




It is a real pleasure to welcome you to the second edition of the HIEDA Journal. The positive feedback and enthusiasm following our first edition affirmed the importance of knowledge-sharing amongst professionals in the health in education sector.
A strong theme running through this edition is mental health and emotional resilience – from proactive support to digital mindfulness We also explore the evolving roles of health professionals, with perspectives on international students, strengthening the bridge between health centres and boarding houses, and how technology is shaping our practice
At HIEDA, we champion a sense of belonging for everyone working in health roles within education – especially for those in smaller teams or working alone. We hope this Journal helps nurture that connection and that you find it helpful in your role
We are incredibly grateful to all contributors for sharing their expertise If you would like to submit article ideas for our next edition, or if you have any queries, please do get in touch via info@hieda org uk

Bethan Hudson MTIOB, Director, HIEDA
Bethan is Director of BAISIS and HIEDA and leads on all consultancy and INSET services across BSA Group as Executive Director, Consultancy Before joining BSA in 2017, Bethan was a pastoral lead and houseparent, in state and independent, coeducational and girls’ and UK and international schools Bethan is a keen advocate for youth opportunity and social mobility worldwide and believes confident, well trained, and supported practitioners can be a positive force for young people and their development
Sylvia Meadows, Lead Nurse, Oundle School
When I arrived as Lead Nurse in June 2019, the team had experienced no manager for more than two years. The pupils had received excellent nursing care. However, due to being short-staffed, there was limited opportunity to reflect and develop a service that ensured pupils’ needs were fully met. Not long after my arrival, Covid hit, delaying any planned changes.
On our return to school, we lost more staff and morale was low. We had to provide a service in stressful times. Over time, we recruited four new nurses When time allowed, our team embraced the challenge of reviewing our service. We asked ourselves what we did well, what could be better, and where could we make a difference to the pupils’ school experience? We set out to build a new strategy for the department, aiming to ensure our pupils felt they were being supported in their physical, emotional and social wellbeing
We identified the importance of receiving buy-ins from the wider community From the senior leadership team to admissions staff, and from House Masters and Mistresses to Matrons, everyone offered their services Working groups were held, ideas and opinions were shared, and we redesigned our service
We reviewed our protocols and policies, started with our new joiners, realising the importance of them receiving information in a timely manner at the start of their time with us. From this evolved the introduction of House Nurses. Each House now has a nominated nurse who is the contact for parents, pupils and staff. The nurse arranges new joiner medicals, visiting the pupils in their own House They keep care plans up to date, ensure medication is correctly dispensed, offer teaching and well-being sessions for staff and pupils, and help to support and educate pupils on how to look after themselves We are all passionate about promoting physical, mental and social wellbeing that is crucial for individual development
At Oundle, we have a full-time Emotional Wellbeing Team. When I arrived, there was little synergy between the two departments Over the past 18 months, we have worked closely to ensure that we provide a cohesive service to our pupils, offering confidential advice, counselling and support services, responding promptly to pupils’ needs The two departments meet regularly to reflect on cases, ensuring both sides are kept well informed. I have also joined the Pastoral Select Committee and the Child Protection Welfare Group, and both meets regularly to ensure the Health Centre has a voice, as well as keeping us up to date with any current concerns.

We have come a long way We now have a presence around school, teaching in Learning for Life, providing pitch-side first aid, and being involved in educational days for all year groups as required The team was delighted to receive such positive feedback following our inspection for the Seacole standard in February, and proud at subsequently being named HIEDA’s Health and Wellbeing Champion for all-round Excellence Award 2024
Recently, the ISI inspectors arrived to carry out a routine inspection Usually, this is a time when everyone feels anxious and nervous as we all want to show off our school in the best possible light After all the hard work, dedication and commitment the team has shown over the past couple of years, we were immensely proud to demonstrate with evidence that Oundle School Health Centre is a workplace that demonstrates excellent health and wellbeing provision. We provide a high standard of care, addressing the physical, mental and social health and wellbeing of our pupils

Working groups were held, ideas and opinions were shared, and we redesigned our service.
The inspectors noted how we as a school promote the wellbeing of the children We were compliant with, and exceeded, all National Minimum Standards There were positive comments about the full and enriching boarding experience, which is something that permeates pastoral care across all the Houses The staff, parent and pupil questionnaires were incredibly positive Many pupils filled in the questionnaire, and one thing that made me happiest was that most pupils reported that they are happy at school
Sylvia Meadows, Lead Nurse, Oundle School
Sylvia trained as a Registered General Nurse and Midwife in Edinburgh Her career has ranged from selling anti-inflammatory drugs for a large pharmaceutical company to owning a children’s shop But she missed the people contact and job satisfaction she enjoyed as a nurse Sylvia began living and working with her family in a boarding school environment 15 years ago She has been a School Nurse, Matron and Housemistress, and in 2019, just before Covid, she became Lead Nurse at Oundle School Pupil welfare is at the heart of life at Oundle and Sylvia’s department has received two prestigious accolades from HIEDA

the importance of first-response provision and training
In an emergency or situation that requires medical intervention, statistics show it is unlikely that a medical professional will be the first on scene. First-response management is therefore critical, highlighting the importance of all school staff being well informed about the medical conditions of the children in their care. In addition, it has been widely reported that children’s mental health and wellbeing are currently affected by factors such as social media, with the Covid pandemic posing a new challenge for schools. It is clear that a whole-school approach to health education is vital to ensure the most positive outcome for these young people. It is my aim to always give time to hear the child’s voice and to be an advocate for their health needs in school.
As a dual-trained nurse (adults and children) with more than eighteen years’ experience, my passion is working within the independent education sector to support children as they navigate school life and various stages of their development. To offer this support successfully, all staff in schools should be equipped with the tools and knowledge to deal with health education

The term ‘health education’ is broad. It includes the tools needed to provide a first-aid response, knowledge of signs and triggers of potential mental health concerns, plus the skills to support medically when needed. My vision is to improve awareness of this need – and to
develop standardised processes within independent school health care to provide non-medically qualified staff with the confidence and knowledge to support pupils. I have worked in several independent schools, varying in size and with different approaches to health. My view is that a robust, integrated education and health service is imperative.
Our Health and Wellbeing Centre is a safe space for children to come if they feel vulnerable, or if they need or want to talk freely in a nonjudgemental space
A medical practitioner will not be present at all times in a school setting. It is therefore crucial that all staff feel confident to make the decisions that need to be made. At the independent school where I work, there are a range of chronic medical conditions among the pupils, aged from two to 19. These children require specialist care to ensure staff can safely support their day-to-day wellbeing in school. Our Health and Wellbeing Centre networks extensively with medical professionals in the area, across several specialities, to support our children and parents in the best possible way should their expertise be required. I have put in place a ‘Health and Wellbeing Centre Staff Medical Guide,’ which contains key information and guidance that is easy to follow, specifically tailored for our school setting. Unfortunately, such a guide does not guarantee that everyone will know what to look for and what to do in a medical situation. This is why we also focus on our first-aid training, to ensure there is a qualified member of staff available in all areas of the school.
Nationally, mental health is a growing epidemic within our schools, and it is critical for staff to recognise the signs to prevent episodes that require medical intervention, such as self-inflicted injuries. Along with physical symptoms, children could be feeling several emotions, from anxiety to depression, and we work closely with our GP practice
which offers excellent support and resources for the Health and Wellbeing Centre team. Eating disorders can also result in physical symptoms that require careful management. We work closely with staff, including teachers, who may be able to identify potential signs, and the catering team, who meet the nutritional needs of the children. Our Health and Wellbeing Centre is a safe space for children to come if they feel vulnerable, or if they need or want to talk freely in a non-judgemental space.
I continue to promote the importance of hearing the child’s voice and consider new ideas and opportunities to improve by delivering a health presentation to all staff at the start term. This is an opportunity to share tailored health information to all staff together, continuously supporting the medical needs of our children at school. I am currently in the process of developing a ‘Mental Health and Wellbeing Centre Staff Guide’ and consider new ideas and opportunities to improve.
We look to learn from all situations that may arise, and we also embrace feedback from our staff, parents and children. Recently, there was a situation that required an immediate first-aid response from a House Parent at the school where I work. The colleague was composed, calm and handled the situation in a manner that resulted in glowing feedback from all involved, including the child and hospital staff. This is all that we can ask from our colleagues: to provide the best possible response to care, in unpredictable and unexpected situations. We must help to prepare them for such situations, empowering them with knowledge and with the confidence to act in the best interests of the children in our care.

Camilla Walter, Head of Health and Wellbeing Centre, Stonar School
Camilla trained at Nottingham University as an adult and children’s nurse. She has nearly 20 years’ nursing experience within both the acute and community setting. In recent years, Camilla has worked full-time within school settings, developing high standards of healthcare to support parents, pupils and staff. With an emphasis and ethos on listening to the child’s voice, she supports and advocates pupils’ physical and emotional wellbeing. Camilla demonstrates a clear passion for improving healthcare within a school setting. This includes raising awareness, enhancing clear processes, and building strong connections with fellow healthcare professionals to support children’s needs, maintaining and improving healthcare.

