Cardiovascular News – Issue 79 – November 2025 (US)
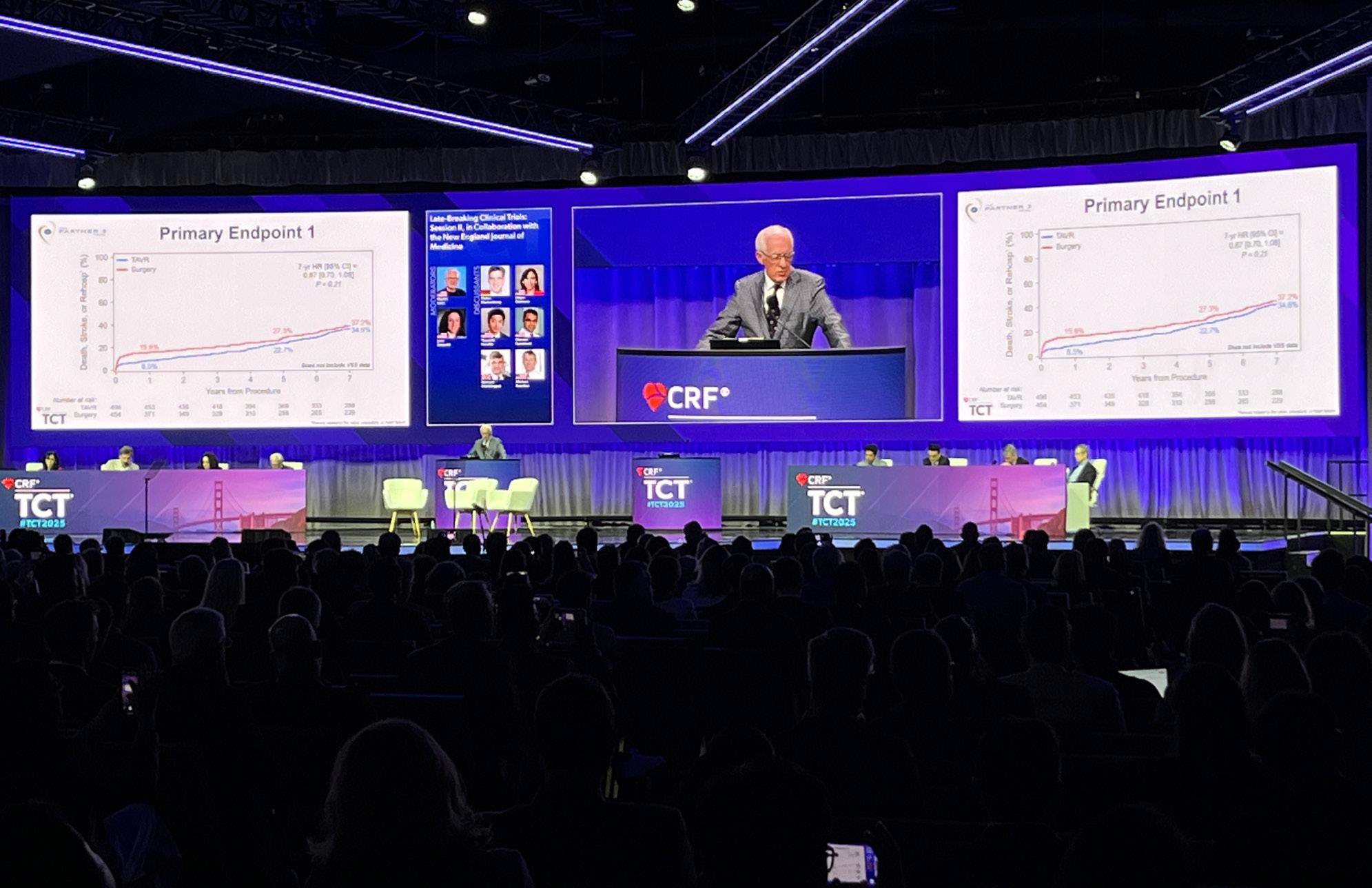
Seven-year outcome data from the PARTNER 3 trial of transcatheter aortic valve implantation (TAVI) and surgical aortic valve replacement (SAVR) in low surgical risk patients with severe, symptomatic aortic stenosis have shown similar rates of death, stroke or rehospitalisation for both therapies, though TAVI’s early advantage has narrowed over time.
The latest results from the trial, which are among the longest follow-up data for TAVI in low risk patients, were shared in a late-breaking trial session at the 2025 Transcatheter Cardiovascular Therapeutics (TCT) meeting (25–28 October, San Francisco, USA), presented by Michael Mack (Baylor Scott & White Research Institute, Dallas, USA), and published simultaneously in the New England Journal of Medicine (NEJM).
“As TAVI is increasingly performed in younger patients with longer life expectancy, understanding long-term transcatheter and surgical valve durability is essential to inform patientcentred decision-making,” Mack said in his presentation of the results at TCT.
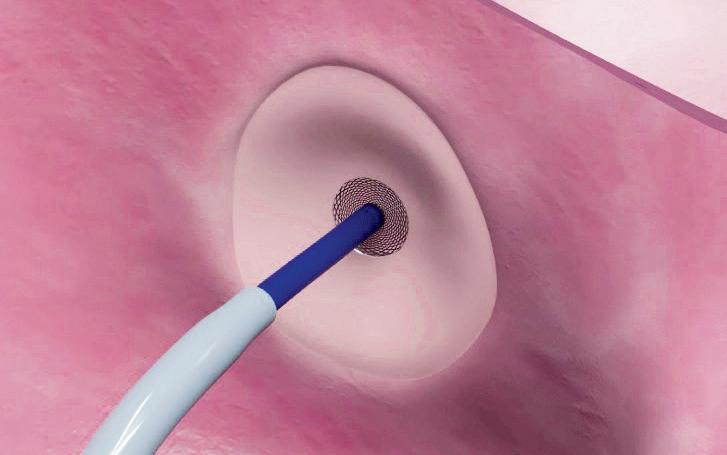
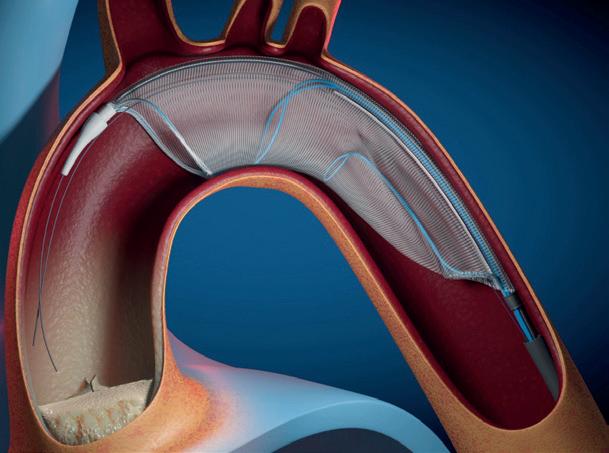
The trial enrolled 1,000 patients with severe symptomatic aortic stenosis between March 2016 and October 2017 who underwent either TAVI using the Sapien 3 (Edwards Lifesciences) balloon-expandable valve or surgery for severe aortic stenosis.
At the time of randomisation, the mean age was 73.3 years, 69.3% of patients were male, and the mean Society of Thoracic Surgeons (STS) predicted risk of mortality score was 1.9%, Mack detailed. The as-treated population included 496 TAVR and 454 surgery patients. Of those, 495 TAVR and 453 surgery patients received the intended valve.
Results at one and two years demonstrated superior or similar results for TAVI for the primary endpoints of death, stroke or rehospitalisation, though data from the trial at five
years, presented at TCT in 2023, showed an attenuation of the differences between the two groups in the primary endpoint.
From baseline to seven years, the first primary endpoint, consisting of a non-hierarchical composite of death, stroke, or rehospitalisation—defined as being related to the procedure, valve or heart failure—occurred in 37.2% of surgery patients compared with 34.6% of TAVI patients.
Death from any cause was 19.5% for TAVI versus 16.8% for surgery, stroke was 8.5% for TAVI versus 8.1% for surgery, and rehospitalisation occurred in 20.6% of TAVI patients compared with 23.5% for surgery. No significant differences were noted in rates of cardiovascular or non-cardiovascular death between TAVI and surgery at seven years.
AI model improves STEMI triage accuracy
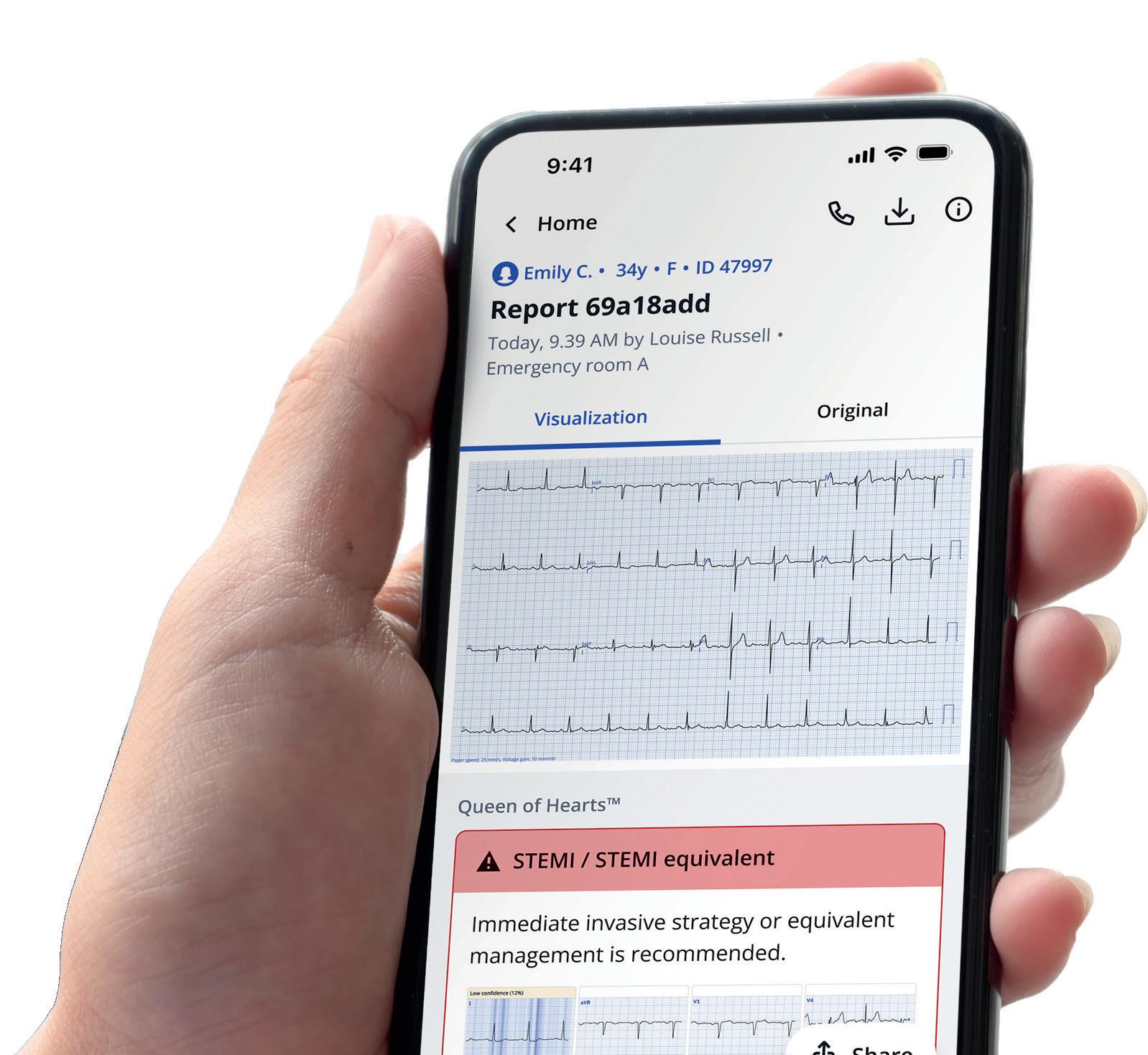
THE USE OF AN ARTIFICIAL intelligence (AI) algorithm to analyse electrocardiograms (ECG) may significantly improve the detection of ST-elevation myocardial infarction (STEMI) and STEMI equivalents, potentially shortening time to treatment and reducing false positive readings.
At the 2025 Transcatheter Cardiovascular Therapeutics (TCT) conference (25–28 October, San Francisco, USA) conference, Timothy Henry (The Christ Hospital Medical Center, Cincinnati, USA) presented the results of a retrospective analysis of the STEMI AI ECG model—Queen of Hearts (PMcardio)—using data from over 1,032 patients from three US primary PCI centres. Findings of the analysis were published simultaneously in JACC: Cardiovascular Interventions Rapid restoration of blood flow using percutaneous coronary intervention (PCI) is the standard of care in STEMI treatment; however, delays in achieving the guidelinerecommended time to reperfusion still persist, especially at centres not specialising in PCI and in rural areas. Time to reperfusion longer than 90 minutes is associated with threefold higher rates of mortality.
The win ratio for the second primary endpoint consisting of a hierarchical composite of death, disabling stroke, non-disabling stroke, and rehospitalisation days was 1.04.
Other key assessments including all-cause bioprosthetic valve failure (BVF) per VARC-3 criteria, which stood at 6.9% in the TAVI group and 7.3% in the surgery group, the report of the findings in NEJM detailed. At seven years, 73.4% of the patients in the TAVI group and 75% of the patients in the surgery group were alive without BVF. Aortic valve reintervention was required in 6.7% of TAVI patients and 6% of surgery patients. On functional and health-status endpoints, the investigators
“We’ve made tremendous progress in the treatment of STEMI over the last 20 years with primary PCI, and we can expect mortality of less than 4%. But there are still challenges,” Henry said, pointing out that in the region of 15–30% of STEMI activations have been shown to be false positives. Added to this, a high proportion may be STEMI equivalents, indicating a coronary occlusion without meeting the specific ST-elevation criteria.
The Queen of Hearts AI model has been trained on more than 2.5 million ECGs to identify both typical and atypical occlusions, and to distinguish them from benign patterns like early repolarisation or left ventricular hypertrophy.
Continued on page 3
PARTNER 3 shows similar outcomes for SAVR and TAVI at seven years in low-risk patients
Continued from page 1
report that the percentage of patients who were alive with New York Heart Association (NYHA) class I or II symptoms at seven years was 72.9% in the TAVI group and 75.9% in the surgery group.
Disease-specific health status at seven years appeared to be similar in the two groups, with a mean Kansas City Cardiomyopathy Questionnaire overall summary (KCCQOS) score of 84.9 in patients in the TAVI group and 86.2 in patients in the surgery group. At the seven-year timepoint, 233 of 395 patients (59%) in the TAVI group and 210 of 332 patients (63.3%) in the surgery group were alive with a KCCQ-OS score of more than 75; 65.5% and 66.6%, respectively, were alive with a KCCQ-OS score of more than 60 with a decline of 10 points or less from baseline.
The mean aortic valve gradient was 13.1±8.5mmHg in the TAVI group and 12.1±6.3mmHg in the surgery group, whilst the mean aortic-valve areas stood at 1.9±0.6cm2 and 1.8±0.5cm2, respectively. Mild, moderate, or severe paravalvular aortic regurgitation was present in 17.7% of the patients in the TAVI group and in 2% of the patients in the surgery group.
In the TAVI group, the investigators report that the seven-year mortality appeared to be similar among patients with no or trace paravalvular aortic regurgitation at 30 days after the procedure and among those with mild paravalvular regurgitation at 30 days after the procedure (18.7% and 20.7%, respectively).
Discussing the findings at TCT, Mack noted that from treatment through to the seven-year follow-up there had been a disparity in the number of patients available for analysis, with 36 TAVI patients lost to follow-up compared to 63 patients in the surgical arm—equating to 92.7% of patients available for follow-up in the TAVI group at seven years and 86% for surgery.
To address the missing data, researchers performed a vital status sweep, combing patient records and publicly available information to determine the mortality status on all patients. “We were able to find enough patients so that we had 95% follow-up in the TAVI arm and 94% in the surgery arm, so that we have mortality data on 95% of patients and about equal between TAVI and surgery,” said Mack. He noted that the analysis unearthed 13 patients in the surgery arm that had died and three patients in the TAVI arm.
“When surgery is the control group, there is less enthusiasm on the part of patients to come back for followup. Despite all efforts possible, that is what happens over and over again with surgical trials,” Mack commented, when asked to reflect on some of the reasons potentially underlying this disparity at TCT.
“What you can always speculate is patients that didn't come back because they're doing well or because they’re not doing well and they died. What we found is that in looking at this vital status sweep, there were 13 patients in the surgery arm that had died and three patients in the TAVI arm that had died. So, it means patients aren't coming back more commonly because they're not doing well, rather than because they're doing great and don't feel the need to come back.”
In their discussion of the findings in NEJM, Mack et al note that while TAVI is now accepted as an alternative therapy for eligible patients with severe, symptomatic aortic stenosis, recent randomised trials have also suggested that a change be made in the clinical management of severe, asymptomatic aortic stenosis, with an emphasis on the benefits of early referral and prompt aortic-valve replacement.
“Since low-risk patients are generally younger, longterm follow-up to assess late clinical outcomes and valve durability are needed to inform lifetime patient-care decisions,” they write. “Five-year results of randomised trials comparing TAVI with surgery in low-risk patients showed similar clinical outcomes and valve durability. This report of the seven-year outcomes from the PARTNER 3 trial extends these findings, showing no between-group differences in either of the composite primary end points or in their individual components.”
A consistent finding in the results has been an attenuation
Perhaps early benefits of a lessinvasive TAVI treatment with reduced periprocedural complications were counterbalanced by an increased vulnerability to late adverse events in low-risk patients.”
of the between-group difference in primary endpoint events, the authors note, which favours TAVI over surgery in the first year with no between-group differences apparent during longer follow-up.
“A greater number of deaths, from both cardiovascular and non-cardiovascular causes, occurred from year one to year seven among patients who were assigned to TAVI than among those assigned to surgery. Greater numbers of strokes and rehospitalisations in the TAVI group than in the surgery group after the first year were also observed. Perhaps early benefits of a less-invasive TAVI treatment with reduced periprocedural complications were counterbalanced by an increased vulnerability to late adverse events in low-risk patients.”
Patients will be followed out to 10 years.
Editor-in-chief: Simon Redwood | Publisher: Stephen Greenhalgh
Senior editor: Will Date will@bibamedical.com | Editorial contribution: Jamie Bell, Jocelyn Hudson and Éva Malpass
New joint guidelines from the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) lay out a series of updated recommendations for the treatment of heart valve diseases. Key among the revisions is a lowered age threshold for transcatheter aortic valve implantation (TAVI) for the treatment of aortic stenosis, as well as a greater emphasis on transcatheter options in the treatment of both mitral and tricuspid valve disease.
For more on this story go to page 4.
n LATEST DCB DATA:
New coronary device technologies took centre stage at the 2025 Transcatheter Cardiovascular Therapeutics (TCT) meeting (25–28 October, San Francisco, USA). Christian Spaulding (Paris, France) presented late-breaking data from the SELUTION DeNovo trial, showing encouraging results with the Selution SLR (Cordis) drug-eluting balloon (DEB) in de novo coronary artery disease.
For more on this story go to page 9.
n EDWARDS INTERVIEW:
Following a series of high-profile acquisitions and investments over the last 18 months, Edwards Lifesciences’ vice president for EMEA, Canada and Latin America, Annette Brüls, speaks to Cardiovascular News about the company’s ambitions to grow its footprint in the structural heart space.
For more on this story go to page 27.
Scan the QR code to subscribe
If you have comments on this issue or suggestions for upcoming editions write to will@bibamedical.com
AI model improves STEMI triage accuracy Continued from page 1
The study used a multicentre STEMI registry from the University of California Davis (Davis, USA), UT Health Houston (Houston, USA), and Beth Israel Deaconess (Boston, USA), involving STEMIs occurring between January 2020 and May 2024, retrospectively comparing the AI model to the standard decision of activation.
Each patient’s initial ECG underwent analysis by the STEMI AI ECG Model trained to detect acute coronary occlusion, including STEMI equivalents, and differentiate from benign mimics. Angiography and biomarkers confirmed that 601 (58%) were STEMIs and 431 (42%) were false positives. The AI ECG model did better than standard triage, detecting 553 of 601 confirmed STEMIs vs. 427 detected by standard triage on the initial ECG. AI ECG had a false positive rate of 7.9% vs. 41.8% for standard triage, representing a fivefold reduction.
“The overall results show a sensitivity and specificity that were significantly higher compared to the standard of care,” Henry said of the results. “In particular there was a remarkable drop in the false positive rate, which I think is really important.”
The study also highlighted variability of STEMI activation within the three centres.
“In some sites the problem is too many false positives, where they're activating too much. Other sites are too slow in activating,” Henry said. “This has the ability to decrease that variability.”
Overall, Henry said that adoption of the AI model could help to reduce false positives and identify more STEMI patients on the index ECG, leading to shorter time-to-treatment and reducing triage variability across sites.
“Emergency departments or hospitals in the middle of the night are extremely busy” he commented. “If you get an ECG, you can imagine a system will use the AI, which will then put out,
Our goal is to get to the cath lab as fast as possible, and this will help.”
this is highly likely, or this is positive or probable, and then that will generate a call directly to the cardiologist, that’ll activate the system.
“What we want to do is be more accurate in who comes to the cath lab in the middle of the night with a STEMI, because it's a
Semaglutide prevents cardiovascular events regardless of weight loss
Analysis of the SELECT trial—assessing the cardiovascular impact of the diabetes and anti-obesity medication semaglutide (Wegovy, Novo Nordisk)—has found that the use of the drug significantly reduced the risk of major adverse cardiovascular events (MACE) regardless of the amount of weight individuals lost.
FINDINGS OF THE PRESPECIFIED analysis of the trial, published in The Lancet, suggest that semaglutide and possibly other glucagon-like peptide-1 receptor agonists (GLP-1Ras) should be reconceptualised as disease-modifying treatments rather than solely medications for glycaemic control or weight loss, the study’s authors have suggested. Results of the SELECT trial, which originally studied over 17,000 adults with heart disease and a body mass index (BMI) ≥27kg/m², comparing semaglutide to placebo, demonstrated that that those taking the drug for more than three years had a 20%
life-threatening situation, and it’s very time sensitive.
“Most of these patients make it to the cath lab eventually, but if you have longer time to treatment, you end up with bigger infarcts, and those patients are more likely to have heart failure or to have cardiac arrest while they're waiting. Our goal is to get to the cath lab as fast as possible, and this will help.”
