Welcome to the latest issue of Bioscientist Magazine, where we explore the cutting-edge developments and profound insights that shape the world of bioscience. The boundaries of human knowledge continue to expand, and the biosciences continue to unravel the mysteries of life itself. We are delighted to bring you a diverse range of articles that capture the essence of exploration, innovation, and the relentless pursuit of knowledge that defines our field.
For this issue, our central theme is ‘New Beginnings,’ where we delve into novel avenues for personalised medicine, stem cell research, disease prevention, mental health, and even appreciation for social media as a way for scientists to communicate with each other Moreover, our magazine is enriched with valuable inputs from various academics speaking out about well-being and career advice, mainly targeting Biomedicine students, but also inviting them to explore other paths of interesting tips and tricks on how to best prepare for your prospects
We are honoured to have featured articles in the form of interviews with University of Cambridge academic Craig Brierley and the IBMS (Institute of Biomedical Science) Executive Head for Education, Sue Jones. Indeed, it is a matter of pride for us and the whole University as The Bioscientist reaches new levels and gains increased recognition with time. We thank Craig and Sue for their time and willingness to participate in Issue 4
We remain committed to delivering thought-provoking content that fosters a deeper appreciation for the wonders of bioscience and hopes to inspire you to engage with the scientific community, ask questions, and explore everything this issue offers Thank you for your continued support, and may your reading be as enlightening as the discoveries we present within these pages Enjoy!
Sara Alnasir Kassam and Wiktoria Wisniewska
CO-EDITORS-IN-CHIEF
Markella Loi discusses how childhood cancer treatment is related to cardiomyopathies
Harriet Burrow delves into the
and personal encounters with
Stem Cells and Blood Transfusion
Smoking and Vaping: Preventing and Quitting
Long COVID - Widespread Impact
Socioeconomic issues impacting dental healthcare
Biomaterial that heals tissue from inside out
TOPICS IN BIOMEDICINE
Advantages and Issues with Stem Cell
Therapy in the Treatment of Type 1
Diabetes
Alzheimer’s Progression and Effect
IVF - Why is it failing?
Is the ethical dilemma in embryonic stem cell research saving lives or protecting human-biased sentiments?
SALFORD SCIENCE
Markella tells us about her project in collaboration with Kidscan
Mary Yuhanna asks Arijit what the future of genomic sequencing may be and which secrets it shall unlock They are also discussing genomic sequencing as a tool for personalised healthcare
BIOSCIENTIST MAGAZINE
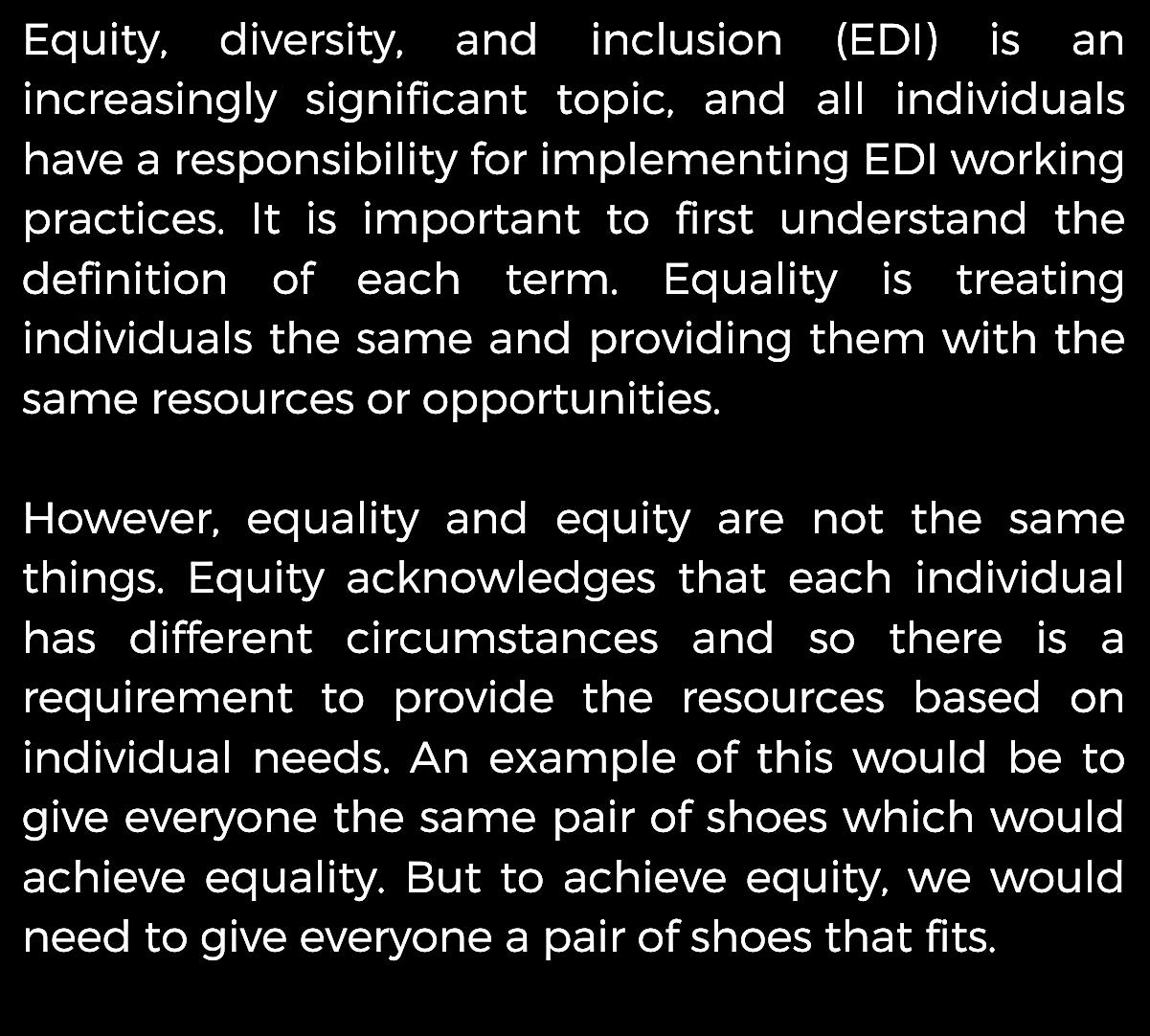
Tahmina Hussain on the importance of EDI efforts to ensure respect and celebration of all backgrounds within a workplace
Our alumni Hani describes her journey to becoming a MSc Physician Associate student
Lloyd Mcleggon-Watkinson talks about his experiences with mental health in the workplace and gives our readers advice
Craig Brierley from University of Cambridge discusses careers in Science
Sue Jones tells us the IBMS’ approach to developing our future biomedical
Dr Sara Namvar talks about key events to look forward to
Hani, a Salford alumna, discusses her journey to Physician
Associate studies and what the application process entails
Lloyd McleggonWatkinson recalls 7 years working in a lab and how he maintained his mental wellbeing
Course reps collective article on how best to prepare for the start of the academic year
Congratulations to Ashleigh Howard
Explore what type of support is provided by the University of Salford’s Student Support Service: AskUS
Joy explains how promising the stem cell derived β-cell-like organoids can be in the treatment of Type 1 Diabetes
BIOSCIENTIST MAGAZINE
THE BIOMEDICINE SOCIETY
HOW TO GET INVOLVED
Some information on what is involved in the Biomedicine Society and how to join
SOCIETY YEARLY ROUNDUP
Sara Alnasir Kassam, the society’s secretary, discusses the events within the society this year including the Beehive Sessions Sports Collab sessions and much more!
COLLABORATING WITH KIDSCAN
Julia Cassarotti speaks about the society’s charity collaborations this year, specifically highlighting the importance of childhood cancer research
PASSIONFLASH 2023
Hear from Yamen Toumeh, this year ’ s Passionflash winner, who shares his experience as a participant
BIOART COMPETITION
Bioart Support Bee Tasfia Hazari reflects on the competition this year, with the Bioart exhibition being an unmissable event
LONG COVIDLONG IMPACT
Wiktoria explores the newfound research as well as guided treatment initiatives against long Covid
RESTORE TRIAL: LAB-MADE BLOOD
Aisha sheds a light on the future of blood transfusions from lab-grown blood cells
pg.2 pg.2
SCIENCE IN THE NEWS SCIENCE IN THE NEWS
Read about the term long covid, smoking/ Read about the term long covid, smoking/ vaping and how it can be prevented and vaping and how it can be prevented and RESTORE trials influence on blood transfusion
RESTORE trials influence on blood transfusion
pg.10 pg.10
RESEARCH SPOTLIGHT RESEARCH SPOTLIGHT
We put a spotlight on the increasing prevelnace
We put a spotlight on the increasing prevelnace of fear of dentists and how this can be reduced of fear of dentists and how this can be reduced and the future use of biomaterial to heal tissues and the future use of biomaterial to heal tissues
pg.14 pg.14
TOPICS IN BIOMEDICINE TOPICS IN BIOMEDICINE
Students discuss the use of stem cells in Type 1
Students discuss the use of stem cells in Type 1 diabetes, the progression of Alzheimer’s Disease, diabetes, the progression of Alzheimer’s Disease, IVF success in ethnic minorities and early IVF in ethnic minorities and early research into embryonic stem cells research into embryonic stem cells
pg.25 pg.25
SALFORD SCIENCE SALFORD SCIENCE
Exciting insight into ongoing
Exciting insight into ongoing research on research on childhood cancer treatments relating to childhood cancer treatments relating to cardiomyopathies and an interview with Dr Arijit cardiomyopathies and an interview with Dr Arijit Mukhopadhyay discussing genomic Mukhopadhyay discussing genomic advancements and the future of whole exome advancements and the future of whole exome ssequencing equencing
NHS Blood and Transplant (NHSBT) and the University of Bristol are working together on the first ever clinical trial for transfusing red blood cells developed in vitro. This seminal study is called ‘Recovery and survival of stem cell originated red cells’ (RESTORE), (NHS Blood and Transplant, 2022) and it compares how long lab-made red blood cells can survive in the body compared to donated red blood cells⁴ . The trial started in August 2018 and is projected to last until May 2024² The RESTORE clinical trial has been planned meticulously. It is a phase one randomised, single blind clinical trial: the participants do not know whether they are in the control group or the experimental group receiving the labgrown red blood cells² This clinical trial is a true multicentre effort, with input from experts at three different centres (Figure 1)
their Advanced Therapies Unit in Filton make the red blood cells using CD34+ cells isolated from the donors’ blood⁴⁵ .
Then the Radiopharmacy Unit at Guy’s and St Thomas’ Hospital labels the manufactured red blood cells (mRBCs) with a tracer element to help keep track of the cells once they are transfused into the participants⁴ . Finally, at the Clinical Trials Unit at Addenbrookes’ Hospital Cambridge, the mRBCs are transfused into healthy participants sourced through the NIHR BioResource⁴ . Two small transfusions of around 10 mL were made with a gap of at least four months between the first and second transfusion⁴⁶ As of November 2022, two people have received the lab-made blood transfusions and no adverse effects have been observed No further transfusions have been publicly reported, but the researchers are hoping to perform these transfusions on at least 10 participants⁴
1: The mRBCs journey starts at NHSBT Filton with haematopoietic stem cells from initial blood donors making its way to patients in Addenbrookes' hospital⁴ .
Figure
Manufactured red blood cells have the potential to change how blood is sourced for transfusions. The immediate aim for the researchers is for mRBCs to be used for patients with rare blood types and patients with blood disorders who require regular transfusions² For rare blood types, finding a donor can be difficult especially when looking worldwide³ While Bristol is also home to the International Blood Group Reference Laboratory which can aid in this search, there are instances when a donor cannot be found³ . Similarly, with patients who require regular blood transfusions, the chance of developing antibodies against different blood types increases each time they have a blood transfusion which can lead to the donor pool becoming narrow¹ While this clinical trial is important with many benefits if the initial findings are positive, the researchers believe that this technology can only really be used in complex scenarios meaning blood donors will still have a significant role to play in saving lives⁴ .
Previous research suggests that it takes about 21 days to make red blood cells from haematopoietic stem cells using various growth media⁷ Combined with the fact that the number of haematopoietic stem cells being isolated from donor blood is low, it means that it is difficult to scale up the production of red blood cells⁷ . There are alternative sources of stem cells like induced pluripotent stem cells and embryonic stem cells These alternatives are different due to their relatively infinite supply which means that they could be more scalable⁷
With the ongoing research in this area of transfusion science, the possibility of a future with blood transfusions without donors feels more probable day by day. However, in the meantime life-saving blood transfusions are needed every day, so signing up to become a blood donor is something you can do today to help
References:
The link below can provide more information on how to donate: https://www blood co uk/
2
3
4
5
6
7
Alves V M Martins P R Soares S Araújo G Schmidt L C Costa, S S, Langhi, D M, & Moraes-Souza, H (2012) Alloimmunization screening after transfusion of red blood cells in a prospective study Rev Bras Hematol Hemoter, 34(3), 206211 https://doiorg/105581/1516-848420120051
1 Anonymous (2023) Recovery and survival of stem cell originated red cells ISRCTN Retrieved 07/03/2023 from https://wwwisrctncom/ISRCTN42886452
Nance S J & Ms M S (2007) The utilization of rare blood donors ISBT Science Series, 2(2), 59-63 https://doiorg/101111/j1751-2824200700113x
NHS Blood and Transport (2022) First ever clinical trial of laboratory grown red blood cells being transfused into another person Retrieved 05/08/2023 from https://wwwnhsbtnhsuk/news/first-ever-clinical-trial-oflaboratory-grown-red-blood-cells-being-transfused-intoanother-person/
NHS Blood and Transport (nd) Recovery and survival of stem cell originated red cells Retrieved 05/08/2023 from https://wwwnhsbtnhsuk/clinical-trials-unit/current-trials-andstudies/restore/
University of Bristol (nd) RESTORE clinical trial Retrieved 05/08/2023 from https://wwwbristolacuk/btru/work/trial/
Zhou P Ouchari M Xue Y & Yin Q (2020) In Vitro Generation of Red Blood Cells from Stem Cell and Targeted Therapy Cell Transplantation, 29, 0963689720946658 https://doiorg/101177/0963689720946658
Smoking and Vaping: A Mission of Prevention and Quitting
There are several pathophysiological features that contribute to cardiovascular disease, a significant risk factor caused by cigarette smoking. A mixture of toxic chemicals including nicotine, carbon monoxide, and oxidant chemicals found within cigarette smoke are involved in the pathogenesis of cardiovascular disease Nicotine is a central nervous system stimulant and expresses its cardiovascular effect by increasing heart rate, blood pressure, and cardiac output Myocardial oxygen demand is increased as a result Carbon monoxide exposure to patients with coronary artery disease can cause adverse effects such as increased ventricular arrhythmia, ventricular dysfunction, and exercise-induced ischeemia Substances that may play a leading role in developing atherosclerosis would be oxidant gases The presence of oxidising chemicals, including nitrogen oxides and free radicals, in cigarette smoke is a primary cause of endothelial dysfunction in smokers⁸
Furthermore, tobacco is the main substance causing inflammation, endothelial dysfunction, changes to lipid profile and insulin resistance These all work together as pathobiological mechanisms for atherothrombosis, a major cause of cardiovascular death¹¹
Smoking prevalence
Although the prevalence has reduced in recent years, tobacco smoking is still one of the main causes of premature death and diseases worldwide. Many smokers acknowledge the harmful effects on their physical health yet continue to smoke The reason being that nicotine in cigarettes is highly addictive, making the negative consequences associated with smoking easy to overlook¹²
It has been estimated by the World Health Organisation (WHO) that in the 1990s, there were approximately four million tobacco-related deaths per year worldwide This estimate increased to around five million in 2003, and six million in 2011, and is expected to reach eight million per year by 2030²
Health implications and pathophysiological features related to cardiovascular disease and smoking.
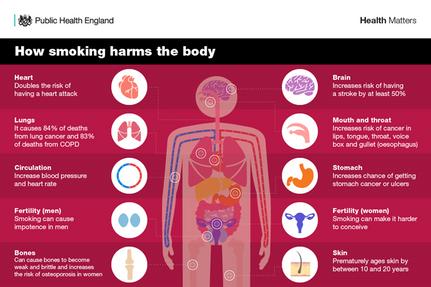
Cigarette smoking is associated with increased mortality and morbidity Smoking is associated with an increased risk of cardiovascular diseases, as well as respiratory disorders such as emphysema and chronic obstructive pulmonary disease (COPD)
Figure 1: Summary of various pathophysiological mechanisms of tobacco in developing cardiovascular disease. BP, blood pressure; HR, heart rate; NO, nitric oxide⁸.
Figure 2: Impacts of smoking on health⁷.
Smoking during pregnancy causes the risk of complications such as miscarriage, stillbirth, premature birth, foetal growth restriction, and a group of congenital abnormalities that are also significantly increased¹⁰ .
Smoking tobacco can lead to a variety of diseases including lung and stomach cancer or ulcers, pancreatic, kidney, cervical, and ovarian cancer, as well as leukaemia⁹
Vaping to quit smoking
One of the most effective methods of quitting smoking is nicotine vaping. E-cigarettes are electronic devices that allow you to inhale nicotine as a vapour rather than smoke E-liquids are available in various strengths of nicotine and can be controlled to help with withdrawal symptoms By reducing the health risks of smoking cigarettes, vaping can help to achieve this It is effective if expert help is gained from an individual’s local Stop Smoking Service Advice about the right device and nicotine strength can be given
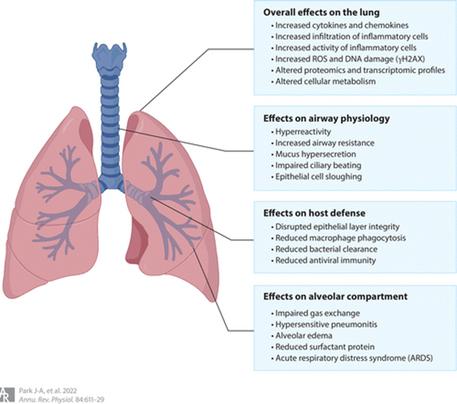
Even though nicotine vaping had previously been an effective method of quitting smoking, the New England Journal of Medicine reported several outbreaks of acute respiratory failure among electronic cigarette users in 2019. Inhalation of toxic environmental agents from electronic cigarettes causes injury to the airways and lung parenchyma The outcomes of these lung injuries are dependent on the dose of inhaled toxic compounds, solubility, and chemical composition Patients may develop a range of symptoms dependent on these factors including minor respiratory tract discomfort, acute airway injury and damage, parenchymal pneumonitis, alveolar oedema, hypoxemic respiratory failure, and death⁶ .
Long-term effects of vaping are still unknown and common side-effects include mouth and throat irritation, shortness of breath, and coughing or a dry throat⁴ Furthermore, research has shown that electronic cigarettes cause adverse respiratory effects such as increasing the chances of pneumothorax (total or partial collapse of the lung⁶ This is due to the toxins within the vapour such as nicotine and non-nicotine compounds which are associated with lung epithelial cell injury and inflammation¹³ . Therefore, smoking cessation programs may be more useful for quitting smoking altogether⁴
Smoking cessation
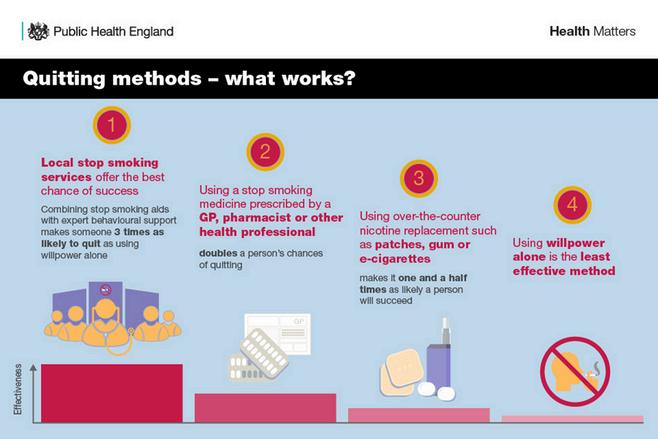
Reinforcing the necessity of quitting smoking can be done by repeated consultation and smoking cessation services. Furthermore, counselling by health workers can increase the rates of quitting smoking These methods of intervention have been shown to be effective as they are provided by healthcare providers who are able to maintain a good relationship with smokers and are therefore trusted by the public As well as clinical counselling, medication can be used as an effective treatment This includes nicotine replacement therapy (NRT) such as patches, gums, inhalers, and nasal spray³ .
