




















By LaUra FreeMan
From cornerstone to completion in less than two years, the new Cooper Green Medical Center opened with a ribbon cutting November 20. A phased move,
department by department, has begun to allow a near-seamless transition through December with a few finishing touches as clinics settle into their new home.
“We will be leading with urgent care and cancer treatment, then begin



moving the specialty clinics, as much as possible over weekends so they will be ready to see patients on Monday,” David Randall, CEO of Cooper Green Mercy Health Services Authority and Chief Strategy Officer for UAB Health System,



said. “It’s going to be exciting working in such a beautiful, well-designed facility. So much thought has gone into creating a space that will allow us to enhance quality and expand the services we offer
(CONTINUED
By steve spencer
If you’re reading this and you’re over 40, odds are you’ve had at least one experience with back pain. In fact, back pain is the second most common reason people visit the doctor, behind only head colds.
Enter Bradley Goodman, MD. Goodman, who practices with OrthoAlabama Spine & Sports, has always been an early adopter of medical technology. He was the first doctor in the United States to offer Superion, a minimally invasive
implant to treat spinal stenosis. He was also the first in the country to perform the Intracept procedure to treat vertebrogenic pain.
So naturally when ReActiv8® came on the scene, Goodman was excited. “The beauty of ReActiv8® is that it’s designed to rehabilitate, not just alleviate pain,” he said. “Over the years, I’ve joked that when dealing with pain, I was a glorified hairdresser. I didn’t get rid of the gray hair. I was just putting color in
(CONTINUED











At the heart of one of the most highly regulated industries in the nation, health care facilities and providers face challenges that draw attention and resources away from their mission to provide quality patient care.
Burr & Forman’s health care team works alongside you to address and anticipate your needs by providing preventative guidance and pragmatic solutions, enabling you to focus on providing care and achieving healthy outcomes.
Alabama Health Care Team
Birmingham | Mobile | Montgomery
Jessie Bekker
Howard Bogard
Richard Brockman
Kelli Carpenter Fleming
Jim Hoover
Catherine “Cat” Kirkland
Garrett Lucey
Angie Cameron Smith



our patients. I’m confident it will become a national benchmark for improving care in the communities we serve.
“I’m particularly excited about the physical therapy department. It’s unlike any I’ve seen in this area. There are both indoor and outdoor facilities, including a veranda where patients can do their therapy in the fresh air. There’s a water therapy area, low impact water treadmill and a zero G gait system. Overall the department has the look and feel of a firstclass gym.
“We have a new MRI, and the pharmacy is larger and designed for better flow to make it easier for patients to pick up prescriptions. There is an eye clinic with optical shop, and the hematology/ oncology clinic has infusion bays where patients can receive treatment in a semiprivate space with natural light and entertainment.”
Returning patients are probably already be familiar with the new parking deck that was completed earlier in cooperation with UAB. Now they will be able to walk straight from the parking deck into urgent care with easy access to primary care and clinics.
Designed by architect Gresham Smith and built by Brasfield & Gorrie, the 211,000 square feet of space on Sixth Avenue South will also house a range of on-site specialty clinics similar to those in the Kirklin Clinic. These will be situated over four of the five stories with some of the space on the fifth floor reserved for support facilities and future growth. The center also offers several multipurpose spaces that can be used for meetings, education and training seminars. There is also a walking trail for patients and employees.
“As a county hospital, most of our patients come from Jefferson County,” Randall said. “However, anyone who needs our help is welcome. About a third of our patients have insurance and some have Medicare or Medicaid. Our mission is to provide quality health care when it’s needed. No one should have to wait for
access until their economic circumstances are better.
“The new facilities are fantastic, but one of our greatest strengths is the commitment of our staff. Those who choose to work in a county hospital are special people. Their first motivation has to come from the heart. They go into health care because they want to help others.”
Originally known as Mercy Hospital when it opened in 1972, it was renamed to honor former mayor Cooper Green. As the next generation hospital, urgent
care facility and clinics move into the rhythm of a new setting, Randal looks forward to expanding its outreach in preventive medicine and wellness.
“Why wait for someone to become sick and come to us?” he said. “If we can go to them and show them how to stay healthy and avoid diabetes, hypertension, heart disease and so many other preventable conditions, they win with a better quality of life. The county’s health care budget also wins with more dollars that can be used to help someone else.
“Community outreach offering services like flu and pneumonia shots doesn’t just save expensive hospitalizations. It can save lives.”
When people need the best of lifesaving care for serious illnesses and injuries, the new Cooper Green Medical Center is here for them. It is also here for them to help protect their health so they can enjoy every day of a longer, healthier life.