Georgie Sullivan, School Nurse, Queen Anne’s School
Mental health is a state of wellbeing that enables people to cope with the stresses of life, realise their abilities, learn and work well, and contribute to their community. It has intrinsic and instrumental value and is integral to our well-being. (WHO, 2022)
Mental health and wellbeing are critical considerations in pastoral care provision in our independent day and boarding girls school The transition from home life to the school environment can be particularly challenging for young people, especially in a setting where boarding and day students coexist Bohnenkamp, J H , Stephan, S H , Bobo, N , (2015) estimate that school nurses spend 33% of their time addressing student mental health issues
Our students face significant challenges as they navigate the complexities of growing up, tackling academic pressure, social dynamics, family issues and personal identity exploration. Any or all of these can significantly impact their mental and emotional health.
For boarders, being away from home, family and familiar surroundings can lead to feelings of loneliness, homesickness and anxiety. Coping strategies they might employ at home may be less effective in a new surrounding, particularly where language creates a further barrier. Living with peers can be great but can also further contribute to stress and mental health issues.
Fostering a community where students feel comfortable discussing mental health can reduce the stigma associated with seeking help. Peer support groups and mental health education can empower students to take charge of their wellbeing. The Health Centre plays a critical role in managing the mental health of students, acting as a bridge between healthcare and education. By providing early identification and intervention, the school nurse can address mental health concerns before they escalate. This begins with creating a supportive and welcoming environment, where students feel comfortable discussing their feelings. The recently refurbished Health Centre building includes a student designed ‘quiet room’ and has been a welcoming hub for students with anxiety conditions this year. It provides them with a quiet and relaxing place to recharge their confidence and positivity before returning to lessons.
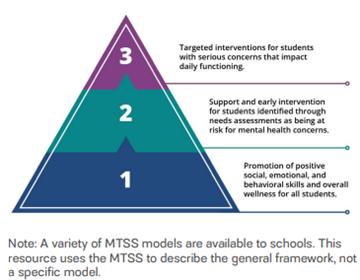
A multi-tiered programme of support, as described by CDC (2023), underpins the care provision for our students.
Queen Anne’s proactive wellbeing strategy includes regular check-ins with all students, prompted by the school’s award winning weekly ‘Wellbeing Survey’. These inform conversations which help the team monitor students’ wellbeing and identify those who may need additional support. When signs of anxiety, possible depression or stress are detected, the Health Centre can offer immediate care and refer students to school counsellors or external mental health professionals. Click here for an example of the weekly questionnaire. The weekly questionnaire is sent to students every Monday, with a follow up for anyone who missed it on Tuesday mornings. This proactive measure aims to assess students’ physical, mental and overall wellbeing, addressing concerns ranging from sleep and nutrition to the challenges they face each week. This initiative is not just a survey, it’s a mechanism that offers immediate support for those who need it.
Students identified as needing additional support complete a Pastoral Student Support Plan (PSSP) which, with the students’ consent, is then shared with designated safeguarding leads (DSLs), academic staff, tutors, parents, counsellors and boarding House Parents. Students are, of course, always told that if we have safeguarding concerns, confidentiality is not something we can commit to. The PSSP helps students and the adults they trust to identify some of their stresses and coping mechanisms. This is monitored by the Health Centre team on a student voluntary basis, in that if a student declines to participate in further follow up, this is communicated to those involved. We also encourage students to make use of available online support organisations. Our experience has taught us to offer only two or three organisations initially. Giving students too many options is overwhelming and has a much lower likelihood of uptake.
Our locally commissioned online support comes through Tellmi. Tellmi (2024) is a digital mental health service that delivers anonymous, pre-moderated peer support with counsellor intervention to young people aged 11-plus. By providing a safe space where young people can help themselves by helping each other, they can also discuss their challenges and provide each other with support, advice, and empathy. This has been evidenced to improve emotional resilience, social functioning and overall mental health outcomes. To find out more, please visit: tellmi.help/what-istellmi
Counsellors play a crucial role for both day and boarding students, providing essential targeted support for students’ mental, emotional and social wellbeing. Their presence is key in fostering a healthy school environment where students can thrive academically and personally. Students read and sign a consent form to counselling which has allowed us to maximise attendance at counselling sessions, making full use of our counselling slots. Where a student’s care needs extend beyond our school abilities and resources, we refer quickly to local children’s services.
In a boarding environment, we aim to foster a supportive community where students feel safe and valued. Schools with effective pastoral care must provide access to mental health resources, including counsellors and wellness programmes, to help students navigate the emotional demands of boarding life.
Regular check-ins, both formally through counselling sessions and informally through house parents or tutors, can help identify and address issues early.
Education and prevention are vital. Understanding mental health resources early builds resilience and the ability to utilise those resources. NIMH (2020) note that early treatment can help prevent more severe, lasting problems as a child grows up. This is supported by CDC (2023) who describes mental health literacy as including knowledge and understanding of mental health, as well as skills that support help-seeking (for example, reaching out for mental health support when needed). The pastoral team can offer workshops on topics like stress management, healthy relationships and coping mechanisms, equipping students with tools to navigate their emotions. They can work with teachers to integrate mental health education into the curriculum, fostering a culture of awareness and understanding. The Peer Education Project (MHF, 2004) provides free resources for school assemblies and sessions focussed on mental health.
Mindfulness has become one of the supportive tools we offer to our students, with a weekly session in a six-part series talking through formal and informal mindfulness techniques. Practicing mindfulness can help students manage stress in their everyday lives and regulate their emotions and behaviours (CDC, 2023). CDC goes on to cite classroom based mindfulness education being associated with reduced anxiety, reduced depressive symptoms, reduced negative coping behaviours and increased positive coping behaviours.
Even before the pandemic, the mental and emotional needs of children were growing. Covid has exacerbated these trends (APA, 2021). As school nurses, whilst we may not be experts, and are continuously learning about the complexities of mental health, the early support we can provide to students in challenging situations is a crucial part of identifying and treating their mental health needs.
World Health Organization. (2021). Mental health: strengthening our response. Mental health (who.int) Bohnenkamp, J.H., Stephan, S.H., Bobo, N., (2015) Supporting Student Mental Health: The role of the school nurse in coordinated school mental health care. Journal of School Health, 52(7), 714-727. SUPPORTING STUDENT MENTAL HEALTH: THE ROLE OF THE SCHOOL NURSE IN COORDINATED SCHOOL MENTAL HEALTH CARE - Bohnenkamp - 2015 - Psychology in the Schools - Wiley Online Library Centers for Disease Control and Prevention. (2023). Mental health in schools. Promoting Mental Health and Well-Being in Schools: An Action Guide for School and District Leaders (cdc.gov) Tellmi (2024) Digital Mental Health Service for Young People https://www.tellmi.help/what-is-tellmi National Institute of Mental Health. (2020). Child and adolescent mental health. Retrieved from Child and Adolescent Mental HealthNational Institute of Mental Health (NIMH) (nih.gov) Mental Health Foundation. (2024). Mental health resources for schoolscaregivers and young people. Mental health resources for schools, caregivers and young people | Mental Health Foundation American Psychological Association. (2021). Bringing psychological science to school-based mental health. Bringing psychological science to school-based mental health (apaservices.org)

Georgie Sullivan, School Nurse, Queen Anne’s School
With 40 years’ experience as an adult and paediatric nurse, Georgie holds specialist qualifications in paediatric A&E, burns and plastics, and palliative care. She sought a gentler, community-focused role, and moved into school nursing, quickly discovering the vital importance of mental health support in this setting. She feels fulfilled in helping students to identify and manage their mental health needs early, fostering resilience and wellbeing. She has trained in Youth Mental Health First Aid and as a Mindfulness Instructor, and both are now key tools in her approach. She is proud to be part of Queen Anne’s School’s outstanding, award-winning pastoral team.


Excellence in health and medical provision


SEACOLE SEACOLE
STANDARD STANDARD
Join the growing list of school Health Centres gaining recognition for a high standard of treatment and care.
Find out more and register via hieda.org.uk/the-seacole-standard/


The issues encountered by students within a boarding community that can affect wellbeing are often a reflection of wider society. As experienced professionals, every one of us could write a list of the challenges that many of our boarding students may face during adolescence, and we would likely end up with broadly similar content, regardless of our geographical location or socioeconomic status.
Boarding schools have increasingly robust systems in place to ensure the safeguarding and pastoral care of students. Beyond the retrospective support mechanisms often utilised when a student’s wellbeing is already wavering, there is a tremendous opportunity within our communities to proactively address issues before they ever occur by providing students with tools to manage their own wellbeing. To this end, at TASIS England, we created a boarding wellbeing and mentoring programme
called Thrive, which we launched in August 2022.
In its pilot year, Thrive began life as a 35-week programme of topics, with accompanying lesson plans. The conceptual journey of Thrive was set in motion when we – Matt Kiely and myself – teamed up to combine our ideas. Matt, then Director of Boarding, recognised the importance of a boarding wellbeing programme, while I had previously launched a mentoring and coaching pilot in my boarding house, due to my background in coaching. We made the decision to deliver our programme via 1:1 mentoring.
The objective was to educate students around topics that would help them take ownership of their own wellbeing. Each week, students were provided with knowledge, skills and support based around key themes, ranging from sleep health to nutrition and developing healthy relationships. We
also integrated practical sessions, such as self-defence and cookery, providing skills to take into life beyond school. Students (mentees) engaged in weekly guided discussions with an assigned staff mentor to consider how these issues impacted their own wellbeing, thereafter developing strategies to make positive changes in their lives. Each year, we have adapted our programme in response to staff and student surveys, and at the end of Year 2, I started work on an action research report for the BSA Certificate in Boarding Practice (Boarding Management module), which has informed Year 3 in a much deeper way. More on that later.
Mentoring is an evidence-based approach to providing support, guidance and advice. There is sufficient evidence underpinning the benefits of mentoring students, including improved learning, a greater sense of belonging, improved relationships and increased development of
There is tremendous opportunity within our communities to proactively address issues...
interpersonal skills, for us to have confidence in our method of delivery. Providing students with a mentor also places our wish to develop connection and a sense of belonging at the heart of this initiative. Encouraging strong connections sits firmly within our school mission and boarding principles, and the Thrive programme seeks to demonstrate our commitment to building a healthy social system in which our students can flourish.
We have used the terms ‘mentoring, mentor and mentee’ to describe the conversations had between staff and students within the structure of the Thrive programme. In fact, our mentors are encouraged to discern whether their mentees require some guidance and direction (mentoring) or would benefit more from being encouraged to work through an issue themselves, finding a solution that best fits them and their unique circumstances (coaching). Mentoring in this sense can therefore be taken as a hybrid approach that encompasses the skills and tools of both mentoring and coaching.
Most mentoring programmes feature recruitment processes that rely upon volunteer mentors, and mentees who self-elect to engage with the mentoring. With Thrive, mentors have been required to work with an assigned number of boarding students in their house, and all boarding students are required to engage with their mentor. Having taken away the element of choice (although students are encouraged, not mandated to participate), our challenge was and remains “how do we help our participants feel comfortable, able and willing to engage with a mentor/mentee relationship?” My research paper helped me to find answers to this question. Firstly, in understanding the importance of the ‘contemplative stage’ (Keller, 2005) of programme development, with