Vaping as a smoking cessation aid could be considered if a smoker is still struggling to quit despite undergoing counselling, NRT, and prescription medication However, they must be well-informed of the negative aspects of vaping Whilst the use of e-cigarettes may be advantageous for smokers to quit, it is important to ensure that public health policies do not attract younger non-smokers This can be done through various policies such as taxation, flavour bans, advertisement, and age restrictions¹ .
Figure 3: Mechanistic overview of adverse effects of electronic cigarettes on the lungs. As a primary organ, the lung is damaged and impaired by electronic cigarette use⁶.
NHS 2024 Smoking Cessation Service for patients
In line with the NHS's long-term plan to make England smoke-free as a society, acute NHS trust patients with a Tobacco Dependency service will be offered smoking cessation support. All individuals admitted to the hospital should be offered NHSfunded tobacco treatment services by March 2024 Follow-up after patient discharge and 12 weeks of smoking cessation support are given to patients who have had their smoking status determined Acute NHS trusts can refer patients to a chosen pharmacy so they can receive continued treatment, support, and advice to quit smoking when discharged One of the problems with this service is that only patients who have been referred from an acute NHS trust during their discharge will be eligible to receive advice and treatment. However, it aims to decrease morbidity and mortality from tobacco cigarette smoking as well as address the gap between secondary and primary care handover Patients will be offered ongoing consultation as well as Nicotine Replacement Therapy, which must be provided by a trained pharmacist⁵
In summary, smokers looking to quit may look towards smoking cessation services such as NRT and various medications However, if there is a failure to do so, vaping may be introduced as a smoking cessation aid if the individual is well-informed of the side effects, including the damage it can cause to lung epithelium. To overcome this situation, the NHS has decided to offer patients smoking cessation support as of 2024, the only shortcoming being that acute NHS trusts can refer patients to this service
References: Al-Hamdani, M, & Manly, E (2021) Smoking cessation or initiation: The paradox of vaping Preventive Medicine Reports 22 101363 https://doiorg/https://doiorg/101016/jpmedr2021101363
1 Henningfield J Sweanor David T Hilton Matthew J & Rose Christine A (2023) Smoking - Tobacco Retrieved 04/03/2023 from https://wwwbritannicacom/topic/smoking-tobacco
3
2 Heydari G Masjedi M Ahmady A E Leischow S J Lando H A Shadmehr M B, & Fadaizadeh, L (2014) A comparative study on tobacco cessation methods: a quantitative systematic review International journal of preventive medicine,5(6),673-678
6
7
8
4 NHS Business Services Authority (nd) NHS Smoking Cessation ServiceReferral from Secondary Care into Community Pharmacy Retrieved 05/08/2023 from https://wwwnhsbsanhsuk/pharmacies-gp-practices-andappliance-contractors/dispensing-contractors-information/nhs-smokingcessation-service-referral-secondary-care-community-pharmacy
National Health Service (nd) Vaping to quit smoking Retrieved 05/08/2023 fromhttps://wwwnhsuk/better-health/quit-smoking/vaping-to-quit-smoking/
5 Park J A Crotty Alexander L E & Christiani D C (2022) Vaping and Lung Inflammation and Injury Annu Rev Physiol, 84, 611-629 https://doiorg/101146/annurev-physiol-061121-040014
Public Health England (2019) Health matters: stopping smoking – what works? Retrieved 05/08/2023 from https://wwwgovuk/government/publications/health-matters-stoppingsmoking-what-works/health-matters-stopping-smoking-what-works
Salahuddin S Prabhakaran D & Roy A (2012) Pathophysiological Mechanisms of Tobacco-Related CVD Glob Heart 7(2) 113-120 https://doiorg/101016/jgheart201205003
Scherübl H (2021) [Smoking tobacco and cancer risk] Dtsch Med Wochenschr 146(6) 412-417 https://doiorg/101055/a-1216-7050 (Tabakrauchen undKrebsrisiko)
10 Viles-Gonzalez J F Fuster V & Badimon J J (2004) Atherothrombosis: A widespread disease with unpredictable and life-threatening consequences EuropeanHeartJournal 25(14) 1197-1207 https://doiorg/101016/jehj200403011
12
11 West R (2017) Tobacco smoking: Health impact prevalence correlates and interventions Psychology & Health, 32(8), 1018-1036 https://doiorg/101080/0887044620171325890
13
Wieckowska J, Assaad, U, & Aboudan, M (2021) Pneumothorax secondary to vaping Respiratory Medicine Case Reports 33 101421 https://doiorg/https://doiorg/101016/jrmcr2021101421
Figure 4: Range of quitting methods and their effectiveness⁷.
SCIENCE IN THE NEWS
BY WIKTORIA WISNIEWSKA
Long COVID– The Past and The Present
In the previous issue of the ‘Bioscientist Magazine,’ Ruby Naylor-Adamson discussed the continuation of COVID-19 symptoms months after the initial infection, also known as "Long COVID"⁷ The article featured COVID-19 prevalence statistics, risk factors, and promising potential therapeutic approaches according to information available at the time of publication With emerging research, more is being discovered about the long-term implications, as well as the genetic and environmental factors playing a role in clinical presentations This article will expand on the facts understood at the time and compare them with novel findings about this complex health condition⁷
Symptoms and Prevalence – Novel Insights
The list of symptoms has expanded to include neurological, digestive, musculoskeletal, mental, and dermatological manifestations, as of March 2023⁹ In the UK, the people at highest risk of long COVID are 35 to 69 years old females, people residing in deprived areas, social care workers, unemployed teenagers aged 16 and over, and people whose health condition prohibits them from leading an active life, with fatigue continuing to be the most common symptom⁸ Women are four times more susceptible to long COVID-19 than men, however, men have higher mortality rates with acute infection, due to women ’ s innately stronger immune responses as an adaptation to support pregnancy Studies have shown that women have an increased IgG antibody production in the early phase of exposure, which can lead to longer-lasting inflammation if the levels are maintained at an all-time high
The inflammatory marker IL-6 is increased, even months after infection⁴ In addition, female immune T-cells are more active than male T-cells due to the large, upregulated expression of peripheral blood mononuclear cells¹ This hyperactivity introduces a risk of developing autoimmune conditions, which is a known connection to long COVID-19 The cardiopulmonary symptoms are more severe in females, as SARS-CoV-2 infection impairs post-exercise control of heart rate and total lung capacity, which further enhances the feeling of dread and tiredness This contributes to fear of unemployment, as women become chronically exhausted Women have reported an 83% increase in depression rates compared to 36% of men, highlighting serious psychological disturbances caused by COVID-19 Note that these reports can be subject to bias and misrepresentation because of gender disparities in reporting concerns⁴
Figure 1: A picture of the SARS-CoV-2 virus.
Autoantibodies
SARS-CoV-2 infection is characterised by heightened levels of pro-inflammatory cytokines as well as expression of specific chemokines which recruit neutrophils and monocytes to maintain inflammation. The pattern of chemokine antibodies in COVID correlates to the severity of the condition. A recent study showed that the monoclonal antibodies taken from COVID-19 convalescents bound to the chemokine impaired cell migration, and since the chemokines modulate immune cell trafficking, they also modulate the inflammatory response⁵ Through examining 3 independent COVID-19 cohorts’ plasmas, scientists found that the appearance of autoantibodies against specific chemokines helped identify acute and long COVID individuals They have also found that high expression of specific chemokine antibodies was associated with favourable disease outcomes, and the autoantibodies against chemokines were omnipresent after SARSCoV-2 infection The derived from patient plasma samples monoclonal antibodies blocked leukocyte migration There was a weak negative correlation between the age of the patient and the sum of all chemokine IgG reactivities There were no significant differences in the COVID-19-specific chemokine antibodies between genders Post-COVID, autoantibodies against these chemokines did not match the antibodies against the virus Unsurprisingly, the spike receptor binding domain antibodies were significantly in unvaccinated convalescents, compared to those who received at least one dose of mRNA-based vaccine Contrastingly to natural infection, there was no notable change in antibody reactivity to these chemokines upon the mRNA vaccination of SARS-CoV-2 naïve patients at 4 months post-vaccination. The concentrations of antibodies to spike receptor binding domain fell over time, but the ones of some chemokine antibodies during acute state increased over 1 year.
The long-term persistence of symptoms was associated with specific patterns of chemokine antibodies at 6 months. Furthermore, the specific patterns of autoantibodies against the chemokines differentiated the different COVID-19 trajectories, as well as identified other autoimmune disorders and infections
Due to the nature of chemokine function by promoting inflammation and tissue remodelling, it was suggested that the autoantibodies seem to reduce the damage caused by the inflammatory response⁵ .
The high concentrations of chemokine antibodies can distort cellular migration, but the variety and levels may modulate the inflammatory response in a nondestructive manner, which then impacts the severity and clinical presentation of long COVID Autoantibodies have an antagonising effect on the activation of chemokines and so retention of T and B lymphocytes Researchers are encouraged to study the chemokine-targeting agents to assess their impact on early inflammation and the development of the disease⁵ If there was a drug developed that could target the chemokine system, it could reduce the chances of developing long COVID, providing a potential approach to the treatment of the disease
UK and COVID-19
In the UK, the NIHR has invested more than 50 million to aid the understanding, diagnosis, treatment, and recovery from SARS-CoV-2 Their website reports the findings to evaluate novel approaches studied in clinical trials to ensure maximum safety and effectiveness of treatment This information is relayed to the General Medical Council which sets the standards of good medical practice, hence the best treatment method based on the best available evidence⁶ There are 19 funded studies, and their feedback aids in the development of a personalised rehabilitation programme to help people recover from long COVID The information is fully accessible to the public and allows for a newsletter sign up meaning that everyone can explore the supportive interventions the governments are putting in place to combat COVID-19²
Treatment and Guided Research
The treatment of COVID-19 remains widely symptom-based; however, new pathobiology studies offer promising explanations for the condition’s mechanisms and so propose novel initiatives
The understanding of long COVID remains incomplete, although antigen persistence, dysregulation of the immune response, reactivating latent viral infections, damaging microvasculature, gut dysbiosis, and many more, give valuable clues for targeted management Long COVID can be prevented by safe and effective mRNA technology vaccines For example, glucocorticoid receptors inhibit inflammatory cytokine, chemokine, and prostaglandin expression, hence regulating the immune balance Drugs like oral dexamethasone and prednisolone contribute to lower hospitalisation rates and less persistent symptoms at 8-month follow-up Anti-inflammatory agents such as JAK inhibitors, IL-6, and TNF-blockers displayed improvement in acute COVID manifestations Treatments for myalgic encephalomyelitis/chronic fatigue syndrome (condition overlapping with long COVID), such as low dosage of naltrexone (LDN) and aripiprazole, are not only antiinflammatory but also immunomodulatory, making a safe, orally active, and low-cost alternative for long COVID therapeutic trials LDN suppresses microglia cells of the central nervous system and weakens proinflammatory cytokines and in turn reduces hypoactivity. Since there is insufficient data to suggest definite improvement, a double-blinded placebocontrolled study with 160 participants is planned, and estimated to complete in April 2024. Aripiprazole is an antipsychotic agent with pleiotropic properties; antiinflammatory and immune-modulatory through reduction in activation of microglial cells and modulation of immune-related genes. Patients report an improvement in symptoms; however, further research is needed to establish the efficacy, tolerability, and safety of the drug³ SARS-CoV-2 infection has also been linked to changes in gut microbiome, particularly increased inflammation In this dysbiosis, the Ruminococcus and Bacteroides concentrations rise, and Faecalibacterium fall and generas such as Prevotella and Veillonella were linked to increased inflammation In a study focusing on plantbased fiber or fermented foods in healthy adults,
It has been found that a highly fermented diet enhances microbial diversity and decreases cytokine, chemokine, and other inflammatory serum proteins (IL-6, IL-10, and IL-12b) This suggests that this type of diet can prove to be a powerful, non-invasive modulator of the human gut microbiome and immune system axis, introducing an alternative to treating long COVID symptoms, however, further analysis is needed³.
Those research focus strategies are being undertaken to offer tailored long COVID management and offer a blueprint for pathways yet to be discovered Even though the vast majority is decently understood, more studies and well-designed clinical trials are needed for an evidence-based approach to tackle this major global healthcare strain³
References
1 Anonymous (2022) Researching long COVID: addressing a new global health challenge National Institute for Health and Care Research Retrieved 05/08/2023 from https://evidence nihr ac uk/themedreview/researching-long-covidaddressing-a-new-global-health-challenge/
Agrawal S Salazar J Tran T M & Agrawal A (2021) Sex-Related Differences in Innate and Adaptive Immune Responses to SARSCoV-2 [Original Research] Frontiers in Immunology, 12 https://doi org/10 3389/fimmu 2021 739757
2 Bonilla, H , Peluso, M J , Rodgers, K , Aberg, J A , Patterson, T F , Tamburro R Baizer L Goldman J D Rouphael N Deitchman A Fine J Fontelo P Kim A Y Shaw G Stratford J Ceger P Costantine, M M , Fisher, L , O’Brien, L , McComsey, G A (2023) Therapeutic trials for long COVID-19: A call to action from the interventions taskforce of the RECOVER initiative [Review] Frontiers in Immunology, 14 https://doi org/10 3389/fimmu 2023 1129459
3 D Annibale L D Annibale D Ramasamy A (2022) Why are women more susceptible to long COVID? Gender and Public Health Emergencies Retrieved 05/08/2023 from https://www genderandcovid-19 org/editorial/why-are-womenmore-susceptible-to-long-covid/
4 Muri J Cecchinato V Cavalli A Shanbhag A A Matkovic M Biggiogero, M , Maida, P A , Moritz, J , Toscano, C , Ghovehoud, E , Furlan R Barbic F Voza A De Nadai G Cervia C Zurbuchen Y Taeschler P Murray L A Danelon-Sargenti G Robbiani D F (2023) Autoantibodies against chemokines post-SARS-CoV-2 infection correlate with disease course Nature Immunology 24(4) 604-611 https://doi org/10 1038/s41590-023-01445-w
5 National Health Service (2022) Your COVID Recovery - Research Retrieved 05/08/2023 from https://www yourcovidrecovery nhs uk/research/
7
6 Naylor-Adamson, R (2022) Long COVID, The Short Story The Salford Bioscientist Magazine, (3) https://issuu com/bioscientistmagazine/docs/bioscientist magazine issue 3/6
9
Office For National Statistics (2023, 30/03/2023) Prevalence of ongoing symptoms following coronavirus (COVID-19) infection in the UK Retrieved 05/08/2023 from https://www ons gov uk/peoplepopulationandcommunity/healthand socialcare/conditionsanddiseases/bulletins/prevalenceofongoingsy mptomsfollowingcoronaviruscovid19infectionintheuk/30march2023
8 Scottish Government (n d , 13/03/2023) Signs and symptoms of long COVID NHS Inform https://www nhsinform scot/long-term-effectsof-covid-19-long-covid/about-long-covid/signs-and-symptoms-oflong-covid
RESEARCH SPOTLIGHT
BY HAJRAH HUSSAIN
Fear of the dentist is prevalent in all age groups and classes, a fear that may be brought on by something as simple as the depiction of dentists as ominous figures in books and television or, in some cases, trauma caused by a previous visit to the dentist. Overall, this fear of the dentist or odontophobia can really make us think: Is the person delivering dental care, a dentist or the devil¹?
Research has shown that up to 30% of adolescents show moderate dental anxiety whose anxiety then impacts the child, their carer, and the dental professional themselves as they all play an integral part in the maintenance of good oral health for the patient⁷ The fear of the dentist is something that is learned and can happen through limitless experiences that can be direct or indirect. The threat of trauma or trauma itself induced in a dental situation, experienced by the individual themselves is an example of a direct experience This fear from experience can be likened to the psychological modelling of Pavlovian classical conditioning For example, the stimulus of pain may be felt during a procedure involving a dentist and their dental tool, eliciting a high level of fear. Although it is the tool I.e., the drill that caused the pain, the fear created will be attached to the dentist conditioning the individual to believe that the dentist causes pain in then causing fear Fear obtained through an indirect experience happens through a learning method known as modelling, where children vicariously feel fear through the traumatic experiences of others such as parents, siblings, and friends, for example, either through visually experiencing these situations themselves or by simply hearing about them For the treatment of odontophobia, the knowledge of these learning paradigms is essential³
Odontophobia has a vicious cycle, as patients tend to avoid any forms of maintenance for their mouth, consequently suffering from more caries and ultimately extractions Due to their poorer oral health, they are then inevitably in more need of the dentist and dental treatments This increase in dental exposure to these already anxious adolescents makes it vital that anxiety control methods are essential to be known by any professionals in the dental sector.
