
TRAINING MANUAL
INTRODUCTION TO REACH4LIFE
Reach4Life is a comprehensive, Christian life skills programme for young people – with a particular focus on identity, sexuality and relationships – that brings about holistic spiritual and behavioural transformation. It is based on the idea that comprehensive behavioural change is only possible once there is a spiritual revolution in the hearts and minds of young people. It was initially developed for teens between the ages of 12 and 18, however it has been found to be effective with pre-adolescents from as young as 10 (before the onset of sexual activity) right up to young adults in their early 20s who are still facing questions of who they are and how they can make wise life choices.
The core of the programme is the Reach4Life Bible that contains – in addition to the full text of the New Testament (using the New International Readers Version or NIrV) – lessons and stories that guide young people to faith in Christ, belief in themselves, and gives them the essential life skills and resilience to face the many challenges and temptations facing youth today.
There is a special focus on building a strong identity in Christ, helping young people address the central question: Who am I? The programme takes young people through 4 life journeys with 10 lessons in each, addressing issues like sex, relationships, emotional pain, drug and alcohol use and social media.
The programme is facilitated in a small group context and is taught by peer educators –mostly young people who have had to make some of the same difficult choices that teens face – recognising that lasting transformation only happens in relationships where authenticity and trust is present. Peer educators serve as role models and mentors where they have the opportunity to help youth at risk achieve their fullest potential.
To exist, all you have to do is breathe. But to live, to really live, you must believe. Reach4Life challenges you to breathe heaven’s air supply. It is designed to inspire you to plug into a relationship with God, the raw power of the Bible, the wisdom of saving lovemaking for marriage, the support of a local church, the beauty of a transformed life, and the opportunity to change the world one person at a time!
HISTORY OF REACH4LIFE
One of the biggest ongoing tragedies in sub-Saharan Africa is the HIV/AIDS pandemic. Africa has 70% of all HIV infections, with southern and eastern Africa accounting for over half of all global infections.
Although AIDS is no longer necessarily a terminal disease, as it can be managed with antiretroviral drugs, there is still no cure. And one thing that is very clear from the history of the HIV/ AIDS pandemic in Africa is that there is a direct link between the spread of the disease and poverty. For young people mired in poverty, there are few opportunities and little hope for the future. Hopelessness leads to risky behaviour, including sexual promiscuity and drug and alcohol abuse. For young men, there are few good male role models and young women are vulnerable to sexual exploitation and abuse.
In the face of such intractable social and moral problems, a few sex education classes and handing out free condoms is not the answer! Only a total transformation of the heart and mind can bring about true and lasting behavioural change. And how can such a change happen? Through meeting Jesus Christ as Lord and Saviour and having your whole life transformed through the Word of God. The goal is therefore not just sexual purity, but holistic spiritual transformation.
It was this realisation that led the Biblica team in South Africa to develop the Reach4Life programme back in 2004. After consulting with experts in HIV/AIDS, sexuality, educational psychology, and theology, all the additional material was written that, together with the text of the New Testament, forms the heart of the programme. Most of the additional material was written by a youth pastor from Cape Town, South Africa, whose own father had died of AIDS. The programme comprises 40 lessons delivered throughout the year in a small group context by peer educators who serve not just as teachers, but also as mentors and role models. Once a young person gives their life to Christ, they are connected to a local church where they can continue to receive the community support they need to thrive. Many young people who have gone through the programme have gone on to become peer educators themselves.
The 40 lessons are divided into 4 Journeys:
1. Believe – the gospel message of salvation.
2. Grow – how to grow in faith and spiritual maturity.
3. Live – how to deal with the practical challenges of life as a young person.
4. Change – how to be a change agent and work for God’s Kingdom.
There are also special additional sections that deal with sexuality and relationship-related issues (Hot topics) and overcoming hurdles to growing closer to God (That’s deep).
The programme was first run in schools but soon started being used in church youth groups, universities, prisons, drug rehabilitation centres, orphanages, and refugee camps. Wherever there were young people gathered, Reach4Life proved to have a powerful impact.
In 2015 a significantly revised version was released that shifted the focus from HIV/AIDS to a broader focus on sexuality and relationships in general, and introduced the easier-to-read New International Readers Version (NIrV) of the Bible.
After further research and consultation, a third version was released in 2019. This truly global version now incorporated the insights and experience of Biblica staff all over the world who had been running the Reach4Life programme. A new front section was developed that dealt with the primary developmental challenge of adolescence: developing a healthy and stable sense of personal and social identity – of which gender and sexual identity is just one part.
The fourth version was launched in 2024, celebrating 20 years of Reach4Life. The new edition features Biblica’s global redesign, brand new introductions to each book of the Bible and 3 additional Hot topics. The biggest change to the print edition is that the additional content is placed before and after the Bible book block. This means that it can be printed with either a New Testament or a full Bible, and it now includes both the Who am I? and Sex is everywhere sections.
Globally, Reach4Life has been implemented effectively in over 40 countries and has been translated into 40 languages. Biblica partners with organisations, both large and small, who run the programme in all kinds of settings. Millions of young people have been impacted by the programme as we continue to see lives transformed through God’s Word.
ESSENTIAL ELEMENTS OF REACH4LIFE
There are some essential elements that have been developed over many years that form the heart and soul of the Reach4Life programme:
1. It is a long-term discipleship programme, not just a product or free giveaway.
2. It is designed to be facilitated by peer educators in a small group context.
3. It works best when Scripture is read aloud, together.
4. It is not so much about teaching a lesson as creating space for discussion; in other words, the young people should be talking more than the facilitator!
5. It provides a safe space where young people feel free to ask any questions without being judged.
6. It is designed for young people to learn to think critically and biblically for themselves –not just to be given the right answers.
7. It can be used flexibly as the core content is designed to be adaptable to different contexts and cultures.
8. The ultimate goal is to get young people reading and engaging with the Bible for themselves – and reading whole books instead of just a few verses here or there.
THE THEORY UNDERPINNING REACH4LIFE
There are several core theoretical assumptions that the Reach4Life programme is based on. These may not all be visible on the surface – in other words, they may not be obvious by just skimming through the content, which sometimes appears deceptively simple. They do, however, serve as the foundation that the whole programme is built on. Or to use another analogy: the programme is like an iceberg of which the largest portion is below the water’s surface – the unseen section (the theory underpinning the programme) keeps the entire iceberg (Reach4Life) afloat!
1. Reach4Life is firmly based on the belief that only the Bible, as witness to Jesus Christ as Lord and Saviour, bears the truth that will set young people free from the burden of sin and condemnation; that will restore them to the wholeness of the image of God in which they were created; and will give them identity, community, meaning and purpose.
2. Reach4Life is a holistic discipleship programme that believes true and lasting change in behaviour only flows out of long-term relationships of authenticity and trust, where peer educators spend time with young people in small groups and where circles of trust are created where young people feel they can be themselves, speak honestly and become vulnerable without the fear of rejection.
3. Reach4Life is a non-judgmental approach to youth development that believes young people cannot be forced into behavioural change through fear and condemnation, but rather are attracted and inspired by a positive message of faith, hope and love, without compromising on the truth that the Bible reveals about God’s will for people.
4. Through extensive global research, it is clear that young people all over the world face the same struggles. Research shows that the biggest issues and challenges facing young people are: relationships and sexuality; substance abuse and addiction; social media and online activity (especially pornography). It is therefore important to address these issues head-on without avoiding the sensitive topics. However, it is also clear that these are symptomatic issues (or behavioural fruits) that can only be transformed and healed by addressing the underlying causes (or spiritual roots). Only by addressing the spiritual roots of identity, values, meaning and purpose, can negative and self-destructive behaviours be replaced by healthy and life-giving fruit.
5. Developmental psychology shows us that the core challenge and task of early adolescence is creating a secure and authentic social self, and that the centre of gravity at this stage of human development is peer group, sex, and society (having shifted from a focus on the family in childhood). The aim of Reach4Life is therefore to provide a positive, biblical approach to this psycho-social identity formation.
6. The purpose of salvation in Christ is not simply to go to heaven when one dies, but rather to be transformed and renewed here and now, and to join God’s mission in the world to preach the gospel and heal and restore the hurting and broken. Therefore, Reach4Life emphasises not just what we are saved from but also what we are saved for. Throughout the programme, and especially in Journey 4: Change, young people are inspired and equipped to become doers of the Word and to join the Great Commission that Jesus describes in Matthew 28:18–20.
THE 4 JOURNEYS
The 4 Journeys, and the 40 lessons covered therein, form the heart of the Reach4Life programme. The progression of the 4 Journeys – from Believe to Grow to Live to Change – illustrates the development and growth that is required for a young person to evolve to full maturity in their faith. This is well illustrated by the image of a tree that grows from a seed, to a small sapling, to a mature tree that produces fruit and seeds for new trees to grow.
BELIEVE GROW LIVE CHANGE
1. Believe: Takes youth through all the essential elements of the Christian faith. After going through all 10 lessons they will understand why they need God, who Jesus is, what his death and resurrection achieved for them, and what it means to accept Christ and commit their lives to serving him.
2. Grow: Works systematically through the core doctrines of Christianity. It starts with an understanding of the Bible as the inspired Word of God and the Church as God’s family, and then leads youth through all the things they need to grow in faith in Christ into spiritual maturity.
3. Live: Deals with all the issues that young people face in the world today – from the role that media and peer pressure play to the dangers of drugs, alcohol, and promiscuous sexual activity. This Journey also helps teens develop a healthy self-image and self-discipline and teaches them how to deal constructively with emotional pain.
4. Change: Helps young people to understand that following Jesus is not just about their own salvation. The purpose of Christian faith is service to others. And working towards the salvation and healing of all creation is the calling of every believer.
SPECIAL SECTIONS
1. Who am I?: Knowing who you are is one of the most important questions in life. This section guides young people to discover their built-in identity and purpose by putting Jesus at the centre.
2. The story: A look at the great rescue plan woven through all the books of the Bible. This is the Gospel message with an invitation to take the first steps in the adventure of walking with God.
3. Sex is everywhere: Introducing God’s plan for sex against the background of intense pressure from media and peers. Sex is a gift from God. No matter your past, you can begin again.
4. Hot topics: A biblical approach to 23 sex and relationship issues that many young people struggle with. You could call this the FAQ (frequently asked questions) section of Reach4Life. The aim is not to give simplistic answers to complex questions, but rather to help young people ask the right questions and think through the issues in mature, critical and biblical ways.
5. That’s deep: Answers to 12 hurdles to drawing closer to God, providing practical help to deal with faith issues commonly faced by young people.
HOW TO START AND RUN A GROUP
There are detailed instructions for how to start your own Reach4Life group at the end of the Reach4Life book, explaining who can start a group, how to go about running one, and some essential guidelines for facilitating a group.
It is important to note that although the 4 Journeys and the 10 lessons in each are designed with a logical sequence in mind, it is quite acceptable to change the order of the Journeys or lessons to suit the needs of your specific context. For example, some people choose to start with Journey 3: Live, as it grabs the attention of young people and deals with the most pressing issues, before going back to Journey 1: Believe.
It is important that you stick to the following guidelines; it will help trust and authenticity to develop in your group over time:
1. Prepare your lesson well and pray for your group before each meeting.
2. Create clear boundaries and expectations. Set some ground rules at the beginning of the lesson and create a safe space for young people to share by instructing them to:
◊ Be real with and respectful of each other.
◊ Give everyone a chance to talk – listen more than you speak and don’t interrupt.
◊ Commit to not sharing what you have heard outside of the group unless granted permission.
◊ Recognise that some things are difficult to share in a group. You may pass anytime you are not comfortable sharing.
◊ Laugh with each other, but not at each other.
◊ Keep your mind and heart open to God and his Word.
3. Stay on topic. When conversation begins to go off-topic, always bring it back to the main purpose of what you are there to discuss.
4. Watch for dominant speakers. If you notice one or two people who are constantly answering questions and dominating the conversation, try to encourage others to participate.
5. Establish positive relationships with each member of your group. This will improve their openness and receptiveness to what you have to say. Truth and honesty are key.
BASIC COUNSELLING TECHNIQUES
As a group leader, you may find young people approaching you, wanting to speak confidentially about problems they are struggling with. It is important to acknowledge that even if you are not a trained counsellor, you can still help a lot by just listening to their stories. But if there is anything they share with you that you think needs more help than you can give, refer them to a teacher, counsellor, pastor, or social worker who is trained to deal with more complex problems.
Here are a few basic counselling techniques to help you have meaningful conversations with young people:
1. Active listening: The most important part of building a trusting relationship is listening. Do not rush to respond. Be present with the person, actively listening to both what they are saying and what they are not saying. Watch for non-verbal signals indicating that there is more to the story. Be prepared to go in-depth and encourage them to focus on and process their feelings. Often, just telling their story is the first step to healing. Remember to keep your words and actions positive and accepting, to enable them to continue to share freely.
2. Empathising: Before responding, give yourself time to think. Use frequent, short responses. Using non-verbal communication (eye contact, nodding) throughout the conversation reminds the individual that you are listening and that you care. Remember, unconditional acceptance is a must so that the person can reveal and disclose themselves without the fear of rejection. The aim is to reflect God’s love and acceptance to promote a deeper level of self-understanding. Empathy is communicated by reflecting the feelings that the person is expressing back to them. It helps the person sharing to identify and connect with the appropriate emotion and encourages further exploration of their feelings. Responses to the expression of feelings may be a single word, a phrase, or a reflection of their experience or action. For example: You feel [name emotion] because/when [indicate experience or behaviour].
3. Comforting: Your goal in comforting someone is to address and reduce their grief or distress so that they can experience the presence of God as a reality and as a source of consolation.
4. Probing: Do not be afraid to ask questions and get more details about their story. The aim is not to interrogate (fire questions) but to encourage storytelling and self-disclosure. For instance, ask: Could you tell me more about that? Why did you say that? And how did you feel about that?
5. Interpreting: Assess and analyse the information you have received to gain insight into the individual’s unique situation. Think about how their story lines up with God’s story, and what he wants to do in the young person’s life.
