

The Science of Hair Rejuvenation Publications
1927nm Laser and Topical Growth Factor Serum
Did you know 49% of women will experience hair loss at some point in their lives.*
This is just one statistic that is driving the hair rejuvenation market to grow at over 16%**, continuing strongly through 2030 and beyond. Adding a hair rejuvenation offering to your clinic will ensure you maximise your opportunity with current and new patients.
Optimise Your Hair Restoration with KeraFactor and LaseMD ULTRA
At the forefront of hair restoration, the synergy between KeraFactor and LaseMD ULTRA offers a revolutionary approach to treating hair thinning and loss. This innovative combination ensures optimal patient outcomes by leveraging advanced laser technology and potent growth factors.
KeraFactor Hair and Scalp Rejuvenation
KeraFactor is a non-invasive hair treatment that provides a cutting-edge solution for hair and scalp rejuvenation. Suitable for both men and women, discover the science behind our innovative treatments and enhance your aesthetic practice offering today.

A patented and proprietary formulation targets deficiencies that can cause poor scalp health
• Contains six biomimetic growth factors, two skin proteins, and two 2 compounds, each chosen to support scalp and hair health
• Developed in high concentrations not available from other sources
• Delivered in a nano-liposome carrier for increased absorption
KeraFactorMD™ Treatment Serum contains one new growth factor, Follistatin, and two new compounds, PDRN, and NanoFluorosomes, to accelerate the original serum's effectiveness. This combination enables the maximum activation of the scalp-specific ingredients that promote a healthy scalp leading to hair that appears smoother, thicker, and fuller. Our new and improved serum features a DHT-combating compound, amplifying results.
At

home
In office
ULTRA 1927nm Laser
Ultra™ is the superior solution to maintaining skin. Equipped with a 200 μm beam diameter, Ultra’s magnetic roller tracking system can complete a full-face treatment in only 6-8 minutes. Virtually painless and with little to no downtime, LaseMD Ultra is essential for every aesthetic practice.
Key Benefits

• Unmatched power ensures fast treatments that are adaptable to multiple skin areas including the scalp
• Gentle yet comprehensive enhancements to improve all skin types year-round
• Provides comfortable treatments with very little downtime and instant results for pigment, sun damage, tone, and texture
• An intuitive display simplifies navigation and provides practitioners with essential insights for consistently achieving exceptional results
• The specialised comb tip allows you to easily part the hair to ensure maximised laser delivery to the scalp
Why choose Kerafactor and LaseMD ULTRA?
Combining the LaseMD ULTRA laser with KeraFactor serum offers a comprehensive solution for hair restoration. This dual approach not only addresses the symptoms of hair loss but also targets the root causes, ensuring long-lasting and effective results. Whether you're treating the early signs of thinning or looking to improve overall scalp health, this treatment provides a safe, effective, and non-invasive option.








Before and after 18 months
Before and after 8 weeks
Before and 2 weeks post 2nd treatment Courtesy of Julie Winfield, MD USA
After two weeks and 8 weeks
* Dinh QQ, Sinclair R. Female pattern
Fractional Thulium Laser Combined with a Topical Growth Factor Serum Increases Hair Density and Thickness in Male and Female Androgenic Alopecia: A Pilot Study
Fractional Thulium Laser Combined with a Topical Growth Factor Serum Increases Hair Density and Thickness in Male and Female Androgenic Alopecia: A Pilot Study
Fractional Thulium Laser Combined with a Topical Growth Factor Serum Increases Hair Density and Thickness in Male and Female Androgenic Alopecia: A Pilot Study
Amy
Amy F. Taub, MD I Lincolnshire, Illinois, USA I drtaub@advdermatology.com; R.G. Calderhead, MSc, PhD I Seoul, South Korea; Jingmei Li, MD I Seoul, South Korea
Amy F. Taub, MD I Lincolnshire, Illinois, USA I drtaub@advdermatology.com; R.G. Calderhead, MSc, PhD I Seoul, South Korea; Jingmei Li, MD I Seoul, South Korea
F. Taub, MD I Lincolnshire, Illinois, USA I drtaub@advdermatology.com; R.G. Calderhead, MSc, PhD I Seoul, South Korea; Jingmei Li, MD I Seoul, South Korea
Disclosure: Dr. Taub has equity in SkinQRI. Complimentary growth factor serum was supplied to the researchers.
Disclosure: Dr. Taub has equity in SkinQRI. Complimentary growth factor serum was supplied to the researchers.
Disclosure: Dr. Taub has equity in SkinQRI. Complimentary growth factor serum was supplied to the researchers.
ABSTRACT
ABSTRACT
ABSTRACT
Introduction: A new treatment consisting of 1927nm fractional laser followed by application of a sterile growth factor solution has potential to treat androgenic alopecia (AGA). We set out to assess the efficacy of 1927nm laser as a topical assisted delivery system with a proprietary growth factor serum to improve androgenic alopecia, as well as to determine the number of treatments needed.
Introduction: A new treatment consisting of 1927nm fractional laser followed by application of a sterile growth factor solution has potential to treat androgenic alopecia (AGA). We set out to assess the efficacy of 1927nm laser as a topical assisted delivery system with a proprietary growth factor serum to improve androgenic alopecia, as well as to determine the number of treatments needed.
Introduction: A new treatment consisting of 1927nm fractional laser followed by application of a sterile growth factor solution has potential to treat androgenic alopecia (AGA). We set out to assess the efficacy of 1927nm laser as a topical assisted delivery system with a proprietary growth factor serum to improve androgenic alopecia, as well as to determine the number of treatments needed.
Methods: Ten subjects with mild to moderate AGA had a fiducial point tattooed on the temporal or parietal scalp. The subjects were split into three groups based on the number of treatments. A 1927nm laser was applied to the scalp followed by topical application of the sterile hair growth solution. Clinical and quantified trichoscopic photography were performed at baseline and then at 6, 12, and 24 weeks after the final treatment session.
Methods: Ten subjects with mild to moderate AGA had a fiducial point tattooed on the temporal or parietal scalp. The subjects were split into three groups based on the number of treatments. A 1927nm laser was applied to the scalp followed by topical application of the sterile hair growth solution. Clinical and quantified trichoscopic photography were performed at baseline and then at 6, 12, and 24 weeks after the final treatment session.
Methods: Ten subjects with mild to moderate AGA had a fiducial point tattooed on the temporal or parietal scalp. The subjects were split into three groups based on the number of treatments. A 1927nm laser was applied to the scalp followed by topical application of the sterile hair growth solution. Clinical and quantified trichoscopic photography were performed at baseline and then at 6, 12, and 24 weeks after the final treatment session.
Results: All 10 subjects reported no side effects and were subjectively satisfied with their result. Hair parameters showed increased hair density and diameter, both achieving statistical significance over the six-month period. There was no difference between the groups of varying numbers of treatments.
Results: All 10 subjects reported no side effects and were subjectively satisfied with their result. Hair parameters showed increased hair density and diameter, both achieving statistical significance over the six-month period. There was no difference between the groups of varying numbers of treatments.
Results: All 10 subjects reported no side effects and were subjectively satisfied with their result. Hair parameters showed increased hair density and diameter, both achieving statistical significance over the six-month period. There was no difference between the groups of varying numbers of treatments.
Conclusion: Combining fractional 1927nm laser treatments with a growth factor topical solution is safe and effective in the treatment of AGA. Three treatments at 4-weekly intervals is the best choice for treatment protocol.
Conclusion: Combining fractional 1927nm laser treatments with a growth factor topical solution is safe and effective in the treatment of AGA. Three treatments at 4-weekly intervals is the best choice for treatment protocol.
Conclusion: Combining fractional 1927nm laser treatments with a growth factor topical solution is safe and effective in the treatment of AGA. Three treatments at 4-weekly intervals is the best choice for treatment protocol.
Keywords: androgenetic alopecia, fractional laser, hair density, hair diameter, laser assisted topical delivery system
Keywords: androgenetic alopecia, fractional laser, hair density, hair diameter, laser assisted topical delivery system
Keywords: androgenetic alopecia, fractional laser, hair density, hair diameter, laser assisted topical delivery system
INTRODUCTION
INTRODUCTION
INTRODUCTION
Androgenic alopecia (AGA) commonly occurs in both males and females and is also known as male and female pattern hair loss.1 In males, AGA is usually seen when they reach their 30s or 40s, but it can occur in the teens and twenties with around 50% of the male population being affected. In females, approximately 25% of AGA is associated with menopause, but 40% are affected by hair loss by age 50.2 In male pattern AGA, the most common pattern is with the hairline receding to give the characteristic “M” pattern concomitantly with thinning at the parietal area (in hair transplant literature this is referred to as the mid-scalp), with the potential for the two areas to coalesce.1 In females, thinning tends to start more at the parietal area and midline, with loss at the hairline being seen more towards the later stages.1
Androgenic alopecia (AGA) commonly occurs in both males and females and is also known as male and female pattern hair loss.1 In males, AGA is usually seen when they reach their 30s or 40s, but it can occur in the teens and twenties with around 50% of the male population being affected. In females, approximately 25% of AGA is associated with menopause, but 40% are affected by hair loss by age 50.2 In male pattern AGA, the most common pattern is with the hairline receding to give the characteristic “M” pattern concomitantly with thinning at the parietal area (in hair transplant literature this is referred to as the mid-scalp), with the potential for the two areas to coalesce.1 In females, thinning tends to start more at the parietal area and midline, with loss at the hairline being seen more towards the later stages.1
Androgenic alopecia (AGA) commonly occurs in both males and females and is also known as male and female pattern hair loss.1 In males, AGA is usually seen when they reach their 30s or 40s, but it can occur in the teens and twenties with around 50% of the male population being affected. In females, approximately 25% of AGA is associated with menopause, but 40% are affected by hair loss by age 50.2 In male pattern AGA, the most common pattern is with the hairline receding to give the characteristic “M” pattern concomitantly with thinning at the parietal area (in hair transplant literature this is referred to as the mid-scalp), with the potential for the two areas to coalesce.1 In females, thinning tends to start more at the parietal area and midline, with loss at the hairline being seen more towards the later stages.1
One of the major causative factors of AGA is the effect of male hormone on the hair follicle. Conversion of testosterone to dihydrotestosterone (DHT)3 reduces the functioning of the dermal papilla in the hair bulb, thereby interfering with the anagen growth phase of the hair growth cycle. This shift of the hair follicles from anagen into catagen and telogen leads to shorter anagen growth phases, increased senescence of the dermal papilla, and production of hairs with ever-decreasing individual diameters. Not only are the number of hairs diminished, resulting in clinical evidence of hair loss, but the hair that does exist is finer and more fragile. Adults suffering from AGA are increasingly seeking treatment from dermatologists in addition to the growing number of specialist hair loss clinics. Treatments have been mostly associated with the application of minoxidil solution as well as oral anti-androgens for men and women, although finasteride/dutasteride are contraindicated in premenopausal females with spironolactone having some efficacy as monotherapy.2 The antiandrogens slow down the conversion of
One of the major causative factors of AGA is the effect of male hormone on the hair follicle. Conversion of testosterone to dihydrotestosterone (DHT)3 reduces the functioning of the dermal papilla in the hair bulb, thereby interfering with the anagen growth phase of the hair growth cycle. This shift of the hair follicles from anagen into catagen and telogen leads to shorter anagen growth phases, increased senescence of the dermal papilla, and production of hairs with ever-decreasing individual diameters. Not only are the number of hairs diminished, resulting in clinical evidence of hair loss, but the hair that does exist is finer and more fragile. Adults suffering from AGA are increasingly seeking treatment from dermatologists in addition to the growing number of specialist hair loss clinics. Treatments have been mostly associated with the application of minoxidil solution as well as oral anti-androgens for men and women, although finasteride/dutasteride are contraindicated in premenopausal females with spironolactone having some efficacy as monotherapy.2 The antiandrogens slow down the conversion of
testosterone to DHT by blocking the action of the compound 5-alpha reductase. 2 Another recent addition to the hair loss armamentarium that has gained popularity is platelet-rich plasma injections (PRP).4 PRP contains growth factors that are used for wound healing, including some that also stimulate certain portions of the hair life cycle. Although many patients have improvement with these treatments, the variables or incomplete response leads them to seek alternative or additional therapies. A new topical product that is suitable for both males and females contains growth factors and peptides influencing each stage of the life cycle. This formula is specific to hair growth needs. However, the formulation is not a drug and is not intended to be injected (for more information, see patent: https://uspto.report/patent/grant/10,894,074).
One of the major causative factors of AGA is the effect of male hormone on the hair follicle. Conversion of testosterone to dihydrotestosterone (DHT)3 reduces the functioning of the dermal papilla in the hair bulb, thereby interfering with the anagen growth phase of the hair growth cycle. This shift of the hair follicles from anagen into catagen and telogen leads to shorter anagen growth phases, increased senescence of the dermal papilla, and production of hairs with ever-decreasing individual diameters. Not only are the number of hairs diminished, resulting in clinical evidence of hair loss, but the hair that does exist is finer and more fragile. Adults suffering from AGA are increasingly seeking treatment from dermatologists in addition to the growing number of specialist hair loss clinics. Treatments have been mostly associated with the application of minoxidil solution as well as oral anti-androgens for men and women, although finasteride/dutasteride are contraindicated in premenopausal females with spironolactone having some efficacy as monotherapy.2 The antiandrogens slow down the conversion of
Several approaches have been reported to overcome the skin barrier to assist the intradermal delivery of active ingredients, including photobiomodulation (low level light therapy, or LLLT),5 microneedling with or without radiofrequency,6,7 and lasers.8,9 One laser wavelength that has recently attracted favorable attention to deliver actives to the dermis is 1927nm delivered by the thulium fiber laser, as reported by Cho and colleagues.10 The present study used the latest version of the system applied in the Cho study (LaseMD ULTRA, Lutronic Corp, Goyang, South Korea), a thulium fiber laser delivering a fractionated beam at the 1927nm wavelength, combined with topical application of a different patented growth factor serum.
testosterone to DHT by blocking the action of the compound 5-alpha reductase. 2 Another recent addition to the hair loss armamentarium that has gained popularity is platelet-rich plasma injections (PRP).4 PRP contains growth factors that are used for wound healing, including some that also stimulate certain portions of the hair life cycle. Although many patients have improvement with these treatments, the variables or incomplete response leads them to seek alternative or additional therapies. A new topical product that is suitable for both males and females contains growth factors and peptides influencing each stage of the life cycle. This formula is specific to hair growth needs. However, the formulation is not a drug and is not intended to be injected (for more information, see patent: https://uspto.report/patent/grant/10,894,074). Several approaches have been reported to overcome the skin barrier to assist the intradermal delivery of active ingredients, including photobiomodulation (low level light therapy, or LLLT),5 microneedling with or without radiofrequency,6,7 and lasers.8,9 One laser wavelength that has recently attracted favorable attention to deliver actives to the dermis is 1927nm delivered by the thulium fiber laser, as reported by Cho and colleagues.10 The present study used the latest version of the system applied in the Cho study (LaseMD ULTRA, Lutronic Corp, Goyang, South Korea), a thulium fiber laser delivering a fractionated beam at the 1927nm wavelength, combined with topical application of a different patented growth factor serum.
testosterone to DHT by blocking the action of the compound 5-alpha reductase. 2 Another recent addition to the hair loss armamentarium that has gained popularity is platelet-rich plasma injections (PRP).4 PRP contains growth factors that are used for wound healing, including some that also stimulate certain portions of the hair life cycle. Although many patients have improvement with these treatments, the variables or incomplete response leads them to seek alternative or additional therapies. A new topical product that is suitable for both males and females contains growth factors and peptides influencing each stage of the life cycle. This formula is specific to hair growth needs. However, the formulation is not a drug and is not intended to be injected (for more information, see patent: https://uspto.report/patent/grant/10,894,074). Several approaches have been reported to overcome the skin barrier to assist the intradermal delivery of active ingredients, including photobiomodulation (low level light therapy, or LLLT),5 microneedling with or without radiofrequency,6,7 and lasers.8,9 One laser wavelength that has recently attracted favorable attention to deliver actives to the dermis is 1927nm delivered by the thulium fiber laser, as reported by Cho and colleagues.10 The present study used the latest version of the system applied in the Cho study (LaseMD ULTRA, Lutronic Corp, Goyang, South Korea), a thulium fiber laser delivering a fractionated beam at the 1927nm wavelength, combined with topical application of a different patented growth factor serum.
SUBJECTS AND METHODS
SUBJECTS AND METHODS
SUBJECTS AND METHODS
Ten Korean subjects (7 males and 3 females, ages ranging from 29 to 50 years old) with mild to moderate AGA (Norwood Ia-IIb) were recruited into the study. Each subject’s scalp was divided into the left and right sides, and fiducial markers were tattooed onto the scalp just into the
Ten Korean subjects (7 males and 3 females, ages ranging from 29 to 50 years old) with mild to moderate AGA (Norwood Ia-IIb) were recruited into the study. Each subject’s scalp was divided into the left and right sides, and fiducial markers were tattooed onto the scalp just into the
Ten Korean subjects (7 males and 3 females, ages ranging from 29 to 50 years old) with mild to moderate AGA (Norwood Ia-IIb) were recruited into the study. Each subject’s scalp was divided into the left and right sides, and fiducial markers were tattooed onto the scalp just into the
Fractional Thulium Laser Combined with a Topical Growth Factor Serum Increases Hair Density
Fractional Thulium Laser Combined with a Topical Growth Factor Serum Increases Hair Density and Thickness in Male and Female Androgenic Alopecia: A Pilot Study
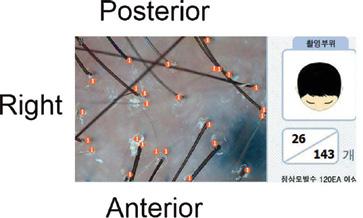
hairline at the bilateral area of frontal hair loss (7 subjects) or just into the hairline on the left side of the parietal hair loss area and the right-side area of the frontal hair loss area (3 subjects) (Figure 1).
FIGURE 3. An example of a typical image captured by the hair and scalp analysis system used in the present study, with the orientation of the image additionally shown relative to the tattooed fiducial spot in the top left corner. The two amounts in the box on the lower right are the hair density calculated by the system.
and Thickness in Male and Female Androgenic Alopecia: A Pilot Study
Amy F. Taub, MD I Lincolnshire, Illinois, USA I drtaub@advdermatology.com; R.G. Calderhead, MSc, PhD I Seoul, South Korea; Jingmei Li, MD I Seoul, South Korea
Amy F. Taub, MD I Lincolnshire, Illinois, USA I drtaub@advdermatology.com; R.G. Calderhead, MSc, PhD I Seoul, South Korea; Jingmei Li, MD I Seoul, South Korea
ABSTRACT