“For


By Jane ehrhardt
“We’re still so early in learning so much about the gut microbiome. It’s in its infancy right now,” says Carmen Lopez, MD, gastroenterologist with G.I. Associates of West Alabama. So far, 19 conditions from six systems or organs in the body—none of them the stomach— have shown an association to the health of the gut microbiome. They run from cardiovascular disease, Alzheimer’s, and rheumatoid arthritis to hyperthyroidism and multiple sclerosis.
As the largest surface of interaction between the external world and internal environment, knowledge of the GI tract continues to expand and accepted practices go out of date. Or some seem to have become forgotten, though they remain true.
Should aspirin be prescribed to help prevent colorectal cancer?
Patients taking aspirin for certain cardiovascular risk factors have shown a decreased rate of colorectal cancer.
“Some of the early data seen in these patients had lower rates of colon cancer,” Lopez says. “But it’s not yet to the point where we would automatically put someone who is at risk on aspirin.” Nonethe-
less, if a patient has another indication for aspirin, adding that it can also help protect from colon cancer might be useful motivator.
The caveat to colorectal screening
Starting colorectal screening at age 45 is now a given for every average-risk patient. “The caveat to this, though, is that if you have a family history of colorectal cancer, especially in a first-degree relative, then you should begin your screening at 10 years younger than the age of diagnosis of your relative or at age 40, whichever is younger,” Lopez says. So if a parent was diagnosed with colorectal cancer at age 45, then start screening that patient at age 35. If the parent was 60 years old when diagnosed, start at 40.

matory bowel disease.
Probiotics. Yes or no?
“There are three things I check for to make sure I really believe someone has IBS before just slapping that diagnosis on them,” Lopez says. “Whenever I suspect that they might have IBS with diarrhea, I always rule out celiac disease.” She also checks thyroid levels to rule out a thyroid condition leading to their diarrhea, and she checks for a stool inflammatory marker, such as a fecal calprotectin to make ensure they don’t have inflam-
“Patients ask all the time whether or not they should be on probiotics,” Lopez says. “The answer to that question right now is ‘no’. We don’t have enough data suggesting that probiotics are beneficial. The data is inconsistent. The biggest problem with studying probiotics is the large number of brands that use so many different strains and different numbers of bacteria. We don’t know yet which probiotic is actually going to be the best probiotic.
And my suspicion is that each individual patient is probably going to need some different combination of bacteria.
“If a patient is insistent on trying probiotics, I suggest they try one for 30 days. If they don’t feel better, switch probiotics. I haven’t seen any evidence of any harm in probiotics. The only real negative is you are spending money on something that may not be helpful.”
How is IBS affected by a woman’s hormones?
“I don’t think it’s well-known that estrogen increases sensitivity to pain or anxiety and inflammation,” Lopez says. “During menstruation, women often report much more frequent symptoms, and menopause and hormone replacement worsen their symptoms. So if they have significant IBS symptoms, hormone replacement becomes a risk/benefit discussion with the primary care. Unfortunately, birth control hasn’t shown to help with IBS symptoms.”
What are primary cares missing about managing IBS?
“Probably the biggest thing would be offering patients the low FODMAP diet,” Lopez says. The diet eliminates high fermentable-carbohydrate foods for two to
(CONTINUED ON PAGE 7)







Dr. Charles Hunt and our staff at Alabama Vein are dedicated to administering personal, compassionate, and state-of-the-art therapies in the treatment of saphenous vein re ux disorder and varicose veins. Dr. Hunt is board certi ed by the American Board of Venous and Lymphatic Medicine and in General and Cardiovascular Surgery.
• Patient coordinators for immediate response to referrals and questions