6. Discerning: Reflect prayerfully and critically to gain a clearer and deeper understanding of the situation. Use your own experiences to connect the young person with the will of God and to apply the ethics of God’s love to their situation.
7. Responding: The way in which you respond further should always be in the best interest of the person you are counselling. Here are some ways you may choose to respond:
◊ Prayer: Ask if you can pray for them and what they would most like you to pray for them. Pray that God will meet their needs and give them peace and courage to face their situation.
◊ Professional counselling: They may need the kind of help you are not qualified to give. If they are showing signs of severe distress or trauma, connect them immediately with a professional counsellor or community service. Make note of the contact information of available professional help in advance, including applicable government services.
◊ Medical help: If the person is injured or has been sexually assaulted, help them get medical attention as soon as possible. Sexual assault victims must seek medical attention within 72 hours in order to collect evidence, determine pregnancy and to test for sexually transmitted infections. Tell them not to wash before visiting the hospital or clinic.
◊ Legal authorities: Engaging legal authorities is a serious decision. It should be made based on your specific community and any applicable laws regarding your responsibility to report a potential crime.
If connecting the person to counselling, medical or legal assistance, offer to accompany them.
GROUP FACILITATION METHODS
• Have group members read aloud.
• Use drama and role play.
• Use diagrams, charts, graphs, posters, pictures (visual aids).
• Use an object to make a point (e.g. show how the battery in a cell phone is like God’s spirit in us: without it, there is no power).
• Use stories to demonstrate a point.
• Get the group to draw pictures showing a concept or story.
• Get the group involved; have them do something (stand, sit, clap, shout out, stamp feet) when they hear certain words in a passage or story (When they hear the word wind they make noise like the wind; when they hear the word rain, they make noise like rain).
• Write down real-life situations on pieces of paper and have each group member pull them out of a hat. Have them say what they would or should do (Your friend picks up some fruit at the market without paying and says you should too – what would you do?).
• Use analogies (Life is like a painting that’s not done yet).
• See through the eyes of each character in a story (In the story about the xxxx, if I were the xxxx, I would have felt …).
• Finish the sentence (What I like about this story is … ; What’s hard to understand in this story is … ; I can relate most to the character of xxxx in this story, etc.).
• Use words from current popular songs (How do they relate to a lesson topic? Does the song encourage right or wrong behaviour? etc.).
• For each lesson, ask what the good and bad outcomes would be if the main point of the lesson was or was not applied (E.g. for Self-image: if they remember their value as a person, they won’t have sex before marriage; if they forget their value, they might have sex – and discuss the impact of that).
• Do a word association activity (What comes to mind when you hear the word xxxx?).
• Have a Letters to God box to collect their prayer requests or questions.
• Have group members keep a journal or diary.
WRITING A LESSON PLAN
A lesson plan is a step-by-step guide that lists the group leader’s plan for what the group will learn that day. It involves setting goals, deciding what methods you will use to teach the concept, thinking of activities, and making a note of what materials you will need.
Objectives and goals
Here you will write what you want your group to know or be able to accomplish after the lesson is completed.
Materials needed
Think about what materials you will need. (You will always need your Reach4Life book and training manual.) If you have other materials or props (pictures, newspaper, etc.), collect them and have them ready to take with you on the day of the group meeting.
Introduction
The purpose of the introduction is to:
• Say or do something that gets the group interested in what you have to say.
• Tell the group briefly what the lesson will be about.
• Talk about how this ties in with what you have talked about before.
• Find out what the group already knows about this subject (question and answer).
• Tell the group what you would like them to know after hearing this lesson.
Instruction
If your lesson plan were a hamburger, then the instruction section would be the meat. After stating your goals and giving the introduction, you are ready to do the lesson. Examples of methods of instruction are listed in the previous section and include discussion, group activities, role-playing, etc.
When deciding on your methods of instruction, consider the following questions:
• Group members have different ways of learning – by hearing, seeing, moving around, and feeling. How can I try to use as many of these ways as possible?
• What materials (books, things to show, props, etc.) can I use for this lesson?
• Are there any words (vocabulary) from the lesson that I need to explain?
• How can I get the group members to participate in discussions or activities? Try to think of fresh, new ways to get them involved. Don’t just stand in front of the group and talk at them. Be excited, and the group will get excited, too!
Application
In the application section of your lesson plan, write how the group will show that they understand the lesson material or concepts you gave them during instruction. At the end of the lesson:
• Group members should be able to show you that they understood.
• You should observe how well the main point was understood to help you when teaching other lessons later.
• Correct any mistakes in their understanding that you pick up on.
Closing
Closing is the time when you pull together what they have learned, and help group members organise the information in a meaningful way in their minds:
• A quick summary of the main points is often helpful.
• You can also have a quick discussion about what exactly they learned and what it means to them now.
• Look for anything they might be confused about and explain it again if necessary.
• Repeat the most important point so that they will remember it for later lessons.
• It is not enough to simply say, ‘Are there any questions?’ Ask questions and listen to see if they have understood the main point.
Assessment
At the end of the lesson, take some time to think about how it went. Did the group members seem to understand the material? Were they able to give you some examples of what you were trying to teach them? How can you do it better next time?
SAMPLE LESSON PLAN ON SELF-IMAGE: LIVE 7
Objectives and goals
Teach the young people that they have value and that God has a plan for them.
Materials needed
Reach4Life book, cup of water, empty Coke can (without opening it, poke small holes in the bottom and drain ahead of class), pieces of paper to write names on, diagram of butterfly (or actual butterfly or caterpillar).
Introduction
Today we are going to talk about the way you see yourself. You will see that you have value and that God has a plan for your life.
Look at this cold drink (Coke or something similar) and this cup of water. Which would you choose to drink?
The cold drink looks good on the outside but it is empty on the inside. The cup of water doesn’t look very exciting, but what is on the inside is full of something that gives us life –water! We cannot live without water! Sometimes we see ourselves and others in the wrong way.
Ask: What are some ways people might feel bad about themselves? Write the list on the board or have someone else write the list. Here are some examples:
• their bodies (tall, short, etc.)
• the clothes they wear
• where they live
• feeling like they are not smart (school is hard for them)
• feeling like there is nothing special about them.
Instruction
What does the Bible say about how God sees us? Turn to the journey on Self-Image: Live 7, in your Reach4Life book and let’s read it.
Next let’s read Psalm 139:1–18. What do verses 1–6 say God knows about us? (When we sit, when we stand, our thoughts, where we go, our ways, our words.) God knows everything about us all the time.
What do verses 7–12 say about the places where he is with us? (In the heavens, in the depths, on the wings of the dawn, on the far side of the sea.) Is there anywhere that God is not with us?
What do verses 13–16 say God knew about us before we were born? (He made us; he saw us as we were developing; he knows all of the days of our life before we were born.) God knows who we are and what we are going to be.
What do verses 17–18 say about when he is with us? (Even when we are asleep.)
Sometimes people think of themselves based on what other people think of them. You must not let others determine your worth. This is a job for God and God alone. We can do some things to start seeing ourselves as God sees us:
• Get to know God. You may not be able to choose your situation, but you can choose to trust God and love him.
• Believe that God has a plan for your life. We can read about that in Ephesians 1:3–6. He chose us to be his children.
• Be willing to let God change you. When an artist starts painting, often it looks like a lot of messy smudges of colour and brush strokes. But as they work, the smudges and strokes are filled in to become what the artist wanted to paint. Our lives may look like that sometimes. We have to trust that God will fill in the smudges of our lives with beautiful strokes of his brush. He will if we let him.
Butterflies are among the most beautiful and delicate creatures in God’s creation. Did you know that all butterflies used to be caterpillars at first? It works like this: First the caterpillar spins itself into a cocoon of white-looking thread. Then while inside the cocoon the caterpillar changes itself into a beautiful butterfly. The way it does this is strange, but the caterpillar actually digests itself and becomes a gooey mess inside the cocoon! If you were to open the cocoon, caterpillar soup would ooze out – not a pretty sight. But while in its soupy state, special cells begin to grow and multiply, and it becomes a butterfly. The butterfly eats the cocoon from the inside out and emerges as the beautiful butterfly we see flying around in the air.
In the same way, God has put in us what he needs to make us – something very special and beautiful. Sometimes we may feel a little like that caterpillar mush or soup before we become what he wants us to be.
God gives us all different gifts and abilities. Use the gifts that God has given you! You can also work harder to get better at something, even if it is not easy for you. For example, you could study hard in school. In sports, you can practise more.
Help others become what God wants them to be. Smile at others; listen to others; encourage others; be willing to help when there is a problem; defend others.
Application
How can having a bad self-image affect the choices we might make regarding sexual behaviour? (If you feel bad about yourself, you don’t value yourself and may let others take advantage of you.)
Describe someone who looked nice on the outside but wasn’t a nice person on the inside (don’t use names, and it can’t be anybody in the group).
Write one thing you like about the person sitting to your right. When everyone is done, pass it to that person.
So, how can you respond to bad things people say about you or others?
Assessment
• Did the group members participate?
• Did they listen well?
• Did they answer the questions in a way that showed they understood the main point?
• Were they excited?
• What part of the lesson were they most interested in?
• Did they lose interest in any part?
• Did it seem like they didn’t really understand any part of the story?
LESSON PLAN TEMPLATE
Date:
Age level:
Subject:
Objectives and goals:
Materials needed:
Introduction:
Instruction:
Application:
Closing:
Assessment and follow-up:
REPORTING AND ACCOUNTABILITY
A vital part of the Reach4Life programme is keeping a good record of what you have done. Reporting is essential for 4 reasons:
1. It provides a written record of the quantitative and qualitative impact of the programme.
2. It is a form of monitoring and evaluation, helping us see what we are doing well and how we can improve.
3. It assists with reporting to ministry investors what the spiritual return is on their investments.
4. We can share compelling stories that will attract new ministry investors and ensure the long-term sustainability of the programme.
The exact system of reporting and accountability will differ from one organisation to another, but it is vital that there is a system in place. Group leaders need to report their activities to designated coordinators; coordinators need to collate the information, and this needs to be fed back to Biblica at regular intervals.
Reporting should be both quantitative (numbers) and qualitative (stories). Quantitative reporting keeps track of things like how many young people are actively engaged in the programme, how many have given their lives to Christ, and how many have made commitments to purity. Qualitative reporting keeps track of how young people are responding to the programme, ideally in their own words.
Stories or testimonies can be recorded formally (ask group members to write down what Reach4Life has meant to them and what difference it has made in their lives), however, sometimes what is said without having been asked to share can be even more compelling.
For example, a group member might say, ‘I’m so happy I learned that God loves me. It helps me now that my sister is very sick. Now I know that I am not alone.’ Write this down as soon as possible in a notebook so that you don’t forget. Also record the name of the person who said it. Lastly, always ask permission to share people’s testimonies and whether they are happy for you to include their name.
Photographic or video reporting is often even more powerful than just a written testimony. This is because humans were visual creatures long before we invented symbolic, written language. A well-taken picture or video can communicate more than pages of descriptive writing. Always make sure you ask permission when taking a photo or video of someone. Where children are involved get the permission of their guardian or teacher as well as from the children themselves.
SCHOOL MINISTRY GUIDELINES
School staff are interested in providing learners with a quality education. The Reach4Life programme encourages learners to reach their fullest potential. This means the school and the programme are working toward the same goal. The Reach4Life programme also provides moral guidance which will have a positive effect on both the learners and the classroom. For things to work smoothly in the classroom, meet with the teacher whose classroom you will be using beforehand. During the meeting:
• Be professional and courteous.
• Briefly explain the basics of the programme.
• Find out how much time you will have and stick to it.
• Ask how many learners are in the class.
• Don’t ask the teacher for supplies; bring your own pencils, etc.
• Learn what the classroom rules and methods of discipline are.
• Find out if the school has any special policies and procedures you should be aware of.
• Are there any safety procedures (fire drills, school lockdowns, other emergencies)?
• Is there a dress code for the teachers?
• If someone comes and asks the learner to go with them, how should you respond?
• If possible, ask to be introduced to teachers in classrooms nearby.
• Find out where the restrooms are. Tour the building to become familiar with the layout.
• Ask the teacher if they have any preference as to whether the learners call you by your first name or your surname.
• Ask where you should store your personal items (coat, purse, bag).
• Thank the teacher for letting you come into their classroom and let them know you are looking forward to working in their classroom.
Establishing authority in the classroom
Establishing yourself as an authority figure may seem uncomfortable, especially if it is the first time you have taken on such a role. To gain the respect of the learners, you must look and act the part of a confident, capable leader. This means:
• Standing: You will spend the majority of your days on your feet. This gives you a height advantage over most learners and establishes you as an authority right away.
• Dressing appropriately: Look at what you wear on the job as your work clothes. If you are wearing something sloppy or inappropriate you will lose the respect of the learners, your co-workers, supervisors and parents.
• Smiling confidently: Even if you aren’t in a great mood or feeling confident you need to project a positive attitude. This gives the learners confidence and will probably help to turn your mood around.
• Speaking slowly and clearly: Thinking before you speak is extremely important. Make sure that what comes out of your mouth is professional and it will gain you respect.
Dealing with confrontational learners
One difficult issue for teachers is dealing with confrontational learners. Here are some ideas and tips to help in this situation:
• Do not lose your temper: This can be harder than it sounds. However, you must remain calm. You have a classroom full of learners watching you. If you lose your temper and start shouting at a confrontational learner, you have given up your position of authority and lowered yourself to the learner’s level. Instead, take a deep breath and remember that you are the authority figure in the situation.
• Do not raise your voice: Raising your voice will simply make things worse. Instead, it is better to talk quietly as the learner gets louder. This will help you keep control and appear less confrontational to the learner, thereby helping to calm the situation.
• Do not get other learners involved: It doesn’t help to get other learners involved in the confrontation. For example, if the learner is making an accusation about something you did or did not say, do not turn to the rest of the class to ask them what you said. The confrontational learner might feel backed into a corner and become even more angry. A better response would be to say that you will be happy to speak with them about the situation after the class is over.
