CAP Advancements Spring 2025
RN 2
Amber Craig, BSN, RN
Sadie Dooley, BSN, RN
Kayla Duncan, RN
Jessica Kimball, RN
Brittany Spence, MSN, RN, CEN
Kayle Stanley, BSN, RN, IBCLC
RN 3
Sarah Frewin, MSN, RN, PCCN
Kathryn H. Willis, BSN, RN, PCCN
“
A Critique of the systematic review:
Effects on Exercise Prehabilitation in Patients undergoing CABG surgery”
By: Maura Kloski, BSN, RN, CCRN
At Roanoke Memorial Hospital Carilion Clinic, the Cardiovascular Institute has cardiothoracic patients attend Pre-Surgical Testing (PST). One responsibility of a PST registered nurse (RN) is to review the prehabilitation goodie bag. In this bag are protein drinks, a glucose drink, chlorhexidine wipes, an incentive spirometer, and general instructions on exercise and oral care. These bags and education are especially important for patients undergoing coronary artery bypass surgery (CABG). During the perioperative process, CABG patients are asked about their compliance to the materials of their goodie bag, with a specific question being “did the patient walk/exercise?” A systematic review by Yamikan et al. (2025) investigated the effects of exercise-based prehabilitation on functional exercise capacity, intensive care unit (ICU) length of stay, postoperative complications, and mental health on patients undergoing a CABG (p.41).
This was a systematic review utilizing the patient/population/problem, intervention, comparison, and outcome method (PICO). The PICO method includes participants, intervention, comparator outcomes, and study design. Inclusion criteria included studies where participants were over the age of 18 and scheduled for isolated CABG surgery, while exclusion criteria eliminated studies with patients undergoing percutaneous coronary intervention or those on a transplant list. Yamkin et al. (2025) conducted comprehensive literature research that was screened by independent and blinded researchers to ensure appropriate full text and peer reviewed studies were selected (p.42). After a risk of bias analysis (utilizing the Cochrane Collaboration risk of bias tool and PEDro scale items) was completed, five articles were selected.
Ultimately, the five articles encompassed a total of 616 patients. Exercise interventions varied: aerobics, resistance, and high-intensity interval training were included, with program durations ranging from two to twelve weeks. Exercise frequency varied from five days to sixteen weeks, and sessions between 40 and 90 minutes.
Systematic literature reviews are excellent tools to identify gaps in research and synthesize reliable, and non-biased data. Yamkin et al. (2025) applied a strict inclusion methodology, though narrowing the sample size may limit generalizability, it reduced their sample size to five studies with a total patient population of 616 where 88.38% were male (p.43). The smaller sample size of female participants reduces our Continued on next page
understanding of the correlation between preoperative exercise and reduced hospital stay as well as post operative complications in female CABG patients. Future studies should aim to have a more proportionate female to male ratio to make the study appropriate. Interestingly, Harik et al. (2023) found that female patients have a worse outcome following CABG procedures than their male counterparts. There have been several proposed reasonings for this such as other comorbidities, smaller coronary artery size, anemia, and pathophysiology of coronary artery disease. However, similar to Yamkin et al. (2025), Harik et al. (2023) noted the need for further research and a higher participation rate of female CABG patients in order to identify and address the gap in female vs male CABG success.
The interventions used across studies included both supervised and unsupervised exercise-based prehabilitation. Three studies used the Short Form-36 and MacNew questionnaire to investigate the perceived effect of exercise training, two studies utilized a cyclo ergometer to evaluate cardiopulmonary fitness, and three studies of the five also included the 6-minute walk test (Yamkin et al, 2025, pg. 44-45). These instruments were appropriate for measuring functional capacity and improvement in cardiac health; however, inconsistency across studies complicates direct comparison and limits the strength of the conclusions.
Outcomes showed that exercise prehabilitation provides an improvement in functional capacity (Yamkin et al, 2025, p.49). There was moderate evidence to suggest exercise based prehabilitation reduced postoperative complications and reduced the length of hospital stay. There was conflicting evidence that prehabilitation exercise improves the generalized quality of life for patients (such as effects on depression, anxiety, perceived self, etc.). While this evidence is clinically significant, exercise-based prehabilitation could be recommended, and the evidence could impact presurgical testing processes, more studies particularly with more female participants, are necessary to reinforce these findings.