• Conscious sedation by a board-certifi ed CRNA


• Detailed initial evaluation and exit letters sent to the referring doctor









- By
Marianne Kolbasuk









Our HERO is the ambitious Practice Manager whose life is wrapped up in the success of the business – income, mortgage, retirement, even the kids’ college. They have a sense of humor but are constantly thinking about ways to improve their business, maximize productivity, and MANAGE RISK. They’re passionate about their business and take it personally when a competitor, hacker, or employee threatens their mission to improve the world.
McGee | Nov 1, 2024 | Gov Info Security



- By Paul Bischoff | Nov 5, 2024 | comparitech.com Embargo ransomware group claims attack on American Associated Pharmacies




Apathetic or complacent US businesses who are willing to accept UNLIMITED RISK by ignoring today’s threats. Business owners who think, “it won’t ever happen to me.” Foreign Governments seeking footholds in the US or leverage. Cybercriminals who believe that all Americans are rich and therefore justified targets. Global crime syndicates who employ thousands in an Enterprise organizational structure. IT and Cybersecurity companies who take advantage of unwitting customers with Projects and Hourly Billing. The Cybersecurity industry as a whole, which has bored and confused the entire US public into a state of wanton vulnerability, while the hackers get better every day.

- Posted by Steve Alder | Nov 14, 2024 | The HIPAA Journal










Schedule a 10-minute discovery call, and we’ll donate $150 in your name to Hand in Paw. Doctor hit with $500K HIPAA fine: feds worse than hacker









Practice Managers who are mature enough to understand that THEY OWN ALL THEIR COMPANY’S RISK, and who are willing to have routine, honest, and candid discussions about CYBER RISK MANAGEMENT and CYBERSECURITY / REGULATORY COMPLIANCE. They understand that by getting buttoned up and taking RISK seriously, they can maximize productivity, retire earlier, and send the kids to college debt-free. We are for HAVING FUN while making clients SAFER FROM CYBERCRIME. You know, CybertechnoLOLogy!


The solo “IT Guy” who doesn’t have the time, desire, or skills to keep up with ever-changing threats and subsequent countermeasures. Technology companies that baffle their customers into spending money on things they don’t need. MIND-NUMBING CYBERSECURITY TRAINING AND CONTENT that BORES AND CONFUSES NORMAL PEOPLE INTO NEVER GETTING ANY SAFER FROM CYBERCRIME. ANTIcybertechnoLOLogy.


CybertechnoLOLogist www.sipoasis.com


howard e. Bogard, esq
Every health care provider has “credit balances,” which occur when a provider receives more money than it is owed for services rendered. Credit balances can be caused by a number of factors, including incorrect coding, duplicate payments, medical necessity errors, overpayments by patients or payers and miscalculated coinsurance or out-of-pocket costs. Health care providers should establish formal procedures to work credit balances on a regular and consistent basis in order to return such balances to the appropriate payer or patient in a timely manner. If the beneficiary of a credit balance cannot be identified or found, Alabama law requires that the applicable overpayment amount be submitted to the State as unclaimed property.
A failure to return credit balances to a commercial insurer in a timely manner may result in a breach of the agreement between the provider and insurer, thereby giving the insurer the right to terminate the provider agreement. However, a failure to return credit balances to Medicare or Medicaid in a timely manner can result in significant financial penalties well in excess of the amount of the credit balance. On November 1, 2024, the Centers for Medicare and Medicaid Services (“CMS”) revised its rules regarding the identification, reporting and return of Medicare and Medicaid credit balances and in doing so imposed on providers strict time-frames to return overpayments owed to either program (the “Final Rule”). The Final Rule becomes effective