PRISON MINISTRY GUIDELINES
• Know your facility. Find out what the rules are and follow them. Rules will be different at different facilities. If there are any written instructions for volunteers, ask for a copy.
• Be sure you understand when you will be allowed to come in. Then be on time.
• Wait patiently to be processed. The officers are very busy, and you may be delayed.
• Allow time in your schedule for this. Be courteous and respectful of the facility staff.
• Bring current ID (no expired driver’s licence).
• Do not ask for special privileges from the facility (for example, asking them to let you in even if you forgot your ID).
• Clothing should be neat and clean, but not flashy. Women should dress modestly.
• Don’t chew gum or bring it with you. It can be used in harmful ways.
• Leave your cell phone, keys, small knives, etc., at home or someplace else.
• Do not take anything into or out of the facility without the permission of the facility’s programme administrator. If you are given permission to hand something out (Bible verses, for example), find out if the inmates are allowed to keep it, or if you need to collect it from them before you leave.
• When moving around within the facility, stay to the side of the corridor and keep a safe distance while staff and inmates pass. Allow them to go through the door first. Don’t walk ahead of the officer when being escorted; let them lead you.
• Find out if the facility requires two or more volunteers to go in at the same time, or if you are allowed to go in by yourself.
• Don’t do any favours for inmates. Don’t pass messages or take anything out of or into the facility on behalf of a family or friend. You may be smuggling in drugs or contraband without knowing it.
• If an officer does not stay with you, find out how to reach one quickly.
• Be aware of interactions between the inmates. Disagreements can quickly turn into fights. If you see that things are getting out of hand, ask an officer for help immediately. Do not try to break up a fight!
• It is very important to be aware of manipulation. Always be professional – do not become friends with the inmates. Treat them with respect but keep a distance. Inmates who try to be extra friendly, or pay you compliments, may be trying to eventually get to the point where they feel they can ask you for favours.
• If you are asked for a favour, say: ‘Our organisation doesn’t allow us to do that, but I will let the officer in charge know that you need something.’
• If you have a question about whether something is allowed, or if you need clarification on a policy, ask the officer in charge.
• If inmates share why they are there, that’s fine, but never question them about it. Don’t comment on what they have done.
• Don’t say that you are with a specific church or denomination. Remind your group that you are not sharing your opinion, but what the Bible says.
• Do not give any of the inmates your personal information (phone number, address, etc.). If you are allowed to have contact with them after they are released, give them a neutral number (your church). Some inmates, once released, might become a threat. Make outside connections carefully, and preferably in a neutral location such as your church.
APPENDICES
The purpose of the appendices in this training manual is to give you – the Reach4Life peer educator or group facilitator – a concise summary of the best available information on the major issues that young people face in contemporary society.
The list is not exhaustive, and the summaries do not cover everything you possibly need to know to facilitate a group of young people going through the Reach4Life programme, as they may ask you questions that are not specifically covered. However, this information is pulled together in one handy volume in your training manual, so that you can carry it with you to your Reach4Life group meetings and quickly refer to the relevant section and give reliable information on the topic you are covering or when you are asked a spontaneous question.
The appendices are designed to give you factual and helpful information on the topics. For the biblical perspective, please refer to the relevant Journey or Hot Topics answer that relates to the topic.
Lastly, do your own research – especially regarding youth issues specific to your own country or community – and be sure you know what resources are available locally to assist young people struggling to overcome any of these challenges.
SEX, GENDER AND SEXUAL ORIENTATION
What is the difference between your sex, your gender, and your sexual orientation? Defining these terms is important because they are often confused. What also confuses people are the two related issues of:
1. Whether variations in sex, gender and sexual orientation actually exist.
2. Whether the existence of variations means it is morally acceptable to express your gender and sexuality in any way you want to.
A simple way to make the distinction is by remembering that: Your sex is about your body, your gender is about who you feel yourself to be, and your sexual orientation is about to whom you are sexually attracted.
A small number of people are atypical in their biological sex (sex), or their feeling of being male or female (gender), or who they are sexually attracted to (sexual orientation). In other words, some people are born with variances in their biological sex; some people question whether their gender matches their biological sex; and some people feel sexually attracted to people of the same sex, or both. The reason for these differences is very complex and not yet fully understood by physical and social scientists.
However, the fact that these developmental differences exist in a small number of people, does not mean that how we live out our gender and sexuality is simply a matter of choice. The Bible gives clear guidelines for God’s will for human identity and sexual relationships, as spelled out throughout the Reach4Life book. We therefore need to be compassionate and understanding towards people struggling with their gender identity or sexual orientation, but still be clear on what the Bible says and what God’s will is for the life choices we make. And most importantly, communicate that grace and hope are available for all who trust in Christ’s redemption!
Now here’s the longer answer:
Sex is the term we use to refer to a person’s sexual anatomy (the sexual body parts). So if a doctor were to say that a girl is female in terms of her sex chromosomes, her sex organs, and hormonal make-up, the doctor is referring to the girl’s sex (her body). People with disorders of sex development (DSD) are born with a sex type that is different from most men and most women. Rather than being male typical or female typical, people with DSD have one or more sex atypical traits. That means a woman with DSD has some sex traits that are relatively unusual for females, and that a man with DSD has some sex traits that are relatively unusual for males. So DSD is an umbrella term covering a wide variety of conditions in which sex develops differently from typical male or typical female development. People with DSD are sometimes referred to as intersex.
Gender identity is the innermost concept of self as male or female – how individuals perceive themselves and what they call themselves. For most people their sense of self is directly related to their biological sex, for example, they are biologically male and perceive themselves to be male. However, a small percentage of people question this in themselves and identify more with the opposite sex, or with no particular gender. This is commonly called transgender (or trans for short). However, as mentioned above, the fact that some people legitimately struggle with their gender identity does not therefore mean it is simply a lifestyle choice. God’s will for how he wants us to live out our gender and sexuality is clearly spelled out in the Bible (Gen 1:27 and Gen 2:22–24).
Gender role is slightly different to gender identity in that it refers to social roles that are expected by a society according to your gender. These roles are concepts of what it means to be masculine or feminine. Expected gender roles can differ from one culture to another, and gender roles have been changing a lot in the last hundred years, as many societies have become less restrictive about what roles men and women may take on. Sometimes when someone does not fit the expected gender roles of their society or culture, they may mistakenly question their gender identity.
Sexual orientation is the term used to refer to a person’s sexual (erotic) feelings. While most people are attracted to the opposite sex (heterosexual or straight), a small minority of people find themselves being attracted to the same sex (homosexual or gay/lesbian), or both sexes (bisexual). The reasons for these variations in sexual attraction in some people are still poorly understood but are very complex. The experience of an atypical sexual orientation itself, therefore, cannot be described as moral or immoral, but how one chooses to act certainly is. And God’s grace is sufficient for all those who struggle with their sexuality.
The ethics of gender identity and sexual orientation
Statistically speaking, most females are anatomically sex-typical: they gender-identify as women, and they are sexually oriented towards men. Statistically speaking, most males are anatomically sex-typical: they gender-identify as men, and they are sexually oriented towards women. But some people experience variations in these combinations of sex, gender identity, and sexual orientation because human development is biologically and psychologically very complex.
However, the fact of these differences does not mean we can live any way we want to. Some behavioural choices are unhealthy and destructive because they go against the will of God for human and societal flourishing. The Bible is clear that the right place to express our sexuality is in the marriage between a man and a woman.
For those who are struggling with their gender identity or sexual orientation, our attitude ought to be one of love, compassion and understanding, but without condoning a lifestyle that goes against the will of God. We also want to remind all of those struggling, of the Bible’s amazing promises – that God loves us, that he has a way through for us, that our honouring of God in this is both for our good and for his glory.
SEX AND PREGNANCY
The reproductive organs
A number of organs and structures in both the woman and the man are needed to make a baby. These are called the reproductive organs and genitals.
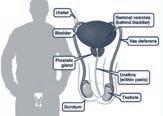
In males, the reproductive organs and genitals include:
• testes: also called testicles; a pair of oval-shaped glands that produce sperm
• scrotum: the pouch of skin that contains the testes
• penis: the male reproductive organ, through which urine and semen pass
• prostate gland: a gland that produces some of the fluid part of semen
• seminal vesicles: a pair of glands that also produce some of the fluid part of semen
• vas deferens: a pair of ducts leading from the testes to the seminal vesicle, through which the sperm travel

In females, the reproductive organs and genitals include:
• ovaries: two organs on either side of the lower abdomen that release an egg cell every month
• vagina: a muscular tube that receives the penis during sex, through which sperm travel on their way to fertilise the egg, and through which a baby passes during childbirth
• fallopian tubes: a pair of tubes running from the ovary to the uterus, through which an egg cell travels, and where fertilisation with sperm usually occurs
• uterus: an organ, also called the womb, where the fertilised egg cell implants and grows into the unborn baby during pregnancy
• vulva: the outer folds that surround the openings of the vagina and the opening from the bladder called the urethra
What exactly is pregnancy?
Simply put: for pregnancy to happen, a man’s sperm needs to meet up with a woman’s egg cell. Pregnancy officially starts when the fertilised egg implants in the lining of the uterus (womb). It takes up to 2–3 weeks after sex for pregnancy to happen. But pregnancy is a pretty complicated process that has several steps.
Step 1: Ejaculation and ovulation
Sperm are microscopic cells that are made in testicles. Sperm mix with other fluids to make semen, which comes out of the penis during ejaculation. When the man reaches climax/orgasms during sex, the equivalent of about one teaspoon of semen – containing millions of sperm – is released into the vagina. But it only takes one sperm cell to meet with an egg for pregnancy to happen.
Eggs live in ovaries. The hormones that control the menstrual cycle cause a few eggs to mature every month. These hormones also make the lining of the uterus thick and spongy, which gets the body ready for pregnancy. About halfway through a menstrual cycle, one mature egg leaves each ovary – called ovulation – and travels through the fallopian tube towards the uterus. The egg remains for about 12–24 hours, slowly moving through the fallopian tube, to see if any sperm are around.
Step 2: Fertilisation
If semen gets in the vagina, the sperm cells can swim up through the cervix and uterus and into the fallopian tubes, looking for an egg. They have up to 6 days to find an egg before they die. When a sperm cell joins with an egg, it’s called fertilisation. The fertilised egg moves down the fallopian tube toward the uterus. It begins to divide into more and more cells, forming a ball as it grows. The ball of cells (called a blastocyst) gets to the uterus about 3–4 days after fertilisation.
Step 3: Implantation
The ball of cells floats in the uterus for another 2–3 days. If the ball of cells attaches to the lining of the uterus, this is called implantation – when pregnancy officially begins; the start of a new human life. Implantation usually starts about 6 days after fertilisation and takes about 3–4 days to complete. The embryo develops from the cells on the inside of the ball. The placenta develops from the cells on the outside of the ball.
How do you get pregnant?
The most common way people get pregnant is through vaginal sex – when a penis enters a vagina during sex. This is the case even if:
• the girl has not had her first period
• the girl is having her period
• it is the first time she has had sexual intercourse
Ovulation is the ideal time for a pregnancy to occur if a man and woman have unprotected sex. But it is quite possible for a woman to also become pregnant even if:
• sex occurs at another time in the menstrual cycle
• the man withdraws his penis from her vagina before ejaculating (this is because sperm is also present in the pre-cum – the clear fluid released from the penis before ejaculation)
• any semen, including pre-cum, is deposited in or just outside the vagina
• she has not had an orgasm during intercourse.
How does a woman know she is pregnant?
Many people notice symptoms early in their pregnancy, but others may not have any symptoms at all. Common signs and symptoms of pregnancy can include:
• missed period
• swollen or tender breasts
• nausea and/or vomiting
• feeling tired
• bloating
• constipation
• peeing more often than usual
Some early pregnancy symptoms can sometimes feel like other common conditions (like PMS). So the only way to know for sure if you are pregnant is to take a pregnancy test. You can either take a home pregnancy test (the kind you buy at the drug or grocery store) or get a pregnancy test at your doctor’s office or local clinic.
Why is a missed period often the first sign of pregnancy?
Because pregnancy dates from the time of the last period, a woman might be 4, 5, 6 or more weeks pregnant before she realises it. She may not experience other physical symptoms (such as fatigue, nausea, and breast tenderness) until a little later. An egg that has been successfully fertilised by a sperm cell remains in the lining of the uterus. Rather than being shed, this lining stays to nourish the egg. That’s why women don’t get periods when they’re pregnant. If an egg doesn’t meet up with sperm, or a fertilised egg doesn’t implant in the uterus, the thick lining of the uterus isn’t needed, and it leaves the body during the period. Up to half of all fertilised eggs naturally don’t implant in the uterus – they pass out of the body during the period.
TEEN PREGNANCY
What is teen pregnancy?
Teenage pregnancy is pregnancy in a woman 19 years of age or younger. A woman can get pregnant if she has vaginal sex with a man at any age after she’s begun having regular monthly periods – which includes her teen years! A teenage pregnancy can change the course of a young mom’s life. It puts her in a place where she’s responsible not only for herself, but also for another human being.
How teen pregnancy affects the mother
Physical impact
Teens are at a higher risk for pregnancy-related high blood pressure (preeclampsia) and its complications than average-age mothers are. Preeclampsia can also harm the kidneys or even be fatal for mother or baby.
Pregnant teens also have a higher chance of becoming anaemic. Anaemia is a reduction in the number of red blood cells. This can make you feel weak and tired and can affect your baby’s development.
Although modern medicine has made giving birth safer than ever, childbirth is still more dangerous for a teen than for a woman 20 or older. According to the World Health Organization (WHO), complications during pregnancy or childbirth are the leading cause of death globally for girls ages 15 to 19.
After giving birth, teenage mothers may neglect their physical health while caring for their babies. They may also not have access to or know about healthy foods and eating.
Psychological impact
If you get pregnant as a teen, you might feel frightened and worried about telling your family and friends. Not talking to someone and not getting the help and support you need can make you feel more isolated and depressed. This can lead to problems at home and at school.
Teenagers who give birth are at greater risk for mental health concerns than older moms. Being a new mom at any age isn’t easy, and especially so if you are a teenager. Becoming a mom not only creates physical changes; women also go through mental changes.
