2 Guest editorial Senior surgeons: Options beyond the operating room
12 Comment Fedor Lurie, MD, ponders appropriate outcome measures for deep reflux as new valve tech emerges
14 CLTI New BEST-CLI costeffectiveness data drop
18 Clinical trials Recent study probes ‘significant’ gap between randomized and real-world data
www.vascularspecialistonline.com
$ VAM2025
Helping OBL vascular surgeons fight the squeeze
SVS Section on Ambulatory Vascular Care (SAVC) set to announce set of new initiatives designed to help office-based lab (OBL) vascular surgeons combat rising costs and stagnant payments during jampacked session focused on the outpatient setting at the 2025 Vascular Annual Meeting (VAM) in New Orleans (June 4–7).
By Bryan Kay
The way Anil Hingorani, MD, sees it, vascular surgeons operating in the OBL outpatient setting are feeling the pinch amid an unforgiving economic climate. With the omnipresent threat of Medicare cuts, stagnant or decreasing payments, and escalating inflationary pressure, they are hurting, the SAVC chair explains. Many private-practice specialists behind OBLs are choosing to shutter their practices. Others with the means are converting their facilities into the OBL’s outpatient cousin, ambulatory surgery centers (ASCs).
For many vascular surgeons in this OBL, the personal costs run high, Hingorani, a vascular surgeon in Brooklyn, New York, details. “This is putting a lot of stress on private practitioners who have invested very
SVS Vice President Linda Harris, MD, extolled the values of “coelevation” in her presidential address at the 7th annual Women’s Vascular Summit (May 2–3), invoking lessons on teamwork from the world of sport to argue that a united vascular specialty is greater than the sum of its parts.
HARRIS, PROFESSOR OF surgery and past chief of vascular surgery at the University at Buffalo in Buffalo, New York, addressed the summit as its founder and first outgoing president.
“Dr. Linda Harris has established her legacy as a trailblazer in vascular surgery on all fronts,” said incoming president Palma Shaw, MD, as she introduced Harris at the Chicago gathering.
Harris’ address centered on uniting those involved in vascular care across lines of geography, sex, race and specialty. “We have to talk together, and we have to walk together,” she opined, “otherwise we will not succeed, and that goes for working with our friends across the pond, men and women, Black and white, private practice and academic, vein and artery,” emphasizing also the importance of collaborating with interventional radiology and cardiology colleagues.
Focusing on the summit and its associated International Society for Women Vascular Surgeons (ISWVS)—which Harris founded in 2023 to promote education about vascular disease in women and promote women in the vascular field—the presenter paid homage to the team around her, in particular Shaw, Kathleen Ozsvath, MD, Kellie Brown, MD, and Joann Lohr, MD.
Harris stressed that a strong,
See page 6
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | John F. Eidt, MD | Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD | James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS | Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Saranya Sundaram, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Senior Director for Public Affairs and Advocacy
Megan Marcinko, MPS
Communications Specialist
Marlén Gomez
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Managing Editor/Head of U.S.
Operations Bryan Kay bryan@bibamedical.com
Editorial contribution Jocelyn Hudson, Will Date, Jamie Bell and Éva Malpass
Design Josh Lyon and Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe
526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America
155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA News. Content for the news from SVS is provided by the Society for Vascular Surgery. | The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA News will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein. | The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. |
RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com | For missing issue claims, e-mail subscriptions@bibamedical. com. | Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA News. | Printed by Ironmark |
Senior vascular surgeons: 10 options beyond the operating room
By Kenneth Ouriel, MD, Daniel Clair, MD, Alan Dietzek, MD, and Enrico Ascher, MD
As vascular surgeons advance in their careers, many begin to consider alternative professional paths that draw upon their clinical expertise, while offering greater flexibility, intellectual stimulation or new challenges outside the traditional confines of full-time clinical practice. Whether motivated by physical demands, shifting professional interests or a desire to contribute in new ways, seasoned vascular surgeons have a wide array of fulfilling and impactful options. These career directions are open to those from clinical, academic or hybrid backgrounds.
1. Clinical research and leadership in clinical research organizations
Experienced vascular surgeons often move into roles centered on clinical research. Their procedural knowledge and understanding of patient care position them well to serve as principal investigators or advisors within clinical research organizations (CROs) or their academic-based counterparts, academic research organizations (AROs). Responsibilities in these roles span protocol development, site selection, safety endpoint adjudications, evaluation of study outcome data, review of core laboratory images, and assisting with the overall operational aspects of the clinical trial.
In AROs and CROs, surgeons can advise on regulatory and scientific strategies for clinical studies and can ensure that trials measure outcomes and endpoints that truly matter to patients and clinicians. Awareness of clinical workflows enables the identification of practical challenges a priori, helping to develop realistic, relevant study designs that avoid impediments to efficient enrollment and adequate patient follow-up. These positions are frequently structured for parttime or hybrid work and may be performed remotely.
2. Part-time or locum tenens practices
In later years, a surgeon may wish to continue clinical practice, but at a slower pace or with reduced call commitments. This may be accomplished by moving to a remote hospital setting affiliated with a larger healthcare system. With the shortage of vascular surgeons expected to worsen over the next decade, this option offers community and physician benefits. Many practices would welcome even part-time coverage or assistance. Further, there may be opportunities to assist in the outpatient setting in a larger practice or to see patients in an outreach clinic. Sharing a practice with either another senior peer or, alternatively, a younger surgeon who may have significant out-of-hospital personal commitments may satisfy a desire for both individuals to stay clinically active at a desirable, individualized pace. Sometimes these arrangements can be done with periodic travel so that the senior surgeon can maintain their current residence.
3.
Transition to non-operative practice
As senior vascular surgeons contemplate transitioning to retirement, they may consider alternatives short of completely
leaving their practice. One such alternative is to shift to a solely office-based, non-operative practice. This approach is less technically and physically challenging and can be done on either a full- or part-time basis. An office-based practice allows senior vascular surgeons to continue to be involved with patient care, utilizing their vast experience and wisdom to evaluate and nonoperatively manage patients. By referring patients who require interventions or open surgical procedures to practice associates, senior vascular surgeons can increase the overall efficiency of the practice and enhance physician satisfaction. Additionally, performing office-based minimally invasive procedures—for instance, venous procedures or wound care—can bring personal fulfillment while providing a continued source of income.
4. Academic teaching and mentorship
Education remains a natural extension for many vascular surgeons. For some, teaching residents and fellows was always a part of their responsibilities. As clinical responsibilities diminish, there’s an opportunity to expand this role. Senior surgeons may take on responsibilities as clinical faculty, giving student and resident lectures, bedside teaching on patient rounds, and participating in simulation training. Some academic institutions are open to part-time faculty appointments, making this an attractive option for surgeons to ease into semi-retirement. In some academic systems, senior surgeons can act as mentors or coaches for junior faculty to help guide younger surgeons’ academic, teaching or clinical careers. In addition, as junior surgeons may struggle with entering clinical practice, having a senior surgeon to assist with complex operations may be a role that provides professional fulfillment for a senior surgeon, and real value to the more junior surgeon and the healthcare organization.
Separate from face-to-face interactions, teaching can also take the form of medical writing and engaging in contributions to literature in the form of white papers, original research articles or chapters in textbooks.
5. Board and advisory services in healthcare organizations
Vascular surgeons increasingly contribute to governance roles on hospital boards, nonprofit foundations, health systems and professional societies. Their clinical insight can offer invaluable perspective to discussions on quality improvement, strategic direction and innovation. These roles often involve participation on quality or finance committees, or advisory input on clinical initiatives. Structured as part-time commitments, these roles can provide meaningful engagement without the demands of full-time clinical practice. Working for non-healthcare nonprofit organizations or local community organizations can be equally rewarding.
Surgeons can also serve roles in larger healthcare systems
As junior surgeons may struggle with entering clinical practice, having a senior surgeon to assist with complex operations may be a role that provides professional fulfillment
continued on page 5
From top: Kenneth Ouriel, Daniel Clair, Alan Dietzek, and Enrico Ascher
*All: drug, scaffold, resorbable excluding platinum markers. 1. Reintervention defined as CD-TLR. 2. Brian G. DeRubertis et al., Two-Year Outcomes of the LIFE-BTK Randomized Controlled Trial Evaluating the Esprit™ BTK Drug-eluting Resorbable Scaffold for Treatment of Infrapopliteal Lesions, VIVA 2024.
INDICATIONS The Esprit™ BTK Everolimus Eluting Resorbable Scaffold System is indicated for improving luminal diameter in infrapopliteal lesions in patients with chronic limb-threatening ischemia (CLTI) and total scaffolding length up to 170 mm with a reference vessel diameter of ≥ 2.5 mm and ≤ 4.00 mm.
Esprit™ BTK Everolimus Eluting Resorbable Scaffold System
INDICATIONS
The Esprit™ BTK Everolimus Eluting Resorbable Scaffold System is indicated for improving luminal diameter in infrapopliteal lesions in patients with chronic limb-threatening ischemia (CLTI) and total scaffolding length up to 170 mm with a reference vessel diameter of ≥ 2.5 mm and ≤ 4.00 mm.
CONTRAINDICATIONS
The Esprit™ BTK Everolimus Eluting Resorbable Scaffold System is contraindicated for use in:
• Patients who cannot tolerate, including allergy or hypersensitivity to, procedural anticoagulation or the post-procedural antiplatelet regimen.
• Patients with hypersensitivity or contraindication to everolimus or structurally related compounds or known hypersensitivity to scaffold components poly(L-lactide), poly(D, L-lactide), and platinum.
WARNINGS
• This device is intended for single use only. Do not reuse, reprocess, or re-sterilize. Note the product “Use-by” date on the package. Reuse, reprocessing, or re-sterilization may compromise the structural integrity of the device and / or delivery system and / or lead to device failure, which may result in patient injury, illness, or death. Reuse, reprocessing, or resterilization may also create a risk of contamination of the device and / or cause patient infection or cross-infection, including, but not limited to, the transmission of infectious disease(s) from one patient to another. Contamination of the device and / or delivery system may lead to injury, illness, or death of the patient.
• The Esprit™ BTK System is intended to perform as a system. The scaffold should not be removed for use with other dilatation catheters.
• The Esprit™ BTK System should not be used in conjunction with other non-everolimus drug eluting devices in the same vessel as the Esprit™ BTK Scaffold.
• It is not recommended to use this scaffold to treat lesions located at any joint or other hinge points, such as the knee or ankle. The recommended region for below-the-knee (BTK) treatment with the Esprit™ BTK Scaffold is the infrapopliteal arteries at a location ≥ 10 cm above the proximal margin of the ankle mortise. The Esprit™ BTK Scaffold has not been tested for use outside the recommended implant locations.
• This product should not be used in patients with aneurysms immediately adjacent to the scaffold implantation site.
• Insertion of the Esprit™ BTK System and implantation of the scaffold should be performed only under fluoroscopic observation with radiographic equipment providing high resolution images.