recruitment being the best time for establishing mutual understanding of the purpose of the programme and for clarifying roles and responsibilities of staff and students involved. It’s a time to ground mentor and mentee expectations in reality and carefully manage those expectations.
Providing mentors with confidence in efficacy, through high quality mentoring skills training, emerged as a theme of my own ‘in-house’ research study and was mirrored in the larger scale research work I came across. These two key pieces of learning have resulted in a more informed 3rd year cycle of the Thrive programme and outcomes have included the following actions:
Pre-match (mentor/mentee) student questionnaires, to get a better understanding of hopes, expectations and preferences regarding their mentor relationship, frequency and goals.
Improved communication with boarding students and staff about the benefits, challenges and commitments of mentoring relationships and the Thrive program.
Mentor Skills Training delivered within school Staff Personal Development days.
Resources: mentors have access to a comprehensive set of resources that includes (but is not limited to): skills development, session guides and topic content. Mentors now use these resources in response to student interests, goals and needs, rather than in a set program of topics.
We have also improved ongoing match support, monitoring, evaluation and review processes as a result of the action research report findings.
All schools claim that boarding promotes wellbeing, independence and resilience, but evidencing this has often been difficult. Through the Thrive programme, we are able to produce usable evidence via student and staff surveys in conjunction with mentor records, to demonstrate that we as a school are having a positive impact on student wellbeing.
There are many other benefits to our Thrive programme that we have noted so far. Thrive incorporates theoretical knowledge and practical skills that students will be able to use in school and beyond, to manage their own physical, emotional and social wellbeing.
We are gathering evidence about boarder wellbeing that can be used to inform future planning. Above all, boarders are forging strong relationships with their mentors over an extended period and the mentors can see how they are affecting positive changes in the lives of their mentees. Interestingly, we are also comparing year-on-year data from CPOMS (Child Protection Online Monitoring Service) to identify where there are reductions in issues of emotional wellbeing, anxiety, stress, self-harm, suicide ideation and more.
The action research project led me to Nancy Kline’s work on ‘thinking environments’ (Kline 1999), about the power of high quality listening. This is something I observed for myself over and over again when I was coaching. An engaged and attentive listener often has a transformative impact on the person receiving this quality of attention. It is the skill and art of attentive listening that I would like us, as a team of mentors, to continue to develop. The mentoring meetings provide students with ‘thinking sessions’ – time and space to connect with their intuition, their best ideas and to understand themselves as their own best resource. This also provides the very best environment for inviting students to engage with topics that are meaningful and helpful to them now, and later in life.

Matt
Student survey results from last year provided us with ample testimonials of the many benefits they felt from having a mentor. These range from helping them to settle into school and boarding life, to dealing with exam stress and understanding good learning habits. This is the evidence that we need to keep going, further embed Thrive into our boarding programme and continue upskilling our mentors.
Through Thrive, we have created a research-based blueprint or theories of change for new boarding initiatives. This allows us to harness the interests, experience and knowledge of our boarding team within informed growth and creativity. Thrive has been joined by Quest (our long-established and comprehensive programme of activities), and other programmes designed to develop student leadership, opportunities for service and creativity are now being developed by the team.
It is unrealistic to expect our students to be happy 100% of the time, but if we can make even marginal differences in the wellbeing of the young people under our care, then developing Thrive has been incredibly valuable. We are proud of the proactive steps that we have taken in creating a bespoke wellbeing programme for our students and would happily share our experiences with other schools.
Garringer, M. MENTOR, (2015) Elements of Effective Practice for Mentoring 4th Edition. Available at: https://www.mentoring.org/resource/elementsof-effective-practice-for-mentoring/ Keller, T. E. (2005) The Stages and Development of Mentoring Relationships, in Dubois, D.L. and Karcher, M.J. Handbook of Youth Mentoring. Thousand Oaks, CA: Sage Publications Kline, N. (1999) A Time to Think. UK: Octopus Books
Rolfe, A. (2020) Mentoring, Mindset, Skills and Tools. 4th edn. Australia: Mentoring Works. Schwartz, S. E., Rhodes, J. E., & Herrera, C. (2012). The influence of meeting time on academic outcomes in school-based mentoring. Children and Youth Services Review, 34(12), 2319–2326.
http://dx.doi.org/10.1016/j.childyouth.2012.08.0 12
Spencer, R. (2007) It’s Not What I Expected, A qualitative study of youth mentoring relationship failures, Journal of Adolescent Research 22(4), pp. 331 - 354
Starting a Mentoring Program. MENTOR. A selfpaced tutorial on how to conceptualize and develop a mentoring program.
https://www.mentoring.org/resource/starting-ayouth-mentoring-program/
Star, J. (2021) The Mentoring Manual. 2nd edn. UK: Pearson
Kiely, Boarding Manager, TASIS England
Matt’s career spans 24 years across state, international and independent boarding schools. He began as a stooge and a rugby coach, and always had a keen interest in holistic wellbeing. Matt’s progress in pastoral leadership has given him the freedom and scope to develop his boarding programmes to achieve the best possible outcomes for the students in his care. Matt describes his work with Elaine on the Thrive programme as the “most rewarding experience” of his career to date.
Elaine Luckham, House Parent and Deputy Director of Boarding (Pastoral), TASIS England
Elaine’s long career in education has centred around providing pastoral care, advice and guidance, as a higher education advisor, coach, mentor and boarding house parent. With an abiding interest in student wellbeing, Elaine co-created a wellbeing and mentoring program for boarding students with colleague Matt Kiely, and now takes the lead on its future development.



✅ First Aid at Work (FAAW)
✅ Emergency First Aid at Work (EFAW)
✅ Paediatric First Aid at Work (PFAAW)
✅ Emergency Paediatric First Aid (PEFAW)
✅ Combined Paediatric and First Aid at Work (FAAW)
✅ Mental Health First Aid Adult
✅ Mental Health First Aid Youth
✅ Mental Health First Aid Champion (Adult or Youth)