Teen moms, already stressed by their challenging circumstances, face added stress from:
• sleepless nights
• arranging childcare
• making doctor’s appointments
• attempting to finish high school
Teen moms might face a number of mental health conditions related to childbirth and being a new mom. Examples of these conditions include:
• Baby blues is when a woman experiences symptoms for one to two weeks after giving birth. These symptoms include mood swings, anxiety, sadness, feeling overwhelmed, difficulty concentrating, trouble eating and difficulty sleeping.
• Postpartum depression involves more severe and significant symptoms than baby blues. Teen moms are twice as likely to experience postpartum depression than their adult counterparts. Women sometimes mistake postpartum depression for the baby blues. Baby blues symptoms will go away after a few weeks. Depression symptoms won’t.
Additional symptoms of postpartum depression include:
• difficulty bonding with your baby
• overwhelming fatigue
• feeling worthless
• anxiety
• panic attacks
• thinking of harming yourself or your baby
• difficulty enjoying activities you once did
How teen pregnancy affects the baby
Physical impact
Teen mothers are more likely to give birth to premature babies. A healthy pregnancy lasts 40 weeks. A baby that’s delivered before 37 weeks of pregnancy is premature. Sometimes, these premature babies lack complete development in their bodies and brains. Depending on how premature the baby is, this can lead to lifelong difficulties with health and development.
Premature babies also tend to be underweight. Underweight babies might have trouble breathing and feeding as infants. Adults who were underweight as babies are more susceptible to diseases such as diabetes and heart disease. Low birth weight also affects brain development. Children who were born underweight have been observed to have learning difficulties.
In addition to having an increased risk of being underweight, infants born to teenage mothers are also at a higher risk of infant mortality.
Lifelong effects on the child
Children born to adolescent parents face greater challenges throughout their lives. These challenges include getting less education and worse behavioural and physical health outcomes like:
• being less prepared to enter kindergarten
• relying more heavily on publicly funded health care
• being more likely to be incarcerated at some time during adolescence
• being more likely to drop out of high school
• being more likely to be unemployed or underemployed as a young adult
These effects can create a perpetual cycle for teenage mothers, their children, and their children’s children.
How teen pregnancy affects the father
Fathering a child as a teenager can be a frightening and life-changing event. Even though teen fathers don’t have to worry about the health implications of pregnancy and childbirth, they could face difficulties staying in school and earning a living similar to the challenges that teen moms have.
Country laws vary on the legal age for people to have sexual intercourse. Arrest or legal action against sexually active teens can have devastating effects. A young man may be required to register as a sex offender if he has reached the legal age (age 18 in some countries) and his partner has not (age 17 or under).
Financial consequences of teen pregnancy
Many pregnant teens drop out of school, and some never complete their education. That means a lot of mothers who get pregnant as teenagers live in poverty. Women who first get pregnant as teens are more likely to have more than one child. About one in five births to a teen mother is a repeat birth. A woman with little education and multiple children to care for will find it very difficult to earn a living.
Teenage moms are more likely to have positive mental health and financial outcomes when they finish high school. Some high schools will make arrangements with a teen mom to help her finish her education. While finishing school can be an extra stressor, it is important for the future of a teen mom and her baby.
How can teen pregnancy be prevented?
The only way to be sure you won’t get pregnant is to not have sexual intercourse.
Many communities offer counselling and support programmes that help prevent teen pregnancy. These groups can provide information on birth control and help teens understand their sexual limits so they don’t get into situations where they might have sex.
What to do if you are a pregnant teen
If you are a teenager and a parent, there are ways to help yourself and your child. Getting support from your family, friends, adult role models and services in the community can help you cope with being a young parent:
• See if there’s a way you can finish school if you haven’t already. This might mean studying at night while a partner, friend, or parent minds your child. In the long run, having an education will help with your chances of finding a job, and studying can help you to feel less lonely.
• If you can stay with your parents while your child is young, this may help you deal with the pressures of caring for your child or coping financially. Your parents might also be able to give you some support when you need it, and even share some tips from when you were a baby.
• If you are on your own or living away from your family, find out what sorts of government financial support you can get to help with living expenses and rent.
• Find out about support groups for teen parents. These groups can provide emotional support as well as information on child development and health care.
• See if your local clinic can put you in touch with a counselling service. Counselling can help parents with their own issues as well as those associated with being a parent at a young age.
• Speak to different experts whom you come in contact with – such as your doctor, or a clinic nurse – to learn about creating the best home environment for your child. They can also help you learn about topics such as nutrition, health, and emotional development.
SEXUAL ASSAULT
What is sexual assault?
Sexual assault is any unwanted sexual act done by one person to another. Sexual assault is never OK and if it has happened to you, it is not your fault. In essence, it is an act of violence committed by a person to feel power over another person. It can come in different forms:
• Sexual touching is touching of any kind that is unwanted or coerced, including kissing, groping, or fondling.
• Rape means being forced to have vaginal, oral, or anal sex against your will or without your full consent, including penetration with objects or body parts.
• Acquaintance sexual assault is when a person is attacked by someone they know such as a classmate, neighbour or friend.
• Date rape is a specific type of acquaintance sexual assault which occurs when a person is attacked by someone they know and may be interested in (like a partner).
Other forms of sexual violence include sexual harassment, sexual abuse, sexual exploitation, sex trafficking, voyeuristic behaviours and unwanted sexting.
If you have been sexually assaulted
Sexual assault of any type can be a very traumatic experience, even if you are able to get away from the attacker. It is important to remember:
• It is not your fault: Sexual assault is always the attacker’s fault, not yours and no one has the right to touch you sexually without your permission. It is not true that a person was asking for it because of what they were wearing or how they were acting. If sex is forced without someone’s consent, that is rape. It is still rape if the people are dating, married or have had sex together before. Remember that you never owe someone sex.
• Sexual assault isn’t always violent: If you say no or don’t say anything at all, and the person continues, it is still sexual assault if you did not give your permission. This is true even if you don’t resist.
• Sexual assault isn’t always about sex: Sex without consent is an act of violence and aggression – it is not about love and respect. Someone who cares about you will not force you to do anything sexual without your permission.
It is important to get support immediately.
Many communities have sexual assault or crisis lines that allow you to talk to someone about what you are feeling. You can also talk to family, friends, teachers, counsellors, or someone else you trust. If you are comfortable with it, you may choose to contact the police.
But contacting the police is your decision. If you have been sexually assaulted and are thinking about reporting it, here are some things to remember:
• Don’t bathe or change your clothes after the assault until you have gone to the hospital for an examination.
• Go to the hospital or clinic after you have been sexually assaulted so the staff can make sure you are not physically hurt.
• Hospital staff can talk to you about testing for sexually transmitted infections (STIs) and pregnancy if needed.
• Hospital staff can look for physical evidence in case you decide to press charges against the attacker.
• Even if some time has passed since the sexual assault took place, you can still report it.
• If you want more information before you decide to report a sexual assault, you can call the police anonymously to learn more about the process.
• You can call a local sexual assault or crisis line. You can find their numbers online or ask hospital staff for more information.
Common myths about sexual assault
Myth: It is OK to force someone to have sex if they are drunk, wear provocative clothing or agree to go out on a date with the person.
Fact: It is never OK to force someone to have sex. No reason justifies sexual assault – you must get consent every time.
Myth: Males always commit the sexual assaults.
Fact: People of any gender can commit sexual assault or be sexually assaulted.
Myth: Sexual assaults are usually committed by a stranger.
Fact: You’re more likely to be assaulted by someone you know than by a stranger. (This is called acquaintance sexual assault.)
What is consent?
At the core of sexual assault and rape is the issue of consent. Consent means to give permission for something to happen or be done. With this in mind we practise consent in nearly every social or interpersonal contact we have throughout our days – from asking to sit next to a stranger on the bus to asking a friend if you can borrow money. These exchanges force us to engage with another person, to not assume their comfort level or response, to pay attention to their words as well as non-verbal cues and to abide by their answer, regardless of our feelings about it. In the case of sexual consent, it is no different.
Consent is also an ongoing process throughout a sexual encounter and can be withdrawn at any time. This means that a person can consent to oral sex but not consent to vaginal intercourse and if this occurs it can be considered sexual assault or rape.
Additionally, consent is never assumed, even in the context of a relationship. Past sexual activity, an intimate relationship or marriage does not provide blanket consent for future sexual activity.
The impact of sexual violence on survivors
Every person who experiences sexual violence responds to the trauma differently. This can be due to a variety of factors including past history with abuse or violence, personality traits, established coping strategies, support systems, relationship with the offender or even where the assault took place. It is important to understand that there is no right way for a survivor to respond to an assault and they may present for help and support either immediately following or even weeks, months or years later. Although there is no one way survivors will respond there are some common responses we tend to hear.
Common emotional responses:
• shock
• embarrassment (I’m sorry you have to hear about this … )
• shame
• self-blame (I can’t believe I invited them back to my apartment … )
• guilt (I must have been leading them on, I mean I did flirt with them all night … )
• anger
• vulnerability or fear (I have tried going out and being normal but everyone I see reminds me of them … )
• denying or minimising the severity of the assault (I know people have much worse things happen to them, maybe mine wasn’t so bad … )
• concern for the offender (I want them to know what they did was wrong, but do you think they will be kicked out of school?)
• mood swings
Common physical responses:
• feeling dirty and needing to repeatedly shower/bathe
• pain
• anxiety/panic attacks
• depression
• changes in sleeping/eating patterns
• flashbacks Common long-term impacts:
• mental health issues
• substance use issues
• difficulty concentrating (impacts at work and/or school)
• a higher likelihood of ongoing physical health conditions
The impact of sexual violence on others
Sexual violence tends to cause a ripple effect of trauma onto other people that the survivor knows and cares about, including anyone from family members and intimate partners to roommates or fellow school members. Acknowledging these far-reaching impacts allows us to remember that healing from this violence often includes providing support to secondary victims. Secondary victims can have many similar feelings to those of a survivor including shock, anger, a sense of vulnerability and helplessness. By validating these feelings and also providing them with resources to better understand the experience of the survivor and how to be most supportive, we are not only caring for their needs but also helping to create a supportive environment for the survivor to heal.
The impact of sexual violence on the community and society
When cases of sexual violence occur – in schools, workplaces, neighbourhoods, campuses, and cultural or religious communities – many community members may feel fear, anger, or disbelief that this has happened to someone they know. This response can come from a place of shock that a person similar to them has been victimised as culturally many people still believe that victims are somehow different to themselves.
Additionally, there are financial costs to communities. These costs include medical services, criminal justice expenses, crisis and mental health services fees, and the lost contributions of individuals affected by sexual violence. Most importantly, the contributions and achievements that may never happen because of the trauma from sexual violence is a cost to society that can’t be measured.
Drug-facilitated sexual assault
Drug-facilitated sexual assault occurs when alcohol or drugs are used to compromise an individual’s ability to consent to sexual activity. These substances (called date rape drugs) create vulnerabilities in a person and make it easier for a perpetrator to commit sexual assault because of the victim’s limited ability to resist and, in some cases, remember the assault.
It is quite common for survivors of drug-facilitated sexual assault to exhibit self-blame, especially when they weren’t forced to take, or were tricked into taking the drug or alcohol. It is not the survivor’s fault as no one has the right to take advantage of another while they are vulnerable.
Perpetrators use a variety of substances to incapacitate a victim:
• Alcohol is the most commonly used substance in drug-facilitated sexual assault.
• Prescription drugs like sleep aids, anxiety medication, muscle relaxants, and tranquillisers may also be used by perpetrators.
• Street drugs, like GHB, Rohypnol, ecstasy, and ketamine can be added to drinks without changing the colour, flavour, or odour of the beverage.
Common signs a drug may have been ingested include the following:
• nausea
• loss of bowel or bladder control
• difficulty breathing
• feeling drunk without consuming any alcohol or very limited amounts
• sudden increase in dizziness, disorientation, or blurred vision
• sudden body temperature changes that could be signalled by sweating or chattering teeth
• waking up with no memory or missing large portions of memories
If a person identifies any of these signs or believes they may have been drugged, it is important to preserve the evidence as quickly as possible. Many of these substances are processed through the body within 12–72 hours and therefore obtaining a blood or urine sample as soon as possible is critical.
Recovery from sexual assault
As traumatic as sexual assault is, it is important to emphasise that recovery is possible. However, it is vital to seek help, and the sooner after the assault the better. Ideally, a trained counsellor with knowledge of trauma counselling should be sought, but in the absence of a trained professional, a wise and trusted mentor or friend can be of great value in dealing with the aftermath of a sexual assault.
SEX TRAFFICKING
What is sex trafficking?
Sex trafficking is human trafficking for the purpose of sexual exploitation, including sexual slavery. A victim is forced, in one of a variety of ways, into a situation of dependency on their trafficker(s) and then used by these trafficker(s) to give sexual services to customers.
Sex trafficking is one of the biggest criminal businesses and it has been described as ‘the fastest growing criminal industry in the world’. Due to the covert nature of sex trafficking, obtaining accurate, reliable statistics is difficult for researchers. The global commercial profits for sexual slavery are staggering.
Most victims find themselves in coercive or abusive situations from which escape is both difficult and dangerous. Locations where this practice occurs span the globe and reflect an intricate web between nations, making it very difficult to construct viable solutions to this human rights problem.
Sex trafficking occurs in a range of venues including fake massage businesses, via online ads or escort services, in residential brothels, on the street or at truck stops, or at hotels and motels.
Sex trafficking misconceptions
Human trafficking (of which sex trafficking is one kind) is not to be confused with human smuggling. Human trafficking for sexual or other labour may involve transporting victims across international borders, but to meet the definition of trafficking, there needs only to be exploitation of an individual after they have been coerced or deceived, so it does not necessarily involve transportation across national borders.
Sex trafficking is also commonly conflated with prostitution. The difference is that prostitutes claim it is entirely their choice, while those who have been sex trafficked are victims. Some argue that prostitution is also a kind of sex trafficking in the sense that it is often their last option to earn money.