ABSTRACT
The fiducial markers were used to ensure that the same areas were assessed for density and individual hair diameter with a dedicated trichoscopic analysis system at each visit.
Disclosure: Dr. Taub has equity in SkinQRI. Complimentary growth factor serum was supplied to the researchers.
Disclosure: Dr. Taub has equity in SkinQRI. Complimentary growth factor serum was supplied to the researchers.
and after the treatment, and any adverse side effects, such as burning, itching, blistering, erythema, or edema, and subjectively assess their satisfaction with the treatment.
Introduction: A new treatment consisting of 1927nm fractional laser followed by application of a sterile growth factor solution has potential to treat androgenic alopecia (AGA). We set out to assess the efficacy of 1927nm laser as a topical assisted delivery system with a proprietary growth factor serum to improve androgenic alopecia, as well as to determine the number of treatments needed.
Introduction: A new treatment consisting of 1927nm fractional laser followed by application of a sterile growth factor solution has potential to treat androgenic alopecia (AGA). We set out to assess the efficacy of 1927nm laser as a topical assisted delivery system with a proprietary growth factor serum to improve androgenic alopecia, as well as to determine the number of treatments needed.
Methods: Ten subjects with mild to moderate AGA had a fiducial point tattooed on the temporal or parietal scalp. The subjects were split into three groups based on the number of treatments. A 1927nm laser was applied to the scalp followed by topical application of the sterile hair growth solution. Clinical and quantified trichoscopic photography were performed at baseline and then at 6, 12, and 24 weeks after the final treatment session.
Methods: Ten subjects with mild to moderate AGA had a fiducial point tattooed on the temporal or parietal scalp. The subjects were split into three groups based on the number of treatments. A 1927nm laser was applied to the scalp followed by topical application of the sterile hair growth solution. Clinical and quantified trichoscopic photography were performed at baseline and then at 6, 12, and 24 weeks after the final treatment session.
Having had the elements of the trial fully explained to them, including possible results and adverse side effects, all subjects gave written informed consent for their participation in the pilot study and for the use of their clinical photography. The study was carried out adhering to the precepts of the World Medical Association Declaration of Helsinki (2013).
Results: All 10 subjects reported no side effects and were subjectively satisfied with their result. Hair parameters showed increased hair density and diameter, both achieving statistical significance over the six-month period. There was no difference between the groups of varying numbers of treatments.
RESULTS
Results: All 10 subjects reported no side effects and were subjectively satisfied with their result. Hair parameters showed increased hair density and diameter, both achieving statistical significance over the six-month period. There was no difference between the groups of varying numbers of treatments.
The treatment period for all 10 subjects was 12 weeks. Treatment sessions for all subjects were carried out with the fractional thulium laser over the entire scalp using a plastic tip to part the hairs that allows the 1927 to emit at a power output of 1W, pulse energy of 1mJ in dynamic mode, for 4 passes total (approximately 4-5% density overall). The interaction between the 1927nm energy and tissue at these parameters was minimally invasive and subablative with virtually no downtime, as discussed below.
Conclusion: Combining fractional 1927nm laser treatments with a growth factor topical solution is safe and effective in the treatment of AGA. Three treatments at 4-weekly intervals is the best choice for treatment protocol.
Conclusion: Combining fractional 1927nm laser treatments with a growth factor topical solution is safe and effective in the treatment of AGA. Three treatments at 4-weekly intervals is the best choice for treatment protocol.
Keywords: androgenetic alopecia, fractional laser, hair density, hair diameter, laser assisted topical delivery system
Keywords: androgenetic alopecia, fractional laser, hair density, hair diameter, laser assisted topical delivery system
INTRODUCTION
INTRODUCTION
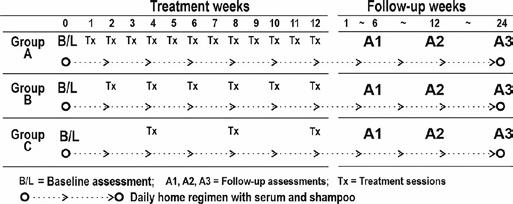
Thulium laser treatment along the rows of the scalp at approximately 1cm intervals in the affected areas was immediately followed by topical application of the sterile vial of solution (approximately 7cc), and gentle massage. All subjects were given supplies of home-use solution and shampoo (less concentrated than the sterile serum); they were instructed to use the shampoo daily in the morning and solution twice per day throughout the 12-week treatment and the 6-month follow-up period. The 10 subjects were split into three groups with different protocols for the treatment sessions as follows: Group A (3 subjects) had 12 sessions at weekly intervals, Group B (5 subjects) had 6 sessions at 2-week intervals, and Group C (2 subjects) had 3 sessions at 4-week intervals (Figure 2).
Androgenic alopecia (AGA) commonly occurs in both males and females and is also known as male and female pattern hair loss.1 In males, AGA is usually seen when they reach their 30s or 40s, but it can occur in the teens and twenties with around 50% of the male population being affected. In females, approximately 25% of AGA is associated with menopause, but 40% are affected by hair loss by age 50.2 In male pattern AGA, the most common pattern is with the hairline receding to give the characteristic “M” pattern concomitantly with thinning at the parietal area (in hair transplant literature this is referred to as the mid-scalp), with the potential for the two areas to coalesce.1 In females, thinning tends to start more at the parietal area and midline, with loss at the hairline being seen more towards the later stages.1
Androgenic alopecia (AGA) commonly occurs in both males and females and is also known as male and female pattern hair loss.1 In males, AGA is usually seen when they reach their 30s or 40s, but it can occur in the teens and twenties with around 50% of the male population being affected. In females, approximately 25% of AGA is associated with menopause, but 40% are affected by hair loss by age 50.2 In male pattern AGA, the most common pattern is with the hairline receding to give the characteristic “M” pattern concomitantly with thinning at the parietal area (in hair transplant literature this is referred to as the mid-scalp), with the potential for the two areas to coalesce.1 In females, thinning tends to start more at the parietal area and midline, with loss at the hairline being seen more towards the later stages.1
One of the major causative factors of AGA is the effect of male hormone on the hair follicle. Conversion of testosterone to dihydrotestosterone (DHT)3 reduces the functioning of the dermal papilla in the hair bulb, thereby interfering with the anagen growth phase of the hair growth cycle. This shift of the hair follicles from anagen into catagen and telogen leads to shorter anagen growth phases, increased senescence of the dermal papilla, and production of hairs with ever-decreasing individual diameters. Not only are the number of hairs diminished, resulting in clinical evidence of hair loss, but the hair that does exist is finer and more fragile. Adults suffering from AGA are increasingly seeking treatment from dermatologists in addition to the growing number of specialist hair loss clinics. Treatments have been mostly associated with the application of minoxidil solution as well as oral anti-androgens for men and women, although finasteride/dutasteride are contraindicated in premenopausal females with spironolactone having some efficacy as monotherapy.2 The antiandrogens slow down the conversion of
All 10 subjects completed the full trial protocol, including the follow-up assessments and the home-care regimen. Subjects reported very little or no discomfort during or after treatment with transient and very mild erythema lasting 1-2 hours as the only side effect, and all subjects were satisfied with the results.
testosterone to DHT by blocking the action of the compound 5-alpha reductase. 2 Another recent addition to the hair loss armamentarium that has gained popularity is platelet-rich plasma injections (PRP).4 PRP contains growth factors that are used for wound healing, including some that also stimulate certain portions of the hair life cycle. Although many patients have improvement with these treatments, the variables or incomplete response leads them to seek alternative or additional therapies. A new topical product that is suitable for both males and females contains growth factors and peptides influencing each stage of the life cycle. This formula is specific to hair growth needs. However, the formulation is not a drug and is not intended to be injected (for more information, see patent: https://uspto.report/patent/grant/10,894,074).
One of the major causative factors of AGA is the effect of male hormone on the hair follicle. Conversion of testosterone to dihydrotestosterone (DHT)3 reduces the functioning of the dermal papilla in the hair bulb, thereby interfering with the anagen growth phase of the hair growth cycle. This shift of the hair follicles from anagen into catagen and telogen leads to shorter anagen growth phases, increased senescence of the dermal papilla, and production of hairs with ever-decreasing individual diameters. Not only are the number of hairs diminished, resulting in clinical evidence of hair loss, but the hair that does exist is finer and more fragile. Adults suffering from AGA are increasingly seeking treatment from dermatologists in addition to the growing number of specialist hair loss clinics. Treatments have been mostly associated with the application of minoxidil solution as well as oral anti-androgens for men and women, although finasteride/dutasteride are contraindicated in premenopausal females with spironolactone having some efficacy as monotherapy.2 The antiandrogens slow down the conversion of
Clinical macrophotography was taken with a digital camera under identical lighting and distance conditions at baseline and at 6, 12, and 24 weeks after the final treatment session. At the same assessment points, the tattooed fiducial markers were used to position the scanner of the D-vella Hair & Scalp trichoscopic diagnostic system (KC Technical, Seoul, Korea) to measure the hair density over a given sample area (6mm × 4mm, 0.24cm²) and to simultaneously measure the thickness or diameter of individual hairs in that area. Figure 3 shows an example of the readout from the system. Subjects were asked to report any discomfort during
Several approaches have been reported to overcome the skin barrier to assist the intradermal delivery of active ingredients, including photobiomodulation (low level light therapy, or LLLT),5 microneedling with or without radiofrequency,6,7 and lasers.8,9 One laser wavelength that has recently attracted favorable attention to deliver actives to the dermis is 1927nm delivered by the thulium fiber laser, as reported by Cho and colleagues.10 The present study used the latest version of the system applied in the Cho study (LaseMD ULTRA, Lutronic Corp, Goyang, South Korea), a thulium fiber laser delivering a fractionated beam at the 1927nm wavelength, combined with topical application of a different patented growth factor serum.
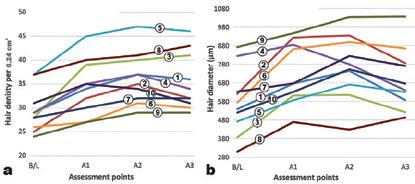
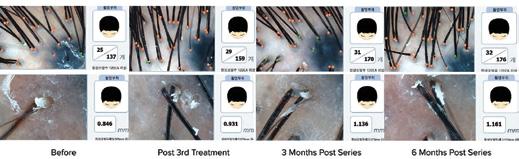
The clinical photography in all cases demonstrated increased hair density that reached maximum effect in most subjects at the 12-week assessment point with some reduction at the 24-week assessment (representative cases illustrated in Figure 4). These findings were echoed in the objective trichoscopic data, with the greatest improvement generally seen at the 3-month assessment point. High statistical significance (p .0004-.0001) was seen between baseline findings and all assessment points, including the 6-month point. Statistical significance shown between baseline and assessment point data, illustrated graphically for each subject in Figure 5, and with representative trichoscopic imaging findings for density and diameter for Case 1 in Figure 6.
testosterone to DHT by blocking the action of the compound 5-alpha reductase. 2 Another recent addition to the hair loss armamentarium that has gained popularity is platelet-rich plasma injections (PRP).4 PRP contains growth factors that are used for wound healing, including some that also stimulate certain portions of the hair life cycle. Although many patients have improvement with these treatments, the variables or incomplete response leads them to seek alternative or additional therapies. A new topical product that is suitable for both males and females contains growth factors and peptides influencing each stage of the life cycle. This formula is specific to hair growth needs. However, the formulation is not a drug and is not intended to be injected (for more information, see patent: https://uspto.report/patent/grant/10,894,074). Several approaches have been reported to overcome the skin barrier to assist the intradermal delivery of active ingredients, including photobiomodulation (low level light therapy, or LLLT),5 microneedling with or without radiofrequency,6,7 and lasers.8,9 One laser wavelength that has recently attracted favorable attention to deliver actives to the dermis is 1927nm delivered by the thulium fiber laser, as reported by Cho and colleagues.10 The present study used the latest version of the system applied in the Cho study (LaseMD ULTRA, Lutronic Corp, Goyang, South Korea), a thulium fiber laser delivering a fractionated beam at the 1927nm wavelength, combined with topical application of a different patented growth factor serum.
4. Results of three cases from groups A, B, and C at (from left to right) baseline, 3-month assessment, and 6-month assessment. Top set shows the improvement in Case 1 (38-year-old male), center set shows the improvement in Case 8 (49-year-old female), and bottom set shows improvement in Case 4 (29-year-old female).