Leanne Rowlands, Assistant Head, Pastoral & Deputy Designated Safeguarding Lead, and M Jolly, Director of Wellbeing and Inclusion, both Charterhouse School
The Netflix series Adolescence has struck a nerve, and we’ve all heard the call to action. While it is a masterclass in acting and technical filmmaking, its disturbing portrayal of the insidious and far-reaching effects of the internet on teenagers is impossible to ignore. To make matters worse, we are now passively co-dependent on the very technology we critique – and the confusing evidence base on the benefits it can offer. We are left with a paradoxical love-hate relationship that challenges us to think creatively about how to keep ourselves, and especially young people, safer online.
The tragedy is that this is no longer news, despite the huge amount of media coverage that we have seen lately. The good news, however, is that it’s never too late to develop the work. Many of us have witnessed first-hand the corrosive impact of social media on the physical and emotional wellbeing of young people. It can wreak havoc with force, spurred on by AI and algorithmic momentum. With Ofcom reporting that nine in 10 children own a smartphone by age 11 and 99% spend time online, school leaders now, more than ever, have an unavoidable responsibility to help weather the digital storm.
The Office of the Surgeon General has told us that it is a distressing reality that “extreme, inappropriate, and harmful content remains easily and widely accessible” to minors. It spreads through design, direct pushes, and unsolicited content exchanges. Adding to the concern, Meta’s recent policy changes are expected to roll back protections that, according to the Molly Rose Foundation, “will sharply increase suicide and self-harm risks”. Indeed, Papyrus suggests that many young people considering suicide “can easily access information, discussion and graphic imagery online which compound suicidal feelings or, worse, encourage suicide behaviours”. Advocates like Ian Russell MBE, Ellen Roome and other bereaved parents are doggedly demanding action from the government and Ofcom, while many of us want to help but aren’t always sure how. That’s not our fault.
Who knew what the red pill and the blue pill symbolised when they first appeared? Online harms are complex and prolific, blending old dangers with new threats: exploitation, manipulation, cyberbullying, reputational damage, extremism, addiction, and a profound impact on mental health. These harms can affect developing brains in ways we don’t yet fully understand. Jonathan Haidt describes the internet as “the largest uncontrolled experiment humanity has ever performed on its own children”. It’s not their fault, either.
Internet Matters note that in every ‘C’ – conduct, compulsion, contact, content – young people with offline vulnerabilities are, unsurprisingly and unfairly, most at risk online. Those struggling with mental health, special educational needs, limited support, discrimination, or who identify as LGBTQ+ are disproportionately vulnerable. This is especially so for individuals with eating disorders, those who have care experience or who have caring responsibilities. In each case, it is important to be able to look at the context and the length of time that young people are spending online. For the most vulnerable, social media can be a place where they may thrive, and enforced abstention may cause more distress. How do we create balance and distinguish between what might help and what might harm?
This is not just a single issue—it’s the intersection of gender, race, disability, and sexuality. The Department for Digital, Culture, Media & Sport (DCMS) suggests that boys are suffering, particularly through exposure to inappropriate content such as pornography or dangerous stunts. Girls are also suffering, particularly through pressures on body image and unsolicited contact. And so are young people who don’t fit neatly into either category. Does this mean that we are all vulnerable in some way? No wonder we find ourselves shaking our heads and throwing our hands up in frustration—if we can even focus long enough to read the statistics. From Gen X to Gen Z, our attention span
has reportedly dropped from 15 to 8 seconds (Persuasion Nation).
As educators, leaders, parents and peers, we must remain alert and engaged. We need to have open, honest, and non-judgmental conversations with young people. That means understanding and using the right language – deepfakes, sextortion, indecent imagery, ‘Incel’ culture, harmful influencers – the list goes on. We must understand how easily children can access violent, disturbing or indecent content, often within just a few clicks. Thanks to AI, these images might even contain their own face or depict recognisable people in graphic virtual assaults.
We must empower ourselves to stand beside them through this journey. Ask ourselves: how healthy is our own use of social media? How good is our own digital literacy? What are we role modelling to young people? We must protect ourselves first – apply our own oxygen masks – to avoid psychological and vicarious trauma, and ensure we have the right support and infrastructure in place. Have you thought about supervision and the benefits of finding space for professional reflection?
Safeguarding children is everyone’s responsibility. Our foundational knowledge and instincts apply both in the real world and online. We know that this work takes courage, curiosity, and vigilance. Ask: is this behaviour
normal for this young person? Is it appropriate, or cause for concern? What is their behaviour telling you, and what action do you need to take and how are you sharing information? Look for changes, such as withdrawal, a dip in academic performance, altered eating habits. You likely know more and can do more than you realise.
We must develop a strategy for navigating this ever-changing online world – building relationships that place young people at the centre. We must listen, hear, and co-create boundaries with young people. We need to build a team of experts to support this. Consider who should be at the table: representatives from health, wellbeing, IT, pastoral care, academic departments, support staff or co-curricular, as well as youth representation. This multi-disciplinary working group should be championed by senior leadership and budget holders, and may need to begin with a thorough audit. Critical friends like us can help.
Is a full digital audit overdue? Every conversation, every policy, and every process must be consistent, dynamic and responsive to change.

Create policies and risk assessments that reflect these challenges. Review your IT infrastructure: what are you doing to make systems safer? How are you filtering and monitoring content? Do you receive real-time alerts? Who receives them, and how are they followed up? Are you restricting smartphones? Is a full digital audit overdue? Every conversation, every policy, and every process must be consistent, dynamic and responsive to change.
As someone once said, we need education, education, education. The response will need to be proactive and reactive, and we must take the stance that “it does happen here”. This means upskilling parents, staff, governors and pupils – it’s not just about avoiding risks, but about resilience and problem-solving. We need to empower young people to develop skills to make good choices online, to self-regulate and self-moderate, and to learn from mistakes. And, as Dr Jane Gilmore suggests, we must forgive them when they struggle – because their brains are still developing and wired for risk-taking and novelty – and ensure that they have the confidence to seek help when things go wrong.
Inevitably, things will go wrong, and we need to be able to support in a crisis. What services are available in and outside of your school? What partnerships do you need? Does your behaviour policy allow for restoration and recovery? What does your Personal, Social, Health and Economic (PHSE) curriculum include – and how can its messages be embedded across the curriculum? The opportunities to make a difference are just as complex and wide-ranging as the challenges we face.
Our next step is to talk to each other. To build networks. To share ideas, resources, and a momentum for change. Please get in touch if you’d like to be part of our network.



Leanne Rowlands, Assistant Head, Pastoral & Deputy Designated Safeguarding Lead, Charterhouse
Leanne has more than 20 years of boarding experience, at St Edwards’ Oxford, Marlborough College (UK and Malaysia), Tudor Hall, Bradfield College and currently Charterhouse School, where she has responsibility for online safety. For 13-plus years, she ran both horizontal and vertical boarding houses and then moved to Malaysia in 2012 to set up girls’ boarding for Marlborough College. Previous roles include Head of Girls Sport and Head of Department (Academic Physical Education and Psychology). Leanne is also responsible for overseeing the International Pupils’ Co-ordinator, Lead Nurse and Guardians at Charterhouse. She has been instrumental in establishing coeducation, overseeing and auditing national minimum standards.
M Jolly, Director of Wellbeing and Inclusion, Charterhouse School
M is the Director of Wellbeing and Inclusion at Charterhouse and a recent member of the BSA Group, HIEDA, and the Health, Education and Wellbeing Advisory Board (HEWAB). As a counsellor, clinical supervisor, educator, and school leader, M has developed and implemented comprehensive, award-winning wellbeing and DEI strategies that promote safety, belonging, and mental health in young people in a variety of school settings.

Using data to gain deeper insights into the effectiveness of treatments while reducing administrative burdens. The Yes We Can Healthcare Group achieved this with its self-developed intelligent applications. Digital innovation ensures their team can focus on what truly matters: guiding young adults (called fellows) aged 13 to 25 who struggle with mental health issues, addictions and behavioural problems, towards recovery.
For a long time, the Yes We Can Healthcare Group sought a solution to monitor treatment outcomes transparently and streamline record-keeping. Existing software solutions failed to meet their specific needs. Refusing to compromise, Yes We Can chose to innovate This led to the creation of the app Discovery by Hawking, part of the Yes We Can Healthcare Group. The results have been transformative. By reducing the administrative burden on youth coaches, counsellors, psychologists and psychiatrists, Discovery has saved them hours of reporting time each day Instead of spending nearly two hours writing reports, coaches now spend less than half an hour. The combination of smart technology and artificial intelligence delivers structured, predictive data that leads to better care outcomes, more efficient workflows and sharper insights into fellows’ treatment progress.
When designing Discovery, the team at Hawking prioritised solving the most pressing issue: the administrative workload of the Yes We Can team “I want to spend as much time as possible with the young people,” says Bram, Team Captain of Youth Coaches at Yes We Can. “They follow an intensive programme, and we build a close bond with each other in a short time. I don’t want to walk around with a laptop or tablet, as that would only get in the way of the connection That’s why we only started reporting once the fellows are in bed ” Previously, after late shifts, coaches would spend hours typing up reports. Now, these reports are quickly compiled using predictive tags and tailored headings This allows them to focus on meaningful data while spending more time engaging with fellows. “Thanks to Discovery, reporting takes me far less time, which gives me more peace of mind and literally more sleep ”
The Youth Coaches are with the fellows in the clinic all day They act like a brother or sister and offer support when needed. They have continuous interaction with the fellows, which results in seeing everything that happens in the group and developing a sixth sense to perceive things that are not seen or spoken out loud This allows the Youth Coaches to gather essential information about the fellows treated at Yes We Can The findings are shared during daily multidisciplinary meetings with therapists, counsellors, nursing staff and psychiatrists, and everything is now kept track of in Discovery This not only saves time but also provides valuable input, optimization suggestions for the treatment process and gives the multidisciplinary team a clear, real-time view of each fellow’s development
“Yes We Can demonstrates how digital innovation, when tailored to real-world needs, empowers healthcare professionals to provide life-changing care. ”
Johan Linssen, CEO of the Yes We Can Healthcare Group, explains: “All our applications must enable our colleagues to work smarter in significantly less time. We achieve this with Discovery, but also, for example, with Honeygrid. Based on a model developed by three renowned psychiatrists, Honeygrid allows colleagues to intuitively compile symptom patterns. Using artificial intelligence, they can quickly create a diagnosis and treatment plan. It’s still completely personalised and tailored to each fellow, but in less time and with far greater insight. At Yes We Can, we have one goal: ‘Everything for the fellow.’ This can only be achieved if we enable our colleagues to fully focus on them.”
At Yes We Can, the motto ‘Everything for the fellow’ is not just a phrase, it’s a guiding principle embedded in the whole organisation and in every treatment method. Tools like Discovery and Honeygrid demonstrate how digital innovation, when tailored to real-world needs, empowers healthcare professionals to provide life-changing care. By working smarter, Yes We Can ensures every second is spent where it truly matters: helping young people take back control of their lives and achieve lasting recovery.
And their approach has proven to be very successful. More than 74% of former fellows no longer need specialised care after completing the residential treatment and aftercare programme. Every year, Yes We Can treats over 1,000 young people aged 13 to 25 who struggle with mental health issues, addictions and behavioural problems. Together with other fellows from all around the world, they learn to recognise and acknowledge their problems, ask for help and speak out. In a place where unconditional warmth, safety and confrontation at the right time are pivotal, over 500 highly specialised healthcare professionals work hard to help fellows and their families turn hopelessness into happiness. Parallel to their treatment, parents and/or carers participate in an intensive family coaching and counselling programme.
Do you want to learn more about Yes We Can Youth Clinics or need any assistance for one of your pupils? Our team is always here to offer advice and guidance. Call +31 (0)85 020 1222 or email info@yeswecanclinics.com for more information.