• Quantitative imaging is strongly recommended to accurately measure and confirm appropriate vessel sizing (reference vessel diameter ≥ 2.5 mm). If quantitative imaging determines a vessel size < 2.5 mm, do not implant the Esprit™ BTK Scaffold.
• Adequate lesion preparation prior to scaffold implantation is required to ensure safe delivery of the scaffold across the target lesion. It is not recommended to treat patients having a lesion that prevents complete inflation of an angioplasty balloon.
• Successful pre-dilatation with residual diameter stenosis of < 30% by visual estimation is required for treatment of the target lesion; < 20% by visual estimation is preferred.
• Ensure the scaffold is not post-dilated beyond the allowable expansion limits.
• Use of appropriate anticoagulant and / or antiplatelet therapy per standard of care is recommended for use of this scaffold system.
• This product should not be used in patients who are not likely to comply with the recommended antiplatelet therapy.
• Judicious selection of patients is necessary, since the use of this device carries the associated risk of
scaffold thrombosis, vascular complications, and / or bleeding events.
PRECAUTIONS
• Scaffold placement should not be performed in patients with known allergies to contrast agent that cannot be medically managed.
• It is not recommended to treat patients having a lesion with excessive tortuosity proximal to or within the lesion.
• When multiple scaffolds are required, only combinations of Esprit™ BTK Scaffolds must be used. Any potential interaction with other drugeluting or coated devices has not been evaluated.
• The delivery system is intended for deployment of the scaffold only and should not be used to dilate other locations.
• I mplantation of the scaffold should be performed only by physicians who have received appropriate training.
• A s with all catheter-based procedures, scaffold placement should be performed at facilities where patient can be prepared for necessary intervention and / or surgical removal of the device and vessel repair as per facility protocol.
• P re-dilatation should be performed with an angioplasty balloon. Cutting or scoring balloons can be used per physician discretion, if the lesion appears to be mildly calcified.
• Failure to pre-dilate the vessel may impair nominal / optimal scaffold delivery.
• I mplanting a scaffold may lead to dissection of the vessel distal and / or proximal to the scaffold, requiring additional intervention.
Note: In cases of bailouts, bailout treatment of the target lesion can be done using the Esprit™ BTK Scaffold of the appropriate length. If an appropriate length Esprit™ BTK Scaffold is not available, physicians should use standard of care.
• A n unexpanded scaffold may be retracted into the introducer sheath one time only. An unexpanded scaffold should not be reintroduced into the artery once it has been pulled back into the introducer sheath.
• Post-dilatation is strongly recommended for optimal scaffold apposition. When performed, postdilatation should be performed at high pressure (> 16 atm) with a non-compliant balloon up to 0.5 mm larger than the nominal scaffold diameter.
• Use an appropriately sized non-drug coated balloon to pre-dilate the lesion. When treating a long lesion, scaffold the distal portion of the lesion prior to scaffolding the proximal portion of the lesion.
• Ensure that the scaffolded area covers the entire lesion / dissection site and that no gaps exist between scaffolds.
• The extent of the patient’s exposure to drug and polymer is directly related to the number of scaffolds implanted. The safety of everolimus, polymer, and polymer breakdown products was evaluated in preclinical studies and the biocompatibility assessment of the Esprit™ BTK Scaffold.
• The safety and effectiveness of the Esprit™ BTK Scaffold in patients with prior brachytherapy of the target lesion or the use of brachytherapy for treatedsite restenosis in the Esprit™ BTK Scaffold have not been established. Both vascular brachytherapy and the Esprit™ BTK Scaffold alter arterial modeling. The potential combined effect on arterial remodeling by these two treatments is not known.
• The safety and effectiveness of the Esprit™ BTK System have not been established in clinical trials with the use of either mechanical atherectomy devices (directional atherectomy catheters, rotational atherectomy catheters) or laser atherectomy catheters.
• Formal drug interaction studies have not been performed with the Esprit™ BTK Scaffold because of limited exposure to everolimus eluted from the scaffold.
• Everolimus, the Esprit™ BTK Scaffold’s active pharmaceutical ingredient, is an immunosuppressive agent. Therefore, consideration should be given to patients taking other immunosuppressive agents or who are at risk for immune suppression.
• Oral everolimus use in renal transplant and advanced renal cell carcinoma patients was associated with increased serum cholesterol and triglyceride levels, which in some cases required treatment.
• Non-clinical testing has demonstrated the Esprit™ BTK Scaffold is MR Conditional. A person with the Esprit™ BTK Scaffold may be safely scanned under the following conditions. Failure to follow these conditions may result in injury.
• Static magnetic field strength of 7 Tesla or less
• The Esprit™ BTK Scaffold should not migrate in this MRI environment. MRI at 7 Tesla or less may be performed immediately following the implantation of the Esprit™ BTK Scaffold.
POTENTIAL ADVERSE EVENTS
Potential adverse events include, but are not limited to:
Allergic reaction or hypersensitivity to contrast agent, anesthesia, scaffold materials (poly[L-lactide] [PLLA], poly[D, L-lactide] [PDLLA], platinum, or everolimus), and drug reactions to anticoagulation or antiplatelet drugs
• Vascular access complications which may require transfusion or vessel repair, including:
CAUTION: This product is intended for use by or under the direction of a physician. Prior to use, reference the Instructions for Use, inside the product carton (when available) or at manuals.eifu.abbott for more detailed information on Indications, Contraindications, Warnings, Precautions and Adverse Events. This material is intended for use with healthcare professionals only.
Illustrations are artist’s representations only and should not be considered as engineering drawings or photographs. Photo on file at Abbott.
Information contained herein for DISTRIBUTION in the U.S. ONLY.
Abbott
3200 Lakeside Dr., Santa Clara, CA 95054 USA, Tel: 1.800.227.9902
™ Indicates a trademark of the Abbott Group of Companies. www.cardiovascular.abbott
The risks described below include the anticipated adverse events referenced in the contraindications, warnings, and precautions sections of the everolimus labels / SmPCs and / or observed at incidences ≥ 10% in clinical trials with oral everolimus for different indications. Refer to the drug SmPCs and labels for more detailed information and less frequent adverse events.
• A bdominal pain
• A nemia
• A ngioedema (increased risk with concomitant angiotensin-converting enzyme [ACE] inhibitor use)
• A rterial thrombotic events
• Bleeding and coagulopathy (including hemolytic uremic syndrome [HUS], thrombotic thrombocytopenic purpura [TTP], and thrombotic microangiopathy; increased risk with concomitant cyclosporine use)
• Constipation
• Cough
• Diabetes mellitus
• Diarrhea
• D yspnea
• Embryo-fetal toxicity
• Erythema
• Erythroderma
• Headache
• Hepatic artery thrombosis (HAT)
• Hepatic disorders (including hepatitis and jaundice)
• Hypersensitivity to everolimus active substance, or to other rapamycin derivates
• Hypertension
• I nfections (bacterial, viral, fungal, or protozoan infections, including infections with opportunistic pathogens). Polyoma virus-associated nephropathy (PVAN), JC virus-associated progressive multiple leukoencephalopathy (PML), fatal infections and sepsis have been reported in patients treated with oral everolimus.
• K idney arterial and venous thrombosis
• Laboratory test alterations (elevations of serum creatinine, proteinuria, hypokalemia, hyperkalemia; hyperglycemia, dyslipidemia including hypercholesterolemia and hypertriglyceridemia; abnormal liver function tests; decreases in hemoglobin, lymphocytes, neutrophils, and platelets)
• Lymphoma and skin cancer
• Male infertility
• Menstrual irregularities
• Nausea
• Nephrotoxicity (in combination with cyclosporine)
• Wound healing complications (including wound infections and lymphocele)
There may be other potential adverse events that are unforeseen at this time.
FROM THE COVER HELPING OBL VASCULAR SURGEONS FIGHT THE SQUEEZE
continued from page 1
heavily in OBLs—personal investment quite a bit of the time—and they are often personally liable,” he says.
So, the SVS and its section dedicated to the issues facing outpatient practices are taking action through a series of new initiatives aimed at helping OBLs cut costs. The exact details of the SVS plans are set to unveiled toward the end of the pair of back-to-back SAVC sessions taking place at VAM 2025 on Friday, June 6 (2–5 p.m.) in the Morial Convention Center host venue (Second Floor, Room 224).
“Without revealing too much ahead of time, these SVS initiatives are about cost-savings for OBLs amid the cuts, and I think these will be especially important for the smaller practices, because those are the ones that are being hurt the most,” says Hingorani, who will be one of the moderators of the SAVC sessions. “They are the ones that I think we can help the most. We’ve done some preliminary work on this already, and I would say is going to be a key component, for one-, two- or three-practitioner practices. And, these don’t have to be just vascular-surgeon-only practices; they can be multispecialty groups as well.”
The economic headwinds impacting on OBL surgeons and driving the SVS and SAVC to action are stark, Hingorani explains. “Some of the transition going on is being dictated by
CMS [the Centers for Medicare & Medicaid Services]. Some of it is because the RVU [relative value unit] conversion rate has not increased for 30 years, and inflation has clearly been going up over the last couple of years,” he continues. “So, if you’re in the OBL, you’re getting it from both ends. If your costs are increasing and your payments are the same—or decreased in some parts of the OBL—that’s a squeeze financially. That’s one of the reasons why these OBLs are being converted into ASCs. That also takes considerable investment. A lot of reasons why places open as OBLs is that ASCs are expensive, have much higher regulation and require a lot more investment, so it is a higher-stakes game to convert a pre-existing OBL to an ASC. Hopefully some of these new SVS initiatives will make a significant impact.”
The SAVC sessions at VAM 2025 feature the spectrum of issues related to practice in OBLs and ASCs.
Highlights include a couple of talks that focus on artificial intelligence (AI) use in ambulatory centers. Uwe Fischer, MD, an assistant professor of surgery at Yale School of Medicine in New Haven, Connecticut, is bringing expertise on AI’s use to improve vascular diagnostics and treatment outcomes, while Alisha Oropallo, MD, a professor of surgery at Hofstra University/Northwell in Lake Success, New York, will offer insight on how AI chatbots might improve chronic vascular
by providing guidance and oversight for specialty care at regional practices where they exist. There are also often roles for individuals to oversee pricing and product standardization across a healthcare system. In addition, surgeons have long considered the electronic medical record (EMR) as a barrier to patient care efficiencies. Leveraging clinical experience to enhance the EMR can be a service well appreciated by all stakeholders in the system.
6. Medical director positions in startup medical device and biotechnology companies
Some vascular surgeons move into entrepreneurship—founding companies or advising early-stage ventures. Many earlystage companies seek part-time medical directors with firsthand clinical experience. Vascular surgeons are especially valued in companies developing endovascular tools, imaging platforms or artificial intelligence (AI)-enabled solutions. These engagements may be structured as short-term projects or long-term relationships, and often align well with surgeons who enjoy innovation, collaboration and problem-solving. These positions are often remote, involve minimal travel and offer compensation through consulting fees, equity, or both. Surgeons in these roles influence clinical trial design, user interface development and postmarket strategies. They also often contribute to fundraising pitches, serve as key opinion leaders, and guide regulatory or reimbursement planning.