In an accompanying editorial comment, published in JACC:
Cardiovascular Interventions, Mohamad Alkhouli (Mayo Clinic, Rochester, USA) said the researchers should be “commended for developing an operational AI model aimed at
complex and error-prone aspects of interventional cardiology practice— STEMI activation.”
However, he emphasised that the AI model employed in the study should be interpreted with caution, as it was originally developed to detect occluded arteries rather than STEMI and necessitates further prospective validation across diverse patient populations.
“The true challenge is not proof of accuracy alone, but readiness—to integrate, regulate, and interpret AI as a complement to human judgment, particularly in high-stakes, timesensitive clinical settings,” Alkhouli said.
lower risk of heart attack, stroke or death due to cardiovascular disease and lost an average of 9.4% of their body weight.
In their latest study, the researchers found that the reduction in MACE was similar regardless of a participant’s weight at the start of the trial—with those only marginally classed as overweight (BMI of 27kg/m2) seeing similar benefits to those with a much higher BMI. Greater waist circumference reduction at 20 months was associated with a lower subsequent MACE risk, they reported, which accounted for an estimated 33% of the observed benefit of the drug.
“These findings suggest that the cardioprotective effects of semaglutide extend beyond its impact on adiposity, with important implications for clinical practice and understanding of the mechanisms responsible for the benefits from GLP1-Ras,” John Deanfield (University College London, London, UK) and colleagues write in their Lancet paper detailing the results.
Several potential mechanisms may explain the cardiovascular benefit of semaglutide beyond adiposity reduction, the study’s authors suggest, including effects on endothelial function and other
You don’t have to lose a lot of weight and you don’t need a high BMI to gain cardiovascular benefit.”
atherosclerotic pathways, modulation of inflammation, or effects on blood pressure control, for example.
“These pleiotropic effects of GLP-1Ras on multiple organ systems indicate a complex network of beneficial mechanisms that might be independent of adipose tissue reductions reflected by weight or waist circumference change,” the authors write.
“Furthermore, adipose tissue biology undoubtedly changes before the mass of adipose tissue is measurably reduced, and this may in part mediate the earliest effects of semaglutide on MACE.”
The temporal dissociation between weight loss and MACE reduction observed in our study supports the hypothesis that these and other mechanisms may play a key role in vascular protection, the authors add.
“This work has implications for how semaglutide is used in clinical practice,” Deanfield said of the findings. “You don’t have to lose a lot of weight and you don’t need a high BMI to gain cardiovascular benefit. If your aim is to reduce cardiovascular disease, restricting its use to a limited time only and for those with the highest BMIs doesn’t make sense.”
“At the same time, the benefits need to be weighed against potential side effects. Investigations of side effects become especially important given the broad range of people this medicine and others like it could help.”
The authors of the study note some limitations, including the predominantly white male population, and that analysis of MACE outcomes according to post-randomisation changes in weight or waist circumference within the treatment groups is subject to confounding and therefore cannot prove causation or define mechanisms.
Queen of Hearts AI platform
Trial data prompt change in age threshold for TAVI in European valvular heart disease guidelines
The latest randomised trial evidence has contributed to new joint guidelines from the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) for the management of valvular heart disease, which include revised age thresholds for transcatheter aortic valve implantation (TAVI), among other major updates.
LAUNCHED AT THE ESC’S 2025 Congress (29 August–1 September, Madrid, Spain), the new guidelines, published in the European Heart Journal, replace a previous iteration of the document released in 2021, and reflect new evidence in the treatment of aortic, mitral and tricuspid disease.
On aortic stenosis, the guideline prompts heart teams to consider factors including clinical characteristics such as age, estimated life expectancy, concomitant conditions and patient preference, as well as access and valve anatomy, alongside the potential need for future procedures, when weighing up TAVI or surgical aortic valve replacement (SAVR).
Among the most notable of the amended recommendations, the age threshold for TAVI has been extended to cover anatomically suitable patients aged 70 years or older— down from 75 years in the previous version—irrespective of the estimated surgical risk, if they have tricuspid valve anatomy.
“The taskforce felt that this age cut-off better reflects the population of patients that has been included into randomised controlled trials that compare surgical aortic valve replacement with transcatheter aortic valve implantation in a sizeable population across surgical risk, and these trials—if we summarise them in a quick way—show that TAVI is noninferior at least to surgical aortic valve replacement,” said Fabien Praz (Bern University Hospital, Bern, Switzerland), who co-chaired the joint ESC and EACTS guidelines task force that drafted the document alongside Michael Borger (Leipzig Heart Center, Leipzig,
Germany), during a press conference at ESC 2025.
“There is an increasing amount of data from these randomised trials in patients aged 70 and over demonstrating very good early and mid-term outcomes and therefore we felt comfortable lowering the age limit,” added Borger.
Borger acknowledged that this amendment has drawn a degree of controversy amongst the cardiac surgery community and he was questioned on the rationale for the change in the age threshold for TAVI when he set out details of the new guidelines at the 2025 EACTS annual meeting (8–11 October, Copenhagen, Denmark), where he commented that this was the recommendation “that we get criticised the most for”. However, he said that the emergence of data from the DEDICATE study, demonstrating non-inferiority of TAVI to SAVR in low- or intermediaterisk patients at one year, as well as the publication of the results of a metaanalysis in the Journal of the American College of Cardiology (JACC) showing a decreased rate of all-cause death in TAVI compared to SAVR and a significantly decreased rate of all-cause death or stroke at five years—both of which occurred during the drafting of the guidelines—had a significant bearing on the recommendations. The weight of randomised trial data favouring TAVI, from trials including PARTNER 3, Evolut Low-Risk and UK TAVI, which did not show any worse outcomes for TAVI at five years compared to surgery, he said, had also tipped the balance.
“If you are dealt those cards as a guidelines taskforce chairman, I would please ask somebody here to try to come up with a better recommendation than
that earlier intervention is a recurring theme across the guidelines, pointing to new recommendations for the treatment of severe primary mitral regurgitation (MR), including a new class Ia recommendation for early surgical repair of asymptomatic patients. “We want to operate earlier in the patient's disease process to prevent long-term negative consequences, that is a recurring theme throughout the guidelines—intervene earlier, operate earlier, before it is too late,” Borger said.
Michael Borger and
Fabien
Praz
what we ended up with here,” he said at the EACTS meeting. “Retrospective data will not cut it; we need prospective randomised trials with wins for surgery. There are no wins for surgery in SAVR versus TAVI trials thus far.”
Borger also acknowledged that though life expectancy is theoretically a better determinant of treatment outcome than age alone, challenges in predicting this across a wide geographical area, make age cutoffs a more pragmatic choice for inclusion in the guidelines. “Life expectancy is very difficult to determine, and is very regional, even within countries it is hard to tell how long a patient is going to live, and therefore age is the best surrogate that we all agreed to,” he said.
This age cut-off better reflects the population of patients included in randomised trials.”
Elsewhere in the guidelines, treatment of patients with asymptomatic severe high-gradient aortic stenosis now carries a class IIa recommendation encouraging early intervention—albeit agnostic to treatment modality— reflecting new evidence in this area from trials including EARLY TAVR and EVOLVED.
“The overall feeling of the taskforce was that the evidence was there for this level of recommendation, but that the overall way the trials were designed in terms of the number of patients included and the endpoints of the trials were not convincing enough to make it a level I recommendation,” commented Praz. “The final decision needs to be made in the heart team.”
Speaking at EACTS, Borger said
Reflecting data from the UK Mini Mitral trial, which found comparable outcomes and quality of life in patients who received minimally invasive or conventional surgical mitral valve repair, the guidelines support the use of minimally invasive mitral valve surgery—particularly via minithoracotomy or similar approaches—as a viable option in experienced centres for patients with primary mitral regurgitation (class IIb, level B).
Other updates in mitral valve disease include revised guidelines for transcatheter edge-to-edge repair (TEER) for primary MR in high-risk patients now carries a class IIa, level B recommendation, and may be considered in symptomatic patients with severe atrial secondary MR who are not eligible for surgery. In patients with heart failure and symptomatic severe ventricular secondary mitral regurgitation (left ventricular ejection fraction [LVEF] <50%) fulfilling specific criteria, TEER has a class I recommendation to reduce heart failure hospitalisations and improve quality of life.
“We are still learning about this valve but there have been major advances since 2021 that have been reflected,” said Praz on how the guidelines reflect new evidence on treatment options for the tricuspid valve. Changes have seen the indication for concomitant tricuspid valve repair in patients undergoing leftsided surgery associated with moderate or severe tricuspid regurgitation reinforced, while transcatheter treatment of the tricuspid valve is considered to improve quality of life and right ventricular (RV) remodelling in highrisk patients with symptomatic severe tricuspid regurgitation (TR).
The new document also acknowledges the increasing role of advanced imaging techniques, such as 3D echocardiography, cardiac computed tomography (CCT), and cardiac magnetic resonance (CMR) imaging in screening and evaluating patients with valvular heart disease.
Joint decision-making sits at the core of many of the recommendations, with the importance of shared and patient-centred decision-making by multidisciplinary expert heart teams working within a regional network having been reinforced. Additionally, the guidelines establish the importance of referring patients with complex conditions or requiring complex procedures to high-volume centres, where corresponding expertise is concentrated to ensure highquality treatment.
CRACKING THE NEXT BIG THING TOGETHER
Shockwave Medical is Now Part of J&J MedTech
Shockwave IVL transformed the way you treat calcified vessels. What’s next? We’re powering up to generate a new wave of IVL innovation thanks to the added strength of the global leader in healthcare.
“Site-less” trial offers glimpse at the scale of undiagnosed valvular heart disease
Investigators behind a “site-less” trial involving remote screening for valvular heart disease of subjects recruited at pharmacies across the USA say their study points towards a large population of older adults living with significant, undiagnosed aortic, mitral or tricuspid valve disease throughout the country.
RESULTS FROM THE PREVUE-VALVE STUDY, presented by David J Cohen (St Francis Hospital and Heart Center, Roslyn, USA) at the 2025 Transcatheter Cardiovascular Therapeutics (TCT) conference (25–28 October, San Francisco, USA) point towards at least 4.7 million adults aged between 65–85 living with moderate or greater valvular heart disease in the USA, and at least 10.6 million with clinically significant valvular disease, most of whom are unaware of their condition. The prevalence of valve disease increases sharply with advanced age, the researchers state.
“With the ageing population, we know the incidence and prevalence of valvular heart disease are increasing in the USA as well as around the developed world. Despite a number of novel treatments for valve disease, patients often remain untreated or are treated too late,” said Cohen, setting out the rationale for the study. “In order to optimise our screening efforts and improve patient access to these therapies, we need to understand the true prevalence of valvular heart disease. But, all studies previous to this have had important methodological limitations that preclude getting a truly accurate assessment of valve disease prevalence.”
To reach a group of patients that was felt to be more representative of the wider US population, the study team used databases of customers of the CVS and Walgreens pharmacy chains to identify, sample, and recruit a random sample of individuals aged 65–85 to
participate in the study using a combination of e-mail, text messaging, and direct mail. Individuals were encouraged to participate by being offered a US$25 Amazon voucher.
“The strategy for sampling was based on age, sex, as well as predicted race and ethnicity to ensure that the study cohort was broadly representative of the US population,” explained Cohen.
most common type of valvular disease followed by aortic stenosis (3.1%), mitral regurgitation (2%) and aortic regurgitation (0.7%).
When study participants with mild to moderate valvular disease were also included, the overall prevalence increased to 18.4% with the rate also increasing with age (31.4% in the 80–85 cohort compared with 12.1% for 65–69 years of age).
After initial screening, a total of 3,000 people then received an at-home visit during which a 12-lead electrocardiogram and a formal echocardiogram were performed. Blood samples (upon patient consent) and standardised health status assessments were also collected. Electrocardiogram and echocardiogram assessments (including diagnosis and assessment of severity of valvular heart disease) were performed by independent core laboratories.
The study’s primary endpoint was the population prevalence of moderate or greater valvular heart disease and its individual components including aortic stenosis, aortic regurgitation, mitral stenosis, mitral regurgitation or tricuspid regurgitation. The study found that the overall prevalence of moderate or greater valvular disease was 8.2%. The prevalence increased with advanced age (5.1% in patients 65–69, 7% for 70–74, 10.5% for 75–79 and 14.7% for 80–85 years of age). Tricuspid regurgitation (3.7%) was the
AI helps smartwatch ECG sensors to detect structural heart disease
An artificial intelligence (AI) algorithm paired with the single-lead electrocardiogram (ECG) sensors on a smartwatch accurately diagnosed structural heart diseases, presented at the 2025 American Heart Association scientific sessions (7–10 November, New Orleans, USA) has demonstrated.
RESEARCHERS SAID THIS IS the first prospective study to show that an AI algorithm can detect multiple structural heart diseases based on measures taken from a single-lead ECG sensor on a smartwatch.
“Millions of people wear smartwatches, and they are currently mainly used to detect heart rhythm problems such as atrial fibrillation. Structural heart diseases, on the other hand, are usually found with an echocardiogram, an advanced ultrasound imaging test of the heart that requires special equipment and isn’t widely available for routine screening,” said study author Arya Aminorroaya (Yale School of Medicine, New Haven, USA).
“In our study, we explored whether the same smartwatches people wear every day could also help find these hidden structural heart diseases earlier, before they progress to serious complications or cardiac events.”
Researchers developed the AI algorithm using more than 266,000 12-lead ECG recordings from more than 110,000 adults. Based on this library of data, they developed an algorithm to identify structural heart disease from a single-lead ECG that can be obtained using smartwatch sensors. For this purpose, researchers isolated only one of the 12 leads of the ECG, which resembles the single-lead ECG on smartwatches. They also accounted for random interference in ECG signalling or “noise” that could arise during the recording of a singlelead ECG using smartwatches. The model was externally validated using data from people seeking care at community hospitals, as well as data from a population-based study from Brazil. They prospectively recruited 600
Tricuspid regurgitation was the most common type of valvular disease (10.7%) when including mild to moderate disease.
A further analysis using census data from the USA suggested that at least 4.7 million people between the ages of 65–85 are living with moderate or greater valvular disease, and at least 10.6 million have greater than mild disease. Based on current census projections, the absolute prevalence of moderate or greater valvular disease is projected to increase by about 1.8 million by 2060, the study’s authors suggest, driven largely by a 74% increase among the 80–85-year-old age group.
PREVUE-VALVE also found that age-adjusted and sex-adjusted prevalence of valvular disesae is approximately 20% lower among Black versus White individuals in the USA, driven largely by lower rates of aortic valve disease.
“Our study demonstrates the power of using novel approaches to recruit and enrol individuals who are broadly representative of the US population,” Cohen said of the potential impact of the research “I'm hopeful that application of these concepts to future clinical trials can greatly enhance their generalisability to the full spectrum of affected individuals.”
The study was an investigator-initiated study sponsored by the Cardiovascular Research Foundation funded by investigator-initiated grants from Abbott, Edwards Lifesciences, and Philips.
participants who underwent 30-second, single-lead ECGs using a smartwatch to gauge the algorithm’s accuracy in a real-world setting.
The analysis found, using single-lead ECGs obtained from hospital equipment, the AI model was very effective at distinguishing between people with and without structural heart disease, scoring 92% on a standard performance scale.
Among the 600 participants with the single-lead ECGs obtained from a smartwatch, the AI model maintained high performance at 88% for detecting structural heart disease. Additionally, the algorithm accurately identified most people with heart disease (86% sensitivity) and was accurate in ruling out heart disease (99% negative predictive value).
Researchers used a database of
We plan to evaluate the AI tool in broader settings and explore how it could be integrated into communitybased heart disease screening programmes.”
266,054 ECGs from 110,006 patients who received testing and treatment at Yale New Haven Hospital between 2015 and 2023 to develop the AI-ECG algorithm. The algorithm was matched to ultrasound scans to see whether they had structural heart disease or not.
The AI model was then validated in 44,591 adults seeking care at four community hospitals and 3,014 participants from the population-based ELSA-Brasil study. The Brazilian Longitudinal Study of Adult Health (ELSA-Brasil) gathers important information about how chronic diseases develop and progress, focusing mainly on cardiovascular diseases and diabetes.
During the study, 600 patients wore the same type of smartwatch with a single-lead ECG sensor for 30 seconds on the same day they were getting a heart ultrasound. The median age of the participants was 62 years, and about half were women, 44% were non-Hispanic white, 15% non-Hispanic Black, 7% Hispanic, 1% Asian and 33% others. About 5% were found to have structural heart disease on the heart ultrasound.
Study limitations include a small number of patients with the actual disease in the prospective study and the number of false positive results.
“We plan to evaluate the AI tool in broader settings and explore how it could be integrated into communitybased heart disease screening programmes to assess its potential impact on improving preventive care,” Aminorroaya said.
David J Cohen
Enable imaging for all patients
Enhancing structural heart interventions with integrated imaging solutions
At the heart of our innovation is the patient.
With our expansive AI-driven portfolio of integrated, comprehensive imaging solutions, we help harness the power of precision medicine, empowering clinicians to confidently manage the entire continuum of cardiovascular care - from early detection to post-procedure assessment. Designed to increase procedural consistency, improve visualization, and enhance workflow efficiency, we’re setting a new standard in the treatment of structural heart disease, helping to improve both patient outcomes and overall hospital performance.
Timing DAPT based on risk score may reduce risk of adverse events
Tailoring dual antiplatelet therapy (DAPT) for patients who have undergone percutaneous coronary intervention (PCI) based on a risk score—taking into account the patient’s ischaemic and bleeding risk—lowers their risk of net adverse clinical events (NACE) compared to a standard 12-month DAPT regime.
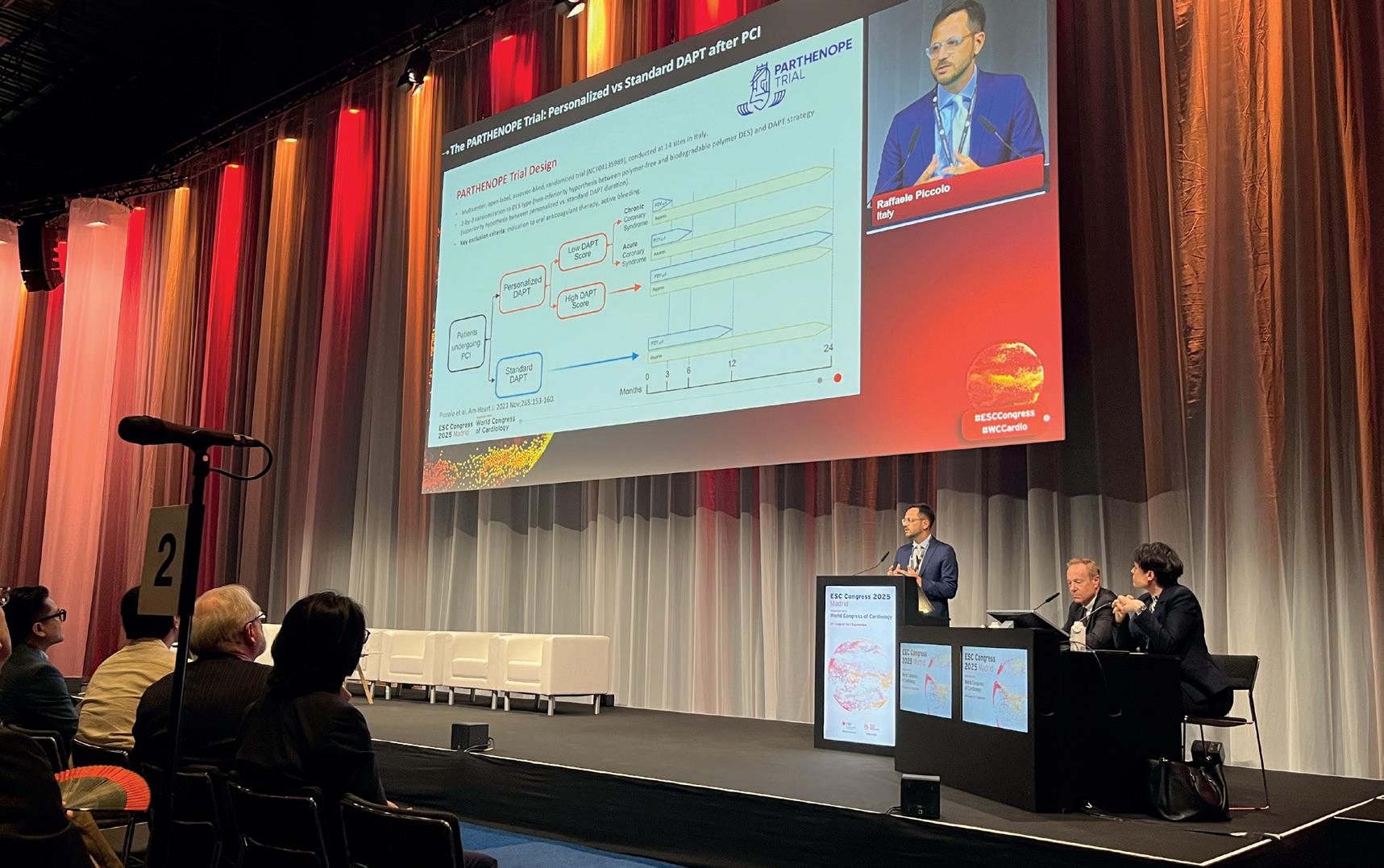
THIS IS THE HEADLINE FINDING OF THE PARTHENOPE trial, a randomised trial comparing outcomes in patients who received a “personalised” course of DAPT lasting either three, six or 24 months based upon their risk score criteria, against those undergoing the standard 12 months of DAPT in line with guideline recommendations.
Presenting findings of the study at the 2025 European Society of Cardiology (ESC) congress (29 August–1 September, Madrid, Spain), Raffaele Piccolo (University of Naples Federico II, Naples, Italy) reported that the benefit of the personalised DAPT regime was principally related to a lower risk of ischaemic events, including myocardial infarction (MI) and urgent target-vessel revascularisation, and the strategy was not associated with any excess of bleeding compared to a standard approach.
Current guidelines recommend DAPT for 12 or six months followed by aspirin monotherapy after PCI in chronic coronary syndrome patients and for 12 months after PCI in patients with acute coronary syndrome, said Piccolo during his presentation of the trial’s results at ESC 2025, though the optimal duration of DAPT remains highly debated.
“In the past few years several risk scores have been proposed to guide the duration of DAPT; however, there has been no prospective validation of these
scores, and in this context the DAPT score is probably a unique tool that enables evaluation at the same time as the ischaemic and bleeding risk profile,” he said.
