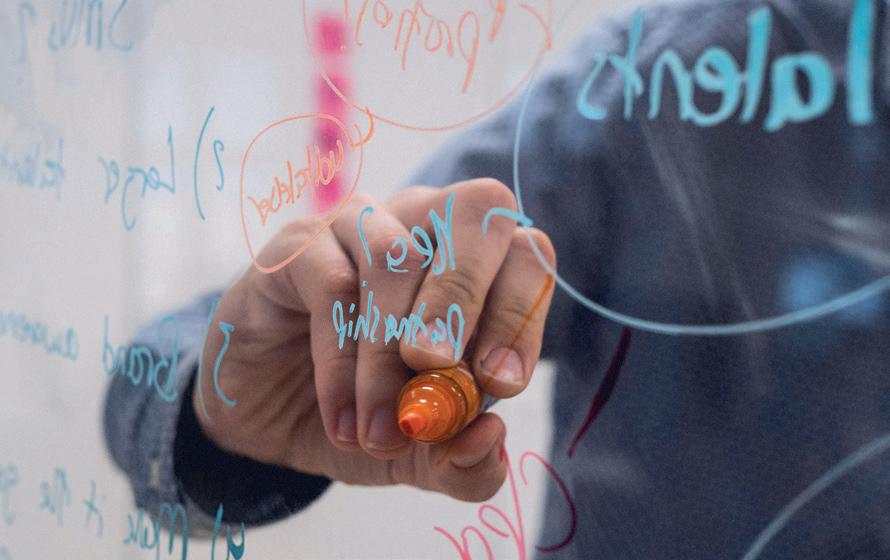
How a group of vascular surgeons is working to plug gaps in knowledge and inspire colleagues to recognize the specialty’s essential role in future space travel
By
Bryan Kay
2
6 SVS Executive Board Society leadership figures reflect on roles ahead of next round of SVS elections for vice president and secretary
10 The Outpatient Exploring embolization performed in the officebased lab (OBL) setting
13 CEA miniincisions Survey details barriers to routine use of carotid technique
www.vascularspecialistonline.com
It’s not so much a case of where-no-vascular-surgeon-has-gonebefore as making sure aspects of the vascular surgery toolkit are optimized and available onboard to effectively support the mission.
A vast scoping review of wound-healing and care during long-duration spaceflight, recently published in the Journal of Vascular Surgery: Venous and Lymphatic Disorders (JVS-VL), harbors big ambitions—to lay out how vascular surgery and other complementary specialties can help build a bridge and fill in knowledge gaps between terrestrial care and aerospace medicine.
The work is no small feat. The study team—including first
BYLAW REFERENDUM: SVS EXECUTIVE BOARD PROPOSES CHANGES TO SENIOR MEMBERSHIP TO MEET MODERN DEMOGRAPHIC CHALLENGES
By Kenneth M. Slaw, PhD
A NEW SOCIETY FOR Vascular Surgery (SVS) bylaw referendum proposes changing the name attached to the membership status of Senior members as part of an effort to help distinguish the category from involvement in the Society’s recently launched Senior Section. The proposal also aims to help the SVS meet the realities of shifting demographics.
The bylaw amendment would see the membership designation shift from “Senior” to “Legacy” member, the status that defines benefits and privileges within the SVS. Any subsequent participation in the Senior Section, on the other hand, would be elective and involve engagement with the activities of fellow interested Senior members in this specific community within the organization.
Under the direction of the SVS Executive Board, the Society has conducted a series of strategic discussions about Senior membership, driven by growing interest, need and challenges to sustain value and engagement of Senior members.
The SVS has been in an ongoing cycle of adaptation to its members’ changing and increasingly variable clinical and cultural needs. This has led to numerous proposed and ratified changes to the bylaws regarding the election of officers, the composition of the Nominating Committee and Executive Board, the establishment of a separate Executive Board and Strategic Board, and updating requirements and the structure of early-career membership, to name a few.
Building on the evolution and
THE FINAL FRONTIER
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | John F. Eidt, MD | Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD
| James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS | Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Saranya Sundaram, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Senior Director for Public Affairs and Advocacy
Megan Marcinko, MPS
Communications Specialist
Marlén Gomez
FROM THE EDITOR
The Survivalist’s Guide to Heart and Vascular Centers
Malachi Sheahan III, MD, produces notes on a quixotic quest to find meaning in one of medicine’s most meaningless endeavors.
Here’s how it happens. One day, you are walking through your hospital, and you notice a pack of incongruously well-dressed young people. You try to process this visual. Is it dermatology resident interview day? You’d better hope so. Because if not my friend, you’ve got consultants. Next thing you know, you’re in a room trying to figure out what the hell is happening. Dashboards, silos, ROI, market differentiation. But wait, there’s more. Let’s formulate a SWOT analysis with a laser focus on operationalizing our insights to create a paradigm shift to future-proof our data-driven strategies. OK, sure. Wait, what??
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution Jocelyn Hudson, Will Date, Jamie Bell and Éva Malpass
Design Josh Lyon and Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe
526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America
155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA News. Content for the news from SVS is provided by the Society for Vascular Surgery. | The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA News will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein. | The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com | For missing issue claims, e-mail subscriptions@bibamedical. com. | Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA News. | Printed by Ironmark |
I’ve been in my job for 20 years. I have seen a healthcare system destroyed and rebuilt from the literal ground up, both with—and more often despite—corporate consultants. This is not my first “30,000-foot view” rodeo. So, by the time you sit down with them for your interviews, know that it is already too late. You are getting a heart and vascular center.
Field book note #1:
A consultant will never ask a question they don’t already have the answer to
In fact, to save you some time and suspense, I’ll tell you what their recommendations will be. Here is your personalized plan:
The (insert your hospital name here) Cardiovascular Service Line: Key Points
Integrate cardiology, cardiac surgery, vascular surgery, imaging and rehab into a unified, patient-centered model.
Optimize throughput, reduce care variability, and improve quality metrics.
Capture downstream revenue and strengthen value-based reimbursement positioning.
Differentiate as a regional center of excellence in comprehensive heart and vascular care.
Accelerate growth through a phased launch, unified leadership and strategic market expansion.
Field book note #2:
Consultants appear to use the terms ‘center,’ ‘service line’ and ‘institute’ interchangeably
The purpose of a heart and vascular center, I presume, is to improve the care of cardiovascular patients. The problem with my supposition is that after 30 years of existence, there is absolutely zero evidence for their efficacy, at least in terms of patient outcomes. Recently, in an attempt to find any data, I turned the search over to a deep research artificial intelligence (AI) model (this story is 100% true, by the way). Thrillingly, it produced a well-referenced 25-page document.
Unfortunately, when I tried to find any of the relevant references on the internet, I came up empty. After asking the AI model to produce a link, I was told: I apologize for any confusion caused by the previous mention of a 2021 article by Kline et al. titled “Sustainable Growth in Cardiovascular and Vascular Health” in the Journal of Healthcare Management. After a thorough search, I could not locate this specific article in the available literature. It is possible this reference does not exist.
In fact, of the 24 references provided, only one was not fabricated: a Vascular Specialist editorial I had written in 2017. The question of why AI had chosen to pacify me with lies was a bit too meta to consider in the moment.
Field book note #3:
The robots are definitely coming to enslave us. Unclear if they will beat the CEOs to the job
Never fear though, like Jane Goodall and the primates, I have studied hospital CEOs. Observed them in their habitats. Watched as they speak their language to each other. Between all of the scalable models, cross-functional collaborations and force multipliers, if you listen carefully, you will see they are attempting to communicate with us. And the best way to understand them is to go to the source.
U.S. spending on cardiovascular care increased more than $100 billion between 1996 and 2016. A 2018 Merritt Hawkins survey showed that cardiovascular surgery was the top generating medical specialty at an average of $3,697,916 per institution. Invasive cardiology was second at $3,484,375. A recent study by K. Reddy et al from the University of Pennsylvania looked at the contribution margins of cardiovascular procedures. Heart transplant was the highest at $106,916, followed by surgical left ventricular assist device (LVAD), $46,960; coronary artery bypass grafting (CABG), $10,038; amputation, $8,942; transcatheter aortic valve replacement (TAVR), $7,997; and abdominal aortic aneurysm (AAA), $6,919. When factoring volume, CABG and TAVR were the two highest total financial contributions to their institutions, although amputation was third.
This data alone, however, still doesn’t explain why our specialties are being crammed together under one umbrella. It can’t just be our beneficial profit margins. No one tried to shove neurosurgery and orthopedics together and said, “I dunno, ortho guys like to lift, call it Brains and Gains.”
I am absolutely convinced that I know the true incentive to create this unholy matrimony between cardiology, vascular surgery and cardiothoracic surgery—we order similar tests
There are many purported financial benefits of a heart and vascular center. Branding, research funding, efficiency and alignment with value-based care models are the most commonly cited. But none of them really account for the amount of time and effort hospitals are willing to burn
1. Reintervention defined as CD-TLR. 2. Brian G. DeRubertis et al., Two-Year Outcomes of the LIFE-BTK Randomized Controlled Trial Evaluating the Esprit™ BTK Drug-eluting Resorbable Scaffold for Treatment of Infrapopliteal Lesions, VIVA 2024.
