As for many , 2023 was a year with mainly financial challenges for Brussels IVF too. Especially due to rising salary costs and increasing costs for energy and consumables, most Belgian hospitals suffered important financial losses. So did ours. Fortunately, our activities held up well with a new record of over 5,700 oocyte pick-ups and over 5,000 frozen embryo transfers performed in 2023. Consequently, our figures were still written in black. But with more than 200 employees needed for supporting a very labour-intensive treatment process, we too bear a very heavy labour cost. Furthermore, our suppliers of consumables do not shy away from making 2-digit price corrections, whether justified or not. We therefore need to keep a close eye on the price loyalty of our suppliers in the future in the best interest of our patients.
Fortunately, all these financial woes did not affect the quality of our services. The latest BELRAP report proves this: the probability of and delivery in the reference group was 42.1% versus an average of 31.8% for the 17 other verified Belgian IVF-centres.
What does have an impact on these numbers is our underperformance towards pregnancy follow-up with an important backlog in follow-up of deliveries after frozen embryo transfers. Since we apply a freeze-all policy in 1 out of 3 treatment cycles, and while our results after vitrification do not differ from fresh embryo transfers, our cumulative statistics do not, to this date, reflect correctly our hard work. Although probably the price to be paid being one of the biggest centres in Europe, we need to change and adjust our follow-up data from patients giving birth in other hospitals, cities and countries.
Extra efforts are also needed towards our patients as we witness a quiet transition from Gen-Z to Zoomer. No, nothing to do with a digital meeting platform, just a neologistic contraction of Gen-Z and Boomer. Our new patients are tech-savvy and they have grown up with apps and social media. They swipe, tap and scroll through life. Our revamped website BrusselsIVF. be is already responding to this as it has a “funneled” design. In layman language: in max. 3 taps you get from the landing page to the information you are looking for.
But unlike what their online behaviour would suggest they are also rewriting the code; Zoomers turn out to be very individualistic too. They aspire to take control of their own life, they are open to change and very open-minded, they take diversity for granted, yet they value personal and authentic interactions.
Therefore, our ongoing policy plan “Moving ForwART” aims to
provide an holistic approach to health care. In doing so, we must strive to maximally involve our patients to guide their informed choices instead of making choices for them.
Not easy, because while doing so, we must also take into account a third, yet unknown stakeholder: the child-to-be. And this third stakeholder is entitled to the ‘reasonable welfare principle’: the future child must be given the opportunity to develop normal human interests and achieve life goals, which are widely regarded as goals that make human life worth living.
A challenging task and responsibility not to be taken lightly as our dilemma is best summerised as, “everyone has the right to desire having a child, but no one has the right to a child”.
This annual report, therefore includes a reflection on our socio-ethical framework where we try at our best to reconcile the wants and needs of all present and future stakeholders involved.
For Brussels IVF, 2023 was an eventful year, as almost every year. Yet, despite all our activities and renovations, the inventiveness and flexibility of our employees remains unwavering.
You can count on us: in 2024 we will go the extra mile, as we do every year!
With many thanks for your trust in our team and with warm regards,
Preface
Prof. dr. Herman Tournaye Medical & Scientific Director
The collaboration between Brussels IVF and the Centre of Medical Genetics of UZ Brussel (CMG) can be considered one of Europe’s excellence programmes in embryo testing.
Couples who are carriers of an inherited disorder and have a desire to have children of their own, can seek treatment with preimplantation genetic testing, or PGT, at UZ Brussel.
PGT means that embryos, obtained through in vitro fertilisation (IVF), are first genetically tested to see whether or not they carry the hereditary disorder Only after genetic analysis is the embryo transferred back into the uterus to obtain a healthy pregnancy.
The PGT pathway is possible thanks to close cooperation between Brussels IVF and the Centre for Medical Genetics (CMG) at UZ Brussel. The couple is followed up by a fertility doctor and a doctor-geneticist together with specialised midwives who coordinate the PGT pathway.
The PGT team has set clear goals and focus points such as closer contact with referral doctors and transparent communication with (potential) patients: a PGT webinar is foreseen in the future, updated brochure, online presence,....
Within Brussels IVF, prof. dr. Mackens and dr. Roelens are the expert doctors specialising in PGT.
The geneticists specialising in PGT are Prof. dr. Keymolen and Dr. Pölsler.
dr. Caroline Roelens
prof. dr. Shari Mackens
prof. dr. Kathelijn Keymolen
dr. Laura Pölsler
Helena Deryckere
Pascale De Becker
Katrien De Rooms
Martine De Rycke
Pieter Verdyck
Meet the team
Elia Fernandez Gallardo
Veerle Berckmoes
Yves Vandeskelde
Kim De Hauwere
Rani Cooreman
Marleen Carle
Christiane Winter
Julie Nekkebroeck
Yanissa Van Buggenhout
Anick De Vos
Kiani Collier
Anne-Marie Dekens
Annelies Callens
Inez Bogaerts
Debby Van Boxstael
Febe Lambeets
Prof. dr. Shari Mackens PGT-A
FOCUS ON Our socio-ethical framework
ETHICAL RESPONSIBILITY AND CARE FOR THE CHILD’S WELLBEING
About 16% of people with an active desire to have children struggle with fertility issues. It is a known fact that the absence of pregnancy as well as the transition to parenthood has a major psychological impact.
As health workers and psychologists in the field of reproductive medicine we face a context of what increasingly looks like a ‘makeable world’. As fertility psychologists, we try to navigate between a legal framework, our clinic’s own ethical framework and the requests of prospective parents. New fertility treatments and their applications are strongly linked to the evolving social context in which an increasing number of people are postponing parenthood and the diversity of family forms is increasing. Traditional heterosexual, single and lesbian couples make up only part of our patient population. Consider fertility preservation for medical and non-medical reasons, co-parenting, surrogacy, ... .
Fertility problems are not to be considered purely a medical problem, but have long been approached from a biopsychosocial model, with specific attention to the wellbeing of the prospective parent(s) as well as the future child. In this field of medicine we are shifting from a cure model to a care model.
Switching between medical, psychological, psychotherapeutic, psychiatric, social, legal, anthropological, ethical themes and knowledge is a must and makes the fertility psychologist a true ‘psy-cialist’ in a multidisciplinary environment. In this contribution, we offer a glimpse into our daily practice as fertility psychologists at Brussels IVF, the reproductive medicine centre of UZ Brussel, where support, counselling and screening of patients are at the core.