PARTHENOPE investigators used the DAPT score developed by Robert Yeh (Beth Israel Deaconess Medical Center, Boston, USA), which uses nine clinical variables including age, smoking status,
If one focuses on patients at high ischaemic risk—a high DAPT score—there is no additional risk of extending DAPT in terms of bleeding.”
diabetes, prior MI or PCI and others to stratify patients’ risk from low to high to inform their strategy for DAPT.
“We are used to seeing score validation based on calibration and discrimination metrics, which is great,” Piccolo comments to Cardiovascular News. “However, a true test of a score’s utility is whether randomisation to a score-guided versus unguided strategy is clinically
DUAL-ACS trial finds “less is more” for DAPT after acute MI
A three-month course of dual antiplatelet therapy (DAPT) after an acute myocardial infarction (MI) appears to come with a better rate of survival and a lower risk of bleeding than the standard 12 months of DAPT, data presented at the 2025 European Society of Cardiology (ESC) congress (29 August–1 September, Madrid, Spain) have shown.
THE DATA—WHICH ARE consistent with prior meta-analyses showing similar signals—should prompt a reconsideration of guidelines recommending 12 months of DAPT among this patient population, the trial’s lead investigator, David Newby (University of Edinburgh, Edinburgh, UK) has said.
Newby presented the results of DUAL-ACS, an open-label, investigator-initiated, randomised trial, which compared outcomes of both DAPT regimens amongst acute MI patients at centres in Scotland, England and New Zealand, during an ESC hot line trial session on day three of the 2025 congress.
useful. This is probably one of the principal novelties of PARTHENOPE.”
Patients randomised to the standard DAPT arm received DAPT for 12 months with P2Y12 inhibitors and aspirin, followed by aspirin monotherapy for a further 12 months.
For those randomised to the personalised therapy arm, if they had a low DAPT score, those with chronic coronary syndrome received P2Y12 inhibitors plus aspirin for three months, followed by aspirin monotherapy up to 24 months, or P2Y12 inhibitors plus aspirin for six months followed by aspirin monotherapy up to 24 months for those with acute coronary syndromes. Patients with high DAPT scores received P2Y12 inhibitors plus aspirin for the full 24 months.
The primary NACE endpoint of the trial was a composite of all-cause death, MI, stroke, urgent target vessel revascularisation and BARC type II, III or V bleeding. Among the 2,107 patients enrolled in the trial, Piccolo reported that there was a high prevalence of diabetes, whilst acute coronary syndrome made up more than 70% of the cases. Patients had a median DAPT score of 2, whilst 60% were considered to have a high score.
Among the patients randomised to personalised DAPT, 15.2% of patients had three months, 24.5% six months, and 60.3% had 24 months.
The primary endpoint occurred in 22.2% of patients in the standard DAPT group, Piccolo detailed, compared to 18.6% in the personalised DAPT group, with a statistically significant p-value of 0.04 which corresponded to a relative reduction of 20% for the risk of NACE.
“If we look at the components of the primary endpoint, I think it is important to highlight that most of the benefit was driven by a decreased risk of any myocardial infarction and urgent target vessel revascularisation,” Piccolo explained. “There was no excess of bleeding in the patients randomised to the personalised versus standard DAPT strategy.”
Landmark analysis of the data revealed that most of the benefit was seen late—from 12 to 24 months—and was attributable to a reduction in ischaemic rather than the bleeding component of the endpoint.
“In an almost all-comer PCI population, a personalised DAPT duration, gradually extended from three to 24 months based on the DAPT score, was superior to a standard 12-month approach in terms of net clinical benefit,” Piccolo said in his concluding remarks. “The benefit from personalised DAPT emerged during late follow-up—from 12 to 24 months—and the reduction in NACE was principally related to a lower risk of ischaemic events, including myocardial infarction and urgent target-vessel revascularisation.
Initially intended to recruit more than 17,000 patients, enrolment was cut short due to the COVID-19 pandemic, he explained, which only allowed the investigators to randomise 5,052 patients among the two study groups. Patients had a mean age of 63 years and 27% were female. Following the index admission, 23% received medical management only, 70% underwent percutaneous coronary intervention (PCI) and 6% had coronary artery bypass graft (CABG) surgery.
Results of the trial after follow-up of 15 months showed that the primary endpoint of all-cause mortality occurred in 2.7% of patients in the three-month DAPT group and 3.4% of patients in the 12-month DAPT group, with a hazard ratio (HR) of 0.78, with no difference in cardiovascular death or non-fatal MI
(HR 1.04). Fatal and non-fatal major bleeding occurred in 3.2% of patients in the three-month DAPT group and 4% of patients in the 12-month DAPT group (HR 0.78).
“In the absence of demonstrable benefit, and certain signals of harm that are consistent with prior data, really we should be giving patients three months of antiplatelet therapy after a heart attack and not 12 months,” said Newby.
“For patients, I am sure they would want to take the tablets for the least time possible, but also given that there is no benefit to extending that treatment, and there are real signals of harm, we really do need to be pulling back on this.”
“I would suggest to you that less is more, and that we should now reconsider what the guidelines say,” Newby summarised.
Sirolimus-eluting balloon meets primary endpoints in de novo and ISR trials
Results of the SELUTION DeNovo and SELUTION4ISR trials, presented during a late-breaking trials session at the 2025 Transcatheter Cardiovascular Therapeutics (TCT) meeting (25–28 October, San Francisco, USA), have demonstrated the safety and efficacy of the Selution SLR drug-eluting balloon (DEB, Cordis) for the treatment of de novo coronary artery disease and coronary in-stent restenosis (ISR).
SELUTION DENOVO WAS THE first of two major late-breaking trials involving the Seluton SLR DEB to gain major prominence on the TCT main arena stage. The trial, which enrolled an all-comer population of over 3,000 percutaneous coronary intervention (PCI) patients from Europe and Asia, compared a DEB strategy to routine drug-eluting stent (DES) implantation for the treatment of de novo coronary disease.
Persistent rates of adverse events seen with DESs, which number in the region of 2–4% per year, have driven an interest in strategies that potentially minimise the need for metallic stent implantation to reduce late events, SELUTION DeNovo principal investigator Christian Spaulding (Hôpital Européen GeorgesPompidou, Paris, France) commented.
The trial, which has been described as the largest coronary DCB trial to date, tested both strategies against a primary endpoint of target vessel
failure—comprised of cardiac death, target vessel-related myocardial infarction (MI) and clinically driven target vessel revascularisation in both arms, with an assumed event rate of 6% in both arms and a margin for noninferiority of 50%.
The DEB strategy comfortably met this mark at one year, with a reported event rate of 5.3% compared to 4.4% in the DES strategy group. Investigators will follow patients out to five years to assess long-term non-inferiority and potential superiority of the DEB.
“With no acute or late safety concerns, these results apply to a significant segment of PCI procedures including high-risk patients and complex lesions,” said Spaulding.
Critics of the trial have pointed to the relatively wide margin for noninferiority and the fact that around one-fifth of patients in the DEB group required bailout stenting, though Spaulding commented at TCT that the target vessel failure (TVF) rate in
patients receiving only the DEB stood at around 5%, showing that this had not greatly influenced the result.
“There was applause in the room, but the full publication is still pending, so caution is warranted,” Davide Capodanno (University of Catania, Catania, Italy) wrote in a post on his X account. “This is particularly true since analyses were reported as intention-totreat, which in a non-inferiority trial does not tell the whole story (it would be important to see the as-treated and per-protocol analyses), and because some statistical interactions were not immediately clear and somewhat
The same device featured in a second randomised trial, SELUTION4ISR, conducted among more than 400 patients in the USA, in which Selution SLR was compared to a standard-ofcare control group consisting of 80% DESs and 20% balloon angioplasty for the treatment of bare-metal and DES in-stent restenosis (ISR).
counterintuitive. In any case, an absolute difference of 0.9% between the two arms appears acceptable at one year, especially if noninferiority is maintained at five years and a benefit emerges consistent with the expected advantages of leave-nothing-behind strategies.”
Alteplase fails to impact outcomes in STEMI patients with high thrombus burden
Low-dose intracoronary fibrinolysis infusion during primary percutaneous coronary intervention (PCI) for ST-segment elevation myocardial infarction (STEMI) has been shown not to be effective in reducing major adverse cardiovascular events (MACE).
THIS WAS THE HEADLINE FINDING FROM the STRIVE multicentre, randomised, double-blind, placebo-controlled trial, in which it was found that low-dose administration of the recombinant tissue plasminogen activator (tPA) alteplase in patients with large-territory STEMI and high thrombus burden undergoing primary PCI did not improve outcomes.
Shamir Mehta (McMaster University and Hamilton Health Sciences, Hamilton, Canada) presented the findings during a late-breaking presentation at the 2025 Transcatheter Therapeutics (TCT) conference (25–28 October, San Francisco, USA), and the data were simultaneously published in the Journal of the American College of Cardiology
Approximately one-half of patients with apparently successful primary PCI for STEMI have distal embolisation of thrombus causing coronary microvascular obstruction and reduced myocardial tissue perfusion, Mehta detailed. This leads to larger infarct size and higher rates of heart failure, cardiogenic shock and mortality.
The STRIVE trial evaluated a strategy to prevent and treat microvascular obstruction and reduce major cardiovascular events by delivering alteplase, a
fibrin-specific thrombolytic, directly into the culprit coronary artery.
Patients who presented with STEMI within six hours of symptom onset and were referred for primary PCI were eligible for the study. All patients were required to have evidence of large territory STEMI on electrocardiogram (ECG) and evidence of large thrombus burden on coronary angiography.
A total of 210 patients were randomised to receive the study drug or placebo (68 received alteplase 10mg, 69 received alteplase 20mg and 70 were given placebo). After antegrade flow was established, a delivery catheter was inserted into the infarct-related artery distal to the culprit lesion and the study drug was infused over three minutes. Primary PCI was performed per standard practice.
With no acute or late safety concerns, these results apply to a significant segment of PCI procedures including highrisk patients and complex lesions.” STRIVE does not support the routine administration of alteplase.”
The trial’s primary endpoint was target lesion failure (TLF) consisting of cardiac death, target vessel MI, or clinically driven target lesion revascularisation at one year. TLF occurred in 15.2% of the group randomised to the DEB compared with 13.5% in the blended standardof-care group by intention-to-treat. Rates of cardiac death (1.9% vs 1.4%), target vessel MI (7.1% vs. 4.8%), and clinically driven TLR (11.9% vs. 11.5%) were not statistically different between study arms.
The results appear significant as to date, only one DCB technology has been approved for the treatment of ISR in the USA—Boston Scientific’s paclitaxel-based Agent DCB—and in Europe a 2024 update to the European Society of Cardiology (ESC) chronic coronary syndrome (CCS) guidelines favoured DES over DCB in ISR.
“For the first time, we’ve shown that a sirolimus-eluting balloon can match the outcomes of standard care for in-stent restenosis while avoiding yet another metal layer. This opens the door to treating restenosis in a simpler, safer way,” the trial’s co-principal investigator Roxana Mehran (Icahn School of Medicine at Mount Sinai, New York, USA) said of the results.
The primary outcome was the composite of MACE at 30 days, Thrombolysis in Myocardial Infarction (TIMI) risk score myocardial blush grade 0/1, distal embolisation or failure to achieve 50% ST segment resolution at 30 minutes post-PCI.
MACE included the first occurrence of cardiovascular death, re-MI, cardiogenic shock and new-onset heart failure at 30 days. The primary safety outcomes were major bleeding or the composite of major bleeding or clinically relevant bleeding at 30 days.
The primary outcome occurred in 73 patients (53.3%) in the alteplase groups versus 37 (52.9%) in the placebo group. Results were consistent across all components of the primary outcome and for each dose group versus placebo. Major or clinically significant bleeding occurred in one patient in the trial (in the alteplase 20mg group). During study drug administration, there were more episodes of ventricular fibrillation in the alteplase groups compared to the placebo group (10.2% vs 1.4%).
“Microvascular obstruction after primary PCI remains the single most important unresolved issue limiting the efficacy of primary PCI in STEMI patients,” said Mehta. “STRIVE does not support the routine administration of alteplase and it joins the growing list of previously promising therapies that have not succeeded in improving this important issue.”
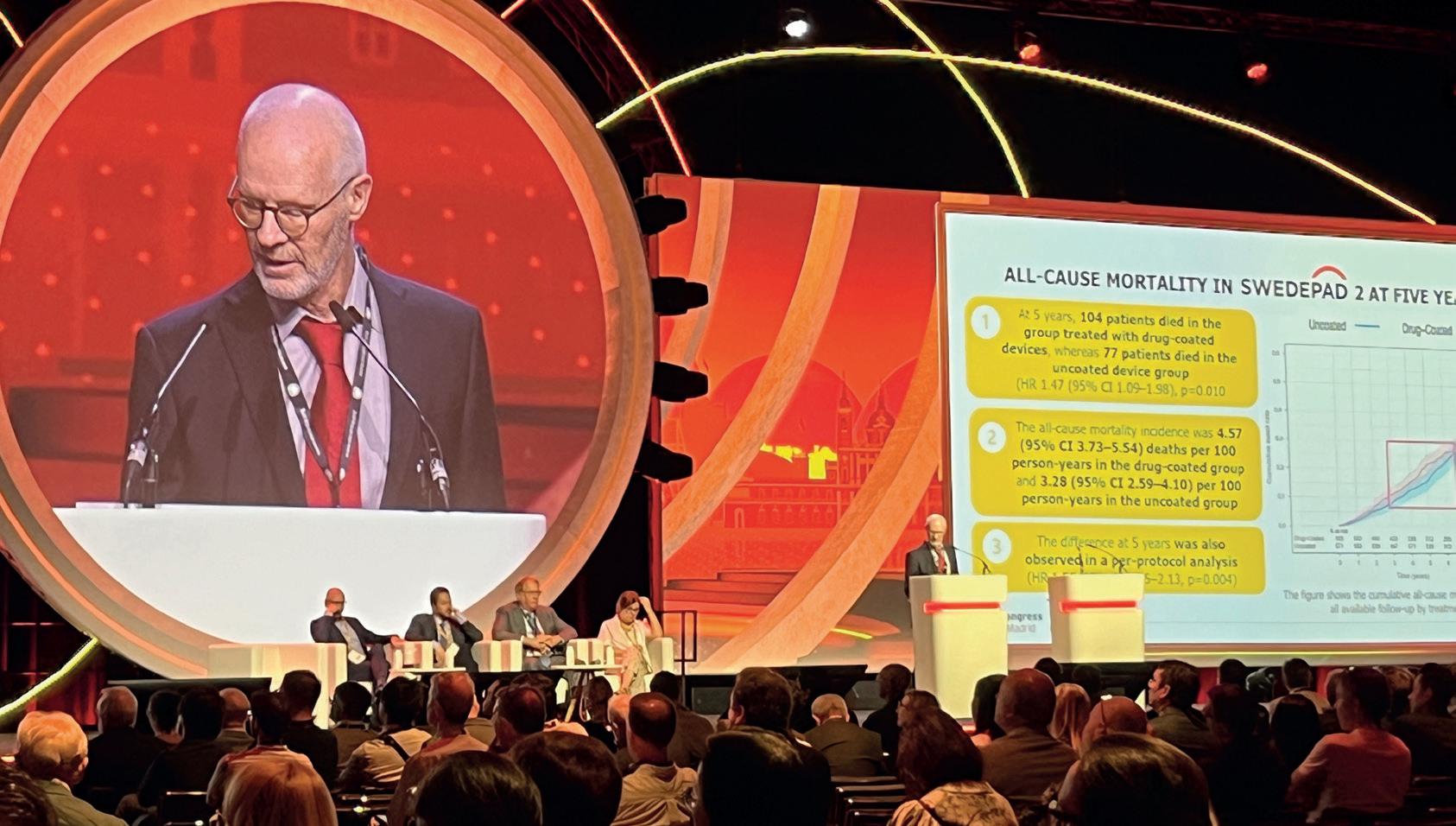
Mårten Falkenberg
SWEDEPAD re-opens paclitaxel
safety discussion, finds drug-coated devices do not improve outcomes
Drug-coated balloons (DCBs) and stents were not associated with reduced risk of amputation or improved quality of life compared with uncoated devices in the SWEDEPAD 1 and 2 trials, whilst a higher five-year mortality with drug-coated devices in patients with intermittent claudication has led researchers to stress that the safety of paclitaxel-coated devices—previously believed to have been resolved—is an “ongoing discussion”.
SWEDEPAD 1 and 2 were pragmatic, participantblinded, registry-based randomised trials that set out to determine the clinical impact of drugcoated technology on patients with peripheral arterial disease (PAD). Late-breaking findings from the trial were presented at the 2025 European Society of Cardiology (ESC) congress (29 August–1 September, Madrid, Spain) and published in The Lancet
“Drug-coated balloons and stents have been shown to reduce restenosis and the need for reinterventions in the endovascular treatment of PAD. However, there are uncertainties regarding whether drug-coated devices improve outcomes that are meaningful to patients, quality of life and reducing amputations, and there are some concerns over safety,” coprincipal investigator Joakim Nordanstig (University of Gothenburg, Gothenburg, Sweden) said of the rationale for the trial at ESC. “We investigated these and other endpoints in two trials in PAD—one in chronic limb-threatening ischaemia [CLTI] and one in intermittent claudication—comparing drug-coated and uncoated devices.”
In SWEDEPAD 1, 2,355 patients with CLTI (Rutherford stage 4–6) undergoing infrainguinal endovascular treatment were randomised 1:1 to drug-coated or uncoated balloons or stents. In nearly all of the drug-coated devices implanted, the drug delivered was paclitaxel (>99%). There was no significant difference in the primary endpoint of time to ipsilateral above-ankle amputation with drugcoated versus uncoated devices (hazard ratio [HR] 1.05; 95% confidence interval [CI] 0.87–1.27) over five years of follow-up. Target vessel reinterventions were reduced in the drug-coated group during the first year (HR 0.81; 95% CI 0.66–0.98), but this difference disappeared with longer follow-up. There was no difference in all-cause mortality or in quality of life (as assessed using the VascuQoL-6 questionnaire).
In SWEDEPAD 2, 1,155 patients with intermittent
claudication (Rutherford stage 1–3) undergoing infrainguinal endovascular treatment were randomised 1:1 after successful guidewire crossing to receive either drug-coated or uncoated balloons or stents. All drug-coated devices implanted delivered paclitaxel. There was no difference in the primary efficacy endpoint of quality of life between the drug-coated and uncoated groups at 12 months (mean difference in VascuQoL-6 scores: –0.02; 95% CI –0.66–0.62). Target vessel reintervention rates were not different at one year or over a median follow-up of 6.2 years. All-cause mortality did not differ over 7.1 years (HR 1.18; 95% CI 0.94–1.48), although higher five-year mortality was noted with drugcoated versus uncoated devices (HR 1.47; 95% CI 1.09–1.98).
Summarising the findings, co-principal investigator Mårten Falkenberg (Sahlgrenska University Hospital and the University of Gothenburg, Gothenburg, Sweden), said: “Paclitaxel-coated devices were not effective in preventing amputation in chronic limb-threatening ischaemia or improving quality of life in intermittent claudication. Given the signal of increased mortality with intermittent claudication, clinicians should carefully evaluate the potential risks and benefits when considering these expensive devices. Devices incorporating antiproliferative agents other than paclitaxel warrant further investigation in PAD.”
At ESC, Nordanstig commented that the results are “a bit different” to those of previously conducted pivotal trials and meta-analyses on drug-coated technology in patients with PAD, which “consistently demonstrated” reduced reintervention rates. “The big difference here I think,” Nordanstig said, “is this is a strategy trial rather than a single device trial, and [the SWEDEPAD findings] might be what is happening when broadly introducing these therapies in a more everyday patient population.”
Nordanstig also touched on the finding in SWEDEPAD 2 that higher five-year mortality was noted with drug-coated versus uncoated devices, stressing that the safety of paclitaxel-coated devices is “still an ongoing discussion” following the identification in 2018 by Katsanos et al of a late mortality signal. He remarked: “It’s hard for us to ignore the fact that it seems that we mirrored that signal in SWEDEPAD 2, but not in SWEDEPAD 1.”
Speaking to Cardiovascular News at the European Society for Vascular Surgery (ESVS) annual meeting (23–26 September, Istanbul, Türkiye), Nordanstig said that the data had been “well received”, but that further insight into the mortality signal seen in SWEDEPAD 2 would be a priority.
“Obviously there has been interest regarding this potential safety signal in SWEDEPAD 2, that we were very surprised about as well, and that raises certain questions we need to address, both as trialists but also as clinicians,” he said. “As we wrote in the Lancet papers, I think at this stage it’s very reasonable to say that we need to carefully consider when we use these devices and for what reasons.”
Nordanstig shared plans for future research. “More data will come out of this and a very high priority for us now is to scrutinise the mortality signal in SWEDEPAD 2,” he revealed. “We are in a good position to study cause-specific mortality, which I think is a new piece in this intriguing puzzle.”
The conversation around the paclitaxel mortality signal continues with the publication of the final report from SAFE-PAD, which differs in findings from SWEDEPAD. The study—which was commissioned by the US Food and Drug Administration (FDA) and helped inform the reversal of regulatory warnings against routine use of drugcoated devices—was published in the European Heart Journal (EHJ), and shows no evidence of long-term mortality risk associated with drug-coated devices used for femoropopliteal revascularisation.
In their EHJ paper, authors Robert M Kim and colleagues at Beth Israel Deaconess Medical Center (Boston, USA), including senior author Eric A Secemsky, note that SAFE-PAD was a retrospective cohort study of 168,553 Medicare fee-for-service beneficiaries aged 66 years and older who underwent femoropopliteal artery revascularisation between 2015 and 2018.
Clinicians should carefully evaluate the potential risks and benefits when considering these expensive devices.”
The authors share that device exposure to either drug-coated devices or non-drug-coated devices was identified using Medicare claims data, with the primary outcome being all-cause mortality. Secondary outcomes included all-cause hospitalisations, repeat revascularisation, major amputation, and cardiovascular medication use.
Kim and colleagues report that, at a median follow-up of 4.3 years, drug-coated device use was not associated with increased mortality, meeting a prespecified 5% non-inferiority relative margin. They add that secondary outcomes showed similar hospitalisation and amputation rates between groups but an increase in repeat revascularisation with drugcoated devices.
AQUATIC trial cautions against use of aspirin in chronic coronary syndrome patients receiving anticoagulation
New evidence cautions against the use of aspirin in patients with chronic coronary syndrome who have had prior stenting and require long-term oral anticoagulation.