I would highly recommend this article to my peers, especially fellow nurses cross-trained in the presurgical testing area. In addition, this article can be shared with the physician assistant who coordinates presurgical testing for cardiothoracic patients. These results should be taken into consideration when educating patients in the presurgical testing process. Carilion could further their research and understanding of prehabilitation exercise in the success of cardiothoracic surgeries, specifically with CABG patients. An emphasis could be placed on the “please walk/exercise” section of the information packet, as there is scientific
Continued on next page
evidence to back the positive effects of prehabilitation. Furthermore, the evidence found could expand upon current presurgical testing practices, positively impacting the surgical and inpatient experience of the patients.
References
Yamikan, H., Ahiskali, G. N., Demirel, A., & Kütükcü, E. C. (2025). The effects of exercise-based prehabilitation in patients undergoing coronary artery bypass grafting surgery: a systemic review of randomized controlled trials. Heart & Lung: The Journal of Acute and Critical Care, 69,41-50. https://doi.org/10.1016/ j.hrtlng.2024.09.007
Harik, L., Perezgrovas-Olaria, R., Jr Soletti, G., Dimagli, A., Alzghari, T., An, K. R., Cancelli, G., & Gaudino, M. (2023). Sex differences in coronary artery bypass graft surgery outcomes: A narrative review. The Journal of Thoracic Disease 15(9), 5041-5054. https://doi.org/10.21037/jtd-23-294
Society of Trauma Nurses TraumaCon 2025
Kansas City, Missouri
By: Jennifer Bath, DNP, RN, AGCNS-BC, CBIS, TCRN, CEN
I had the honor of presenting on Diaphragm Pacemakers and attending TraumaCon this April. Some of the sessions I attended included Mission Critical Medicine: Operating in and on Multidisciplinary Teams.
This session discussed high performance of communication between routine and critical communication. Issues arise in the MDT when half of the team is in routine communication mode while the other half is in critical communication mode. During times of critical communication, messages should be brief/ concise, projected, assertive and unemotional. How a team moves between routine and critical communication determines how well the team performs. Examples of times when teams move from routine to critical communication include alerts such as rapid responses, codes, trauma, strokes, etc. The speaker talked about the “sterile cockpit” that aviation uses. It is illegal to talk about anything other than flying the plane when the altitude is <10,000 feet as that is when three critical things are happening: the plane is taking off, landing, or about to crash. An example we use in trauma is when the patient arrives, someone yells quiet to the room, so everyone is focused on patient care and no side conversations are happening around the patient.
How a team signals the move back to routine communication after critical communication has occurred varies, it could be physical sign such as moving the patient from the regular room to ICU, or the patient moves from the trauma bay to the OR; a signal such as “all clear” or a transition of leadership like the code team turning over care to the ICU team. The Department of Surgery utilizes TeamSTEPPS as our communication methods, which was born out of crew resource management, from the aviation industry.
The Global Burden of Trauma.
This session was a panel of international trauma program directors from Lebanon, Norway, Australia/New Zealand, Brazil, South Africa, and Thailand, who presented on what their trauma programs entailed and trauma statistics for their country. It was eye-opening to see some of the access to care issues in some countries, such as Australia, where they only had one Level I trauma center for the entire country. Other issues some countries faces are lack of specialty consultants such as neurosurgery or lack of technology and equipment that we take for granted, such as dedicated OR space and sterile rooms/equipment.
Continued on next page
Family Perspectives in Trauma: The Moments that Matter.
A very emotional presentation by a man whose entire family (wife and three children) were T-boned by a driver with known seizure history driving on a suspended license. His wife and 5-month-old daughter went to one trauma hospital while his 5- and 3-year-old sons went to another one. He spoke of the warring priorities of which hospital to go to first, making decisions to withdraw care and donate the organs of his 5year-old son and 5-month-old daughter, and all the things that the care team does not think about beyond the patient. In his case, it was the lack of ability to go between the two hospitals quickly due to travel times of 30-40 minutes and having children that are dying that you want to be with at the same time but are not able too. He spoke about what we could do as providers and humans. That we should not ask what to do for them, just do it. For example, friends and neighbors kept calling about doing yardwork, shopping, and cleaning the house. He did not have the bandwidth to make those decisions at the time. He said the greatest help was those who just showed up and mowed the lawn, cleaned the house, came with cooked meals/groceries, etc. He also mentioned that he was in a state of “analysis paralysis” where he could not make decisions at first because there was so much information coming at him from so many people at one time. He said, we as providers, need to remember that the family is dealing with so many overwhelming issues on the worst day of their life, so we need to be patient with them and their indecisiveness, provide support people, and just be compassionate.