CBT (Cognitive Behavioural Therapy) which is a form of treatment against fear that is being looked at in this article is efficient at reducing dental anxiety and avoidance and is a form of treatment that can be carried out by varying degrees of expertise from specially trained dentists to clinical psychologists whose practice is behaviourally oriented⁴
There are many behavioural techniques that can be used to manage anxious paediatric patients but interest in the psychological approach has peaked in recent years, specifically the idea of introducing CBT CBT is essentially a treatment therapy based on communication, turning irrational and unhelpful thoughts into ones that are more positive and can aid the child in a calmer state of mind
The overall use of CBT is an effective treatment, however, access to therapy treatment is limited due to availability and cost-effectiveness issues Therefore, in this specific study into using CBT to overcome dental phobia a self-help resource was developed allowing the children to take part in their behavioural therapy to overcome their dental anxiety. In this specific case CBT is introduced to reduce the child's anxiety and not just manage it⁶
The self-help CBT method was a communication method known as a ‘Message to Dentist’ (MTD) a part of a greater CBT approach⁷ . One hundred and five paediatric patients who were deemed as ‘dentally anxious’ were invited to participate with their mean age being 11 6
They were all asked to complete the MTD form before and after treatment making notes of factors such as ranking anticipated pain levels and how worried they were on a scale of 1 to 10. They were also asked to think of and write coping mechanisms and then contemplate their experience post-treatment Results showed a significant reduction in self-reported anxiety with scores dropping from 4 9 to 2 1 and anticipated pain results dropping from 5 1 to 2 0
Analysis of the main themes from the survey highlighted concerns about pain, certain procedures such as scale and polish, extractions and fillings, and issues with sedation such as inhalation sedation and general anaesthesia. The MTD format allowed specific communication between the patient and dental team allowing clearing of doubts and anxiety before and after treatments
The main theme we can see is the importance of communication and the use of the MTD is excellent in terms of it highlighting individual and general fears children have regarding dentistry, and how dental professionals can now easily acknowledge and handle these concerns bringing ease to all parties involved. These concerns do not just start and stop with adolescents but can carry with us through to adulthood. This ‘fear of a medical catastrophe’ that these children suffered is in line with previous research findings and is prevalent in dentally anxious adults also Without this form of CBT and many others, an end to fear-inducing beliefs would never happen, causing a lack of essential dental healthcare interventions from professionals
The focus of CBT is orientated around the current adversities a person is facing, with a great emphasis on the present looking for new ways to improve the patient's state of mind, without these negative thoughts clouding them and now for them to have a new beginning² In recent years, researchers at King’s College London have set out to gain more information on odontophobia in turn learning more about the talking therapy that is CBT and then eventually psychologists alongside dental patients at King’s have developed the UK’s first dental phobia-dedicated CBT service and the training model has been shared in many locations across the UK. Their primary goal was to allow patients to receive dental treatment without the need for sedation which is a huge goal as sedation is usually needed to decrease anxiety levels and efficiently perform treatments for those who suffer from extreme dental anxiety
Success is evident within the work done at King’s with study results showing 93% of dental-phobic patients who completed the course of CBT went on to be treated without the use of sedation This is a huge breakthrough and with the development and rollout of their training programme, odontophobic patients across the United Kingdom will have the chance to work on a better relationship with their dental environment leading to a new beginning for all involved⁵
References
7
1 Fenn K &Byrne M (2013) Thekeyprinciplesofcognitive behaviouraltherapy InnovAiT 6(9) 579-585 https://doiorg/101177/1755738012471029
Doherty R (2017) Fearofthedentist BritishDentalJournal 222(9) 670-671 https://doiorg/101038/sjbdj2017400
3 Gordon D Heimberg R G Tellez M &Ismail A I (2013) Acritical reviewofapproachestothetreatmentofdentalanxietyinadults JournalofAnxietyDisorders 27(4) 365-378 https://doiorg/https//doiorg/101016/jjanxdis201304002
5 Porritt J Rodd H Morgan A Williams C Gupta E Kirby J Creswell C Newton T Stevens K Baker S Prasad S & Marshman Z (2017) DevelopmentandTestingofaCognitive BehavioralTherapyResourceforChildrensDentalAnxiety JDR Clinical&TranslationalResearch 2(1) 23-37 https//doiorg/101177/2380084416673798
6 Rodd H Timms L Noble F Bux S Porritt J &Marshman Z (2019) MessagetoDentist:FacilitatingCommunicationwith DentallyAnxiousChildren DentistryJournal 7(3)
RESEARCH SPOTLIGHT
BY JESSICA MARIA SINGH
Have you ever wondered if we could heal tissues in the body from damage that can be detrimental?
In December 2022, a journal on Nature, brought to light by the University of California San Diego, discovered a new biomaterial that can heal tissues from the inside out¹³ Karen Christman, professor of bioengineering at the University of California San Diego and the lead researcher for the team that developed the biomaterial, stated, “It is a new approach to regenerative engineering¹ ”
Christman and colleagues developed a hydrogel produced from the natural scaffolding of cardiac muscle tissue known as the extracellular matrix (ECM)¹ This can be injected into the damaged heart tissue via a catheter, forming a structure in damaged areas of heart tissue and assisting in new cell growth and cell repair¹ However, this hydrogel needed to be injected directly into the heart as well as using the hydrogel only one week or more after a heart attack – due to needlebased injection procedures; this caused a risk of damage¹ This biomaterial was tested, and it has effectively treated tissue damage caused by heart attacks in rodents and large animals¹ Initial proof of concept in rodent models strongly suggests that the biomaterial could potentially be beneficial to patients with traumatic brain injury and pulmonary arterial hypertension¹ Christman stated that studies to test the safety and efficiency of the biomaterial on human subjects could start within one or two years¹
How is this biomaterial created?
Initially, researchers in Christman’s laboratory used hydrogel they developed that enabled intravenous injections as part of safety trials¹ However, the hydrogel particles were too large to target leaky blood vessels, this was resolved by a Ph.D. student Sprang by centrifuging the hydrogel particles into nanoparticle size¹
In the USA, approximately 785,000 new heart attack cases arise every year¹ . When a person recovers from a heart attack, they are left with scar tissue and muscle function decline leading to congestive heart failure. Currently, there are no treatments for repairing cardiac tissue damage¹
The liquid ECM hydrogel was centrifuged at 15,000 RCF at 4 ℃ for 45 minutes, which separated the bigger-sized particles away to extract only the nano-size particles¹² After centrifuging, the supernatant iECM (infusible ECM) was out through dialysis, then sterile filtering, and finally, freeze-dried¹² .
How does this biomaterial work?
Patches of decellularised extracellular matrix and locally injected hydrogels have been used as therapies in animal models of disease² .
For the Future?
Christman and Ventri Bio, Inc., are now amid seeking FDA approval to conduct a study on human hearts of the biomaterial’s applications in heart conditions¹
References
1
Patringenaru, I (2023) This Injectable Biomaterial Heals Tissues From the Inside Out UC San Diego Today https://today ucsd edu/story/thisgroundbreaking-biomaterial-heals-tissues-fromthe-insideout#:~:text=The%20biomaterial%20was%20teste d%20and%20proven%20effective%20in,with%20 traumatic%20brain%20injury%20and%20pulmo nary%20arterial%20hypertension
2.
Spang, M. T., Middleton, R., Diaz, M., Hunter, J., Mesfin, J , Banka, A , Sullivan, H , Wang, R , Lazerson, T S , Bhatia, S , Corbitt, J , D’Elia, G , Sandoval-Gomez, G , Kandell, R , Vratsanos, M A , Gnanasekaran, K , Kato, T , Igata, S , Luo, C , Christman, K L (2022) Intravascularly infused extracellular matrix as a biomaterial for targeting and treating inflamed tissues Nature Biomedical Engineering https://doi org/10 1038/s41551-02200964-5
3
University of California - San Diego (2023) This groundbreaking biomaterial heals tissues from the inside out ScienceDaily Retrieved 20th February 2023 from www sciencedaily com/releases/2023/01/23013014 4805.htm
Figure 1: The biomaterial is based on the hydrogel that was produced in Christman’s laboratory¹-³.
TOPICS IN BIOMEDICINE
BY JOY CHUKWUDOLUE
Excess mortality due to complications in Type 1 Diabetes Mellitus emphasises the significance of preventative strategies and the need for treatments¹² In a particular study, the uncorrected rate of mortality from any cause for individuals with Type 1 Diabetes Mellitus (T1DM), including children, was 11 7% per 1000 person-years²³
Current Treatment of Type 1 Diabetes
A chronic autoimmune disease, Type 1 Diabetes Mellitus is marked by a deficiency in insulin and leads to hyperglycaemia¹¹ Presently, no cure exists, and patients depend on insulin injections for life¹⁴ . In England, patients get their prescription of insulin for free by using a medical exemption certificate¹⁰ In other parts of the world such as America, this is not the case. In the US in 2016, T1DM patients paid close to $6000 out of pocket for insulin³¹ Moreover, some older patients with dementia may forget whether they have or have not taken their insulin which can lead to hypoglycaemia or hyperglycaemia² . The discrepancies in the cost of treatment and difficulty taking current treatments are reasons that further strengthen the need for a cure
Reason For Stem Cell Therapies
Exogenous insulin that is administered cannot mimic the endogenous insulin that is normally secreted⁶ . This is because exogenous insulin cannot regulate blood glucose levels physiologically Usually, exogenous insulin is administered to ameliorate hyperglycaemia⁶ Stem cell therapies are being developed to produce beta (β) cell islet organoids in vitro and insulin-producing cells (IPCs) which in theory control blood sugar levels normally This gives the hope that a cure can be found⁶ .
Causes of Type 1 Diabetes
While the aetiology of T1DM is not fully understood, some parts have been Circulating immune T-cells are thought to mediate the destruction of β cells, the insulin-producing cells of the pancreas¹⁴ . More specifically, CD8+ and CD4+ T-cells and macrophages target β cells which ultimately causes hyperglycaemia¹² Environmental and genetic factors destroy β cells as well²² In genetically susceptible individuals, one or more environmentrelated factors trigger the irreversible immunological destruction of β cells. These environmental factors include viruses such as gut microbiota, enteroviruses, and rubella. And in the diet, examples of these factors are cereals, and vitamin D²² .
Diagnosis of Type 1 Diabetes
Type 1 diabetes usually starts in childhood or adolescence, but up to 50% of cases begin in adulthood¹¹ Unfortunately, early onset T1DM is on the rise meaning that many more children are being affected²² . The reason behind this rise is remains unknown¹⁶ Type 1 diabetes mellitus is diagnosed by measuring fasting blood glucose levels or measuring random blood glucose levels in an individual with symptoms¹¹ These symptoms include polyuria, polydipsia, and polyphagia⁴ A positive result would be a concentration on or above 7.0 mmol/L (126 mg/dL) for fasting blood glucose and above 11.1 mmol/L (200 mg/dL) post satiation¹¹ . Glycated haemoglobin (HbA1c) indicates the level of glucose bound to haemoglobin in the blood²⁵ Glycated haemoglobin (HbA1c) is less sensitive for diagnosis than the first two tests, so it is not used much for the diagnosis of T1DM¹¹ In a diabetic patient, HbA1c concentration will be above 48 mmol/mol (6.5%)¹¹ . This lack of sensitivity for diagnosis may be because HbA1c reflects the glycaemic history of the past two to three months²⁵ This is good for long-term complications associated with diabetes and for measuring chronic hyperglycaemia²⁵ This indicates HbA1c is not effective for tracking dysglycaemia that progresses quickly
Embryonic Stem Cells
Embryonic stem cells (ESCs) are pluripotent stem cells. From a blastocyst which is an early embryo, ESCs are separated from the inner cell mass⁶ In vitro, these ESCs can differentiate into many types of adult cells⁶ In therapeutics, ESCs have a significant potential to produce copious quantities of insulin-producing cells (IPCs), for example, β cells⁷
Aims of Stem Cell Therapy
Generally, the aims of stem cell therapies are to replace β cells or control the autoimmune response to insulin-expressing cells¹ Stem cell transplantation seems like a promising alternative to islet β cell transplantation which is a current treatment While the latter is successful, it is not used as frequently because it relies on the availability and number of donors and the lifelong use of immunosuppressive drugs³⁰
Induced Pluripotent Stem Cells And hESCs In Diabetic Mice
Using Yamanaka factors, induced pluripotent stem cells (iPSCs) are reprogrammed from adult somatic cells into an embryonic-like pluripotent state. Human embryonic stem cells (hESCs) and human induced pluripotent stem cells (hiPSCs) can be used to replace β cells iPSCs and hESCs are both pluripotent stem cells³⁰ The production of insulin-producing cells from both ESCs and iPSCs involves the successive regulation of certain signaling pathways controlling the development of the pancreas⁶
In diabetic mice transplanted with greatly enriched pancreatic and duodenal homeobox 1 (PDX1+) pancreatic progenitor cells (from hESCs), normal blood glucose levels were restored⁶⁷ This evidence therefore suggests that stem cell therapies and transplantations have the potential to reverse or prevent T1DM¹
Production Of Insulin Producing Organoids and Cells
hESCs and human induced pluripotent stem cells (hiPSCs) are sources of islet organoids in vitro and IPCs⁶ Organoids are 3D structures that are produced from stem cells²⁸ . Inside a 3D gelatinous chamber, induced pluripotent stem cells (iPSCs) are differentiated into insulin-producing cells This structure forms an organoid similar to an islet in humans. After the organoid, as seen in Figure 1, is activated using hormones and growth factors, the islet-like cells can produce insulin in response to glucose These organoids are used for transplantation⁸
Research has shown that different islet types interact with each other, and this helps maintain glucose homeostasis⁶ Islet-like organoids that responded to glucose were created from human pluripotent stem cells (hPSCs)¹⁵ . Experiments with conditions of elevated glucose stimulation suggest that 3Dinduced IPCs, such as 3D islet organoids, are more sensitive to the stimulus of glucose than 2D-induced cells⁶ . In another study to produce β cells ex vivo, pluripotent stem cells and facultative progenitor cells from the pancreas and liver that are organ-specific were used¹ The generated β cells would be used for transplantation
Figure 1: Growth of pancreatic organoids. Induced pluripotent stem cells (iPSCs) are being differentiated into insulin producing cells²⁹.
Diabetic Patient-Derived iPSCs
One advantage of creating patient-specific iPSCs for diabetics (DiPSCs) is that they can overcome immune mismatch and immune rejection which are current issues faced in stem cell therapy⁶ In a particular study, human stem cells derived beta cells (SC-β), which were themselves derived from DiPSCs, were shown to resemble adult β cells in function⁶
One disadvantage of iPSCs is that the reprogramming processes for these stem cells have excessive costs and low efficiency due to the methodologies used Now, small molecule gene inducers are being used and methodologies for reprogramming are being improved⁷ T1DM patients are diverse and thus a bigger number of stem cell lines that are compatible with a wide range of patients are required for future medical use⁶ Moreover, it was found using flow cytometry that only 15.9% of DiPSCs generate insulin-producing cells compared to 25-50.5% of non-diabetic iPSCs⁶ This low result may be due to dysmetabolism causing epigenetic changes in T1DM6 These epigenetic changes will result in changes in insulin secretion¹³ . Contrasted to hESCs, iPSCs have limited clinical utility due to incomplete maturation of cells that are differentiated, chromosomal aberrations, and oncogenic potential⁷
Autoimmune Issues
Autoimmune and alloimmune responses are still a big problem for cell replacement therapies with β cells derived from hESCs or iPSCs⁶ . While encapsulation technology has progressed, the engraftment of β cells or transplanted pancreas progenitors that are derived from hPSCs still faces issues. These problems include engraftment rejection which is caused by the immune system. To overcome these difficulties, immune modulation techniques for hPSCs sound promising⁶ Currently, more immunosuppressive strategies are being developed. A few strategies involve eliminating certain Human Leukocyte Antigen (HLA) genes or specific HLA classes⁶²⁷ Some mesenchymal stem cells (MSC) also have immunosuppressive properties In clinical trials in 2010, there was no definitive result about the use of mesenchymal stromal cells to modify the autoimmune response¹
Contrastingly, by 2020, it was found that tolerogenic dendritic cells (MSC) and autologous haemopoietic stem cells (HSCs) that were modified in vitro had preservative effects¹⁷ Without hindering immune surveillance, these cells could protect newly created and endogenous β cells from the autoimmune response This is done through the immunomodulatory properties the autologous stem cells possess which preserve β cells and limit autoimmunity¹⁷ However, further modification is required for the methods used to generate cells so that they can meet safety and quality standards for clinical purposes¹⁷
Efficacy Of Stem Cell Transplantation
One key question scientists are trying to answer is how effective stem cell transplants are in treating T1DM. In early studies, there was no clear conclusion on the efficacy of stem cell transplants in T1DM patients¹⁹ Among a review article featuring thousands of articles, an agreement was that MSC and HSC co-transplantation did significantly improve T1DM e.g. in HbA1c levels¹⁹
Conclusion
β cell-like organoids made from human stem cells do seem promising in the treatment of T1DM In previous studies, cotransplantation of MSCs and HSCs seemed to improve T1DM in the patients in the study¹⁹ . In 2022, there were 6 clinical trials using hPSCs for the treatment of T1DM²⁶ Most of the six clinical trials are measuring the efficacy, tolerability, and safety of certain hPSCs lines, e.g., VX-880, in T1DM patients³ The results of almost all of these trials have yet to be published so a general outcome cannot be made yet More clinical trials of stem cell transplantation need to be done to see if this potential treatment option is safe for widespread use in humans With more clinical trials and research, more of the limitations of stem cell therapy for type 1 diabetes mellitus could be overcome.
