INSIGHTS, FACTS & FIGURES
Brussels IVF
annual report

2022
40 years of 1991



Brussels IVF
annual report
40 years of 1991

27,5% of all IVF treatments in Belgium were performed here.
43,1% chance of a live born child after fresh embryo transfer in reference group (vs. rest of Belgium: average 29,5%)
38,1% chance of a live born child per embryo transfer if under age 36 (all ranks) (vs. rest of Belgium: average 28,7%)
BRUSSELS IVF performs
83% of all IVM cycles
74% of all ICSI cycles with fresh surgically retrieved sperm
66% of all oocyte donations
*Belgian Register for Assisted Procreation - 2020 data on 34 Belgian IVF centres (incl. 18 B-centres)

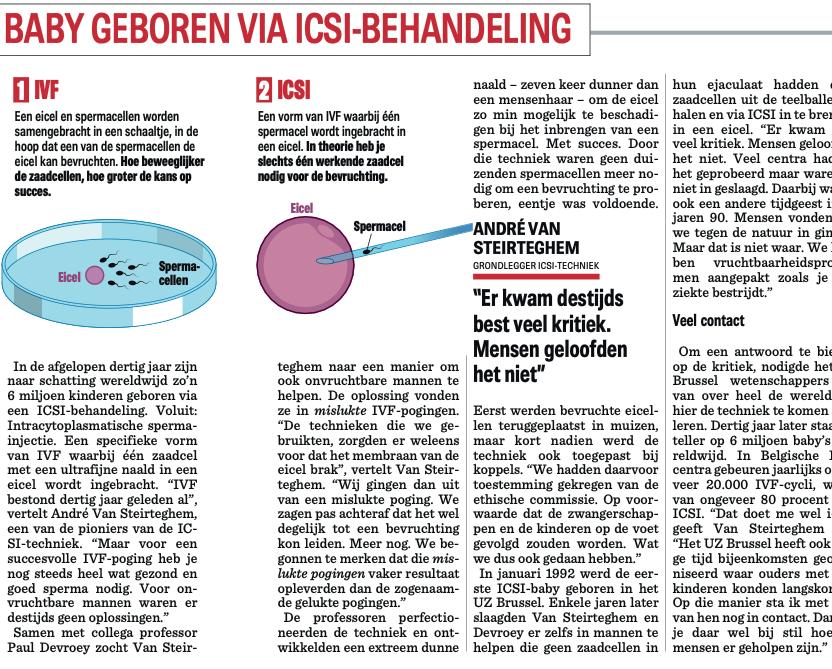
Last year we celebrated 30 years of ICSI, the ART technique that definitively put us on the world map in 1992. Today, worldwide, ICSI has superseded ‘classic IVF’ as a routine technique. According to the most recent figures, ‘our Brussels’ technique is used, rightly or wrongly, in more than 70% of IVF treatments worldwide.
This year we can also blow out candles because our Centre for Reproductive Medicine, now Brussels IVF, had its official start in 1983! Indeed, in 1983 the Centre for Reproductive Medicine was officially ‘christened’ by our CEO, the late Louis Tielemans. At the time, it was an unprecedented ‘joint venture’ between two units from two different departments at our institution, the fertility unit of the gynecology-obstetrics department led by Paul Devroey and the RIA lab (radioimmunology lab) of the Clinical Chemistry department led by André Van Steirteghem.
In that starting year 1983, 155 oocyte aspirations were performed, a volume we reach in about 10 days now 40 years later.
On 7 May we celebrated our ruby wedding together with 1200 visitors at our Children’s Return Day. In the past 40 years more than 41.000 children were born thanks to our reproductive efforts. And this
figure remains underestimated, because of the follow-up issues once a patient becomes pregnant, a problem that all of us are probably familiar with.
Although the SARS-COVID epidemic is finally behind us, 2022 was again an eventful year for Brussels IVF. And above all, a busy year. Where a few years ago the understaffing in the IVF lab led to great work pressure, in 2022 we were faced with frontline staffing problems. From the Contact Centre to the medical staff, many links were missing to smoothly manage our patient flow, resulting in a sharply increased workload for many of us in the front office. Yet all of us, from Contact Centre to MD’s, were prepared to go the extra mile so that we could close 2022 with an ART activity comparable to 2019, our pre-COVID peak year.
Nevertheless, COVID also accelerated other developments. Online meetings and online teaching became commonplace, including so at Brussels IVF. We introduced very successful webinars to support our (future) patients. Webinars that will be further developed in the coming years to target specific groups in need of ART with new topics. For our internal training, online learning was also introduced courses through the ‘Brussels IVF Academy’.
Although 2022 was a year of transition, 2023 will also have its challenges. Indexation, a typical Belgian mechanism by which salaries are being continuously synchronized with the cost of
living, together with the rise in the cost of energy, reagents and disposables, among other things, force us to look for solutions to cut costs without neglecting our mission and especially without compromising on quality.
Indeed, for years we have been able to achieve high success rates. According to the latest official report of BELRAP, the compulsory Belgian data registration to obtain reimbursed treatment, Brussels IVF accounted for 28% of all IVF treatments in our country. Yet the live birth rate in the ‘reference group’ was 36% per initiated cycle, without inclusion of surnumerary frozen-thawed embryos, while the average figure for Belgium as a whole was 25,7%. Per single fresh embryo transfer at Brussels IVF this figure was 43% vs 29,5% for the remaining 17 other B-centres.
Yet, as still too many patients do not reach parenthood despite all our efforts quality cannot only be expressed by live birth rates. Therefore, in Brussels IVF we will also focus more on psychological patient support during the ARTjourney itself, hoping to increase our patient retention and eventually chance to parenthood.
A lot of challenges, but also a lot of achievements. Achievements do not just come like that. Every day, 7/7, a team of about 200 dedicated employees put all their efforts in providing the best care and support for our patients. Again, I would like to thank them in the first place. I would
also like to thank our referrers for all the confidence they have in Brussels IVF. However my gratitude also goes to our most important partners: our patients. Thanks to them, we can realize our dream: helping them to make their dream to come true.
Herman Tournaye Medical & Scientific Director Brussels IVF
Prof. dr. Christophe Blockeel Senior Medical Director
Expertise: Reproductive endocrinology
Prof. dr. Willem Verpoest
Senior Medical Director
Expertise: Reproductive genetics & Immunology
Prof. dr. Shari Mackens
Medical Director
Dr. Michelle Soares Junior Medical Director
Expertise: Fertility diagnostics & treatment
Dr. Julie Praet Junior Medical Director
Expertise: Fertility diagnostics & treatment
Prof. dr. Michel De Vos Senior Medical Director
Prof. dr. Herman Tournaye Head of Department
Expertise: Andrology & Oncofertility
Dr. Liese Boudry
Junior Medical Director
Expertise: Reproductive infectiology
Expertise: Recurrent miscarriage & Implantation failure
Dr. Caroline Roelens
Junior Medical Director
Expertise: Fertility diagnostics & treatment
Expertise: Reproductive endocrinology & Oncofertility
Dr. Veerle Vloeberghs Medical Director
Expertise: Andrology & Oncofertility