SUBJECTS AND METHODS
SUBJECTS AND METHODS
Ten Korean subjects (7 males and 3 females, ages ranging from 29 to 50 years old) with mild to moderate AGA (Norwood Ia-IIb) were recruited into the study. Each subject’s scalp was divided into the left and right sides, and fiducial markers were tattooed onto the scalp just into the
The trial protocol called for the subjects to be allocated to three groups with different frequency of laser treatment protocols during the 12-week treatment period. Group A had 12 sessions at weekly intervals, Group B had 6 sessions at 2-week intervals, and Group C had 3 sessions at 4-week intervals. Figure 7 compares changes in density and diameter among the three groups with no group showing higher
Ten Korean subjects (7 males and 3 females, ages ranging from 29 to 50 years old) with mild to moderate AGA (Norwood Ia-IIb) were recruited into the study. Each subject’s scalp was divided into the left and right sides, and fiducial markers were tattooed onto the scalp just into the
FIGURE
FIGURE 1. Schematic illustrating the placement of the fiducial points tattooed into the scalp, and the area treated with the ULTRA system.
FIGURE 2. The 12-week and 6-month protocols for both clinic (Tx) and at home (open circle) treatments for Groups A, B, and C.
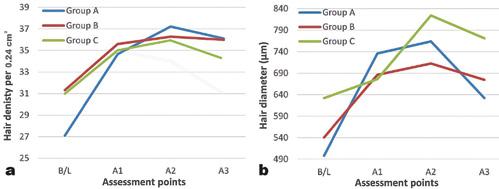
5. Line graphs illustrating the course of improvement for each individual subject in hair density as hair counts per 0.24cm2 sample area (a) and individual hair diameter expressed in μm (b) as assessed by the trichoscopic diagnostic system.
Fractional Thulium Laser Combined with a Topical Growth Factor Serum Increases Hair Density and Thickness in Male and Female Androgenic Alopecia: A Pilot Study
Amy F. Taub, MD I Lincolnshire, Illinois, USA I drtaub@advdermatology.com; R.G. Calderhead, MSc, PhD I Seoul, South Korea; Jingmei Li, MD I Seoul, South Korea
has been a grassroots movement to highlight adverse effects such as impotence, erectile dysfunction, and depression for men who take them, leading to reluctance and/or poor compliance by patients.13 Females can only safely take them if they are post-menopausal, and they seem to have less response to them than males.14 Females are also given oral spironolactone, which seems to work much better as an acne therapy than as a hair loss therapy (personal observation by author).
Fractional Thulium Laser Combined with a Topical Growth Factor Serum Increases Hair Density and Thickness in Male and Female Androgenic Alopecia: A Pilot Study
Amy F. Taub, MD I Lincolnshire, Illinois, USA I drtaub@advdermatology.com; R.G. Calderhead, MSc, PhD I Seoul, South Korea; Jingmei Li, MD I Seoul, South Korea
Disclosure: Dr. Taub has equity in SkinQRI. Complimentary growth factor serum was supplied to the researchers.
Disclosure: Dr. Taub has equity in SkinQRI. Complimentary growth factor serum was supplied to the researchers.
ABSTRACT
ABSTRACT
density and in the bottom row hair thickness.
Introduction: A new treatment consisting of 1927nm fractional laser followed by application of a sterile growth factor solution has potential to treat androgenic alopecia (AGA). We set out to assess the efficacy of 1927nm laser as a topical assisted delivery system with a proprietary growth factor serum to improve androgenic alopecia, as well as to determine the number of treatments needed.
Introduction: A new treatment consisting of 1927nm fractional laser followed by application of a sterile growth factor solution has potential to treat androgenic alopecia (AGA). We set out to assess the efficacy of 1927nm laser as a topical assisted delivery system with a proprietary growth factor serum to improve androgenic alopecia, as well as to determine the number of treatments needed.
Topical minoxidil is the oldest therapy that has scientific evidence of efficacy. The mechanism of action is believed to be dilation and expansion of the capillary bed in the scalp to increase nutrition to the papillae, counteracting the miniaturization process. Although this is widely utilized with some success, it often isn’t successful at all or only partially, or has some other characteristics, such as stickiness of formulation or initial shedding of hair, that lead many to abandon it.15
Methods: Ten subjects with mild to moderate AGA had a fiducial point tattooed on the temporal or parietal scalp. The subjects were split into three groups based on the number of treatments. A 1927nm laser was applied to the scalp followed by topical application of the sterile hair growth solution. Clinical and quantified trichoscopic photography were performed at baseline and then at 6, 12, and 24 weeks after the final treatment session.
Methods: Ten subjects with mild to moderate AGA had a fiducial point tattooed on the temporal or parietal scalp. The subjects were split into three groups based on the number of treatments. A 1927nm laser was applied to the scalp followed by topical application of the sterile hair growth solution. Clinical and quantified trichoscopic photography were performed at baseline and then at 6, 12, and 24 weeks after the final treatment session.
Results: All 10 subjects reported no side effects and were subjectively satisfied with their result. Hair parameters showed increased hair density and diameter, both achieving statistical significance over the six-month period. There was no difference between the groups of varying numbers of treatments.
statistical significance in improvement. Because of the low number of subjects in each group, the statistical power is also very low, but a trend towards a similar level of efficacy is clearly seen among all three groups.
Results: All 10 subjects reported no side effects and were subjectively satisfied with their result. Hair parameters showed increased hair density and diameter, both achieving statistical significance over the six-month period. There was no difference between the groups of varying numbers of treatments.
Conclusion: Combining fractional 1927nm laser treatments with a growth factor topical solution is safe and effective in the treatment of AGA. Three treatments at 4-weekly intervals is the best choice for treatment protocol.
Conclusion: Combining fractional 1927nm laser treatments with a growth factor topical solution is safe and effective in the treatment of AGA. Three treatments at 4-weekly intervals is the best choice for treatment protocol.
Keywords: androgenetic alopecia, fractional laser, hair density, hair diameter, laser assisted topical delivery system
Keywords: androgenetic alopecia, fractional laser, hair density, hair diameter, laser assisted topical delivery system
INTRODUCTION
INTRODUCTION
7. Line graphs illustrating the course of improvement in Groups A, B, and C in hair density (a) and hair diameter (b) from baseline through assessment points A1, A2, and A3. The pattern is the same among the three groups with greatest efficacy at A2, and no statistical significance seen among the groups.
DISCUSSION
Androgenic alopecia (AGA) commonly occurs in both males and females and is also known as male and female pattern hair loss.1 In males, AGA is usually seen when they reach their 30s or 40s, but it can occur in the teens and twenties with around 50% of the male population being affected. In females, approximately 25% of AGA is associated with menopause, but 40% are affected by hair loss by age 50.2 In male pattern AGA, the most common pattern is with the hairline receding to give the characteristic “M” pattern concomitantly with thinning at the parietal area (in hair transplant literature this is referred to as the mid-scalp), with the potential for the two areas to coalesce.1 In females, thinning tends to start more at the parietal area and midline, with loss at the hairline being seen more towards the later stages.1
As mentioned, DHT is recognized as one of the major causative factors in the induction of pattern baldness. The driving force behind anagen, the growth phase in the hair cycle, is the influence of the dermal papilla on the active differentiation of stem cells within the hair bulb.11 These stem cells are “pushed” by the dermal papilla to differentiate to produce keratinocytes and keratin, which forms the cortex, the bulk of the growing hair shaft, and the protective cuticle.12 DHT interferes with the signaling processes that support differentiation and induces breakdown of the anagen phase thereby forcing the hair into catagen (transformational phase) and prolonged telogen (resting phase). Subsequent anagen phases become shorter and hairs become progressively thinner and weaker. The growth factor solution in this study contains a specific patented blend of synthetic oligo- and polypeptides designed to augment the protein signaling processes and boost the driving power of the dermal papilla during the anagen phase of hair growth, thereby counteracting the deleterious effects of DHT, thus prolonging the anagen phase.
The problem with topical products of any kind is that they need to reach the dermis to be effective. The hair follicle bulb, where the dermal papilla does its critical work, is deep in the scalp subcutis. The epidermis, in particular the stratum corneum, the waterproof outer layer of the epidermis, plays a very important role as part of the skin barrier function, preventing toxic substances, microbials, and allergens from entering the dermis and causing harm to dermal cells and extracellular matrix. Unfortunately, the skin barrier function equally prevents beneficial substances from reaching the dermis, and the role of the laser is to temporarily defeat, but not permanently destroy, the power of the skin barrier function, especially the stratum corneum. Although each polypeptide in the treatment preparations is wrapped individually in liposomes and have been proven to penetrate hair follicles to the bulge where most of the growth factor receptors are present, laser assisted topical delivery was hypothesized to greatly increase the potential concentration of actives reaching the dermis, as has been shown with other topical therapies.16
Androgenic alopecia (AGA) commonly occurs in both males and females and is also known as male and female pattern hair loss.1 In males, AGA is usually seen when they reach their 30s or 40s, but it can occur in the teens and twenties with around 50% of the male population being affected. In females, approximately 25% of AGA is associated with menopause, but 40% are affected by hair loss by age 50.2 In male pattern AGA, the most common pattern is with the hairline receding to give the characteristic “M” pattern concomitantly with thinning at the parietal area (in hair transplant literature this is referred to as the mid-scalp), with the potential for the two areas to coalesce.1 In females, thinning tends to start more at the parietal area and midline, with loss at the hairline being seen more towards the later stages.1
One of the major causative factors of AGA is the effect of male hormone on the hair follicle. Conversion of testosterone to dihydrotestosterone (DHT)3 reduces the functioning of the dermal papilla in the hair bulb, thereby interfering with the anagen growth phase of the hair growth cycle. This shift of the hair follicles from anagen into catagen and telogen leads to shorter anagen growth phases, increased senescence of the dermal papilla, and production of hairs with ever-decreasing individual diameters. Not only are the number of hairs diminished, resulting in clinical evidence of hair loss, but the hair that does exist is finer and more fragile. Adults suffering from AGA are increasingly seeking treatment from dermatologists in addition to the growing number of specialist hair loss clinics. Treatments have been mostly associated with the application of minoxidil solution as well as oral anti-androgens for men and women, although finasteride/dutasteride are contraindicated in premenopausal females with spironolactone having some efficacy as monotherapy.2 The antiandrogens slow down the conversion of
One of the major causative factors of AGA is the effect of male hormone on the hair follicle. Conversion of testosterone to dihydrotestosterone (DHT)3 reduces the functioning of the dermal papilla in the hair bulb, thereby interfering with the anagen growth phase of the hair growth cycle. This shift of the hair follicles from anagen into catagen and telogen leads to shorter anagen growth phases, increased senescence of the dermal papilla, and production of hairs with ever-decreasing individual diameters. Not only are the number of hairs diminished, resulting in clinical evidence of hair loss, but the hair that does exist is finer and more fragile.
testosterone to DHT by blocking the action of the compound 5-alpha reductase. 2 Another recent addition to the hair loss armamentarium that has gained popularity is platelet-rich plasma injections (PRP).4 PRP contains growth factors that are used for wound healing, including some that also stimulate certain portions of the hair life cycle. Although many patients have improvement with these treatments, the variables or incomplete response leads them to seek alternative or additional therapies. A new topical product that is suitable for both males and females contains growth factors and peptides influencing each stage of the life cycle. This formula is specific to hair growth needs. However, the formulation is not a drug and is not intended to be injected (for more information, see patent: https://uspto.report/patent/grant/10,894,074). Several approaches have been reported to overcome the skin barrier to assist the intradermal delivery of active ingredients, including photobiomodulation (low level light therapy, or LLLT),5 microneedling with or without radiofrequency,6,7 and lasers.8,9 One laser wavelength that has recently attracted favorable attention to deliver actives to the dermis is 1927nm delivered by the thulium fiber laser, as reported by Cho and colleagues.10 The present study used the latest version of the system applied in the Cho study (LaseMD ULTRA, Lutronic Corp, Goyang, South Korea), a thulium fiber laser delivering a fractionated beam at the 1927nm wavelength, combined with topical application of a different patented growth factor serum.
Most DHT blockers are oral prescription medications. There
Adults suffering from AGA are increasingly seeking treatment from dermatologists in addition to the growing number of specialist hair loss clinics. Treatments have been mostly associated with the application of minoxidil solution as well as oral anti-androgens for men and women, although finasteride/dutasteride are contraindicated in premenopausal females with spironolactone having some efficacy as monotherapy.2 The antiandrogens slow down the conversion of
testosterone to DHT by blocking the action of the compound 5-alpha reductase. 2 Another recent addition to the hair loss armamentarium that has gained popularity is platelet-rich plasma injections (PRP).4 PRP contains growth factors that are used for wound healing, including some that also stimulate certain portions of the hair life cycle. Although many patients have improvement with these treatments, the variables or incomplete response leads them to seek alternative or additional therapies. A new topical product that is suitable for both males and females contains growth factors and peptides influencing each stage of the life cycle. This formula is specific to hair growth needs. However, the formulation is not a drug and is not intended to be injected (for more information, see patent: https://uspto.report/patent/grant/10,894,074). Several approaches have been reported to overcome the skin barrier to assist the intradermal delivery of active ingredients, including photobiomodulation (low level light therapy, or LLLT),5 microneedling with or without radiofrequency,6,7 and lasers.8,9 One laser wavelength that has recently attracted favorable attention to deliver actives to the dermis is 1927nm delivered by the thulium fiber laser, as reported by Cho and colleagues.10 The present study used the latest version of the system applied in the Cho study (LaseMD ULTRA, Lutronic Corp, Goyang, South Korea), a thulium fiber laser delivering a fractionated beam at the 1927nm wavelength, combined with topical application of a different patented growth factor serum.
SUBJECTS AND METHODS
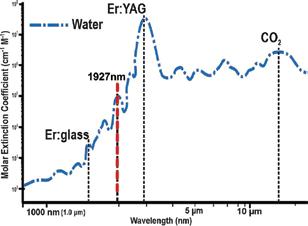
The 1927nm laser wavelength was chosen because it has a better absorption in water than the 1540nm wavelength typical of nonablative Er:glass lasers, but less than the fully ablative wavelengths of the Er:YAG (2940 nm) and CO2 (10600 nm) lasers (Figure 8). Figure 9 illustrates the histology of the 1927nm fractional laser’s impact on skin at the parameters used in the present study. The stratum corneum has been temporarily disrupted, the tight cell-cell adhesion of the stratum spinosum has been transiently degraded, and very mild and controlled coagulation has occurred in the very superficial dermis with minimal disruption to the dermoepidermal junction. This combination of events should allow topically applied solution to make its way more easily through the epidermis and into the dermis, especially when the ingredients are encapsulated in nanoliposomes. Additional benefits arise from the
FIGURE 8. The water absorption curve in the near and mid-infrared waveband showing the absorption coefficients for the nonablative Er:glass and ablative Er:YAG and CO2 lasers compared with the subablative LaseMD ULTRA.
SUBJECTS AND METHODS
Ten Korean subjects (7 males and 3 females, ages ranging from 29 to 50 years old) with mild to moderate AGA (Norwood Ia-IIb) were recruited into the study. Each subject’s scalp was divided into the left and right sides, and fiducial markers were tattooed onto the scalp just into the
Ten Korean subjects (7 males and 3 females, ages ranging from 29 to 50 years old) with mild to moderate AGA (Norwood Ia-IIb) were recruited into the study. Each subject’s scalp was divided into the left and right sides, and fiducial markers were tattooed onto the scalp just into the
FIGURE
FIGURE 6. Imaging from the hair & scalp trichoscopic diagnostic system for Case 1, showing in the top row hair
FIGURE
FIGURE 9. Histological specimen showing a typical ULTRA impact in human skin at low parameters: see text for details. (Hematoxylin-eosin stain, scale bar 200 μm)
Fractional Thulium Laser Combined with a Topical Growth Factor Serum Increases Hair Density and Thickness in Male and Female Androgenic Alopecia: A Pilot Study
Fractional Thulium Laser Combined with a Topical Growth Factor Serum Increases Hair Density and Thickness in Male and Female Androgenic Alopecia: A Pilot Study
eters were used for the 1927nm laser, and there was a slightly better result on the portion of scalp receiving solution that was not statistically significant. One cannot discount the fact that through absorption, the growth factors could have also stimulated the opposite side of the scalp because all patients had one portion of their scalp with solution applied immediately after treatment as well as use of take-home product.
Amy F. Taub, MD I Lincolnshire, Illinois, USA I drtaub@advdermatology.com; R.G. Calderhead, MSc, PhD I Seoul, South Korea; Jingmei Li, MD I Seoul, South Korea
CONCLUSION
Amy F. Taub, MD I Lincolnshire, Illinois, USA I drtaub@advdermatology.com; R.G. Calderhead, MSc, PhD I Seoul, South Korea; Jingmei Li, MD I Seoul, South Korea
Disclosure: Dr. Taub has equity in SkinQRI. Complimentary growth factor serum was supplied to the researchers.
ABSTRACT