Howard E. Bogard, Esq.
January 1, 2025.
By way of background, the federal overpayment rule, sometimes referred to as the “60-Day Refund Rule,” was enacted as part of the 2010 Affordable Care Act and requires providers to report and return Medicare and Medicaid overpayments within 60 days after the overpayment is “identified.” A failure to comply with the 60-Day Refund Rule can result in the imposition of a civil monetary penalty of up to $24,947 for each separate overpayment. Further, a failure to timely refund an overpayment to Medicare or Medicaid may result in the violation of the federal False Claims Act (“FCA”), which includes additional financial penalties and, in some cases, may subject the provider to a government imposed compliance plan called a Corporate Integrity Agreement.
Prior to the adoption of the Final Rule, CMS took the position that an overpayment is deemed to have been “identified” when the recipient has either actually determined or should have determined “through the exercise of reasonable diligence” that it received an overpayment and has “quantified the amount of the
overpayment.” CMS had suggested that “most” overpayment investigations should be completed within 180 days, but did not impose a formal deadline. Accordingly, investigations undertaken in good faith and with reasonable diligence could last beyond the 180-day period.
Following a 2018 ruling by the U.S. District Court for the District of Columbia finding that the “reasonable diligence” standard under the then existing 60-Day Refund Rule was improper, CMS revised its definition of “identified” in the Final Rule to align it with the FCA definition of “knowingly.” Specifically, CMS revised the definition of when an overpayment has been “identified,” thus triggering the 60-day report-and-return clock, as follows: “A person has identified an overpayment when the person knowingly receives or retains an overpayment. The term “knowingly” has the meaning set forth in [the federal civil False Claims Act].” For purposes of FCA liability, the term “knowingly” is defined as having “actual knowledge” of false information and/or acting in “deliberate ignorance” or “reckless disregard” of the truth or falsity of information. Thus, a failure to actively and routinely work credit balances could trigger a finding that the provider acted in deliberate ignorance or reckless disregard of the need to return the overpayment.
the provider conducts a “timely, goodfaith investigation” to determine whether related overpayments exist, the 60-day deadline for reporting and returning the initially identified overpayment and related overpayments will remain suspended until the earlier of:
(A) The date that the investigation of related overpayments has concluded and the aggregate amount of the initially identified overpayments and related overpayments is calculated; or
(B) The date that is 180 days after the date on which the initial overpayment was identified.




Under the Final Rule, CMS has, for the first time, established a hard deadline to return any Medicare or Medicaid overpayments to avoid liability. The Final Rule provides that when an initial overpayment has been identified (under the FCA definition of “knowingly”) and
The end result is: (1) a maximum of 180 days to investigate and quantify in good faith any overpayment with the clock starting at the point the provider has “actual knowledge” of the first overpayment or acts in deliberate ignorance or reckless disregard of the first overpayment, plus (b) another 60 days to return the overpayment, which runs from the earlier of the date the investigation is concluded or 180 days after the date the initial overpayment was identified. If a provider does not undertake a “timely, good-faith investigation” with respect to a possible overpayment, the provider only has 60 days to return the overpayment. If a provider does undertake a “good-faith investigation” the 60day period is suspended for up to 180 days to investigate both the initially identified overpayment but also “related overpayments” that are suspected to “arise from the same or similar cause” as the initially identified overpayment. This approach by CMS results in a provider having no more than 180 days to resolve all factually similar overpayments, even if the provider identifies a related overpayment on, for example, day 150 of the investigation. Further, if the provider has not completed its good faith investigation within the 180-day time period, it faces FCA liability based on a finding that it was not acting in good faith due to the failure to complete the investigation in a timely manner.





