosome Number 84, Structural Chromosomal Alterations 84
Genes 85
Distribution and Function of Genes 86, Mitochondrial Genes 86, Gene Alterations and Disease 86, Gene Alterations That Decrease Risk of Disease 87, Genetic Variation: Single Nucleotide Polymorphisms and Copy Number Variants 88
Principles of Inheritance 88
Mendelian Pattern of Inheritance 88
Dominant Versus Recessive Disorders 88, Autosomal Dominant 88, Autosomal Recessive 89, X-Linked 89, X Inactivation 91, Y-Linked Disorders 91
Variability in Classic Mendelian Patterns of Inheritance 91
Theoretic Framework 117, Levels or Systems 117, Nursing Application 119
Temperament Theory 119
Theoretic Framework 119, Nursing
Application 120
Resiliency Theory 120
Theoretic Framework 120, Nursing Application 121
Influences on Development 121
Growth and Development by Age Group 122
Newborn (Up to 1 Month) 122
Physical Growth and Development and Prenatal Influences 122
Cognitive Development 124
Psychosocial Development 124
Infant (1 Month to 1 Year) 126
Video Understanding Growth and Development 126
Cognitive Development 126
Psychosocial Development 130
Video Stages of Play 130, Personality and Temperament 130, Communication 130
Toddler (1 to 3 Years) 131
Physical Growth and Development 131
Cognitive Development 131
Psychosocial Development 132
Play 132, Personality and Temperament 133, Communication 133
Preschool Child (3 to 6 Years) 134
Physical Growth and Development 134
Cognitive Development 135
Psychosocial Development 135
Play 135, Personality and Temperament 135, Communication 137
School-Age Child (6 to 12 Years) 137
Physical Growth and Development 138
Cognitive Development 139
Psychosocial Development 139
Play 139, Personality and Temperament 140, Communication 140, Sexuality 140
Adolescent (12 to 18 Years) 140
Physical Growth and Development 140
Cognitive Development 140
Psychosocial Development 141
Activities 141, Personality and Temperament 142, Communication 142, Sexuality 142
Chapter 6
Child and Family Communication 146
Communication and the Nurse–Child–Family Relationship 147
Forms of Communication 147
Verbal Communication 147
Nonverbal Communication 147
Facial Expressions 149, Body Language 149, Eye Contact 149, Touch 150, Physical Appearance 150
Factors Influencing Communication with Children and Their Families 150
Medical Jargon 150
Gender 151
Child’s Health Status 151
Nursing Attitudes 151
Developmental and Cognitive Considerations for Communication with Children 152
Newborn 152
Infant 152
Toddler and Preschooler 153
School-Age Child 154
Adolescent 154
The Child with Special Needs 154
Communicating with the Child with an Alteration in Visual Perception 154, Communicating with the Child with an Alteration in Hearing Perception 155, Communicating with the Child Who Does Not Speak English 155
Nursing Management 155
Chapter 7
Pediatric and Newborn Assessment 163
Obtaining the Child’s History 164
Communication Strategies 164
Strategies to Build Rapport with the Family and Child 164
Data to Be Collected 165
Patient Information 165, Physiologic Data 165, Psychosocial Data 167, Developmental Data 168
Developmental Approach to the Examination 168
Newborns and Infants Under 6 Months of Age 169
Infants over 6 Months of Age 169
Toddlers 169
Preschoolers 169
School-Age Children 169
Adolescents 169
Anatomic and Physiologic Characteristics of Infants and Children 169
General Appraisal 171
Anthropometric Measurements 171
Infants and Toddlers 171, Preschoolers and School-Age Children 172, Older Children and Adolescents 173
Assessing Skin and Hair 173
Inspection of the Skin 173
Skin Color 173
Palpation of the Skin 174
Temperature 174, Texture 174, Moistness 174, Resilience (Turgor) 174
Capillary Refill Time 174
Skin Lesions 175
Inspection of the Hair 175
Palpation of the Hair 175
Assessing the Head and Face 175
Inspection of the Head and Face 175
Palpation of the Skull 176
Sutures 176, Fontanels 176
Assessing Eyes and Vision 177
Inspection of the External Eye Structures 177
Eye Size and Spacing 177, Eyelids and Eyelashes 178, Eye Color 178, Pupils 178
Inspection of the Eye Muscles 178
Extraocular Movements 179, Corneal Light Reflex 179, Cover–Uncover Test 179
Superficial and Deep Tendon Reflexes 210 Superficial Reflexes 212, Deep Tendon Reflexes 212
Analyzing Data from the Physical Examination 213
Newborn Assessment 214
Newborn Transition 214
Assessment at Birth 214
Assessment of the Newborn 214
Gestational Age Assessment 215, Size for Gestational Age 219, General Appearance 220, Vital Signs 220, Skin 220, Head 221, Eyes 222, Ears 223, Nose 223, Mouth 223, Neck 223, Chest and Lungs 223, Heart 223, Abdomen 224, Genitalia and Anus 224, Extremities 224, Neurologic System 225
UNIT III
Health Promotion and Maintenance Through Childhood 228
Chapter 8
Concepts of Health Promotion and Maintenance 229
Definitions of Health Promotion and Maintenance 230
Application of Resilience and Ecologic Theories 231
Health Supervision in the Pediatric Healthcare Home 234
Components of Health Promotion and Maintenance Visits 236 Contacts with the Family 237
General Observations 237
Growth and Developmental Surveillance 237
Nutrition 239
Physical Activity 240
Oral Health 241
Mental and Spiritual Health 241 Relationships 244
Disease Prevention Strategies 244
Injury Prevention (Safety) Strategies 246
Additional Topics 247
Nursing Management 247
Chapter 9