Currently, Brussels IVF’s multidisciplinary team includes six psychologists. Their activities mainly consist of assessing access to treatment and providing psychological support.
DEVELOPING A SOCIO-ETHICAL FRAMEWORK
Amid the broad clinical treatment domain of reproductive medicine, the proliferation of reproductive options and the vagueness and limitations of legislation, fertility clinics need to develop their own ethical framework and draw up their own guidelines. In developing the procedure for screening requests for treatment at Brussels IVF, we have relied on a number of principles.
• First, there is the Law on Medically Assisted Reproduction, which states that “fertility centres shall ensure great transparency of their options regarding the accessibility of treatment; they may invoke the conscience clause with regard to requests addressed to them” (Kamer van Volksvertegenwoordigers, 2007, Art. 5). This implies that fertility centres can autonomously decide which treatments to offer or not and are never obliged to carry out any treatment. This implies that the team should develop an ethical charter with criteria on the basis of which decisions are made to treat or not to treat patients.
• Second is medical deontology, where the principles of ‘do no harm’ and ‘be careful’ before ‘treating’ apply.
• Furthermore, the Convention on the Rights of the Child (1989) contains a number of important principles that state that every child has the right to be brought up in the best possible conditions. Thus, parents have primary responsibility for the child’s upbringing and development. The best interests of the child are their paramount concern (Art. 18.1). The child has the right to the enjoyment of the highest possible degree of health (Art. 24.1). And every child has the right to a standard of living adequate for his/her physical, mental, moral and social development (Art. 27.1).
• The ‘principle of the welfare of the child’ has been described by Pennings, among others (Pennings, 1999; Pennings et al., 2007). We have a responsibility towards the children born with our help. Pennings developed the principle of ‘reasonable wellbeing’, which implies that the child should have the opportunity to achieve life goals that are generally considered meaningful to human life.
• Finally, many publications screened for risk factors (and protective factors) in a child’s development, such as the socio-economic level of the parent(s), the presence of psychiatric disorders in the parent(s), the use of psychopharmaceuticals, the presence of a social network around the parent(s), and so on. Not only the welfare of the future child but also that of the prospective parent(s) is important. Knowledge of vulnerabilities in prospective parents is important because they are the best predictor of maladaptive coping strategies during a fertility journey. For instance, a history of depression significantly increases the likelihood of decompensation during fertility treatment. Stress levels during a fertility trajectory are similar to these in cancer patients. Advice from GP’s and other treating specialists who know the patient, are important tools for arriving at an assessment of well-being and coping capacity. We therefore ask patients to provide us with reports from these colleagues. This also creates the possibility of timely deployment of necessary psychological support.
• Good medical practice respects and evaluates the cost-investment ratio in relation to the success rate. In Belgium, social security reimburses a fixed number of fertility treatments, such as inseminations and IVF, up to a certain age limit. The reimbursement scheme is mainly based on success rates. The chance of becoming pregnant after the age of 43 (the age limit for reimbursement) using IVF is below 5%. Even if someone is willing to pay for the entire treatment on their own afterwards, the reasonableness of the treatment should be questioned.
At Brussels IVF we are convinced that we have a duty to run a clinic where not only ethical and moral principles apply, but where, above all, we work with a long-term vision: in addition to the desire of one or more adults to have children, there is a responsibility to consider the possible impact of our interventions on the well-being of children who would not be born without our intervention. We therefore consider it important to identify the risk and protective factors that may affect the well-being of future children and intended parents, and to act accordingly.
The clinic team has therefore created a quality manual with an ethical charter. This describes all care procedures, specified by type of treatment or request, with inclusion and exclusion criteria. It includes eligibility requirements for treatment and what absolute contraindications are. They also include when patients should be referred to the psychologist. The manual is a dynamic tool that is regularly updated in response to new technical possibilities, legal changes and societal developments. Its contents have been
shared with other fertility centres at home and abroad and have been adopted by a large number of colleagues or have served as a basis for developing their own policies.
MULTIDISCIPLINARY SOCIO-ETHICAL REVIEW BOARD
The team’s work is overseen by an ad hoc socio-ethical review board. This working group consists of members from Brussels IVF and the Centre for Medical Genetics. Here, department heads, psychologists, doctors, the care manager, embryologists, a psychiatrist, an ethicist, a lawyer specialising in family law and an obstetrician discuss twenty to thirty cases each month about which there are questions or concerns. After multidisciplinary discussion, the board is able to issue a binding recommendation (positive|pending|negative). In the context of transparency, the psychologist always communicates the individual recommendation, verbally or by phone, to the patient, including the reason(s) in case of a negative outcome. A written confirmation of the final recommendation is provided as well.
Brussels IVF psychologists
Eveline Buyse Lize Leunens Julie Nekkebroeck
Rani Cooreman Eline Devriese Jasmijn Van De Putte
FOCUS ON Holistic care: FerMet programme
FerMet fertilty and metabolism
FerMet is a cooperation between the experts of Clinical Nutrition and fertility experts of Brussels IVF that benefits prospective parents in their journey towards parenthood. FerMet combines cutting-edge science with compassionate care to help achieve the dream of conceiving and delivering a healthy baby.
How did the FerMet project come to life?
A balanced diet can have a big impact on a patient’s healing process. My experience in the intensive care unit and research on patients with a long-term illness, such as people with a cancer diagnosis, show that a well-planned nutritional policy can support the medical protocol and thus the healing. In general, we see a shift from curative medicine to preventive medicine. Obviously, prevention is better than having to cure or repair. In different areas of physical, but mental health as well, we see that ‘lifestyle’ is also an influential factor. This includes sufficient physical activity, but also sufficient relaxation, a good sleep pattern and a healthy, balanced, diet. Coincidentally, my husband is a gynaecologist and fertility expert and so the curiosity and opportunity to collaborate on this topic surfaced.
What are the advantages for a fertility patient to be counselled by a clinical nutritionist/dietitian during or before fertility treatment?
The causes of infertility can be diverse and sometimes, however difficult for the patient itself, can remain idiopathic.
Body composition or lifestyle can also contribute to a reduced fertility or sometimes even show a causal correlation. For example, being underweight can cause hormonal disruption or amenorrhea which leads to a disturbance of the menstrual cycle, which is detrimental to a woman trying to conceive.