Pressure Injury Reduction in the Trauma Population: A Performance Improvement Project.
This session was a project presentation of a trauma center that has a goal of decreasing HAPIs by 50% in FY24. They started by pulling together a multidisciplinary team that met biweekly. They first identified opportunities for improvement with a focus on prevention. They performed a gap analysis and then developed a multimodal approach to addressing the issue. They reached their goal of decreasing HAPIs by 50% and device related pressure injury rates dropped 65%. They engaged bedside staff by having Skin Champions, Unit councils, and staff seeing the positive results of the program with data presented at monthly staff meetings. The interventions included:
1. Photographing all high risk for pressure injury areas on admission by nursing (they had EPIC and nurses had iPhone to photograph with).
2. Placing turn wedges in all inpatient rooms.
3. Creating wound care guidelines
4. Created high risk criteria for patients and those who met the criteria got daily photos uploaded to the EHR.
5. Camera cards were posted on the doors of the patients’ rooms that required daily photos.
6. Prevention skin rounds were done weekly on all ICUs that included the Wound Care Team, Clinical Nurse Specialist, and Unit leadership (unit director, operation manager or CTL).
7. Created a pressure injury prevention (PIP) sheet as part of nursing education and it was also posted in each ICU and on patient room doors for all high-risk patients.
Management of the Transgender Trauma Patient.
This session discussed the important clinical concepts that one must know when caring for a transgender (TG) trauma patient. Males that transition to females are put on high doses of estrogen which increases their baseline risk for VTE even before they have a traumatic injury. Trauma significantly increases VTE risk for any person. Females transitioning to male get a lot of spironolactone which is a diuretic, and can volume deplete a patient before they have trauma, which can lead to even more volume loss. 70% of transgender patients have experienced discrimination by healthcare providers in a healthcare setting. 1/3 of TG patients postpone or avoid seeking care due to the fear of being discriminated against, and 1/5 of TG patients have not disclosed their TG status to the healthcare providers caring for them.
Potential problems with TG Trauma patients include:
Less likely to have insurance, four times more likely to live in poverty,
Often have no medical records/history available
Often registered under wrong sex at birth which can be an issue especially with blood transfusions
Staff comments such as not respecting patients’ chosen pronouns on purpose.
Increases risk of intimate partner violence, assault and suicide leading to traumatic injuries. <60% TG population are victims of assault and >40% have attempted suicide at least once in their life.
>42% have a history of non-suicidal self-injury
Vocal cords may be surgically altered, affecting airway management.
When caring for a TG patient it is important to establish trust, asked them respectfully what their chosen name, gender, and pronouns are during the initial encounter. Contact their PCP or HCP to determine how far they are in their transition and if their family is aware of their TG status. DO NOT disclose TG status without patient’s permission. Screen for abuse at every encounter. When getting history, be sure to include if they are on hormone therapy, have silicone implants, surgeries to transition, any possible undiagnosed medical comorbidities, and if there is any family/social support and if so, are they aware of TG status.
Jen Bath presented on IGF-1 as a biomarker for symptom severity in adolescent traumatic brain injury and on IGF-1 as a biomarker for symptom severity in adult traumatic brain injury.
CPHQ Certified– Director Infection Prevention & Control Maimuna Jatta, MSN, RN, CIC, CPHQ on her recent achievement of her Certified Professional in Healthcare Quality (CPHQ) certification! Earning a CPHQ certification demonstrates our Carilion Clinic values of Commitment of her profession, and also a commitment to healthcare quality and safety. Certification is associated with decreasing adverse events, reducing infection rates, and improving patient safety & outcomes.
Thank you for your commitment to our community and improving quality care for our patients!
Congratulations on this outstanding achievement!