Emily Elliot, Therapeutic Counsellor and Eye Movement
Desensitization and Reprocessing (EMDR) Practitioner, DLD College London
Emily is registered with the British Association for Counselling and Psychotherapy (BACP) and is an Integrative Therapeutic Counsellor, and EMDR Therapist and Counselling Supervisor with accreditation. She operates a private practice and serves at DLD College in London.
I work in a vibrant, multicultural school in central London, home to approximately 400students. Our student body comprises mostly international boarders, alongside a mix ofday students and local attendees. The team comprises two part time counsellors. The predominant reasons for students seeking support are anxiety, relationships andneurodivergence, particularly autism and ADHD. Our therapy room sits in the wellbeingarea ideally placed opposite Matron with plenty of plants and art to help students feel atease whilst they wait.
In both the classroom and the therapy room, the battle for focused attention rages on. This is not solely attributable to the rising diagnoses of neurodivergence. A broader challenge lies in managing modern digital habits. Students often share stories of ‘doomscrolling’, or spending upwards of 13 hours daily on social media. While this brings them comfort, it also fosters an attachment they find hard to break. Many experience palpable anxiety when separated from their devices.
Establishing a safe therapeutic space is paramount, allowing students to release their anxiety and trust in the value of counselling. During initial assessments, which cover their history, lifestyle, medical background, and goals, often an alarming pattern emerges: unbalanced lifestyle habits that exacerbate anxiety and deteriorate mental health.
Counselling, therefore, revolves around attentive listening – helping students analyse the pros and cons of their current habits, acknowledging contradictions and identifying discrepancies to instigate change. This is a
gradual process requiring collaboration where possible with boarding staff or parents. Joined up pastoral support plays a critical role in fostering meaningful progress.
Cultural perceptions of vulnerability present additional hurdles. Students from Asian and Eastern European backgrounds often view seeking help as socially unacceptable. Instead, they may somatise their issues, presenting with physical symptoms. Frequent visits to the school Matron become a subtle cry for help, offering an opportunity to encourage counselling in a non-intrusive manner. When students are waiting to see Matron, I might have a brief friendly chat with them which helps them to feel welcome and seen. If a student is upset or dysregulated, they can use the wellbeing area to calm down with friends or a member of staff and, when free, we see them for drop-ins.
Warm, approachable communication is crucial for breaking down these barriers. Simple methods such as appointment reminders sent via team messages adorned with emojis – a thumbs-up or smiley face – help bridge cultural divides. These symbols resonate naturally, especially with students accustomed to pictorial communication.
Even casual interactions in corridors hold value. A friendly greeting and a warm smile when passing can make a significant difference. Strikingly, some students who initially avoid eye contact might later reach out to book a session, finding comfort in those brief, positive encounters.
Therapeutic sensory aids have proven transformative for both students, and staff. Quiet fidget toys or puzzles provide tactile engagement, which not only occupies students’ hands but also fosters a sense of safety, especially for those who struggle with direct eye contact. These tools often act as icebreakers. Students may initially visit to collect a tactile keyring or toy and, in the process, familiarise themselves with the counselling space, paving the way for future sessions. Holding a fidget aid opens up the conversations. I have seen a huge shift working with neurodivergent students who open up and talk whilst their hands are sorting a puzzle or creating a pattern.
Nancy Kline’s Time to Think outlines the importance of uninterrupted attention in creating a respectful, empowering environment. By bracketing my own preoccupations and tuning in fully, I aim to hold a space where students feel heard. This focused attention enhances their ability to think independently and develop the self-empowerment necessary for positive change.

In an era where psychotherapeutic language has entered mainstream vernacular, words like “trauma”, “panic attack” and “narcissistic” are often used casually, diluting their clinical significance. Part of my role is to neutralise these terms and help students reframe their experiences.
Cultural sensitivity is integral to my practice. Showing genuine curiosity about students’ names, the significance of their birthdays, or their cultural observances fosters trust and opens avenues for deeper connection. These personal conversations often lead students to share more about their families and home lives, further enriching the counselling process.
Fidget toys or puzzles provide tactile engagement to foster a sense of safety
As counsellors, we are trained to offer empathy, unconditional positive regard, and congruence. While the first two establish the foundation of trust and safety, congruence becomes essential as the relationship develops. It enables constructive challenges to students’ thinking or behaviour, promoting growth in a manner that feels collaborative rather than confrontational. However, this delicate balance can be disrupted by breaks in school routines, underscoring the importance of maintaining safety and consistency in each session. Congruence aids the student to take responsibility and empower them with their decision making, critical thinking and choices.
For instance, if a student describes having a “breakdown”, I might reflect back: “It sounds like you were very upset, what happened?” This approach validates their feelings without amplifying the language. Students often use hyperbolic expressions to seek care. Sometimes students will say one thing to a staff member and the opposite to another, a behaviour known as “splitting”. Focusing on the underlying needs driving this behaviour, echoing the principle that all behaviour is an expression of need is key. Alice Sheldon’s Why Weren’t We Taught This at School is an excellent resource for delving deeper into such dynamics.
Students themselves have embraced technology to support their mental health. One student overcame selfharming tendencies by using MySoberApp, while another with autism found a helpful companion in Brain in Hand, an app likened to a personal assistant. Others recommend Notion for organising schedules or Quizlet for revision tools, including memory-enhancing games. For staff and parents, Additude e-magazine offers invaluable advice on managing neurodivergence.
With anxiety being a prevalent issue, our school has adopted proactive measures to address it. Posters in classrooms guide students through deep-breathing exercises, equipping them to manage early signs of panic without leaving the room. This initiative has significantly reduced both classroom disruptions and counselling referrals related to panic attacks.

In counselling sessions, breathing exercises form a cornerstone of anxiety management. Students learn and practise abdominal breathing with us to re-engage their prefrontal cortex and recognize signs of “amygdala hijack”. Alongside psychoeducation about the brain, these sessions emphasise curiosity and self-awareness around body signals and cues. Over time, students are guided to reframe their inner narratives, fostering compassion and reducing selfcriticism.
Students can self-refer by emailing or messaging us on the school systems. Staff can refer a student after an incident or when a student requests it. When a student self refers it is a good sign that they are motivated to engage and taking that step of responsibility towards it. Once clients are established, we then see an increase in referrals naturally as word gets round via student network that we are useful. We see on average about 20% of the student cohort. We don’t give students a limited amount of sessions, as with all the natural school breaks it can take a while for the therapeutic alliance to form. With the barriers mentioned earlier and English being a second language, building a strong therapeutic relationship takes longer.
We see students outside their lessons and off timetable so some sessions are slightly shorter than the 50 minutes one would normally have in the UK. We review every six sessions and we generally have a mix of long and short-term clients. Every Autumn term, a member of the counselling service will speak to the student body. We explain briefly what counselling is, debunk some myths, establish the limits to confidentiality and give examples of what students come in for. The amount of people coming in tends to peak at the
end of the spring term, as any exam anxiety has usually been dealt with. However, towards the end of terms there is a slight increase in drop-ins, as a student might not want to return home in the holidays, or a safeguarding issue comes up.
The counselling team has access to Reach reports that boarding staff make concerning students, and a quick overview of clients can often give context without the need for verbal updates. We also have a pastoral meeting that meets fortnightly to discuss students of concern. Referrals come from these meetings too. Without breaking confidentiality of the session content, we can offer our professional overview to the team, hear team updates or concerns, or raise attendance issues and contribute to next steps. We also have a SEN and a wellbeing link in boarding that works closely with us, meeting once per month. We discuss matters that are already in pastoral staff awareness and can together come up with practical and creative solutions for students that maintain their wellbeing. For example, suggesting a role or a responsibility for a student with social anxiety, or how to engage a student with autism, such as asking for their help during a boarding event or trip.
Breathing exercises form a cornerstone of anxiety management
I often connect with experts and ask for their advice when working with complex needs.
As for myself, I have monthly clinical supervision and fortnightly peer supervision during the terms. I absolutely switch off at weekends and ensure that I maintain regular physical fitness which boosts my own mental health and resilience. I try to have a balance of being sociable with the need to be quiet, to be in nature and be in solace. I find acknowledging the threshold I am working in to be helpful in managing frustration, as we are often dealing with students who are complex or critical and needing specialist support. The specialist support can bring barriers for international students, as we cannot put in place state support when a summer break is about to take place, or if parents are not engaged, or when the student is discharged, as not meeting the very high state threshold yet, they are above our own threshold to support. In these cases I acknowledge that I hold the risk and the care with the pastoral team and the parents. Knowing that we are working together tightly to achieve positive outcomes helps me. I often connect with experts in the field and ask for their advice when working with complex needs. I liaise with the specialist clinical team asking for advice in how we manage these students in the meantime.
Working towards endings is paramount. Ending sessions will often identify what they got out of the counselling and what is still needed to be worked on. We look at where they can go for future support at university and beyond. Sometimes a student will want us to write a letter to their university, and we get them into the counselling service early as a result. The chaplaincy at university is often another great resource for them. At breaks and end of terms, we email students with urgent and emergency support services. They know that they cannot access us during the holidays, but we want them to feel held in between those long breaks.
By integrating cultural sensitivity, therapeutic tools and a focus on responsibility and empowerment, we aim to create an inclusive, supportive environment that helps students navigate their challenges with resilience and confidence.