By providing professional guidance on lifestyle and food intake, we can support prospective parents, both women and men, to achieve a healthy body weight but especially a healthy body composition.
In some cases, as is very evident for severely underweight women with amenorrhea, this can even have a beneficial impact on the chances of obtaining a pregnancy.
Interview with Prof. dr. Elisabeth De Waele
Head of the Department of Clinical Nutrition at UZ Brussel Medical Director of the Intensive Care Department and Associate Professor at VUB and Erasmus Hogeschool Brussel.
Since 2018 she is Member of the Executive Board of the European Society for Clinical Nutrition and Metabolism.
She graduated from Vrije Universiteit Brussel in 2004, completed postgraduate training in general surgery in 2010 and became a certified Intensive Care Physician in 2012. In 2008 she obtained a Bachelor diploma in Clinical Nutrition (Odisee Graduate School).
Above all, we strive to ensure that if a pregnancy is obtained, it can proceed optimally and is less likely to develop complications during pregnancy (e.g. gestational diabetes or gestational hypertension) or complications during childbirth.
This care pathway is in line with the vision of Brussels IVF, which looks beyond obtaining a pregnancy and strives for a healthy baby and a healthy parent.
Is this lifestyle coaching to support medical treatment a new initiative?
The concept in medicine is not new, as many international studies proceed us and confirm; working to address the cause of a situation is more valuable for the patient, and for society, than just treating the consequences.
In the past, it was often identified that a certain BMI score could have a negative impact and the patient was told to make a change. However, it is about more than just a number. As a healthcare provider, you can look further by mapping lifestyle, drawing up a physical activity profile and discovering eating patterns together. This can help the patient to consciously break patterns and, much more importantly, install new, achievable and healthier patterns. More than the weight, the patient’s body composition is of importance. The core of our practice is looking at the patient’s individual body composition and thus individual nutritional needs and requirements. In health care, this has been applied for some time now for kidney patients and patients admitted
to intensive care, for instance. At UZ Brussel, since March 2021, we also apply this for fertility patients at Brussels IVF.
What is your experience in the FerMet programme working with fertility patients?
The FerMet programme can be very valuable for this population since they already have to give up a lot of ‘control’ during a fertility treatment. As prospective parents are to follow the rhythm of the woman’s body and menstrual cycle, working on a healthier diet and lifestyle can – besides the primary effect of improving general health and chances of a healthy pregnancy, have the potential secondary effect of giving back a piece of ‘control’ to this prospective parent.
What are the most important pointers for prospective parents to consider?
Eating habits: balance and regularity
We often see elevated avoidance of carbs and an increase in protein intake (lots of protein shakes, Skyr, protein bars, ...). There is also a strong belief that carbs such as pasta and bread should be avoided at all costs.
But, in fact, there is a need for balance and regularity. We often detect a food intake that is not qualitatively balanced. This while balance between fats, carbs and proteins is crucial for optimal health. Further it is important that there is regularity in the dietary habits, this consists of 3 main meals and 2-3 snacks.
Quantity
The second pillar is that many people struggle with determining or sensing how much food a body needs. A balanced body is one that can absorb what it needs to function. Food has become part of our culture. It is not evident sometimes to listen to our body when it comes to feelings like ‘hunger’ and ‘satiety’. The intention of our programme is not to achieve a temporary result quickly. In the context of a family, we want to work sustainably around lifestyle (nutrition and physical activity) with long-term prospectives.
What results have been obtained since the FerMet programme was launched?
We see very good results for pregnancy rates linked to underweight. Successful pregnancies have already been observed after obtaining a correct body composition. There are women who may have a low BMI, but who are healthy and have a balanced body composition. We see that the menstrual cycle is functioning better again. They respond better to the stimulation medication and show fewer complications.
In the case of overweight, the evaluation is a little more complex. Often, we see an unbalanced diet. Women who are overweight or obese often face a stigma and sometimes try to overcompensate because of the focus on weight and BMI. They think that they need to eat very limited meals to lose proper weight very fast, because of the desire to have children. But in fact, they eat so few calories that we see
the inverse effect, they gain weight (starvation mode). We use two methods to determine the calorie needs for each patient. The first method is the Indirect Calorimetry, which gives us the REE (Resting Expenditure Energy). The second method is the BIVA (Bio -Electrical Impedance Analysis) to determine the body composition.
It is as research with oncology patients had shown us: a more balanced body is prone to less unplanned hospitalisation and suffers fewer side effects of the treatment. The body is better armed to face challenges. We work on the body’s resilience with a balanced diet just like a psychologist works on your mental resilience. The doctor and dietician guide you to a stronger more resilient body to give primary therapy, e.g. IVF, every chance.
Meet the team
The team consists of three dieticians and two doctors who also look at endocrinological aspects. We have a weekly monitoring meeting to go over every patient with our team.
Numbers over the years
Since the start of the project until June 2023, 921 patients started at FerMet. Of all patients referred to the FerMet project from Brussels IVF, almost 90% start a trajectory of nutritional counselling. In total, we did 2951 consultations with our team.
As you can see in the graphic below, we did 930 consultations in 2021, in 2022 it was 1364 and in 2023 until June 657 consultations at FerMet.
l.t.r.: Lieselot Sablon, Magalie Vanmeerbeek & Femke Van De Velde
FOCUS ON Patient’s perspective
Falke (31) and Lies (34), Ghent region, wanted to grow their family and turned to Brussels IVF to help them achieve their dream.
Their story: www.instagram.com/hetavontuurvanbabybalou/
How did you end up at Brussels IVF and what was your first impression?
Lies: After trying to get pregnant for some time, we had additional tests done through our GP and my gynaecologist. On Friday evening, the 24th of November 2022, the results came in through the online patient platform, Cozo. There it was, in writing: SMI 0,66% dead.
We couldn’t reach our GP or gynaecologist at that time for further interpretation because it was a Friday evening. We fell into each other’s arms, crying, helpless and clueless of the road ahead.
Falke: On Monday, we were able to reach the doctor and were referred to a nearby university hospital. We felt hopeful. But because Lies, at a younger age, had donated eggs at UZ Brussel,
INTERVIEW
Lies (34) & Falke (31)
she wanted to be treated there. As she knew her way around, she felt comfortable. We also knew that people from all over the world come to Jette to get help when it comes to fertility, so UZ Brussel was our first choice of hospital.