Types of sex trafficking
The situations that sex trafficking victims face vary dramatically. Many victims become romantically involved with someone who then forces or manipulates them into prostitution. Others are lured in with false promises of a job, such as modelling or dancing. Some are forced to sell sex by their parents or other family members. They may be involved in a trafficking situation for a few days or weeks or may remain in the same trafficking situation for years.
Pimp-controlled trafficking
In pimp-controlled trafficking, the victim is controlled by a single trafficker, sometimes called a pimp. The victim can be controlled by the trafficker physically, psychologically, and/ or emotionally. To obtain control over their victims, traffickers will use force, drugs, emotional tactics as well as financial means. In certain circumstances, they will even resort to various forms of violence, such as gang rape and mental and physical abuse. Traffickers sometimes use offers of marriage, threats, intimidation, brainwashing and kidnapping as their means of obtaining victims.
A common process is for the trafficker to first gain the trust of the victim, called the grooming stage. They seek to make the victim dependent on them. The trafficker may express love and admiration, make lofty promises such as making the victim a star, offer them a job or an education or buy them a ticket to a new location. The main types of work offered are in the catering and hotel industry, in bars and clubs, modelling contracts, or au pair work. Once the victim is comfortable, the pimp moves to the seasoning stage, where they will ask the victim to perform sexual acts for the pimp, which the victim may do because they believe it is the only way to keep the trafficker’s affection. The requests progress from there and it can be difficult for the victim to escape.
Another tactic is for traffickers to kidnap their victims, and then drug them or secure them so they cannot escape.
After the victim has joined the offender, various techniques are used to restrict the victim’s access to communication with home, such as imposing physical punishment unless the victim complies with the trafficker’s demands and making threats of harm and even death to the victim and their family. Sometimes, the victims will form a trusting relationship with the captures (called the Stockholm syndrome) because their captors will pretend to love and need them, even going so far as to promise marriage and future stability. This is particularly effective with younger victims because they are more inexperienced and therefore easily manipulated.
Those who traffic young girls into prostitution are often women who have been trafficked themselves. As adults, they use personal relationships and trust in their villages of origin to recruit additional girls.
Gang-controlled trafficking
Gang-controlled sex trafficking and pimp-controlled sex trafficking run their operations in very similar ways. The largest difference between the two is that gang-controlled trafficking is run by a large group of people whereas pimp-controlled trafficking is run by only one person. One money-making source that many people do not necessarily associate with gangs is human sex trafficking. Gangs are now turning to sex trafficking as it is seen as safer and more lucrative than drug trafficking. The gangs can make larger amounts of money quicker by selling other people’s bodies and are less likely to get caught.
In certain circumstances, gangs may team up with other gangs in the area and work together as a sex ring. There are a several reasons that gangs make this decision. One reason is that it enables them to increase profits by trading different girls, women, boys, or men. This gives their client, also known as a john, a greater variety of options to choose from. Clients are often willing to pay a larger price for a sexual experience with someone new. Another reason that gangs will share females is because this makes it more difficult for law enforcement to keep track of the victims, ultimately preventing them from making a positive identification.
Gang members often wear certain types of clothing or colours to prove their commitment or loyalty to the gang. It is also very common to represent your gang by branding your body with tattoos. Unfortunately, many victims of sex trafficking are being branded as well. By forcing a tattoo onto their victims, they are essentially marking their territory and officially displaying ownership of that person.
Familial trafficking
In familial trafficking, the victim is controlled by family members who allow them to be sexually exploited in exchange for something of value, such as drugs or money. For example, a mother may allow a boyfriend to abuse a child in exchange for housing. Usually, it begins with one family member and spreads from there. Familial trafficking may be difficult to detect because these children often have a larger degree of freedom and may still attend school and after-school functions. These children may not understand that they are being trafficked or may not have a way out.
Familial trafficking is considered by some to be the most prevalent form of human sex trafficking. Many families from impoverished areas (India, Thailand, Philippines, etc.) find themselves in situations where debt or tradition calls for the selling of a loved one, most commonly female. In Thailand, there is a tradition known as bhun kun, which establishes the youngest daughter as financially responsible for her parents as they grow old. Many children are sold to repay debts, or merely to put food on the table for their family for a month.
Forced marriage
A forced marriage is a marriage where one or both participants are married without their freely given consent, often being threatened by family members or the bride/groom.
A forced marriage qualifies as a form of human trafficking in certain situations. If a woman is sent abroad, forced into the marriage, and then repeatedly compelled to engage in sexual conduct with her new husband, then her experience is that of sex trafficking. If the bride is treated as a domestic servant by her new husband and/or his family, then this is a form of labour trafficking.
Survival sex
In survival sex, the victim is not necessarily controlled by another person but feels they have to perform sexual acts to obtain basic commodities to survive. In addition to money, persons engaging in survival sex may trade sexual favours for food, shelter, or drugs. The most reported cases are those of youth that perform sexual acts for shelter or a place to sleep. Those who perform the trafficking include immediate family, boyfriends, employers, and strangers. Those who are at a higher risk of survival sex include runaways, homeless youth, foster kids, and orphans.
Who
is most at risk of sex trafficking?
When people think or talk about sex trafficking a very common question people will ask is, ‘Where do they find people to traffic?’ In many cases, traffickers will scope girls out at malls and parties. They also often seek out female runaways from their neighbourhood. Many of the girls they look for have been physically or sexually abused, have low self-esteem, struggle with drug and alcohol dependency, or are seeking a home/family environment.
Traffickers are using the internet and social media at an increasing rate to find victims, research potential victims, control their victims and advertise their victims. Traffickers also use social media posts to establish patterns and track the locations of potential victims. Traffickers often target people who post things that indicate that they are depressed, have low self-esteem or are angry with their parents.
Vulnerable populations are frequently targeted by traffickers, including runaway and homeless youth, as well as victims of domestic violence, sexual assault, war, or social discrimination.
How to prevent sex trafficking
Social media can be used for recruiting victims, but it can also be a useful tool in preventing sex trafficking. Since teenagers are constantly going through X (Twitter) and Instagram, posting possible prevention methods and information on the topic is a great way to inform your peers. It is also a fast way of posting potential dangerous/suspicious areas to avoid.
Small but crucial safety tips should be taught in school and at home for children to be more cautious and aware of their surroundings when they could be in danger.
One of the most common places for abduction/coercion are parking lots, especially if it is dark outside and there are not many people around. It is important to always be looking at your surroundings if you are in this position.
PORNOGRAPHY
Pornography (porn) has been peddled in the last few decades as harmless, natural, and innocent. Many label pornography as acceptable, but the truth is: pornography is harmful. It can entwine a person so tightly, that it feels like there is no way to ever be free from its grasp. The biggest reason that pornography is so dangerous is because it doesn’t leave physical evidence of its presence. There are too many ways to hide its usage. The other reason is that people refuse to acknowledge it except in hushed whispers – which doesn’t exactly create an environment where you can feel like it is acceptable to find help if it becomes a problem for you.
Who consumes pornography?
The average age of introduction is 11 years old. That means that many children see it earlier than that. Many are first introduced to pornography by accidentally stumbling across it online. Porn sites and streaming services form a shockingly large percentage of all online material. Unfortunately, most teens aren’t properly informed or prepared for it and therefore the primary pornography consumer group is boys between ages 12 and 17.
Pornographers may also disguise their sites (stealth sites) with common brand names, including Disney, Barbie, ESPN, etc., to entrap children. They know that porn is addictive and they want to catch people at the earliest ages possible so that they will have a customer for life. And child molesters often use pornography to seduce their prey, to lower the inhibitions of the victim, and to serve as an instruction manual. Pornography companies know what they’re doing.
So, coming across pornography for most teens is pretty much inevitable; it is how you deal with it that counts. The first line of defence is implementing an internet filter. It makes accidental exposure nearly impossible and makes it much more difficult to access material intentionally.
Pornography and addiction
Studies show pornography is progressive and addictive for many. Online pornography is giving rise to a new form of sexual compulsiveness. A substantial portion of online-porn regulars develop sexual behaviour that disrupts their lives. The internet is the crack cocaine of sexual addiction; pornography consumption can be as mood-altering and as addictive as drugs.
It acts like a drug by spiking the dopamine levels and other hormones in the brain. This gives you a high, which means that you will crash down later … which sends you into a depression of self-loathing and regret over what you just witnessed.
Pornography and relationships
Pornography distorts the natural development of personality. If the early sexual stimulus is pornographic images, the adolescent can become conditioned to become aroused through images. Once this pairing is rewarded a number of times, it is likely to become permanent. The result to the individual is that it becomes difficult for that person to seek out relations with appropriate people in real life.
Men who view pornography are more likely to suffer from erectile dysfunction than men who do not use pornography. People who view porn regularly are less likely to get married than those who do not. This is because users see porn as a substitute for marital sexual gratification.
Porn portrays women as nothing more than objects of sexual pleasure and makes men out to be nothing but sexual prowlers. It limits what it means to be a man or a woman to merely your sexuality and distorts your idea of gender roles.
How pornography changes the brain
Though many people use porn to relax or relieve stress, it can actually cause more mental health issues in both men and women such as anxiety, depression, insecurity, and body image issues, to name a few. It affects a person’s life, causing loss of motivation, self-esteem, and overall shame. Though many porn users begin using porn which aligns with their morals and sexual tastes, porn, over time, can alter sexual tastes so that the users believe the acquired tastes are natural. Thus, porn essentially rewires the brain with frequent use.
Pornography and divorce
The internet plays an increasingly significant role in recent divorces. Whereas pornography used to have an almost non-existent role in divorce before the internet, now online pornography has been shown to increase marital infidelity by 300 percent, according to a 2004 study in Social Science Quarterly. People who use porn are more likely to feel less love for their spouse/ partner and are more dissatisfied with their spouse/partner than people who do not use porn.
Pornography and sexual assault
Research gathered over the past few decades demonstrates that pornography contributes to sexual assault, including rape and the molestation of children. The more people use pornography, the more likely they are to believe that violence against women is acceptable, research suggests. The study which drew this conclusion also noted an increase in overall aggression that came with pornography use.
A multibillion-dollar industry
To say that the porn industry is very profitable is an understatement; pornography is a multibillion-dollar-a-year industry. Pornography websites receive more traffic and visitors every month than Netflix, X (Twitter), and Amazon combined. And the size of the pornography industry is only growing bigger.
Lastly, the reality is that behind every porn star there is a real person. It is not a safe environment to work in: the industry is rife with physical abuse and most contract STIs.
Recovery from porn addiction
Recovery from a porn addiction is possible, but as with all forms of addiction, it is a long hard road to recovery. Those who seek help and have a trusted mentor or group to whom they can be accountable are for more likely to successfully beat the addiction.
HIV/AIDS
What is HIV/AIDS?
In short: AIDS is a chronic, life-threatening disease caused by HIV (a virus).
HIV is short for the human immunodeficiency virus. It is a type of virus which causes disease by infecting and killing blood cells central to the body’s immune system – which helps the body to defend itself against infection and disease. As these cells are progressively wiped out, the body becomes less and less able to defend itself against common illnesses.
AIDS is short for acquired immunodeficiency syndrome. It is the final stage of HIV infection where a person’s immune system has been weakened to the point where it can no longer fight disease. This leaves the body open to a wide range of potentially deadly diseases known as opportunistic infections. So strictly speaking, AIDS isn’t a specific illness but a collection of many different conditions in the body – thus syndrome.
As such, HIV can be considered the cause and AIDS the effect of the infection.
How do you get infected?
The virus is mainly transmitted through sexual intercourse (vaginal/anal/oral) but can also be passed down from an infected mother to her child:
• during pregnancy
• during childbirth
• during breastfeeding or acquired via infected blood:
• when getting a blood transfusion
• through the sharing of needles (e.g. during drug use)
• through needle-stick injuries (if you are a healthcare worker, for example).
Once you are infected, the virus remains in your body for life.
It is important to realise that you cannot get infected through:
• mosquito and other insect bites
• urine or sweat
• public toilets, saunas, showers, gym equipment, swimming pools or water fountains
• sharing towels, linen or clothing
• going to school with, socialising or working with HIV-positive people
• sharing cutlery or crockery
• sneezes or coughs
• touching, hugging, shaking hands with or dry kissing a person with HIV
• (sexual) contact with animals (HIV is strictly a human virus and isn’t carried by animals)
• breathing the same air as someone who has HIV
What are the symptoms?
While it is impossible to look at someone and know whether they have HIV, the majority of people will have some symptoms about three weeks after they become infected with the virus. The period after infection, but before the production of antibodies (causing the initial symptoms), is called the window period. During this time, an HIV test may be negative.
These initial symptoms usually last 1–2 weeks and may include the following:
• fever and night sweats
• aching muscles and tiredness
• sore throat
• swollen glands
• diarrhoea
• skin rash and ulceration of the inside surface of the mouth and genitals
• headache, sore eyes and sensitivity to light
HIV is regarded as a chronic disease because, after experiencing these initial symptoms, most people don’t have any other symptoms for many years. During this time, they may look and feel perfectly well. This explains why so many people are unaware that they are infected with HIV. But even though they feel healthy, they can still transmit the virus to others. This is why HIV/AIDS is often called the silent epidemic and why getting tested is so important. Only a blood or fluid sample can reveal the presence of the virus. The length of time it takes for HIV to become AIDS varies from person to person and depends on your access to treatment, health status and health-related behaviours. Therefore, if you are HIV-positive, you will need ongoing monitoring and regular clinic visits to determine the progression of the disease.
When symptoms associated with the advance of HIV to AIDS occur, they appear roughly in the following order:
• unexplained weight loss (more than 10% of body weight)
• swelling of glands in the neck, armpit or groin
• easy bruising
• recurring and unusual skin rashes (often itchy)
• a thick, white coating of the tongue or mouth (oral thrush) or vagina (vaginal thrush), which is severe and recurs
• ongoing vaginal discharge and pain in the lower abdomen
• sinus fullness and drainage
• recurrent herpes
• shingles
• persistent sore throat
• recurring fevers lasting more than 10 days without an obvious cause
• night sweats or chills
• persistent cough and/or shortness of breath
• persistent severe diarrhoea (longer than a month)
• changes in vision
• pain, loss of control and strength of muscles, paralysis
• discoloured or purplish growths on the skin or inside the mouth or nose
• difficulty concentrating, inability to perform mental tasks that have been done in the past, confusion, personality change
Is there a cure?