Please join us in celebrating Ellen Harvey on her well-deserved induction into the AmericanAcademy of Nursing 2025 Class of Fellows-one of the highest honors in the nursing profession.
Ellen’s unwavering dedication to advancing nursing practice, her leadership in clinical excellence, and her commitment to improving patient outcomes have made a profound impact on our organization and the broader healthcare community.
This prestigious recognition reflects not only her individual achievements but also the strength of nursing innovation and expertise we’re proud to support.
Congratulations, Ellen, and thank you for your continued contributions to nursing and patient care!
April 2025 - June 2025
Bond, D. (2025, April 17). STOP surgery and trauma opioid project. Carilion Research Day. Virtual
Bath, J. (2025, April 17). Comparison of traditional simulation to non-traditional simulation format in trauma education. Carilion Research Day. Virtual
Jetta, M. (2025, April 17). Whole genome sequencing unravels the Mystery. Carilion Research Day. Virtual
Davis, Y. (2025, April 17). Who are the nurse detectives?? Surgical clinical reviewers. Clinical Research Day. Virtual
Bond, D. (2025, May 19-21). Buprenorphine: Not just for addiction. AACN National Teaching Institute & Critical Care Exposition (NTI). New Orleans, LA.
Bath, J. (2025, April 23-25). Pacing: It’s not just for the heart! Diaphragm pacing review. Society of Trauma Nurse’s Annual TraumaCon. Kansas City, MO.
Beels, S., Martin, M. (2025, June 4–5). Igniting Carilion Clinic’s vascular surgery ‘stop smoking’ initiative. Society of Vascular Nursing Vascular Quality Initiative. Society of Vascular Nursing Vascular Quality Initiative. New Orleans, LA.
Bath, J. (2025, June 12-14). IGF-1 as a biomarker for symptom severity in adolescent traumatic brain injury and IGF-1 as a biomarker for symptom severity in adult traumatic brain injury. Carolinas/ Virginias Chapter of the Society of Critical Care Medicine’s annual symposium. Charlottesville, VA.
Bramblett, H., Littleton, B. (2025, April 9-10). Reducing readmissions: One discharge at a time. Virginia nurses Association 2025 Spring Conference, Empowering the Nurse. Virtual
Manchin, K., diamond, A. (2025, June 16-18). Engaging travel nurses to improve infection prevention bundle compliance and HAI reduction. Association for Professionals in Infection Control and Epidemiology. Phoenix, AZ..
Beels, S., Walls, K., Tokala, M. (2025, April 10-12) Using a Combined Implementation of stress first aid and the 4-A Models to Improve Resiliency (6SICU). Preventative Cardiology Nurses Association 31st Annual Cardiovascular Nursing Symposium. Orlando, FL. (Nightingale Award)
Beels, S., Martin, M., Sydenstricker, E. (2025, June 45). Improving awareness & elimination barriers to discharge medication guideline compliance. Society of Vascular Nursing Vascular Quality Initiative. New Orleans, LA. (selected people’s choice award at conference)
Beels, S., Martin, M., Sydenstricker, E. (2025, June 45). Improving awareness & elimination barriers to discharge medication guideline compliance. Society of Vascular Nursing Vascular Quality Initiative. New Orleans, LA. (selected best poster at conference)
April 2025 - June 2025
Poster PresentationsArt & Science of Nursing Showcase
Cindy Ward, DNP,APRN-CNS, RN-BC, CMSRN,ACNS-BC was selected as a Fellow of theAcademy of Medical Surgical Nurses!
Bramblett, H., Littleton, B. (2025, May –9). Reducing readmissions: One discharge at a time.
Whitehead, P., Harvey, E. (2025, May 5-9). Optimizing your CNS professional journey. (Voted People’s Choice)
Beels, S., McCaffery, S., Evans, T. (2025, May 5-9). Combining stress first aid and the 4-As models to improve resiliency.
Beels, S., Walls, K., Tokala, M. (2025, May 5-9). Using a Combined Implementation of Stress First Aid and the 4-A Models to Improve Resiliency (6SICU).
Beels, S., Martin, M., Sydenstricker, E. (2025, May 5-9). Improving awareness & eliminating barriers to discharge medication guideline compliance.