INVESTIGATORS IN THE
AQUATIC trial, a double-blind placebocontrolled trial in chronic coronary syndrome patients after stenting receiving long-term oral anticoagulants conducted at more than 50 centres in France, found that the addition of aspirin was associated with increased cardiovascular events, death and major bleeding when compared with placebo.
Martine Gilard (Hospital Cavale Blanche, Brest, France) presented the findings during a hot line session at the 2025 European Society of Cardiology (ESC) meeting (29 August–1 September, Madrid, Spain), with the data published simultaneously in the New England Journal of Medicine (NEJM).
“In AQUATIC, adding aspirin to oral anticoagulants increased significantly the risk of the primary outcome, major bleeding and all-cause death,” Gilard told attendees at ESC 2025. “These results confirm and extend the results of prior trials in a much higher risk—more than seven-fold higher risk—population of patients who have received stents.
a history of percutaneous coronary intervention (PCI) during an acute coronary syndrome, or a history of PCI outside the context of acute coronary syndrome but with high-risk features such as diabetes, chronic kidney disease, diffuse multivessel disease, history of complex PCI or peripheral arterial disease.
Patients were randomised 1:1 to aspirin or placebo on top of oral anticoagulation. The trial’s primary efficacy endpoint
My conclusion is that stented patients on oral anticoagulants should not receive long-term aspirin, even if they are at high atherothrombotic risk.”
As many as 15% of patients with chronic coronary syndrome receive long-term anticoagulation therapy, Gilard and colleagues write in their NEJM paper, noting that these patients are often at high risk for both atherothrombotic and bleeding events.
In the trial, investigators defined a high atherothrombotic risk as either
Deferring treatment of nonculprit lesions
“remains an option” for STEMI in multivessel disease
New data suggest that interventionalists can safely opt to defer the treatment of nonculprit lesions when addressing ST-segment elevation myocardial infarction (STEMI) and multivessel coronary artery disease.
THIS IS THE FINDING AT three years of a trial of two revascularisation strategies for STEMI in patients with multivessel disease, in which instantaneous wave-free ratio (iFR)-guided revascularisation was shown not to be superior to staged treatment guided by cardiac magnetic resonance imaging (CMR) against outcomes including death, recurrent myocardial
of all-cause mortality in the aspirin group. The 872 patients randomised had a mean age of 72 years and 14.5% were female.
The primary efficacy outcome occurred in significantly more patients in the aspirin group than the placebo group (16.9% vs. 12.1%), with all-cause death also observed significantly more in patients with aspirin vs. placebo (13.4% vs. 8.4%).
Primary endpoint
was a composite of cardiovascular death, myocardial infarction (MI), stroke, systemic embolism, coronary revascularisation and acute limb ischaemia. The key secondary safety endpoint was major bleeding according to the International Society on Thrombosis and Haemostasis (ISTH) definition.
The trial was stopped early on the advice of the trial’s independent Data Safety Monitoring Board after a median follow-up of 2.2 years due to an excess
infarction (MI), or hospitalisation for heart failure.
Robin Nijveldt (Radboud University Medical Center, Nijmegen, the Netherlands) presented the three-year findings of the iMODERN trial at the 2025 Transcatheter Therapeutics (TCT) conference (25–28 October, San Francisco, USA), and the data were simultaneously published in the New England Journal of Medicine (NEJM).
The trial enrolled 1,146 patients across 41 hospitals in 14 countries, who were randomly assigned to either immediate physiology-guided treatment guided by iFR, a non-invasive diagnostic tool, or staged treatment guided by CMR, carried out within four days to six weeks after the initial episode.
At the three-year timepoint, the trial found no significant difference in major outcomes between the two approaches against the combined endpoint of death, repeat MI, or hospitalisation for heart failure.
Cardiovascular News that the trial’s results should cement deferred, complete revascularisation as an option for cath lab teams when treating multivessel STEMI patients, running counter to guidelines that recommend immediate revascularisation in the setting of STEMI and multivessel disease.
“If you have an acute event during the day, stenting the culprit lesion, and you have an additional stenosis, with your team around you and a little bit of time, then you can easily do additional stenting of the non-culprit lesion—then the patient is
Robin Nijveldt
The risk of major bleeding was more than three-fold higher in the aspirin group than the placebo group (10.2% vs. 3.4%), Gilard detailed. A total of 467 and 395 serious adverse events were reported in the aspirin and placebo groups, respectively.
In their NEJM paper, the authors note several limitations of their study, most notably its early termination, as well as the fact that all of the centres involved were located in a single country. Enrolment was also impacted by the COVID-19 pandemic, and women were under-represented in the trial.
However, in light of the findings the researchers suggest that the data should be considered in future ESC guidelines to build on current recommendations, which are based on expert consensus.
fully revascularised and everything set,” Nijveldt comments. “On the other hand, if you are in the middle of the night or some other acute event comes up, you also know that you can defer, and with a stress CMR scan you can pick a significant lesion up as well at a later timepoint.”
Nijveldt adds the population of patients seen in the trial will be familiar to cath lab teams, with as many as half of patients with STEMI presenting with multivessel disease. Several trials have demonstrated benefits of complete revascularisation for treating multivessel disease; however, whether to treat nonculprit lesions immediately or perform a staged PCI remains a point of contention, he said, though many interventionalists are reluctant to address multivessel disease without first waiting for symptoms.
“Should you do it directly during the initial event, or can you also wait? There are a few trials that tried to see whether that was non-inferior during the initial phase compared to waiting,” he detailed. “In that way, our trial is different to others. We used a pragmatic approach, where we said that if you have to wait, you can do it non-invasively.”
“These results show us that the direct assessment of stenting with iFR is not superior to waiting and doing cardiac MRI stress perfusion scans,” he said. “I think it gives the physician a little bit more of an option to know what to do. We already know that doing nothing is not the right way to do it, so now you have more methods to treat the patient the right way.”
Now you have more methods to treat the patient the right way.”
Aspirin group Placebo group
Martine Gilard
Light-reactive technology offers promise for preventing vein graft failure
TREATING VEIN GRAFTS WITH a photoreactive dye may improve graft patency and reduce rates of saphenous vein graft failure seen during coronary artery bypass graft (CABG) surgery.
Isaac George (Columbia University Medical Center, New York, USA) offered details of the technique—known as photochemical tissue passivation—at the 2025 European Association for Cardio-Thoracic Surgery (EACTS) annual meeting (8–11 October, Copenhagen, Denmark), saying it could be a solution to “astounding” current failure rates for saphenous vein grafts.
The platform technology used in the process is under development by Durvena and could be used in other applications including heart valves, George said during his EACTS presentation, where he was announced as the recipient of the association’s Techno-College Innovation Award.
“The saphenous vein graft is harvested from the leg to use as a conduit to bypass blocked arteries. Normal internal vein pressure is 10mmHg, but when placed in the arterial position it experiences pressures over 100mmHg, and because of this, veins fail due to increased pressure leading to adverse remodelling and thus intimal hyperplasia,” George stated.
Photochemical tissue passivation utilises a photo-initiator—Rose Bengal dye—that is applied to the outside surface of the blood vessel. Once treated the vein is placed in a sterile, single-use chamber, which is itself placed into a light-emitting device where it is exposed to light for around five minutes.
George said that, upon coming into contact with the light, the dye enters an “excited state”, creating a reactive oxygen species which facilitates formulation of a collagen crosslink that binds with the surface of the vessel.
According to George, the technique works by strengthening the veins and reducing stretching. In-vitro testing has shown tensile strength to be three times higher in treated veins compared to untreated veins.
Study of the technique in animals has been conducted, with three- and sixmonth angiographic follow-up showing treated veins to have significantly less dilated and a reduction in intimal hyperplasia at six months.
A first-in-human safety study has also been performed in three patients, totalling four grafts, with no major adverse cardiovascular events (MACE) or serious adverse events (SAE) at 30 days or six months. All treated vein grafts were patent at three months, and three out of the four vein grafts were patent at six months, George reported.
Studies shed new light on antiplatelet therapy after CABG surgery
New evidence offers fresh insights into the merits of dual antiplatelet therapy (DAPT) following coronary artery bypass graft (CABG) surgery and calls into question current guideline recommendations for anticoagulation post-bypass, according to investigators.
TOP-CABG and TACSI were among two hot line trials presented during the final day of the 2025 European Society of Cardiology (ESC) congress (29 August–1 September, Madrid, Spain), both focusing on anticoagulation strategies following bypass surgery.
The TACSI trial investigated whether 12 months of DAPT with ticagrelor and aspirin reduces the risk of cardiovascular outcomes compared with aspirin alone in patients with acute coronary syndrome (ACS) undergoing CABG. At 12 months, the incidence of major adverse cardiovascular events was similar with DAPT and aspirin alone, but major bleeding increased with DAPT, the trial’s investigators showed.
The TOP-CABG trial, meanwhile, compared 12 months of DAPT with 12 months of de-escalated DAPT—DAPT for three months followed by aspirin monotherapy for nine months—in patients after CABG, assessing the impact of the two strategies on rates of graft occlusion alongside the risk of clinically relevant bleeding. The trial showed that the rate of graft occlusion was non-inferior between de-escalated DAPT and standard DAPT, but clinically relevant bleeding was less frequent with de-escalation.
“Current guidelines recommend dual antiplatelet therapy after CABG in patients with acute coronary syndrome, but these guidelines are based on very thin data, mainly sub-studies of larger ACS studies and investigations in PCI [percutaneous coronary intervention] patients,” Anders Jeppsson (Sahlgrenska University Hospital, Gothenburg, Sweden), the principal investigator in the TACSI trial told journalists at a press conference at the ESC meeting.
TACSI, an investigator-initiated pragmatic, open-label, registry-based randomised randomised patients undergoing their first isolated CABG 1:1 to either DAPT (ticagrelor 90mg twice daily plus aspirin 75mg once daily) or aspirin only (75–160mg daily according to local protocols) for 12 months. The primary efficacy endpoint of major adverse cardiovascular events (MACE) was a composite of all-cause death, myocardial infarction, stroke or new coronary revascularisation within 12 months, alongside a primary safety endpoint of major bleeding.
The 2,201 patients included had a mean age of 66 years and 14.4% were women. The primary endpoint of MACE occurred in a similar proportion of patients in each group: 4.8% of patients in the DAPT group and 4.6% in the aspirin only group,
whilst major bleeding was more frequent in the DAPT group.
“Dual antiplatelet therapy with ticagrelor and aspirin was not more effective than aspirin alone to prevent cardiovascular events but increases the risk for major bleeding,” said Jeppsson of the trial’s findings. “The results question current guideline recommendations, which recommend 12 months of dual antiplatelet therapy in patients undergoing CABG after acute coronary syndrome,” he added.
With a focus on graft occlusion, TOP-CABG, a double-blind, parallel-controlled randomised trial, compared the effects of de-escalated DAPT and a standard 12-month DAPT regimen on patency and bleeding events for one year after CABG. Patients undergoing planned CABG with at least one saphenous vein graft were randomised 1:1 to de-escalated DAPT or to DAPT. The primary non-inferiority efficacy endpoint was 100% occlusion of the saphenous vein graft within one year after CABG at the per-graft level, with occlusion assessed by coronary computed tomography
The results question current guideline recommendations.”
angiography (CCTA) or coronary angiography, with a prespecified non-inferiority margin of 3.5%. The primary superiority safety endpoint was clinically relevant bleeding at the per-patient level within one year. Among the 2,290 patients enrolled in the trial, 20.6% were female and the mean age was 61.5 years.
Sharing the results at ESC 2025, Xin Yuan (Fuwai Hospital, Beijing, China) reported that non-inferiority was demonstrated for the primary efficacy endpoint of graft occlusion, which occurred in 10.79% of patients’ grafts in the de-escalated DAPT group and 11.19% in the DAPT group, whilst the primary safety endpoint of clinically relevant bleeding was less frequent with de-escalated DAPT vs. DAPT (8.26% vs. 13.19%). There was no difference between the groups for secondary outcomes including graft failure, any graft stenosis, any graft occlusion or major adverse cardiac and cerebrovascular events, he reported.
Anders Jeppson presents at ESC 2025
Intensive cholesterol lowering fails to shift the dial on vein graft failure
Intensive LDL cholesterol lowering with evolocumab does not reduce saphenous vein graft failure after coronary artery bypass graft (CABG) surgery compared to placebo, results of a randomised controlled trial have shown.
THIS IS THE HEADLINE FINDING OF NEWTON-CABG CardioLink-5, an investigator-initiated randomised, placebo-controlled trial, involving more than 700 patients from sites in Canada, Australia, Hungary and USA.
Subodh Verma (St Michael’s Hospital, Toronto, Canada) presented primary findings of the trial at the 2025 European Society of Cardiology (ESC) congress (29 August–1 September, Madrid, Spain) alongside publication in The Lancet, reporting that the 24-month vein graft disease rate was not significantly different between the groups—21.7% with evolocumab and 19.7% with placebo.
Among the 782 randomised participants evolocumab achieved a mean 48.4% placebo-adjusted LDL-C reduction at 24 months (−52.4% vs. −4%). However, despite its efficacy in reducing LDL-C levels, there were no significant differences between the groups receiving evolocumab and placebo in the primary and key secondary efficacy endpoints of the trial, including the percentage of totally occluded grafts at 24 months (17% vs. 16%, respectively) and the proportion of patients with at least one totally occluded graft at 24 months (30% vs. 28%, respectively).
Verma and colleagues then sought to investigate any potential ethnicity-related differences in the finding by comparing the trial’s 122 South Asian and 384 white patients, reasoning that patients of South Asian descent are a high-risk population who make up a large proportion of atherosclerotic cardiovascular disease cases worldwide.
“We know that the accelerated and disproportionate rates of atherosclerosis seen in this population are often seen prematurely; there is a greater severity of the disease and there is amplified and unexplained risk that cannot be explained simply because of an accumulation of multiple cardiometabolic risk factors,” Verma said, presenting the results of the subanalysis at the European Association for Cardio-Thoracic Surgery (EACTS) annual meeting (8–11 October, Copenhagen, Denmark).
As the primary outcome of evolocumab versus placebo was not different in the overall trial, for the purposes of the ethnicity analysis, investigators combined both the placebo and the active treatment groups.
According to Verma, South Asian patients enrolled in the trial were on average younger (62 vs. 67 years), had a lower body mass index (BMI, 26.2 vs. 29kg/m2), a lower EuroScore (0.74 vs. 0.99), and a lower rate of smoking history compared to the white patients.
Results of the trial showed that the vein graft disease rate, defined as ≥50% stenosis or complete occlusion in the vein graft stood at 27% in South Asians patients, compared to 17.6% in white patients. Secondary outcomes, including the proportion of saphenous vein grafts that were 100% occluded (22.1% vs. 13.3%), and the participants with more than one saphenous vein graft 100% occluded (37.7% vs. 24.7%) were also higher in South Asians compared to white patients after adjustment for baseline characteristics, including age, sex, diabetes status.
These findings underscore the need for more dedicated studies to focus on ethnicitybased revascularisation strategies.”
The analysis showed no difference in the efficacy of evolocumab compared to placebo by ethnicity on vein graft disease rates.
“Translationally, these findings underscore the need for more dedicated studies to focus on ethnicity-based revascularisation strategies,” Verma told attendees of the EACTS meeting. “Such efforts are essential, I would suggest, to enhance our understanding of optimal revascularisation approaches and potentially develop targeted interventions, both pharmacological as well as surgical to mitigate this risk in a high-risk cohort that contributes to a large number of global patients undergoing bypass surgery.”
Imaging after aortic intervention heightens cancer risk for patients, study finds
CUMULATIVE RADIATION EXPOSURE
from imaging systems used to monitor patients who have undergone thoracic endovascular aortic repair (TEVAR) may be associated with the development of malignant cancers in the long term.
This is according to the findings of a single-centre retrospective analysis of more than 500 patients to have undergone TEVAR at the University of Freiburg (Freiburg, Germany), presented at the 2025 annual meeting of the European Association for Cardio-Thoracic Surgery (EACTS, 8–11 October, Copenhagen, Denmark). Joseph Kletzer (University of Freiburg, Freiburg, Germany) reported that over the 13-year span of the study, 19 of the 542 patients followed were found to have developed some form of malignancy.
“With the implementation of TEVAR, both intraoperative management and postoperative monitoring rely heavily on advanced imaging, particularly CT [computed tomography] angiography. Whilst these tools are essential, repeated radiation exposure is an unavoidable consequence, raising justifiable concerns about the potential for induced malignancies over time,” Kletzer said.
Capturing long-term clinical data and imaging histories, Kletzer and colleagues were able to assess the possible relationship between the cumulative radiation dose and cancer amongst patients undergoing TEVAR at their centre.
They found that patients who developed malignancies had undergone substantially more CT angiograms during follow-up. In his presentation of the results, Kletzer detailed a “consistent association” between the number of CT angiograms and cancer emergence, meaning patients who received a more frequent follow-up protocol were more likely to develop malignancies compared to those who received imaging less often.
The association held true after adjusting for confounding factors, Kletzer said, adding: “These data suggest that radiation exposure from imaging postoperatively has a measurable oncogenic risk, demanding a careful balance between the aortic events and the potential for late harm.”
Factors such as history of smoking or age did not show any significant association with the occurrence of malignancy within the study, whilst higher periprocedural X-ray times seemed to reduce the hazard of malignancy. “This might be because of survivorship bias; more complicated TEVAR leads to lower life expectancy, leading to a lower signal of malignancies in these patients, when in fact it is just because of a high rate of death,” said Kletzer.
Additionally, the analysis showed that there was a significant association between the average frequency of postoperative CT scans and subsequent cancer risk in patients receiving TEVAR. Using one CTA per year as a reference point, the investigators observed that increasing imaging beyond this threshold was linked with a rise in malignancy.
Up to half of patients may experience AF after coronary surgery, but burden is low
A prospective study indicates that the prevalence of new-onset atrial fibrillation (AF) after coronary artery bypass graft (CABG) surgery may be significantly higher than previously reported, but the extremely low burden of the disease calls into question the need for long-term oral anticoagulation for patients undergoing the procedure.
THESE AND OTHER TALKING POINTS emerged from the CABG-AF trial, an investigatorinitiated study of the incidence and burden of AF following CABG procedures. For the trial, surgeons at two cardiac centres in Germany implanted insertable cardiac monitors in 198 patients with three-vessel or left main coronary artery disease and no history of arrhythmias who underwent a bypass procedure between November 2019 and November 2023. Patients were monitored continuously for 12 months for any occurrence of AF lasting two minutes or longer.
“Large-scale contemporary studies investigating new-onset AF after cardiac surgery have been limited methodologically by their temporally restricted application of in-hospital telemetry and intermittent short-term monitoring after discharge,” said Florian Herrmann (Ludwig-Maximilians-Universität München, Munich, Germany), detailing the findings at the European Association for Cardio-Thoracic Surgery (EACTS) annual meeting (8–11 October, Copenhagen, Denmark), alongside their publication in the Journal of the American Medical Association (JAMA).
Herrmann reported that new-onset AF, the trial’s primary endpoint, occurred in 95 of the 198 patients studied, resulting in a cumulative incidence of 48%.
The median length of AF episode seen in the study was six minutes, with a median time to AF of 3.3 days. Of these episodes, 63% of episodes were asymptomatic,
and 67% went undetected by standard monitoring.
The median AF burden at 12 months was 0.07%, corresponding to six hours 10 minutes of AF throughout the 12 months of monitoring. In 90 of the 95 patients in which episodes of AF occurred, these happened within the first 30 days after surgery. In total, 77% of the time in AF recorded during the study occurred within 30 days of surgery.
after discharge and were not detected with standard monitoring.
One year after surgery, seven patients (7.4%) with and seven (6.8%) without new-onset AF experienced at least one major adverse cardiac and cardiovascular even; three patients (3.2%) with and one (1%) without AF died during follow-up. No patient with new-onset AF developed a stroke during follow-up, whereas two patients (1.9%) without did develop a stroke. Both strokes were non-disabling and occurred during the initial hospitalisation.
Most episodes had a length of under one hour, Herrmann detailed, with only 15 episodes lasting 24 hours or more, a duration that has been linked to an increased risk of stroke. Eight of the 15 episodes lasting 24 or more hours occurred in eight patients prior to discharge and were detected with both continuous and standard monitoring. Seven episodes lasting 24 or more hours occurred in three patients
Given the known bleeding risk with oral anticoagulants, the very low AF burden questions current ESC and EACTS guidelines.”
New preclinical data show early patency of coronary tissue engineered vessel
Humacyte has announced the publication of new preclinical data as part of a study evaluating the coronary tissue engineered vessel (CTEV) as a coronary artery bypass graft (CABG) conduit in a non-human primate model.
IN THE STUDY, PUBLISHED in JACC: Basic to Translational Science, the CTEV was observed to sustain blood flow, recellularise with the animals’ host cells, and remodel to reduce the initial size mismatch between the CTEV and the animals’ native artery.
“Innovation in CABG has been stagnant for far too long,” said Alan Kypson (UNC REX Hospital, Raleigh, USA). “Our results suggest that we may be on the verge of a new option— one that remodels to match the native artery and recellularises with host cells,
potentially providing superior patency relative to saphenous vein grafts. The CTEV has the potential to address a significant unmet clinical need in coronary bypass surgery and ultimately improve patient outcomes.”
CABG is a standard of care treatment for coronary artery disease, however saphenous vein grafts—used in 80%90% of CABG cases—can have poor long-term patency. Many patients also lack usable autologous veins or arteries due to prior harvest, ablation, or poor quality, highlighting the unmet clinical need for alternative conduits.
“The incidence of new-onset AF within the first year after CABG was higher than previously reported; however, the AF burden was low during the first year, especially later than 30 days after surgery,” Herrmann said. “Given the known bleeding risk with oral anticoagulants, the very low AF burden questions current ESC [European Society of Cardiology] and EACTS guidelines recommending long-term oral anticoagulation. If oral anticoagulation is initiated for new-onset AF after CABG, the indication should be reassessed 30 days after surgery.”
Commenting on the data following the presentation at EACTS, Matthias Siepe (University of Bern, Bern, Switzerland) expressed surprise at the high rate of AF seen within the study, but questioned whether the finding would have any clinical implication, given the low burden of the disease. “Postoperative atrial fibrillation is not the same as atrial fibrillation in other cohorts, so I wonder with this information will necessarily trigger other treatment, because I am not sure if clinical endpoints will be influenced by this high incidence,” he commented.