Ten years ago, when I first started my role as a nurse within the Health Centre team at an independent all-girls full boarding school, the majority of the work revolved around managing sporting injuries, minor ailments, and the occasional accident. At that time, the Health Centre was staffed by qualified nurses working 24 hours a day, with support from a GP who attended for one hour, five days a week. A private physiotherapist also came in once a week to treat pupils referred to by the GP. The staffing levels for nurses and doctors remain unchanged to this day, with the same commitment to providing round-the-clock care and support for the pupils.
At this time, mental health concerns were few, although still present. The school had one full-time counsellor who, despite being fully booked, managed to accommodate pupils in need of support However, as awareness of mental health increased, the school’s approach to supporting pupils’ mental well-being began evolving The number of counselling staff gradually increased, reaching a total of three counsellors, equivalent to two full-time roles, in response to the growing demand.
With the onset of the Covid pandemic, isolation had a significant impact on the mental health of pupils. As pupils returned to school and the routines of daily life
resumed, there was a noticeable escalation in mental health concerns. Pastoral staff found themselves feeling untrained and ill-equipped to support the pupils experiencing these challenges.
Communication from the pupils also changed. Prepandemic, pupils were becoming more comfortable discussing their feelings, but post-pandemic, they struggled to articulate their emotions. The introduction of technology, particularly the use of Microsoft Teams, allowed pupils to communicate more comfortably, helping them to express themselves without the anxiety of face-to-face conversations.
As a result of these changes, it became clear that the school needed to explore additional avenues of support. It was felt that the pastoral staff needed more options to direct pupils to appropriate help. To address this, the decision was made to expand the visiting therapist service. The Health Centre, with its existing versatile space of a therapy room, was adapted to provide a welcoming and comfortable environment for these additional services.
In expanding the range of therapeutic support offered to boarding pupils, therapists from the local area were carefully selected. These therapists were either recommended directly by healthcare professionals within the school or were chosen based on positive feedback and experiences shared by previous pupils who had benefited from their services.
Before being integrated into the school’s therapeutic team, each therapist underwent a thorough vetting process. The HR department ensured that all safer recruitment procedures were followed, guaranteeing that the therapists met the necessary professional and ethical standards to work within the school environment. This process included background checks, verification of qualifications, and references to ensure the safety and well-being of the pupils. By following these steps, we ensured that the therapeutic services provided were both high quality and aligned with the school’s safeguarding policies, allowing us to offer pupils the support they needed with confidence and security.
The first to join the visiting therapist team was a hypnotherapist, who specialised in working with anxiety, phobias, and stress. Hypnotherapy, an ancient practice, has evolved alongside our growing understanding of the brain, emotions, and behaviour. Clinical hypnotherapy uses advanced techniques, such as deep relaxation and visualisation, to help individuals alleviate medical or psychological problems where emotions play a significant role.

Speech and language therapist was requested, to support pupils with communication difficulties, including issues with eating, drinking or swallowing. This specialist can assess and treat speech, language and communication problems, tailoring their approach to each pupil’s needs.
Another addition was a nutritionist who works with pupils to improve their physical health through diet and lifestyle changes. The nutritionist helps manage physical conditions like IBS, auto-immune conditions, weight challenges, hormonal issues and skin problems, while also working to improve pupils’ relationships with food.
Reflexology was introduced, a non-invasive complementary therapy, which promotes deep relaxation and wellbeing by reducing stress. It is particularly effective in optimising health and building resilience. Reflexology involves applying gentle pressure to specific points on the feet, lower legs, hands and other areas of the body, which correspond to different internal systems. This therapy helps manage stress and supports pupils’ mental and physical wellbeing.
Sports massage therapy is another vital addition to the school’s health provisions. Designed to assist in correcting soft tissue imbalances caused by physical activity and trauma, sports massage enhances performance, aids recovery, and helps prevent injury.
This therapy is particularly beneficial for active pupils involved in sports, offering them additional physical care to support their overall wellbeing, at times working with the physiotherapist and the sports department.
The next ambition is for expansion of neurodiversity support, further addressing the needs of pupils with different neurological conditions. These services ensure that pupils with ADHD, autism and other neurodivergent traits receive the tailored support they need to thrive academically and socially.
As awareness of mental health increased, the school’s approach began evolving.
All of these therapists are able to easily communicate with the Health Centre team, who can then provide feedback to the school GP, the Deputy Pastoral Head, and the parents. This seamless communication ensures that all parties are kept informed and involved in the pupil’s care. By working together, the Health Centre team, therapists, medical professionals and pastoral staff are able to provide optimal support and care for the pupils, ensuring their physical and mental wellbeing are holistically addressed. This integrated approach fosters a strong support network for the pupils, enhancing their overall experience at school.
By offering on-site therapy and support, the school has been able to provide valuable resources to pupils who
might otherwise struggle to access such services. With therapies like hypnotherapy, reflexology, speech and language therapy, nutrition and sports massage, we can ensure that pupils have multiple avenues of support for their mental and physical health.
The first to join the visiting therapist team was a hypnotherapist...
Parents are given reassurance that all therapists involved in the school’s support network meet the institution’s safeguarding regulations and are qualified, experienced professionals in their respective fields. To maintain transparency, parents are provided with the therapists’ details and encouraged to make direct contact with them. This allows parents to discuss any private fees associated with the therapies, as well as any necessary consents or permissions for their child to receive the treatment.
Once parental consent is obtained, the therapist will then liaise directly with the Health Centre to arrange the use of the therapy room. This ensures that all logistical aspects are taken care of and that pupils can receive their therapy in a professional, confidential and safe environment. This joint process fosters clear communication between parents, therapists and the

Health Centre, ensuring a smooth experience for everyone involved.
The integration of these services into the Health Centre not only ensures that care is easily accessible, but also fosters medical staff, therapists and pastoral teams to work together. This integrated approach guarantees that pupils receive optimal care and support, reassuring both pupils and staff that their mental, emotional, and physical needs are being met in a holistic and effective manner. This comprehensive support structure helps foster a healthier, more resilient pupil body, better equipped to navigate the complex challenges faced by boarding pupils today.

Alice had a diverse NHS career, specialising in orthopaedics and becoming Ward Sister on the elective orthopaedic ward. She then moved into clinical site management at a busy acute hospital, working with multidisciplinary teams to ensure patients were allocated to the right specialists. Alice moved into practice nursing before joining Sherborne Girls’ nursing team. She became Health Centre Manager and her role has developed into Health and Wellbeing Lead. She focuses on promoting physical and mental health, empowering students to understand their bodies, build resilience and develop lifelong healthy habits. Alice is passionate about guiding young women through their formative years, helping them grow into confident, well-rounded individuals.

Tracey Read, Manager and Lead Nurse of the Health Centre, Wellington College
Wellington College aims to provide an ambitious and aspirational environment in which the potential of each pupil is brought out and developed across all aspects of themselves as unique individuals (James Dahl, Master). As a Health Centre team, we aspire to provide healthcare for pupils that supports their emotional and physical growth and development to help them navigate life at Wellington and prepare them for the outside world. So, how do we facilitate this in a pioneering coeducational institution, with more than 1,100 pupils?
At Wellington, we are fortunate to have a team of 12 nurses who provide 24-hour care, seven days a week during term time. The service operates an open-door policy whereby pupils can drop in at any time to be assessed by a nurse Although pupils who are ill or injured know where to access nursing or GP services, this model alone does not provide a proactive approach to healthcare and health promotion, nor cultivates meaningful relationships. To deliver exceptional healthcare, we have utilised the Link Nurse role, which is continually reviewed and adapted to suit the evolving healthcare needs of our pupils
Link nurses are not a new concept in children’s nursing. The role has existed since the 1980s and has been implemented in various healthcare settings. Legg et al (2017) believe that establishing link nurse roles enhances
leadership, knowledge, and development, a sentiment widely shared throughout the literature McQuire and Bagallon (2021) suggest that filling the “missing link” in healthcare enables solid and valuable relationships to be developed
Within boarding school environments, this missing link may be nurses, house staff and pupils working together By bridging this gap using the Link Nurse role, we can ensure that relationships are nurtured, in turn providing an opportunity to establish communities of good practice (RCN, 2021). I believe that good practice within the school environment takes a holistic approach and needs to ensure overlap between house staff and healthcare staff to optimise each pupil’s physical, emotional, and psychological health at all stages of their development, not simply when they are unwell or in crisis.
The beauty of the Link Nurse role is that it can be remodelled to fit different disciplines of nursing care in different healthcare environments Wellington College has 16 boarding houses and two day houses A nurse is allocated to each house and becomes the initial point of contact for:
Targeted health promotion through discussions, presentations, and talks
Drop-in clinics in houses at times that benefit pupils (such as break or lunch times)
Writing and reviewing individual healthcare plans for pupils with specific health needs
Supporting house staff with correct storage, administration, and documentation of medications through termly audits
Our nurses have found that drop-in sessions in houses allow for an organic way to build trusting relationships, which enhances the care and support pupils experience when they need assistance through illness, injury or emotional upset at the Health Centre
In addition to house allocations, each nurse has a link role relating to their own special interest in a particular health condition, for example, travel health, sexual health and relationships, disordered eating, diabetes, allergies and anaphylaxis Through increasing their knowledge in specialist areas, link nurses act as resources for other team members, share information, and increase
clinical effectiveness through discussion and in-house training.
We have received positive feedback regarding the link nurse role, reflecting the RCN’s (2021) theory that the role improves organisational energy surrounding health promotion, effective communication, and better engagement of staff and pupils with the nursing team It has been a privilege as a leader to see the nurses in the Health Centre team act as role models for our pupils, and become visible advocates when present in boarding and day houses
Although the Link Nurse role brings many benefits, it would be remiss not to acknowledge potential barriers regarding consistency, sustainability and efficacy. Hasson et al (2008) report several challenges when implementing the Link Nurse role within a community setting, including:
Having the required cover so normal services can continue while releasing nurses for link duties
Time pressures and current demand on services
Lack of confidence or experience among junior nurses
Resistance from staff who may perceive the role as intrusive
All school nurses, whether in private or public sectors, can relate to these pressures, especially during busy winter months when illnesses and injuries peak To overcome such barriers, it is essential that leaders
consider the support required from their nursing team, especially regarding flexibility and offering protected time to keep staff motivated about the Link Nurse role
This itself brings challenges for lead nurses, as providing this level of support requires addressing issues surrounding staffing levels, recruitment and retention, and sufficient budgets Operating as a larger team with nurses who work full and part-time, there remain challenges in balancing colleague support with day-to-day service demands, while effectively fulfilling the Link Nurse role. Ensuring parttime colleagues have a proportional workload to those who work more hours is difficult when there are eighteen houses to account for, and a mismatch in time available versus increasing workloads can cause staff to feel overwhelmed
Morale and motivation feature heavily in literature as precursors to successful Link Nurse implementation. As the lead nurse of the Health Centre, I offer to cover staff so they can have protected time to fulfil their roles I use regular one-to-one meetings and the appraisal process to provide feedback and reinforce the value of each nurse working in a Link Nurse capacity, helping to keep morale and motivation elevated throughout the team
We also reflect on the role during staff meetings to discuss what is working well and what can be improved. This allows for consistency regarding topics covered, while enabling enough bespoke work to engage with the specific needs of pupils in different houses.
The RCN (2021) states that to be successful, Link Nurses must possess certain core values to educate, advocate, and communicate effectively with pupils and house staff These values include being approachable, nonjudgmental, reflective, respectful, passionate, responsible for one’s actions, and an active and willing participant, although I would argue these are values every nurse needs to provide high-standard care The Nursing and Midwifery Council’s Code of Conduct, alongside Wellington’s values-based interview approach to recruitment, helps identify potential nurses who embody these values, as demonstrated by our outstanding Seacole Award-winning Health Centre team
It is well-evidenced that Link Nurse roles are important in providing high-quality, proactive and effective