INDICATIONS The Esprit™ BTK Everolimus Eluting Resorbable Scaffold System is indicated for improving luminal diameter in infrapopliteal lesions in patients with chronic limb-threatening ischemia (CLTI) and total scaffolding length up to 170 mm with a reference vessel diameter of ≥ 2.5 mm and ≤ 4.00 mm.
MAT-2408411 v3.0 48% fewer patients require reinterventions through 2 years.1,2 Go above expectations with the only device that does it all for CLTI.*
IMPORTANT SAFETY INFORMATION
Esprit™ BTK Everolimus Eluting Resorbable Scaffold System
INDICATIONS
The Esprit™ BTK Everolimus Eluting Resorbable Scaffold System is indicated for improving luminal diameter in infrapopliteal lesions in patients with chronic limb-threatening ischemia (CLTI) and total scaffolding length up to 170 mm with a reference vessel diameter of ≥ 2.5 mm and ≤ 4.00 mm.
CONTRAINDICATIONS
The Esprit™ BTK Everolimus Eluting Resorbable Scaffold System is contraindicated for use in:
• Patients who cannot tolerate, including allergy or hypersensitivity to, procedural anticoagulation or the post-procedural antiplatelet regimen.
• Patients with hypersensitivity or contraindication to everolimus or structurally related compounds or known hypersensitivity to scaffold components poly(L-lactide), poly(D, L-lactide), and platinum.
WARNINGS
• This device is intended for single use only. Do not reuse, reprocess, or re-sterilize. Note the product “Use-by” date on the package. Reuse, reprocessing, or re-sterilization may compromise the structural integrity of the device and / or delivery system and / or lead to device failure, which may result in patient injury, illness, or death. Reuse, reprocessing, or resterilization may also create a risk of contamination of the device and / or cause patient infection or cross-infection, including, but not limited to, the transmission of infectious disease(s) from one patient to another. Contamination of the device and / or delivery system may lead to injury, illness, or death of the patient.
• The Esprit™ BTK System is intended to perform as a system. The scaffold should not be removed for use with other dilatation catheters.
• The Esprit™ BTK System should not be used in conjunction with other non-everolimus drug eluting devices in the same vessel as the Esprit™ BTK Scaffold.
• It is not recommended to use this scaffold to treat lesions located at any joint or other hinge points, such as the knee or ankle. The recommended region for below-the-knee (BTK) treatment with the Esprit™ BTK Scaffold is the infrapopliteal arteries at a location ≥ 10 cm above the proximal margin of the ankle mortise. The Esprit™ BTK Scaffold has not been tested for use outside the recommended implant locations.
• This product should not be used in patients with aneurysms immediately adjacent to the scaffold implantation site.
• Insertion of the Esprit™ BTK System and implantation of the scaffold should be performed only under fluoroscopic observation with radiographic equipment providing high resolution images.
• Quantitative imaging is strongly recommended to accurately measure and confirm appropriate vessel sizing (reference vessel diameter ≥ 2.5 mm). If quantitative imaging determines a vessel size < 2.5 mm, do not implant the Esprit™ BTK Scaffold.
• Adequate lesion preparation prior to scaffold implantation is required to ensure safe delivery of the scaffold across the target lesion. It is not recommended to treat patients having a lesion that prevents complete inflation of an angioplasty balloon.
• Successful pre-dilatation with residual diameter stenosis of < 30% by visual estimation is required for treatment of the target lesion; < 20% by visual estimation is preferred.
• Ensure the scaffold is not post-dilated beyond the allowable expansion limits.
• Use of appropriate anticoagulant and / or antiplatelet therapy per standard of care is recommended for use of this scaffold system.
• This product should not be used in patients who are not likely to comply with the recommended antiplatelet therapy.
• Judicious selection of patients is necessary, since the use of this device carries the associated risk of
scaffold thrombosis, vascular complications, and / or bleeding events.
PRECAUTIONS
• Scaffold placement should not be performed in patients with known allergies to contrast agent that cannot be medically managed.
• It is not recommended to treat patients having a lesion with excessive tortuosity proximal to or within the lesion.
• When multiple scaffolds are required, only combinations of Esprit™ BTK Scaffolds must be used. Any potential interaction with other drugeluting or coated devices has not been evaluated.
• The delivery system is intended for deployment of the scaffold only and should not be used to dilate other locations.
• Implantation of the scaffold should be performed only by physicians who have received appropriate training.
• As with all catheter-based procedures, scaffold placement should be performed at facilities where patient can be prepared for necessary intervention and / or surgical removal of the device and vessel repair as per facility protocol.
• Pre-dilatation should be performed with an angioplasty balloon. Cutting or scoring balloons can be used per physician discretion, if the lesion appears to be mildly calcified.
• Failure to pre-dilate the vessel may impair nominal / optimal scaffold delivery.
• Implanting a scaffold may lead to dissection of the vessel distal and / or proximal to the scaffold, requiring additional intervention.
Note: In cases of bailouts, bailout treatment of the target lesion can be done using the Esprit™ BTK Scaffold of the appropriate length. If an appropriate length Esprit™ BTK Scaffold is not available, physicians should use standard of care.
• An unexpanded scaffold may be retracted into the introducer sheath one time only. An unexpanded scaffold should not be reintroduced into the artery once it has been pulled back into the introducer sheath.
• Post-dilatation is strongly recommended for optimal scaffold apposition. When performed, postdilatation should be performed at high pressure (> 16 atm) with a non-compliant balloon up to 0.5 mm larger than the nominal scaffold diameter.
• Use an appropriately sized non-drug coated balloon to pre-dilate the lesion. When treating a long lesion, scaffold the distal portion of the lesion prior to scaffolding the proximal portion of the lesion.
• Ensure that the scaffolded area covers the entire lesion / dissection site and that no gaps exist between scaffolds.
• The extent of the patient’s exposure to drug and polymer is directly related to the number of scaffolds implanted. The safety of everolimus, polymer, and polymer breakdown products was evaluated in preclinical studies and the biocompatibility assessment of the Esprit™ BTK Scaffold.
• The safety and effectiveness of the Esprit™ BTK Scaffold in patients with prior brachytherapy of the target lesion or the use of brachytherapy for treatedsite restenosis in the Esprit™ BTK Scaffold have not been established. Both vascular brachytherapy and the Esprit™ BTK Scaffold alter arterial modeling. The potential combined effect on arterial remodeling by these two treatments is not known.
• The safety and effectiveness of the Esprit™ BTK System have not been established in clinical trials with the use of either mechanical atherectomy devices (directional atherectomy catheters, rotational atherectomy catheters) or laser atherectomy catheters.
• Formal drug interaction studies have not been performed with the Esprit™ BTK Scaffold because of limited exposure to everolimus eluted from the scaffold.
• Everolimus, the Esprit™ BTK Scaffold’s active pharmaceutical ingredient, is an immunosuppressive agent. Therefore, consideration should be given to patients taking other immunosuppressive agents or who are at risk for immune suppression.
• Oral everolimus use in renal transplant and advanced renal cell carcinoma patients was associated with increased serum cholesterol and triglyceride levels, which in some cases required treatment.
• Non-clinical testing has demonstrated the Esprit™ BTK Scaffold is MR Conditional. A person with the Esprit™ BTK Scaffold may be safely scanned under the following conditions. Failure to follow these conditions may result in injury.
• Static magnetic field strength of 7 Tesla or less
• The Esprit™ BTK Scaffold should not migrate in this MRI environment. MRI at 7 Tesla or less may be performed immediately following the implantation of the Esprit™ BTK Scaffold.
POTENTIAL ADVERSE EVENTS
Potential adverse events include, but are not limited to: Allergic reaction or hypersensitivity to contrast agent, anesthesia, scaffold materials (poly[L-lactide] [PLLA], poly[D, L-lactide] [PDLLA], platinum, or everolimus), and drug reactions to anticoagulation or antiplatelet drugs
• Vascular access complications which may require transfusion or vessel repair, including:
CAUTION: This product is intended for use by or under the direction of a physician. Prior to use, reference the Instructions for Use, inside the product carton (when available) or at manuals.eifu.abbott for more detailed information on Indications, Contraindications, Warnings, Precautions and Adverse Events. This material is intended for use with healthcare professionals only.
Illustrations are artist’s representations only and should not be considered as engineering drawings or photographs. Photo on file at Abbott.
Information contained herein for DISTRIBUTION in the U.S. ONLY.
Abbott
3200 Lakeside Dr., Santa Clara, CA 95054 USA, Tel: 1.800.227.9902
™ Indicates a trademark of the Abbott Group of Companies. www.cardiovascular.abbott
The risks described below include the anticipated adverse events referenced in the contraindications, warnings, and precautions sections of the everolimus labels / SmPCs and / or observed at incidences ≥ 10% in clinical trials with oral everolimus for different indications. Refer to the drug SmPCs and labels for more detailed information and less frequent adverse events.