“That is exactly the point; this study shows a higher incidence but a very low burden,” Herrmann said in response. “While we expected that there would be much more AF, we actually showed the opposite, that there is a low, low burden of AF that should maybe let us question whether we should be anticoagulating so many patients.”
The recent study follows five adult baboons undergoing CABG to the right coronary artery with the CTEV. All CTEVs remained patent throughout the six-month study. At the end of follow-up, the CTEV was observed to have recellularised with host cells to form a multi-layered tissue, including transanastomotic neomedial tissue that effectively reduced the initial size mismatch with the right coronary artery (RCA). The results suggest that the CTEV may be a durable alternative CABG conduit.
The CTEV is 3.5mm blood vessel produced in the same bioengineering manufacturing system as Humacyte’s acellular tissue engineered vessel (ATEV). The CTEV is also referred to as the small-diameter ATEV, or sdATEV.
Humacyte also announced that it plans to advance the CTEV into its first-in-human study in CABG. To support human study, the company
anticipates filing an investigational new drug application with the US Food and Drug Administration (FDA) during the fourth quarter of 2025. The company’s current plans for filing an IND are based on the outcome of a meeting held early this year with the FDA, including agreements reached with the agency.
“We’re pleased that this new publication of preclinical data demonstrates the promise of CTEVs as an alternative for native vessel grafts in CABG,” said Laura Niklason, founder chief executive officer of Humacyte.
“As one of the leading causes of early death, coronary artery disease poses unique challenges for patient care. We are looking forward to proceeding into the first-in-human study of the CTEV in CABG and hopefully offering surgeons another option for treating this disease.”
The CTEV is an investigational product and has not been approved for sale by the FDA or any other regulatory agency.
Florian Herrmann
to choose outcome measures, how to power a trial—but trials greatly impact our guidelines.
PATRICK MYERS
Serving as the secretary general of the European Association for Cardio-Thoracic Surgery (EACTS) since 2022, Patrick Myers (Zurich University Hospitals, Zurich, Switzerland) has helped to steer the organisation into the post-pandemic era. In this interview he talks to Cardiovascular News about the need for more high-level trials in cardiac surgery, thawing relationships with cardiology, and future training needs for the field.
What drew you to medicine and cardiac surgery in particular?
I’ve always been passionate about understanding how the human body works, even from a very young age. When I was 11 years old, I underwent an operation which put me in contact with the medical world; it seemed natural to want to understand how the body works and how to make things better. Why cardiac surgery? I always did a lot of things with my hands—making model airplanes and boats, or very precisely painting Warhammer characters. Before medical school, I didn't know what specialty I was interested in, I just knew I wanted to be a doctor. As a student I had to complete an elective working as a nurse’s aide, and I was able to go to the operating room at the end of the elective. The first procedure I saw was a pulmonary lobectomy, which I thought was interesting, but the second was a coronary artery bypass graft (CABG), and seeing the attention to detail, the precision, my immediate reaction was a big “wow, that’s for me!”.
Which mentors have shaped your career?
Training in Switzerland, I knew it was a small country and it was hard to see the full breadth of diseases and surgical techniques, so from the very start I planned to do a fellowship in the USA. Working with Larry Cohn at Brigham and Women's Hospital was just a fantastic experience. He was a tough mentor. Being in the operating room with him was like jousting: he would push you hard, but he was waiting for you to respond, to see if you could meet or exceed his expectations. He had a big smile hidden under his mask the whole time.
After that I spent time in congenital cardiac surgery at Boston Children’s Hospital and worked with Pedro del Nido and his team. He is one of the brightest minds I've had the privilege of encountering—seeing how everything can be so simple when you have a mind like that is astonishing and inspiring.
How has the field of cardiac surgery changed since you began your career? It is changing tremendously, in that we have fantastic technologies for treating coronary artery disease or treating valvular heart disease, that mean a lot of simple cases can be handled non-operatively. That makes training much harder as the complexity of surgical cases is increasing, and we have to find a way to train residents well in that.
Surgeons need to embrace these technologies. Transcatheter aortic valve implantation (TAVI) is a fantastic technology, and I think we are currently in the euphoria phase. Adoption and indications have spread much further than the evidence supports. When I was in training, the euphoria around
percutaneous coronary intervention (PCI) was huge and the volume of CABG was decreasing tremendously. After the SYNTAX trial was published and three-vessel and left main disease became surgical diseases again. CABG now represent more than 50% of most cardiac surgeons’ practice.
Will cardiac surgeons of the future need to master open and transcatheter skills?
Fundamentally, surgeons should be able to do both. My colleagues from vascular surgery are now vascular and endovascular surgeons. They choose which treatment modality would be the best for their patient without any conflict of interest. Cardiac surgeons need to do that and come to the heart team discussion knowing exactly the pros and cons of both options. On the other hand, you can’t be an expert in everything. We need expertise, and this comes from intense focus. We are increasingly sub-specialising within surgery. I am mostly a coronary surgeon, but we now have heart failure, mitral valve repair, aortic surgeons, and each one of these operates in a very specialised way, at a high level. You have to be doing the same procedure all day every day to get excellent at it. I worry about saying everyone has to be able to do everything. You can't be good at everything you do.
What can the surgical community do to adapt to the changing face of cardiovascular medicine?
Surgeons need to lead or be involved in leading these trials, which is a very different skillset to the one we have to use in our daily practice and not something you can do sustainably in parallel to a busy clinical practice. That is why my main focus in EACTS has been working with other cardiothoracic surgery associations around the world and with cardiology associations. Its fantastic that we are now invited to European Society of Cardiology (ESC) meetings and we have joint sessions at the American Heart Association (AHA) meeting, so we are really working on the heart team approach.
How has EACTS worked to build bridges between the interventional cardiology and cardiac surgery communities?
To answer that fully you have to go back to 2018/19. Most of the research surgeons were producing at the time was from single centre, observational studies, which were producing vastly underpowered, biased data comparing one modality versus another, where little causal inference could really be made. That can be important, but it is low-quality evidence and should not be guiding our practice. Surgeons were not involved in trials and didn’t understand the finesse of methodology—how
FACT FILE
CURRENT APPOINTMENTS
Cardiac surgeon University Hospital Zurich, Zurich, Switzerland
Secretary general European Association for Cardio-Thoracic Surgery
International director Society of Thoracic Surgeons
President CTSNet
TRAINING AND EDUCATION
Cardiovascular surgery residency Geneva University Hospitals (Geneva, Switzerland)
Adult cardiac surgery fellowship Brigham & Women's Hospital and Harvard Medical School (Boston, USA)
Paediatric cardiovascular surgery residency Boston Children's Hospital (Boston, USA)
At the 2019 EACTS meeting in Lisbon, my predecessor, Domenico Pagano, began a trial updates session, which is now a regular Saturday morning session at our annual meeting. That started a very big controversy when the surgical principal investigator for the EXCEL trial explained that he had withdrawn his name from the trial, stating his co-investigators of dishonesty. Ultimately, that was a wake-up call and it led to us realising that, as surgeons, we can't be on the sidelines, we have to be involved. We have to understand how these trials are designed, how they are run, how we choose outcome measures, and we are still doing that today.
Fundamentally, we all want the best for our patients and we believe in what we do. I always put in my disclosures that I am a surgeon, so obviously I am going to say surgery is best. I like Friedrich Nietzsche’s aphorism, “there are no facts, only interpretations”. We see that in guideline committees, where we can be looking at exactly the same trial but read it in a completely different way, because we read it with our biases. There is no ill intent behind that, I think we are just trying to do the best for our patients and what we believe in.
The EXCEL controversy made relations with our colleagues across the heart team a little complicated; my role has been to try and calm things down. The people I get along with the best every day at my home institution are interventional cardiologists. We help each other all the time, so why can’t we achieve that in our associations?
At the ESC congress in Madrid (29 August–1 September, Madrid, Spain) our leadership were invited to participate in major sessions there; at our annual meeting in Copenhagen (8–11 October, Copenhagen, Denmark) ESC leadership is participating actively in discussions, we have three joint sessions with European Association of Percutaneous Cardiovascular Interventions (EAPCI), which is fantastic. Even if they feel like they are going into the lion’s den—just as we feel a little nervous when we go to the cardiology meetings—we reassure them that we are here to listen, and it opens up the discussions so much.
How did you come to be involved with EACTS and how has participation in the association benefitted your career?
I started in EACTS more than 15 years ago as a resident in what used to be called the Surgical Training and Manpower committee, now the Residents’ committee. That committee was chaired by Rafael Sadaba and Matthias Siepe, the current president of EACTS and the editor-in-chief of our journal, the European Journal of Cardio-Thoracic Surgery (EJCTS). Along with Peyman Sardari Nia, who is the editor-in-chief of Interdisciplinary CardioVascular and Thoracic Surgery (ICVTS), and a few other people who have all continued within the association, it gave us the opportunity to talk with people from all over Europe and share our perspectives, as well as get in contact with the leaders of our field and be mentored by them. In a natural way it has developed—we each contributed more and more to the association and were recruited for junior leadership roles, then leadership roles. EACTS’ annual meeting is the largest
cardiothoracic surgery meeting in the world; more than 5,000 people attend, and the buzz and interaction is fantastic. You hear the top science, but more than that, you can meet friends from all over the world—what I would dub our EACTS family.
Being a part of EACTS, you have this larger community you can rely on, and if I have a particularly complex case for an operation I don't do routinely and I don't have a colleague locally to whom I can refer the case, I'll call up one of my friends in EACTS and ask them for tips and tricks, or have them give me a hand.
Which has been the most impactful recent research paper you have read?
If I have to pick one, it’s one that hasn’t been published yet—the 10-year results of the PARTNER 2A trial, comparing TAVI versus SAVR [surgical aortic valve replacement] in intermediate-risk patients. This was published on the US Food and Drug Administration (FDA) website, and it shows there is a survival benefit at 10 years of SAVR over TAVI.
This is what we have been saying as a
surgical group; the operations we do carry an initial hazard, even if we do a minimally invasive procedure it takes time to recover from that, and for a patient, psychologically, it is maximally invasive so you have to have a very good reason to do it. Many of the trials have short-term follow-up. What we tell our patients is the reason we pick CABG or SAVR over percutaneous options is because they have an expected survival that is 10 years or more, and the benefit of our treatments show during this long follow-up. Our trials need to have long-term follow-up, but most of the TAVI versus SAVR trials have only published five-year results.
The very long-term results we have only come from one trial, NOTION, which is in very elderly patients with surgical valves which are off the market now because of their early degeneration, so the only prospective randomised data that we have out there says that there is no difference at 10 years.
What is interesting to me about the PARTNER 2A results is—even if it is an older patient population with a lot of competing
“We all want the best for our patients and we believe in what we do.”
risks, and over 80% of the patients passed away at 10 years—there is a difference between the groups and SAVR does have better long-term survival.
What does your life outside of medicine look like?
I've got two children, who are 17 and 15. Living in Switzerland, I have access to mountains for hiking and skiing, and sailing on the lakes. I’m an avid runner, I run three to four half marathons per year. If ever I am in New York, I love running in Central Park—where you have the ultramarathoner who is running circles around everybody at a blistering pace, and someone much less fit, going very slowly but happy they are out doing it. Seeing that reminds me that we are each running our own race—against ourselves. I love the expression from George Bernard Shaw: ‘We don’t stop playing because we grow old, we grow old because we stop playing’. After years of skiing and snowboarding, this summer I started wakeboarding—and it’s fantastic.
Native vessel PCI no longer the default strategy for patients with previous CABG
Should interventionalists prioritise native or saphenous vein graft percutaneous coronary intervention (PCI) when treating coronary disease in patients with previous post-coronary artery bypass graft (CABG) surgery?
THIS WAS THE QUESTION AT THE HEART of the PROTCTOR trial, a multicentre, open-label, randomised trial comparing clinical outcomes between the two strategies in post-CABG patients presenting with saphenous vein graft failure.
Ruben W de Winter (Amsterdam University Medical Centers, Amsterdam, the Netherlands) presented oneyear outcomes of the study at the 2025 Transcatheter Cardiovascular Therapeutics (TCT) meeting (25–28 October, San Francisco, USA), where he reported that saphenous vein graft PCI in the high-risk and complex post-CABG patient population led to improved oneyear clinical outcomes compared with native vessel PCI. The findings of the trial, which was sponsored by Abbott, were simultaneously published in the Journal of the American College of Cardiology (JACC).
“CABG’s long-term durability is limited by both bypass graft failure and progression of disease in the native coronary arteries. As a result, there’s a substantial number of patients that experience recurrent angina symptoms and ischaemia, affecting up to six out of 10 patients at 15 years after surgery,” said de Winter.
“Many prior CABG patients return to the cath lab for repeat coronary angiography and further revascularisation therapy. In patients with previous CABG who require repeat revascularisation, current guidelines recommend PCI of the native coronary artery over PCI of the diseased bypass graft with a class 2A level of evidence B based entirely on
observational data.”
In a bid to answer this question, investigators randomised 220 patients with prior CABG and significant saphenous vein graft stenosis one to one to either a strategy of native vessel PCI (n=108) or saphenous vein graft PCI (n=112) at 14 centres in Europe between January 2019 and December 2023.
The primary endpoint was one-year major adverse cardiovascular events (MACE), a composite of allcause mortality, non-fatal target coronary territory myocardial infarction (MI) and clinically driven target coronary territory revascularisation. At one year, MACE occurred in 37 (34.3%) patients in the native vessel PCI group and 21 (18.7%) patients in the saphenous vein graft (SVG) PCI group.
No significant differences in rates of all-cause
Trials find comparable outcomes for IVL alternatives in calcified coronary disease
Cutting balloon angioplasty and the use of a super-high-pressure non-compliant balloon have been shown to be non-inferior to intravascular lithotripsy (IVL) in separate randomised trials comparing the calcium modification techniques to IVL.
THESE ARE THE FINDINGS of two trials presented during a late-breaking trials session at the 2025 Transcatheter Cardiovascular Therapeutics (TCT) conference (25–28 October, San Francisco, USA)— ShortCUT and VICTORY—which examined strategies for preparing calcified coronary lesions prior to PCI.
“There are multiple device options available for calcium modification, however, there are limited direct comparisons between these devices, many of which have different mechanisms of action and carry substantial differences in cost,” said Suzanne Baron (Baim Institute for Clinical Research, Boston, USA), an investigator in the ShortCUT trial, which compared the safety and efficacy of cutting balloon angioplasty to IVL prior to stenting.
The trial enrolled 413 patients with stable or unstable coronary artery disease with de novo calcified coronary lesions and was stratified to include two cohorts of patients: those with
planned up-front rotational atherectomy (n=208) and those in whom up-front rotational atherectomy was not planned (n=205). In each cohort, patients were randomised to receive IVL- or cutting balloon-facilitated lesion preparation.
ShortCUT’s primary endpoint was post-procedural stent area at the site of maximal calcification as measured by core lab-adjudicated, high-definition intravascular ultrasound assessment.
The study found that for the postprocedural minimal stent area (MSA), the mean was 8.6 mm2±2.5 for IVL and 8mm2±2.4 for the cutting balloon strategy. Baron detailed that, when the primary endpoint was stratified by atherectomy plan, results were similar to the overall study cohort in those patients who underwent planned atherectomy but in patients who did not undergo planned atherectomy, cutting balloon angioplasty did not meet noninferiority. “This may
mortality were observed between the two groups (5.6% native vessel versus 3.6% SVG). However, both non-fatal target coronary territory MI (22.6% native vessel versus 11.7% SVG) and clinically driven target coronary territory revascularisation (18.4% native vessel versus 9.1% SVG) occurred more frequently in patients assigned to native vessel PCI.
De Winter commented that the difference in outcomes between the two approaches had been influenced by fewer PCI-related MIs and clinicallydriven target coronary territory revascularisation, adding that the results challenge current guidelines at one-year clinical follow-up. Long-term data will be essential to show if the advantage continues for saphenous vein graft PCI continues over time, he said. Critiquing the paper in an accompany editorial in JACC, Yousif Ahmad (University of California, San Francisco, San Francisco, USA), Rohin Reddy (Imperial College London, London, UK) and Robert Yeh (Beth Israel Deaconess Medical Center, Boston, USA) point to the relatively complex nature of the lesions in the native vessel PCI group, where 83% comprised chronic total occlusions (CTO) and over half of procedures requiring a retrograde approach.
Native vessel PCI should not be considered the default approach, particularly if the native intervention is likely to be exceptionally complicated and higher risk.”
have been partly due to differences in vessel size between groups, as stent expansion and indices of calcium fracture were similar,” she said.
Average stent expansion at the site of maximum calcification was similar with 97.7±24 for IVL and 97.7±25.9 for the cutting balloon. The procedural cost difference was US$3,632 with the main cost difference being driven by the cost of the randomised device.
Strategy success, defined as stent delivery with a residual stenosis less than 20% in the absence of significant angiographic complication and not having to use alternative calcium modification devices, was similar with 89.7% for IVL compared with 89.2% for the cutting balloon. Thirtyday major adverse cardiovascular and cerebrovascular event (MACCE) outcomes 2.9% in both groups.
VICTORY compared IVL to the NC balloon (SIS Medical), a super-highpressure coronary
balloon, for lesion preparation. The primary endpoint was final stent expansion assessed by optical coherence tomography (OCT) determined by an imaging core laboratory.
Matthias Bossard (Luzerner Kantonsspital Heart Center, Lucerne, Switzerland) detailed that a total of 282 patients at three sites in Switzerland and Canada were randomised one to one to IVL (n=142) or the super-high-pressure balloon (n=140).
The balloon group achieved a median of 85% stent expansion compared with 84% in the IVL group, meeting non-inferiority. The use of the balloon resulted in similar rates of acute procedural (98.6% versus 97.1%) and strategy success (98.6% for both) compared with IVL. The results were consistent across a number of patient subgroups. In addition, there were no significant differences in safety outcomes including coronary artery dissections, perforations, or side branch occlusions.
There are multiple device options available for calcium modification, however, there are limited direct comparisons between these devices.”
Suzanne Baron
Ruben W de Winter
ABSTRACTS
Accepted abstracts published in JACC Interventions
DEADLINE: November 21, 2025
CRT PRACTICE
INTERESTING CASES
CRMIC Publication Opportunity
DEADLINE: December 5, 2025
DEADLINE: Dec. 19, 2025
EARLY CAREER LEADERSHIP
FELLOWS WOMEN IN CARDIOLOGY
INNOVATORS
DEADLINE: January 16, 2026
NURSE & TECH INTERESTING CASES
Top 3 cases will be published in Cath Lab Digest
CRT EVIDENCE
LATE-BREAKING CLINICAL TRIALS & CLINICAL SCIENCE
Simulatenous Publication Opportunities
CRT INNOVATION
BEST INNOVATION COMPETITION
The Top Innovation will be the recipient of our CRT 2026 Innovations Award
DEADLINE: January 9, 2026
Associate Faculty
• Waived CRT 2026 registration fee
• Discounted Community Premium Access, includes all current CRTmeeting videos, PPT/PDF presentations, and archives
• Complimentary subscription to Cardiovascular Revascularization Medicine the official peer-reviewed journal of CRT
Submit Your Science Apply For Scholarships
Structural Heart Interventions
Transseptal TMVR system shows promise in patients unsuited for surgery or TEER
Results of a pivotal clinical trial evaluating the safety and efficacy of a fully percutaneous transseptal mitral valve replacement (TMVR) procedure—Sapien M3 (Edwards Lifesciences)— in patients with symptomatic, moderate-to-severe mitral regurgitation (MR) who are not eligible for surgery or mitral-transcatheter edge-to-edge repair (M-TEER) procedures, demonstrated effective MR reduction with low rates of complications and mortality.
One-year data from the Edwards Lifesciences-funded ENCIRCLE trial, presented by David Daniels (Sutter Health, San Francisco, USA) during a late-breaking trials session at the 2025 Transcatheter Cardiovascular Therapeutics (TCT) conference (25–28 October, San Francisco, USA), simultaneously published in The Lancet, demonstrated low rates of mortality and heart failure hospitalisation for patients treated with the device.
“Percutaneous transseptal TMVR with the Sapien M3 system achieved the primary endpoint with a one-year composite rate of death or heart failure hospitalisation significantly below the performance goal, significant and sustained reduction in mitral regurgitation severity, meaningful and durable improvements in functional status and quality of life, and an observed 30-day mortality markedly lower, onetenth, than the predicted surgical risk,” Daniels said of the results.
Baseline characteristics of the study population included an average age of 75.5 years, a risk of mortality for surgical mitral valve replacement of 6.6% based on the Society of Thoracic Surgeons (STS) risk score at 30 days, with 28.8% of patients stratified as high risk based upon STS score.
Daniels noted that 71.2% of patients had moderate-to-severe or severe congestive heart failure symptoms, significantly elevated pro-BNPs, and a 69.9% rate of atrial fibrillation (AF) at baseline.
The trial’s primary endpoint, a composite of all-cause mortality and rehospitalisation for heart failure at one year, stood at 25.2%, compared to a prespecified performance goal of 45%. All-cause death and heart failure hospitalisation rates were 13.9% and 16.7%, respectively.
Prespecified secondary endpoints included improvement in MR grade, NYHA class, Kansas City Cardiomyopathy Questionnaire overall score (KCCQ-OS), and Left Ventricular End Diastolic Volume index (LVEDVi).
The device, which is fully retrievable, is delivered transfemorally in a two-stage procedure under transoesophageal echocardiogram (TEE) and fluoroscopy guidance.
“Initially we advance a nitinol dock with a hydrophilic sleeve through the medial commissure and three times around the mitral apparatus. This is the base station, this is where we implant the valve—the dock. The sleeve is then removed and we check the adequacy of implantation,” Daniels said of the procedure. “Once we are happy, we release the dock and then we go to the second stage which is to do a balloon-expandable transcatheter heart valve implant that is very similar to a mitral valve-in-valve procedure.”
Trialists screened a total of 1,171 patients at 56 sites in the USA, Canada, Europe, Israel and Australia. Thirty-five percent of those screened were excluded based on anatomic eligibility criteria, with other exclusion criteria including the presence of severe left ventricular (LV) function or dilatation, the potential need for other valvular interventions within the next 12 months, irreversible pulmonary hypertension, severe heart dysfunction or significant renal insufficiency.
Ultimately, 299 patients with mitral regurgitation (MR) ≥3+, New York Heart Association (NYHA) class ≥II, unsuitable for surgery or commercially available transcatheter treatment options due to clinical, anatomic, or technical considerations, were treated. Of these, 287 patients had a valve implanted. Follow up was completed at 30 days, six months and one year.