Disclosure: Dr. Taub has equity in SkinQRI. Complimentary growth factor serum was supplied to the researchers.
ABSTRACT
Introduction: A new treatment consisting of 1927nm fractional laser followed by application of a sterile growth factor solution has potential to treat androgenic alopecia (AGA). We set out to assess the efficacy of 1927nm laser as a topical assisted delivery system with a proprietary growth factor serum to improve androgenic alopecia, as well as to determine the number of treatments needed.
mild damage caused to the scalp as illustrated in Figure 9, resulting in a gentle wound healing response delivering some rejuvenating effect and improving the dermal environment, potentially increasing blood supply to the dermal papillae as part of the wound healing mechanism. Because the resulting reaction is gentle and subablative, downtime for the patient is extremely short and discomfort is virtually nonexistent (occasional mild sunburn sensation that resolves within a few to 48 hours).
Methods: Ten subjects with mild to moderate AGA had a fiducial point tattooed on the temporal or parietal scalp. The subjects were split into three groups based on the number of treatments. A 1927nm laser was applied to the scalp followed by topical application of the sterile hair growth solution. Clinical and quantified trichoscopic photography were performed at baseline and then at 6, 12, and 24 weeks after the final treatment session.
Methods: Ten subjects with mild to moderate AGA had a fiducial point tattooed on the temporal or parietal scalp. The subjects were split into three groups based on the number of treatments. A 1927nm laser was applied to the scalp followed by topical application of the sterile hair growth solution. Clinical and quantified trichoscopic photography were performed at baseline and then at 6, 12, and 24 weeks after the final treatment session.
This pilot study has demonstrated that a fractional 1927nm laser acts as an efficient topical delivery system for a proprietary growth factor solution, producing statistically significant results for both hair density and hair diameter, and clinically apparent hair growth with patient satisfaction that lasted until the six-month follow-up. Further studies with larger populations are encouraged and needed to confirm the optimistic results of this small population study.
Introduction: A new treatment consisting of 1927nm fractional laser followed by application of a sterile growth factor solution has potential to treat androgenic alopecia (AGA). We set out to assess the efficacy of 1927nm laser as a topical assisted delivery system with a proprietary growth factor serum to improve androgenic alopecia, as well as to determine the number of treatments needed.
References
Results: All 10 subjects reported no side effects and were subjectively satisfied with their result. Hair parameters showed increased hair density and diameter, both achieving statistical significance over the six-month period. There was no difference between the groups of varying numbers of treatments.
1. Vary JC, Jr. Selected disorders of skin appendages—acne, alopecia, hyperhidrosis. Med Clin North Am (Review). 2012; 99:1195-1211.
Results: All 10 subjects reported no side effects and were subjectively satisfied with their result. Hair parameters showed increased hair density and diameter, both achieving statistical significance over the six-month period. There was no difference between the groups of varying numbers of treatments.
Conclusion: Combining fractional 1927nm laser treatments with a growth factor topical solution is safe and effective in the treatment of AGA. Three treatments at 4-weekly intervals is the best choice for treatment protocol.
Conclusion: Combining fractional 1927nm laser treatments with a growth factor topical solution is safe and effective in the treatment of AGA. Three treatments at 4-weekly intervals is the best choice for treatment protocol.
Keywords: androgenetic alopecia, fractional laser, hair density, hair diameter, laser assisted topical delivery system
Keywords: androgenetic alopecia, fractional laser, hair density, hair diameter, laser assisted topical delivery system
INTRODUCTION
INTRODUCTION
There was little difference in the efficacy for both increased hair density and thicker hair diameter among the groups in the study (Figure 7). Being able to demonstrate a statistically significant increase in both hair density and hair diameter was the most important finding of the study. Most patients are concerned with the appearance of the coverage of their scalp or the ability to visualize the scalp beneath the hair. The hair diameter finding gives the added benefit of making the hairs appear thicker as well as more numerous.
Androgenic alopecia (AGA) commonly occurs in both males and females and is also known as male and female pattern hair loss.1 In males, AGA is usually seen when they reach their 30s or 40s, but it can occur in the teens and twenties with around 50% of the male population being affected. In females, approximately 25% of AGA is associated with menopause, but 40% are affected by hair loss by age 50.2 In male pattern AGA, the most common pattern is with the hairline receding to give the characteristic “M” pattern concomitantly with thinning at the parietal area (in hair transplant literature this is referred to as the mid-scalp), with the potential for the two areas to coalesce.1 In females, thinning tends to start more at the parietal area and midline, with loss at the hairline being seen more towards the later stages.1
2. Famenini S, et al. Demographics of women with female pattern hair loss and the effectiveness of spironolactone therapy. J Am Acad Dermatol. 2015; 73(4):705-706.
3. Tai T, Kochhar A. Physiology and Medical Treatments for Alopecia. Facial Plast Surg Clin North Am. 2020(May); 28(2):149-159.
Androgenic alopecia (AGA) commonly occurs in both males and females and is also known as male and female pattern hair loss.1 In males, AGA is usually seen when they reach their 30s or 40s, but it can occur in the teens and twenties with around 50% of the male population being affected. In females, approximately 25% of AGA is associated with menopause, but 40% are affected by hair loss by age 50.2 In male pattern AGA, the most common pattern is with the hairline receding to give the characteristic “M” pattern concomitantly with thinning at the parietal area (in hair transplant literature this is referred to as the mid-scalp), with the potential for the two areas to coalesce.1 In females, thinning tends to start more at the parietal area and midline, with loss at the hairline being seen more towards the later stages.1
One of the major causative factors of AGA is the effect of male hormone on the hair follicle. Conversion of testosterone to dihydrotestosterone (DHT)3 reduces the functioning of the dermal papilla in the hair bulb, thereby interfering with the anagen growth phase of the hair growth cycle. This shift of the hair follicles from anagen into catagen and telogen leads to shorter anagen growth phases, increased senescence of the dermal papilla, and production of hairs with ever-decreasing individual diameters. Not only are the number of hairs diminished, resulting in clinical evidence of hair loss, but the hair that does exist is finer and more fragile.
One might have assumed that a higher number of treatment sessions with shorter intervals between treatments would have produced better results than a lower number of sessions with longer intervals, but no such advantage was seen in the present study. It could well be, given the large interindividual differences seen among the subjects (Figure 5), that a study with a larger patient population for the three groups would show an advantage for more laser treatment sessions and shorter intervals. It is also possible that the papillae or bulbs have limits to the degree or time in which they can produce more or better hairs. However, it is not always possible either from the viewpoint of finance or time constraints for patients to attend more frequently, so the preliminary results from this pilot study should give hope that this will be a more practical therapeutic option. The 24-week time point is a strength of the study, with hair density and diameter remaining statistically significantly improved versus baseline. Given the fact that many did see the hair counts start to fall could indicate that a treatment every 3 months may be optimal. A weighting of products to determine usage of home therapy was not undertaken.
One of the major causative factors of AGA is the effect of male hormone on the hair follicle. Conversion of testosterone to dihydrotestosterone (DHT)3 reduces the functioning of the dermal papilla in the hair bulb, thereby interfering with the anagen growth phase of the hair growth cycle. This shift of the hair follicles from anagen into catagen and telogen leads to shorter anagen growth phases, increased senescence of the dermal papilla, and production of hairs with ever-decreasing individual diameters. Not only are the number of hairs diminished, resulting in clinical evidence of hair loss, but the hair that does exist is finer and more fragile.
Adults suffering from AGA are increasingly seeking treatment from dermatologists in addition to the growing number of specialist hair loss clinics. Treatments have been mostly associated with the application of minoxidil solution as well as oral anti-androgens for men and women, although finasteride/dutasteride are contraindicated in premenopausal females with spironolactone having some efficacy as monotherapy.2 The antiandrogens slow down the conversion of
The major limitations of this study are its size and the lack of a control group. It may be possible that either the 1927nm fractional laser treatments or the treatment solution alone caused the results. The main aim of this pilot study was to assess the efficacy of the fractional 1927nm thulium laser as laser assisted topical delivery for the growth factor solution, and this efficacy was clearly illustrated for both hair density and individual hair diameter. A previously performed similar study using the 1927 laser, a 12 × 1 week time point, and a different proprietary solution showed good results with respect to hair counts and diameter as well.10 In the prior study, more aggressive param -
Adults suffering from AGA are increasingly seeking treatment from dermatologists in addition to the growing number of specialist hair loss clinics. Treatments have been mostly associated with the application of minoxidil solution as well as oral anti-androgens for men and women, although finasteride/dutasteride are contraindicated in premenopausal females with spironolactone having some efficacy as monotherapy.2 The antiandrogens slow down the conversion of
testosterone to DHT by blocking the action of the compound 5-alpha reductase. 2 Another recent addition to the hair loss armamentarium that has gained popularity is platelet-rich plasma injections (PRP).4 PRP contains growth factors that are used for wound healing, including some that also stimulate certain portions of the hair life cycle. Although many patients have improvement with these treatments, the variables or incomplete response leads them to seek alternative or additional therapies. A new topical product that is suitable for both males and females contains growth factors and peptides influencing each stage of the life cycle. This formula is specific to hair growth needs. However, the formulation is not a drug and is not intended to be injected (for more information, see patent: https://uspto.report/patent/grant/10,894,074). Several approaches have been reported to overcome the skin barrier to assist the intradermal delivery of active ingredients, including photobiomodulation (low level light therapy, or LLLT),5 microneedling with or without radiofrequency,6,7 and lasers.8,9 One laser wavelength that has recently attracted favorable attention to deliver actives to the dermis is 1927nm delivered by the thulium fiber laser, as reported by Cho and colleagues.10 The present study used the latest version of the system applied in the Cho study (LaseMD ULTRA, Lutronic Corp, Goyang, South Korea), a thulium fiber laser delivering a fractionated beam at the 1927nm wavelength, combined with topical application of a different patented growth factor serum.
4. Ferrando J, et al. A proposal of an effective platelet-rich plasma protocol for the treatment of androgenetic alopecia. Int J Trichol. 2017(Oct-Dec); 9(4):165-170.
5. Darwin E, et al. Low-level laser therapy for the treatment of androgenic alopecia: a review. Lasers Med Sci. 2018; 33:425-434.
6. Kim YC, Park JH, Prausnitz MR. Microneedles for drug and vaccine delivery. Adv Drug Deliv Rev. 2012; 64:1547-1568.
7. Yu AJ, et al. A pilot split-scalp study of combined fractional radiofrequency microneedling and 5% topical minoxidil in treating male pattern hair loss. Clin Exp Dermatol. 2018; 43:775-781.
8. Searle T, et al. Lessons learned from the first decade of laser-assisted drug delivery. Dermatol Ther (Heidelb). 2021; 11:93-104.
9. Dabek RJ, et al. Laser-assisted hair regrowth: fractional laser modalities for the treatment of androgenic alopecia. Plast Reconstr Surg Glob Open. 2019(Apr); 7:e2157. Published online 2019 Apr 11.
10. Cho SB, et al. Therapeutic efficacy and safety of a 1927-nm fractionated thulium laser on pattern hair loss: an evaluator-blinded, split-scalp study. Lasers Med Sci. 2018; 33:851-859.
11. Driskell RR, et al. Hair follicle dermal papilla cells at a glance. J Cell Sci. 2011; 124(Pt 8):1179-1182.
12. Santos Z, et al. Drug discovery for alopecia: gone today, hair tomorrow. Expert Opin Drug Discov. 2015(Mar); 10(3):269-292.
13. Shin YS, et al. Finasteride and erectile dysfunction in patients with benign prostatic hyperplasia or male androgenetic alopecia. World J Mens Health. 2019; 37(2):157-165.
testosterone to DHT by blocking the action of the compound 5-alpha reductase. 2 Another recent addition to the hair loss armamentarium that has gained popularity is platelet-rich plasma injections (PRP).4 PRP contains growth factors that are used for wound healing, including some that also stimulate certain portions of the hair life cycle. Although many patients have improvement with these treatments, the variables or incomplete response leads them to seek alternative or additional therapies. A new topical product that is suitable for both males and females contains growth factors and peptides influencing each stage of the life cycle. This formula is specific to hair growth needs. However, the formulation is not a drug and is not intended to be injected (for more information, see patent: https://uspto.report/patent/grant/10,894,074). Several approaches have been reported to overcome the skin barrier to assist the intradermal delivery of active ingredients, including photobiomodulation (low level light therapy, or LLLT),5 microneedling with or without radiofrequency,6,7 and lasers.8,9 One laser wavelength that has recently attracted favorable attention to deliver actives to the dermis is 1927nm delivered by the thulium fiber laser, as reported by Cho and colleagues.10 The present study used the latest version of the system applied in the Cho study (LaseMD ULTRA, Lutronic Corp, Goyang, South Korea), a thulium fiber laser delivering a fractionated beam at the 1927nm wavelength, combined with topical application of a different patented growth factor serum.
SUBJECTS AND METHODS
14. Iamsumang W, Leerunyakul K, Suchonwanit P. Finasteride and its potential for the treatment of female pattern hair loss: evidence to date. Drug Des Devel Ther. 2020; 14:951-959. Published 2020 Mar 2.
SUBJECTS AND METHODS
Ten Korean subjects (7 males and 3 females, ages ranging from 29 to 50 years old) with mild to moderate AGA (Norwood Ia-IIb) were recruited into the study. Each subject’s scalp was divided into the left and right sides, and fiducial markers were tattooed onto the scalp just into the
15. Messenger AG, Rundegren J. Minoxidil: mechanisms of action on hair growth. Br J Dermatol. 2004(Feb);150(2):186-94.
16. Waibel JS, et al. Update of ablative fractionated lasers to enhance cutaneous topical drug delivery. Adv Ther. 2017; 34(8):1840-1849. n
Ten Korean subjects (7 males and 3 females, ages ranging from 29 to 50 years old) with mild to moderate AGA (Norwood Ia-IIb) were recruited into the study. Each subject’s scalp was divided into the left and right sides, and fiducial markers were tattooed onto the scalp just into the
LasersinMedicalScience
LasersinMedicalScience
LasersinMedicalScience
https://doi.org/10.1007/s10103-018-2437-5
https://doi.org/10.1007/s10103-018-2437-5
https://doi.org/10.1007/s10103-018-2437-5
ORIGINALARTICLE
ORIGINALARTICLE


Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
SungBinCho 1,2
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Abstract
Abstract
Abstract
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Introduction
Introduction
Introduction
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
* HeesuKim yollikim@gmail.com
* HeesuKim yollikim@gmail.com
* HeesuKim yollikim@gmail.com
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
LasersinMedicalScience
LasersinMedicalScience
https://doi.org/10.1007/s10103-018-2437-5
https://doi.org/10.1007/s10103-018-2437-5
ORIGINALARTICLE
Table1 Experimentalsettingsof1927-nmfractionatedthuliumlaser treatmentforinvivoexperimentalhairlessmousestudy Power(W)Energy(mJ)Fluence(J/cm2)Pulseduration(ms)
Table1 Experimentalsettingsof1927-nmfractionatedthuliumlaser treatmentforinvivoexperimentalhairlessmousestudy Power(W)Energy(mJ)Fluence(J/cm2)Pulseduration(ms)
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
water,candamageorevenscarhairshafts,leadingtohairloss. Additionally,wepreviouslysuggestedthattreatmentwiththuliumlasersmaystimulatetheproliferationoffollicularand perifollicularcellsinthescalp,which,alongwithlaserassisteddrugdelivery,couldbemajorcontributingfactorsto thesuccessoflaser-assistedhairrestorationtherapy[5].Our studygrouppreviouslydemonstratedinapilot,comparative clinicalstudythatcombinedtreatmentwithafractionatedthuliumlaser,andpolydeoxyribonucleotide(PDRN) intraperifollicularinjectionsaremoreeffectiveatimproving hairdensityandthicknessthancombinedtreatmentwith mesotherapyandPDRNinjectiontreatments[5].
water,candamageorevenscarhairshafts,leadingtohairloss. Additionally,wepreviouslysuggestedthattreatmentwiththuliumlasersmaystimulatetheproliferationoffollicularand perifollicularcellsinthescalp,which,alongwithlaserassisteddrugdelivery,couldbemajorcontributingfactorsto thesuccessoflaser-assistedhairrestorationtherapy[5].Our studygrouppreviouslydemonstratedinapilot,comparative clinicalstudythatcombinedtreatmentwithafractionatedthuliumlaser,andpolydeoxyribonucleotide(PDRN) intraperifollicularinjectionsaremoreeffectiveatimproving hairdensityandthicknessthancombinedtreatmentwith mesotherapyandPDRNinjectiontreatments[5].
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
Abstract
Abstract
Inthisstudy,weaimedtoevaluatetheefficacyandsafety ofa1927-nmfractionatedthuliumlaserdevicefortreating PHL.Todoso,aninvivohairlessmousestudyandan invivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedtopreclinicallyevaluate skininteractionswithfractionatedthuliumlaserenergyatdifferentpowerandenergysettings.Additionally,weperformed aprospective,evaluator-blinded,split-scalpstudytoevaluate hairthicknessesanddensitiesfor10PHLpatientstreatedwith 12sessionsofthefractionatedthuliumlaserdevice,withor withoutpost-lasertreatmentapplicationofgrowthfactorcontaining(GF)solution,atbaselineandat4and12weeks afterthefinaltreatment.
Inthisstudy,weaimedtoevaluatetheefficacyandsafety ofa1927-nmfractionatedthuliumlaserdevicefortreating PHL.Todoso,aninvivohairlessmousestudyandan invivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedtopreclinicallyevaluate skininteractionswithfractionatedthuliumlaserenergyatdifferentpowerandenergysettings.Additionally,weperformed aprospective,evaluator-blinded,split-scalpstudytoevaluate hairthicknessesanddensitiesfor10PHLpatientstreatedwith 12sessionsofthefractionatedthuliumlaserdevice,withor withoutpost-lasertreatmentapplicationofgrowthfactorcontaining(GF)solution,atbaselineandat4and12weeks afterthefinaltreatment.
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Materialsandmethods
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Materialsandmethods
Animalstudy
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Animalstudy
Introduction
Introduction
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
(parameter3),werealsodeliveredtountreatedbackskinof thehairlessmiceoverasinglepulseinastaticoperatingmode. At1h,3days,and7daysaftertreatment,biopsyspecimensof fullthicknessfromthehairlessmouseskinwereobtainedand fixedin10%bufferedformalin.Then,serialsectionsof5 μm inthicknesswerepreparedandstainedwithhematoxylinand eosin.Theexperimentalmiceweresacrificedforsamplingthe treatedskininahumanemanneraccordingtostandard protocols.
(parameter3),werealsodeliveredtountreatedbackskinof thehairlessmiceoverasinglepulseinastaticoperatingmode. At1h,3days,and7daysaftertreatment,biopsyspecimensof fullthicknessfromthehairlessmouseskinwereobtainedand fixedin10%bufferedformalin.Then,serialsectionsof5 μm inthicknesswerepreparedandstainedwithhematoxylinand eosin.Theexperimentalmiceweresacrificedforsamplingthe treatedskininahumanemanneraccordingtostandard protocols.
Environmentalscanningelectronmicroscopy
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
* HeesuKim yollikim@gmail.com
* HeesuKim yollikim@gmail.com
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
Environmentalscanningelectronmicroscopy
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
AllexperimentalprotocolswereapprovedbytheethicscommitteeoftheInstitutionalAnimalCareandUseCommitteeof InternationalSt.Mary ’sHospital,CatholicKwandong UniversityCollegeofMedicine,Incheon,Korea.Atotalof 18male,hairlessmice(Hr-1,JapanSLCInc.,ShizuokaKen, Japan;6weeksold)wereusedtoconductallexperiments,and allexperimentswerecarriedoutinaccordancewithapproved guidelines.Generalanesthesiawasachievedwithanintraperitonealbolusinjectionof0.2mg/kgofZoletil®(Vibrac, Carros,France)and5mg/kgofxylazinehydrochloride.The backsoftheexperimentalmicewerecleansedwith70%alcoholandmarkedwithinklinestooutline1-cm2 gridsforeach treatmentparameter(atotalof8grids/mouse;8cm2).Then, 1927-nmfractionatedthuliumlaser(LASEMD™;Lutronic Corp.,Goyang,Korea)treatmentwasdeliveredtotheback skinatthepowersettingsof1,3,and5W;attheenergy settingsof5mJ(63.7J/cm2),10mJ(127.3J/cm2),15mJ (191J/cm2),and20mJ(254.7J/cm2);andoverasinglepulse inastaticoperatingmode(Table 1).Additionally,presettreatmentparametersforthisdevice,includingapowerof3Wand anenergyof1.6mJ(20.4J/cm2)(parameter1),4Wand2mJ (25.5J/cm2)(parameter2),and5Wand2.4mJ(30.6J/cm2)
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
AllexperimentalprotocolswereapprovedbytheethicscommitteeoftheInstitutionalAnimalCareandUseCommitteeof InternationalSt.Mary ’sHospital,CatholicKwandong UniversityCollegeofMedicine,Incheon,Korea.Atotalof 18male,hairlessmice(Hr-1,JapanSLCInc.,ShizuokaKen, Japan;6weeksold)wereusedtoconductallexperiments,and allexperimentswerecarriedoutinaccordancewithapproved guidelines.Generalanesthesiawasachievedwithanintraperitonealbolusinjectionof0.2mg/kgofZoletil®(Vibrac, Carros,France)and5mg/kgofxylazinehydrochloride.The backsoftheexperimentalmicewerecleansedwith70%alcoholandmarkedwithinklinestooutline1-cm2 gridsforeach treatmentparameter(atotalof8grids/mouse;8cm2).Then, 1927-nmfractionatedthuliumlaser(LASEMD™;Lutronic Corp.,Goyang,Korea)treatmentwasdeliveredtotheback skinatthepowersettingsof1,3,and5W;attheenergy settingsof5mJ(63.7J/cm2),10mJ(127.3J/cm2),15mJ (191J/cm2),and20mJ(254.7J/cm2);andoverasinglepulse inastaticoperatingmode(Table 1).Additionally,presettreatmentparametersforthisdevice,includingapowerof3Wand anenergyof1.6mJ(20.4J/cm2)(parameter1),4Wand2mJ (25.5J/cm2)(parameter2),and5Wand2.4mJ(30.6J/cm2)
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
ForESEMstudy,a40-year-oldmaleparticipantwithnoremarkablepastmedicalhistorywastreatedwithasinglesessionof1927-nmfractionatedthuliumlaser(LASEMD™) treatmentonthelowerback,afterobtainingwritteninformed consent.ThisESEMstudywasapprovedbytheInstitutional ReviewBoardofInternationalSt.Mary’sHospital,Catholic KwandongUniversityCollegeofMedicine(IS16SSSI0008). Thepowerandenergysettingswere1Wand5mJ,5Wand 3mJ(38.2J/cm2),5Wand10mJ,and5Wand20mJ, respectively,andasinglepassofeachlasersettingwasdeliveredunderastaticoperatingmode.Then,toobtainfull-thickness,verticallyexcisedskinspecimens,punchbiopsiesof 3mmindiameterofeachsettingwereperformedbyDr. GooBimmediatelyafterthelasertreatment.Thespecimens werehydratedthroughouttheirpreparation.Immediate1927nmfractionatedthuliumlaser-inducedtissuereactionswere evaluatedbyafieldemissionESEM(PhilipsXL30FEG; FEI/PhilipsElectronOptics,Eindhoven,Netherlands)witha resolutionoflessthan2nm,aprimaryelectronbeamacceleratingvoltageoflessthan30kV,amagnificationrangeof10–
ForESEMstudy,a40-year-oldmaleparticipantwithnoremarkablepastmedicalhistorywastreatedwithasinglesessionof1927-nmfractionatedthuliumlaser(LASEMD™) treatmentonthelowerback,afterobtainingwritteninformed consent.ThisESEMstudywasapprovedbytheInstitutional ReviewBoardofInternationalSt.Mary’sHospital,Catholic KwandongUniversityCollegeofMedicine(IS16SSSI0008). Thepowerandenergysettingswere1Wand5mJ,5Wand 3mJ(38.2J/cm2),5Wand10mJ,and5Wand20mJ, respectively,andasinglepassofeachlasersettingwasdeliveredunderastaticoperatingmode.Then,toobtainfull-thickness,verticallyexcisedskinspecimens,punchbiopsiesof 3mmindiameterofeachsettingwereperformedbyDr. GooBimmediatelyafterthelasertreatment.Thespecimens werehydratedthroughouttheirpreparation.Immediate1927nmfractionatedthuliumlaser-inducedtissuereactionswere evaluatedbyafieldemissionESEM(PhilipsXL30FEG; FEI/PhilipsElectronOptics,Eindhoven,Netherlands)witha resolutionoflessthan2nm,aprimaryelectronbeamacceleratingvoltageoflessthan30kV,amagnificationrangeof10
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
LasersinMedicalScience
LasersinMedicalScience
https://doi.org/10.1007/s10103-018-2437-5
https://doi.org/10.1007/s10103-018-2437-5
ORIGINALARTICLE
500,000,andavacuumrangeof10–10 8 Torr.ThisexaminationwasperformedattheKoreaInstituteofScienceand Technology(KIST,Seoul,Korea).Then,thezonesofthulium laser-inducedtissuecoagulation(LITC)intheESEMimages wereestimatedusingImageJsoftware,version1.50(National InstitutesofHealth,Bethesda,MD,USA).
Objectiveclinicalevaluation
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
Patientsandtreatmentprotocol
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
Received:16April2017/Accepted:3January2018
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
# Springer-VerlagLondonLtd.,partofSpringerNature2018
Abstract
Abstract
Atotalof10Koreanmalepatients(meanage42.6± 10.5years;agerange25–69years)withPHLwereenrolled inthisstudy.DiagnosisofPHLwasmadebyphysicalexaminationandphototrichogramstoevaluatetheclinicalfeatures ofminiaturizedterminalhairsand/orareducednumbersof hairswithnegativehairpulltests.Inthisstudy,patientswho hadbeentreatedforPHLwithtopicalandoralmedications, includingminoxidil,alfatradiol,prostaglandinanalogs,finasteride,dutasteride,andanti-androgens;mesotherapyand intraperifollicularinjectiontherapy;laser/light-basedtherapy, includingfractionatedlasertreatmentandlow-levellighttherapy;intraperifollicularplatelet-richplasmapreparationinjection;andhairtransplantationwithinthepreceding6months wereexcluded.ThisstudywasapprovedbytheInstitutional ReviewBoardofInternationalSt.Mary’sHospital,Catholic KwandongUniversityCollegeofMedicine(IS16SSSI0008).
Forobjectiveevaluation,theparticipants’ scalpsweremarked withblack-coloredtattooink(Intenze;SouthRocellePark, NJ,USA).First,thepointofintersectionofthemid-sagittal lineandthecoronallinewasdesignatedasastandardpoint (P1),andthen,referencepointsweremadeoneachsideofthe scalpalongthecoronallinewiththesamedistancefromthe standardpoint(P2andP3)[5, 9].Digitalimagesofthescalp andhairswerecapturedat1-foldmagnificationusingadigital singlelensreflexcamera(Sonya-7;SonyCorp.,Tokyo, Japan)andata50-foldmagnificationusingacomputerized handheldUSBcameraPTsystem(Follioscope®;LeedM Corporation,Seoul,Korea)atbaselineandat4and12weeks afterthefinaltreatment.Thereafter,relativevaluesofhair numbersandthicknessweremeasuredwiththeanalyzeand measureplug-inusingImageJsoftware.Also,ateachtreatmentsessionandat4and12weeksafterthelasttreatment, PHLpatientsweresurveyedinregardstoanysideeffectsthat couldbeassociatedwiththetreatment,includingintolerable pain,scalprednessandedema,oozing,bleeding,scalingor crusting,orremarkablehairloss.
Statisticalanalysis
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Introduction
Introduction
Afterobtainingwritteninformedconsent,atotalof10patientsreceived12sessionsof1927-nmfractionatedthulium laser(LASEMD™)treatmentatweeklyintervals.Todoso, thescalpwasfirstcleansedwith70%ethanol,afterwhich thuliumlasertreatmentatapowerof5Wandanenergyof 4mJ(50.9J/cm2)or6mJ(76.4J/cm2)underastaticoperating modewasdeliveredonthefrontal,mid,andvertexareas. Approximately,atotalof100–140pulsesweredeliveredon thescalp,andeachpulsegenerated40fractionatedthermal injuryzonesina10mm×4mmareaonthescalpskin.All procedureswereperformedwithoutlocalanesthesia.
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
* HeesuKim yollikim@gmail.com
* HeesuKim yollikim@gmail.com
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
Immediatelyafterthethuliumlasertreatment,aGFsolution(LASEMD™ CKAmpoule;LutronicCorp.)wasapplied onarandomlyselectedhalfofthescalpatadoseof1.5to 2ml.TheingredientsintheGFsolutionincludedkeratinocyte growthfactor;humancordbloodcell-conditionedmedia, whichmainlycontainedplatelet-derivedgrowthfactor,vascularendothelialgrowthfactor,hepatocytegrowthfactor, insulin-likegrowthfactor1,andfibroblastgrowthfactor;genistein; Scutellariabaicalensis root ’sextract; Paeonia suffruticosa root’sextract;hydrolyzedsodiumhyaluronate; sodiumhyaluronate;mannitol;glycerin;andpurifiedwater. Theparticipantswereinstructedtoapplyabout1mlofthe GFsolutiononthesamehalfofthescalponceadayfor 12weeks.Noothertreatments,exceptforthefractionated thuliumlasertreatment,wereperformedontheothersideof thescalp.Duringthecourseoftreatmentandfollow-up,other treatmentmodalitiesfortreatingPHLwereprohibited.