7. Executive medical leadership
at
large medtech companies
Some surgeons take on full-time leadership roles within major medtech firms—such as divisional chief medical officers or medical affairs directors. Responsibilities may include global trial oversight, regulatory engagement, physician education and management of key opinion leader networks. These positions require strong communication skills and the ability to collaborate across clinical, engineering and commercial functions. In some roles, surgeons may assist in the management of clinical studies, or guide direction outside of their primary specialty, working with physicians across specialties and procedures. Though demanding, these roles allow surgeons to influence device strategy and patient care. Surgeons in these roles often serve as a critical link between practicing clinicians and corporate leadership, ensuring that innovation remains clinically grounded.
8. Regulatory service with the FDA
An often-unrecognized path is service within the Food and Drug Administration (FDA), either on a full- or part-time basis. The Center for Devices and Radiological Health (CDRH) routinely recruits physicians with domain-specific expertise to review premarket submissions, participate on advisory committees (panels), and guide the design of
wound management outcomes in OBLs and ASCs. Much of the work presented comes from SAVC research and seed grants, and recaps prior years as well as points ahead to new work coming up. Meanwhile, the annual Excellence in Community Practice Awards will again take place toward the end of the SAVC program, Hingorani notes.
SAVC’s focus on research in this arena seeks to fill a void, the section chair points out. “The reason why we are trying to open up this space for research is because there really has not been a lot in the OBL or ASC space,” he says. “I think part of that has been financial directives of the field and trying to stay afloat but also support.
“Part of the reason why we have this session is to give a platform for people to present heir work, but also for the seed grants. Specifically, this is to give support to hire statisticians, get a database, or to help input the data, analyze the data, present the data—to help the process of actually getting your research out. If we say that more than 50% of lower extremity angioplasties are performed in the outpatient space, where are the data? We have the numbers. But where are the results, what are the challenges, what are the opportunities, what are the changes that take place when you start doing these procedures as an inpatient and then transfer them to an outpatient?”
continued from page 2
postmarket surveillance study design. Vascular surgeons bring a unique ability to critically evaluate clinical evidence while understanding device function in real-world practice. Opportunities at the FDA include full-time roles or work as special government employees (SGEs) on a consulting basis.
9.
Legal consulting and expert witness services
Legal consulting is another avenue that allows surgeons to remain intellectually engaged while working flexibly. Vascular surgeons may offer litigation support, conduct case reviews, or testify in malpractice or patent-related legal matters. Since this work mandates maintenance of at least part-time clinical activities, it is a nice option for surgeons interested in a transition out of full-time practice. These roles appeal to those who enjoy applying clinical knowledge in high-stakes analytical contexts and can be pursued independently or through legal advisory networks. However, the choice of working exclusively for plaintiffs or defendants can sometimes create personal or ethical conflicts. Attorneys may exploit such decisions by questioning a surgeon’s impartiality before a jury, underscoring the importance of consistency, transparency and preparation in this line of work.
10.
Insurance adjudication and utilization review
Another growing area of opportunity for senior vascular surgeons is in the insurance
and healthcare payor sector. In these roles, surgeons participate in the adjudication of claims and conduct utilization reviews to assess the appropriateness and necessity of vascular procedures and hospital stays. With their deep clinical experience, surgeons can evaluate the medical justification for treatments and ensure alignment with evidence-based guidelines. These positions can be structured on a part-time or consulting basis and are almost always performed remotely.
Conclusion: Designing a fulfilling late career
Vascular surgeons are not confined to a binary choice between clinical practice and full retirement. The options outlined here are not the only choices available, and the choices one has to transition a career are continuing to expand. An increasing range of meaningful, intellectually rich, and flexible roles are available for those who wish to remain active contributors in the field.
It is also important to recognize that a senior surgeon need not be limited to a single, ultimate career transition choice.
KENNETH OURIEL is executive vice president of medical device contract research organization NAMSA in New York; DANIEL CLAIR is chair and professor of vascular surgery at Vanderbilt University Medical Center in Nashville; ALAN DIETZEK is chair of vascular surgery at Jersey Shore University Medical Center in Neptune, New Jersey; and ENRICO ASCHER is a clinical professor of surgery at New York University.
PEDIATRICS
Taking the lead: The vascular surgeon in the pediatric vascular surgical space
By Bryan Kay
IT’S A BIT LIKE REALIGNING THE NARRATIVE, EVER so slightly. “I want us to feel, as a collective specialty, that pediatric vascular care falls under our purview,” says Dawn Coleman, MD, a leading voice in the vascular surgical care of pediatric patients, as she emphasizes an emerging need for her vascular surgeon colleagues to own their role in the space. Or, put another way: when vascular surgeons look at colleagues like Coleman who are deeply entrenched in the care of pediatric patients with vascular pathologies, the message is: don’t overlook or diminish the role vascular surgeons can play in the care of these patients.
Vascular and pediatric surgical collaboration has been the emblem of efforts in recent years to optimize the multidisciplinary approach to pediatric vascular care. But for a flagship session at VAM this year, organized by the SVS Pediatric Vascular Surgery Interest Group, that collaboration is momentarily giving way to a laser focus on vascular surgery’s
pivotal role. “This year, we are being quite intentional, urging and empowering our peers to realize, as vascular surgeons, the critical role we play in this space, even those who may not be super comfortable caring for these kids independently,” Coleman, chief of vascular surgery at Duke University in Durham, North Carolina. “In the past, we have been intentionally inclusive of our APSA [American Pediatric Surgical Association] partners in these sessions. This year, while not intending to be exclusive of our partners, the omission of our pediatric surgical colleagues and the focus on vascular surgeons aims to emphasize our professional accountability to this patient demographic. We believe that our invited speakers will help our members realize their value in this space, as surgeons and multidisciplinary collaborators, and be inspired not just to engage in the care of these children, but to be leaders in that care.”
need us also, and that we add value. For example, if you are going to have a level 1 pediatric trauma center, you must have the capability of vascular surgeons to support that. If you’re going to have a major pediatric surgical oncology program, you must have capability for vascular reconstruction.”
The intentionality of this session—taking place Friday, June 6 (2–3:30 p.m.), on the Morial Convention Center host venue’s Second Floor (Room 217-219)—is captured in the title: The Critical Role of Vascular Surgeons in the Children’s Hospital. Zoom out from the vascular workforce operating in pediatric care to the vascular surgery workforce at large, and a similar picture of some of the specialty’s existential concerns—declining population of surgeons, valuation in hospital systems, public branding and visibility—begin to form. “As our workforce continues to feel incremental patient volume, complexity and burden of operational inefficiencies, more than ever our hospitals need us,” explains Coleman. “The SVS is committed to helping comprehensive entities appreciate how much value we bring to an institution. We want to emphasize, with this session, that pediatric hospitals
FROM THE COVER ‘RISE TOGETHER’: HARRIS URGES UNITY IN WOMEN’S VASCULAR SUMMIT PRESIDENTIAL ADDRESS
continued from page 1
unified team was central not only to the creation of the summit and ISWVS, but will also be key to their longevity. “I don’t ever want an organization or something I create to be at the best when I create it or when I’m leading,” she said. “I want it to be the best it’s been to that date, but I want it to be better when my successors come along, because otherwise I’m not succeeding.”
To ensure unity within a team, Harris proposed the concept of “co-elevation.” She explained: “Leaning on someone does not mean you’re weak. It means you recognize your areas of weakness, and you complement them with someone else’s strengths, and they do the same for you and you rise together.”
company work, and a civilization work.”
“Other sports legends have echoed the same thing,” the presenter continued, noting that blue chip basketball player Michael Jordan has previously said that “talent wins games, but teamwork and intelligence is what wins championships.”
“We will not succeed if we leave people behind,” Harris continued. “We need to encourage deliberate, intentional inclusivity and encourage people to learn their unconscious biases.”
To support her argument, Harris shared lessons to be learned from the world of sport about sacrificing personal gain for the greater good of group success. In the first of several sporting references, Harris shared the words of football coach Vince Lombardi: “Individual commitment to a group effort is what makes a team work, a
Harris used another basketball reference to demonstrate how individual ambition can lead to a divided, unsuccessful team.
Referencing Los Angeles Lakers teammates Kobe Bryant and Shaquille O’Neal, She stated: “When they were put together, the team actually did worse because they were both ‘the guy who had to be the guy,’ and they weren’t willing to work in a united fashion. They had to be the superstar.”
Caveating her argument for unity, Harris was keen to stress that this should not be confused with uniformity, urging the audience to avoid “groupthink.” Instead, the presenter encouraged discussion of differing viewpoints as a core tenet of any successful team.
‘Listen to each other’
Speaking to Vascular Specialist following her summit address, Harris homes in on the ways in which teams can unify. “I think the simplest thing that we need to do is
The coming together of the SVS and APSA was intentional too. Coleman is a co-chair alongside John White, MD—who will also co-moderate the VAM session—on the SVS side of a joint taskforce with APSA to tackle pediatric vascular surgery issues. As the ability to extend the lives of children improves and population health threats continue to rise, says Coleman, the incidence and nature of pediatric vascular problems is ever increasing in frequency and complexity. The taskforce continues to pursue meaningful interventions to advance the understanding and care of these low-volume but critical pediatric vascular problems, alongside shifts in training paradigms that may impact the comfort levels of surgeons from both specialties, Coleman explains. There are “major educational gaps, and clinical gaps regarding what best practice can and should be,” she says. “And disappointingly, we continue to often extrapolate from adult vascular care.”
The session explores pediatric iatrogenic vascular injury, oncovascular reconstruction, rare cases of pediatric venous anomalies, and the nuances of pediatric dialysis care. For Coleman, overlap with other specialties in areas of pediatric vascular care underscores the need for vascular surgeons to step up. “At a local level, hospitals find the teams and build the teams that the kids need,” she says, “and I think vascular surgeons should be valued as critical assets and leaders on these teams.”
we need to get in groups together, either virtual or real, and actually listen to each other,” she says, highlighting a current problem of individuals “digging their trenches” instead of working collaboratively.
Looking ahead, Harris notes that she intends for unity to be a key theme of her future SVS presidency, which is due to commence in 2026.
Harris will be the second woman to assume the lofty role, which she hopes will soon become a moot accolade. “Obviously
“We need to encourage deliberate, intentional inclusivity and encourage people to learn their unconscious biases”
LINDA HARRIS
it’s an amazing honor,” Harris remarks, “but I want to get to a point where it’s not a unique honor because I’m a woman. It’s just an honor.”
The focus, Harris believes, must rest firmly on her skillset, and, in particular, her “ability to bring people together and to empower and to help to elevate those around [her].”
Fostering unity, Harris posits, will allow the specialty to deal with a multitude of current and future challenges. “There are so many things that we need to deal
with,” she comments, referencing artificial intelligence (AI), entrepreneurship and advocacy as just three of several key topics that the specialty “needs to work together on.”