 Dr. Guy Verhulst Consultant
Prof. dr. Michael De Brucker Consultant
Dr. Sien Delattre Consultant
Dr. Elisabeth Soete Senior Clinical Fellow
Dr. Valerie Uvin Senior Clinical Fellow
Dr. Guy Verhulst Consultant
Prof. dr. Michael De Brucker Consultant
Dr. Sien Delattre Consultant
Dr. Elisabeth Soete Senior Clinical Fellow
Dr. Valerie Uvin Senior Clinical Fellow
Junior clinical fellows

• Dr. Sara Loreti
• Dr. Billie Frederix
• Dr. Maria Francesca Brutto
• Dr. Ezgi Darici
• Dr. Emma Goyens
• Dr. Letizia Li Piani
• Dr. Margot Moeykens
• Dr. Pasquale Petrone
Associated research fellows
• Dr. Valerie Schutyser
• Dr. Maria Petra Agius
• Dr. Sylvie De Rijdt
• Dr. Panagiotis Drakopoulos
• Dr. Biljana Popovic
The Reproductive Skills Centre Brussels (RSCB) is Brussels IVF’s ART training centre. The RSCB consists of a training room with two complete ICSI and vitrification set ups and a clinical training room with simulators for oocyte pick-up, embryo transfer, hysteroscopy and laparoscopy.
The training rooms are used for internal training of our medical staff, nurses and midwifes, lab technicians and embryologists. But the RSCB provides external courses as well, thanks to close collaboration with companies. The RSCB courses offer a comprehensive training in the clinical and laboratory aspects and practices of assisted reproductive technologies and reproductive surgery.
In addition to the RSCB, ‘Brussels IVF Academy’ was introduced to further professionalise our training programme, providing a platform and structured course

materials to help prepare subspecialist trainee MD’s and midwives for the ESHRE subspeciality exam leading to certification as a subspecialist fellow or counselor in reproductive medicine.
The RSCB is led by Prof. dr. Herman Tournaye, Clinical and Scientific Director at Brussels IVF, UZ Brussel. Faculty include senior Brussels IVF staff.
The Reproductive Skills Centre Brussels is located at the university hospital UZ Brussel.
Get in touch:

rscb.brusselsivf.be
rscb@uzbrussel.be
Dr. Florence Belva graduated as a paediatrician and has been a scientific associate at the Centre for Medical Genetics at UZ Brussel since 2003. Her research focuses on the followup of children born after fertility treatment. She completed her PhD thesis in 2012 on the health of children born after intracytoplasmic sperm injection (ICSI). Currently, the focus of her research is on the long-term effects of this treatment and, more specifically, on the risk of infertility in the adolescents themselves who were born after parental fertility treatment. Furthermore, within the department, Dr. Belva is responsible for the start-up and follow-up of studies in the context of the medical follow-up of children born after the various fertility treatments including Pre-implantation Genetic Testing, oocyte vitrification and in vitro maturation of oocytes.