Anormalitytestwasperformedforclinicaldatausing Kolmogorov-Smirnovtest,andthen,resultswereanalyzed byapaired t testandadjustedbaselinelinearmixedmodel procedurewithBonferroniposthocanalysisbyparametric criteriausingSASsoftwareversion9.2(SASInstituteInc., Cary,NC,USA).Differenceswith P valuesoflessthan0.05 wereconsideredstatisticallysignificant.
Results
Invivoexperimentalhairlessmousestudy
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
Tomorphometricallyevaluate1927-nmfractionatedthulium laser-inducedtissuereactionsandtodeterminetheoptimal lasersettingsfortreatingpatientswithPHL,aninvivoexperimentalhairlessmousestudywasperformed.Immediately aftertreatment,invertedcone-shapedzonesofLITCwere foundintheepidermisanduppertomid-dermiswithoutremarkableablativetissueinjuryinallexperimentalsettings (Fig. 1).Whenincreasingthepowerataconsistentlevelof energy,thepulsedurationwasshortened.Thereby,atthesame energysetting,higherpowercreatednarroweranddeeper zonesofLITCinthedermis,withhigherdegreesoftissue coagulation.Meanwhile,whenincreasingtheenergyataconsistentpower,thepulsedurationwasprolonged.Thereby,at thesamepowersetting,higherenergygeneratedwiderand deeperzonesofLITCintheepidermisanddermis,with LasersMedSci ORIGINALARTICLE
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
LasersinMedicalScience
LasersinMedicalScience
https://doi.org/10.1007/s10103-018-2437-5
https://doi.org/10.1007/s10103-018-2437-5
ORIGINALARTICLE
ORIGINALARTICLE
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
SungBinCho 1,2 &
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser
onpatternhairloss:anevaluator-blinded,split-scalpstudy
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Abstract
Abstract
Fig.1 Invivohairlessmouse studyatvarioustreatment settings.Immediatetissue reactionsof1927-nmfractionated thuliumlasertreatmentininvivo hairlessmouseskinusing a a powerof1Wandanenergyof 5mJ(63.7J/cm2), b 3Wand 1.6mJ(20.4J/cm2), c 4Wand 2mJ(25.5J/cm2),and d 5Wand 2.4mJ(30.6J/cm2).Onehour afterthuliumlasertreatment, invertedcone-shapedzonesof laser-inducedtissuecoagulation werefoundintheepidermisand uppertomid-dermiswithout remarkableablativetissueinjury inallexperimentalsettings (brokenlines).Hematoxylinand eosinstain,originalmagnification ×400,scalebar=100 μm
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
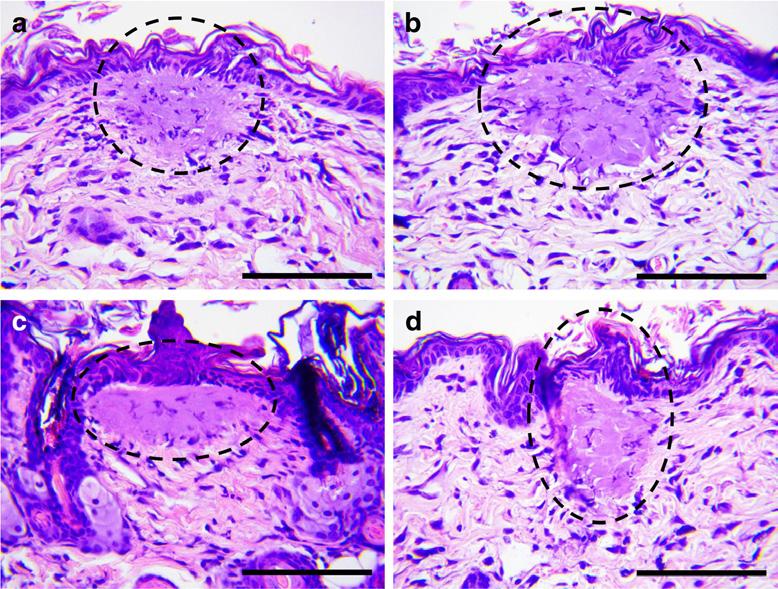
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
similardegreesoftissuecoagulation(Fig. 2).Thestructural integrityofthecoagulatedepidermalanddermalareaswas wellpreservedinalltreatmentsettings.Additionally,hairfollicleswithinoraroundLITCzonesexhibitedcoagulationof follicularconnectivetissueandtheouterrootsheath,butno destructionthereof.
Introduction
Introduction
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
* HeesuKim yollikim@gmail.com
* HeesuKim yollikim@gmail.com
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
Tissuespecimensatpost-treatment3daysshowed hypereosinophilicdermalcollagenfibersalongwithnotable increasesinfibroblastsandinflammatorycellsinallexperimentalsettings(Fig. 3a,b).Atpost-treatment7days,the epidermalpartsofLITCzoneswerealmostcompletelyrecovered,andvacuolarchangesinthedermoepidermaljunction wereobserved(Fig. 3c,d).Additionally,inthedermis,fibroblastsanddermalcollagenfiberswereremarkablyincreased andpresentedregularhorizontalrearrangement.Nonetheless, noexcessiveirregularcollagenbundleformation,which wouldbesuggestiveofskinscarring,wasfoundinanyof theexperimentalsettings,andfollicularstructureswerewell preserved.Accordingly,fortreatingPHLpatientsinthisstudy, wedecidedtouseapowerof5Wandanenergyof4or6mJ underastaticoperatingmodeinordertogeneratenarrower anddeeperLITCzonesinthedermis,comparedtotheother experimentalsettings.
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
zonesofnon-ablativeLITConthesurfaceofthestratum corneuminallexperimentalsettings.Themeandiametersof theLITCzonesintheESEMimageswereestimatedas129.7 ±17.7 μmatthesettingsof5Wand3mJand216.5±24 μm at5Wand20mJ.Furthermore,theexperimentalsettingsof 1Wand5mJand5Wand3mJelicitedmultiple,small, heterogeneous,roundholeswithameandiameterof6.7± 4.1 μmthatlikelyformedaswaterevaporatedfromslightly depressedLITCzones(Fig. 4a).Meanwhile,theexperimental settingsof5Wand10mJand5Wand20mJelicitedthe formationofdome-shaped,papularLITCzoneswithahigher degreeofthermalcoagulationandnosmallholestherein, comparedtotreatmentswith1Wand5mJand5Wand 3mJ(Fig. 4b).
Splithumanscalpstudy
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
Environmentalscanningelectronmicroscopy
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
TheESEMstudy,whichwasperformedimmediatelyafter 1927-nmfractionatedthuliumlasertreatmentoninvivohumanbackskin,revealedtheformationofroundtooval-shaped
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
Atthepointofintersectionofthemid-sagittallineandthe coronalline(P1),themeanbaselinehaircountwas163.7± 31.1hairs,withameanhairthicknessof0.047±0.009mm (Figs. 5 and 6).Incomparisontothesebaselinevalues,both haircountsandthicknessincreasedsignificantlyto195.3± 34.3(P <0.001)and0.059±0.01mm(P <0.001),respectively,at1weekaftercompletingthe12sessionsof1927-nm fractionatedthuliumlasertreatment;to197.5±33.6 (P <0.001)and0.059±0.01mm(P <0.001),respectively, at1monthafterthefinaltreatment;andto188.8±38.3(P = 0.001)and0.06±0.012mm( P <0.001),respectively,at 3monthsafterthefinaltreatment.
LasersinMedicalScience
LasersinMedicalScience
https://doi.org/10.1007/s10103-018-2437-5
LasersMedSci
https://doi.org/10.1007/s10103-018-2437-5
ORIGINALARTICLE
ORIGINALARTICLE
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 &
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Fig.2 Invivohairlessmouse studyatapowerof5W. Immediatetissuereactionsof 1927-nmfractionatedthulium lasertreatmentininvivohairless mouseskinusing a anenergyof 5mJ, b 10mJ(127.3J/cm2), c 15mJ(191J/cm2),and d 20mJ (254.7J/cm2).Onehourafter thuliumlasertreatment,zonesof laser-inducedtissuecoagulation werefoundintheepidermisand uppertomid-dermis(broken lines).Atthesamepowersetting, higherenergygeneratedwider anddeepercoagulationzonesin theepidermisanddermis. Hematoxylinandeosinstain, originalmagnification×400, scalebar=100 μm
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Abstract
Abstract
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
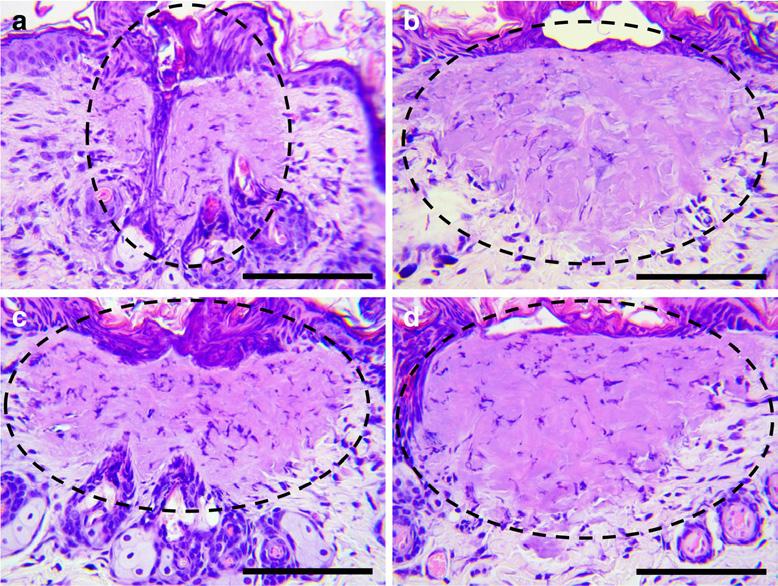
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
AtP2,whichwastreatedonlywith12sessionsof 1927-nmfractionatedthuliumlasertreatment,themean baselinehaircountwas187.2±39.4hairs,withamean hairthicknessof0.047±0.011mm.Comparedtothe baselinevalues,bothhaircountsandthicknessincreased
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
significantlyto217.3±42.4( P <0.001)and0.059± 0.01mm(P <0.001),respectively,at1weekaftercompletingthe12sessionsoflasertreatment;to203.3±38.3 ( P <0.001)and0.057±0.01mm(P <0.001),respectively, at1monthafterthefinaltreatment;andto197.1±36.6
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Introduction
Introduction
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
* HeesuKim yollikim@gmail.com
* HeesuKim yollikim@gmail.com
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
Fig.3 Invivohairlessmouse studyatapowerof5Wandan energyof20mJ.Tissuereactions of1927-nmfractionatedthulium lasertreatmentininvivohairless mouseskinat a, b 3daysand c, d 7dayspost-treatment.Tissue specimensat3daysposttreatmentexhibited hypereosinophilicdermal collagenfibers,alongwith notableincreasesinfibroblasts andinflammatorycells.At7days post-treatment,theepidermal partsofcoagulationzoneswere almostcompletelyrecovered,and fibroblastsanddermalcollagen fiberswereremarkablyincreased inthedermis.Hematoxylinand eosinstain,originalmagnification a, c ×100,scalebar=200 μm, b, d ×400,scalebar=100 μm
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
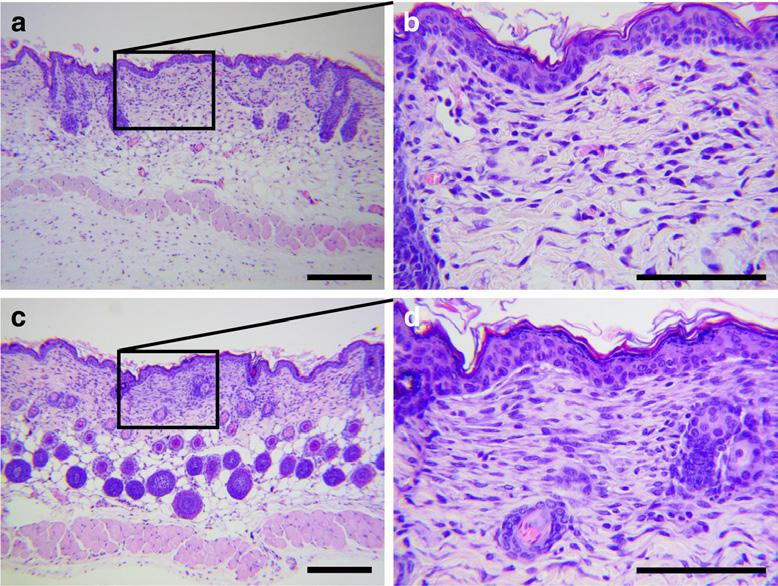
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
HeesuKim
KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
LasersinMedicalScience
LasersinMedicalScience
https://doi.org/10.1007/s10103-018-2437-5
https://doi.org/10.1007/s10103-018-2437-5
ORIGINALARTICLE
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
SungBinCho 1,2 & BoncheolLeoGoo
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Abstract
Abstract
Fig.4 Environmentalscanningelectronmicroscopy.Thuliumlaserinducedtissuecoagulationzones(brokenlines)onthestratumcorneum oftheinvivohumanbackskinimmediatelyafter1927-nmfractionated
( P >0.05)and0.056±0.009mm( P <0.001)at3months afterthefinaltreatment.
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
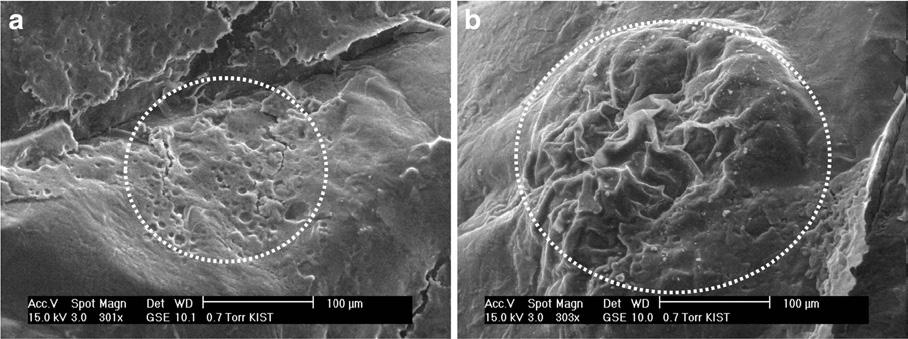
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
AttheP3,whichwastreatedwith12sessionsof1927-nm fractionatedthuliumlasertreatmentand12-weekapplication ofaGFsolution,themeanbaselinehaircountwas178.2±35 hairs;themeanhairthicknesswas0.047±0.011mm.Incomparisontobaselinevalues,bothhaircountsandthicknessincreasedto227.6±35.5( P <0.001)and0.06±0.011mm (P <0.001),respectively,at1weekaftercompletingthecombinationtreatment;to197.8±35.1(P =0.001)and0.058± 0.009mm(P <0.001),respectively,at1monthafterthefinal
Keywords
thuliumlasertreatmentatthetreatmentsettingsof a 5Wand3mJ(38.2J/ cm2)and b 5Wand20mJ.Scalebar=100 μm
treatment;andto197.7±40( P =0.031)and0.058± 0.012mm(P <0.001),respectively,at3monthsafterthefinal treatment.
Linearmixedmodelanalysis
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Inthelinearmixedmodelanalysis,thevariablesofhaircount andhairthicknesswerepresentedaschangesfrombaseline, andanadjustedbaselinelinearmixedmodelwasapplied (Table 2;Fig. 7).Bydoingso,themixedmodelanalysisof haircountsrevealedasignificantinteractioneffectbetween
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Introduction
Introduction
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
* HeesuKim yollikim@gmail.com
* HeesuKim yollikim@gmail.com
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
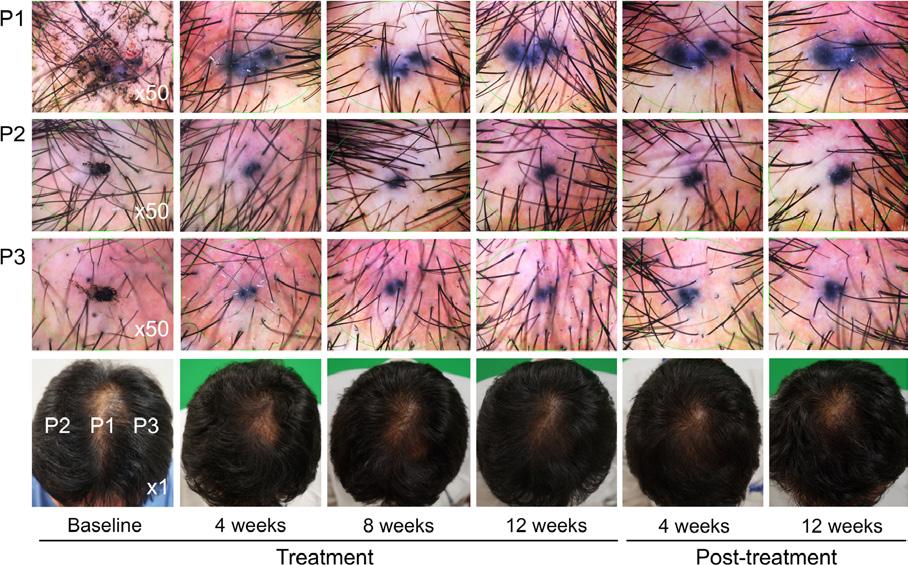
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
Fig.5 RepresentativedigitalimagesofhairsatpointsP1,P2,andP3.P1, thepointofintersectionofthemid-sagittallineandthecoronalline;P2, thereferencepointonthesplitscalptreatedwith12sessionsofthulium
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
laser;P3,thereferencepointonthesplitscalptreatedwith12sessionsof thuliumlaserand12-weekapplicationofsolution
SungBinCho
& Jin-SooKang 2 & HeesuKim 1
LasersinMedicalScience
LasersinMedicalScience
https://doi.org/10.1007/s10103-018-2437-5
https://doi.org/10.1007/s10103-018-2437-5
ORIGINALARTICLE
ORIGINALARTICLE
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
SungBinCho
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 &
Received:16April2017/Accepted:3January2018
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
# Springer-VerlagLondonLtd.,partofSpringerNature2018
Abstract
Abstract
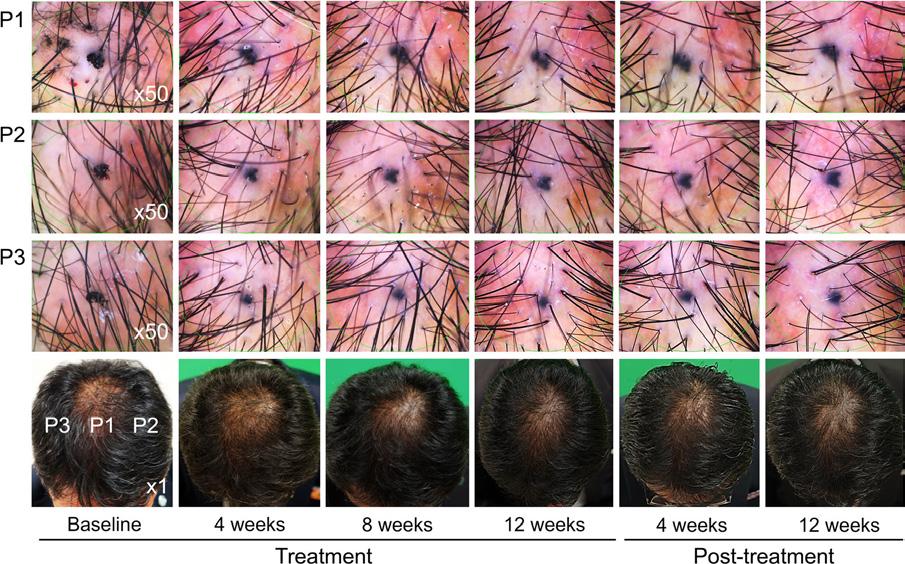
Fig.6 RepresentativedigitalimagesofhairsatpointsP1,P2,andP3.P1, thepointofintersectionofthemid-sagittallineandthecoronalline;P2, thereferencepointonthesplitscalptreatedwith12sessionsofthulium
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
laser;P3,thereferencepointonthesplitscalptreatedwith12sessionsof thuliumlaserand12-weekapplicationofsolution
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
treatmentandtime(P =0.006).Bonferroniposthocanalysis ofP1,P2,andP3,whichreflecteddifferenttreatmentsettings, revealedsignificantdifferencesinchangesfrombaselinebetweenP1andP2atthe8thweekoftreatment(P =0.013)and post-treatment4weeks(P =0.002),betweenP1andP3atthe
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
12thweekoftreatment(P =0.002),andbetweenP1andP2at the4th(P =0.031),8th(P =0.001),and12thweeks(P = 0.001)oftreatment.Meanwhile,themixedmodelanalysis ofhairthicknessexhibitedasignificanteffectfromtime (P <0.001),butnotindividualthetreatments(P >0.05).
Introduction
Introduction
Table2 Split-scalpcomparison of1927-nmfractionatedthulium laserwithorwithoutagenistein andgrowthfactor-containing solutionapplicationfortreating patternhairlossusinganadjusted baselinelinearmixedmodel
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
Hairnumbers
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
* HeesuKim yollikim@gmail.com
* HeesuKim yollikim@gmail.com
GroupTimeGroupxtime
4weeks13.314(4.129)7.159(3.077)16.827(4.915)0.005<0.0010.006 8weeks27.414(4.46)14.959(3.321)31.127(5.319)
12weeks31.414(5.137)30.259(3.822)49.427(6.144) 16weeks33.614(4.999)16.259(3.72)19.627(5.977) 24weeks24.914(7.01)10.059(5.208)19.527(8.42)
Hairthicknesses
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
4weeks0.008(0.002)0.009(0.001)0.009(0.002)NS<0.001NS
8weeks0.009(0.001)0.011(0.001)0.009(0.001)
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
12weeks0.012(0.001)0.012(0.001)0.013(0.002)
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
16weeks0.012(0.002)0.01(0.001)0.011(0.002)
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
24weeks0.013(0.002)0.009(0.002)0.011(0.003)
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
P1,thepointofintersectionofthemid-sagittallineandthecoronalline;P2,thereferencepointonthesplitscalp treatedwith12sessionsofthuliumlaser;P3,thereferencepointonthesplitscalptreatedwith12sessionsof thuliumlaserand12-weekapplicationofsolution
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
NS notsignificant
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