• Bleeding and coagulopathy (including hemolytic uremic syndrome [HUS], thrombotic thrombocytopenic purpura [TTP], and thrombotic microangiopathy; increased risk with concomitant cyclosporine use)
• Constipation
• Cough
• Diabetes mellitus
• Diarrhea
• Dyspnea
• Embryo-fetal toxicity
• Erythema
• Erythroderma
• Headache
• Hepatic artery thrombosis (HAT)
• Hepatic disorders (including hepatitis and jaundice)
• Hypersensitivity to everolimus active substance, or to other rapamycin derivates
• Hypertension
• Infections (bacterial, viral, fungal, or protozoan infections, including infections with opportunistic pathogens). Polyoma virus-associated nephropathy (PVAN), JC virus-associated progressive multiple leukoencephalopathy (PML), fatal infections and sepsis have been reported in patients treated with oral everolimus.
• Kidney arterial and venous thrombosis
• Laboratory test alterations (elevations of serum creatinine, proteinuria, hypokalemia, hyperkalemia; hyperglycemia, dyslipidemia including hypercholesterolemia and hypertriglyceridemia; abnormal liver function tests; decreases in hemoglobin, lymphocytes, neutrophils, and platelets)
• Lymphoma and skin cancer
• Male infertility
• Menstrual irregularities
• Nausea
• Nephrotoxicity (in combination with cyclosporine)
• Wound healing complications (including wound infections and lymphocele)
There may be other potential adverse events that are unforeseen at this time.
FROM THE COVER WOUND HEALING IN SPACE
continued from page 1
author Dóra Babócs, MD, from the Advanced Aortic Research Program at Baylor College of Medicine in Houston, and M. Mark Melin, MD, a vascular surgeon focused on wound care at the Mayo Clinic in Rochester, Minnesota—scoured more than 4,000 scholarly articles, covering a diverse study population in both space and terrestrial environments, to assemble a comprehensive picture. Not unlike the vastness and unknown quantities of the future endeavors their work seeks to support, Babócs, Melin—both members of the Space Surgery Association—and colleagues pieced together a rich tapestry of the state of wound healing in space: what is known about the subject, what is unknown and where opportunities for progress linger.
“One of the things we realized is that while we have so many approaches related to wound care and wound healing, we still don’t know enough yet,” explains Babócs. “Many of these cannot really be addressed without people being trained in this field. So, we are also trying to encourage and inspire vascular surgeons to participate more in aerospace medicine and space surgery because there are so many gaps in knowledge that require a collaboration between aerospace medicine professionals and vascular surgeons, general surgeons and interventional radiologists. Space and spaceflight are going to be a huge project for humanity if we are to go back to the
moon and even go to Mars. We are trying to bridge Earth-based vascular surgery with aerospace medicine.”
But it’s not just about evaluating the effectiveness of current wound-healing treatments in interventional and exposure areas like the International Space Station (ISS), terrestrial high- and low-volume vascular settings, and low-resource austere environments such as Antarctica. It’s also about spin-offs for care back on Earth, says Melin. For instance, information gleaned from a deep vein thrombosis (DVT) event that occurred in the internal jugular vein of an astronaut in space not only changed how women who want to use menstrual suppressants during space travel are cared for, but also those who do so back on terra firma. It’s these types of spin-offs that underscore the essential role of vascular surgeons in the space race, Melin relates.
people heal. All of this medical knowledge is really important to what we are doing in terms of research here on the ground as well. There are great connections here.”
The JVS-VL paper—which also includes as authors Baylor’s chief of vascular surgery Gustavo Oderich, MD, and Monika Gloviczki, MD, formerly of Mayo’s Gonda Vascular Center—targets the NASA Human Research roadmap as part of the effort to fill knowledge gaps.
“There are applications that we are using all the time in terms of fluid shift,” he says. “On Earth, we see a lot of fluid shifts to the legs. The astronauts are dealing with fluid shifts to the head and neck that create retinal changes, even swelling in the brain that takes a full two years to fully go away. And it changes how
GRANDFATHER OF VASCULAR QUALITY INITIATIVE RETIRES FROM FIVOS
By Marlén Gomez
JACK L. CRONENWETT, MD, CONSIDERED THE “Grandfather of the VQI,” will retire as the chief medical officer (CMO) for Fivos, the medical data solutions technology partner for the Vascular Quality Initiative (VQI). Cronenwett took on the role of CMO at Fivos after completing his term as medical director of the VQI in 2016. His tenure was marked by significant efforts to collaborate with the Food and Drug Administration (FDA) and vascular device manufacturers to promote the use of real-world evidence for postmarket device evaluation.
During this time, Fivos developed multiple such projects to evaluate vascular devices more efficiently using VQI data. One important project was launched to obtain funding from the Centers for Medicare & Medicaid Services (CMS) for surveillance of transcarotid artery revascularization (TCAR).
Cronenwett began his training in surgery at the Univer-
“We wanted to include the pathophysiological background, why events have happened, how can we prevent them and, once they have already happened, what we can do about them,” explains Babócs. And, going forward, the stakes could not be higher for those aboard space missions, she continues. “Until now, humanity’s goal was to go onto the ISS and do research there. Now, because of lunar and Mars missions, these are going to be so much longer in duration, and the distances are going to be significantly farther. If something happens on the ISS requiring any invasive or surgical treatment, we have the opportunity to evacuate to Earth, where the patients can receive definitive treatment at an Earthbased clinical hospital facility. But, if something happens halfway to Mars or on
sity of Michigan. In 1984, he transitioned from Mich igan to Dartmouth, an institution he considers as having a long history of quality improvement.
The Dartmouth Institute for Health Policy and Clinical Practice, founded by Jack Wenberg, MD, in 1988, emphasizes quality improvement and catalyzed the creation of the Vascular Study Group of New England—the seeds of the VQI—in a bid to improve the quality of vascular healthcare.
“The key concept that we focused on when we first developed the VQI was that all physicians want to achieve the best results, and if they’re provided with data that shows that they have an opportunity to improve, they will act to make improvements. That concept remains the cornerstone of the VQI,” said Cronenwett.
the moon, we are not going to have this opportunity, because just a one-way trip to Mars is going to be nine to 11 months. If something happens, we will inevitably have communication delays, and so it will be very useful to have a comprehensive manual on how to prevent these problems, or for what to do when they have already happened. Even if only some smaller surgical procedure, for example stitching a wound or closing a wound, everything is going to be different. The behavior of the tissue is going to be different. The regeneration of the cells is going to be different. We need to get ready.”
The team behind the JVS-VL paper, which also includes Rowena Christiansen, MD, from the University of Melbourne Medical School, Australia, and medical students Krishi Korrapati and Cooper Lytle, has published extensively on the topic, and, for Melin, future surgeons like Babócs, a postdoctoral research fellow at Baylor, hold the key to progress in this niche area. “Dóra is inspiring vertically and horizontally,” he says. “She is inspiring old guys like me, but also the next generation coming up, because it’s those folks who are going to make really significant sacrifices and take on servant leadership to be able to accomplish much of this. It also creates this aspirational view, where it just creates a whole new vantage point: it’s really energized me late in my career for what we are doing bedside with patients to be able to improve outcomes.”
SVS with the American Association for Vascular Surgery (AAVS), creating the organization that the SVS is today.
As he gets ready to leave his position, Cronenwett shared some parting wisdom for his successor.
“If you aim to move quickly, work solo; if you intend to achieve great distances, collaborate with others,” he said. This advice stems from his experience working collaboratively with others who share optimism for a project, urging leaders to disregard inevitable critics, he explained.
Cronenwett also served as Society for Vascular Surgery (SVS) president from 2002–2003, during which time he collaborated with Thomas Riles, MD, for the merger of the
“ The key concept that we focused on when we first developed the VQI was that all physicians want to achieve the best results”
JACK L. CRONENWETT
“There will always be naysayers about any new idea,” said Cronenwett, emeritus professor of surgery at Geisel School of Medicine at Dartmouth in Hanover, New Hampshire. “Eventually, when it becomes successful, the naysayers will come around. It was difficult to convince the SVS to take over the then-nascent VQI in 2011, when it was starting to expand beyond New England. But there were several influential people within the SVS at that time who recognized the potential and were able to work with us to achieve that.”
The VQI’s 14 registries contain demographic, clinical, procedural and outcomes data from more than a million procedures performed across the U.S., Canada and Singapore, with each record including information from the patient’s initial hospitalization and at one-year follow-up.