For larger institutions, such as hospitals and nursing homes, meeting the 180-day time period may prove to be very challenging, especially for complex or multi-faceted related overpayments. Nonetheless, it is important for all providers to act diligently in identifying, investigating and returning any credit balances owed to the Medicare and Medicaid programs in a timely manner and to document the date of identification and the provider’s “good faith” investigation process.
Howard Bogard is a Partner at Burr & Forman LLP and works exclusively with health care providers on corporate and regulatory matters. He can be reached at (205) 458-5416 or at hbogard@burr.com.
there. Now we can actually do something about pain rather than just offering palliative treatments like nerve blocks.”
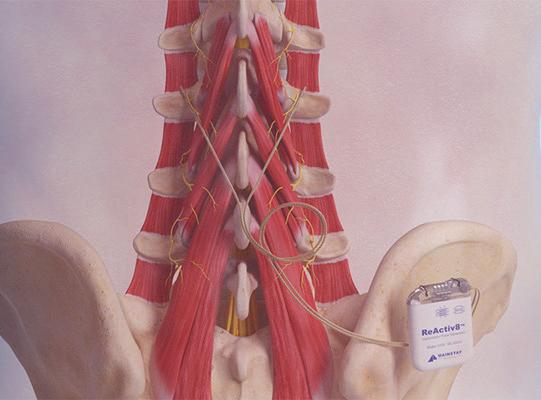
ReActiv8® focuses on mechanical chronic lower back pain (CLBP), one of the most common types of CLBP. Many people with CLBP find themselves unable to sit for an extended period without their pain increasing. The pain is often unrelenting. Mechanical CLBP can start from a number of issues, anything from a herniated disc to a vertebral fracture. Regardless of the cause, the pain can become debilitating, and as a person reacts by moving less and less, the multifidus muscle, which runs along the length of the spine, begin to atrophy. This is critical because the multifidus stabilizes the back, and when it’s weakened, it leads to instability in the lower back, causing chronic pain.
“We can see the atrophied multifidus on an MRI,” Goodman said. “But over the 30 years I’ve been doing this, I ignored it because there’s nothing we could do about it. We can put patients in physical therapy, but because that muscle has been disinhibited for so long, the therapist can’t really reactivate it. After months or maybe years of disuse, the brain has turned off that pathway.”
The ReActiv8® Restorative Neurostimulation system changes this. ReActiv8® is a small generator, about the size of a matchbox, that is implanted under

the skin in the lower back through a minimally invasive outpatient procedure. Similar to a TENS unit, it targets the nerves that innervate the multifidus muscle with electrical pulses delivered through lead technology. The stimulator is bypassing the neural pathway that has been shut off to reactivate the multifidus muscle. After the procedure, the patient uses the stimulator with twice a day, 30-minuate sessions, which can feel like a deep tissue massage. Now that the multifidus muscle is reengaged, they can also participate in physical therapy.
So far, the device has proved to be very effective. In a trial, clinicians asked patients to rate their pain intensity using
continued from page 1
a visual analog scale (VAS) score before the device was implanted. Three years later, when the same patients were asked to rate their current pain level, 77 percent of them reported a pain reduction of 50 percent or greater.
One of Goodman’s early patients was Kelly East. Her pain was constant. She was unable to sleep on her left side, and she was having spasms. Her hip and her legs would go numb. She’d be up until 2:00 a.m., straining to get comfortable, trying to sleep. This woman who used to enjoy working in the yard, cutting grass and weed eating, now could barely bend over to pick up a plate. She had been getting nerve blocks, but they only worked for two or three weeks. Doctors found multifidus atrophy on an MRI and referred her to Goodman. After the ReActiv8® procedure had reactivated her multifidus muscle, she started physical therapy. Today, she is back to cutting the grass, engaging comfortably in all the activities she did before.
Not everyone is a candidate for ReActiv8®, but for the many people whose chronic back pain is due to multifidus atrophy, there is finally a therapy that doesn’t just alleviate the symptoms; rather, one that can actually attack the source of the problem.
continued from page 4
six weeks, then slowly reintroduces them one at a time to identify which foods trigger the IBS symptoms. The list of foods is long.
Primary care physicians could also recommend a natural over-thecounter peppermint oil. “It’s a supplement that has been proven to help with the abdominal pain discomfort and bloating associated with IBS,” Lopez says. “These are often two of my first go-tos that are really minimal risk and well tolerated.”
What’s next?
“As we go forward, I think we’ll find that the gut microbiome is connected to everything—heart disease, Alzheimer’s, mental health, obesity, diabetes,” Lopez says. “Right now, it’s easy to focus on the problem that a patient is presenting with. But I think that in the future we’ll have more holistic thinking about gut health and its role in not just managing, but preventing some of these diseases.”