a Dataarepresentedasestimatedmean(standarderror)changesfrombaseline
HeesuKim 1
LasersinMedicalScience
LasersinMedicalScience
https://doi.org/10.1007/s10103-018-2437-5
https://doi.org/10.1007/s10103-018-2437-5
ORIGINALARTICLE
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
onpatternhairloss:anevaluator-blinded,split-scalpstudy
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
Abstract
Abstract
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
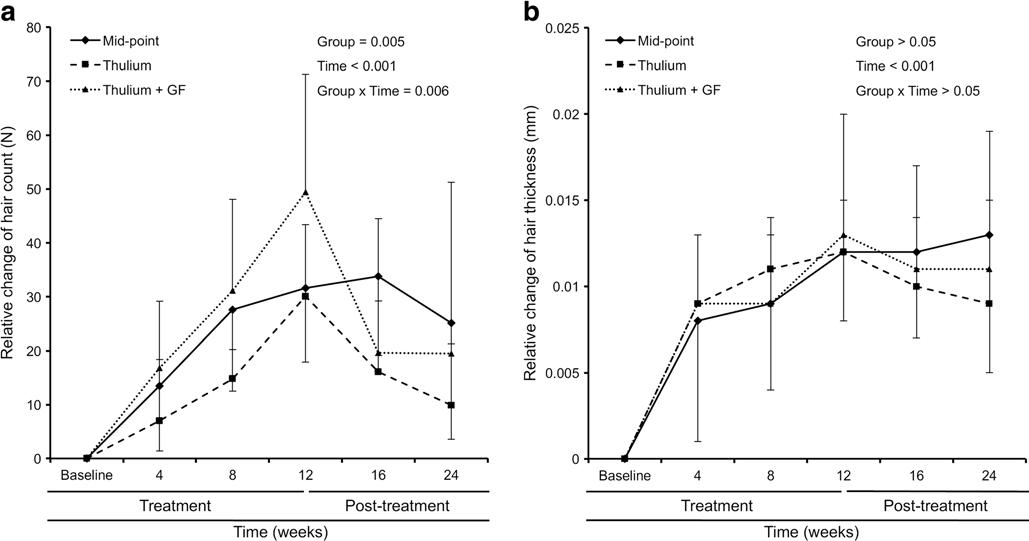
Fig.7 Split-scalpcomparisonanalysisusinganadjustedbaselinelinear mixedmodelprocedure.Relativechangesof a haircountand b hair thickness.Mid-point,thepointofintersectionofthemid-sagittalline andthecoronalline;thulium,splitscalptreatedwith12sessionsof
Adverseevents
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
thuliumlasertreatment;andthulium+GF,thereferencepointonthe splitscalptreatedwith12sessionsofthuliumlaserand12-weekGF solutionapplication
Discussion
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Introduction
Introduction
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
* HeesuKim yollikim@gmail.com
* HeesuKim yollikim@gmail.com
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
Inalloftheparticipants,post-thuliumlasertreatmentrednessinthescalpwasmildandtransient,withoutremarkabledifferencesattheP1,P2,andP3areas.Allpatients toleratedlasertreatment-associatedpainwell.Noneofthe 10patientsshoweddiseaseprogressionofPHL. Moreover,nosignificanttrichoschisisbylasertreatmentinducedphysicaldamagetoha irshafts,alopeciaareata, anageneffluvium,ortelogeneffluviumwasobservedover thecourseofthetreatmentandpost-treatmentfollow-up periodof3months.Milditchingsensationswerereported bythreepatientsthatspont aneouslydisappearedwithin 3days,andamildburningsensationwasrecordedfor onepatientthatspontaneouslyresolvedwithin1day. Amongthe10PHLpatients,sevenpatientspresented mildtomoderateseborrheicdermatitisatbaseline,althoughtheoverallseverityoftheseborrheicdermatitis lesionsimprovedinsix(85.7%)patients,particularly alongthescalphalftreatedwiththuliumlaserandaGF solution.Nopatientexperienceddevelopmentorprogressionofseborrheicdermatitisinthescalpupontreatment withthelaserdevice.Nootherpossiblesideeffects,includingbleeding,oozing,crusting,secondarybacterial, mycobacterial,viral,andfunga linfections,folliculitis,furuncles,carbuncles,andpost-therapyscarringwerereportedinall10PHLpatients.
Inapreviousstudy,ourstudygroupdemonstratedthatacombinationofthuliumlasertherapyandPDRNintraperifollicular injectionsremarkablyimprovedhairdensityanddiameterin PHLpatients[5].Comparedtoacombinationofmesotherapy andPDRNintraperifollicularinjections,whichelicitedincreasedhaircountsandthickness,thuliumlaserandPDRN intraperifollicularinjectiontreatmentprovidedmarkedly greaterefficacyinimprovinghairdiameter,butsimilarefficacyinhaircounts[5].Thesefindingsledustobelievethat similarorsuperioreffectsontheregenerationofhairfollicles couldbeobtainedwiththuliumlasertreatment,comparedto themesotherapy[5].However,thetherapeuticeffectsofa 1927-nmfractionatedthuliumlaseraloneonPHLhadnot beenreported.
Inthepresentstudy,wefoundthat12sessionsof1927-nm fractionatedthuliumlasermonotherapyonthescalpofPHL patientsat1-weekintervalsresultedinsignificantincreasesin hairdensityandthickness.Moreover,thepost-lasertreatment applicationofGFsolutiononthescalpprovidedadditional therapeuticefficacybyfurtherimprovinghairdensityand thickness.Overthecourseof3monthsafterfinishingtreatment,haircountsgraduallydecreased,althoughthey remainedremarkablyhigherinnumber,comparedtocounts atbaseline,particularlyattheintersectionpoint(P1)andatthe split-scalppoint(P3)treatedwithtopicalapplicationofaGF
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
LasersinMedicalScience
LasersinMedicalScience
https://doi.org/10.1007/s10103-018-2437-5
https://doi.org/10.1007/s10103-018-2437-5
ORIGINALARTICLE
ORIGINALARTICLE
solution.Overall,hairthicknessesalsograduallydecreased overthe3monthsaftertreatment.Accordingly,PHLmight resumeitsprogressionafterstoppingtreatment,particularlyat thinnerhairfollicles.Notwithstanding,thickenedhairfollicles seemedtobemaintainedalongthescalpforalongerduration thanthinnerfollicles.
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
Therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaser onpatternhairloss:anevaluator-blinded,split-scalpstudy
stimulatoryeffectsof1927-nmfractionatedthuliumlaserinducedphotothermolysisonthescalpandtheformationof effectiveroutesfortransdermaldrugdeliveryuponthulium lasertreatment.However,theresultsofthispilotinvestigation requirefurtherconfirmationinalargerpopulation.
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
Received:16April2017/Accepted:3January2018
Received:16April2017/Accepted:3January2018 # Springer-VerlagLondonLtd.,partofSpringerNature2018
# Springer-VerlagLondonLtd.,partofSpringerNature2018
Abstract
Abstract
Inthisstudy,thehistologicfeaturesof1927-nmfractionated thuliumlaser-inducedtissuereactionswereevaluatedusing invivoexperimentalhairlessmouseskin.Thelasersettings fortreatingPHLinthisstudywereapowerof5Wandan energyof4or6mJ,whichwefoundcouldgeneratenarrower degreesofepidermalcoagulationanddeeperLITCzonesinthe dermiswithoutdamagingthestructuralintegrityofappendages,comparedtotheotherexperimentalsettings.Atthenoted treatmentsetting,noremarkablephysicaldamagetothehair shaftswasfound.Nevertheless,accurateseparationofhair shaftsasshowninourpreviousreportandpropercouplingof thelasertipwiththescalpskinarerecommendedtoprevent unexpectedlasertreatment-induceddamagetohairshafts[5].
SungBinCho 1,2 & BoncheolLeoGoo 3 & ZhenlongZheng 4,5 & KwangHoYoo 1 & Jin-SooKang 2 & HeesuKim 1
Acknowledgements WewouldliketothankHyeSunLee,PhD (DepartmentofBiostatistics,YonseiUniversityCollegeofMedicine, Seoul,Korea)forherhelpwiththestatisticalanalysesandAnthony ThomasMilliken,ELS,atEditingSynthase(https://editingsynthase.com) forhishelpwiththeeditingofthismanuscript.Wealsowouldliketothank HeeJunShin(LutronicCorp.,Goyang,Korea)forhisassistancein technicalsupport.
Compliancewithethicalstandards Allauthorswerewellinformedofthe WMADeclarationofHelsinki(EthicalPrinciplesforMedicalResearch InvolvingHumanSubjects)andconfirmedthatthepresentstudyfirmly fulfilledthedeclaration.
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Conflictofinterest Theauthorsdeclarethattheyhavenoconflictof interest.
References
1.YooKH,KimMN,KimBJ,KimCW(2010)Treatmentofalopecia areatawithfractionalphotothermolysislaser.IntJDermatol49: 845–847
Laser-orlight-assistedtherapieshavebeenusedtoimprovetheperifollicularenvironmentbyupregulatingtheexpressionof growthfactorsandsignalingmoleculesforhairrestoration.Theaimofourstudywastopreclinicallyandclinicallyevaluatethe therapeuticefficacyandsafetyofa1927-nmfractionatedthuliumlaseronpatternhairloss(PHL).Aninvivohairlessmouse studyandaninvivohumanskinenvironmentalscanningelectronmicroscopy(ESEM)studywereperformedwithdifferent powerandenergysettings.Thereafter,anevaluator-blinded,split-scalpstudywasconductedtoevaluatehairthicknessand densityin10PHLpatientstreatedwith12sessionsoffractionatedthuliumlasertreatmentwithorwithoutpost-lasertreatment applicationofagrowthfactor-containing(GF)solution.Ininvivohairlessmouseskin,invertedcone-shapedzonesofthulium laser-inducedtissuecoagulation(LITC)werenotedimmediatelyaftertreatmentintheepidermisanduppertomid-dermis withoutremarkableablativetissueinjury.TheESEMstudyrevealedroundtooval-shapedzonesofnon-ablativeLITConthe surfaceofthestratumcorneumofahumansubjectimmediatelyafterlaserirradiation.InPHLpatients,12sessionsofthulium lasermonotherapyat1-weekintervalsresultedinsignificantlyincreasedhairdensityandthickness.Post-lasertreatmentapplicationofGFsolutionofferedadditionaltherapeuticefficacybyimprovinghairdensityandthicknessonthesplitscalp.Theuseof afractionatedthuliumlaserwithorwithoutpost-lasertherapyapplicationofGFsolutiontotreatPHLelicitedremarkable improvementsinhairthicknessandhaircounts.
Introduction
Introduction
Theprecisemechanismsofthuliumlaser-inducedfollicular regenerationhavenotbeenfullyinvestigated.Nonetheless, photothermalstimulationbythuliumlasertreatmentcould havewokendormanthairfollicles,aswasobservedfortreatmentofPHLwithplatelet-richplasma[10].Furthermore,repetitivepower-andenergy-regulatedwoundingcouldhave sufficientlystimulatedWnt-dependenthairfollicleneogenesis fromepithelialcells[11].Also,onestudyhasshownthathair folliclestemcellsinminiaturizedhairfolliclesareeliminated throughtheepidermisuponproteolysisoftypeXVIIcollagen (COL17A1/BP180)[ 12 ].Duringtheprocessof transepidermalelimination,hairfolliclestemcellsexhibiting COL17A1proteolysislosestemnesssignaturesandterminally differentiateintoepidermalkeratinocytes[12].Accordingly, theseepidermalkeratinocytes,whichhavedifferentiatedfrom hairfolliclestemcells,couldbesuggestedasanimportant targetofthuliumlasertreatment.
2.LeeGY,LeeSJ,KimWS(2011)Theeffectofa1550nmfractional erbium-glasslaserinfemalepatternhairloss.JEurAcadDermatol Venereol25:1450–1454
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Keywords Patternhairloss Thuliumlaser Splitscalp Growthfactor Transdermaldrugdelivery
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
Deliveryoflaserorlightenergytothescalphasbeenusedas alternativeoradditionaltreatmentmodalitiesintreating
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
* HeesuKim yollikim@gmail.com
* HeesuKim yollikim@gmail.com
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
1 DepartmentofDermatologyandCutaneousBiologyResearch Center,InternationalSt.Mary’sHospital,CatholicKwandong UniversityCollegeofMedicine,Simgokro100gil25Seo-gu, Incheon22711,RepublicofKorea
OnESEMimagesobtainedimmediatelyafter1927-nm fractionatedthuliumlasertreatmentoninvivohumanback skin,wediscoveredroundtooval-shapednon-ablativezones ofLITCalongthesurfaceofthestratumcorneumwithnumeroussmallheterogeneousroundholes.Meanwhile,postlasertreatmentapplicationofaGFsolutioneffectivelyenhancedtheclinicalefficacyofthethuliumlasertherapy. Accordingly,wesuggestthatthethuliumlasercouldhave formedeffectiveandsaferoutesfortransdermaldrugdelivery tothescalp.
SungBinChoandBoncheolLeoGooequallycontributedtothiswork.
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
2 KangskinDermatologyClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
3 NaeumDermatologyandAestheticClinic,Seoul,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
4 CutaneousBiologyResearchCenter,InternationalSt.Mary’s Hospital,CatholicKwandongUniversityCollegeofMedicine, Incheon,RepublicofKorea
3.KimWS,LeeHI,LeeJWetal(2011)Fractionalphotothermolysis lasertreatmentofmalepatternhairloss.DermatolSurg37:41–51
4.ChoS,ChoiMJ,ZhengZ,GooB,KimDY,ChoSB(2013)Clinical effectsofnon-ablativeandablativefractionallasersonvarioushair disorders:acaseseriesof17patients.JCosmetLaserTher15:74–79
Inconclusion,ourdatademonstratedthatthuliumlaser monotherapyeffectivelyimprovedhaircountsandthickness inPHLpatientswithoutremarkableadverseevents. Furthermore,betterclinicalimprovementinhairdensityand diameterwasachievedbyapplyingaGFsolution.Wesuggest thattheactionmechanismscouldbeassociatedwithboththe
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
5 DepartmentofDermatology,YanbianUniversityHospital, Yanji,China
5.ChoSB,ZhengZ,KangJS,KimH(2016)Therapeuticefficacyof 1,927-nmfractionatedthuliumlaserenergyand polydeoxyribonucleotideonpatternhairloss.MedLaser5:22–28
6.ByunJW,MoonJH,BangCY,ShinJ,ChoiGS(2015) Effectivenessof308-nmexcimerlasertherapyintreatingalopecia areata,determinedbyexaminingthetreatedsidesofselectedalopecicpatches.Dermatology231:70–76
7.SemaltyM,SemaltyA,JoshiGP,RawatMS(2011)Hairgrowth andrejuvenation:anoverview.JDermatologTreat22:123–132
8.StewartN,LimAC,LowePM,GoodmanG(2013)Lasersand laser-likedevices:partone.AustralasJDermatol54:173–183
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
9.LeeSH,ZhengZ,KangJS,KimDY,OhSH,ChoSB(2015) Therapeuticefficacyofautologousplatelet-richplasmaand polydeoxyribonucleotideonfemalepatternhairloss.Wound RepairRegen23:30–36
patternhairloss(PHL),alopeciaareata,andscarringalopecia [1–6].Presentlyavailabledevicesforthesepurposesinclude low-levellightdevices,308-nmexcimerlasers,1540-or 1550-nmerbium/glassfractionatedlasers,10,600-nmcarbon dioxidefractionatedlasers,and1927-nmfractionatedthulium lasers[1–6].Althoughthepreciseactionmechanismsthereof haveyettobethoroughlyinvestigated,laser/light-assistedhair restorationtherapyhasbeenfoundtoinduceproliferation/ differentiationofprogenitorcellsinfollicularunits,toimproveperifollicularenvironmentalfactors,particularlyvascularcomponents,andtoincreasetheexpressionofgrowthfactorsandsignalingmolecules[2–4, 6, 7].
10.MiaoY,SunYB,SunXJ,DuBJ,JiangJD,HuZQ(2013) Promotionaleffectofplatelet-richplasmaonhairfolliclereconstitutioninvivo.DermatolSurg39:1868–1876
11.ItoM,YangZ,AndlTetal(2007)Wnt-dependentdenovohair follicleregenerationinadultmouseskinafterwounding.Nature 447:316–320
12.MatsumuraH,MohriY,BinhNTetal(2016)Hairfollicleagingis drivenbytransepidermaleliminationofstemcellsviaCOL17A1 proteolysis.Science351:aad4395 LasersMedSci
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
Thuliumlaserenergyatawavelengthof1927nmisbetter absorbedbywaterthanerbium/glasslaserenergyat1540or 1550nm,althoughnotquiteaswellascarbondioxidelaser energyat10,600nm[8].Thus,bycontrollingthepowerand energysettingsofthethuliumlaser,thedepth,width,and degreeoflaser-skintissueinteractioncanbeaccuratelyregulatedwithoutgeneratingexcessivethermalinjurytosurroundingtissue:carbondioxidelasers,althoughbetterabsorbedby
Healite II