Dóra Babócs
M. Mark Melin
Jack L. Cronenwett
SVS leadership figures reflect on roles ahead of elections
The Society for Vascular Surgery (SVS) is entering a transformative period as Vice President Linda Harris, MD, transitions to the role of SVS president-elect, while Secretary William Shutze, MD, completes his term, making way for the election of their successors. Here, the SVS leadership tandem reflect on the importance of effective leadership in furthering advancements in vascular surgery. By Marlén Gomez
HARRIS PORTRAYS HERSELF AS AN ACCESSIBLE leader for SVS members, which she considers essential. She highlights the importance of open communication in providing organizational support and creating an equitable environment that prioritizes the wellbeing of patients and the community.
“Our members need to have forums and channels to reach physician leadership and our staff professionals if they have questions,” Harris says. “Organizations can often be large and complex, leaving people unsure where to start. We must work to simplify that process.”
The SVS secretary serves a three-year term, while the vice president serves for one year, followed by a year as president-elect before becoming SVS president. Nominations for vice president and secretary positions were announced in April, with active voting scheduled from May 15–June 5.
“The role of secretary has allowed me to be involved with our strategic priorities at a higher leadership level and provide meaningful input,” Shutze says.
Shutze notes that one of his proudest accomplishments
during his tenure was his role in reorganizing the Communications Committee into the Communications and Branding Committee.
In 2024, the SVS launched Your Vascular Health, a comprehensive, patient-focused website designed to bridge the information gap between patients and vascular care providers. This site helps individuals navigate the complexities of vascular health with easy-to-understand resources.
Shutze played a crucial role in launching the site, which included a dedicated day of syndicated programs featuring more than 20 interviews about the SVS’ new Highway to Health campaign.
“As the SVS collaborates more with other societies and specialties, the secretary will play a larger role in fostering cooperation and collegiality,” he says.
In her position, Harris supported the president and president-elect with various initiatives. The most memorable of these began before she assumed her current role, specifically the task force formed to explore the status of the Vascular Surgery Board. “We need unity, regardless of opinions on a free-standing board or financial issues before Congress, whether inpatient or outpatient,” Harris says. “The new vice president must continue breaking down barriers to foster collaboration.”
Both leaders plan to assist incoming officers during the transition by offering guidance on their roles. Reflecting on future challenges, Harris adds, “Regardless of the vote or decision, we need to support one another; for divisive issues, bringing together those with differing views will help us move forward.”
SVS names candidates
The SVS announced the nominees for vice president and secretary positions in April. Early Active, Active and Senior SVS members are eligible to vote during the voting period, May 15–June 5. The candidates nominated for vice president are Andres Schanzer, MD, and Shutze.
“The intensity of the work required for the campaign and its rollout was significant,” he says. “The good news is that vascular surgeons are skilled at managing time.”
Shutze believes branding and public awareness will remain central to the role as the secretary’s duties evolve. Currently, he has regular meetings with SVS professional staff to ensure progress.
FROM THE COVER BYLAW REFERENDUM: SVS EXECUTIVE BOARD
For the secretary position, the nominees are Rabih A. Chaer, MD; Michael S. Conte, MD; Sherene Shalhub, MD; and Malachi Sheahan III, MD. With four candidates for the position of secretary, the SVS will also utilize rank-ordered voting for the first time. Details associated with this process are available on the elections webpage: vascular. org/Election. The election results will be announced on June 6 during the Annual Business Meeting at the 2025 Vascular Annual Meeting (VAM) in New Orleans.
PROPOSES CHANGES TO SENIOR MEMBERSHIP TO MEET MODERN DEMOGRAPHIC CHALLENGES
success of the SVS establishing a section model, Calligaro proposed establishing an SVS Senior Section, which recently gained Executive Board approval. The effort, which included input from more than 150 later-career members, is now led by Enrico Ascher, MD, recently appointed chair by the Executive Board. This section establishes a voice for the later-career community on the SVS Strategic Board and seeks to meet the needs of its members through education and other engagement programs.
“Establishing the section and understanding the needs and opportunities has been a big advance for the SVS,” said SVS President Matt Eagleton, MD. “Now comes the hard work of cultural and organizational change, and establishing a contemporary model of membership, engagement and resource support that is sustainable for both members and the SVS long term.”
What’s in a name?
As the Executive Board began discussing a future model for Senior membership within the SVS, confusion was immediate: the challenge became making clear the Society was working to maintain a Senior member membership category while also establishing a new Senior Section. For this reason, the SVS conducted a nomenclature review of terminology used by other medical societies to inform a change for the SVS. This process allowed
for broad consideration of potential names, with both the SVS Membership Committee and Executive Board ultimately deciding against options such as “Senior,” “Emeritus,” or “Honorary.” Consensus was eventually found for moving forward with the new “Legacy” name to represent the community’s membership status.
One size no longer fits all
A second significant challenge came in understanding the demographics of the later-career population of members, and it became clear that members approach latercareer transition at vastly different times, for different reasons, and with very different capacities. The current bylaws for Senior members, developed decades ago, were intended for vascular surgeons who were fully and completely retired from practice and experienced a significant decline in professional income but desired to stay engaged. The bylaws permitted members to notify the SVS of the change and, once affirmed, move from full Active status to Senior member, going from paying full dues to $0.
Advance the clock 20 years, and the conditions of today are quite different. Many vascular surgeons are choosing to retire or semi-retire from practice in their 50s and 60s, and retirement does not necessarily imply a significant decline in professional income, as many members seek new opportunities and career transitions. Many vascular surgeons are
continued from page 1
working well into their 70s, remaining fully active in practice.
As a result, determining eligibility for Senior membership has become more challenging. Following deliberations between the Membership Committee, Senior Section leadership and the Executive Board, agreement was reached that applying strict “means-testing” or “policing” does not fit well with the SVS’s desired culture.
Therefore, the bylaw referendum proposes a shift from “means-testing” over the nature of career transition to “agebased” eligibility and choice that can be applied to all. In short, the referendum proposes that eligible members may select the tier of Legacy membership that best suits their needs and interests. The first Legacy membership tier is optionable at age 70, the second at age 78—each with significant adjustments in dues and commensurate changes in benefits and privileges. The second Legacy tier will also be accessible for members who require special accommodations.
Building a sustainable model
Currently, 875 Senior members have transitioned from Active member status ($700) to Senior ($0). This number is increasing by about 100 per year and is likely to accelerate due to the fact that more than one-third of Active members is aged 60 and over. A strong consensus is that later-career members should have
significant discounts on dues and other program-related fees and benefits. There is also a strong consensus that, as a Society, all members have a responsibility to help support the ongoing mission of the SVS.
“The current reality—where a quarter to a third of SVS members is paying $0 dues, with a greater percentage expected in coming years—is simply not a sustainable financial model,” noted SVS Treasurer Thomas Forbes, MD. “Thankfully, the SVS is very financially sound, and, due to great diversity in revenue sources, only 13% of total revenue comes from dues. This is very healthy and shows good management by the Society, but none of our practices could stay viable if 25–33%% of our patients went from full-pay to no-pay status, expecting the same level of care and services.” The Senior Section has a number of ideas and plans to build value for later-career members, explained Ascher. “I support this bylaw referendum because it takes resources and support to create new opportunities for Senior engagement.”
The bylaw referendum charges the Executive Board with developing and approving a dues, benefits and privileges schedule to fit the two new tiers of Legacy membership. A pro forma model has been developed to achieve the desired balance. Those who elect Legacy membership at age 70 will receive a 40% discount in dues, while those who opt for the category at age 78 will be asked to pay a nominal fee of less than $100 each year. Should the referendum pass in June, the Executive Board will finalize the dues and benefit grid in consultation with the SVS Membership Committee and Senior Section leadership. It would then be implemented for 2026.
Kenneth M. Slaw is executive director of the SVS.
William Shutze (top) and Linda Harris
POWER AND PRECISION:
INDICATIONS FOR USE
Caution: Federal (USA) law restricts the use of the system by or on the order of a physician. Refer to Directions for Use and/or User Manual provided with the product for complete Instructions, Warnings, Precautions, Possible Adverse Effects and Contraindications prior to use of the
EVAR founding fathers invoke revolutionary past to predict path ahead for aortic stent graft development
By Bryan Kay
The next spring forward in aortic stent grafting will be rooted in a greater understanding of the biomechanical forces acting upon devices alongside continued advances and specialization in imaging, according to some of the founding fathers of endovascular aneurysm repair (EVAR) who were gathered at the 2025 Charing Cross (CX) International Symposium in London, England (April 23–25) to mark more than four decades of EVAR development. “When you think about aortic aneurysms, all of the devices are rigid, they are stiff, and the body changes with time,” said Christopher Zarins, MD, of Stanford University, a former Society for Vascular Surgery (SVS) president, who was involved in early development efforts at Stanford University. “For example, when you’re 6ft tall at the age of 20, you’re 5ft tall at the age of 80. You shorten, but the stent graft doesn’t… so we need to look at new materials and new devices that can reflect the changing environment of the body itself.”
As imaging modalities progress, added Rodney White, MD, from Torrance, California, also involved early on
FROM
at Stanford, and “we can look more at diseases and the natural history—and the devices and how they need to change—I think we are all going to become imaging specialists, which is going to drive where these changes come from and show us how we have to progress.”