References
1
Aguayo-Mazzucato C, & Bonner-Weir S (2010) Stem cell therapy for type 1 diabetes mellitus Nat Rev Endocrinol 6(3) 139-148 https://doiorg/101038/nrendo2009274
Alzheimer's Society (nd) Remembering diabetes medications and avoiding hypos when you have dementia Retrieved 22/07/2023 from https://wwwalzheimersorguk/getsupport/publications-and-factsheets/dementiatogether-magazine/remembering-diabetesmedications-when-you-have-dementia
2 Anonymous (2023) A Safety Tolerability and Efficacy Study of VX-880 in Participants With Type 1 Diabetes Retrieved 01/08/2023 from https://clinicaltrialsgov/study/NCT04786262? cond=NCT04786262&rank=1&limit=10
4
3 Atkinson M A, Eisenbarth G S, & Michels A W (2014) Type 1 diabetes Lancet 383(9911) 69-82 https://doiorg/101016/s0140-6736(13)60591-7
Blum B, & Benvenisty N (2008) The tumorigenicity of human embryonic stem cells Advances in cancer research, 100, 133-158 https://doiorg/101016/S0065230X(08)00005-5
6
5 Chen S Du K & Zou C (2020) Current progress in stem cell therapy for type 1 diabetes mellitus Stem Cell Res Ther, 11(1), 275 https://doiorg/101186/s13287-020-01793-6
Chhabra P & Brayman K L (2013) Stem cell therapy to cure type 1 diabetes: from hype to hope Stem Cells Transl Med, 2(5), 328-336 https://doiorg/105966/sctm2012-0116
7 Collins F (2020) Insulin-Producing Organoids Offer Hope for Treating Type 1 Diabetes Retrieved 30/05/2023 from https://directorsblognihgov/2020/09/24/insulinproducing-organoids-hope-for-treating-type-1diabetes/#:~:text=Not%20only%20did%20the%20trans plantedeven%20longer%20periods%20of%20time
9
8 de Miguel-Beriain I (2015) The ethics of stem cells revisited Advanced drug delivery reviews, 82, 176-180 https://doiorg/101016/jaddr201411011
10
Diabetes UK (nd) Free Prescriptions (England) Retrieved 22/07/2023 from https://wwwdiabetesorguk/guide-to-diabetes/life-withdiabetes/free-prescriptions
18 Lysy P A , Weir G C , & Bonner-Weir S (2012) Concise review: pancreas regeneration: recent advances and perspectives Stem cells translational medicine 1(2) 150-159 https://doi org/10 5966/sctm 2011-0025
19 Madani S M A Aghayan H R Setudeh A Rezaei N Rouhifard M , & Larijani B (2022) Investigating the safety and efficacy of hematopoietic and mesenchymal stem cell transplantation for treatment of T1DM: a systematic review and meta-analysis Systematic Reviews 11(1) 1-18 https://doi org/https://doi org/10 1186/s13643-022-01950-3
20 Merriam Webster (n d ) Tumorigenic Definition & Meaning Retrieved 01/08/2023 from https://www merriamwebster com/dictionary/tumorigenic
21 Orive G , Hernández R M , Gascon A R , Calafiore R , Chang T M S , Vos P D , Hortelano G , Hunkeler D , Lacik I , & Shapiro A M J (2003) Cell encapsulation: promise and progress Nature medicine, 9(1), 104-107 https://doi org/10 1038/nm 0103-104
22 Paschou S A , Papadopoulou-Marketou N , Chrousos G P , & Kanaka-Gantenbein C (2018) On type 1 diabetes mellitus pathogenesis Endocr Connect, 7(1), R38-r46 https://doi org/10 1530/ec-17-0347
23 Ruiz P L D , Chen L , Morton J I , Salim A , Carstensen B , Gregg E W , Pavkov M E , Mata-Cases M , Mauricio D , & Nichols G A (2022) Mortality trends in type 1 diabetes: a multicountry analysis of six population-based cohorts Diabetologia 65(6) 964-972 https://doi org/10 1007/s00125022-05659-9
24 Sanz E Gómez-López T & Martınez-Quintas M J (2001) Perception of teratogenic risk of common medicines European Journal of Obstetrics & Gynecology and Reproductive Biology, 95(1), 127-131 https://doi org/10 1016/s0301-2115(00)00375-4
25 Sherwani S I , Khan H A , Ekhzaimy A , Masood A , & Sakharkar M K (2016) Significance of HbA1c test in diagnosis and prognosis of diabetic patients Biomarker insights, 11, BMI S38440 https://doi org/10 4137/BMI S38440
26 Sordi V Monaco L & Piemonti L (2022) Cell therapy for type 1 diabetes: from islet transplantation to stem cells Horm Res Paediatr https://doi org/10 1159/000526618
12
11 Gillespie K M (2006) Type 1 diabetes: pathogenesis and prevention Cmaj 175(2) 165-170 https://doiorg/101503/cmaj060244
13
DiMeglio L A, Evans-Molina C, & Oram R A (2018) Type 1 diabetes Lancet 391(10138) 2449-2462 https://doiorg/101016/s0140-6736(18)31320-5
Jerram S T, Dang M N, & Leslie R D (2017) The Role of Epigenetics in Type 1 Diabetes Curr Diab Rep 17(10) 89 https://doiorg/101007/s11892-017-0916-x
14
Katsarou A, Gudbjörnsdottir S, Rawshani A, Dabelea D, Bonifacio E Anderson B J Jacobsen L M Schatz D A & Lernmark Å (2017) Type 1 diabetes mellitus Nat Rev Dis Primers, 3, 17016 https://doiorg/101038/nrdp201716
16
15 Knip M (2012) Descriptive epidemiology of type 1 diabetes is it still in? Diabetologia 55(5) 1227-1230 https://doiorg/101007/s00125-012-2522-4
17
Kim Y Kim H Ko U H Oh Y Lim A Sohn J W Shin J H, Kim H, & Han Y M (2016) Islet-like organoids derived from human pluripotent stem cells efficiently function in the glucose responsiveness in vitro and in vivo Sci Rep, 6, 35145 https://doiorg/101038/srep35145
Loretelli C, Assi E, Seelam A J, Ben Nasr M, & Fiorina P (2020) Cell therapy for type 1 diabetes Expert Opin Biol Ther, 20(8), 887-897 https://doiorg/101080/1471259820201748596
27 Torikai H , Mi T , Gragert L , Maiers M , Najjar A , Ang S , Maiti S Dai J Switzer K C Huls H Dulay G P Reik A Rebar E J , Holmes M C , Gregory P D , Champlin R E , Shpall E J , & Cooper L J (2016) Genetic editing of HLA expression in hematopoietic stem cells to broaden their human application Sci Rep 6 21757 https://doi org/10 1038/srep 21757
28 Torras N , García-Díaz M , Fernández-Majada V , & Martínez E (2018) Mimicking epithelial tissues in three-dimensional cell culture models Frontiers in bioengineering and biotechnology 6 197 https://doi org/10 3389/fbioe 2018 00197
29 Trafton A (2021) Engineers grow pancreatic organoids” that mimic the real thing MIT News Retrieved 04/08/2023 from https://news mit edu/2021/pancreatic-organoidscancer-0913
30 Wan X X Zhang D Y Khan M A Zheng S Y Hu X M Zhang Q , Yang R H , & Xiong K (2022) Stem cell transplantation in the treatment of type 1 diabetes mellitus: from insulin replacement to beta-cell replacement Frontiers in endocrinology, 13, 859638 https://doi org/10 3389/fendo 2022 859638
31 Willner S , Whittemore R , & Keene D (2020) “Life or death”: experiences of insulin insecurity among adults with type 1 diabetes in the United States SSM-population health, 11, 100624 https://doi org/10 1016/j ssmph 2020 100624
TOPICS IN BIOMEDICINE
BY HARRIET BURROW
Dementia is a very common term used usually referring to a disease of the brain However, dementia is a broad word meaning a variety of symptoms including memory loss, and lack of motivation which interfere with everyday activities Therefore, dementia is not just one disease In fact, there are many disorders that cause a patient to have dementia such as Alzheimer’s disease (AD), vascular dementia, frontotemporal dementia, and mixed dementia²
After being bereaved of my great-grandmother, Eileen, in 2017 due to AD, I began to research the condition, and to say there were 50 million people worldwide with dementia in 2020, is definitely not talked about enough Eileen passed away at the age of 89 after living with AD for approximately 9 years The first signs of illness showed in the usual way, forgetfulness, and repetition of conversations however the more revealing factor that she was suffering from AD was her monthly medication was lasting for much shorter periods of time When left unsupervised she would retake her medication forgetting she had already done so. She also began to act out of character becoming aggressive and distant towards family members she was once close with This caused concern with family members resulting in a scan where she was diagnosed with AD The days became monotonous for those caring for her, every day her routine was identical to the last, and the repetition of meals, conversations, and music became draining. However, to my great-grandmother, every day was a new beginning, songs that she had been listening to for 10 years were suddenly brand new and brought her joy, a meal she’d been eating every day for the past week was an exciting flavour she had never tasted before and stories from when she used to dance as a young girl, which the majority of the already family know and love, are unheard and she must tell them again And though over the 9 years she battled this disease the endless conversations and tasks felt constant to us, for her these new beginnings brought happiness Each morning she no longer had AD, she was a young girl again dancing ballet in the old school hall, she was working on the farm where she lived till the day she passed, she was just Eileen
What is Alzheimer’s disease?
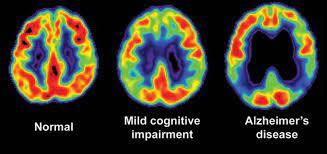
It is a progressive neurodegenerative disorder caused by the accumulation of beta-amyloid plaques and tau protein tangles in the brain⁴ Progressive and neurodegenerative are very similar, meaning worsen over time and gradually slow down the nervous system Beta-amyloid plaques are brain proteins that fail to function normally, these build up in the gaps between brain cells Tau protein tangles are twisted fibres of protein that build up inside cells The build-up of these two substances triggers the release of toxins which causes damage to neurons and neuronal synapses, inducing decreased levels of Acetylcholine This causes areas of the brain to shrink³⁵ The reason we associate memory loss with AD is that the cerebellum and prefrontal cortex shrink first - these are the areas that control procedural learning (everyday tasks such as brushing your teeth) and motor learning (getting out of bed) Evidence of this shrinkage of the brain can be visualised through a CT or MRI scan. There is also research into using PET scans (positron emission tomography) to identify AD The progression of AD occurs at varying rates due to several contributing factors such as gender, ethnicity, family history, depression, autoimmune diseases, physical inactivity, lifestyle (e g , smoking, alcohol consumption), and head injury⁵ However, in every case presented there are seven stages of Alzheimer’s disease as follows:
Pictured: Eileen with her family
Stage One - There is no impairment at this stage and AD is undetectable, no memory problems are evident.
Stage Two - Very mild decline begins, minor memory problems which cannot be distinguished from age-related cognitive decline
Stage Three - Memory problems become noticeable and performance on memory tests is affected, this can be seen through the forgetting of names or losing things around the house
Stage Four - A moderate decline of congestive function where symptoms are apparent, short-term memory is severely impaired and there are noticeable changes in long-term memory.
Stage Five - Moderately severe decline meaning patients now need assistance with everyday activities, are unable to recall simple details, and experience significant confusion
Stage Six - Severe decline, constant supervision is needed due to unawareness of environment and surroundings, loss of bladder and bowel control, and behavioural problems
Stage Seven - The final stage, resulting in loss of ability to communicate or respond and eventual loss of the ability to swallow AD is a terminal illness therefore the majority of cases lead to death.
Fortunately, medical professionals can keep AD patients as comfortable as possible during this time¹
Pictured: Eileen, of whom this article tells the story.
References
3
1 Bobinski, M, de Leon, M J, Wegiel, J, Desanti, S, Convit, A, Saint Louis, L A, Rusinek, H, & Wisniewski, H M (2000) The histological validation of post mortem magnetic resonance imaging-determined hippocampal volume in Alzheimer's disease Neuroscience 95(3) 721-725 https://doiorg/101016/s0306-4522(99)00476-5
Anonymous (2021) What Are the 7 Stages of Alzheimers Disease? Retrieved 27/04/2023 from https://wwwalzheimersnet/stages-of-alzheimers-disease
2 Harris, K M, & Kater, S B (1994) Dendritic spines: cellular specializations imparting both stability and flexibility to synaptic function Annu Rev Neurosci, 17, 341-371 https://doiorg/101146/annurevne17030194002013
4
Mayo Clinic Staff (2023) Alzheimer's disease Retrieved 22/04/2023 from https://wwwmayoclinicorg/diseasesconditions/alzheimers-disease/symptoms-causes/syc20350447
6
National Health Service (2021) Alzheimer's diseaseCauses Retrieved 27/04/2023 from https://wwwnhsuk/conditions/alzheimersdisease/causes/#: :text=The%20likelihood%20of%20devel oping%20Alzheimer's,the%20condition%20are%20under %2065
5 Emagine (2023) Brain imaging for alzheimer’s & dementia: Pacific Brain Health Center, Pacific Brain Health Available at: https://wwwpacificneuroscienceinstituteorg/brainhealth/diagnostics-procedures/brain-imaging/ (Accessed: 29 August 2023)
Figure 1: Brain imaging during development of Alzheimer’s Disease⁶.
TOPICS IN BIOMEDICINE
BY EGHOSA ENORIOMWANIHA
In vitro fertilisation (IVF) is a fertility technique for individuals that cannot conceive naturally. It consists of collecting eggs from ovaries which are fertilised in vitro with sperm to form an embryo which is then transferred to the uterus to develop⁶¹⁰
Is IVF a successful fertility treatment in the UK?
It is widely reported that IVF is a safe and successful fertility treatment, although factors such as age (women between the ages of 20 and 30 are more likely to have a successful treatment), embryo and sperm quality, and underlying conditions like PCOS have an impact on the success rate¹ . There are also physicochemical factors that can contribute to the outcomes of IVF procedures in the laboratory such as regulating the temperature, preserving osmolarity and pH, and preventing harmful chemicals² The governing body that oversees the guidelines that laboratories must follow for IVF treatment is the Human Fertilisation and Embryology Authority (HFEA).
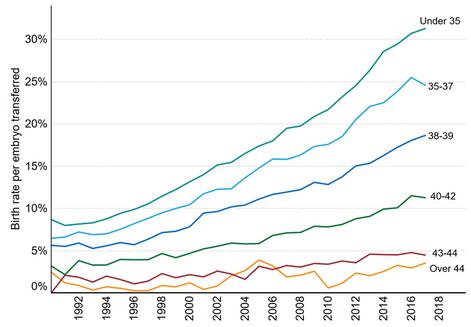
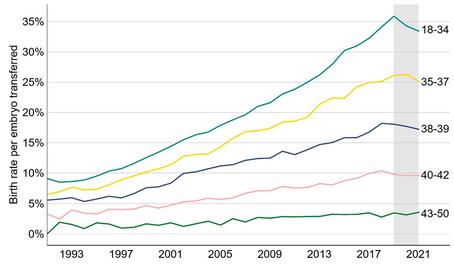
According to the Human Fertilisation and Embryology Authority, in 2016, there was a 4% increase in the number of IVF procedures carried out³ . The average birth rate per transferred embryo with IVF has increased over the years, reaching 23% in 2018. In 2018, the highest birth rate with this treatment was among those under 35 which has increased since HFEA was founded in 1991 (Figure 1)⁴ Since the early 2000s, there has been a steady increase in the success rate of IVF for most age groups In fact, all women under the age of 43 undergoing IVF now have higher chances of having a live birth thanks to medical advancements.
IVF therapy was performed on almost 55,000 people in 2021 at UK fertility clinics with HFEA licenses, an increase from about 53,000 patients in 2019⁵ Additionally, data indicates that the IVF birth rate employing fresh embryo transfers improved or stayed the same in all age groups (Figure 2)⁷
Figure 1: Rates of births per embryo implanted using patient eggs by age group, from 1991 to 2018 in the UK⁴.
Figure 2: The average birth rate per embryo transferred using patient eggs from 1991 to 2021 in the UK relating to fresh embryo transfers⁷.
In terms of numerical impact, IVF has resulted in more than 390,000 babies being born in the UK. This is a combined result of 260,000 donor insemination treatments and 595,000 IVF from partner egg/sperm⁵
Is IVF treatment successful in ethnic minority communities in the UK?
In 2013, 4,613 women from ethnic minority backgrounds used IVF in the UK, which rose to 5,563 by 2018, a 20.6% increase overall. In the UK, the number of Chinese women using IVF increased by 38%, and the number of women of Indian origin increased by 24% Furthermore, there were 20% more women of Pakistani origin in 2018 than there were in 2013 accessing IVF treatment, rising from 744 to 885⁴⁶ .
According to an HFEA study, women from ethnic minorities who receive fertility treatment are less likely to become pregnant, with Black patients having the lowest success rates Black patients aged 30-34 have an estimated birth rate of 23%, compared to 30% for mixed-race and White patients⁶ . Compared to only 18% of all the patients, a study found that 31% of Black fertility patients experience problems with their fallopian tubes Studies have also shown that Black individuals begin IVF approximately two years later than other ethnic groups⁶ . While Black patients experience the greatest disparities, other ethnic minorities also have low fertility treatment outcomes. Asian patients, who make up 7% of the UK population and 14% of IVF patients, have a challenge obtaining access to donor eggs In 52% of IVF cycles with an Asian patient, the eggs of white donors are used because 89% of egg donors are White, 4% are Asian, 3% are Mixed, and 3% are Black⁶ .
Actions in place to reduce inequalities in IVF treatment
The poor outcomes in ethnic minority communities can be influenced by several factors such as age, underlying conditions, and lifestyle There are also significant difficulties with getting egg and sperm donors, which coupled with cultural issues and fear of prejudice that delay accessing treatment may feed into IVF success rates⁹
Disparity in healthcare is also widely documented, so the possibility of discrimination from healthcare professionals through the journey of access and completion of IVF is possible Indeed, eligibility for free IVF treatment through the NHS depends on the area they live in, which may disproportionally disadvantage ethnic minority coupled⁶
There is currently no specific reason to explain the inequalities in ethnic minority groups when receiving IVF treatment, but some studies found that the eggs of the donors and recipients are associated with the race of the patients and the outcome of the treatment For example, research showed that in comparison to women who used Hispanic oocytes, which often had better outcomes despite the recipient race, Black women were likely to have poorer outcomes when using oocytes from young and healthy donors⁸
Some actions that have been placed by the HFEA to tackle the poor outcomes and disparities of ethnic minority groups when using IVF include:
Making sure that patients' ethnicity is recorded which will facilitate future studies as in the register, it was discovered that 12% of patients had no information on their ethnicity
Using the feedback provided by patients to improve the services.
Doing further research on the inequalities experienced by ethnic minority groups using this treatment
Working with other companies and organisations to gain an understanding of cultural and religious beliefs that may influence the outcomes of the treatment such as the Royal College of Obstetricians and Gynaecologists which launched the Race Equality Taskforce to educate individuals and the Fertility Network UK which is a charity that launched peer support groups for women of different ethnicities⁶ .
Conclusion
These actions will allow new beginnings as there will be an improvement in the trends of IVF efficacy which will also have a positive effect on the public as it will encourage and motivate them to try the treatment.
References
2
3
4
5
6
Amini P Ramezanali F Parchehbaf Kashani M Maroufizadeh, S, Omani Samani, R, & Ghaheri, A (2021)
Factors Associated with In Vitro Fertilization Live Birth Outcome: A Comparison of Different Classification
Methods International Journal of Fertility and Sterility 15(2) 128-134
https://doiorg/1022074/ijfs2020134582
1 Consensus Group Cairo (2020) ‘There is only one thing that is truly important in an IVF laboratory: everything Cairo Consensus Guidelines on IVF Culture Conditions
Reproductive BioMedicine Online 40(1) 33-60
https://doiorg/101016/jrbmo201910003
Human Fertilisation & Embryology Authority (2018) IVF treatment safer, more available and more successful than ever before, new report shows https://wwwhfeagovuk/about-us/news-and-pressreleases/2018-news-and-press-releases/press-release-ivftreatment-safer-more-available-and-more-successfulthan-ever-before-new-report-shows/
Human Fertilisation & Embryology Authority (2020)
Fertility treatment 2018: trends and figures https://wwwhfeagovuk/about-us/publications/researchand-data/fertility-treatment-2018-trends-and-figures/
Human Fertilisation & Embryology Authority (2021)
Fertility treatment 2019: trends and figures https://wwwhfeagovuk/about-us/publications/researchand-data/fertility-treatment-2019-trends-and-figures/
Human Fertilisation & Embryology Authority (2021)
Fertility treatment less successful for ethnic minority patients new figures reveal https://wwwhfeagovuk/about-us/news-and-pressreleases/2021-news-and-press-releases/fertility-treatmentless-successful-for-ethnic-minority-patients-new-figuresreveal/
Human Fertilisation & Embryology Authority (2023)
Fertility treatment 2021: preliminary trends and figures https://wwwhfeagovuk/about-us/publications/researchand-data/fertility-treatment-2021-preliminary-trends-andfigures
7 Liu, Y, Hipp, H S, Nagy, Z P, Capelouto, S M, Shapiro, D B Spencer J B & Gaskins A J (2021) The effect of donor and recipient race on outcomes of assisted reproduction American Journal of Obstetrics and Gynecology, 224(4), 374e371-374e312 https://doiorg/101016/jajog202009013
8 Mosalanejad, L, Parandavar, N, & Abdollahifard, S (2013) Barriers to infertility treatment: an integrated study Glob J Health Sci 6(1) 181-191 https://doiorg/105539/gjhsv6n1p181
9 National Health Service (2021) Overview - IVF Retrieved 05/08/2023 from https://wwwnhsuk/conditions/ivf/ 10
To be able to understand these cells better let us look at distinct types of stem cells and their brief description
Adult stem cells:
The most popular and the least controversial stem cells These are extracted from the patient’s own bone marrow and replaced back into the patient’s affected area to repair damage
Limitations of using these cells are their availability is low and they are difficult to isolate and purify Adult stem cells might have their DNA damaged by sunlight and might contain toxins that would limit their usefulness⁵
Umbilical cord cells:
These stem cells are extracted from various parts of the umbilical cord or placenta at birth and can develop into several types of blood cells However, umbilical cord-derived stem cell therapies for adults have been particularly challenging and have not shown major improvement, another limitation is that they can only treat blood-related conditions⁵ .
Foetal stem cells:
Provide stem cells capable of differentiating into all cell types. These are extracted from a foetus after an abortion if the family has given consent. A key limitation is that foetal stem cells can only be extracted from 8–9-week-old foetuses and have limited proliferation capacity⁵ .
Embryonic Stem Cells are far from the most controversial stem cell type To be able to carry out research many stem cells are required due to these being unstable and delicate This is because these cells must be kept under specific conditions to allow their growth in the lab
What are embryonic stem cells?
After fertilisation, the zygote’s first divisions are called cleavage which distribute the cytoplasm equally among the blastomeres (cells formed after cleavage) Compaction leads to the formation of the primitive cyst consisting of eight cells, these eight cells further divide forming sixteen cells; this is called a morula, which divides into a sphere of cells (64 cells) called a blastocyst Blastocysts have an inner cell mass where all these embryonic stem cells (ESCs) are found All these processes take five to six days after fertilisation In normal embryonic development, after the seventh day, they start forming tissue layers that end up forming the foetus. ESCs can be extracted from the inner cell mass and cultured in the laboratory where if kept in the desired conditions proliferate indefinitely³ .