Andrews, S., Blakenship,, S., DePriest, M., Gillenwater,A., Fish-Huson, C., Kotz, C., Stover, S., Sutphin, C. (2025, May 5-9). Unlocking learning styles: A nurse resident’s key to success.
Contact Chris FishHuson with your ideas so that we can find funders to support you!
Using a Combined Implementation of Stress First Aid and the 4-A Model to Improve Workplace
Wellness: A Pilot Quality Improvement Study
By: Katelin Walls, MSN, RN-III, CNL, CCRN-CSC & Suzanne Beels, MSN, RN, AGCNS-BC, CCRN
Project Aim
The purpose of the CVI Retention Committee Quality Improvement (QI) project is to determine if using the Stress First Aid (SFA) model will decrease the impact of stress and burnout for Cardiac Surgery
ICU (CSICU) employees. The CVI Retention committee aimed to improve overall well-being and sense of moral distress as measured by the modified MMD-HP and SFA ProQOL survey.
Current State of Knowledge
Review of Literature
The CVI Retention Committee utilized the Carilion Schwartz Center (SC) as a resource to jumpstart this QI project. The SC started SFAeducation at Carilion. The CVI Retention Committee also used the Carilion Library and reviewed theAmericanAssociation of Critical Care Nurses (AACN) professional organization to expand our literature review. The team included literature written within the last ten to fifteen years.
Moral Distress/ Moral Residue
Moral Distress is defined as "a phenomena that occurs when nurses cannot carry out what they believe to be the ethically appropriate action because of internal (personal) or external (institutional) constraints" (Epstein & Hamric, 2009). Initial distress occurs the moment a situation unfolds. Reactive distress, or moral residue, are the lingering feelings after the acute phase. Moral residue is more challenging to characterize because it does not have a time frame or pattern, but it does exist and is experienced through feelings of anxiety, depression, professional avoidance of patients, or leaving the profession entirely. Moral Residue Crescendos is the interaction between moral distress and moral residue (Epstein & Hamri, 2009).
Once a healthcare professional experiences a morally distressing situation, they feel a high level of moral distress. After some time, the moral distress feeling de-crescendos, or decreases, until the healthcare professional experiences another morally distressing scenario (in which moral distress spikes again). However, the healthcare professional is never able to decease back to their baseline moral distress level (Epstein & Hamric, 2009).
Resilience
Many interventions have been suggested to reduce or decrease moral distress such as educational interventions, enhancing the ICU environment with ethics committees, include debriefings after morally charged events, adding multidisciplinary rounding, and assisting individuals in building stronger coping skills in work environment (Abbasi, Ghafari, Shahriari & Shahgholian, 2019). These types of interventions promote resiliency through mindfulness-based stress reductions, self-reflections, cognitive flexibility, and improved communication.
MMD-HP
Measure of Moral Distress- Healthcare Professionals (MMD-HP) scale. This scale is an adaptation of the Moral Distress Scale- Revised (MDS-R). The MMD-HP scale includes 27 items and is usable by all healthcare professionals in any setting.
SFA ProQOL
Stress FirstAid Professional Quality of Life scale. This scale is intended for any “helper” (medical professional, first responder, service workers, etc.). It is utilized as a screening tool for “helpers” to measure the impact of providing care on their personal wellbeing, positive or negative (Watson & Westphal, 2020). The higher the reported score, the greater the level of stress/trauma the individual experiences (Watson & Westphal, 2020). & Westphal, 2020).
Schwartz Center Rounds Stress First Aid
The foundation for the SFAmodel is the 7 C’s- Check, Coordinate, Cover, Calm, Connect, Competence & Confidence. Stress FirstAid, the 7 C's, is a framework that healthcare workers can utilize to improve recovery from stress reactions (Watson & Westphal, 2020). The model aims to help us identify stress reactions in self and amongst others in a continuum, and to help reduce the long-term effects/problems of untreated stress. The model focuses on “five evidence-informed factors that help people recover from stress and adversity” (The Schwartz Center, 2022). The factors include safety, calm, connection, self-efficacy, and hope.