Brussels IVF is world-renowned for its ICSI technique, but what does the research tell us about the outcomes?
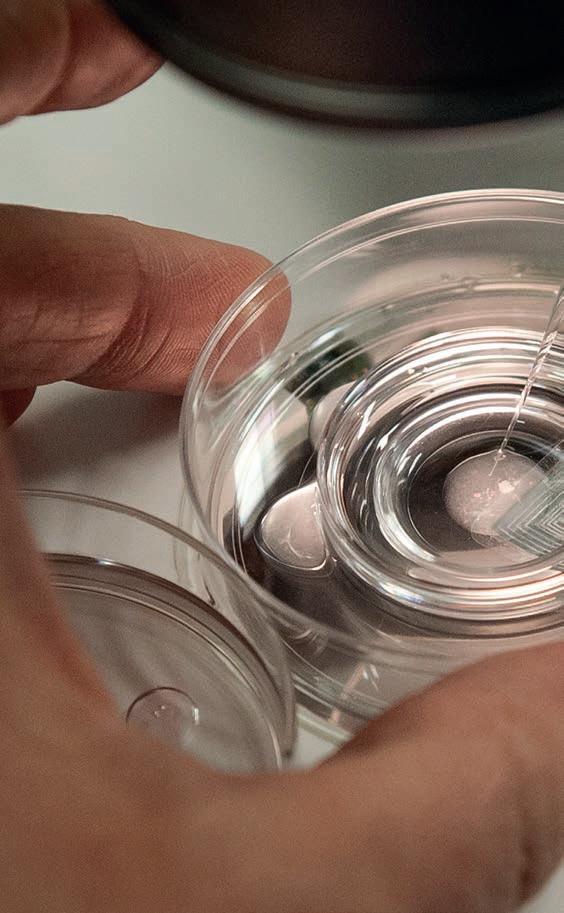
Intracytoplasmic sperm injection means the injection of one sperm cell into one egg cell, a fertility technique used mainly when the male partner has fertility problems. If there are too few usable sperm cells in the ejaculate to apply the classical IVF technique, ICSI is chosen. However, even if classical IVF, in which several sperm cells are brought together near an egg cell, does not result in fertilisation, ICSI can be applied in a subsequent attempt to increase the chances of embryo formation.
Since the introduction of IVF and ICSI at Brussels IVF, a large follow-up study for children born after Assisted Reproductive Technologies (ART) has been installed at the Centre for Medical Genetics. The follow-up program includes both questionnaires and physical examinations at the age of 3-6 months and at 2 years.
Our database with detailed information on the performed treatment and on the health of the children and their parents, provides a unique opportunity to study short- and long-term outcomes after ART, including ICSI.
Dr. FLORENCE BELVA Centre forFrom birth up to 2 years
Increased risk of preterm birth, lower birth weight, chromosomal abnormalities and congenital anomalies compared with the general population. These risks are not higher with ICSI than with IVF.
Higher birthweight in children born after transfer of frozen-thawed embryos compared to fresh embryos but no differences in weight, height and health outcomes (developmental problems, surgery, hospital admissions, medication intake) at 2 years between children born after frozen-thawed or fresh embryo transfer. [1]
At the age of 5 years
Confirmation of increased risk of congenital anomalies, but overall physical examination was similar.
At the age of 8 years
Similar health parameters and growth before puberty but higher blood pressure in the ICSI group compared to the control group of children born after spontaneous conception.
At the age of 14 years
Similar blood pressure for boys and girls in the ICSI group. ICSI girls showed an increased risk of central, peripheral and total fat accumulation. Only ICSI boys who were further pubertally developed showed an increased risk of peripheral fat accumulation. In a smaller subgroup, similar levels of male sex hormone and inhibinB (marker for sperm cell production) were found in ICSI boys compared to their peers born after spontaneous fertilisation.
At the age of 18 to 22 years
Blood pressure and risk of metabolic syndrome (a cluster of conditions that increase the risk of cardiovascular disease and other health problems) as well as fat distribution in girls were overall similar between adolescents born after ICSI and after spontaneous conception. ICSI boys showed more peripheral fat accumulation compared to boys born after spontaneous conception.
The levels of sex hormones and also the number of follicles in the ovaries were similar in girls born after ICSI and after spontaneous conception. [2]
The levels of sex hormones were similar in boys born after ICSI and after spontaneous conception. A twofold lower total sperm count and sperm concentration were found in ICSI boys when compared to controls born after spontaneous conception. Also, ICSI boys were more likely to have sperm concentrations and sperm counts below the reference values of the World Health Organization. [3]
The finding of abnormal sperm parameters rises the concern of transmission of infertility from father to son and is further explored.
At the age of 2 years
Mental and motor development of ICSI children was similar to that of naturally conceived children.
At the age of 5 to 10 years
Cognitive, motor and socio-emotional development of ICSI children was similar to that of children born after natural conception. [4]
Parental well-being, family functioning and parentchild relationships were also similar to those of families with naturally conceived children.
[1] Impact of embryo vitrification on children’s health, including growth up to two years of age, in comparison with results following a fresh embryo transfer. Belva F, Blockeel C, Keymolen K, Buysse A, Bonduelle M, Verheyen G, Roelants M, Tournaye H, Hes F, Van Landuyt L. Fertil Steril. 2023;119(6):932-941. doi: 10.1016/j. fertnstert.2023.02.006.
[2] Serum reproductive hormone levels and ultrasound findings in female offspring after intracytoplasmic sperm injection: first results. Belva F, Roelants M, Vloeberghs V, Schiettecatte J, Evenepoel J, Bonduelle M, de Vos M. Fertil Steril. 2017;107:934-939
[3] Endocrine and reproductive profile of boys and young adults conceived after ICSI. Belva F, Bonduelle M, Tournaye H. Curr Opin Obstet Gynecol. 2019;31(3):163-169. doi: 10.1097/ GCO.0000000000000538.
[4] Follow-up of cognitive and motor development of 10-year old children born after ICSI compared to spontaneously conceived children. Leunens L, Celestin-Westreich S, Bonduelle M, Liebaers I, Ponjaert-Kristoffersen I. Hum Reprod. 2008;23:105-111
One in six people have difficulties to have children. When talking about “medically assisted reproduction”, we should be aware that medical assistance should also include psychological support. When starting a fertility treatment, intended parents have already gone through an emotionally intense turmoil. Often a grieving process is associated to their trajectory, either just because of not getting pregnant spontaneously or because of the need of using donor gametes. Suffering from infertility is often both invisible and underestimated by the outside world. For many patients there is a high barrier to seek help for such a personal and intimate problem. Moreover, as coping may differ between partners, relational problems may arise.
At Brussels IVF, for years we have a strong focus on the children’s welfare, as evidenced by our continued children follow-up studies on both physical and psychological well-being of the children born after ART. There is, however, also a need to improve awareness on the psychological well-being of the prospective parents.
While some patients meet with our psychologist by default, e.g. when in need of donor gametes, other patients are referred by their doctor or look for psychological support themselves. While poor prognosis is one important reason to withdraw from further treatment, emotional distress is the second important reason for discontinuing fertility treatment, eventually leading to childlessness, an even heavier psychological burden. Although in theory psychological support should be part of any fertility treatment from the start, in practice, this support often comes in when patients are already psychologically grounded.
Apart from evaluating specific treatment requests, our Brussels IVF psychologists also provide support before, during and after ART treatment. Such support is crucial for improving continuation rates eventually enhancing the chances for achieving parenthood and for patients general well-being.
In recent years, we paid more attention to the accessibility of our psychological support. By creating easy-access for psychological support and by developing webinars focusing on the mental wellbeing and resilience during IVF-treatment. Besides offering remedial support, we also focus on prevention by helping patients to prepare for stress-management during their ART trajectory. We are ready to give our patients the guidance they need when starting their journey to parenthood.