On the 5th of January, the moment arrived and we had our first consultation with a fertility specialist. As I walked out of the elevator and around the corner into the waiting room, the feeling immediately overwhelmed me; “we are not alone”. The crowded waiting room felt very much in contrast to the vast taboo surrounding infertility and the feeling that it is something you face alone as a couple.
Lies: Moments later, we were welcomed by our treating physician, Dr. Uvin, who came across as very friendly and transparent as she went straight to the facts based on the
results of our tests: ICSI. It was a relief that we could get started right away and that ‘our family’ was one step closer. Or at least the road towards it. Talking and comparing to other couples in our network, we were under the impression that you get a more extensive examination at Brussels IVF, which also reassured us.
So you started the treatment plan after counselling, how did you experience the medical part?
Lies: I knew how an oocyte retrieval worked because I had donated eggs before. On that front, everything went smoothly. The stimulation phase to grow my follicles was shorter than was the case for my retrieval as a donor. The discomfort of the medication was also less and the recovery went smoother. I remember during my last retrieval that the nurses in the operating theatre were discussing women’s undergarments and there were many jokes made on the topic, which made the atmosphere very pleasant and relaxed. I could easily join in and laugh along: the best pick-up ever!
Falke, on the other hand, was suffering from performance pressure quite a bit. We often joke that the man shouldn’t complain about an IVF procedure, but the confrontation with a sterile cubicle is anything but pleasant. Thankfully a second sample was unnecessary that day!
Falke: I remember 22 eggs were retrieved, 21 were fertilised and 7 embryos evolved until day 5 and were frozen. We know, also from talking to other couples, that these are very good numbers -although emotionally it still feels like an elimination race.
In May 2023, our first transfer was a fact. The 12 days of waiting that followed were incredibly stressful.
Lies: He constantly asked me if I felt anything. I had felt some cramping on day 5 after the transfer so we were hopeful for implantation. Full of excitement, we took a pregnancy test on day 11 at home. Tears of happiness because it was positive. But we still felt very uncertain because we didn’t know whether the hormones we had to administer could have affected the test.
The following day, we were allowed to have a blood test at the hospital and unfortunately we got a disappointing phone call after. The hcg hormone was indeed slightly elevated, which explained the positive test. But the pregnancy had not progressed further.
Falke: After two embryo transfers, we had another appointment with our treating doctor. There, we were immediately given a clear and straightforward explanation.
Based on our patient file and the known results, they expected that a pregnancy should be possible within 3 transfers. If this was not the case, further examinations would be scheduled. The additional tests were planned immediately. If we did get pregnant from the third transfer, we could still cancel all the appointments.
We felt like we had gained some time through efficient planning and that felt very good. That is one of the aspects for which we are very grateful: that there is such forward thinking at Brussels IVF.
Lies: Unfortunately, we were not pregnant after transfer number 3. Further investigations followed: a biopsy of my uterus and an extra blood test. This led to a breast examination, referral to the rheumatologist and 2 courses of antibiotics. After 4 months, we could finally get back to our treatment plan and the next transfer. This was an embryo transfer in my natural cycle. Hallelujah, because administering those hormones was not fun for me at all.
Falke: It was only after 5 transfers that we finally got the long-awaited phone call that we were pregnant. We were full of disbelief, even though Lies’s menstruation remained absent. Because somehow you hardly dare to hold out hope. We cried, and cried some more. But this time they were tears of happiness. Even after a positive test, we were closely monitored every week, which felt really good. A piece of your carelessness is stolen by an IVF treatment. Follow-up is a reassurance we really needed to have the courage to believe it was really happening for us.
Did you make use of any of the extra support or services offered at Brussels IVF (webinars, psychological counseling, nutritional advice, clinical studies, blood tests or ultrasound closer to home,...)?
Lies: Only at the fifth transfer I had my blood tests done at a hospital closer to home. We were always asked about the option during our treatment but I preferred to go to Jette because it felt so familiar. In hindsight, it is nice that this option is offered. It can save a lot of time and there were clear instructions and forms which made it very easy to have blood sampling done at another hospital. So it’s very thoughtful for the patient that this is possible.
During your treatment, there were also renovation works happening on the Brussels IVF nursing unit. Did you notice anything about this?
Falke: We noticed during the embryo transfer that there was some impact from the renovation work. This made it an extra stressful day for us because our familiar structure had changed. It took some time find the right route: registration, blood sampling, signing the contract, registering again at the temporary reception desk and the route to the operating theatre upstairs. We also saw many couples being sent back for blood sampling or to the reception area. Fortunately, all care staff always remained kind and helpful in getting the patients to their correct destination.
Lies: Maybe it can be useful to send patients with a ‘roadmap’ or instruction video with their appointment to reduce the stress of finding their way within a big hospital.
Brussels IVF offers a virtual 360° tour so prospective parents are able to visit the locations in our centre, e.g. how blood collection happens, what the lab looks like,...
Take a look @
Are there any aspects you will specifically remember that you would like to share?
Lies: I didn’t know it was an option to have an embryo transfer performed in a natural cycle (in that case, often only a single injection is administered to trigger and properly time the ovulation). I personally found this a big advantage. I myself had stopped taking the pill for years because of the impact the hormones had on me. These caused quite an emotional rollercoaster for me on top of the treatment. So I definitely found this an added value.
Falke: As a (male) partner, you still often feel overlooked. As a woman undergoing the treatment, you admittedly need more medical help and have to do most of the work in the process. But as a man, you are often on the side line, quite powerless, just wanting to be more involved in every step.
Lies: We both noticed that sometimes instructions were only explained to me and he just sat there. When we discussed this with friends, joking around, many couples shared that they had a similar experience. Unfortunately, this seems to be the case at many centres. But it is something that really needs more attention because you share this dream of growing your family and you really go through the process as a couple.
Falke: We do however hold fond memories of the OR, where the embryo transfer took place. Every time everyone was warm, both the nurses, who always came to meet us in the waiting room with a smile, and the doctors. There was also attention to the nice seasonal decorations that were spread throughout the corridors so we didn’t feel quite like we were in a hospital.
Do you have any ideas of your own to optimise guidance or support during a fertility treatment?
Lies: It might be a nice idea to have an Instagram account linked to the fertility centre. This would be a place where photos of the department, staff members, tips and tricks, videos from the lab, stories of other patients,... can be shared. Because at the beginning of our journey, we really felt incredibly alone.