Shaw assumes WVS presidency
Following the address, Harris passed the torch to Shaw, who she described as the “next great leader” and one she hopes will “surpass [her] success.” “I have every belief she will,” Harris remarked, “as will those who follow behind her.”
Shaw, professor of surgery at Upstate Medical University in Syracuse, New York, tells Vascular Specialist that her aim for the summit is to lead by Harris’ example, and continue to promote unity and collaboration. Specifically, she intends to do so on a global scale.
“What I bring to the table is the international component,” Shaw shares, highlighting her experience as president of the International Society of Endovascular Specialists (ISEVS), secretary general of the World Federation of Vascular Societies (WFVS) and—from September—Society for Vascular Surgery (SVS) U.S. representative to the European Society for Vascular Surgery (ESVS).
Shaw details that she intends to take the summit and ISWVS to the world stage via dedicated sessions at the Pan American Vascular Congress 2025, VEITHsymposium 2025 and Charing Cross (CX) International Symposium 2026. “I want to try to expand our international membership, and maybe set up international chapters,” Shaw notes, alongside “continuing to add to the fabric of everything that Linda has already developed.”
Dawn Coleman
Palma Shaw
Linda Harris
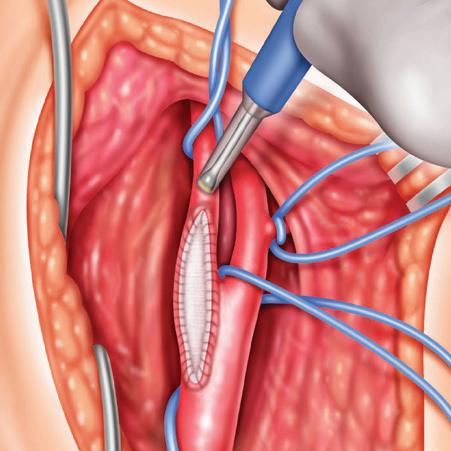
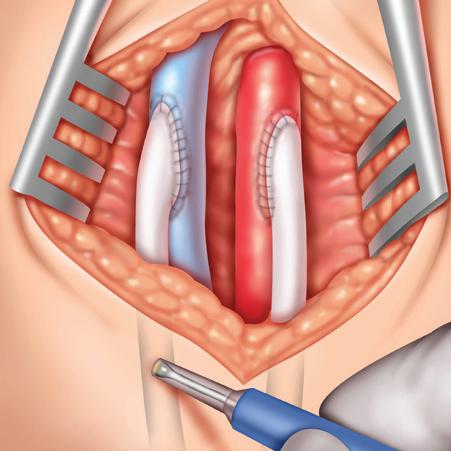
Advancing dialysis access outcomes with extravascular support: A triangulated clinical research approach
By C. Keith Ozaki, MD
Arteriovenous fistula (AVF) creation remains one of the most frequent, yet frustrating procedures performed by vascular surgeons. While AVFs stand as a cornerstone of care for end-stage kidney disease (ESKD) patients, the reality is more than half of AVFs fail to mature without additional interventions.1 The downstream impacts of maturation failure are prolonged central venous catheter (CVC) dependence, procedure fatigue for patients and families, financial penalties for dialysis centers, and increased cost to hospitals, payors, and patients. Over recent decades, multiple basic research teams including our own—recognized the complex interplay among physical hemodynamic forces, including circumferential wall strain, patient phenotype and vascular remodeling.
Building upon this science, the VasQ extravascular support device (Laminate Medical) was designed as a scaffold to guide AVF remodeling into an optimized configuration to produce a more laminar flow profile, while providing mechanical reinforcement against wall tension from excessive transluminal pressure that can lead to juxta-anastomotic stenosis. VasQ is the first to close this translational gap with a Food and Drug Administration (FDA)-approved product and the clinical research continues to support its adoption.
VasQ’s body of evidence includes 15 peer-reviewed publications to date, all reporting significant patient benefit, including a randomized-controlled trial in the United Kingdom.2 Our group actively participated in several of the U.S. initiatives, and here I provide a high-level overview of three recently published peer-reviewed U.S. studies, which converge to form a compelling, triangulated argument for VasQ’s safety, efficacy and impact in selected patients.
In summary, VasQ patients experienced higher functional success rates at earlier timepoints, as well as reduced intervention rates and reduced CVC exposure at six months when compared to traditional AVF patients.3-5 Each of these three studies fills a distinct and essential gap in our understanding of VasQ’s impact.
Pivotal study: A foundation of safety and efficacy3
Published in the Journal of Vascular Surgery, the U.S. pivotal study by Dillavou et al was a prospective, single-arm, 16-center trial that assessed AVFs created with VasQ in 144 patients. The results demonstrated:
• Excellent safety profile, with no device-related adverse events
• 88% functional success (two-needle cannulation) by a median of 56 days in dialysis patients compared to 72% and 81 days in the HFM study1
• 1.07 interventions/patient-year compared to the 1.8 reported for AVFs in the U.S.6
• 68.3% CVC removal by six months compared to 47.2% reported by the USRDS7
• 76.6% cumulative patency at 24 months compared to 53.7% from a recent meta-analysis8
• 0.7% aneurysms and 4.2% steal requiring revision at two years compared to 14% and 9% in literature 9
The U.S. pivotal study established that VasQ-supported AVFs can reliably achieve faster, more frequent functional success in the short term, with fewer complications over the longer term.
Matched claims analysis:
A broader US concept4
Despite its strengths, the pivotal study lacked a control group for direct comparison. To address this, Lucas et al conducted a matched comparative effectiveness study using Medicare claims data from the same surgeons and institutions that participated in the pivotal study. Key findings from the 144 VasQ patients vs. 782 matched controls included:
• Higher primary patency at six months (66% vs. 36%; odds ratio 3.27; p<0.0001)
• Reduced interventions (0.97 vs. 1.91 per patient-year; p<0.0001)
• Greater functional success at 90 days
(43.4% vs. 26.7%; p=0.005) and 180 days (72.5% vs. 53.7%; p=0.004)
• Lower CVC exposure at six months (31.3% vs 47.2%; p<0.001)
Although claims data lack granularity in AVF type or vessel diameter, the scale and rigor of this study provide powerful external validation of VasQ’s benefits in a real-world setting.
Retrospective vesselmatched analysis: Controlling for anatomy5
To complement the matched claims data and address its limitations, Hussain et al next applied the same pivotal study inclusion/ exclusion criteria in a retrospective chart review to generate a control with matched fistula type and vessel diameters from six of the pivotal study centers
In this direct, site-matched comparison (52 VasQ vs. 52 controls), they found:
Study Design
Pivotal study
Matched claims analysis
Retrospective vesselmatched analysis
Multicenter, singlearm, prospective with performance goal
Propensity-score matched claims comparator from the same pivotal study surgeons
Comparison between prospective pivotal patients to a historical control from high-enrolling sites using the study inclusion/ exclusion criteria
not only reinforce the Lucas et al claims study conclusion, but do so while addressing the anatomical and procedural variables that may impact successful AVF creation.
Implications for contemporary practice
Early functional success and reliable longterm accesses correlate with reduced CVC dwell times, fewer infections and lower mortality. The VasQ device addresses core mechanical and hemodynamic vulnerabilities that impede AVF maturation10 by enhancing functional success of one of our worst operations, and has the potential to minimize the need for additional procedures.
In an era that demands value-based care, VasQ not only delivers better clinical outcomes but has the potential to lower system costs by reducing reinterventions and comorbidities that occur with CVC dependence.
And, with the VasQ’s durable inflow reg-
• No device-related adverse events
• Primary endpoint met* (p=0.021)
• Two-year low risk of aneurysms with high cumulative patency
*Six-month primary patency against a literature-derived performance goal of 55%. #Functional success was defined as confirmed continuous use via two-needle cannulation for >30 days
• Shorter time to first use (56 vs. 85 days; p=0.04)
• Fewer interventions to support maturation (0.23 vs. 0.51 per patient; p=0.035)
• Higher unassisted functional success (Figure 2) at three months (46% vs. 23%; p=0.013) and six months (65% vs. 45%; p=0.03)
• Multivariate analysis identified VasQ implantation as the only factor significantly associated with improved success and reduced reintervention
Statistical significance was observed for unassisted functional success at three months (p=0.013) and six months (p=0.03). Statistical differences were not observed between any other functional status. These findings
We finally have a truly novel adjunct to our traditional hemodialysis
access creation
practices that moves us toward better outcome
ulation, one can speculate that the device may prevent long-term high flow driven complications (cephalic arch stenosis, steal, heart failure, arm edema, etc.).
We finally have a truly novel adjunct to our traditional hemodialysis access creation practices that moves us toward better outcomes, including AVFs that succeed more often, sooner, and with fewer interventions. Certainly, the VasQ device provides us with a real tool to move the hemodialysis access creation field truly toward “catheter last.”
References
1. Allon et al Am J Kidney Dis 2018 May; 71(5):677–689
2. Karydis et al Am J Kidney Dis 2020 Jan; 75(1):45-53
3. Dillavou et al J Vasc Surg. 2023; 78:1302-12
4. Lucas et al J Vasc Access (in press)
5. Hussain et al J Vasc Surg-VI (in press)
6. Yang et al J Vasc Access 2017;18 (Suppl. 2):8-14
7. Leake et al J Vasc Surg 2015; 62:123-7
8. Hajibandeh et al Vascular 2022; 20:1021-33
9. Arnaoutakis et al J Vasc Surg 2017; 66(5):1497-1503
10. Bozzetto et al J Vasc Access 2024; 25(1): 60–70
C. KEITH OZAKI is a vascular surgeon at Mass General Brigham, Harvard Medical School, in Boston.
VasQ device
SVS releases updated guidelines for intermittent claudication
By Marlén Gomez
The Society for Vascular Surgery (SVS) has issued a comprehensive update to its clinical practice guidelines for the management of intermittent claudication, urging clinicians to prioritize conservative treatment strategies and patient-centered care.
The new guidelines, published in April 2025, reflect the latest evidence on antithrombotic therapy, exercise interventions and revascularization procedures. They replace the SVS’s 2015 recommendations and aim to provide a more nuanced, evidence-based framework for treating patients with intermittent claudication.
“Intermittent claudication is a complex condition that affects millions of people worldwide,” said Michael S. Conte, MD, chair of the guideline writing group and professor of surgery at the University of California, San Francisco. “Our updated recommendations are designed to help clinicians tailor treatment to the individual patient, based on their symptoms, comorbidities, and personal goals.”
Conte will moderate a session at VAM 2025 on Friday, June 6 (2–3:30 p.m.) in the Morial Convention Center (Second Floor, Room 228–230) titled Translation of Clinical Guidelines to Practice: A Patient-Centered Approach to Management of Intermittent Claudication, which includes
Michael S. Conte Bernadette Aulivola
six talks, followed by discussion.