ESCs can differentiate into a variety of somatic cells, properties that make these cells exceptional ES cells can be cultivated in vitro, these continue dividing and increasing the numbers of cells indefinitely These cells can be kept for a prolonged period, and they retain their properties e g , pluripotency, which is the ability to develop into any cell type in an adult body)²
Pluripotency is promising great advancement in, disease modelling, toxicology, drug discovery, and cellular therapy development In summary, these cells would revolutionise clinical practice as they offer the prospective of personalised medicine One point to take into consideration is that these cells are extracted from the inner cell mass of 5day-old embryos which brings about ethical concerns
There are four sources of human embryonic stem cells (hESCs) used in research:
1 Immature aborted foetuses (EG cells)
2 Fertilisation in the lab by donated eggs and sperm
3. ‘’Spare’’ embryos from in vitro fertilisation (IVF) clinics
4. Embryos created through SCNT (somatic cell nuclear transfer)
The use of human embryonic stem cells (hESCs) creates an ethical dilemma for many, with religion quite often influencing people's points of view on matters such as when exactly life begins Whilst some people hold the view that abortion is always the woman's choice, for others abortion is only acceptable in exceptional circumstances, for instance, if it improves quality of life or health
Of course, there are those who completely disagree with abortion and so the use of hESCs is never acceptable The consensus is that the use of ‘’ spare ’’ embryos from IVF is ethical This is because these embryos are created for reproductive not scientific purposes Many people believe that the ‘’ spare ’’ cells could potentially save lives and just wasting them cannot be justified by anybody's beliefs or thoughts There are two ways in which we can further divide the ethical viewpoints: fatalistic and feministic⁴
Fatalistic: This discusses the moral status of the embryo
Different religions have their own interpretations of whether embryos have a status or not according to some at the time of conception life has started therefore, killing the embryo is taking a life
Scientists believe that religion confuses “fertilisation” and “conception ” Conception is the natural formation of the zygote that grows in the womb and forms a human being On the other hand, fertilisation can occur in the lab by growing cells in a petri dish, this has no possibility of forming a human being unless implanted into a womb These cells are genetically human but do not present human characteristics, neither conscious nor self-aware, hence not moral status⁴
Feministic: The second major problem of embryonic stem cell research is that many eggs are required to keep up with this, and many women donors are needed These volunteers go through an uncomfortable procedure which is painful and carries medical risks
In conclusion, allowing embryonic stem cell research could potentially lead us to experiment with different major diseases in more depth Allowing us to understand human life better as well as bringing change in its quality However, I want to also make a point about how not allowing embryonic stem cell research is staying in the safe zone Ask yourself, is extracting eggs from women who are not really being educated about the potential risks of the process itself ethical? You cannot forget the fact that although, here in the UK, the donors do go through a secure procedure, not everyone around the world is equally privileged Therefore, in my opinion, we are saving lives by not allowing embryonic research because this is a way to prevent many violations of human rights
The following newspapers ’ article proves how something similar has happened in East Europe:
In 2006 unanimous reports were found that young women from Russia, Ukraine, and Poland were paid to sell their eggs These women were left uninformed about the potential risks associated with egg donation Moreover, they lacked awareness about the specific that were being used and the potential side effects A woman confessed that she donated her eggs only for financial reasons and kept this decision concealed from her family Not only this, but she also proceeded to reveal that she knew 20 other women who had done the same Clearly, these young women were exploited Serving as a means to procure eggs, which were then made available to Western women who were willing to pay substantial amounts to fulfill their dreams of parenthood Moreover, selective breeding also occurred while picking the eggs, because the donors were often individuals with gifted genes, tall, healthy, and intelligent¹
References
Barnett A & Smith H (2006) Cruel cost of the human egg trade https://www theguardian com/uk/2006/apr/30/health hea lthandwellbeing 1
Ilic D & Ogilvie C (2017) Concise Review: Human Embryonic Stem Cells What Have We Done? What Are We Doing? Where Are We Going? Stem Cells, 35(1), 17-25 https://doi org/10 1002/stem 2450 2 Klimanskaya, I , & Lanza, R (2006) Methods in Enzymology - Embryonic Stem Cells (Vol 418)
3 Nambisan P (2017) Chapter 3 - Stem Cell Research In P Nambisan (Ed ), An Introduction to Ethical, Safety and Intellectual Property Rights Issues in Biotechnology (pp 55-81) Academic Press https://doi org/https://doi org/10 1016/B978-0-12-8092316 00003-X
Real Stories (2019) Stem Cells: Medical Miracle Or Science Gone Too Far? (Medical Documentary) | Real Stories https://www youtube com/watch?v=Nv14cCbU8t0
SALFORD SCIENCE
BY MARKELLA LOI
According to the World Health Organization (WHO), 149 per million children will be diagnosed with cancer worldwide annually, while 90,000 will die of cancer and its associated complications every year³ . Despite the continual advances in cancer research and treatment resulting in an impressive increase in childhood cancer survival, approximately 75% of these surviving children will suffer from the late effects of chemotherapies, such as cardiac complications and develop chronic life-threatening illnesses
Cancer research continues to thrive as an enduring and captivating field of study with the pursuit of new developments and innovation offering hope for a brighter future Research on the long-term cardiac implications following cancer treatment marks a new beginning in the quest to mitigate these side effects and extend the lifespans of survivors.
Anthracyclines are a class of anti-tumour compounds, commonly used as part of the treatment regime for childhood cancers, like osteosarcoma and rhabdomyosarcoma⁴ Daunorubicin (DAUN) and doxorubicin (DOX) are the most widely utilised compounds within the family of anthracyclines. Unfortunately, exposure to these drugs has been linked to the development of heart failure, affecting the majority of childhood cancer patients⁷ This cardiac dysfunction typically appears following remission and can occur up to 20 years after treatment⁷
The mechanisms that underpin this toxicity are not fully understood. Nonetheless, it is suspected that anthracycline-mediated cardiotoxicity is a result of excess production of reactive oxygen species (ROS) and thus elevated levels of oxidative stress (OS) These elevations damage cellular DNA, leading to the dysregulation of cellular functions, and ultimately cell death¹ Previous research has demonstrated that oxidative stress “significantly contributes” to cancer cell cytotoxicity² . Surprisingly, not many studies have been conducted on the specific role of reactive oxygen species production following treatment with anthracyclines in cardiac cells
Therefore, the debate about the actual mechanism of action of these anticancer agents continues The aim of our study was to address:
if anthracyclines, DOX and DAUN, kill cancer based on oxidative stress alterations
2
if anthracycline-mediated heart cell death can be prevented with the use of commercially available antioxidants, such as N-acetylcysteine (NAC)
The viability of both cancer (data not shown) and cardiac cells was initially assessed using a colourbased assay As expected, both anthracyclines reduced cancer cell viability, specifically by 50 % at 0 312 μM for doxorubicin and 0 156 μM for daunorubicin In this case, a concentrationdependent mode of action is observed for doxorubicin.
Figure 1: Oxidative stress of different treatments in cardiac cells Different anthracycline treatments and their corresponding levels of fluorescence, as assessed via the DCF-DA assay
To answer how exactly anthracyclines induce cell death in both cancerous and cardiac cells, we aimed to indirectly measure oxidative stress levels induced by DOX and DAUN using the DCF-DA assay The specific technique relies on the oxidation of the dye by the ROS present, causing it to emit fluorescence proportional to oxidative stress levels⁵⁶
Doxorubicin treatment in osteosarcoma cells, showed a significant dose-dependent increase in oxidative stress between different concentrations (p<0 05, n = 3), but daunorubicin did not, compared to control cells (data not shown)
The same alterations in fluorescence in the presence of anthracyclines were detected in cardiac cells (Figure 1). Doxorubicin and daunorubicin increased oxidative stress significantly compared to the combination treatments with N-acetylcysteine (p<0 05, n = 3)
Interestingly, cardiac cell viability was also reduced in a similar pattern to that of the cancer cells. Doxorubicin and daunorubicin decreased the viability of the cardiomyocytes, with a 50 % decline recorded at 0 156 μM for both compounds The addition of N-acetylcysteine in combination with anthracycline treatment decreased its cardiotoxic effects, as cell viability did not decline to the previous extent with just anthracyclines (Figure 2).
Figure 2: The cardiotoxic effect of anthracyclines was mitigated through co-treatment with N-acetylcysteine. Cardiac cells were exposed to various treatments of anthracyclines alone or combined with 1mM NAC and viability was assessed employing MTT assays.
Increased cardiac cell viability and extremely low ROS levels in its presence suggest compelling evidence that elevated oxidative stress results in cancer and cardiac cell death.
Our findings propose that oxidative stress has a pivotal role in the way anthracyclines kill cancer cells and damage cardiac cells, leading to cardiotoxic side effects This reveals that further targeting of reactive oxygen species production may decrease the likelihood of long-term cardiac complications in childhood cancer survivors, providing a new beginning for mitigating these side effects and increasing survivor lifespans This study also highlights that the use of the commercially available antioxidant Nacetylcysteine may offer a cheap, safe, and readily available strategy to mitigate cardiac complications Consequently, further research on cardioprotective strategies related to oxidative stress is strongly advised to better understand the global impacts of this treatment strategy and to evaluate if more specific reactive oxygen species pathway inhibitors are more effective than Nacetylcysteine at alleviating chemotherapyinduced cardiac dysfunction.
Acknowledgements
I would like to thank Kidscan Children’s Cancer Research for funding my industrial placement year and supporting the laboratories research into new treatments for chemotherapy induced cardiac dysfunction I would also like to thank Dr David Greensmith (Reader in Cardiac Physiology, University of Salford), Dr Amy Foster (Research Assistant, University of Salford) and Dr Matthew Jones (Lecturer in Physiology) for their constant support and guidance during my placement year and throughout the final year of my degree
References
Berthiaume, J M , Kirk, J A , Ranek, M J , Lyon, R C , Sheikh, F , Jensen, B C , Hoit, B D Butany J Tolend M Rao V & Willis M S (2016) Chapter 8 - Pathophysiology of Heart Failure and an Overview of Therapies In L M Buja & J Butany (Eds ) Cardiovascular Pathology (Fourth Edition) (pp 271-339) Academic Press
https://doi org/10 1016/B978-0-12-4202191 00008-2
1 Carrasco, R , Castillo, R , Gormaz, J , Carrillo, M , & Thavendiranathan, P (2021) Role of Oxidative Stress in the Mechanisms of Anthracycline-Induced Cardiotoxicity: Effects of Preventive Strategies Oxidative Medicine and Cellular Longevity, 2021, 1-16. https://doi org/10 1155/2021/8863789
2 Jin, Y , & Lyu, Q (2020) Basic research in childhood cancer: Progress and future directions in China Cancer Letters 495 156164
3 Samuel, L , Cummings, J , & Shaw, P (1998) Daunorubicin cardiotoxicity in childhood cancer Lancet, 352(9134), 1150
5
Thermofisher Scientific (2006) Reactive Oxygen Species (ROS) Detection Reagents Retrieved 12/08/2023 from https://www thermofisher com/documentconnect/document-connect html?
url=https://assets thermofisher com/TFSAssets%2FLSG%2Fmanuals%2Fmp36103 pdf
7
Thermofisher Scientific (n d ) Invitrogen™ H2DCFDA (H2-DCF, DCF) Retrieved 12/08/2023 from https://www thermofisher com/order/catalog /product/D399
6 Zamorano Gómez, J L , Ramos, J , Alcidi, G , & Galderisi M (2017) Chapter 27Cardiotoxicity of Childhood Cancer Treatments In P Lancellotti, J L Zamorano Gómez & M. Galderisi (Eds.) Anti-Cancer Treatments and Cardiotoxicity (pp 309-326) Academic Press
Genomics Advancements: The Future Of Whole Exome Sequencing
DR ARIJIT MUKHOPADHYAY IN CONVERSATION WITH MARY YUHANNA
EDITED BY WIKTORIA WISNIEWSKA
Novel genomic research comes with very promising and revolutionising prospects in disease monitoring and treatment The newest findings of whole exome sequencing and gene editing
CRISPR technologies are major contributing factors to a newly found DNA profile-targeted approach in the growing field of personalised medicine
In this interview Mary Yuhanna spoke with Dr Arijit Mukhopadhyay a reader in human genetics at the University of Salford about his passion for human genetics dedicated interest in glaucoma neurodegeneration research and the future of personalised medicine-driven National Health Service
How and when did you become so passionate about genetics?
I do not think there was one specific day when I suddenly decided, it was complex Interestingly, I always liked biology, but I also liked pure sciences: physics, chemistry, and maths When I had to choose my undergraduate subjects, I chose chemistry with physics and maths, and I went on to do a master’s in pure chemistry as well Then, my career started with working in the chemical industry as a research technician After 18 months I decided to jump in the unknown and started a PhD in human genetics My father is an anthropologist, I grew up listening to him, talking to his students about human pedigrees and human evolution and I am sure that played a role
I grew up in India and was privileged to grow up in an academic family which played a role in shaping my views I was fortunate enough that I did not have to think about earning money to support my family I want the young readers to know that it is completely random luck that I had those privileges This made it easier for me to take risks without thinking about job security, otherwise, it would not be possible
Most people in the biological field studying genetics or genomics tend to move toward RNA as it is a little bit more complex. What shifted your mindset from DNA to RNA?
I cannot pinpoint a particular reason or a particular time or day As a scientist when you do your PhD which is a training in science you understand how to ask questions how to design experiments and how to interpret them objectively When you start to think about bigger questions you realise that you are a small player on a big canvas Then you start to think about bigger questions and in the biomedical space, you think about either understanding nature or solving problems, diseases in this case Technically speaking, you start your journey with DNA, then you realise that DNA does not give you all the answers
"DNA IS AN IMPORTANT CONTRIBUTOR, BUT IT IS JUST ONE CONTRIBUTOR."
Measurable phenotypes are very complex outcomes of many factors DNA is an important contributor but it is just one contributor After my PhD I spent about six years part as a postdoctoral fellow and part as a principal investigator on DNA trying to answer bigger questions based on DNA With every project I increasingly realised that DNA would only answer so much and not beyond I moved to the next level of complexity in the biological system, which is RNA If you think about the rest of your career as an academic scientist, you understand the limitations of your field, and then you try to incorporate more complex things to get a clearer answer
When you realise DNA can do so much, you incorporate RNA It is not one replacing the other, it is adding the complexity because your ability to handle complexities improves and that is the natural transition nothing special about me
Recently you published an article about using whole exome sequencing, which revealed novel candidate genes in familial forms of glaucomatous neurodegeneration What is whole exome sequencing and how far can we take this in genetic, this genetic advancement in scientific research?
First, glaucoma is a disease of the eye It is a wide variety of diseases, not one particular phenotype, all these put together cause neurodegeneration That is why the technical term for glaucoma is glaucomatous neurodegeneration The paper is in glaucoma genetics Exome means all the exons of all the genes put together
These days you hear a lot of words which have "-ome" at the end Proteome exome lipidome, genome: -ome means all. Coming from to the central dogma of molecular biology, DNA makes RNA and RNA makes proteins For the human genome, for our cells, that central dogma DNA to RNA to protein is the linear part of the central dogma, there are non-linear parts as well Only 2% of our genome makes proteins When you deal with human diseases, the first place to start looking for problems are the proteins, which do not answer all the questions That is why scientists figured out a way, back in around 2010, to capture only this 2% from the entire genome, and remove the 98% that is not coding for protein Because of this technology, exons (which make mRNA and proteins) are all grouped together that is why it is called an exome
The human genome is 3 billion base pairs 2% of that about 62 megabases that is what exome is It has been around for more than 10 years now and it is quite widely adopted If you have a reason to hypothesise that the disease or the phenotype you are trying to figure out genetically has a protein as a key molecule, then it makes sense to not look at the rest That is why exome sequencing has been powerful For the experimental part, it is not necessarily cheaper than whole genome sequencing because capturing this 2% is cost-intensive, but the analysis is easier because you are only looking at 62 million base pairs instead of 3 billion base pairs
Analysis-wise, it is quicker In the UK, the NHS regularly uses it as part of clinical service, not for all diseases though In diseases where the phenotype is not obvious, where we do not know the genes, but it looks like a rare and penetrant disease then doctors in the NHS can prescribe exome sequencing This would be done in one of the genomic services of NHS to get the data so that that is not even futuristic; it is widely used across the world
Do you know, per patient, how much that costs?
The way I do it as an academic researcher in the lab, and the way NHS will do it would be different What I mean by that is for any omics type of work and the very nature of these technologies, is that if you do a smaller number of samples, per sample, the cost is higher compared to the greater number of samples When NHS does it, they do work in volume When academics do it, they work on one family at set a time
For the paper you mentioned we worked on total 30 individuals That experiment happened three to four years ago. That experiment was done in India on Illumina platform All these parameters are important because when you change the technology and the country, the costs change This was done in India for a smaller number of samples, and that costed us approximately £3000 per sample
How far can we take this genetic advancement in scientific research?
If you think that all these technologies, these are all at the DNA level First, any genetic condition that is not on DNA, can be an epigenetics, RNA level problem, an environmental problem and would not be answered by exome sequencing If the answer is in DNA then it may or may not be in that 2% of the genome
Diseases like cystic fibrosis Duchenne muscular dystrophy Huntington disease are quite aggressive in genetic terms We call it highly penetrant If you come up with a patient with those phenotypes genetically well-known phenotypes, and you know which gene to look at, then you do not have to go through the process of capturing these 2% of the genome and sequencing them You can use exome sequencing when the disease looks penetrant enough, but the gene is not known, so that it is rational to hypothesise that the mutation would be disrupting a protein function When you are dealing with a condition with more uncertainty, the whole genome sequencing is a better approach, as it gives a wider search space to get the answer to your question
Do you agree that due to the current genetic advancements, we are heading towards a disease-free future by 2050?
It is not going to happen I think it should be mandated that everyone reads the book called ‘The Code Breaker ‘The Code Breaker’ book came out in 2021 is on the CRISPR discovery, from the point of view of Jennifer Doudna If you said 100 years, I’d probably have said yes or 200 years, I would probably have said yes By 2050, which is 25 years, probably not We now have a technology where we can change any nucleotide on the DNA We learnt only to rewrite the code post 2012 The technology is getting perfected, you might change something else, inadvertently
Unless it is perfected to that level we would not be able to cure all diseases Known inherited diseases mentioned before will probably get cured through CRISPR in 25 years We understand how to read those pages of the genome so well that we feel comfortable rewriting them CRISPR, as it stands now, is now being applied to RNA In addition to DNA, CRISPR is now starting to come out that they can edit epigenome as well, but these are much earlier in the process of a perfection They will take longer; most diseases will have an epigenetic component
For sickle cell anaemia, thalassemia, it is quite advanced It might happen in next five years that it is quite advanced across the world, not only in the UK or US Many places in the world are doing that so that will happen sooner for HIV There were efforts where this has been successfully done in the stem cell If you think of applying CRISPR to cure diseases it depends on at what level you detect the disease If you are dealing with an adult who has trillions of cells in their body and if they have an inherited mutation which is presenting all cells of their body, and if they suffer from a disease that affect multiple organs, then where do you correct using CRISPR? Conceptually speaking, the best outcome of a gene editing technology for curing the disease would come if you can cure at the stem cell stage because then all the cells will be cured, the corrected genome That will also play a crucial role in which disease this can be cured and in which it cannot e are not far from a time where you can buy a gene editing kit on a super supermarket shelf, people will be able to do it at home It will be as simple as at administering insulin onto your body
It will be as simple as at administering insulin onto your body It will be as simple as doing a pregnancy test or doing Covid test at home These are also biology experiments if you think about it but we have made it so streamlined that people can do it at home As this famous line goes that with greater power comes greater responsibility Now, where do you draw the line? Who decides that? Does a parents get to choose and change their foetus? Designer baby? Where do we draw the line so that we do not fall in the trap of eugenics again? You are trying to see that before CRISPR is widely used to cure all the problems we must first define what is a problem and what is not a problem The ethics and the legality of it must catch up before these can be utilised for greater good so that we do not create monsters
The NHS has completed the ‘Hundred Thousand Genomes Project’ and aims to have genomic sequencing as part of healthcare routines What do you think about personalised medicine and its future impact?