These visions of the future came as the assembled faculty reflected on the seminal moments of stent graft technology in the 1970s and into the early 1980s. Krassi Ivancev, MD, of Lund, Sweden, summarized the broad sweep of device development, including the revolutionary work of the late Nicolai Volodos, MD, in Soviet Ukraine and Juan Parodi, MD, from Buenos Aires, Argentina, between the Cleveland Clinic in the United States and in his homeland, which exhibited the simultaneous efforts taking place in the east and west as the pioneering journey proceeded. From the Gianturco stent in the earliest moments, through the advanced devices of today, the roots are clear, Ivancev said. “No question, Volodos was the first, but what started the revolution with stent
grafting was Parodi, and that was reinforced by several teams working together worldwide.”
Contributing thoughts via a prerecorded video, Parodi remembered how his work started in 1976, culminating in his first clinical case for an abdominal aortic aneurysm (AAA) in 1990. “That was a long journey, a lot of work, a lot of opposition,” he said, as he described performing the first AAA case in the world in the Argentinian capital with Julio Palmaz, MD, who was behind the balloonexpandable stent. Also in a video message, Frank Veith, another former SVS president and pioneer from New York City, involved in the first EVAR performed for a AAA Stateside, reflected how despite early resistance and scepticism, younger vascular specialists helped eventual widespread adoption. “We wanted to do everything that hadn’t been done before, so every one of our cases was a first,” he said. “This included ruptured aneurysms and things of that nature. We were treated as pariahs when we thought that we should be treated as messiahs.”
THE EDITOR THE SURVIVALIST’S GUIDE TO HEART AND VASCULAR CENTERS
to develop such a center. In fact, I am absolutely convinced that I know the true incentive to create this unholy matrimony between cardiology, vascular surgery and cardiothoracic surgery—we order similar tests. Your hospital CEO will likely tell you that they can’t factor downstream revenue into any financial account of your services. This is the big lie. Downstream revenue is so critical that your simple free-standing vascular clinic represents an existential threat to the hospital. Think of all the computed tomography angiographies (CTAs), stress tests, magnetic resonance imagings (MRIs) and blood work that you order. What if they were performed at (gasp) an outside institution? Double that for the cardiologists.
Field Book note #4:
Downstream revenue means nothing. But, in a much more real sense, it means everything
So rather than risk this downstream revenue going down a stream to another facility, your hospital wants to put a wall around you and your cardiology friends. Everything under one roof. Their roof.
I’m not sure exactly what edition of the heart and vascular institute/service line we are on in my institution. Three I think. Last year, I received an invitation to participate in the development of a new system-wide cardiovascular service line. The announcement stated our goal was to become the premier destination for “cardiology care” in the Gulf South.
Field Book note #5:
Sooner or later, these guys always show their cards
At the first meeting I was presented an org chart proposal for an executive steering committee. At the top was a chair and a vice chair (cardiologist, cardiologist). Next to them was a service line administrator and a CEO partner
continued from page 2
(suit, suit). Under that was a system service line advisory panel consisting of eight “voices.” I, as chief of the only medical or surgical specialty to provide unified coverage across our entire healthcare system, including a Veterans Administration (VA) and two medical schools, was assigned Voice #6.
Two weeks earlier, I had taken off an afternoon to see our son, Luke, in his school play. After looking at the program I offered (perhaps ungenerously), my disappointment that I took time away to see him as Fern #3: well, it seems Luke had a bigger role to play in Geology Rocks! than I would in our heart and vascular center.
The challenges for vascular surgeons in a heart and vascular center clearly outweigh the benefits. Marketing dollars and resource allocation are limited. Will these assets go to you or to a transplant program that promises a contribution margin of $50–100k? Who will control the scheduling conflicts, case competition and strategic decisions? Likely the cardiologist they put in charge.
Field Book note #6:
The national anthem of cardiology should be ‘This Land Is My Land. This Land Is Also My Land’
Finally, consider your referral patterns. It is likely that a wide range of specialists and primary care physicians send you patients. The average age of a patient requiring a vascular procedure is 63. The average age of a first-time referral to a cardiologist is 50. So, when you are co-located with the cardiologist, who will the patient referred to you for a vascular issue see? You or the cardiologist they have an established relationship with?
Now, I am sure a few of you will tell me that your heart and vascular center works well for them and I don’t know what I’m talking about. To those folks, I want to make two important points. Number one, everything is local and your experience is not typical. And second, everyone hates you.
We are at 1,400 words and I haven’t even laid out what
a heart and vascular center/institute/service line is. Probably because I don’t know. There are no standard models, quality metrics or milestones. U.S. News and World Report does not rank these entities. There is absolutely no patient outcome data. It’s almost as if the idea did not even come from medicine.
The best way for a vascular surgeon to mitigate the risks of a heart and vascular institute is not to be in one. If the process is inevitable, here are the steps to take:
1. Appoint a vascular surgery service line director: Ensure dedicated leadership and control over operational, strategic and quality planning.
2. Allocate dedicated hybrid operating room time and vascular lab access: Ensure access for elective and urgent vascular cases.
3. Develop a limb salvage and complex vascular pathway: Formalize vascular referral protocols for chronic limb-threatening ischemia (CLTI), dialysis access and complex aortic disease, ideally to you.
4. Establish multidisciplinary conferences led or co-led by vascular surgery: For aortic disease, CLTI, carotid revascularization, venous thromboembolism.
5. Create dedicated vascular research support: Assign staff or seed funds to initiate vascular-specific research or industry partnerships.
6. Track and share outcomes transparently: Publish service-line dashboards by condition (not just by specialty). Include: amputation rates, stroke-free survival, hybrid case utilization, door-tointervention times. Benchmark against vascular and cardiology registries.
7. Align incentives: This is the biggie. A lot of the turf issues will evaporate if the salaries/payments/ bonuses can be aligned and linked to service-line metrics rather than individual case volume.
Good luck out there. Please send in your experiences. If nothing else, maybe we can start to provide some data.
MALACHI SHEAHAN III is the medical editor of Vascular Specialist
How likely are your surgical patients to have disruptive bleeding?
COMMENT& ANALYSIS
THE OUTPATIENT
EMBOLIZATION
IN THE OBL
By Daniel Torrent, MD
Embolization is often not very familiar to vascular surgeons. With the exception of type II endoleaks, these cases often get referred to interventional radiology (IR). As a result, there is little—if any—exposure to these procedures in vascular training. Once in practice, we don’t really think about them, despite the fact that they fit nicely into an outpatient practice.
At the hospital my practice covers, there is not much of an IR presence, so vascular surgery provides the emergency embolization services. Between the cold legs and ruptured aneurysms, we are also handling the gastrointestinal bleeds, ruptured spleens and postpartum hemorrhages. This has resulted in increasing comfort with these procedures. The anatomy and technical details are not dissimilar to what we do on a daily basis.
CORNER STITCH
In addition to the hospital practice, we also have a busy office-based lab (OBL). In the context of this setting, we were asked by a gynecologist in the area about providing uterine artery embolization (UAE) for fibroids. Given our exposure to embolization procedures in the inpatient setting for emergencies, this felt like a very reasonable extension of our outpatient practice.
UAE has several characteristics that make it an ideal procedure for the outpatient setting. It is purely elective, which makes it practical to schedule. The patients are generally younger and lower risk than the typical vascular patient. The procedure itself is also low risk, with only relatively small sheaths required and the option for radial access. UAE also tends to be fairly routine and predictable. In a
setting where significantly prolonging the day is not an option, there is a benefit to knowing, with a reasonable degree of certainty, how long the procedure will take. Most importantly, the patients are happy because they get relief of their symptoms while avoiding a larger operation.
We had the advantage of already having experience with embolization procedures. However, for a surgeon who already has a significant endovascular practice, extending to offer these procedures is not significant. It would
Uterine artery embolization has several characteristics that make it an ideal procedure for the outpatient setting
Why residency is the best time to pursue device innovation
By Richard Shi, MD
WE LIVE IN THE GOLDEN ERA OF VASCULAR surgery. Novel devices are improving the lives of increasingly sick patients in minimally invasive ways, and vascular surgeons and interventionalists have been at the forefront of these inventions. Our work lends us to being natural innovators, but it can be unclear where one should start. However, I would suggest that vascular surgery residency can be the best time to engage in device development.
Boots on the ground
The first step of medical device design is identifying unmet clinical needs. Device companies spend considerable effort and money to understand the challenges providers face and discover opportunities for innovation.
Yet, we experience these things daily as vascular surgery residents. We spend thousands of hours learning patient care on inpatient floors and surgical skills in operating rooms, and we understand the pain points that exist within the lives of ourselves and colleagues. Residents also offer fresh perspectives, being some of the newest workers in the hospitals. With every inefficiency we encounter, we ask, “Why are things done this way?” Or, “Is there a better way to do this?” Ultimately, our innumerable patient care hours and eager mindsets provide a strong foundation to initiate the innovation process.