Psychology team:

• Julie Nekkebroeck
• Rani Cooreman
• Lize Leunens
• Eveline Buyse
Psychologist appointment: info@brusselsivf.be or +32 2 477 66 99
Webinar: Mental health and resilience during fertility treatment
Tuesday 3/10/2023 at 8 p.m.
Tuesday 21/11/2023 at 8 p.m.
Registration: www.uzbrussel.be > search: webinar
More information: webinarbrusselsivf@uzbrussel.be




On May 7th, 40 years after the foundation of Brussels IVF, more than 300 families with children aged between 7 and 9 returned to the place where it all started for them. During this day, children playfully learned about our fertility centre and the various fertility treatments we practise there to fulfil our patients’ desire to have children.











Patients are the centre of Brussels IVF. We have a long history of conducting patient satisfaction surveys and involve patients in our operation and strategy. We take patient feedback and complaints seriously. That is why we have a dedicated quality manager who follows up on these complaints and tries to find a solution in close cooperation with the patient. We invest in a culture where also internal reporting is valued. Complaints from employees, but also ideas and improvements can be reported and implemented.
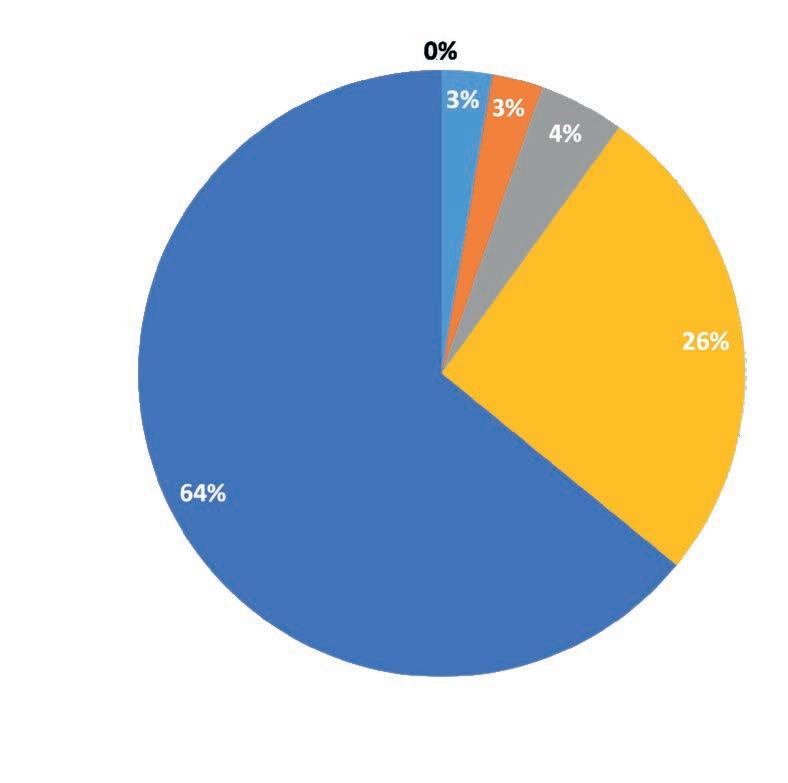
90% overall satisfaction with Brussels IVF
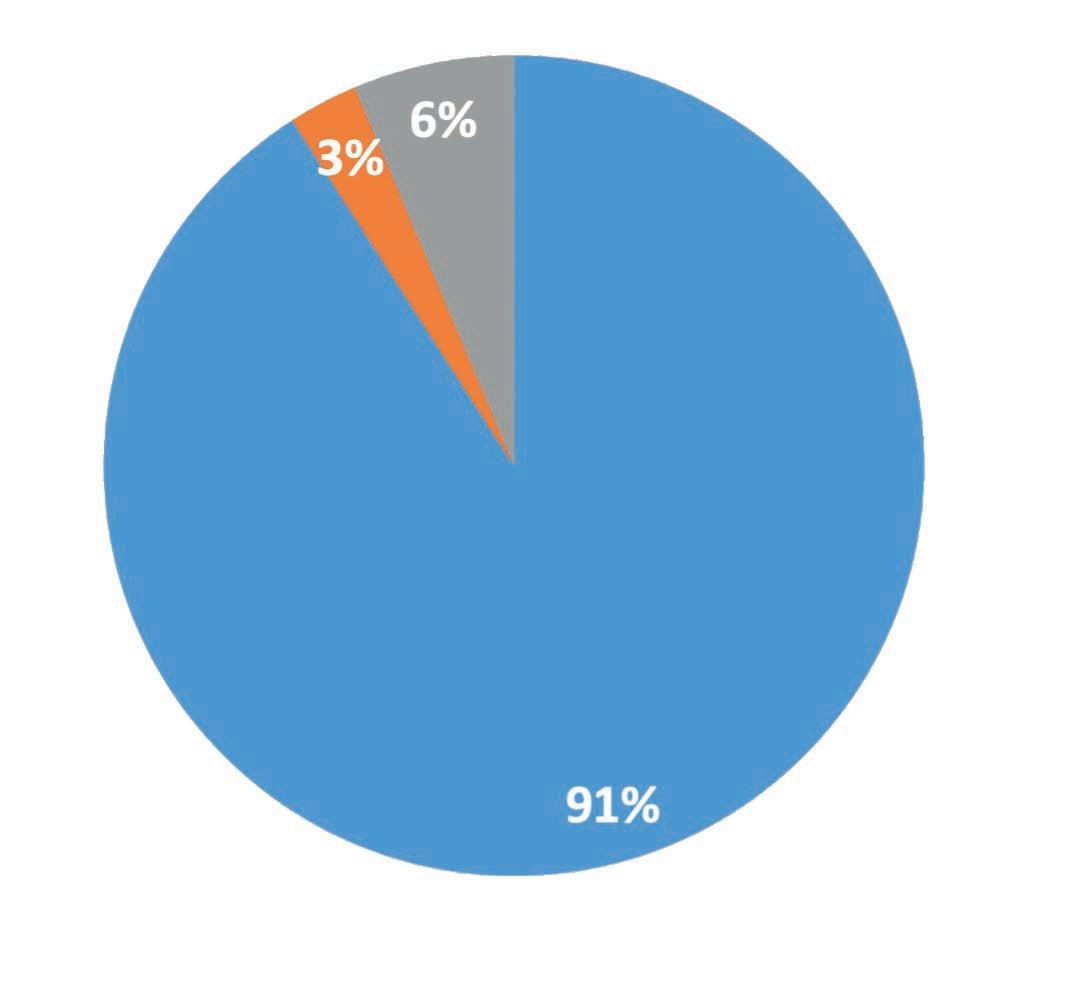
91% would recommend Brussels IVF to others
In welke mate bent u tevreden over Brussels IVF in het algemeen?
Zou u Brussels IVF aanbevelen bij anderen?
ISO

Feedback & complaints:

Mrs. Dina Brackman Quality manager Brussels IVF


Email: crgpatientfeedback@uzbrussel.be
Each year we organise patient focus groups in order to better understand the needs of our patients and their partners. This qualitative approach to patient satisfaction has become indispensable and of great value. In 2022, the first focus group was organised since the COVID pandemic. This was an excellent opportunity to bring patients together and, in an open conversation, share experiences, ideas and opinions.