Although there currently isn’t a cure for HIV, antiretroviral therapy (ART) helps to keep the virus under control and enables people living with HIV to lead a full, productive life. ARTs also help to prevent the onward transmission of HIV, i.e. if you’re HIV-positive, and on ART, there is a lower risk of transmitting the disease to others.
If left untreated, the average survival time for a person with AIDS is between six and 19 months. By contrast, a 35-year-old started on antiretroviral therapy (ART) can achieve a life expectancy equal to that of the general population.
Ultimately, treatment is key to the avoidance of HIV-related illnesses and the restoration of immune function. Even in persons with advanced disease, the implementation of ART can suppress HIV’s ability to replicate.
Myths about HIV/AIDS
Myth: I’m HIV-positive – my life is over.
Fact: Thanks to ART, people with HIV can now live long and productive lives.
Myth: I would be able to tell if my partner is HIV-positive.
Fact: It is impossible to look at someone and know whether they have HIV. Many people don’t show symptoms for years. The only way to know for sure is to get tested.
Myth: Male circumcision prevents HIV.
Fact: Circumcision lowers the risk of female-to-male sexual transmission of HIV by about 60%. However, it does not prevent HIV.
Myth: I can get cured if I have sex with a virgin.
Fact: There is no cure for HIV/AIDS.
Myth: I can get cured if I have sex with someone who is HIV-negative.
Fact: In all likelihood, you will infect your partner. There is no cure for HIV/AIDS.
Myth: If I test for HIV while I’m taking ART and my result is negative, it means that I am HIV-negative.
Fact: Being on any form of ART will give a false-negative result. You are still HIV-positive.
Myth: If I have HIV, I can’t have a baby.
Fact: It’s possible to have a baby if you have HIV, as long as your viral load is suppressed for at least six months before conception and it remains suppressed.
How do I prevent myself from getting infected?
Know your HIV status. If you don’t get tested, you won’t know if you’re HIV-positive or not. During the first three months of infection (the window period), it is hard to pick up the virus in the body. That’s why testing every six months is the best way to be sure.
• Avoid having sex. This isn’t easy for most people, but it is the one way of making sure that you don’t become HIV-positive as a result of sexual contact.
• Stay away from drugs. Note that one of the consequences of drug use is also that being high can make you forget about the rules of safe sex.
• Avoid blood contact. If you are helping a bleeding person, avoid getting any of their blood into any sores or cuts you may have on your skin. Also protect your eyes and mouth. There should be gloves in all first-aid kits – use them.
• Consider circumcision. This procedure, in which the foreskin of the penis is removed, has been shown to reduce the risk of HIV transmission from women to men.
• Take action if you have been exposed to HIV. Post-exposure prophylaxis (PEP) means taking antiretroviral treatment after you have been exposed to HIV. It must be taken within 72 hours of exposure and reduces your chances of becoming HIV-positive. PEP is often given to people who work in a medical environment (after a needle-prick incident) and to those who have been sexually assaulted. PEP must be taken for 28 days and has some side effects, such as nausea. Note that it is not a substitute for normal HIV preventative measures.
• These days, there is also much focus on treatment as prevention (TasP). This refers to HIV prevention methods and programmes that use antiretroviral treatment (ART) to decrease the risk of HIV transmission. Experts now know that if an HIV-positive person’s viral load is so suppressed that it is undetectable, they are unlikely to pass the virus on to others.
SEXUALLY TRANSMITTED INFECTIONS (STI s )
What are STIs?
Sexually transmitted infections (STIs) – sometimes also called sexually transmitted diseases (STDs) – are diseases that are spread by sexual contact. STIs can cause severe damage to your body – even death. Except for colds and flu, STIs are the most common contagious (easily spread) infections in the world, with millions of new cases each year.
STIs affect both men and women, but in many cases the health problems they cause can be more severe for women. If a pregnant woman has an STI, it can cause serious health problems for the baby.
How are STIs transmitted?
A person with an STI can pass it to others through contact with skin, genitals, mouth, rectum, or bodily fluids. Anyone who has sexual contact – vaginal, anal, or oral sex – with an infected person, may get an STI. Some STIs, such as hepatitis, can also be transmitted without sexual contact, by coming into contact with an infected person’s blood. Others, such as gonorrhoea, can only be transmitted through sexual contact.
Sometimes STIs may not cause symptoms (asymptomatic STIs), but even if there are no symptoms, your health can be affected, and you can pass the infection on.
How do you prevent getting infected?
Thinking or hoping a sexual partner doesn’t have an STI is no protection – you need to know for sure. And although condoms, when properly used, are highly effective in reducing transmission of some STIs, no method is foolproof.
The only reliable way to avoid infection is to not have any anal, vaginal, or oral sex.
What causes STIs?
STIs are caused by bacterial, yeast, parasitic or viral infections. There are more than 20 types of STIs. Antibiotics can treat STIs caused by bacteria, yeast, or parasites. There is however no cure for STIs caused by a virus, but medicines can often help with the symptoms and keep the disease under control. Some of the most common types of STIs include:
• chlamydia
• gonorrhoea
• genital herpes
• human immunodeficiency virus (HIV)
• human papillomavirus (HPV)
• syphilis
What happens when an STI goes untreated?
If untreated, STIs can increase your risk of acquiring another STI such as HIV. This happens because an STI can stimulate an immune response in the genital area or cause sores – either of which might raise the risk of HIV transmission. Some untreated STIs can also lead to infertility, organ damage, certain types of cancer or death.
STI symptoms aren’t always obvious. If you think you have STI symptoms or if you think you may have been exposed to an STI, see a doctor immediately. It is essential to be evaluated, and – if diagnosed with an STI – get treated. It is also essential to inform your partner so that they can be evaluated and treated.
Who is most vulnerable to contracting an STI?
The following factors increase the risk of getting an STI:
• having more than one sexual partner
• having a sexual partner who has or has had more than one sexual partner
• having sex with someone who has an STI
• having a history of STIs
• using intravenous drugs (injected into a vein) or having a sexual partner who uses intravenous drugs
SEXUALLY TRANSMITTED INFECTION (STI)
Chlamydia [bacterial]
AFFECTED AREA
genitals
SYMPTOM ONSET
1–3 weeks after exposure
Gonorrhoea [bacterial]
genitals mouth throat eyes anus
Trichomoniasis [parasitic]
men: urinary tract women: vagina
10 days to several months after exposure
Genital herpes [viral] (highly contagious)
genitals
5–28 days after exposure
a few weeks after exposure (once-off or recurrent)
SYMPTOMS
Mild and passing, thus easily overlooked:
• Painful urination
• Lower abdominal pain
• Discharge from penis/vagina
• Painful sex
• Bleeding between periods
• Testicular pain
• Discharge from penis/vagina
• Painful/swollen testicles
• Painful or burning urination
• Anal itching
• Painful bowel movements
• Bleeding between periods/heavy periods
Mild to severe symptoms:
• Discharge from penis
• Painful urination
• Painful sex
• Strong vaginal odour
• Irritation or itching of vagina/ inside penis
• Vaginal discharge: clear/white/ greenish/yellowish
Possibly NONE or only very mild:
• Painful urination
• Flu-like symptoms
• Pain/itching in the genital area, buttocks, and inner thighs
• Small red bumps becoming blisters or ulcers on the genitals, anus and nearby areas (not always)
High risk human papillomavirus (HPV) [viral] (very common)
NONE or … women: cervix
cancer can take up to 20 years after infection to develop
NO SYMPTOMS in men and women, but …
Heightened risk for women to develop cervical cancer
SEXUALLY TRANSMITTED INFECTION (STI)
Genital warts [viral]
AFFECTED AREA
SYMPTOM ONSET SYMPTOMS
genitals anus mouth throat within weeks/ months/years of exposure
Hepatitis A, B & C [viral] liver several weeks after exposure
Possibly NONE, or …
• Discomfort/itching in genital area
• Bleeding during sex
• Small, flesh-coloured/grey swellings in genital area
• Cauliflower-like collection of warts (1mm–large clusters)
Possibly NONE, or …Inflamed liver, causing:
• Fatigue
• Nausea and vomiting
• Jaundice
• Loss of appetite
• Fever
• Dark urine
• Muscle/joint pain
• Itching
• Abdominal discomfort or pain
Syphilis [bacterial]
Primary syphilis (stage 1)
genitals anus skin mucous membranes
Secondary syphilis (stage 2) any body area
10 days to 3 months after exposure
A single small painless sore [chancre] – where the infection was first transmitted (rectum/tongue/ lips/genitals)
3–6 weeks after the chancre
Latent syphilis (stage 3)
NONE infectious phase: less than 2 years after infection; dormant phase: 2+ years after infection
Lasting a few weeks or recurring over a year:
• Fever
• Enlarged lymph nodes
• Fatigue
• Soreness and aching
• Rash (rough, red/reddish-brown, penny-sized sores)
NONE
SEXUALLY TRANSMITTED INFECTION (STI)
AFFECTED AREA
Tertiary syphilis (stage 4) internal organs
SYMPTOM ONSET
years after first infection BUT this stage doesn’t always develop!
Neurosyphilis nervous system at any stage when the bacteria spreads to the nervous system
Congenital when a pregnant mother passes it on to her unborn infant
HIV [viral]
SYMPTOMS
Organ damage, causing:
• Lack of coordination
• Numbness
• Paralysis
• Blindness
• Dementia
• Death
Possibly NONE, or …
• Headache
• Behavioural changes
• Movement problems
Disabling/life-threatening
[see separate section on page 40]
ALCOHOL USE AND ADDICTION
Alcohol is a legal, controlled substance. It is a central nervous system (CNS) depressant, so it slows down mental and bodily processes. With the first drink of alcohol, users may experience a decrease in anxiety and lowered inhibitions. It also has a broad range of side effects, from loss of coordination to slurred speech. Alcohol is commonly consumed as a drink in various forms, including beer, wine and hard liquor.
Not everyone who drinks is an alcoholic, but anyone whose life is negatively affected by alcohol on a consistent basis is considered having alcohol use disorder (AUD).
What is alcohol use disorder (AUD)?
Alcohol use disorder is a chronic disease that affects your brain. Sometimes genes passed down to you from your parents can put you at risk. However, your environment or psychological make-up also play a significant role.
How do you know when you have crossed the line from alcohol use to alcohol abuse and even addiction?
Because alcohol is legal and widely accepted in society, it can be hard to tell the difference between casual use and abuse. In general, any usage of alcohol that results in negative consequences is considered abuse.
Some of the negative consequences of heavy drinking include:
• physical harm or illness
• strained relationships
• problems at work or school
• financial difficulty
When abuse becomes more frequent, it can escalate into an addiction.
Signs that someone may have alcohol use disorder (AUD) include:
• an uncontrollable urge to drink
• lack of control over how much you drink
• negative thoughts when you are not drinking alcohol
• drinking in risky situations
• drinking that interferes with fulfilling obligations
• continuing to drink even though it causes problems or makes them worse
• stopping or doing fewer important activities because of alcohol
The more of these that describe you, the more severe your AUD is likely to be:
• you can’t relax or fall asleep without drinking
• you need a drink in the morning to get going
• to be social, you have to drink
• alcohol serves as your escape from feelings
• after drinking, you drive
• you mix alcohol and medications
• you drink when you are pregnant or caring for small children
• when loved ones ask how much you drink, you don’t tell the truth
• you hurt people or become angry when you drink
• it is tough for you to remember what you did when you were drinking
• your responsibilities suffer because of your drinking
• drinking has caused you legal problems
• you tried to stop drinking but failed
• you can’t stop thinking about drinking
• to feel the effects of alcohol, you have to drink more and more
• you have withdrawal symptoms after you stop drinking for too long, like shakiness, nausea, trouble sleeping, or seizures
Binge drinking
A subset of problem drinkers – binge drinkers – are men who consume five or more alcoholic drinks or women who consume four or more over a two-hour period. An infrequent binge drinker may be able to stop on his or her own. Someone addicted to alcohol, however, may want to stop drinking and not be able to without help. In many cases, prolonged binge drinking can develop into alcoholism.
Physical effects of AUD
Even a mild case of AUD can have a serious impact on your physical and mental health. Often, AUD causes other problems, which you in turn try to avoid by drinking. This creates a negative cycle.
In the short term, AUD can cause:
• memory loss
• hangovers
• blackouts
Long-term effects include:
• stomach problems
• heart problems
• cancer
• brain damage
• permanent memory loss
• pancreatitis
• high blood pressure
• cirrhosis, or scarring on your liver
You’re also more likely to take dangerous risks. This raises your chances of being injured or dying from:
• car accidents
• homicide
• suicide
• drowning
AUD affects those around you, too. Your drinking may damage relationships with loved ones because of anger problems, violence, neglect, and abuse. Women who are pregnant, risk having a miscarriage. Their baby is more likely to have foetal alcohol syndrome and a higher chance of dying from sudden infant death syndrome (SIDS).
Short-term effects
In the short term, drinking too much can be very dangerous, sometimes deadly. Effects can include:
• nausea
• vomiting
• headaches
• slurred speech
• impaired judgment
• anxiety
• insomnia
• trouble concentrating
• memory loss
• problems breathing
• coma
• death
Long-term consequences
Risk of significant personal harm is increased with chronic alcohol consumption. Alcohol abusers are at an increased risk of:
• mouth, oesophageal, throat, liver, and breast cancer
• heart problems
• brain damage
• weakened immune system
• liver disease
• pancreatitis
• ulcers
• thiamine deficiency
Teen alcohol abuse
Adults are not the only ones who can suffer from alcohol abuse. Many teenagers are at risk of developing an alcohol abuse problem due to the accessibility of the substance and peer pressure. Alcohol tops the list of drugs used by teenagers.