The guidelines reaffirm that firstline treatment for intermittent claudication should focus on education, smoking cessation, risk factor control, optimal medical therapy and structured exercise programs. Revascularization, whether surgical or endovascular, should be reserved for patients with lifestyle-limiting symptoms who do not respond to conservative therapy.
“Too often, patients are rushed into procedures without fully exploring non-invasive options,” said Bernadette Aulivola, MD, a vascular surgeon at Loyola University Chicago, and co-author of the guidelines. “We want to change that narrative.”
The updated guidelines include 12 formal recommendations and two best practice statements. Among them are:
• Dual pathway antithrombotic therapy—combining low-dose rivaroxaban (2.5 mg twice daily) with aspirin—is suggested for patients with intermittent claudication and highrisk comorbidities such as diabetes, heart failure or polyvascular disease, as well as for those who have undergone revascularization. This approach has been shown to reduce the risk of cardiovascular events, though it carries a modest increase in bleeding risk.
servative measures have failed. Shared decision-making is essential and should include a discussion of potential risks-including mortality, major adverse cardiovascular events and limb complications-as well as expected benefits such as improved mobility and quality of life.
• Infrapopliteal interventions are discouraged in patients with IC due to a lack of evidence supporting their benefit and concerns about potential harm.
• For femoropopliteal lesions longer than 5cm, the use of drug-coated balloons, drug-eluting stents or bare metal stents is recommended over plain balloon angioplasty to reduce the risk of restenosis and reintervention.
“Too often, patients are rushed into procedures without fully exploring noninvasive options”
BERNADETTE AULIVOLA
• Supervised exercise therapy (SET) is recommended as the gold standard for improving walking performance. Patients should walk at least three times per week for 12 weeks. For those unable or unwilling to participate in SET, structured home-based walking programs are recommended.
• Revascularization should only be considered after con-
VQI VASCULAR QUALITY INITIATIVE TO HOST ANNUAL MEETING AT VAM 2025
By Marlén Gomez
THE VASCULAR QUALITY
Initiative (VQI), in collaboration with the SVS, will convene its ninth annual conference (June 3–4) during VAM 2025 in the Morial Convention Center (Second Floor, R08–R09), bringing together healthcare professionals to advance the quality and safety of vascular care.
This two-day event will spotlight VQI’s latest achievements, including the expansion of its registry network, the launch of a new educational series, and enhancements to its data reporting platform. With more than 1,000 participating centers and more than one million vascular procedures recorded, the VQI continues to be a cornerstone of data-driven quality improvement in vascular health. According to the 2024 SVS VQI Annual Report, the initiative has
seen steady growth, now encompassing a diverse mix of academic institutions (26%), teaching hospitals (30%), and community hospitals (44%). Physician participation spans multiple specialties, with vascular surgeons making up 42% of contributors, followed by interventional cardiologists, radiologists and other specialists.
“The impact of VQI data on clinical practice and patient outcomes cannot be overstated,” said Jens Eldrup-Jorgensen, MD, the SVS Patient Safety Organization (PSO) medical director. “Our collaborative efforts have not only improved care delivery but also fostered global partnerships through the International Consortium of Vascular Registries [ICVR].”
This year’s conference introduces a number of updates:
The guideline development process included a panel of patient advisors, individuals with lived experience of PAD and claudication. Their input helped shape the recommendations and underscored the importance of clear communication, individualized treatment goals and transparency about the risks and benefits of various therapies. Patient advisors also called for the development of a “patient-friendly” version of the guidelines and expressed interest in peer support networks where individuals considering treatment could speak with others who have undergone similar procedures. Despite advances in pharmacotherapy and endovascular technology, the SVS identified several critical gaps in the evidence base. These include a lack of large-scale comparative effectiveness studies, limited data on long-term outcomes following revascularization and insufficient research on the optimal design of home-based exercise programs.
Ultimately, the updated guidelines aim to shift the focus from a one-size-fits-all approach to a more thoughtful, individualized model of care. Clinicians are encouraged to weigh the risks and benefits of each treatment option in the context of the patient’s overall health, preferences and life goals.
• Renaming of Participation Awards: The SVS VQI Participation Awards program, launched in 2016, has been renamed the Commitment to Vascular Quality Improvement Award to better reflect its mission of encouraging active engagement in quality initiatives.
• New VQI Centers: Northwestern Medicine Palos Hospital (Mid-America) and Our Lady of Lourdes Memorial Hospital, Inc. (Mid-Atlantic) have joined the VQI network.
• Smoking Cessation
Educational Series:
A 12-part monthly series that launched in January 2025 will provide comprehensive education on smoking cessation. Developed by Director of Quality Betsy Wymer, DNP, the series is open to physicians, nurses, advanced practice providers (APPs) and patients.
“Smoking cessation remains the most important task healthcare workers can offer their patients,” said Kendra Smith, RN. “This series is a powerful tool for change.”
On Tuesday, June 3, attendees will receive updates on the Fivos PATHWAYS platform, the secure, cloud-based system that powers VQI’s real-time data collection and long-term outcomes tracking. Enhancements include security toolkits to enhance the security posture of its systems.
Wednesday’s sessions will focus on the third National Quality Initiative (NQI), introduced in 2023, with a deep dive into the Smoking Cessation NQI. This underscores the VQI’s commitment to addressing modifiable risk factors and longterm outcomes.
“As the VQI continues to grow and evolve, its mission remains clear: to harness the power of data and collaboration to elevate vascular care. With new tools, expanded participation and a renewed focus on education and equity, the 2025 conference promises to be a pivotal moment in the journey toward better vascular health for all,” said EldrupJorgensen.
For more information, visit vqi.org.
Compiled by Marlén Gomez and Bryan Kay
The role of surgical robotics in vascular surgery
PROOF OF THE EMERGING purchase of robotics in the vascular surgery world might come in the form of a postgraduate education course taking place at VAM this year, according to Alan Lumsden, MD, one of the session moderators. For a number of years, Lumsden, medical director at Houston Methodist Hospital, Texas, has been exploring the question of whether the world of vascular surgery can return to the core therapeutic components of open surgery, unite them with the skillset brought by the endovascular revolution, and combine with a robotic surgery delivery system to create a third revolution in the space.
Alongside co-moderator Linda Le, MD, also a vascular surgeon at Houston Methodist, the session will hear from the likes of Samuel Money, from Oschner Health in New Orleans, and Charudatta Bavare, MD, who is at the vanguard of Houston Methodist’s Debakey Heart and Vascular Center efforts to build out its vascular robotics program. Titled Surgical Robotics in Vascular Disease: How We Can Play Catch Up!, it will also feature a debate between Lumsden and Frank Arko, MD, chief of vascular and endovascular surgery at Atrium Health, Sanger Heart and Vascular Institute, in Charlotte, North Carolina, over the specialty’s future and the role of robotic vascular surgery in it.
“It’s not going to be going away from the things we have learned, it’s how do we combine these things together, work with the smart people in the endovascular world to give us tools that can be delivered with the robot,” says Lumsden.
Vascular Live at VAM
BE SURE TO SAVE TIME FOR THE Vascular Live 25-minute presentations held during exhibit hours on Thursday and Friday of VAM 2025.
Exhibitors will be presenting new ideas, showcasing some of the cutting-edge research, breakthrough technologies and innovative products that are shaping vascular surgery.
All events take place at the Vascular Live stage in the Morial Convention Center (First Floor, Hall B). No registration is needed.
The stage will play host to 11 presentations from 10 companies. Vascular Live talks are not eligible for CME credit.
EXPERTS TAKE CENTER STAGE WITH VAM 2025 LECTURES
VAM 2025 IS SET TO SHOWCASE PIVOTAL advances alongside aspects of the past in the field of vascular surgery during a pair of distinguished lectures set to be delivered by two leading vascular voices.
On Thursday, June 5, at 9:30 a.m. Central Time, guests are invited to the Morial Convention Center’s First Floor, Great Hall A, where Sherene Shalhub, MD, will present the Roy Greenberg Distinguished Lecture on Innovation. Her talk, titled “The aortic vulnerability spectrum: Reshaping the future of aortic surgery,” promises to delve into groundbreaking concepts that could transform patient care and surgical approaches in aortic surgery.
Free professional headshots for attendees
VAM 2025 ATTENDEES ARE IN FOR a treat, as the event will feature a complimentary professional headshot service. The headshot booth will be on the Morial Convention Center, First Floor, Great Hall Pre-Function area near SVS Central.
The headshot station is open from 10 a.m.–2 p.m. on Thursday and Friday. The SVS encourages participants to enhance their professional image while attending the conference.
Following that, on Saturday, June 7, at 10:45 a.m. Central Time, attendees can look forward to a talk by Jerry Goldstone, MD, who will deliver the John Homans Lecture on the Second Floor, Room 208–210. His lecture—titled “Who put the vascular in vascular surgery?”—is expected to explore the critical contributions of vascular titans in evolution of vascular surgery.
Both lectures are part of a comprehensive program aimed at enhancing knowledge and sparking dialogue among vascular professionals, making VAM 2025 a pivotal gathering for those invested in the advancement of surgical practices and patient care in the vascular field.
SVS Central: Your VAM 2025 hub
MAKE SURE TO STOP BY SVS Central, a space outside the VAM 2025 exhibit hall that contains several facets of the Society for members to approach with inquiries. This year, the setup is located on the Morial Convention Center, First Floor, Great Hall PreFunction area. These SVS facets are found in SVS Central:
● SVS FOUNDATION: The philanthropic arm of the Society is stationary within the hub, where staff are prepared to answer any Foundation-centric questions, including the Step Challenge at VAM. Don’t forget to register for the Scavenger Hunt, an interactive twist to this year’s challenge featuring a step-powered scavenger hunt designed to get participants moving throughout the conference and host city. Register at vascular.org/STEPatVAM
● JOURNAL OF VASCULAR SURGERY ( JVS ): Back by popular demand, representatives at the JVS booth can answer questions regarding journal subscriptions and/or any of the five publications in the JVS portfolio.
● SVS MEMBERSHIP: Anyone looking to become an SVS member, pay their dues, check their membership status or inquire about membership benefits can connect with members of the membership team in SVS Central. If you are having trouble with your SVS account, the team members can assist. Be sure to stop by to grab SVS merchandise.
● SVS EDUCATION: The SVS education team is setting up shop in SVS Central to spread the word about new, returning and useful initiatives and products. Visit to learn about and register for the Complex Peripheral Vascular Interventions (CPVI) Skills Course, find out how to access frequently updated coding and reimbursement resources, and more. Learn more at vascular.org/ CPVI25 and vascular.org/Coding25
● SVS QUALITY PRACTICE: The quality practice team will be armed with copies of the OBL Handbook, which is available for purchase.