“All nurses/midwives always helpful, empathetic and friendly”
“Webinar very positive in overview of treatment, helpful to be offered at beginning of course”
“My husband and I would like to just THANK the whole team of doctors and nurses and administrative workers”
Share your experience with us and others
Willems M, Seβenhausen P, Gies I, Vloeberghs V, Tournaye H, Van Saen D, Goossens E. Intratesticular xenografting of Klinefelter pre-pubertal testis tissue as potential model to study testicular fibrosis. Reprod Biomed Online. 2022 May;44(5):896-906.
Patients with Klinefelter syndrome undergo testicular fibrosis, a process still poorly understood. This study shows that xenografting can be a model for studying this fibrotic process.
Mertens J, Regin M, De Munck N, Couvreu de Deckersberg E, Belva F, Sermon K, Tournaye H, Blockeel C, Van de Velde H, Spits C. Mitochondrial DNA variants segregate during human preimplantation development into genetically different cell lineages that are maintained postnatally. Hum Mol Genet. 2022 Oct 28;31(21):3629-3642.
Mutations in the mtDNA induce coexistence of different mtDNA variants within a single cell. The inheritance and accumulation of deleterious variants can cause severe progressive mitochondrial diseases but may also affect cell aging, development of cancer and neurodegenerative disorders. This study suggests the existence of selection mechanisms during preimplantation embryo development that eventually filter out pathogenic variants.
Must read papers from 2022
Boudry L, Essahib W, Mateizel I, Van de Velde H, De Geyter D, Piérard D, Waelput W, Uvin V, Tournaye H, De Vos M, De Brucker M. Undetectable viral RNA in follicular fluid, cumulus cells, and endometrial tissue samples in SARS-CoV-2-positive women. Fertil Steril. 2022 Apr;117(4):771-780.
In this observational study women infected with SARS-CoV-2 who had IVF, viral RNA remained undetectable in the follicular fluid, cumulus cells, and endometrium. Although on a limited sample, yet reassuring findings.