Many teenagers who choose to drink can easily develop an abuse problem due to binge drinking. Binge drinking is defined as drinking at least four drinks (for women) or five drinks (for men) in two hours or less.
Teenagers who have an alcohol abuse problem may exhibit signs and symptoms to indicate there is a problem. Teen alcohol abuse symptoms include:
• having alcohol paraphernalia
• smelling of alcohol
• low energy
• concentration problems
• problems with coordination
• mood swings
• changing social circles
• declining academic performance
• behavioural issues
Teen alcohol use may not seem like a huge issue, however, alcohol is considered a drug and must be treated as one. Most teenagers cannot handle the effects of alcohol and are not responsible enough to deal with it. While many parents and guardians assume other drugs, such as marijuana, are worse than alcohol, they must realise how easily accessible alcohol is, and how much damage it can do to a teen.
Teens who abuse alcohol are at an increased risk in several ways. Studies have shown teens that drink are more sexually active and participate in unprotected sex more often than teens who do not consume alcohol. These teens are also at an increased risk of becoming a victim of rape or assault. They may also get injured or die in car crashes involving alcohol.
Not only can alcohol abuse alter how a teen acts, it can also have adverse effects on the brain. Studies show that brain development continues past the teenage years. Alcohol abuse during the brain’s formative years can negatively impact how the brain develops and can also lead to learning problems. According to the US National Institute of Health, teens who abuse alcohol at a young age are much more likely to develop a dependency on alcohol when they get older.
Alcoholism treatment
It is important for people with alcohol abuse and addiction problems to get help as soon as possible. The earlier they get help, the better their chance of recovery. Many people who struggle with alcohol addiction find it difficult or impossible to quit without the help or support of others.
Alcohol treatment centres are designed to help individuals who are addicted or who abuse alcohol in a number of ways. Typically, treatment centres require an individual to stay at the centre for a specific amount of time. Many centres offer both long- and short-term treatment options.
During treatment, individuals go through detoxification (detox). Detoxification is the interventions used to keep a person safe as they readjust to a lack of alcohol in the body. Medical detox is extremely important for someone dependent on alcohol because withdrawal can cause delirium and potentially life-threatening seizures, along with other very serious symptoms.
Treatment centres are designed to provide support in the form of individual therapy, as well as group therapy and educational classes on addiction. During therapy sessions, alcoholics can explore the reasons behind their excessive alcohol consumption, as well as what they can do to overcome their abusive behaviour. Counsellors and therapists at treatment centres are trained to provide recovering individuals with the tools to resist cravings and maintain their sobriety.
Outpatient treatment is also an option for many alcoholics. Outpatient treatment centres and support groups like Alcoholics Anonymous are designed to provide recovering alcoholics with a place to explore their destructive behaviour. Many outpatient treatment centres provide group meetings, as well as other programmes to help recovering individuals overcome their issues. With outpatient treatment, individuals are not placed in a controlled environment and may be vulnerable to outside temptation during treatment. Typically, this type of treatment is ideal for those who have successfully completed an inpatient treatment programme and want a step-down level of care or those whose addiction is subjectively not as severe.
NICOTINE USE AND ADDICTION
Nicotine is a highly addictive substance found in tobacco – a plant grown for its leaves. Tobacco products can generally be divided into two types: smoked tobacco and smokeless tobacco. Smoked tobacco includes cigarettes, cigars, hookah, and e-cigarettes (vaping), while smokeless tobacco includes chewing tobacco, snuff, and tobacco gum. Passive or second-hand smoking is when you inhale nicotine just by being around people who are smoking.
How addictive is nicotine?
Nicotine is highly addictive. More than two-thirds of nicotine users will become dependent on the drug. And only six percent of smokers are able to quit in a given year.
Nicotine is unique because the drug’s intoxicating effects are less intense than most other substances. Perhaps this is the reason that nicotine addiction is the most common addiction worldwide. As a stimulant, nicotine increases levels of dopamine in the brain. This triggers euphoria, boosts mood and enhances memory. Although it is a stimulant, nicotine doesn’t produce the high levels of energy or euphoria that drugs like cocaine do. It stimulates adrenal glands, which causes a rise in blood pressure and respiration.
People addicted to tobacco products have a physical desire to continue using tobacco, but they also have a psychological desire because of memories associated with using. These memories trigger the urge to use tobacco.
Almost everyone who smokes or uses tobacco can remember how their addiction started and how they never intended to become addicted. Most people pick up nicotine products based on a cultural perception that it is cool. Most people who use tobacco started in their teens. Of those who smoke, 90 percent started by the age of 18.
For those who started smoking at a young age, quitting later in life can be harder than for those who started smoking when they were older – regardless of how many years they have been smoking. This is because addiction changes the biochemical make-up of the brain, so it follows that it becomes harder to quit the earlier a person starts using. Young people are more susceptible to forming an addiction. This is because addictive substances like tobacco activate the brain reward system, which is still developing in teens. This part of the brain plays a huge role in the production of memories and addictive behaviour.
Ironically, most people with an addiction to nicotine are aware of the harm tobacco causes yet they continue to use the substance. This abusive behaviour is characteristic of addiction. Another feature of addiction is that you build up a tolerance to the substance, needing higher doses to feel the same initial effect. The good news is that the sooner a person decides to quit, the easier it will be. But no matter how long a person has been addicted to tobacco, quitting is absolutely possible and has tangible health and financial benefits.
Recognising nicotine addiction
Because of the widespread use of cigarettes, it can be difficult to spot an actual addiction to nicotine. Many people addicted to nicotine are in denial. They may be social smokers who only use tobacco while they are out with friends, or they may be smokers who believe they can quit when they are ready. Recognising the signs of an addiction to nicotine is important to overcoming denial and getting over the addiction.
Common signs of addiction:
• Requiring more tobacco to feel satisfaction or using tobacco in larger amounts than intended
• Going out of your way to get tobacco
• Having a desire to quit or decrease use but being unable to do so
• Continued tobacco use despite awareness of consequences and health risks
• Experiencing physical withdrawal symptoms. Withdrawal from nicotine occurs because the addicted brain can no longer naturally produce adequate levels of certain chemicals, like dopamine. These symptoms can crop up in as little as two hours after not using tobacco and tend to be the worst 2–3 days after quitting. These include:
◊ trouble concentrating
◊ anxiety and panic attacks
◊ depression
◊ trouble sleeping
◊ irritability and frustration
◊ increased appetite and weight gain
◊ headaches
• Experiencing psychological symptoms. Once a person’s brain is rewired for tobacco addiction, scenarios that are associated with tobacco use (psychological triggers) can cause cravings for and intense urges to use tobacco. Common triggers for people with a nicotine addiction are:
◊ driving
◊ drinking
◊ music
◊ work
The risks of nicotine use
Exposure to nicotine can be fatal. Tobacco causes nearly 6 million deaths each year. There are more tobacco-related deaths each year than all deaths from illicit drugs, alcohol, car accidents and murders combined. On average, smokers live 14 years less than non-smokers. Most people, including those who use tobacco, are aware of the serious health risks associated with using tobacco. It is unsurprising that about 70% of tobacco users have a desire to quit. But quitting, no matter how long you have been using tobacco, significantly reduces your odds of having tobacco-related health issues.
Negative side effects of nicotine use include:
• coughing or wheezing
• breathing problems
• increased heart rate
• chest pain
• heart palpitations
• dizziness or confusion
• nausea, sweating or diarrhoea
• decreased appetite
• excess amounts of saliva and phlegm
• tremors
Some of the long-term health risks associated with tobacco use include:
• infertility
• COPD (chronic obstructive pulmonary disease)
• stroke
• asthma
• type 2 diabetes
• heart disease
• cancer (mouth / oesophageal / lung)
• while nicotine does not cause cancer, tobacco products contain a variety of cancer-causing compounds, such as tar and acetaldehyde.
Teens and nicotine
Fewer people are smoking these days because an increasing number of teens aren’t picking up tobacco. Teens educated about the health risks involved often won’t pick up tobacco in the first place. Those in the 12 to 17 age group have some of the lowest rates of smoking compared to other demographics. Unfortunately, the rates of tobacco use in the 18 to 25 age group makes up some of the highest rates of use.
In recent years, more teens have turned to vaping. This method of nicotine use involves inhaling the vapour produced by an electronic cigarette or similar device. Adolescents can easily become addicted to tobacco products. Teens are particularly at risk for the long-term effects of nicotine because their brains are still developing. This makes them more vulnerable to addiction than adults.
Treating nicotine addiction
A combination of medications and behavioural treatments can assist people in abstaining from nicotine products. Behavioural therapies use self-help literature and counselling to teach people to recognise triggers that contribute to continued nicotine use. Many smokers participate in nicotine replacement therapies that help people relieve withdrawal symptoms and slowly taper their exposure to nicotine. The products include chewing gum, transdermal patches, inhalers, lozenges and nasal sprays.
DRUG ABUSE AND ADDICTION
Drug addiction is a chronic disease characterised by drug seeking and drug use that is compulsive, or difficult to control, despite harmful consequences. People from all walks of life can experience problems with their drug use, regardless of age, race, or background. Abusing drugs can lead to addiction – leaving you feeling helpless, isolated and ashamed.
Drug abuse and addiction is less about the type of substance consumed and more about the consequences of that drug use. If your drug use is causing problems in your life – at work, school, home, or in your relationships – you likely have a drug abuse or addiction problem.
Recognising that you have a problem is the first step on the road to recovery, one that takes tremendous courage and strength. If you are ready to seek help, you can overcome your addiction and build a satisfying, drug-free life for yourself.
Why do people abuse drugs and risk getting addicted in the first place?
Some experiment with drugs:
• out of curiosity
• to have a good time
• because friends are doing it
• to ease problems such as stress, anxiety or depression
If the drug fulfils a valuable need, you may find yourself increasingly relying on it. You may take illegal drugs to calm or energise yourself or make you more confident. If you are using drugs to fill a void in your life, you are more at risk of addiction. To maintain a healthy balance in your life, you need to have positive experiences and feel good about your life without any drug use.
Drug abuse may start as a way to connect socially. People often try drugs for the first time in social situations with friends and acquaintances. A strong desire to fit into the group can make it feel like doing drugs with them is the only option.
Abuse of and addiction to prescription medication
It is not just illegal drugs, such as cocaine or heroin, that can lead to addiction. Prescription medications can cause similar problems. An addiction to opioid painkillers can be so powerful that it has become the major risk factor for heroin abuse.
Many people initially start taking prescription drugs to cope with a specific medical problem –to relieve pain, cope with panic attacks, or improve concentration at school or work. However, over time increased doses are needed to achieve the same level of efficacy. So some users can become physically dependent, experiencing withdrawal symptoms if they try to quit. One of the earliest warning signs of a developing problem is going through the medication at a faster-than-expected rate.
To avoid developing problems with a prescription medication, it is important to take it only as directed, use the lowest dose for the shortest period possible, and to talk to your doctor about other methods of treating the problem. Being aware of any signs of dependency can help identify prescription drug problems at an early stage and help to prevent them progressing into an addiction.
In other cases, people start abusing medication not prescribed for them to experience a high, relieve tension, increase alertness, or improve concentration.
Drug addiction and the brain
While each drug produces different physical effects, all abused substances share one thing in common: repeated use can alter the way the brain functions:
• Taking the drug causes a rush of the hormone dopamine in your brain, which triggers feelings of pleasure. Your brain remembers these feelings and wants them repeated. But you need to take more and more of the substance to achieve the same feelings of pleasure – an effect known as tolerance. These brain adaptations often lead to the person becoming less and less able to derive pleasure from other things they once enjoyed, like food, sex or social activities.
• Long-term use also causes changes in other brain chemical systems and circuits (not only the reward system), affecting functions that include memory, learning, decision-making, stress, etc. The changes in your brain will interfere with your ability to think clearly, exercise good judgment, control your behaviour and feel normal without drugs.
• When you become addicted, the substance takes on the same significance as other survival behaviours, such as eating and drinking.
• No matter which drug you are addicted to, the uncontrollable craving to use grows more important than anything else, including family, friends, career, and even your own health and happiness.
• The urge to use is so strong that your mind finds many ways to deny or rationalise the addiction. You may drastically underestimate the quantity of drugs you are taking, how much it impacts your life, and the level of control you have over your drug use.
How drug abuse and addiction develop
There is a fine line between regular drug use and drug abuse and addiction. Very few drug abusers or addicts are able to recognise when they have crossed that line. While the frequency or amount of drugs consumed do not necessarily constitute drug abuse or addiction, they can often be indicators of drug-related problems.
As drug abuse takes hold, you may miss or frequently be late for work or school, your job performance may progressively deteriorate, and you may start to neglect social or family responsibilities. Your ability to stop using is eventually compromised. What began as a voluntary choice has turned into a physical and psychological dependence. Eventually drug abuse can consume your life, stopping social and intellectual development. This only reinforces feelings of isolation.
Myths about drug addiction
Myth: Overcoming addiction is simply a matter of willpower. You can stop using drugs if you really want to.
Fact: Prolonged exposure to drugs alters the brain in ways that result in powerful cravings and a compulsion to use. These brain changes make it extremely difficult to quit by sheer force of will.
Myth: Using drugs like opioid painkillers are safe since they’re prescribed by doctors.
Fact: Short-term medical use of opioid painkillers can help to manage severe pain after an accident or surgery, for example. However, regular or longer-term use of opioids can lead to addiction. Misuse of these drugs or taking someone else’s medication can have dangerous –even deadly – consequences.
Myth: Addiction is a disease; there’s nothing that can be done about it.
Fact: Most experts agree that addiction is a disease that affects the brain, but that doesn’t mean anyone is helpless. The brain changes associated with addiction can be treated and reversed through therapy, medication, exercise, and other treatments.
Myth: Addicts have to hit rock bottom before they can get better.
Fact: Recovery can begin at any point in the addiction process – and the earlier, the better. The longer drug abuse continues, the stronger the addiction becomes and the harder it is to treat. Don’t wait to intervene until the addict has lost everything.
Myth: You can’t force someone into treatment; they have to want help.