Until we set up an anonymous account ourselves to make the subject open to discussion and thus help others. It turned out that there are lots of peers, with lots of questions, active on Instagram. Quite a magical little world. It would be nice if Brussels IVF were to be found among them. It might also be a low-threshold way for people to ask questions and/or share their story.
“To this day, there is still a bit of disbelief, but also incredible gratitude towards the growing belly.
Without Brussels IVF, we might have been childless. So a big ‘thank you’ to the team in Jette who always reassured us, helped us, answered our many, many questions, during appointments, by phone and via emails, and that ultimately helped fulfil our desire to have a child and grow our family.”
At the time of the interview, Lies and Falke are 19 weeks pregnant.
Pictures by Maxime Claeys.
FOCUS ON Digital approach tools for patient empowerment
Clear instructions and professional guidance in your back pocket.
The Brussels IVF mobile application: Robin app Brussels IVF has developed a mobile app to provide patients with guidance via a user-friendly informative application on their smartphone during their treatment at Brussels IVF.
In the -soon to be released- app, the patient has access to her personal treatment plan, her medication instructions and the upcoming blood/ultrasound appointments at Brussels IVF. All information and notifications in the app were designed with attention to optimal discretion, security of the patients’ data and patient privacy.
From the summer of 2024 the app should be available at the Play store (android) or App store (iOS). Once downloaded, it provides access to our centre’s contact details and general information articles on fertility, medically assisted reproduction and early pregnancy.
Only when the patient engages in an active treatment, can the app be linked to her patient file. During the counselling session with a Brussels IVF midwife, the patient can opt in for communication via the Robin app by signing the informed consent. The counsellor will then register the account to link the patient file to the app and provide user instructions.
Guidance from start till trigger
The mobile application will be able to provide active guidance from the time of the first blood sample at the start of treatment to the administration of the trigger medication to induce ovulation.
The patient can also use the app to contact Brussels IVF and ask (non-urgent) questions, or to consult her scheduled appointments.
Robin our mobile application
Our team of the Daily Monitoring (DM) will no longer phone that patient to give instructions during the treatment. Instructions will be provided via a notification in the Robin app. When something changes in the patients’ treatment, she will receive a notification on the home screen of her phone. Whenever the patient receives a notification, she’ll have to confirm if the received instructions, were clear. If the received instructions are not clear, the patient can indicate this in the app. In that case, the DM will contact her by phone for additional explanation. She can also set personal alerts, at her time of choice, to help remember medication and/or appoinments.
By adopting this digital approach, we want to organise the follow-up and instructions during treatment in a more patient-friendly way: to consult the information when it is most convenient and be able to review it, if or when necessary.
The future
We are continuing to invest in our digital accessibility and information through our smartphone application. In the next phase of the app, we want to expand support across the entire treatment; up to the oocyte retrieval, embryo transfer and a successful pregnancy.
In time, we want to make it possible to book an appointment in our centre using the Robin app. It is our dream to provide a partner app that can be linked to the patients’ app to make it possible for couples, who consent to this, to have a more equal experience together.
BrusselsIVF.be our new website
www.brusselsivf.be
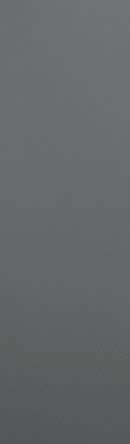
At the end of 2023 the new Brussels IVF website was launched to better guide prospective parents from the start in their personal journey and with their specific needs and questions.
The website was therefore constructed around 6 care paths that help filter the right information for the right person/ couple.
An accessible gateway with correct, transparent and clear information so patients can navigate or even co-construct their own journey in an informed way.
The website is designed to be an accessible gateway with correct, transparent and clear information so that patients can navigate their own journey in an informed way.
Our website aspires to do more than purely providing medical information; through a 360° experience you can make a virtual visit to the centre, you will find book and podcast tips on various fertility related topics, get info on our webinars, can read testimonials from other patients,...
FOCUS ON Our new Day Care Unit
Brussels IVF continuously invests in improving the experience of prospective parents in our centre. In almost every case, these are young people who do not feel sick. But medical help, even regarding something as intimate as a desire to have children, requires stepping into a hospital. Therefore, we strive to make this setting as ambient as possible and pay careful attention to the autonomy of the patient and the intimacy of the couple. This in terms of processes and flows but also in the design of spaces up to the interaction with staff.
After just over a year of severe remodelling, the new Day Care Unit at Brussels IVF was inaugurated.The remodelling was necessary to provide a more pleasant stay with more consideration for the privacy of a fertility process. The former Nursing Unit has been renamed ‘Day Care Unit’ because it now offers ambulatory care (such as insemination, blood sampling, ultrasound) in addition to outpatient admissions.
All care operations are thus centralised on the first floor of the fertility centre. Consultations and counselling will continue to take place on the second floor.
The inauguration also marked the merger of two teams: the nurses/midwives of the former nursing unit and our midwife-counsellors. The merging of these two teams ensures closer cooperation within the centre and optimal continuity of care for patients as well as more development opportunities for Brussels IVF staff.
The reception desk at our Andrology lab was also renovated to provide a more pleasant environment to make a sample and generate more privacy for men.
Single room (the norm at oocyte retrieval)
Lounge
Andrology reception desk
Waiting room
Team Day Care Unit & Counselling
FOCUS ON Collaborations, regional approach and patient-centered care
Regional colaboration for patient-centered care
Brussels IVF invests in collaborations with other hospitals and fertility centres both within Belgium and abroad. This is one of our growth models that we are particularly proud of. The key aspect of this model is that patients can receive the intake and follow-up care close(r) to home, while still benefiting from the expertise of a top notch centre.
There are various ways for doctors and centres to collaborate with Brussels IVF.
First, there is the ‘in-house’ model, where only the initial intake of the patient occurs at the local doctor or centre, and the rest of the treatment including monitoring is performed by Brussels IVF.
Then there is the ‘drive-in’ model, where the external physician comes to Brussels IVF to perform the medical procedures after monitoring the patient.
We also offer the ‘network’ model where a counselor from Brussels IVF is seconded to another hospital to perform counseling tasks there while the monitoring is performed by the external doctor.