Roelens C, Racca A, Mackens S, Van Landuyt L, Buelinckx L, Gucciardo L, Tournaye H, De Vos M, Blockeel C. Artificially prepared vitrified-warmed embryo transfer cycles are associated with an increased risk of pre-eclampsia. Reprod Biomed Online. 2022 May;44(5):915-922.
This study shows a higher incidence of pre-eclampsia after frozen embryo transfer in artificial hormone replacement cycles compared to transfer in a natural cycle. These findings may result in a change in our clinical practice with a preference for natural cycle transfer in ovulatory patients.
Strypstein L, Van Moer E, Nekkebroeck J, Segers I, Tournaye H, Demeestere I, Dolmans MM, Verpoest W, De Vos M. First live birth after fertility preservation using vitrification of oocytes in a woman with mosaic Turner syndrome. J Assist Reprod Genet. 2022 Feb;39(2):543-549.
This world-first case report documents the first live birth achieved using cryopreserved oocytes in a woman diagnosed with mosaic Turner syndrome.
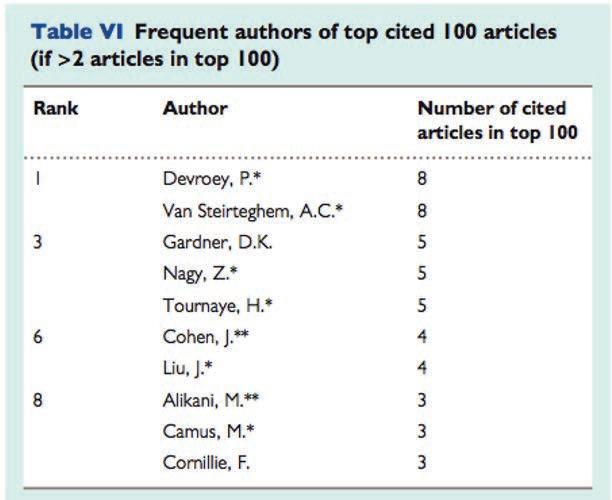