AACN 4- A Model: American Association of Critical Care Nursing 4-A Model. Ask, Affirm, Assess, & Act
To improve healthcare workers professional life by decreasing and alleviating moral distress by
Continued on next page
Description of Population & Benefit
Employees of CSICU, all experience, skill, education, and age levels will comprise the population for this project. Please refer to the project aims; increase “this facility helps me deal with stress and burnout” score, decreased moral distress & improved sense of well-being and resilience.
IRB Determination
The Carilion Clinic Institutional Review Board (IRB) has determined that the above reference project does not meet the definition of human subjects’research as outline in 45 CFR 46.102(d), and therefore does not require IRB oversight or approval. This determination has been made because the intent of your study is not to contribute generalizable knowledge but rather is designed to providing coping and resilience skills to improve overall wellness of the nursing staff to decrease turnover and improve job satisfaction at Carilion. As such, the study qualifies as a quality assurance/quality improvement activity and not as human subject’s research.
Methods & Procedures
April of 2022 pre-project surveys were distributed to participating departments (MMD-HP and SFA ProQOL). May 27th, 2022, Carilion Schwartz Center SFAeducation was launched on Cornerstone for all nursing staff and education was provided on the AACN 4-AModel. CVI Retention committee held their first (stationary) town hall June 3rd, 2022. CVI senior directors, Chaplains, Employee Assistant Program (EAP), Carilion Wellness, Principal (retirement education and information), Schwartz Center Rounds, Grief Counseling, Morningside Urban Farm, and the TRUST team participated in Town Hall and provided education about each organization/entity for staff to attend. The purpose of the Town Hall was to disseminate further education about the SFA model and the 4 A Model, educate nurses about Carilion resources, and to create an environment where nurses’ feelings were validated. CVI Retention Committee also began introducing monthly Newsletters (CV-I Care Newsletters) in July 2022 which incorporate education and highlighted
Continued on next page utilizing the 4A's (Savel & Monroe, 2015). 1.Ask-the goal is to be aware of moral distress presence. 2.Affirm- validate the feelings and perceptions of the individual or coworkers. 3.Assess- the goal of this stage is to prepare an action plan. 4.Act-create and implement an action plan to preserve the individual's integrity and authenticity. The acting stage will vary by individual.
events in the Roanoke Valley and Carilion resources that promote resiliency, wellness and decrease moral distress.
Assessment & Data Collection
Since the beginning of this project inApril 2022, the CVI Retention Committee has since created monthly Since the beginning of this project inApril 2022, the CVI Retention Committee has since created monthly newsletters, re-administered MMD-HP & SFAProQOLsurveys every 6 months and have hosted quarterly mobile town halls where team members round to every CVI unit with therapy dogs, snacks, and SFAand moral distress education.
Findings & Discussion
Implementation of SFAand 4-As skills improved resiliency and the unit benefited through decreased turnover. Levels of distress and resiliency were measured through use of the MMD-HP scale and Stress
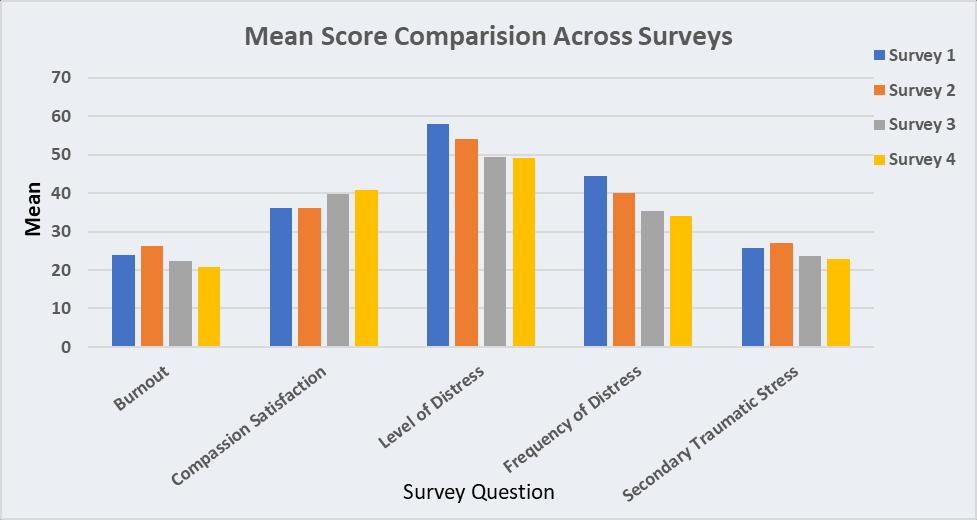
FirstAid ProQOL. The higher the reported score, the greater the level of stress/trauma the individual experiences (Watson & Westphal, 2020). Aseries of four surveys across two years were completed by frontline employees on the CSICU (6 South ICU), 6 months apart. The results are as follows:
Continued on next page
Key Observations:
Burnout generally increases from Survey 1 to Survey 2, but decreases in later surveys. Compassion satisfaction shows a positive trend, with higher scores in Survey 3 and Survey 4. Distress scores and MMDHP frequency show high variability, especially in Survey 1 and Survey 2. Secondary traumatic stress appears lowest in Survey 4, while it is moderate to high in the earlier surveys.