By steve spencer
25 to 30 million Americans suffer from venous reflux disease. This problem starts when the valves in the saphenous veins are damaged. The great saphenous vein is the longest vein in the body, running along the medial side of the leg from the foot to the top of the thigh. The small saphenous vein runs along the inner thigh.
“When we stand, gravity wants to pull the blood from our head to our feet,” said Charles Hunt II, MD, FACS, RVT of Alabama Vein & Restoration. “To prevent the blood from flowing the wrong direction and staying in our legs, we have 21 valves in the great saphenous vein and between nine and 12 in the small saphenous vein. This prevents reflux down the vein. With venous reflux disease, either through dilation or damage to the valves, blood begins flowing backwards in the saphenous veins causing congestion in the leg. Now we have excessive amounts of pressure within these veins and fluid. The pressure gets so great that the water leaks out of the veins into the tissue which causes your leg to swell. Also, red blood cells can leak out and then they deposit iron in your skin which results in discoloration.”
In addition to swelling and discolor-
ation, other signs of the disease can include leg pain or heaviness; cramping; or restless leg syndrome.
The etiology of restless leg syndrome involves several factors including sleep apnea. However, in about one-third of venous reflux patients who also have restless leg, the restless leg gets better after treatment. “Many venous reflux sufferers are constantly moving their legs unconsciously because moving causes the calves to pump the blood out of your legs which alleviates the pain,” Hunt said.

introduce a needle into it. It’s like a piece of leather wrapped around wood.
“You can get venous ulcers on the bottom of your foot or on the tip of your toe, open lesions that won’t heal. It’s terribly painful. After we ablate the damaged veins that are causing the venous reflux, the wound will heal. In one case, I saw a man who had been treated for venous ulcers for 10 years, and following the ablation, the ulcers healed in a month.
blood thinners as some form of anticoagulant for a period of at least three to six months to make sure that resolves.”
If left untreated, venous reflux disease can cause a number of complications. It can negatively impact the lymphatic system by causing excessive fluid buildup in the tissues, which overwhelms the lymphatic system’s ability to drain fluid, leading to potential damage to lymphatic vessels and ultimately resulting in lymphedema.
Venous reflux disease can also lead to destruction of the patient’s skin. “Through swelling, the skin stretches and then the arterial blood flow can’t get to your skin and it starts to die,” Hunt said. “I’ve had patients with skin so hard that you can’t
“Venous reflux disease is also considered the underlying cause of varicose veins. We think of them as cosmetic, but while I can’t predict the odds of a blood clot, if you get a blood clot in a varicose vein, it’s been my experience that 40 percent of the time, there is the risk that it can propagate or grow into the deep system. Now you go from superficial thrombophlebitis to deep vein thrombosis. And as a consequence, that clot can then mobilize and go to your lungs where it can block a lung artery resulting in a pulmonary embolus, which can be fatal.
“When we have a patient with superficial thrombophlebitis, we put them on
At UAB Medical West, our team of orthopedic specialists are dedicated to helping patients restore mobility and enhance their quality of life. We are committed to bringing quality orthopedic care to the residents of West Jefferson County, AL, and are thrilled to welcome Dr. Jay Fitts to our team. Dr. Fitts specializes in spine surgery and is now accepting new patients at both our main hospital location and our Hoover location. To schedule an appointment, call us today at (205) 481-8570.


Hunt treats conditions that result from venous reflux, like varicose veins, while performing the ablation procedure to treat venous reflux itself. He uses a 1320 nanometer wavelength laser, which requires less heat to close the vein, and has a 99 percent efficacy rate of closing the treated vein. The laser targets water in the vein wall, unlike older lasers that target blood, which makes the procedure more comfortable with minimal post-op bruising or swelling. It’s an outpatient procedure, using local anesthetic, and usually takes around 45 minutes. Patients usually go home the same day.
While minimally-invasive, ablative treatment is the ultimate solution, and the disease must be treated before it devolves into conditions like skin discoloration, skin hardening, and ulcers, there are a few steps people can take to help alleviate the symptoms: wear compression stockings to help blood flow; elevate your legs to reduce swelling; exercise regularly to improve circulation. Ultimately, early intervention is critical to prevent progression of the disease.