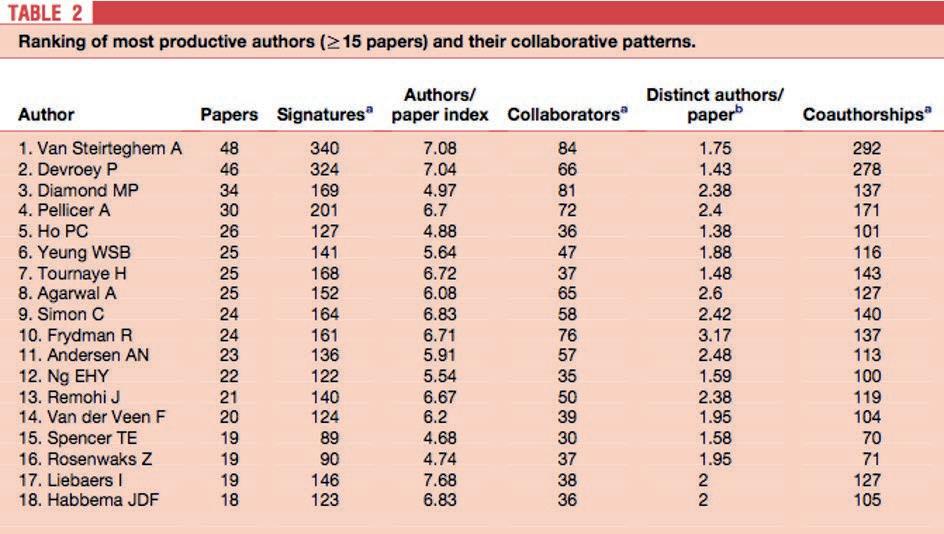
Some landmark papers in 40 years of reproductive health
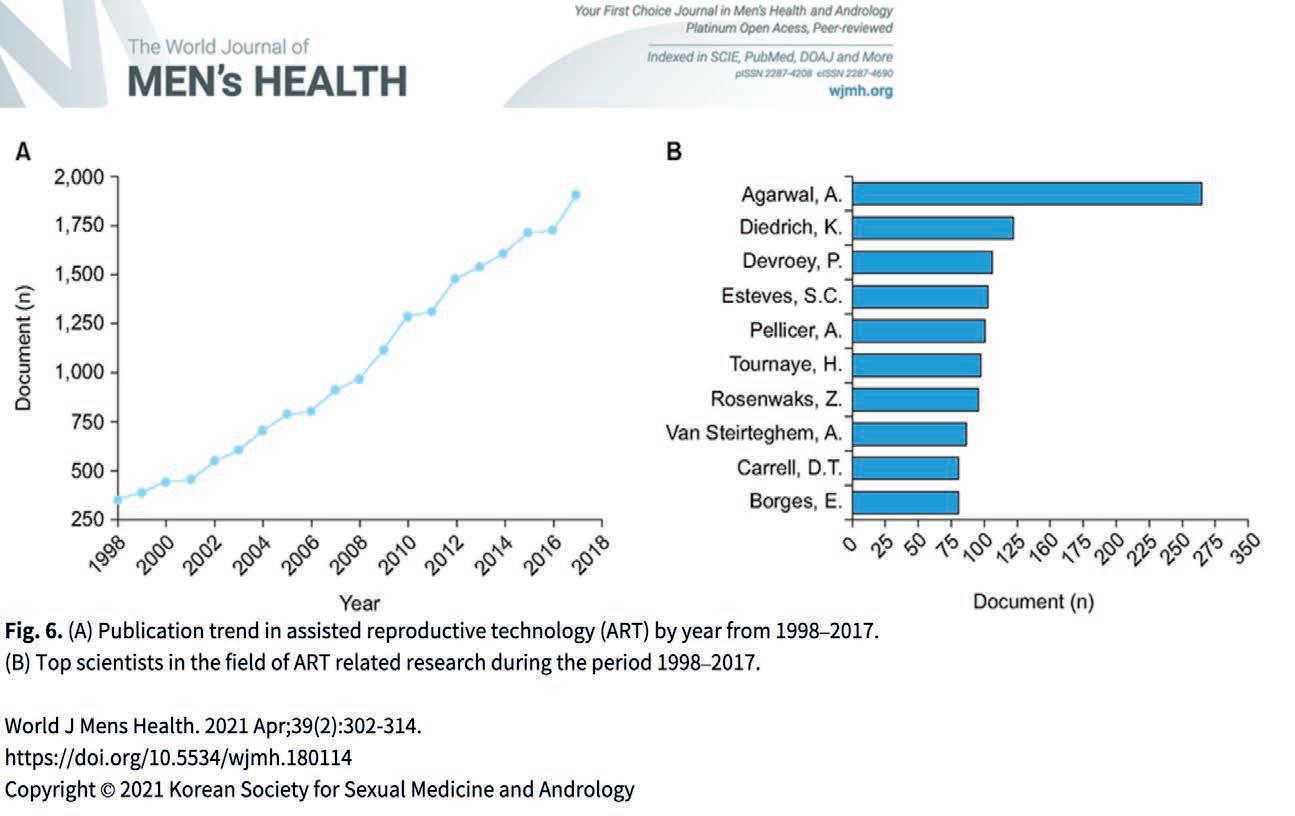
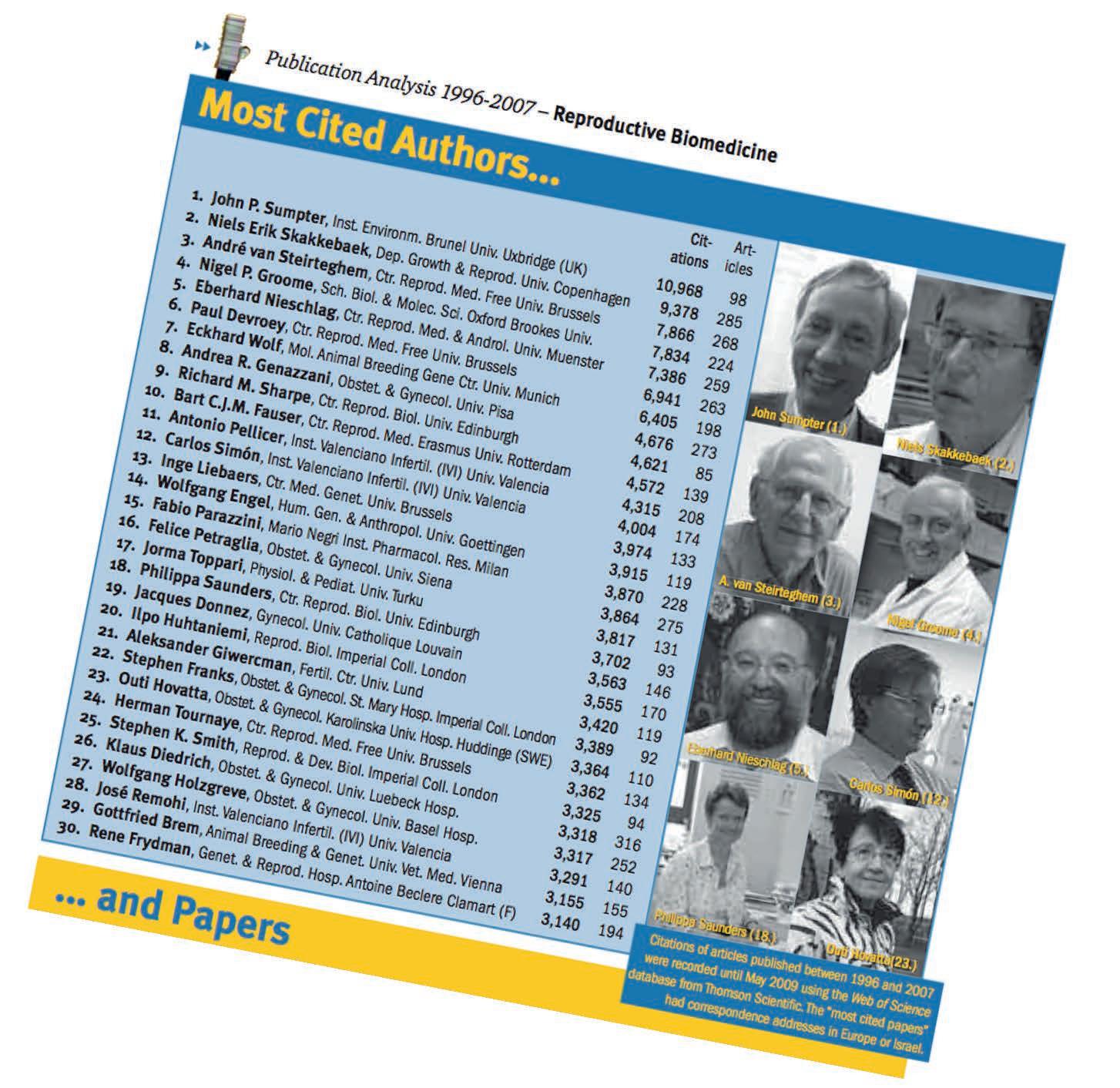
Publication Analysis 1996-2007
As in most other life science disciplines, England also dominates reproduction research in terms of publication and citation numbers. Top cited, in particular, are papers and authors addressing the manifold causes of fertility problems.
In February 2008, the European Parliament (EP) issued a recommendation that research on reproduction should become a priority for the life sciences. The unquestionably growing public and scientific interest in reproduction issues was the reason given. This, in turn, hasn’t come as a real surprise considering current catchwords from reproductive biomedicine such as fertility decay, sperm density decline, assisted reproduction, embryo transfer, nuclear transfer and cloning, stem cell research, reproductive toxicology, endocrine disruptors of reproduction and reproductive diseases like preeclampsia or endometriosis.