Link Nurses must possess certain core values
healthcare However, to break down barriers and reap the benefits of the Link Nurse role, it is not only essential that nurses hold the right values, but also that pastoral and Senior Leadership Teams champion the role and provide a robust support system to allow it to flourish
At Wellington, we are fortunate to be well-supported by our Senior Leadership Team and HR department, who backed a recent business case to increase nursing provision This, along with a Deputy Head Pastoral who is passionate about developing the Link Nurse role within boarding houses as a means of proactively addressing health issues and challenges that our young people face as teenagers, has established a firm foundation for the ongoing success and development of the Link Nurse role at Wellington College.
Legg, M , Cleary, A , Shackelton, J , & Hampton, S (2017) ‘Establishing link nurse roles to enhance leadership, knowledge and development’, BMJ Supportive & Palliative Care, 7(Suppl 2), p A113
McQuire, R and Bagallon, G (2021) ‘Development and evaluation of an intravascular link nurse to sustain improvements in practice’, British Journal of Nursing, 30(2)
Royal College of Nursing (RCN)(2021) The role of the link nurse in infection prevention and control (IPC): Developing a link nurse framework London: RCN Hasson, F , Kernohan, W G , Waldron, M., Whittaker, E. and McLaughlin, D. (2008) ‘The palliative care link nurse role in nursing homes: barriers and facilitators’, JAN: Leading Global Nursing Research, October. MacArthur, C. (1998) 'Title of the article', Journal of Diabetes Nursing, 2(2), pp. 55-58.
Tracey Read, Manager and Lead Nurse of the Health Centre, Wellington College
Tracey has been a Paediatric Nurse for over 21 years, having completed her training at Southampton University in 2003. She spent 18 years working in the NHS on Paediatric Wards, gaining experience across a range of nursing disciplines. Her career progressed to leadership, culminating in her role as Ward Sister of a 44-bedded Paediatric Unit. In 2021, she joined Wellington College as the Nurse Manager of the Health Centre, delivering nursing care and health promotion to over 1,100 pupils and working closely with the pastoral team. Parenting a young child with autism and ADHD, alongside two teenagers, provides Tracey with a deep, personal insight into the daily challenges faced by young people and their families. This perspective continues to shape her clinical practice and leadership.

Adam Eustace, lead physio at Wellington College and Shrewsbury School, and Director of Modus Physiotherapy and Modus Education
Ankle injuries are a common sporting injury within the school setting, especially in sports such as netball, football, hockey and rugby. Though most will recover well over two to three weeks with rest and simple exercises, evidence shows that 25% of ankle injuries will go on to result in chronic ankle instability (Lin et al, 2021).
Given this, it is imperative that good early diagnosis and management is carried out This article will highlight the most common ankle injuries presenting within a school health centre setting, namely a lateral ankle sprain, high ankle sprain and fracture.
As the name would suggest, this refers to damage sustained to the lateral ankle following an ‘inversion’ of the ankle Usually occurring when the foot is pointing down (plantar flexion) and then twists inwards, such as rolling the ankle during running, walking downstairs or on uneven ground Pain and swelling presents mostly along the outside of the ankle, just under the lateral malleoli (bony lump on outside of ankle).
25% of ankle injuries will go on to result in chronic ankle instability (Lin et al, 2021)


Though not as common as the lateral ankle sprain, high ankle sprains make up around 11% of all ankle injuries (Prakash et al, 2020), and are often misdiagnosed
Usually occurring when the foot is planted, and an external rotation (outward rotation) is forced upon the
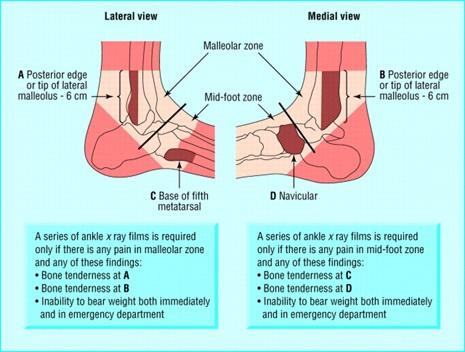
ankle, such as when the knee falls inwards with a planted foot
Pain and swelling presents through the middle of the ankle, along the ‘ankle mortise’ (between the fibula and tibia) These often take significant longer to recover from then lateral ankle sprains
Ankle fractures account for over 12% of all fractures within the paediatric population (Rammelt et al, 2016) Often fractures are a result of an inversion or eversion injury, making them hard to diagnose without X-ray due to associated ligament damage. Within the school health centre, a low threshold for suspecting a fracture should be taken, with the use
of the Ottawa rules (see image) being a key tool in making decisions around referring pupils for an X-ray
When assessing an ankle injury, thorough subjective assessment should been taken, establishing pain level, location of pain, mechanism of injury, aggravating factors, previous injuries and any neurological symptoms Once this has been achieved, an objective assessment may be carried out, including the following:
Assess for any bony deformity, swelling, bruising or abrasions
Ensure to carry out the Ottawa rules for a suspected fracture, palpating for bony tenderness (see previous image).
If any deformity is noted, ensure to carry out palpation of ankle pulses such as dorsalis and posterior tibial artery (see image).
Palpate for pain and swelling below the lateral malleoli for potential damage sustained in an inversion injury.
Palpate between the medial and lateral malleoli (mortise) for pain and swelling sustained in a high ankle sprain.

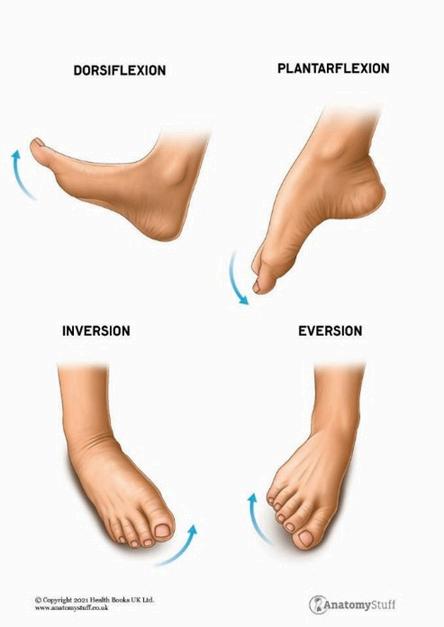
If the patient is unable to take >3 steps they are Ottawa rules positive and should be sent for an X-ray.
Pain with ankle inversion suggests a lateral ankle sprain.
Pain with ankle dorsi-flexion, or when performing a squat with ‘knees pushed over toes’ is suggestive of a high ankle sprain.
Watch for ‘increased inversion’ (compared to opposite side) with little pain. This may suggest a ligament rupture and should be assessed by a physiotherapist.
Correct acute injury management should be taken such as rest, ice, compression and elevation
As with all injuries, correct acute injury management should be taken such as Rest, Ice, Compression and Elevation, alongside analgesia if required. In the instance that the patient is Ottawa rules positive, they should be sent for an X-ray.
If the patient has high function, e.g., can walk, squat, lunge and even hop, then a period of relative rest of five to 10 days may be required, ensuring to reassess the pupil prior to return to sport. It is recommended to have an ankle exercise and advise sheet for such patients to ensure some form or rehabilitation has taken place.
In more severe cases in which the patient does not have good function, it is advised they seek a physiotherapist for a full assessment and rehabilitation program prior to returning to sport.
I hope this article has been informative. It is not intended to be a comprehensive description of an ankle assessment, rather some key points for you to consider when carrying out your own ankle assessment