Fact: Treatment doesn’t have to be voluntary to be successful. People who are pressured into treatment by their family, employer, or the legal system are just as likely to benefit as those who choose to enter treatment on their own. As they sober up and their thinking clears, many formerly resistant addicts decide they want to change.
Myth: Treatment didn’t work before, so there’s no point trying again.
Fact: Recovery from drug addiction is a long process that often involves setbacks. Relapse doesn’t mean that treatment has failed or that sobriety is a lost cause. Rather, it is a signal to get back on track, either by going back to treatment or adjusting the treatment approach.
Common signs and symptoms of drug abuse and addiction
Although different drugs have different physical effects, the symptoms of addiction are similar.
Drug abuse:
• Neglecting responsibilities at school, work, or home (e.g. flunking classes, skipping work, neglecting your children).
• Using drugs under dangerous conditions or taking risks while high, such as driving while on drugs, using dirty needles, or having unprotected sex.
• Experiencing legal trouble, such as arrests for disorderly conduct, driving under the influence, or stealing to support a drug habit.
• Problems in your relationships, such as fights with your partner or family members, an unhappy boss, or the loss of friends.
Drug addiction:
• You’ve built up a drug tolerance. You need to use more of the drug to experience the same effects you used to attain with smaller amounts.
• You use drugs to avoid or relieve withdrawal symptoms. If you go too long without drugs, you experience symptoms such as nausea, restlessness, insomnia, depression, sweating, shaking, and anxiety.
• Loss of control over your drug use. You often do drugs or use more than you planned, even though you told yourself you wouldn’t. You may want to stop using, but you feel powerless.
• Your life revolves around drug use. You spend a lot of time using and thinking about drugs, figuring out how to get them, or recovering from the drug’s effects.
• You have abandoned activities you used to enjoy, such as hobbies, sports, and socialising, because of your drug use.
• You continue to use drugs, despite knowing that it is hurting you. It is causing major problems in your life – blackouts, financial issues, infections, mood swings, depression, paranoia – but you use anyway.
Warning signs of drug abuse in teens
Drug abusers often try to conceal their symptoms and downplay their problem. If you are worried that a friend or loved one might be abusing drugs, look for the following warning signs:
Physical warning signs of drug abuse or addiction:
• bloodshot eyes, pupils larger or smaller than usual
• changes in appetite or sleep patterns
• sudden weight loss or weight gain
• deterioration of physical appearance or personal grooming habits
• unusual smells on breath, body, or clothing
• tremors, slurred speech, or impaired coordination
Behavioural warning signs of drug abuse or addiction:
• drop in attendance and performance at work or school
• unexplained financial problems; borrowing or stealing
• engaging in secretive or suspicious behaviours
• sudden change in friends, favourite hangouts and hobbies
• frequently getting into trouble (fights, accidents, illegal activities)
Psychological warning signs of drug abuse or addiction:
• unexplained change in personality or attitude
• sudden mood swings, irritability or angry outbursts
• periods of unusual hyperactivity, agitation or giddiness
• lack of motivation; appears lethargic or spaced out
• appears fearful, anxious or paranoid
Symptoms of commonly abused drugs
• Marijuana: Glassy, red eyes; loud talking or inappropriate laughter followed by sleepiness; loss of interest or motivation; weight gain or loss.
• Stimulants (including amphetamines, cocaine, crystal meth): Dilated pupils; hyperactivity; euphoria; irritability; anxiety; excessive talking followed by depression or excessive sleeping at odd times; may go long periods of time without eating or sleeping; weight loss; dry mouth and nose.
• Inhalants (glues, aerosols, vapours): Watery eyes; impaired vision, memory and thought; secretions from the nose or rashes around the nose and mouth; headaches and nausea; appearance of intoxication; drowsiness; poor muscle control; changes in appetite; anxiety; irritability; lots of cans/aerosols in the trash.
• Hallucinogens (LSD, PCP): Dilated pupils; bizarre and irrational behaviour including paranoia, aggression, hallucinations; mood swings; detachment from people; absorption with self or other objects; slurred speech; confusion.
• Heroin: Contracted pupils; no response of pupils to light; needle marks; sleeping at unusual times; sweating; vomiting; coughing; sniffling; twitching; loss of appetite.
• Opioid painkillers (including OxyContin, Vicodin, Norco): Drooping eyes, constricted pupils even in dim light; sudden itching or flushing; slurred speech; drowsiness, lack of energy; inability to concentrate, lack of motivation, decline in performance at work or school; neglecting friendships and social activities.
• Anti-anxiety medications, sedatives, and hypnotics (including Xanax, Valium, Ambien): Contracted pupils; drunk-like, slurred speech; difficulty concentrating; clumsiness; poor judgment; drowsiness; slowed breathing.
• Prescription stimulants (including Ritalin, Concerta, Adderall, Dexedrine): Dilated pupils; reduced appetite; agitation; anxiety; irregular heartbeat; high body temperature; insomnia; paranoia.
Why do some people become addicted to drugs while others don’t?
No one factor can predict if a person will become addicted to drugs. A combination of factors influences risk for addiction. The more risk factors a person has, the greater the chance that taking drugs can lead to addiction.
• Biology. The genes that people are born with account for about half of a person’s risk for addiction. Gender, ethnicity, and the presence of other mental disorders may also influence risk for drug use and addiction.
• Environment. A person’s environment includes many different influences, from family and friends to economic status and general quality of life. Factors such as peer pressure, physical and sexual abuse, early exposure to drugs, stress, and parental guidance can greatly affect a person’s likelihood of drug use and addiction.
• Development. Genetic and environmental factors interact with critical developmental stages in a person’s life to affect addiction risk. Although taking drugs at any age can lead to addiction, the earlier that drug use begins, the more likely it will progress to addiction. This is particularly problematic for teens. Because areas in their brains that control decision making, judgement, and self-control are still developing, teens may be especially prone to risky behaviours, including trying drugs.
Recovery from drug addiction
Professional help is essential for full recovery from drug addiction. Ideally, this will involve an extended stay in a drug rehabilitation centre, followed by long-term support with group and individual therapy. Narcotics Anonymous offers free, long-term group support for recovering drug addicts and is active in most countries.
In a drug rehab centre, as with treatment for alcohol addiction, individuals go through detoxification. Detoxification is the set of interventions used to keep a person safe as they readjust to a lack of drugs in the body. Medical detox is extremely important for someone dependent on drugs because withdrawal can cause delirium and potentially life-threatening seizures, along with other very serious symptoms.
Treatment centres are designed to provide support in the form of individual therapy, as well as group therapy and educational classes on addiction. During therapy sessions, addicts can explore the reasons behind their drug abuse, as well as what they can do to overcome their abusive behaviour. Counsellors and therapists at treatment centres are trained to provide recovering individuals with the tools to resist cravings and maintain their sobriety.
SOCIAL MEDIA USE AND ADDICTION
If you use Facebook, TikTok, X (Twitter), Pinterest, Instagram, Snapchat, YouTube, Tumblr, WhatsApp, or Reddit (to name just a few), you are a user of social media.
There is absolutely nothing wrong with using social media. After all, technologies such as Skype, Instagram, and Facebook allow us to stay in contact with family and friends on the other side of the planet. But when someone spends hours a day updating their status, uploading pictures, commenting on walls, playing games or searching for friends to add … it is safe to say there is a problem. If you spend unhealthy amounts of time on these platforms, you may have become a social media addict – it is just that you don’t know it yet.
Don’t be fooled: behavioural addictions, like spending time on social media, can be serious. Often it goes hand-in-hand with other internet applications that a teenager is addicted to, such as online gaming or sexting. The focus becomes the digital world and the person is less and less engaged in the physical world of relationships.
What is social media addiction?
Although social media addiction is not a formal clinical diagnosis, it is fair to say that many people spend far too much time on social media and may at the very least describe themselves as being obsessed, if not addicted. In recent years the mental health community has become increasingly interested in the impact that modern technology has on our lives.
Generally speaking, addiction is any compulsive behaviour that has a negative impact on someone’s life. In the case of social media addiction, it refers to someone compulsively using social media causing it to have a negative effect on them.
What makes social media addictive?
Whenever people give you a like, comment on your post, or share it, it makes you feel validated, as if they agree with you and your self-esteem is boosted. You also feel less alone, you feel a connection to others and that someone cares about you. This is because these likes/ comments/shares trigger the reward centre in your brain. Brain cells are stimulated to release dopamine – a chemical that signals other nerve cells to improve your mood. This is why it can be addictive.
MRI scans of the brains of subjects taken while talking about themselves reveal that self-disclosure communication activates the pleasure areas in the brain. Put simply, it makes people happy when they talk and think about themselves. And talking about yourself is a large part of what you do when you use social media.
These rewards and the pleasures you receive from using social media condition your mind to crave more. If sustained over the long term, it can quickly become a habit and grow into a full-blown disorder.
How do you know you are addicted to social media?
It is not that easy to tell if someone is a social media addict. If you spend a few hours a day checking updates and reading random posts, does that make you an addict? What if you mostly use social media to read news or find entertainment to pass the time – are you then also a social media addict?
Behavioural symptoms
If you want to know whether you are a social media addict, look at how you live your life and how you spend your time. Because social media addiction is classified as a habitual disorder, the signs can be identified from what you do each day. If you identify with most of the behaviour described below, there is a high chance that you are addicted to social media:
• social media is the first thing you check in the morning or whenever you are free
• you waste your time looking at nonsense and procrastinate other tasks
• you check in (share your location) everywhere you go
• you compulsively check notifications
• you only want to interact with and talk to your friends via social media and rarely socialise face-to-face (and video calls don’t count!)
• you tend to over-share (saying too much and regretting it afterwards) and lack healthy privacy
• you constantly monitor how many likes and shares your posts receive
• you spend so much time on social media that your relationships start to suffer
• you crave having internet connection when there is none available
• you take photos of almost everything and post them
• you use social media to forget about personal problems
• social media is your whole life; you lose interest in other activities and neglect responsibilities
Psychological symptoms
• You generally feel dissatisfied and depressed: One reason is that social media conjures up a perception that everyone else is always happy and living their best lives. You end up comparing your life to an unattainable ideal when all you see is people curating a perfect version of themselves. You find yourself also wanting to post jealousy-inducing updates of your own. Another reason you get depressed is because of the lack of real human contact. While social media does provide the convenience of connecting with others, one cannot entirely ignore our basic need as humans for physical interaction with others. Ironically the more time people spend on social media, the more socially isolated they become.
• You experience raised levels of anxiety: Social media addicts can never sit still when unoccupied. They obsessively check updates on their mobile phones or laptops. And if they do not have access to social media, it triggers feelings of anxiety and worry.
Other negative effects of social media
• Cyberbullying: People feel they can say whatever they want and get away with it on the internet, including on social media platforms. When people intimidate or threaten others online it is a very serious issue because the victim experiences huge amounts of stress – even resulting in suicide in some cases.
• Distraction and a drop in productivity: Not only are people unable to focus on work because of constant notifications interrupting them, but they often put off starting to work in the first place because they would rather be on social media. If you spend your most productive hours on social media, you will have less motivation and energy to work on more important tasks later.
• Fatigue and stress: Staring at your computer screen or mobile phone for hours on end will make you feel tired and stressed. Social media is overstimulating on a sensory level – there are so many things to check out and to see – and this is tiring. Instead of resting properly when you take a break from work, you go on social media and become more fatigued and stressed out as a result.
• Health issues:
◊ blurry vision due to strained eyes and/or headaches from staring at the screen for long hours
◊ back and neck pain from constantly bending your neck down to look at your phone
◊ carpal tunnel syndrome in your wrist from repetitive motion of your hands and arms when typing on the phone or computer
◊ sleep deprivation as a side effect of disturbed sleep, which results from checking social media just before going to bed
How to overcome social media addiction?
Like all other illnesses and problems, there are cures and solutions to social media addiction. The key is to commit to following through. Make social media a tool that you control rather than it controlling your life. Some useful suggestions:
• Get rid of notifications: If social media accounts cannot notify you about any updates, there is a higher chance that you will not check them. Plus, if you always get distracted by notifications, you cannot concentrate well on your tasks at hand. It can cause negative feelings like stress and anger.
• Limit the time you spend on social media: Choose to spend only a certain amount of time a day on social media. Or allow yourself to only go onto the platform at a certain time of day. A good strategy is to restrict yourself from using social media in certain places, e.g. at the office, the dinner table, or the bedroom – get yourself an alarm clock instead of using your phone as an alarm. There are a number of apps designed to help you limit time spent on social media by logging you out or blocking you from using the platform when you exceed your allocated time.
• Delete apps from your mobile phone: If all else fails, delete the app from your mobile phone. Just delete the app so there is no way you can check updates or get notifications from the convenience of your smartphone. Using your computer for social media is less convenient. The effort it takes will automatically lower your desire to want to go onto social media.
• Keep yourself occupied: Keep yourself busy so that you will have no free time to check social media and not automatically pick up your smartphone. Replace free time spent on social media with other activities, e.g. sports or hobbies.
• Create your own reward system: Reward yourself every time you resist the urge to use social media or you successfully stay within the allowed time usage: praise yourself, get yourself a snack or do some other activity you enjoy. In so doing you are teaching your brain that there is something better than spending time on social media.
• Disconnect and unplug yourself: Instead of merely deleting social media apps, you can completely disconnect yourself from the internet or simply switch off your phone to unplug. When you have no way to access the internet, you avoid the temptation to use social media. It is a good idea to do this every evening and instead spend quality time with your family rather than mindlessly scrolling for updates.
• Get an accountability partner: Most people understand that they should decrease their time spent on social media, but they just can’t do it. Tell your parents, your siblings, your classmates and your friends to remind you to stop if they spot you spending time on social media platforms. This will create social pressure and force you to stop. It is highly effective because you are making a public commitment and others are helping you rather than leaving you to solve the problem all by yourself.
• Do a weekly self-reflection: Ask yourself what you have spent the most time on over the previous week. Review what you have accomplished and set goals for the following week. Asking these self-reflective questions allows you to evaluate yourself and keep yourself on track.

UK R4L V4 TRAINING MANUAL