Main Hospital 5000 Medical West Way, Suite 404 Bessemer, AL 35022
Hoover Primary & Specialty Care 5310 Medford Drive Hoover, AL 35244

















































UAB Epidemiologist Receives AHA Population Research Prize

Virginia Howard, PhD, Distinguished Professor at the UAB School of Public Health, received this year’s Population Research Prize at the American Heart Association’s Scientific Sessions 2024. Her research career focuses on stroke and many factors contributing to the unequal burden of stroke.
Howard is the lead stroke epidemiologist for the national Reasons for Geographic and Racial Differences in Stroke study, a 25-year cohort study, sponsored by the NIH. She has been one of the lead clinical trial epidemiologists for five major stroke primary or secondary prevention multicenter clinical trials. She is a longtime co-director of the Analysis Core and mentor on UAB’s Deep South Resource Center for Minority Aging Research funded by National Institute on Aging.
Governor Ivey has appointed Brittney Anderson, MD of Anderson Family Care in Demopolis to the board of trustees of the Alabama School of Healthcare Sciences which opens in the fall of 2026. The school will be located in Demopolis and offer high school students a STEMM curriculum focused on healthcare. Through partnerships with health systems and educational institutions, it will help alleviate the rural healthcare workforce shortage in Alabama while providing skilled professional training for in-demand jobs to
low-income youth.
“It is an honor to be appointed by Gov. Ivey to the Board of Trustees,” Anderson said. She grew up on a small family farm in Autauga County, and attended Duke University for undergraduate studies and obtained a Master’s Degree in Rural and Community Health from The University of Alabama. She received her medical degree from UAB School of

Brittney Anderson, MD
Medicine in Birmingham in 2014.
In 2020, she was presented with the University of Alabama School of Medicine Distinguished Young Alumni Award. She is the current President of the Alabama Chapter of the American Academy of Family Physicians and serves as an officer with the Medical Association of the State of Alabama.
With over 25 years in the healthcare industry, Jarrod Johnson has been named the CEO of UAB Callahan Eye. Johnson comes to UAB from the University of Pittsburg Medical Center in Pennsylvania, where he served as president of UPMC Carlisle. There he headed up recruitment efforts, expanded service lines and improved patient access, while achieving cost savings through reduced lengths of stay.
Prior to the UPMC post, he served as COO of Cook County Health Sys-
tem in Chicago, and had roles at Erie County Medical Center in Buffalo; Brooks Memorial Hospital in Dunkirk, New York; Optim Health System in Savannah; UK King’s Daughters Medical Center in Ashland, Kentucky; and Alegent Health Omaha.

Jarrod Johnson
Johnson holds a Bachelor of Arts degree in economics from Lehigh
University in Pennsylvania and an MBA from Howard University. He also received a certificate in managing health care delivery from Harvard.
“UAB Callahan Eye has a rich history of excellence in eye care, and I am excited to be part of such a dedicated group of professionals,” Johnson said.
Health care providers with business interests across the South turn to Phelps for counsel on their legal needs.
Physician groups, health care systems, rural hospitals, dental practices, individual physicians and everything in-between, turn to Phelps for day-to-day-counsel as well as for their most pressing legal issues and business opportunities. It’s more than our casework that sets us apart. It is our energy and passion for solving our clients’ challenges.
Physician groups, health care systems, rural hospitals, dental practices, individual physicians and everything in-between, turn to Phelps for day-to-day-counsel as well as for their most pressing legal issues and business opportunities. It’s more than our casework that sets us apart. It is our energy and passion for solving our clients’ challenges.
Physician groups, health care systems, rural hospitals, dental practices, individual physicians and everything in-between, turn to Phelps for day-to-day-counsel as well as for their most pressing legal issues and business opportunities. It’s more than our casework that sets us apart. It is our energy and passion for solving our clients’ challenges.