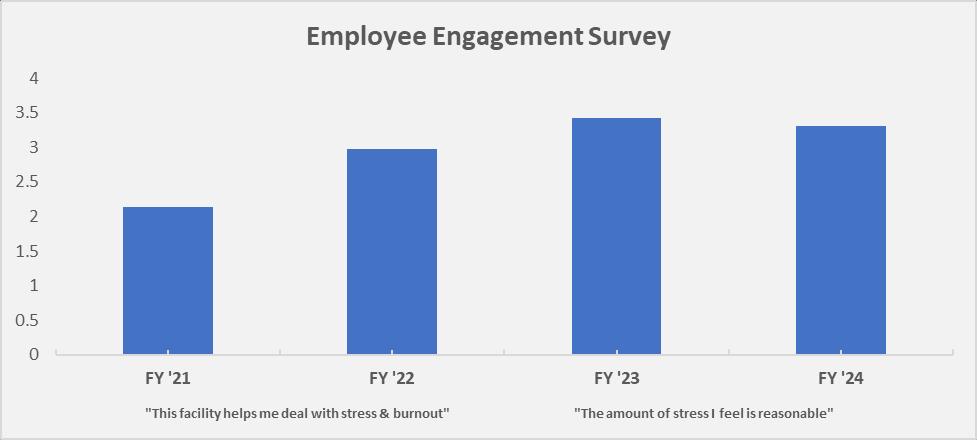
Employee Engagement Survey
“This facility helps me deal with stress and burnout” “The amount of job stress I feel is reasonable”
Continued on next page
The annual employee engagement survey used a numeric rating scale of 0-5. The statement specific to this project was “This facility helps me deal with stress and burnout”. In fiscal year (FY)2021, the ICU scored 2.13. In FY2022, the score improved to 2.97. Unfortunately, the survey question changed in 2023 to “The amount of job stress I feel is reasonable”, so an equal comparison could not be made. The score for FY2023 was 3.42, decreasing to 3.31 in 2024. This project reflected an overall net improvement across 3 years.
Limitations
These surveys were anonymous, and the team was not able to ensure that the same nurses participated in both surveys. Employee attrition rates, travel nurses, new hires and patient unit acuity impacted survey completion. Lastly, some surveys were not fully completed, which impacted data collection.
Implications for Change
Implementation decreased feelings of stress and burnout and improved feelings of support from leaders. A nurse said to project leaders, “it is like you’ve become our best friend”. The staff verbalized feelings of support when they are having a difficult event along with grace when they needed time for decompression. Morally distressing situations are common in healthcare. Educating employees on prompt identification of moral distress and appropriate resource engagement decreased feelings of stress and burnout. Town Halls provided an opportunity for staff to verbalize their needs to decision makers. Many discussions occurred on how nurses viewed and alleviated moral distress and what steps they could take to become better self-stewards. Learning to approach and support one another during adversity took practice and grace to accomplish. It continues to be a work in progress. Future work includes continued education, development of onboarding programs, rollout to other areas of the facility, ongoing Town Halls, monthly newsletters and evaluation of staff needs.
Conclusion
This QI project lends credence to the benefits of educational and interactive (Town Hall) interventions. The team successfully provided education about moral distress to nursing staff in CVI, however, there is room for improvement through additional educational opportunities, town hall events, and surveying cycles.