Achieve Optimal Hair Health by integrating Kerafactor Serum with Healite
II Low Level Light Therapy
Combining KeraFactor with Lutronic Healite II offers a cutting-edge solution for hair restoration, ensuring superior patient outcomes through the synergy of growth factors and light therapy.
• 830/590, 633 & 415nm phototherapy system
• Photo-sequencing technology
• Proprietary OLAT technology for deeper more intensive treatments
• Treat more than 20 indications
• Clinically backed and efficacious
• Zero consumablesno added running costs
• Outstanding return on your investment

830 nm with 590 nm Indicated for Wound Healing, Pain Reduction and Skin Rejuvenation.



633 nm* Indicated for Post Care, Skin Rejuvenation, Collagen Stimulation and Hair Rejuvenation. 415 nm* Indicated for Acne. *Only available with combo model
Advanced Thulium Laser
A superior fractional, non-ablative 1927nm laser for advanced skin resurfacing. Effective technology that provides consistent and reproducible results for glowing, healthy and elastic skin without any costly or unnecessary consumables. The world’s most advanced Thulium Laser now with treatments to support scalp health.
Intuitive
• Easy-to-navigate display provides valuable feedback with selectable coverage rate, total energy delivered per treatment session, density and interval options.
Effective
• LaseMD ULTRA™ is the only device available in the market that can deliver a maximum power of 20 W with a Top-Hat beam profile for the fastest and most incomparably consistent treatments possible. LaseMD ULTRA™ increases permeability with minimal thermal disruption of the stratum corneum.
Dependable
• LaseMD ULTRA™ rebuilds glowing, healthy and skin through gentle, non-ablative fractionated treatments with minimal cost of ownership and no shot limit per procedure.
Innovative
• Fastest resurfacing treatment solution with bigger beam diameter (200 µm and 350 µm) and scan size (4 by 10 and 6 by 10). Tunable from mild to aggressive treatment provides customized outcomes.
Provide Results Your Patients Demand
Full range of applications
• Actinic Keratosis
• Benign Pigmented Lesions
• Melasma
• Lentigines
• Freckles
• Café au Lait Macules



Rejuvenation & Pigmentation
Courtesy of W. Loverme, MD, USA



Rejuvenation & Pigmentation
W. Loverme, MD, USA


Decollete Rejuvenation & Pigmentation
Courtesy of W. Loverme, MD, USA




USA

LaseMD Ampoule Series
A premium skincare solution crafted with no more than 8 pure ingredients, each formulated to target specific skin concerns. Designed to work independently, or with the LaseMD ULTRA device for optimal absorption.


LaseMD ULTRA™ is my favourite new addition to my practice. It allows me to treat multiple areas quickly, effectively, and for very low cost. My patients are loving the comfortable treatments and impressive results with very little downtime.
– Dr. Joel Cohen, MD
Courtesy of
Hair Loss
Courtesy of W. Loverme, MD,
Square Tip
Comb Tip C5 Tip Roller Tip
Both Cynosure and Lutronic have long been at the forefront of innovation in the aesthetics industry. Founded in 1991, Cynosure revolutionised the field with its cutting-edge energy-based device technologies. Lutronic, established in 1997, quickly became a leader in medical aesthetics. Together, these two category leaders bring together over 50 years of industry experience, a wealth of expertise, creating a powerful synergy that continues to push the boundaries of aesthetic innovation and clinical results.
Cryomed Aesthetics is proud to be the exclusive distributor of the Cynosure Lutronic portfolio across Australia and New Zealand. Our commitment to providing the highest quality equipment is rooted in our core principles: better technology, better service and better value, to ultimately better lives. At Cryomed, we understand the needs of the aesthetic and medical communities and are driven to ensure our partners have access to the best technologies to deliver safe, effective, and cutting-edge treatments to their patients. Based in Sydney with offices in Melbourne, Brisbane, Perth and Auckland, the success and strength of Cryomed is derived from its dynamic and diverse team of expert industry professionals with extensive experience in the medical, cosmetic and aesthetics fields. We are a major technology partner with many of Australia’s and New Zealand’s most successful medical-aesthetic groups. We understand the needs of aesthetic businesses from small, to medium and large-scale, as well as the importance of delivering exceptional return on your investment.

©2025 Cynosure, LLC. ©2025 Lutronic Corporation. All rights reserved. The information in this booklet is compiled for medical professionals for educational and informational purposes only. All opinions, experiences, and views expressed (including, but not limited to, the use of Cynosure Lutronic products, Cynosure products, and Lutronic products) belong solely to the authors. Cynosure Lutronic does not endorse or approve, and assumes no responsibility for the content, accuracy, or completeness of the information included herein.
cynosurelutronicanz.com cynosurelutronicanz info@cryomed.com.au