● SVS PAC: The SVS Political Action Committee (PAC) will be present in a lounge area. Knowledgeable individuals will be present and prepared to answer questions. Computers will be set up to take donations and register those interested in attending an inaugural advocacy conference, taking place Sept. 14–15 in Washington, D.C. Visit vascular.org/advocacyconference25
“We strongly encourage all attendees to take advantage of this free service,” said SVS President Matthew Eagleton. “Updating your portfolio with a fresh and professional headshot can make a big difference in how you present yourself to colleagues and potential employers.”
SVS Connect@VAM: Celebrate in New Orleans!
THE VASCULAR Quality Initiative (VQI), Society for Vascular Ultrasound (SVU), and Society for Vascular Nursing (SVN) invite all attendees to kick off VAM with an unforgettable evening at SVS Connect@VAM: Welcome to New Orleans!
The event will take place immediately after the 2025 edition of the Keynote Speaker Series on Wednesday, June 4. Enjoy handcrafted cocktails and savor traditional New Orleans cuisine while connecting with colleagues in a lively atmosphere. The celebration is scheduled for 5:45 p.m. on the Morial Convention Center First Floor, Great Hall Pre-Function area. Don’t miss out on this opportunity to network and unwind in true Big Easy style.
Accreditation information for VAM, VQI
THE SVS DESIGNATES VAM 2025 FOR a maximum of 25.75 AMA PRA Category 1 Credit(s)™ and 10.75 American Board of Surgery (ABS) Self-Assessment Continuing Medical Education (SA-CME) credits. Physicians should only claim the credit commensurate with the extent of their participation in the activity. The last day to claim CME credits for VAM 2025 is Monday, July 7.
The SVS designates the Vascular Quality Initiative (VQI) Annual Meeting for a maximum of 13.5 AMA PRA Category
1 Credit(s). VAM and the VQI will provide a Certificate of Participation/Attendance that nurses and physician assistants (PAs) can use towards their continuing education requirements.
Sherene Shalhub Jerry Goldstone
Why FLEX FIRST?
FLEX FIRST across Diverse Patient Populations for Positive Clinical Outcomes in Complex Lesions
FLEX FIRST AV Registry 6-month Primary Efficacy – TLPP ** FLEX + PTA*
Fistulas* (n=97) Cephalic Arch* (n=35)
Graft * (n=32)
0% Serious Adverse Events* (reported through 1 month) Scan to see Full AV Registry Results
AV Registry 6-month data. Data on file. **TLPP: Target Lesion Primary Patency. The FLEX Vessel Prep™ System is intended for use with percutaneous transluminal angioplasty (PTA) catheters to facilitate dilation of stenoses in the femoral and popliteal arteries and treatment of obstructive lesions of native or synthetic arteriovenous dialysis fistulas. Indications, contraindications, warnings, and instructions for use can be found in the product labeling supplied with each system. CAUTION: Federal law in USA
COMMENT& ANALYSIS
VENOUS DISEASE
Answering
the questions of appropriate outcome measures after intervention for deep reflux as promising venous valve technology emerges
By Fedor Lurie, MD
There is an old saying that goes, “As surgeons, we change the anatomy to improve physiology.” Correction of physiological abnormality should, then, result in clinical improvement. The assumptions behind such a three-step logic (anatomy-function-clinical outcome) are frequently challenged, modified and, sometimes, refuted when subjected to scientific examination. Recent developments in the field of chronic venous disease (CVD) make clear the need for such scientific examination of several ba sic assumptions, with one the role of reflux. Epidemiological studies and clinical ob servations consistently demonstrate that patients with primary CVD have either deep or superficial venous reflux, or both. Superficial reflux is relatively easy to treat. Multiple clinical trials have shown that ablation leads to clinical im -
LETTER TO THE EDITOR
provement. Deep reflux data are less convincing. The introduction of surgical repair for deep venous valves1 generated several observational studies showing excellent long-term functional and good clinical outcomes. 2 However, this operation requires the presence of a correctible valve, while most patients with deep reflux have valves damaged by the thrombotic process. Since valvuloplasty was universally performed in patients with terminal venous disease, consensus
statements and guidelines restricted recommendations for deep vein reconstruction to patients with venous ulcers.3,4 More than 50 years of clinical experience performing deep reflux correction still did not answer the question of its role in the progression of CVD and the degree to which such correction changes the natural history of this disease process.
There is a definite need for a practical solution for deep reflux correction. Correction in patients with both primary and secondary CVD—preferably in non-terminal stages of the disease—should answer this question and define the place for such a procedure in clinical practice. Fortunately, several devices are currently in pre-clinical and clinical stages of testing, and the hope is that some solutions will be available soon. However, the path from initial trials to meaningful clinical data will not be easy.
The path from initial trials to meaningful clinical data will not be easy
The first challenge is patient selection. Hemodynamics play an important role in the early stages of venous disease, but have minimal influence in advanced stages.5 The terminal stage is much more a chronic wound process, and correction of hemodynamic abnormalities, although beneficial, has a less clear benefit compared to earlier stages. Limiting the use of deep reflux correction to patients with venous ulcers will not answer the question of whether such a procedure can prevent disease progression. An
addition, safe lysis of chronic obstructive thrombus at a physiological level over a period of weeks would be a potentially transformative therapy. Such novel strategies would facilitate the management of chronic ischemia, not only in chronic limb-threatening ischemia (CLTI), but also in other vascular tissue beds (the heart, brain, lungs and kidneys, etc.).
Dear editor:
THE SEVERITY OF CHRONIC ISCHEMIA ARISING from progression of multi-level arterial occlusion is attenuated by neovascularization (NV). NV is effected by shear stress-induced growth of collateral arteries (arteriogenesis) and hypoxia-induced formation of new capillaries, arterioles and venules (angiogenesis). NV maintains blood flow until overwhelmed by arterial disease progression.
Chronic ischemia is also exacerbated by the thrombus that forms as the atherosclerotic plaque burden attenuates blood flow. Spontaneous recanalization of chronic thrombus by endogenous fibrinolysis is uncommon. Prolonged (>48 hours) intravascular infusion of potent fibrinolytic agents has variable benefit and carries a significant risk of hemorrhage.
Restoring NV by addressing specific obstacles that arise owing to progressive multi-level arterial occlusive disease offers the promise of a durable, safer and less expensive alternative to invasive revascularization. In
No matter how clever and refined our surgical/ interventional procedures have become, the emphasis needs to change if we are truly committed to achieving durable, low-risk, cost-effective solutions for our chronic ischemia patients.
The irony is that the pathway to successful NV is plain as can be. No vascular surgeon was involved in creating the 60,000 miles of vasculature present at birth. These vessels arose from just two cells at conception. Nor was vascular expertise needed to maintain perfusion during our subsequent growth. NV is clearly evident in wound healing. There is also ample evidence of collateral arterial growth during the early phases of vascular disease. Clearly, nature knows how to do this. Nature would continue to do it if the biological milieu remained favorable. Our achievable goal is to overcome the obstacles nature encounters, such as attenuation of the endothelial shear stress stimulus, the unhealthy biosynthetic environment in ischemic tissue, the progenitor cell deficit associated with vascular disease, and the presence of chronic thrombus.
additional challenge is choosing outcome measures that are related more to hemody namic correction than to other aspects of ulcer management. The only prospective randomized trial of deep venous valvu loplasty showed that patients with stable disease, or those that remained in the same clinical class for five years before surgery, do not benefit from deep valve repair, while those who progress to more severe disease have a significant clinical improvement. This suggests that it is reasonable to use reflux correction procedures in patients in early CVD stages who experience relatively fast progression.
Another challenge is to demonstrate the relationship between improvement in hemodynamics and clinical outcomes. Ex isting measures of venous hemodynamics and the severity of venous disease are far from perfect and likely to be inadequate for addressing this challenge. The current defi nition of reflux, although clinically useful, has no meaning in terms of physiological or fluid dynamics. Reverse flow in venous segments is frequently a normal event, even when all valves are competent. time of reversed flow depends on many factors outwith the presence or absence of valvular incompetence. The variability of reflux time measurements is so large that the same patient can be classified as having reflux if tested at different times by the same sonographer using the same procedures and equipment.
continued on page 14
The advantage of the surgical and interventional strategies vascular surgeons continue to employ and refine is that patients typically experience immediate benefit. However, the variable durability and escalating costs remain frustrating to patients and to healthcare systems. The financial rewards of delivering and refining these strategies exist because of the lack of an alternative approach. However, these rewards dissuade the development of an alternative approach. With all the advances in the biological and physical sciences in past decades, the time has come for the Society of Vascular Surgery (SVS) to prioritize a major push toward a more acceptable and durable approach to chronic ischemia, focused on tissue-level revascularization guided by restoration of nature’s innate NV and fibrinolytic capacity. A recent article I authored, published in the Journal of Vascular SurgeryVascular Insights in January, provides a 2025 summary of the mechanisms and cellular participants of NV and fibrinolysis. It also provides a path for further research based on clinical and proteomic data obtained from CLTI patients.
Sincerely,
Darwin Eton MD, FACS, DFSVS, Vasogenesis, Inc., Boston
WAKE UP! THIS IS THE 21ST CENTURY
How likely are your surgical patients to have disruptive bleeding?
COMMENT& ANALYSIS
CONTINUED FROM PAGE 12
ANSWERING THE QUESTIONS OF APPROPRIATE OUTCOMES MEASURES AFTER INTERVENTION FOR DEEP REFLUX AS PROMISING VENOUS VALVE TECHNOLOGY EMERGES
continued from page 12
flow are physiologically relevant remain unknown. Suggested candidates range from the volume of blood refluxing back, the flow rate, velocity, vein wall sheer stress and near-wall sheer rate, to a combination of all these measures. Even if the specific factor is defined, ultrasound-based measurements provide information only on one venous segment at a time. The impact of a single segmental reflux correction on the global hemodynamics of extremities is
more likely to be clinically relevant and important to assess. Unfortunately, the only existing test for assessing global hemodynamics is plethysmography.
The instruments that are used to assess CVD severity were developed by expert consensus (the Venous Clinical Severity Score, or VCSS) or even by a single person (the Villalta score). They reflect more on current perceptions of what constitutes more-or-less severe disease, rather than on scientifically based indicators of disease severity. The exception would be some of the patient-reported outcomes—such as VEINES-QOL—that were psychometrically constructed and tested for several aspects of validity.
Like the physiological questions about deep venous valves, the question of appropriate outcome measures of reflux correction is likely to be answered by future clinical experience with valve correction devices. As a community of practitioners managing patients with venous disease, we are at an exciting juncture—when many questions can be answered and the health of our patients can be improved. All we need is a solution that is practical and efficient.
Cost-effectiveness outcomes defy expectations in latest BEST-CLI data drop
By Jocelyn Hudson
The open surgical approach will prove to be “slightly superior” to endovascular intervention in terms of cost per life year gained, while the latter will be slightly superior to open surgery with regard to cost per quality-adjusted life year gained, pending results from a cost-effectiveness BEST-CLI analysis show.