Morally distressing situations are hard to eliminate in totality. While the team did not achieve statistical significance in all surveying criteria, current literature proposes that prompt identification of nurses’ moral distress and appropriate resource engagement can both decrease moral distress levels and frequency. This QI project has improved how CSICU nurses view moral distress, how they alleviate their moral distress, and to become better self-stewards. The team continues to host quarterly Town Hall’s, produce monthly newsletters with education about moral distress and SFA, and continues to promote resiliency in nursing staff.
Continuous use of SFAand the 4-As framework was vital in fostering an accepting and inclusive culture. Initially, staff experienced discomfort and hesitation when approaching one another. Incorporating case studies could have enhanced their confidence and ease in discussing stress levels with peers. Senior Leadership played a pivotal role by modeling desired behaviors, increasing visibility on the frontlines, managing budgets effectively, and actively supporting these initiatives.
Lessons learned
Significant knowledge gaps regarding hospital resources were identified. To address this issue, it was essential to develop and provide staff with a comprehensive resource list including numbers for crisis support. Integrating both programs into onboarding education was necessary.
Reference List
Abbasi, S., Ghafari, S., Shahriari, M., & Shahgholian, N. (2019). Effect of moral empowerment program on moral distress in intensive care unit nurses. Nursing Ethics, 26(5). Retrieved from 10.1177/0969733018766576
Epstein, E. G., & Hamric,A. B. (2009). Moral distress, moral residue, and the crescendo effect. The Journal of Clinical Ethics, 20 (4).
Epstein, E. G., Whitehead, P. B., Prompahakul, C., Thacker, L. R., & Hamric,A. B. (2019). Enhancing Understanding of Moral Distress: The Measure of Moral Distress for Health Care Professionals. AJOB empirical bioethics, 10(2), 113–124. https://doi.org/10.1080/23294515.2019.1586008
Kidd, M., Grove, K., Kaiser, M., Swoboda, B., & Taylor,A. (2014).Anew patient-acuity tool promotes equitable nurse-patient assignments. American Nurse Today. 9(3). https://www.myamericannurse.com/ wp-content/uploads/2014/03/ant3-Workforce-Management-Acuity-304.pdf
Molazem, Z., Tavakol, N., Sharif, F., Keshavarzi, S., & Ghadakpour, S. (2013). Effect of education based on the “4AModel” on the Iranian nurses’moral distress in CCU wards. Journal of Medical Ethics and History of Medicine, 6(5). Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3740193/
Samoya,A. (2019). Creating healthy work environments:An evidence-based toolkit for nurses. Retrieved from https://www.aacn.org/~/media/aacn-website/nursing-excellence/healthy-work-environment/ hwetoolkit.pdf?la=en
Savel, R. H., & Munro, C. L., (2015). Moral distress, moral courage. American Association of Critical-Care Nurses, 24 (4). Retrieved from http://dx.dol.org/10.4037/ajcc2015
Stamm, B. H. (2022). Professional quality of life: Compassion satisfaction and fatigue (ProQOL). Retrieved from ProQOL.org
The Schwartz Center. (2022). What is stress first aid? Retrieved from https://www.theschwartzcenter.org/ stress-first-aid-private/
Ulrich, B., Barden, C., Cassidy, L., & Var-Davis, N. (2019). Critical care nurse work environments 2018: Findings and implications. Critical Care Nurse, 39(2), 67-84. Downloaded on 6/25/2020 from http:// aacnjournals.org’ccnonline/article-pdf/39/2/67/116850/67
Watson, P., & Westphal, R.J. (2020). Stress FirstAid for Health Care Workers. National Center for PTSD.
C L A S S E S
Basic Research for the Healthcare Professional NR-CE333L
October 16* 8A - 12P December 18 12P - 4P
NR-CE165L Leadership Tips & Tools for Coaching Staff August 21 ~ 2P - 4P
NR-CE373L Research Methods & Statistics October 21 ~ 12P - 3P
NR-CE377L Practical Healthcare Applications October 23 ~ 1P - 4P
*Class will be held in the Seay Center Class Room E
“The World is a book, and those who do not travel read only a page.” – Saint Augustine
Palm
United Kingdom
Lake Buena Vista
Williamsburg
Natl. Harbor, MD
Greenville
Nottingham
Anaheim
Aurora