By offering this comprehensive range of collaboration options, Brussels IVF provides significant benefits for both patients and external centres. For patients, the advantages include local care, allowing them to stay close to home for routine procedures such as blood tests and ultrasounds, thereby enhancing their comfort and convenience. Despite receiving local care, patients benefit from the advanced technology and expertise of a leading fertility centre, which optimises their chances of successful treatment outcomes. Furthermore, close collaboration and regular evaluations ensure the quality and continuity of care.
For external centres, the benefits are equally compelling. Flexibility is a key advantage, as external centres can choose from various collaboration models that best fit their capabilities and needs. Partnering with Brussels IVF facilitates knowledge sharing and training, which improves the overall quality of services provided by these centres.
Additionally, the ability to outsource specific tasks to Brussels IVF can enhance the efficiency and effectiveness of external centres’ services. Finally, regular evaluations and consultations allow for continuous optimisation and innovation in collaborations, leading to better outcomes and advancements in care.
‘There has been a wonderful partnership between OLV Aalst and Brussels IVF for almost five years now. The addition of a counsellor present at the OLV is certainly an added value for our patients. We look forward to helping even more families together to make the most marvelous wonder, new life, possible.’
Dr. Sien Delattre, OLV Aalst
‘This collaboration allows my patients to benefit from the skills and professionalism offered by Brussels IVF and yet be monitored closer to home, making the combination of a fertility treatment and work-life, more feasible. They don’t have to spend hours commuting to get an ultrasound or blood sample. I am glad we can offer this to patients. Many of them are very enthusiastic about the team at UZ Brussel. They like both the personal contact and counselling with me, as their treating physician, and the expert follow-up at Brussels IVF.’
Dr. Evi De Brakeleer, AZ Glorieux, Ronse
Scientific Research & Training
Since its creation in 1983, Brussel IVF has been driven by three strong missions: Providing the best healthcare, research & development and knowledge sharing.
Thanks to this powerful combination, Brussels IVF, often together with the Centre for Medical Genetics (CMG) - has achieved several breakthroughs in the high-tech field of infertility.
Most of the research is conducted by scientific staff at the Assisted Reproductive Technologies laboratories. However, we also collaborate with other researchers. Genetic research mostly takes place in the laboratories of the CMG, for example. Together, the CMG and Brussels IVF make up the PGT clinic, where we test the embryos genetically before they are transferred to the prospective mother’s womb and help couples with genetic problems to have a child free of the genetic defect.
We also work with the Human Embryonic Stem Cell laboratory (hESC lab) and with the REGE (Reproductive Genetics), REIM (Reproduction and Implantation), FOBI (Follicle Biology) and BITE (Biology of the Testis) research groups of the Vrije Universiteit Brussel (VUB).
Research at the clinical level
Reproductive endocrinology
Regarding ovarian stimulation, a lot of clinical questions remain unanswered. We are searching for the optimal protocol to treat poor responder patients in two clinical studies. Besides, progesterone at the end of the follicular
phase is one of our hobbyhorses. Individualisation of the preparation of a frozen embryo transfer cycle is an important topic in our research. Another clinical study deals with the influence of the thyroid function on pregnancy outcome.
Endometrial receptivity and implantation
To reach a successful implantation three elements are essential: a competent embryo, a receptive endometrium and an adequate synchronization between both. In several clinical and basic research protocols we aim to further unravel the role of the endometrium in this rate-limiting step. Our goal is to better understand how it prepares for implantation/ pregnancy and which factors influence the process.
In new upcoming research projects, we will work towards a standardized diagnosis and treatment of chronic endometritis and we will investigate its impact on implantation following IVF. Emerging new technologies like for example culturomics will be explored within this context. Furthermore, we will also focus on the later stages of implantation with the first trimester screening program that tries to identify patients who are pregnant following ART and are at increased risk for placental dysfunction and the development of preeclampsia.
Polycystic Ovary Syndrome (PCOS)
PCOS is one of the most common endocrine conditions in women of reproductive age. We have an active focus on translational and clinical research aimed at the understanding of transgenerational effects of PCOS on health of the offspring; optimising success rates after fertility treatment in subfertile women with PCOS; reducing the risk of obstetric complications in pregnant women with PCOS.
Laboratory techniques
The aim is to improve existing techniques in the fertility clinic and to develop and validate new procedures in the following sub-domains:
• laboratory techniques to fertilise an oocyte outside the body (IVF and ICSI);
• conditions under which embryos grow outside the body;
• best protocols to freeze and store embryos;
• techniques to remove a few cells from the embryo for genetic diagnosis (embryo biopsy);
• refinement and fine-tuning of existing molecular techniques to check DNA mutations, hereditary disorders and chromosomal abnormalities in embryos.
Embryonic development and implantation of the embryo in the uterus
Embryonic development starts when the egg is fertilised by a sperm cell. A fertilised egg develops into a multicellular embryo, a morula and a blastocyst. Research into embryonic development and implantation in-vitro is aimed at understanding why embryos grow poorly or do not implant. Our aim is a better understanding of the function of the genes and proteins that play a crucial role in early embryonic development. We hope this will lead to better diagnosis and treatment of couples with fertility problems.
Genetic make-up of the embryo
This domain studies techniques to examine the DNA of embryos before they are returned to the uterus. The bestknown application is pre-implantation genetic testing (PGT), in which we remove a few cells or a little tissue from the embryo for analysis in the lab. There are two main reasons to genetically examine embryos:
• to prevent embryos with a genetic disorder from being transferred during a fertility treatment;
• to find out which genes play a role in embryonic development and implantation.
Embryonic
stem cell research
A human embryo of about five days old (the blastocyst) contains unique stem cells that, under certain conditions, can develop into any type of cell in the human body, such as nerve cells, muscle cells, blood cells, eggs and sperm. This research wants to investigate whether these stem cells can be used in the future to replace damaged cells in diseases such as Parkinson’s, heart failure and diabetes.
Genome modification
The aim of this research is to determine whether it is possible to modify the DNA of a human embryo safely and efficiently. This can be useful for two reasons:
• to avoid serious diseases by correcting the gene responsible for the disease;
• to conduct scientific research on genes that play a crucial role in early embryonic development. We do this by eliminating them and studying their effects on embryonic development.
Research in the ART lab
Must read publications in 2023: selected for you
Enzymatic tissue processing after testicular biopsy in non-obstructive azoospermia enhances sperm retrieval.
Vloeberghs V, De Munck N, Racca A, Mateizel I, Wouters K, Tournaye H
Hum Reprod. 2023 Oct 18; 2023(4): hoad039.