The study found that all patients had an improvement in MR grade with more than 95% of patients having ≤1+ total MR at 30 days and one year. NYHA improvement was observed in 73.4% of patients at one year, and ~88% of patients were considered as having NYHA class I or II at one year.
The improvement in KCCQ-OS was 18.4±1.68 with ~43% of patients having ≥20-point score improvement at one year. Rates of stroke, clinically significant leaflet thrombosis, and haemolysis were 9.3%, 6.7%, and 7.1%, respectively at one year.
“No comparative group was directly available for this patient population, and the performance goal was derived in consultation with FDA [US Food and Drug Administration] and based on event rates from optimised medical therapy arms of randomised controlled trials that were investigating M-TEER intervention available at the time that this trial designed,” Daniels said of the design of the study’s endpoint.
Daniels added: “These findings will help guide clinical practice by providing an alternative treatment option for patients who are not suitable for conventional surgery or TEER procedures.”
These findings will help guide clinical practice by providing an alternative treatment option for patients who are not suitable for conventional surgery or TEER procedures.”
UK survey highlights wealth disparities in heart valve care
Research published by Heart Valve Voice, a UK charity, reveals that delays in heart valve disease diagnosis are disproportionately affecting those living in the most deprived areas of the country.
A survey of over 300 heart valve disease patients has shown that three-quarters of respondents in the lowest income decile said their diagnosis had been delayed (with just one in four reporting they were diagnosed without delay). Contrastingly those living in the least deprived decile were unlikely to experience delays, only one in five reported delays to diagnosis, most (64%) were diagnosed without delay).
“In areas of social deprivation many people don’t know anything about heart valve disease and certainly don’t know the symptoms. Moreover, they often don’t present to their GP or follow conventional treatment pathways. Valve disease symptoms often creep in slowly and it’s easy for patients to brush them off or put them down to normal ageing, sometimes until they are seriously ill and end up presenting in A&E,” commented Phil MacCarthy (Kings College Hospital, London, UK).
For most patients, delayed diagnosis was due to issues arising in primary care—the most common reason cited was GPs not spotting their symptoms (14%). Symptoms not taken seriously (9%), symptoms misdiagnosed (9%) or needing to see the GP multiple times (9%) were also common challenges. In a minority of cases, it was the patient themselves not taking symptoms seriously which contributed to their delay (6%).
However secondary care also presented challenges in many cases, with delays to diagnostics like echocardiogram or other tests reported. When asked about the greatest impact of their delay, a quarter of patients cited worsening symptoms, while 15% pointed to the toll on their mental health. Seven percent said it had forced them to take extended time off work. Around a third of patients reported that delays had led to increased use of healthcare services, with 11% requiring frequent GP appointments, 9% making repeated visits to A&E, and a further 11% needing emergency ambulance transport.
Thirty-nine percent of patients experienced delays accessing treatment after being diagnosed, with NHS waiting lists given as the most common reason for about half of these patients (49%). Staff shortages and limited access to specialists were also highlighted.
MITRAL
David Daniels
Sapien M3
Tendyne
system shows promise in patients with mitral annular calcification
A trial of transcatheter mitral valve replacement (TMVR) with the Tendyne system (Abbott) led to successful treatment of severe mitral annular calcification (MAC) in nearly all patients, coupled with significant improvements in heart failure symptoms and quality-of-life parameters, prompting hopes of an effective treatment in a patient population currently with limited options.
THESE ARE FINDINGS OF THE SUMMIT-MAC trial, presented during a late-breaking trials session at the 2025 Transcatheter Cardiovascular Therapeutics (TCT) conference (25–28 October, San Francisco, USA) by Paul Sorajja (Abbott Northwestern Hospital, Minneapolis, USA), published simultaneously in the Journal of the American College of Cardiology (JACC).
MAC is a fibrous, degenerative calcification of the mitral valve support ring that is associated with mitral regurgitation (MR), stenosis, or a combination of these valvular lesions, and can pose challenges for surgical correction, limiting treatment options.
“We've known for a long time that safe options are needed for patients with severe MAC,” said Sorajja, noting that SUMMIT-MAC is the first non-randomised, prospective, multicentre clinical study to assess a dedicated TMVR system in this patient population.
years), with nearly half aged 80 years or older, and the majority were women (57%). Significant comorbidities, including atherosclerosis, renal disease, chronic lung disease, and pulmonary hypertension, were common.
Most patients (97.1%) had MR grade 3+ or 4+ at baseline, and severe mitral stenosis (MS) was present in 12 patients (11.7%). Baseline mitral gradient in these patients was 5.3±2.2 mmHg. The average MAC volume for the SUMMIT-MAC cohort was 5,679±5,670mm3, with 46% of patients expected to have some encroachment of the valve frame due to the configuration of the MAC. However, the device was successfully implanted in all cases, Sorajja reported.
The primary endpoint of freedom from all-cause mortality and heart failure hospitalisation at one year was met, and one-year freedom from all-cause mortality and freedom from heart failure hospitalisation rates were 79% and 69.9%, respectively. Bleeding was the most common severe adverse event with apical access site bleeding occurring in 5.8% of patients.
At one year, 97% of patients had mild or no mitral valve regurgitation. In addition, heart failure symptoms improved significantly with only 13% of patients having New York Heart Association (NYHA) class III symptoms compared with 73% prior to the procedure. Quality of life also improved at one year with an average 18.7-point increase in the Kansas City Cardiomyopathy Questionnaire (KCCQ) score.
Features of the device, which is retrievable and repositionable, include dual frame design, tether and apical pad. However, the need to deliver the device transapically is one potential drawback.
All patients enrolled in the trial had severe MAC, were considered high surgical risk and were approved by a case-review committee. An echocardiography core laboratory performed independent assessments of mitral disease for study inclusion and assessed all follow-up echocardiograms.
A total of 103 patients with severe MAC and mitral valve disease (either mitral regurgitation or stenosis) underwent an attempted procedure with this transcatheter mitral valve system at 37 centres in the USA.
The trial’s population was described as elderly (78±6.5
“These patients actually don’t have a good option,” said Sorajja, summing up the results of the trial and speculating on whether the results could prompt a change in guidelines for the treatment of MAC. “These are patients who were not qualified for surgery and not qualified for any available transcatheter option.
“What we showed in this trial is for a group of patients that had no options, we finally have an option that met the study endpoint and was meaningful in terms of clinical benefit. So, I do believe that this will change the clinical guidelines.”
Sorajja was quizzed on whether there may be alternatives to the transapical delivery, which he commented may warrant careful heart team consideration when deciding which patients to treat.
“The total apical or thoracotomy fatality rate was 2.9%. So, about a 3% risk of dying from this wound. Can we pick patients that may be a lot less risk; somebody who's not on steroids, somebody who has good chest cavities, somebody who's younger? Probably. I think with surgical experience, in the setting of left ventricular (LV) dysfunction, there's an experience factor for that. So, I think it's a heart team discussion.”
Multicentre study to assess outcomes of TAVI and SAVR in bicuspid valves
Cedars-Sinai (Los Angeles, USA) has been awarded US$26 million by the Patient-Centered Outcomes Research Institute (PCORI) to study outcomes of transcatheter aortic valve implantation (TAVI) and surgical aortic valve replacement (SAVR) in patients with bicuspid aortic stenosis.
LED BY INTERVENTIONAL
cardiologist Raj Makkar, the six-and-ahalf-year award from PCORI will fund a multicentre clinical trial of patients 50 years and older who were born with a bicuspid aortic valve, a condition in which the aortic heart valve has two flaps regulating the flow of blood rather
than the normal three.
Bicuspid aortic valve is the most common congenital heart condition, affecting approximately 2% of people, but little data exist comparing current treatments.
“Transcatheter aortic valve replacement has changed the paradigm
Sustained remodelling achieved at two years with transcatheter LV restoration system
Two-year results from an analysis of early clinical studies evaluating the Accucinch (Ancora Heart) transcatheter left ventricular (LV) restoration system have been published in the journal Structural Heart, demonstrating that reverse remodelling achieved with the system was sustained through two years, along with improvements in heart function, quality of life, and reduced heart failure hospitalisations.
“REVERSE REMODELLING IS usually associated with reduced heart failure events and mortality,” said Daniel Burkhoff, director, Heart Failure, Hemodynamics and MCS Research at the Cardiovascular Research Foundation (CRF). “From a clinical perspective, the fact that reverse remodelling is maintained at two years is particularly meaningful.”
The analysis evaluated clinical outcomes from 51 symptomatic heart failure with reduced ejection fraction (HFrEF) patients from multiple sites in the USA and Europe. Key outcomes include sustained reverse remodelling with a mean decrease in left ventrical (LV) end-diastolic volume of 30.0±38.8 mL (p<0.001) and an increase in ejection fraction of 5.4±9% (mean ± SD; p<0.001).
Improvements were also seen in functional status and symptoms, including a median 19.5-point increase in Kansas City Cardiomyopathy Questionnaire (KCCQ) score (p<0.001), improvement by at least one New York Heart Association (NYHA) class in 60% of patients, and 98% either improved or remained stable. The rate of heart failure hospitalisation two years following implant was significantly reduced compared to the year prior to the implant.
for non-surgical treatment of aortic stenosis, but it needs to be studied more rigorously in patients with bicuspid aortic valves,” said Makkar, a principal investigator of the study and vice president of Cardiovascular Innovation and Intervention at CedarsSinai. “We look forward to addressing this important evidence gap with this PCORI-funded randomised controlled trial in collaboration with our esteemed co-investigators.”
Patients with bicuspid aortic valve stenosis will be randomly assigned to have their aortic valve replaced via open-heart surgery or by a transcatheter procedure. Investigators will review results from both groups to understand which option results in better outcomes.
“This research is a prime example of how Cedars-Sinai fosters innovation
and brings leading-edge and clinically effective research directly to patient care,” said Shlomo Melmed, CedarsSinai’s executive vice president of Medicine and Health Sciences and dean of the Medical Faculty. “The findings from this clinical trial will help doctors globally advise their patients born with a bicuspid aortic valve on the best and safest approach for treating their cardiac condition.”
The award has been approved pending completion of a business and programmatic review by PCORI and issuance of a formal award contract.
PCORI is a non-profit organisation with a mission to fund research designed to provide patients, their caregivers and clinicians with the evidence-based information needed to make betterinformed health care decisions.
Tendyne
Latest data “reassuring” on safety and effectiveness of transcatheter tricuspid interventions
Analysis of data from the Society of Thoracic Surgeons (STS) and American College of Cardiology (ACC) TVT registry, charting early US commercial experience with the Evoque (Edwards Lifesciences) transcatheter tricuspid valve replacement (TTVR) system, has demonstrated favourable short-term safety and effectiveness of the device, according to investigators.
Rahul Sharma (Stanford Unversity, Palo Alto, USA) presented 30-day clinical and quality-of-life data from the first 1,034 patients treated with Evoque in the USA in a late-breaking presentation at the 2025 Transcatheter Cardiovascular Therapeutics (TCT) meeting (25–28 October, San Francisco, USA), describing the findings as “very reassuring”.
Evoque was the first tricuspid valve replacement system to receive US Food and Drug Administration (FDA) approval for the treatment of tricuspid regurgitation (TR), when it was approved in February 2024, indicated for the improvement of health status in patients with symptomatic severe TR despite optimal medical therapy, for whom tricuspid valve replacement is deemed appropriate by a heart team. This came after CE-mark approval in October 2023.
The system is comprised of a nitinol self-expanding frame, intra-annular sealing skirt and tissue leaflets made from bovine pericardial tissue, which is delivered transfemorally. “It’s designed to seal within the native tricuspid annulus using both an intra-annulus sealing skirt and the presence of the frame and interaction with the leaflets,” Sharma said.
Six-month results from the randomised controlled pivotal trial, TRISCEND II, presented at TCT in 2023, reported favourable safety and effectiveness outcomes, demonstrating superiority to optimal medical therapy alone and meeting all primary endpoints. Key findings in the trial included significant reduction or elimination of TR and significant and sustained quality-oflife improvement.
Using data from the TVT registry, Sharma and colleagues sought to categorise the procedural, clinical, echocardiographic, functional and quality-of-life outcomes at 30 days among patients who underwent commercial TTVR with Evoque in the US between February 2024 and March 2025.
Patients had an average age of 77 years, Sharma reported, noting that there was a significant number (69%) females treated. Nearly three quarters were New York Heart Association (NYHA) class III or IV, and nearly half had a heart failure hospitalisation in the preceding year. Sharma noted that the average procedure time stood at around 103 minutes, similar to what was seen in TRISCEND II, with the device successfully implanted in over 98% of patients. A significant proportion of patients were discharged to home with the average
hospital length-of-stay at two days, shorter than what was seen in the randomised trial.
Rates of in-hospital and 30-day all-cause mortality stood at 2.3% and 3.1% respectively. Rates of bleeding, meanwhile, at 6.9% in-hospital and 7.9% at 30 days, were lower than those seen in TRISCEND II, Sharma noted.
A “significant” improvement in TR status was seen at 30 days in both unpaired and paired analysis of the data, with the vast majority of patients having non-trace or mild tricuspid regurgitation at the 30-day timepoint. There was a trend towards improved positive right ventricular (RV) remodelling demonstrated by an improvement in end-diastolic mid-RV diameter and RV systolic pressure, Sharma commented of the echocardiographic parameters, adding that tricuspid valve gradients remained acceptable. Similarly, there was a significant improvement in NYHA functional class and Kansas City Cardiomyopathy Questionnaire (KCCQ) scores in patients paired data between baseline and 30 days.
stay of two days.”
Also at TCT 2025, Jonathan Schwartz (Sanger Heart & Vascular Institute, Charlotte, USA) presented insights from a continued access study of patients who underwent an attempted tricuspid transcatheter edge-to-edge repair (TEER) procedure with the Triclip (Abbott) procedure in the TRILUMINATE pivotal trial. Similar to Abbott’s Mitraclip mitral repair technology, Triclip is a transfemorally delivered system that works by clipping together a portion of the leaflets to repair the tricuspid valve and reduce TR. US Food and Drug Administration (FDA) approval for the system was granted in April 2024, following CE mark in 2020. The TRILUMINATE pivotal trial, which randomised patients with severe TR either to TEER with Triclip or optimal medical therapy, showed that at two years, patients treated with the device were less likely to be hospitalised for recurrent heart failure than patients, not treated with the device though rates of all-cause mortality in the two arms were similar.
Schwartz presented 30-day follow-up data from patients included in the randomised arm of the pivotal trial, a single-arm trial, and patients enrolled in the continued access study, totalling 847 attempted Triclip procedures.
Detailing the characteristics of the patient cohort, Schwartz reported that patients had an average age of 79 years, 59% were female, 26% had been hospitalised for heart failure within the year prior to their Triclip procedure, and, significantly, 27% had an implantable electronic device.
Implant success was high, with a rate of 98.7%, with patients receiving an average of two devices. Procedure time averaged 146 minutes, with an average of 82 minutes for the device implant. Patients had an average length of hospital stay of one day, with 96.2% discharged to home.
Describing the results as “very reassuring”, Schwartz detailed that around 82% of patients had moderate or less TR at 30-day follow-up, with KCCQ scores improving on average by 17 points from baseline. Adverse event rates were low, with allcause mortality occurring in 0.5% of cases, major bleeding in 3%, and heart failure hospitalisation in 3%.
“Specifically looking at patients that have electronic devices implanted, this can make the procedure much more complicated, both from an imaging perspective and then navigating around the leads,” Schwartz commented, adding that outcomes among these patients were “very reassuring as well”,
“There are, of course, limitations with a real-world study,” said Sharma. “The echocardiographic assessments were performed by the sites and site-reported without the presence of core lab adjudication. The events themselves were also sitereported with the absence of a centralised clinical events committee review.”
Nevertheless, he commented that the data demonstrate low mortality and heart failure hospitalisation rates seen with the Evoque device.
“The elimination of TR with more than 97% of patients achieving mild or less residual tricuspid regurgitation, significant improvements in functional capacity and quality of life, and lower pacemaker and lower bleeding rates compared to what we experienced in the randomised trial,” Sharma said. “Almost all patients were discharged home with a median hospital
More than 97% of patients achieved mild or less tricuspid regurgitation.”
with adverse event rates that were broadly in line with patients without implantable devices.
Schwartz also presented analysis stratifying procedural outcomes, adverse events and TR reduction based upon the experience levels of the centres performing the cases, which appeared to show that outcomes improved as the centres gained more proficiency with the procedure.
“As the experience grew, pretty much every category improves,” he commented. “Device times dropped significantly, procedure times down, clip numbers down, intensive care unit [ICU] admissions, adverse event rates, moderate TR or less increased slightly, and TR grade reduction also.”
Rahul Sharma
Triclip
Evoque
Dapagliflozin does not add to quality-of-life benefit gained from TAVI
Patients receiving dapagliflozin after transcatheter aortic valve implantation (TAVI) saw no additional improvement in quality-of-life compared to patients receiving only the standardof-care treatment.
THIS IS THE HEADLINE FINDING of an analysis of the investigatorinitiated DapaTAVI trial, a randomised study promoted by Spanish Society of Cardiology (SEC) and Cardiovsacular National Center of Cardiovascular Research (CNIC, Madrid) investigating the addition of the drug—known as Farxiga (AstraZeneca)—after TAVI.
Primary results of the trial, which were presented at the 2025 American College of Cardiology (ACC) scientific session (29–31 March, Chicago, USA), showed that the addition of dapagliflozin among older adults undergoing the procedure, resulted in a significantly lower incidence of death or worsening heart failure than standard of care alone.
For the latest, prespecified analysis of the trial, investigators assessed the change in Kansas City Cardiomyopathy Questionnaire (KCCQ) score—which uses patient-reported outcomes to measure symptoms, physical and social limitations—from baseline to three and 12 months in both arms of the study to chart the potential impact of the addition of the drug on quality of life after the procedure.
What the investigators saw was that
among the 964 trial patients who had a baseline KCCQ score, there was no significant difference between the two groups in the magnitude of their improvement at three or 12 months.
At 12 months, similar proportions of patients in the dapagliflozin and control groups showed clinically meaningful improvements, with 43.4% vs 45.4%, respectively, improving by >50 points, the investigators report in their publication of the findings in the Journal of the American College of Cardiology (JACC).
“These results highlight the profound effect of TAVI on symptom relief and quality of life in older adults with severe aortic stenosis,” study author Clara Bonanad-Lozano (Clinic University Hospital of Valencia, Valencia, Spain) and colleagues write in the JACC paper. “However, no additional improvement in health status—assessed by the KCCQ—was observed with dapagliflozin in those patients. Importantly, the prognostic benefit of dapagliflozin on the composite endpoint of all-cause death or worsening heart failure was consistent across the full range of baseline KCCQ-overall
summary scores.”
The principal investigator of DapaTAVI trial, Sergio RaposeirasRoubin (Alvaro Cunqueiro Hospital, Vigo, Spain), stated that there is a plausible biological rationale for expecting health status improvements with dapagliflozin in this context, as even after successful valve replacement, many patients continue to experience impaired functional capacity secondary to residual diastolic
modifying—aimed at reducing clinical events—rather than enhancing perceived health status, adding: “Clinicians should not necessarily expect improvements in symptoms or quality of life attributable to dapagliflozin beyond those achieved by valve replacement alone.”
Several potential mechanisms may explain why dapagliflozin did not improve health status in this specific clinical context, despite its benefits in patients with heart failure, they add, noting that in patients with chronic heart failure, dapagliflozin has been shown to improve symptoms and quality of life through mechanisms such as natriuresis, reduction in ventricular filling pressures, improved left ventricular compliance, anti-inflammatory effects, and weight loss—effects that are particularly relevant in patients with persistent congestion and systemic neurohormonal activation.
dysfunction, subclinical congestion, or myocardial fibrosis, mechanisms that SGLT2 inhibitors may positively influence through their diuretic, antiinflammatory, and metabolic effects. Based upon their findings, however, they state that the role of dapagliflozin appears to be primarily disease
“Minimalist” approach to TAVI may be an option for most patients
A “minimalist” transcatheter aortic valve implantation (TAVI) strategy—using local anaesthesia without sedation—has been shown to be non-inferior to a standard approach involving sedation for a composite primary endpoint of cardiovascular events and complications at 30 days.
THIS IS THE HEADLINE FINDING OF THE DOUBLE-CHOICE trial, an investigator-initiated, open-label, 2×2 factorial randomised trial, conducted at 10 centres in Germany, in which investigators assessed the two approaches in more than 750 patients. Results were presented at the 2025 European Society of Cardiology (ESC) congress (29 August–1 September, Madrid, Spain).
“Minimalist treatment strategies for TAVI—such as using local anaesthesia without sedation—have been widely adopted due to continued procedural evolution. However, large, randomised trials comparing the minimalist approach with the standard of care have not been performed,” investigator Mohamed Abdel-Wahab (Heart Center Leipzig at Leipzig University, Leipzig, Germany) said of the research. “Furthermore, while several head-to-head trials of different TAVI devices have been conducted, comparisons are lacking between different contemporary self-expanding devices in patients with well-defined anatomy.”
The study included patients with severe, symptomatic aortic stenosis whose anatomy was considered suitable for the procedure using either the Evolut Pro, Pro+ or FX (Medtronic) or the now discontinued Acurate neo2 valve platforms.
Patients were randomised either to undergo a minimalist procedure, which included isolated local anaesthesia with no sedation, central venous lines, additional arterial lines for blood pressure monitoring, or urinary catheters. Patients in the standard anaesthesia group were sedated with continuous CO2 monitoring, supplemental oxygen and the use of central venous catheters, additional arterial lines and urinary catheters according to local practice.
In patients with severe symptomatic aortic stenosis undergoing TAVI, however, the primary determinant of symptoms and impaired health status is the fixed mechanical obstruction caused by the stenotic aortic valve. “Once this obstruction is relieved by valve replacement, there is an immediate and profound haemodynamic improvement that drives substantial symptomatic and functional recovery,” the investigators note.
Future trials should consider patients with persistent congestion, elevated biomarkers, or low KCCQ scores after TAVI, to better identify those patients who may benefit symptomatically from SGLT2 inhibition, Bonanad-Lozano et al suggest.
30-day combined endpoint that included all-cause mortality, stroke, moderate or severe prosthetic valve regurgitation, and permanent pacemaker implant.
The 752 patients in the intention-to-treat anaesthesia comparison had a median age of 83 years and almost 60% were women. The primary combined endpoint at 30 days occurred in numerically fewer patients with minimalist vs. standard care: 22.9% vs. 25.8%. Around 19% of patients crossed over to the standard-care group, mostly due to pain or discomfort.