First-hand access
A unique aspect of vascular surgery training is the number of medical devices with which we become familiar. Whether ubiquitous technologies such as the self-expanding stent, or
involve gaining familiarity with the branch anatomy of the internal iliac artery and with embolization agents. In UAE, microparticles or liquid agents are often used. Comfort with radial access— less often used in vascular procedures— is helpful. Finally, relationships with gynecologists need to be developed, as they make these treatment decisions and referrals.
There are other elective embolization procedures that can be explored. While we’ve had minimal experience with it, prostate artery embolization is also well suited to the outpatient setting. Geniculate artery embolization is a newer procedure that has shown promise for patients with osteoarthritis who are not surgical candidates. Overall, when done well and with input from the relevant specialists, these are excellent procedures to expand an outpatient vascular practice.
DANIEL TORRENT is a vascular surgeon at the Longstreet Clinic in Gainesville, Georgia.
novel innovations like the thoracoabdominal multibranched endoprosthesis, we work with devices daily and experience their advantages and disadvantages. Thus, we have unprecedented access in learning how medical devices work, giving us concept inspirations when designing our own.
Furthermore, our relationship with medical device companies provides us valuable product knowledge through the likes of simulation sessions and personal samples to practice with. As residents, we can utilize these opportunities to develop and validate our own designs.
Resource havens
Many of us train at large academic hospitals, which may be affiliated with local universities that have systems in place that support medical device development.
For example, affiliated engineering schools can provide engineers to assist with device design, design workshops
for prototyping, and laboratories for device testing. Major academic institutions will also have technology transfer offices and patent attorneys to support intellectual property protection and commercialization efforts. Universities will also host innovation grants and business plan competitions offering equity-free funding. These are invaluable resources we have access to as residents at major academic institutions that can support our careers in device innovation.
At the Medical University of South Carolina (MUSC) in Charleston, I am part of the Human Centered Design Program, an incubator developing startups based on novel solutions created by surgical attendings and residents that address unmet clinical needs. We have partnered with the Georgia Institute of Technology’s Biomedical Engineering Program to help prototype and test solutions, and the MUSC Zucker Institute for Innovation Commercialization to pursue intellectual property protection. This program has fostered my work on a device to achieve rapid hemostasis in arteriovenous fistulas and grafts post-dialysis cannulation.
These opportunities, offered by my residency institution, have ultimately become lifelong skills that can advance both an academic and private-practice career.
The best time is now
While medical devices are an integral part of our practice, we should also recognize the history of harmful cases some devices have caused.
As vascular surgeons, we must serve as gatekeepers of novel technologies and understand how devices are developed—and their clinical data—before we recommend them to patients. Thus, we have a responsibility to participate and establish ourselves within the innovation process.
For vascular surgery residents, the best time to begin is now.
RICHARD SHI is a postgraduate year (PGY) 3 research resident at MUSC.
GOVERNMENT
GRAND ROUNDS
Primer on the reconciliation process for budget bills
By Kyle Gerron and Dylan Lopez
AS ADMINISTRATION OFFICIALS AND LEADERS in Congress align their priorities this year, the congressional reconciliation process is poised to become a crucial tool for legislative action. This parliamentary process is often discussed in the news around our issues, but rarely fully explained. Below is a brief explanation on what reconciliation is and why it matters.
What is reconciliation?
Reconciliation is a special legislative process used by Congress to expedite the passage of certain budget-related bills. This process allows for a bill to pass the Senate with a simple majority (51 votes, or 50 votes plus the vice president’s tie-breaking vote), bypassing the usual 60vote threshold needed to overcome a filibuster.
How does the reconciliation process work?
Budget resolution: The process begins with the adop-
tion of a budget resolution by both the House and Senate. This resolution is a framework that sets the overall spending and revenue levels for the upcoming fiscal year and includes “reconciliation instructions” for specific committees.
Committee action: The committees specified in the reconciliation instructions then draft legislation that meets the established budgetary targets. These bills are then combined into a single omnibus reconciliation bill.
Debate and vote: Next, the reconciliation bill is considered under special rules that limit debate time and prohibit filibusters. In the Senate, debate is limited to 20 hours. The bill then proceeds to a vote, where it can pass with a simple majority.
Health Care and Education Reconciliation Act of 2010, which made key changes to the Affordable Care Act, the American Rescue Plan Act of 2021, and the Inflation Reduction Act of 2022.
Reconciliation has often served as a viable mechanism for passing significant healthcare legislation
Byrd rule: Named after the late Sen. Robert Byrd, this rule restricts the inclusion of “extraneous” provisions in reconciliation bills. Provisions must directly affect the budget and cannot increase the federal deficit beyond a 10-year period.
Including healthcare proposals in reconciliation
Reconciliation has often served as a viable mechanism for passing significant healthcare legislation, such as the
Healthcare legislation can be included in a reconciliation bill if it meets the criteria set by the Byrd rule. For example, changes to Medicare, Medicaid or health insurance subsidies that impact federal spending and/or revenue can be part of the reconciliation process. In the current reconciliation bill being negotiated by Congress, possible healthcare provisions include reducing spending for Medicaid, adjusting subsidies for health insurance under the Affordable Care Act, or introducing new healthcare programs. Items that could be included to help offset the costs to the overarching bill include pharmacy benefit manager (PBM) reform, as well as site neutrality proposals. These changes must comply with budgetary constraints and goals.
The SVS is monitoring current discussions relating to a forthcoming reconciliation bill and will share information relating to any potential impact on our priorities.
KYLE GERRON AND DYLAN LOPEZ are the SVS legislative advocacy manager and advocacy and public affairs manager, respectively.
EQUIVALENT OUTCOMES SEEN AMONG FEMALE, MALE PATIENTS IN REALWORLD ANALYSIS OF PACLITAXEL-ELUTING STENT USE
By Bryan Kay
The use of a paclitaxel-eluting stent to treat femoropopliteal occlusive disease led to equivalent outcomes in male and female patients in “a diverse and complex real-world cohort,” a new study found, set against previous question marks over the effectiveness of the technology in women.
A research team from the University of South Florida (USF) in Tampa retrospectively looked at their institutional experience with the Zliver PTX device (Cook Medical), analyzing major adverse limb events (MALEs), amputation-free survival and freedom from target limb revascularization out to five years.
Maria Peñuela, MD, a vascular surgery resident at USF, delivering the data during the 2025 Society for Clinical Vascular Surgery Annual Symposium in Austin, Texas (March 29–April 2), laid out how the Zilver PTX randomized trial data demonstrated clinical durability with improved freedom
question of whether these data were “reflective of real-world utilization and outcomes” remained, as 91% of the included patients presented with claudication, 34% were female and the mean lesion length was less than 100mm.
The USF single-center retrospective review, therefore, sought to assess the long-term clinical effectiveness of Zilver PTX stents over a seven-year study period from 2013–2019. With a primary outcome measure of MALE at one, two and five years, the review looked at 252 patients with 265 treated limbs that met inclusion criteria. The cohort bore a median age of 65 years and was made up of 37% female patients.
“Overall, the female and male groups were similar with respect to demographics and preop comorbidities; however, male patients more frequently had hyperlipidemia and tobacco use,” Peñuela told SCS 2025.
MALE was defined as reinterventions, stent occlusion or major amputation, she explained, with overall rates similar between both groups and stent occlusion representing the most common event among male and female patients in the cohort, she continued. “Overall mortality was similar between both groups at five years, and amputation-free survival rates were similar across time points for both groups,” Peñuela said. Treatment length did not have any influence on MALE, overall survival or amputation-free survival based on Kaplan-Meier or univariate analysis, she added.
Acknowledging study limitations, Peñuela pointed out the single-center, retrospective nature of the review, further conceding that “we also lacked an institutional endo-comparator, and we had minimal anatomic data, such as calcium burden or GLASS [Global Limb Anatomic Staging System] scores.”
Postponed: Complex Wound Care Masterclass now set to be held from 2026
THE SOCIETY FOR VASCULAR SURGERY (SVS), in collaboration with the Society for Vascular Nursing (SVN) and the American Podiatric Medical Association (APMA), has postponed the Complex Wound Care Masterclass initially scheduled for June 7 this year, now to be held alongside the Vascular Annual Meeting (VAM) from 2026–2028. The workshops were previously set to commence at VAM 2025 in New Orleans.
The masterclass is part of the Wound Care Curriculum, which includes an online module containing 27 short on-demand videos that is currently available on the SVS VascuLEARN website. The online module provides learners with the fundamentals of wound care for vascular surgeons, physician assistants, vascular nurses and podiatrists.