Micro RNA in Semen/Urine from Non-Obstructive Azoospermia Patients as Biomarkers to Predict the Presence of Testicular Spermatozoa and Spermatogonia.
Willems M, Devriendt C, Olsen C, Caljon B, Janssen T, Gies I, Vloeberghs V, Tournaye H, Van Saen D, Goossens E Life (Basel). 2023 Feb 23; 13(3): 616.
Individualized luteal phase support using additional oral dydrogesterone in artificially prepared frozen embryo transfer cycles: is it beneficial?
Mackens S, Pais F, Drakopoulos P, Amghizar S, Roelens C, Van Landuyt L, Tournaye H, De Vos M, Blockeel C
Reprod Biomed. 2023 Jun; 46(6): 939-945.
Impact of embryo vitrification on children’s health, including growth up to two years of age, in comparison with results following a fresh embryo transfer.
Belva F, Blockeel C, Keymolen K, Buysse A, Bonduelle M, Verheyen G, Roelants M, Tournaye H, Hes F, Van Landuyt L
Fertil Steril. 2023 Jun; 119(6): 932-941.
Electronic witnessing in the medically assisted reproduction laboratory: insights and considerations after 10 years of use.
Sterckx J, Wouters K, Mateizel I, Segers I, De Vos A, Van Landuyt L, Van de Velde H, Tournaye H, De Munck N
Hum Reprod. 2023 Aug 1; 38(8): 1529-1537.
Main research ongoing Research
40+ peer-reviewed articles published in 2023
50+ ongoing research projects
Important studies in the clinic
A randomised, double-blind, placebo-controlled trial to assess the efficacy and safety of FE 999049 for treatment of men with idiopathic infertility (Trial 000400 - ADAM)
Tournaye H.
Live birth after additional tubal flushing with oilbased contrast versus no additional flushing: a randomized multicenter, parallel group pragmatic trial in infertile women with at least one patent tube at Hysterosalpingo-foam sonography (Hyfoil study)
Blockeel C.
Hyalobarrier®GEL ENDO versus no Hyalobarrier®GEL ENDO following operative hysteroscopy for improving reproductive outome in women with intrauterine pathology wishing to become pregnant (AGNOHSTIC trial)
Schutyser V., Tournaye H.
AURORA-REC (Aurora test for patients treated with recombinant gonadotropins): an observational cohort study to evaluate the expression profiles of oocytepotency-related genes in ovarian cumulus cells from ICSI patients that are treated with recombinant gonadotropins (AURORA study)
Blockeel C.
The “Lady De” study: Luteal phase ovarian stimulation with Follitropin delta and dydrogesterone: a randomized cross over pilot trial
Blockeel C.
The FLORA-project: in search for the microbial cause of chronic endometritis and the most appropri-ate treatment to obtain a successful pregnancy IVF/ICSI Mackens S.
At high-risk for pre-eclampsia after assisted reproductive technology (HEART) Mackens S.
The influence of different thyroid autoantiboldies on thyroid function and preganancy outcome after assisted reproductive technology (TGAB-study)
Uvin V., De Brucker M., Unuane D.
Effect of recombinant FSH dosing following corifollitropin alfa in patients undergoing IVF/ICSI in a GnRH antagonist protocol: a randomized controlled dose-finding study (CORIPRO study)
Blockeel C., Racca A.
Natural cycle versus hormone replacement therapy cycle for a frozen-thawed embryo transfer in PGT patient (HRT_NC-FET study)
Blockeel C., Roelens C.
fRozen thawed EMbryo replacement using Oral Dydrogesterone or vaginal progEsterone for Luteal phase support (REMODEL study).
Blockeel C., Roelens C.
The circadian variability of serum progesterone during the day of a frozen embryo transfer in an artificially prepared cycle and in a modified natural cycle (CIRCAPRO)
Blockeel C., Loreti S.
Clinical efficacy of virtual reality for acute pain and anxiety management during outpatient hysteroscopy and endometrial biopsy in subfertility patients (HYSVIR trial)
Schutyser V., Tournaye H.
Histological and Transcriptional Changes caused by Endometrial Flushing with Lipiodol: A Cross Over Study (Lipiodol study)
Blockeel C., Racca A.
Double trigger and ovum retrieval vs. conventional antagonist ovarian stimulation protocol in poor prognosis women undergoing IVF/ICSI: a randomized pilot study (DUOPICK study)
Boudry L., Blockeel C.
Initiation of ovarian stimulation with recombinanthuman FSH (Bemfola®) in the late follicular phase, a randomised controlled pilot study (D2D12Bemfola study)
Blockeel C., De Rijdt S.
Oral dydrogesterone (OD) versus micronized vaginal progesterone (MVP) for luteal phase support (LPS) in IVF/ICSI: pharmacokinetics and the impact on the endometrium, the microbiota of the genital tract and the peripheral immunology (DYDRA study)
Mackens S., Blockeel C., Van de Velde H., Tournaye H.
Clinical pregnancy rate for Frozen embryo transfer with HRT: a pilot study comparing 1 versus 2 weeks of treatment (Short-trial)
Blockeel C., Racca A.
PCOS TRIALS
A comparison between corifollitropin alfa and recombinant FSH for follicular recruitment in women with polycystic ovaries who undergo IVM treatment (IVM-ELONVA study)
De Vos M., Tournaye H., Segers I.
Translational research trial investigating the development potential of embryos obtained after in-vitro oocyte maturation (IVM) of oocytes from follicles <10mm following a pre-maturation culture (CapacitationCAPA-IVM) modulating the maintenance of meiotic arrest and the resumption of meiosis (IVM-CAPA study)
De Vos M., Tournaye H., Segers I.
Trial investigating the developmental potential of embryos obtained after biphasic in vitro oocyte maturation (IVM) of oocytes including a pre maturation culture step (‘capacitation step’) compared with standard IVM (IVMCAPA Sibling study)
De Vos M., Verheyen G., Segers I., Anckaert E.
Is in vitro maturation of oocytes influenced by the origin of gonadotropins used in maturation medium: is there a difference in efficiency when using urinary versus recombinant produced Follicle Stimulating hormone and human Chorionic Gonadotropin (IVM_FSHhCG)
De Vos M., Segers I.
Conventional ovarian stimulation vs. in-vitro oocyte maturation (IVM) followed by in-vitro fertilisation (IVF): differences in patients’ emotional adjustment and quality of life (EMAQOL-study)
De Vos M.