Adam Eustace, lead physio at Wellington College and Shrewsbury School, and Director of Modus Physiotherapy and Modus Education
Adam is a specialist musculoskeletal (MSK) physiotherapist who has been instrumental in developing fully integrated sports management systems within schools, through staff and pupil education seminars, optimised pitch-side care, and access to physiotherapy triage clinics. With more than 10-years’ experience in the school sector, Adam understands the challenges sports injury management presents to medical teams. As a result, he has developed the only sports management course tailored to school nursing teams and sports staff through Modus Education, already teaching over 100 schools across the country.
The adoption of digital management tools have revolutionised how schools approach head injury management

Michelle Edge, Lead Nurse, Denstone College
Sport and physical activity play a crucial role in a student’s development, imparting frameworks for learning, resilience, and discipline. However, these activities also come with risks, particularly concerning head injuries, which can lead to significant short and long-term consequences if not promptly identified and effectively managed.
In recent years, increased awareness regarding concussion, evolving medical protocols, and the adoption of digital management tools have revolutionised how schools approach head injury management Denstone has taken a proactive stance by adhering to the latest national guidelines and implementing structured, clinically informed protocols
This article details Denstone's journey and highlights the broader shifts in national guidelines It also introduces emerging tools which are setting new benchmarks for student safety and overall wellbeing.
For many years, the approach to head injuries in schools, particularly those occurring during sports, was inconsistent. At Denstone, it became clear that discrepancies existed between the information shared by sports coaches and nursing staff. Pupils were often eager to return to play, leading to situations where they downplayed symptoms or insisted they were fine Coaches lacking medical training sometimes supported these decisions. Meanwhile, school nurses relying on second hand information were cautious and occasionally misinformed
The result was a communication gap, a lack of consistent follow-up, and increased
vulnerability for pupils It became apparent that a more robust, evidence-based system was needed, not only to ensure the physical safety of pupils but also to safeguard staff through clear protocols and documentation.
Head injuries are not exclusive to contact sports Pupils may sustain concussions from classroom accidents, collisions in corridors, or slips and trips around the school Symptoms such as dizziness, visual disturbances, nausea, memory lapses, or confusion may appear immediately or several hours later The complexity of head trauma and the variability of symptoms demand a system capable of detecting, assessing, documenting, and responding to each injury with precision and care.
Significant strides have been made at national level to support safer concussion management in schools.
In 2022, the International Football Association Board (IFAB) implemented concussion substitution guidelines for under 12 matches in grassroots football This landmark move laid the foundation for extending best practices to school environments, helping to reduce the risks associated with a premature return to play
April 2023 marked the launch of the UK Government’s Landmark
Concussion Guidance for Grassroots Sport. This was the first UK-wide protocol, developed jointly by
clinicians, academics, and sport governing bodies, with the aim to:
Identify symptoms early
Establish structured recovery pathways
Promote multidisciplinary involvement
Provide clear criteria for return to play or school
Crucially, the guidance acknowledged that the absence of protocols within schools poses a risk not only to physical health but also to the mental wellbeing of children.
Denstone College adapted the national guidance into a school wide protocol that includes:
A clear algorithm for post head injury response
Updated accident reporting systems
Laminated Concussion
Recognition Tools (CRT6)
Parent facing documentation on symptoms, home care, and reengagement with school/sport Training across all staff roles, from academic staff and nurses to coaches
Academic staff were included in the training to identify post injury issues, such as reduced concentration, fatigue, or sensitivity to noise and light, ensuring that support extended beyond the playing field
Denstone implemented a structured protocol for any incident involving a
a potential head injury. Key steps include:
Assessment: staff are trained to identify warning signs, such as dizziness, nausea, blurred vision, or confusion, and refer pupils to the Health and Wellbeing Centre for further evaluation.
Neurological assessment:
Nurses assess pupils using a structured neurological chart, including checks for pupil reaction, motor skills, speech coherence, and coordination 4-hour monitoring: pupils presenting with symptoms are monitored every 15 minutes for a minimum of four hours Blood pressure, pupil reaction, and cognitive awareness are assessed throughout
Parental communication: parents receive a full report on the injury, findings, and next steps If further care is required, a hospital referral is made and supporting documentation is provided
Documentation and follow-up: Every incident is logged, with an emphasis on continuity of care both in school and at home
This ensures no assumptions are made regarding a pupil’s fitness to return to activity, and that all key decisions are supported by clinical observations and records
Return2Play (R2P) is a new standard for concussion management in schools; an evidence-based, clinically overseen digital platform designed to manage the full journey from head injury to return to activity It removes uncertainty from decision making and ensures consistency across staff, pupils, and parents
At its core, R2P combines structured clinical protocols, real time communication tools, and professional medical input to provide complete oversight of every concussion case.
Many schools have historically relied on pupils self-reporting or informal assessments by coaches to determine when a pupil could return to sport However, this approach can be unreliable and unsafe R2P addresses these issues by:
Minimising the risk of premature return to play
Standardising recovery timelines
Introducing clinician-led medical oversight
Providing clear documentation and traceability.
The R2P programme follows a sixstage graduated return to play pathway:
Symptom rest: 24–48 hours of cognitive and physical rest
Light aerobic activity: e.g. walking, stationary cycling
Sport specific activity: Light non-contact drills
Non-contact training: More complex movement patterns
Full contact practice: Once cleared by a clinician
Return to competition: Full resumption of normal sport
A pupil must be symptom free for 24 hours before progressing to the next stage Any recurrence of symptoms requires returning to the previous stage
Each pupil’s recovery is logged in a secure digital injury tracking system that:
Alerts staff when pupils are ready to move to the next stage
Provides real time updates to school nurses and coaches
Enables parents to access medical progress notes
Supports safeguarding audits and injury history reviews.
R2P gives schools access to trained clinicians who:
Perform initial and follow-up concussion assessments
Confirm medical clearance at key stages
Provide consultations for persistent symptoms
Offer reassurance and guidance to parents.
This support is invaluable for schools with limited or part-time medical staffing.
The benefits of R2P for schools include the ability to demonstrate safeguarding diligence, reduced exposure to liability, clear protocols to support staff, and improved communication with families and external medical professionals.
Denstone adopted R2P in September 2024 The steps included:
Staff training during the summer term
Integration with the college’s sports systems (SOCS)
Parent briefings
Documentation updates
R2P has enabled Denstone to deliver a policy driven, data informed, and person-centred concussion response It supports every pupil through a recovery that prioritises long-term health over short-term performance
An essential part of Denstone’s success has been changing the culture around head injuries This has involved:
Equipping staff with the CRT6 Concussion Recognition Tool
Mandatory “Headcase” training from England Rugby
Sports Trauma Training for nurses and fixture leads
This holistic approach ensures that every adult in the school community is part of the safety net, not just medical or PE staff.
Despite advances, schools still face hurdles in delivering consistent head injury management, due to:
Time pressures during fixtures, which can lead to rushed decisions Budget constraints that may limit access to digital tools or external training
Persistent cultural norms around ‘toughness’ that can discourage pupils from reporting symptoms
However, Denstone is prioritising safety, embracing innovation, and advocating policy change
In conclusion, head injuries are among the most serious and underestimated risks in school sports and daily activities The move towards a structured, medically led approach is an essential evolution. By adopting national guidelines, leveraging tools like R2P, and embedding training and culture change throughout the school,
Denstone is demonstrating what comprehensive, compassionate, and clinically sound concussion care looks like.


Michelle qualified as a paediatric nurse in 1993 and spent 25 years at the Royal Stoke Hospital, specialising in acute medicine on the wards. During her tenure, she gained extensive experience in caring for children with conditions such as asthma, diabetes, epilepsy, and acute medical emergencies. She also provided mental health support for children and facilitated their transition from hospital back home, including the use of non invasive ventilation. In 2018, Michelle joined Denstone College, advancing to the role of Lead Nurse in 2023. She is passionate about ensuring that pupils with ongoing medical conditions receive comprehensive support and have full access to all aspects of education, regardless of their health challenges.
AUG 29 Medicines training annual refresher
AUG 29 Suicide awareness
SEP 2 School nurses’ annual update training
SEP 11 Approaching puberty: tackling tricky topics with confidence
SEP 15 NMS and inspection: a refresher for medical staff
SEP 16 New to the role: school nurses
SEP 23 Sports injury rehabilitation with a physio focus
SEP 25 Sports nutrition
SEP 30 Contextual approaches to vaping behaviour
SEP 30 Head injury management and assessment
OCT 1 Medication management for matrons
OCT 2 Supporting pupils with anxiety – practical tips and strategies
OCT 3 Leading a nursing team
OCT 6 Managing allergies, asthma and anaphylaxis
OCT 7 Coffee morning forum
OCT 7 First aid for mental health (2 days)
OCT 8 Diabetes in schools
OCT 9 Medical essentials for new boarding staff
OCT 10 Supporting colleagues through perimenopause and menopause
OCT 13 NMS and inspection: a refresher for medical staff
OCT 16 Migraine management in schools
OCT 20 Level 3 safeguarding certificate for school nurses (including DSL)
OCT 22 Epilepsy in schools
OCT 23 Understanding gillick competence and medical confidentiality