What I think about personalised medicine I think that should happen Consider siblings, we have all seen you both take a tablet of medicine, and you develop an allergy, and your sibling does not The idea is that you would react differently to an exposure, or you react differently to a drug, which is also an exposure that is quite common I do not think it is practical to think that there will be medicine designed for you as a person What might happen, or what is already happening, and that will get better with time is that rather than giving a generic drug for a generic condition will be able to subgroup people into their predispositions based on their genetic makeup We would be able to tell that this group of people is allergic to this drug so we should be able to check from the genetic data and then give an alternative drug It is personalised but as a group rather than a single person. In another scenario, there might be a future where you go into a clinic, they investigate your DNA profile and your other biological parameters, and then maybe there is a drug 3D printed for you These are possible, but I think it is more likely that we will be able to form smaller groups of people who would behave similarly given an external exposure either to a drug or to an environmental exposure such as COVID-19, for example In the NHS-led 100K Genome project, the summary of that vision is that HS foresees a future where genetic information would be the first layer of health management The project has not only sequenced the whole genome, but they have also done the whole exome for a part of the samples There are different layers of data and all this data is part of the UK Biobank which researchers can access for a fee Now there is a newborn screening programme announced as part of the Hundred Thousand Genome Project I foresee a future where every child soon after they are born the parents will their genome information in a card like a credit card with a microchip I dream of a future (albeit with my personal bias) where when a person goes to a doctor, a swipe of that card will tell the doctor of all the disease predispositions encoded in their genome The major hurdle is the ethics of consent, confidentiality, and ownership of the data We are entering an exciting era in healthcare where it will be data driven, from multiple sources, and artificial intelligence will integrate it together to get a better understanding of health
Do you think that it will happen? Are you saying that it should happen?
I think it will happen The companies like Illumina who holds more than 90% share in the genomics market has a vision to make genomics a consumer item like any other daily consumables such as toothpaste It means they want to get it to every household so that public does not have to deal with this complexity of talking to researchers and people like me who talks in language that most people do not get, so that barrier is removed I am not saying it should happen, I am saying it will most likely happen The ethics will become increasingly more important with increasing access to genomic technologies What do you do with the data? We need more genetic counsellors who will be that bridge between lab scientists or clinicians and the members of public who can alleviate the anxieties, who can tell them what to do, what not to do, and how not to extrapolate, how not to sensitise themselves with the information And even before that, empower the public to choose if they even want to know what their genome holds? Those things need to be figured out before it reaches a consumer level Technically we are there now but ethically we are far away We have sequencing machines that are smaller than a smart phone
If a baby has a genome sequenced, who should know that information? Should the future employers know? Should the insurance companies know?
British Society of Genomic Medicine is the formal organisation in this country who informs parliament and the ministries about the policies, guidelines, and changes Back in 2019, they published a new guideline for ethics of genomics data I was fortunate enough to part of the sub-committee who drafted that guideline I went through the process of the debate and discussions what should be there or should not be there It is not that we reached a definitive answer but the point I am trying to make is that debate needs to be continued across all stakeholders clinicians scientists students of science public everybody should have a say on these Until we have figured it out a situation or everybody is reasonably satisfied Until then we are not ready to use that technology
You spoke about obviously personalised medicine and how much data we are getting from the NHS now Do you think currently we have enough people to look through and analyse this data? And if not, why is that?
The answer is no, we do not Currently for 64 million people, we have less than 500 genetic counsellors only in this country, most of the other countries are even worse For your question about data analysis, it is even less promising now What we know now is that genomics is more data science than biology The reason I see it that way is because most of the data generation part, which is the biological experimental side part has now been automated
Now you do not need a human being to operate a genomic instrument a robot can do the analysis most of it; the basic analysis is also automated It happens in the cloud with AI but when you are trying to explain a phenotype which is still a very human driven side of the process We do not have enough people who understands data and can deal with complex data parameters from a computational point of view and understands biology Biologists cannot do it Data scientists cannot do it We need people skilled in interdisciplinary areas such as genetic counsellors and genome informaticians
Finally, do you have a thoughtprovoking question for our readers?
Just because we can, should we sequence everyone ’ s genomes?
pg.32 pg.32
CAREER ADVICE CAREER ADVICE
Tahmina Hussain discusses Equity, Diversity and Inclusion within the workplace
pg.34 pg.34
CAREER STORIES CAREER STORIES
An insight into the transition from life as a Biomedicine student to life as a Physician Associate student and how to maintain your mental health and wellbeing in the laboratory
pg.38 pg.38
CAREER INSIGHTS CAREER INSIGHTS
Interview with Craig Brierley from the University of Cambridge on science communication Also, Sue Jones explores how the IBMS are preparing our future biomedical scientists
REPRESENTATION MATTERS. YOU CANNOT BE WHAT YOU CANNOT SEE!
CAREER STORIES
University of Manchester, but I started my academic journey at the University of Salford where I studied Biomedical Science
Out of college, I knew I enjoyed Biology but was still confused career-wise Therefore, I chose this Biomedical Programme because it was accredited and offered a unique opportunity to complete a placement year within my degree to gain some real-world experience This turned out to be one of my best decisions because the entire Bioscience team was fantastic, and the programme turned out to offer so many opportunities to take part in that other universities did not In my placement year, I gained a lot of hospital and research experience, which really boosted a newfound passion for Medicine and gave me a clearer idea of the career I wanted. After returning from my placement year into my final year I decided to no longer be in “Auto-mode” and to participate in all the opportunities that the university offered.
The first opportunity that came along was when Dr Sara Namvar and Prof Niroshini Nirmalan announced a presentation competition called Salford PassionFlash. I decided to get out of my shell and took part. I was stunned to be one of the winners with my presentation on ‘The Advancement of Homo Sapiens.’ From here I joined the Biomed Society which really allowed me to experience different opportunities, like presenting at the University Future Health conference and helping with events like secondary school science outreach I also joined GEMMS (Graduate Entry Medicine Mentoring Scheme), which really equipped me with the skills and knowledge I needed to complete the Physician Associate application process Being around such an inspiring and fantastic group of people that really supported me through my degree and beyond, affirmed my decision to get out of my shell and take every opportunity Once I graduated, I applied to a neverending list of jobs and was fortunate to secure a Research Assistant position at the University of Manchester where I now research agricultural health hazards I initially applied for Medicine, but I was concerned about the course duration and having to leave home to study in another city
Therefore, after researching and speaking to many different Physician Associates, I realised that the Physician Associate course and career were extremely suitable to my character and circumstances The Physician Associate application process was quite different when I applied because each University had a different process In my personal statements, I mentioned the skills and experiences I gained from my degree, placement year, Biomed Society, GEMMS, and voluntary work I also made sure to link the experiences I had to the skills that are essential for this line of work and highlighted how this will help me be a good Physician Associate The key points I mentioned included effective communication, interpersonal skills, teamwork, and compassion, alongside my Biomedical knowledge.
The interview process for the University of Manchester Physician Associate course was an MMI (multiple mini-interview) based interview, which involved 5 10-minute stations that each contained a different question or scenario. The interview process was very nerve-wracking, but GEMMS regularly set up mock MMI interviews which really helped me get used to the format and practise my answers I must have spent weeks practising for the interviews and after some ups and downs, it finally worked out when I was accepted to the University of Manchester I have recently started the Physician Associate course and I am absolutely loving it Being able to turn theoretical scientific knowledge into practical skills is a new skill set that I am excited to learn and using my Biomedical Science knowledge to help people in a clinical setting feels extremely rewarding In hindsight, I am so glad that I became more active in my academic journey and took part in the opportunities because I gained new experiences and skills that propelled me to where I am now and allowed me to interact with so many inspiring and supportive individuals from this University
CAREER STORIES
Managing Mental Health And Wellbeing While Working In A Laboratory
BY LLOYD MCLEGGON-ATKINSON
Working in medical laboratories has undoubtedly been a fruitful journey over the last 7+ years. I have picked up numerous skills, first in Microbiology as a Medical Laboratory Assistant and more recently in Immunology as an Assistant Practitioner (AP) I take a great deal of pride in providing the best possible patient care, which gives me a sense of fulfillment and helps me sustain a high level of quality
My reflection followed the methodology of the ERA reflective method which simply analyses what happened, the significance, and the following action (Experience, Reflection, Action)² . I looked and my mood and behaviour had become lower and more irritable The significance was a reduced enthusiasm to be in work, but fortunately, the care I put into my work I did not feel was impacted Another question was ‘why?,’ on reflection I struggle to delegate tasks, making me feel I take on more than I should This can have an impact on the quality of work performed as stress increases
The workplace can be a naturally stressful environment, with high workloads and everchanging scenarios including staff sickness. In times of stress, it is often the case to try and power through and avoid asking for assistance The resolution for my problem was simple, a discussion with management to spread the workload between other colleagues I now recognise that I must delegate and ask for help earlier With the apprenticeship degree alongside my role in the lab, it is more important now to ensure some kind of balance to maintain a healthy work/study/life balance and take effective steps to maintain fitness to practice, not only for me but all registered/nonregistered healthcare science staff
Multitasking is an important skill in the lab. For instance, at any time, I may be processing specimens, supervising junior staff, and communicating with the support staff registered Biomedical Scientists (BMS), which can be stressful at times but manageable Being fully competent, I am often asked to provide additional support for colleagues at my level and registered scientists due to the experience I have gained. Three years ago, I had an opportunity to be involved in a project in the department focused on HIV monitoring in developing countries My role in this project evolved into developing and implementing the official in-house standard operating procedure, completion of risk assessment and COSHH, and provision of training for all staff involved This was the moment I had noticed the impact of stress in the workplace.
Figure 1: A diagram of the ERA Reflection Cycle⁴
Mental health is described as a person ’ s state of mental well-being, enabling them to work well, communicate, build relationships, and cope with stresses in life⁵ , with well-being viewed as an individual’s positive outlook on their life with the absence of negative thoughts, combined with physical wellbeing1 This does not mean that there will never be bad days, some days are worse than others and at times it can be difficult to handle It is natural as human beings that tolerance wanes from time to time The ability to identify, interpret, and manage these feelings is what enables me to balance my mental health and well-being. Without balance, emotions can soon spiral out of control.
A lack of self-understanding and balance may lead to slight distractions and irritation, an outburst in emotions, mood changes, lack of concentration, or may even lead to physical illness For me (with the help of my colleagues), the irritation and low mood were noticed, and I took steps to resolve the issue by identifying the root causes
I had to reflect on myself and my feelings and analyse why my behaviours and mood had changed, without being so formal as to document my feelings on paper The stress container model is a method of summarising stress management³ The container is your individual capacity of storing stress with one main outlet for allowing ‘water’ to exit Water stored in the container represents the various sources of stress (e g , family, work, loneliness, money) If stress exceeds the container capacity or fills faster than it empties, water overspills just like stress overspills into outward emotions. Extra holes can let the water and stress escape from the container and prevent overfilling, such as talking with friends, exercise, resting, doing something personally satisfying.
Managing mental health and well-being is an ongoing effort and never ends Looking after yourself and others in the laboratory benefits not only myself but my colleagues and the patients we care for.
If you do want to speak to someone then talk to a close friend, or family member, AskUs at the University of Salford, occupational health/MHFA in the workplace, or a support service. If you need help, please ask.
List of Mental Health and Well-being support services and information
Time to Change - https://www time-tochange org uk/mental-health-andstigma/help-and-support
Local GP Practice
999 in emergencies
Occupational Health in the workplace
Figure 2: A diagram of the stress container model³
References
2
3
4
5
CDC (2018, 31/10/2018) Well-Being Concepts
Centers for Disease Control and Prevention Retrieved 06/02/2023 from https://www cdc gov/hrqol/wellbeing htm
1 Jasper, M (2003) Beginning reflective practice Nelson Thornes MentalHealthUK (2023) The Stress Bucket Retrieved 06/02/2023 from https://mentalhealth-uk org/blog/the-stressbucket/
Miller K (2022) In-depth Explanation of ERA Cycle of Reflection Writing Retrieved 25/07/2023 from https://crowjack com/blog/strategy/reflectionmodels/era-cycle WHO (2022)
Mental Health: strengthening our response Retrieved 06/02/2023 from https://www who int/news-room/factsheets/detail/mental-health-strengthening-ourresponse#:~:text=Mental%20health%20is%20a%2 0state and%20contribute%20to%20their%20com munity
WHO (2022) Mental Health: strengthening our response Retrieved 06/02/2023 from https://www who int/news-room/factsheets/detail/mental-health-strengthening-ourresponse#: :text=Mental%20health%20is%20a%2 0state and%20contribute%20to%20their%20com munity
CAREER INSIGHTS
In this interview, Alia Boda, a Human Biology and Infectious Diseases student, had an opportunity to speak to the Head of Research Communications at the University of Cambridge to gain insights on effective communication in science, particularly showcasing novel research
Please will you tell us a little bit about yourself and your role?
I am the Head of Research Communications at the University of Cambridge My team here is responsible for telling the stories about research that takes place across the University That is through media relations and via our website to public audiences and other stakeholders to people across the university, other researchers, researchers outside the university, Industry collaborators, policymakers, etc
What research have you come across that you have found interesting?
That's a really difficult question because there is so much that I come across on a day-to-day basis that is fascinating For me, one of the genuine privileges of doing this job is that I am working with some of the people who are at the absolute top of their field, and these are the people who will sit down and explain their research to you and talk you through it It is genuinely quite exciting to be able to do that For example, I was speaking to a researcher who is using virtual reality gaming to try and help people overcome anxiety, so that is really cool when you get to play with a bit of kit and experiment with yourself Likewise, there are other times when you'll sit down with somebody that does very fundamental research that on paper could sound boring, but when you get chatting with them you can see the passion in them and that can be quite exciting; you realise that you're probably one of the first people in the world to be hearing about this. Just last week I went across to meet one of the heads of one of our colleges (former UK ambassador to Russia and Afghanistan) who spent half an hour with us telling us about Ukraine and Russia why Russia had invaded Ukraine and what his thoughts are on the war and so on To get access to somebody like that is really, really quite something
The possibilities provided by modern research amaze me too. What interested you in science communication?
I studied physics at university quite a long time ago and I really enjoyed it. I enjoyed science, I found it quite good fun I was never very good at practical experiments, so I tended to go down a bit more of the theoretical physics route While I was doing my degree, there was a course called Communication of Scientific Ideas which I thought sounded interesting As part of the course, you had to follow a researcher in a different department to yours, one where you were not an expert in you had to interview them, and you had to write a news story feature I got a botanist, but his particular area of focus was looking at how plants absorb nuclear isotopes, and this was in relation to what was done with nuclear waste, burying nuclear waste underground. I found it interesting trying to tease the story out and write about it When I went to interview him, I spotted a book in Russian on his shelf and just happened to ask him, 'Oh, do you speak Russian?' He told me this story about how he had gone to Chernobyl in the aftermath of the nuclear reactor meltdown there He was telling me all about how it was like a deserted village that had just been abandoned. It looked like an empty village I got a really, fascinating interview out of it and so that really excited me That was the point where I realised that I was quite interested in science communication Like many people, I began a PhD but not really knowing what I wanted to do, or why I wanted to do a PhD, or even really whether I wanted to do a PhD, it was the natural route. Three months in, I realised that this just was not for me You have to have a particular mindset to be a scientist, and I did not have that in me I was still passionate about science, but I was interested in the result, let somebody else do all the hard work and then come in and help them communicate their findings to the outside world. That was the route that I ended up going down I quit my PhD and after a short break, came back and went down the science communication route
and then come in and help them communicate their findings to the outside world That was the route that I ended up going down I quit my PhD and after a short break, came back and went down the science communication route
What do you think is the most important part of effective science communication?
I think an ability to take a step back outside of science and look at it from an external perspective You will often find when you are talking to researchers that they are very focused on their particular piece of research but sometimes they can miss the bigger picture Often, it takes somebody as an outsider to come in and ask stupid questions that are sometimes more challenging than the questions from their peers because they have not necessarily thought about that. I think an ability to ask and not to be afraid to ask what may seem like stupid questions is crucial because often these can get the best answers out of your researchers.
Do you think social media networks pose a new beginning for science communication?
I'm not sure I would describe it as a new beginning, they are just new tools that science communicators can use. They give more opportunities to people to communicate their research, whereas 20 years ago, researchers would rely on their press offices or their communications offices to get their research out. Now they have opportunities to get it out to a wider audience directly through social media channels I was at a workshop yesterday where somebody said that these days, a lot of early career researchers are being encouraged to have social media profiles and to build their own profiles on Twitter and other social media outlets Of course, there are challenges to using social media, in part because the platforms can change so much It used to be all about Facebook then it was about Twitter, and we are increasingly finding that Twitter is not as effective as it used to be for getting our stories out LinkedIn has come to prominence for us, as a university, for getting our research stories out where we tend to get more engagement
Essentially, if you are a researcher, it probably would do you good to have a social media profile but do be careful not to allow it to become too distracting, which is obviously one of the challenges of social media Do look at what other people are doing on social media, how they are using it, and see if there are ways that other people are using it particularly well that you could model yourself on
One other thing to do is think about which is the most appropriate platform for the people that you are trying to reach and consider what the best style is for that. For example, if you are trying to reach other researchers, often Twitter is the best way for that. If you are trying to communicate to the public, well actually you might find that it is TikTok. If you are trying to appeal to a young, particularly young demographic, then definitely get on to TikTok
One of the questions I had related to my own observations – public awareness. A lot of the public does not have much awareness about the research that takes place. With the use of social media apps becoming more widespread and becoming more significant in people's lives, have you found that social media has had an impact on general awareness of current research?
I am not sure to what extent social media has influenced that There are things that externally influence how engaged people are with research For example, during the COVID pandemic, it was interesting going into that very few people knew anything about immunology or epidemiology, and, six months into it, you would be having a conversation in a pub with a friend about Rnumbers There are things that influence how engaged people get with research One of the challenges with social media is misinformation and social media has made it so much easier for misinformation to spread We saw that with COVID misinformation or disinformation about the vaccines, for example One thing people need to be aware of when they are using social media as a consumer is, is the source of this reliable Where is this information coming from?
There is a lot of research that takes place within Cambridge, especially within the scientific community. Does the fast pace of research sometimes pose a significant challenge? If so, are there procedures put in place to keep work efficient and effective?
We are well-resourced in our research communications team at the university, but even so, you can imagine that across the university there are several thousands of people doing research It is impossible to keep abreast of everything that is taking place there Having said that, a lot of research is incremental. We would not necessarily be writing about every single research paper that is coming out We have to pick the stories that we think will appeal to a wide audience and there are various criteria that we use to select those stories, but we end up only covering an exceedingly small fraction of the research that goes on at the university Part of the work of our team is awareness raising around the university, showing what we can do to support them and how we can help them communicate their research to a wider audience Most researchers are very receptive to our help, but it is not necessarily something that they are always thinking about Most researchers tend to be very focused on their research, not necessarily on how they communicate it to a wider world. We must get active and convince them that they should be doing this and show them how we can support them
Do you have any advice for students who may be considering a career in science communication?
I'd say go ahead and try it. If you want to pursue a career in science communication, it is becoming increasingly competitive to get a job in it From a recruiter's perspective, what you are looking for in applicants is somebody who demonstrates that they have a passion for science communication It is all very well for people simply saying, “I'm passionate about science communication!” but if you have done nothing to show this then it is less likely that we will take a punt on you If you are based at a university, then look for opportunities to write about the research that goes on there, even if it is just writing pieces for your departmental website, or speak to your university communication office, to see if there are any opportunities to help them or to volunteer for a week or so. Likewise, there are public engagement opportunities that you can get involved in For example, at the University of Cambridge, we have a Cambridge Festival every year which involves public talks, workshops, and hands-on activities
"THROW YOURSELF INTO THESE AND GET INVOLVED."