The workshops will be the hands-on companion to the online content tailored to vascular care teams’ unique needs. The confirmed agenda for 2026 includes topics such as methods of debridement, dressing management and oxygen therapy. Proposed topics for 2027 include skin substitutes, fluorescence imaging and infrared imaging, while the proposed agenda for 2028 will cover total contact casting and removable devices, with final confirmation slated for the summer before each event. For more information, visit vascular.org/WoundCare.—Marlén Gomez
Maria Peñuela
Survey suggests greater exposure to mini-incision carotid endarterectomy during training may dispel perceived limitations to approach
While a recent survey found that a majority of those who responded had performed mini-incision carotid endarterectomy (CEA) at least once in their practice careers, most answered that they did not perform the surgery routinely. By
Bryan Kay
IN THE WORLD OF GENERAL
surgery, no one would opt for a large abdominal incision if they could perform a mini-incision laparoscopic procedure, ponders Alan Dietzek, MD, the chair of vascular surgery at Jersey Shore University Medical Center, Hackensack Meridian Health, in Neptune, New Jersey. Yet, “in the vascular world,” he says, “for whatever reason, having a large neck incision is still acceptable versus having a small one.”
Dietzek was speaking to Vascular Specialist in the aftermath of a recent survey that showed more than 65% of those who responded had carried out a mini-incision CEA on at least one occasion and 19.2% always did so. Furthermore, respondents who performed the operation less fre -
quently were significantly more likely to report that it provides less exposure and that patients are unconcerned about incision size.
The survey, sent to 1,110 Society for Clinical Vascular Surgery (SCVS) members, garnering a 13% response rate, sought to establish barriers to routine use of mini-incision CEA. The results were presented at the 2025 SCVS Annual Symposium in Austin, Texas (March 29-April 2) by Keerthivasan Vengatesan, MD, a general surgery resident at Dietzek’s previous institution, Danbury Hospital in Danbury, Connecticut.
Dietzek says that among those barriers, as outlined by the survey, was “the fact that surgeons are afraid there won’t be enough exposure.”
CAROTID ENDARTERECTOMY OUTPERFORMS STENTING AMID ‘TREMENDOUS OVERUSE’ OF BOTH PROCEDURES IN 10-YEAR COHORT STUDY APPROPRIATE USE
By Jocelyn Hudson
A RETROSPECTIVE, NATIONWIDE COHORT study has revealed carotid endarterectomy (CEA) performed better than carotid artery stenting (CAS) in France over the course of a decade, while also highlighting the overuse of both procedures in the same period.
Based on their findings, the research team calls for the suspension of interventions for carotid artery disease until appropriate studies are conducted.
The investigation—which authors Eric Steinmetz, MD, a vascular surgeon at CHU Dijon Bourgogne in Dijon, France, and colleagues note involved the largest
More importantly, he continues, “if they have never done mini-incision carotid surgery, they are not likely to do it. Those who are coming out of training are likely to do the surgery if someone else in their practice is already doing the surgery. Or if they haven’t learned it in training, but if there are others in their practice that are doing mini-incision carotid surgery, there is a good chance that they will likely perform mini-incision carotid surgery.”
features such as high bifurcation, short or obese neck, and redo surgery, although this was not observed in those who always utilized shunts during mini-incision CEA, Dietzek and colleagues established.
The survey laid out that only 31.5% of respondents were trained to perform mini-incision CEA prior to beginning practice, and that those surgeons were significantly more likely to have performed the operation in practice. Additionally, surgeons who always performed the surgery with patch angioplasty were significantly more likely to do so even in patients with higher-risk
“If you teach your fellows or residents how to do the procedure, that is the most important factor in them going forward in practice doing the procedure”
ALAN DIETZEK
cohort of asymptomatic carotid procedures ever studied—was recently published as an Editor’s Choice paper in the European Journal of Vascular and Endovascular Surgery (EJVES).
Steinmetz et al begin by stating that it was their objective to compare periprocedural stroke or death within 30 days of a procedure in patients who underwent either CEA or CAS. The researchers used data from the PMSI (Plan de financement à l’acte) hospital database, including in their study all patients who underwent either CEA or CAS between 2010 and 2019 in France.
Steinmetz and colleagues share that, between 2010 and 2019, 164,248 patients underwent a carotid artery procedure in France, comprising 156,561 CEA and 7,687 CAS procedures. They note that asymptomatic women made up around 25% of the total cohort and high-risk
The authors report in EJVES that the rate of periprocedural stroke or death within 30 days was 1.5% overall, 1.3% in asymptomatic patients, and 3.3% in symptomatic patients. They detail that, after matching and adjustment, the risk of periprocedural stroke or death within 30 days was statistically significantly greater in patients who underwent CAS than in patients who underwent CEA.
In their conclusion, Steinmetz et al stress that many patients in the study—specifically asymptomatic
Although the CEA patient population tends to be slightly older and less concerned with cosmetic outcomes, Dietzek considers, “I don’t think anybody would prefer to have a larger incision than a smaller incision unless they thought their outcomes would be worse.” To this end, Dietzek points to data in the literature showing outcomes after mini-incision CEA “are just as good as any other incision for carotid surgery.”
Therefore, Dietzek says, teaching fellows and residents how to do the operation is the most important factor in them then adopting it when they head out into practice.
“Having done this for more than 20 years, I would say that I can’t even recall having to extend the incision during an operation because I’ve had inadequate exposure,” Dietzek adds, explaining how the exposure—sometimes measuring as low as 4cm or less—is achieved by dividing the platysma muscle beyond the skin incision, enabled with the use of retraction. “It does occur but it’s so uncommon that it is not the kind of thing where you have to be fearful that you’re going to be boxed in when you are doing the operation in this manner. If you do have to extend the incision, that’s something you probably may have to do early on when you are first learning how to do it.”
women, high-surgical-risk patients, and patients undergoing CAS—received procedures that were more likely to be harmful than beneficial, according to the results of past randomized trials.
In addition, the authors write that “despite the huge number of asymptomatic carotids treated in the present sample, there is currently no proven benefit for asymptomatic carotid intervention compared with best medical treatment alone, or for screening for carotid artery disease.”
Based on these conclusions, Steinmetz and colleagues propose that “there should be a moratorium on procedures for carotid artery disease until appropriate studies are conducted to determine whether [these procedures are] beneficial and for whom,” adding that studies are warranted to assess whether screening to detect carotid stenosis improves outcomes compared with non-invasive care directed only by clinical risk factors and without arterial imaging.
Furthermore, Steinmetz et al highlight a “tremendous overuse” of carotid procedures and an “urgent need to reconsider guidelines that encourage carotid artery procedures when there is no evidence of procedural benefit, and concurrent ongoing proof of procedural harm and significant cost.”
The researchers go on to state that “CAS should not be considered an alternative to CEA” and propose that changes in practice, health service remuneration and guidelines for CAS are needed.
Eric Steinmetz
Alan Dietzek
SOCIETY BRIEFS
Compiled by Marlén Gomez
SVS continues success with smoking cessation webinar series
THE SVS VASCULAR QUALITY
Initiative (VQI) is hosting a monthly webinar series throughout 2025 on smoking cessation, which so far has garnered positive participant feedback. The educational content consists of a 12-month program that draws on insights gained by Betsy Wymer, DNP, SVS director of quality, during her training for tobacco specialist certification.
The audience for this series includes physicians, advanced practice providers (APPs), nurses and patients.
To register for the webinars, visit vqi.org/ smoking-cessation-webinar-series
VQI? There’s an app for that
THE SVS HAS DEVELOPED A NEW mobile app for members of the VQI, which will be available on both the Apple and Google Play stores in May. The smartphone app offers easy access to critical news, events and resources. With the app, VQI members can explore regional groups, submit direct inquiries and connect with VQI representatives.
For further support, members can visit vqi.org/SVS-VQI-app-support
SVS FOUNDATION ANNOUNCES VC4U PROJECT GRANT RECIPIENT
The SVS Foundation has selected Olamide Alabi, MD, to receive a Vascular Care for the Underserved (VC4U) grant for her project, “Implementation of a data-guided ‘Circulation Health’ community-outreach initiative: Reaching people where they are.”
Alabi, a vascular surgeon and chief quality officer in the Division of Vascular Surgery and Endovascular Therapy at Emory University School of Medicine in Atlanta, is recognized for her expertise in peripheral artery occlusive disease and her dedication to improving access to quality healthcare. She also serves as the Society for Black Vascular Surgeons (SBVS) president.
The SVS Foundation’s VC4U grants support initiatives that address significant disparities in vascular surgery care across the U.S. The donations collected during the 2024 Vascular Health Step Challenge funded the VC4U Award, which raised awareness and support for peripheral arterial disease (PAD).
Alabi’s project will employ data-driven strategies to promote equitable PAD care. Her proposal outlines the establishment of multidisciplinary teams to conduct “Circulation Health” screenings for community members in collaboration with local partners. Additionally, she plans to develop a community-based participatory research team involving PAD stakeholders. “Thank you to my division leadership, Dr. Yazan Duwayri, for allowing us to participate in such high-impact, communityengaged initiatives,” Alabi said. “This proposal represents a collaboration with SVS and Society for Vascular Nursing [SVN] members, representatives from the SBVS, students [MPH, MD, PA], faculty from Emory and Morehouse School of Medicine, our podiatry colleagues and more. We are grateful for the opportunity to utilize this competitive award in our local and statewide community.”