The data, revealed during the 2025 Charing Cross (CX) International Symposium (April 23–25) in London, England, were part of a series of four podium-first presentations from the landmark BEST-CLI and BASIL-2 trials delivered at the meeting that aimed to add nuance to the ongoing conversation around the best treatment option for chronic limb-threatening ischemia (CLTI) patients. Sharing the main conclusion from new BEST-CLI cost-effectiveness data, Matthew Menard, MD, from Brigham and Women’s Hospital in Boston, told CX 2025: “I can tell you that, based on the data that we have— with the caveat that the final results are pending—we would predict that open will prove to be slightly superior to endo[vascular] with regard to cost per life year gained and that endo[vascular] will be slightly superior to open with regard to cost per quality-adjusted life year gained.”
Topline results from this trial were shared at the American Heart Association (AHA) scientific sessions in 2022, with investigators revealing that surgical bypass with adequate single-segment great saphenous vein is a more effective revascularization strategy for
patients with CLTI who are deemed suitable for either an open or endovascular approach. Both strategies were deemed safe and effective for CLTI treatment.
At CX, Menard added a further prediction that “given the small and statistically insignificant magnitude of the differences in the relevant inputs, it is very unlikely we will detect any meaningful cost-effectiveness difference,” noting that more granular data will be released later in the year. Andrew Holden, MD, from Auckland City Hospital, New Zealand, moderating, expressed surprise at the results.
“Before you shared these data,” he said, “I intuitively thought that endovascular, while not being successful overall, was going to be more cost-effective and I thought it would be driven by lower hospital stay and certainly lower intensive care stay, but you actually found the opposite, so I find that counterintuitive.”
References
1. Kistner RL. Surgical repair of the incompetent femoral vein valve. Arch Surg. 1975 Nov;110(11):1336–42
2. Masuda EM, Kistner RL. Long-term results of venous valve reconstruction: A four- to twenty-one-year follow-up. J Vasc Surg. 1994 Mar;19(3):391–403
3. Lurie F et al. Invasive treatment of deep venous disease. A UIP consensus. Int Angiol. 2010 Jun;29(3):199–204.
4. O’Donnell TF Jr et al. Management of venous leg ulcers: Clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. J Vasc Surg 2014 Aug;60(2 Suppl):3S–59S
5. Welkie JF et al. Hemodynamic deterioration in chronic venous disease. J Vasc Surg. 1992 Nov;16(5):733–40
6. Makarova NP, Lurie F, Hmelniker SM. Does surgical correction of the superficial femoral vein valve change the course of varicose disease? J Vasc Surg. 2001 Feb;33(2):361–8
7. Lurie F. Anatomical Extent of Venous Reflux. Cardiol Ther 2020 Dec;9(2):215–218
8. Lurie F et al. Multicenter assessment of venous reflux by duplex ultrasound. J Vasc Surg. 2012 Feb;55(2):437–45
FEDOR LURIE is an associate director of the JOBST Vascular Institute in Toldeo, Ohio.
when all of the costs that are associated with CLTI revascularization are assessed in aggregate over time. Hospital stay—almost always the key driver in cost-effectiveness analyses, he stressed—appears to be the “key metric” in their evaluation as well.
BASIL-2 trialist Matthew Popplewell, MD, from the University of Birmingham in Birmingham, England, noted that he was “quite relieved” on hearing the new findings. He explained that the length of stay in the BASIL-2 health economic analysis has been criticized for being “really long,” with the suggestion being that this could be due to a healthcare system issue. “Clearly it’s not, because it’s happening on both sides of the pond,” Popplewell commented.
Holden added that a “new lesson” to take from these cost-effectiveness data is that the driver of shorter hospital stay in these patients is perhaps not a less invasive procedure but, instead, making progress with wound healing to facilitate discharge.
Holden asked Menard whether he could explain the findings, to which Menard responded that “our goal was to undertake a very comprehensive analysis, in which all costs associated with the initial index procedure and hospitalization were captured, along with all of the costs of follow-up reinterventions, hospitalizations and rehabilitation care. The challenge is figuring out what’s relevant to the disease,” he said, adding that “this is how the data are looking”
Could primary endo ‘actually burn bridges’?
Subsequently, Alik Farber, MD, from Boston Medical Center in Boston, shared a new subset analysis from BEST-CLI. “We found that primary endo may actually burn bridges for secondary bypass,” the presenter concluded, noting that primary bypass was associated with “significantly better” outcomes. Farber went on to add that the BEST-CLI dataset is a “treasure trove for CLTI research” and will continue to add to a “badly needed evidence base.”
A question from the audience probed whether there are enough granular data available to know how a primary endovascular intervention “actually burns the bridge.” Farber responded: “There are many potential reasons as to how endovascular therapy may
burn bridges for a future bypass. It may occur due to disruption of vulnerable plaque, wire injury, compromise to collateral vessels, damage to run-off vessels, compromise of a bypass target, progression of tissue loss and concomitant loss of optimal window for intervention, or it could simply be a marker for a higher-risk patient or disease pattern. Which of these reasons are at play is not clear; however, our findings do show that the amputation rates are higher after secondary bypass.”
Here, Farber pointed to future research that might bring answers. He shared that the Novo Nordisk Foundation has provided a grant to the BEST-CLI team to fully unpack the BEST-CLI dataset. Menard added that the National Institutes of Health (NIH) has granted the BEST-CLI team permission to look more closely at the first major adverse limb event (MALE) data in the trial: “We have been able to obtain the source data and so will be able to look at the etiology of treatment failures. We are hopeful this will help us understand the important questions related to the need for reinterventions following an initial open or endovascular revascularization.”
Summarizing this part of the discussion, Holden remarked: “I think it’s fair to say that we are learning that endo may burn bridges, and I never used to like to hear that, but I think it is potentially true.”
“We would predict that open will prove to be slightly superior to endo with regard to cost per life year gained”
MATTHEW MENARD
Matthew Menard
Alik Farber
The Doppler Designed for the Modern OR
It’s the next generation of our Trans-Q-taneous Intraoperative (TQI) Doppler System, combining the reliability and cost effectiveness of the original TQI Doppler with new, user-friendly features.
RELIABLE
VTI’s single-use surgical Doppler probes provide a higher degree of performance reliability since probe failure due to reprocessing is eliminated. You’ll reach for your Doppler with confidence!
COST EFFECTIVE
Single-use surgical Doppler probes eliminate reprocessing costs as well as the hidden expenses associated with the malfunctioning of reusable probes such as lost OR time.
EASIER TO USE
Increased Portability
In addition to its smaller size, the TQI 2.0 Doppler now features an IV pole mount and a handle for easy transport.
Greater Control
The modern design of the TQI 2.0 Doppler allows for a foot pedal for increased control from the surgical field.
Improved Sound
The TQI 2.0 Doppler System is optimized for clear audio signals for both intraoperative and transcutaneous use.
Compiled by Marlén Gomez
SVS HIGHWAY TO HEALTH INFORMATIONAL SESSION
PROMOTES
VASCULAR
HEALTH AWARENESS
THE SOCIETY FOR VASCULAR SURGERY (SVS) held a virtual informational session to kick off its latest public awareness and education campaign on Wednesday, April 30. The initiative, Highway to Health, is aimed at promoting vascular health and highlighting the vital role of vascular surgeons in both the prevention and treatment of vascular diseases.
The session, which drew a significant audience, provided attendees with insights on campaign resources, which are available at no cost to all SVS members. Participants were encouraged to leverage these resources across social media platforms and within their institutions or practices. Key materials shared during the session included the Highway to Health member and patient toolkits, and the SVS Strong Vessel Score one-pager.
For those who missed the live broadcast, check your SVS emails for the link to the recorded session. The recording will allow individuals interested in learning about the Highway to Health: Fast Track Your Vessel Health campaign to catch up and discover what it takes to become a Highway to Health Ambassador.
Megan Marcinko, senior director of advocacy and public affairs at the SVS, can answer any
questions regarding the Highway to Health initiative or the Ambassador Program.
Search for new SVS PSO medical director ends
“This initiative promises to be a significant step in raising awareness about vascular health and strengthening community engagement in prevention and treatment efforts.
The SVS encourages all members to participate and help spread the message of vascular health,” said SVS President Matthew Eagleton.
Visit vascular.org/Your-Vascular-Health
“ This initiative promises to be a significant step in raising awareness about vascular health and strengthening community engagement”
MATTHEW EAGLETON
THE SOCIETY FOR VASCULAR SURGERY (SVS) WILL announce a new medical director for its Patient Safety Organization (PSO) during the 2025 Vascular Quality Initiative (VQI) Annual Meeting (June 3–4) in New Orleans. Jens Eldrup-Jorgensen, MD, who has served as medical director since 2017, will step down after a transition period.
The SVS PSO operates as part of the VQI, which includes 18 regional quality improvement groups and Fivos, its commercial technology partner. In 2025, the VQI and PSO will support more than 100 quality projects nationwide at hospitals and in vascular divisions. Since its inception, there have been over 900 peer-reviewed publications based on VQI data.
“Our membership has significantly increased in recent years. We now have almost 1,000 centers across the United States, Canada, and Singapore,” Eldrup-Jorgensen said. “Our focus is on quality improvement using a data-driven approach.”
Eldrup-Jorgensen was a founding member of the Vascular Study Group of New England, the oldest regional study group. He is also a professor of surgery at Tufts University School of Medicine in Boston.
“Participation in the VQI is voluntary and we need to continue to demonstrate the value of participation to ensure the sustainability and growth of the VQI,” Eldrup-Jorgensen said.
After stepping down, Eldrup-Jorgensen has an initial goal of catching more fish. However, his plans beyond that are still unclear. “I’m not ready to walk away completely. I’d like to stay engaged with quality improvement and the vascular community. I am particularly interested in enhancing care for underserved populations and addressing social disparities in healthcare,” he added
Jens EldrupJorgensen
The mission of this meeting is to provide the highest quality continuing medical education experience to all clinicians who care for patients with chronic wounds and from this, improve patient outcomes by maintaining focus on the most modern and effective management techniques
For more information about sponsorship, please contact: Jennifer Cheetham at Jennifer@wellassembled.com 503-545-2662
William Marston, MD Chief, Division of Vascular Surgery University of North Carolina at Chapell Hill Chapell Hill, NC
Robert McLafferty, MD, MBA Professor of Surgery, Division of Vascular Surgery Medical Director, Wound and Hyperbaric Center OHSU School of Medicine Portland, OR OUR VISION To be the leading continuing medical educational forum for all wound care specialists in the United States by providing regular rotating regional meetings that maintain an intimate and personal learning atmosphere.
What is this meeting about?
A true interdisciplinary approach to wound care with input from leading experts
A focus on treatments in/out of the wound care center that will heal wounds
Case-based studies that bring to light novel ways to treat patients
Proactive audience participation & interaction with national wound care experts
Emphasis on networking with social events that capitalize on that opportunity Better information sharing on how to better care for patients in wound centers
CLINICAL&DEVICENEWS
Compiled by Jocelyn Hudson and Bryan Kay
Reality check: Study brings ‘significant’ gap between randomized and real-world vascular patient populations into sharp focus
THE RANDOMIZED DATA FOUNDATION ON WHICH clinicians base decision-making for vascular surgery patients is derived from populations that do not represent the patients they see and treat on a day-to-day basis, a new research paper from the United Kingdom has found.