The trial’s primary combined endpoint at 30 days included all-cause mortality, vascular and bleeding complications, infections requiring antibiotic treatment and neurologic events. The use of the two device platforms was also compared with a primary
Around 80% of patients can be safely managed with the minimalist approach.”
In per-protocol and as-treated analyses, the difference in favour of the minimalist approach was more pronounced and statistically significant in the as-treated analysis, Abdel-Wahab detailed.
Across 855 patients in the device comparison, the primary combined endpoint at 30 days occurred in 15.4% of patients with Acurate neo2 valve and 30.4% with Evolut valves, a difference that was mainly driven by lower pacemaker implantation in the Acurate group—11.2% vs. 26.5%, respectively.
“Our results indicate that around 80% of patients can be safely managed with the minimalist approach,” Abdel-Wahab said of the results. “Further analyses may help to better inform in which subgroups the minimalist approach is most or least suitable.
“Regarding devices, we found that Acurate neo2 valves were superior to Evolut valves in our trial, which was conducted by highly experienced operators with careful patient selection. Acurate neo2 valves have since been withdrawn, but reductions in pacemaker implantation observed with these devices indicate that aspects of their design could be used to inform future valve development.”
Mohamed Abdel-Wahab
Report seeks to level the playing field for women in heart valve care
For Jacqueline Lewis, a former nurse and pharmaceutical industry executive, the path to heart valve surgery was far from straightforward. In early 2024, shortly after turning 63, she found herself frequently feeling out of breath during her day-today activities, which, she said, was out of character for someone who had regularly run and practiced yoga throughout her life.
Concerned by these warning signs, Lewis consulted her GP, where she was told that the symptoms could be linked to anxiety or the menopause, but was nevertheless referred to a cardiologist who promptly diagnosed left ventricular hypertrophy, necessitating an angiogram.
“The results of the angiogram came back and they said it wasn’t angina—but I hadn’t thought that was what it was, as I wasn’t getting chest pain—it was palpitations and breathlessness. At that point I was discharged,” Lewis tells Cardiovascular News of the confusion and worry associated with her diagnosis and initial care.
After trying and failing to seek further consultation to get to the root of the problem, in between which she was forced to give up work due to her deteriorating health, Lewis eventually sought the advice of another cardiologist, who, upon listening to her heart with a stethoscope, immediately recognised that she would need aortic valve surgery, which she underwent successfully some 12 weeks later. “If I hadn’t had the knowledge I have got, and the confidence to stand up and say ‘I need to be listened to now’, where would I be?” Lewis says, reflecting on how her previous experience of having worked in the healthcare industry ultimately helped her to achieve a satisfactory outcome.
Many women, however, may not be so fortunate. A new report from Global Heart Hub, an international alliance of heart patient organisations—Shaping the future for women with heart valve disease—suggests that Lewis’s experience is far from isolated and that, for a multitude of reasons, heart valve disease is going undiagnosed and untreated in scores of women worldwide.
Interdisciplinary action
Lewis is among the contributors to the report, one of several patients to provide a perspective on the care pathway for the detection, treatment and management of heart valve disease, alongside clinicians such as Marta Sitges, a non-invasive cardiologist at Hospital Clinic Barcelona (Barcelona, Spain), bringing expertise from the healthcare community. Both Lewis and Sitges are co-chairs of this initiative. Drafting of the report followed structured interviews and a subsequent in-person roundtable to reach a set of recommendations actions to drive change across a broad set of areas from diagnosis to clinical recruitment and elsewhere.
Sitges tells Cardiovascular News that, in her view, there are a host of reasons why the treatment of heart valve disease may require a different approach when dealing with women compared to men. “There are differences in the type of disease, there are differences in the way they present, and, this is more difficult to prove, but definitely there are differences in the
way the symptoms are interpreted,” she says.
Important distinctions highlighted in the report include, for example, that in females, aortic stenosis is typically characterised by less calcification and more fibrotic remodelling of the aortic valve when compared to males, whilst mitral valve disease is more often associated with mitral valve prolapse or rheumatic disease in women, who have a higher prevalence of mitral stenosis when compared to men.
engage women in research— because ‘no I have to take care of my family; I can’t come to the consultations’— this is something we have an idea of, but this is not something we can objectively prove,” she adds, highlighting that even the reasons underlying the historic poor recruitment of women in trials is poorly understood.
What’s more, Sitges says, women may have a harder time in convincing their healthcare provider that their symptoms are indeed related to heart valve disease at all, echoing Lewis’s difficulty in having her symptoms correctly diagnosed.
There are definitely differences in the way symptoms are interpreted.” Marta Sitges
A key contributor to this issue is the historic disparity in the number of women recruited to clinical trials in cardiovascular medicine, particularly of device-based treatments, and relatively few studies focused on female-only populations—meaning that much of the current consensus on treatment is driven by studies with overwhelmingly male cohorts. Addressing this is among the main action points within the Global Heart Hub report, which sets out steps to ensure that research on heart valve disease reflects sex and gender-specific differences by actively including women in clinical studies.
“More recently, with the advent of transcatheter therapies, there have been some randomised studies in patients with heart valve disease—typically comparing one transcatheter therapy to conventional surgery or even medical therapy. In these studies many have been in a male population, not so much through the restriction of entry criteria, but rather, that these diseases involve more frequently men,” comments Sitges.
“Then comes the hypothesis of gender-related issues, that maybe sometimes it is more difficult to
Recent studies, including the RHEIA trial, which compared transcatheter aortic valve implantation (TAVI) to surgical aortic valve replacement (SAVR) in an exclusively female population, show that some steps are being taken to bridge this long-held data gap, whilst the latest guidelines form the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) on valvular heart disease contain, for the first time, distinct recommendations for clinicians to consider when treating female patients. Sitges welcomes both developments but says the pace of change still falls some way short of what is required.
Future steps
“This is why this work is important, to increase the awareness of this problem,” she adds, commenting on the relevance of the recommendations within the Global Heart Hub report. “The medical community is moving forward to personalised medicine, but medicine is still very based on evidence and evidence is quite global. It is for the median, it is not personalised.”
Other action points in the report include the development of comprehensive educational material to provide patients with the knowledge to recognise risks and symptoms of heart valve disease, and to better understand their treatment options, alongside implementing educational activities to promote understanding of how heart valve disease presents and progresses in women.
Expanding access to detection and diagnostic technologies to improve early detection in underserved and high-risk populations, in particular, is also advocated, alongside the establishment of screening campaigns to identify undiagnosed cases of heart valve disease among women in these high-risk groups.
Finally, the report calls for all stakeholders, including policymakers, healthcare providers, patient organisations and wider society to work together to establish person-centred care based on equal access and opportunities at every stage.
Global Heart Hub in collaboration with Heart Valve Voice UK and Heart Valve Voice Canada will host a session titled ‘Learning from Lived Experience and Contemporary Evidence: Shaping the Treatment of Women with Heart Valve Disease’. It will take place on the second morning of the upcoming PCR London Valves meeting (16–18 November, London, UK). The session will feature a patient and several clinicians, highlighting the lived experience of women with valvular heart disease, and discussing diverse perspectives of the unique challenges of the detection, diagnosis, treatment and follow-up of women with these conditions.
To access the report
scan here: Scan the QR code to read a full copy of Shaping the future for women with heart valve disease
Marta Sitges Jacqueline Lewis
Edwards’ Brüls outlines company’s move to specialise on structural heart disease”
When Cardiovascular News sits down with Annette Brüls at the 2025 European Society of Cardiology (ESC) congress (29 August–1 September, Madrid, Spain), Edwards Lifesciences’ corporate vice president for EMEA, Canada, and Latin America is in a bullish mood, buoyed by the release of new European guidelines for the management of valvular heart disease which, in her words, underscore the growing confidence in transcatheter therapies for the treatment of aortic, mitral and tricuspid valve disease.
FOR A COMPANY THAT HAS bet big on growth in the structural heart field—selling its critical care business in mid-2024 to fund a slew of investments and acquisitions in its structural heart portfolio— the guidelines’ strengthened recommendations for transcatheter therapies represent a welcome development.
Headlines from the latest guideline document—which has been jointly compiled by both the ESC and the European Association for CardioThoracic Surgery (EACTS)—include a new, lower, age threshold for transcatheter aortic valve implantation (TAVI) in patients with severe aortic stenosis, a class IIb recommendation for transcatheter procedures for patients with atrial secondary mitral regurgitation, as well as stronger backing for transcatheter procedures in the treatment of tricuspid valve disease.
The guidelines also nudge clinicians towards earlier intervention in selected asymptomatic patients with severe aortic stenosis, supported in part by evidence from the Edwards-sponsored EARLY TAVR trial, in which it was shown that patients randomised to TAVI with the Edwards Sapien 3 platform experienced superior outcomes compared to clinical surveillance.
“We have been working on this for many years, and it is a new era,” says Brüls of this update. “For patients with
severe aortic stenosis, they should now be considered for treatment, even independent of having symptoms and independent of their ejection fraction— which is major.”
Brüls believes there is a case to be made from both a patient and a healthcare provider perspective in treating more asymptomatic aortic stenosis—which, she says can exceed some forms of cancer for mortality if left untreated—and makes the argument that more proactive management of the disease can reduce burden on healthcare systems.
“Until now, the guidelines were saying you have to wait until you have symptoms, but these can be severe symptoms, hospitalisations, decompensation and deaths. With our latest technologies, the risk related to an intervention is really close to zero and there is no reason to wait.”
She acknowledges, however, that there will be significant challenges in many regions in moving towards a more proactive treatment approach, particularly in regard to treatment capacity, with some healthcare systems already facing sizeable waiting lists, and says that Edwards, with a fresh CE mark indication for the Sapien valve for the treatment of asymptomatic aortic stenosis, has a role to play in helping to bring this therapy to patients at an earlier stage in the treatment pathway.
“We have to find ways in this constricted system to help to get ahead
of the curve, because otherwise it only gets worse. Once you start to get ahead of the curve, these emergent cases will diminish and then suddenly you get to a new steady state which is much better, so I think we need to manage that transition carefully.
“The good news is it all starts with the guidelines. Now we have a mandate to look at these patients, and I think that is the big breakthrough.”
In particular, Edwards is seeking to highlight the potential cost effectiveness of early intervention, with data presented at EuroPCR 2025 (20–23 May, Paris, France) pointing towards lower healthcare system costs, shorter hospital length of stay, and fewer rehospitalisations when patients were treated before symptom onset.
Outside of TAVI, Brüls underlines Edwards’ ambition across the structural heart space, with recent acquisitions
Structural heart disease it is probably one of the most innovative areas, and most complex areas that there is in interventional cardiology.”
bolstering the company’s established device portfolio which includes the Pascal mitral repair system and Evoque tricuspid valve replacement system.
“If you look at structural heart disease, it is probably one of the most innovative areas, and most complex areas that there is in interventional cardiology. The advancements that we can make there are massive. There are a lot of unmet needs,” she comments.
“We see it as an area that is highly complex but where we have a lot of
Smart implant for pressure-guided heart failure decongestion wins TCT 2025 Shark Tank prize
Relief Cardiovascular—developer of a smart implant designed to haemodynamically monitor and treat congestion in heart failure—has been named as the recipient of the Shark Tank innovation prize at the 2025 Transcatheter Cardiovascular Therapeutics (TCT) conference (25–28 October, San Francisco, USA).
THE RELIEF SYSTEM WAS ONE OF SIX technologies competing for the prize, which included a next-generation transcatheter Endo-Bentall system (P&F Products), a leaflet resection and extraction system from Tresquare, circulatory decongestion support (Pulnovo Medical), and artificial intelligence (AI)-guided robotic imaging navigation platform (Laza Medical). Pathwai, a next-generation cardiac screening technology, was the runner up.
The Relief system features a pressure-guided active valve implanted in the vena cava which is designed to dynamically reduce cardiac preload and enhance renal vein flow. The technology integrates haemodynamic monitoring with an adaptive haemodynamic therapy
expertise. We have been in the space of helping patients with valvular disease for 65 years, we are the category leader, so we believe we have the expertise to bring in new areas. It is a huge unmet need which has a huge impact on society; these patients are decompensated, they have heart failure, they are frequently hospitalised, so it is really one of these patient populations where the clinical but also the economic benefit for the system is massive, and we are the pioneers.”
Brüls comments that Edwards has sought out potential disruptors in the structural heart space as it seeks to refocus its business solely into this segment.
Acquisitions and investments announced by the company over the last 12 months include the proposed agreement to acquire JenaValve, maker of the Trilogy TAVI system for the treatment of aortic regurgitation; JC Medical, which is also developing a device for aortic regurgitation; Innovalve Bio Medical, developer of an early-stage transcatheter mitral valve replacement (TMVR) technology; as well as an agreement with Affluent Medical relating to the company’s mitral valve technologies; and a deal to acquire Endotronix, the developer of the Cordella pulmonary artery (PA) sensor, an implantable heart failure patient management platform. In August 2025, the US Federal Trade Commission (FTC) moved to block the JenaValve acquisition due to concerns that the acquisition would limit access to devices for the treatment of aortic regurgitation due to Edwards, however Brüls tells Cardiovascular News that the company remains committed to seeing the deal over the line. “I can say that we are committed to this and we will do everything we can,” she comments.
“We think we have very compelling arguments, that show that this is a very good thing for patients, for innovation, and that with our knowledge and expertise we can really bring to market and to patients, so we are continuing.”
into a single transcatheter implant system.
Relief Cardiovascular recently announced the successful first-in-human use of the system, performed in the Republic of Georgia as part of a feasibility study evaluating the device’s safety.
Implantations were carried out by Tamaz Shaburishvili, Levan Sulakvelidze, and Gigi Shaburishvili at Tbilisi Heart and Vascular Center (Tblisi, Georgia), with support from Alex Rothman University of Sheffield (Sheffield, UK).
“Managing heart failure often feels like aiming at a moving target,” said Rothman. “In small cohorts of patients, clinical teams track remotely measured pressures and continuously adjust medications to optimise therapy, which has been proven to improve outcomes.”
Annette Brüls
Product News
Hearflow’s next-generation Plaque Analysis algorithm gains US FDA clearance
Heartflow has received US Food and Drug Administration (FDA) 510(k) clearance for its next-generation Heartflow Plaque Analysis algorithm and the platform is now available.
The technology features an updated algorithm, expanded nomogram, and advanced 3D color-coded visualisation of plaque type, volume, and distribution.
Heartflow Plaque Analysis is an AI-powered plaque quantification tool with a reported 95% agreement with the gold standard, intravascular ultrasound (IVUS), using blinded core lab adjudication, Heartflow says in a press release. The latest algorithm advancement shows 21% improvement in plaque detection compared to the first-generation algorithm, so clinicians can be confident in their diagnosis and management of coronary artery disease.
“Understanding not only how much plaque is present, but also plaque type and distribution, is critical in predicting patient risk and guiding personalised treatment,” said Matthew Budoff (David Geffen School of Medicine at the University of California Los Angeles [UCLA] Medical Center, Los Angeles, USA). “With these enhanced capabilities, Heartflow Plaque Analysis provides clinicians with the clarity we need to move from detection to decision with speed and confidence.”
Heartflow recently shared insights from the DECIDE registry, showing Heartflow Plaque Analysis led to medical management change in over 50% of patients beyond coronary CTA alone, resulting in an expected ~15% event reduction.
Medtronic partners with DASI Simulations to bring AI modelling technology to US TAVI centres
Medtronic and DASI Simulations have announced a strategic partnership to enhance access to DASI technology to optimise outcomes for patients undergoing transcatheter aortic valve implantation (TAVI) in the USA. Integrating DASI Simulations’ advanced AI-based predictive modelling and digital twin technology into the TAVI workflow will give clinicians access to independent and device-agnostic actionable insights that support more precise, individualised treatment decisions for patients living with aortic stenosis, the organisations said in a press release.
“Effective pre-case planning is essential to achieving optimal outcomes in TAVI,” said Matthew Summers, interventional cardiologist at Sentara Heart Hospital, Norfolk, USA. “Integrating DASI’s predictive modelling into our workflow has allowed us to better visualise anatomy, anticipate risks, and tailor valve decisions to each patient. It’s helped us focus on individual factors like annular rupture, coronary occlusion, and paravalvular leak, while also planning for future reinterventions.”
DASI’s US Food and Drug Administration (FDA)-cleared platform leverages real patient computed tomography (CT) anatomies and retrospective outcomes to simulate multiple transcatheter heart valve (THV) deployment scenarios. Using these data-driven reports will help mitigate human error, predict complications, and optimise longterm management for structural heart patients, the press release adds.
Medtronic has also announced the launch of the Stedi Extra Support guidewire, designed to enhance stability during TAVI valve deployment, particularly in conjunction with its Evolut platform.
Compatible with all commercially available TAVI systems for patients with severe aortic stenosis, the Stedi guidewire combines a stiff proximal main body, gradual stiffness transition, and distal curve designed for stability, predictability, and safety, the company says in a press release.
“The Stedi Extra Support guidewire represents a meaningful advancement in TAVI,” said Tanvir J Bajwa (Advocate Health, Milwaukee, USA). “It enhances stability and predictability during valve deployment, especially when paired with techniques like simplified cusp overlap, and reinforces procedural consistency with the Evolut platform. This innovation supports more predictable outcomes and the precision we strive for in treating patients with severe aortic stenosis.”
Bench testing in a simulated anatomy has demonstrated that use of the Stedi guidewire, during deployment, when compared to less supportive wires with the Evolut platform, provides a reduction in ventricular movement, improved stability, and a more coaxial deployment, the company’s press release adds. Additionally, when used with the cusp overlap technique, extra support guidewires have been shown to be associated with a lower rate of permanent pacemaker implantation at 30 days.
The Stedi Extra Support guidewire has US Food and Drug Administration (FDA) clearance and is currently available in the USA.
Elixir Medical’s LithiX HC-IVL system gets full market release Elixir Medical has announced full
market release of its LithiX Hertz Contact (HC) intravascular lithotripsy (IVL) system, following CE mark approval earlier this year.
The LithiX HC-IVL system is an advanced intravascular lithotripsy technology designed to optimise device expansion in calcified coronary artery blockages during an angioplasty procedure.
The LithiX device is a highly deliverable balloon-based system with integrated low-profile metallic hemispheres to create focal pressure amplification based on Hertz Contact Stress principle.
The Hertz Contact Lithotripsy hemispheres work selectively on calcium within the target lesion, breaking apart and fragmenting the hardened plaque under low balloon inflation pressure. The hemispheres create multiple highly localised points of contact force to create deep and wide fractures while sparing the adjacent non-calcified vessel tissue.
Following CE mark announcement and limited market release in early April, Elixir Medical has announced that over 400 patients have been treated with LithiX HC-IVL across 16 countries in Europe and Asia
“LithiX quickly became our primary calcium modification tool. As a high-volume centre, we value its effectiveness and versatility enabling us to treat the most complex calcified lesions in patients with advanced heart disease, as well as its cost effectiveness in our practice through reduced use of additional calcium modification devices and a simpler procedure flow,” said Tamil Selvan Muthusamy of Cardiac Vascular Sentral Kuala Lumpur (CVSKL) Hospital, Kuala Lumpur, Malaysia.
The successful completion of the limited market release enables Elixir Medical to continue expansion of LithiX HC-IVL into global markets, Elixir Medical said in a press release.
J-Valve TAVI system granted approval for treatment of aortic regurgitation in China
Genesis MedTech’s structural heart subsidiary, Suzhou Jiecheng, has received approval from China’s National Medical Products Administration (NMPA) for the J-Valve transfemoral transcatheter aortic valve implantation (TAVI) system (J-VALVE TF), the first transfemoral TAVI system approved in China for the treatment of aortic regurgitation (AR).
The J-VALVE TF offers an alternative to open-heart surgery by using a minimally invasive transfemoral approach, which is intended to reduce surgical trauma and procedural risk while shortening
procedure time. J-Valve features a patented anchoring design, which is designed to ensure secure valve placement, protecting coronary flow and reducing the risk of complications such as paravalvular leak and conduction block.
“Behind every innovation lies a patient. We are excited as this approval brings new hope to patients with severe aortic regurgitation who previously had few safe options,” said Warren Wang, chairman and chief executive officer of Genesis MedTech. “With J-Valve TF, we can now offer patients a minimally invasive solution that is safer and a faster path to recovery.”
In August 2024, Genesis MedTech announced the sale of JC Medical to Edwards Lifesciences, in a deal that included the intellectual property and commercial rights of the J-Valve system. As part of the transaction, Genesis MedTech maintained the exclusive right to develop, manufacture and commercialise the J-Valve system in Greater China.
Terumo announces US FDA clearance for OpusWave imaging system
Terumo Interventional Systems has received 510(k) clearance from the US Food and Drug Administration (FDA) for its OpusWave dual-sensor imaging system, the company has announced.
The system, which features the DualView imaging catheter, combines optical frequency domain imaging (OFDI) and intravascular ultrasound (IVUS) to enable simultaneous views and the ability to comprehensively evaluate coronary artery disease (CAD).
The clearance marks Terumo’s imaging debut in the US market, having already entered the single-modality imaging space in Japan, Terumo said in a press release.
The DualView catheter offers a 150mm maximum pullback length, a 2.6Fr imaging profile, 6Fr guide compatibility, advanced hydrophilic coating, and a variable pullback speed of up to 40mm/second in dual mode.
“The OpusWave imaging system is an ideal technology for interventional cardiologists who perform imageguided PCI,” said Michael J Martinelli, Terumo chief medical officer. “This innovative imaging system provides the opportunity for physicians to take advantage of the benefits of both OFDI and IVUS in the assessment and treatment of any lesion morphology. Instead of having to commit to one imaging tool, they now have the flexibility to access both imaging modalities with a single catheter.”
Tria mitral valve launches in India Foldax has announced the launch of the Tria mitral valve in India, marking the first time a polymer heart valve has been made commercially available to patients anywhere in the world.
Traditional valves made from animal tissue are prone to calcification and degradation, limiting their durability
LithiX HC
Plaque Analysis
and often leading to repeat surgeries, especially for younger patients. Mechanical valves, while durable, are prone to thrombosis and require lifelong anticoagulation therapy that can impact a patient’s long-term quality of life. Foldax’s vision for its novel polymer heart valves is to address the limitations of tissue and mechanical valves by making its valves durable, with the future goal of avoiding the requirement for lifelong anticoagulation, the company says in a press release.
Mitral valve disease is a concern in India, with rising surgical volumes and increased need for long-term treatment solutions. The Tria mitral valve is positioned to offer a new option for patients seeking a durable solution without the lifestyle limitations of mechanical valves.