ONCOFERTILITY TRIALS
Autologous testicular tissue transplantation for fertility restoration
Vloeberghs V., Tournaye H.
Follow-up of fertility in young adults who did or did not store testicular tissue before gonadotoxic treatment for fertility preservation
Goossens E., Tournaye H., Vloeberghs V., Gies I., Van der Werff Ten Bosch J., Braye A.
COmbining Interventions of fertility preservation to Mitigate fertility loss after BReAst cancer (COIMBRA)
De Vos M.
DEPO-Trigger trial: GnRH agonist DEPOt TRIGGER for final oocyte maturation in breast cancer patients undergoing fertility preservation: a pilot study
De Vos M.
Important studies in the lab
Effect of abstinence duration on embryo development: a prospective sibling oocyte study
De Munck N., Verheyen G., Mateizel I.
Embryo culture at a stable temperature of 36.6°C or 37.1°C: a randomized controlled trial
Wouters K., De Munck N.
Evaluation of embryo quality after sperm selection using microfluidic technology: study on sibling oocytes
Wouters K.
Inhibitor treatments and microscopy in human embryos to understand cell fate specification in early human embryonic development (CREPE)
Van de Velde H.
Exploring the first lineage segregation in the human embryo: is GATA3 the gatekeeper of trophectoderm differentiation? (GATA)
Van de Velde H.
“Simply the best”: embryo selection for IVF using noninvasive biomarkers
Van de Velde H.
Defining signaling pathways regulating cell fate decisions during human peri-implantation development (LINDIF)
Van de Velde H.
Generation of a sub-cellular organization map defining the transition from pre- to post - implantation human development (SUBCEL)
Van de Velde H.
Characterization of sperm population following different selection procedures (CROSP)
Mateizel I.
Optimization of the cryopreservation procedure of very-low number of human spermatozoa (Cryolow)
Krunic M.
Novel regulators of embryonic development: identifying missing components of embryo culture medium for IVF (DRIVE)
Van de Velde H.
Optimising endometrial assembloids for human embryo implantation (EUTOPIA)
Van de Velde H.
Can testicular sperm be recruited more easily after a density gradient versus the standard mincing method, without loss of quality?
Krunic M.
Evaluation of a short warming protocol for human blastocysts (SHOW)
Van Landuyt L.
The sunbeam, a new medical device to integrate sperm selection and in vitro fertilization (IVF)
Wouters K.
Quality assessment of frozen/thawed and fresh human ovarian tissue in a clinical fertility preservation programme.
Segers I.
BRUSSELS IVF IN THE PRESS IN 2023
In-vitro maturation
70 x Brussels IVF in the press
Written press: 52
TV: 11
Radio/podcast: 7
About Brussels IVF and its history
Since 1983, the Centre for Reproductive Medicine, now Brussels IVF, has been active within UZ Brussel, the university hospital of the Free University of Brussels (VUB).
As a centre specialising in reproductive medicine, Brussels IVF has performed groundbreaking work developing and improving reproductive techniques and their application. A worldwide breakthrough was realised in 1991 with the introduction of the ICSI technique. Worldwide, around 30 percent of fertility treatments are carried out by IVF and 70% by ICSI. A quick calculation shows that there are now more than six million ICSI children in the world, which is roughly the population of the whole of Denmark. The break-through and success is based on continuous scientific research. For decades, our centre has been at the forefront of its expertise, both nationally and internationally.
The centre accounts for more than a quarter of all in-vitro fertilisation treatments carried out in Belgium (based on the latest Belrap data). For years, it has achieved markedly higher pregnancy and live birth rates than the national average.
Brussels IVF is compliant with the highest international quality standards (ISO 15224:2017 and ISO 15189:2012).
Scientific research lies at the heart of our activities. We have our own in-house training centre: the Training Centre Devroey-Van Steirteghem. Moreover, Brussels IVF provides accredited trainings for the European Board and College for OBGYN (EBCOG), the European Society of Human Reproduction and Embryology (ESHRE) and the European Academy for Andrology (EAA). Brussels IVF is a certified ESHRE centre for good clinical practice.
Prof. Em. André Van Steirteghem wrote down the rich history of the centre in his new publication: Egg cell seeks sperm cell for steady relationship - A Brussels triumph of science over infertility, Borgerhoff Lamberigts, 2024.
About UZ Brussel & VUB
Universitair Ziekenhuis Brussel (University Hospital Brussels) stands for quality medical care. It offers both basic care and innovative, hightech healthcare solutions at regional, national and international level at an affordable cost.
UZ Brussel continues to work every day to be a future-proof hospital in our capital city.
The structural work on the Landmark building was completed in 2023. This will contain the new main entrance and also a conference centre with office areas for supporting services. The start of the relocation is scheduled for autumn 2024.
The completion of the structural shell of the Medical Technical Block is also a fact. This the largest building project at the back of the hospital where medical imaging, the oncology centre, intensive care medicine haemodialysis, anatomo-pathology, the operating theatre, the surgical day hospital, the cathlab and logistics support services will be housed.
In 2023, UZ Brussel accounted for as many as 29,980 multiple day hospitalisations and 39,243 day-admissions.
A total of 446,620 consultations and 14,788 interventions took place. 75,296 patients came through the Emergency Department.
It was with pride that UZ Brussel once again received the title of top employer and pioneering employer in 2023. Rewarding, as its people are the driving force of the hospital.
The hospital’s clinical excellence, scientific commitment and human-oriented tuition ensure the highest degree of competence in many fields. The almost 5,000 multilingual employees are driven by the patients’ quality of life. Care is provided in a respectful way, regardless of origin, language or religion.
Vrije Universiteit Brussel (VUB, the Free University of Brussels) is a dynamic and modern university with two parkland campuses in the Brussels Capital Region. The main campus in Etterbeek is home to eight faculties.
Brussels IVF is located on the expansive and green Brussels Health Campus in Jette. This campus also houses the Faculty of Medicine and Pharmacy of the Vrije Universiteit Brussel (VUB), alongside the teaching hospital UZ Brussel. The close proximity fosters high-quality research, tailored education, and a strong social commitment to addressing tomorrow’s challenges.
This material is protected by copyright. No part of this report may be reproduced without prior permission in writing from the responsible publisher. Inappropriate or unlawful use is an infringement of the copyright and is a criminal offence.