The review, recently published in BJS Open, involved a comparison of 307 randomized clinical trials including 66,449 patients and UK National Vascular Registry (NVR) data for 119,019 patients. Based on their results, authors Joseph Cutteridge, MD, from York and Scarborough Teaching Hospitals NHS Foundation Trust in York, England, and colleagues conclude: “There are significant differences in demographic and clinical factors between patients recruited to vascular surgery randomized clinical trials and the realworld [NVR] vascular surgery patient population.”
Specifically, the UK-based research team found that randomized clinical trial patients were younger across all operations and that, for carotid endarterectomy, bypass and major lower limb amputation trials, there were differences in female patient representation. The authors note that further comparisons were limited by the insufficient baseline data reporting across randomized clinical trials, and that there was no consistent reporting of ethnicity, body mass index (BMI) or alcohol consumption in the NVR.
Senior author Kasia Bera, MD, from the University of Oxford, England, notes that the importance of basing clinical decisions on the best available evidence, and specifically randomized clinical trials, is instilled in medical school.
Often, however, she notes that “the evidence doesn’t fit the patient in front of us,” highlighting a gap between the data on paper and the patients presenting in clinical practice.
“It is difficult to know if the evidence we have—and we have some really good evidence in vascular surgery—applies to our patients,” Bera says. “If I see someone in clinic who is diabetic, might be of Asian origin and might be female, I look at the trials, and there are just very few patients who are like this.”
Bera posits that the vascular surgery specialty “needs to do better” with regard to making research more representative of the population, which should in turn help clinicians to “make treatment more personalized.” Proposing some specific recommendations, Bera and colleagues suggest in BJS Open that minimum reporting standards for baseline data should be defined to allow future randomized clinical trials to represent “real-world” patient populations and ensure the external validity of their results.
“There’s a lot of power in a journal saying we’ll only publish your study if you adhere to minimal reporting standards,” she says.
In addition, Bera highlights the need for clinical units to be active in research. She comments that this is something currently done “pretty well” in the UK, before stressing the importance of “making sure everyone in the country has access to a research-active unit rather than having a few hubs.” The result, Bera suggests, would be that “no matter where you live, you have the option to participate in research, and that means the whole country is much better represented”.
“ There’s a lot of power in a journal saying we’ll only publish your study”
KASIA BERA
Bera shares that agreeing on these reporting standards is the “first step”—one that can realistically be achieved within the next year. The next is awareness, with Bera underlining the importance of ensuring support from funding bodies and journal editors.
Taking a step back, Bera is of the opinion that there is a need to look outside of vascular surgery for some “novel ideas” when it comes to improving randomized trial design. For example, she references the success of adaptive platform trials such as the RECOVERY trial conducted during the COVID-19 pandemic, as well as the concept of randomized, embedded, multifactorial adaptive platform (REMAP) trials that are being used in the critical care space.
“I think we should really learn from some of these methodologies and use them for our trials to make them even better in the future,” Bera suggests. “I think historically we didn’t have the computational power to do this sort of thing, whereas now we don’t have that excuse, so we should be able to have trials where the default would be for all patients who want to participate having the choice to do so.”
Bera also encourages a move away from the laser-focus on randomized clinical trials.
VQI ‘NOISE’ AUDIT’ UNCOVERS ‘SUBSTANTIAL VARIABILITY’ IN PERIPHERAL DEVICE SELECTIONS ACROSS 15 COMMON VASCULAR SCENARIOS
An audit of “noise”—or variability in expert judgments made by different decision-makers evaluating similarly poised cases—in the Vascular Quality Initiative (VQI) peripheral vascular intervention (PVI) registry identified “substantial variability” across a set of common vascular presentation scenarios.
The study showed that similar patients bearing similar pathologies received vastly different peripheral devices. The authors behind the audit, recently published in the Journal of Vascular Surgery (JVS), said the “tremendous amount of noise” in device selection they detected calls for “comparative effectiveness research to improve device selection and, ultimately, patient care.”
The research, led by senior author Daniel Bertges, MD, chief of the Division of Vascular Surgery and Endovascular Therapy at the University of Vermont Medical Center in Burlington, Vermont, involved the development of eight clinical- and seven lesion-based mock scenarios commonly seen in vascular
Endospan announces positive 30-day outcomes from TRIOMPHE IDE study
practice. The VQI was then queried for all procedures—covering both claudication and chronic limb-threatening ischemia patients—matching these descriptions from 2010–2021. Device selection was then identified for each procedure, the authors report, with a treatment hierarchy to designate the primary device class along with a separate accounting of specialty balloons. “Variability was then quantified in each mock patient scenario using the most commonly used device as the reference standard,” they explain.
The number of patients matching the criteria for each clinical-based scenario ranged from 223–1,379. The most commonly used device in a given scenario ranged from 32–72%. Variation in device selection was significant for all scenarios (p<0.0001), Bertges et al report. The use of special balloons ranged from 4%–53%, with variation in their use found to be significant for all scenarios (p<0.0001). Meanwhile, the number of patients matching the criteria for each lesion-based scenario ranged from 6,166–26,241, the
ENDOSPAN RECENTLY ANNOUNCED THE presentation of 30-day results from the statistical dissection primary arm of the TRIOMPHE investigational device exemption (IDE) clinical study. The data were presented during the late-breaking trial session at the American Association for Thoracic Surgery (AATS) annual meeting (May 2–5) in Seattle.
The TRIOMPHE study is a prospective, multicenter, three-arm trial designed to assess the safety and effectiveness of the Nexus aortic arch stent-graft system in patients with aortic arch pathologies (dissection, aneurysm, penetrating aortic ulcer [PAU]/intramural hematoma [IMH]).
It was reported during the session that the 30-day results from the TRIOMPHE study are promising for aortic arch treatment in zone 0 with the Nexus system.
Further, core lab analysis of stent-graft sealing shows no type Ia, no type Ib and no type III endoleaks, suggesting good sealing at 30 days.
“The 30-day data from the TRIOMPHE study are highly encouraging for the treatment of aortic arch disease,” said Brad Leshnower, MD, a cardiothoracic surgeon at Emory University School of Medicine in Atlanta, national cardiac principal investigator.
“The low stroke rate, in particular, is a significant achievement. This data is very promising while we await one-year follow-up of the study patients.”
“As a vascular surgeon, I am excited about the potential of the Nexus aortic arch stent-graft to provide a less invasive treatment option for patients with complex aortic arch pathologies,” added Ross Milner, MD, chair of vascular surgery at UChicago Medicine, national vascular principal investigator.
Daniel Bertges
authors note. The most commonly used device in a given scenario ranged from 34–67%. Variation in device selection was
“ The VQI should consider reporting the selection of device class for a limited set of common patient presentations and anatomies”
DANIEL BERTGES ET AL
VVT Medical welcomes Antonios Gasparis to medical advisory board
VVT MEDICAL RECENTLY ANNOUNCED THE appointment of Antonios Gasparis, MD, to its medical advisory board.
A press release notes that Gasparis brings more than two decades of expertise in vascular surgery, with a distinguished career dedicated to advancing the treatment of venous disease.
Gasparis currently serves as the system chief for the ambulatory vascular and vein program at Northwell Health in New York, where he is spearheading the development of a comprehensive venous disease program across the health system. He previously held prominent roles at Stony Brook University, New York, including professor of surgery, director of the Center for Vein Care, and director of the phlebology fellowship.
Gasparis’ leadership has extended to national platforms, having served as president of the American Venous Forum (AVF). He is also the founder and co-director of the Venous Symposium.
Imperative Care announces completion of enrollment in the SYMPHONY-PE study
IMPERATIVE CARE HAS ANNOUNCED THE COMPLETION OF PATIENT enrollment in its SYMPHONY-PE study, a pivotal investigational device exemption (IDE) trial evaluating the safety and efficacy of the company’s Symphony thrombectomy system for the treatment of acute pulmonary embolism (PE).
Designed to expand Symphony’s current indication for use to include PE, the study was conducted at 19 leading interventional radiology, interventional cardiology and vascular surgery centers across the U.S.
“While progress has been made in the treatment of pulmonary embolism, there is still a need for therapies that may offer improvements in safety, efficiency and long-term patient outcomes,” said interventional radiologist Vivian L. Bishay, from Mount Sinai Health System in New York City, and national co-principal investigator of the SYMPHONY-PE study. “This study represents a promising step forward in evaluating next-generation technology to expand treatment options for physicians and their patients.”
significant for all scenarios (p <0.0001). The use of special balloons ranged from 9–39%, with variation found to be significant for all scenarios (p<0.0001).
Discussing their findings, the authors note that when “experts render judgments in response to a similar clinical or procedural scenario, it can be reasonably expected that these decisions should be relatively similar.” While bias is “a known threat to this logic,” variation, or noise, in such decisions “has been shown to represent a far more significant impact on sound decision-making than previously realized.”
In the VQI, Bertges and colleagues show “a surprising amount of noise” in PVI device selection, with all of the mock scenarios—clinical- and lesion-based— demonstrating “significant variation.”
The authors conclude that “awareness, acknowledgement and understanding” of noise in device selection are the first steps toward addressing the wide variation.
“To this end, the VQI should consider reporting the selection of device class for a limited set of common patient presentations and anatomies,” they write in JVS. “The SVS [Society for Vascular Surgery] may consider expert review of the available randomized and observational data and publish lesion-specific recommendations for device selection.”
Three-year VenoValve first-inhuman trial data published
THE MANUSCRIPT behind the 36-month results for the new VenoValve device (enVVeno Medical)—“Three-year outcomes of surgical implantation of a novel bioprosthetic valve for the treatment of deep venous reflux”—has been published in the in the peer-reviewed journal, Annals of Vascular Surgery
The VenoValve was surgically implanted in the femoral vein of 11patients with active or healed venous ulcers (CEAP classifications C5–C6). Eight subjects completed threeyear follow-up, with key findings including a primary patency rate of 79% (Kaplan-Meier curve); a seven-point improvement in Venous Clinical Severity Score (VCSS); and an 84% reduction in pain on the Visual Analog Scale (VAS).
The VenoValve remained safe and effective, achieving target patency and maintaining competence and clinical benefits, the study found.
The VenoValve is a potential first-in-class, surgical replacement venous valve for patients with chronic venous insufficiency (CVI), according to enVVeno Medical.
A press release issued by the company states that it has submitted a premarket authorization (PMA) application for the device to the Food and Drug Administration (FDA), with a decision anticipated in the second half of 2025.
SAME SHOCK, BIGGER WAVES
Shockwave Medical is Now Part of J&J MedTech
As part of J&J MedTech, we’ll continue to deliver our same unmatched commitment to innovation, customer service and improving patient outcomes — with the added energy of the global leader in healthcare.