For more information about the VC4U project grants, visit vascular.org/VC4U
CPVI Skills Course registration opens
A NEW YEAR INTRODUCES updated and reduced registration rates for the 2025 SVS Complex Peripheral Vascular Intervention (CPVI) Skills Course. Registration opened May 7, with early-bird rates available until June 11.
Designed by vascular surgeons, the CPVI Skills Course focuses on the latest innovations and techniques for treating patients with peripheral artery disease (PAD). This two-day course features didactic sessions, case-based learning and extensive hands-on training, allowing participants to practice advanced procedures on cadavers and benchtop models during small-group simulations.
Participants in the course can expect to learn about several key topics, including deep venous arterialization, retrograde access to the tibial and pedal arteries, and pedal loop imaging techniques.
Vascular surgeons of all training levels and specialists seeking to stay current in vascular surgery and endovascular therapy can register.
Visit vascular.org/CPVI25
Olamide Alabi
CLINICAL&DEVICENEWS
Debate: Carotid endarterectomy maintains its golden hue
THE ESTABLISHED “GOLD-STANDARD” APPROACH to carotid revascularization remained enshrined as the go-to operation as far as a 2025 Charing Cross (CX) International Symposium audience assembled in London, England (April 23–25), was concerned.
Some 76% of those who voted in the post-debate poll sided with Barbara Rantner, MD, chief of vascular surgery at Ludwig-Maximillian University Hospital in Munich, Germany, after she made the case for carotid endarterectomy (CEA), long established as the gold-plated method of tackling carotid disease requiring intervention. Transcarotid artery revascularization (TCAR) and transfemoral carotid artery stenting (CAS) each drew 12% of the audience share apiece, with the proposition for TCAR put forward by Michael Stoner, MD, chief of vascular surgery at the University of Rochester in Rochester, New York, and that of CAS made by Christopher Metzger, MD, an interventional cardiologist at OhioHealth in Columbus, Ohio.
Rantner, a co-chair of the 2023 European Society for Vascular Surgery (ESVS) carotid guidelines, looked at CEA through the prisms of gender, age and timing of procedure. “There is no gender issue, there is no age issue, there are no
Early feasibility study for Velocity pAVF system now fully enrolled
VENOVA MEDICAL HAS ANNOUNCED the completion of patient enrollment in the company’s VENOS-2 early feasibility study of the Velocity percutaneous arteriovenous fistula (pAVF) system for hemodialysis access.
The multicenter study is being performed under an Investigational Device Exemption (IDE) granted by the Food and Drug Administration (FDA) and is intended to provide proof-of-concept and initial clinical safety data. “Percutaneous AV fistulas provide a minimally invasive alternative to surgically created fistulas and potentially a shorter time to fistula maturation, reducing the exposure to and risks associated with hemodialysis catheters,” said Rishi Razdan, MD, a VENOS-2 study investigator.
R3 Vascular announces first patient treated in ELITE-BTK pivotal trial
R3 VASCULAR RECENTLY ANNOUNCED that the first patient in its ELITE-BTK pivotal trial has been treated by Brian DeRubertis, MD, chief of vascular surgery at New York-Presbyterian and Weill Cornell Medicine in New York City.
The trial evaluates R3 Vascular’s next-generation drug-eluting bioresorbable scaffold, Magnitude, for below-the-knee (BTK) peripheral arterial disease (PAD).
“I have spent much of my career researching novel devices for vascular disease, including bioresorbable scaffolds, and, while there have been some recent successes in the BTK PAD trial landscape, there remain significant unmet needs in this area,” DeRubertis commented.
limitations in timing of treatment,” she declared, pointing out the absence of a superiority trial showing an alternative revascularization option that has been proven to perform better.
Among the articles invoked in support, she referenced 10-year ACST-1 trial results that showed surgery equally benefited male and female asymptomatic patients. Symptomatic females undergoing CAS in CREST, Rantner said, “suffered from significantly higher periprocedural complications” when compared to CEA. Focusing on age, trial analysis showed that CAS was not a benefit for patients aged 65 or older. “Implementing endarterectomy remains standard of care, and also in the elderly population of 80 years and older,” Rantner added. In terms of timing, data demonstrated CAS “very significantly increased risk when we looked at early treatment onset,” she said.
Michael Stoner
The case for TCAR, meanwhile, rests in its minimal-access benefits for high-risk patients, the fact the procedure takes embolic risk in the aortic arch off the table, its safety profile, which is “as good—or better—than CEA,” the fact that it is “highly reproducible and scalable,” and its “rapid learning curve for contemporary vascular surgeons,” argued Stoner. He led attendees through the three ROADSTER studies, which produced data in support of TCAR, and looked at how the procedure compares to CAS. “TCAR is safer than CAS in any trial that has looked at this,” Stoner said. “How does it compare to CEA, the ‘gold standard’? Well, the gold standard doesn’t fare as well as TCAR. We have equivalent stroke/death rates, improved myocardial infarction, postprocedural hypertension and length of stay, and thus one can see a sustained benefit for TCAR.”
01: 4.5” x 5.625”
Terumo Neuro receives FDA approval for carotid stent system
TERUMO NEURO’S CAROTID STENT system has received premarket approval (PMA) from the Food and Drug Administration (FDA).
This milestone marks the first dual-layer micromesh carotid stent approved in the U.S., the company stated in a press release. The system is indicated for the treatment of carotid artery stenosis in patients at increased risk for adverse events following a carotid endarterectomy procedure.
The device is intended to treat patients with de novo atherosclerotic or post-endarterectomy restenotic lesions in the internal carotid arteries, or at the carotid bifurcation, with ≥50% stenosis in symptomatic patients or ≥80% stenosis in asymptomatic patients—as determined by angiography.
According to Terumo Neuro’s recent release, the device also accommodates vessel reference diameters between 3.5mm and 9mm at the target lesion.
“Percutaneous CAS is plagued by procedural embolic risk and worse outcomes over time in at-risk patients,” Stoner summarized. “TCAR solves the CAS embolic problem. Hard outcomes are equivalent to CEA or even better, and there is a strong patient preference toward minimal-access surgery.”
Taking up the case for CAS, Metzger reasoned that all of the carotid revascularization strategies “are excellent” and that there is no single gold standard. Clear-cut gains for transfemoral stenting include no general anesthesia and less stress on older or sicker patients, he said.
Disadvantages, on the other hand, include the fact that not all patient anatomies are suitable for CAS, Metzger noted. The case for CAS includes four randomized trials in which the strategy went up against CEA and, in one, medical therapy. “The last four randomized trials of carotid stenting versus endarterectomy have produced outstanding results for both therapies and their equivalent,” he said. With newer carotid stents emerging and contemporary results in CREST-2, “the results keep getting better.”
“There is no gender issue, there is no age issue, there are no limitations in timing of treatment”
BARBARA RANTNER
GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface*
Consult Instructions for Use eifu.goremedical.com
INDICATIONS FOR USE IN THE U.S.: The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in superficial femoral artery de novo and restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 – 7.5 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in superficial femoral artery in-stent restenotic lesions up to 270 mm in length with reference vessel diameters ranging from 4.0 – 6.5 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is indicated for improving blood flow in patients with symptomatic peripheral arterial disease in iliac artery lesions up to 80 mm in length with reference vessel diameters ranging from 4.0 – 12 mm. The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is also indicated for the treatment of stenosis or thrombotic occlusion at the venous anastomosis of synthetic arteriovenous (AV) access grafts. CONTRAINDICATIONS: The GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface is contraindicated for non-compliant lesions where full expansion of an angioplasty balloon catheter was not achieved during pre-dilatation, or where lesions cannot be dilated sufficiently to allow passage of the delivery system. Do not use the GORE® VIABAHN® Endoprosthesis with Heparin Bioactive Surface in patients with known hypersensitivity to heparin, including those patients who have had a previous incident of Heparin-Induced Thrombocytopenia (HIT) type II. Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available.
Compiled by Bryan Kay, Jocelyn Hudson and Jamie Bell
GORE® VIABAHN®
Endoprosthesis with Heparin Bioactive Surface*
NOW
Scan to learn more
5-YEAR PATENCY IN COMPLEX, REAL-WORLD SFA LESIONS.
The VIABAHN® Device demonstrated 85% primary patency at 1 year and 62% at 5 years.1
Patent VIABAHN® Device at 6-year follow-up
Images courtesy of Osamu Iida, M.D. Used with permission.
* As used by Gore, Heparin Bioactive Surface refers to Gore’s proprietary CBAS® Heparin Surface.
1. Iida O, Ohki T, Soga Y, et al. Five-Year outcomes of the GORE VIABAHN Endoprosthesis for the treatment of complex femoropopliteal lesions from a Japanese post-market surveillance study. Vascular Medicine 2024;29(4):416-423. W. L. Gore & Associates, Inc. Flagstaff, Arizona 86004 goremedical.com
Please see accompanying prescribing information in this journal.
Products listed may not be available in all markets.