Get involved in evening talks in the pub, for example, anything that just demonstrates that you really do want to do this
Just jumping back to your earlier question about social media Social media gives you more opportunities as somebody who wants to get into science communication to have a chance at it Try your hand at doing a TikTok video or series of TikTok videos that explain some of the science in your area.
That reminds me of a lot of students within the last week, I have spoken to who say that they have YouTube channels to explain scientific concepts. Sounds like that is a great method of science communication as well.
Absolutely As I said, if you then come to apply for a job in science communication, you have got something in your portfolio that you can show
Thank you so much. Craig. Those are all my questions. That was useful because we have identified that a lot of people know about research, but not a lot of students know that they can go down the science communication route. One of the aims of Bioscientist magazine is to inform students about a variety of career pathways. Right now, anyone doing Biomedical Sciences thinks that they can only become a Biomedical Scientist, and anyone who does what I do, Human Biology and Infectious Diseases, believes that they can only go on to do a master's degree and go on to do a Ph.D. There are many career prospects available for students studying biomedicine courses, one of them being science communication. This is going to be inspirational for a lot of students.
CAREER INSIGHTS
Bridging The Gap: How Is the IBMS Preparing Our Future Biomedical Scientists?
SUE JONES IN CONVERSATION WITH
SARA ALNASIR KASSAM
Sara Alnasir Kassam sat down in conversation with Dr Sue Jones, Executive Head of Education at the Institute of Biomedical Science (IBMS) Dr Jones joined the IBMS in June 2022 and recently celebrated her first anniversary at the Institute Sara and Dr Jones discuss how the IBMS is working to help students jump from life as a student to life as a Biomedical Scientist in the working world.
Can you shine a light on what the IBMS is doing to help nurture students studying Biomedical Science?
We're doing a few different things. As far as students at universities are concerned, we accredit specific degree programmes The IBMS has a role in making sure the curriculum is current and up to date. We're looking at what we teach students at universities to ensure that the understanding that they gain is fit for purpose We also work hard to support students in their transition into employability to ensure our graduates can get a job Completing an IBMS-accredited degree does not mean that you must go to work in practice; there are lots of other careers for graduates to explore but we look to bridge the gap in employability skills and work readiness for students on our accredited courses to pursue whatever career they want to
How does the IBMS monitor IBMS-accredited Biomedical Science programmes to ensure they meet expectations and follow standards?
Every five years, we ask universities to share documentation We check if the content being delivered is mapped to the QAA subject benchmark statement We also examine how the students are taught and whether practitioners (biomedical scientists) actively contribute to educating them To summarise, the accreditation and re-accreditation process looks to ensure the degree programme delivered has good assessment strategies and if the programme is organised to support students well by scaffolding their learning and skill development.
How advantageous is your educational background for fulfilling your role and ensuring students obtain as much as possible from accredited Biomedical Science degree programmes?
I always look at student feedback When we look at the programme's quality, we look at employees' and students' points of view and take them into account I'm looking at the course, how it has been developed, and how it is running Universities and academic teams complete an annual report for the IBMS, and they tell us if they made any changes and what those changes are A vital piece of our monitoring is around student feedback, we always ask programmes about student feedback and analyse this in detail
How would you describe the transition from university to the workplace? How do you aim to make the transition smoother?
The student's transition from university to the workplace can be a massive jump, it's hugely different For students, the main question is: How do you know how big that jump is unless you've been in a work environment? One of the things that I'd like to do is get as many students as possible to visit clinical laboratories During the COVID-19 Pandemic, many universities had to do online open days Universities had to film their teaching labs and make [the lab tour] into a video, that kind of thing I'd really like to do that for clinical pathology laboratories because getting all the students to visit is difficult I am working with the comms team at the IBMS to work out how we can organise virtual pathology laboratory tours for students. I will endeavour to make [the videos] an accessible resource The students may then use the videos to look at the different disciplines and decide what they like Post-COVID, some universities have been able to organise a trip to a local hospital, but it is not always easy to do; sometimes it works, sometimes it doesn't Having freely accessible video laboratory tours is just taking that barrier away It's thinking about everybody having that access and it being free We're also starting to do the monthly IBMS support hubs to help develop our students to be confident to make that jump. More details on all IBMS Support Hubs in 2023 can be found here
Why would you encourage more biomedicine students to attend these support hubs? How can we benefit from them?
We've now got a series that will go through to December Due to the IBMS Congress, we won't hold a support hub session in September. The support hub topics are planned to help bridge that gap between the university and the workplace We picked a theme for each support hub that we think will be useful. They only take an hour of your time. Each support hub session is held on Wednesdays at lunchtime We did this purposefully because we hope most students will be free to allow as many as possible to attend and use the support provided. We also picked this time to allow people in practice to access the sessions, which should coincide with their lunch hour What is fantastic about the support hub sessions is that if you look at the topics we cover, we're trying to time them with when they might be helpful for people, such as placement interviews in May, for example I highly recommend that students attend these sessions in large numbers or access the videos from the IBMS web pages to watch anytime
What are your aims for introducing the HCPC SoPs so early on? And what are your aims for students to get from it?
The HCPC has two sets of standards: the standards of education and training and the standards of proficiency These are the 2 bits of the jigsaw puzzle that you need to meet to be able to register with the HCPC to practice as a biomedical scientist This is where the IBMS comes in; we look at the curriculum you're taught at university and ensure that it contains the appropriate content in the right depth and breadth We use the HCPC Standards of Education and Training to inform what we ask of universities regarding the programme they deliver You might have heard about the HCPC Standards of Proficiency when you've had laboratory sessions, when discussing your critical skills, or in preparation for a clinical placement The objective of the clinical placement is to allow you to complete the IBMS registration training portfolio Completing this portfolio demonstrates that you have met the HCPC Standards of Proficiency By integrating some of the HCPC SoPs into your programme delivery, you are familiar with some of those standards already within your degree, so they don't seem foreign when you are on placement.
What is the difference between the IBMS and HCPC?
The IBMS and the HCPC, work together, but we're not the same We're slightly different organisations and do different things; the HCPC is a regulator and has a duty to protect patients and ensure everyone is trained appropriately The IBMS accredits degree programmes, provides the IBMS registration training portfolio, provides laboratory
training approval, and organise the assessment of the portfolio to sign people off to say they've successfully met the standards of proficiency This will allow them to register with the HCPC after they successfully complete the portfolio and their IBMS-accredited degree programme
How are you preparing those students who are slightly younger to enter the Biomedical Science field?
The short answer is that we don't do enough of it now I want to get involved with careers advisors and have done so by writing a blog for UCAS that goes to teachers and careers advisors, but I realise that it's something we need to do earlier For primary schools, we have a comic book called 'Superlabs' that is tailored for primary school-age children; getting them involved in science is excellent One of the things I did when I worked at a university was set up a science club and partnered with the local primary school; they loved it Primary school children loved science experiments; it's cool, it's brilliant We do have some resources online and on the IBMS web page, which are to support people to be able to go into schools and do practicals, talk about biomedical science, and all those kinds of things but we don't have many resources, and we're relying on people having the time and ability to go to raise awareness We've got influential ambassadors in our students who could be our IBMS ambassadors and go out and talk to pupils at primary and secondary schools If you were to go to your school and say, I came here five years ago, and this is what I'm doing now That's much more powerful than me turning up and saying, this degree/field is quite a good thing Student IBMS ambassadors could be genuinely a widespread and effective initiative
The IBMS established Biomedical Science Day, which is a fantastic notion, but I feel like sometimes Biomedical Science Day, it being a day, it's just not enough. You said that having student IBMS ambassadors would be a good idea. How can these ambassadors make every day a Biomedical Science Day?
We are missing a trick by not showing people enough about Biomedical Science I agree with you that having a day to celebrate and drawing attention to it, is good, but we can't have one day in 365 to raise our profile We're looking at our online presence and being able to do more. I think there's something in us providing resources to give to people for them to take and use to promote biomedical science Once we've got resources, it makes it so much easier for people to have those conversations or think about what to say when they go
We often wait for people to come to us, for example, we might have these conversations during a university open day, and that's great At the IBMS, we could do more to go out and spread our message and awareness Sometimes, if you ask, "What is a Biomedical Scientist?" – people don't know, but we've got little videos on our YouTube channel, that help get the message across A few examples can be found here:
What is Biomedical Science? What happens to your sample? The Biographies of Biomedical ScientistsFrom the IBMS Website
We have the IBMS Congress coming up in September. I'm looking forward to it because you have a Student Session tailored for Biomedical Science students. Thus, can you delve into why the IBMS Congress is super important?
IBMS Congress aims to raise awareness; it's about people knowing what is out there At Congress, we aim to have a suitable range of things for people Congress also helps unlock people's understanding of some of the terminology; I think sometimes we forget that not everybody understands all the words we say For example, what is the difference between the IBMS and HCPC? What is STP? What can you go on to after your degree? What's it like being a biomedical scientist? I'm thinking of getting graduates who graduated a while ago to come along and talk about where they are now, which helps inspire students. Again, it's much easier for you to talk to somebody like you afterward; IBMS Congress is a fantastic place for that networking to take place
It is incredible that the IBMS works hard to ensure students feel confident when they graduate. Can you shed light on how you endeavour to build this confidence in us?
It's preparing students to take on challenges and making it less scary because during your degree you know exactly what you are doing day to day as it is all planned. When you finish your degree, you can think I have known exactly what I was doing for three years, and I've got to the end of that, now what? The less scary the point of graduation is, the better. It is really important to build confidence and knowledge about available options for careers and take the next steps You don't need to have a defined route It's reassuring for students that you don't need to have every element of your life planned out It will sort itself out; it will be OK I think that's quite an important message for students
Would you like to share any final thoughts, Doctor Jones? What has been your new beginning?
My new beginning was when I started at the IBMS in June last year I think it's helpful for me to reflect on the IBMS where it is now; it is in a good place and already does a lot of good stuff, but we need to move with the times and be more relevant and relatable That's what I see my role being We could modernise what we do and be more interaction friendly The new beginning, as far as learning and teaching are concerned and education and training for the IBMS is about updating and improving what we've got It's about moving forward and making ourselves as relevant as possible to people like the student members, the newly graduated members and the licentiate members
pg.45 pg.45
ADDRESS BY PROGRAMME ADDRESS BY PROGRAMME LEADS LEADS
Dr Sara Namvar reflects on the year so far and offers key advice for our incoming students
pg.46 pg.46
COFFEE WITH CAROLINE
Biomedical Academic answering your wellbeing queries and concerns
pg.49 pg.49
WELLBEING AND MENTAL HEALTH WELLBEING AND MENTAL HEALTH
Wellbeing advice from your 2023 Biomedicine course reps on how to best prepare for academic year
pg.50 pg.50
MY JOURNEY TO SALFORD MY JOURNEY TO SALFORD
Microbiology Society Award winner and Salford alumni discuss their time at the University of Salford
pg.53 pg.53
BIOMEDICINE SOCIETY BIOMEDICINE SOCIETY
Biomedicine Society students talk about Kidscan collaboration, PassionFlash and BioArt competitions
ADDRESS BY BIOMEDICINE PROGRAMME LEAD
DR SARA NAMVAR
PROGRAMME LEAD FOR BIOMEDICAL SCIENCE AND DIRECTORATE LEAD FOR STUDENT EXPERIENCE
I would like to begin by welcoming all students to the university For those of you who are brand new to the institution, you have chosen well, as the University of Salford offers so much more than just a degree! You have a beautiful campus with excellent social spaces, a vibrant and welcoming students union, a fantastic academic team and a phenomenal student society. Welcome back to all those returning to campus, we are looking forward to what the next year has in store. This is hopefully our collective return to ‘normal’!!! Whilst we will retain some of the flexible ways of working, I think it’s safe to say we have all missed the human element, the real on campus buzz and the richness that comes with university life So, I take the opportunity to encourage you to be present! Make every moment count, whether it’s a lecture, tutorial, an extracurricular event or a chance to socialise These are the best years of your life, and you are financially invested in your programme of study – so lets nurture this investment together
Looking to the academic year, I want to take the opportunity to remind you of the importance of your personal goals and getting the most out of university. As returning students you will already be aware, but for those of you who are new, please look out for opportunities via the programme site, email, society communication and students’ union The opportunities, activities and events we offer as a subject area are designed to boost your employability – you will usually see these tagged with #BeeGradReady So, whether its joining (and engaging with) one of the careers working groups, the student society, attending the careers festival, taking part in outreach opportunities, Salford PassionFlash, art exhibitions, book clubs and much more…know that these things will absolutely make the difference to your experience and ultimately job prospects You will hear lots more about these opportunities during induction week I’d like to take the opportunity to welcome you once more and wish you every success in the coming academic year
COFFEE WITH CAROLINE
How can I effectively balance my time and prioritise tasks while facing personal challenges?
I am the kind of person who likes working to deadlines, so I need a deadline to motivate me. I often structure my week around things that must happen this week but also look ahead to the future and make sure that I am planning enough time to complete upcoming tasks
I use my Outlook Calendar, not just to show when I have meetings or taught sessions but also to block out sections of time to work on specific tasks My days will have a set of blocked-out wedges of time, for instance, ‘I'm going to spend an hour on preparing a lecture,’ or ‘I'm going to spend 2 hours on preparing a piece of writing for something’, and I try and stick to it as much as I can Sometimes things happen that throw your
It must be as good as it can be in an hour, and then I must move on to the next thing ’ Working like that takes practice because often we like getting things done perfectly and when you are busy, you cannot do that, it just needs to be good enough. Sticking to setting times for working on things and not agonizing over things being perfect is the way that I handle the workload, but we are all different so find what works for you.
How can I deal with conflicts and disagreements with people in group projects?
It helps to know that everyone responds differently. Some people want to jump straight in and get their point of view across and fight for their opinion, other people will withdraw and find conflict difficult and seem not engaged in it at all. An effective way to manage this is to find a way for each person to contribute to the discussion on how to resolve it, including those who just want to avoid conflict Everyone has their own way of coping and there is no right or wrong way of doing that The key is, to find a way for everyone to feel like they have had their say
My next piece of advice would be to let a bit of time pass for the emotions to cool down before you propose a plan of action When people get into an agitated and stressed state, it is difficult for people to take feedback It can be difficult for people to think logically when they are feeling very emotional so try finding a way for everybody to have their say in a way that is not going to fuel the conflict more Try talking to people individually and then leaving a bit of time for people to cool off before proposing a plan of action
It is challenging, but a valuable experience because that is how it can be in the workplace I would be curious about why that person is not contributing; it might be that there is something going on in their life that you are not aware of and that they do not feel comfortable sharing My first question would be, ‘Are you OK? Is something going on because I notice you are not completing the tasks you agreed to and wonder if you need support?’ By taking a compassionate view to start with, hopefully, they would respond well If not, then it comes down to the fact that this person is not contributing We need the work to be done as a group From the individual's perspective, you want a good mark for this piece of work so it can be frustrating, and you may need to take more control and responsibility for the work than you originally wanted to. There is usually a reason someone is not doing what they say they are doing, so trying to find the underlying cause of that might be a productive way to move forward as a group.
What advice do you have for someone struggling to decide between careers?
It is an exciting position that you find yourself in when you graduate from university with so many options ahead of you, but it can be daunting as well How to know what to choose? Some have a very clear goal in mind, for others it comes down to trial and error If you have the chance to try, through work experience or placements, try a particular role. If that is not possible, try to speak to people that work in those jobs and find out what their day looks like, how they spend their time. Does it sound like something you would enjoy? Use career websites like Prospects.com and do your research to find out what that role entails.
There will be some obvious things that stand out, e g , if you are a people person, going into a very solitary laboratory-based position might not be for you You might want to do something a bit more person-facing, like being a Physician Associate Think about what you enjoy about the university, do you love being in the lab? Where do you get pleasure from your studies? It is normal to go through those periods where you are just like ‘I'm sick of this, I want it to be over, ’ especially with years of long training and decades of studying It is about finding joy in the process What are the little things that make your days happier and worthwhile?
It's a particular subject that you like studying, that you can immerse yourself in, or maybe it's the people that you meet at university that you go to the library with and do assignments with? Think of a bigger picture goal but you also need to give yourself other motivations as well like little rewards along the way I really love going on holiday, who doesn't? Try setting these reward goals e g I must get through this month and then have a weekend away or a meal with my best friend Find ways to motivate yourself daily so you can get through this lengthy period of work that will get you to a bigger goal.
Do you have any advice for securing research placements?
The trick with successful applications is to be able to make a statement about your strengths, but also support it with some kind of evidence. If I were to say, ‘I am an excellent communicator,’ the kind of thing that people like to say on CVs, someone could read it and think ‘OK, but how do I know that?’ Or I could say ‘I am an excellent communicator; I have been invited to speak at XY and Z external conferences and received positive feedback from the audience ’ In the second example, I have given some evidence to support my claim that I am an excellent communicator
You can also demonstrate my skills in the way that I present my documents, get my grammar and punctuation right, lay out my application and CV nicely, and use good sentence formation
This is another way that I am evidencing that I am a good written communicator You might not necessarily have professional experience, but you might have experience in other areas of your life That is why we have so many opportunities for extracurricular activities here as well, because if you want to talk about your excellent communication skills, you could then talk about the PassionFlash competition, or when you volunteered to lead a group delivering an oral presentation. It is about thinking about how you can evidence what you are saying about your strengths and making it as applicable as possible to the role when it comes to research placements
Make sure you know about the research, the group, and the supervisor, if relevant If you make it clear that you have read some of their research, this can make you a more attractive candidate because you have taken the time to understand what it is they are doing and what you are passionate about. Sometimes as academics, we get emails such as 'I’m interested in cancer research; do you have any space in your lab?’ It does not stand out If somebody were to send an email and say ‘I am really interested in Cancer Research I have read your work on medulloblastoma and how certain types of treatments might enhance outcomes for patients and help reduce harmful side effects I would love to work on this kind of project. Do you have any capacity for a student?’, it's a really different experience to receive that kind of email.
How can I deal with impostor syndrome?
Impostor syndrome is a common human experience People often will go through it at some point in their lives, and often that happens when they are under pressure What has helped me in the past is sharing those feelings with people around me. ‘You're not good enough, you should know how to do this all by yourself’. These kinds of toxic messages that we tell ourselves can become a lot quieter when we share them I would start with somebody that I trust and care about and just tell them What you will get back is different from the feedback you are giving yourself
The more people that you can have the courage to share what you are experiencing with, the more likely you are to get positive feedback because the reality is you would not be at university if you were not capable of being at university Those facts can sometimes escape us when we are in that stressed state and we are feeling inadequate The act of sharing your fears can shrink them because you get someone else's perspective instead of just your own, which is distorted and overly negative because often that is sadly how we talk to ourselves. How great would it feel to have your personal tutor say, ‘Of course you could do this, look at the marks you got last year, the contributions that you have made, the things that you ’ ve learned ’ We are all good at different things and cannot be excellent at everything It is tempting to give yourself a hard time with the things that you are not as good at It can be helpful to accept that not everybody is brilliant at everything. That is a much more peaceful place to work towards than constantly feeling like you are less than the people around you I did feel that kind of imposter syndrome and that fear that I was not good enough and I was not clever enough earlier in my life I tried to do everything on my own, but I enjoy learning as part of a team and a group I now know after years of experience, that I would have felt more comfortable studying with other people, discussing aspects that I did not understand with them. I would have a lot more out of the experience, but I was so worried about being seen as not good enough that it stopped me from having those conversations and those types of relationships Now as I am older and wiser, I can accept that there are just some things that I am not so good at and there are other things that I am great at Comparing yourself to other people is tempting, but it is rarely a beneficial thing to do because we are all so different
WELLBEING ADVICE
FROM BIOMEDICINE COURSE REPS 2022/23
Even while enjoying everything our university offers, it is easy to get caught up in the whirlwind of academic pressure Amidst the chaos of student lives, there is invaluable support and guidance from someone who walks in the same shoes: our course representatives. They are the bridge between the students and staff members, ensuring our academic journey goes as smoothly as possible. Now they are here to share their tips and strategies on how to make the most of your university experience while nurturing your physical, emotional, and mental health.