Health Promotion and Maintenance of the Newborn 252
Early Contacts with the Family 253
Prenatal 253
Prenatal Assessment of Risk and Protective Factors 253
At Birth 254
Assessment of Risk and Protective Factors 255
Newborn Visit Following Hospital Discharge 257
Routine Health Supervision Visits 257
General Observations 257
Growth and Developmental Surveillance 258
At Birth 258
Assessing Growth and Development in the Outpatient Setting 259
Nutrition 260
Breastfeeding 260
Formula Feeding 262
Physical Activity 263
Oral Health 263
Mental and Spiritual Health 263
Promoting Maternal Mental Health 264
Promoting Newborn Mental Health 264
Relationships 267
Disease Prevention Strategies 269
Injury Prevention Strategies 270
Nursing Management 270
Chapter 10
Health Promotion and Maintenance of the Infant 275
Early Contacts with the Family 276
General Observations 276
Growth and Developmental
Surveillance 277
Nutrition 279
Physical Activity 280
Oral Health 281
Mental and Spiritual Health 282
Relationships 284
Family 284
Social Interactions 286
Disease Prevention Strategies 286
Injury Prevention Strategies 288
Nursing Management 288
Chapter 11
Health Promotion and Maintenance of the Toddler and Preschooler 295
General Observations 296
Growth and Developmental
Surveillance 297
Nutrition 299
Physical Activity 301
Oral Health 302
Mental and Spiritual Health 304 Relationships 307
Disease Prevention Strategies 309
Injury Prevention Strategies 311
Nursing Management 314
Chapter 12
Health Promotion and Maintenance of the School-Age Child 319
General Observations 320
Growth and Developmental Surveillance 321
Nutrition 322
Physical Activity 324
Oral Health 326
Mental and Spiritual Health 326
Self-Concept 326
Sexuality 328
Sleep 328
School 328
Mental Health Disorders 329
Spiritual Health 329
Nursing Role 329 Relationships 329
Disease Prevention Strategies 330
Injury Prevention Strategies 332
Nursing Management 334
Chapter 13
Health Promotion and Maintenance of the Adolescent 340
General Observations 341
Growth and Developmental Surveillance 342
Nutrition 343
Physical Activity 346
Oral Health 347
Mental and Spiritual Health 347
Self-Concept 347
Sexuality 348
Sleep 348
School 349
Mental Health Disorders 349
Spiritual Health 349
Nursing Role 349
Relationships 349
Disease Prevention Strategies 351
Injury Prevention Strategies 352
Nursing Management 354
UNIT IV
Child Healthcare Settings and Considerations 358
Chapter 14
Nursing Care of the Child in the Community 359
Community-Based Health Care 360
Characteristics of Community-Based Health Care 360
Roles of Nurses in Community Settings 361
Role of the Pediatric Nurse in an Office or Health Center Setting 361
Identifying Severely Ill and Injured Children 361, Telephone Advice 362, Educating the Child and Family 362, Identifying Community Resources 363, Ensuring a Safe Environment for Children 363
Role of the Pediatric Nurse in a Hospital Outpatient Setting 363
Specialty Care Ambulatory Clinics 363, Urgent Care or Emergency Department Settings 364
Role of the Nurse in a School Setting 364
Community Health Focus 367, School-Based Health Centers 367, Preparation for Emergencies 367, Children with Special Healthcare Needs 368, Facilitating the Child’s Return to School 369
Nursing in Childcare Settings 369
Reducing Disease Transmission 370, Health Promotion 370, Environmental Safety 370, Care for Children with Illnesses 370, Emergency Care Planning 370
Other Community Settings 371
Role of the Nurse in Camp Settings 371
Home Healthcare Nursing 371
Characteristics of Children in Home Care
Services 372, Role of the Pediatric Nurse in Home Care 372
Nursing Management 372
Community Health Nursing 374
Emergency Care Planning 377
Emergency Medical Services for Children 377 Important Pediatric Physiologic Differences 377
Disaster Preparedness 378
Clinical Manifestations 379, Clinical Therapy 379
Nursing Management 380
Chapter 15
Nursing Care of the Hospitalized Child
385
Effects of Hospitalization on Children and Their Families 386
Children’s Understanding of Health and Illness 386
Nurse’s Role in the Child’s Adaptation to Hospitalization 393
Planned Hospitalization 393
Unexpected Hospitalization 394
Nursing Care of the Hospitalized Child 394
Special Units and Types of Care 394
General Pediatric Care Unit 395, Short-Stay, Outpatient, and Ambulatory Surgical Units 395, Emergency Care 395, Intensive Care Unit 396, Isolation 396, Rehabilitation 396
Etiology and Pathophysiology 563, Clinical Manifestations 563
Collaborative Care 563
Diagnostic Tests 563, Clinical Therapy 563
Nursing Management 564
Poisoning 564
Etiology and Pathophysiology 565, Clinical Manifestations 565
Collaborative Care 565
Diagnostic Tests 565, Clinical Therapy 565
Nursing Management 567
Ingestion of Foreign Objects 567
Nursing Management 568
Chapter 21
Pain Assessment and Management 573
Pain 574
Pathophysiology of Pain 574
Neonatal Pathophysiology 575
Misconceptions About Pain in Children 575
Developmental Aspects of Pain Perception, Memory, and Response 575
Cultural Influences on Pain 576
Physiologic Consequences of Pain 577
Effects on Newborns 577
Pain Assessment 577
Pain History 577
Pain Assessment Scales 578
Behavioral Pain Scales for Newborns 578, Behavioral Pain Scales for Infants and Young Children 579, Assessing Children with Cognitive Impairment 579, Self-Report Pain Rating Tools for Children 579