As part of the launch, Foldax has initiated the Evolve training & certification programme to ensure high-quality outcomes and surgeon preparedness. Physicians who complete training will be certified to implant the valve at participating hospitals.
The Tria mitral valve in the USA is limited to investigational use only. The Tria mitral valve is approved for use in India by Central Drugs Standard Control Organisation (CDSCO).
Imperative Care receives FDA 510(k) clearance for Symphony thrombectomy system Imperative Care has announced US Food and Drug Administration (FDA) 510(k) clearance of its Symphony thrombectomy system to treat pulmonary embolism (PE).
This clearance expands the use of Symphony, which had previously only been authorised for the treatment of venous thrombosis.
The clearance follows the successful completion of the SYMPHONY-PE study, a pivotal investigational device exemption (IDE) trial evaluating the safety and efficacy of Symphony for the treatment of acute PE. The study was led under the oversight of the national co-principal investigators, Vivian L Bishay, associate professor in the Department of Diagnostic, Molecular and Interventional Radiology at Mount Sinai Health System in New York, USA and Sripal Bangalore, professor in the Department of Medicine at NYU Grossman School of Medicine in New York, USA.
“The study data clearly demonstrate Symphony’s safety, efficacy and efficiency, marking a significant advancement in the treatment of patients with pulmonary embolism,” said Bishay. “These results underscore Symphony’s potential to address a critical unmet need by enabling rapid, controlled clot removal while maintaining a strong safety profile. I look forward to incorporating this important new technology into my practice to improve care for patients facing this life-threatening condition.”
“In the treatment of pulmonary embolism, reducing right heart strain is
of critical importance. The more rapidly we can remove thrombus and restore stable haemodynamics, the greater the benefit for patients,” said Bangalore.
“Based on my initial clinical experience with the Symphony thrombectomy system, I believe it has the potential to advance clinical practice by merging large-bore continuous aspiration with the safety and precision of real-time vacuum control.”
Protaryx Medical submits premarket notification to US FDA for transseptal puncture device
Protaryx Medical has submitted a 510(k) premarket notification to the US Food and Drug Administration (FDA) for its proprietary transseptal puncture device.
The device is a novel catheter system designed to improve the safety, accuracy and ease of transseptal puncture to facilitate access to the left atrium for procedures such as left atrial appendage closure (LAAC), transcatheter mitral valve procedures, and atrial fibrillation (AF) ablation. The device features an atraumatic, echogenic retractable nitinol mesh, as well as an extendable distal catheter, which are intended to enhance imaging visibility and aid deployment.
“Achieving 510(k) submission is a pivotal milestone for Protaryx,” said David Mester, chief executive officer of Protaryx. “Our team has worked with laser focus to solve one of the core workflow and ease-of-use challenges in structural heart procedures: transseptal puncture and left-atrial access. This submission brings us one step closer to offering a solution that enables physicians of all experience levels to operate with greater precision, less fluoroscopy, and a faster learning curve.”
Protaryx co-founder and system chief of cardiac surgery at Johns Hopkins Health System (Baltimore, USA), James Gammie, added: “The results from the FIH [first-in-human] study show that this device not only meets unmet needs in transseptal access but has the potential to set a new standard for safety, ease-of-use, and efficiency in left-heart interventions.”
Navitor TAVI valve picks up expanded CE mark for lowrisk patients
Abbott’s Navitor transcatheter aortic valve implantation (TAVI) system has received CE mark for the treatment of symptomatic, severe aortic stenosis in patients who are at low or intermediate risk for surgery.
The announcement of the expanded
indication for the device follows the presentation of late-breaking 30-day and one-year data from the VANTAGE study, which assessed the safety and efficacy of the device in the low- and intermediate-risk population, at the European Society of Cardiology (ESC) 2025 Congress (29 August–1 September, Madrid, Spain). The study’s results were simultaneously published in JACC: Cardiovascular Interventions
“The VANTAGE study provides the scientific backbone for expanding Navitor’s indication to low- and intermediate-risk patients. The data are exceptional across both populations, confirming that the Navitor valve performs precisely as designed,” said Nicolas van Mieghem, (Thoraxcenter, Erasmus University Medical Centre, Rotterdam, the Netherlands), who serves as principal investigator of the VANTAGE trial.
empowering physicians across the USA to offer a critical treatment option for patients with failing transcatheter heart valves who are at high surgical risk,” said Michael Caskey, attending cardiothoracic surgeon at Abrazo Arizona Heart Hospital in Phoenix (USA). “This advancement also benefits patients considering a new TAVI procedure today, giving patients options for future intervention and has the potential to profoundly improve their long-term outcomes and quality of life.”
In addition to the FDA approval, Medtronic has launched the RESTORE study to evaluate the outcomes of Redo TAVI in patients experiencing symptomatic bioprosthetic valve failure.
“Up to 50% of younger patients with aortic stenosis will also get coronary artery disease in later years, and Navitor’s design preserves options and ability for lifetime disease management if future cardiac interventions are required.”
The self-expanding device features a fabric cuff that is designed to reduce or eliminate paravalvular leak (PVL), as well as intra-annular leaflets and large frame cells to facilitate future access to the coronary arteries.
Results from the VANTAGE study showed Navitor met all safety and effectiveness primary endpoints. Among the first 262 patients with 12-month follow-up completed, there was a 2.3% rate of all-cause mortality or fatal/disabling stroke. No patients had moderate or greater PVL at 30 days and 13.6% had mild PVL at the same timepoint. There was a high rate of technical success (97%) with no procedural deaths, and the device sustained a favourable haemodynamic performance at 12 months.
Evolut TAVI systems gain US FDA approval for redoTAVI procedures
Medtronic has received US Food and Drug Administration (FDA) approval for the expanded redo-transcatheter aortic valve implantation (TAVI) indication of the Evolut TAVI system.
This approval allows for the implantation of a new Evolut transcatheter aortic valve (TAV) inside any failed previously implanted transcatheter aortic valve (TAV) and follows CE mark for Evolut PRO+, FX and FX+ systems.
The redo-TAVI procedure is indicated for patients experiencing failure of any TAV, including but not limited to severe aortic stenosis, who are at high-risk for open-heart surgery.
“FDA approval for Redo-TAVI with the Evolut system marks a significant milestone in patient care,
This pivotal study will enrol 225 participants and follow them for up to five years, focusing on both immediate and long-term clinical outcomes. The study aims to assess 30-day procedural success rates, one-year freedom from mortality and stroke, and additional measures of safety, technical success, and quality of life.
CMS finalises coverage decision for renal denervation systems
The Centers for Medicare & Medicaid Services (CMS) has finalised its National Coverage Determination decision, meaning both radiofrequency and ultrasound renal denervation for uncontrolled hypertension will now be covered under Medicare.
Medtronic and Recor Medical, which both produce renal denervation devices used to treat high blood pressure, hailed the decision in press releases.
Jason Weidman, senior vice president and president of Medtronic’s coronary and renal denervation arm, said: “This milestone enables physicians to offer patients more choices when managing hypertension, potentially leading to better outcomes for a population in urgent need of new options. We congratulate CMS and recognise all the work it took to get to this point.”
Medtronic’s Symplicity Spyral radiofrequency system was approved by the U.S. Food and Drug Administration (FDA) in 2023.
Likewise, Recor’s Paradise ultrasound renal denervation system gained approval the same month, with the company’s chief executive officer, Lara Barghout, saying: “By formally recognizing the proven clinical value of renal denervation and extending Medicare coverage, CMS is paving the way for broader, more equitable access to this breakthrough therapy. This decision not only reinforces the robust body of evidence supporting the Paradise [ultrasound renal denervation] system as a safe and effective adjunctive treatment but also delivers renewed hope to patients striving for better hypertension control and improved cardiovascular health.”
Protaryx transseptal puncture
Navitor
Clinical News
Interim RAPID-PE study reveals ‘excellent’ safety data in first 50 patients
Prespecified interim analysis data from the first 50 patients in RAPID-PE have demonstrated “excellent safety” and “remarkably efficient lab times” in patients receiving on-the-table pharmacomechanical lysis without any post-procedure infusion with the Bashir endovascular catheter (Thrombolex) for the treatment of intermediate-risk acute pulmonary embolism (PE).
The findings were presented during the 2025 Transcatheter Cardiovascular Therapeutics (TCT) conference (25–28 October, San Francisco, USA).
RAPID-PE, a single-arm, prospective, multicentre US study, protocol delivers 4mg recombinant tissue plasminogen activator (r-tPA) into each pulmonary artery (8mg total for bilateral PE) by multiple handinjected pulse sprays using an expanded 8Fr device. The dual mechanism of action is designed to create immediate mechanical fissures to restore blood flow while enabling low-dose lytic to act within and beyond the clot.
Interim data for the primary endpoint showed no mortality or haemodynamic decompensation at seven days. Major bleeding was seen in 2% and the median total procedure time was 43.5 minutes, with a median catheter dwell time of 17.5 minutes.
Presenting author Wissam Jaber (Emory University Hospital, Atlanta, USA), RAPID-PE co-national principal investigator, commented: “This interim cohort demonstrates that [the device] can democratise the catheterbased treatment of intermediate-risk PE patients with excellent safety and remarkably efficient lab times, often without the need for an ICU stay.”
Three-year results demonstrate “durable” impact of radiofrequency renal denervation Medtronic has announced new, longterm results from its final report of the SPYRAL HTN-ON MED randomised clinical trial, showing that patients treated with the Symplicity Spyral renal denervation (RDN) procedure experienced significantly greater reductions in blood pressure compared to sham patients through three years.
The data were presented as part of featured clinical research during the 2025 TCT conference.
“Radiofrequency renal denervation with the Symplicity blood pressure procedure continues to demonstrate a
durable and clinically meaningful blood pressure–lowering effect,” said David Kandzari (Piedmont Heart Institute and Cardiovascular Service, Atlanta, USA), co-principal investigator of the SPYRAL clinical programme.
“Through three years, sustained reductions in blood pressure were observed among subjects treated with the Symplicity Spyral RDN system, including those from the treatment arm and the approximately three quarters of patients from the control arm that were later treated with Symplicity.”
At three years, patients who underwent RDN (N= 206) showed significantly greater reductions in both 24-hour ambulatory systolic blood pressure (ABPM) and officebased systolic blood pressure (OSBP) compared to sham patients (N= 131), despite similar medication burden.
Additionally, no renal artery stenosis greater than 70% was observed in the RDN group through three years.
SPYRAL HTN-ON MED is a global, randomised, sham-controlled trial investigating the blood pressure lowering effect and safety of RDN with the radiofrequency-based Symplicity RDN system in hypertensive patients who have been prescribed up to three anti-hypertensive medications.
First-in-human study of Cardiac Leaflet Enhancer reaches enrolment milestone
Nyra Medical has announced the initiation of its first-in-human clinical study evaluating its novel Cardiac Leaflet Enhancer (CARLEN) system in patients with functional (secondary) mitral regurgitation (FMR).
The study, focused on clinical safety and technical performance, has enrolled more than 10 patients, many with at least 30-day follow-up to date.
Nyra Medical’s proprietary transcatheter technology is designed to repair FMR by augmenting the native mitral valve. The CARLEN system is a single-leaflet implant designed to restore coaptation while preserving the valve’s natural motion and orifice area.
“We are entering a new era of transcatheter therapy where meaningful mitral repair is finally within reach. The data we’ve seen so far is compelling and gives us confidence to push forward thoughtfully but decisively,” said Azeem Latib (Montefiore Medical Center, New York, USA).
The ongoing first-in-human study is being conducted at international centers in the Republic of Georgia, Paraguay and Uzbekistan with enrolment expected to broaden over the coming months as additional patients are screened and treated. Insights gained from the early clinical experience will play a critical role in refining procedural workflows and device performance ahead of expanded clinical investigation.
The data will directly inform the
company’s global regulatory strategy, including engagement with the US Food and Drug Administration (FDA) and other regulatory bodies. The findings will shape the design of future clinical studies, including a potential early feasibility study and pivotal trial in the USA.
Pivotal trial of tricuspid annuloplasty system to commence following IDE approval
Micro Interventional Devices has announced US Food & Drug Administration (FDA) investigational device exemption (IDE) approval for its MIA-T annuloplasty system for the treatment of tricuspid annular disease.
The approval will enable the commencement of a pivotal clinical trial—STTAR-US—of at several US hospitals. The pivotal trial will assess annular treatment utilizing Micro Interventional Devices’ proprietary, polymeric PolyCor anchors developed specifically for use in cardiac tissue. The anchors are deployed into the tricuspid annulus via 12Fr delivery catheters. The technology is designed to treat functional tricuspid valve disease by reducing annular area, minimising tricuspid regurgitation (TR), and encouraging natural healing.
The STTAR-US steering committee is led by two principal investigators Bassem Chehab (University of Kansas, Wichita, USA) and Saibal Kar (Los Robles Regional Medical Center, Thousand Oaks, USA).
“This approval marks a critical milestone in the development of MIA-T. As one of the first percutaneous annular repair devices, we believe MIA-T will play a significant role in the emerging TTVR market,” said Michael Whitman, chief executive officer of Micro Interventional Devices.
Enrolment completed in CONFORM pivotal trial of LAAO system
Conformal Medical has announced the initiation of patient enrolment in the European Union (EU) for the CONFORM pivotal trial. The first EU procedure was successfully performed at the Institut Cardiovasculaire Paris Sud (ICPS) in Paris, France by Philippe Garot.
The CONFORM pivotal trial is evaluating the CLAAS AcuFORM LAAO device, a novel foam-based implant designed to provide a simplified, anatomy-conforming solution for stroke prevention in patients with non-valvular atrial fibrillation (AF).
“The CLAAS AcuFORM system represents an important innovation in LAAO, with the potential to simplify procedures, expand access, and improve outcomes for patients with non-valvular AF,” said Garot. “We are excited to participate in the CONFORM pivotal trial and to help bring this next-generation therapy to patients across Europe.”
The expansion of the CONFORM trial into the EU marks a significant
milestone for Conformal Medical, underscoring both the scalability of the study and the global opportunity for the CLAAS AcuFORM system, the company said in a press release. This phase of the trial is designed to generate robust real-world evidence, drive physician adoption, and lay a strong foundation for future commercialisation.
“Partnerships with leading European centres strengthen our global presence, accelerate innovation, and position us to deliver the benefits of our differentiated technology to patients worldwide,” said James Reinstein, president and chief executive officer of Conformal Medical. “We believe the CLAAS AcuFORM system will be a competitive offering, with its ability to conform to individual anatomies, simplify procedures with just two device sizes, and provide reliable seal confirmation.”
US FDA approves IDE for investigation of FLOWer embolic protection device
AorticLab has announced that the US Food and Drug Administration (FDA) has approved its investigational device exemption (IDE) for the FLOWer system pivotal clinical investigation.
The FLOWer system is a full-body embolic protection device designed for use during transcatheter intracardiac procedures such as transcatheter aortic valve implantation (TAVI). Since obtainment of the CE mark in Q1 2024, FLOWer has been successfully utilised in very complex procedures, in several EU countries, AorticLab said in a press release.
The IDE approval allows the commencement of a clinical investigation at US centres including Montefiore Medical Center in New York, with the study evaluating procedural safety, device efficacy, and early clinical outcomes.
“FDA approval of the FLOWer IDE marks a major milestone for AorticLab, with the aim of providing US patients a safe and effective device to improve outcome of structural heart interventions,” said Franco Osta, chief executive officer of AorticLab.
Enrico Pasquino, chief scientific officer of AorticLab, added: “The FLOWer system was designed with TAVI procedural integration, full embolic protection and patient safety in mind. This US pivotal clinical investigation will provide critical evidence to address the unmet need for total embolic protection, especially in patients at higher risk of stroke during cardiology interventions.”
FLOWer
Bashir endovascular catheter
Industry News
SpectraWAVE appoints Jonathan Hill as chief medical officer SpectraWAVE has announced the appointment of Jonathan Hill as chief medical officer.
Hill, an interventional cardiologist from Royal Brompton Hospital in London (UK), brings expertise in coronary artery disease, complex percutaneous coronary intervention (PCI), intravascular imaging, physiology, cardiovascular innovation, and clinical study design and implementation, the company says in a press release.
“Jonathan is a highly respected clinician and innovator whose leadership will be critical as SpectraWAVE accelerates commercial adoption and advances its clinical evidence strategy both in the USA and worldwide for our expanding product portfolio,” said Eman Namati, chief executive officer of SpectraWAVE. “His experience integrating intravascular imaging and physiology into daily clinical practice and being at the front lines of medicine with multiple major worldwide clinical studies will strengthen our partnerships with physicians, research groups, and support our commitment to improving outcomes for coronary artery disease patients.”
The announcement comes as SpectraWAVE surpasses thousands of commercial HyperVue imaging system cases in cath labs across the USA and achieves multiple clinical study milestones, the press release adds.
Shruthi Narayan appointed president of Penumbra Penumbra has announced the promotion of Shruthi Narayan to president of the company, effective 1 September 2025.
A company press release states she will continue to report to Adam Elsesser, who served in the role of president prior to this promotion and will continue in his role as both chairman of the board and chief executive officer of Penumbra.
“Shruthi is a dynamic, seasoned leader whose passion for innovation and proven ability to inspire global teams make her the obvious choice for this critical role,” said Elsesser. “Her vision and focus on excellence will undoubtedly help sustain Penumbra’s exceptional growth and market leadership, expanding access to our life-saving technology to patients around the world.”
“I am honoured to join SpectraWAVE at such a pivotal time,” said Hill. “The company’s approach to combining intravascular imaging and physiology in a comprehensive and easy-to-use form factor is going to transform decision-making in the cath lab. I look forward to collaborating with the incredible team and the global clinical community as we expand the impact of HyperVue and introduce new technologies and clinical indications beyond intravascular imaging.”
Conference calendar
28–30 January
British Cardiovascular Intervention Society (BCIS) Advanced Cardiovascular Intervention (ACI) London, UK milbrook-events.co.uk
29 January–1 February Society of Thoracic Surgeons (STS) annual meeting New Orleans, USA sts.org
Cardiac Dimensions appoints William T Abraham as chief medical officer
Cardiac Dimensions has announced the appointment of William T Abraham as chief medical officer.
Abraham will help lead the company’s clinical and regulatory strategies as it advances toward US regulatory approval and continues to expand European commercial sales of the Carillon mitral contour system.
Abraham most recently served as the chief medical officer at V-Wave, where he led the US pivotal trial and played a key role in advancing the company’s transcatheter interatrial shunt therapy, culminating in a significant heart failure-focused acquisition by Johnson & Johnson.
CORE-MD consortium announces recommendations on clinical assessment of high-risk medical devices
The CORE-MD—Coordinating Research and Evidence for highrisk Medical Devices—consortium has published new consensus recommendations in The Lancet Regional Health Europe, setting out scientifically robust methodologies for clinical investigations of high-risk medical devices.
The recommendation have been issued in direct respond to a request from the European Commission to provide expert advice on trial design, addressing what is described as a longstanding gap in guidance for the evaluation of high-risk technologies such as cardiovascular implants, orthopaedic devices, and systems for managing diabetes.
A 20-year veteran in the medical device industry, Narayan was most recently president of Penumbra’s interventional business, where she led the day-to-day operations, and oversaw the growth initiatives of both the company’s neuro and vascular franchises. She joined Penumbra in 2013 as a product manager, starting off on the stroke franchise before transitioning to help build the peripheral vascular division, commercialising Penumbra’s vascular portfolio of embolisation and thrombectomy products globally. Narayan began her medical device career at Medtronic in 2006, working in engineering, regulatory affairs and the cardiovascular sales organisation.
“Penumbra has been at the forefront of blood clot care for more than 20 years, advancing the most innovative technologies to address conditions from head-to-toe like stroke and pulmonary embolism,” said Narayan. “I am honoured to carry on and expand our legacy of innovation, and look forward to continuing this paradigm shift in patient care.”
4–6 February JIM GISE Rome, Italy jimgise2026.it
5–6 February Controversies & Advances in the Treatment of Cardiovascular Disease Beverly Hills, USA promedicacme.com/controversies
“We are delighted to welcome Dr Abraham to the Cardiac Dimensions leadership team,” said Rick Wypych, president and chief executive officer of Cardiac Dimensions. “Bill’s impact on the heart failure field is unmatched. His input and influence on the Carillon therapy will help drive the success and adoption of this much-needed therapy. In addition, his experience with large-scale clinical trials and regulatory pathways will be instrumental to the completion of our pivotal US landmark study—The EMPOWER trial.”
Unlike medicines, which are required to demonstrate safety and efficacy before market entry, high-risk medical devices in Europe are required to provide only “sufficient clinical evidence”—a standard that is not defined in detail.
The CORE-MD analyses confirm that many devices have entered the market without robust evidence from randomised trials, often with little data in the public domain.
“I’ve spent my career working to bring novel and impactful therapies to people living with heart failure,” said Abraham. “What drew me to Cardiac Dimensions is the Carillon therapy’s unique position in the heart failure treatment paradigm. It offers a physiologically elegant approach to reducing mitral regurgitation, preserving future treatment options, and modifying the disease process itself. I’m particularly encouraged by the consistent data showing favourable atrial and ventricular remodelling, symptom improvement, and an excellent safety profile—even in patients with proportionate mitral regurgitation who are often excluded from other therapies.”
The Carillon mitral contour system has received CE mark and is available for sale in Europe.
2–4 March Technology and Heart Failure Therapeutics (THT) Boston, USA thtmeeting.com
5–7 March
The Houston Aortic Symposium Houston, USA promedicacme.com/houston-aortic
8–11 March Cardiovascular Research Technologies (CRT) Washington, DC, USA crtmeeting.org
28–30 March American College of Cardiology (ACC) scientific session New Orleans, USA expo.acc.org
Key recommendations from the CORE-MD consortium include a four-stage framework for clinical investigations, from initial studies through to long-term follow-up; greater use of randomised controlled trials, including sham-controlled trials with appropriate ethical safeguards; efficient large-scale trials embedded in registries to accelerate evidence generation; mandatory transparency of study design, protocols, and results; and, tailored approaches for breakthrough or orphan devices, requiring post-market confirmatory studies.
The CORE-MD consortium—funded by the EU Horizon 2020 programme, and led by the European Society of Cardiology (ESC) with the Federation of National Societies of Orthopaedics and Traumatology (EFORT)—brought together 100 leading academic trialists, clinicians, regulators, patients, and health technology assessment experts across Europe.
21– 23 April
Charing Cross (CX) Symposium London, UK cxsymposium.com
19–22 May EuroPCR 2026 Paris, France course.pcronline.com