Kassouf & Co Director
Gerard Kassouf was named one of Money’s Best Financial Planners in 2024, one of the 80 best financial planners in the United States.
“It is an honor to be recognized among this group of dedicated advisors. This recognition is a testament to how we help clients through every life stage at Kassouf and Kassouf Wealth Advisors. Excellent client service is at the core of everything we do,” said Gerry Kassouf. He is a CERTIFIED FINANCIAL PLANNER™ practitioner, Certified Public Accountant, Personal Financial Specialist, Chartered Global Management Accountant®, and Accred-

ited Estate Planner®.
Money surveyed 1,000 financial planners, examining qualifications, trust, services, and customer service. Gerry Kassouf is the only financial planner in Alabama to earn the honor.
“This award is a testament to my father’s attention to his clients and knowledge of financial planning. It is amazing to see how he has served clients for multiple generations. They not only trust him with their own finances, but they trust him with their children’s and grandchildren’s finances. There is no better example of trust,” said Kassouf Managing Director Jonathan Kassouf.
Starting October 1st, Cooper Green no longer charges enrolled patients whose enrollment status qualifies them to be covered by the indigent care fund for generic prescription medication, in addition to significant reduction in brand name medication pricing.
Recently enrolled patients at Cooper
Green can now find their health plan code printed directly on their issued cards. Patients with a health plan code A through E qualify for the new savings. There are no restrictions to quantity or frequency of prescriptions covered. Cooper Green will refill prescriptions within one week of the patient’s running out of the medication.

As the #1 cause of mortality in the United States, cardiovascular disease has long been a focus for medical researchers like Steven Rothenberg, MD, assistant professor in the University of Alabama at Birmingham Marnix E. Heersink School of Medicine Department of Radiology.
With the help of the Bill L. Harbert Institute for Innovation, the university’s hub that provides the infrastructure to commercialize inventions by the campus community, Rothenberg has cofounded Body Check, a UAB startup



Confused by recent news of Blue Cross awarding a sole source contract to just one lab? Don’t worry. We’re right in your backyard, and we remain accessible for all your lab needs as a BCBS of AL in-network lab.


focused on developing artificial intelligence algorithms that identify patients with underlying cardiovascular diseases such as cardiomegaly, or enlarged heart.
“Currently, the diagnosis of cardiomegaly is subjective and inconsistent,” said Rothenberg, a cardiopulmonary radiologist. “Even though cardiomegaly is highly predictive of future cardiovascular events, it is typically underreported, resulting in inconsistent care. Body Check, which recently received FDA clearance, can ensure access to care for high-risk individuals.



Steve
VICE
Jason Irvin
CREATIVE DIRECTOR
Katy Barrett-Alley
CONTRIBUTING WRITERS
Jane Ehrhardt, Ashley Franco, Laura Freeman, Lynne Jeter, Marti Slay
Birmingham Medical News
270 Doug Baker Boulevard, Suite 700-400, 35242 205.215.7110
AD SALES: Jason Irvin, 205.249.7244
All editorial submissions should be e-mailed to: editor@birminghammedicalnews.com
In November, the Alabama Chapter of the Association of Medical Facility Professionals (AMFP) celebrated their Official Launch with a large crowd of healthcare built environment professionals at Dread River Distillery. The Alabama group is the 29th Chapter of AMFP which has experienced rapid growth since 2019. Through the end of 2024, AMFP will have established 31 Chapters across the US with plans to launch 10 New Chapters in 2025.
AMFP Alabama is dedicated to improving the healthcare built environment in Alabama by being a hub where industry leaders share ideas, gain knowledge, solve challenges, connect with peers, and shape the future of the industry. The AMFP is bringing together hospital administrators, facility managers, real estate directors, medical property owners, planners, architects & designers, contractors, consultants, vendors, and academics specializing in various healthcare environments.

Orlando Health has donated $25,000 to the Baptist Health Foundation’s New Generation Nurses Fund. Contributions to the fund are matched dollar-per-dollar by the Baptist Health Foundation and the Baptist Health System, bringing the total gift to $75,000. The funds will be used to support the Moffet & Sanders School of Nursing at Samford. A scholarship will be awarded to a student each year in the nursing school who has financial need and plans to practice in the greater Birmingham area.
“This scholarship will help grow the nursing profession in Central Alabama,” said Kelly Edmondson, vice president of nursing and patient care, Orlando Health.
After identifying Central Alabama’s nursing shortage as the most urgent crisis in patient care, the Baptist Health Foundation and Baptist Health System established the fund in 2023.
“After reaching our initial goal of
a $1.5 million endowment, we are now focusing on surpassing $2 million,” said

birminghammedicalnews.com