Arooj Afzal
Level 5 Biomedicine Course Rep
“As a student myself, I understand the importance of prioritising mental and emotional well-being throughout our academic journey but also how hard it can be During exams, it is natural to feel overwhelmed, but remember, you are not alone Reach out to friends, family, or university resources for support. Taking care of ourselves is crucial; let’s remember to find moments for self-care amidst the busyness Whether it is going for a walk, enjoying your favourite meal, or getting a good night's sleep ”
Tasfia Hazari
Level 4 Biomedicine Course Rep
“I understand how stressful the transition from college to university life can be especially since I recently ended my first year of university. It can be very difficult navigating through lectures and trying to make your notes for revision Although very overwhelming you must try to take care of your physical and mental health;
Try focusing on perfecting your revision techniques so when you are closer to exams you have the perfect tools that work for you.
Avoid staying up later than necessary, aim for at least 8 hours of sleep each night, and keep up a balanced diet
Try to socialise and establish new friends despite the full academic schedules You will soon find that your peers can be quite helpful in preserving your mental health and just making your university life a little more tolerable
Your course representatives and wellbeing officers are available to you at any time and always willing to chat with you to take your mind off the stress factors of university as well as personal life."
WINNING THE MICROBIOLOGY SOCIETY
AWARD - MY JOURNEY TO SUCCESS
BY ASHLEIGH HOWARD
I am a final year Microbiology student at Salford, and I chose to do this course as microbiology has always been a huge interest to me I am employed as a Research Assistant at the Liverpool School of Tropical Medicine in the Liverpool Vaccine Group In this position, I am responsible for processing human samples from our Experimental Human Challenge models with a particular focus on pneumococcal disease I obtained the role without a degree due to my previous experience in laboratories and my desire to work in the field I always felt like an underdog not having a degree but working in an academic environment.
If I have any advice that might help someone, it would be not to hold yourself back! Even if others think they know what you are capable of, they will almost certainly be wrong, because only you know what you can do! Don’t be afraid to speak up or ask for help that is the best way to learn and develop Engage with people who interest you and never stop progressing yourself It can be surprising what you can achieve in a small amount of time if you are willing to focus and put effort into it.
Pictured: Ashleigh Howard holding her Microbiology Society Award with Prof Richard Birtles
I felt that people may be judging me I was always thinking and exploring the option of obtaining a degree, but it would mean giving up my job and changing my lifestyle, something I was not willing to do. When COVID struck, I saw an opportunity to finally do a degree, as everything was being taught online and I just thought now is the time and if you do not do it now, you never will!
I spoke to my manager and expressed my interest, and she gave me the green light as she wanted to support me knowing I would be a better scientist for her team and on a more personal level, I could fill skills gaps When Salford accepted my application, I was so excited but apprehensive as I would be going in as a mature student who has been out of the game for many years. My previous learning was very different from my current teaching methods, so I thought I was going to struggle I was right, degrees are hard and demanding! Much more than I thought but it is still the best thing I have done I have put 100% of my effort into this as I want to achieve the highest possible mark, network, and develop myself as a person
Three years on, I now look back at everything I have achieved Since my degree began, I have had a promotion and become a senior scientist. I attended a conference to present my research to others in the field. I have led presentations, been part of public engagement events and in Uni I won the Microbiology Society award! All of this would not have been possible without attending university I have gained a great deal of confidence by engaging in lectures and asking for help and advice. The conference I attended for work was made easier as we did posters for the microbial communities and interactions module, this is proof that what we are taught really can help us in the future I have applied a lot of the knowledge I have gained from the course to my role, and it has inspired me to continue exploring my career in academia. I now believe in myself that anything is possible if you put your mind to it
BY ABBIE STORAN
I dropped out of university after two months in 2017 because I was struggling with my mental health Now I have graduated and am a proud Salford alum.
As an autistic person, I struggled throughout school. I wasn’t diagnosed until 16, so was never given the appropriate support However, even after my diagnosis, I was left to figure things out for myself, because support for teenagers with autism is lacking
I had a love/hate relationship with school and college. On the one hand, learning is something I genuinely enjoy, particularly English Literature and Science. On the other hand, having autism means I find everything to do with social communication completely alien, and it takes longer for me to process and make sense of information I have a limit for how much I can take in before becoming overwhelmed and unable to do anything at all. So that made school and college quite difficult.
Autism is a neurological condition, but in other ways a physical one too. I spent months out of school and college, doing my learning from home because I was so physically and mentally unwell by just the thought of going in
My literature tutors at college really encouraged me to study English at university, while my medical science tutor told me I would do well in a science degree My family also believed I was going to pursue literature because it was the subject, I'd always been most praised in since primary school.
I chose to study Literature and Creative Writing at Salfordeven though I did my best I was never happy during that time. I realised I didn’t really like the subject at this level, and I was hardly attending because of the toll it was taking on my mental health, so I knew I didn’t want to continue the degree
Officially leaving took a while; there are hundreds of guides on how to get into university, but none on how to get out It took a year and a half for me to work on my mental health and on living with Autism. During that time, I began thinking about where I wanted to be in the future – what could I see myself doing happily and confidently? The answer was Biology
I then applied originally to Biomedicine in late 2018 but changed my mind after attending the applicant visit day We had a lecture from the Biosciences Department outlining the different courses, and I remember David Greensmith talking about Human Biology and Infectious Diseases – a course I hadn’t even heard of until that day – and immediately knew it was more suited to me. I didn’t even know what I wanted after my degree, just that those specific modules would interest me most
I was right In my final year, I did an internship with a Mast Cell charity I had the support that I require as a disabled student, and I know what I want to do after university. But more importantly, I'm so much happier now.
DISABILITY AND INCLUSION
The University of Salford actively promotes inclusivity and diversity The University believes in ensuring those with disabilities can reach their potential. Some links to the disability support services and information can be found via AskUS.
For information on support offered by the university, visit:
Disability Inclusion Service
Reasonable Adjustment Plans
AskUS
You can also get in touch with AskUS via: Email - disability@salford ac uk Phone - 0161 295 0023 (option 1 then option 2)
BY SARA ALNASIR KASSAM, SECRETARY FOR 2022/23
The Salford Biomedicine Society was established in 2017 by former Salford Biomedicine Students The Society was now in its 5th year, and dare I say it, its most successful year yet. My name is Sara Alnasir Kassam, and I was the Secretary of the Society for the year 2022-2023. Let’s journey together through this past year and celebrate the achievements we will remember for many years
The newly elected committee started their term early in June 2022, with Biomedical Science Day Working closely with Tahmina Hussain, the Committee volunteered on this day, raising awareness of the Biomedical Scientist profession being #attheheartofhealthcare 24 hours, seven days a week. A few weeks later, the Society was introduced to prospective students via our Biomedicine Summer School, where a Q&A session was held to further inform our future Salford students of the support and fun we offer
We swiftly moved on to Freshers’ Week to get as many members as possible from the Biomedicine cohort and the other faculties at the University of Salford We had a massive presence at the Freshers Fair and during the induction activities for our newly joined Biomedicine students Our vast presence was further intensified via our Freshers’ promo video, informing everyone about the perks of joining the society featuring our new Committee We were also featured in the IBMS Student e-Newsletter
The Super Bees, the Main Bees and the Support Bees worked collectively to deliver our Sports, BioArt, and Book Club sessions and the newly founded Employability Support Sessions The Employability Support Initiative included a placement preparation series and the “Back 2 Basics: Student Edition” series Both series proved popular and were delivered online on MS Teams Our events managers also worked hard to set up social events, including a Bowling Social and a winter-themed Ice Skating Social. Something new for this year was the Sports Collaboration with the other sport-themed societies at the University We also had a Kidscan Support Bee, who focused on collaborations between the Society and Kidscan
We supported the IBMS Manchester branch’s “Equity, Diversity and Inclusion” event in January 2023. Our committee represented the society and built connections with key professionals. January 2023 was the month we received a shoutout from the SU via their Society Spotlight initiative
Considering our aim of making our members more employable, the society worked hard to deliver the student-led day of the Human and Natural Sciences (HANS) Careers Fest 2023 We provided live Employability Support Sessions on interview prep and CV writing, and for the first time, included interview simulations We also organised upskilling sessions with the academics
The two most significant events of the year – The Bioart Competition and Salford Passionflash – were indeed the highlights for the society as a whole A lot of preparation went into making these events unique Our participants, winners and audiences loved the little personalised touches, making the events ones that have never been experienced at Salford before.
We ended the year with 150+ members (making the society the biggest at the University) and two SU awards nominations (Most Improved Society and Academic Society of the Year) These milestones genuinely reflect the work the committee put in throughout the year Being involved in the society has been a matter of pride. Here’s wishing the new Committee the best of luck for the year ahead. I can't wait to see what is in store for the Salford Biomedicine Society.
Go Team Biomed!
Pictured: The Salford Biomedicine Committee 20222023's Super Bees: Alia Boda (President), Zohaib Altaf (Treasurer), Sara Alnasir Kassam (Secretary) and Saira Iqbal (Wellbeing Officer).
Picture was taken during Passionflash in March 2023.
Since the beginning of November 2022, I have been representing the Biomedicine Society as the Kidscan Support Bee In this role, I work and communicate with Kidscan, as well as assist in creating volunteering opportunities These outreach programs help raise awareness of paediatric cancer for the public Cancer is the leading cause of death in children and advances in research and treatments have not always been as successful when compared to adults Studies have shown that research on child cancer corresponds to only 5% of general cancer research⁴ Therefore, Kidscan, as a children’s cancer charity institution, aims to support the development of new therapeutic approaches for treating childhood cancer and relieving the long-term side effects of these treatments¹
An exceedingly small number of novel chemotherapy drugs have been developed As evidenced by the U S Food and Drug Administration (FDA) only 6 out of 126 chemotherapy drugs were approved for paediatric oncology patients during 20 years Furthermore, a 3-year European study showed that over half of medications considered to be fundamental for paedriatic oncology were granted class waivers² The reason is that funding for these treatments is very restricted, especially in rare types of childhood cancer Consequently, it is important to highlight how fundamental it is to develop novel approaches to these treatments as these tend to be “aggressive” with side effects to treatments lasting a lifetime To allow a phased movement to fewer toxic treatments, advances in immunotherapy and gene editing could be a new beginning
The gene editing technique of CRISPR/Cas9 has shown promising results for immunotherapy in clinical trials for cancer patients CAR- T-cells from the patient’s immune system are taken and altered by CRISPR/Cas9 in vitro and then reintroduced to the patient’s body to challenge cancerous cells Clinical trials at the University of Pennsylvania were the first to enable the cure of a paediatric patient (Emily Whitehead) from acute lymphocytic leukaemia using a CAR T-cell therapy called tisagenlecleucel (Kymriah)⁵ Another study has demonstrated how axicabtagene ciloleucel CAR T-cell therapy has been successful in the treatment of B-cell lymphoma³ . Statistics show that in 82% of patients with cancer immunotherapy decelerated or prevented the growth of cancerous cells Interestingly, slightly over half of the patients showed no signs of cancer after the treatment and a year after the study³⁵
Sometimes we may think: How can we help in assisting these treatments? Is it possible? The answer is yes Fundraising is a splendid example! In December 2022 and April 2023, Kidscan had a lot of volunteering opportunities for us at the University of Salford As the Kidscan support bee I was responsible for gathering volunteers willing to support money collections in Manchester City Centre As well as being a fantastic means to contribute to the lives of those impacted by Cancer, this was a great CV-enhancing opportunity for the volunteers. Volunteering allows the development of communication skills, teamwork and relationship building, confidence (by gathering people to donate), time management, and even empathy, by relating to others and creating strong bonds of compassion Fundamental for scientists to better comprehend how their work impacts and influences others
Moreover, our collaboration with Kidscan helped to give the charity more integrity and recognition in the wider community This ultimately supports research into childhood cancer, which is extremely rewarding. I strongly encourage students to participate in future volunteering opportunities I truly look forward to seeing more of you engaging and supporting this vital cause
References: Kidscan (n d ) Our Research: Kidscan Children’s Cancer Research. Retrieved 05/08/2023 from https://kidscan org uk/our-research/
2
1 Laetsch, T W , DuBois, S G , Bender, J G , Macy, M E , & Moreno, L (2021) Opportunities and Challenges in Drug Development for Pediatric Cancers. Cancer Discov, 11(3), 545-559 https://doi org/10 1158/2159-8290 Cd-20-0779
3
Neelapu, S S , Locke, F L , Bartlett, N L , Lekakis, L J , Miklos, D B , Jacobson, C A , Braunschweig, I , Oluwole, O. O., Siddiqi, T., Lin, Y., Timmerman, J. M., Stiff, P. J., Friedberg J W Flinn I W Goy A Hill B T Smith M R , Deol, A , Farooq, U , Go, W Y (2017) Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma. The New England journal of medicine, 377(26) 2531-2544 https://doi org/10 1056/NEJMoa1707447
5
Syrimi, E , Lewison, G , Sullivan, R , & Kearns, P (2020) Analysis of Global Pediatric Cancer Research and Publications JCO global oncology 6(6) 9-18 https://doi org/10 1200/JGO 19 00227
4 Zhao, L , & Cao, Y J (2019) Engineered T Cell Therapy for Cancer in the Clinic. Frontiers in Immunology, 10, 2250-2250 https://doi org/10 3389/fimmu 2019 02250
From a small passion to a 1st place winner! From a small passion to a 1st place winner!
As I missed most of the opportunities last year, I have made my decision to make them up this year, and that is what I did I was patiently anticipating the announcement of the TedTalk PassionFlash and participating in this great competition to reveal for the first time in front of people my passion for the piano by playing a small piece of Titanic theme right at the start of 'my presentation; I named my topic ''The Keys to The Brain''.
My passion to learn playing on piano started a long time ago but I did not have the chance to start it until 6 months ago though I was successfully able to learn by myself by YouTube only! Because I love the melodic sounds that come with it, I feel as though it is a language I can express through my fingertips which the touch of the little piano keys, like neurones in the brain making new connections and pathways just by continuous repetition and learning that new skill which is absolutely magical and fascinating to know what is going on behind the scenes just by sitting on that chair and starting to play with full emotions and passion!
I have only won this competition because my aim was to show the real meaning of having a passion infused with my current scientific education in an entertaining way! I was the winner because of the support that I received from the organisers, module leaders, and my lectures, or in other words “My second family” that embraced my talent and my passion warmly, as well as the audience that voted for me and engaged with my presentation I want to thank every single one of them for believing in me and my musical scientific passion I do strongly recommend and encourage everyone to get involved and share their passion, it is a chance to prove who you truly are to other people and explore your hidden talents that you will be immensely proud of and impressed by your newly unlocked skills and abilities. I have gained a lot of confidence just from an 8minute presentation combining my piano with my science attraction in an entertaining and interesting way!
Yamen Toumeh
Pictured: Yamen Toumeh and the Participants of Salford Passionflash 2023
SALFORD BIOMEDICINE SOCIETY’S BIOART COMPETITION AND EXHIBITION 2023
BY TASFIA HAZARI, BIOART SUPPORT BEE
The 2023 BioArt competition was a tremendous success It was wonderful to witness the fantastic compositions created by our creative cohort The theme being ‘New Beginnings,’ many students submitted exquisite renditions, ranging from the Tree of Life to the beginning of human life and so much more It was quite difficult to determine the winners, but with the aid of our voters’ engagement, three stunning artworks were chosen
The second runner-up was Arooj Afzal with her composition representing the beginning of spring, where she beautifully captured the essence of spring and its symbolism of fresh starts and new beginnings The first runner-up was Danielle Rawlinson, with her composition of G O D and how on the third day G O D created Earth, truly a new beginning of time Finally, our winner was Mohna Akhter with her very touching interpretation of the theme where she portrays a young Syrian refugee hoping for a new beginning in life far away from the wars, conflict, and mass destruction
Along with the art pieces, we had a plethora of varied activities aligned with the main theme of the event. For instance, we set up a henna tattoo station where volunteers could take part in embracing and educating themselves about the Middle Eastern and Asian significance of new beginnings. We have also put in place crafting stations, especially for crocheting and beading, where our guests could learn to appreciate the simplicity of materials combined to create something beautiful. Our exhibition also offered graduation hat gift bags, plant potting, as well as many more creative activities for our guests to participate in and thoroughly enjoy
“The portrait I have drawn is inspired by a photograph of a young Syrian refugee. The forest in the background represents her home. The fire represents war and destruction. The seedling she is holding is a metaphor for a piece of home that she is protecting from the fire and taking with her on the journey to find refuge. It symbolises 'hope', for a new beginning.”
And on the 3rd Day, G.O.D Created Earth.
“An alternative take on the theory of creation but with a comedic twist! Two aliens designing Earth, prokaryotes, and the vital systems which life needs to grow and live. The two green men are shown working hard, perfecting their new planet down to the smallest atom. Hologram projectors are enabling them to zoom and spin their creations. The creations in question are cyanobacteria, which are known to be a green/blue algae, A double helix; to aid Earths life forms to mutate and evolve, a simple bacterium, an oxygen atom, and Earth itself. 'New beginnings' aren't just related to birth, new scientific research, or new life experiences, but from the beginning of the new planet 'Earth'.”
New Spring
“At the beginning of a new spring in a blossoming purple wisteria tree, the blue jay (Cyanocitta cristata) feeds its young hatchlings in its nest. From their cocoons, butterflies emerge to consume the nectar of the wisteria's cascading flowers.”
Iimaan Araleh Iimaan Araleh
Rebecca Jones Rebecca Jones
Tasfia Hazari Tasfia Hazari
Assia Iqbal Assia Iqbal
Nooria Shakeel Nooria Shakeel
Maryam Zahra Shaikh Maryam Zahra Shaikh
Joy Chukwudolue Joy Chukwudolue
Hannah Birmingham Hannah Birmingham
Alvina Imran Alvina Imran
Fathima Imran Fathima Imran
Jade Taylor Jade Taylor
Emma Holt Emma Holt Real Adam Real Adam
Aribah Mirza Aribah Mirza Amna Alawzi Amna Alawzi
Afifah Makda Afifah Makda
Dinesh Subramaynian Dinesh Subramaynian
Lara El-Farji Maymouni
Yann-Pierre Duncan Franc Yann-Pierre Franc
Hina Rehman Khalil
Hina Rehman Khalil
Haroon Sulimankhiel Haroon Sulimankhiel
EXPLORE THE WORLD OF BIOMEDICINE WITH US
EDITORS-IN-CHIEF / WIKTORIA WISNIEWSKA, SARA ALNASIR KASSAM
ACADEMIC SUPPORT / SARA NAMVAR
GRAPHIC DESIGN / ALIA BODA , HARRIET BURROW, SARA ALNASIR KASSAM, WIKTORIA WISNIEWSKA
COVER ART / DANIELLE RAWLINSON
bioscientistmagazine@salford ac uk Instagram | @salfordbiosoc X | @salfordbiosoc
issuu.com/bioscientistmagazine openjournals salford ac uk/bioscientist