Good arguments, indeed. Alas, according to a Nature Medicine gist Gérard Chaouat from the Université Paris sud Orsay, such a commitment of the EP has not yet been translated into appropriate funds for European reproduction research (vol. 14: 1218-20). However, in the light of the slow-moving wheels of European research bureaucracy, perhaps Chaouat was a little too impatient at that time.
growth of interest in resear
couple of years is reflected by the publication output of European laboratories? Therefore, as usual in this ranking column, we compared the European countries’ publication performances in more than 60 specialist journals exclusively devoted to research on reproduction-relevant issues during the period 1996 to 2007 (for a complete list see journal listing “Reproductive Medicine” at medbioworld.com).
Regrettably, articles on reproduction which appeared in multidisciplinary journals such as had to be excluded from this comparison because Thomson Scientific’s database , used for this analysis, doesn’t provide any tools to extract reproduction-relevant articles from them

55x Brussels IVF in the press

Written press: 40x
TV: 10x
Radio/Podcast: 5x
525 followers on LinkedIn
490 followers on Twitter
60.162 website visits
227 participants in 8 patient webinars
 virtual tour Brussels IVF
virtual tour Brussels IVF









© Brussels IVF, UZ Brussel
This material is protected by copyright. No part of this report may be reproduced without prior permission in writing from the responsible publisher. Inappropriate or unlawful use is an infringement of the copyright and is a criminal offence.
Photography:
© Bart Moens
© Jo Robberechts
© Lies Willaert
© UZ Brussel
Responsible publisher:
Ulrike Dragon
Brussels IVF
Universitair Ziekenhuis Brussel
Laarbeeklaan 101
1090 Brussel
Belgium
Publication date: June 2023


UZ Brussel (University Hospital Brussels) has a staff of more than 4.100 employees. It is attached to the Faculty of Medicine and Pharmacy of the Vrije Universiteit Brussel (Free University of Brussels) on the Brussels Health Campus in Jette. With 721 hospital beds, it accounts for 30.779 admissions of patients each year from Belgium and abroad, 412.246 consultations (emergencies not included) and 78.840 patients at the emergency care. Its philosophy is founded on three principles: Dutch-speaking, pluralist and social. As a university hospital, it also has a teaching mission and conducts scientific research.
Oncofertility: www.brusselsoncofertility.be
PGT: www.brusselsgenetics.be
Sperm donation: www.spermadonor.be
Egg donation: www.idonatehappiness.be
Reproductive Skills Centre Brussels (RSCB): www.rscb.brusselsivf.be
Follow us on social media: Twitter: @BrusselsIVF

LinkedIn: Brussels IVF
CONTACT US

www.brusselsIVF.be
www.uzbrussel.be
CONTACT CENTRE
+32 2 477 66 99
Explore Brussels IVF in a virtual tour
